Embed Size (px)
Citation preview

The Renal Function

Anatomy
The kidneys are a pair of fist-sized organs that are located on either side of the spinal column.
A kidney consists of an outer layer (renal cortex) and an inner region (renal medulla).
The functional unit of the kidney is the nephron.
M. Zaharna Clin. Chem. 2009
2

Nephron
Structural and functional unit of the kidney
1 million nephrons per kidney Consists of 2 parts
1. Glomerulus (filtering system) tuft of capillaries surrounded by
Bowman’s capsule
2. Tubules
M. Zaharna Clin. Chem. 2009
3

Nephron
M. Zaharna Clin. Chem. 2009
4
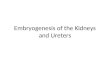
Renal artery
Glomerulus
Bowman’s capsule
Proximal tubule
Distal tubule
Collecting duct
Henle’s Loop
Afferent arteriole

Nephron - Bowman’s capsule
Bowman’s capsule: funnel with tubules as stem
Blood carried to glomerulus by afferent arteriole
Afferent arteriole divides to form capillary network.
These capillaries reunite to form efferent arteriole, which carries blood out of the glomerulus
M. Zaharna Clin. Chem. 2009
5

Nephron - Bowman’s capsule
Blood filtered in glomerulus; some water and small molecules removed Size cutoff value of approximately 66,000 Da,
about the molecular size of albumin. Glomerular filtrate collected in
Bowman’s capsule and enters tubules. Specific reabsorption occurs in tubules.
Most water and soluble nutrients reabsorbed
M. Zaharna Clin. Chem. 2009
6

Tubule System Proximal convoluted tubule
located in the cortex Reabsorption of Glucose,
water, amino acids, Na, Cl & others Loop of Henle
composed of the thin descending limb, which spans the medulla, and the ascending limb, which is located in both the medulla and the cortex,
More water reabsorbed Distal convoluted tubule
located in the cortex Sodium and hydrogen ion reabsorption
M. Zaharna Clin. Chem. 2009
7

Tubule System The collecting duct
formed by two or more distal convoluted tubules as they pass back down through the cortex and the medulla to collect the urine that drains from each nephron.
collecting tubules, then ureters → bladder → urethra
M. Zaharna Clin. Chem. 2009
8
1000 liter of blood through glomerulus per day; 100 liters of glomerular filtrate formed; 1 liter of urine produced

Functions of Kidney
Urine formation Regulate body fluid, osmolality and
volume Regulate electrolyte balance Regulate acid-base balance Excrete waste products and foreign
substances Produce and excrete hormones
M. Zaharna Clin. Chem. 2009
9

Urine Formation Removal of potentially toxic waste
products 3 processes involved
Filtration, Reabsorption, Secretion
M. Zaharna Clin. Chem. 2009
10
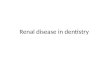
• Substance A is filtered and secreted, but not reabsorbed; • Substance B is filtered and a portion reabsorbed• Substance C is filtered and completely reabsorbed

Glomerular Filtration Glomerular filtration rate (GFR) is
approximately 130 mL/min Cells and large plasma proteins
unable to pass through the semipermeable membrane
Glomerular filtrate is essentially plasma without proteins.
water, electrolytes, glucose, amino acids, low-molecular-weight proteins, urea, and creatinine, pass freely through the basement membrane and enter the proximal convoluted tubule
M. Zaharna Clin. Chem. 2009
11

Proximal Convoluted Tubules
The next part of the nephron to receive filtrate
This filtrate contains waste products, and substances that are valuable to the body.
One function of the PCT is to return the bulk of each valuable substance back to the blood circulation. Glucose, water, amino acids, Na, Cl & others
Organic acids and bases, hydrogen ions and ammonia may be secreted into the tubular fluid
M. Zaharna Clin. Chem. 2009
12

Proximal Convoluted Tubules
Reabsorption may be active or passive Active — against a concentration
gradient (glucose, amino acids, low mw proteins, sodium, etc.) — regulated by kidney according to levels of
these substances in the blood Passive — no energy involved — water
and urea Tubular secretion may also be
passive or active M. Zaharna Clin. Chem. 2009
13

Loop of Henle Descending limb is highly permeable
to water Passive reabsorption of water in
descending loop Ascending loop is impermeable to
water but actively reabsorbs sodium and chloride
it lowers the salt concentration
M. Zaharna Clin. Chem. 2009
14

Distal Convoluted tubule
The function is to effect small adjustments to achieve electrolyte and acid-base homeostasis
Small amount of sodium, chloride, water are reabsorbed
Under influence of AVP (ADH) increase water permeability of tubule (reabsorbs water)
Potassium also reabsorbed or secreted Aldosterone - sodium reabsorption and
potassium secretion
M. Zaharna Clin. Chem. 2009
15

Collecting Duct The collecting ducts are the final
site for either: concentrating or diluting urine
Also under control of ADH & aldosterone Reabsorption of water, sodium and
chloride
M. Zaharna Clin. Chem. 2009
16

Regulation of Fluid and Electrolyte Balance Water:
body water (weight) remains constant day to day — ability of kidney to excrete or conserve water
Water balance is controlled by voluntary intake (thirst) and urinary loss
Sodium: freely filtered through the glomerulus and
reabsorbed by tubules Active reabsorption of Na+ results in passive
transport of Cl- and bicarbonate and passive reabsorption of water.
M. Zaharna Clin. Chem. 2009
17

Potassium: Both the distal convoluted tubule and the
collecting ducts can reabsorb and excrete potassium, and this excretion is controlled by aldosterone
Chloride: parallels sodium but reabsorption is passive in proximal tubules and active in distal tubules and collecting duct
M. Zaharna Clin. Chem. 2009
18
Regulation of Fluid and Electrolyte Balance

M. Zaharna Clin. Chem. 2009
19

Acid-Base Balance
Secretion of hydrogen ions from tubular cells Hydrogen ions generated in proximal and
distal tubules as a result of carbonic acid
H2O+CO2 → H2CO3 → H + HCO3-
React with bicarbonate ions React with buffers — phosphate ions React with ammonia (deamination of
gluatamine) to form ammonium ion Excretion as free hydrogen ions
M. Zaharna Clin. Chem. 2009
20

Nitrogenous Waste Excretion
When low GFR, levels of nitrogenous wastes increase in blood — NPN’s Urea Creatinine Uric Acid
M. Zaharna Clin. Chem. 2009
21

Primary Endocrine Functions
Kidneys synthesize renin, prostaglandins and erythropoietin
Renin: Renin is the initial member of the
renin-angiotensin-aldosterone system help regulate sodium and potassium in
the blood, fluid levels in the body, and blood pressure.
M. Zaharna Clin. Chem. 2009
22

Primary Endocrine Functions
Prostaglandins A group of potent cyclic fatty acids Behave like hormones Prostaglandins produced by the kidney
increase renal blood flow, sodium & water excretion
They oppose renal vasoconstriction due to angiotensin
M. Zaharna Clin. Chem. 2009
23

Primary Endocrine Functions
Erythropoietin It is a single chain polypeptide. It is produced by cells close to the proximal
tubules. Its production is regulated by blood oxygen
levels "hypoxia increases its production". Erythropoietin acts on the erythroid progenitor
cells in the bone marrow, causing their maturation and increasing the number of RBCs.
In chronic renal insufficiency, erythropoietin production is significantly reduced causing anemia.
M. Zaharna Clin. Chem. 2009
24

Secondary Endocrine Functions
The kidneys are the target locus for the action of aldosterone
For the catabolism of insulin, glucagon and aldosterone
The point of activation for vitamin D
M. Zaharna Clin. Chem. 2009
25

Renal Disorders
Acute Glomerulonephritis Nephrotic Syndrome Tubular Diseases Urinary Tract Infection Acute Renal Failure
M. Zaharna Clin. Chem. 2009
26

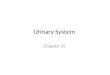
Acute Glomerulonephritis
Acute inflammation of the glomeruli Results in oliguria, hematuria,
increased BUN and serum creatinine, decreased GFR and hypertension
Red cell cast finding are of great importance
Proteinuria also present
M. Zaharna Clin. Chem. 2009
27Red cell cast

Nephrotic Syndrome Massive proteinuria, edema,
hypoalbuminemia, hyperlipidemia, and lipiduria
Has many cuases Characterized by increased
glomerular membrane permeability — loss of protein (greater than 2-3 grams per day)
M. Zaharna Clin. Chem. 2009
28

M. Zaharna Clin. Chem. 2009
29

Tubular Diseases Depressed secretion or reabsorption
of specific biochemicals Or Impairment of urine dilution and
concentration mechanisms Renal Tubular Acidosis — most
important Low values of phosphorus in serum,
and presence of glucose and amino acids in urine
M. Zaharna Clin. Chem. 2009
30

Urinary Tract Infection Bladder — cystitis Kidneys — pyelonephritis Bacterial concentrations
>100,000 colonies/mL is considered diagnostic for infection
Increased number of white blood cells
Increased number of red blood cells may be present
White blood cell casts is considered diagnostic of pyelonephritis
M. Zaharna Clin. Chem. 2009
31

Acute Renal Failure Defined as occurring when the GFR is
reduced to less than 10 mL/minute. Prerenal — before blood reaches the
kidney Hypovolemia Cardiovascular failure
Renal — occuring in kidney Acute tubular necrosis Glomerulonephritis
Postrenal — after urine leaves kidney Obstruction
M. Zaharna Clin. Chem. 2009
32

Usually accompanied by oliguria Associated with varying degrees of
proteinuria, hematuria, and presence of red cell casts and other casts
BUN and creatinine increase rapidly Can progress to chronic renal
insufficiency or failure
M. Zaharna Clin. Chem. 2009
33

M. Zaharna Clin. Chem. 2009
34

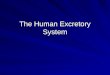
Renal Calculi Renal calculi, or
kidney stones, are formed by the combination of various crystallized substances. Of these, calcium oxalate stones are by far the most commonly encountered
M. Zaharna Clin. Chem. 2009
35

Renal Function Tests Tests of Glomerular Function
Creatinine Clearance Most sensitive method of assessing renal
function Tests of Tubular Function
Concentration — Dilution Studies Non-protein nitrogen compounds
Urea nitrogen Creatinine Uric acid
Urinalysis and Microscopy pH, Chemical Analyses (glucose, protein,
bilirubin/urobilinogen & others)M. Zaharna Clin. Chem. 2009
36

Renal Function Tests Cystatin C is a low-molecular-weight protein
produced by nucleated cells. It is freely filtered by the glomerulus, reabsorbed, and
catabolized by the proximal tubule. Produced at a constant rate, levels remain stable if
kidney function is normal. Plasma concentrations appear to be unaffected by
gender, race, age, and muscle mass. Studies have shown measurement of cystatin C to be
at least as useful as serum creatinine and creatinine clearance in detecting early changes in kidney function.
A rise in cystatin C is often detectible before there is a measureable decrease in GFR or increase in creatinine.
Cystatin C can be measured by immunoassay methods. M. Zaharna Clin. Chem. 2009
37

Renal Function Tests
β2-Microglobulin is a small, peptide found on the surface of
most nucleated cells levels of β2-M remain stable in normal
patients β2-M is easily filtered by the glomerulus.
About 99.9% is then reabsorbed by the proximal tubules and catabolized.
Measurement of serum β2-M is used clinically to assess renal tubular function in renal transplant patients, with elevated levels indicatingorgan rejection
M. Zaharna Clin. Chem. 2009
38

Microalbumin The term microalbuminuria describes small
amounts of albumin in urine Urine microalbumin measurement is important in
the management of patients with diabetes mellitus, who are at serious risk of developing nephropathy over their lifetimes
Increased glomerular capillary permeability. This permeability allows small (micro) amounts of albumin to pass into the urine.
If detected in this early phase, rigid glucose control, along with treatment to prevent hypertension, can be instituted and progression to end-stage renal disease (ESRD) prevented.
M. Zaharna Clin. Chem. 2009
39

Case Study
Jennie had a sore throat. She did not go to the doctor and recovered without medication.
However, a few weeks later Jennie was still listless and unwell.
She noticed that her urine was very dark and tinged red; she was also not producing much urine.
Jennie’s mother took her to their primary care physician.
M. Zaharna Clin. Chem. 2009
40

Test Result
Antistreptolysin-O (ASO) titer
Positive
Plasma creatinine Increased
Blood urea nitrogen Increased
Plasma sodium Increased
Creatinine clearance. Increased
Protein in urine Positive
Red blood cell casts Positive
M. Zaharna Clin. Chem. 2009
41

Comment As a consequence of Jennie’s streptococcal
infection, a portion of the functional units in Jennie’s kidney lost their ability to filter waste products from her blood.
The infection provoked an antibody response, which resulted in the formation of antigen-antibody complexes circulating in her blood, as indicated by her high ASO titer.
The complexes caused inflammation of the renal glomeruli, which resulted in reduction of the filtration capability of the glomeruli and, consequently, the reduction of the flow of waste products from blood to urine.
M. Zaharna Clin. Chem. 2009
42