Embed Size (px)
Citation preview

The Role of Primary Cancer Diagnosis in Determining Costs and Caregiver Burden Associated with
Palliative Home Care
by
Ruby Redmond-Misner
A thesis submitted in conformity with the requirements for the degree of Master of Science
Institute of Health Policy, Management and Evaluation University of Toronto
© Copyright by Ruby Redmond-Misner 2014

ii
The Role of Primary Cancer Diagnosis in Determining Costs and Caregiver Burden Associated with Palliative Home Care
Ruby Redmond-Misner
Master of Science
Institute of Health Policy, Management and Evaluation University of Toronto
2014
Abstract Community-based palliative home care (CBPHC) has been repeatedly endorsed for expansion
in Ontario. The objective of this thesis is to assess the role of primary cancer diagnosis in the
costs and caregiver burden associated with CBPHC.
Patients from two Ontario CBPHC programs were categorized using the World Health
Organization’s International Classification of Diseases (10th Ed.), differentiating tumour sites (i.e.
breast) rather than tumour type (i.e. carcinoma). Diagnosis was integrated into econometric
models alongside other important covariates, identified by conceptual frameworks of cost and
burden, in order to ascertain its role in both.
Findings suggest that there are differential care demands associated with recipients of CBPHC
that are related to primary cancer diagnosis. Several tumour sites emerged as significant drivers
of costs and caregiver burden. This is useful for the level of care and associated strain that can
be expected upon admission into CBPHC, the maintenance CBPHC and its unpaid caregivers,
and the personalization of care.

iii
Acknowledgements
In culminating my Master’s degree, I have so many people to thank. Thank you to anybody that has encouraged me and supported me along the way.
I gratefully acknowledge my thesis supervisor, Dr. Peter C. Coyte, for your guidance and for always reviewing my work promptly and thoroughly. I could not have completed my degree so quickly without your dedication. I also thank my committee member, Dr. Audrey Laporte, for econometric counsel, encouragement and for involving me with the Canadian Centre for Health Economics.
My sincerest appreciation goes to the members of my examination committee: Drs. Jan Barnsley (University of Toronto) and Daryl Bainbridge (McMaster). Thank you for your time and for providing valuable insight and feedback.
I would like to thank those at the Canadian Centre for Applied Research in Cancer Control (ARCC) who facilitated my incredibly helpful mock defense. Thank you Drs. Jeffrey Hoch, Wanrudee Isaranuwatchai and Rebecca Mercer and Jaclyn Beca for asking challenging questions and giving useful advice.
Thank you to my fellow students for being so encouraging and such great role models. I felt very welcome as soon as I started at IHPME and I wish you all the best. We will be in touch.
I gratefully acknowledge Adrian Rohit Dass for his econometric counsel, recommendations and revisions of my use of Allison’s hybrid model.
Last but not least, I thank my mother Kelly, aunt Karen, and sister Rachel for providing support and comic relief throughout and prior to my pursuit of higher education. Mom and Karen, thank you for the sacrifices you have made for Rachel and I to have privileges that were not afforded to you. We love and appreciate you very much.
iv
Table of Contents Acknowledgements ....................................................................................................................... iii
List of Tables ................................................................................................................................. vi
List of Figures ............................................................................................................................... vii
List of Appendices ....................................................................................................................... viii
Chapter 1 ....................................................................................................................................... 1 1.1 What is palliative care? ........................................................................................................ 1 1.2 Background: Palliative home care in Canada ...................................................................... 2 1.3 Research purpose and rationale ......................................................................................... 5 1.4 Research questions and hypotheses .................................................................................. 6
Chapter 2 ....................................................................................................................................... 9 2.1 Search strategy .................................................................................................................... 9 2.2 Palliative home care cost ................................................................................................... 12 2.3 Caregiver burden in palliative care .................................................................................... 19 2.4 Neoplasm specific palliative care research ....................................................................... 27 2.5 Summary ........................................................................................................................... 32
Chapter 3 ..................................................................................................................................... 33 3.1 Overview of the larger study .............................................................................................. 33 3.2 Data ................................................................................................................................... 34
3.2.1 Data origin ................................................................................................................... 34 3.2.2 Data description .......................................................................................................... 34 3.2.3 Variable description ..................................................................................................... 36 3.2.4 Variable assessment ................................................................................................... 42 3.2.5 Variable inclusion ........................................................................................................ 42 3.2.6 Categorical variable interpretation and baseline ......................................................... 43
3.3 Descriptive statistics .......................................................................................................... 44 3.4 Cost analyses .................................................................................................................... 44
3.4.1 Logarithmic transformation and quadratic forms ......................................................... 44 3.4.2 Aggregated costs ........................................................................................................ 45 3.4.3 Disaggregated cost ..................................................................................................... 48
3.5 Caregiver burden analysis ................................................................................................. 51 3.6 Diagnostics ........................................................................................................................ 52
3.6.1 Hausman test .............................................................................................................. 52 3.6.2 Allison’s hybrid method ............................................................................................... 52 3.6.3 Standard diagnostics .................................................................................................. 54
3.7 Summary ........................................................................................................................... 55
Chapter 4 ..................................................................................................................................... 56 4.1 Descriptive statistics .......................................................................................................... 56 4.2 Cost analyses .................................................................................................................... 58
4.2.1 Aggregated costs ........................................................................................................ 59
v
4.2.2 Service-specific cost analysis results .......................................................................... 66 4.3 Caregiver burden ............................................................................................................... 73 4.4 Diagnostics/Additional information .................................................................................... 74 4.5 Summary ........................................................................................................................... 78
Chapter 5 ..................................................................................................................................... 81 5.1 Findings vis-à-vis the hypotheses ..................................................................................... 82 5.2 Comparisons and inferences from the literature ................................................................ 85 5.3 Policy implications ............................................................................................................. 90 5.4 Limitations .......................................................................................................................... 95 5.5 Summary ........................................................................................................................... 96
Chapter 6 ..................................................................................................................................... 97 6.1 Thesis summary ................................................................................................................ 97 6.2 Future work ...................................................................................................................... 100
References ................................................................................................................................ 104

vi
List of Tables
Table 1: ICD-10 categories ......................................................................................................... 37
Table 2: AHCR framework for the identification of palliative care costs ...................................... 38
Table 3: Caregiver burden scale in end-of-life care .................................................................... 40
Table 4: Categorical variable baselines ...................................................................................... 44
Table 5: Summary of patient and caregiver demographics ......................................................... 57
Table 6: Hausman test results, final estimator(s) ........................................................................ 59
Table 7: Determinants of societal costs of CBPHC ..................................................................... 60
Table 8: Determinants of CBPHC Ministry of Health costs ......................................................... 62
Table 9: Determinants of CBPHC unpaid caregiver costs .......................................................... 65
Table 10: Determinants of receiving any medications and their cost .......................................... 67
Table 11: Probability of hospitalization among CBPHC recipients .............................................. 69
Table 12: Determinants of having a home appointment and its associated cost ........................ 71
Table 13: Determinants of caregiver burden in CBPHC ............................................................. 73
Table 14: Significant findings across all analyses ....................................................................... 78

vii
List of Figures
Figure 1: PRISMA flow chart for home care cost literature search ............................................. 13
Figure 2: PRISMA flow chart for caregiver burden literature search ........................................... 20
Figure 3: PRISMA flow chart for palliative oncology literature search ........................................ 28
Figure 4: Observations per time period ....................................................................................... 35
Figure 5: Charlson comorbidity index .......................................................................................... 41
Figure 6: Algorithm for deciding which estimator(s) to use ......................................................... 54
Figure 7: Raw and log-positive distribution of public medication cost ......................................... 76
Figure 8: Raw and log-positive distribution of public home appointment cost ............................ 77
Figure 9: Raw and log scale burden scores ................................................................................ 78

viii
List of Appendices Appendix A ................................................................................................................................ 117
Appendix B ................................................................................................................................ 123
Appendix C ................................................................................................................................ 129
Appendix D ................................................................................................................................ 134
Appendix E ................................................................................................................................ 137
Appendix F ................................................................................................................................ 138
Appendix G ................................................................................................................................ 139
Appendix H ................................................................................................................................ 141
Appendix I ................................................................................................................................. 143

1
Chapter 1 Introduction
The objective of this thesis is to comprehensively analyze the financial and caregiver
burdens associated with community-based palliative home care (CBPHC) for people
with cancer so as to identify significant determinants. This will be done with special
attention paid to the primary cancer diagnosis of the patients, which is hypothesized to
have a role in palliative care needs and outcomes. These are defined by solid tumour
site (i.e. breast or brain) as opposed to type (i.e. carcinoma or sarcoma) in congruence
with the World Health Organization’s (WHO) International Classification of Diseases (10th
Ed.) (ICD-10). There is little in the existing literature that assesses multiple neoplastic
primary diagnoses simultaneously to allow comparative inferences to be made. In fact,
treating all patients with cancer as a homogenous group is the norm.
1.1 What is palliative care?
A note on terminology
The term palliative care is often used interchangeably with end-of-life (EoL) care (Health
Canada, 2009). It is important to define precisely due to the ambiguity and obscurity
introduced by this latter term. The broad goal of palliative care is to improve quality of life
(QoL) for people facing terminal illnesses through pain and symptom management,
normalizing death and supporting those affected by the impending death into
bereavement (WHO, 2014; Health Canada, 2009). Referral into palliative care may
therefore commence at the time that curative treatment has stopped, shifting to symptom
management while the patient has some time left to live. For palliative patients with
cancer, this is often when neoplastic malignancies have metastasized, relapsed or are
inoperable (Gaertner et al, 2011). Conversely, counseling and other supports may be
offered to family members and unpaid caregivers beyond the death of the patient (WHO,
2014; Health Canada, 2009). These are points in the palliative trajectory that would not
constitute the EoL, which is why this term can obscure palliative care into something that
is provided only when death is imminent.

Chapter 1: Introduction R. Redmond-Misner
2
The Temmy Latner Centre for Palliative Care (TLCPC), from which data for this thesis
were derived, provides an idea of the services that go into providing palliative care at
home (2013). An interdisciplinary team of doctors, nurses, personal support workers
(PSWs), grief counselors, spiritual community members and volunteers may visit the
patient in their home to assist with activities of daily living (ADLs) or provide medical
care. The final, fundamental members of CBPHC teams (CBPHCTs) are unpaid
caregivers: family and friends who care for the patients in lieu of the formal CBPHCT.
Unpaid caregivers are becoming increasingly central to facilitating health care at home
(Guerriere, 2012), which is an important piece of information to precede the following
overview of palliative home care in Canada.
1.2 Background: Palliative home care in Canada
Current context
Restructuring of health care in Canada has been partially characterized by shifting
services into the community (Guerriere, 2012; Laville et al, 2007; Spalding, 2005;
Skinner, 2005). This is true of palliative care, which is commonly used by cancer patients
with terminal prognoses (Alesi et al, 2011; Balducci, 2003; Brink et al, 2008). While
concerns about the practicality of shifting a greater volume of services into the
community are emerging, it remains a popular option among influential health and public
policy research institutions. Recent endorsements for the further development of CBPHC
include the Health Council of Canada’s (2013) Progress Report, Health Quality Ontario’s
(HQO) (2012) Report on Ontario’s Health System, the Ontario Seniors’ Secretariat’s
(2013) Action Plan for Seniors, and Drummond et al’s (2012) Commission on the Reform
of Ontario’s Public Services.
Improving palliative care is a global public health priority, on the agendas of the WHO
and United Nations (UN) (Broad et al, 2013). Home- and community-based service
shifting has been proposed and implemented as a means of improving health care
sustainability internationally (Docherty et al, 2008; Drummond et al, 2012), which will
become apparent in the literature review. The Organization for Economic Cooperation
and Development (OECD) has written extensively on this as part of a broader shifting of

Chapter 1: Introduction R. Redmond-Misner
3
responsibility for health and social services onto community members, referring to
unpaid service providers as the “social economy” (Greffe, 2007).
Broad issues being raised
Ontario’s health critics, across political parties, express the idea that a demographic
crisis with serious implications for palliative care is pending. “Unless something is done
in the next few years, we’re going to be in a crisis situation on a number of fronts
including palliative care” said Christine Elliott, Ontario Progressive Conservative health
critic (Nash et al, 2013). France Gelinas, the Ontario New Democratic Party (NDP)
health critic (Nash et al, 2013), made a similar statement. Apprehension about an
impending demographic crisis is driven by unprecedented aging, cancer incidence and
life expectancies allowing for more chronic illness, but also by labour force changes
wherein most people work and people have fewer children (Jiwani, 2003; Kirkey, 2010;
Nash et al, 2013; Dennis et al, 2011). These trends jeopardize primary sources of
unpaid care: spouses and children (Seow, 2009). Yet we are still moving in a direction
that increases patient dependence on unpaid care.
Variability in the accessibility of public home care services that do exist is also a
concern. While some Local Health Integration Networks (LHINs) have fully staffed
CBPHCTs, others have very little in the way of home care (Yu, 2011). Residing outside
the protection of the Canada Health Act (Yu, 2011), the precarious position of CBPHC
prompts ongoing inquiry about the role of the state, public-private financing, unpaid
family caregivers, and models of delivery spanning the past two decades (Baranek,
2000). The Canadian Cancer Society (CCS) has attributed regional inconsistencies in
institutional and home death on the national level to the inconsistent structure of CBPHC
(Kirkey, 2010). With no comprehensive, province-wide plan for CBPHC, regional
disparities exist within Ontario as well (Yu, 2011; Kirkey, 2010). Home care receipt in
Ontario is sensitive to a number of factors including socio-economic status (SES)
(Motiwala et al, 2006), the availability of unpaid caregivers (Aoun et al, 2013), and home
care availability related to rurality and centrality (Skinner, 2005; Funk et al, 2010;
Kuluski, 2010; Bainbridge et al, 2011).
Families that do access home care reportedly experience high financial and
psychosocial burden. The CCS estimates costs of care for families facilitating home care

Chapter 1: Introduction R. Redmond-Misner
4
to be higher than $1,000 a month premised solely on the items that inpatient care would
provide: medications, nutritional supplements, special meals, vitamins, diapers,
dressings, aids for bathing and so on (Kirkey, 2010). This estimate does not include lost
income from time off work, use of vacation time or, in some cases, complete job loss
(Haley, 2003). Research has found that outcomes and quality of palliative care are
largely dependent on the stability and wellness of the caregiver. The catch twenty-two is
that it is compromised by their participation in caregiving (Brink, 2008; Cain et al, 2004).
The unpaid caregivers of palliative patients are more vulnerable to stress and
depression than their non-caregiver (Haley, 2003; Funk et al, 2010) and non-palliative
caregiver counterparts (Williams et al, 2014). The CCS advocates for extending
caregiver tax benefits from six to twenty-six weeks (Kirkey, 2010). In the June 2014
provincial election, a caregiver tax credit was on the platform of the NDP (Campion-
Smith, 2014), demonstrating the political momentum and attention being drawn by
community-based services and unpaid caregivers.
Despite growing interest in the burden placed on unpaid caregivers (Docherty et al,
2008; Bachner, 2007; Ryn et al, 2011; Parker Oliver, 2013), many cost studies in
CBPHC adopt a Ministry of Health (MoH) perspective if for no other reason than a data
deficit (Klinger et al, 2010; Cartoni et al, 2007). This excludes a considerable proportion
of the spending and labour time that is actually required to facilitate CBPHC. It has been
estimated that 80-90% of in-home care is provided by unpaid caregivers in Canada
(Haley et al, 2003). The palliative care sector in Canada generally is highly reliant on
volunteer labour. The Hospice Association of Ontario (HAO) reports that volunteers
provide 600,000 hours of work annually in over 400 communities (Shephard, 2004). The
value of unpaid care provided at home, if it were provided by paid workers, has been
estimated from $1 billion for cancer patients over seventy in the United States (Hayman
et al, 2001) to $35 billion for all unpaid care in Australia (Stajduhar et al, 2007). Other
developed nations using this type of home care model have given similar estimates
(Aoun et al, 2005). Projects assessing determinants of cost that adopt a societal
perspective – accounting for all costs irrespective of payer (Neumann, 2009) – are
therefore in demand.
Nature of existing findings
The determinants of cost and caregiver burden often overlap given that these are not

Chapter 1: Introduction R. Redmond-Misner
5
mutually exclusive dimensions of the palliative trajectory. Many are socio-demographic
and related to the living situation of the patient (Guerriere et al, 2010; Chai et al, 2013;
Gardiner et al, 2014), the comorbidity of the patient (Glajchen, 2012) and its associated
demands on their unpaid caregiver (Hirdes et al, 2012). Differences in cost have also
been noted across disease groups (Enguidanos et al, 2005), and this brings us to the
research purpose and rationale. “Cancer” is often grouped together and rarely treated as
distinct diseases requiring variable attention beyond curative treatment, but this may be
a significant variable in predicting the magnitude of cost and caregiver burden
associated with palliative cancer patients.
1.3 Research purpose and rationale
A key to stabilizing and improving CBPHC is identifying and mediating factors
associated with service use and caregiver burden, which may impinge on one another.
The objective of this thesis is to comprehensively analyze the determinants of the
financial and caregiver burdens associated with CBPHC for people with cancer. This will
be done with consideration for different stakeholders in this service and their cost
perspectives. Several gaps in the literature will be touched upon in this thesis, including
1) analysis of cost from multiple payer perspectives and at the micro-level, 2)
longitudinal analysis of caregiver burden, and finally, 3) to analyze these outcomes
taking into consideration specific primary cancer diagnoses (categorized by tumour
site vis-à-vis the ICD-10). In previous analyses of palliative care outcomes for this
population, the presence of any cancer and cancer stage have been used as clinical
indicators (Motiwala et al, 2006; Fairfield et al, 2012; Sussman et al, 2011; Sims et al,
1997).
The College of Physicians and Surgeons of Ontario’s (CPSO) (2002) “Decision-making
for the End of Life” policy statement asserts that emergency service use is often related
to the caregivers’ reservations about care tasks. Caregivers report clinical uncertainty
regarding medications, disease progression, side effects, symptoms, or whether to call
for assistance, as one of the most stressful dimensions of unpaid caregiving (Ryn et al,
2011). Palliative oncologic literature suggests that the aforementioned points of obscurity
may differ from malignancy to malignancy (Alesi et al, 2011; Dennis et al, 2011; Von

Chapter 1: Introduction R. Redmond-Misner
6
Roenn et al, 2011; Janjan, 2011). This research can speak to whether differential care
needs related to primary diagnosis persist beyond curative stages of treatment.
Palliative and oncologic care have previously been conceptualized as mutually exclusive
disciplines (Ramchandran et al, 2013), but literature embracing their interaction has
followed Temel et al’s (2010) seminal paper regarding mixed palliative-oncologic
treatment for patients with metastatic non-small cell lung cancer (NSCLC). This
illuminated the heterogeneity of cancer patient needs in the palliative trajectory. In 2011,
the journal Oncology dedicated an entire volume to the reconciliation of these disciplines
to improve QoL and individual-specific palliative care (Dennis et al, 2011; Von Roenn et
al, 2011; Janjan, 2011). Metastasized NSCLC has been the focus of the succeeding
literature (Ryn et al, 2011; Irwin et al, 2012) in addition to haematologic malignancies
that are recognized as having uniquely unpredictable and intensive care needs
(Simoens et al, 2010; Cartoni et al, 2007). While some studies have assessed palliative
outcomes for one neoplasm subgroup (Temel et al, 2010; Bergman et al, 2009;
Ceilleachair et al, 2011), there is little that assesses multiple neoplastic primary
diagnoses simultaneously, allowing comparative inferences to be made.
There is motive and logic to investigate the role of primary cancer diagnosis in the
magnitude of palliative home care burden, both financial and caregiver-related. In
addition to the unique needs of NSCLC and haematologic patients that has been
investigated, the Canadian Institute of Health Information (CIHI) recently reported that
lung and colorectal cancer patients are highly represented among deaths in acute
settings (CIHI, 2013) which are also associated with high cost (Simoens et al, 2010).
Given the CPSO’s (2002) attribution of EoL hospital admissions to caregiver burden, this
also suggests that the magnitude of burden and service use differs depending on
disease site. Disease specific care requirements may demand different levels of
commitment or complexity to be handled by unpaid caregivers in an informal setting.
Neoplasm specific Standard Operating Procedures (SOPs) for palliation have been
developed by Gaertner et al (2011) for nineteen malignancies.
1.4 Research questions and hypotheses
This thesis is focused on the following research questions:
Do primary cancer diagnoses, as defined by the ICD-10, have a determinant role in

Chapter 1: Introduction R. Redmond-Misner
7
palliative home care cost controlling for other pertinent predictors (i.e. SES, home care
agency, etc.)? and
Do primary cancer diagnoses, as defined by the ICD-10, play a determinant role in
caregiver burden controlling for other pertinent predictors (i.e. SES, home care agency,
etc.)?
Hypothesizing about CBPHC cost
Based on both existing studies and the Andersen and Newman model of health services
use (Section 3.1.3), it is expected that cost will be driven by both clinical and socio-
demographic variables. Comorbidity scores, marital status and living arrangement have
been found to be significant in societal perspective studies (Guerriere et al, 2010; Chai
et al, 2013). Differences across different diseases (cancer and other) have been found in
Enguidanos et al’s (2005) MoH perspective study. It was also found that SES, which is
indicated by education and employment status in these data, drove cost from an unpaid
caregiver perspective (Gardiner et al, 2014). Therefore, these are the variables that are
expected to show significance in the societal perspective model that integrates all of
these payers. However, when isolating the payer perspectives, there may be a
differential effect attributable to them. These covariates correspond most strongly with
Andersen and Newman’s ‘predisposing’ (i.e. demographics) and ‘need’ (i.e. comorbidity)
factors (1973).
With respect to statistical analysis of aggregated and service-specific (disaggregated)
costs of home care, it is hypothesized that:
H1: The influence of primary cancer diagnosis (need factor) on costs will be statistically
significant. (Primary)
H2: Costs will be driven by caregiver burden, which in turn will be driven by primary
cancer diagnosis. (Primary)
H3: Socio-demographic variables, or predisposing factors, will be statistically
significant, particularly SES indicators, marital status and patient living
arrangement. (Secondary)

Chapter 1: Introduction R. Redmond-Misner
8
Hypothesizing about caregiver burden
Much of the burden articulated by caregivers in the literature review is reportedly driven
by uncertainty surrounding patient-specific care tasks (Docherty et al, 2008; Parker
Oliver et al, 2014). Palliative oncologic literature suggests that these care tasks differ
from patient to patient based on primary cancer diagnosis, and therefore this variable is
expected to have a significant predictive role in caregiver burden. Time spent providing
care has been positively associated with caregiver burden (Hirdes et al, 2012) and it is
expected that the analysis will reproduce this finding. Living arrangement and marital
status have also been found to be influential; being married to or living with the patient
can especially limit opportunities for respite (Glajchen, 2012).
With respect to statistical analysis of caregiver burden scores, it is hypothesized that:
H4: The influence of primary diagnosis (need factor) in caregiver burden will be
statistically significant. (Primary)
H5: Caregiver burden will be driven by time spent providing care, which will be
determined by primary diagnosis in the analysis of unpaid caregiver cost. (Primary)
In the following chapter, a more in-depth description of the literature that informed these
hypotheses is given. This is followed by a description of the methodologies used to test
the hypotheses and the results that were derived. The results, and whether or not the
hypotheses proved to be true, will be discussed in the final chapter of the thesis. These
results will inform future research by indicating whether the inclusion of primary cancer
diagnosis adds anything to the analysis. The analyses use data collected through a
much larger project; a detailed description is contained in Section 3.1.

9
Chapter 2 Literature Review
This literature review takes a systematic approach that is thematically stratified to
capture the multi-faceted, multi-stakeholder landscape that is faced by decision-makers
with respect to the future of CBPHC. The methodology used is conducive to research
using various designs (Section 2.1). The three upcoming sections focus on 1.) the cost
of palliative home care (Section 2.2), 2.) caregiver burden (Section 2.3), and 3.)
indications from palliative oncologic research that primary diagnosis could play a role in
both cost and caregiver burden (Section 2.4).
In addition to the Andersen and Newman model that is explained in the Methodology
(Section 3.1.3), this review of the literature illuminates independent variables other than
primary diagnosis that have been found significant for dependent variables of cost and
caregiver burden. It therefore informs what to include in analytic models, as well as what
could be expected with regard to the hypotheses. These are searched separately
because they are measuring different dependent variables. The third section discusses
an independent variable: primary cancer diagnosis, and describes the existing research
base that lead to hypothesizing that it will have significant influence over these
dependent variables. Whether or not this is the case could be informative and useful to
those working in palliative care, which is very often utilized by people with cancer.
2.1 Search strategy
Overview of each section of the review
1.) Palliative home care cost (Section 2.2)
Given political and demographic contexts that favour the further development of CBPHC,
it is important to understand as many aspects of its relative cost from as many
stakeholder perspectives as possible. It can be expected that existing studies use
different methodologies and assess different aspects of cost, be it determinants of cost,
comparative cost, or standalone approximations of cost. Studies considering these

Chapter 2: Literature Review R. Redmond-Misner
10
dimensions of cost for palliative home care specifically were included. Search terms
included “palliative,” “home care,” “cost” and “community-based.” Further diversification
of terminology did not produce different or new results. Hand-searched journals included
Health Economics, Palliative Medicine and Journal of Palliative Care. Hand-searching
journals is a snowball technique used to acquire articles that were not identified through
the search by looking through journals that published other suitable articles.
2.) Caregiver burden in palliative care (Section 2.3)
Community-based health care is characterized by reliance on unpaid sources of labour
(Greffe, 2007). This is often in the form of family members with little to no training in
providing health care (Docherty et al, 2008; Parker Oliver et al, 2014). Caregiver burden
is an important consideration for CBPHC, especially if it is expanded in coming years. It
is important to understand the needs of unpaid caregivers and predictors of having a
psychologically, physically or economically detrimental caregiving experience. It can be
expected that existing studies use different methodologies and assess different aspects
and determinants of caregiver burden. Studies addressing the determinants of
psychological, physical or economic caregiver burden were included. Search terms used
included “end-of-life,” “home care,” “palliative” and “caregiver burden.” Diversifying
terminology further did not produce new findings and all articles may be found with
combinations of these search terms. Hand-searched journals included Palliative
Medicine, Journal of Palliative Care and Social Science & Medicine.
3.) Insight from palliative oncologic literature
People with cancer are the most intensive consumers of palliative home care (Alesi et al,
2011; Brink et al, 2008). In the light of recent findings that specific malignancies require
disease-specific treatment and respond differently than other cancers, particularly
NSCLC and haematologic tumours (Temel et al, 2010; Simoens et al, 2010; Tzala,
2005), improved cooperation between palliative and oncologic disciplines is occurring.
Palliative care is becoming increasingly specific and tailored to the individual patient, and
this is true for their specific primary diagnosis as well (Gaertner et al, 2011). Studies that
discussed palliative care processes specific to a disease site were included. Search
terms used included palliative, “supportive care,” “palliative care,” “cancer,” “oncology,”

Chapter 2: Literature Review R. Redmond-Misner
11
“integration” and “end-of-life.” Further diversification of terminology did not produce new
articles. Hand-searched journals included Oncology and Supportive Oncology.
Review strategy
Research on home care cost, caregiver burden and palliative oncology use variable
study designs and outcome measures, often not in the form of a randomized controlled
trial (RCT). The review reconciles the approaches taken by Docherty et al (2008),
Gardiner et al (2013) and Rodby et al (2014) to accommodate non-RCT studies.
Reviewing the literature this way involves appraising journal articles and charting the
design, sample, setting, focus, methods, outcomes, results and weaknesses of selected
studies. This allows for the inclusion of cohort, case control and qualitative studies that
may represent reality more accurately than the controlled environment created by
inclusion criteria for RCTs (external validity) (Coates, 2012) and be nuanced by
qualitative factors such as caregiver perspective. Considered articles were critically
appraised using tools created by Oxford University’s Critical Appraisal Skills Programme
(CASP) (Appendix A). This is the method by which abstracts were included or excluded.
This section discusses parts of the review process that are unanimous across subtopics,
whereas topic-specific details are held in its designated section. Databases searched
include Cochrane Library, MEDLINE, PubMed, Embase, EconLit and the Cumulative
Index to Nursing and Allied Health Literature (CINAHL) up to June 2014. Articles moved
through stages of Identification, Screening, Eligibility and Inclusion in accordance with
the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA,
2014). For each section, an initial search for systematic reviews in the Cochrane Library
took place to inform the time period component of the inclusion criteria. Various Boolean
searches were done until results were saturated with duplicates. Nothing prior to the
year 2000 is included, as prior to this was thoroughly searched and/or deemed irrelevant
(Simoens et al, 2010). All are English language articles limited to palliative home care
for adult patients, unless another setting had relevance to home care.
This review is vulnerable to several types of bias. Positive and significant findings are
more likely to be (a) published (publication bias), (b) published quickly (time lag bias), (c)
published more than once (multiple publication bias), and (d) cited (citation bias)
(Hopewell et al, 2009; Cochrane Collaboration, 2011). The articles within the review, too,

Chapter 2: Literature Review R. Redmond-Misner
12
have associated and documented biases. Non-English language publications,
commentaries, editorials, letters and special articles were not excluded from the search,
but very rarely made it to the final review.
2.2 Palliative home care cost
Two systematic reviews on this topic were found through this search. Simoens et al
(2010) searched articles from 2000-2009 focusing on the cost of palliative care in any
setting. They report many of their included studies to be relatively old, taking a hospital
perspective, and internationally variable (whether this is a limitation is up for debate).
The 2000 cut off is due to the questionable relevance and usability of older research,
and this review adopts the same cut off for this reason. Gardiner et al (2014) review the
value of home-based unpaid caregiving, searching articles from database inception to
2012. This review will focus on home-based palliative care, consider all cost
perspectives, and search from 2000-2014. Therefore, while there is a possibility for
some overlap with these reviews, there are also unsearched years and cost
perspectives that were not reached by them.
Figure 1 depicts the process by which articles were selected, culminating in eighteen
articles from thirteen journals being charted and synthesized. These include two
systematic reviews (11%), a qualitative/narrative review (5.5%) and fifteen original
studies (83%), representing 4,879 subjects (patients, caregivers, patient-caregiver dyads
or other providers) controlling for double publication. This was allowed in two instances
because the analyses were different and relevant. All cohorts are palliative but have
variable diseases. Eight countries are represented by the original studies. Thematically,
the articles produce comparative cost, specific estimates of cost or payer shares of the
cost, determinants of cost, and Lavergne et al (2011) consider the generalizability of
such results.
Discussion of whether home care was more or less costly than conventional treatment
was a common topic in the existing literature. Many of the findings are contradictory and
the methodologies are informative; it becomes apparent that the payer perspective
adopted can drastically change the results. This discrepancy is what leads to research

Chapter 2: Literature Review R. Redmond-Misner
13
findings that make this mode of palliative care delivery attractive to decision-makers and,
conversely, research findings that generate concern around sustainability and pressure
on unpaid caregivers.
Wong et al’s (2013) prospective cohort study included forty-four advanced heart failure
(HF) patients in Singapore with prognoses of less than one year between 2008-2010.
Figure 1: PRISMA flow chart for home care cost literature search
Cost reduction was defined as a decline in hospitalizations, and 71% of the patients
experienced reduced hospitalization after admission to an advanced care program
(ACP) delivered at home. This is a hospital or Ministry of Health cost perspective,
however, the additional cost of home visits and how this may counteract reductions in
hospitalization, even within this perspective, is not described.
Iden
tific
atio
n S
cree
ning
E
ligib
ility
In
clud
ed
Records identified through database searching (N=675)
Records identified through other sources (N=10)
Records after duplicates removed (N=300)
Records screened (N=300)
(N=600)
Records excluded (n=264)
(N=564)
Full-text articles assessed for eligibility (N=36)
Articles excluded (N=18)
Double publication (N=1) No applicable design (N=6) Minimal relevance (N=11)
Studies included (N=18)

Chapter 2: Literature Review R. Redmond-Misner
14
Simoens et al (2010) conducted a systematic review of the costs associated with
different palliative care settings. Findings that lead them to suggest that home care was
less costly were related to reduced hospitalizations, similarly to Wong et al (2014). They
caution that this may not be true for patients with haematological malignancies who
require frequent transfusions. While this conclusion was not the sole purpose of the
review, the data for which this particular conclusion was drawn was among the most
outdated.
Shnoor et al’s (2007) case control cohort study followed 146 patients with metastatic
cancer who lived with their families and received either conventional (N=73) or home
care (N=72) in 2003 in Israel. They were not randomized into these groups but receiving
their chosen type of care. The average cost to the health system for the last two months
of life for home and conventional care was found to be $3,467 and $12,434 ($US 2003,
average exchange to $CDN = 1.3), respectively. While the patients are matched by
disease, there is a selection bias in that patients selecting home care are opting for
palliation whilst conventional care was more focused on life-extension. This
compromises comparability and implies more intensive treatment for what is defined as
the conventional care group. The disparity in cost was tied to a difference in the number
of treatments received.
Enguidanos et al’s (2005) case control study included 159 home care recipients and 139
controls diagnosed with cancer, congestive heart failure (CHF) or chronic obstructive
pulmonary disease (COPD). Patients in the intervention group were found more likely to
die at home across all primary diagnoses and to reduce costs by approximately $5936
for people with cancer, $11,325 for people with COPD and $8,445 ($US 2001, average
exchange to $CDN = 1.5) for people with CHF. The study took place in the United
States, meaning that these costs correspond with what patients might have been billed.
This is a unique instance where the health care savings are attributable to the patient
and caregiver, however, the compensatory unpaid caregiving or out-of-pocket costs that
replaced formal services are not considered.
Cartoni et al’s (2007) cohort study included 144 patients enrolled in a specialized home
care program for haematologic malignancies between 2004-2006 in Italy. Their cost
analysis included health care providers, materials and medicines, transfusions and
laboratory (blood chemistry and microbiology). The home care costs associated with

Chapter 2: Literature Review R. Redmond-Misner
15
various stages of haematologic cancer were found to be lower than the corresponding
hospital charges.
Brumley et al’s (2007) RCT compared usual care (N=152) to usual care plus in-home
palliative care (N=145) in Colorado and Hawaii. They found the intervention group to be
more satisfied, more likely to die at home, and less likely to visit the emergency
department or be admitted to the hospital. Admissions to the emergency department or
hospital were associated with higher costs. However, new costs for the additional
services and unpaid care are not considered. There are also ethical issues surrounding
offering additional services only to some patients; many studies in this field are restricted
to case controls where the patients select their preferred treatment option for this reason
(Shnoor et al, 2007).
At this point in the review, it is notable that all studies assessing comparative cost that
fall into the “less costly” list used Ministry of Health and hospital perspectives. There is a
lack of consensus in the literature, with several studies arguing it to be more costly. The
first of which to be included here is Tzala et al’s (2005) case control study and cost-
minimization analysis that included 27 home care recipients and 25 controls with
haematologic cancers in 2002 in Greece. Interestingly, this study also adopts the
perspective of the hospital. However, home care recipients had to be more frequently
monitored for full blood count and blood cross-tests in order to proceed at home while
the hospital cohort was only tested during admission. Transfusion requirements were the
same in both groups. This does not consider the additional cost of unpaid caregiving and
is not generalizable to other palliative patients, but illuminates the potential for costly
increased surveillance in CBPHC. It is also notable for the broader thesis that the
magnitude of cost is attributed to this particular cancer diagnosis.
Ostgathe et al’s (2008) qualitative study derives cost estimates for the palliative care of
patients with NSCLC by attributing costs to the home care, hospital care and day care
projections of a team of experts. Consensus was formed among an oncologist, surgeon,
palliative specialist and radiotherapist participating on the negotiation committee of a
hospital finance department in Germany. The cost of the first and follow-up visits was the
same for all scenarios and home care was believed to reduce hospitalization. However,
home care had a higher overall estimate due to projections of longer, more frequent
visits and travel costs, even if the patients lived close by. These estimates are

Chapter 2: Literature Review R. Redmond-Misner
16
hypothetical rather than premised on empirical data, and therefore cannot actually verify
that higher appointment costs counteract reduced hospitalizations and vice versa. This is
again a hospital perspective on cost.
Jacobs et al’s (2011) prospective cohort study included 192 patient-caregiver dyads
receiving home care between 2005-2006 in five Canadian cities: Halifax, Montreal,
Winnipeg, Edmonton and Victoria. The focus of the study is the economic loss of unpaid
caregivers. They found that 9% of families incurred economic losses greater than 10% of
their pre-study income, and low-income status increased from 27-40%. It is argued that
this is a greater cost to caregivers than would be alternative palliative care settings,
however there is no control group. Some patients in the cohort had multiple unpaid
caregivers that might minimize one another’s economic burden, therefore these
estimates may be conservative. At this point in the review, it is notable that studies
presenting home care as more costly, although not always, tend to factor in unpaid
labour. This illuminates the importance of cost perspective and the significant difference
that consideration for unpaid caregivers makes in study conclusions.
Specific estimates and payer shares of cost
Specific monetary values were estimated by six studies. In addition to the estimates of
Shnoor et al (2007) ($1,733.50/month to the Israeli health system), estimates of cost or
payer shares are given by Klinger et al (2011), Guerriere et al (2010), Dumont et al
(2009), and Chai et al (2014). Guerriere et al (2010) estimate the average monthly cost
for palliative home care patients with cancer in Ontario, Canada, to be approximately
$24,549. Family caregivers account for 70% of this total. Their costing method used a
societal perspective guided by the Ambulatory Home Care Record (AHCR). Dumont et
al (2009) found the share of the cost of resource utilization by palliative home care
recipients to be 71.3%, 26.6% and 1.6% among the public health care system, families,
and not-for-profit organizations respectively. Costing was guided by the Canadian
Coordinating Office for Health Technology Assessment (HTA). This considers multiple
payers, but only goods and services that are explicitly paid for whereas the former study
incorporated the economic cost of caregiver time. Chai et al (2014), using members of
the same cohort and the same costing method as Guerriere et al (2010), estimate the
cost share among unpaid caregivers time, the Ministry of Health and out-of-pocket
expenses at proportions of 77%, 21% and 2%, respectively.

Chapter 2: Literature Review R. Redmond-Misner
17
The societal estimates are considerably higher than that produced by Klinger et al’s
(2010) hospital perspective. Klinger et al’s (2011) cohort study included Ministry of
Health cost data associated with ninety-five cancer patients over a fifteen-month period
in 2005 and 2006. Data was gathered from the Community Care Access Centre (CCAC),
Enhanced Palliative Care Team (EPCT) fee schedule and Ontario Health Insurance Plan
(OHIP) fee schedule. They found the overall cost to be $1.626 million; $17,112 per
patient and $117 per patient day. Estimates are based on a retrospective assessment of
administrative data. The Ontario Drug Benefit (ODB), out-of-pocket spending, unpaid
caregiving and emergency services are not included. This is also unable to address
variability in cost across patients.
Determinants of home care expenditures
Clinical determinants will be discussed first. Simoens et al (2010) and Cartoni et al
(2007) both identified the transfusion requirements of people living with haematologic
malignancies as a significant driver of costs. The closer monitoring of blood count and
blood tests for this population was what caused Tzala et al (2005) to deem home care
more costly than inpatient care, where patients can be less frequently tested. This is not
generalizable to all palliative care recipients or non-haematologic cancer patients, but
that affirms the research question and hypotheses. Multiple studies found expenses to
rise as the patient came closer to death (Dumont et al, 2010; Guerriere et al, 2010;
Gardiner et al, 2014). Guerriere et al (2010) found higher costs among patients with
lower physical functioning. These studies have already been synopsized here.
In terms of socio-demographic determinants, Chai et al (2013) found that the public
share of costs was significantly lower for older and married home care recipients. These
people may have more unpaid care available to them through their spouse and their
spouse may be more likely to be retired. Conversely, it was found by Guerriere et al
(2010) that, from a societal perspective, costs were higher among patients who were
living with someone. This may, too, be related to higher availability of unpaid care,
translating into higher unpaid costs.
Finally, in considering the cumulative implications of these studies, Lavergne et al’s
(2011) Canadian case control study suggests potential for selection bias in study
recruitment. This has already been alluded to in the Introduction (Section 1.2) with
respect to determinants of receiving home care at all, and is certainly relevant to this

Chapter 2: Literature Review R. Redmond-Misner
18
thesis. With the intention of assessing the generalizability of community-based program
cost estimates, Lavergne et al (2011) compared eligible participants who agreed to the
study, eligible participants who refused, the entirety of program enrollees and all cancer
decedents in the provincial cancer registry. They found that eligible and receptive
patients were generally younger, enrolled for longer, and lived closer to the palliative
care program than those who declined or were not eligible. Therefore many studies will
be vulnerable to selection bias, and many that rely on informal reporting may have recall
or social desirability biases (Guerriere et al, 2010).
Summary
Thematically, the literature available through the searched databases discussed the
comparative and actual cost of home care, payer shares of this cost and determinants of
cost. Whether home care was deemed more or less expensive than other settings was
largely dependent on the payer perspective used, with hospital and Ministry of Health
perspectives tending to find that these programs are cost saving and societal and
caregiver perspectives finding it to be more expensive. Similarly, standalone estimates
of the cost of home care were drastically different depending on which of these
perspectives was taken, with the societal estimates being considerably higher than the
ministerial ones.
Determinants of cost were found to be both clinical and socio-demographic in nature,
with certain diagnoses and patient-caregiver characteristics driving higher or lower
service utilization and cost. Enguidanos et al (2005) found cancer patients to have lower
savings than patients with heart conditions, but did not distinguish among cancer
patients. This will be controlled for in the analyses of this thesis. Lower physical function,
found to exacerbate cost by Guerriere et al (2010), will be controlled for with comorbidity
scores generated using a validated comorbidity measure (see Section 3.1.3). Marital
status and living arrangements, found to be significant by Guerriere et al (2010) and
Chai et al (2013), will be included as well. SES, illuminated by Gardiner et al’s (2014)
systematic review, will be controlled for by caregiver employment status and caregiver
and patient education levels. Finally, ethnicity was found to be significant (Gardiner et al,
2014); ethnicity, race and migration status are not in these data, indicating a weakness
of the analyses in later chapters.

Chapter 2: Literature Review R. Redmond-Misner
19
In addition to the technical weaknesses of this review outlined in the Search Strategy
(Section 2.1), there are gaps in the literature that the broader thesis will attempt to
address. This includes a dearth of literature looking at disaggregated (service-specific)
costs as opposed to aggregated public or unpaid expenses. Most studies adopt the
former Ministry of Health perspective which, too, is a weakness. The societal perspective
that is commonly endorsed for health economics research is lacking (Nuemann et al,
2009; Weinstein et al, 1996). Finally, while there is a proportionately high amount of
work focusing on cancer patients – potentially the most intensive users of palliative
home care (Alesi et al, 2011; Brink et al, 2008) – there is little that analyzes their clinical
characteristics and tumour sites comparatively or at all. The two diagnostic groups
currently represented are haematologic malignancies (Tzala et al, 2005) and NSCLC
(Temel et al, 2010). The charts for this section of the review are found in Appendix B.
2.3 Caregiver burden in palliative care
Community-based health care is characterized by reliance on unpaid sources of labour
(Greffe, 2007). This is often in the form of family members with little to no training in
providing health care (Docherty et al, 2008; Parker Oliver et al, 2014). Caregiver burden
is a weakness of CBPHC should it be expanded in coming years, thus it is important to
understand the needs of unpaid caregivers and predictors of having a psychologically,
physically or economically detrimental caregiving experience.
One systematic review on this topic was found through this search, done by Glajchen
(2012). This review drew on articles published between 1963-2011 from PubMed and
CINAHL only, focusing on the physical aspect of caregiver burden. The cut off for this
review will be the year 2000, again due to questionable relevance, and the overlap with
Glajchen’s (2012) review is justified by their narrower focus on physical outcomes only.
This review contributes consideration for psychological and economic impacts, and the
unsearched years from 2011 to 2014.
Figure 2 depicts the process by which articles were selected, culminating in eighteen
articles in fourteen journals being charted and synthesized. These include one
systematic review (5.5%) and seventeen original studies (94.5%), representing 6973

Chapter 2: Literature Review R. Redmond-Misner
20
units of patient-caregiver dyads, bereaved caregivers or other service providers
participating in caregiver burden related studies. All care was palliative, with most
patients having cancer. Eleven countries are represented by the original studies.
Thematically, the articles discuss health problems associated with caregiver burden,
unmet needs reported by caregivers, and determinants of satisfaction and burden.
Figure 2: PRISMA flow chart for caregiver burden literature search
Health problems associated with caregiver burden
Health problems associated with unpaid caregiving are first identified with Glajchen’s
(2012) systematic review of international studies considering physical health impacts of
unpaid caregiving. It was found that more than half of caregivers in these studies
reported health problems including heart problems, hypertension and arthritis. These
Iden
tific
atio
n S
cree
ning
E
ligib
ility
In
clud
ed
Records identified through database searching (N=2498)
Records identified through other sources (N=3)
Records after duplicates removed (N=~1000)
Records screened (N=~1000)
(N=600)
Records excluded (n=~971)
(N=564)
Full-text articles assessed for eligibility (N=29)
Articles excluded (N=11)
Minimal relevance/unoriginal (commentary) (N=9)
Studies included (N=18)

Chapter 2: Literature Review R. Redmond-Misner
21
issues were linked to assisting cancer patients with ADLs (eating, dressing, bathing,
etc.), instrumental ADLs (IADLs) (cooking, shopping, providing transportation, etc.), and
performing tasks formerly done by home care nurses (dispensing medication, changing
patches, monitoring symptoms, etc.). The physical health problems were driven by the
patient’s cancer stage, disability, mobility, dependency and pain. Living with the patient
was found to diminish opportunities for respite and enhance the magnitude of physical
impairment experienced by oncology caregivers.
Götze et al’s (2014) cohort study of 106 patient-caregiver dyads in Germany measured
psychological distress among caregivers using the Hospital Anxiety and Depression
Scale (HADS) and European Organization for Research and Treatment of Cancer’s
(EORTC) Quality of Life Questionnaire (QLQ C-15-PAL). They found 33% of caregivers
to have high anxiety and 28% to have depression, which was highly correlated with
patient anxiety and depression, financial burden and low social support. Spousal
caregivers tended to have the highest psychological distress.The authors caution, with
regard to the relationship with patient depression, that the HADS instrument uses
anhedonia as an indicator for depression that may not be suitable for the EoL, when this
is a very common symptom.
Grov et al’s (2006) cross-sectional analysis of ninety-six Norwegian caregivers in
palliative home care measured burden using dimensions of the Caregiver Reaction
Assessment (CRA). They assessed dimensions of family support, self-esteem, finances
and impact on daily schedule as dependent variables with a series of health measures
as independent variables. These included physical QoL, anxiety, depression and social
support. It was found that depression had the strongest relationship with these aspects
of caregiver burden, if not constituting a dimension of burden in itself. This study is
vulnerable to bias via self-selection into the study. Many declined because they were too
tired, making these findings potentially conservative.
Kenny et al’s (2010) observational study assessed the health-related QoL (HRQoL) of
178 home-based caregivers during 2005-2006 in Australia. Using a cross-sectional
survey administered to the general population, it was found that unpaid caregivers had
comparatively better physical health and worse mental health. While the mental health
finding is unsurprising and congruent with other research, the finding of better physical
health contrasts the studies that have found physical detriments to caregivers (Glajchen,

Chapter 2: Literature Review R. Redmond-Misner
22
2012). Weaknesses of this study include that that the survey is inherently retrospective
and therefore vulnerable to recall bias. Also, the cross-sectional nature of the data
inhibits them from seeing changes in health over time. While they have better health in
that static instance, longitudinal observation might illuminate more rapid deterioration
among unpaid caregivers.
Unmet needs of unpaid caregivers
The unmet needs reported by informal caregivers are first identified here with Aoun et
al’s (2005) observational study that administered surveys to twenty caregivers, six
volunteers and twenty-three service providers in Australia. Lack of information,
communication, service provision and support from community services were among the
prominent unmet needs. Caregivers wished they had learned how to comfort patients,
what to expect, how to deal with symptoms and how to acquire aids (walking frames,
wheelchairs, etc.). There is potential for selection bias that caregivers who were
particularly devoid of information were more likely to participate in this study. At this point
in the review, it is helpful for cross-chapter coherence to recall the broader research
rationale which touched on informational deficits. The care tasks and symptoms to which
caregivers are responding may differ across diagnoses and thus manifest in a different
caregiver burden.
Docherty et al’s (2008) systematic review focused on the unmet informational needs
reported by unpaid caregivers. They critically appraised the included studies in terms of
the strength of the evidence, and found the strongest evidence for pain and symptom
management informational needs. As a result, they emphasize the importance of
effective communication between patient, caregiver and service provider, and a
secondary need for welfare and social support information. The included studies were
ethnically homogenous, small-scale and largely focused on cancer patients.
Sheehy-Skeffington et al’s (2013) qualitative observational study held caregiver focus
groups in Ireland to discuss their experiences managing medications. Polypharmacy
emerged as a significant burden and the importance of vivid instructions was
emphasized. Caregivers coveted the ability to give medications as needed for symptom
control, and a lack of clinical insight was a barrier to doing this. While this is congruent
with the findings of Docherty et al (2008), it is likely that there is more to learn in terms of

Chapter 2: Literature Review R. Redmond-Misner
23
polypharmacy information deficits. With only three focus groups, this study may not have
achieved saturation. These participants also hail from a region with no specialist
inpatient palliative unit, meaning caregivers in other regions or countries may have better
access to instruction from health service providers.
Parker Oliver et al’s (2014) observational study of 146 bereaved caregivers in the United
States found similar themes during their interview process. Only thirty-eight (26%)
interviewees discussed pain and symptom management-related concerns, and their
responses were thematically analyzed. Difficulty with the administration of medications,
uncertainty about side effects and insecurity with pain assessment culminated with
frustration toward the health care team. This was related to feelings that important
aspects of caregiving, namely the responsibility of actually treating the patient, were
never explicitly communicated. Because this study was retrospective, there is potential
for recall bias. The low proportion of caregivers discussing this need does not
convincingly show it to be a prominent concern without the validation of other studies.
Ryn et al’s (2011) observational study included 677 home-based caregivers of colorectal
and lung cancer patients in the United States. The cohort responded to a self-
administered survey and those who reported providing more than 50% of informal care
to the patient were included. In addition to ADLs and IADLs, caregivers provided cancer-
specific care such as watching for treatment side effects (68%), helping manage pain,
nausea or fatigue (47%), administering medicine (34%), deciding whether to call a
doctor (30%), deciding whether medicine was needed (29%), and changing bandages
(19%). Half of caregivers reported that they did not not get the training they perceived as
necessary. Questionnaires were done approximately four months into bereavement and
responses are vulnerable to recall bias.
Determinants of caregiver burden
Service related determinants of caregiver burden or satisfaction are first identified with
Diwan et al’s (2004) observational study of 150 caregivers of palliative patients with
dementia in the United States, aimed at identifying challenges associated specifically
with dementia. Data was collected through interviews using the Caregiver Strain Index
(CSI), Revised Memory and Behaviour Problems Checklist and the Katz Index of ADLs.
Included dimensions of the CSI were role, personal and emotional. Instead of dementia

Chapter 2: Literature Review R. Redmond-Misner
24
specific struggles, it was found that perceived lack of support from the health care team
enhanced personal and emotional strain. The authors note that this was an ethnically
homogenous sample.
Guerriere et al’s (2013) prospective cohort study included 104 caregivers of CBPHC
patients in Ontario and assessed caregiver satisfaction with home-based nursing and
physician care. Interviews were conducted bi-weekly from the patient’s admission into
the program until their death, and satisfaction was assessed using the Quality of End-of-
Life Care and Satisfaction with Treatment (QUEST) questionnaire. They found that
characteristics of the service providers were significant predictors of overall satisfaction,
including “always spent enough time,” “never arrived late,” “never been hard to reach,”
“always responded quickly,” and several others. Due to small sample size, there were
limitations around including too many variables in the statistical analysis, which may
have led to omitted variable bias.
Hirdes et al’s (2012) cross-sectional analysis included 3,929 patients assessed using the
interRAI pilot from 2007-2009 in Ontario. The service related determinants of caregiver
burden and satisfaction identified through this study included the specific home care
agency, hospitalizations and nursing visits. They also identified patient and caregiver
related predictors. Patient clinical instability, depressive symptoms, cognitive impairment
and positive outlook were significantly associated with caregiver distress levels. Hours of
unpaid care also determined caregiver burden. Unfortunately, the interRAI does not
include caregiver demographics such as sex and age and the data used for this analysis
was cross-sectional rather than longitudinal. In Kenny et al’s (2010) previously described
study, they found patient symptom severity, but not caregiver time input, to be predictive
of burden.
Carlsson et al’s (2003) Swedish observational study featured 183 caregivers of patients
in home care. Caregiver questionnaires and patient medical records were analyzed.
They found that caregivers of patients who died at home, while they experienced more
sleep deprivation, felt there was a more positive impact on patient QoL than did
caregivers of patients who died in other settings. They were more satisfied with their own
achievement. Caregivers of patients dying elsewhere and with lower satisfaction
reported that patients had to leave home due to acutely developing symptoms that they

Chapter 2: Literature Review R. Redmond-Misner
25
were unable to manage. This is a retrospective study, making the reports of caregivers
vulnerable to recall bias.
Hudson et al’s (2006) prospective cohort study in Australia included 35 primary
caregivers of people with cancer receiving home care. Data were obtained at entry and a
five-week follow-up using the HADS measure of preparedness, competence, social
support, anxiety and self-efficacy. Self-reported anxiety at admission was associated
with caregivers having lower levels of psychosocial functioning five weeks later.
Therefore the baseline mental health status of informal caregivers can predict
susceptibility to caregiver burden and potentially identify vulnerable caregivers in
advance. This was a secondary analysis of existing data, thus some independent
variables of interest were not included, and this is also a particularly small sample size.
Singer et al’s (2005) case control study in Israel found that facilitating care at home
came with considerable financial and emotional burden. However, through 159
interviews with caregivers of patients with and without access to home care, it was found
that home-based caregivers were still more satisfied with their caregiving experience for
having facilitated the preference of the patient. This is congruent with the findings of
Carlsson et al (2003). There was a relatively low response rate for this study leading to
potential selection and convenience biases, and most caregivers were not spoken to
until 6 months into bereavement, leading to potential recall bias or social desirability
bias.
Wasner et al’s (2013) qualitative study with twenty-seven caregivers of patients with
malignant brain tumours in Germany assessed QoL vis-à-vis burden of care. Only eight
patient-caregiver dyads used home care, however, this diagnostic group is a novel
amidst the literature. Caregiver QoL was most determined by the burden of care, the
patient’s mental state and cognitive impairment. The sample, particularly the home care
sample (N=8), is obviously very small. Due to critical conditions, many patients were
unable to complete the HADS assessment of their mental health. This may indicate brain
cancer as a vulnerable population with high ADL and IADL needs.
Summary
In conclusion, the literature currently available through the searched databases
discusses health problems associated with caregiver burden, unmet needs reported by

Chapter 2: Literature Review R. Redmond-Misner
26
caregivers, and determinants of satisfaction and burden. Unpaid caregivers are
susceptible to worsening of their physical and mental wellbeing, though there was less of
a consensus around physical health with Kenny et al (2010) finding it better than the
general population in their cross-sectional analysis. The health of the caregiver tends to
deteriorate with that of the patient, which was found using diverse validated burden
measurement instruments (HADS, EORTC, CRA, etc.). Many of the unmet needs of
caregivers are related to information and guidance around providing care. The
heightened involvement of health professionals was among determinants of satisfaction
for caregivers. Determinants of burden were related to service utilization, patient
condition and the amount of time they spent providing care.
The findings of this review will inform variable inclusion for the analyses and illuminate
missing variables. Glajchen (2012) found disability and mobility to drive caregiver
burden, which is adequately captured by the comorbidity measure used in this thesis.
They also found that the living arrangements of patients were significant determinants of
caregiver burden, which, too, is in these data. Götze et al (2014) found marital status
influential, while Hirdes et al (2012) identified the home care agency, hours of unpaid
care and hospitalizations to be important, which are also in these data. However, patient
depression was also found to be important (Götze et al, 2014) and is not adequately
captured by the comorbidity measure. Guerriere et al (2013) found characteristics of
service providers to drive burden and satisfaction, which these data also do not have.
Gardiner et al’s (2014) paper, included in the previous section, found variability in
caregiver strain to be tied to SES and ethnicity. Carlsson et al (2003) found place of
death significant in their retrospective study of caregiver satisfaction. While these data
contain places of death, it will not be included as predictive of burden due to temporal
order; this may impact satisfaction in bereavement, as was observed by Carlsson et al
(2003), but cannot logically affect burden before death has happened as is the case with
prospectively gathered data.
Finally, in addition to the limitations outlined in the Search Strategy (Section 2.1), there
are gaps in the current literature that weaken this review. The broader thesis will attempt
to address some of these. Common weaknesses across the existing studies include
small sample size, homogenous cohorts, and a lack of longitudinal data tracking the size
and determinants of caregiver burden over the palliative trajectory (Wasner et al, 2013;
Kenny et al, 2010; Docherty et al, 2008). Three longitudinal studies were included, one

Chapter 2: Literature Review R. Redmond-Misner
27
of which only had one follow-up. While caregivers are interested in disease specific care
information, most studies do not control for primary diagnoses or thoroughly describe
their sample clinically. Rather comorbidity-type measures are used, which are inherently
secondary to the primary diagnosis. This review also brings to light the physical health
problems associated with caregiving, which the analyses found here will not be able to
speak to. The charts for this section of the review are found in Appendix C.
2.4 Neoplasm specific palliative care research
Palliative care is becoming increasingly specific and tailored to the individual patient, and
this is true for their specific primary diagnosis as well (Gaertner et al, 2011). One
systematic review on this topic was found through this search, Lester et al (2012), which
focuses on specific palliation regimens for NSCLC. A modest increase in survival is
associated with this disease specific approach based on 14 RCTs. The contribution of
these findings to this thesis is the fundamental and broad suggestion that symptoms and
palliation needs vary from malignancy to malignancy, and may therefore be influential in
predicting cost and caregiver burden. This review will consider articles discussing
malignancy-specific symptom control so as to find any traces of this ostensible gap in
the home care cost (Section 2.2) and caregiver burden (Section 2.3) literature.
Figure 3 depicts the process by which articles were selected, culminating in seven
articles in seven journals being charted and synthesized. These include one systematic
review (14%), one narrative review (14%) and five original studies (72%), representing
538 study subjects and three countries. These proportions speak to the topics’ relative
scarcity compared to the former two topics of discussion. Much of the palliative
oncologic literature has followed Temel et al’s seminal article published in 2010, thus this
research base is relatively small and currently overwhelmed by commentary and review
articles, generally written by physicians. Given that this is the case, many articles were
excluded for “No applicable design,” but some of these will be discussed. First, charted
articles will be described, all of which discuss palliative care for specific neoplasms.
Bakitas et al (2013) interviewed thirty-five oncology clinicians in the United States in their
qualitative study to gage their perspectives on caring for advanced cancer patients. They

Chapter 2: Literature Review R. Redmond-Misner
28
generally agreed with the early integration of palliative care, and identified haematologic
patients as “different” than other cancer patients due to the unpredictability and rapidity
with which symptoms can develop. It is consequently more difficult to live at home or
receive informal care from unpaid caregivers without complications and rehospitalization.
This is consistent with previous articles in this chapter and fortifies the existing literature.
Weaknesses include that the oncologists in this study work in a palliative oncologic team
setting that is very uncommon and may not representative of American oncologists
generally. They are also based in an ethnically and racially homogenous region.
Figure 3: PRISMA flow chart for palliative oncology literature search
Bukki et al’s (2013) observational study assessed symptoms and treatment intensity
over the palliative trajectory among ninety-six decedents in Germany between 2009-
2011. Forty-three had haematologic cancers and forty-nine had solid tumours while four
Iden
tific
atio
n S
cree
ning
E
ligib
ility
In
clud
ed
Records identified through database searching (N=3876)
Records identified through other sources (N=2)
Records after duplicates removed (N=2307)
Records screened (N=2307)
(N=600)
Records excluded (n=2267)
(N=564)
Full-text articles assessed for eligibility (N=40)
Articles excluded (N=33)
No applicable design (N=33)
Studies included (N=7)

Chapter 2: Literature Review R. Redmond-Misner
29
had unknown primaries. Data on the last two weeks of life were available for sixty-two
patients, of which forty-seven received aggressive EoL care and fifteen used palliative
care services. While palliative radiotherapy and antineoplastic treatments at the EoL
have been shown as helpful among the NSCLC population, they were associated with
hospital death and greater symptoms in this cohort. As a retrospective chart review, the
study may be vulnerable to assessor bias. It is also a cross-sectional analysis and small
sample. This study groups solid tumours together as is seemingly customary in existing
research.
Fauci et al’s (2012) chart review studied care utilization and reason for hospitalization
during the last six months of life among 268 American decedents with gynecologic
cancers between 2007-2010. About 58% of them received antineoplastic treatments
during the last six months of life and 81% had at least one admission to the hospital. The
most common complaint for this particular neoplastic category was gastrointestinal
complications. They were generally referred to palliative care relatively late, dying thirty
days after referral on average. Earlier referral for this population was promoted to reduce
hospitalizations. This, too, is an ethnically homogenous cohort that was analyzed via
retrospective chart review.
Gaertner et al (2011) worked with an interdisciplinary group (palliative care, oncology,
radiotherapy) to specify timing and early integration approaches to palliative care for
nineteen malignancies. The objective was to outline disease specific approaches to
palliative cancer care. SOPs were generated that outlined a disease-specific point in
each disease trajectory to initiate early integration of palliative care with disease-specific
green and red flags. Many malignancies shared metastasis as a green flag for palliation
referral, however, others do not and secondary green flags are entirely variable. While
the merits of early integration are widely accepted, these SOPs are merely suggestions
made by the authors and are not similarly widely accepted or standard procedures. They
have not been implemented, tested or validated. Notably, they do discriminate between
solid tumours rather than homogenizing them.
Lester et al’s (2012) systematic review of NSCLC-specific palliative care needs
synthesized results from 14 RCTs administering radiotherapy to the intervention group.
They did not find strong evidence supporting symptom control; conversely, they found
high dose regimens to worsen toxicity. However, they did find evidence that it extends

Chapter 2: Literature Review R. Redmond-Misner
30
survival for the patients with these higher doses. Consequently, for this particular cancer
subpopulation, it is a trade-off to consider. Focus on this treatment has followed Temel
et al’s (2010) research and contributes to that existing literature. It is included here
because it contributes to the evidencing of variability in symptom control across
malignancies, therefore justifying the inclusion of a diagnostic predictor variable.
Manitta et al’s (2010) narrative review focused on haematological cancer patients in
palliative care. Evidence suggests that these patients access palliative and home care
much less frequently. They are also more likely to die in hospital as they require many
more treatments, namely regular blood transfusions. These patients present a well-
known challenge to prognostication due to the speed at which an event may become
fatal. This literature review is non-systematic and may have assessor bias, publication
bias or English language bias.
McGrath et al’s (2007) study, too, focuses on haematologic patients in palliative care
and entailed interviews with 25 palliative care nurses. They reported need for the
integration of disease-specific palliative care in haematology. This further established the
distinction of haematologic cancers from other primary cancer diagnoses, but also
perpetuates the lack of diagnostic diversity.
Temel et al’s (2010) RCT included 151 patients with NSCLC in the United States with
palliative radiotherapy extended to randomly selected participants. The outcome was
QoL rather than life extension, as it has been in similar RCTs. QoL was measured at
baseline and week twelve using the Functional Assessment of Cancer Therapy-Lung
(FACT-L) and HADS. It was found that patients referred into early palliation had a better
QoL and were less likely to experience depression than those receiving standard care.
The study took place in a specialized tertiary care site with a group of thoracic oncologist
care providers and the patient group is ethnically and racially homogenous.
Non-original review articles
There is a plethora of review and special articles that emerged with this search that were
not conducive to the typical review process, but were considered due to lack of literature.
These articles do not present hard evidence, but the input of people working in the field
vis-à-vis the evidence that does exist.

Chapter 2: Literature Review R. Redmond-Misner
31
There is a general consensus across these articles, often written by oncologists and
other doctors, that palliative cancer patients will follow unique trajectories determined in
part by their oncologic characteristics (Von Roenn et al, 2011; Rocque et al, 2013;
Rangachari et al, 2013; Ramchandran et al, 2013; Dennis et al, 2011; Janjan, 2011;
Flechl et al, 2013). Janjan et al (2011) provides an example of pulmonary emboli (PE)
being much more common in lung cancer patients, implicating an alternative appropriate
caregiver response to the symptom of mild chest pain than could generally be advised.
Flechl et al (2013) discuss the unique symptoms associated with glioblastoma
multiforme (brain cancer), including cognitive deficits that can compromise patient ability
to communicate symptoms. One might also note that they are all relatively recent, with
the earliest belonging to the previously mentioned Oncology volume dedicated to this
topic in 2011.
Studies presenting diagnosis-specific considerations for palliative care delivery cannot
explicitly speak to cost and caregiver burden. Because it has not been explicitly studied
in the known literature, potentiality for determinacy of primary cancer diagnosis can only
be inferred by reconciling the fragmented bodies of literature presented in the three
sections. In lieu of diagnostic diversity in existing literature, the analyses in this thesis
cannot only address this gap but illuminate whether such distinctions are necessary and
informative, or if proceeding with the convention of homogenizing solid tumours is
sufficient and inconsequential. This gap in the research literature has only been
thoroughly looked into with respect to NSCLC and haematologic tumours at this point.
Finally, this analysis will not be able to address the ethnic homogeneity that is found yet
again in this review (Bakitas et al, 2013; Fauci et al, 2012; Temel et al, 2010).
The broader thesis will attempt to address some of these. Common weaknesses across
the existing studies include small sample size and samples that are both
demographically and clinically homogenous. There is disproportionate focus on
haematologic malignancies and NSCLC, though Gaertner et al (2011) illuminate need to
identify other vulnerable patient groups within cancer. Single-neoplasm studies are
useful in illuminating differences between primary diagnoses, but statistical comparative
inferences cannot be made. This study assembles a clinically diverse population in the
same program and dataset. The charts for this section of the review are found in
Appendix D.

Chapter 2: Literature Review R. Redmond-Misner
32
2.5 Summary
This literature review looked at palliative home care cost research, caregiver burden
research, and palliative oncologic research. This was done so that inferences could be
made in order to justify the analysis of primary cancer diagnosis as it impacts on cost
and caregiver burden. Also, so that it could inform the inclusion of independent variables
alongside primary cancer diagnosis in the analytic models. This will help to form the
most comprehensive possible analyses to draw inference about the role of diagnosis
from.
Variable inclusion is also guided by the Andersen and Newman model (Section 3.1.3),
which the cumulative findings of this review generally corroborate. This model
conceptualizes determinants of service use, not caregiver burden. Findings in the first
section identified ‘need factors,’ including having cancer (no distinction) (Enguidanos et
al, 2005) and lower physical function (Guerriere et al, 2010), as determinant of home
care cost. While these analyses did not include primary cancer diagnoses
(conceptualized here as the ICD-10 categories), the third section expressed differential
treatments and expectations depending on this patient characteristic (Lester et al, 2012;
Gaertner et al, 2011; Manitta et al, 2010). The analyses can speak to whether or not
such differential treatment processes result in significantly different service use and
thereby cost. ‘Predisposing factors’ were also identified as significant drivers of cost,
including marital status, living arrangement (Guerriere et al, 2010; Chai, 2013), and SES
(Gardiner et al, 2014).
The caregiver burden search also corresponded with the conceptual framework. An
‘enabling factor,’ home care agency, was found to be significant by Hirdes et al (2012).
‘Need factor’ of comorbidity and ‘predisposing factors’ of marital status and living
arrangement (Glajchen, 2012) were also found to be significant and are able to be
implemented given the data. Caregivers also reported difficulty with care tasks (Parker
Oliver et al, 2014; Docherty et al, 2008) which is where it coincides with the third section,
where research suggested that these tasks are variable depending on diagnosis (Janjan
et al, 2011; Flechl et al, 2013). One predisposing factor that is underrepresented,
potentially significant, and cannot be addressed by this study is race and ethnicity
(Temel et al, 2010; Fauci et al, 2012; Diwan et al, 2004; Docherty et al, 2008).
33
Chapter 3 Methodology
3.1 Overview of the larger study
The data used for this thesis are part of a larger study of caregiver burden over the
palliative trajectory and place of death among CBPHC patients (Guerriere, 2012). The
primary investigators are Drs. Denise Guerriere and Peter C. Coyte . Co-investigators
are Drs. Amna Husain (MD), Denise Marshal (MD), Hsien Seow (PhD), Kevin Brazil
(PhD), Eric Nauenberg (PhD) and Julie Darnay.
The study is focused largely on place of death, particularly home death (Guerriere,
2012). Shifting end-of life careand the site of death away from institutional settings to the
family home is a major part of the incentive to establish CBPHC. It is also a common
preference among patients. The study sought to identify modifiable factors that
influenced place of death among cancer patients in home care. In addition, it sought to
identify differences in resource utilization between patients dying in institutional settings
versus dying at home. Similarly to what was seen with health care cost estimates in the
literature review, the proposal evokes the importance of perspective; home death is
often associated with inherently lower cost, and this is perhaps true to the Ministry of
Health, but it may be more complex when factoring in unpaid caregiving.
The Andersen and Newman model was used to inform predictors of place of death and
therefore the data that was collected. The use of the framework by those who collected
the data is what enabled this study to have the majority of the desirable covariates be in
the data. The patients in this sample died in long-term care facilities (LTC), hospices,
hospitals or at home.
This is a prospective cohort study with data collected bi-weekly over the course of the
palliative trajectory. Patients and caregivers were recruited from Toronto’s Temmy
Latner Centre for Palliative Care at Mount Sinai Hospital and Hamilton Niagara
Haldimand Brant LHIN Community Palliative Care Teams. Collecting longitudinal data is
intended to enable assessment of cost of an entire episode of palliative care and also to
factor in the differential length of treatment, which was exhibited in the data description
(Figure 4). Caregivers recruited into the study had to be a) the primary caregiver, b)
Chapter 3: Methodology R. Redmond-Misner
34
caregiver to a patient with cancer, c) fluent in English and d) > 18 years of age. The
criteria for cancer was imposed because 85% of admissions into the program live with
cancer, and also to ensure diagnostic homogeneity (Guerriere, 2012).
Ethics approval has been gained for these data through the University of Toronto.
Standard procedures were followed to keep patients and caregivers anonymous and
encrypted in all analytic datasets.
3.2 Data
3.2.1 Data origin
Data were collected during 2011 and 2012 from caregivers of patients admitted into two
CBPHC programs in Ontario. They include the TLCPC at Mount Sinai Hospital in
Toronto and the Hamilton Niagara Haldimand Brant (HNHB) LHIN’s CBPHCT in
Hamilton.
3.2.2 Data description
Researchers collected the TLCPC and HNHB LHIN data via successive interviews
(N=1,940) with caregivers of patients (N=327) on a bi-weekly basis from admission into
the program until death. Prospective cohort studies, whilst vulnerable to social
desirability bias in caregiver reporting (Guerriere et al, 2010), are resilient against the
recall bias associated with retrospective studies (Kenny et al, 2010). Selection biases
may exist given that the data collection is contingent on willingness to partake. In Jacob
et al’s (2011) study, multiple caregivers per patient threatened to obscure and bias their
results, but this is not common in this sample.
There are both challenges and advantages with these data. The collection process is
subject to the unpredictability of the palliative trajectory; some patients exceed their
prognosis while others are in the program for a very short time. Patients enter and exit
the data at different times. Using the months or years to define time, in this context,
would be a meaningless measure. It would not tell us where any of the patients are in
their palliative trajectory. This has been addressed by using a time variable that

Chapter 3: Methodology R. Redmond-Misner
35
measures every two weeks prior to death, resulting in an unbalanced panel. This is to
say that, of forty-three time periods spanning 602 days before death, not every patient
appears in each one. Recall the distinction between EoL and palliative care that was
made in Section 1.1; some patients are in palliation long before the EoL. Figure 4 shows
the number of interviews conducted for each time period. The quantity dwindles off as
the distance from death becomes greater, which is not surprising. Ultimately, it makes
much more sense to assess costs across patients defining time this way than to
compare the costs incurred in an arbitrary month. If patients did not die or dropped out
during the study, resulting in no recorded date of death, their observations cannot be
used because the time period is not calculable.
Figure 4: Observations per time period
In light of the additional complexity associated with panel data, it also has considerable
analytic advantages in terms of robustness. One of the most common weaknesses in the
literature review were the limitations to accuracy in cross-sectional data; namely, that
they represent a static health status or other outcome (Aoun et al, 2005). It is unknown
whether associations that appear in cross-sectional analyses hold true over time, while
relationships that hold true over the palliative trajectory are more convincing. Panel
estimators and their error terms control for unobserved heterogeneity and systematic
drop out (Hill et al, 2011). The trouble with utilizing the unbalanced panel for the sake of
the time series element is that the majority of the explanatory variables are time-
invariant, categorical variables that cannot be incorporated into some conventional
050
100
150
200
250
Careg
ivers
Interv
iewed
0-14
15-28
29-42
43-56
57-70
71-84
85-98
99-11
211
3-126
127-1
4014
1-154
155-1
6816
9-182
183-1
9619
7-210
211-2
2422
5-238
239-2
5225
3-266
267-2
8028
1-294
295-3
0830
9-322
323-3
3633
7-350
351-3
6436
5-378
379-3
9239
3-406
407-4
2042
1-434
435-4
4844
9-462
462-4
7647
7-490
491-5
0450
5-518
519-5
3253
3-546
547-5
6056
1-574
575-5
8858
9-602
Time Period (Days Before Death)
Observations per Time Period

Chapter 3: Methodology R. Redmond-Misner
36
econometric models for panel data such as fixed effects (FE) regressions (Hill et al,
2011). Predictors of interest here are often socio-demographic and clinical in nature and
therefore do not change over time like the dependent variables do.
3.2.3 Variable description
Andersen and Newman model of health services utilization
The Andersen and Newman framework for the use of health services informed data and
variable collection (Andersen et al, 1973). This framework articulates three broad
determinants of health service use including a.) predisposing factors (i.e. demographics),
b.) enabling factors (i.e. community characteristics, employment) and c.) need factors
(i.e. comorbidity, illness severity) (Guerriere, 2012). As will be shown in the discussion of
the Ambulatory Home Care Record (AHCR), these costs are generated based on the
services that the patient has used in a given time period. Therefore the extrapolation of
this model onto cost is not a big jump. The Andersen and Newman model has since
been updated (Andersen, 1995), however the three main factors given here are still the
primary drivers of utilization.
a.) Predisposing factors
Predisposing factors are generally demographic and speak to the socio-cultural
characteristics that might inform service use. Data were collected for the socio-
demographic predictors established in previous research (Skinner, 2005; Motiwala,
2006; Aoun et al, 2013; Kuluski, 2010; Bainbridge et al. 2011). Sex, education, age, and
marital status were collected for all patients and caregivers. The living arrangement of
the patient, relationship of the caregiver to the patient, and caregiver burden scores were
also collected. Caregiver burden scores were generated using the Canadian Caregiver
Burden Scale in End-of-Life Care (CBS-EOLC) (Dumont et al, 2008).
b.) Enabling factors
Enabling factors are those that might enable/disable one from obtaining care, including
community characteristics, availability of services and accessibility/affordability of
services. The city of residence, which corresponds with which program the patient was
enrolled in, is a potentially explanatory community characteristic. This has been found to

Chapter 3: Methodology R. Redmond-Misner
37
be significant by Hirdes et al (2012). Covariates that may effect caregivers’ ability to
provide care include caregiver employment status, days spent caregiving overnight, and
caregiver burden scores.
c.) Need factors
Patient comorbidity and their primary cancer diagnosis were both collected. Comorbidity
scores were generated using the Charlson comorbidity index. Primary diagnoses were
coded using the WHO’s ICD-10, which provides categories that are premised on the site
of the tumour. Haematologic malignancies are not represented here, as this
categorization reflects the prominent cancer types in the sample. Table 1 gives their
composition.
Table 1: ICD-10 categories
ICD-10 Directory Patients (Obs.) Reference “Malignant neoplasms of respiratory and intrathoracic organs” (C30-39)
75 (398) Lung
“Malignant neoplasms of urinary tract” (C64-68) 17 (95) Urinary “Malignant neoplasms of digestive organs” (C15-26) 94 (432) Digestive “Malignant neoplasms of eye, brain and other parts of central nervous system” (C69-72)
14 (68) Brain
“Malignant neoplasm of breast” (C50) 33 (159) Breast “Malignant neoplasms of female genital organs” (C51-58)
22 (150) Gynecologic
“Malignant neoplasms of male genital organs” (C60-63)
18 (119) Male organs
Other 37 (241) Other
The presence of two cancer sites or an unknown primary diagnosis could complicate this
approach, but such problems were very limited. Patients with unknown primaries were
categorized as ‘other.’ Patients with multiple disease sites were rare and had multiple
disease sites in the same category, thus it did not complicate their categorization. For
example, one patient had malignancies of the pancreas and duodenum (digestive); one
had malignancies of the bladder and kidney (urinary); another had malignancies of the
bronchus and lung.

Chapter 3: Methodology R. Redmond-Misner
38
Conceptual framework for caregiver burden
Many existing conceptual frameworks for caregiver burden focus on dementia, namely
Alzheimer’s disease (Pallett, 1990; Conde-Sala, 2010). Though the conceptual
framework used by Giverns et al (2004) is largely in agreement with Alzheimer’s oriented
models such as the stress process model (Conde-Sala, 2010), it is intended for patients
with cancer. In fact, it is similar to the Andersen and Newman framework in terms of the
independent variables it prioritizes.
Given et al’s (2004) approach considers patient and caregiver characteristics as well as
patient symptom experience. It emphasizes a.) patient and family characteristics (i.e.
demographics, relationship to patient), which is also prioritized by Pallett (1990), Conde-
Sala et al (2010) and Andersen and Newman (1973); b.) ‘care situation’ or sources of
demand on the caregiver (i.e. comorbidity); and c.) ‘care process,’ which does not
correspond with the independent variables but the prospective cohort study design that
captures the longitudinal care process. Their study collected many of the same variables
assembled by the researchers who collected these data. Both a.) and b.) correspond
well with Andersen and Newman’s ‘predisposing’ and ‘need’ factors, indicating that many
of the independent variables are going to be the same with this dependent variable as
with costs. What is missing is the ‘enabling’ factors that implicate the home care agency,
however, due to the broader conceptualization of these themes on behalf of Given et al
(2004), this may be considered part of the care situation.
Ambulatory home care record
The cost of care was estimated using the AHCR (©Coyte & Guerriere 1998; Guerriere et
al, 2011), a prospective questionnaire that measures the cost of ambulatory and home-
based care from a societal perspective (Chai et al, 2013). Costs fall into categories of
public, private and unpaid care costs, shown in Table 2.
Table 2: AHCR framework for the identification of palliative care costs
Expenditure category Resource Public costs Ambulatory
All services financed by the government Healthcare professional appointments Clinic visits

Chapter 3: Methodology R. Redmond-Misner
39
Inpatient Home
Laboratory and diagnostic tests Treatment (chemotherapy and radiation) Medications Supplies and equipment Emergency room visits Hospitalizations Nursing home Hospice care Home care: nursing, personal
support/homemaking, occupational therapy, physiotherapy, oxygen therapy, diagnostic tests
Private costs Out-of-pocket Third-party insurance
All healthcare costs not publicly insured and/or financed
Healthcare professional appointments Home caregivers Travel expenses Medications Supplies and equipment Insurance payments Healthcare appointments Medications Hospitalizations Supplies and equipment
Unpaid care costs Time devoted by family, friends/neighbours to caregiving
Time lost from paid market labour Time lost from leisure/household work
(Chai et al, 2013)
Psychometric properties refer the ability of the tool to actually measure the construct of
interest consistently. The psychometric properties of the AHCR have been validated in a
CIHR-funded study focusing on adults with Cystic Fibrosis (Guerriere et al, 2006). It has
since been used in more than ten studies including respondents of diverse age, care
setting and clinical condition as well as in multiple countries (Guerriere, 2012).
Caregiver burden scale in end-of-life care
Caregiver burden was assessed using the CBS-EOLC (Dumont et al, 2008) that was
developed among Canadian caregivers of family members or friends with cancer in
palliative care (Dumont et al, 2008; Guerriere, 2012). Items in the questionnaire relate to
emotional, social and physical burden but not financial burden. Higher scores reflect
stronger caregiver agreement with a series of statements shown in Table 3.
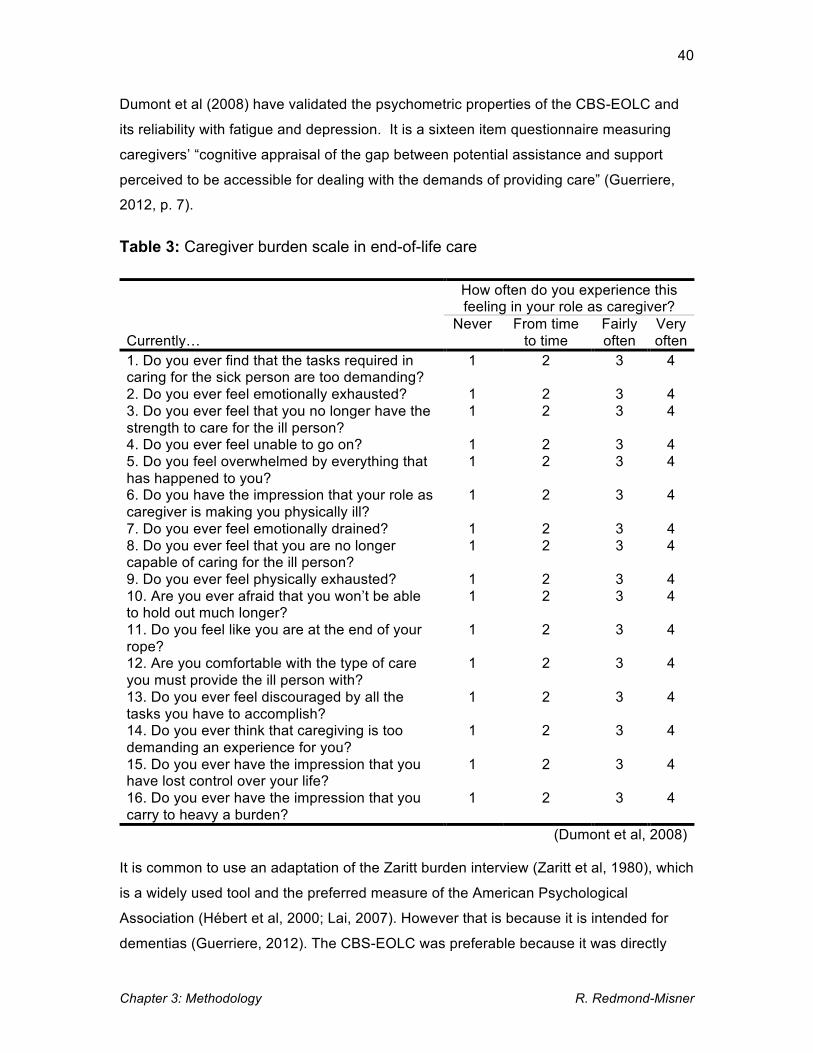
Chapter 3: Methodology R. Redmond-Misner
40
Dumont et al (2008) have validated the psychometric properties of the CBS-EOLC and
its reliability with fatigue and depression. It is a sixteen item questionnaire measuring
caregivers’ “cognitive appraisal of the gap between potential assistance and support
perceived to be accessible for dealing with the demands of providing care” (Guerriere,
2012, p. 7).
Table 3: Caregiver burden scale in end-of-life care
How often do you experience this feeling in your role as caregiver?
Currently…
Never From time to time
Fairly often
Very often
1. Do you ever find that the tasks required in caring for the sick person are too demanding?
1 2 3 4
2. Do you ever feel emotionally exhausted? 1 2 3 4 3. Do you ever feel that you no longer have the strength to care for the ill person?
1 2 3 4
4. Do you ever feel unable to go on? 1 2 3 4 5. Do you feel overwhelmed by everything that has happened to you?
1 2 3 4
6. Do you have the impression that your role as caregiver is making you physically ill?
1 2 3 4
7. Do you ever feel emotionally drained? 1 2 3 4 8. Do you ever feel that you are no longer capable of caring for the ill person?
1 2 3 4
9. Do you ever feel physically exhausted? 1 2 3 4 10. Are you ever afraid that you won’t be able to hold out much longer?
1 2 3 4
11. Do you feel like you are at the end of your rope?
1 2 3 4
12. Are you comfortable with the type of care you must provide the ill person with?
1 2 3 4
13. Do you ever feel discouraged by all the tasks you have to accomplish?
1 2 3 4
14. Do you ever think that caregiving is too demanding an experience for you?
1 2 3 4
15. Do you ever have the impression that you have lost control over your life?
1 2 3 4
16. Do you ever have the impression that you carry to heavy a burden?
1 2 3 4
(Dumont et al, 2008)
It is common to use an adaptation of the Zaritt burden interview (Zaritt et al, 1980), which
is a widely used tool and the preferred measure of the American Psychological
Association (Hébert et al, 2000; Lai, 2007). However that is because it is intended for
dementias (Guerriere, 2012). The CBS-EOLC was preferable because it was directly

Chapter 3: Methodology R. Redmond-Misner
41
applicable to this population and caregiver environment as opposed to this widely used
measure that is technically intended for dementia caregivers.
Charlson comorbidity index
The Charlson comorbidity index is a prospectively applicable tool for measuring
comorbid conditions in longitudinal studies (Charlson et al, 1987). This, too, is a
validated and widely used measure that is delineated and endorsed by the WHO
(Sundararajan et al, 2004). The index, shown in Figure 6, factors neoplastic
malignancies into the comorbidity score but attributes the same number of points to any
solid tumour, leukemia or lymphoma and any metastasized disease. Thus it does not
distinguish among primary diagnoses or measure the same thing as the categorical
diagnostic variable created using the ICD-10.
Figure 5: Charlson comorbidity index
Scoring: Comorbidity (Apply 1 point to each unless otherwise noted) 1. Myocardial Infarction 2. Congestive Heart Failure 3. Peripheral Vascular Disease 4. Cerebrovascular Disease 5. Dementia 6. COPD 7. Connective Tissue Disease 8. Peptic Ulcer Disease 9. Diabetes Mellitus (1 point uncomplicated, 2 points if end‐organ
damage) 10. Moderate to Severe Chronic Kidney Disease (2 points) 11. Hemiplegia (2 points) 12. Leukemia (2 points) 13. Malignant Lymphoma (2 points) 14. Solid Tumor (2 points, 6 points if metastatic) 15. Liver Disease (1 point mild, 3 points if moderate to severe) 16. AIDS (6 points)
Scoring: Age
1. Age <40 years: 0 points 2. Age 41‐50 years: 1 points 3. Age 51‐60 years: 2 points 4. Age 61‐70 years: 3 points 5. Age 71‐80 years: 4 points
Source: http://www.uroweb.org/fileadmin/livesurgery/Charlson_Comorbidity_Index.pdf……..

Chapter 3: Methodology R. Redmond-Misner
42
The points attributed to each condition in Figure 6 can be used to calculate comorbidity
scores that reflect the extent to which the patient has comorbid conditions, but also to
calculate life expectancy (Sundararajan et al, 2004). That is not how it is used here. It is
used as the formerly described representation of comorbidity severity and predictor of
costs and caregiver burden vis-à-vis the conceptual frameworks that posit its potential
role in both. It has been used this way in similar studies (Guerriere et al, 2010).
3.2.4 Variable assessment
Regression techniques function under the assumption that independent variables are not
collinear (Hill et al, 2011). In addition to the literature review and conceptual frameworks,
independent variable inclusion will be guided by a series of tests to derive correlation
coefficients. Correlation matrices were generated using Pearson’s correlation coefficient
for continuous variables (detailed description: Appendix E), phi coefficients for binaries
(detailed description: Appendix F), Cramér’s V test for association between nominal
variables (Appendix F), and polychoric coefficients for correlation between continuous,
ordered and binary variables (see Ekström, 2008). Results were used to inform
inclusion/exclusion of independent variables in the econometric models.
These correlation coefficients have all originated with the work of Pearson (1900; 1907;
1913; Ekström, 2008). While they are calculated differently, they are interpreted the
same way (Sanyal et al, 2009). For all of these correlation coefficients, -0.3 to 0.3 is
considered indicative of little or no association, -/+0.3 to -/+0.7 is considered weak
association, and -/+0.8 to -/+1.0 is considered a strong association (Sanyal et al, 2009).
3.2.5 Variable inclusion
Collinearity testing informed which variables were included in the final models. All
correlation coefficients outlined in Section 3.1.4 (phi, Cramér’s V, Pearson, polychoric)
are reported in Appendix G. While some authors have expressed acceptability for
correlations as strong as 0.7 (Sanyal et al, 2009), coefficients greater than 0.35 were
generally excluded. This was the case for patient and caregiver sex (phi=-0.5412);
patient living arrangement and marital status (Cramér’s V=0.5757); patient marital status
and caregiver relationship to the patient (Cramér’s V=0.5691); caregiver relationship to
the patient and patient living arrangement (Cramér’s V=0.5209); ministerial cost and

Chapter 3: Methodology R. Redmond-Misner
43
emergency room visits (polychoric=0.4802); societal cost and emergency room visits
(polychoric=0.4017); hospitalization and emergency room visits (polychoric=0.6509); and
caregiver days overnight and hospitalization (polychoric=0.7773). All aggregated costs
were highly correlated, as can be expected (polychoric & Pearson > 0.7). The
independent variables in the final models do not exceed correlation coefficients of 0.35.
Several data generating processes with different combinations of correlatively safe
independent variables were assessed for higher R2 values. These values indicate the
proportion of variability in the data that the model can explain (Hill et al, 2011). The
combination that consistently produced higher R2 values included site (Toronto or
Hamilton), patient age (and a quadratic form, patient age squared), comorbidity score,
caregiver education, patient education, caregiver employment, ICD-10 category, patient
living arrangement and caregiver sex. Most of these had correlation coefficients < 0.3,
but patient living arrangement was chosen at the expense of relationship to the patient
and caregiver sex is included at the expense of patient sex, with which they were highly
collinear and only one could be included at a time. Caregiver burden scores will be
included as a predictor in the cost regressions and time-spent caregiving will be included
as a predictor of caregiver burden scores.
3.2.6 Categorical variable interpretation and baseline
Many of the independent variables are categorical. These covariates are incorporated
into linear regressions using dummy coding, 1 if the condition is true and 0 otherwise.
The interpretation of the results, specifically beta coefficients (βx), is different from
continuous variables wherein the direction the relationship with the dependent variable is
expressed (Hill et al, 2011). For categorical variables, coefficients express the difference
in means for the indicated subgroup, and ‘otherwise’. If the coefficient for caregiver sex
were negative for male caregivers in a regression on out-of-pocket cost, it would suggest
that their out-of-pocket expenses were lower than their female caregiver counterparts.
For non-binary categorical variables, a dummy variable is created for each condition and
one category is excluded to avoid perfect multicollinearity. The excluded category
essentially serves as a baseline to compare other categories to the way that male was
just interpreted vis-à-vis female. The baseline categories for the categorical independent
variables are shown in Table 4.

Chapter 3: Methodology R. Redmond-Misner
44
Table 4: Categorical variable baselines
Variable Baseline Site Toronto Caregiver education High school Caregiver employment Retired Primary diagnosis Lung Patient education High school Caregiver sex Female Patient living arrangement With spouse
3.3 Descriptive statistics
Descriptive statistics (frequencies) were generated in Stata 13 (StataCorp, 2013) for
demographic characteristics of both patients and caregivers.
3.4 Cost analyses
3.4.1 Logarithmic transformation and quadratic forms
Financial variables are often positively skewed or heteroskedastic due to a lack of non-
negative values (Hill et al, 2011; Frees 2010; Manning et al, 2001). Logarithmic
transformation is used to normalize the distribution of the dependent variable, thus
satisfying the distributional assumption and ensuring the best linear unbiased estimators
(BLUE) (Hill et al, 20111; Manning et al, 2001). This method is easily applicable to the
aggregated costs, which do not contain zeros.
Frequently, cost variables will contain zeros that are problematic for the truncation of the
variable via logarithmic transformation. Given how the logarithm is calculated, it cannot
be practically used for zero or negative values. In national-level databases, for example
the Medicare reimbursement data used by Beeuwkes Buntin et al (2003), many people
will not have received any reimbursement ($0.00). This skews the data but these
observations are also dropped by logarithmic transformation. This will become a

Chapter 3: Methodology R. Redmond-Misner
45
prominent consideration in the modeling of disaggregated costs that do contain zeros in
Section 3.3.3.
Although lines of fit are straight, forms with log, quadratic or cubic transformed variables
have a different slope at every point (Hill et al, 2011). This changes how the output is
interpreted. In log-log regression output, the βx parameter reflects the elasticity of y to x
rather than slope (Hill et al, 2011). In a linear-log model, the slope is βx/y, meaning that
the slope declines or becomes less steep as y increases. Log-linear models, like the
ones in this thesis, exhibit the inverse. If βx > 0, the slope becomes steeper as y
increases (Hill et al, 2011).
In discussing the linearizing of potentially nonlinear components of the data generating
process, it is also notable that a quadratic form will be included for any age used as an
independent variable. Quadratic forms represent curvilinear relationships. The direction
that age drives many variables, such as income or health status, can peak and decline
as age grows rather than following a consistent +/- causal trajectory (Hill et al, 2011).
This nonlinearity can be addressed by using a polynomial model with a quadratic form,
age squared, in addition to age. This is conventional practice, though it may be a more
contestable assumption in the context of palliative or EoL care given that it has been
shown that costs rise as death approaches (i.e. as age rises) (Guerriere et al, 2010) and
patients are often not in the sample long enough for their age to change. However, such
a peak and decline may exist across patients.
3.4.2 Aggregated costs
Payer perspectives
The literature review revealed considerable disagreement surrounding the cost of home
care that was seemingly rooted in the payer perspective adopted by the author. The
AHCR is conducive to observing these mutually exclusive perspectives independently as
well as accumulatively, representing a societal perspective that acknowledges cost
irrespective of payer. The direction and magnitude of determinacy attributable to the
independent variables – particularly the variable of interest, primary diagnosis – may
differ depending on payer. Aggregated costs will be analyzed from the perspective of the
a.) Ministry of Health, b.) unpaid caregivers, and c.) society. This can also illuminate the
branch of societal costs driving the coefficients from that data generating process.

Chapter 3: Methodology R. Redmond-Misner
46
a.) Ministry of Health perspective
This dependent variable constitutes aggregated components of the public cost of home
care vis-à-vis the AHCR (Table 4), including healthcare professional appointments, clinic
visits, laboratory and diagnostic tests, treatment (chemotherapy and radiation),
medications, supplies and equipment, emergency room visits, hospitalizations, nursing
home and hospice care, home care nursing, personal support and homemaking,
occupational therapy, physiotherapy and oxygen therapy (Chai et al, 2013). These costs
were generated using fee-for-service rates for physician and laboratory costs; Toronto
CCAC rates for home-based provider services; the Ontario Drug Benefit (ODB) for
medication costs.
b.) Unpaid caregiver perspective
This dependent variable constitutes aggregated components of the unpaid cost of home
care vis-à-vis the AHCR (Table 4). This includes time devoted by the primary caregiver
to caregiving, time lost from paid market labour and time lost from leisure and household
work. It will also include the out-of-pocket spending on behalf of unpaid caregivers
(travel expenses, medications, supplies etc.). Time losses were valued using the human
capital approach, which takes the average earning by age and gender to value the time
withdrawn from leisure and work (Guerriere, 2012; Rice, 1989).
c.) Societal perspective
This dependent variable aggregates all components of the AHCR (public, private [i.e.
third-party insurance], and unpaid care) (Table 4). These were collected bi-weekly.
Estimator
The advantage of panel over cross-sectional data is the potential to observe the
dependent and independent variables over time, within- and between-individuals (Hill et
al, 2011). Cross-sectional multiple regression analysis summarizes the data generating
process as:
(ln)yi = β0 + β1x1 + β2x2 + … βnxn + 𝜀i. (1)
Chapter 3: Methodology R. Redmond-Misner
47
The dependent variable, (ln)yi, is estimated as a function of the y-intercept or constant
term, β0, the beta coefficients (βn) and values for each independent variable (xn), and an
error term accounting for unobservable noise, 𝜀i.
In the context of this study, we are interested in how x (particularly cancer diagnosis)
effects y across individuals in each group. We want to know how the patients in each
subgroup differ from patients in other subgroups as opposed to how each patient differs
from each other patient. This is permitted by the random effects (RE) model, which
accounts for unit variance, 𝜇i, outside of and in addition to the error term, 𝜀it. RE may be
written as:
(ln)yit = β̂0 + β1x1it + β2x2it + … βnxnit + 𝜀it + 𝜇i, (2)
stratifying the observations for (ln)y and xn by time series, t, in addition to cross-
sectional, i, elements (Hill et al, 2011). When estimating the effect of x on y in the fixed
effects (FE) model, variance over time is examined within individual units rather than
among or between them (Hill et al, 2011). The coefficient estimates are based on
changes in y and x over time within each person, thus the FE estimator cannot generate
estimates for variables that are time-invariant within individuals (Hill et al, 2011). This
can be considered an advantage in some contexts, but would be detrimental in the
context of wanting to observe the determinacy of variables that are heterogeneous
across the sample, but invariant on the unit level (i.e. most demographic variables). This
is the case for these analyses, where the RE estimator is strongly preferred.
However, one does not simply use the RE estimator due to one of its fundamental
assumptions: that the individual random effect and explanatory variables are
independent. Unobserved individual characteristics are captured by the error
component, 𝜇i, if not explicitly accounted for in the regression. If these uncontrolled
characteristics are correlated with the variables in the regression, it violates the
assumption that cov(𝜇i, xnit) = 0 (Hill et al, 2011). FE does not assume this, meaning that
that estimator is consistent whether or not a correlation exists. If the correlation does not
exist, however, the RE estimator is consistent and more efficient (Hill et al, 2011). This
is evaluated using the Hausman test (Section 3.5.1). This test is done by storing and
comparing the estimates from RE and FE models, so both must be run to evaluate the
robustness of RE. In the event that RE rejects the null hypothesis of the Hausman test

Chapter 3: Methodology R. Redmond-Misner
48
(that RE and FE estimates do not differ), both results will be presented alongside a
modification outlined by Allison (2009) (Section 3.5.2).
3.4.3 Disaggregated cost
Estimator
This section looks at selected service-specific costs for the same logic of dividing cost
perspectives: to assess use of more specific services and better illuminate what might
drive the coefficients in aggregated cost analysis, namely the Ministry of Health
aggregate. This demonstrates a more vivid relationship between independent variables
and more tangible sources of spending. The unpaid arm is clearly associated with
unpaid caregiving time, while the Ministry of Health expenses are spread across a
plethora of services. Hospitalization, publicly financed home appointments and publicly
provided medications will be dependent variables. The former two, in the literature
review, were regarded as costly enough to independently determine the cost-
effectiveness of home care (Ostgathe et al, 2008; Wong et al, 2013).
Cost variables with heavy right-tails and a spike of zero values were alluded to in
Section 3.1.1 (re: logarithms). This is very common for dependent variables in health
economics and will be the case with these disaggregated costs (Beeukes Buntin et al,
2004; Neelon et al, N/A; Manning et al, 2001). This is commonly dealt with using two-
part or frequency-severity models in both health and actuarial sciences (Frees, 2010).
This approach analyzes any usage,
𝑦!" =1 𝑖𝑓 𝑦!" > 00 𝑖𝑓 𝑦!" = 0 , (3)
and its probability using probit or logit links (Part 1) separately from variability in the
costs greater than zero (Part 2):
𝑦!" = 𝑚!" 𝑖𝑓 𝑦!" > 0 . 𝑖𝑓 𝑦!" = 0 . (4)
Part 2 uses generalized linear models (GLM) on raw-scale cost or OLS (in this case,
generalized least squares [GLS] for panel data) on log-scale cost (Beeukes Buntin et al,

Chapter 3: Methodology R. Redmond-Misner
49
2004). The probability of any cost, 𝑃𝑟𝑜𝑏(𝑦 > 0), and what the patient is expected to
incur, 𝐸(𝑦|𝑦 > 0), can theoretically give the overall expectation of y accommodating the
zeros:
𝐸 𝑦 𝑥 = 𝑃𝑟𝑜𝑏 𝑦 > 0 ∗ 𝐸 𝑦 𝑦 > 0 . (5)
There are compelling reasons for selecting this method, which gives each part
independent and useful meaning. Cragg (1971) first used a two-part model with differing
independent variables in each part, and the usefulness of this aspect was extrapolated
onto health care data by Mullahy (1998). Using tobit models that have a single latent
variable and the same predictors has been problematized because the decision to
consume a service may be generated differently than the magnitude of consumption.
This argument is based on the principal-agent model, which conceptualizes Part 1 as
representative of patient (principal) choice to seek health services, and Part 2 as
representative of the frequency of visits that is determined by the health professional
(agent) (Mora et al, 2013).
Longitudinal two-part models appear infrequently in the literature but simply augment
traditional two-part form with corresponding panel models. Olsen & Schafer (2001) and
Liu et al (2011) employed RE logit links in the first part and GLMs in the second part.
Mora et al (2013) use a RE probit for the first part followed by a GLM panel regression
on raw scale cost > 0, and determine the appropriate link and distribution functions (i.e.
gamma, Poisson or Guassian) using the Park (1966) test (2013). The use of GLMs is
common because they analyze the raw-scale cost, and there are notable concerns
about retransforming to original scale in log-linear GLS models in the presence of
heteroskedasticity. Special retransformation techniques have been offered, namely
Duan’s (1983) smearing estimator (Manning et al, 1998; Beeukes Buntin et al, 2004). In
this particular instance, obtaining the raw-scale expected value of y or coefficients is not
of interest so much as the most precise coefficients to draw conclusions about the
predictor variables and comparative determinacy of ICD-10 categories. Given this
objective, RE regression is a highly efficient and desirable estimator (Hill et al, 2011).
Available panel probit options for the first part include RE and population-averaged (PA).
These predict different population parameters for which RE is preferable (Hu et al,
1998). For example, the PA probit estimates the probability of an average married

Chapter 3: Methodology R. Redmond-Misner
50
person experiencing the outcome compared to the average unmarried person, whereas
RE estimates give the probability of the outcome for a married person compared to the
same person experiencing the outcome if not married, taking into account their other
characteristics (Neuhaus, 1992; Neuhaus et al, 1991). The RE probit model, first
specified by Heckman and Willis (1976), can be written as
𝑦!"∗ = 𝑥!"𝛽 + 𝜇! + 𝜀!" (Guilkey et al, 1993). (6)
The observed dependent variable in (3), yit, takes the value of one if the service has
been used and zero if not. 𝑦!"∗ in equation (6) denotes an unobserved latent variable
premised on yit that is linearly related to k explanatory regressors, xit. β represents k
deterministic coefficients in a k x 1 vector (Bertschek et al, 1998). xit constitutes a 1 x k
vector of explanatory variables. Similar to the RE regression explained in Section 3.3.1,
𝜇i and 𝜀!" are independent error terms controlling for effects not accounted for by
regressors; 𝜇i within individuals and 𝜀!" across individuals (Guilkey et al, 1993).
FE and RE panel regressions will be run on log-transformed costs in the second part
and a Hausman test will be conducted to test whether FE or RE is the preferred
specification. In the presence of heteroskedastic residuals or rejection of the null
hypothesis of the Hausman test, the modification proposed by Allison (2009) will be
implemented (Section 3.5.2). Cost components for analyses include those associated
specifically with hospitalization (public), medication (public), and home appointments
(public). These particular cost components were chosen due to relatively high costs
amidst the zeros (i.e. one hospitalization = $5,558), therefore representing a potentially
more strenuous expense when use does occur. Hospitalizations and public home
appointments were of particular interest in the literature review. These also demonstrate
more specific sources of cost in the Ministry of Health arm of the aggregated cost of
home care, which is dispersed over many services. There were other costs
characterized by attribute of high cost among the zeros (out-of-pocket travel, out-of-
pocket home appointments, public supplies), but they were unable to yield statistically
significant results.

Chapter 3: Methodology R. Redmond-Misner
51
3.5 Caregiver burden analysis
Estimator
Caregiver burden score is a count variable on a scale from 1-64 representing how many
aspects of caregiver burden the caregiver has reported for a given time period and how
intensely they rank them on the Likert scale in Table 3. Hausman, Hall and Griliches
established FE and RE Poisson models in 1984, extending control for unobserved
heterogeneity in panel data to count variables (Wooldridge, 2012). Linear models, when
the dependent variable only takes nonnegative integer values, is not ideal because they
tend to follow a Poisson distribution and cannot be normalized by logarithmic
transformation (Wooldridge, 2012). Therefore, a RE Poisson model will be applied to this
dependent variable. This model can handle heteroskedasticity, discrete outcomes, the
panel aspect of the data, and generates appropriate non-negative predictions
(Wooldridge, 2012). The Hausman test can be similarly applied to FE and RE estimates
to ascertain the reliability of RE, which is preferable for the inclusion of time-invariant
observations within individuals.
The model is structured as
𝑦!"|𝒙! , 𝑐!~𝑃𝑜𝑖𝑠𝑠𝑜𝑛[𝑐!𝑚 𝒙!" ,𝜷! ] (Wooldridge, 2012), (7)
where yit is the dependent variable, 𝒙! is the observed explanatory variables (1 x k
vector), 𝑐! is the unobserved and time constant effect and 𝑚 𝒙!" ,𝜷! is the model for the
conditional mean (𝜷! is a k x 1 vector of parameters). An alternative but similar model
would be the RE negative binomial model. The negative binomial model can relax the
distributional assumption of Poisson (mean = variance) in the case that the dependent
variable is over-dispersed (Wooldridge, 2012). Both models were explored but results
did not differ.

Chapter 3: Methodology R. Redmond-Misner
52
3.6 Diagnostics
3.6.1 Hausman test
To ensure the RE model is consistent, the Hausman test will be applied to the estimates
from FE and RE versions of each regression. This tests the null hypothesis, H0, that 𝜇i
are independent from the independent variables, with rejection of H0 indicating the
alternative hypothesis, Ha, that 𝜇i are correlated with independent variables. It does this
by comparing the parameters from the FE and RE models.
The catch is that, irrespective of the Hausman test results, the FE estimator is
completely undesirable for the purpose of this thesis. Hausman is a notoriously sensitive
test that will reject the null hypothesis for any reason that causes the coefficients from
RE and FE models to differ (Wooldridge, 2012). Considering that the preliminary FE
estimatation will drop many of the independent variables, it is expected that the
Hausman test will reject in some instances, even if it is attributable to an artificial
exaggeration of coefficient differences induced by different groups of independent
variables (and consequently, degrees of freedom) in each model. This dilemma has
been acknowledged and analyzed extensively by Allison (2009), who has proposed
redeeming modifications to RE model specification.
3.6.2 Allison’s hybrid method
Allison’s hybrid method is a slight modification to RE specification. It is simply the
implementation of RE with the mean and deviation from the mean of time-varying
covariates entered as separate independent variables.
The RE and FE models differ with respect to their use of between- and within-person
variability. Premising coefficients on within-individual variability is what prevents the FE
model from generating estimates for time-invariant covariates with no within-individual
variability; their deviations from the mean will be zero. RE estimates on time-varying
variables are a weighted average of “within” and “between” coefficients. Recall equation
(2) for RE, and observe the structure of FE:
(ln)yit = β0i + β1x1it + β2x2it + … βnxnit + 𝜀it. (8)

Chapter 3: Methodology R. Redmond-Misner
53
all intercepts, β0i, are different for individuals and the coefficients, βn, are constant (Hill et
al, 2011). Individual intercepts are included to “control” for individual-specific covariates
that do not change over time, thus there is no term for unit variance, negating the
assumption that cov(𝜇i, xnit) = 0. This makes FE more consistent than RE, with RE’s
consistency being compromised by violation of that assumption. If the correlation does
not exist, however, the RE estimator is consistent and more efficient (Hill et al, 2011).
Failure of the Hausman test can be an instance when FE would be preferable to RE, or
alternatively, if the researcher wants to drop all time-invariant covariates (both observed
and unobserved). However, in the case that time-invariant covariates are important, the
Hausman test rejected, and pooled cross-sections are highly undesirable, Allison’s
hybrid method can be used to generate FE-type estimates (that are robust to cov(𝜇i, xnit)
≠ 0). It also provides ways to infer whether or not the estimates are being really affected
or altered by presenting the results alongside RE and FE.
Allison’s (2009) hybrid method involves separating within- from between-person
variation in the RE model by subtracting individual-specific means from the time-varying
covariates to obtain their deviations from the mean, as well as including the means as
explanatory variables. Because putting the data in deviation form is part of FE
estimation, this gives the best of both worlds: obtaining FE-type estimates for time-
varying covariates, which are cleansed of all time-invariant variables (observed and
unobserved), while still obtaining estimates on the time-invariant ones (Allison, 2009).
The variation across individuals is being controlled for by the individual-specific means
(Allison, 2009). The deviation coefficients can be interpreted as if they were FE
coefficients.
By including the time-invariant, individual-specific means and time-varying deviations
from the mean in the RE specification, you can make inferences from the coefficients.
The coefficients on the FE-type RE estimates in the hybrid model and the actual FE
estimates should be identical in balanced panels. In unbalanced panels, they won’t be
identical, but they should be similar (Allison, 2009). Similarity between these FE-type RE
estimates and actual FE estimates indicates that RE is behaving despite having failed
the Hausman test.
Whether or not RE is appropriate can also be evaluated by looking at the congruency
between the deviation and mean variables in the hybrid regression. The coefficients on

Chapter 3: Methodology R. Redmond-Misner
54
the mean and deviation should be similar if the assumptions of the RE model are
correct, namely that 𝜇i, is uncorrelated with xnit (Allison, 2009). When the coefficients on
the mean and deviation of the time-varying covariates are substantially different, it offers
insight into the appropriateness of a standard RE model.
In conclusion, Allison’s hybrid model offers reliable estimates on all of the independent
variables that allows one to circumvent some of the challenges associated with the RE
and FE models. The challenge with the RE model is meeting its assumption that 𝜇i is
uncorrelated with xnit, the violation of which compromises the consistently of the results.
When this assumption is violated, one would typically resort to FE. The challenge with
FE is that it only considers within-individual variability, and consequently drops all time-
invariant variables. It does not consider variance across-individuals which is undesirable
as well. Therefore, the Allison hybrid approach seems to represent an appropriate
alternative approach to estimation. The algorithm that decides whether or not Allison’s
hybrid method is required is shown in Figure 6.
Figure 6: Algorithm for deciding which estimator(s) to use
If the RE model passes the Hausman test thus satisfying important assumptions and
being the most efficient estimator, no modifications will be made to model specification
and only RE results will be reported. If the Hausman test rejects the null hypothesis, RE
estimates will be presented alongside Allison’s hybrid and FE estimates.
3.6.3 Standard diagnostics
In addition to logarithmic transformations intended to correct heteroskedasticity, the
panel/cluster-robust standard error estimator will be applied to the final models.
Run Hausman test
Accept Reject
Report robust RE regression estimates
Report robust RE, FE and hybrid estimates
Run RE and FE regressions

Chapter 3: Methodology R. Redmond-Misner
55
The robust models will undergo the Breusch and Pagan Lagrangian multiplier test for
random effects. While the Hausman test assesses the reliability of RE, this tests the
appropriateness of RE. The H0 of this test is that there is no difference across units
(patients) or no “panel effect” (Torres-Reyna, 2007). Rejecting this hypothesis validates
the appropriateness of a panel regression for these data, whereas accepting the null
suggests that a cross-sectional ordinary least squares (OLS) or pooled regression would
suffice and yield similar results (Torres-Reyna, 2007).
3.7 Summary
This chapter has discussed the independent and dependent variables, conceptual
frameworks, and analytic estimators that will be applied to the data. The independent
variables will generally adhere to socio-demographic, clinical, and service/community-
related predictors. This has been informed by the literature, the Andersen and Newman
framework, and the caregiver burden framework used by Given et al (2004).
The following chapter will reveal how these predictors determine cost from three payer
perspectives: societal, Ministry of Health, and informal caregiver. In addition, service
specific costs will be analyzed using two-part models to see if further variation emerges
and potentially illuminate relationships between different independent variables and
different components of the costs associated with CBPHC. Hospitalization, public
medication, and public home appointments will be looked at. Finally, their influence over
caregiver burden will be analyzed.

56
Chapter 4 Results
The results section will discuss the socio-demographic characteristics of the sample
followed by the results of the analyses and diagnostics described in Chapter 3. Chapter
3 also explained the conceptual frameworks used to identify important independent
variables, with one of the most consistent determinants in the generation of costs and
burden being ‘need’ factors related to symptom severity and clinical characteristics
(Andersen & Newman, 1973; Givens, 2004). This brings us back to the focus of the
thesis which concerns the role of the primary cancer diagnoses as outlined by the ICD-
10 diagnostic codes, which distinguishes among tumour sites (i.e. breast, brain) as
opposed to tumour types (i.e. carcinoma, sarcoma), in determining cost and burden.
This chapter presents findings from analyses of a) aggregate costs of CBPHC from three
stakeholder perspectives (society, the Ministry of Health, and unpaid caregivers)
(Section 4.2.1), b) service-specific public costs associated with CBPHC (medication,
hospitalization, home appointments) (Section 4.2.2), and c) caregiver burden scores
generated using the CBS-EOLC (Dumont et al, 2008) (Section 4.2). Intrathoracic
(primarily lung) cancers served as the baseline category for the ICD-10 variable.
4.1 Descriptive statistics
As mentioned in the data description section (Section 3.1.2), there was an attrition rate
of 4.6% (N=15) related to dropout or outliving the study period. The time periods are
based on the date of death, which prohibited the calculation of time periods and
integration into the analysis for those who dropped out or outlived the study. Table 4
reports descriptive data on 312 of 327 patients and their primary caregivers who
remained in the study through their palliative trajectory.
The socio-demographic composition of the cohort is consistent with and evocative of
some of the trends outlined by Seow (2009) and Jiwani (2003). Spouses (46.8%) and
children (40.6%) of the patient constituted an overwhelming proportion of the unpaid
caregivers. These sources of unpaid labour may decline in coming years due to an
abating propensity to rear children and fewer opportunities for spouses to retire.

Chapter 4: Results R. Redmond-Misner
57
Prospects for retirement among Ontario’s population are stagnating as incomes have not
grown with the cost of living (Yalnizyan, 2007). With that said, being retired was the most
common employment status among caregivers (35.8%), followed by full-time work
(30.2%). Most dyads were from Toronto (66%). The majority (52%) of patients had an
educational level of high school or less, while most caregivers had a post-secondary
education. The sex distribution of the patients was virtually equal, but the majority of
caregivers were women (64.5%). Caregivers were generally younger than the patients;
the average age was 58 for caregivers (range: 20-94) and 71 for patients (range: 27-96).
Diverse living arrangements are represented in these data. Living with a spouse was by
far the most common (59%), and the proportion living with children (16.3%) indicates
that most patients who received unpaid care from their children did not actually live with
them. Only 16.7% of patients lived alone, which is an underrepresented group in home
care and therefore in existing research (Aoun et al, 2013).
Table 5: Summary of patient and caregiver demographics
Demographic Characteristics
Patients (N=312) Caregivers (N=318) N n (%) N n (%)
Sex Male Female
312 148 (47.4%) 164 (52.6%)
312 104 (33.3%) 208 (66.7%)
Education Any college High school or less Any university Post grad Missing
312 54 (17.3%)
164 (52.6%) 63 (20.2%) 31 (9.9%)
-
312 47 (15.1%) 91 (29.2%) 90 (28.8%) 52 (16.7%) 32 (10.3%)
Site Toronto Hamilton
312 206 (66%) 106 (34%)
312 206 (66%) 106 (34%)
Marital status Divorced/separated Never married Widow Married Missing
312 33 (10.6%) 10 (3.2%)
82 (26.3%) 187 (59.9%)
-
312 28 (9%)
26 (8.3%) 6 (1.9%)
243 (77.9%) 9 (2.9%)
Relation to patient Child Spouse Friend Sibling Other family Other
–
– – – – – –
312 131 (42%)
142 (45.5%) 8 (2.6%)
11 (3.5%) 2 (0.6%)
18 (5.8%)
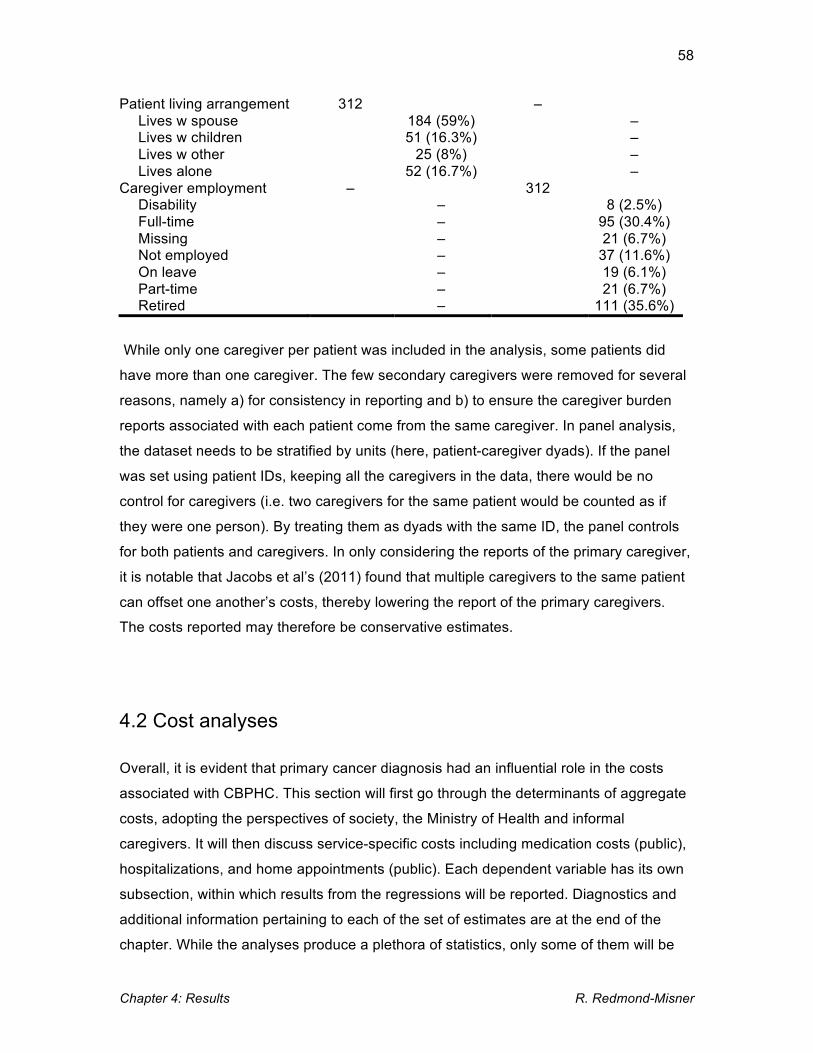
Chapter 4: Results R. Redmond-Misner
58
Patient living arrangement Lives w spouse Lives w children Lives w other Lives alone
312 184 (59%) 51 (16.3%)
25 (8%) 52 (16.7%)
– – – – –
Caregiver employment Disability Full-time Missing Not employed On leave Part-time Retired
– – – – – – – –
312 8 (2.5%)
95 (30.4%) 21 (6.7%)
37 (11.6%) 19 (6.1%) 21 (6.7%)
111 (35.6%)
While only one caregiver per patient was included in the analysis, some patients did
have more than one caregiver. The few secondary caregivers were removed for several
reasons, namely a) for consistency in reporting and b) to ensure the caregiver burden
reports associated with each patient come from the same caregiver. In panel analysis,
the dataset needs to be stratified by units (here, patient-caregiver dyads). If the panel
was set using patient IDs, keeping all the caregivers in the data, there would be no
control for caregivers (i.e. two caregivers for the same patient would be counted as if
they were one person). By treating them as dyads with the same ID, the panel controls
for both patients and caregivers. In only considering the reports of the primary caregiver,
it is notable that Jacobs et al’s (2011) found that multiple caregivers to the same patient
can offset one another’s costs, thereby lowering the report of the primary caregivers.
The costs reported may therefore be conservative estimates.
4.2 Cost analyses
Overall, it is evident that primary cancer diagnosis had an influential role in the costs
associated with CBPHC. This section will first go through the determinants of aggregate
costs, adopting the perspectives of society, the Ministry of Health and informal
caregivers. It will then discuss service-specific costs including medication costs (public),
hospitalizations, and home appointments (public). Each dependent variable has its own
subsection, within which results from the regressions will be reported. Diagnostics and
additional information pertaining to each of the set of estimates are at the end of the
chapter. While the analyses produce a plethora of statistics, only some of them will be

Chapter 4: Results R. Redmond-Misner
59
thoroughly discussed as significant or relevant to the research question and purpose.
Appendix H contains an explanation of the lesser discussed statistics reported.
A note on Hausman test results
The algorithm for selecting estimator(s) in the Methodology chapter showed that the
adopted approach is contingent on the result of the Hausman test. The Hausman test
determines whether Random Effects (RE) specification alone is sufficient, therefore
additional estimates derived from alternative specifications (Allison’s hybrid and fixed
effects(FE)) are provided when the Hausman test indicates that RE may be biased
(‘Reject’). While this is a diagnostic test, most of which will be presented at the end of
the chapter, Hausman test results precede the finalized estimations presented here to
illustrate why each approach was taken. By dependent variable, Table 6 gives the model
specifications that can be expected for each dependent variable. This is to show the
general direction for the chapter, but a fuller discussion is provided in the Diagnostics
section.
Table 6: Hausman test results, final estimator(s)
Dependent variable Accept/reject Hausman Estimation Societal perspective cost Reject (Prob > Chi2 = .0004) RE, FE, hybrid Ministy perspective cost Reject (Prob > Chi2 = .0011) RE, FE, hybrid Unpaid caregiver costs Reject (Prob > Chi2 = .0154) RE, FE, hybrid Public medication costs Accept (Prob > Chi2 = .8848) RE (two-part) Hospitalizations N/A (No FE probit) RE Probit only Public home appointment costs Accept (Prob > Chi2 = .0053) RE (two-part) Caregiver burden score Accept (Prob > Chi2 = .5030) RE Poisson
4.2.1 Aggregated costs
Societal perspective
It is apparent from the regression models reported in Table 7 (RE, FE, Allison’s hybrid)
that the brain cancer group was associated with significantly higher societal costs.
Statistically significant findings also emerged from the other covariates that were
indicated by the Andersen and Newman framework. ‘Enabling’ factors of city of
residence and days spent over night were found to be significant; lower societal costs
were found for residents of Hamilton and costs were higher when caregivers spent more

Chapter 4: Results R. Redmond-Misner
60
days overnight. Living with children was associated with higher costs, as opposed to
living with spouses (baseline), with others or alone. Caregiver burden was also strongly
significant, driving costs higher as caregiver burden increased. These results were
invariant to model specification and are therefore quite robust. The percentage of
variability accounted for by the model is given by R2 values, which are as high as 20% in
the hybrid specification.
Table 7: Determinants of societal costs of CBPHC (RE, FE & Allison’s hybrid)
Dependent Variable: (ln)Societal Cost Independent Variable RE Coef. Hybrid Coef. FE Coef. Site
Hamilton
-.1130987*
-.1816811*
Patient age Patient age2
-.0309784 .0002126
-.0329119 .0002262
Comorbidity score .0209617 .0315624 Caregiver burden
Mean Deviation
.0307182*** .0152143** .0368713***
.0368737***
Caregiver education (Baseline: < High school)
College Any university Post grad Missing
-.0650912 -.1423874 -.0727493 -.0556227
-.0787003 -.1244516 -.0474793 .0251493
Caregiver employment (Baseline: Retired)
Disability Full time Missing Not employed On leave Part time
.1227241 -.1367954 -.1463374 .0818035 .1760111 -.0689561
.0818017 -.1375489 -.0165935 .1201743 .1985637 -.0685794
Cancer type (Baseline: Intrathoracic)
Digestive organs Female organs Brain Breast Male organs Urinary tract Other
.1038947
.1606436 .4971476***
.081204 -.0930862 -.0655134 .1213257
.157179 .2164067
.5292978*** .0679875 -.0725099 -.0020805 .1528889
Patient education (Baseline: < High school)
College University Post grad
.1257612 .109098
.1064619
.1294936
.0636265
.0480916

Chapter 4: Results R. Redmond-Misner
61
Table 7 exhibits that there are few time-varying covariates in the data generation
process. The implication of few time-varying covariates is simply that, in instances where
Allison’s hybrid and FE coefficients are presented, there is little to compare between
them. The two time-varying covariates, days spent overnight and caregiver burden
scores, are where FE and Allison’s FE-type parameters (deviation) can be compared.
These results exhibit strong similarity between FE and Allison’s FE-type parameters,
which is what is being looked for in augmenting the RE estimator. Similarity
demonstrates that RE estimation is not producing drastically different results than the FE
estimation. Granted similarity between Allison’s hybrid RE and FE estimates, both the
RE and hybrid results are interpretable. Discrepancies between them can speak to the
sensitivity of the results (i.e. if a variable is significant in one specification and not in the
other).
Ministry of Health perspective
In Table 8, brain cancer emerges as a predictive characteristic for Ministry of Health
costs, as do female cancers (primarily ovarian in this sample). This suggests that brain
1 The meaning of asterisks beside coefficients will remain consistent throughout.
Caregiver sex Male
-.1136043
-.0652709
Patient living (Baseline: With spouse)
Alone With children With others
.1462281 .2662788* -.2818415
.1238164 .2649985* -.3058154
Days overnight Mean Deviation
.0776996*** .0458273** .0798558***
.0800069***
Intercept 8.794154 9.162876 7.669735 Overall R2 Between R2 Within R2 Wald Chi2 Prob > Chi2 Σe Σu Rho
.1854 (18.5%)
.1945 (19.5%)
.1258 (12.6%) 295.23
.000 .47238208 .47546074 .50324804
.1963 (19.6%)
.2067 (20.7%)
.1282 (12.8%) 264.2 .000
.47191569
.47895282
.50740033
.0807 (8%)
.0521 (5%) .1285 (12.8%)
.47238208
.62232207
.63444625 *p=<.05 **p=<.005 ***p=<.0001
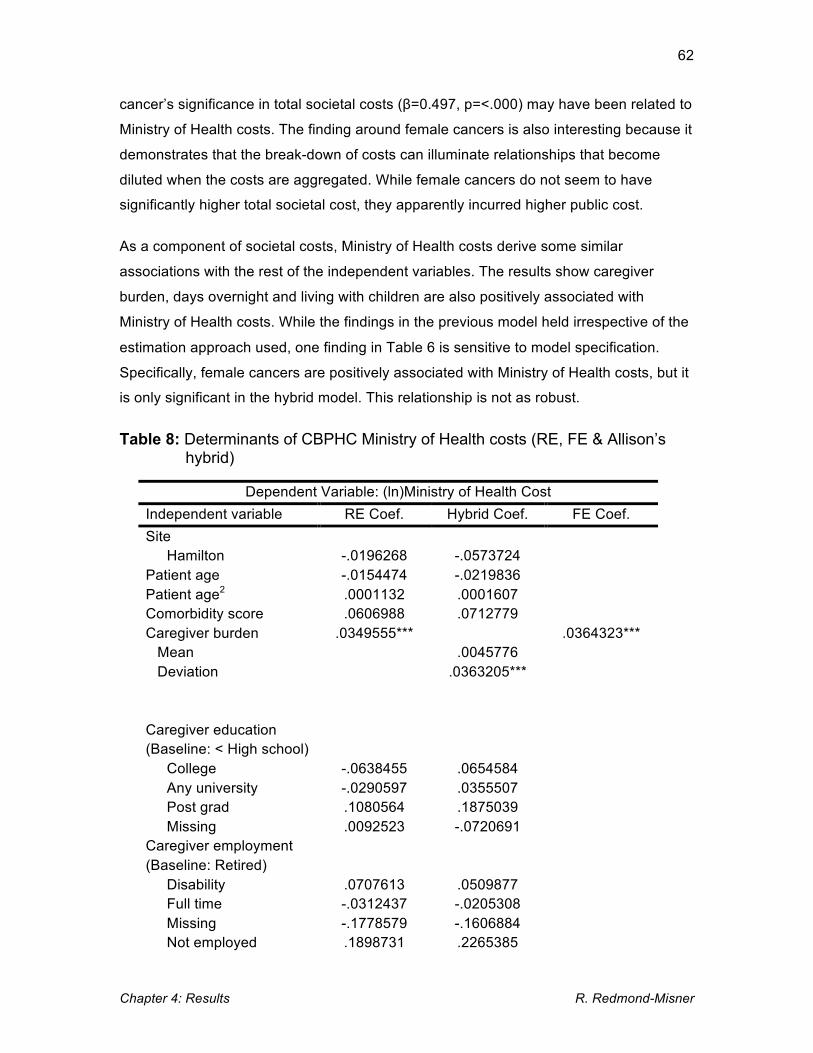
Chapter 4: Results R. Redmond-Misner
62
cancer’s significance in total societal costs (β=0.497, p=<.000) may have been related to
Ministry of Health costs. The finding around female cancers is also interesting because it
demonstrates that the break-down of costs can illuminate relationships that become
diluted when the costs are aggregated. While female cancers do not seem to have
significantly higher total societal cost, they apparently incurred higher public cost.
As a component of societal costs, Ministry of Health costs derive some similar
associations with the rest of the independent variables. The results show caregiver
burden, days overnight and living with children are also positively associated with
Ministry of Health costs. While the findings in the previous model held irrespective of the
estimation approach used, one finding in Table 6 is sensitive to model specification.
Specifically, female cancers are positively associated with Ministry of Health costs, but it
is only significant in the hybrid model. This relationship is not as robust.
Table 8: Determinants of CBPHC Ministry of Health costs (RE, FE & Allison’s hybrid)
Dependent Variable: (ln)Ministry of Health Cost Independent variable RE Coef. Hybrid Coef. FE Coef. Site
Hamilton
-.0196268
-.0573724
Patient age Patient age2
-.0154474 .0001132
-.0219836 .0001607
Comorbidity score .0606988 .0712779 Caregiver burden
Mean Deviation
.0349555*** .0045776
.0363205***
.0364323***
Caregiver education (Baseline: < High school)
College Any university Post grad Missing
-.0638455 -.0290597 .1080564 .0092523
.0654584
.0355507
.1875039 -.0720691
Caregiver employment (Baseline: Retired)
Disability Full time Missing Not employed
.0707613 -.0312437 -.1778579 .1898731
.0509877 -.0205308 -.1606884 .2265385

Chapter 4: Results R. Redmond-Misner
63
On leave Part time
.0166669 -.0059202
.0461801
.0378089 Cancer type (Baseline: Intrathoracic)
Digestive organs Female organs Brain Breast Male organs Urinary tract Other
.1543349
.2978083 .5552936*
.12887 -.0135634 .115685
.2179945
.226099 .3903798* .6255724** .1235337 .0004234 .184768
.2503838
Patient education (Baseline: < High school)
College University Post grad
.2121052
.0717804 .143288
.2279943
.0486106 .122122
Caregiver sex Male
.0017382
.0139336
Patient living (Baseline: With spouse)
Alone With children With others
.4286443* .3111334** -.0460779
.4146304* .3155617** -.0799712
Days overnight Mean Deviation
.1341513*** .1309083*** .1338707***
.1338186***
Intercept 6.50808 7.118581 6.355416 Overall R2 Between R2 Within R2 Wald Chi2 Prob > Chi2 Σe Σu Rho
.1031 (10%) .147 (14.7%) .0909 (9.1%)
336.47 .000
.69313764
.59739958
.42622137
.1311 (13%)
.1709 (17%) .0914 (9%)
185.51 .000
.69250399
.59272823 .4228326
.0402 (4%)
.0402 (4%) .0918 (9.2%)
.69313764 .7939662 .5674917
There are several differences in the determinants of Ministry of Health costs compared
to those that drove societal costs. Living alone emerged as a determinant of increased
Ministry of Health costs despite not having produced any significant determinacy in total
societal costs. While the Hamilton site was associated with lower societal costs, it was
not associated with lower Ministry of Health costs compared to the Toronto site. This
suggests that a.) while patients living alone did not have higher costs overall, a lack of
Chapter 4: Results R. Redmond-Misner
64
unpaid caregiving might mask the fact that they actually use public services more than
patients living with someone else, b.) city of residence/home care agency may be more
closely linked with unpaid caregiving costs than the costs borne by the Ministry of
Health, and c.) that different variables do affect different stakeholders differently.
Unpaid caregiver cost perspective
The results of the unpaid caregiver cost analyses are presented in Table 9. They fit
logically with the determinants of aggregated societal (Table 7) and Ministry of Health
(Table 8) costs and further illustrate the rationale for an examination of these differential
cost perspectives. The Hamilton site, which was associated with lower societal cost but
had no effect on Ministry of Health costs, was associated with lower caregiver costs than
their Torontonian counterparts. Living alone, which drove Ministry of Health costs
upwards, was negatively, but non-significantly associated with unpaid caregiver costs.
Patients living with others, who were associated with lower societal costs but had no
effect on Ministry of Health costs, were significantly associated with lower unpaid
caregiver costs. Significantly lower unpaid cost among patients living with others
suggests that less unpaid care could explain their markedly lower societal costs.
Caregivers on leave from work were associated with higher unpaid caregiver costs.
There are also consistencies across societal, Ministry of Health and unpaid caregiver
costs. In contrast to the findings discussed in the previous paragraph where Ministry of
Health and unpaid caregiver care costs were oppositely driven by certain characteristics
(i.e. living alone has a higher Ministry of Health and lower unpaid caregiver cost), some
characteristics drove expenses upward irrespective of payer. These include higher
caregiver burden, more days overnight, living with children as opposed to spouses,
others or alone, and having brain cancer as opposed to the other ICD-10 denominations
found in the sample. Driving cost unanimously upward suggests that despite being more
intensive users of public services, patients with brain cancer (primarily glioblastoma
multiforme in this sample) were also receiving more unpaid care than most people in the
program. The same is true for patients whose caregiver was experiencing high burden,
patients whose caregiver spent many days overnight, or those who lived with children.

Chapter 4: Results R. Redmond-Misner
65
Table 9: Determinants of CBPHC unpaid caregiver costs (RE, FE & Allison’s hybrid)
Dependent Variable: (ln)Unpaid Caregiver Cost Independent variable RE Coef. Hybrid Coef. FE Coef. Site
Hamilton
-.2318017*
-.2794294*
Patient age Patient age2
-.0457998 .0003089
-.0438953* .0002923*
Comorbidity score -.0033099 .0084026 Caregiver burden
Mean Deviation
.0316818*** .0158273** .0374144***
.0375295***
Caregiver education (Baseline: < High school)
College Any university Post grad Missing
-.1705292 -.2368761 -.2312876 .0007709
-.2089305 -.2503827 -2148301 .139797
Caregiver employment (Baseline: Retired)
Disability Full time Missing Not employed On leave Part time
.2261023 -.1784909 -.1874397 .0021671 .3016255* -.122424
.2074949 -.185674
-.0737118 .0445025 .3284185* -.1491987
Cancer type (Baseline: Intrathoracic)
Digestive organs Female organs Brain Breast Male organs Urinary tract Other
.0790303 .004515
.5322952** .0793724 -.1582612 -.2442645 .1138028
.1323618
.0503773 .545301** .0644224 -.1278603 -.1653247 .1638022
Patient education (Baseline: < High school)
College University Post grad
.0226484
.1078051
.0359023
.0169526
.0324579 -.0786854
Caregiver sex Male
-.1471362
-.1651238
Patient living

Chapter 4: Results R. Redmond-Misner
66
(Baseline: With spouse) Alone With children With others
-.1797427 .2795824* -.5030078*
-.2130987 .2687588
-.5258394**
Days overnight Mean Deviation
.0313074*** -.0536556* .0379052***
.0358283***
Intercept 8.996259 9.247193 6.96068 Overall R2 Between R2 Within R2 Wald Chi2 Prob > Chi2 Σe Σu Rho
.1967 (19.7%)
.1938 (19.4%) .0857 (8.6%)
1714.75 .000
.60266598
.73980838 .5298672
.1889 (18.9%) .1916 (19%) .0868 (8.7%)
193.32 .000
.60247802
.64579173
.53465727
.0688 (6.9%)
.0278 (2.8%)
.0884 (8.8%)
.60266598
.82545998
.65229791
4.2.2 Service-specific cost analysis results
Public medication costs
In order to accommodate the distribution of costs where many patients did not incur any
costs, public medication costs were analyzed using a RE probit model for the probability
of any cost (0 if no costs were incurred, 1 otherwise) and RE generalized least squares
(GLS) regression to assess costs greater than zero. Publicly financed medications were
received by 242 (77.5%) patients at some point in their palliative trajectory. The bi-
weekly cost ranged from $0 to $5,200 and had an average of $119. The results are
sparse in terms of statistically significant findings, and are given in Table 10.
Cancers of the digestive and gynecologic organs reduced the probability of receiving any
medication, while patients with the highest level of education were associated with
significantly higher medication costs when costs were incurred. Cancer diagnosis has
been a consistent determinant in the analyses, though there is now variability in which
category is significant and in what direction. The most consistent diagnostic driver so far,
brain cancer, is not significant here. This lack of effect suggests that medications are not
behind brain cancer patient’s elevated public cost.

Chapter 4: Results R. Redmond-Misner
67
Table 10: Determinants of receiving any medications and their cost (RE probit and GLS)
Dependent Variable
Any cost incurred (binary)
(ln)Public medication cost > 0
Independent variable RE Probit RE GLS Site
Hamilton
-.1470933
-.0689471 Patient age Patient age2
.0764394 -.0004008
.0126442 -.0001443
Comorbidity score -.0434624 .0146193 Caregiver burden .0045518 .0105105 Caregiver education (Baseline: < High school)
College Any university Post grad Missing
-.0119788 -.1857371 .2453136 .4181955
.2915087
.0689206
.2084064
.2224894 Caregiver employment (Baseline: Retired)
Disability Full time Missing Not employed On leave Part time
.8117905
.2977489 -.3998645 .3976619 -.1481287 .5322104
.2716082
.2127579 -.3591463 .3759479 .2036561 .0445465
Cancer type (Baseline: Intrathoracic)
Digestive organs Female organs Brain Breast Male organs Urinary tract Other
-.433949* -.7921458* .5306406 -.4280103 -.0943561 -.4676685 -.272698
.1942796 -.038057 .2672141 -.2487115 -.0427441 -.0694487 .0079689
Patient education (Baseline: < High school)
College University Post grad
.147035 -.1476198 -.4347936
.2825997
.1088122 .0942958*
Caregiver sex Male
.0177658
-.0234747
Patient living (Baseline: With spouse)

Chapter 4: Results R. Redmond-Misner
68
Hospitalization cost
Hospitalization costs took on one of two values: zero and the cost of a single
hospitalization ($5,558). This is because no patients experienced more than one
hospitalization in a given two-week time period. As a result, only a RE probit is required
given that there is no variability in the cost that would be analyzed using a RE GLS
model. Over the palliative care trajectory, 109 (34%) patients were hospitalized, making
this a less common but very costly aspect of CBPHC.
The RE probit results for the probability of hospitalization are given in Table 11. RE
probit is not subject to the Hausman test because a FE version of probit is not available
(StataCorp, 2013). Non-linear FE estimation is associated with practical and
methodological shortcomings, namely the “incidental parameters problem” that is
believed to irredeemably bias non-linear FE estimates (Greene, 2002). Hospitalizations
were significantly higher for patients with cancers of the digestive organs, caregivers
experiencing higher burden, and those who lived alone. In the aggregated costs, living
alone was only a significant predictor of Ministry of Health spending. The association
between living alone and Ministry of Health cost may be attributable in part to
heightened use of hospitals.
Alone With children With others
-.1261921 .1390012 .1292038
.0810581
.0339595 -.1645129
Intercept -2.95923 Overall R2 Between R2 Within R2 Wald Chi2 Prob > Chi2 Σe Σu Rho (ln)Σu2
46.91 .0254
.8745786 .4333917 -.2680262
.0497 (5%) .1062 (10.6%)
.0013 (1%) 40.46 .0767
1.0729366 .74413165 .32478376
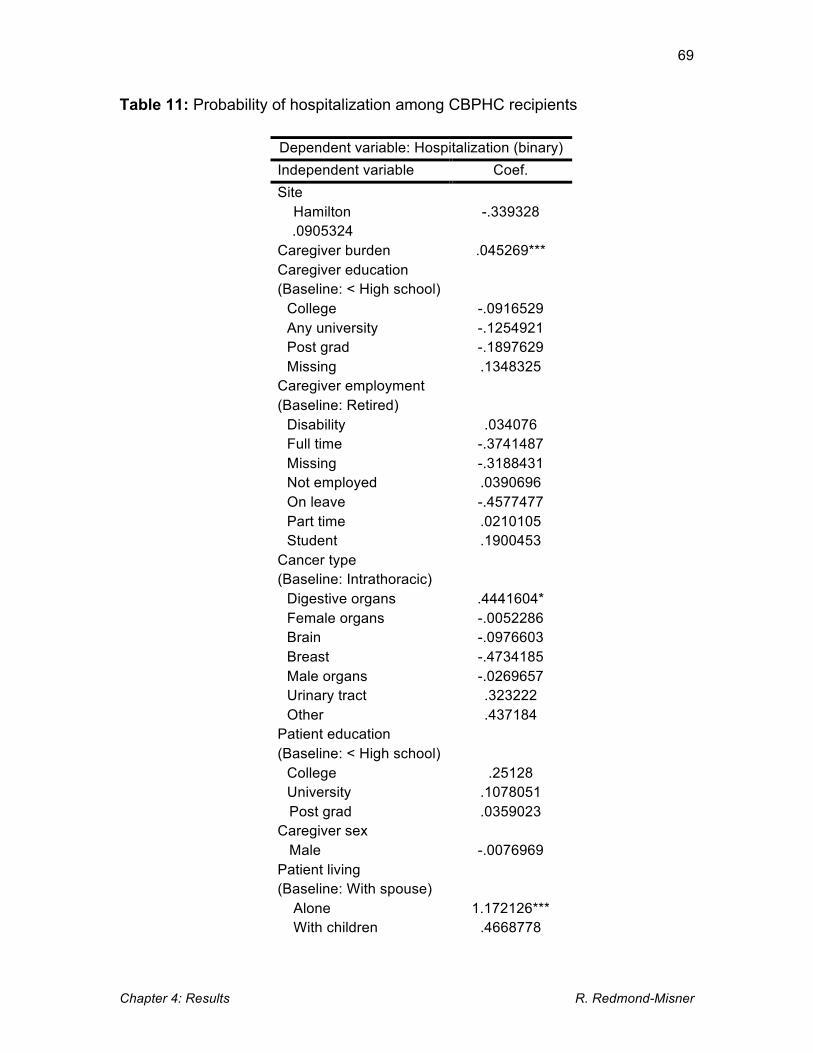
Chapter 4: Results R. Redmond-Misner
69
Table 11: Probability of hospitalization among CBPHC recipients
Dependent variable: Hospitalization (binary) Independent variable Coef. Site
Hamilton
-.339328 .0905324
Caregiver burden .045269*** Caregiver education (Baseline: < High school)
College Any university Post grad Missing
-.0916529 -.1254921 -.1897629 .1348325
Caregiver employment (Baseline: Retired)
Disability Full time Missing Not employed On leave Part time Student
.034076 -.3741487 -.3188431 .0390696 -.4577477 .0210105 .1900453
Cancer type (Baseline: Intrathoracic)
Digestive organs Female organs Brain Breast Male organs Urinary tract Other
.4441604* -.0052286 -.0976603 -.4734185 -.0269657 .323222 .437184
Patient education (Baseline: < High school)
College University Post grad
.25128 .1078051 .0359023
Caregiver sex Male
-.0076969
Patient living (Baseline: With spouse)
Alone With children
1.172126*** .4668778

Chapter 4: Results R. Redmond-Misner
70
With others .0013056 Intercept -.5239812 Wald Chi2 Prob > Chi2 Σu Rho (ln)Σu2
77.42 .000
.7413276
.3546583
.7413276
The rationale behind the service-specific cost analyses was to illustrate more specific
drivers of the aggregate Ministry of Health costs. The aggregated cost to the Ministry of
Health is more ambiguous because it is spread over many services. While variability in
hospitalization costs could not be analyzed (due to lack of variability), the probability of
incurring such costs was assessed. Several covariates that drove Ministry of Health
costs were associated with higher probability of hospitalization in this analysis. However,
it is noticeable that brain cancer is not significant for this service. Similar to medication
costs, this suggests that hospitalizations do not drive the positive and significant
association brain cancer has with Ministry of Health costs.
Public home appointment cost
Home appointments were used by 310 (99%) of the patients at some point in their
palliative trajectory. Bi-weekly costs ranged from $0 to $17,000, with an average of
$955. One of the benefits of two-part analysis was the use of different independent
variables in the data generation process of the two dependent variables (Mullahy, 1998;
Cragg, 1971; Mora et al, 2013). This was performed by using a different diagnosis
variable in the first and second part. Separate variables were used because all urinary
tract cancer patients had home appointments in all time periods, skewing their probit
coefficients drastically. A seven-category ICD-10 variable was used in the probit
specification where urinary tract cancer patients were categorized as “other” to
circumvent this issue. Lung cancer was still used as the baseline comparator.
The results of the RE probit on the incidence of home appointments and on RE
generalized least squares (GLS) regression on costs are presented in Table 12, showing
several significant findings. Both caregiver burden and female cancers negatively
influenced the probability of a home appointment, yet they positively determined costs.
Paradoxical findings such as this are the justification of separate analyses. Cragg (1971)

Chapter 4: Results R. Redmond-Misner
71
and Mullahy (1998) first used two-part analysis to use differing independent variables in
each part premised on the suspicion that these aspects of cost (any usage vs. extent of
usage) would be generated differently. Mora et al (2013) used the principal-agent model
to explain that each component may be determined by different people (i.e. any usage
by the patient/caregiver and the extent of service use by doctors) whose decisions are
influenced differently by the independent variables. The findings pertaining to caregiver
burden and gynecologic cancers suggest that whether or not a public home appointment
occurs, and the cost of the care provided at the home appointment, are determined
differently. While these patients may not have had home appointments as consistently
over time, they required extensive care or multiple appointments in the time periods
when they did. Patients who had post-graduate educations, lived in Hamilton and lived
alone were also associated with fewer visits.
The cost of services provided at home appointments are positively associated with both
female and brain cancers. Brain cancer has been a consistently positive driver of
aggregate costs, but was not significant when it came to medication or hospitalization
costs. Public home appointments however, contribute at least partially to their higher
costs. While gynecologic malignancies did not drive societal or unpaid costs, they were a
significant predictor of Ministry of Health costs. This result suggests that the positive
impact of female malignancies on Ministry of Health expenses could also be related to
public home appointments.
Table 12: Determinants of having a home appointment and its associated cost (RE probit and GLS)
Dependent variable
Any cost incurred (binary)
(ln)Home appointment cost > 0
Independent variable Probit GLS Site
Hamilton
-.838226*
-.0968293 Patient age Patient age2
.0154411
.0001287 .041956
-.0002556 Comorbidity score -.1885314 .0527401 Caregiver burden -.0283992* .0268329*** Caregiver education (Baseline: < High school)
College Any university
.5572194 -.0273343
-.0635957 -.1174621

Chapter 4: Results R. Redmond-Misner
72
Post grad Missing
.8871087 -.5419388
.0346318
.0193709 Caregiver employment (Baseline: Retired)
Disability Full time Missing Not employed On leave Part time
-.5469074 .1663302 .3165967 .7937325 .7487401 .4491194
.287002 .0720758 -.0857068 .0904596 .1862101 -.1497837
Cancer type (Baseline: Intrathoracic)
Digestive organs Female organs Brain Breast Male organs Urinary tract Other
-.5728867 -1.09672* -.3543498 .094809
.7776071
1.071584
.254821 .5518785* .6220284** .3191997 -.110943 .526638
.1035797 Patient education (Baseline: < High school)
College University Post grad
-.1404788 -.8395315 -1.314628*
-.0598004 -.0000761 .0000666
Caregiver sex Male
.9573216*
-.0520232
Patient living (Baseline: With spouse)
Alone With children With others
-1.672275** -.9444785 -.9393589
.171116 .1492152 .2009693
Intercept 3.830204 Overall R2 Between R2 Within R2 Wald Chi2 Prob > Chi2 Σe Σu Rho (ln)Σu2
25.59 .5695
1.084338 .5403967 .1619397
.0733 (7%) .0789 (7.9%) .0382 (3.8%)
68.51 .000
.73604573
.64634202
.43538168
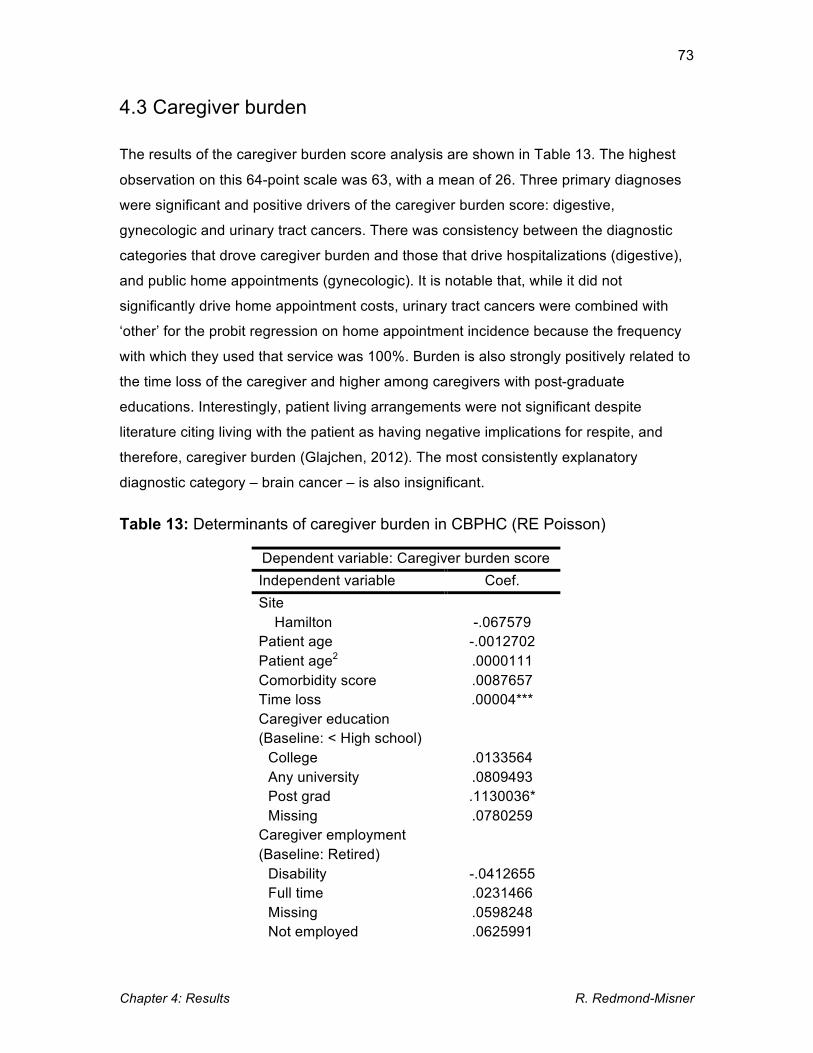
Chapter 4: Results R. Redmond-Misner
73
4.3 Caregiver burden
The results of the caregiver burden score analysis are shown in Table 13. The highest
observation on this 64-point scale was 63, with a mean of 26. Three primary diagnoses
were significant and positive drivers of the caregiver burden score: digestive,
gynecologic and urinary tract cancers. There was consistency between the diagnostic
categories that drove caregiver burden and those that drive hospitalizations (digestive),
and public home appointments (gynecologic). It is notable that, while it did not
significantly drive home appointment costs, urinary tract cancers were combined with
‘other’ for the probit regression on home appointment incidence because the frequency
with which they used that service was 100%. Burden is also strongly positively related to
the time loss of the caregiver and higher among caregivers with post-graduate
educations. Interestingly, patient living arrangements were not significant despite
literature citing living with the patient as having negative implications for respite, and
therefore, caregiver burden (Glajchen, 2012). The most consistently explanatory
diagnostic category – brain cancer – is also insignificant.
Table 13: Determinants of caregiver burden in CBPHC (RE Poisson)
Dependent variable: Caregiver burden score Independent variable Coef. Site
Hamilton
-.067579 Patient age Patient age2
-.0012702 .0000111
Comorbidity score .0087657 Time loss .00004*** Caregiver education (Baseline: < High school)
College Any university Post grad Missing
.0133564
.0809493 .1130036* .0780259
Caregiver employment (Baseline: Retired)
Disability Full time Missing Not employed
-.0412655 .0231466 .0598248 .0625991

Chapter 4: Results R. Redmond-Misner
74
On leave Part time Student
-.0085026 .0291817 -.1638782
Cancer type (Baseline: Intrathoracic)
Digestive organs Female organs Brain Breast Male organs Urinary tract Other
.10859* .1407698* .0349128 .0274689 .0558959 .1654493* .064661
Patient education (Baseline: < High school)
College University Post grad
.0249797 -.0306019 -.0644647
Caregiver sex Male
.0108964
Patient living (Baseline: With spouse)
Alone With children With others
.0059566 -.0081153 -.0070816
Intercept 3.003243***
Wald Chi2 Prob > Chi2 (ln)α Α
126.17 .000
-2.867784 .0568247
4.4 Diagnostics/Additional information
This section will discuss the diagnostics outlined in Section 3.5 and give additional
information about the analyses where appropriate.
Societal cost: Additional analysis information
The Hausman test applied to RE and FE analyses of societal costs rejected the null
Chapter 4: Results R. Redmond-Misner
75
hypothesis (H0) that the difference in coefficients between estimators was not systematic
(Prob > Chi2 = 0.0004). The alternative hypothesis indicates potential for predictions to
be inconsistent and biased, however the Hausman test will reject the null for any reason
that causes difference in RE and FE estimates, including the different degrees of
freedom (DF) after FE drops most covariates (RE=29 DF, FE=6 DF). What this test picks
up is the difference in RE and FE estimates; if the assumptions underlying the use of RE
hold, the estimates should be similar (Hill et al, 2011). In the succeeding subsections,
the interpretation of the Hausman test will remain the same.
In order to assess the accuracy of the RE results, which can still be valid despite the
result of the Hausman test, the RE results are presented alongside Allison’s hybrid
model and a FE model in Table 7. The results indicate that RE is behaving consistently
with FE. Coefficients on days overnight and caregiver burden, the only time-varying
covariates in this regression, agree across the standard RE, FE, and Allison’s hybrid FE-
type parameters on deviations from the mean in an RE specification.
Standard diagnostics were performed including graphing residuals and fitted values
(Appendix I), robust standard errors and the Breusch & Pagan Lagrange multiplier. All
GLS coefficients in this chapter are derived from models with heteroskedasticity-robust
standard errors. The Breusch & Pagan Lagrange multiplier test for the RE model
rejected the null hypothesis that there is no random effect (Prob > chibar2 = 0.000) in the
generation of CBPHC’s societal cost. The presence of random effects means that the
RE model is preferable to and more precise than a pooled or OLS model, and
consequently, the optimal model for this particular analysis. In the succeeding
subsections, the diagnostic interpretation of these statistics will be the same.
Ministry of Health cost: Additional analysis information
The RE model has rejected the null hypothesis of the Hausman test (Prob > Chi2 =
0.0011) despite otherwise affirming diagnostics. The residuals of the RE model are
homoskedastic and the fitted values slightly over predict (Appendix I); the variability
explained by the data generation process is much less for this aggregated cost (R2 =
10%). The coefficients in Table 8 show that the hybrid’s deviation variables’ and FE
parameters agree, which suggests that the RE estimator is behaving. The Breusch and
Pagan test detected random effect (Prob < chibar2 = 0.000), validating the
appropriateness of the estimator.

Chapter 4: Results R. Redmond-Misner
76
Unpaid caregiver cost: Additional analysis information
The unpaid care analysis rejected the Hausman test (Prob > Chi2 = 0.0154) and as well
as the Breusch and Pagan test (Prob < chibar2 = 0.000). The Hausman test result
means that the RE model should be augmented with Allison’s hybrid approach and
presented alongside FE estimates. The Breusch and Pagan test results indicate that
there are random effects in the panel and that RE is an appropriate estimator. The
residuals produce slightly more heteroskedasticity than the past two models (Appendix
I), which the use of Huber-White standard errors control for. Consistency across the RE,
FE and hybrid estimates are shown in Table 9. These models had a considerably higher
R2 than that reported in the Ministry of Health analysis (~19%).
Publicly funded medication: Additional analysis information
For the second part (GLS on costs > 0), the RE model accepted the null hypothesis of
the Hausman test (0.8848). Therefore, only the robust RE model is reported in Table 10.
The Breusch and Pagan Lagrange multiplier confirmed RE as the appropriate estimator
(Prob < chibar2 = 0.000). The graphs in Figure 10 show the distribution of the dependent
variables in the RE probit and GLS models. The left-hand-side (LHS) graph
demonstrates the high proportion of zeros in the data that needed to be modeled
separately. The right-hand-side (RHS) graph shows that the logarithms of the positive
values form an appropriate distribution for regression analysis. The overall R2 statistic for
the RE GLS is low (5%), but it is higher for the variability between individuals (10%).
Figure 7: Raw and log-positive distribution of public medication cost
0.1
.2.3
.4De
nsity
0 2 4 6 8Log-Transformed Medication Cost
Log Positive Public Medication Cost
0.0
01.0
02.0
03.0
04.0
05De
nsity
0 1000 2000 3000 4000 5000Medication Cost
Public Cost of Medications

Chapter 4: Results R. Redmond-Misner
77
Public home appointment: Additional analysis information
The second part of the model did not reject the Hausman test (Prob > Chi2 = 0.0053)
meaning that only the RE estimator is used on the log positive observations. The
Breusch and Pagan test confirmed that it is again the most appropriate model. Figure 9
shows the distributions of the dependent variables, demonstrating that there were zeros
requiring separate modeling (LHS) and that the logarithm of the positive observations
formed an appropriate distribution for the estimator (RHS). The overall and between-
individual R2 statistics on the RE GLS are both ~7%.
Figure 8: Raw and log-positive distribution of public home appointment cost
Caregiver burden scores: Additional analysis information
RE Poisson is subject to the Hausman test, and the null hypothesis was
accepted (Prob > Chi2 = 0.5030). As shown in Figure 10 (LHS), the distribution of the
variable is skewed, but because it is not genuinely continuous, cannot be addressed
through logarithmic transformation as shown by the graph on the RHS. The data is count
in nature and conforms to a Poisson distribution, although they are slightly over-
dispersed (variance < mean). Running a negative binomial that relaxes distributional
assumptions made no difference in results.
0.1
.2.3
.4.5
Dens
ity
2 4 6 8 10Log-Transformed Home Appointment Cost
Log Home Appointment Cost >0
02.
0e-0
44.
0e-0
46.
0e-0
48.
0e-0
4De
nsity
0 5000 10000 15000 20000Public Home Appointment Cost
Raw Scale Home Appointment Cost
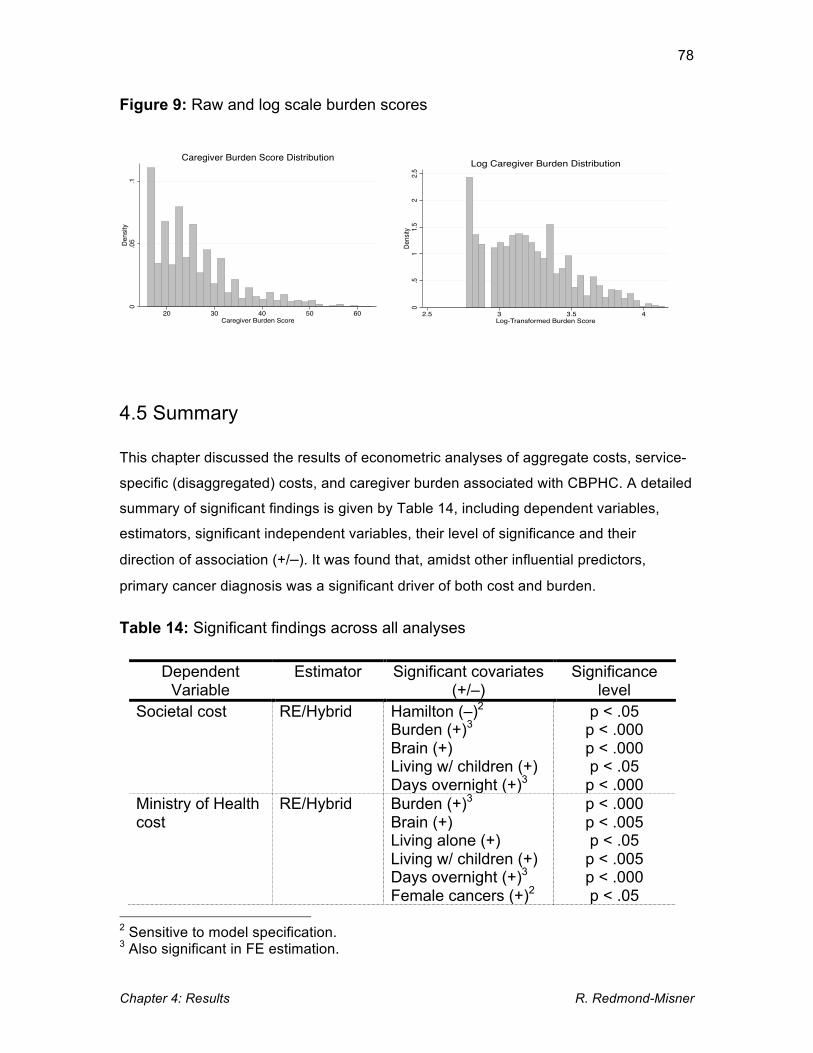
Chapter 4: Results R. Redmond-Misner
78
Figure 9: Raw and log scale burden scores
4.5 Summary
This chapter discussed the results of econometric analyses of aggregate costs, service-
specific (disaggregated) costs, and caregiver burden associated with CBPHC. A detailed
summary of significant findings is given by Table 14, including dependent variables,
estimators, significant independent variables, their level of significance and their
direction of association (+/–). It was found that, amidst other influential predictors,
primary cancer diagnosis was a significant driver of both cost and burden.
Table 14: Significant findings across all analyses
Dependent Variable
Estimator Significant covariates (+/–)
Significance level
Societal cost RE/Hybrid Hamilton (–)2 Burden (+)3 Brain (+) Living w/ children (+) Days overnight (+)3
p < .05 p < .000 p < .000 p < .05
p < .000 Ministry of Health cost
RE/Hybrid Burden (+)3 Brain (+) Living alone (+) Living w/ children (+) Days overnight (+)3 Female cancers (+)2
p < .000 p < .005 p < .05
p < .005 p < .000 p < .05
2 Sensitive to model specification. 3 Also significant in FE estimation.
0.0
5.1
Dens
ity
20 30 40 50 60Caregiver Burden Score
Caregiver Burden Score Distribution
0.5
11.
52
2.5
Dens
ity
2.5 3 3.5 4Log-Transformed Burden Score
Log Caregiver Burden Distribution

Chapter 4: Results R. Redmond-Misner
79
Unpaid caregiver cost
RE/Hybrid Hamilton (–) On leave (+) Brain (+) Living w/ others (–) Living w/ children (+)2 Days overnight (+)3 Burden (+)3
p < .05 p < .05
p < .005 p < .005 p < .05
p < .000 p < .000
Public medications
RE probit Digestive cancers (–) Female cancers (–)
p < .05 p < .05 p < .05 RE Post-grad education
(caregiver) (+) Hospitalization RE probit Burden (+)
Digestive (+) Living alone (+)
p < .000 p < .05
p < .000 Public home appointment cost
RE probit Hamilton (–) Burden (–) Female cances (–) Post-grad education (caregiver) (–) Male (caregiver) (–) Living alone (–)
p < .05 p < .05 p < .05 p < .05
p < .05
p < .005 p < .000 p < .05
p < .005
RE Burden (+) Female cancers (+) Brain (+)
Caregiver burden RE Poisson Time loss (+) Post-grad education (caregiver) (+) Digestive cancers (+) Urinary cancers (+) Female cancers (+)
p < .000 p < .05 p < .05 p < .05 p < .05 p < .05
Given the context and previous literature described earlier in the thesis, these findings
are of interest for several reasons. Differences in how costs are generated across
payers speaks to the trend in the literature reporting opposing conclusions that adopt
different payer perspectives. Conversely, some drivers of cost are consistent across
payer perspectives; this is true for caregiver burden and brain cancer.
The literature review found a strong focus on haematologic malignancies and NSCLC.
These results are able to speak to alternative denominations of cancer that have not
been as thoroughly reviewed in the palliative care literature. Specialized programming
and treatment have resulted from the neoplasm-specific palliative care research that has
taken place around haematologic and NSCLC (Temel et al, 2010; Cartoni, 2007).
Chapter 4: Results R. Redmond-Misner
80
Therefore, these findings may be of interest to providers, decision-makers looking to
foster a more individual-specific palliative care experience, or those interested in the
establishment of palliative care as a specialized field (Shadd, 2008).
The following chapters will discuss how these results correspond to previous research,
the hypotheses, generalizability and future work, It is evident that primary cancer
diagnosis is an important driver of both economic costs (irrespective of perspective) and
caregiver burden associated with CBPHC. This suggests that cancer site has a role in
shaping the experience of CBPHC.

81
Chapter 5 Discussion
The objective of this thesis was to comprehensively analyze the financial and caregiver
burdens associated with CBPHC for people with cancer so as to identify key
determinants. Specifically, whether or not primary cancer diagnosis (ICD-10 cancer
categories) influenced the magnitude of costs and/or burden was of interest given the
paucity of research in those areas. The results showed that, for this Ontarian cohort,
some cancer sites played a role in the costs and caregiver burden associated with
CBPHC, from the perspectives of all considered stakeholders (society, the Ministry of
Health and unpaid caregivers). This chapter offers an overview of the findings vis-à-vis
the hypotheses stated in Chapter 1, followed by a discussion of the findings and the
literature. This leads into policy implications, and the chapter is concluded with
disclosure of the study limitations.
In Chapter 4, the results showed that the costs and caregiver burden associated with
CBPHC were significantly associated with four of the ICD-10 categories: brain, digestive,
gynecologic and urinary tract malignancies. Brain cancer was positively associated with
the aggregated cost of CBPHC from all payer perspectives and the service-specific cost
of home appointments (publicly funded); digestive cancers were associated with
increased probability of hospitalization and higher caregiver burden; gynecologic
cancers were associated with higher home appointment cost, caregiver burden and
Ministry of Health cost (albeit sensitive to model specification); urinary tract cancer was
associated with higher caregiver burden. The socio-demographic and care-related (i.e.
home care agency, days overnight, etc.) covariates also played significant roles that
were generally consistent with the conceptual frameworks and literature that influenced
their inclusion. Some of the hypotheses outlined in Chapter 1 pertained to these socio-
demographic covariates and they will be discussed with regard to the applicable
hypothesis in Section 5.1, whereas the ICD-10 variable of interest will be discussed
more in-depth.

Chapter 6: Conclusion R. Redmond-Misner
82
5.1 Findings vis-à-vis the hypotheses
While the hypotheses were informed by previous research (Section 1.4), the Andersen
and Newman framework (Section 3.1.3) informed data collection and the type of
variables conceptualized as generating health service use. In this study, service use is
represented by its monetary cost. The framework posits that determinants of health
service use include predisposing, enabling and needs-based factors. Variables from all
of these subsets were significant. Predisposing factors of caregiver employment status,
education and patient living arrangement were predictive of all aggregated costs and the
probability of hospitalization. The one enabling factor that was included in the statistical
models, which was a dummy for which home care agency the patient was enrolled in,
was significant for societal and unpaid costs. Need factors included the diagnostic
variable and comorbidity scores, of which the diagnostic categories were consistently
significant. This latter type of predictor has been described as “illness severity”
(Guerriere, 2012), thus it is notable that the diagnostic variable does not actually
attribute differential severities to the categories and treats them as nominal. This section
will describe the results pertaining to specific independent variables in relation to the
specific hypotheses.
H1: The influence of primary diagnosis on cost will be statistically significant.
The diagnostic variable was statistically significant for all cost regressions. However, the
magnitude, direction and ICD-10 category of significance varied. Malignancies of the
brain and gynecologic organs were both important drivers of each cost component, while
malignancies of the digestive organs significantly drove the probability of hospitalization.
These three diagnostic categories were the only significant diagnostic variables in the
cost or service usage equations. Brain cancer was consistently positive across all payer
perspectives and for public home appointment costs. Gynecologic cancers were
significant determinants of aggregated Ministry of Health costs (albeit sensitive to model
specification and therefore not as robust), and for the cost of public home appointments.
Most of the patients in the female organs cancer category had ovarian cancer.
H2: Costs will be driven by caregiver burden, which will be driven by primary diagnosis.
Evidence supported this two-part hypothesis. Aggregate costs were positively driven by
Chapter 6: Conclusion R. Redmond-Misner
83
caregiver burden scores irrespective of payer, as were the disaggregated costs. The
probability of a hospitalization was also higher as burden scores rose. However, while
costs were most consistently driven by brain cancer, caregiver burden was not. This is
further discussed under H4. Caregiver burden may conceptualized as an ‘enabling’ factor
in the Andersen and Newman framework, because the extent to which the caregiver
feels burdened may impact on their ability to provide care.
H3: Socio-demographic variables will be statistically significant predictors of cost,
particularly SES indicators, marital status and patient living arrangement.
The former two hypotheses were more central to the research question and have fewer
sources of verification and justification in previous literature. The suspicion that socio-
demographic variables will be significant, particularly SES and living arrangement, is
based much more on the results of previous research (Gardiner et al, 2014; Guerriere et
al, 2010; Chai et al, 2013). However the SES indicators – education and employment
status – were not overly predictive in the analysis. One category from each, post-
graduate education and ‘on leave’ employment status, produced significant results. Post-
graduate educated caregivers were associated with higher public medication cost and
higher caregiver burden; caregivers ‘on leave’ were associated with greater unpaid
caregiver cost. The post-graduate caregiver education level was also associated with
significantly fewer home appointments, which suggests that burden may be greater
among dyads receiving fewer visits from the CBPHCT.
Patient living arrangements were also consistent drivers of cost. Patients living alone,
who are not frequently observed in existing research, had a significant and positive
effect on Ministry of Health costs. Living alone was also associated with a higher
probability of hospitalization, which helps to explain their elevated cost from the Ministry
of Health’s perspective. Patients living with children were associated with higher costs
from all perspectives, though the source of those positive coefficients was not further
illuminated by the analysis of service-specific costs. Patients living with others
experienced smaller unpaid costs. Because the possibility of living with multiple people
is implied by the term “others,” it is perhaps possible that the obscured/lowered cost
reporting that was attributed to multiple caregivers by Jacobs et al (2011) is happening
here.

Chapter 6: Conclusion R. Redmond-Misner
84
In addition to these variables, city of residence was a significant determinant of unpaid
caregiver time. Hamilton was associated with less societal and less unpaid caregiver
costs than Toronto. Because all caregivers were valued the same way (human capital
approach, described in Section 3.4.2), this difference must be attributable to less time
spent caregiving. This suggests that Toronto and Hamilton residents may differ in
unobserved ways. The experience of home care is expected to differ depending on
location due to the level of services available (Kuluski, 2010). Other explanations may be
that Toronto residents had higher wages that allowed them to work less overall; perhaps
the Toronto program was busier resulting in more necessity for unpaid caregivers to
supplement care; or perhaps suburban Hamilton residents were more likely to know their
neighbours and have help from more people which offset the demand on the primary
caregiver.
H4: The influence of primary diagnosis in caregiver burden will be of statistically
significant.
Caregiver burden scores were associated with malignancies of digestive organs, female
organs and the urinary tract. Interestingly, urinary tract cancers did not determine
anything else. This is part of a trend of disassociation between the cancer-related
determinants of cost and burden that was alluded to under H2; brain cancer, which drove
all costs, did not drive caregiver burden at all. Digestive and female organs were also
associated with use of public services including hospitalization and home appointments.
Many of the patients in the ‘digestive’ category lived with colorectal cancer, which CIHI
(2013) found to be highly represented among hospital deaths. CPSO (2002) associated
hospital admission with caregiver burden. In Given et al’s (2004) conceptual framework
for assessing caregiver burden of people caring for cancer patients, this would be
considered a ‘care situation’ factor that determines the demands on the caregiver.
With regard to urinary tract cancers seemingly only driving caregiver burden, recall that
the urinary tract cancer category had to be moved into ‘other’ in the home appointment
probit regression because the frequency with which they used that service was 100%
which was skewing the estimates. Despite high frequency, their actual costs related to
home appointments were not found to be significant.
H5: Caregiver burden will be driven by time spent providing care, which will be

Chapter 6: Conclusion R. Redmond-Misner
85
determined by primary diagnosis in the analysis of unpaid caregiver cost.
The caregiver burden score was driven significantly by time spent providing care, which
was positively associated with brain cancer. However, as outlined in H4, caregiver
burden was also driven by the primary diagnosis of the patient. Unpaid caregiver cost
(which is primarily time cost) and caregiver burden were driven by slightly different
diagnoses in the regressions where they were the dependent variables. Burden was
associated with malignancies of the digestive and female organs, which is most
congruent with the determinants of public cost. It was not associated with brain cancer,
which was the only diagnostic category to predict unpaid caregiver costs to a significant
degree. This suggests that, in addition to having a causal relationship with the amount of
unpaid time devoted to the patient, burden also has a close relationship with public
costs. This is further congruent with statements and the CPSO (2002) and findings
under H4 that indicate that worsening/intensification of caregiver burden instigates the
use of public services or hospitals. This usage trajectory may therefore be associated
more strongly with some diagnoses than others.
5.2 Comparisons and inferences from the literature
The primary research question of this thesis pertained to whether or not primary
diagnosis (defined by tumour site as per the ICD-10) played a role in costs and caregiver
burden associated with CBPHC. CBPHC is a growing service and evolving policy area
that is not yet reinforced by stable funding. In fact, it is increasingly reliant on unpaid
care because funding has not grown proportionately with demand following health care
restructuring (TLCPC. 2014). Therefore, establishing points of vulnerability can inform
admission and referral into these programs by understanding predictors of excessive
caregiver burden, hospitalization, or demand for public home appointments in advance.
In Ostgathe et al’s (2008) study, a panel of experts used prior knowledge of NSCLC
treatment to project what palliative home care would cost. Neoplasm-specific services
have been been developed and implemented in the case of haematologic malignancies
in response to their higher propensity for service use and neoplasm-specific needs (i.e.
transfusions, blood laboratory, etc.) (Cartoni et al, 2007).

Chapter 6: Conclusion R. Redmond-Misner
86
Brain cancer is the most glaring subgroup in terms of elevated cost across all considered
cost dimensions. The majority of these patients lived with glioblastoma multiforme.
Gliomas are the most common subgroup of primary brain tumours, glioblastoma being
stage IV (Davis et al, 2011). There are unique and significant symptoms associated with
brain cancer from the perspective of both health professionals and unpaid caregivers.
Focal neurologic deficit, cognitive deficit and seizures are often already present at the
time of diagnosis (Flechl et al, 2013). The rapidity of symptom development is
unpredictable, echoing the concerns that underlie special focus on haematologic
malignancies (Bakitas et al, 2013). Depending on the location of the tumour, the
memory, personality or physical function of the patient can be suddenly compromised
(Cahill et al, 2011). People living with glioblastoma multiforme are usually bedbound at
the EoL, for as short as a week or as long as three months (Flechl et al, 2013). This is
consistent and fits logically with Wasner et al’s (2013) study in which the brain cancer
patients were unable to complete mental health assessments due to critical conditions
and had high I/ADL needs. Additional services sought by this particular group include
cognitive rehabilitation services (Davis et al, 2011). Thus there are several
characteristics of this tumour site that might explain why it differs from others in terms of
cost. Declining cognition impacts on caregivers emotionally and can have implications
for communicating symptoms according to Flechl et al (2013), although this was not
corroborated by the caregiver burden analysis.
Gynecologic malignancies did emerge as predictive of caregiver burden. This may be
because while brain cancer patients are potentially bedridden, many gynecologic
patients are actively pursuing various medical treatments during the palliative trajectory
according to Fauci et al (2012). The sample in their study was also largely comprised of
ovarian cancer sufferers. More than half of patients were undergoing radiation and
chemotherapy in the last six months of life, and more than 80% were hospitalized at
least once (maximum 14 times). The patients commonly suffered gastrointestinal
complications and required surgical procedures related to that, namely paracentesis
(removal of excess peritoneal fluid) (Fauci et al, 2012). Therefore being associated only
with Ministry of Health costs makes sense, and higher caregiver burden may be related
to the travel, time and stress of the patient undergoing more procedures during their
palliative trajectory even if they do not translate into exponentially more time.
Gynecologic cancers were also associated with higher publicly financed home

Chapter 6: Conclusion R. Redmond-Misner
87
appointments; the doctors in Ostgathe et al’s (2008) study regarded home appointments
as costly enough in their own rite to make home care more costly than conventional
treatment.
Malignancies of digestive organs were shown to be important determinants of both
hospitalization and caregiver burden. Many of the patients in this category had colorectal
cancer. Hospitalization generally was a common focus when assessing the relative
success or cost of home care (Wong et al, 2013; Simoens et al, 2010). The finding that
colorectal cancer patients had a higher probability of being hospitalized is congruent with
the paucity of literature concerning this group. CIHI (2013) recently reported that
colorectal cancers are highly represented in hospital deaths. CPSO (2002) attributed
EoL hospital admissions to caregiver burden, it is interesting that this diagnostic
category drives both. The CIHI (2013) report also cited lung cancer amidst high EoL
hospitalization; in this analysis, lung cancer was the baseline category that digestive
cancer patients were significantly more probable than, so that part of the report is not
corroborated. While the CPSO’s (2002) attribution of EoL hospital admission to caregiver
burden and trouble with interpreting symptoms (also reported by Docherty et al, 2008
and Parker Oliver et al, 2014) is being drawn on to explain this trend, there is little in the
literature that explicitly tries to answer why this might be the case.
The final ICD-10 category that played a significant role was that of urinary tract cancers
on caregiver burden. The literature is especially sparse for this population, although
Ershler (2003) points out that it is particularly prevalent in older patients (80+). These
latter categories indicate areas for future research. The remaining groups that did not
diverge significantly from the expenditure or burden level associated with lung cancer
include male genital cancers, breast cancer, and ‘other.’ The results relating to the
variable of interest, ICD-10 category, imply that what enrollees can expect from palliative
home care will be dependent on the primary diagnosis of the patient. This information
could be helpful in terms of referral and predicting vulnerable caregivers (i.e. colorectal
cancer) and foreseeing higher demand on the CBPHCT (i.e. brain cancer).
The variability in cancer types that drive cost and burden seemingly validate the primary
hypotheses and answer the research question by showing that significant variability
does exist between patients with different types of cancer. The other clinical indicator,
comorbidity scores, had no significant influence. This suggests that in addition to being

Chapter 6: Conclusion R. Redmond-Misner
88
inherently secondary to the patient’s primary affliction, comorbidities are secondary in
their capacity to determine cost and caregiver burden. Yet this has been a more
common measure in the existing literature. It has also been found to be significant in
previous palliative care research (Masucci, 2011; Guerriere, 2012).
Cancer diagnoses constitute a ‘need factor’ in the broader conceptual framework that
also includes predisposing and enabling factors (Andersen & Newman, 1973). While the
Andersen and Newman framework applies to health services use, Given et al (2004)
outlined similar predictors of caregiver burden. There are additional notable associations
with cost and burden that were derived from the analysis. Living alone enhanced the
probability of hospitalization among CBPHC patients. This is a ‘predisposing’ factor that
can also be found in the literature as a source of potential vulnerability in home care
(Aoun et al, 2013). In the aggregated costs, living alone was only a significant predictor
of Ministry of Health spending. That may be attributable in part to heightened use of
hospitals, which may be related to unavailability of unpaid caregivers. The unavailability
of unpaid caregivers has been cited as a barrier to accessing home care at all in past
literature (Aoun et al, 2013). The Hamilton program enrollees produced negative
coefficients across the board. This is an enabling factor and may be attributable to
unobserved program characteristics that were found to impact on caregiver burden by
Guerriere et al (2013). Differences across home care agencies were also found by
Hirdes et al (2012).
Another aspect of the literature that the results resonate with is that estimations of cost
are highly sensitive to payer perspective. This has been particularly true in the case of
conventional and home care cost estimations that do or do not consider the cost of
unpaid care. Most Ministry of Health studies, including Wong et al (2013) and Klinger et
al (2010) find home care less expensive, whereas societal and caregiver perspective
studies find it more costly (Jacobs et al, 2011). Not only are estimates going to be
different, but these results indicate that the data generation process will be too. This
means that, while it seems that primary diagnosis plays a role, different predictors may
have different implications for different payers. For example, the aggregated cost results
presented here indicate that Toronto residents receive much more unpaid care while the
difference in cost is insignificant to the Ministry of Health or home care program.
Caregiver burden on the other hand inflates costs across the board and is in everyone’s
interest to curb. So does living with children of the patient. Conversely, while living alone

Chapter 6: Conclusion R. Redmond-Misner
89
drives public cost, it does not place strain on an unpaid caregiver.
Despite some disjointedness in the significant predictors of cost and burden, caregiver
burden is a strong predictor of the costs associated with CBPHC. Caregivers are
invaluable to the sustainability of home care. Thus determinants of their burden are
useful for stabilizing this mode of delivery for palliative care. Caregiver burden was
strongly positively related to the time loss of the caregiver, although findings to the
contrary have also been made (Kenny et al, 2010). The rise in informal caregiving is not
an extraneous effect of the shift to community-based services inherent in the
restructuring of health case, but an intentional part of the plan (Church et al, 2002; Yu,
2011). Their preservation is of interest for all stakeholders. In Ward-Griffin et al’s (2012)
study, caregivers reported acting as coworkers with the palliative care team and felt that
attention on their needs was primarily for the purpose of ensuring that they continued
working as caregivers. Interestingly, patient living arrangement was not significant
despite literature citing living with the patient as having negative implications for respite
and therefore caregiver burden (Glajchen, 2012).
Many predictors that were found to be significant in the literature were able to be
included as covariates in the analyses, but some variables of determinacy were unable
to be included. This is true for the role of provider characteristics (Guerriere et al, 2013)
and ethnicity (Gardiner et al, 2014). The latter was reported as a weakness of several
studies (Temel et al, 2010; Docherty et al, 2008). While the non-diagnostic variables
were not of paramount interest, they were included in the statistical models in order to
form the most comprehensive and informed data generation process to assess primary
diagnosis amidst. The role of primary diagnosis emerged among the majority of
significant determinants established in previous literature. This fortifies the finding and
congruency with past research also suggests that this is not a particularly unique or
abnormal home care sample. That said, some potentially important covariates from the
literature could not be assessed.
Some of the trends in the data also speak to the policy concerns that were discussed at
the outset of the thesis. A large proportion of the caregivers were children and spouses;
sources of unpaid care that are expected to gradually lessen due to retirement
postponement and people having fewer children (Jiwani, 2003). As CBPHC shifts toward
a source of labour that is projected to be sparse, identifying predictors of strain on them

Chapter 6: Conclusion R. Redmond-Misner
90
can be helpful with planning, even at the agency level. Conversely, due to health care
restructuring, agencies themselves struggle to spread their resources across all the
demand (TLCPC, 2014), therefore it is also important to identify characteristics
associated with their strain. The following section will elaborate on the policy situation
that CBPHC is currently in and how this pertains to the research findings.
5.3 Policy implications
Home care is currently in a position where funding is not growing proportionately with
demand (TLCPC, 2014). It is therefore of interest to avoid high costs and high burden so
as to maintain unpaid caregivers (DeMiglio et al, 2012). Profiling patients to circumvent
financial strain and navigate provision, for all stakeholders and providers, has
manifested in personalized medicine (Kamal et al, 2013; Unroe et al, 2013) and
advocacy for the specialization of palliative care (Shadd, 2008). Personalized medicine
posits that the management of patients should be nuanced by specific demographic
characteristics and risk factors in order to predict burdens in advance. This study
revealed three subgroups that are associated with greater burden for service providers.
Brain cancer was associated with higher service use and unpaid caregiver time;
digestive cancers (primarily colorectal in this cohort) had a higher probability of
hospitalization; brain and gynecologic cancers (primarily ovarian in this sample)
predicted home appointments; gynecologic and digestive cancers predicted caregiver
burden felt by unpaid caregivers.
Home care’s lack of recognition in Canada’s national insurance plan leaves it to the
discretion of the province to organize (DiMiglio et al, 2012). Prominent representatives
such as Dr. Larry Librach of the Temmy Latner Centre for Palliative Care and Palliative
Care Council in Toronto have argued that palliative care needed distinct policy
representation (Ogilvie, 1998). The Romanow and Kirby reports both called for home-
based palliative care to become an insured service under the Canada Health Act
(Romanow, 2002; Kirby, 2002). In coming years, palliative home care specifically can be
expected to rise due to the demographic and epidemiologic composition of Canada.

Chapter 6: Conclusion R. Redmond-Misner
91
Prior acknowledgement of risk factors for future diseases or complications, as opposed
to treating existing problems as they come, can be an avenue for prevention as well as
cost saving through the prevention of things like unforeseen hospitalization.
Understanding the service usages associated with different ICD-10 denominations of
neoplastic malignancy could enhance the personalization and specificity of CBPHC.
Gaertner et al (2011) propose a disease-specific approach that entails standard
operating procedures (SOPs) for nineteen disease sites (categorized similarly to those
here). To date, internationally, specialized programming has been created for patients
with haematologic cancers (Cartoni et al, 2007), and specialized treatment regimens
have been developed for patients with NSCLC (Temel et al, 2010). Conversely, if some
cancers are associated with particularly high cost and/or caregiver burden, perhaps
there are better settings for them to receive care.
The senior’s population will double by 2036 and cancer is the leading cause of death in
Canada (Kirkey, 2010). Improving palliative and EoL care and setting up sustainable
infrastructure for it is a global public health priority on the agendas of both the WHO and
UN (Broad et al, 2013). The current funding model for CBPHC and the institutions that
people might use to in lieu of home care, such as hospices, relies on charitable
donations and unpaid labour (Nash et al, 2013). The goal of shifting care to unpaid
community members (Spalding, 2005; Yu, 2011) combined with the aforementioned
demographic prognoses means that the importance of CBPCTs (DeMiglio et al, 2012)
and unpaid caregivers (Haley, 2003) are going to rise even more substantially (Seow,
2009). Currently, many unpaid caregivers of patients with cancer lose considerable
savings and require health services themselves after bereavement (Bachner, 2007).
In the Ontario context, the province is divided into fourteen LHINs within which are
CCACs that facilitate community-based health care services on an even more
compartmentalized level (Klinger et al, 2011). CCAC’s were created in Ontario as the
single access point for home care services, palliative or not (Ogilvie, 1998; Seow, 2009).
Not-for-profit and for-profit agencies compete for CCAC home care service contracts by
which the CCAC acts as their case manager, point of access and coordinator (DiMiglio
et al, 2012). This was preceded by Pain and Symptom Management Coordinators
responsible for forming palliative care resource teams, but they too experienced financial
constraints and were implemented by the province under the assumption that teams
could be formed without using additional resources (Howell, 2003). Thus to achieve the

Chapter 6: Conclusion R. Redmond-Misner
92
sustainability evoked by the WHO and UN at present, this service is contingent on
austere use of their resources. This can be guided and aided through profiling recipients
and their associated strain on providers, including those that are unpaid.
The intention of capping future costs fuels policy interest in gradually transforming
volunteers, previously conceptualized as complementary to public services, into
legitimate service providers and self-sustaining public service substitutes (Eakin et al,
2009; Stajduhar et al, 2010). The results found here suggest that this is happening. For
the government to reimburse informal caregivers in the ways that other interest groups
have proposed, such as the Canadian Cancer Society or the NDP, would defeat the
purpose of the shift to community-based care. While community-based care might drive
up invisible unpaid costs, there are potential savings to be derived from these
alternatives from a ministerial perspective. Baranek (2000) argues that because
representation for societal spending on community-based care is more weakly
organized, government interests have been dominant in policy outcomes which favour
the public portion of the funding mechanics. In a survey conducted among Ontario’s
fourteen CCACs, the goal of “optimal health, independence and/or quality of life” was
second only to “cost-effective resource use,” bespeaking the thin spread of resources in
palliative care (King, 2002, p. 65). Thus the need to distribute resources optimally is
certainly felt by and of interest to service providers.
In moving palliative care in a more complex, specialized and encompassing direction,
recognizing it as a specialization has been advocated (Shadd, 2008;). This could
reformulate palliative care to further accommodate personalized care, give it more
legitimacy to compete for funding, and perhaps lead to the national insurance once
advocated by Romanow (2002) and Kirby (2002). “Common assessment tools,
standards of practice, central inventories of resources, shared information systems,
acute PC designed beds, and common access points to care” are necessary not only for
effective provision of palliative care, but capacity to prove effectiveness and better
qualify for funding consideration (Bainbridge et al, 2011, p. 275). Howell’s (2003)
research concluded that “Home as the place of care at the end-of-life and place of death
can be supported if there is a willingness to allocate the maximum level of services
allowable through … [the Ministry of Health]” (p. xiv). The current logic of finite and
intermittent block funding could be related to state hesitance to legally commit to the
unknown future costs of palliative care. In the mean time, professionals at the program

Chapter 6: Conclusion R. Redmond-Misner
93
level can only assess the suitability of the patient and presumably the intensity of their
needs in the palliative trajectory based on socio-demographic and clinical aspects of
their profile.
Some of the solutions, such as neoplasm-specific standard procedures for palliative care
(Gaertner et al, 2011), do imply relatively specialized and sophisticated services.
CBPCTs are intended to have physicians, nurses, psycho-spiritual counseling,
bereavement counseling, administrative staff and case managers working through
CCACs, but this is not always the case. The scope of a respective LHIN’s CBPCT is
dependent on their capacity to finance this (Bainbridge et al, 2011; Seow, 2009). If some
CBPCTs struggle to finance full teams, it is likely that they will face barriers in moving
toward or implementing the type of neoplasm-specific programming seen with
haematologic malignancies and NSCLC. Some regions with less resources may have
partial teams limited to one nurse (Nash et a, 2013) or restrict the times services are
available to a day time model as it is (with the ideal availability being 24/7) (Bainbridge,
2011; Sussman et al, 2011). It is also possible that with enough cost-driving barriers
experienced simultaneously, certain regions cannot feasibly or cost-effectively be
provided with a CBPCT at all (Kuluski, 2010). Recognizing palliative care as a
specialization may attract more funding and personnel to enable this (Shadd, 2008).
In these highly sensitive areas, it can be expected that the burden on unpaid caregivers
will be greater. So determining characteristics associated with high burden or service
use can illuminate the practicality of referring someone to home care. Some of the
predictors found in previous literature included time spent providing care (Hides et al,
2012), living arrangement and marital status (Glajchen et al, 2012). Urban and rural
capacity for development of community-based services is one of the most prominent
disparities among Ontario LHINs (Schuklenk, 2011). This study identified gynecologic
and digestive malignancies as predictive of caregiver burden, presumably due to
associated symptoms and demands of care. The often foreign clinical demands of home
care have been reported as a stressor by unpaid caregivers (Docherty et al, 2008); the
CPSO (2002) attributed EoL hospitalization to the panic that can be induced by rapidly
developing symptoms. These types of cancer were also associated with elevated
hospitalization and home appointment cost. Therefore the profiling of patients including
the risks associated with their malignancy may reduce caregiver burden. Going forward,
the primary diagnosis of the patient could be indicative at the onset of palliative care
Chapter 6: Conclusion R. Redmond-Misner
94
whether or not home care would be exceedingly strenuous on any providers, especially
unpaid caregivers. This neoplasm-specific SOPs outlined by Gaerner et al (2011) that
attempt to customize the palliative trajectory according to primary diagnosis.
The potential for the results of this study to inform policy and practice is relatively broad.
These data pertain to two Ontario CBPHC programs, but the care demands associated
with a given cancer site can speak to palliative home care for people with cancer
anywhere. The WHO’s World Cancer Report (Stewart & Wild, 2014) recently stated that
cancer is expected to surge globally over the next twenty years should no major
preventative measures be taken (including behavioural changes of the patients, i.e.
smoking). Cancer rates also rise with an aging population, and many developed
countries are currently experiencing this demographic trend (Hume & Christensen,
2014). The literature review included studies from several countries (Canada, US,
Singapore, Israel, Italy, Germany and Greece). This type of care is emerging in
response to the growing demand in order to circumvent some of the cost by sharing the
responsibility for care with community members. The ICD-10 defines cancer by tumour
site (i.e. breast, brain) rather than tumour type (i.e. sarcoma, carcinoma), which is also
beneficial and preferable for many reasons. This is how both patients with cancer and
specialized cancer organizations typically identify themselves (i.e. Canadian Breast
Cancer Foundation, Prostate Cancer Canada, Brain Tumour Foundation of Canada,
etc.). It is also how previous neoplasm-specific research has defined the type of
neoplasms they are focusing on (Temel et al, 2010; Gaertner et al, 2011).
In conclusion, the extent of the usefulness of these findings is contingent on policy
decisions. Currently, this knowledge can be utilized for personalized medicine; the use of
risk factors and patient characteristics to assess suitability of the patient for the service
and to foresee their potential complications. To implement more specialized
programming, as has been done with haematologic malignancies or NSCLC, may
require more infrastructural support for the palliative care field.

Chapter 6: Conclusion R. Redmond-Misner
95
5.4 Limitations
There are several limitations to this study. Firstly, generalizability may be limited by
sample size, regional differences in the level of CBPHC available, and unknown
differences between recipients and non-recipients. The sample size and number of
observations in these data are generous meaning that the results are generally
dependable, especially with the validation of previous literature. It is simply with regard
to the diagnostic variable of interest, for which there is little research (hence this thesis),
that further research and validation is needed. There is no control group to show how
this population compares to non-recipients or how representative it is of the general
population. It has been shown in previous research that receiving home care at all is
sensitive to a number of factors including SES (Motiwala et al, 2006), the availability of
unpaid caregivers (Aoun et al, 2013), and home care availability related to rurality and
centrality (Skinner, 2005; Funk et al, 2010; Kuluski, 2010; Bainbridge et al, 2011).
However, it presumably reflects the recipients of home care, for whom the main
inferences from the findings are intended (i.e. caregivers of patients with digestive organ
cancers in home care are vulnerable to burden).
Second, these data and analyses are missing potentially important variables. Ethnicity
was found to be an important predictor by Gardiner et al (2014). Several studies in the
literature review reported ethnically homogenous samples as a limitation to
generalizability, and this study cannot contribute to filling this gap either. However, it is
notable that lack of data does not necessarily equate to a racially/ethnically homogenous
sample, with Toronto being a very diverse city (Guerriere, 2012). It is simply
unrepresented in the data and can therefore not be spoken to, even if ethnic diversity did
exist.
Third, the costs in this study are reported by unpaid caregivers which opens the data up
to several types of bias including selection bias, social desirability bias and recall bias
(Guerriere et al, 2010). In Wasner et al (2013) and Grov et al’s (2006) studies, patients
and caregivers experiencing worse symptoms were unable to participate. The people
who are receptive to bi-weekly interviews may therefore represent dyads with lesser
burden or lesser costs. Comorbidity scores were not found to be significant and this
could always be because patients with the worst comorbidities did not partake. The
AHCR has been validated, with caregiver reports closely matching administrative data

Chapter 6: Conclusion R. Redmond-Misner
96
and demonstrating minimal impact for this potential bias (Guerriere et al, 2006).
Moreover, because the data were gathered prospectively, they are much more resilient
against recall biases found in retrospective studies. The interviews could have been
conducted even closer together to further defend against this type of bias, but two week
intervals were chosen by the research team who collected this data in order to mediate
between minimizing recall bias and minimizing interview burden for the participating
caregivers.
5.5 Summary
This chapter discussed the findings as they pertained to the hypotheses, the literature,
and policy implications. The research question was whether or not primary cancer
diagnosis would impact costs and caregiver burden, thus the broad hypothesis (broken
down into 5 hypotheses in Sections 1.4 and 5.1) was that primary diagnosis would play a
role in both. This broad hypothesis was supported by the evidence. The literature was
used to interpret the findings surrounding brain, digestive and gynecologic cancers and
their relationships with cost, hospitalization, public home appointments and caregiver
burden. The findings had implications for policy and personalized medicine, wherein they
could inform the planning of palliative trajectories taking into account these risk factors
so as to curb the strain on providers. This is important to the maintenance and
sustainability of this service given the current policy context that is characterized by
minimal funding and reliance on unpaid care.
97
Chapter 6 Conclusion
The objective of this thesis was to comprehensively analyze the financial and caregiver
burdens associated with CBPHC for people with cancer and evaluate the role of their
primary diagnosis. Primary cancer diagnosis (as defined by the ICD-10) was found to be
a consistently significant determinant of both CBPHC costs and caregiver burden. In the
concluding chapter, a summary of the thesis will be given, followed by recommendations
for future work.
6.1 Thesis summary
The central hypothesis of this thesis was that primary cancer diagnosis would play a
significant role in the generation of CBPHC cost and caregiver burden. The conceptual
framework articulated by Andersen and Newman posits that health services use
(represented by cost in this study) is determined through socio-demographic, clinical and
community-related factors. Many conceptual frameworks for caregiver burden include
similar predictors (Givens et al, 2004). Clinical factors in previous analytic models have
used comorbidity scores, the presence of any cancer, and cancer stage (Motiwala et al,
2006; Fairfield et al, 2012; Sussman et al, 2011; Sims et al, 1997). Many studies also
focused on one disease site, with much of the disease-specific studies focusing on
haematologic malignancies and NSCLC (Temel et al, 2010; Cartoni et al, 2007). While
still controlling for comorbidity, this study integrated a nominal cancer variable defined by
the ICD-10 categories that the patients fell into. The ICD-10 distinguishes among tumour
(i.e. breast, brain) sites as opposed to tumour types (i.e. carcinoma, sarcoma). This does
not only represent previously underrepresented neoplasm subgroups, but allows nine
disease sites to be observed side-by-side for comparative inference among brain,
breast, male, female, digestive, urinary, lung and other cancers.
This research was informed by the literature on home care costs, caregiver burden, and
palliative oncologic care. The literature on the cost of home care included research
discussing the comparative and actual cost of home care, payer shares of this cost, and
determinants of cost. Whether home care was deemed more or less expensive, and

Chapter 6: Conclusion R. Redmond-Misner
98
standalone estimates of its cost, were drastically different depending on the payer
perspective that is used. It was therefore decided to analyze cost from different payer
perspectives, which may be generated differently when it comes to determinants of cost.
This is allowable through the data which uses the comprehensive Ambulatory Home
Care Record for costing, which adopts a societal perspective but categorizes costs
according to payer (considered here: societal cost, Ministry of Health cost, and unpaid
caregiver cost). Determinants of cost in the existing literature included physical function
(represented here by comorbidity scores) (Guerriere et al, 2010), SES (represented here
by education and caregiver employment status) (Chai et al, 2013), marital status and
living arrangements (Guerriere et al, 2010). The analytic models presented in this thesis
were able to control for these important predictors alongside the key variable of interest,
namely, primary cancer diagnosis. One variable that was missing was ethnicity.
The literature on caregiver burden focuses on problems associated with caregiver
burden, unmet needs reported by caregivers, and determinants of satisfaction and
burden. Determinants of burden were related to service utilization, patient condition and
the amount of time they spent providing care. Disability, living arrangements, marital
status, SES, hours of unpaid care, and home care agency were the variables found to
be significant in the previous literature that were controlled for alongside primary cancer
diagnosis (Glajchen, 2012; Götze et al, 2014; Hirdes et al, 2012). It was found that in
addition to the psychosocial burden that is documented through the caregiver burden
scale, caregivers also experience physical burden and health problems (Glajchen, 2012)
that are not represented by the caregiver burden scale. Gardiner et al (2014) also tied
ethnicity to caregiver burden, which was once again not able to be included in the
analyses. Carlsson et al (2003) found place of death to predict burden among bereaved
caregivers in their retrospective study; while this data was collected, the prospective
data collection means that place of death was not known when reporting burden and
therefore was not included as a covariate.
The literature discussing palliative care for oncologic patients was sought for justification
of the inclusion of the diagnostic variables. While neoplasm-specific palliative care is a
relatively new and sparse research area, some interesting findings were derived.
Malignancy-specific symptom control was interpreted as a trace of this ostensible gap in
the literature. The contribution of these findings to this thesis is the fundamental and
broad suggestion that symptoms and palliation needs vary from malignancy to

Chapter 6: Conclusion R. Redmond-Misner
99
malignancy, and may therefore be influential in predicting cost and caregiver burden. It
seemed that the NSCLC and haematologic cancers were the most thoroughly
researched diagnoses to date, however Gaertner et al (2011) presented customized
SOPs for nineteen malignancies which reinforced the idea of analyzing them separately.
The analyses in this thesis notonly address this gap but illuminate whether such
distinctions are necessary and informative, or if proceeding with the convention of
homogenizing solid tumours is sufficient and inconsequential. Finally, ethnic
homogeneity was cited several times in the literature (Bakitas et al, 2013; Fauci et al,
2012; Temel et al, 2010), which cannot be addressed by this thesis.
Costs were analyzed taking advantage of the detail of the Ambulatory Home Care
Record. Payer perspectives, which were suspected to produce differential results based
on the literature, were divided into Ministry of Health, unpaid caregiver, and societal.
This helped to illuminate the branch of societal costs driving the coefficients in the
societal cost regression, and demonstrated how public and unpaid dimensions of home
care might stand in for one another (i.e. living alone is associated with higher Ministry of
Health cost, but lower unpaid care cost). Being that Ministry of Health costs are spread
across a variety of services, some smaller components of that cost were looked at
separately to derive what specific service usage might drive Ministry of Health cost
(particularly, publicly provided medication, hospitalization, and home appointments).
Caregiver burden scores were calculated using the CBS-EOLC, which measures
psychosocial burden (Dumont et al, 2008). Items in the questionnaire relate to
emotional, social and financial burden but not physical symptoms or changes.
Conceptual frameworks of caregiver burden, directed at both dementias and cancers,
prioritize patient and caregiver characteristics as well as the demands of care related to
patient symptoms (Givens et al, 2004). Thus this analysis, as well as the cost analyses,
were controlling for many of the most important covariates when assessing the role of
primary cancer diagnosis.
It was found that, amidst other influential predictors, primary cancer diagnosis was
frequently a driver of both costs and burden. Particularly, brain cancer drove aggregated
cost irrespective of payer, while female and digestive cancers drove both hospitalization
and burden. These are the only ICD-10 categories that were significant predictors in the
analyses. The literature review found a strong focus on haematologic and NSCLC.
Chapter 6: Conclusion R. Redmond-Misner
100
These results are able to speak to alternative denominations of cancer that are
underrepresented. Specialized programming and treatment have resulted from the
research that has taken place around palliative care for haematologic and NSCLC.
Therefore, these findings may be of interest to providers, decision-makers looking to
foster a more individual-specific palliative care experience or further specialize the
palliative care field (Shadd, 2008). Currently, it is particularly useful for profiling the
recipients of this care in advance so that complications leading to hospitalizations or
caregiver burden can be mediated and anticipated. Restructuring of health care in
Canada has been partially characterized by shifting services to the community
(Guerriere, 2012; Laville et al, 2007; Spalding, 2005; Skinner, 2005). While there are
demographic signs that the patient base is going to grow as the caregiver population
shrinks, further development of palliative home care has been endorsed in several
influential policy reports and is likely the direction that Ontario is going in. Recent
endorsements for the further development of community-based palliative home care
(CBPHC) include the Health Council of Canada’s (2013) Progress Report, Health Quality
Ontario’s (HQO) (2012) Report on Ontario’s Health System, the Ontario Seniors’
Secretariat’s (2013) Action Plan for Seniors, and Drummond et al’s (2012) Commission
on the Reform of Ontario’s Public Services.
6.2 Future work
To build on this work, there are several avenues that future research could take:
verification of the results, clinical interpretation of the results, caregiver interpretation of
the results, comparative analysis and places of death analysis.
Verification of the findings
Future work should endeavor to verify these results by analyzing the ICD-10 diagnoses
among other samples to enhance generalizability. It would be useful to diversify the
home care context within Canada, as the programs studied here are in metropolitan
areas with more resources than their rural counterparts. The studies that emerged in the
literature review were internationally variable, but had many consistencies across the
caregivers of home care recipients. Thus it would also be useful and complementary to

Chapter 6: Conclusion R. Redmond-Misner
101
yield international results. The further development and preservation of community-
based services is of international interest as trends of an aging population and growing
cancer incidence are not limited to Canada (Stewart & Wild, 2014). Future analytic
models could surpass the comprehensiveness of these ones should they include
additional variables of interest that were missing here. The inclusion of ethnicity could be
important and explanatory for both cost and caregiver burden analyses (Gardiner et al,
2014). For caregiver burden analyses, provider characteristics such as those in the
Quality of End-of-Life Care and Satisfaction with Treatment (QUEST) questionnaire
would be ideal to include as per the work done by Guerriere et al (2013).
Clinical interpretation of the findings
This study constitutes an analysis and attainment of patterns in cost and caregiver
burden across ICD-10 diagnostic categories. The purpose of this is so that they can be
useful and interpretable to people shaping policies, working and providing care in
CBPHC. There would be definite value in the clinician interpretation of the results; what
is it about brain cancer that makes it more costly in the home care context? What is it
that makes home appointments more frequent among brain and gynecologic cancers?
What is it that makes hospitalization more frequent among gynecologic and digestive
cancer patients? In-depth clinical insight into the differences among these neoplasms
could enhance personalized palliative care and inform more specialized care, as has
been implemented for NSCLC and haematologic malignancies. Previous studies have
premised their recommendations for (Gaertner et al, 2011) and anticipated demands
associated with home care (Ostgathe et al, 2008) entirely on professional/clinician
opinions and projections.
Caregiver interpretation of the findings
Caregiver experiences with symptom management tasks emerged as a source of
uncertainty and stress in the literature (Docherty et al, 2008; Parker Oliver, 2014). This is
part of why it was expected that clinical characteristics that determine those symptoms
would drive caregiver burden differentially. Care tasks are used as a broad, generalizing
term, but specific burdensome dimensions of caregiving have been identified in the case
of polypharmacy (Sheehy-Skeffington et al, 2013). Future work could pursue a more in-
depth explanation of the results by eliciting the interpretation and specific experiences of

Chapter 6: Conclusion R. Redmond-Misner
102
unpaid caregivers of patients with different malignancies. The two subgroups that were
associated with higher burden in this study were gynecologic and digestive cancers.
Unpaid caregivers could help to interpret why these malignancies may be more
burdensome. In the case of digestive cancers, which were significantly associated with
hospitalization, they may be able to illuminate specific explanations for that elevated
probability. This, combined with the interpretation of clinicians, could shape an idea of
the palliative trajectories that characterize these differential costs and further validate or
otherwise nuance the results.
Comparative analysis/extension to other settings
It is important to keep in mind that the analysis and findings of this thesis can only speak
to variability among a specific group of palliative home care patients. While some
characteristics have been identified as “more costly” or associated with “more burden,”
this is only within recipients of CBPHC. Whether or not these more expensive and
intensive patients exceed the cost or demand on caregivers experienced in other
settings is unknown. It was found by Singer et al (2005) that unpaid caregivers in the
home setting, despite being more sleep deprived and possibly contributing more time,
were still happier due to the facilitation of the patient’s preference. Therefore it would
also be interesting to look at the role of primary diagnosis across settings.
Places of death analysis
While costs and caregiver burden are of prominent interest in CBPHC research, so is
place of death (Brink et al, 2008). From a Ministry of Health perspective, CBPHC is
appealing for curbing institutional death, but it is also appealing to patients for facilitating
often-preferred home death. This is a commonly studied outcome in the field that also
has not been assessed vis-à-vis primary diagnosis. It would be complementary to this
topic and to personalized palliative care to further assess the role of primary diagnosis
through its impact on place of death.
This research found primary cancer diagnosis to be a consistently significant
determinant of CBPHC cost and associated unpaid caregiver burden. In a fragile sector
that must prioritize the maintenance of unpaid caregivers and optimize the distribution of
resources, it is incredibly useful to be aware of characteristics that are predictive of these
aspects of care. As Ontario shifts palliative care into the community, patients are being

Chapter 6: Conclusion R. Redmond-Misner
103
discharged faster at higher levels of complexity (Laporte & Rudoler, 2013). By profiling
vulnerable candidates for home care, patients who are at much greater risk of
hospitalization, high caregiver burden or excessive service use may be foreseen. This is
not only of interest to precariously funded home care programs to be able to form a
preliminary expectation, but also for caregivers to understand the magnitude of burden
they may be more likely to experience caring for someone with gynecologic, digestive or
urinary tract cancers.

104
References Alesi, E., Fletcher, D., Muir, C., Beveridge, R. & Smith, T.J. (2011). Palliative Care and
Oncology Partnerships in Real Practice. Oncology, vol. 25(13), 1287-1293.
Allison, PD. (2009). Fixed Effects Regression Models. SAGE Publications, University of Pennsylvania: Pennsylvania, USA.
Andersen, R. & Newman, JF. (1973). Societal and Individual Determinants of Medical Care Utilization in the United States. The Milbank Memorial Fund Quarterly: Health and Society, vol. 51(1), 95-124.
Aoun, S. & Skett, K. (2013). A longitudinal study of end-of-life preferences of terminally-ill people who live alone. Health and Social Care in the Community, vol. 21(5), 530-535.
Aoun, S., Kristjanson, L., Currow D. & Hudson P. (2005). Caregiving for the terminally ill: at what cost? Palliative Medicine, vol. 19, 551-555.
Bachner, Y. (2007). Psychometric Properties of a Modified Version of the Caregiver Reaction Assessment Scale Measuring Caregiving and Post-Caregiving Reactions of Caregivers of Cancer Patients. Journal of Palliative Care, vol. 23(2), 80-86.
Bainbridge, D., Brazil, K., Krueger, P., Ploeg, J., Taniguchi, A. & Darnay, J. (2011). Evaluating Program Integration and the Rise in Collaboration: Case study of a palliative care network. Journal of Palliative Care, vol. 27(4), 270-278.
Bakitas, M., Doyle Lyons, K., Hegel, M.T., & Ahles, T. (2013). Oncologists’ perspectives on concurrent palliative care in a National Cancer Institute-designated comprehensive cancer center. Palliative and Supportive Care, vol. 11, 415-423.
Balducci, L. (2003). New Paradigms for Treating Elderly Patients With Cancer: The Comprehensive Geriatric Assessment and Guidelines for Supportive Care. The Journal of Supportive Oncology, vol. 1(2), 30-7.
Balducci, L. (2003). The Elderly Patient With Cancer: New Approaches for Improved Outcomes. The Journal of Supportive Oncology, vol. 1(2), 3-4.
Baranek, P. (2000). Long Term Care Reform in Ontario: The Influence of Ideas, Institutions, and Interests on the Public/Private Mix. Dissertation, University of Toronto: Toronto, ON.
Beeuwkes Buntin, M. & Zaslavsky, AM. (2003). Too much ado about two-part models and transformation? Comparing methods of modeling Medicare expenditures. Journal of Health Economics, vol. 23, 525–542.
Bergman, J., Kwan, L., Fink, A., Connor, SE., & Litwin MS. (2009). Hospice and Emergency Room Use by Disadvantaged Men Dying of Prostate Cancer. The Journal of Urology, vol. 181, 2084-2089,
Bertschek, I. & Lechner, M. (1998). Convenient estimators for the panel probit model.

References R. Redmond-Misner
105
Journal of Econometrics, vol. 87, 329-371.
Brink, P. & Frise Smith, T. (2008). Determinants of Home Death in Palliative Home Care: Using the interRAI Palliative Care to Assess End-of-Life Care. American Journal of Hospice & Palliative Medicine, vol. 25(4), 263-70.
Broad, J., Gott, M., Kim, H., Boyd, M., Chen, H. & Connolly, M. (2013). Where do people die? An international comparison of the percentage of deaths occurring in hospital and residential aged care settings in 45 populations, using published and available statistics. International Journal of Public Health, vol. 58, 257-267.
Brumley, R., Enguidanos, S., Jamison, P., Seitz, R., Morgenstern, N., Saito, S., McIlwane, J., Hillary, K. & Gonzalez, J. (2007). Increased Satisfaction with Care and Lower Costs: Results of a Randomized Trial of In-Home Palliative Care. The American Geriatrics Society, vol. 55(7), 995-1000.
Bukki, J., Scherbel, J., Stiel, S., Klein, C., Meidenbauer, N. & Ostgathe, C. (2013). Palliative care needs, symptoms, and treatment intensity along the disease trajectory in medical oncology outpatients: a retrospective chart review. Support Care Cancer, vol. 21, 1743-1730.
Cain, R., Maclean, M. & Sellick, S. (2004). Giving support and getting help: Informal caregivers’ experiences with palliative care services. Palliative and Supportive Care, vol. 2, 265-272.
Campion-Smith, B. (May 22, 2014). Ontario NDP pledge tax credit for family caregivers. The Toronto Star: Toronto, ON. Retrieved from http://www.thestar.com/news/ontario_election/2014/05/22/ontario_ndp_pledge_tax_credit_for_family_caregivers.html.
Canadian Institute for Health Information (CIHI). (2013). End-of-Life Hospital Care for Cancer Patients. Retrieved from https://secure.cihi.ca/free_products/Cancer_Report_EN_web_April2013.pdf. Accessed on December 6, 2013.
Carlsson, ME. & Rollison, B. (2003). A comparison of patients dying at home and patients dying at a hospice: Sociodemographic factors and caregivers’ experiences. Palliative and Supportive Care, vol. 1, 33–39.
Cartoni, C., Brunetti, GA., D’Elia, GM., Breccia, M., Niscola, P., Marini, MG., Nastri, A., Alimena, G., Mandelli, F. & Foà, R. (2007). Cost analysis of a domiciliary program of supportive and palliative care for patients with hematologic malignancies. The Hematology Journal, vol. 92(5), 666-673.
Ceilleachair, O., Finn, C., Deady, S., Carsin, E. & Sharp, L. (2011). Have developments in palliative care services impacted on place of death of colorectal cancer patients in Ireland? A population-based study. Irish Journal of Medical Science, vol. 180, 91-96.
Chai, H., Guerriere, DN., Zagorski, B. and Coyte, PC. (2014). The magnitude, share and determinants of unpaid care costs for home-based palliative care service provision

References R. Redmond-Misner
106
in Toronto, Canada. Health and Social Care in the Community, vol. 22(1), 30-39.
Chai, H., Guerriere, D., Zagorski, B., Kennedy, J. & Coyte, P. (2013). The Size, Share, and Predictors of Publicly Financed Healthcare Costs in the Home Setting over the Palliative Care Trajectory. Journal of Palliative Care, vol. 29(3), 154-163.
Charlson, ME., Pompei, P., Ales, KL. & MacKenzie, CR. (1987). A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. Journal of Chronic Diseases, vol. 40(5), 373-383.
Church, J., Saunders, D., Wanke, M., Pong, R., Spooner, C. & Dorgan, M. (2002). Citizen Participation in Health Decision-Making: Past Experience and Future Prospects. Journal of Public Health Policy, vol. 23(1), 12-33.
Coates, V. (2012). Randomised controlled trials: still going for gold in 2012? Royal College of Nursing: UK. Retrieved from https://www.rcn.org.uk/__data/assets/pdf_file/0008/449135/Coates_keynote_research_2012.pdf.
Cochrane Collaboration. (2011). Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0). Retrieved from http://handbook.cochrane.org.
College of Physicians and Surgeons of Ontario (CPSO). (2002). Decision-making for the End of Life (Policy Statement #1-06). Retrieved from http://www.cpso.on.ca/uploadedFiles/policies/policies/policyitems/End%20of%20Life.pdf.
Conde-Sala, JL., Garre-Olmo, J., Turro-Garriga, O., Vilalta-Franch, J. & Lopez-Pousa, S. (2010). Differential features of burden between spouse and adult-child caregivers of patients with Alzheimer’s disease: an exploratory comparative design. International Journal of Nursing Studies, 47(10), 1262-1273.
Cragg, John G. (1971). Some statistical models for limited dependent variables with application to the demand for durable goods. Econometrica, vol. 39(5), 829-844.
Cramér, H. (1946). Mathematical Methods of Statistics. Princeton University Press: United States.
DeMiglio, L. & Williams, A. (2012). Shared care: the barriers encountered by community-based palliative care teams in Ontario, Canada. Health and Social Care in the Community, vol. 20(4), 420-429.
DeMiglio, L. & Williams, A. (2012). Factors Enabling Shared Care with Primary Healthcare Providers in Community Settings: The experiences of interdisciplinary palliative care teams. Journal of Palliative Care, vol. 28(4), 282-290.
Dennis, K., Lawrence Librach, S. & Chow, E. (2011). Palliative Care Oncology Leads to Better Care. Oncology, vol. 25(13), 1271-1275.
Diwan, S., Hougham GW. & Sachs, GA. (2004). Strain Experienced by Caregivers of Dementia Patients Receiving Palliative Care: Findings from the Palliative

References R. Redmond-Misner
107
Excellence in Alzheimer Care Efforts (PEACE) Program. Journal of Palliative Medicine, vol. 7(6), 797-807.
Docherty, A., Owens, A., Asadi-Lari, M., Petchey, R., Williams, J. & Carter, Y. (2008). Knowledge and information needs of informal caregivers in palliative care: a qualitative systematic review. Palliative Medicine, vol. 22, 153-71.
Drummond, D., Giroux, D., Pigott, S. & Stephenson, C. (2012). Commission on the Reform of Ontario’s Public Services. Retrieved from http://www.fin.gov.on.ca/en/reformcommission/.
Duan, N. (1983). Smearing estimate: a nonparametric retransformation method. Journal of the American Statistical Association, vol. 78, 605-610.
Dumont, S., Jacobs, P., Turcotte, V., Anderson, D. & Harel, F. (2010). The trajectory of palliative care costs over the last 5 months of life: a Canadian longitudinal study. Palliative Medicine, vol. 24(6), 630-640.
Dumont, S., Jacobs, P., Fassbender, K., Anderson, D. Turcotte, V., & Harel F. (2009). Costs associated with resource utilization during the palliative phase of care: a Canadian perspective. Palliative Medicine, 23(8) 708–717, 10.1177/0269216309346546.
Ekström, J. (2008). An empirical polychoric correlation coefficient. Jan Wallander and Tom Hedelius Research Foundation, project P2008-0102:1.
Enguidanos, SM., Cherin, D. & Brumley, R. (2005). Home-Based Palliative Care Study: Site of Death, and Costs of Medical Care for Patients with Congestive Heart Failure, Chronic Obstructive Pulmonary Disease, and Cancer. Journal of Social Work in End-of-Life & Palliative Care, vol. 1(3), 37-55.
Ershler, W. (2003). Cancer: A Disease of the Elderly. Supportive Oncology, vol. 1(2), 5-10.
Everitt, BS. (2002). The Cambridge Dictionary of Statistics (2nd Ed.). Cambridge University Press: Cambridge, UK.
Fairfield, K., Murray, K., Wierman, H., Han,P., Hallen, S., Miesfeldt, S., Trimble, E., Warren, J., & Earle, C. (2012). Disparities in hospice care among older women dying with ovarian cancer. Gynecologic Oncology, vol. 125, 14-18.
Fauci, J., Schneider, K., Walters, C., Boone, J., Whitworth, J., Killian, E. & Straughn, JM. (2012). The utilization of palliative care in gynecologic oncology patients near the end of life. Gynecologic Oncology, vol. 127, 175-179.
Flechl, B., Ackerl, M., Sax, C., Oberndorfer, S., Calabek, B., Sizoo, E., Reijneveld, J., Crevenna, R., Keilani, M., Gaiger, A., Dieckman, K., Preusser, M., Taphoorn, M. & Marosi, C. (2013). The caregivers’ perspective on the end-of-life phase of glioblastoma patients. Journal of Neurooncology, vol. 112, 403-411.
Frees, E.W. (2010). Regression Modeling with Actuarial and Financial Applications.

References R. Redmond-Misner
108
Cambridge University Press: Cambridge, UK.
Fukahori, H., Yamamoto-Mitani, N., Sugiyama, T., Sugai, T. & Kai, I. (2010). Psychometric properties of the Caregiver Burden Scale for Family Caregivers with Relatives in Nursing Homes: Scale development. Japan Journal of Nursing Science, vol. 7, 136-147.
Funk, L., Stajduhar, K., Toye, C., Aoun, S., Grande, G. & Todd, C. (2010). Part 2: Home-based family caregiving at the end of life: a comprehensive review of published qualitative research (1998-2008). Palliative Medicine, vol. 24(6), 594-607.
Gaertner, J., Wolf, J., Hallek, M., Glossmann, J. & Voltz R. (2011). Standardizing integration of palliative care into comprehensive cancer therapy—a disease specific approach. Support Care Cancer, vol. 19, 1037-1043.
Wang, G., Cheng, Q., Wang, Y., Deng, Y., Ren, R., Xu, W., Zeng, J. & Chen, S. (2008). The Metric Properties of Zarit Caregiver Burden Scale: Validation Study of a Chinese Version. Alzheimer Disease & Associated Disorders, vol. 22(4), 321-326.
Gardiner, C., Brereton, L., Frey, R., Wilkinson-Meyers, L. & Gott, M. (2014). Exploring the financial impact of caring for family members receiving palliative and end-of-life care: A systematic review of the literature. Palliative Medicine, vol. 28(5), 375-390.
Gibbons, R. & Hedeker, D. (1994). Application of Random-Effects Probit Regression Models. Journal of Consulting and Clinical Psychology, vol. 62(6), 285-296.
Given, B. & Given, C. (1991). Family Caregivers of Cancer Patients. In Hubbard, SM., Greene, P. & Knobs, MT (Eds.), Current Issues in Cancer Nursing Practice (pp. 1-9). Philadelphia, USA: J.B. Lippincott Co.
Given, B., Wyatt, G. & Rahbar, M. (2004). Burden and Depression Among Caregivers of Patients with Cancer at the End-of-Life. Oncology Nursing Forum, vol. 31(6), 1105-1117.
Glajchen, M. (2012). Physical Well-Being of Oncology Caregivers: An Important Quality-of-Life Domain. Seminars in Oncology Nursing, vol 28(4), 226-235.
Götze, H., Brähler, E., Gansera, L., Polze, N. & Köhler, N. (2014). Psychological distress and quality of life of palliative cancer patients and their caring relatives during home care. Support Care Cancer, DOI: 10.1007/s00520-014-2257-5.
Greene, W. (2002). The Bias of the Fixed Effects Estimator in Nonlinear Models. Department of Economics, Stern School of Business, New York University: New York, USA.
Greffe, X. (2007). The Role of the Social Economy in Local Development. In OECD. (2007). Social Economy: Building Inclusive Economies (pp. 91-117).
Grov, EK., Fossa, SD., Sorebo, O. & Dahl, AA. (2006). Primary caregivers of cancer patients in the palliative phase: A path analysis of variables influencing their burden. Social Science & Medicine, vol. 63, 2429-2439.

References R. Redmond-Misner
109
Guerriere, DN. (2012). Predictors of Place of Death and Family Caregiver Burden Across the Home-Based Palliative Care Trajectory. Proposal.
Guerriere, DN. & Coyte, PC. (2011). The Ambulatory Home Care Record: A Methodological Framework for Economic Analyses in End-of-Life Care. Journal of Aging Research, vol. 2011, http://dx.doi.org/10.4061/2011/374237.
Guerriere, DN., Zagorski, B. & Coyte, PC. (2013). Family caregiver satisfaction with home-based nursing and physician care over the palliative care trajectory: Results from a longitudinal survey questionnaire. Palliative Medicine, vol. 27(7) 632–638.
Guerriere, DN., Ungar, WJ., Corey, M., Croxford, R., Tranmer, JE., Tullis, E. & Coyte, PC. (2006). Evaluation of the ambulatory home care record: agreement between self-reports and administrative data. International Journal of Technology Assessment in Health Care, vol. 22(2), 203-210.
Guerriere, DN., Zagorski, B., Fassbender, K., Masucci, L., Librach, L. & Coyte, PC. (2010). Cost variations in ambulatory and home-based palliative care. Palliative Medicine, vol. 24(5), 523-532.
Haley, W. (2003). Family Caregivers of Elderly Patients With Cancer: Understanding and Minimizing the Burden of Care. Supportive Oncology, vol. 1(2), 25-29.
Hayman, J., Langa, K., Kabeto, M., Katz, S., DeManner, S., Chemew, M., Slavin, M. & Fendrick, M. (2001). Estimating the Cost of Informal Caregiving for Elderly Patients with Cancer. Journal of Clinical Oncology, vol. 19(13), 3219-3225.
Health Canada. (2009). Palliative and End-of-Life Care. Retrieved from http://www.hc-sc.gc.ca/hcs-sss/palliat/index-eng.php.
Health Council of Canada. (2013). Progress Report 2013: Health care renewal in Canada. Retrieved from http://www.healthcouncilcanada.ca/rpt_det.php?id=481.
Health Quality Ontario (HQO). (2012). Report on Ontario’s Health System. Retrieved from http://www.hqontario.ca/portals/0/Documents/pr/qmonitor-full-report-2012-en.pdf.
Hérbert, R., Bravo, G., & Préville, M. (2000). Reliability, validity, and reference values of the Zarit Burden Interview for assessing informal caregivers of community-dwelling older persons with dementia. Canadian Journal on Aging, vol. 19, 494-507.
Hill, R., Griffiths, W. & Lim, G. (2011). Principles of Econometrics (4th Ed.). John Wiley & Sons, Inc: Hoboken, New Jersey, USA.
Hirdes, J.P., Freeman, S., Frise Smith, T., & Stolee, P. (2012). Predictors of caregiver distress among palliative home care clients in Ontario: Evidence based on the interRAI Palliative Care. Palliative and Supportive Care, vol. 10, 155-163.
Hopewell, S., Loudon, K., Clarke, MJ., Oxman, AD. & Dickersin, K. (2009). Publication bias in clinical trials due to statistical significance or direction of trial results.

References R. Redmond-Misner
110
Cochrane Database of Systematic Reviews, vol. 21(1), 10.1002/14651858.MR000006.pub3.
Hu, F., Goldberg, J., Hedeker, D., Flay, B. & Pentz, M. (1998). Comparison of Population-Averaged and Subject-Specific Approaches for Analyzing Repeated Binary Outcomes. American Journal of Epidemiology, vol. 147(7), 694-703.
Hudson, PL., Hayman-White, K., Aranda, S. & Kristjanson, LJ. (2006). Predicting Family Caregiver Psychosocial Functioning in Palliative Care. Journal of Palliative Care, vol. 22(3), 133-140.
Hume, T. & Christensen, J. (2014). WHO: Imminent global cancer ‘disaster’ reflects aging, lifestyle factors. Retrieved from http://www.cnn.com/2014/02/04/health/who-world-cancer-report/.
Iecovich, E. (2012). Psychometric properties of the Hebrew version of the Zarit Caregiver Burden Scale short version. Age & Mental Health, vol. 16(2), 254-263.
Irwin, K., Greer, J., Khatib, J., Temel, J. & Pirl, W. (2012). Early palliative care and metastatic non-small cell lung cancer: Potential mechanisms of prolonged survival. Chronic Respiratory Disease, vol. 10(1), 35-47.
Jacobs, P., Dumont, S., Turcotte, V. & Anderson, D. (2011). Evaluating the Economic Loss of Caregiving for Palliative Care Patients. Journal of Palliative Care, vol. 27(3), 210-215.
Jiwani, I. (2003). Transformation of Health Organizations and Rhetoric of Accountability in Community-Based Health Care Practices in Ontario. Dissertation, York University: Toronto, ON.
Kamal, A., Nipp, R., Bull, J. & Abernethy, A. (2013). Towards Achieving Personalized Palliative Care: Predicting Symptom Burden in Community-Dwelling Patients With Advanced Ilnness (SA527-B). Journal of Pain and Symptom Management, vol. 45(2), 411-412.
Kao, H. & Acton, G. (2006). Conceptualization and psychometric properties of the caregiver burden scale in Taiwan. Issues in Mental Health Nursing, vol. 27, 853-866.
Kenny, PM., Hall, JP., Zapart, S. & Davis, PR. (2010). Informal Care and Home-Based Palliative Care: The Health-Related Quality of Life of Carers. Journal of Pain and Symptom Management, vol. 40(1), 35-48.
King, M. (2002). Analysis of Case Management as A Service Delivery Model in Ontario’s Home Care Sector. Dissertation, University of Toronto: Toronto, ON.
Kirkey, S. (May 20, 2010). End-of-life care an uncertain ‘patchwork’; Canadian cancer society report; Agency calls for a national caregiver strategy and access to high-quality palliative programs. The Gazette; Montreal, QUE.
Klinger, C., Howell, D., Marshall, D., Zakus, D., Brazil, K. & Deber, R. (2011). Resource

References R. Redmond-Misner
111
utilization and cost analyses of home-based palliative care service provision: The Niagara West End-of-Life Shared-Care Project. Palliative Medicine, vol. 27(2) 115-122.
Kuluski, K. (2010). Homecare or Long-term Care? The Balance of Care in Urban and Rural Northwestern Ontario. Dissertation, University of Toronto: Toronto, ON.
Janjan, N. (2011). Palliative Care: Meaningful Benefit in Oncology Care. Oncology, vol. 25(13), 1244-1256.
Lai, DWL. (2007). Validation of the Zarit Burden Interview for Chinese Canadian caregivers. Social Work Research, vol. 31, 45-53.
Laporte, A. & Rudoler, D. (2013). Assessing Ontario’s Personal Support Worker Registry. Health Reform Observer – Observatoire des Réformes de Santé, vol. 1(1), Article 2.
Lavergne, MR., Johnston, GM., Gao, J., Dumont, S. & Burge, FI. (2011). Exploring Generalizability in a Study of Costs for Community-Based Palliative Care. Journal of Pain and Symptom Management, vol. 41(4), 779-787.
Laville, J., Levesque, B. & Mendell, M. (2007). Diverse Approaches and Practices in Europe and Canada. In OECD. (2007). Social Economy: Building Inclusive Economies (pp. 155-81).
Lester, JF., Macbeth, F., Toy, E. & Coles, B. (2012). Palliative radiotherapy regimens for non-small cell lung cancer. Cochrane Database of Systematic Reviews, Issue 4. Art. No.: CD002143. DOI: 10.1002/14651858.CD002143.pub2.
Liu, L., Cowen, ME., Strawderman, RL. & Shih, YT. (2011). A Flexible Two-Part Random Effects Model for Correlated Medical Costs. Journal of Health Economics, vol. 29(1), 110–123.
Manitta, VJ., Philip, JAM. & Cole-Sinclair, MF. (2010). Palliative Care and the Hemato-Oncological Patient: Can We Live Together? A Review of the Literature. Journal of Palliative Medicine, vol. 13(8), 1021-1025.
Manning, WG. (1998). The logged dependent variable, heteroscedasticity, and the retransformation problem. Journal of Health Economics, vol. 17, 283-295.
Manning, WG., Basu, A. & Mullahy, J. (2005).Generalized modeling approaches to risk adjustment of skewed outcomes data. Journal of Health Economics, vol. 24(3), 465-488.
Manning, WG. & Mullahy, J. (2001). Estimating log models: to transform or not to transform? Journal of Health Economics, vol. 20(4), 461-494.
Masucci, L. (2011). Health Care Service Provision Over the Palliative Care Trajectory. Thesis, University of Toronto: Toronto, ON.
McGrath, PD., & Holewa, HA. (2007). Description of an Australian Model for End-of-Life

References R. Redmond-Misner
112
Care in Patients With Hematologic Malignancies. Oncology Nursing Forum, vol. 34(1), 79-85.
Mora, T., Gil, J. & Sicras-Mainar, A. (2013). The influence of BMI, obesity and overweight on medical costs: a panel data perspective. Health, Econometrics and Data Group: University of York, UK. Retrieved from york.ac.uk/res/herc/hedgwp.
Motiwala, S., Croxford, R., Guerriere, D. & Coyte, P. (2006). Predictors of Place of Death for Seniors in Ontario: A Population-Based Cohort Analysis. Canadian Journal on Aging, vol. 25(4), 363-371.
Mullahy, J. (1998). Much ado about two: reconsidering retransformation and the two-part model in health econometrics. Journal of Health Economics, vol. 17:247–281.
Nash, M., Cunha, J., Mueller, L., Edwards, B. & Jackson, E. (October 10, 2013). The way forward: Ontario is on the cusp of a revolution in the way the province offers palliative care, but the plan hinges on government support. Kanata EMC: Kanata, ON.
Neelon, B. & O’Malley, AJ. (N/A). Two-Part Models for Zero-Modified Count and Semicontinuous Data. Department of Biostatistics and Bioinformatics, Duke University School of Medicine: Durhan, North Carolina, USA.
Neuhaus, JM. (1992). Statistical methods for longitudinal and clustered designs with binary responses. Statistical Methods in Medical Research, vol. 1, 249-273.
Neuhaus, J. M., J. D. Kalbfleisch, and W. W. Hauck. 1991. A comparison of cluster-specific and population-averaged approaches for analyzing correlated binary data. International Statistical Review 59: 25–35.
Neumann, P. (2009). Costing and perspective in published cost-effectiveness analysis. Medical Care, vol. 47(7), S28-32.
Nymphas, L. & Wu, S. (2014). Measurement structure of the caregiver burden scale: Findings from a national community survey in Taiwan. Geriatrics Gerontoloty, vol. 14, 176-184.
Ogilvie, D. (1998). Palliative care in Canada facing a real crisis: only 10% of patients who require home care are getting it. Medical Post, vol. 34(18), 5.
Olsen, MK. & Schafer, JL. (2001) A two-part random effects model for semicontinuous longitudinal data. Journal of the American Statistical Association 2001;96:730–745.
Ontario Senior’s Secretariat, The. (2013). Ontario’s Action Plan for Seniors. Retrieved from https://dr6j45jk9xcmk.cloudfront.net/documents/215/ontarioseniorsactionplan-en-20130204.pdf.
Ostgathe, C., Walshe, R., Wolf, J., Hallek, M. & Voltz, R. (2008). A cost calculation model for specialist palliative care for patients with non-small cell lung cancer in a tertiary centre. Support Care Cancer, vol.16, 501–506.

References R. Redmond-Misner
113
Pallett, P. (1990). Conceptual Framework for Studying Family Caregiver Burden in Alzheimer’s-Type Dementia. Journal of Nursing Scholarship, vol. 22(1), 52-58.
Park, RE. (1966). Estimation with Heteroscedastic Error Terms. Econometrica, vol. 34(4), 888.
Parker Oliver, D., Wittenberg-Lyles, E., Washington, K., Kruse, R., Albright, D., Baldwin, P., Boxer, A. & Demiris, G. (2013). Hospice Caregivers’ Experiences With Pain Management: “I’m Not a Doctor, and I Don’t Know if I Helped Her Go Faster or Slower”. Journal of Pain and Symptom Management, vol. 46(6), 846-859.
Pearson, K. (1900). Mathematical contributions to the theory of evolution: On the correlation of characters not quantitatively measurable. Philosophical Transactions of the Royal Society of Mathematical, Physical & Engineering Sciences, vol. 195, 1-47.
Pearson, K. (1907). Mathematical contributions to the theory of evolution: On further methods of determining correlation. Drapers’ Company Research Memoirs, Biometric Series (Volume 4). London: Cambridge University Press.
Pearson, K. & Heron, D. (1913). On theories of association. Biometrika, vol. 9, 159-315.
Preferred Reporting Items for Systematic Reviews (PRISMA). (2014). Transparent Reporting of Systematic Reviews and Meta-Analysis. Retrieved from http://www.prisma-statement.org/statement.htm.
Ramchandran, K. & Von Roenn, J. (2013). Palliative Care Always. Oncology, Review Article. Retrieved from http://www.cancernetwork.com/palliative-and-supportive-care/palliative-care-always.
Rangachari, D. & Smith, TJ. (2013). Integrating Palliative Care in Oncology The Oncologist as a Primary Palliative Care Provider. The Cancer Journal, vol. 19(5), 373-378.
Rice, DM. (1989). Cost of injury in the United States. University of California, Institute for Health and Aging: San Francisco, CA.
Rocque, GB. & Cleary, JF. (2013). Palliative care reduces morbidity and mortality in cancer. Nature Reviews Clinical Oncology, vol. 10, 80-89.
Rodby, KA., Turin, S., Jacobs, RJ., Cruz, JF., Hassid, VJ., Kolokythas, A. & Antony, AK. (2014). Advances in oncologic head and neck reconstruction: Systematic review and future considerations of virtual surgical planning and computer aided design/ computer aided modeling. Journal of Plastic, Reconstructive & Aesthetic Surgery, http://dx.doi.org/10.1016/j.bjps.2014.04.038.
Romanow, R. (2002). Building on values: the future of health care in Canada. Final report of the Commission on the Future of Health Care in Canada. Saskatoon: Commission on the Future of Health Care in Canada.

References R. Redmond-Misner
114
Ryn, M., Sanders, S., Kahn, K., van Houtven, C., Griffin, J., Martin, M., Atienza, A., Phelan, S., Finstad, D. & Rowland, J. (2011). Objective burden, resources, and other stressors among informal cancer caregivers: a hidden quality issue? Pyscho-Oncology, vol. 20, 44-52.
Sanyal, P. & Babu, S. (2009). Food Security, Poverty and Nutrition Policy Analysis: Statistical Methods and Applications (1st Ed.). Academic Press, Elsevier: London, UK & Amsterdam, NL.
Schuklenk, U., van Delden, J., Downie, J., McLean, S., Upshur, R. & Weinstock, D. (2011). The Royal Society of Canada Expert Panel: End-of-Life Decision Making. The Academies of Arts, Humanities and Sciences of Canada. Accessed November 2013. Retrievable from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3265521/pdf/bioe0025-0001.pdf.
Seow, H. (2009). The Use of End-of-Life Homecare Services in Ontario, Canada: Is it associated with using less acute care services in late life? Dissertation, John Hopkins University: Baltimore, USA.
Shadd, J. (2008). Should palliative care be a specialty?: yes. Canadian Family Physician, vol. 54(6), 840-846.
Sheehy-Skeffington, B., McLean, S., Bramwell, M., O’Leary, N. & O’Gorman, A. (2013). Caregivers Experiences of Managing Medications for Palliative Care Patients at the End of Life: A Qualitative Study. American Journal of Hospice & Palliative Medicine, vol. 31(2), 148-154.
Shephard, T. (May 15, 2004). Etobicoke MPP calls for palliative care standards, policies. Etobicoke Guardian: Etobicoke, ON.
Shnoor, Y., Szlaifer, M., Aoberman, AS. & Bentur, N. (2007). The Cost of Home Hospice Care for Terminal Patients in Israel. American Journal of Hospice & Palliative Medicine, vol. 24(4), 284-290.
Simoens, S., Kutten, B., Keirse, E., Vanden Berghe, P., Beguin, C., Desmedt, M., Deveugele, M., Leonard, C., Paulus, D. & Menten, J. (2010). The Costs of Treating Terminal Patients. Journal of Pain and Symptom Management, vol. 40(3), 436-448.
Sims, A., Radford, J., Doran, K. & Page, H. (1997). Social class variation in place of cancer death. Palliative Medicine, vol. 11, 369-373.
Singer, Y., Bachner, YG., Shvartzman, P. & Carmel, S. (2005). Home Death—The Caregivers’ Experiences. Journal of Pain and Symptom Management, vol. 30(1), 70-74.
Skinner, M. (2005). Voluntarism and Long-Term Care in the Countryside: Exploring the Implications of Health Care Restructuring for Voluntary Sector Providers in Rural Ontario. Dissertation, Queen’s University: Kingston, ON.
Spalding, K. (2005). Policy by Default: How changes in Ontario’s home care sector have

References R. Redmond-Misner
115
impacted providers, children and families. Dissertation, University of Toronto: Toronto, ON.
Stajduhar, K., Funk, L., Toye, C., Grande, G., Aoun, S. & Todd, C. (2010). Part 1: Home-based family caregiving at the end of life: a comprehensive review of published quantitative research (1998-2008). Palliative Medicine, vol. 24(6), 573-593.
StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP.
Sundararajan, V., Henderson, R., Perry, C., Muggivan, A., Quan, H. & Ghali, W. (2004). New ICD-10 version o the Charlson Comorbidity Index predicted in-hospital mortality. Journal of Clinical Oncology, vol. 57, 1288-1294.
Sussman, J., Barbera, L., Howell, D., Yang, J., Husain, A., Librach, S., Viola, R. & Walker, H. (2011). Health system characteristics of quality care delivery: A comparative case study examination of palliative care for cancer patients in four regions in Ontario, Canada. Palliative Medicine, vol. 26(4), 322-335.
Temel, J., Greer, J., Muzikansky, A., Gallagher, E., Admane, D., Jackson, V., Dahlin, C., Blinderman, C., Jacobsen, J., Pirl, W., Billings, J. & Lynch, T. (2010). Early Palliative Care for Patients with Metastatic Non-Small-Cell Lung Cancer. The New England Journal of Medicine, vol. 363(8), 733-744
Temmy Latner Centre for Palliative Care. (2013). What is palliative care? Mount Sinai Hospital: Toronto, ON. Retrieved from http://www.tlcpc.org/palliative-care.
Torres-Reyna, O. (2007). Panel Data Analysis: Fixed & Random Effects. Data & Statistical Services, Princeton University: New Jersey, USA. Retrieved from http://www.princeton.edu/~otorres/Panel101.pdf.
Tzala, S., Lord, J., Ziras, N., Repousis, P., Potamianou, A. & Tzala, E. (2005). Cost of home palliative care compared with conventional hospital care for patients with haematological cancers in Greece. European Journal of Health Economics, vol. 6, 102-106.
Unroe, K. & Meier, D. (2013). Research Priorities in Geriatric Palliative Care: Policy Initiatives. Journal of Palliative Medicine, vol. 16(12),
Von Roenn, J. & Temel, J. (2011). The Integration of Palliative Care and Oncology: the Evidence. Oncology, vol. 25(13), 1258-1266.
Ward-Griffin, C., McWilliam, C. & Oudshoorn, A. (2012). Relational Experiences of Family Caregivers Providing Home-Based End-of-Life Care. Journal of Family Nursing, vol. 18(4), 491-516.
Wasner, M., Paal, P. & Borasio, G.D. (2013). Psychosocial Care for the Caregivers of Primary Malignant Brain Tumor Patients. Journal of Social Work in End-of-Life & Palliative Care, vol. 9(1), 74-95.

References R. Redmond-Misner
116
Weinstein, MC., Siegel, JE., Gold, MG., Kamlet, MS. & Russel, LB. (1996). Recommendations of the panel of cost-effectiveness in health and medicine. Journal of the American Medical Association, vol. 276(15), 1253-1258.
Williams, AM., Wang, L. & Kitchen, P. (2014). Differential impacts of caregiving across three caregiver groups in Canada: end-of-life care, long-term care and short-term care. Health and Social Care in the Community, vol. 22(2), 187-196.
Wong, RCC., Tan, PT., Seow, YH., Aziz, S., Oo, N., Seow, SC., Seah, A., & Chai, P. (2013). Home-Based Advance Care Programme is Effective in Reducing Hospitalizations of Advanced Heart Failure Patients: A Clinical and Healthcare Cost Study. Annals Academy of Medicine Singapore, vol. 42, 466-471.
Wooldridge, J. (2012). Introductory Econometrics: A Modern Approach (5th Ed.). South-Western College Publishing: Boston, Massachusetts, USA.
World Health Organization. (2014). WHO Definition of Palliative Care. Retrieved from http://www.who.int/cancer/palliative/definition/en/.
Yalnizyan, A. (2007). Ontario’s Growing Gap. Canadian Centre for Policy Alternatives. Toronto, ON.
Yu, J. (2011). Home Care Utilization Patterns Among the Elderly Population: a Case Study of Ontario. Thesis, Queen’s University: Kingston, ON.
Zarit, SH., Reever, KE. & Bach-Peterson, J. (1980). Relatives of the Impaired Elderly: Correlates of Feelings of Burden. The Gerontologist, vol. 20(6), 649-655.

117
Appendix A Critical Appraisal Skills Program (CASP) tools4
TOOL 1: 12 questions to help you make sense of cohort study5 Three broad issues need to be considered when appraising a cohort study: • Are the results of the study valid? (A) • What are the results? (B) • Will the results help locally? (C)
(A) Are the results of the study valid? Screening questions 1. Did the study address a clearly focused issue? ☐Yes ☐Can’t tell ☐No HINT: A question can be ‘focused’ In terms of • The population studied • The risk factors studied • The outcomes considered • Is it clear whether the study tried to detect a beneficial or harmful effect? 2. Was the cohort recruited in an acceptable way? ☐Yes ☐Can’t tell ☐No HINT: Look for selection bias which might compromise the generalizability of the findings: • Was the cohort representative of a defined population? • Was there something special about the cohort? • Was everybody included who should have been included? Is it worth continuing? Detailed questions 3. Was the exposure accurately measured to minimize bias? ☐Yes ☐Can’t tell ☐No HINT: Look for measurement or classification bias: • Did they use subjective or objective measurements? • Do the measurements truly reflect what you want them to (have they been validated)? • Were all the subjects classified into exposure groups using the same procedure? 4. Was the outcome accurately measured to minimize bias? ☐Yes ☐Can’t tell ☐No HINT: Look for measurement or classification bias: • Did they use subjective or objective measurements? • Do the measures truly reflect what you want them to (have they been validated)? • Has a reliable system been established for detecting all the cases (for measuring disease occurrence)? • Were the measurement methods similar in the different groups? • Were the subjects and/or the outcome assessor blinded to exposure (does this matter)? 4 This follows the questionnaire verbatim (including punctuation), but spelling has been changed to Canadian where applicable. 5 The succeeding tools will only include questions distinct from Tool 1a.

Appendices R. Redmond-Misner
118
5. (a) Have the authors identified all important confounding factors? ☐Yes ☐Can’t tell ☐No List the ones you think might be important, that the author missed. 5. (b) Have they taken account of the confounding factors in the design and/or analysis? ☐Yes ☐Can’t tell ☐No List: HINT: Look for restriction in design, and techniques e.g. modeling, stratified-, regression-, or sensitivity analysis to correct, control or adjust for confounding factors 6. (a) Was the follow up of subjects complete enough? ☐Yes ☐Can’t tell ☐No 6. (b) Was the follow up of subjects long enough ☐Yes ☐Can’t tell ☐No HINT: Consider • The good or bad effects should have had long enough to reveal themselves • The persons that are lost to follow-up may have different outcomes than those available for assessment • In an open or dynamic cohort, was there anything special about the outcome of the people leaving, or the exposure of the people entering the cohort?
(B) What are the results? 7. What are the results of this study? HINT: Consider • What are the bottom line results? • Have they reported the rate or the proportion between the exposed/unexposed, the ratio/the rate difference? • How strong is the association between exposure and outcome? • What is the absolute risk reduction (ARR)? 8. How precise are the results? HINT: Look for the range of the confidence intervals, if given. 9. Do you believe the results? ☐Yes ☐Can’t tell ☐No HINT: Consider • Big effect is hard to ignore! • Can it be due to bias, chance or confounding? • Are the design and methods of this study sufficiently flawed to make the results unreliable? • Bradford Hills criteria (e.g. time sequence, dose-response gradient, biological plausibility, consistency)
(C) Will the results help locally? 10. Can the results be applied to the local population? ☐Yes ☐Can’t tell ☐No HINT: Consider whether • A cohort study was the appropriate method to answer this question • The subjects covered in this study could be sufficiently different from your population to cause concern • Your local setting is likely to differ much from that of the study • You can quantify the local benefits and harms

Appendices R. Redmond-Misner
119
11. Do the results of this study fit with other available evidence? ☐Yes ☐Can’t tell ☐No 12. What are the implications of this study for practice? HINT: Consider • One observational study rarely provides sufficiently robust evidence to recommend changes to clinical practice or within health policy decision making • For certain questions observational studies provide the only evidence • Recommendations from observational studies are always stronger when supported by other evidence
TOOL 2: 11 questions to help you make sense of case control study
(A) Are the results of the study valid? Screening questions 1. Same as Tool 1. 2. Did the authors use an appropriate method to answer their question? ☐Yes ☐Can’t tell ☐No HINT: Consider • Is a case control study an appropriate way of answering the question under the circumstances? (Is the outcome rare or harmful) • Did it address the study question? Is it worth continuing? Detailed questions 3. Were the cases recruited in an acceptable way? ☐Yes ☐Can’t tell ☐No HINT: We are looking for selection bias which might compromise validity of the findings • Are the cases defined precisely? • Were the cases representative of a defined population? (geographically and/or temporally?) • Was there an established reliable system for selecting all the cases • Are they incident or prevalent? • Is there something special about the cases? • Is the time frame of the study relevant to disease/exposure? • Was there a sufficient number of cases selected? • Was there a power calculation? 4. Were the controls selected in an acceptable way? ☐Yes ☐Can’t tell ☐No HINT: We are looking for selection bias which might compromise the generalizability of the findings • Were the controls representative of defined population (geographically and/or temporally) • Was there something special about the controls? • Was the non-response high? Could non-respondents be different in any way? • Are they matched, population based or randomly selected? • Was there a sufficient number of controls selected?

Appendices R. Redmond-Misner
120
5. Was the exposure accurately measured to minimize bias? ☐Yes ☐Can’t tell ☐No HINT: We are looking for measurement, recall or classification bias • Was the exposure clearly defined and accurately measured? • Did the authors use subjective or objective measurements? • Do the measures truly reflect what they are supposed to measure? (Have they been validated?) • Were the measurement methods similar in the cases and controls? • Did the study incorporate blinding where feasible? • Is the temporal relation correct? (Does the exposure of interest precede the outcome?) 6. (a) What confounding factors have the authors accounted for? List: HINT: List the ones you think might be important, that the author missed. • Genetic • Environmental • Socio-economic 6. (b) Same as question 5. (b) in Tool 1.
(B) What are the results? 7-9. Same as Tool 1.
(C) Will the results help locally? 10-11. Same as Tool 1.
TOOL 3: 11 questions to help you make sense of qualitative studies
Screening questions 1. Was there a clear statement of the aims of this research? ☐Yes☐Can’t tell ☐No HINT: Consider • What was the goal of the research? • Why it was thought important? • Its relevance 2. Is a qualitative methodology appropriate? ☐Yes ☐Can’t tell ☐No HINT: Consider • If the research seeks to interpret or illuminate the actions and/or subjective experiences of research participants • Is qualitative research the right methodology for addressing the research goal? Is it worth continuing? Detailed questions 3. Was the research design appropriate to address the aims of the research? ☐Yes ☐Can’t tell ☐No HINT: Consider • If the researcher has justified the research design (e.g. have they discussed how they decided which method to use)?
Appendices R. Redmond-Misner
121
4. Was the recruitment strategy appropriate to the aims of the research? ☐Yes ☐Can’t tell ☐No HINT: Consider • If the researcher has explained how the participants were selected • If they explained why the participants they selected were the most appropriate to provide access to the type of knowledge sought by the study • If there are any discussions around recruitment (e.g. why some people chose not to take part) 5. Was the data collected in a way that addressed the research issue? ☐Yes ☐Can’t tell ☐No HINT: Consider • If the setting for data collection was justified • If it is clear how data were collected (e.g. focus group, semi-structured interview etc.) • If the researcher has justified the methods chosen • If the researcher has made the methods explicit (e.g. for interview method, is there an indication of how interviews were conducted, or did they use a topic guide)? • If methods were modified during the study. If so, has the researcher explained how and why? • If the form of data is clear (e.g. tape recordings, video material, notes etc) • If the researcher has discussed saturation of data 6. Has the relationship between researcher and participants been adequately considered? ☐Yes ☐Can’t tell ☐No HINT: Consider • If the researcher critically examined their own role, potential bias and influence during (a) Formulation of the research questions (b) Data collection, including sample recruitment and choice of location • How the researcher responded to events during the study and whether they considered the implications of any changes in the research design 7. Have ethical issues been taken into consideration? ☐Yes ☐Can’t tell ☐No HINT: Consider • If there are sufficient details of how the research was explained to participants for the reader to assess whether ethical standards were maintained • If the researcher has discussed issues raised by the study (e.g. issues around informed consent or confidentiality or how they have handled the effects of the study on the participants during and after the study) • If approval has been sought from the ethics committee 8. Was the data analysis sufficiently rigorous? ☐Yes ☐Can’t tell ☐No HINT: Consider • If there is an in-depth description of the analysis process • If thematic analysis is used. If so, is it clear how the categories/themes were derived from the data? • Whether the researcher explains how the data presented were selected from the original sample to demonstrate the analysis process

Appendices R. Redmond-Misner
122
• If sufficient data are presented to support the findings • To what extent contradictory data are taken into account • Whether the researcher critically examined their own role, potential bias and influence during analysis and selection of data for presentation 9. Is there a clear statement of findings? ☐Yes ☐Can’t tell ☐No HINT: Consider • If the findings are explicit • If there is adequate discussion of the evidence both for and against the researchers arguments • If the researcher has discussed the credibility of their findings (e.g. triangulation, respondent validation, more than one analyst) • If the findings are discussed in relation to the original research question 10. How valuable is the research? HINT: Consider • If the researcher discusses the contribution the study makes to existing knowledge or understanding e.g. do they consider the findings in relation to current practice or policy?, or relevant research-based literature? • If they identify new areas where research is necessary • If the researchers have discussed whether or how the findings can be transferred to other populations or considered other ways the research may be used Additional tools and full questionnaires are available at http://www.casp-uk.net/#!casp-tools-checklists/c18f8.

Appendices R. Redmond-Misner
123
Appendix B Detailed characteristics of home care cost papers
Wea
knes
ses
Sm
all s
ampl
e.
Gen
eral
izab
ility
. D
oes
not c
alcu
late
ac
tual
eco
nom
ic
impa
ct.
Doe
s no
t acc
ount
fo
r pot
entia
l ext
ra
cost
of
hom
e
visi
ts.
1 di
seas
e gr
oup.
No
cont
rol g
roup
. H
ospi
tal
pers
pect
-iv
e on
ly.
Sm
all s
ampl
e.
Des
pite
resu
lt, h
ome
care
stil
l hig
hly
pr
efer
red
by
mos
t pa
tient
s.
Onl
y un
til 2
009.
Stu
dies
per
tain
-
ing
to h
ome
care
ar
e ou
tdat
ed.
Stu
dies
per
tain
ing
to
hom
e ca
re a
re
inte
rnat
iona
l.
Res
ults
71%
exp
erie
nced
redu
ced
hosp
italiz
atio
n.
5% h
ad m
ore
frequ
ent
adm
issi
ons.
95
% h
ad n
o w
orse
ning
.
Adj
uste
d fo
r ear
ly d
eath
(e
arly
dea
th =
no/
few
ho
spita
lizat
ions
).
Tran
sdus
ions
con
sist
ent i
n
bo
th g
roup
s, b
ut h
ome
gr
oup
had
to b
e re
gula
rly
mon
itore
d
for f
ull b
lood
co
unt a
nd b
lood
cro
ss-te
sts
in
orde
r to
proc
eed
at h
ome,
w
hich
mad
e th
em
mor
e ex
pens
ive
(hos
pita
l gro
up
only
test
ed a
t adm
issi
on
an
d w
hen
nece
ssar
y
ther
eafte
r).
1998
Spa
in d
ata
sugg
este
d
hom
e ca
re c
heap
er (v
ia
hosp
italiz
atio
n re
duct
ion)
.
Isra
eli s
tudy
sho
wed
that
sp
ecia
lized
hom
e ca
re w
as
30%
che
aper
than
non
-sp
ecia
lized
.
Foun
d th
at h
ome
care
cos
t de
pend
ed o
n th
e di
seas
e
of
th
e pa
tient
(i.e
. ha
emat
olog
ic p
atie
nts
and
trans
fusi
ons)
.
Out
com
e
Hos
pita
lizat
ions
Cos
t (H
ospi
tal
pers
pect
ive)
Con
clus
ions
abo
ut th
e co
st o
f pal
liativ
e ca
re in
va
rious
set
tings
(N/A
)
Met
hods
Dat
a co
llect
ion
from
regi
stry
of
end-
stag
e H
F pa
tient
s re
crui
ted
into
pal
liativ
e ca
re
prog
ram
from
200
8-10
. C
olle
cted
d
emog
raph
ics,
m
edic
atio
ns, l
ab re
sults
from
H
F da
taba
se e
lect
roni
c ho
spita
l rec
ords
.
Sta
tistic
al a
naly
sis
of h
ospi
tal
adm
issi
ons
befo
re a
nd a
fter
enro
lmen
t in
palli
ativ
e ca
re.
Pat
ient
recr
uit J
an-J
une
2002
. E
stim
ated
cos
t per
pat
ient
ex
clud
ing
trans
fusi
ons
and
drug
s th
at w
ere
com
mon
to
both
. Dat
a co
llect
ed fr
om
hosp
ital r
ecor
ds in
fina
nce
depa
rtmen
t. H
ospi
tal s
chem
e in
clud
ed h
otel
cos
t, ut
ilitie
s,
laun
dry,
food
, med
ical
sta
ff,
lab
test
s et
c. b
ased
on
bed
days
. Hom
e sc
hem
e in
clud
es
1-da
y cl
inic
, nur
se v
isits
, lab
te
sts.
Sys
tem
atic
revi
ew o
f
Pub
Med
, Coc
hran
e, E
conL
it an
d ot
hers
. App
rais
e m
etho
ds.
Syn
thes
ize
resu
lts. A
rticl
es
publ
ishe
d 20
00-0
9.
Exc
lude
d st
udie
s th
at
quan
tifie
d ut
iliza
tion
but d
id n
ot
conv
ert i
t to
cost
s.
Focu
s
Adv
ance
d he
art
failu
re p
atie
nts
with
1-
year
exp
ecte
d
surv
ival
; doe
s ho
me-
base
d pa
lliat
ive
care
re
duce
ho
spita
lizat
ion
and
thus
cos
ts?
EoL
hae
mat
olog
ic
canc
er p
opul
atio
n; is
it
chea
per t
o ca
re
for
them
at h
ome
or in
ho
spita
l? H
ome
patie
nts
atte
nd 1
-
day
clin
ic fo
r tra
nsfu
sion
, whi
le
inpa
tient
s oc
cupy
ho
spita
l bed
.
Cos
t of p
allia
tive
ca
re.
Setti
ng
Sin
gapo
re
2008
-10
Mul
tidis
cipl
i-nar
y
palli
ativ
e ho
me
care
pro
gram
; “a
dvan
ced
car
e
prog
ram
” (A
CP
)
Gre
ece
Inte
rnat
iona
l
Sam
ple
39%
mal
e.
Adv
ance
d he
art
failu
re (H
F) in
New
Yor
k H
eart
Ass
ocia
tion’
s (N
YH
A) c
lass
III o
r IV
. With
or w
ithou
t im
plan
tatio
n de
vice
s. C
ompl
iant
w
ith d
iet r
estri
ctio
ns
52 p
atie
nts
with
ha
emat
olog
ic
canc
ers.
25
in
hosp
ital
(con
vent
iona
l ca
re),
27 in
hom
e ca
re
Inte
rnat
iona
l
Des
ign
Pro
spec
tive
co
hort
stud
y
Cas
e co
ntro
l/
cost
m
inim
izat
ion
Sys
tem
atic
re
view
Art
icle
Won
g et
al
(201
3)
AN
NA
LS
Aca
dem
y of
M
edic
ine
Sin
gapo
re
Tzal
a et
al
(200
5)
Eur
opea
n Jo
urna
l of
Hea
lth
Eco
nom
ics
Sim
oens
et a
l (2
010)
Jour
nal o
f Pai
n an
d S
ympt
om
Man
agem
ent

Appendices R. Redmond-Misner
124
Wea
knes
ses
MLR
: Did
they
log
y or
no
t? S
tepw
ise.
Sel
ectio
n bi
as b
etw
een
pat
ient
s w
ho c
hoos
e to
go
int
o H
C a
nd th
ose
who
go
in
to li
fe-e
xten
sion
.
Not
long
itudi
nal d
ata,
ju
st 1
sum
. Pat
ient
s m
atch
ed o
nly
by d
isea
se
and
resi
dent
ial s
ituat
ion.
Pro
spec
tive
– th
is is
ex
pect
ed u
tiliz
atio
n an
d
cost
for t
hese
sp
ecia
lized
ser
vice
s. It
is n
ot b
ased
on
em
piric
al d
ata.
Not
from
a s
ocie
tal
pers
pect
ive.
Doe
s no
t ad
dres
s w
heth
er
redu
ctio
n in
ho
spita
lizat
ion
wou
ld
coun
tera
ct th
e hi
gher
estim
ates
for h
ome
care
.
Cos
ting
met
hod
vuln
erab
le to
con
test
; re
lies
on p
oten
tial
earn
ings
rath
er th
an
actu
al e
arni
ngs.
Gen
eral
izab
ility
.
Rec
all a
nd s
ocia
l de
sira
bilit
y bi
ases
.
Res
ults
Sig
nific
ant d
iffer
ence
in
num
ber o
f tre
atm
ents
. A
vera
ge c
ost o
f hom
e ca
re $
3467
, and
$12,
434
for
co
nven
tiona
l (ov
er 2
mon
ths)
.
Old
er p
atie
nts
chea
per.
The
cost
s of
the
first
visi
t
and
follo
w-u
p
visi
t wer
e es
timat
ed fo
r
all s
cena
rios/
mod
ules
(h
ospi
tal,
hom
e, d
ay-
care
, inp
atie
nt).
Hom
e ca
re th
ough
t to
prev
ent h
ospi
taliz
atio
n
but
had
an
over
all
hi
gher
es
timat
e du
e to
ex
pect
ed lo
nger
and
m
ore
frequ
ent
visi
ts
an
d tra
vel c
ost (
even
with
ass
umpt
ion
that
they
all
live
clos
e).
Pub
licly
fina
nced
cos
ts
acco
unt f
or ~
20%
of t
otal
co
sts
and
incr
ease
d to
war
d de
ath.
Pub
lic c
osts
ar
e dr
iven
by
soci
o-de
mog
raph
ic (o
lder
or
mar
ried
= lo
wer
sha
re o
f co
st fo
r pub
lic) a
nd c
linic
al
char
acte
ristic
s.
Out
com
e
Cos
t
Cos
t es
timat
es
Pub
licly
fina
nced
co
st
Met
hods
Pat
ient
s re
crui
ted
in 2
003.
Com
pare
d co
st o
f car
e fo
r all
pa
tient
s du
ring
the
final
2
m
onth
s of
life
. All
form
al
treat
men
ts a
nd s
ervi
ces
from
the
heal
th s
yste
m w
ere
incl
uded
in th
e co
stin
g,
ob
tain
ed fr
om th
e qu
ality
cont
rol u
nit o
f Cla
lit H
ealth
S
ervi
ces
afte
r the
ir de
ath.
Con
sens
us p
roce
ss a
mon
g on
colo
gist
, sur
geon
, pal
liativ
e sp
ecia
list a
nd ra
dio-
ther
apis
t pa
rtici
patin
g on
neg
otia
tion
com
mitt
ee o
f hos
pita
l fin
ance
de
partm
ent t
o es
timat
e th
e ut
iliza
tion
and
cost
for h
ospi
tal-
base
d, d
ay c
are
and
hom
e
care
.
Cos
ts w
ere
seem
ingl
y
estim
ated
from
a m
inis
teria
l pe
rspe
ctiv
e. U
sed
real
pric
ing
data
for h
ealth
pro
fess
iona
ls.
Bi-w
eekl
y in
terv
iew
s (to
tal
667)
Mul
tiple
regr
essi
on
an
alys
is (l
og -
linea
r).
Focu
s
Hom
e ca
re v
s.
conv
entio
nal c
are
cost
for p
atie
nts
dy
ing
with
m
etas
tatic
can
cer.
Est
imat
ion
of c
ost
give
n th
e ut
iliza
tion
expe
cted
by
expe
rt
parti
cipa
nts.
Pub
licly
fina
nced
co
sts
of p
allia
tive
care
.
Setti
ng
Isra
el
Ger
man
y
Toro
nto,
Ont
ario
, C
anad
a
Sam
ple
146
patie
nts
with
m
etas
tatic
can
cer
73 c
onve
ntio
nal 7
2 ho
me
care
Pat
ient
s in
bot
h gr
oups
live
d w
ith
thei
r fam
ilies
55%
men
NS
CLC
pat
ient
s
(N u
nkno
wn)
129
care
give
rs o
f pa
lliat
ive
patie
nts
from
200
5-20
07
Des
ign
Cas
e co
ntro
l/ co
hort
stud
y
Qua
litat
ive
Pro
spec
tive
coho
rt st
udy
Art
icle
Shn
oor e
t al (
2007
)
Am
eric
an J
ourn
al o
f H
ospi
ce &
Pal
liativ
e M
edic
ine
Ost
gath
e et
al
(200
8)
Sup
port
Car
e C
ance
r
Cha
i et a
l (20
13)
Jour
nal o
f Pal
liativ
e C
are

Appendices R. Redmond-Misner
125
Wea
knes
ses
Lite
ratu
re re
view
non
-sy
stem
atic
; pot
entia
l
sele
ctio
n bi
as.
Arg
ues
that
pub
lic c
over
age
is
mos
t cos
t-effi
cien
t but
do
es n
ot e
xact
ly p
rove
it.
Doe
s no
t spe
ak e
qual
ly to
bo
th a
rgum
ents
or a
t all
to
the
argu
men
t for
priv
ate.
Doe
s no
t rep
ort o
n ge
nera
lizab
ility
of t
he H
alifa
x fin
ding
s to
oth
er g
eogr
aphi
c ar
eas
or ti
me
perio
ds.
Doe
s no
t dis
cuss
thei
r ow
n lim
itatio
ns.
Elig
ibili
ty c
riter
ia m
ay li
mit
gene
raliz
abili
ty.
Util
izat
ion
base
d on
re
trosp
ectiv
e re
view
on
ad
min
dat
a. O
ntar
io D
rug
Ben
efit
(OD
B),
out-o
f-
po
cket
spe
ndin
g or
em
erge
ncy
serv
ices
are
not
re
cord
ed.
No
care
give
r cos
t.
Res
ults
Priv
ate
finan
cing
of c
omm
unity
-bas
ed
serv
ices
incr
ease
s he
alth
car
e co
st in
lo
ng-te
rm th
roug
h in
crea
sed
acut
e
care
ut
iliza
tion.
Incr
ease
d in
dire
ct
cost
s in
the
form
of c
areg
iver
bu
rden
/redu
ced
labo
r mar
ket
parti
cipa
tion
for
c
areg
iver
s.
Stu
dy p
artic
ipan
ts w
ere:
you
nger
, en
rolle
d lo
nger
, liv
ed c
lose
r to
the
P
CP
, and
wer
e m
ore
likel
y to
hav
e ca
ncer
th
an th
e ot
her c
lient
s;
You
nger
, liv
ed c
lose
r to
the
PC
P, a
nd
wer
e m
ore
likel
y to
hav
e ha
d ra
diot
hera
py/ m
edic
al o
ncol
ogy
co
nsul
ts t
han
othe
r can
cer d
eced
ents
; Li
ved
~42
days
long
er a
fter d
iagn
osis
an
d liv
ed c
lose
r to
the
PC
P th
an
elig
ible
clie
nts
who
de
clin
ed. M
ay
mis
estim
ate
cost
of c
arin
g
for a
ll pe
ople
nee
ding
pal
liativ
e ca
re
be
caus
e st
udy
subj
ects
m te
nd to
be
youn
ger a
nd c
lose
r to
the
PC
P.
Tota
l cos
ts fo
r all
patie
nt-r
elat
ed
serv
ices
foun
d to
be
$1,6
25,6
58.0
7
(CA
N 2
007)
; $17
,112
.19/
patie
nt a
nd
$117
.95/
patie
nt d
ay. O
n pa
r with
per
di
em fu
ndin
g fo
r LTC
and
low
er th
an
hosp
itals
as
assi
gned
in O
ntar
io.
Out
com
e
Con
clus
ions
ab
out t
he
focu
s
Diff
eren
ces
amon
g gr
oups
Res
ourc
e ut
iliza
tion/
co
st
Met
hods
Lite
ratu
re re
view
(non
-sy
stem
atic
).
Com
pare
s el
igib
le
parti
cipa
nts
who
agr
ee to
th
e st
udy
to th
ose
who
w
ere
elig
ible
but
refu
sed,
th
e en
tiret
y of
pro
gram
en
rolle
es, a
nd a
ll ca
ncer
de
cede
nts
in th
e
prov
inci
al c
ance
r reg
istry
.
Com
pare
d by
sex
, age
, di
stan
ce to
PC
P,
ho
useh
old
inco
me,
and
su
rviv
al ti
me
afte
r can
cer
diag
nosi
s if
appl
icab
le.
Cos
ts w
ere
track
ed o
ver
15 m
onth
s be
twee
n Ja
nuar
y 20
05-M
arch
200
6 us
ing
CC
AC
, E
PC
T an
d O
HIP
fee
sche
dule
s.
Cos
t-ana
lysi
s fo
rm o
f ec
onom
ic e
valu
atio
n.
Focu
s
The
in/d
irect
co
sts
asso
ciat
ed
with
com
mun
ity-
base
d se
rvic
es in
Can
ada.
Gen
eral
izab
ility
of
com
mun
ity-
base
d pr
ogra
ms
cost
est
imat
es.
Rol
e of
sel
ectio
n bi
as, e
ligib
ility
cr
iteria
, ref
usal
bi
as.
The
cost
of
com
mun
ity-b
ased
pa
lliat
ive
care
in
Ont
ario
from
MoH
pe
rspe
ctiv
e.
Setti
ng
Can
ada
Hal
ifax,
Nov
a
Sco
tia,
Can
ada
Ont
ario
, C
anad
a
Sam
ple
Pap
ers
stud
ying
co
mm
unity
-bas
ed c
are
in C
anad
a
50 p
atie
nts
refe
rred
to
the
palli
ativ
e ca
re
prog
ram
in H
alifa
x be
twee
n Fe
b 7,
200
5 an
d N
ov 2
9, 2
005;
co
mpa
red
to10
10
clie
nts
in th
e P
CP
who
w
ere
not s
ubje
cts
of
this
stu
dy.
45/5
0 ha
d ca
ncer
95 p
atie
nts
in s
hare
d-ca
re/ h
ome-
base
d pa
lliat
ive
care
in ru
ral
Ont
ario
.
87%
had
can
cer.
Ave
rage
age
71
Des
ign
Nar
rativ
e re
view
Cas
e co
ntro
l
Coh
ort s
tudy
Art
icle
Lyzw
insk
i (20
12)
Pal
liativ
e an
d S
uppo
rtive
Car
e
Lave
rgne
et a
l (2
011)
Jour
nal o
f Pai
n an
d S
ympt
om
Man
agem
ent
Klin
ger e
t al
(201
1)
Pal
liativ
e M
edic
ine

Appendices R. Redmond-Misner
126
Wea
knes
ses
Upp
er li
mit
on in
com
e ca
tego
ries
may
hav
e be
en lo
w ($
61,0
00+)
or
had
a lo
t of v
aria
bilit
y.
Did
not
mea
sure
tim
e sp
an o
f car
e be
fore
the
prog
ram
; con
serv
ativ
e es
timat
es. S
ome
patie
nts
had
mul
tiple
ca
regi
vers
(no
t co
ntro
lled
for)
.
Rel
ianc
e on
sel
f-rep
orts
of
car
egiv
er (s
ocia
l de
sira
bilit
y bi
as).
Not
gen
eral
izab
le to
ot
her t
ypes
of p
allia
tive
care
. Met
hods
of c
ostin
g ca
regi
ver t
ime
vuln
erab
le to
con
test
.
Eng
lish
only
.
Mos
t gre
y lit
erat
ure.
UK
ba
sed.
Met
hodo
logi
cally
qu
estio
nabl
e ar
ticle
s in
clud
ed.
Gen
eral
izab
ility
.
Res
ults
9% o
f fam
ilies
incu
rred
ec
onom
ic lo
sses
in
exce
ss o
f 10%
of t
heir
pre-
stud
y gr
oss
annu
al
inco
me.
Low
-inco
me
stat
us in
crea
sed
from
27
% to
40%
.
Mea
n m
onth
ly c
ost p
er
patie
nt $
24,5
49 (2
008
CD
N$)
. Fam
ily
care
give
rs c
onst
itute
70
% o
f tha
t. C
osts
are
gr
eate
r for
pat
ient
s cl
oser
to d
eath
, with
lo
wer
phy
sica
l fu
nctio
ning
, and
who
liv
ed w
ith s
omeo
ne.
Fina
ncia
l cos
t of c
arin
g
for s
omeo
ne a
t the
EoL
is
subs
tant
ial a
nd o
f 3
sour
ces:
wor
k-re
late
d,
out-o
f-poc
k-et
, and
tim
e.
Thes
e re
sulte
d in
maj
or
life
chan
ges
for
care
give
rs. S
train
was
as
soci
ated
with
dis
ease
st
age,
SE
S a
nd
et
hnic
ity.
Out
com
e
Eco
nom
ic
loss
Tota
l cos
t
Con
clus
ions
ab
out
info
rmal
cost
of c
are
Met
hods
Sam
ples
of p
allia
tive
ca
re p
atie
nts
livin
g at
ho
me
and
thei
r mai
n in
form
al c
areg
iver
s re
crui
ted
from
5 c
ities
an
d in
terv
iew
ed b
i- w
eekl
y. P
artic
ipan
ts
aske
d to
pro
vide
det
ails
ab
out t
heir
expe
nses
and
abse
nces
from
wor
k th
at re
late
d to
the
patie
nt’s
con
ditio
n.
Dat
a co
llect
ed fr
om
enro
llmen
t unt
il de
ath
via
inte
rvie
ws
with
ca
regi
vers
. Mul
tivar
iabl
e re
gres
sion
use
d to
as
sess
det
erm
inan
ts o
f va
riabi
lity
in th
e to
tal
cost
s.
Sys
tem
atic
revi
ew o
f M
ED
LIN
E, C
ochr
ane,
E
conL
it, C
INA
HL,
E
mba
se. A
ppra
ise
met
hods
. Syn
thes
ize.
Arti
cles
from
ince
ptio
n
of
data
base
to
2012
.
Focu
s
Impa
ct o
f eco
nom
ic
loss
on
info
rmal
ca
regi
vers
vi
s- à
-vis
Sta
tistic
s C
anad
a’s
low
-I nc
ome
cut o
ff.
Est
imat
ing
the
soci
etal
cos
t of
hom
e-ba
sed
pa
lliat
ive
care
and
de
term
inan
ts
of
varia
bilit
y.
Cos
t of u
npai
d ca
re in
palli
ativ
e ho
me
ca
re.
Setti
ng
Can
ada
Ont
ario
,
Can
ada
Inte
rnat
iona
l
Sam
ple
192
fam
ily u
nits
pr
ovid
ing
care
at
hom
e fo
r a te
rmin
al
patie
nt fr
om
Janu
ary
2005
-O
ctob
er 2
006
in
Hal
ifax,
Mon
treal
, W
inni
peg,
E
dmon
ton
and
Vic
toria
136
patie
nt-
care
give
r dy
ads
in
Ont
ario
hom
e ca
re
prog
ram
s6
Inte
rnat
iona
l
Des
ign
Pro
spec
tive
co
hort
stud
y
Pro
spec
tive
coho
rt st
udy
Sys
tem
atic
revi
ew
Art
icle
Jaco
bs e
t al
(201
1)
Pal
liativ
e C
are
Gue
rrie
re e
t al
(201
0)
Pal
liativ
e M
edic
ine
Gar
dine
r et a
l (2
014)
Pal
liativ
e M
edic
ine
6 Dotted borders indicate instances of double-publication.

Appendices R. Redmond-Misner
127
Wea
knes
ses
The
time
spen
t at h
ome
inst
ead
of in
patie
nt c
are
is n
ot
com
pens
ated
for u
sing
a
soci
etal
per
spec
tive/
acco
untin
g fo
r the
cos
t of c
areg
ivin
g. C
ost
is le
ss b
ecau
se th
ey p
ay fo
r all
the
inpa
tient
ser
vice
redu
cing
ap
plic
abili
ty.
Non
-ran
dom
(sel
ectio
n bi
as).
Sm
all s
ampl
e.
Diff
eren
ces
in s
ocia
l pr
ogra
ms/
polic
ies
betw
een
the
5 pr
ovin
ces
are
not t
aken
into
ac
coun
t.
Mai
nly
canc
er p
atie
nts;
trea
ted
as h
omog
enou
s gr
oup.
Lim
ited
to p
atie
nts
in P
CP
s,
mos
tly c
ance
r pat
ient
s.
Gen
eral
izab
ility
que
stio
nabl
e.
Soc
ial d
esira
bilit
y bi
as- s
ome
cost
s co
llect
ed fr
om p
atie
nts
and
care
give
rs.
Res
ults
Pat
ient
s in
trea
tmen
t gro
up
mor
e lik
ely
to d
ie a
t hom
e an
d re
duce
d c
osts
acr
oss
all
prim
ary
diag
nose
s, w
ith s
ome
diffe
renc
e in
sav
ing
betw
een
them
. Can
cer m
ost c
omm
on.
40%
non
-whi
te. C
ance
r sav
es
$593
6. C
OP
D s
aves
$11
325.
C
HF
save
s $8
445
(US
- pat
ient
pa
ys).
The
publ
ic h
ealth
car
e sy
stem
, th
e fa
mily
, and
not
-for-
prof
it
orga
niza
tions
sus
tain
ed
resp
ectiv
ely
71.3
%,
26.
6%,
an
d 1.
6% o
f the
mea
n to
tal
co
st p
er
patie
nt.
Tota
l cos
t of c
are
inc
reas
ed
from
the
fifth
to
the
last
mon
th o
f life
. A la
rge
part
of
th
is w
as a
ttrib
utab
le to
inpa
tient
car
e. T
he la
rges
t in
crea
se in
out
patie
nt c
are
co
sts
was
ob
serv
ed fo
r hom
e ca
re. I
nfor
mal
car
e co
sts
are
high
est f
or th
e la
st 3
mon
ths.
Out
com
e
Pla
ce o
f dea
th a
nd
cost
of
car
e
Tota
l cos
t/cos
t-
shar
e am
ong
publ
ic
heal
th c
are
syst
em,
th
e fa
mily
and
non
-pr
ofits
whe
re
appl
icab
le
Mon
thly
soc
ieta
l
cost
Met
hods
Trea
tmen
t gro
up re
ceiv
ed
inte
rdis
cipl
inar
y ho
me-
base
d P
C a
nd c
ontro
l rec
eive
d
usua
l ser
vice
s bt
w 1
999
and
2001
. Com
pare
d co
ntro
lling
fo
r pat
ient
dem
o-gr
aphi
cs
and
sym
ptom
sev
erity
(MLR
). C
osts
from
per
spec
tive
of th
e pr
ovid
er K
aise
r Per
man
ente
.
Pro
spec
tive
rese
arch
des
ign
w
ith re
peat
ed m
easu
res.
In
terv
iew
s at
2 w
eek
in
terv
als.
Sta
tistic
al a
naly
ses.
C
ostin
g w
ith re
com
men
datio
- n
of th
e C
anad
ian
Coo
rdin
atin
g O
ffice
for H
TA &
Dru
mm
ond;
el
emen
ts o
f a) q
uant
ities
used
and
b) u
nit c
osts
. S
ocie
tal p
ersp
ectiv
e.
Pro
spec
tive
rese
arch
des
ign
w/ r
epea
ted
mea
sure
s.
Inte
rvie
ws
at 2
wee
k in
terv
als.
Sta
tistic
al a
naly
ses
on m
onth
-by-
mon
th b
asis
for
5 m
onth
s pr
ior t
o de
ath.
Soc
ieta
l per
spec
tive.
Focu
s
Pla
ce o
f dea
th a
nd
cost
of s
ervi
ces
by
prim
ary
diag
nosi
s fo
r pa
tient
s re
ceiv
ing
hom
e-ba
sed
palli
ativ
e ca
re c
ompa
red
to
usua
l car
e.
Cos
t of
reso
urce
ut
iliza
tion
by p
allia
tive
care
reci
pien
ts li
ving
at
hom
e.
Cos
t of
res
ourc
e ut
iliza
tion
over
the
palli
ativ
e tra
ject
ory
(com
mun
ity-b
ased
pr
ogra
ms)
.
Setti
ng
Cal
iforn
ia,
Uni
ted
Sta
tes
Can
ada
Can
ada
Sam
ple
Term
inal
ly il
l pa
tient
s; 1
59 in
ho
me
care
and
139
co
ntro
ls. D
iagn
osed
w
ith c
ance
r, co
nges
tive
hear
t fa
ilure
(CH
F), o
r ch
roni
c ob
stru
ctiv
e pu
lmon
ary
dise
ase
(CO
PD
)
248
patie
nt-
care
give
r dya
ds in
P
CP
s fro
m J
anua
ry
2005
-Dec
embe
r 20
06 in
in H
alifa
x,
Mon
treal
, Win
nipe
g,
Edm
onto
n an
d V
icto
ria
160
patie
nt-
care
give
r dya
ds i
n P
CP
s fro
m J
anua
ry
2005
-Oct
ober
200
6 in
H
alifa
x, M
ontre
al,
Win
nipe
g,
Edm
onto
n an
d V
icto
ria
Des
ign
Cas
e co
ntro
l
Coh
ort s
tudy
Coh
ort s
tudy
Art
icle
Eng
uida
nos
et a
l (2
005)
Jour
nal o
f Soc
ial
Wor
k in
EoL
&
Pal
liativ
e C
are
Dum
ont e
t al
(200
9)
Pal
liativ
e M
edic
ine
Dum
ont e
t al
(201
0)
Pal
liativ
e M
edic
ine

Appendices R. Redmond-Misner
128
Wea
knes
ses
Cos
ting
met
hod
vuln
erab
le to
con
test
; re
lies
on p
oten
tial
earn
ings
rath
er th
an
actu
al e
arni
ngs.
Gen
eral
izab
ility
.
Rec
all a
nd s
ocia
l de
sira
bilit
y bi
as.
Sm
all s
ampl
e.
No
cont
rol g
roup
.
Min
iste
rial c
ost o
nly.
Nov
el m
odel
for
haem
atol
ogic
pat
ient
s;
non-
gene
raliz
able
, ha
rd to
ver
ify o
r co
nfid
ently
end
orse
th
is ty
pe o
f mod
el fo
r ad
optio
n. N
eeds
mor
e re
sear
ch in
this
are
a.
Low
repr
esen
tatio
n
for m
inor
ity g
roup
s.
Gen
eral
izab
ility
. R
elyi
ng o
n ho
me
deat
h, n
ot P
OD
pr
efer
ence
, as
mea
sure
men
t of
patie
nt p
refe
renc
e.
Res
ults
Ave
rage
mon
thly
cos
t was
$14
924
(201
1 C
DN
$) p
er p
atie
nt in
la
st y
ear o
f life
. Unp
aid
care
givi
ng
cost
s– $
11 3
34 –
acc
ount
for 7
7%
follo
wed
by
publ
ic c
osts
($32
11;
21%
) and
out-o
f-poc
ket (
$379
; 2%
). M
onth
ly
cost
s in
crea
sed
with
pro
xim
ity to
de
ath.
Dis
char
ged
early
and
term
inal
phas
e re
quire
d th
e m
ost h
ome
visi
ts (a
vg 2
7.2
and
24.1
), tra
nsfu
sion
s (6
.1 a
nd 6
.8) a
nd d
ays
of
car
e (2
2.8
and
19.7
). M
ean
mon
thly
cos
ts d
eter
min
ed b
y
dise
ase
stat
us a
nd tr
ansf
usio
n re
quire
men
ts. M
MC
for t
erm
inal
pa
tient
s (4
,232
.50€
) and
thos
e di
scha
rged
ear
ly (3
,986
.40€
) wer
e hi
gher
than
thos
e fo
r adv
ance
d (2
,303
.80€
) and
chr
onic
pat
ient
s (1
,488
,30€
). H
C c
ost w
as lo
wer
than
the
corr
espo
ndin
g ho
spita
l ch
arge
s, b
ut e
xcee
ded
the
dist
rict
fare
s fo
r the
HC
of c
ance
r pat
ient
s.
Inte
rven
tion
grou
p re
porte
d gr
eate
r im
prov
emen
t in
satis
fact
ion
at 3
0 an
d 90
day
s, w
ere
mor
e lik
ely
to d
ie
at h
ome,
less
like
ly to
vis
it th
e em
erge
ncy
depa
rtmen
t or b
e ad
mitt
ed to
the
hosp
ital r
esul
ting
in
low
er c
osts
.
Out
com
e
Unp
aid
ca
regi
ving
cos
t, pu
blic
cos
t,
out-o
f-poc
ket
co
st
Rec
ours
e
utili
zatio
n co
st
Sat
isfa
ctio
n,
utili
zatio
n, P
OD
, co
st
Met
hods
Pro
spec
tive
coho
rt st
udy
recr
uite
d pa
rtici
pant
s fro
m P
CP
an
d in
terv
iew
ed b
y-w
eekl
y fro
m a
dmis
sion
unt
il de
ath.
C
ostin
g do
ne u
sing
Am
bula
tory
H
ome
Car
e R
ecor
d. S
ocie
tal
pers
pect
ive.
Sta
tistic
al a
naly
ses.
Dat
a de
scrib
ed fr
om c
linic
al
reco
rds
and
data
base
whe
re
al
l h
ome
activ
ities
wer
e re
cord
ed. C
osts
per
tain
ed to
he
alth
car
e pr
ovid
ers,
mat
eria
ls
and
med
icin
es, t
rans
fusi
ons,
an
d la
bora
tory
(blo
od c
hem
istry
, m
icro
biol
ogy)
. Pat
ient
s di
vide
d in
to te
rmin
al p
hase
, adv
ance
d ph
ase,
chr
onic
pha
se a
nd
“dis
char
ged
early
with
cur
able
di
seas
e.”
152
rece
ive
usua
l car
e an
d 14
5 re
ceiv
e th
e in
terv
entio
n pl
us
usua
l car
e. T
est h
ypot
hesi
s
that
the
new
trea
tmen
t wou
ld
impr
ove
satis
fact
ion
and
cost
.
Focu
s
The
mag
nitu
de,
sh
are
and
dete
rmin
ants
of
palli
ativ
e ho
me
care
cost
s th
at a
re
un
paid
car
egiv
ing.
Cos
t ana
lysi
s o
f ho
me
care
fo
r PC
pa
tient
s w
ith
haem
atol
ogic
m
alig
nanc
ies
spec
ifica
lly.
Usu
al c
are
vs.
usua
l car
e pl
us in
-ho
me
palli
ativ
e ca
re.
Setti
ng
Toro
nto,
C
anad
a
Italy
Col
orad
o
(N
=14)
and
H
awai
i (N
=150
)
Sam
ple
169
patie
nt-c
areg
iver
dy
ads
with
prim
ary
canc
er d
iagn
oses
fro
m T
oron
to (M
ount
S
inai
) btw
Jul
y 20
05
and
Sep
tem
ber 2
007
144
patie
nts
with
ha
emat
olog
ic
mal
igna
ncie
s of
va
riabl
e di
seas
e
stat
us b
tw 2
004-
2006
298
hom
e-bo
und,
term
inal
ly il
l pat
ient
s w
ith C
OP
D a
nd C
HF
Des
ign
Pro
spec
tive
coho
rt st
udy
Coh
ort s
tudy
RC
T
Art
icle
Cha
i et a
l (20
14)
Hea
lth a
nd
S
ocia
l C
are
in
the
Com
mun
ity
Car
toni
et a
l (2
007)
Hae
mat
olog
ica/
the
hem
atol
ogy
jour
nal
Bru
mle
y et
al
(200
7)
Jour
nal o
f the
A
mer
icn
Ger
iatri
cs S
ocie
ty

Appendices R. Redmond-Misner
129
Appendix C Detailed characteristics of caregiver burden papers
Wea
knes
ses
Syn
thes
izes
exi
stin
g
evid
ence
but
do
es
not p
rovi
de m
uch
new
.
Non
-sys
tem
atic
revi
ew,
incl
usio
n cr
iteria
un
clea
r, in
clus
ion/
se
lect
ion
bias
.
Pat
ient
s w
ith n
o
care
give
rs e
xclu
de
(not
the
poin
t of t
his
st
udy,
but
onc
e ag
ain
thei
r out
com
es a
re
mis
sing
).
Com
para
bilit
y; m
ost
stud
ies
are
prim
arily
w
hite
sub
ject
s (th
ough
st
udyi
ng a
noth
er
popu
latio
n is
a
poss
ible
stre
ngth
). Fi
ndin
gs a
re
cons
iste
nt w
ith o
ther
st
udie
s.
Res
ults
Car
egiv
ers
repo
rt un
met
nee
ds fo
r in
form
atio
n, c
omm
unic
atio
n, s
ervi
ce p
rovi
sion
an
d su
ppor
t fro
m h
ealth
and
com
mun
ity
serv
ices
. Wan
t to
know
how
to p
rovi
de
prac
tical
car
e, h
ow to
com
fort
the
patie
nt,
wha
t to
expe
ct, h
ow to
dea
l with
sym
ptom
s,
how
to a
cqui
re a
ids
like
wal
king
fram
es a
nd
whe
elch
airs
etc
. Stu
dy re
veal
ed (i
) bar
riers
to
seek
ing
help
; (ii)
lack
of r
esea
rch-
base
d in
terv
entio
ns fo
cuse
d on
redu
cing
the
nega
tive
aspe
cts
of c
areg
ivin
g; a
nd (i
ii)
impe
dim
ents
to e
ffect
ive
polic
y an
d se
rvic
e de
velo
pmen
t for
fam
ily c
areg
iver
s. L
ack
out
outc
ome
evid
ence
am
ong
care
give
rs- e
thic
s pr
oble
ms
w/ R
CTs
. C
areg
iver
s of
pat
ient
s w
ho d
ied
at h
ome
thou
ght t
hat i
t had
a m
ore
posi
tive
influ
ence
on
the
patie
nts’
QoL
than
was
the
case
in th
e ot
her g
roup
s, w
ere
mor
e sa
tisfie
d w
ith th
eir
own
achi
evem
ent,
but
als
o ex
perie
nced
the
mos
t sle
ep d
epriv
atio
n. c
areg
iver
opi
nion
of
why
pat
ient
s ne
eded
hos
pice
car
e w
as
near
ly th
e sa
me
in g
roup
s 1
and
2:
acut
ely
deve
lopi
ng s
ympt
oms.
Fact
or a
naly
sis
of th
e C
SI
(rol
e, p
erso
nal,
and
emot
iona
l stra
in) f
ound
pat
ient
pro
blem
be
havi
ors
pred
ict a
ll ty
pes
of c
areg
iver
stra
in.
Per
ceiv
ed la
ck o
f sup
port
from
the
heal
th
care
team
pre
dict
ed p
erso
nal a
nd e
mot
iona
l st
rain
. Hig
her i
ncom
e pr
edic
ted
role
stra
in.
Pat
ient
func
tiona
l lim
itatio
ns p
redi
cted
pe
rson
al a
nd ro
le s
train
.
Out
com
e
Com
mon
ly
repo
rted
expe
rienc
es a
nd
unm
et
need
s
Car
egiv
er
expe
rienc
es
Car
egiv
er S
train
In
dex
(CS
I)
scor
es
Met
hods
Lite
ratu
re re
view
(non
-sy
stem
atic
) plu
s
su
rvey
of h
ome
care
pr
ovid
ers
to
valid
ate/
cont
est t
he
findi
ngs
of th
e
lit
erat
ure
revi
ew.
Pat
ient
s re
crui
ted
from
ad
vanc
ed p
allia
tive
hom
e ca
re te
ams
and
a
hosp
ice
in U
ppsa
la
durin
g 1
year
(vag
ue)
stud
y pe
riod.
A
ques
tionn
aire
was
m
aile
d to
car
egiv
ers
an
d m
edic
al re
cord
s w
ere
anal
yzed
.
Dat
a co
llect
ed th
roug
h st
ruct
ured
inte
rvie
ws
w
ith a
ll ca
regi
vers
usin
g C
areg
iver
Stra
in
Inde
x, R
evis
ed
M
emor
y an
d
B
ehav
iour
Pro
blem
s C
heck
list a
nd th
e K
atz
Inde
x of
Act
iviti
es o
f D
aily
Liv
ing
to
unde
rsta
nd s
ituat
iona
l ch
arac
teris
tics.
Focu
s
Bar
riers
to
addr
essi
ng th
e un
met
nee
ds o
f ca
regi
vers
in
palli
ativ
e ho
me
care
.
Doe
s ca
regi
ver
perc
eptio
n of
pa
lliat
ive
care
di
ffer d
epen
ding
on
pla
ce o
f car
e
and
deat
h?
Iden
tifyi
ng th
e is
sues
/ ch
arac
teris
tics
of
pro
vidi
ng
palli
ativ
e ca
re
to
peo
ple
with
de
men
tia
spec
ifica
lly.
Setti
ng
Aus
tralia
Upp
sala
, S
wed
en
Uni
ted
S
tate
s
Sam
ple
20 c
areg
iver
s, 6
vo
lunt
eers
and
23
serv
ice
prov
ider
s su
bmitt
ed
desc
ribin
g th
eir
expe
rienc
e an
d un
met
nee
ds.
Maj
ority
fem
ale
wiv
es/d
augh
ters
ca
ring
for s
omeo
ne
with
can
cer o
r de
men
tia
Car
egiv
ers
to
patie
nts
in h
ome
care
who
die
d a
t ho
me
(N =
63) (
1),
at
hos
pice
(N=
51)
(2),
and
care
in
hosp
ice
dyin
g at
ho
spic
e (N
=69)
(3)
150
prim
arily
bla
ck
care
give
rs o
f pa
tient
s w
ith
dem
entia
in
palli
ativ
e ca
re
Des
ign
Lite
ratu
re
revi
ew/
C
ohor
t stu
dy
Cas
e co
ntro
l
Coh
ort s
tudy
Art
icle
Aou
n et
al
(200
5)
Pal
liativ
e M
edic
ine
Car
lsso
n et
al
(200
3)
Pal
liativ
e an
d S
uppo
rtive
C
are
Diw
an e
t al
(200
4)
Jour
nal o
f P
allia
tive
Med
icin
e

Appendices R. Redmond-Misner
130
Wea
knes
ses
Lack
s si
gns
of th
orou
gh
re
view
i.e.
sta
ges
of t
he
sear
ch, p
roce
ss o
f arti
cle
sele
ctio
n, h
ow m
any
artic
les
re
view
ed.
Lack
of l
ongi
tudi
nal d
ata
on
phys
ical
bur
den.
Sam
ple
size
.
Non
-long
itudi
nal.
HA
DS
inst
rum
ent n
ot
appr
opria
te fo
r eve
ryon
e be
caus
e an
hedo
nia
is a
co
mm
on E
oL s
ympt
om,
Sat
urat
ion
may
not
hav
e be
en
achi
eved
Pos
sibi
lity
that
car
egiv
ers
who
de
clin
ed h
ad d
iffer
ent
expe
rienc
es.
Res
ults
Ove
r ½ o
f hom
e ca
regi
vers
repo
rt he
alth
pro
blem
s,
mai
nly
hear
t pr
oble
ms,
hyp
erte
nsio
n, a
nd a
rthrit
is.
Sta
ge o
f can
cer,
exte
nt o
f p
atie
nt
disa
bilit
y, h
ighe
r per
sona
l car
e ne
eds
of
the
patie
nt, l
ack
of p
atie
nt m
obili
ty,
patie
nt d
epen
denc
y
in in
stru
men
tal
activ
ities
ass
ocia
ted
with
adv
erse
ph
ysic
al c
areg
iver
out
-com
es.
Pat
ient
s’ a
nd c
areg
iver
s’ a
nxie
ty a
nd
depr
essi
on s
core
s w
ere
sign
ifica
ntly
co
rrel
ated
. 33%
of c
areg
iver
s ha
d hi
gh a
nxie
ty a
nd 2
8 %
dep
ress
ion.
¼
patie
nts
had
clin
ical
ly re
leva
nt a
nxie
ty
and ½
had
clin
ic-a
lly s
ympt
omat
ic
depr
essi
on s
core
s.
Them
es: t
he s
igni
fican
t bur
den
of
poly
phar
mac
y; th
e po
sitiv
e im
pact
of
subc
utan
eous
infu
sion
s; th
e va
lue
of
bein
g ab
le to
giv
e m
edic
atio
ns a
s ne
eded
for s
ympt
om c
ontro
l
Out
com
e
Phy
sica
l
heal
th
need
s
of
care
give
rs
Psy
chol
ogic
al
dist
ress
Exp
erie
nces
re
porte
d by
ca
regi
vers
Met
hods
Rev
iew
of P
ubM
ed a
nd
CIN
AH
L us
ing
key
te
rms
“Car
egiv
er b
urde
n,” “
phys
ical
w
ell-b
eing
” and
“adv
erse
ph
ysic
al o
utco
mes
.”
QoL
was
col
lect
ed w
ith th
e E
OR
TC Q
LQ -C
15-P
AL
(pat
ient
s) a
nd th
e S
hort
Form
-8 H
ealth
Sur
vey
(car
egiv
ers)
; Psy
chol
ogic
al
dist
ress
with
Hos
pita
l Anx
iety
an
d D
epre
ssio
n S
cale
(H
AD
S)
Them
atic
con
tent
ana
lysi
s of
fo
cus
grou
ps. D
iscu
ss
poly
phar
mac
y th
e us
e of
sy
ringe
s an
d as
-nee
ded
med
s by
info
rmal
car
egiv
ers.
Focu
s
Iden
tifyi
ng p
hysi
cal
he
alth
nee
ds
and
vuln
erab
ilitie
s o
f pa
lliat
ive
onco
logy
ca
regi
vers
.
Psy
chol
ogic
al d
istre
ss
and
QoL
for
pa
tient
s an
d ca
regi
vers
in
palli
ativ
e c
ance
r ho
me
care
.
Car
egiv
er e
xper
ienc
e m
anag
ing
med
icat
ions
for
palli
ativ
e ca
re
patie
nts.
Setti
ng
Inte
rnat
iona
l
Leip
zig,
Ger
man
y
Nor
th E
ast R
egio
n,
Irela
nd
Sam
ple
Lite
ratu
re
disc
ussi
ng h
ealth
im
plic
atio
ns o
f ca
regi
ving
for
care
give
rs
106
patie
nt
care
give
r dy
ads
in p
allia
tive
onco
logi
c h
ome
care
68%
fem
ale
3 fo
cus
grou
ps
(N=1
8) o
f be
reav
ed
care
give
rs w
ho
care
d fo
r so
meo
ne a
t ho
me
Des
ign
Sys
tem
atic
re
view
Coh
ort s
tudy
Qua
litat
ive
Art
icle
Gla
jche
n (2
012)
Sem
inar
s in
O
ncol
ogy
Nur
sing
Göt
ze (2
014)
Sem
inar
s in
O
ncol
ogy
Nur
sing
She
ehy-
Ske
ffing
ton
et a
l (2
013)
Am
eric
an J
ourn
al
of H
ospi
ce &
P
allia
tive
Med
icin
e

Appendices R. Redmond-Misner
131
Wea
knes
ses
Sel
f-sel
ectio
n in
favo
ur o
f tho
se
with
ene
rgy/
inte
rest
in c
ance
r and
ca
regi
ving
. Sel
ectio
n bi
as. M
ay
be m
ore
dyad
s w
ithou
t con
flict
th
an w
ith. M
any
decl
ined
beca
use
they
wer
e to
o tir
ed.
Res
ults
may
not
refle
ct e
very
one.
S
mal
l sam
ple.
Car
egiv
er s
atis
fact
ion
rath
er th
an
patie
nt- t
his
is p
artia
lly b
ecau
se
patie
nts
coul
dn’t
resp
ond
by th
e
EoL
. Res
ults
may
not
be
gene
raliz
able
to o
ther
pop
ulat
ions
.
Due
to s
ize
of s
ampl
e, li
mite
d in
nu
mbe
r of v
aria
bles
that
cou
ld b
e co
ncur
rent
ly a
sses
sed.
Pot
entia
l om
itted
var
iabl
e bi
as (u
sed
back
war
d st
epw
ise
to c
ount
er
this
). Th
e in
terR
AI P
C d
oes
not i
nclu
de
care
give
r sex
or a
ge. H
as b
een
show
n in
oth
er re
sear
ch th
at
olde
r car
egiv
ers
have
wor
se
perc
eive
d he
alth
and
incr
ease
d pr
escr
iptio
n dr
ug u
se.
Cro
ss-s
ectio
nal d
ata
limits
abi
lity
to s
ee te
mpo
ral o
rder
of
asso
ciat
ions
foun
d.
Res
ults
Sup
ports
the
findi
ng th
at o
nly
care
give
rs’ d
epre
ssio
n ha
s a
dire
ct
sign
ifica
nt a
ssoc
iatio
n w
ith c
areg
iver
bu
rden
, and
sho
ws
tha
t the
effe
cts
of
the
othe
r ind
epen
dent
var
iabl
es o
n bu
rden
are
med
iate
d th
roug
h de
pres
sion
. In
Mod
el 2
, anx
iety
and
de
pres
sion
are
med
iatin
g fa
ctor
s be
twee
n 3
IVs
(soc
ial s
uppo
rt-
depr
essi
on, p
hysi
cal h
ealth
- anx
iety
) an
d ca
regi
ver b
urde
n, a
nd 1
2% o
f the
varia
nce
is e
xpla
ined
.
Eac
h of
the
nine
qua
lity
of c
are
para
met
ers
wer
e co
nsis
tent
ly fo
und
to
be s
igni
fican
t pre
dict
ors
of o
vera
ll
satis
fact
ion
with
pal
liativ
e ca
re. T
hey
w
ere
“alw
ays
spen
t eno
ugh
time,
” “n
ever
arr
ived
late
,” “n
ever
bee
n ha
rd
to re
ach,
” “ne
ver s
eem
ed d
istra
cted
,” “a
lway
s w
illin
g to
list
en,”
“nev
er
treat
ed m
ore
as a
dis
ease
than
a
pers
on,”
“alw
ays
show
ed p
erso
nal
conc
ern,
” “al
way
s re
spon
ded
quic
kly,
” “n
ever
igno
red.
” C
areg
iver
dis
tress
was
evi
dent
for
22
% o
f pa
lliat
ive
hom
e ca
re c
lient
s.
Clin
ical
inst
abili
ty d
epre
ssiv
e
sym
ptom
s, c
ogni
tive
impa
irmen
t, an
d po
sitiv
e ou
tlook
iden
tifie
d as
as
clie
nt-
leve
l pre
dict
ors.
Ser
vice
use
/ pro
vide
r va
riabl
es p
redi
ctin
g ca
regi
ver d
istre
ss
incl
ude
the
spec
ific
hom
e ca
re a
genc
y,
hosp
italiz
atio
ns in
the
last
90
day
s,
and
nurs
ing
visi
ts.
Out
com
e
Car
egiv
er b
urde
n
Sat
isfa
ctio
n w
ith
hom
e c
are
expe
rienc
e
Indi
cato
rs o
f ca
regi
ver d
istre
ss
Met
hods
Wea
knes
ses
Sec
onda
ry a
naly
sis
of a
n ex
istin
g da
tase
t- no
t all
varia
bles
of
pred
icte
d va
riabl
es w
ere
incl
uded
a
prio
ri. C
lust
er m
etho
ds
not
supp
orte
d by
ext
ensi
ve s
tatis
tical
re
ason
ing
(no
defin
itive
test
exi
sts
to d
eter
min
e if
true
clus
terin
g is
pr
esen
t in
the
data
; ge
nera
lizab
ility
.
Faci
litie
s lim
ited
to 1
are
a
in
Japa
n.
Vas
t var
iatio
n in
pos
t-be
reav
emen
t (6
mon
ths
– 2½
ye
ars)
, rec
all b
ias.
Cro
ss-s
ectio
nal,
cann
ot s
ee h
ow it
ch
ange
s ov
er ti
me.
Can
not s
ee
caus
al d
irect
ion
as w
ell.
Car
er’s
men
tal s
tate
may
influ
ence
as
sess
men
t of
self-
repo
rted
mea
sure
Rec
all b
ias
Res
ults
Sel
f-rep
orte
d an
xiet
y an
d
com
pete
nce
subs
cale
tota
l sco
res
at
the
time
of
com
men
cem
ent
wer
e as
soci
ated
with
ca
regi
vers
at r
isk
of lo
wer
leve
ls o
f ps
ycho
soci
al fu
nctio
ning
5 w
eeks
late
r. P
ossi
ble
to id
entif
y vu
lner
able
car
egiv
ers
early
.
Fact
or a
naly
sis
resu
lted
in 2
9 it
ems
and
8 fa
ctor
s: B
urde
n of
Car
e, C
once
rns
abou
t H
ome
Car
e D
octo
r, B
alan
ce o
f Wor
k an
d C
are,
Pat
ient
’s P
ain
and
Con
ditio
n, C
once
rns
abou
t Vis
iting
Nur
se, C
once
rns
abou
t Hom
e C
are
Ser
vice
, Rel
atio
nshi
p be
twee
n Fa
mily
C
areg
iver
s an
d th
eir F
amili
es, a
nd F
uner
al
Pre
para
tions
.
Car
ers
foun
d to
hav
e be
tter p
hysi
c-al
hea
lth
and
wor
se m
enta
l hea
lth th
an th
e ge
nera
l po
pula
tion.
35%
repo
rted
thei
r hea
lth to
be
wor
se th
an it
was
on
e ye
ar a
go. H
RQ
OL
of
care
rs w
hose
he
alth
had
det
erio
r-at
ed in
the
pr
evio
us y
ear w
as a
ssoc
iate
d w
ith th
e pa
tient
’s
care
nee
ds b
ut n
ot ti
me
in
put,
unlik
e th
e ca
rers
repo
rting
st
able
hea
lth’s
HR
QO
L.
Car
er’c
cla
ssifi
ed a
s st
able
if th
ey re
porte
d
thei
r hea
lth th
e “s
ame”
as
the
prio
r y
ear.
Out
com
e
Pre
dict
ing
th
e vu
lner
abili
ty o
f in
form
al c
areg
iver
s
Com
plet
ed F
DS
The
HR
QO
L su
rvey
resu
lts o
f hom
e-ba
sed
palli
ativ
e ca
regi
vers
Met
hods
Dat
a ob
tain
ed a
t the
sta
rt of
ho
me-
base
d pa
lliat
ive
care
an
d 5-
wee
k fo
llow
-ups
in
clud
ing
inst
rum
ents
m
easu
ring
prep
ared
ness
, co
mpe
tenc
e, s
ocia
l sup
port,
an
xiet
y an
d se
lf-ef
ficac
y of
ca
regi
vers
(HA
DS
).
Dis
tribu
ted
Fam
ily’s
Diff
icul
ty
Sca
le (F
DS
) sur
vey,
whi
ch
was
der
ived
from
p
ilot
inte
rvie
ws
and
lit
revi
ews,
to
395
bere
aved
car
egiv
ers.
S
tatis
tical
ana
lyse
s.
The
cros
s-se
ctio
nal s
tudy
us
ed th
e S
hort
Form
-36
Hea
lth S
urve
y to
mea
sure
H
RQ
OL.
Thi
s su
rvey
is
adm
inis
tere
d to
the
gene
ral
popu
latio
n an
d m
easu
res
ph
ysic
al fu
nctio
n, b
odily
pai
n,
gene
ral h
ealth
, vita
lity,
soc
ial
func
tion,
em
otio
nal f
unct
ion,
m
enta
l hea
lth.
Focu
s
Pre
dict
ors
of
care
give
r ps
ycho
soci
al fu
nctio
n.
Fam
ily d
iffic
ulty
with
E
oL h
ome
c
are.
Hea
lth-r
elat
ed Q
oL o
f ca
regi
vers
.
Dim
ensi
ons
of th
e C
areg
iver
R
eact
ion
Ass
essm
ent:
self-
es
teem
, lac
k of
fam
ily s
uppo
rt,
finan
ces,
impa
ct o
n da
ily
sche
dule
; wer
e us
ed a
s th
e de
pend
ent v
aria
ble.
Inde
pend
ent
varia
bles
wer
e te
sted
in th
e m
odel
s: p
atie
nt p
ain,
fatig
ue,
an
d na
usea
; car
egiv
ers’
phy
sica
l Q
oL, a
nxie
ty a
nd d
epre
ssio
n,
an
d so
cial
sup
port.
Par
tial
le
ast s
quar
es p
ath
anal
ysis
.
Car
egiv
ers
inte
rvie
wed
biw
eekl
y fro
m h
ome
care
ad
mis
sion
unt
il de
ath.
S
atis
fact
ion
asse
ssed
usi
ng
th
e Q
ualit
y of
End
-of-L
ife c
are
and
Sat
isfa
ctio
n w
ith T
reat
men
t (Q
UE
ST)
que
stio
nnai
re. M
LR
used
to d
eter
min
e th
e ex
tent
to
whi
ch d
emog
raph
ic, q
ualit
y of
ca
re, a
nd s
ervi
ce re
late
d
varia
bles
pre
dict
ed s
atis
fact
ion.
Ass
essm
ents
per
form
ed b
y
case
man
ager
s du
ring
the
inte
rRA
I p
ilot i
mpl
emen
tatio
n
in 2
007-
09. M
ultiv
aria
te
anal
ysis
.
Focu
s
How
var
iabl
es
cont
ribut
ing
to
care
give
r bu
rden
ar
e co
rrel
ated
with
eac
h ot
her.
Car
egiv
er
satis
fact
ion
with
ho
me-
base
d
palli
ativ
e nu
rsin
g/
phys
icia
n ca
re.
Det
erm
inan
ts o
f ca
regi
ver b
urde
n am
ong
hom
e
ca
re c
lient
s.
Setti
ng
Nor
way
Ont
ario
, Can
ada
Ont
ario
, Can
ada
Sam
ple
96 c
areg
iver
s of
ca
ncer
pat
ient
s
in p
allia
tive
hom
e ca
re
104
fam
ily
care
give
rs o
f pa
lliat
ive
hom
e-ba
sed
patie
nts
All
reci
pien
ts o
f co
mm
unity
-
base
d pa
lliat
ive
care
who
wer
e as
sess
ed w
ith
th
e in
terR
AI P
C
Des
ign
Coh
ort s
tudy
Coh
ort s
tudy
Coh
ort s
tudy
Art
icle
Gro
v et
al (
2006
)
Soc
ial S
cien
ce &
M
edic
ine
Gue
rrie
re e
t al
(201
3)
Pal
liativ
e M
edic
ine
Hird
es e
t al
(201
2)
Pal
liativ
e an
d S
uppo
rtive
Car
e

Appendices R. Redmond-Misner
132
Wea
knes
ses
Low
resp
onse
rate
.
No
rand
omiz
atio
n (s
elec
tion/
conv
enie
nce
bias
).
Mos
t par
ticip
ants
wer
e no
t sp
oken
to u
ntil
6 m
onth
s in
to
bere
avem
ent (
reca
ll bi
as).
Gen
eral
izab
ility
.
care
give
rs n
ot li
ving
with
the
patie
nt le
ss a
cces
sibl
e to
the
trial
. Ext
erna
l val
idity
.
Mis
sing
dat
a du
e to
dea
th o
f th
e pa
tient
. Exc
lude
d da
ta
whe
re th
e pe
rson
die
d be
fore
th
e 4-
9- 1
2-w
eek
follo
w-u
ps
Attr
ition
hig
her t
han
expe
cted
, red
uced
pow
er.
Sm
all s
ampl
e si
ze
Ver
y sm
all h
ome
care
sa
mpl
e G
erm
an la
ngua
ge
only
. The
SE
IQoL
-DW
too
dem
andi
ng fo
r som
e pa
rtici
pant
s w
ho re
fuse
d (N
=4).
Dep
ress
ion
and
anxi
ety
of
the
patie
nt c
ould
not
be
asse
ssed
due
to to
o cr
itica
l
of c
ondi
tion
(8/2
7 fil
led
out
HA
DS
).
Res
ults
Dea
th a
t hom
e oc
curr
ed fo
r 80.
3% o
f pa
tient
s w
ith a
cces
s to
hom
ecar
e an
d
20.5
% o
f tho
se w
ithou
t acc
ess.
Des
pite
ca
ring
for a
love
d on
e at
hom
e be
ing
a gr
eate
r fin
anci
al a
nd e
mot
iona
l bur
den,
th
ere
was
mor
e sa
tisfa
ctio
n w
ith th
e ca
ring
expe
rienc
e of
thos
e w
hose
love
d on
es
di
ed a
t hom
e an
d ha
d ac
cess
to th
e ho
mec
are
prog
ram
. HC
pre
fera
ble
to m
ost
care
give
rs.
Sco
res
on th
e G
HQ
-28
fell
belo
w th
e th
resh
old
of 5
/6 in
a th
ird o
f par
ticip
ants
in
each
tria
l arm
at a
ny fo
llow
-up
poin
t. M
ean
scor
es in
the
inte
rven
tion
grou
p w
ere
lo
wer
at a
ll tim
e po
ints
but
diff
eren
ces
wer
e no
t sig
nific
ant.
No
diffe
renc
e w
as
obse
rved
in s
econ
dary
out
com
es. C
arer
s re
ceiv
ing
the
inte
rven
tion
repo
rted
qual
itativ
e be
nefit
.
Fifty
-nin
e pe
rcen
t did
not
rece
ive
any
finan
cial
aid
for h
ome
care
, 33%
had
in
crea
sed
risk
for p
sych
osom
atic
pro
blem
s,
45%
had
anx
iety
, and
33%
incr
ease
d de
pres
sion
leve
ls. T
he c
areg
iver
’s Q
oL
w
as m
ost s
trong
ly a
ffect
ed b
y th
e bu
rden
of c
are
(p <
.001
) and
the
patie
nt’s
men
tal s
tate
(p <
.03)
. The
mos
t
chal
leng
ing
aspe
ct fo
r th
e ca
regi
vers
was
th
e co
gniti
ve im
pairm
ent a
mon
g th
e P
MB
T pa
tient
s. P
artic
ular
ly e
xhau
stin
g an
d tro
ublin
g w
ere
chan
ges
in th
e pa
tient
s’
pers
onal
ity a
nd a
ggre
ssiv
e (u
npre
dict
able
) be
havi
or.
Out
com
e
Sat
isfa
ctio
n an
d ex
perie
nce
with
hom
e
deat
h
Car
egiv
er d
istre
ss
at
4-w
eek,
9-w
eek
and
12-w
eek
follo
w-
up
Car
egiv
er d
istre
ss
Met
hods
A to
tal o
f 159
ca
regi
vers
wer
e in
terv
iew
ed, 7
6
from
the
hom
e pa
lliat
ive
prog
ram
an
d 83
who
had
no
acce
ss to
a
palli
ativ
e ca
re
prog
ram
. Dat
a co
llect
ed a
nd
anal
yzed
.
Inte
rven
tion
(s
peci
alis
t pal
liativ
e ca
re s
ervi
ces)
of 6
w
eekl
y vi
sits
by
a tra
ined
adv
isor
pr
ovid
ed to
the
inte
rven
tion
grou
p.
2001
-200
3.
Inte
rvie
ws
co
nduc
ted
with
ca
regi
vers
and
th
emat
ic c
onte
nt
anal
ysis
with
tra
nscr
ipt d
ata.
Min
i-Men
tal S
tate
E
valu
atio
n (M
MS
E)
for p
atie
nts.
Focu
s
Car
egiv
er e
xper
ienc
e
of h
ome
deat
h w
ith
an
d w
ithou
t ac
cess
to
hom
e ca
re
Car
egiv
er d
istre
ss in
H
C w
ith a
nd w
ithou
t sp
ecia
list
ser
vice
s
Dis
tress
and
bur
den
of c
are
asso
ciat
ed
w
ith b
rain
tum
our
pa
tient
spe
cific
ally
Setti
ng
Neg
ev, I
srae
l
Lond
on, U
K
Ger
man
y
Sam
ple
240
care
give
rs o
f pa
tient
s w
ho d
ied
in a
ho
mec
are
prog
ram
an
d 40
4 ca
regi
vers
of
patie
nts
who
die
d
with
no
acce
ss to
HC
co
ntac
ted
1999
-200
1
1271
info
rmal
ca
regi
vers
sco
ring
over
5 o
n th
e
Gen
eral
Hea
lth
Que
stio
nnai
re (G
HQ
-28
)
27 c
areg
iver
s of
pe
ople
with
prim
ary
m
alig
nant
bra
in
tum
ours
(PM
BT)
(onl
y 8
of th
ese
used
hom
e ca
re) f
rom
200
3-20
09
Des
ign
Cas
e co
ntro
l
RC
T
Coh
ort s
tudy
Art
icle
Sin
ger e
t al
(200
5)
Jour
nal o
f Pai
n an
d S
ympt
om
Man
agem
ent
Wal
sh e
t al
(200
7)
Brit
ish
Jour
nal o
f P
sych
iatry
Was
ner e
t al
(201
3)
Jour
nal o
f Soc
ial
Wor
k in
EoL
&
Pal
liativ
e C
are
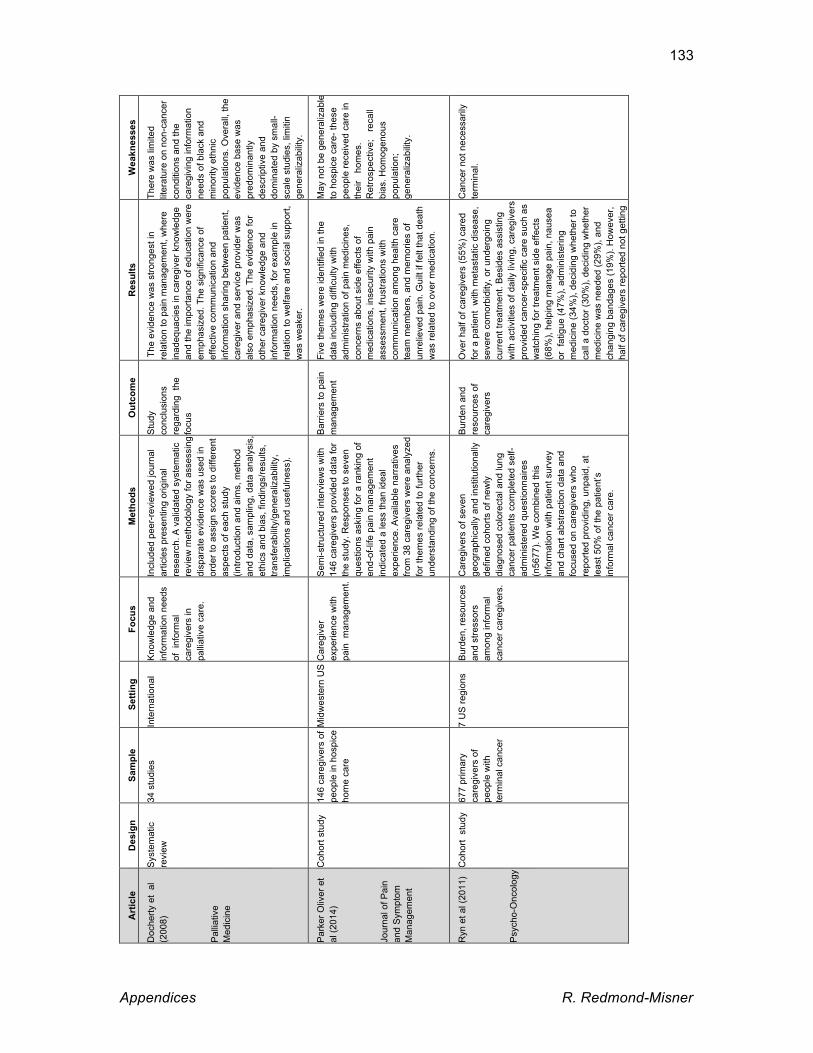
Appendices R. Redmond-Misner
133
Wea
knes
ses
Ther
e w
as li
mite
d lit
erat
ure
on n
on-c
ance
r co
nditi
ons
and
the
care
givi
ng in
form
atio
n ne
eds
of b
lack
and
m
inor
ity e
thni
c po
pula
tions
. Ove
rall,
the
evid
ence
bas
e w
as
pred
omin
antly
de
scrip
tive
and
dom
inat
ed b
y sm
all-
scal
e st
udie
s, li
miti
n ge
nera
lizab
ility
.
May
not
be
gene
raliz
able
to
hos
pice
car
e- th
ese
peop
le re
ceiv
ed c
are
in
thei
r h
omes
. R
etro
spec
tive;
re
call
bias
. Hom
ogen
ous
popu
latio
n;
gene
raliz
abili
ty.
Can
cer n
ot n
eces
saril
y te
rmin
al.
Res
ults
The
evi
denc
e w
as s
trong
est i
n re
latio
n to
pai
n m
anag
emen
t, w
here
in
adeq
uaci
es in
car
egiv
er k
now
ledg
e an
d th
e im
porta
nce
of e
duca
tion
wer
e em
phas
ized
. The
sig
nific
ance
of
effe
ctiv
e co
mm
unic
atio
n an
d in
form
atio
n sh
arin
g be
twee
n pa
tient
, ca
regi
ver a
nd s
ervi
ce p
rovi
der w
as
also
em
phas
ized
. The
evi
denc
e fo
r ot
her c
areg
iver
kno
wle
dge
and
info
rmat
ion
need
s, fo
r exa
mpl
e in
re
latio
n to
wel
fare
and
soc
ial s
uppo
rt,
was
wea
ker.
Five
them
es w
ere
iden
tifie
d in
the
da
ta in
clud
ing
diffi
culty
with
ad
min
istra
tion
of p
ain
med
icin
es,
conc
erns
abo
ut s
ide
effe
cts
of
med
icat
ions
, ins
ecur
ity w
ith p
ain
asse
ssm
ent,
frust
ratio
ns w
ith
com
mun
icat
ion
amon
g he
alth
car
e te
am m
embe
rs, a
nd m
emor
ies
of
unre
lieve
d pa
in. G
uilt
if fe
lt th
at d
eath
w
as re
late
d to
ove
r med
icat
ion.
Ove
r hal
f of c
areg
iver
s (5
5%) c
ared
fo
r a p
atie
nt w
ith m
etas
tatic
dis
ease
, se
vere
com
orbi
dity
, or u
nder
goin
g cu
rren
t tre
atm
ent.
Bes
ides
ass
istin
g w
ith a
ctiv
ities
of d
aily
livi
ng, c
areg
iver
s pr
ovid
ed c
ance
r-sp
ecifi
c ca
re s
uch
as
wat
chin
g fo
r tre
atm
ent s
ide
effe
cts
(68%
), he
lpin
g m
anag
e pa
in, n
ause
a or
fat
igue
(47%
), ad
min
iste
ring
med
icin
e (3
4%),
deci
ding
whe
ther
to
call
a do
ctor
(30%
), de
cidi
ng w
heth
er
med
icin
e w
as n
eede
d (2
9%),
and
chan
ging
ban
dage
s (1
9%).
How
ever
, ha
lf of
car
egiv
ers
repo
rted
not g
ettin
g tra
inin
g pe
rcei
ved
as n
eces
sary
.
Out
com
e
Stu
dy
co
nclu
sion
s re
gard
ing
the
focu
s
Bar
riers
to p
ain
man
agem
ent
Bur
den
and
reso
urce
s of
ca
regi
vers
Met
hods
Incl
uded
pee
r-re
view
ed jo
urna
l ar
ticle
s pr
esen
ting
orig
inal
re
sear
ch. A
val
idat
ed s
yste
mat
ic
revi
ew m
etho
dolo
gy fo
r ass
essi
ng
disp
arat
e ev
iden
ce w
as u
sed
in
orde
r to
assi
gn s
core
s to
diff
eren
t as
pect
s of
eac
h st
udy
(intro
duct
ion
and
aim
s, m
etho
d an
d da
ta, s
ampl
ing,
dat
a an
alys
is,
ethi
cs a
nd b
ias,
find
ings
/resu
lts,
trans
fera
bilit
y/ge
nera
lizab
ility
, im
plic
atio
ns a
nd u
sefu
lnes
s).
Sem
i-stru
ctur
ed in
terv
iew
s w
ith
146
care
give
rs p
rovi
ded
data
for
the
stud
y. R
espo
nses
to s
even
qu
estio
ns a
skin
g fo
r a ra
nkin
g of
en
d-of
-life
pai
n m
anag
emen
t in
dica
ted
a le
ss th
an id
eal
expe
rienc
e. A
vaila
ble
narr
ativ
es
from
38
care
give
rs w
ere
anal
yzed
fo
r the
mes
rela
ted
to fu
rther
un
ders
tand
ing
of th
e co
ncer
ns.
Car
egiv
ers
of s
even
ge
ogra
phic
ally
and
inst
itutio
nally
de
fined
coh
orts
of n
ewly
di
agno
sed
colo
rect
al a
nd lu
ng
canc
er p
atie
nts
com
plet
ed s
elf-
adm
inis
tere
d qu
estio
nnai
res
(n56
77).
We
com
bine
d th
is
info
rmat
ion
with
pat
ient
sur
vey
and
char
t abs
tract
ion
data
and
fo
cuse
d on
car
egiv
ers
who
re
porte
d pr
ovid
ing,
unp
aid,
at
leas
t 50%
of t
he p
atie
nt’s
in
form
al c
ance
r car
e.
Focu
s
Kno
wle
dge
and
info
rmat
ion
need
s
of i
nfor
mal
ca
regi
vers
in
palli
ativ
e ca
re.
Car
egiv
er
expe
rienc
e w
ith
pa
in m
anag
emen
t.
Bur
den,
reso
urce
s an
d st
ress
ors
am
ong
info
rmal
ca
ncer
car
egiv
ers.
Setti
ng
Inte
rnat
iona
l
Mid
wes
tern
US
7 U
S re
gion
s
Sam
ple
34 s
tudi
es
146
care
give
rs o
f pe
ople
in h
ospi
ce
hom
e ca
re
677
prim
ary
care
give
rs o
f pe
ople
with
te
rmin
al c
ance
r
Des
ign
Sys
tem
atic
re
view
Coh
ort s
tudy
Coh
ort
stud
y
Art
icle
Doc
herty
et
al
(200
8)
Pal
liativ
e M
edic
ine
Par
ker O
liver
et
al (2
014)
Jour
nal o
f Pai
n an
d S
ympt
om
Man
agem
ent
Ryn
et a
l (20
11)
Psy
cho-
Onc
olog
y
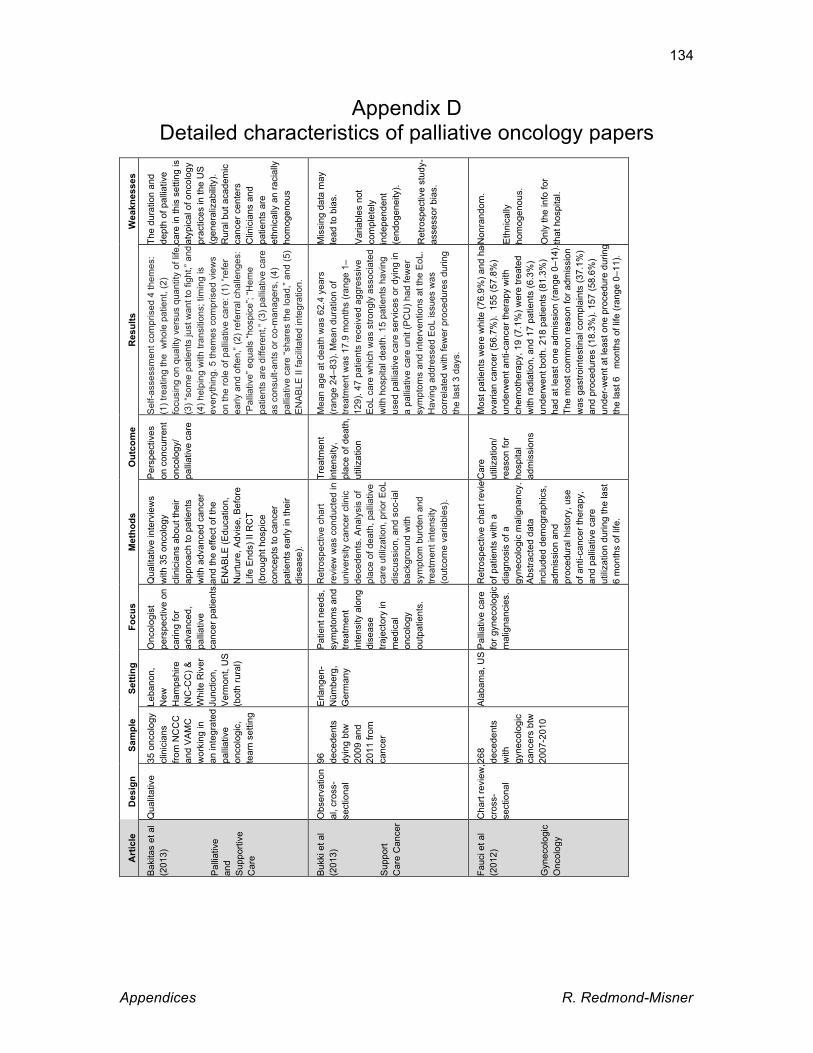
Appendices R. Redmond-Misner
134
Appendix D Detailed characteristics of palliative oncology papers
Wea
knes
ses
The
dura
tion
and
dept
h of
pal
liativ
e ca
re in
this
set
ting
is
atyp
ical
of o
ncol
ogy
prac
tices
in th
e U
S
(gen
eral
izab
ility
). R
ural
but
aca
dem
ic
canc
er c
ente
rs
Clin
icia
ns a
nd
patie
nts
are
et
hnic
ally
an
raci
ally
ho
mog
enou
s
Mis
sing
dat
a m
ay
lead
to b
ias.
Var
iabl
es n
ot
com
plet
ely
inde
pend
ent
(end
ogen
eity
).
Ret
rosp
ectiv
e st
udy-
as
sess
or b
ias.
Non
rand
om.
Eth
nica
lly
hom
ogen
ous.
Onl
y th
e in
fo fo
r th
at h
ospi
tal.
Res
ults
Sel
f-ass
essm
ent c
ompr
ised
4 th
emes
:
(1) t
reat
ing
the
who
le p
atie
nt, (
2)
focu
sing
on
qual
ity v
ersu
s qu
antit
y of
life
, (3
) “so
me
patie
nts
just
wan
t to
fight
,” an
d (4
) hel
ping
with
tran
sitio
ns; t
imin
g is
ev
eryt
hing
. 5 th
emes
com
pris
ed v
iew
s
on th
e ro
le o
f pal
liativ
e ca
re: (
1) “r
efer
ea
rly a
nd o
ften,
” (2)
refe
rral
cha
lleng
es:
“Pal
liativ
e” e
qual
s “h
ospi
ce”;
“Hem
e pa
tient
s ar
e di
ffere
nt,”
(3) p
allia
tive
care
as
con
sult-
ants
or c
o-m
anag
ers,
(4)
palli
ativ
e ca
re “s
hare
s th
e lo
ad,”
and
(5)
EN
AB
LE II
faci
litat
ed in
tegr
atio
n.
Mea
n ag
e at
dea
th w
as 6
2.4
year
s (r
ange
24–
83).
Mea
n du
ratio
n of
tre
atm
ent w
as 1
7.9
mon
ths
(ran
ge 1
–12
9). 4
7 pa
tient
s re
ceiv
ed a
ggre
ssiv
e E
oL c
are
whi
ch w
as s
trong
ly a
ssoc
iate
d w
ith h
ospi
tal d
eath
. 15
patie
nts
havi
ng
used
pal
liativ
e ca
re s
ervi
ces
or d
ying
in
a pa
lliat
ive
care
uni
t (P
CU
) had
few
er
sym
ptom
s an
d in
terv
entio
ns a
t the
EoL
. H
avin
g ad
dres
sed
EoL
issu
es w
as
corr
elat
ed w
ith fe
wer
pro
cedu
res
durin
g th
e la
st 3
day
s.
Mos
t pat
ient
s w
ere
whi
te (7
6.9%
) and
had
ov
aria
n ca
ncer
(56.
7%).
155
(57.
8%)
unde
rwen
t ant
i-can
cer t
hera
py w
ith
chem
othe
rapy
, 19
(7.1
%) w
ere
treat
ed
with
radi
atio
n, a
nd 1
7 pa
tient
s (6
.3%
) un
derw
ent b
oth.
218
pat
ient
s (8
1.3%
)
had
at le
ast o
ne a
dmis
sion
(ran
ge 0
–14)
. Th
e m
ost c
omm
on re
ason
for a
dmis
sion
w
as g
astro
inte
stin
al c
ompl
aint
s (3
7.1%
) an
d pr
oced
ures
(18.
3%).
157
(58.
6%)
unde
r-w
ent a
t lea
st o
ne p
roce
dure
dur
ing
the
last
6
mon
ths
of li
fe (r
ange
0–1
1).
Out
com
e
Per
spec
tives
on c
oncu
rren
t on
colo
gy/
palli
ativ
e ca
re
Trea
tmen
t in
tens
ity,
pl
ace
of d
eath
, ut
iliza
tion
Car
e
ut
iliza
tion/
re
ason
for
hosp
ital
adm
issi
ons
Met
hods
Qua
litat
ive
inte
rvie
ws
with
35
onco
logy
cl
inic
ians
abo
ut th
eir
appr
oach
to p
atie
nts
w
ith a
dvan
ced
canc
er
and
the
effe
ct o
f the
E
NA
BLE
(Edu
catio
n,
Nur
ture
, Adv
ise,
Bef
ore
Life
End
s) II
RC
T (b
roug
ht h
ospi
ce
conc
epts
to c
ance
r pa
tient
s ea
rly in
thei
r di
seas
e).
Ret
rosp
ectiv
e ch
art
revi
ew w
as c
ondu
cted
in
univ
ersi
ty c
ance
r clin
ic
dece
dent
s. A
naly
sis
of
plac
e of
dea
th, p
allia
tive
care
util
izat
ion,
prio
r EoL
di
scus
sion
, and
soc
-ial
back
grou
nd w
ith
sym
ptom
bur
den
and
treat
men
t int
ensi
ty
(out
com
e va
riabl
es).
Ret
rosp
ectiv
e ch
art r
evie
w
of p
atie
nts
with
a
diag
nosi
s of
a
gyne
colo
gic
mal
igna
ncy.
A
bstra
cted
dat
a
in
clud
ed d
emog
raph
ics,
ad
mis
sion
and
pr
oced
ural
his
tory
, use
of a
nti-c
ance
r the
rapy
, an
d pa
lliat
ive
care
ut
iliza
tion
durin
g th
e la
st
6
mon
ths
of li
fe.
Focu
s
Onc
olog
ist
pers
pect
ive
on
carin
g fo
r ad
vanc
ed,
palli
ativ
e
canc
er p
atie
nts.
Pat
ient
nee
ds,
sym
ptom
s an
d tre
atm
ent
inte
nsity
alo
ng
dise
ase
traje
ctor
y in
m
edic
al
onco
logy
ou
tpat
ient
s.
Pal
liativ
e ca
re
for g
ynec
olog
ic
mal
igna
ncie
s.
Setti
ng
Leba
non,
N
ew
Ham
pshi
re
(NC
-CC
) &
Whi
te R
iver
Ju
nctio
n,
Ver
mon
t, U
S
(bot
h ru
ral)
Erla
ngen
-N
ümbe
rg,
Ger
man
y
Ala
bam
a, U
S
Sam
ple
35 o
ncol
ogy
clin
icia
ns
from
NC
CC
an
d V
AM
C
wor
king
in
an in
tegr
ated
pa
lliat
ive
onco
logi
c,
team
set
ting
96
dece
dent
s dy
ing
btw
20
09 a
nd
2011
from
ca
ncer
268
de
cede
nts
w
ith
gyne
colo
gic
canc
ers
btw
20
07-2
010
Des
ign
Qua
litat
ive
Obs
erva
tion
al, c
ross
-se
ctio
nal
Cha
rt re
view
, cr
oss-
se
ctio
nal
Art
icle
Bak
itas
et a
l (2
013)
Pal
liativ
e
and
Sup
porti
ve
Car
e
Buk
ki e
t al
(201
3)
Sup
port
C
are
Can
cer
Fauc
i et a
l (2
012)
Gyn
ecol
ogic
O
ncol
ogy

Appendices R. Redmond-Misner
135
Wea
knes
ses
Mer
its o
f EI g
ener
ally
w
idel
y re
cogn
ized
,
but t
hese
spe
cific
S
OP
s no
t nec
essa
rily
(they
are
new
)
Eng
lish
lang
uage
bi
as?
Trie
d to
avo
id
the
othe
r sys
tem
atic
re
view
bia
ses
Res
ults
SO
Ps
wer
e de
velo
ped
for
19 m
alig
nanc
ies
(a) t
o id
entif
y a
dise
ase-
spec
ific
poin
t in
each
dis
ease
tra
ject
ory
to in
itiat
e E
I (“
gree
n fla
gs”)
and
to
prov
ide
(b)
a c
lear
de
linea
tion
and
sem
antic
di
ffere
ntia
tion
of P
C
assi
gnm
ents
[“pa
lliat
ive
care
” v
s. “s
uppo
rtive
” or
“pal
liativ
e th
erap
ies”
(“gr
een”
vs
. “re
d fla
gs”)
]. P
. 103
9
for S
OP
gre
en fl
ags.
Ther
e is
no
stro
ng
evid
ence
that
any
regi
men
gi
ves
grea
ter p
allia
tion.
H
ighe
r dos
e re
gim
ens
give
m
ore
acut
e to
xici
ty,
espe
cial
ly e
soph
agiti
s.
Ther
e is
evi
denc
e fo
r a
mod
est i
ncre
ase
in
surv
ival
(5%
at 1
yea
r and
3%
at 2
yea
rs) i
n pa
tient
s w
ith b
ette
r per
form
ance
st
atus
(PS
) giv
en h
ighe
r do
se ra
diot
hera
py.
Som
e re
gim
ens
are
asso
ciat
ed
with
an
incr
ease
d ris
k of
ra
diat
ion
mye
litis
.
Out
com
e
Sta
ndar
d op
erat
ing
proc
edur
e (S
OP
)
for s
peci
fic
mal
igna
ncie
s
RC
T fin
ding
s
Met
hods
A w
orki
ng g
roup
(a) s
peci
fy th
e tim
ing
of e
arly
inte
grat
ion
and
(b) s
peci
fy P
C a
ssig
nmen
ts b
y (c
) pro
vidi
ng m
ore
clea
r-cu
t se
man
tic a
nd c
linic
al
defin
ition
s.
Ann
ual u
pdat
e of
trea
tmen
t gu
idel
ines
(SO
P) f
or e
ach
mal
igna
ncy,
the
need
for
dise
ase-
spec
ific
EI S
OP
s w
as
iden
tifie
d.
The
elec
troni
c da
ta- b
ases
M
ED
LIN
E, E
MB
AS
E, C
ance
rlit
and
the
Coc
hran
e C
entra
l R
egis
ter o
f Con
trolle
d Tr
ials
, re
fere
nce
lists
, han
d-se
arch
ing
of jo
urna
ls a
nd
conf
eren
ce
proc
eedi
ngs,
and
dis
cuss
ion
w
ith e
xper
ts w
e-re
use
d to
id
entif
y po
tent
ially
elig
ible
tri
als,
pub
lishe
d an
d un
publ
ishe
d.
Focu
s
Dis
ease
spe
cific
ap
proa
ch to
pa
lliat
ive
canc
er
care
.
NS
CLC
pal
liativ
e ra
diot
hera
py.
Setti
ng
Col
ogne
, G
erm
any
Inte
rnat
iona
l
Sam
ple
Inte
rdis
cipl
inar
y w
orki
ng g
roup
(PC
, on
colo
gy,
radi
othe
rapy
, etc
.)
14 R
CTs
re: p
allia
tive
radi
othe
rapy
in
NS
CLC
Des
ign
Qua
litat
ive
Sys
tem
atic
re
view
Art
icle
Gae
rtner
et a
l (2
011)
Sup
port
Car
e C
ance
r
Lest
er e
t al
(201
2)
Coc
hran
e Li
brar
y

Appendices R. Redmond-Misner
136
Wea
knes
ses
Non
-sys
tem
atic
(Sel
ectio
n bi
as?
Pub
licat
ion
bias
? E
nglis
h la
ngua
ge b
ias?
)
Not
clin
ical
ly s
peci
fic a
s th
e tit
le
wou
ld im
ply.
Non
rand
om.
Rec
all/s
ocia
l des
irabi
lity
bias
es?
Per
form
ed a
t a s
ingl
e, te
rtiar
y ca
re s
ite w
ith a
spe
cial
ized
gr
oup
of th
orac
ic o
ncol
ogy
prov
ider
s an
d pa
lliat
ive
care
cl
inic
ians
, lim
iting
ge
nera
lizat
ion.
Sam
ple
lack
ed
dive
rsity
with
resp
ect t
o ra
ce
and
ethn
ic g
roup
. Did
not
den
y pa
lliat
ive
care
con
sulta
tions
to
parti
cipa
nts
rece
ivin
g st
anda
rd
care
, and
a s
mal
l min
ority
of
patie
nts
in th
e st
anda
rd c
are
grou
p w
ere
seen
by
the
palli
ativ
e ca
re te
am.
Res
ults
Cur
rent
evi
denc
e su
gges
ts th
at p
atie
nts
with
ha
emat
olog
ical
mal
igna
ncie
s ac
cess
palli
ativ
e ca
re s
ervi
ces
less
freq
uent
ly. F
or
thos
e w
ho d
o, it
tend
s to
occ
ur la
ter i
n th
eir
illne
ss th
an th
eir s
olid
tum
our c
ount
erpa
rt-s.
Th
ese
patie
nts
are
mor
e lik
ely
to d
ie in
ho
spita
l fo
llow
ing
esca
latin
g in
terv
entio
ns.
An
epis
odic
app
roac
h ac
cord
ing
to n
eeds
ra
ther
than
pro
gnos
is m
ay b
e m
ore
valu
able
, as
hae
mat
olog
ic p
atie
nts
intro
duce
diff
icul
ty
in p
rogn
ostic
atio
n; e
chni
cal n
atur
e an
d co
mpl
icat
ions
of t
reat
men
t; sp
eed
of c
hang
e
to a
term
inal
eve
nt; n
eed
for p
atho
logy
test
ing
and
trans
fusi
on o
f blo
od p
rodu
cts
as
deat
h ap
proa
ches
;.
Nur
sing
insi
ghts
indi
cate
that
an
unde
rsta
ndin
g of
end
-of-l
ife c
are
in
haem
atol
ogy
need
s to
be
set i
n a
trilo
gy o
f ov
erla
ppin
g m
odel
s (la
bele
d fu
nctio
nal,
evol
ving
, and
refra
ctor
y) th
at a
ddre
ss th
e co
mpl
exity
of i
ssue
s as
soci
ated
with
pr
ofes
sion
al a
nd h
ospi
tal c
ultu
re.
Of t
he 1
51 p
atie
nts
who
und
erw
ent
rand
omiz
atio
n, 2
7 di
ed b
y 12
wee
ks a
nd 1
07
(86%
of t
he re
mai
ning
pat
ient
s) c
ompl
eted
as
sess
men
ts. P
atie
nts
assi
gned
to e
arly
pa
lliat
ive
care
had
a b
ette
r qua
lity
of li
fe th
an
did
patie
nts
assi
gned
to s
tand
ard
care
. In
addi
tion,
few
er p
atie
nts
in th
e pa
lliat
ive
care
gr
oup
than
in th
e st
anda
rd c
are
grou
p ha
d de
pres
sive
sym
ptom
s (1
6% v
s. 3
8%, P
=
0.01
). D
espi
te th
e fa
ct th
at fe
wer
pat
ient
s in
th
e ea
rly p
allia
tive
care
gro
up th
an in
the
stan
dard
car
e gr
oup
rece
ived
agg
ress
ive
end-
of-li
fe c
are
(33%
vs.
54%
, P =
0.0
5),
med
ian
surv
ival
was
long
er.
Out
com
e
Pal
liativ
e ca
re
co
ncer
ns s
peci
fic to
ha
emat
olog
ic
patie
nts
Nur
se
pe
rspe
ctiv
e
QoL
Met
hods
Lite
ratu
re re
view
Rec
ent h
aem
atol
ogy
clin
ical
gu
idel
ines
reco
mm
end
that
pa
lliat
ive
care
spe
cial
ists
sh
ould
hav
e ce
ntra
l rol
es in
ha
emat
o-on
colo
gy te
ams.
25
nurs
ing
inte
rvie
ws
durin
g tw
o-ye
ar q
ualit
ativ
e st
udy.
Ran
dom
ly a
ssig
ned
patie
nts
to
rece
ive
early
pal
liativ
e
care
inte
grat
ed w
ith s
tand
ard
onco
logi
c c
are
or s
tand
ard
onco
logi
c ca
re a
lone
. QoL
as
sess
ed a
t bas
elin
e an
d 12
w
eeks
late
r usi
ng F
unct
iona
l A
sses
smen
t of C
ance
r Th
erap
y-Lu
ng (F
AC
T-L)
and
H
AD
S.
Focu
s
Hae
mat
olog
ical
pa
tient
s in
pa
lliat
ive
care
.
Pal
liativ
e ca
re fo
r ha
emat
olog
ic
mal
igna
ncie
s.
Con
curr
ent
palli
ativ
e an
d on
colo
gic
treat
men
t fo
r pat
ient
s w
ith
NS
CLC
Setti
ng
Inte
rnat
iona
l
Aus
tralia
Uni
ted
S
tate
s
Sam
ple
N/A
25 n
urse
s
151
patie
nts
with
m
etas
tatic
N
SC
LC
Des
ign
Nar
rativ
e
revi
ew
Qua
litat
ive
RC
T
Art
icle
Man
itta
et a
l (2
010)
Jour
nal o
f P
allia
tive
Med
icin
e
McG
rath
et a
l (2
007)
Onc
olog
y
Nur
sing
For
um
Tem
el e
t al
(201
0)
New
Eng
land
Jo
urna
l of
Med
icin
e

Appendices R. Redmond-Misner
137
Appendix E Pearson Correlation
Pearson’s product-moment correlation coefficient (r) uses the variance and
covariance of two continuous variables to attempt to draw a line of fit between them and
derive their correlation. The sample variance of x is calculated as the average squared
difference from the mean:
𝑣𝑎𝑟 𝑥 = ! !!!! !
!!!, (1)
by subtracting the mean from each observation, squaring the differences (so that
negative and positive deviations do not cancel each other out), summing them and
dividing by N-1. The square root of the variance gives the standard deviation. Sample
covariance of x and y is given by
𝑐𝑜𝑣 𝑥, 𝑦 = !( !!!! !!!! )!!!
. (2)
Pearson’s sample correlation is given by
𝑟!" =!"# !,!
!"# ! !"#(!), (3)
dividing the covariance by the standard deviation of each variable:
𝑟!" =! !!!! !!!!
! !!!! ! ! !!!! !. (4)
This measures the linear relationship between the variables which is why it is only
suitable for continuous variables. Pearson’s r is always between -1 and 1 and can speak
to the direction of the relationship as well. To derive a population correlation, all terms
divided by N-1 are instead divided by 1.

Appendices R. Redmond-Misner
138
Appendix F Phi coefficient and Cramér’s V test
Phi coefficients (mean square contingency coefficients), ∅, measure association
between binary variables and have the same interpretation as the Pearson correlation
(Sanyal et al, 2009). Ranging from -1 to 1, it is the ratio of the Pearson chi-square (x2)
statistic to the total number of observations:
∅ = 𝑥!/𝑁 (or ∅! = !!
!), (1)
where x2 is a measure of association between the two variables. So if we have a 2x2
contingency table for random binary variables x and y,
y = 1 y = 0 Total
x = 1 n1 n4 n7
x = 0 n2 n5 n8
Total n3 n6 n
∅ = !!!!!!!!!!!!!!!!!
(Everitt, 2002). (2)
Cramér’s V test is a “rescaling of phi” to handle tables larger than 2x2 (Cramér,
1946):
𝑉 = 𝑥!/𝑁(𝑘 − 1) , (3)
where N is the number of observations and k is the smaller number of rows and columns
(Sanyal et al, 2009, p. 71). For 2x2 tables, Cramér’s V returns the phi coefficient
because k = 2.

Appendices R. Redmond-Misner
139
Appendix G Correlation coefficients
Phi Caregiver sex Patient sex Site Caregiver sex 1 Patient sex -.5412 1 Site .1748 -.14551 1
Cramér’s V D
iagn
osis
Car
egiv
er
educ
atio
n
Patie
nt
educ
atio
n
Car
egiv
er
mar
ital
Patie
nt
mar
ital
Patie
nt
livin
g
Car
egiv
er
empl
oym
ent
Car
egiv
er
rela
tion
Diagnosis 1 Caregiver education
.224
1
Patient education
.2221 .3568 1
Caregiver marital
.1964 .2748 .1179 1
Patient marital
.2222 .1376 .1724 .3834 1
Patient living
.2201 .1783 .1596 .3744 .5757 1
Caregiver employment
.2287 .2969 .2302 .2783 .2826 .2758 1
Caregiver relation
.2011 .1782 .1999 .333 .5691 .5209 .2406 1
Polychoric (1)
Com
orbi
dity
Car
egiv
er
burd
en
Car
egiv
er
sex
Patie
nt se
x
Site
Em
erge
ncy
visi
ts
Day
s ov
erni
ght
Car
egiv
er
age
Patie
nt a
ge
Comorbidity 1 Caregiver burden
-.0441 1
Caregiver sex .1285 -.1186 1 Patient sex .1701 .2311 -.4263 1 Site -.0075 .2513 .158 -.2763 1 Emergency visits
-.0139 .1274 -.1046 -.0083 -.0195 1
Days overnight
.0359 .168 .0572 .0088 .0834 .3759 1
Caregiver age -.0231 -.019 .0689 .1101 .0116 -.2486 -.0657 1 Patient age .0714 -.018 -.0602 -.0546 .0911 -.0216 -.0278 .1856 1 (ln)Time cost .0769 .2503 -.1276 .0349 .1685 .1002 .0903 .0079 -.1224 (ln)Ministerial cost
.1214 .1924 .0757 -.108 .2251 .4802 .3979 -.1655 .0025
(ln)Societal .0764 .279 -.0499 -.0714 .3111 .4017 .315 -.0769 -.0438

Appendices R. Redmond-Misner
140
cost (ln)Meds -.0399 .1164 .0288 .0406 .0779 .0569 .1121 -.0721 -.0919 Hospitalization .0617 .2409 -.0286 .057 .1445 .6509 .7773 -.1464 -.0841
Polychoric (2) (ln
)Tim
e co
st
(ln) M
inis
teria
l co
st
(ln)S
ocie
tal c
ost
(ln)M
eds
Hos
pita
lizat
ion
(ln)Time cost 1 (ln)Ministerial cost .2932 1 (ln)Societal cost .7358 .7962 1 (ln) meds .0148 .3164 .1851 1 Hospitalization .2204 .953 .888 .1728 1
Pearson O
ut-o
f-po
cket
m
eds
Out
-of-
pock
et
trave
l
Out
-of-
pock
et
supp
lies
Publ
ic m
eds
Publ
ic te
sts
Publ
ic
appo
intm
ents
Publ
ic
hosp
italiz
atio
n
Publ
ic
emer
genc
y ro
om
(ln)S
ocie
tal
(ln)M
inis
teria
l
Out-of-pocket meds
1
Out-of-pocket travel
.0382 1
Out-of-pocket supplies
.0448 .0159 1
Public meds -.0095 .0089 1 Public tests .0519 .2061 .0125 .016 1 Public appointments
.0275 .1884 .0602 .0571 .1401 1
Public hospitalization
.0616 .3737 -.0165 .0189 -.011 .1766 1
Public emerg-ency room
.0211 .17 -.0139 .0582 .0226 .3176 .3378 1
(ln)Societal .0383 .2331 .0893 .1398 .0261 .0845 .3825 .192 1 (ln)Ministerial .025 .2336 .0091 .2229 .0637 .1221 .5032 .2375 .7795 1 (ln)Time cost .1364 .1528 .1084 .0325 -.0038 .007 .1017 .0815 .7966 .2477

Appendices R. Redmond-Misner
141
Appendix H Explanation of lesser-discussed statistics
Statistic Estimator Interpretation
Coefficients GLS7 Log-linear: for a change in x by 1, expect y to change by 100 x β (%). For categorical variables, it is the difference in impact of the x condition on y from the baseline category.
Probit The predicted probability can be calculated using these coefficients. Positive coefficients indicate increasing the probability of y=1 and vice versa.
Poisson For a 1 unit change in x, the difference in the expected count (y) is expected to change by the coefficient on x.
Wald Chi2 All with the same interpretation
This tests the H0 that at least one coefficient is not equal to 0.
Prob > Chi2 All with the same interpretation
This gives the probability of obtaining the Wald Chi2 statistic if the predictor variables had no effect.
P-value All with the same interpretation
The probability of the coefficient under the null hypothesis that the independent variable has no effect. Significant p-values that reject the null hypothesis are generally associated with standard errors > 2.
Σ𝜇 GLS and probit (same interpretation)
The standard deviation of the random effect (panel-level standard deviation); taking the log and squaring it gives you (ln)Σ𝜇2. When Σ𝜇 = 0, the panel component is unimportant and the results are no
7 RE, FE and hybrid RE.

Appendices R. Redmond-Misner
142
different than a pooled model.
Σ𝜀 GLS Standard deviation of 𝜀it.
Rho GLS Rho is the fraction of variance attributable to the 𝜇i term in RE models.
R2 GLS Overall, between and within
Breusch & Pagan GLS Panel GLS considers unobservable heterogeneity across and within individuals over time that cross-sectional analysis cannot capture. Breusch & Pagan tests the H0 that there are no RE, in which case a pooled OLS could do just as adequate a job of analyzing the panel. Rejection of H0 means that GLS is the optimal estimator.
(ln)Σu2 Probit Logarithm of the random effect standard deviation (panel variance).
𝛼 Poisson This is an under/over-dispersion coefficient. Poisson distribution assumes that mean=variance of the dependent variable. Variance greater than the mean is over-dispersion, and the inverse is under-dispersion.
(ln)𝛼 Poisson Logarithm of 𝛼.

Appendices R. Redmond-Misner
143
Appendix I Residuals and fitted values (graphs)
RE Regression on societal cost of CBPHC
RE regression on Ministry of Health cost of CBPHC
RE regression on unpaid caregiver cost of CBPHC
56
78
910
Pred
icted
Val
ues
5 6 7 8 9 10Log-Transformed Societal Cost
Linear prediction Fitted values
Random Effects Regression on Societal Cost: Fitted Values
0.1
.2.3
.4.5
Den
sity
-6 -4 -2 0 2Residuals
Random Effects Regression on Ministerial Cost: Residuals
02
46
810
Pred
icte
d Va
lues
0 2 4 6 8 10Log-Transformed Informal Cost
Linear prediction Fitted values
Random Effects Regression on Informal Cost: Fitted Values
0.2
.4.6
.8De
nsity
-3 -2 -1 0 1 2Residuals
Random Effects Regression on Societal Cost: Residuals
02
46
810
Pre
dict
ed V
alue
s
0 2 4 6 8 10Log-Transformed Ministerial Cost
Linear prediction Fitted values
Random Effects Regression on Ministerial Cost: Fitted Values0
.2.4
.6D
ensi
ty
-6 -4 -2 0 2Residuals
Random Effects Regression on Informa Cost: Residuals





























