Embed Size (px)
Citation preview

The Reliability of Venous Duplex Ultrasound and Clinical Findings for the Diagnosis of Lower Extremity Deep Venous Thrombosis
Katie Adams, BSa, Shyam A. Sheth, DPMb, and Andrew J. Meyr, DPM FACFASc
aStudent, Temple University School of Podiatric Medicine, Philadelphia, PennsylvaniabResident, Temple University Hospital Podiatric Surgical Residency Program, Philadelphia, Pennsylvania
bAssociate Professor, Department of Podiatric Surgery, Temple University School of Podiatric Medicine, Philadelphia, Pennsylvania ([email protected])* *Please don’t hesitate to contact AJM with any questions/concerns. He’s happy to provide you with a .pdf of this poster if you email him.
1. Costantino TG, Goett HJ, et al. Chapter 17. Deep Venous Thrombosis. In: Ma O, Mateer JR, Reardon RF, Joing SA. eds. Ma and Mateer’s Emergency Ultrasound. McGraw-Hill Education, 2014.2. Black, CM. Anatomy and Physiology of the Lower-Extremity Deep and Superficial Veins. J. Tech Vasc Interv Radio, 17(2): 68-73, 2014. 3. Hunter, DW., Mortazavi S., Imaging Venous Disease: Pearls and Pitfalls. J. Tech Vasc Interv Radio, 17(2): 74-81, 2014. 4. Poppoto R, Papanicolaou G., et al. Limited B-mode Venous Imaging Versus Complete Color-Flow Duplex Venous Scanning for Detection of Proximal Deep Venous Thrombosis. J. Vasc Surg, 22(5): 553–557, 1995.5. Saragas, N., Ferrao, P., Saragas, E., & Jacobson, B. The Impact of Risk Assessment on the Implementation of Venous Thromboembolism Prophylaxis in Foot and Ankle Surgery. J. Foot and Ankle Surgery, 20 (2): 85–89, 2014.6. Shibuya N, Frost CH, Campbell JD, Davis ML, Jupiter DC. Incidence of Acute Deep Vein Thrombosis and Pulmonary Embolism in Foot and Ankle Trauma. J. Foot Ankle Surg, 51(1): 63-8, 2012.7. Sierzenski PR, Guhool j, Leech SJ. Chapter 24. Emergency Ultrasound. In: Knoop KJ, Stack LB, Storrow AB, Thurman R. eds. The Atlas of Emergency Medicine. McGraw-Hill Professional, 2013.8. Slaybaugh, R., Beasley, B., & Massa, E. Deep Venous Thrombosis Risk Assessment, Incidence, and Prophylaxis in Foot and Ankle Surgery. Clinics in Pod Medicine and Surgery, 20(2):269-89, 2003.9. Wells PS, Owen C, Doucette S, et al. Does This Patient Have a DVT? J. American Medical Assoc., 295(2):199-207, 2006.10. Zierler, B. Ultrasonography and Diagnosis of Venous Thromboembolism. J. Circulation, 109(14): 1-14, 2004.
DiscussionResults
ReferencesMethodology
Statement of Purpose and Literature Review The routine use of thromboprophylaxis in foot and ankle surgery has been a topic of contemporary debate. Shibuya et al recently reported a low overall incidence of deep vein thrombosis (DVT) and pulmonary embolism following foot and ankle trauma, but found older age, obesity and a higher injury severity score to be significant contributing risk factors. An ACFAS Clinical Consensus Statement found mixed evidence both for and against its routine use in most patient groups. Regardless of whether a foot and ankle surgeon believes that routine post-operative anticoagulation is necessary, a thrombotic event is a potential complication of any lower extremity surgical intervention and surgeons need to be intimately aware of its diagnosis. This topic has additional and specific relevance to the topic of diabetic foot disease as a lower extremity infection will often present with a red, hot, swollen extremity, similar to an acute thrombotic event. We have noticed at our institution a seeming preponderance of false positive clinical examinations resulting in the performance of venous duplex ultrasound (VDU) examination which end up being read as “negative.” The gold standard for the diagnosis of DVT was previously CT venography, but this has been replaced by venous duplex ultrasound (VDU) because it is noninvasive, sensitive, relatively inexpensive, and can be performed at a patient’s bedside. This test is typically administered by a certified vascular technician, and subsequently interpreted by either radiologists, vascular surgeons, or emergency medicine physicians. Zierler revealed the mean sensitivity and specificity of venous ultrasonography for the diagnosis of symptomatic DVT are 97% and 94%, respectively. However, the reliability of VDU is only as good as its interpretation in the presence or absence of a DVT. These are real-time images when performed by the technician, but is often interpreted by the physician based on static images.
The objectives of this investigation were to 1) examine the specificity of clinical findings for the diagnosis of DVT, and 2) examine agreement in the interpretation of VDU between multiple medical specialties.
First, a retrospective chart review was performed of 48 consecutive patients admitted to Temple University Hospital with a foot and ankle surgery consult who received a VDU during their admission. Clinical findings that prompted a VDU included: calf pain with compression, unilateral calf edema, erythema, and warmth. Specificity for these clinical findings as measured against VDU results was calculated. Second, agreement among different physicians who typically interpret VDU images were examined. The physicians were from multiple specialties and included 3 vascular surgeons (VS), 3 emergency medicine physicians (EM), and 1 radiologist. Four complete VDU imaging tests originally obtained for suspected DVT and used for the diagnosis were organized onto a computer program and independently reviewed by the nine physicians. The physicians were asked to review and interpret the VDU imaging test and note (1) whether the test was positive or negative for thrombosis, and if applicable, (2) the location of the thrombus.
The results of this investigation provide unique evidence to physicians with respect to the diagnosis of DVT and the interpretation of VDU:-First, it appears as though the typical clinical indications used for performance of VDU (pain, swelling, redness, warmth) demonstrate low specificity for the diagnosis of DVT. This highlights the potential for the development of an improved clinical diagnostic protocol that could be of value for physicians in order to decrease clinical false positives resulting in the performance of unnecessary VDUs. -Second, we found poor overall agreement in the interpretation of VDU among different physicians from different specialties who routinely interpret this test. We observed well below complete agreement in the interpretation of whether ultrasound images were positive or negative, including disagreement of the venous location of thrombus involved in positive tests. Our observed ICC of 0.292 is well below what be expected from a “gold standard” diagnostic test. We think this is interesting and indicates that VDU may lack the diagnostic accuracy to be considered a gold standard for the diagnosis of lower extremity DVT. We also think this finding highlights the importance of appreciating that VDU is a dynamic evaluation reliant on the clinical knowledge and technical skills of whoever is performing the test. Reviewing static imaging alone may not provide enough information to make the diagnosis consistently.
With respect to the retrospective case series:-Of the 48 consecutive identified cases, 5 (10.4%) were positive for DVT based on the VDU results. The documented clinical indications for performance of the test included calf pain with compression in 21 (43.8%) cases, edema in 20 (41.7%) cases, erythema in 23 (47.9%) cases, and warmth in 1 (2.1%) case. The clinical indication for performance of the test in the 5 positive VDUs was calf pain for each case.
With respect to the VDU interpretation portion of this investigation:-For the first case, 2 physicians diagnosed a positive examination (2 vascular surgeons) while 5 physicians diagnosed a negative examination. The two physicians who diagnosed a positive VDU identified thrombus in the peroneal vein (twice). -For the second case, 4 physicians diagnosed a positive examination (2 vascular surgeons, 2 emergency medicine physicians) while 3 physicians diagnosed a negative examination. The 4 physicians who diagnosed a positive examination located thrombus in the common femoral vein (four times). -For the third case, 4 physicians diagnosed a positive examination (2 vascular surgeons, 2 emergency medicine physicians) while 3 physicians diagnosed a negative examination. The 4 physicians who diagnosed a positive examination located thrombus in the peroneal vein (twice) and popliteal vein (twice). -For the fourth case, 6 physicians diagnosed a positive examination, while 1 physician (1 vascular surgeon) diagnosed a negative examination. The 6 physicians who diagnosed a positive examination identified thrombus in the common femoral vein (four times) and soleal vein (twice).-These findings resulted in an intraclass correlation coefficient (ICC) value of 0.292 indicating a “fair” degree of agreement. A “gold standard” diagnostic test would be expected to have an ICC ranging from 0.8-1.0.
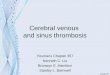
This image is representative of an ultrasound that would typically be read as “positive” for DVT. On the left, one can appreciate two distinct hypoechoic (dark) vessels which are the soleal artery and vein. On the right, the technician is compressing the soft tissue and both vessels are still visible. This indicates something is preventing the vein from being collapsed, namely thrombus.
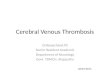
A more dynamic color Doppler can be performed to better visualize flow through the vessel if differentiation between artery and vein is difficult. One this image one can clearly visualize the relatively high flow artery located on top of the relatively low flow vein. Compression of the soft tissue may also be performed on this setting for evaluation of DVT.
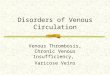
This image is representative of an ultrasound that would typically be read as “negative” for DVT. On the left, one can appreciate two distinct hypoechoic (dark) vessels which are the popliteal artery and vein. On the right, the technician is compressing the soft tissue which results in collapse of the vein (only one hypoechoic vessel is visualized) but the artery remains visible because of the muscular tunica media.
Table 1: Agreement among physicians for the diagnosis of venous duplex ultrasound (VDU).
Figure 1: Static ultrasound image of VDU of a right popliteal vein (POPV).
Figure 2: Color Doppler ultrasound image of VDU of a right common femoral vein (CFV).
Figure 3: Static ultrasound image of VDU of a left soleal vein.
Venous Duplex Ultrasound Cases
Vascular Surgeons
(n=3)
Emergency Medicine
Physicians (n=3)
Radiologist (n=1)
Summary Interpretation
(n=7)
Case 1 2 positive; 1 negative; (2x peroneal vein)
0 positive;3 negative
0 positive;1 negative
2 positive;5 negative;1 location
Case 2 2 positive; 1 negative;(2x common femoral vein)
2 positive;1 negative;(2x common femoral vein)
0 positive;1 negative
4 positive;3 negative;1 location
Case 3 2 positive;1 negative;(2x peroneal vein)
2 positive;1 negative;(2x popliteal vein)
0 positive; 1 negative
4 positive;3 negative;2 locations
Case 4 2 positive;1 negative;(1 x soleal vein; 1 x common femoral vein)
3 positive;0 negative;(3 x common femoral vein)
1 positive;0 negative;(1 x soleal vein)
6 positive;1 negative;2 locations