Embed Size (px)
Citation preview

The research agenda for The research agenda for child health and nutrition: child health and nutrition:
Filling the gapsFilling the gaps
Igor Rudan, Shams El Arifeen and Robert E. BlackIgor Rudan, Shams El Arifeen and Robert E. Black
Child Health and Nutrition Research Initiative (CHNRI)
An initiative of the Global Forum for Health Research
www.chnri.org

Research agenda from the perspective of disease burden reduction:• Assessing the burden correctly

Research agenda from the perspective of disease burden reduction:• Assessing the burden correctly• Understanding the “architecture” of the
burden (identifying key risk factors and measuring exposures in the population)

Research agenda from the perspective of disease burden reduction:• Assessing the burden correctly• Understanding the “architecture” of the
burden (identifying key risk factors and measuring exposures in the population)
• Developing, evaluating and implementing interventions to reduce the burden

Research agenda from the perspective of disease burden reduction:• Assessing the burden correctly• Understanding the “architecture” of the
burden (identifying key risk factors and measuring exposures in the population)
• Developing, evaluating and implementing interventions to reduce the burden
• Setting priorities in future health research investments to reduce the burden systematically, fairly and cost-efficiently

I.
ASSESSING THE BURDEN CORRECTLY

WHO Child Health Epidemiology Reference Group (CHERG):
• Conducted systematic reviews to identify data from the period 1980-2000 on the major causes of morbidity and mortality in children under 5 years in countries with vital registration coverage <90%
• From more than 17,000 papers reviewed, only 308 studies (“information units”) considered likely to provide unbiased estimates of disease burden in a community

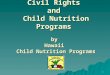
Geographical distribution of 308 studies

0
5
10
15
20
25
30
NU
MB
ER
OF
INF
OR
MA
TIO
N U
NIT
S
MEDIAN YEAR OF FIELD WORK
MAL-MB
MAL-MT
NEO-MT
ARI-MB
ARI-MT
DIA-MB
DIA-MT
Time trends in conducting the 308 studies

The information units are generally very scarce
They tend to cluster in 5 regions: • Northeastern Brazil• West Africa (especially in The Gambia)• East Africa (especially in Tanzania)• Egypt• Bangladesh, North India and Pakistan
(Geographic distribution highlights the role of International Research Centres)

• The level of research output on epidemiology of childhood pneumonia and diarrhoea has fallen sharply since the late 1980s
• This coincides with the development of highly cost-effective interventions to fight the two diseases
• However, 20 years later they still remain the two leading single causes of death in children under 5 years of age globally

Between 1980-2000, CHERG found no units of information in public domain in “gap” countries where 30% of all child deaths occur:
• Middle East and North Africa (Afghanistan, Iran, Iraq, Somalia, Sudan, Yemen) • Sub-Saharan Africa (Angola, Burkina Faso, Madagascar,
Mozambique, Niger, Uganda and Zambia)• Asian countries (China, Laos, Burma, Philippines and Vietnam)
Gaps?

II.
UNDERSTANDING THE “ARCHITECTURE” OF THE
BURDEN

Situation analysis in the population
RISK 1
RISK 3
RISK 2

Situation analysis in the population
RISK 1
RISK 3
RISK 2

Situation analysis in the population
INTERVENTION 1
RISK 1
RISK 3
INTERVENT. 2RISK 2

Understanding the prevalence of exposure to risk factors and intervention coverage globally is improving (e.g. MICS, DHS):
• Prevalence of risk exposures and intervention coverage now estimated for countries housing more than 90% of all under-fives
• The data still missing for a considerable number of countries (up to 20%, depending on the risk factor or intervention): the priorities are Somalia and Afghanistan
• The uncertainty around the estimates is unclear – the inter-country variation is often very large
Gaps?

III.
DEVELOPING AND IMPLEMENTING INTERVENTIONS

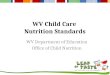
COMPONENTS OF DISEASE BURDEN
UNAVERTABLE
BOX 4
WITH EXISTING(RESEARCH ON NEW
INTERVENTIONS)
INTERVENTIONS
BOX 1:
BURDEN AVERTED WITH CURRENT MIX OF RISK AVOIDANCE AND
COVERAGE BY INTERVENTIONS
BOX 2:
AVERTABLE WITH BETTER DEPLOYMENT
OF EXISTING INTERVENTIONS
(RESEARCH ON HEALTH SYSTEMS AND
POLICY)
BOX 3:
AVERTABLE BY IMPROVING EXISTING
INTERVENTIONS
(RESEARCH TO REDUCE COST/ IMPROVE
DELIVERABILITY)
Impact of interventions on disease burden by instruments of health research (Box 2,3,4)

Promoting the value of health policy and systems research, and of the research on improving the existing interventions
• Health policy and systems research along with multidisciplinary research on original and more creative approaches to delivering interventions could substantially improve the coverage
• The research on improving the existing interventions could make them more deliverable, affordable and sustainable
Gaps?

IV.
SETTING PRIORITIES IN HEALTH RESEARCH
INVESTMENTS

Investing in health research
INVESTMENTS IN
HEALTH RESEARCH
PUBLICATION IMPACT
RESEARCH OPTION
ANSWERABLE?
NEW KNOWLEDGE

A concern:
Prioritization in research funding is partly driven by attractiveness, advocacy and potential for high publication impact
This favours research on new interventions (BOX 4), mainly basic research addressing very difficult upstream technology developments
COMPONENTS
DISEASE
OF
BURDEN
UNAVERTABLE
BOX 4
WITH EXISTING(RESEARCH ON NEW
INTERVENTIONS)
INTERVENTIONS
BOX 1:
BURDEN AVERTED WITH
CURRENT MIX OF RISK AVOIDANCE AND COVERAGE
BY INTERVENTIONS
BOX 2:
AVERTABLE WITH BETTER
DEPLOYMENT OF EXISTING
INTERVENTIONS
(RESEARCH ON HEALTH SYSTEM
AND POLICY)
BOX 3:
AVERTABLE BY IMPROVING EXISTING
INTERVENTIONS
(RESEARCH TO REDUCE COST/
IMPROVE DELIVERABILITY)

Funding
available for BOX 4 research grossly exceeds that on delivery, health policy and systems research
(BOX 2) or on improving the existing interventions (BOX 3)
COMPONENTS
DISEASE
OF
BURDEN
UNAVERTABLE
BOX 4
WITH EXISTING(RESEARCH ON NEW
INTERVENTIONS)
INTERVENTIONS
BOX 1:
BURDEN AVERTED WITH
CURRENT MIX OF RISK AVOIDANCE AND COVERAGE
BY INTERVENTIONS
BOX 2:
AVERTABLE WITH BETTER
DEPLOYMENT OF EXISTING
INTERVENTIONS
(RESEARCH ON HEALTH SYSTEM
AND POLICY)
BOX 3:
AVERTABLE BY IMPROVING EXISTING
INTERVENTIONS
(RESEARCH TO REDUCE COST/
IMPROVE DELIVERABILITY)

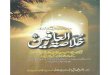
Redefining a “health research option”
INVESTMENTS IN
HEALTH RESEARCH
PUBLICATION IMPACT
RESEARCH OPTION
ANSWERABLE?
NEW KNOWLEDGE
EFFECTIVE?
IMPLEMENTATION
DELIVERABLE?
DISEASE BURDEN REDUCTION
MAX. POTENTIAL EQUITABLE?FOR DBR?

Development of priority setting methodology that should:
• take into account more dimensions relevant for priority setting than attractiveness, level of advocacy and potential publication impact
• be simple enough to gain wider acceptance
• be applicable at different levels and for different priority setting questions and problems
• be systematic, scientifically sound and repeatable
• be fair, transparent and legitimate
Gaps?

The proposed next steps by CHNRI* in developing and applying the new priority setting methodology
• Application in several different topics at the global level (major child diseases, conditions or risk factors), at the national level (in 1 developing country as a model), and within 1 major funding/donor agency
• Testing the application on health policy and systems research avenues (Box 2) across all major diseases / conditions
• Developing user-friendly tool (software) with appropriate user manual to enable child health research priority setting based on the proposed conceptual framework
Child Health and Nutrition Research Initiative of the Global Forum for Health Research; www.chnri.org

Credits:This presentation was compiled using substantial input from a
large number of individuals working for:
• Child Health Epidemiology Reference Group (CHERG)
• CHNRI Board and Secretariat, Dhaka, Bangladesh
• Joint Centre for Bioethics, University of Toronto, Canada
• The University of Phillipines (formerly COHRED)
• Disease Control Priorities Project II
• The World Bank
• Johns Hopkins Bloomberg School of Public Health, Baltimore, USA
• The University of Edinburgh, Scotland, UK