Embed Size (px)
Citation preview
170
ORIGINAL ARTICLE
Acta Medica Indonesiana - The Indonesian Journal of Internal Medicine
The Role of Neutrophyl Lymphocyte Count Ratio as an Inflammatory Marker in Systemic Lupus Erythematosus
Amaylia Oehadian, Hendarsyah Suryadinata, Sumartini Dewi, Riardi Pramudyo, Bachti AlisjahbanaDepartment of Internal Medicine, Padjadjaran University - Hasan Sadikin Hospital, Bandung, Indonesia.
Correspondence mail:Division of Hematology and Medical Oncology Padjadjaran University - Hasan Sadikin Hospital. Jl. Pasteur 38, Bandung 40161, Indonesia. email: [email protected].
ABSTRAKTujuan: menilai rasio hitung netrofil limfosit atau neutrophyl lymphocyte count ratio (NLCR) sebagai
petanda inflamasi lupus eritomatosus sistemik (LES). Metode: penelitian ini merupakan penelitian potong lintang dengan 21 pasien LES derajat ringan dan sedang menurut skor Mex SLEDAI serta 30 subyek normal. Penghitungan sel darah putih dilakukan dengan menggunakan Sysmex XE- 5000. Hitung netrofil absolut dan hitung limfosit absolut ditabulasi dan dibandingkan dengan menggunakan uji t tidak berpasangan. Perbandingan NLCR antara pasien LES dan subyek normal dihitung menggunakan uji Mann-Whitney. Penelitian ini dilakukan di Departemen Ilmu Penyakit Dalam, Rumah Sakit Hasan Sadikin sejak bulan November 2011 hingga Januari 2012. Hasil: tidak ada perbedaan bermakna antara hitung netrofil absolut pasien SLE dan subyek normal (4158+1517 vs 4031+1218 /mm3, p=0,74). Hitung limfosit absolut secara bermakna lebih rendah pada pasien LES dari pada subyek normal (1721+600 vs 2397+587/mm3, p=0,000). Nilai rasio hitung netrofil limfosit (NLCR) lebih tinggi secara bermakna pada pasien LES daripada subyek normal (2,52 (1,01-10,92) vs 1,65 (0,77-4,59), p=0,007). Tidak ada perbedaan bermakna pada NLCR pasien LES derajat ringan dan derajat sedang (2,59 (1,01-10,92) vs 2,01 (1,38-3,98), p= 0,412). Berdasarkan kurva ROC, dengan AUC 0,727, dan titik potong NLCR >1,93, maka didapatkan sensitivitas 70% dan spesifisitas 67% dalam membedakan pasien LES dengan subyek normal. Kesimpulan: NLCR dapat dipakai sebagai parameter inflamasi sederhana pada LES.
Kata kunci: rasio hitung netrofil limfosit (NLCR), lupus eritematosus sistemik (LES), petanda inflamasi.
ABSTRACTAim: to evaluate neutrophyl lymphocyte count ratio (NLCR) as an inflammatory marker in systemic lupus
erythematosus (SLE). Methods: this was a cross sectional study involving 21 SLE patients with mild and moderate disease activity according to Mex SLEDAI score and 30 normal subjects. White blood cells counts were examined with Sysmex XE-5000. The absolute neutrophyl count and absolute lymphocyte count were tabulated and compared between SLE and normal subjects using unpaired t-test. The comparison of NLCR between SLE and normal subject was calculated using Mann-Whitney test. This study was conducted in the Department of Internal Medicine Hasan Sadikin Hospital from November 2011 until January 2012. Results: there was no significant difference in absolute neutrophyl count between SLE and normal subjects (4158+1517 vs 4031+1218 /mm3, p=0.74). The absolute lymphocyte count was significantly lower in SLE than normal subjects (1721+600 vs 2397+587/mm3, p=0.000). NLCR was significantly higher in SLE than normal subjects (2.52 (1.01-10.92) vs 1.65 (0.77-4.59), p=0.007). There was no significant difference in NLCR between SLE with mild and moderate activity (2.59 (1.01-10.92) vs 2.01 (1.38-3.98), p= 0.412). Based on ROC curve, with

Vol 45 • Number 3 • July 2013 Neutrophyl lymphocyte count ratio as an inflmmatory marker in SLE
171
INTRODUCTIONSystemic lupus erythematosus (SLE) is a
chronic autoimmune inflammatory disease with unknown etiology which has diverse clinical manifestation, course of illness and prognosis. The assessment of SLE patiens is therefore difficult for the physician in daily practice. On the other hand, treatment could be diferrent according to disease activity.1-3 SLE can be categorized as mild or severe and life threatening disease. In severe activity, leukopenia and lymphopenia can be found.2
Many clinical and laboratory parameters can be used to evaluate disease activity. The laboratory parameters of disease activity are low complement, increased deoxyribonucleotide (DNA) binding, thrombocytopenia and leukopenia. The problem is how to evaluate disease activity with simple laboratory parameters which is available in almost every health care facility. White blood cell and differential count can be done as part of routine automated hematology analyzer. Recently, neutrophyl lymphocyte count ratio (NLCR) has been evaluated and used as inflammatory marker in malignancies, infection and coronary artery diseases. In infectious disease, NLCR is better predictors of bacteriemia than C reactive protein (CRP) level, white blood cell and neutrophyl count. The use of NLCR as inflammatory marker may be simple and readily available biomarkers.4 Diagnostic performance of NLCR has not been studied in SLE. We assumed that NLCR could be used to characterize inflammatory response in SLE and determine decision of treatment in the future.
This study was conducted to investigate NLCR as a novel inflamatory marker in SLE patients with mild and moderate activity according to the Mex SLEDAI score.
METHODS
SubjectsThis was a cross sectional study conducted
at the Department of Internal Medicine Hasan Sadikin Hospital from November 2011 until January 2012. Twenty one SLE patients with mild and moderate disease activity according to Mex SLEDAI score and 30 normal subjects were evaluated. White blood cells and differential counts were examined with Sysmex XE-5000. The inclusion criteria were SLE patients (according to American Colleague of Rheumatology 1997 criteria), mild and moderate disease acitivity (according to Mex SLEDAI score). Disease activity was categorized as mild (Mex SLEDAI score <2) and moderate (Mex SLEDAI score 2-12). The exclusion criteria were subjects with infection, severe disease activity, treatment with cyclophosphamide in the last 28 days, azathioprine or methotrexate. For comparison we examined the hematology parameter of healthy subjects consisted of medical doctors and laboratory analysts.
Statistical AnalysisThe absolute neutrophyl count and absolute
lymphocyte count data were normally distributed. The difference of absolute neutrophyl count and absolute lymphocyte count between SLE patients and normal subjects were compared with unpaired t-test. The NLCR data was not normally distributed. Comparison of NLCR between SLE and normal subject was calculated using Mann-Withney test. We considered a value of p<0.05 as significant. To evaluate the discrimination value of NLCR for SLE and normal subject, we evaluated the area under the curve (AUC) using receiver operating curve (ROC). Data analyses were performed by using SPSS 17.0.
AUC 0.727, cut off NLCR value >1.93 had 70% sensitivity and 67% specificity in differentiating between SLE and normal subjects. Conclusion: NLCR could be used as simple inflammatory parameter in SLE.
Key words: neutrophyl lymphocyte count ratio (NLCR), systemic lupus erythematosus (SLE), inflammatory marker.
Amaylia Oehadian Acta Med Indones-Indones J Intern Med
172
RESULTS
Clinical CharacteristicsThere were 21 SLE patients (all females)
and 30 normal subjects (10 males, 20 females). There was no significant difference in median age between the 2 groups (Table 1).
The SLE patients consisted of 9 (42.8%) patients with mild activity and 12 (57.2%) patients with moderate activity (Table 1).
White Blood Cells ParameterThe white blood cells parameter can be seen
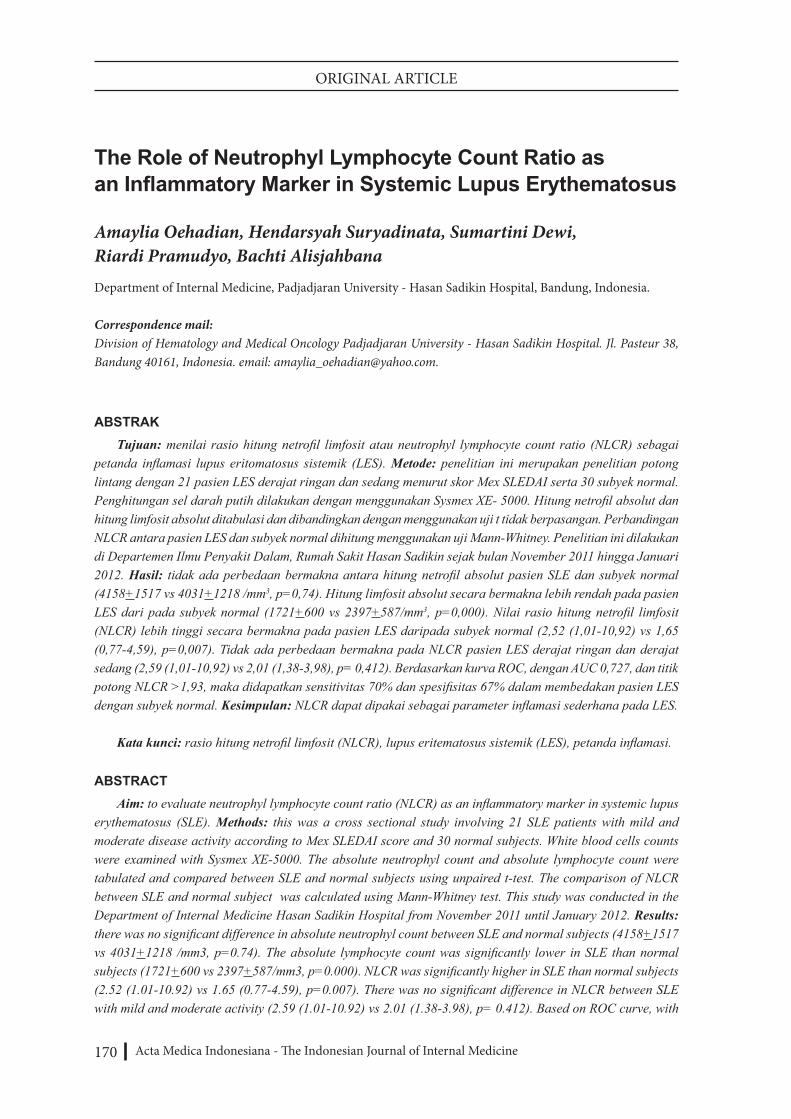
in Table 2. There was no significant difference in absolute neutrophyl count between SLE and normal subjects (4158 + 1517 vs 4031 + 1218 /mm3, p=0.74). The absolute lymphocyte count was significantly lower in SLE than normal subjects (1721 + 600 vs 2397 + 587/mm3, p=0.000). NLCR was significantly higher in SLE than normal subjects (median 2.52 (range 1.01-10.92) vs median 1.65 (range 0.77-4.59), p=0.007) (Figure 1). There was no significant
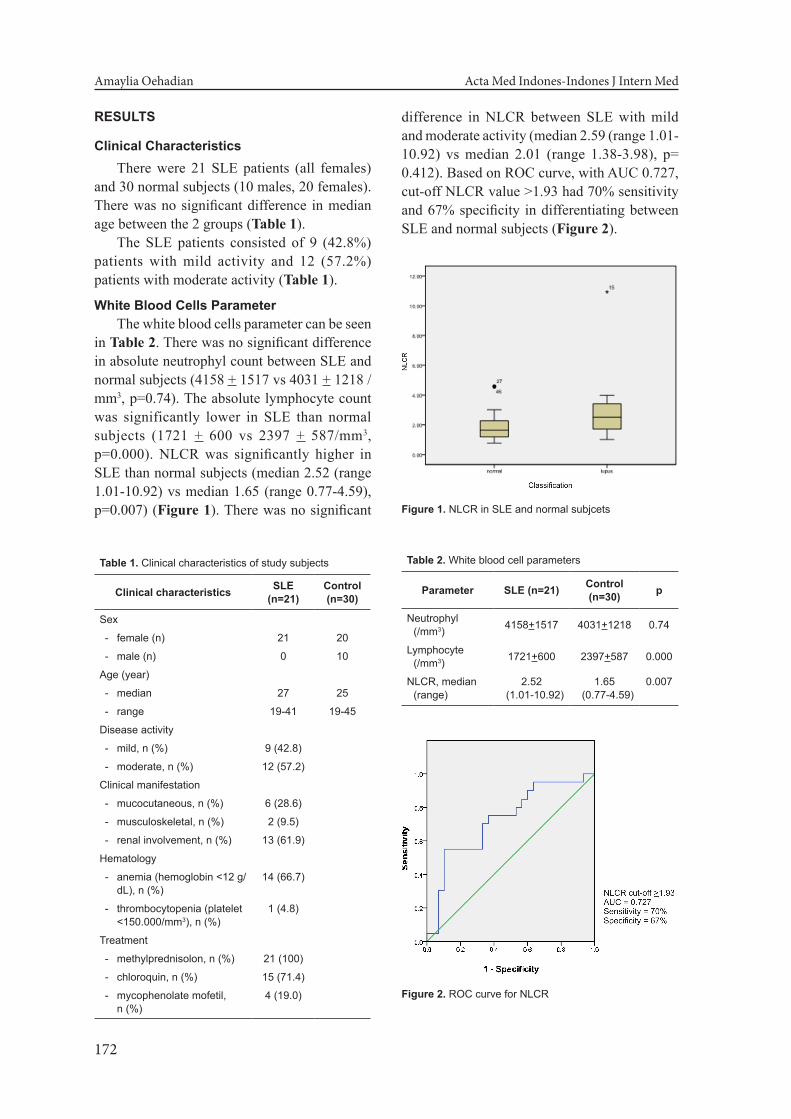
difference in NLCR between SLE with mild and moderate activity (median 2.59 (range 1.01-10.92) vs median 2.01 (range 1.38-3.98), p= 0.412). Based on ROC curve, with AUC 0.727, cut-off NLCR value >1.93 had 70% sensitivity and 67% specificity in differentiating between SLE and normal subjects (Figure 2).
Table 1. Clinical characteristics of study subjects
Clinical characteristics SLE (n=21)
Control (n=30)
Sex
- female (n) 21 20
- male (n) 0 10
Age (year)
- median 27 25
- range 19-41 19-45
Disease activity
- mild, n (%) 9 (42.8)
- moderate, n (%) 12 (57.2)
Clinical manifestation
- mucocutaneous, n (%) 6 (28.6)
- musculoskeletal, n (%) 2 (9.5)
- renal involvement, n (%) 13 (61.9)
Hematology
- anemia (hemoglobin <12 g/dL), n (%)
14 (66.7)
- thrombocytopenia (platelet <150.000/mm3), n (%)
1 (4.8)
Treatment
- methylprednisolon, n (%) 21 (100)
- chloroquin, n (%) 15 (71.4)
- mycophenolate mofetil, n (%)
4 (19.0)
Table 2. White blood cell parameters
Parameter SLE (n=21) Control (n=30) p
Neutrophyl (/mm3) 4158+1517 4031+1218 0.74
Lymphocyte (/mm3) 1721+600 2397+587 0.000
NLCR, median (range)
2.52 (1.01-10.92)
1.65 (0.77-4.59)
0.007
Figure 1. NLCR in SLE and normal subjcets
Figure 2. ROC curve for NLCR

Vol 45 • Number 3 • July 2013 Neutrophyl lymphocyte count ratio as an inflmmatory marker in SLE
173
DISCUSSIONNLRC is a potentially useful clinical
biomarker of systemic inflammatory response. Our subjects consist of 20 SLE (all females) and 30 normal subjects (20 females, 10 males). There were no difference in age between the two groups (median 27 (range 19-41) vs median 25 (range 19-45) years) (Table 1). In our subjects the lymphocyte and neutrophil count were within normal limits. This result could be explain by the mild and moderate activity of Mex SLEDAI in our subjects. However, compared with normal subject, the lymphocyte counts were significantly lower in SLE (mean+SD): 2397+587 v.s. 1721+600/mm3, p=0.000) (Table 2). The prevalence of lymphopenia in SLE ranges from 20 to 81% and its degrees may correlate with disease activity. Both T and B lymhocytes are reduced, while in contrast, NK cells are typically increased.3
The NLCR was significantly higher in SLE compared to normal subjects (median 2.52 (range 1.01-10.92) vs median 1.65 (range 0.77-4.59), p=0.007) (Table 2, Figure 1). Since there is no difference in neutrophyl count between the 2 groups (4158+1517 v.s. 4031+1218/mm3) (Table 2), the higher NLCR in SLE was caused by lower lymphocyte count. Although the degrees of lymphopenia may correlate with disease activity, we did not find significant difference in NLCR between SLE with mild (9 subjects) and moderate activity (11 subjects) (2.59 (1.01-10.92) vs 2.01 (1.38-3.98), p=0.412). Based on ROC curve, we found that NLCR cut-off value of >1.93 could be used as inflammatory marker in SLE subject with AUC 0.727, sensitivity 70% and specificity 67% (Figure 2). As far as we know, there was no previous study about NLCR in SLE.
Clinical usefulness of NLCR has been established in previous studies. In infectious disease the NLCR is a better predictor of bacteremia than routine parameters like CRP levels, WBC and neutrophil counts.5 NLCR is superior to total WBC in predicting adverse outcomes of acute pancreatitis. NLCR cut-off value of >4.7 is a simple indicator of severity in patients presenting with acute pancreatitis.6 In cardiovascular disease, NLCR is associated with
increased cardiac mortality in clinically stable patients with coronary artery disease.7 Elevated NLCR are predictors of significant ventricular arrhythmias in patients undergoing percutaneous coronary intervention (PCI).8 NLCR predicts chemotherapy outcomes in patients with advanced colorectal cancer. NLCR <5 (P=0.003) were associated with improved clinical benefit.4 An elevated NLCR is an independent predictor of overall survival (OS) but not disease free survival (DFS) in stage II colon cancer patients who did not receive adjuvant chemotherapy.9 NLCR is an independent predictor of survival for patients with malignant mesothelioma undergoing systemic therapy. NLCR less than 5 was an independent predictor of longer survival.10
Neutrophil-lymphocyte stress factor, as a NLCR, correlated with the severity of clinical course (according SOFA and APACHE II score) in the population of 90 ICU oncological patients.11
The clinical profile of SLE is characterised by extensive variation among patients as well as in the same patient over time. This variation is explained in part by the protean clinical manifestations of SLE and their severity, fluctuation between remission and exacerbation overtime, and the coexistence of manifestations related to reversible inflammation and to irreversible damage. The assessment of SLE patiens is therefore difficult for the physician in everyday care. Physician global assessment is generally regarded as gold standard for disease activity. However, physician global assessment is subjet to substantial variability, explained in part by variations among physicians in assigning levels of importance to different organ systems or to serologic activity.12
In recent years, many disease activity indices to measure reversible inflammation in SLE have been developed and validated. This include the British Isles Lupus Assessment Group (BILAG), the European Consensus Lupus Activity Measurement (ECLAM), the Systemic Lupus Activity Measure (SLAM) and the SLE Disease Activity Indes (SLEDAI), and revised versions as SLEDAI-2K and Safety of Estrogen in Lupus Erythematosus National Assessment (SELENA) SLEDAI.12
Guzman made simplified modification

Amaylia Oehadian Acta Med Indones-Indones J Intern Med
174
of SLEDAI called Mex SLEDAI with the consideration of availabe resources in developed country.13 A flare of SLE has been defined as an increase in SLEDAI >3, and a SLEDAI score >5 is associated with a probability of initiating or changing therapy in more than 50% of instances.12
Hematological complications are frequently seen in SLE. Anemia, leucopenia and thrombocytopenia may result from bone marrow failure or excessive peripheral cell destruction.Both of them may be immune mediated. Drugs and infection are other common causes.3,14
Haematological disordes are included in the American College of Rheumatology (ACR) Classification criteria for SLE. This includes haemolytic anaemia with a reticulocytosis, leucopenia (<4.0 x 109/L) or lymphopenia (<1.5 x 109/L) on two or more occasions or thrombocytopenia (<100 x109/L) in the absence of offending drugs.3
Leucopenia is a typical feature in SLE, and may occur as a result of lymphopenia, neutropenia or a combination of the two. Neutropenia is also a common feature of SLE, with a prevalence in the order of 47%, and this may be mediated by anti-neutrophil antibodies. Impaired function of the mononuclear phagocytic system, allowing sensitized cells to remain in the circulation may in part compensated for this.3,14
Our study had several limitation; we only measured the hematologic parameter and Mex SLEDAI activity in one occasion and involving a small number of subjects.
CONCLUSION NLCR was significantly higher in SLE
than normal subjects. This findings could be considered as a new insight in characterizing inflammatory response in SLE with simple hematologic parameter. NLCR could be used as a novel inflammatory marker in SLE.
REFERENCES1. Tassiulas IO, Boumpas DT. Clinical features and
treatment of systemic lupus erythematosus. In: Firestein GS, Budd Rc, Harris ED, et al. eds. Kelley’s textbook of rhematology. 8th ed. Philadelphia: Saunders Elsevier; 2009. p. 1263-6.
2. Perhimpunan Reumatologi Indonesia. Rekomendasi diagnostik dan pengelolaan lupus eritematosus sistemik, 2011.
3. Hepburn AL, Narat S, Mason JC. The management of peripheral blood cytopenias in systemic lupus erythematosus. Rheumatol. 2010;49:2243-54.
4. Chua W, Charles KA, Baracos VE, Clarke SJ. Neutrophil/lymphocyte ratio predicts chemotherapy outcomes in patients with advanced colorectal cancer. Brit J Cancer. 2011;104:1288-95.
5. De Jager CPC, van Wijk PTL, Mathoera RB, et al. Lymphocytopenia and neutrophil-lymphocyte count ratio predict bacteremia better than conventional infection markers in an emergency care unit. Crit Care. 2010;14:R192.
6. Azab B, Jaglall N, Atallah JP, et al. Neutrophil-lymphocyte ratio as a predictor of adverse outcomes of acute pancreatitis. Pancreatol. 2011;11:445-52.
7. Celik T, Bugan B. White blood cell count and stable coronary artery disease: The role of neutrophil to lymphocyte ratio. Cardiol J. 2011;18:720.
8. Chatterjee S, Chandra P, Guha G, Kalra V, Chakraborty A, Frankel R. Elevated white blood cell count and neutrophil-lymphocyte (N/L) ratio are predictors of ventricular arrhythmias during percutaneous coronary intervention. Cardiovasc Hematol Disord Drug Targets. 2011 Oct 26. [Epub ahead of print].
9. Hung HY, Chen JS, Yeh CY, et al. Effect of preoperative neutrophil-lymphocyte ratio on the surgical outcomes of stage II colon cancer patients who do not receive adjuvant chemotherapy. Int J Colorectal Dis. 2011;26:1059-65.
10. Kao SCH, Pavlakis N, Harvie R, Vardy JL, Boyer MJ, van Zandwijk N. High blood neutrophil-to-lymphocyte ratio is an indicator of poor prognosis in malignant mesothelioma patients undergoing systemic therapy. Clin Cancer Res. 2010;16:5805-13.
11. Zahorec R. Ratio of neutrophil to lymphocyte counts--rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001;102:5-14.
12. Mosca M, Bombardieri S. Assessing remission in systemic lupus erythematous. Clin Exp Rheumatol. 2006;24:S100-S104.
13. Guzman J, Cardiel MH, Arce-Salinas A, Sanchez-Guerrero J, Alarcon-Segovia D. Measurement of disease activity in systemic lupus erythematosus. Prospective validation of 3 clinical indices. J Rheumatol. 1992;19:1551-8.
14. Quismorio FP Jr. Hematologic and lymphoid abnormalities in systemic lupus erythematosus. In: Wallace DJ, Hahn BH, eds. Dubois’ lupus erythematosus. 7th ed. Philadelphia: Lippincott Williams and Wilkins; 2007. p. 816-20.










![Preoperative neutrophil-to-lymphocyte ratio is a …...82 Annals of Surgical Treatment and Research 2015;89(2):81 86 neutrophil to lymphocyte ratio (NLR) [6]. An NLR can be calculated](https://img.pdfslide.net/doc/110x75/5f20b8d43d033a4ea70d0b87/preoperative-neutrophil-to-lymphocyte-ratio-is-a-82-annals-of-surgical-treatment.jpg)


















