Embed Size (px)
Citation preview
The Role of High-Density Lipoprotein(HDL) Cholesterol in the Prevention andTreatment of Coronary Heart Disease:
Expert Group RecommendationsFrank M. Sacks, MD, for the Expert Group on HDL Cholesterol*
Population studies from all parts of the world haveconsistently reported that a low plasma level of
high-density lipoprotein (HDL) cholesterol is a strongpredictor of coronary heart disease (CHD).1,2 Multiplelines of evidence suggest that HDL has a direct ben-eficial effect on the arterial wall. Metabolically, HDLparticles induce the removal of cholesterol from cells,including those in atherosclerotic plaques.3 Apoli-poprotein A-I (apoA-I), the major protein in HDL,activates the mobilization of cholesterol ester stores inmacrophages, leading to the reduction of the choles-terol content of this major cell type in atherosclerosis.At least 2 specific receptors participate in mediatingthis protective effect. Intravenous infusion of HDL inrabbits prevents atherosclerosis,4 and the introductionand expression of the human apoA-I gene in micestimulates the regression of preexisting atherosclero-sis.5 HDL appears to deliver cholesterol to the liver forexcretion, and this function is termed, “reverse cho-lesterol transport.” HDL, in the form of recombinanthuman apoA-I liposomes, infused into hypercholes-terolemic humans, produced net cholesterol excretionfrom the body, directly demonstrating the stimulationof reverse cholesterol transport.6 HDL also has otherfunctions that may contribute to its ability to protectagainst CHD. Examples include anti-inflammatoryand antioxidant properties.7 Experiments demonstrat-ing the direct antiatherosclerotic potential of HDLstrongly support the findings from epidemiology andclinical trials, that the apparent clinical benefit ofraising HDL cholesterol is not secondary to its relationto other coronary risk factors, and justify renewedevaluation of HDL cholesterol as a target in the pre-vention and treatment of CHD.
Many patients with low levels of HDL cholesterolalso have high triglyceride levels, and elevated con-centrations of highly atherogenic triglyceride-rich li-poprotein remnants (derived from chylomicrons andvery low-density lipoproteins [VLDLs]). ThePROCAM study demonstrates the high risk associatedwith this particular lipid profile.2 Such patients mayhave predominantly abdominal obesity, and have a
high prevalence of insulin resistance, characterized byrelatively high levels of fasting glucose and insulin.Increased VLDL production and impaired VLDL li-polysis link a high triglyceride level with a low HDLcholesterol concentration. A high triglyceride concen-tration may indicate a high concentration of athero-genic chylomicron and VLDL remnants, and thesetriglyceride-rich remnants, which possess apolipopro-tein C-III, are associated with an increased risk forCHD.8 Insulin resistance causes increased VLDL pro-duction. This constellation of metabolically linkedfactors is often termed “the metabolic syndrome.”9
The relation between HDL cholesterol and theincidence of CHD is curvilinear and mirrors that of thecorresponding curve for LDL cholesterol as seen inthe Framingham Heart Study. Low HDL cholesterolpredicts CHD in both sexes (Figure 1), but thestrength of the relation may be greater in women thanin men.1 A meta-analysis of 4 large prospective epi-demiologic studies has defined the relation betweendifferences in HDL cholesterol and shifts in cardio-vascular risk. An increase in HDL cholesterol of 1mg/dl (0.026 mmol/L) is equated with an independentrelative risk reduction in the incidence of coronaryevents by 2% in men and 3% in women.1 In otherwords, depressed levels of HDL cholesterol heraldincreased risk for CHD at all levels of LDL choles-terol and triglycerides, in persons with diabetes and innondiabetics, in men and women, and in persons withand without known CHD.
The US National Health and Nutrition Examina-tion Survey III (1988 to 1991) shows that HDL cho-lesterol levels �40 mg/dl (�1 mmol/L) occur in about35% of adult men and 15% of adult women.10 How-ever, a higher percentage of men and women whodevelop CHD have HDL cholesterol �40 mg/dl. Inthe Framingham Heart Study, 57% of men who de-veloped CHD had an HDL cholesterol �40 mg/dl,11
and in the Cholesterol and Recurrent Events (CARE)trial, about 40% of the women who had had a myo-cardial infarction had HDL cholesterol �40 mg/dl.12
Statin treatment reduces coronary events in pa-tients whose HDL cholesterol concentrations arelow.13–15 Nonetheless, the strong relation betweenbaseline HDL cholesterol and subsequent event rateswas present in statin-treated patients in 513,14,16 of the6 large trials.13–16 For example, in the ScandinavianSimvastatin Survival Study (4S), and in the CAREand Long term Intervention with Pravastatin in Isch-
From the Harvard School of Public Health, Boston, Massachusetts.Manuscript received January 14, 2002; revised manuscript receivedand accepted March 14, 2002.
Address for reprints: Frank M. Sacks, MD, Harvard School ofPublic Health, 665 Huntington Ave, Boston, Massachusetts 02115.E-mail: [email protected].
*A list of participants appears in the Appendix.
139©2002 by Excerpta Medica, Inc. All rights reserved. 0002-9149/02/$–see front matterThe American Journal of Cardiology Vol. 90 July 15, 2002 PII S0002-9149(02)02436-0

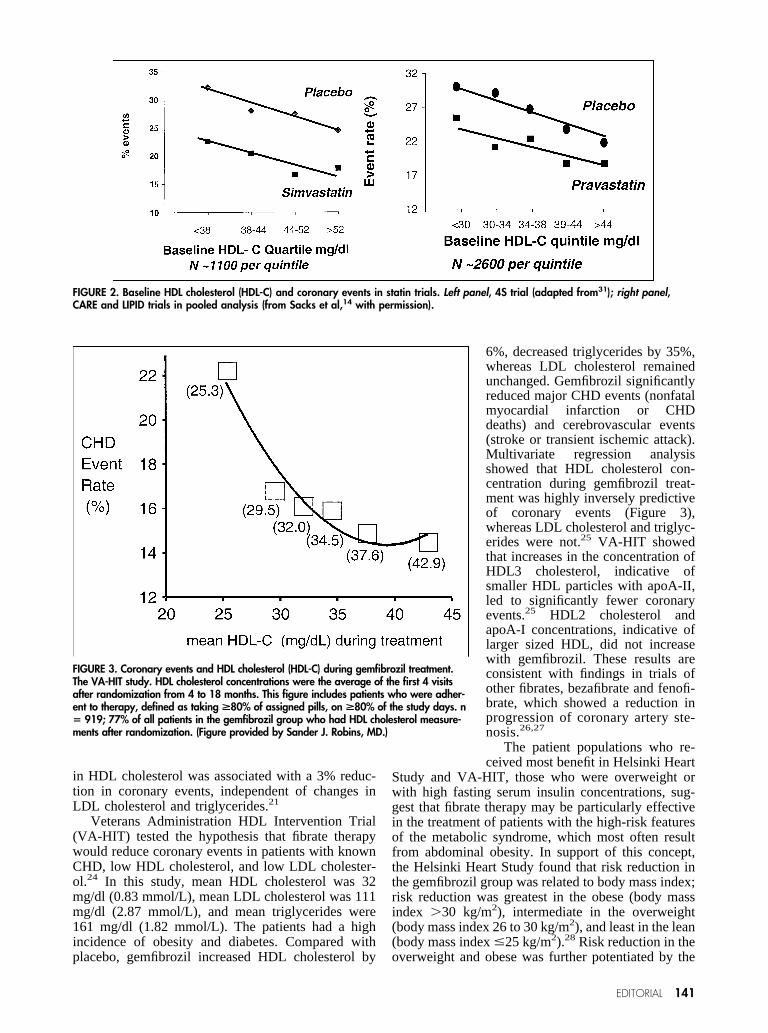
emic Disease (LIPID) trials, coronary event rates de-creased as baseline HDL cholesterol concentrationsincreased with a slope that was nearly identical in thestatin- and placebo-treated patients13,14 (Figure 2). Thus,although trials have consistently shown that statinsreduce coronary events in patients with low HDLcholesterol, those patients with low HDL cholesteroltaking statin therapy continue to have a greater riskthan those with higher HDL cholesterol.
Dietary excess, obesity, and physical inactivity allconspire to lower HDL cholesterol. Smoking causesdepressed HDL cholesterol levels and smoking cessa-tion is an important lifestyle modification in CHDprevention. Regular physical exercise, aerobic, suchas running or strength training, increases HDL cho-lesterol. The intensity of exercise that is practical formost persons modestly increases HDL cholesterol.Weight loss in overweight persons increases HDLcholesterol. Although low-fat, high-carbohydrate dietslower LDL cholesterol, they also lower HDL choles-terol and increase triglycerides.17 This may be partic-ularly important in patients with diabetes or the met-abolic syndrome. For this reason, experts often rec-ommend using unsaturated fats or oils to replacesaturated fat, because HDL cholesterol and triglycer-ide levels are preserved.17 A high fiber content atten-uates the hypertriglyceridemic but not the HDL-low-ering effect of carbohydrates. Regular intake of 1 to 2alcoholic beverages increases HDL cholesterol, and isassociated with reduced total and coronary mortality.However, the benefits of alcohol must be weighedagainst the problems of potential excess.
Lipid therapy with fibrates, nicotinic acid (niacin),or statins increases HDL cholesterol and decreasestriglycerides by mechanisms that are distinct from oneanother. Statins decrease the activity of plasma cho-lesterol ester transfer protein,18 which transfers cho-lesterol ester from HDL to VLDL; the implications ofthis action for atherosclerosis remain unclear. Moreclearly relevant to atherosclerosis, statins increaseapoA-I secretion into plasma in humans.19
It has been difficult to ascertain how much of anincrease in HDL contributes to the clinical benefit ofstatins. In the LIPID trial, which used pravastatin, a
decrease in LDL explained the pre-ponderance of coronary event re-duction, although increases in HDLcholesterol and apoA-I explained aminor reduction, but one that wasstatistically significant (11% to12%).16 The 4S trial, using simva-statin, found similar results.13 InCARE and West of Scotland Coro-nary Prevention Study (WOSCOPS),changes in HDL were not related toevent reduction. In the Air Force/Texas Coronary Atherosclerosis Pre-vention Study (AFCAPS/TEXCAPS)trial, which studied lovastatin, in-creases in apoA-I but not in HDLcholesterol were related to event re-duction.15
Fibrates activate peroxisome proliferator activatedreceptor alpha, a nuclear transcription protein thatproduces several related metabolic actions that stim-ulate reverse cholesterol transport.20 These actionsinclude increased HDL production by the liver, in-creased cholesterol removal from cholesterol-loadedmacrophages to HDL by the transporter ABC-A1 andthe receptor SRB-1, and increased cholesterol uptakefrom HDL to the liver, also by SRB-1. Fibrates raiseHDL by increasing the synthesis of apo A-I and A-IIby the liver.20 Fibrates accelerate lipolysis of triglyc-eride-rich lipoproteins, leading to the formation ofHDL from the association in plasma of the lipolysisproducts, apoA-I, apoA-II, phospholipids, and choles-terol. These multiple actions may help to explain whythe fibrate-induced increase in HDL cholesterol in theHelsinki Heart Study was more strongly related todecreased coronary events than HDL increases in tri-als with cholestyramine or statins. Each percent in-crease in HDL cholesterol with gemfibrozil was asso-ciated with a 3% reduction in coronary events,21 com-pared with a 1% reduction with simvastatin.13
Niacin is also known to significantly increase HDLcholesterol in a dose-dependent manner. Niacin raisesHDL cholesterol by decreasing catabolism of apoA-Iwithout increasing cholesterol transport from HDL tothe liver,22 leaving unanswered the question ofwhether reverse cholesterol transport is affected. Ni-acin does not increase HDL synthesis. However, HDLlevels during combination therapy with simvastatinand niacin were related to improvement in coronaryarterial stenosis and reduction in CHD.23
Both fibrates and niacin are effective in preventingCHD. In the Helsinki Heart Study, a primary preven-tion trial with gemfibrozil, a 9% increase in HDLcholesterol, with a 35% and 8% reduction of triglyc-erides and LDL cholesterol, respectively, resulted in a34% reduction of coronary events.21 Patients whoderived the greatest benefit were those who had lowHDL cholesterol (�42 mg/dl [1.08 mmol/L]) or hightriglycerides (�200 mg/dl [2.3 mmol/L]). Analysis ofthe lipid changes in the Helsinki Heart Study indicateda predominant role for the HDL raising effect of thedrug in preventing coronary events; every 1% increase
FIGURE 1. Coronary heart disease and HDL cholesterol (HDL-C) in men and women.The Framingham Heart Study. (Adapted from Gordon T et al.30)
140 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 90 JULY 15, 2002
in HDL cholesterol was associated with a 3% reduc-tion in coronary events, independent of changes inLDL cholesterol and triglycerides.21
Veterans Administration HDL Intervention Trial(VA-HIT) tested the hypothesis that fibrate therapywould reduce coronary events in patients with knownCHD, low HDL cholesterol, and low LDL cholester-ol.24 In this study, mean HDL cholesterol was 32mg/dl (0.83 mmol/L), mean LDL cholesterol was 111mg/dl (2.87 mmol/L), and mean triglycerides were161 mg/dl (1.82 mmol/L). The patients had a highincidence of obesity and diabetes. Compared withplacebo, gemfibrozil increased HDL cholesterol by
6%, decreased triglycerides by 35%,whereas LDL cholesterol remainedunchanged. Gemfibrozil significantlyreduced major CHD events (nonfatalmyocardial infarction or CHDdeaths) and cerebrovascular events(stroke or transient ischemic attack).Multivariate regression analysisshowed that HDL cholesterol con-centration during gemfibrozil treat-ment was highly inversely predictiveof coronary events (Figure 3),whereas LDL cholesterol and triglyc-erides were not.25 VA-HIT showedthat increases in the concentration ofHDL3 cholesterol, indicative ofsmaller HDL particles with apoA-II,led to significantly fewer coronaryevents.25 HDL2 cholesterol andapoA-I concentrations, indicative oflarger sized HDL, did not increasewith gemfibrozil. These results areconsistent with findings in trials ofother fibrates, bezafibrate and fenofi-brate, which showed a reduction inprogression of coronary artery ste-nosis.26,27
The patient populations who re-ceived most benefit in Helsinki Heart
Study and VA-HIT, those who were overweight orwith high fasting serum insulin concentrations, sug-gest that fibrate therapy may be particularly effectivein the treatment of patients with the high-risk featuresof the metabolic syndrome, which most often resultfrom abdominal obesity. In support of this concept,the Helsinki Heart Study found that risk reduction inthe gemfibrozil group was related to body mass index;risk reduction was greatest in the obese (body massindex �30 kg/m2), intermediate in the overweight(body mass index 26 to 30 kg/m2), and least in the lean(body mass index �25 kg/m2).28 Risk reduction in theoverweight and obese was further potentiated by the
FIGURE 2. Baseline HDL cholesterol (HDL-C) and coronary events in statin trials. Left panel, 4S trial (adapted from31); right panel,CARE and LIPID trials in pooled analysis (from Sacks et al,14 with permission).
FIGURE 3. Coronary events and HDL cholesterol (HDL-C) during gemfibrozil treatment.The VA-HIT study. HDL cholesterol concentrations were the average of the first 4 visitsafter randomization from 4 to 18 months. This figure includes patients who were adher-ent to therapy, defined as taking >80% of assigned pills, on >80% of the study days. n� 919; 77% of all patients in the gemfibrozil group who had HDL cholesterol measure-ments after randomization. (Figure provided by Sander J. Robins, MD.)
EDITORIAL 141
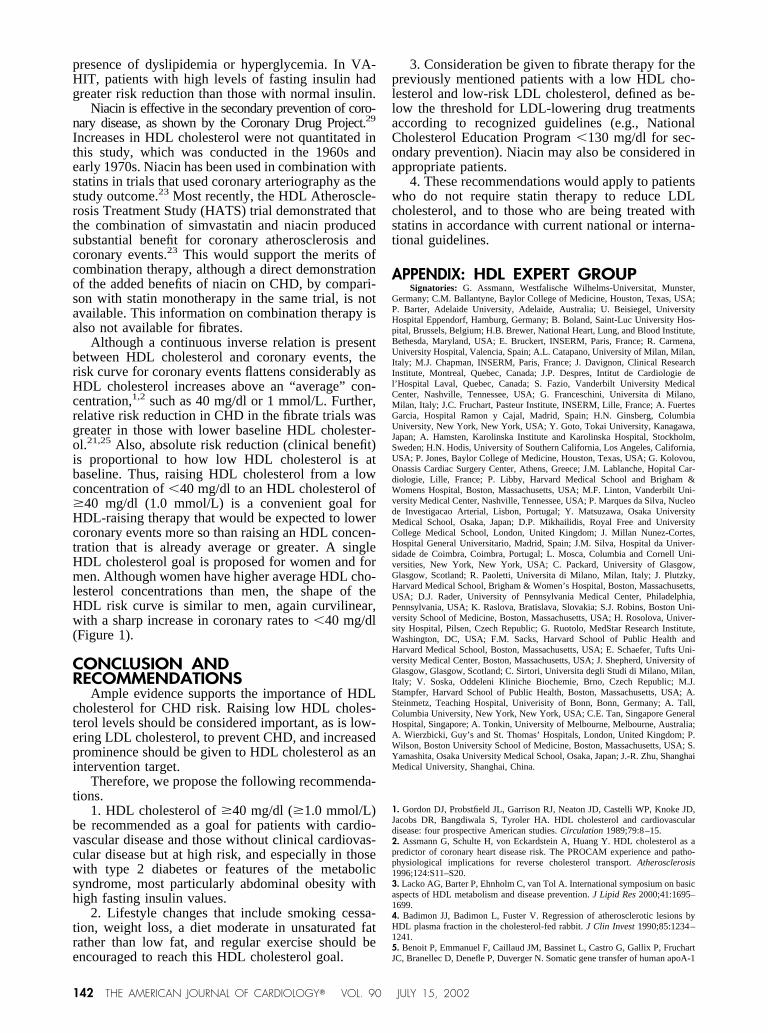
presence of dyslipidemia or hyperglycemia. In VA-HIT, patients with high levels of fasting insulin hadgreater risk reduction than those with normal insulin.
Niacin is effective in the secondary prevention of coro-nary disease, as shown by the Coronary Drug Project.29
Increases in HDL cholesterol were not quantitated inthis study, which was conducted in the 1960s andearly 1970s. Niacin has been used in combination withstatins in trials that used coronary arteriography as thestudy outcome.23 Most recently, the HDL Atheroscle-rosis Treatment Study (HATS) trial demonstrated thatthe combination of simvastatin and niacin producedsubstantial benefit for coronary atherosclerosis andcoronary events.23 This would support the merits ofcombination therapy, although a direct demonstrationof the added benefits of niacin on CHD, by compari-son with statin monotherapy in the same trial, is notavailable. This information on combination therapy isalso not available for fibrates.
Although a continuous inverse relation is presentbetween HDL cholesterol and coronary events, therisk curve for coronary events flattens considerably asHDL cholesterol increases above an “average” con-centration,1,2 such as 40 mg/dl or 1 mmol/L. Further,relative risk reduction in CHD in the fibrate trials wasgreater in those with lower baseline HDL cholester-ol.21,25 Also, absolute risk reduction (clinical benefit)is proportional to how low HDL cholesterol is atbaseline. Thus, raising HDL cholesterol from a lowconcentration of �40 mg/dl to an HDL cholesterol of�40 mg/dl (1.0 mmol/L) is a convenient goal forHDL-raising therapy that would be expected to lowercoronary events more so than raising an HDL concen-tration that is already average or greater. A singleHDL cholesterol goal is proposed for women and formen. Although women have higher average HDL cho-lesterol concentrations than men, the shape of theHDL risk curve is similar to men, again curvilinear,with a sharp increase in coronary rates to �40 mg/dl(Figure 1).
CONCLUSION ANDRECOMMENDATIONS
Ample evidence supports the importance of HDLcholesterol for CHD risk. Raising low HDL choles-terol levels should be considered important, as is low-ering LDL cholesterol, to prevent CHD, and increasedprominence should be given to HDL cholesterol as anintervention target.
Therefore, we propose the following recommenda-tions.
1. HDL cholesterol of �40 mg/dl (�1.0 mmol/L)be recommended as a goal for patients with cardio-vascular disease and those without clinical cardiovas-cular disease but at high risk, and especially in thosewith type 2 diabetes or features of the metabolicsyndrome, most particularly abdominal obesity withhigh fasting insulin values.
2. Lifestyle changes that include smoking cessa-tion, weight loss, a diet moderate in unsaturated fatrather than low fat, and regular exercise should beencouraged to reach this HDL cholesterol goal.
3. Consideration be given to fibrate therapy for thepreviously mentioned patients with a low HDL cho-lesterol and low-risk LDL cholesterol, defined as be-low the threshold for LDL-lowering drug treatmentsaccording to recognized guidelines (e.g., NationalCholesterol Education Program �130 mg/dl for sec-ondary prevention). Niacin may also be considered inappropriate patients.
4. These recommendations would apply to patientswho do not require statin therapy to reduce LDLcholesterol, and to those who are being treated withstatins in accordance with current national or interna-tional guidelines.
APPENDIX: HDL EXPERT GROUPSignatories: G. Assmann, Westfalische Wilhelms-Universitat, Munster,
Germany; C.M. Ballantyne, Baylor College of Medicine, Houston, Texas, USA;P. Barter, Adelaide University, Adelaide, Australia; U. Beisiegel, UniversityHospital Eppendorf, Hamburg, Germany; B. Boland, Saint-Luc University Hos-pital, Brussels, Belgium; H.B. Brewer, National Heart, Lung, and Blood Institute,Bethesda, Maryland, USA; E. Bruckert, INSERM, Paris, France; R. Carmena,University Hospital, Valencia, Spain; A.L. Catapano, University of Milan, Milan,Italy; M.J. Chapman, INSERM, Paris, France; J. Davignon, Clinical ResearchInstitute, Montreal, Quebec, Canada; J.P. Despres, Intitut de Cardiologie del’Hospital Laval, Quebec, Canada; S. Fazio, Vanderbilt University MedicalCenter, Nashville, Tennessee, USA; G. Franceschini, Universita di Milano,Milan, Italy; J.C. Fruchart, Pasteur Institute, INSERM, Lille, France; A. FuertesGarcia, Hospital Ramon y Cajal, Madrid, Spain; H.N. Ginsberg, ColumbiaUniversity, New York, New York, USA; Y. Goto, Tokai University, Kanagawa,Japan; A. Hamsten, Karolinska Institute and Karolinska Hospital, Stockholm,Sweden; H.N. Hodis, University of Southern California, Los Angeles, California,USA; P. Jones, Baylor College of Medicine, Houston, Texas, USA; G. Kolovou,Onassis Cardiac Surgery Center, Athens, Greece; J.M. Lablanche, Hopital Car-diologie, Lille, France; P. Libby, Harvard Medical School and Brigham &Womens Hospital, Boston, Massachusetts, USA; M.F. Linton, Vanderbilt Uni-versity Medical Center, Nashville, Tennessee, USA; P. Marques da Silva, Nucleode Investigacao Arterial, Lisbon, Portugal; Y. Matsuzawa, Osaka UniversityMedical School, Osaka, Japan; D.P. Mikhailidis, Royal Free and UniversityCollege Medical School, London, United Kingdom; J. Millan Nunez-Cortes,Hospital General Universitario, Madrid, Spain; J.M. Silva, Hospital da Univer-sidade de Coimbra, Coimbra, Portugal; L. Mosca, Columbia and Cornell Uni-versities, New York, New York, USA; C. Packard, University of Glasgow,Glasgow, Scotland; R. Paoletti, Universita di Milano, Milan, Italy; J. Plutzky,Harvard Medical School, Brigham & Women’s Hospital, Boston, Massachusetts,USA; D.J. Rader, University of Pennsylvania Medical Center, Philadelphia,Pennsylvania, USA; K. Raslova, Bratislava, Slovakia; S.J. Robins, Boston Uni-versity School of Medicine, Boston, Massachusetts, USA; H. Rosolova, Univer-sity Hospital, Pilsen, Czech Republic; G. Ruotolo, MedStar Research Institute,Washington, DC, USA; F.M. Sacks, Harvard School of Public Health andHarvard Medical School, Boston, Massachusetts, USA; E. Schaefer, Tufts Uni-versity Medical Center, Boston, Massachusetts, USA; J. Shepherd, University ofGlasgow, Glasgow, Scotland; C. Sirtori, Universita degli Studi di Milano, Milan,Italy; V. Soska, Oddeleni Kliniche Biochemie, Brno, Czech Republic; M.J.Stampfer, Harvard School of Public Health, Boston, Massachusetts, USA; A.Steinmetz, Teaching Hospital, Univerisity of Bonn, Bonn, Germany; A. Tall,Columbia University, New York, New York, USA; C.E. Tan, Singapore GeneralHospital, Singapore; A. Tonkin, University of Melbourne, Melbourne, Australia;A. Wierzbicki, Guy’s and St. Thomas’ Hospitals, London, United Kingdom; P.Wilson, Boston University School of Medicine, Boston, Massachusetts, USA; S.Yamashita, Osaka University Medical School, Osaka, Japan; J.-R. Zhu, ShanghaiMedical University, Shanghai, China.
1. Gordon DJ, Probstfield JL, Garrison RJ, Neaton JD, Castelli WP, Knoke JD,Jacobs DR, Bangdiwala S, Tyroler HA. HDL cholesterol and cardiovasculardisease: four prospective American studies. Circulation 1989;79:8–15.2. Assmann G, Schulte H, von Eckardstein A, Huang Y. HDL cholesterol as apredictor of coronary heart disease risk. The PROCAM experience and patho-physiological implications for reverse cholesterol transport. Atherosclerosis1996;124:S11–S20.3. Lacko AG, Barter P, Ehnholm C, van Tol A. International symposium on basicaspects of HDL metabolism and disease prevention. J Lipid Res 2000;41:1695–1699.4. Badimon JJ, Badimon L, Fuster V. Regression of atherosclerotic lesions byHDL plasma fraction in the cholesterol-fed rabbit. J Clin Invest 1990;85:1234–1241.5. Benoit P, Emmanuel F, Caillaud JM, Bassinet L, Castro G, Gallix P, FruchartJC, Branellec D, Denefle P, Duverger N. Somatic gene transfer of human apoA-1
142 THE AMERICAN JOURNAL OF CARDIOLOGY� VOL. 90 JULY 15, 2002

inhibits atherosclerosis progression in mouse models. Circulation 1999;99:105–110.6. Eriksson M, Carlson LA, Miettinen TA, Angelin B. Stimulation of fecal steroidexcretion after infusion of recombinant proapolipoprotein A-I. Potential reversecholesterol transport in humans. Circulation 1999;100:594–598.7. Navab M, Hama SY, Cooke CJ, Anantharamaiah GM, Chaddha M, Lin L,Subbanagounder G, Faull KF, Reddy ST, Miller NE, Fogelman AM. NormalHDL inhibits three steps in the formation of mildly oxidzied LDL. J Lipid Res2000;41:1481–1508.8. Sacks FM, Alaupovic P, Moye LA, Cole TG, Sussex B, Stampfer MJ, PfefferMA, Braunwald E. Very low density lipoproteins, apolipoproteins B, CIII, and Eand risk of recurrent coronary events in the Cholesterol and Recurrent Events(CARE) Trial. Circulation 2000;102:1886–1892.9. Grundy SM. Hypertriglyceridemia, insulin resistance, and the metabolic syn-drome. Am J Cardiol 1999;83(suppl):25F–29F.10. Johnson CL, Rifkind BM, Sempos CT, Carroll MD, Bachorik PS, Briefel RR,Gordon DJ, Burt VL, Brown CD, Lippel K. Declining serum total cholesterollevels amoung US adults: the National Health and Nutrition Examination Sur-veys. JAMA 1993;269:3002–3008.11. Kannel WB. Range of serum cholesterol in the population developingcoronary artery disease. Am J Cardiol 1995;76(suppl):69C–77C.12. Lewis SJ, Sacks FM, Mitchell JS, East C, Glasser S, Kell S, Letterer R,Limacher M, Moye LA, Rouleau JL, Pfeffer MA, Braunwald E. Effect ofpravastatin on cardiovascular events in women after myocardial infarction: theCholesterol and Recurrent Events trial. J Am Coll Cardiol 1998;32:140–146.13. Pedersen TR, Olsson AG, Faergeman O, Kjekshus J, Wedel H, Berg K,Wilhelmsen L, Haghfelt T, Thorgeirsson G, Pyorala K, et al. Lipoprotein changesand reduction in the incidence of major coronary events in the ScandinavianSimvastatin Survival Study. Circulation 1998;97:1453–1460.14. Sacks FM, Tonkin AM, Shepherd J, Braunwald E, Cobbe S, Hawkins CM,Keech A, Packard C, Simes J, Byington R, Furberg CD, for the The ProspectivePravastatin Pooling Project Investigators Group. The effect of pravastatin oncoronary disease events in subgroups defined by coronary risk factors. Circula-tion 2000;102:1893–1900.15. Gotto AM, Whitney E, Stein EA, Shapiro DR, Clearfield M, Weis S, Jou JY,Langendorfer A, Beere PA, Watson DJ, Downs JR, de Cani JS. Relation betweenbaseline and on treatment parameters and first acute major coronary events in theAir Force/Texas Coronary Atherosclerosis Prevention Study. Circulation 2000;101:477–484.16. Simes RJ, Marschner IC, Hunt D, Colquhoun D, Sullivan D, Stewart RA,Hague W, Keech A, Thompson P, White H, Shaw J, Tonkin A. Relationshipbetween lipid levels and clinical outcomes in the Long-Term Intervention withPravastatin in Ischemic Disease (LIPID) Trial. Circulation 2002;105:1162–1169.17. Garg A. High monounsaturated fat diets for patients with diabetes mellitus:a meta-analysis. Am J Clin Nutr 1998;67(suppl 3):577S–582S.18. Guerin M, Dolphin PJ, Talussot C, Gardette J, Berthezene F, Chapman MJ.
Pravastatin modulates cholesteryl ester transfer from HDL to apoB-containinglipoproteins and lipoprotein subspecies profile in familial hypercholesterolemia.Arterioscler Thromb Vasc Biol 1995;15:1359–1368.19. Schaefer JR, Schweer H, Ikewaki K, Stracke H, Seyberth HF, Kaffarkik H,Maisch B, Steinmetz A. Metabolic basis of HDL and apolipoprotein A-I increaseby HMG CoA reductase inhibition in healthy subjects and a patient with coronaryartery disease. Atherosclerosis 1999;144:177–184.20. Fruchart JC, Staels B, Duriez P. The role of fibric acids in atherosclerosis.Curr Atheroscler Rep 2001;3:83–92.21. Manninen V, Elo O, Frick H, Haapa K, Heinonen OP, Heinsalmi P, Helo P,Huttunen JK, Kaitaniemi P, Koskinen P, et al. Lipid alterations and decline in theincidence of coronary heart disease in the Helsinki Heart Study. JAMA 1988;260:641–651.22. Kamanna VS, Kashyap ML. Mechanism of action of niacin on lipoproteinmetabolism. Curr Atheroscler Rep 2000;2:36–46.23. Brown BG, Zhao X-Q, Chait A, Fisher LD, Cheung MC, Morse JS, DowdyAA, Marino EK, Bolson EL, Alaupovic P, Frohlich J, Albers JJ. Simvastatin andniacin, antioxidant vitamins, or the combination for the prevention of coronarydisease. N Engl J Med 2001;345:1583–1592.24. Rubins HB, Robins SJ, Collins D, Fye CL, Anderson FW, Elam MB, FaasFH, Linares E, Schaefer EJ, Schectman G, Wilt TJ, Wittes J. Gemfibrozil for thesecondary prevention of coronary heart disease in men with low HDL-choles-terol. N Engl J Med 1999;341:410–418.25. Robins SJ, Collins D, Wittes JT, Papademetriou V, Deedwania PC, SchaeferEJ, McNamara JR, Kashyap ML, Hershman JM, Wexler LF, Rubins HB. Rela-tion of gemfibrozil treatment and lipid levels with major coronary events. JAMA2001;285:1585–1591.26. Ericsson CG, Hamsten A, Nilsson J, Grip L, Svane B, de Faire U. Angio-graphic assessment of effects of bezafibrate on progression of coronary arterydisease in young male postinfarction patients. Lancet 1996;347:849–853.27. Diabetes Atherosclerosis Intervention Study Investigators. Effect of fenofi-brate on progression of conary artery disease in type 2 diabetes: the DiabetesAtherosclerosis Intervention Study, a randomised study. Lancet 2001;357:905–910.28. Tenkanen L, Manttari M, Manninen V. Some coronary risk factors related tothe insulin resistance syndrome and treatment with gemfibrozil. Experience fromthe Helsinki Heart Study. Circulation 1995;92:1779–1785.29. Coronary Drug Project Research Group. Clofibrate and niacin in coronaryheart disease. JAMA 1975;231:360–381.30. Gordon T, Castelli WP, Hjortland MC, Kannel WB, Dawber TR. Highdensity lipoprotein as a protective factor against coronary heart disease: TheFramingham Study. Am J Med 1977;62:707–714.31. Scandinavian Simvastatin Survival Study Group. Baseline serum cholesteroland treatment effect in the Scandinavian Simvastatin Survival Study (4S). Lancet1995;345:1274–1275.
EDITORIAL 143