Embed Size (px)
Citation preview
THE ROLE OF NURSING STUDENTS IN BEHAVIORAL HEALTH HOMES IN NEW
YORK CITY UNDER MEDICAIDMANAGED CARE
PRESENTED BY
Kathleen Cervasio Ph.D., Ed.D., ACNS-BC, CCRN Alumnus, RNChair, Faculty Affairs, Associate Professor, Harriet Rothkopf Heilbrunn School of Nursing School of Nursing, Long Island University, Brooklyn, New York
Joann Paoletti, PhD (c), MSN, RN-BCDirector of Specialty Clinicals, Assistant Professor, Harriet Rothkopf Heilbrunn School of Nursing, Long Island University, Brooklyn, New York
Why we need health homes
There are approx 4 million people in the U.S. with serious mental illness which includes schizophrenia, schizoaffective disorder, and bipolar disorder.
At any given time, half are receiving no treatment for their illness.
10% are problematic (homeless; in jail or prison).
1% are overtly dangerous (violence against others, including homicides.
How can this population be managed outside of any type of institution?
Directly observed therapy (DOT) Long-acting injection Implantable medication devices Assays of blood or urine Engagement activities
Medicaid Managed Care
Meeting Provider Qualifications and Standards and providing adequate choice within Health Home partnerships
Care Management “Bandwidth” ability to meet needs of all facets of complex populations (e.g., Mental Health, Housing, Substance Use Disorder, etc.)
Promoting a vision to minimize silos and concentrate volume over a few rather than many Health Home networks/systems thereby assuring a more limited accountability structure and more financially viable Health Homes.
Creating choices where applicable between institutional lead and community based lead Health Homes
Medicaid Managed Care
Goal is to decrease hospital readmission by 30%
SAVE $$$$$$$$$
Medicaid Managed Care
Hospitals, clinics, community services Started in NYC in 2012 with about 160 K members Medicaid eligible individual having:◦ At least 2 chronic conditions, ◦ 1 chronic condition and be at risk of developing another, or◦ At least 1 serious and persistent mental health condition.
Management Metrics Functional Status Tool
Health Home Services
Comprehensive care management Care coordination and health promotion Comprehensive transitional care/follow-up Patient and family support Referral to community and social support services Use of health information technology (HIT) Mental Health Integration Program
Medicaid Managed Care
So………we are finally looking at people holistically, identifying all needs that ultimately need monitoring and treatment
We no longer keep mental health members separately from members who need medical follow up. Reality is people have both mental health and medical care needs.
What exactly is a health home?
Health Homes: a place where individuals can come throughout their lifetimes to have their healthcare needs identified and to receive the medical, behavioral and related social services and supports they need, coordinated in a way that recognizes all of their needs as individuals–not just patients.
HH providers integrate and coordinate all primary, acute, behavioral health, and community support services; treating the whole person with the goal to improve care and reduce costs
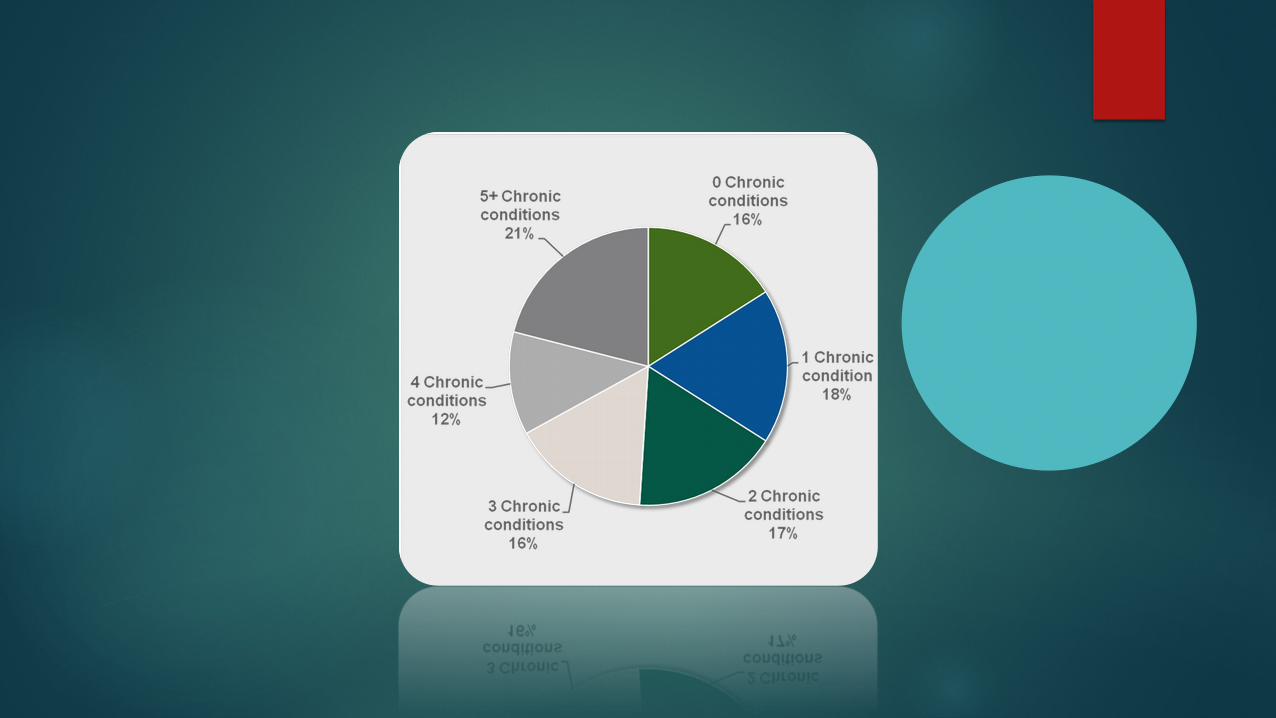
The Number Of Individuals With Chronic Conditions Is Increasing.
More than 40% of the U.S. Population has one or more chronic conditions.
39% of the U.S. working - age population in 2007 had at least one chronic condition.
By 2020, the number of people with multiple chronic conditions is expected to increase to 81 million, up from 57 million in 2000.
Who gets this service?Clients eligible for a CMHC Healthcare Home must meet one of the following three conditions (identified by patient health history):
1. A serious and persistent mental illness,o Community Psychiatric Rehabilitation (CPR) eligible adults
and kids with Serious Emotional Disorder (SED)2. A mental health condition and substance use disorder, or3. A mental health condition and/or substance use disorder and one
other chronic health condition.
Chronic health conditions include:1. Diabetes,2. Cardiovascular disease,3. Chronic obstructive pulmonary disease (COPD),asthma, chronic
bronchitis, or emphysema4. Overweight (BMI >25),5. Tobacco use,6. Developmental disability.
Working Together-The Role of Targeted Case Management(TCMs) in Health Homes
The HH model expands concepts from both converting case management programs and Patient Centered Medical Home model by building additional linkages and enhancing coordination and integration of medical and behavioral health care to better meet the needs of people with multiple chronic illnesses.
In other words, the Health Home takes the Medical Home concept across multiple care disciplines and into the community for high need Medicaid recipients
What TCM offers TCMs were developed to provide community-based case
management to high need Medicaid recipients (HIV+/Mental Health) often disengaged from medical, mental health, and social services
TCMs have years of experience in outreach and engagement of persons difficult to locate and keep in care:
unstably housed mentally ill history of incarceration substance using with multiple chronic illnesses impacted by stigma
Who provides the services
HHs networks were approved only if they included converting case management programs; in many cases multiple case management programs.
Lead HHs are expected to be using the value and expertise of their entire HH network to achieve the goals of the program.
Nurses were never hired to do assessments.
Some History
Case management programs operated successfully, but programs were not anchored into formal comprehensive networks with medical providers.
Under HH case management agencies are transitioning as part of larger networks.
TCMs are accountable to HH Leads; often multiple leads with different requirements.
TCMs work to ensure client outcomes are realized; provide direct service to locate/engage clients and coordinate member care and services.
TCM input into HH policies can help ensure more effective processes.
Fiscal concerns
Fiscal Viability Converting programs ability to generate revenue to cover agency
administrative and infrastructure costs are dependent on volume of assignments, and amount and timing of payments
Concern about future cash flow beyond direct Medicaid billing
Concern about survival beyond legacy rates
Administrative costs must be negotiated with multiple HH Leads and MCOs.
New infrastructure and HIT costs are not built into reimbursement; impacting lead HHs and network partners alike.
Administrative issues
Administrative burden Tracking enrollee status for multiple HH
Reporting to multiple MCOs and HH Leads
Requirements vary - some have added reporting elements beyond state requirements
Maintaining databases/EHRs for multiple HH and ensuring staff are trained to use them
Building capacity
Hiring, training, supervising staff Oversight and quality assurance
Insurance issues
The Affordable Care Act was passed by Congress and signed into law by the President in March 2012.
Section 2703 of the Act adds section 1945 to the Social Security Act to allow states to amend their Medicaid state plans to provide Health Homes for enrollees with chronic conditions.
Other considerations
States may further limit eligibility criteria, e.g., based on diagnosis or risk of institutionalization.
States must offer services to all enrollees who meet the eligibility criteria.
States may not exclude individuals dually eligible for Medicare.
States can limit the geographic area where the program is offered to places where the need is greatest, or where providers are available.
Services offered
The following health home services are to be provided in a comprehensive, timely, and high quality fashion:1. Comprehensive Care Management2. Care coordination 3. Health promotion4. Comprehensive transitional care from inpatient to other settings5. Individual and family support 6. Referral to community and social support services7. The use of health information technology to link services
*States will receive a 90% federal match for these specific services.
Service providers
CMS specific provider types include: 1. A health team, defined as an interdisciplinary, inter-professional team; including
medical specialists, nurses, pharmacists, nutritionists, dieticians, social workers, behavioral health providers, physician’s assistants, etc.
Providers are expected to address functions including but not limited to: 1. Providing quality-driven, cost-effective, culturally appropriate, and person-and
family-centered health home services2. Coordinating and providing access to high-quality health care services informed by
evidence-based guidelines3. Coordinating and providing access to mental health and substance abuse services4. Coordinating and providing access to long-term care supports and services.
Provider requirements
patient access to the health team, including the development of alternatives to face-to-face visits, such as telephone or email, 24 hours per day 7 days per week
Actively use a comprehensive electronic health record (EHR) to conduct care coordination and prescription monitoring for Medicaid participants
Utilize an interoperable patient registry to input annual metabolic screening results, track and measure care of individuals, automate care reminders, and produce exception reports for care planning
Provider role
Routinely use a behavioral pharmacy management system to determine problematic prescribing patterns
Conduct wellness interventions as indicated based on clients’ level of risk
Complete status reports to document clients’ housing, legal, employment status education, custody etc.
Agree to convene regular, ongoing and documented internal Health Home team meetings to plan and implement goals and objectives of practice transformation
Enter senior level BSN students in a community health clinical rotation
Nurse Care Managers – 1 FTE/250 enrollees NO RN staff
Develop wellness and prevention initiatives, provide trainings, track required assessments, administrative support, etc.
Nursing students assuming the role of care managers in numerous settings under faculty direction via technology.
Brooklyn Community Services
BCS Health Home Care Management is a Medicaid funded care management program for individuals with serious health, behavioral health or substance abuse problems.
Health Homes are care management service models where all of an individual's caregivers communicate with one another so that all of a patient's needs are addressed in a comprehensive manner. At BCS, this is done through our care managers who oversee and provide access to all of the services an individual needs to assure that they receive everything necessary to stay healthy, out of the emergency room and out of the hospital. Health records are shared among providers so that services are not duplicated or neglected. BCS Care Management is part of three health home networks:
The Brooklyn Health Home, Coordinated Behavioral Care (CBC) and Comprehensive Health Network (CHN). Our health home services are provided through a network of organizations – providers, health plans and community-based organizations. When all the services are considered collectively they become a virtual "Health Home."
What BCS does
Brooklyn Community Services (BCS) was founded in 1866 and continues to help children and youth reach their full potential, strengthen families, and foster self-sufficiency in adults. Brooklyn Community Services is one of the oldest, not-for-profit, non-sectarian social service providers in New York City and one of the largest in Brooklyn.
Over the years, BCS has strengthened countless families at risk of separation; supported and stabilized people with psychiatric illnesses; helped adults with disabilities participate fully in the community; enabled people to move from welfare to work; and offered guidance, education and support to children and young adults. With programs in 17 Brooklyn locations, Brooklyn Community Services serves more than 13,000 people each year.
Brooklyn Community Services(BCS)
FAMILY PROGRAMS CHILDREN & YOUTH PROGRAMS, Adolescent Employment and
Education, Early learning centers, Brooklyn High School for Leadership and Community Service, Family Day Care,
ADULT PROGRAMS, Mental Health Programs, Vocational Programs,Developmental Disability Programs, Homemaking
Preventative Services, PROS, Club House, Transitional living, Dayhab, Housing, Career services, MSC, Recreation, Residency
So, what have we done
Nursing students have learned to begin transitioning into practice without a faculty member always present
Faculty utilized the following as frameworks to develop this new clinical site where nursing has NOT had a presence:
AACN, Essentials of Baccalaureate Education, public health nurse competencies, white paper for the clinical nurse leader ( CNL), Clinical Prevention and Population Health Curriculum Framework, guidelines for Interprofessional Collaborative Practice and Undergraduate Public Health Education
Details
Approximately 30 students per semester are assigned to various community health sites throughout Brooklyn, NY for 14 weeks, 5 hour days.
Cell phones and texts are used to communicate with faculty. Students check in and out and complete a discussion board weekly on Blackboard with pointed questions related to course objectives.
Students track the number of members seen, follow up on member issues, and attend a weekly seminar to discuss their clinical sites.
What have students learned?
Overcome fear of being alone Talk to and work with multiple other disciplines Communicate with outside agencies such as ACS Refer to primary care physicians Deal with complex and difficulty member and family situations Importance of family nursing Refine assessment skills for members across the lifespan Integrate mental health and primary care Well assessments as well as problem assessments How to develop needed forms

Students have also learned about Effective therapeutic communication Evidence based practice guidelines Information technology Identifying and tracking high risk members on software programs
across the borough to view visits to health care providers, hospitals, attendance at health care classes, ER visits
Operationalizing level of prevention Work with other disciplines Healthcare policy, finance, and regulatory agencies Intervene with problems effectively Represent the profession of nursing
Student responses to the BCS rotation
Not what I thought it would be Hard to practice outside a hospital I can’t control things! I need to study more I get the bigger picture now I like this! Too scary for me! I need to know the money end of all of this!
Faculty responses Collaboration with BCS leadership to foster community partnerships
with the university Meetings with clinical psychologists, physicians, and mental health
workers to problem solve and provide mutual support Give employee wellness seminars Really see the results in student outcomes become practice entry Collaboration on grants and publications BCS starting to hire RNs and APNs, faculty assist in writing job
requirements and salary recommendations Primary care practice with members with multiple disparities Markets the nursing profession Constant accolades of praise from BCS staff for our students!
What services have we provided to BCS members
H&P Case finding Referrals for medical f/u, vaccinations, and social issues, i.e. housing Classes and referrals for– DM, HTN, High cholesterol, medications
including reconciliation, domestic violence, abuse, smoking sensation, drug sensation, men and women's preventative health, STD’s, HIV, CHF, safety in the community
Home visits with social workers for high needs/risk cases Family interventions, including schools and ACS referrals Connected with providers , clinics, and hospitals in the community Follow members and health care facility usage across the system
electronically so interventions can be timely
BCS staff
Extremely dedicated, respectful, helpful to students Executive group recognizes publically they could not do this
initiative without us Faculty assisting now with their quality improvement program as this
evolves Starting to work on collaborative efforts, i.e. grants Recognize the importance of having the NURSE and call on us
constantly, wishing funds were there to hire RN’s. Mutual goal setting Mutual outcome measurements
Overall response from everyone involved
This partnership reminds us all of what people need and live with in the REAL WORLD!!
Thank You!
References
Health Home Website: http://www.health.ny.gov/health_care/medicaid/program/medicaid_health_homes/
Bradshaw, T. & Pedley, R. (2012). Evolving role of mental health nurses in the physical health care of people with serious mental health illness. International Journal of Mental Health Nursing, 21 (3), 266–273.
Cassil, Alwyn. ( 2010) Innovations in preventing and managing chronic conditions: What’s working in the real world?” Center for Studying Health System Change, Issue brief 132, retrieved May 2015 from http://www.hschange.com/CONTENT/1130/?topic=topic17
Chadwick, A., Street, C., Mcandrew, S. & Deacon, M. (2012).Minding our own bodies: Reviewing the literature regarding the perceptions of service users diagnosed with serious mental illness on barriers to accessing physical healthcare. International Journal of Mental Health Nursing, 21 (3),211–219.
References continuedHolt, R. I. (2011). Undoing Descartes: Integrating diabetes care for those with mental illness. Practical Diabetes, 28 (6),270–275.
Nielsen, A., Noone, J., Voss, H. & Mathews, L. Preparing nursing students for the future: An innovative approach to clinical education. Nurse Education in Practice, 13 (4) 301-9.
McGonigle, D., Hunter, K., Sipes, C. & Hebda, T. (2014). Why nurses need to understand nursing informatics. AORN Journal, 100(3), 324-327.
Scott, D. & Happell, B. (2011). The high prevalence of poor physical health and unhealthy lifestyle behaviours in individuals with severe mental illness. Issues in Mental HealthNursing, 32 (9), 589–597.
Wheeler, A., Harrison, J., Mohini, P., Nardan, J., Tsai, A. & Tsai,E. (2010). Cardiovascular risk assessment and management in mental health clients: Whose role is it anyway? Community Mental Health Journal, 46 (6), 531–539.