Embed Size (px)
Citation preview

BREAST CANCER MANAGEMENT 0039-6109/99 $8.00 + .OO
THE ROLE OF RADIATION THERAPY FOR PRIMARY
BREAST CANCER Alphonse G. Taghian, MD, PhD, and Simon N. Powell, MD, PhD
Breast cancer has been more extensively studied by clinical trial than any other discipline in oncology and possibly within medicine as a whole. This intensive study has made possible detailed analysis of each component of treatment, so that the roles of surgery, medical oncology, and radiation oncology are largely driven by evidence rather than by anecdote or experience. The four main applications of radiation therapy in the primary treatment of breast cancer are in treating ductal carcinoma in situ (DCIS), early stage invasive disease, and locally advanced breast cancer, and as postmastectomy therapy. The last two decades have seen the role of radiation therapy for these conditions defined clearly, and it is now understood that radiation therapy not only improves local control of breast cancer, but also works with surgery and chemotherapy to improve the probability of survival. The evidence supporting the use of radiation therapy is outlined in this article, together with an analysis of the remaining controversies concerning treatment and possible complications of treatment.
ROLE OF RADIATION THERAPY IN DUCTAL CARCINOMA IN SlTU OF THE BREAST
As a result of improvements in mammography and an increased emphasis on screening and early detection, the proportion of breast cancers diagnosed as noninvasive has increased from 5% to 31%.78 This change in incidence of DCIS is associated with a change in the clinical presentation. In studies reported before the era of screening mammography, most patients with DCIS presented with a palpable mass, nipple discharge, or both." In contrast, in more recent studies of patients who have had screening mammography, 59% of patients diagnosed
From the Breast Cancer Unit, Department of Radiation Oncology, Massachusetts General Hospital (AGT, SNP); Harvard Medical School (AGT, SNP); Boston Medical Center (AGT); and Boston University School of Medicine (AGT), Boston, Massachusetts
SURGICAL CLINICS OF NORTH AMERICA
VOLUME 79 - NUMBER 5 OCTOBER 1999 1091

1092 TAGHIAN & POWELL
with DCIS were detected exclusively by mammography6 Ductal carcinoma in situ is a biologically and histologically heterogeneous group of lesions?] and its management is still controversial. In the past, when patients presented with palpable masses, mastectomy was considered the treatment of choice for DCIS. The distal and local recurrence rates were in the range of 1% to 2Y0.4~, 61, 68 With breast-conserving surgery being used to treat even invasive disease, mastectomy has recently been considered excessive treatment by many clinicians and pa- tients. In recent years, several investigators have evaluated breast-conserving treatment by excision alone or by excision and radiation therapy to treat DCIS.
In the last decade, Lagios et al', 67 have advocated breast conservation by treating DCIS with excision alone, without irradiation. They treated 79 patients with DCIS prospectively by breast-conserving surgery alone. For this therapy, they adopted strict criteria, among which were requirements that lesions be nonpalpable, discovered mammographically, smaller than 2.5 cm, and free of microcalcifications at postoperative mammography. They reported actuarial local recurrence rates of 12% at 5 years and 16% at 10 years, results that initially seemed satisfactory but might now be regarded as suboptimal. There were no breast cancer-related deaths, and no patients developed distant metastasis.66 Patients with high-grade DCIS and comedo-type necrosis, however, had a local failure rate of 33%; of 43 patients without these features only 1 experienced recurrent disease. Similarly, Schwartz et aP3 reported a 15% absolute local failure rate at 4 years, but 32% of patients with comedo histology experienced local failure. In a recent study by Silverstein et al,Il4 the authors suggested that postoperative radiation did not lower the recurrence rate among patients with DCIS that was excised with margins of 10 mm or more.
Breast-conserving surgery and radiation have been used extensively in the treatment of DCIS. Several retrospective studies were reported initially. In the largest, by Solin et a1,ll6 the authors combined the data of nine institutions in the United States and Europe. In 270 patients with DCIS who were treated with excision and breast irradiation, the 15-year actuarial rate of local failure was 19%. Half the recurrences were DCIS and half were invasive, but the 15-year breast cancer-specific survival rate was still 96%. In 1993, the National Surgical Adjuvant Breast and Bowel Project (NSABP) reported the B-17 trial, the first randomized trial to test the benefit of adding radiation therapy to breast- conserving surgeryz8 A total of 790 patients were randomly assigned to excision and radiation therapy or to excision alone. The 5-year actuarial local recurrence rate was 7% for patients treated with excision and radiation therapy compared with 16.4% for patients treated by excision alone. The 5-year cumulative inci- dence of local failure was reduced by irradiation from 10.4% to 7.5% for recurrent DCIS (P = 0.055) and from 10.5% to 2.9% for recurrent invasive cancers ( P < 0.001). In an update at 8 the incidence of noninvasive local failure was reduced from 13.4% to 8.2% ( P = 0.007) and of invasive local failure from 13.4% to 3.9% ( P < 0.0001). Although the B-17 trial was the first prospective random- ized study for patients with DCIS, its results were highly contr~versial.~~, 88 In an analysis and central review of histopathology slides, Fisher et a136 found that both comedo-type necrosis and close or involved margin status were significant predictors of an increased likelihood of local recurrence. In the updated the authors could not identify a subgroup of patients who could prudently omit radiation therapy. Therefore, these investigators recommended that radiation therapy be used following lumpectomy in all patients with DCIS. It should be noted that the NSABP regards margins as free when the tumor is not transected, and assessments indicating that lesions were close to the margin were not considered to represent a risk.36 In this study, the mammographic and pathologic evaluations were not as detailed as is now possible: magnified-view mammo-

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1093
grams, specimen radiography, and postoperative mammograms to assure the removal of microcalcifications, which are now regarded as standards of care, were not performed routinely.
Several shortcomings of the 8-17 study raised the question of whether these results can be applied generally to all patients with DCIS. Comprehensive mammographic and pathologic evaluations are critical in the treatment of pa- tients with DCIS. With careful mammographic evaluation selected patients with low-grade DCIS smaller than 2.5 cm and completely excised with wide negative margins might have excellent results with local excision alone as suggested in a retrospective analysis by Silverstein et al.ll4 The Radiation Therapy Oncology Group (RTOG) is initiating a trial for patients who fit this profile, randomly assigning them to local excision alone or local excision and radiation (McCor- mick et al, personal communication). The margins should be at least 3 mm and both arms will receive Tamoxifen.
THE ROLE OF RADIATION THERAPY IN EARLY BREAST CANCER
Conservative Surgery and Radiation Versus Mastectomy
For decades, radical or modified radical mastectomy was the primary treat- ment for breast cancer. In the last 20 years, there has been a gradual acceptance of a breast-conserving surgical approach coupled with radiation therapy. After the results of six different randomized trials in the United States and Europe were published (Table l), radiation therapy became an integral part of the treatment of early stage breast cancer. These six prospective trials compared mastectomy with breast-conserving surgery and radiation and demonstrated that the rates of local and regional recurrences, distant metastasis, and overall survival were not significantly different between the two treatments. The NSABP B-06 trialz7 and the Milan trialIz5 showed a nonsignificant survival advantage in favor of breast-conserving surgery and radiation therapy for patients with posi- tive axillary lymph nodes. In an updated meta-analysis of data from the French Institut Gustav Roussy (IGR) trial, the European Organization for the Research and Treatment of Cancer (EORTC) trial, and the National Cancer Institute (NCI) trial in the United States, Morris et alE1 found that the pooled odds ratio for overall survival at 10 years favored breast-conserving surgery and radiation therapy over mastectomy. On the other hand, the Early Breast Cancer Tr ia l i~ ts~~ meta-analysis of nine prospective randomized trials comparing breast-conserv- ing surgery with mastectomy did not show any survival differences in seven of these trials; the local failure rates were 5.9% and 6.2% for the patients receiving breast-conserving surgery with radiation and mastectomy, respectively.
Conservative Surgery Without Radiation Therapy
Whether radiation therapy is required for every patient with invasive breast cancer after breast-conserving surgery is still unresolved. In a phase I1 single- arm trial, the Joint Center of Radiation Therapy (JCRT)I1" selected patients with very favorable prognoses for breast-conserving surgery alone. The inclusion criteria included tumor size smaller than 2 cm, histologically negative lymph nodes, no extensive intraductal component (EIC), no lymphatic and vascular space invasion (LVI), and pathologically documented 1-cm negative margins. The trial was closed prematurely. The rate of local failure was 16% with a

Tabl
e 1.
LO
CA
L R
EC
UR
RE
NC
E A
ND
SU
RV
IVA
L R
ATE
S O
F TR
IALS
CO
MP
AR
ING
BR
EA
ST-
CO
NS
ER
VIN
G S
UR
GE
RY
(B
CS
) A
ND
R
AD
IATI
ON
TH
ER
AP
Y W
ITH
MA
STE
CTO
MY
(M)
Loca
l C
ontr
ol
Sur
viva
l ("/.
I ("/.
I S
tudi
es
No.
of
Dis
ease
A
djuv
ant
Boo
st D
ose
FOIIO
W-U
P
BC
M
B
C
M
(Yea
rs)
(Ref
eren
ce)
Per
iod
Pat
ient
s S
tage
S
urge
ry
Che
mot
hera
py
(GY
)
Mila
n125
19
73-1
980
701
I Q
, RM
C
MF
10
7 4
65
65
18
EOR
TClZ
3 19
80-1
986
874
1-11
LE
/MR
M
CM
F 25
13
9
54
61
8 D
BC
G8
1983
-198
9 90
4 1-1
11
WE,
Q, M
RM
C
MF/
T
10-2
5 5
6 79
82
6
IGR
~
1972
-198
0 17
9 I
WE
/MR
M
Non
e 15
9
14
73
65
15
~~
15
8
1979
-198
7 23
7 1-1
1 L
E/M
RM
A
C
15-2
0 16
6
77
75
10
NSA
BP2
' 19
7G19
84
1219
1-1
1 W
E/M
RM
5-
FU/M
elph
alan
no
boo
st
10
8 63
59
12
NSA
BP
= N
atio
nal
Surg
ical
Adj
uvan
t B
reas
t and
Bow
el P
roje
ct; E
OR
TC =
E
urop
ean
Org
aniz
atio
n fo
r R
esea
rch
and
Trea
tmen
t of
Can
cer;
DBC
G =
Dan
ish
Bre
ast
Can
cer
Gro
up; I
GR
= I
nstit
ut G
usta
v R
ouss
y (F
ranc
e); N
CI
= N
atio
nal C
ance
r Ins
titut
e (U
S); Q
= q
uadr
ante
ctom
y; L
E =
loc
al e
xcis
ion
(1 cm
gro
ss m
argi
ns);
WE
= w
ide
exci
sion
(2
cm g
ross
mar
gins
); M
RM
= m
odif
ied
radi
cal m
aste
ctom
y; R
M =
rad
ical
mas
tect
omy;
CM
F =
Cyt
oxan
met
hotr
exat
e fl
uoro
urac
il; A
C =
Adr
iam
ycin
, Cyt
oxan
; FU
= f
luor
oura
cil;
CM
F/T
= C
ytox
an, m
etho
trex
ate,
fluo
rour
acil/
tam
oxif
en

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1095
median follow-up of 56 months. Several randomized trials compared breast- conserving surgery alone versus breast-conserving surgery and irradiation (Table 2). Among trials, the rate of local failure in patients receiving radiotherapy was reduced by an average of 85%; however, the survival rate was not significantly different from that of patients treated with excision a10ne.l~. 27. 3y, 74, l Z y
Investigators have evaluated the role of chemotherapy without irradiation in preventing local recurrence in the breast after breast-conserving surgery. The Ontario of node-positive patients identified a subset of 121 premeno- pausal patients who had undergone breast-conserving surgery, and for whom breast irradiation was omitted but who received a 12- or 36-week course of systemic chemotherapy. The rate of local recurrences was lower after the longer, 36-week chemotherapy (23%) than after the 12-week treatment (39%) ( P = 0.02). These recurrence rates, however, were not sufficiently reduced to justify replac- ing breast irradiation with chemotherapy. Similar results from other studies, for example, the NSABP B-06 studyZ7 and the Scottish trial,"' showed the positive effect of chemotherapy on local control. The extent of improvement did not, however, reach the level of local control obtained with radiation therapy, with or without chemotherapy.
Despite these findings, the use of wide local excision and tamoxifen without breast irradiation might be appropriate in a selected group of patients, particu- larly those 70 years or older with small, estrogen receptor-positive tumors excised with wide negative margins. In a retrospective study of 122 patients treated with breast-conserving surgery and systemic therapy (no radiation ther- apy), Nemoto et alx4 showed that the overall rate of local failure was 19%. The rate of recurrence in the breast correlated with the size of the tumor and the age of the patient. The rate of local failure in patients older than 70 years and with tumors smaller than 1 cm was significantly lower than for the rest of the group. Two randomized trials are evaluating the role of tamoxifen with and without radiation after breast-conserving surgery. In the NSABP B-21 trial, patients must have tumors smaller than 1 cm and negative lymph nodes. In the Southwest Oncology Group (SWOG) trial, patients must be younger than 70 years and have tumors smaller than 4 cm. Both trials are closed and results are not yet published.
Cosmetic Results
Breast conservative treatment has overall resulted in a rate of excellent or good results in 52% to 95% of patients. Factors related to cosmesis include the size and location of the primary tumor and its relative size in relation to the size of the breast and to total body weight. Cosmesis also depends on the extent of the surgical procedure and the surgeon's technique. Several studies have shown that the boost technique plays a significant role in the overall cosmesis.", 77, 85, 92, In these studies, the rate of good to excellent results varied between 75% to 100% when patients were given a boost by electrons compared with 52% to 91% when patients were given a boost by an interstitial implant. The follow- up in these studies ranged from 1 to 139 months.
Contraindications to Breast-conserving Treatment
The National Cancer Institute Consensus ConferenceH3 on the treatment of early stage breast cancer held in 1990 concluded that "breast-conservation treat-

Tabl
e 2.
LO
CA
L R
EC
UR
RE
NC
E A
ND
SU
RV
IVA
L R
ATE
S O
F TR
IALS
CO
MP
AR
ING
BR
EA
ST-
CO
NS
ER
VIN
G S
UR
GE
RY
ALO
NE
W
ITH
BR
EA
ST-
CO
NS
ER
VIN
G S
UR
GE
RY
AN
D R
AD
IATI
ON
Lo
cal
Axi
llary
C
ontr
ol ("
A)
Su
rviv
al ("
/.I
F~
~~
~~
p
(Ref
eren
ces)
P
erio
d
Pat
ien
ts
Siz
e S
tatu
s S
urge
ry
Rad
ioth
erap
y C
hem
othe
rapy
C
S
CS
+ R
T C
S
CS
+ R
T (m
onth
s)
Stu
dies
N
o. o
f Tu
mor
Ly
mph
Nod
e A
djuv
ant
Mila
n 111129
1987
-198
9 56
7 <
2.5
cm
+
or -
Q
50
Gy/
25 f
r ye
s*
19
2 85
87
48
NSA
BP
B-0
627
1976
-198
4 10
35
< 4
cm
+
or-
L 50
Gy/
25 f
r ye
s' 35
10
58
63
15
0 +
boos
t
no b
oost
Sw
edis
h"
1981
-198
8 38
1 <
2 c
m
-
SR
54G
y/25
fr
none
18
2
90
91
64
no b
oost
O
ntar
ioI7
19
8419
89
837
< 4
cm
-
L 40
Gy/
16 f
r no
ne
29
7 85
87
66
+
boos
t 19
85-1
991
585
< 4
cm
+ or
-
LE
50G
y/25
fr
yes
(all)
24
.5
5.8
78
80
68
+ bo
ost
*Che
mot
hera
py fo
r ly
mph
nod
e-po
sitiv
e pa
tient
s +
= p
ositi
ve; -
= n
egat
ive;
LC
= l
ocal
con
trol;
CS =
bre
ast-c
onse
rvin
g su
rger
y; Q
= q
uadr
ante
ctom
y; L
= l
umpe
ctom
y; S
R =
sec
tor r
esec
tion;
LE
= r
emov
al o
f tu
mor
with
1 cm
mar
gin;
CS+
RT
= c
onse
rvat
ive s
urge
ry +
radi
atio
n th
erap
y; N
SABI
' =
Nat
iona
l Sur
gica
l Adj
uvan
t Bre
ast a
nd B
owel
Pro
ject
.

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1097
ment is an appropriate method of primary therapy for the majority of women with Stage I and I1 breast cancer and is preferable because it provides survival equivalent to total mastectomy and axillary dissection while preserving the breast.“ Absolute and relative contraindications, however, may keep patients from being considered as candidates for breast-conserving surgery and radiation therapy.134 These contraindications were determined in 1991 by a panel of repre- sentatives from the American College of Surgeons, the American College of Radiology, the College of American Pathologists, and the Society of Surgical Oncology:
Absolute contraindications to breast-conserving surgery:
Pregnancy: first and second trimester Multicentricity: two or more gross tumors in separate quadrants Diffuse undetermined or malignant-appearing microcalcifications History of previous irradiation to the breast region viz mantle RT
Relative contraindications to breast-conserving surgery
Large tumor/breast ratio with respect to acceptable cosmetic results Large breast size Tumor location beneath the nipple History of collagen vascular (connective tissue) disease
A tumor located beneath the nipple might not be considered a contraindication to breast-conserving surgery if the patient understands the anticipated deficit and desires the procedure. Extremely large breast size is also not a contraindica- tion to breast-conserving surgery if radiation therapy can assure dose homogene- ity5’ A history of pre-existing collagen vascular diseases, namely, lupus, sclero- derma, or rheumatoid arthritis, or connective tissue diseases has been considered a contraindication to breast-conserving surgery with radiation therapy because of anecdotal reports of severe fibrotic reactions to radiation therapy, in particular among patients with lupus and scleroderma.”, Iflo These data were not confirmed, however, and a different report by Ross et alln3 did not show any increased incidence of complications in patients with connective tissue diseases treated by radiation therapy. In a recent study by Morris and Powell,KZ the authors recom- mend breast-conserving surgery and radiation therapy for patients with rheuma- toid arthritis; for patients with lupus or scleroderma, however, the authors suggested that “an adjustment of RT [radiation therapy] doses or mastectomy” should be considered.
Another important consideration in selecting the type of local therapy is a risk of local recurrence that is greater than the risk of local recurrence following mastectomy. The patient’s desire for breast conservation is an important consid- eration. On the other hand, some patients have medical contraindications, namely physical disabilities such as an inability to lie flat or to adequately abduct the arm, that can make irradiation difficult or impossible.
Prognostic Factors for Local Failure
Prognostic Factors Related to the Tumor
Tumor Size. No evidence suggests that the rate of local recurrence is influenced by the tumor size when a complete excision with negative margins is performed and the patient receives radiation.lR When patients are treated with breast-conserving surgery alone, without radiation therapy, the rate of local

1098 TAGHIAN & POWELL
failure correlates significantly with the tumor size. The data from the NSABP B-06 trial have shown that the rates of local failure in patients treated by lumpectomy alone for tumor sizes of less than 1 cm, 1.1 to 2.0 cm, 2.1 to 3.0 cm, and larger than 3.1 cm were 21%, 32%, 37%, and 44%, respectively. For patients who received irradiation, however, the rate of local failure was not influenced by the tumor size.27
Involvement of Axillary Lymph Nodes. The lymph node status does not seem to be a major factor associated with local failure within the breast.Iz5 The prospective randomized trials from the NSABP:7 the NCI,5* and Milanlz5 have shown that the rate of local failure in patients with positive lymph nodes who received chemotherapy varied between 3% and 7%, compared with 10% to 13% for patients with negative lymph nodes who did not receive chemotherapy.
Extensive Intraductal Component. Extensive intraductal component was first described by the Joint Center of Radiotherapy and, by their definition, consists of intraductal carcinoma comprising 25% or more of the primary inva- sive tumor, with intraductal carcinoma in the breast tissue surrounding the tumor. The definition also includes DCIS in which there are focal areas of in~asion.'~' Approximately 25% to 30% of women with early invasive breast cancer treated by breast-conserving surgery are found to be EIC-positive. In the study from the Joint Center,'31 the 5-year crude rate of local failure in EIC- positive patients was 21%; in contrast, EIC-negative patients had a 5-year crude rate of local failure of only 6% (P < 0.0001). In this study, the microscopic margins of resection were not routinely evaluated. The presence of EIC was associated with an increase in the local failure to approximately 20% at 5 years, (range, 9% to 30%), a risk of 2% to 8% for EIC-negative patients (Table 3). Holland et a15* demonstrated on 217 mastectomy specimens that EIC-positive tumors were significantly more likely to have residual tumor burden following gross excision. On the other hand, in EIC-positive patients with negative mar- gins, the risk of local failure is not increased (Table 4). Therefore, the presence of EIC per se is not a risk factor for local recurrence in patients with uninvolved margins; these patients can be adequately treated with breast-conserving therapy.
Surgical Margins. The assessment and significance of resection margins following breast-conserving surgery have been clearly shown to be an important risk factor for local control, although controversial issues still remain. These controversies result, in part, from the definition of a positive or negative margin and from differences in opinion as to the optimal method for assessing these margins. The NSABP considers a margin to be positive only if cancer cells are present directly at an inked surface. A close margin has been defined as tumor present within 1 mm and a negative margin as no tumor within 1 mm of the inked margins.'Og Margin positivity may be focal (i.e., 3 or fewer power fields)
Table 3. RATE OF BREAST CANCER RECURRENCE RELATED TO THE PRESENCE OF AN EXTENSIVE INTRADUCTAL COMPONENT (EIC)
Breast Cancer Recurrence % (No. Patients Treated) FoIIow-UP
Investigators (References) (Y) EIC-Positive EIC-Negative
Bartelink et a17 Burke et all4 Jacquemier et a159 Salvadori et allos Veronisi et
5 2% (208) 9% (79) 5 2% (369) 10% (69) 5 8% (390) 18% (105)
11 8% (1751) 16% (152) 5 8% (307) 30% (38)

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1099
Table 4. RATE OF BREAST CANCER RECURRENCE RELATED TO MARGINS STATUS IN PATIENTS WITH EXTENSIVE INTRADUCTAL COMPONENT (EIC)
Breast Cancer Recurrence (%)
Follow-up Negative Close or Positive Investigators (References) (y) Margins Margins
Bartelink et a17 5 0 11 Burke et all4 5 2 37 Smitt et al'l5 6.2 0 21 Solin et aP6 4.5 5 66
or diffuse (3 or more power fields). The majority of studies2, 19, 45, 4h, yo, Io9, 123,
demonstrate an increased incidence of breast cancer recurrence in patients with positive margins, although in these studies the magnitude of the risk of local failure varies between 5% and 30% (Table 4).
Prognostic Factors Related to the Patient
Young age has been associated with increased risk of local or distant fail- ure.", 23, 32, 41, 44, h5, 130 Table 5 shows the rate of local failure in younger patients compared with the rate of local failure in older patients. In a recent study from the EORTC of 5569 patients, Vrieling et all3' found that the local failure rate after breast-conserving surgery was significantly increased in women of 40 years of age or younger. The authors explained these results by this younger group of patients having had significantly larger tumors, more frequent re-excision, and more frequent microscopically incomplete excision. In another study from the Curie Institute, de la Rochefordiere et alZ3 reviewed 1425 premenopausal women with small invasive breast cancer treated over a 10-year period. Grade I11 tumors and involved margins were significantly more common in younger patients than in patients older than 40 years. The actuarial rates of local failure were 43%, 30%, and 15% for patients in the age groups of 23 to 35 years, 36 to 40 years, and over 40 years, respectively ( P < 0.0001). The corresponding rates of distant metastasis were 36%, 31%, and 18%, respectively ( P < 0.0001). It should be noted that younger women also have a higher rate of chest wall failure after mastectomy than do older patients.22 Because most young patients today receive
Table 5. EFFECT OF AGE ON THE RISK OF LOCAL FAILURE IN PATIENTS TREATED BY BREAST-CONSERVING TREATMENT
Recurrence
Younger Older Age Criterion Investigators (References) (Y) Number" % Number* %
Clarke et all8 5 34 3/32 10 21/424 5 Fowble et al" 5 35 12/64 19 69/941 7 Veronisi et 5 35 9/95 9 45/1137 4 Boyages et al" 5 34 15/61 25 76/722 11 Kurtz et alh5 5 39 52/243 21 133/1440 9 Fourquet et a14' 5 32 12/35 34 44/483 9
*Number of patients with recurrence/total number of patients

1100 TAGHIAN & POWELL
adjuvant systemic chemotherapy, some of the risk associated with younger age will be reduced. Rose et aPo2 found that in young women, the local failure rate was reduced from 17% to 5% in patients who received chemotherapy compared with those who did not.
Prognostic Factors Related to the Treatment. Treatment-related factors that might be associated with increased risk of recurrence after breast-conserving treatment include incisional biopsy,'24 a radiation dosage lower than 8 Gy/wk,6s and the interval between breast surgery and the start of irradiationla One of the most controversial issues in radiation treatment following breast-conserving surgery is the use of a boost of radiation following the 45 to 50 Gy delivered to the whole breast. It is well accepted that most breast recurrences occur around the primary tumor site. This provides the rationale for a boost dose to the tumor bed. Indirect comparisons among randomized trials, however, suggest that a boost dose does not reduce the risk of local recurrence in patients with clear margins after breast-conserving ~urgery.'~, 27, 74, lz7 A randomized trial from Lyon, France,'"' comparing a 10-Gy boost with no boost for patients with negative margins, showed a 5-year actuarial breast recurrence rate of 3.6% for patients receiving the boost and 4.5% for those receiving no boost. ( P < 0.05).'01 (A large EORTC trial closed in 1996, but no data are available as yet.)
Controversy also exists regarding further management when the pathologist reports microscopic involvement of the resection margins with invasive cancer or DCIS. Solin et aP6 used four different doses of radiation, namely 60 Gy, 62.4 Gy, 64 Gy, and 65 Gy, based on the microscopic status of the margins for negative (greater than 2 mm), unknown, close (smaller than 2 mm), and focally positive margins, respectively. There was no significant difference in the local control rate.
SEQUENCING OF CHEMOTHERAPY AND RADIATION
CONSERVING SURGERY THERAPY IN PATIENTS TREATED WITH BREAST-
Clinical trials have demonstrated the effectiveness of chemotherapy in in- creasing overall survival48 and the need for radiation therapy to assure a local control of the primary site.27 Nonetheless, the optimal relative timing of chemo- therapy and radiation therapy has yet to be defined. Options include giving all chemotherapy before or after irradiation (sequencing), simultaneous initiation of chemotherapy and irradiation (concurrent), or the initiation of radiation therapy during the chemotherapy program (sandwich). Concurrent regimens have the theoretical advantage of initiating both local and regional treatment and systemic therapy at the same time, without a delay in either modality. This approach may lower the risk of breast cancer recurrence but may also result in an increase in acute and chronic complication^.^^ In the University of Pennsylvania Fox Chase Center, patients are treated by concomitant chemotherapy with Cytoxan, metho- trexate, and fluorouracil (CMF) or Cytoxan, doxorubicin, and fluorouracil (CAF) and irradiation, but the methotrexate or doxorubicin component is omitted during the irradiation. The investigators reported on 209 patients, 89% with positive lymph nodes, and found a 79% 10-year overall survival rate and an 84% rate for good and excellent cosmesis. The rate of complications was very low: 2% of patients experienced radiation pneumonitis and rib fractures, and there were no radiation-related cardiac It is possible that delaying the initiation of radiation therapy beyond 16 weeks after breast-conserving surgery might be associated with an increased risk of local failures3; however, the data are conflicting.Is

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1101
Only a few randomized trials have addressed the question of optimum sequencing. In patients treated by mastectomy, Lara-Jimenez et al" have con- ducted a randomized trial assigning patients to three groups: radiation therapy followed by chemotherapy (six cycles of CMF), chemotherapy followed by radiation therapy, or a sandwich approach using three cycles of CMF, radiation therapy, then three cycles of CMF. The number of patients treated was relatively small (80 patients), and the results are published in abstract form The authors observed the best results with the sandwich approach, but any conclu- sion may be somewhat premature because of the number of patients in the study. In another study of patients treated by breast-conserving surgery, Recht et apR randomly assigned 244 patients treated between 1984 and 1992 to receive a 12-week course of chemotherapy either before or after radiation therapy. The median follow-up was 58 months (range, 10 to 124 months). The 5-year actuarial rates of total failure, distant failure, and overall survival in the radiation therapy- first and chemotherapy-first arms were 38% and 31% ( P = 0.17), 37% and 25% (P = 0.05), and 73% and 81% ( P = O . l l ) , respectively. The 5-year crude rate of local failure at the first failure site was 5% in the radiation therapy-first arm and 13% in the chemotherapy-first arm. The risks of distant or regional failure (without simultaneous local failure) were 32% and 20% in the two arms, respec- tively. This difference in the patterns of failure was of borderline statistical significance ( P = 0.07). The study showed that the risk of local failure was higher in the chemotherapy-first arm, and the risk of distant failure was higher in the radiation therapy-first arm. For patients with close, positive, or unknown resection margins, the crude 5-year local failure rates were 5% among patients in the radiation therapy-first group and 23% among patients in the chemother- apy-first group. Among patients with negative margins, however, the risk of local failure was not increased when patients received chemotherapy first.
At present, for the CMF schedule, most patients receive chemotherapy first if the margins are negative and if the interval between surgery and radiation therapy will not exceed 6 months. A randomized trial within the Boston area is being conducted to compare concomitant chemotherapy and radiation therapy with sequential chemotherapy and radiation therapy, using six cycles of CMF in patients with negative or fewer than three positive lymph nodes (Schulman et al, personal communication, 1998).
ROLE OF RADIATION THERAPY AFTER MASTECTOMY
The goal of adjuvant radiation therapy following mastectomy is the steriliza- tion of subclinical disease within the chest wall and peripheral lymphatics in patients at high risk. Several prospective randomized trials of adjuvant postmas- tectomy irradiation without chemotherapy have been conducted.30* 57, R9, Io6 In some of these trials, orthovoltage machines were used, and doses were less than the 45 to 50 Gy usually considered adequate for microscopic disease. Some trials included large proportions of node-negative patients and those with small tumors, who were at low risk for residual subclinical disease and thus unlikely to benefit from adjuvant irradiati~n.~~, lo6 In all these trials, the locoregional recurrence rate was significantly reduced to one third, from 30% to 45% local failure without radiation therapy to 10% to 15% with radiation therapy; however, there was no significant effect on disease-free and overall survival.
The most recent of these trials was conducted in Stockholm between 1971 and 1976.'" The radiation doses and techniques used in this trial are considered adequate to control subclinical diseases. After a median follow-up of 16 years,

1102 TAGHIAN &I POWELL
the locoregional recurrence rate of patients treated by mastectomy alone was 207'0, compared with 4% for those who also received adjuvant radiation therapy. This reduction in local failure rate was found in both node-positive and node- negative patients. Furthermore, in node-positive patients only, the incidence of distant metastasis and death from breast cancer were significantly reduced by the addition of adjuvant radiation therapy. In a combined analysis of the Oslo and Stockholm data, Auquier et a15 showed a significant improvement in rates of locoregional recurrence and disease-free survival and, in node-positive patients receiving adjuvant radiation therapy, a trend towards improvement in overall survival. In their meta-analyses, Cuzick and coworkersz0 concluded that irradia- tion improved breast cancer-specific mortality rates. In more recent trials, how- ever, the irradiation-reduced death rate was offset by an increased number of cardiac deaths. The authors recommend the use of techniques that would mini- mize the cardiac risk.
Fowble et a143 analyzed 627 patients enrolled in an Eastern Cooperative Oncology Group (ECOG) adjuvant chemotherapy study, in which radiation therapy was not used, in an attempt to identify a subgroup of patients treated by mastectomy and adjuvant chemotherapy who would benefit from adjuvant radiation therapy. Among patients with four to seven metastatic axillary lymph nodes, 10% had an isolated locoregional recurrence for tumor smaller than 5 cm and 31% had an isolated local recurrence for tumor larger than 5 cm ( P = 0.001). Among patients with one to three positive lymph nodes, the rate of isolated locoregional recurrence was 6% when the tumor was smaller than 5 cm and 12% when the tumor was larger than 5 cm. Other unfavorable prognostic factors for isolated locoregional recurrence included negative ER status, pectoral fascia involvement, and tumors with necrosis.
The widespread use of adjuvant chemotherapy in patients with lymph node-positive disease has led investigators to reassess the role of adjuvant radiation therapy in patients treated by mastectomy and adjuvant chemotherapy. Two recent trials that are of special interest have shown for the first time a significant improvement in disease-free and overall survival rates from adding postmastectomy irradiation to patients with positive lymph nodes and, in the Danish trial, patients with stage T3NO disease, treated by adjuvant CMF (Table 6).86* 96 The benefit from irradiation was found among all subgroups of patients: patients with one to three positive lymph nodes and those with more than four positive lymph nodes; patients with tumors smaller than 2 cm, 2 to 5 cm, and
Table 6. TEN-YEAR DISEASE-FREE SURVIVAL AND OVERALL SURVIVAL AMONG HIGH RISK WOMEN TREATED WITH CHEMOTHERAPY WITH OR WITHOUT RADIATION
Surviving (%)
Disease-Free Overa I I Survival Survival Investigators FOIIOW-UP
(References) (Y) CT CT+RT P CT CT+RT P Ragaz et 15 41 56 0.007 54 64 0.07 British Columbia
Danish Breast Cancer Overgaard et alR6 10 34 48 0.001 45 54 0.001
CT = chemotherapy; RT = radiation therapy; P = statistical probability

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1103
larger than 5 cm; and patients with grade I, grade 11, or grade I11 tumors. In the Danish however, the axillary lymph node dissection, in which the median number of lymph nodes removed was seven, was considered inadequate by the American standard of care. In both trials CMF chemotherapy was used, and radiation therapy included the chest wall and regional lymph node areas.
Therefore, the indications for postmastectomy radiation therapy include patients with four or more positive lymph nodes, the presence of extracapsular extension, positive or close margins, T3 tumors with positive lymph nodes (some would also include T3NO tumors), any T4 tumors, and pectoral fascia involvement. Although both trials demonstrate a significant benefit from radia- tion therapy in patients with one to three positive lymph nodes, its use for these patients is controversial and is the subject of a randomized trial in preparation (Pierce et al, personal communication). It is the policy at Massachusetts General Hospital to treat this group of patients with irradiation only to the chest wall, including the low axilla and internal mammary nodes but excluding the upper axilla and supraclavicular fossa. The radiation is administered with the assump- tion that the survival effect of locoregional therapy comes from eliminating disease at the primary site or first-station nodes. Excluding the axillary and supraclavicular fields reduces the complications of therapy, principally radiation pneumonitis and arm lymphedema.
ROLE OF RADIATION THERAPY IN LOCALLY ADVANCED BREASTCANCER
The definition of locally advanced breast cancer includes large tumors, extensive regional lymph node involvement, direct involvement of the skin or underlying chest wall, and tumors considered inoperable but without distant metastasis. Patients with locally advanced breast cancer had a poor survival rate after being treated with local therapy alone, whether i r r ad ia t i~n~~ or irradiation and surgery,136 and died from distant metastasis. Over the last three decades, combined modality therapy consisting of chemotherapy, radiation therapy, and surgery has been used to improve local and systemic control and overall sur- vival. The debate concerned the sequence in which these modalities should be used.
Neoadjuvant chemotherapy is chemotherapy delivered before removal of the primary tumor. Neoadjuvant chemotherapy followed by surgery and radia- tion is now emerging as a standard treatment for large carcinomas of the breast.'" It has been used extensively to treat locally advanced breast cancer, with varying degrees of success.21* 56, Recently, neoadjuvant chemotherapy has also been used to treat operable palpable breast cancer.9, 35 Neoadjuvant chemotherapy has several theoretical advantages. The presence of a palpable or radiographically measurable mass permits response to be assessed as a direct in vivo measure of the sensitivity of the tumor cells to the particular drugs used; early detection of a resistant tumor will enable the oncologist to discontinue a worthless therapy, thus avoiding unnecessary toxicity, or to change to a potentially more effective regimen. Also, the earlier the disease is treated, the less likely it is that resistant tumor clones will have emerged spontaneously. Finally, preoperative chemother- apy has been shown to reduce primary tumor size, thus allowing an increased rate of breast-conserving surgery. The rate of breast-conserving surgery used to treat locally advanced breast cancer after neoadjuvant chemotherapy varies between 50% and 90%.'6, 62, 121, IZ6 A correlation between response to chemo- therapy and relapse-free survival has also been indicated in some of these

1104 TAGHIAN & POWELL
studies.', 9, 16, 25, 64 Neoadjuvant chemotherapy has been compared in several randomized trials with adjuvant ~hemotherapy.~~, 79, 95, "' In two of the 111
the neoadjuvant arm was significantly superior to the adjuvant arm in overall"' and disease-free s~rvival.'~ In the other two trials,34, 95 both arms gave equivalent results in disease-free and overall survival. Therefore, neoadjuvant chemother- apy was found to be well-tolerated and effective, with no detriments in overall or disease-free survival, compared with standard adjuvant treatment.
Radiation therapy is an integral part of the multimodality treatment in locally advanced and inflammatory breast cancer. Radiation therapy has been used immediately after induction chemotherapy without surgery in patients who had complete clinical response121 or after surgery, whether mastectomy or lumpe~tomy.~~ In almost all studies, neoadjuvant chemotherapy completely cleared the breast and axillary lymph nodes of any microscopic evidence of invasive tumor as assessed by standard histologic examination in a small num- ber of patients, ranging between 3.5% and 16% of those treated?, 12, 35, 56, 64,
Neoadjuvant chemotherapy has also been shown to convert clinically involved axillary nodal disease to a pathologically negative status in 25% to 38% of breast cancer ~atients.3~. M), This response was shown to have an effect on survival.80
Theoretically, if a complete response is reflective of chemosensitivity in occult distant metastatic sites, patients who have a complete pathologic response in both the primary breast tumor and axillary lymph nodes after neoadjuvant chemotherapy should have higher disease-free survival rates than do patients with a lesser response." In a recent large series, patients with a pathologic complete response did, in fact, have significantly better disease-free and overall survival rates.9, In general, neoadjuvant chemotherapy can achieve a complete clinical response of 12% to 50%, a clinical partial response of 28% to 67%, and a total overall clinical response of 63% to 97%. Fewer than 5% of patients will progress under treatment.9, 25, 55, M), ''sf lz1 When irradiation is used in a neoadju- vant setting, the whole breast and the regional lymph node areas are being treated. The doses and techniques are similar to those described subsequently.
95,
OPTIMAL RADIATION THERAPY TECHNIQUES AND DOSES
Following the local excision of the primary tumor and lymph node dissec- tion (or sentinel node mapping63), radiation is delivered to the entire breast for a total of 4500 to 5000 cGy over 4.5 to 5.5 weeks, using 180 to 200 cGy/treatment. This is usually followed by a supplemental boost of 1000 to 1600 cGy, although the boost issue is not yet of proven benefit. The intact breast is treated with a pair of tangentially oriented photon fields (Fig. 1) to minimize lung and heart exposure, using supervoltage equipment and an isocentric technique.73 The me- dial field usually enters at the midline of the patient, and the lateral field enters about 2 cm below the lateral extent of the breast tissue. The inferior border extends approximately 2 cm below the breast, and the superior border extends beyond all palpable tissue or matches with the supraclavicular field. Adjust- ments must be made based on the patient's anatomy and the tumor location. The patient set-up should be accurately reproduced for each fraction. The dose distribution should be calculated at least at the central axis, with correction for lung density, and dose inhomogeneity should not exceed 10%. This will require the use of wedges or compensators. Computed tomographic (CT) scanning can be used in conjunction with simulation for isodose distribution planning in complex cases (tangents and internal mammary chain fields). Three-dimensional treatment planning is not yet routinely used; however, using the dose calculation

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1105
Figure 1. A central-axis CT slice showing the left breast with the standard tangents technique. The field configurations and isodose lines are for 6 MV photons.
algorithm, doses received by volumes of lung and heart can be estimated from dose-volume histograms.
The role of regional lymph node irradiation in patients with early stage breast cancer and positive lymph nodes is not yet well defined. In patients with histologically negative or one to three positive nodes, the addition of regional irradiation has a nonsignificant effect on the risk of a regional node rec~rrence.~~, 97 In the NSABP B-06 radiation was given to the breast only in both node-negative and node-positive patients. The overall rate of regional recurrence was 5.1% for all patients. Although these data suggest that omitting regional lymph node irradiation might be considered in patients with positive axillary nodes, it is omitted frequently only in patients with one to three positive nodes. It should be noted that in the Danishs6 and British Columbiayh trials of postmastectomy irradiation in node-positive patients, radiation was given to the chest wall and the regional lymph node areas, including the axilla, the supraclavicular, and the internal mammary chain. Regional lymph node irradia-

1106 TAGHIAN & POWELL
tion is only routinely used, however, in patients with four or more positive nodes and with extracapsular extension. Several studies" have failed to demon- strate any advantage in treating the axilla after a thorough lymph node dissec- tion has shown multiple positive nodes with extracapsular extension. Irradiation of the full axilla should be considered in patients with invasive cancers in whom axillary dissection was inadequate or omitted, although level I nodes are usually included within the tangential fields.
If a decision is made to treat the regional nodes, the doses used usually vary between 4500 and 5000 cGy delivered at a rate of 180 to 200 cGy/fraction. Irradiation of the internal mammary chain has always been a subject of contro- versy. On one hand, data from the NSABP B-04 trial3 failed to indicate that irradiation of the internal mammary chain reduced the probability of distant failure in patients with medially located tumors. On the other hand, data from Gustave-Roussy Institute4, 71 from 1195 patients with operable breast cancer and positive lymph nodes showed a significantly higher risk of metastasis and contralateral breast cancer in patients with a medially located primary site who did not receive internal mammary chain irradiation. The authors suggest that treating the internal mammary chain can reduce the risks of death and distant metastases in patients with positive nodes and internally located tumors. In a recent study from Italy137 examining the prognostic role of the site of the primary tumor in 2396 patients with long follow-up, the authors found that the risk of distant metastases and mortality increased by 30% and 20%, respectively, for internal and central tumors. The authors suggested irradiation of the internal mammary chain in these patients. This issue is the subject of an ongoing randomized trial conducted by the EORTC.
The treatment of the internal mammary chain in the context of breast- conserving surgery and radiation therapy is technically difficult. Several tech- niques have been described that differ in the amount of lung and heart in- cl~ded.9~ The use of electrons or a combination of electrons and photons seems to minimize the dose to the lung, heart, and thoracic spine and to reduce the incidence of complications when compared with irradiation by photons alone.
SIDE EFFECTS AND COMPLICATIONS OF RADIATION THERAPY
Radiation therapy to the breast is usually very well tolerated with few side effects. Early side effects include skin erythema, and tenderness leading to dry and then moist desquamation. These effects accumulate gradually over the course of treatment. The magnitude of the side effects can differ among patients, but virtually all patients recover satisfactorily. Another side effect is the development of breast edema and skin thickening, which has not been well studied and quantified. It might be caused by the combination of surgery (in particular the lymph node dissection) and radiation therapy. The effect of breast edema and skin thickening is mostly some discomfort and compromise in the cosmetic results.
The rate of complications from irradiation is usually low. The most frequent complication encountered in the past was arm edema. In a general review from 14 different series, Bretton and NelsonI3 reported an incidence of postmastec- tomy arm edema of 20% to 25%. This rate was increased by axillary irradiation. In breast-conserving treatment, Larson et a170 found that the risk of lymphedema was related to the use and extent of axillary surgery and to irradiation of the

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1107
entire axilla. The actuarial risk of arm edema at 6-year follow-up was 4% for patients treated without axillary surgery and 13% for patients treated with axillary surgery (P = 0.006). When patients were treated with full dissection (stripping of the axillary vein) and axillary radiation therapy, the risk of arm edema was 37%. When axillary surgery was less extensive (level I and 11), and axillary irradiation was used, this risk was only 7% (P < 0.001). In this series, arm edema was mostly mild or moderate, with no patient having severe edema. Other studies report similar 133
One of the possible complications is brachial plexopathy, which usually occurs when the supraclavicular and axillary regions are treated by irradiation. The classic clinical symptoms include shoulder discomfort and progressive par- esthesias and weakness in the arm and hands. Sometimes it becomes difficult to differentiate between radiation-induced plexopathy and plexopathy caused by recurrent lymph node disease in the axilla. Radiation plexopathy is usually related to the total dose and to the dose per fraction. In a study from the Royal Marsden Hospital, Powell et alg4 demonstrated that the incidence of brachial plexus injury was related to the dose per fraction. Patients who received 51 Gy in 15 fractions to the axilla had a 5.9% risk at 6-year follow-up compared with 1% for patients who received 54 Gy in 30 fractions (P < 0.01). The study from the Joint Center of Radiation Therapyg3 showed an incidence of 1.2% with a median time to appearance of 10.5 months. In 80% of patients who developed plexopathy, the symptoms were mild and resolved within 1 year. The study also showed that the risk of brachial plexopathy increased with the use of a third field of radiation, with a total dose larger than 50 Gy to the axilla, and with the use of adjuvant chemotherapyg3 Salner et allo7 described a form of "transient brachial plexopathy," characterized by transient paresthesias and weakness, and with a short latent period (median 4.5 months), which occurs when doses less than 50 Gy are used.
Rib fracture is another rare complication that can be seen in association with breast irradiation. The data from the Joint Center of Radiation Therapy93 showed that among 1624 patients treated, 29 (1.8%) developed this complication. The median time to occurrence was 12 months. This risk increased when 4-MV photons were used, compared with 6 or 8 MV. Among patients treated on a 4- MV machine, the risk increased when doses greater than 50 Gy were used and when adjuvant chemotherapy was given.
Radiation pneumonitis is a recognized complication of thoracic irradiation. Typically, patients present 2 to 6 months after completing radiation therapy with shortness of breath, dry cough, and low-grade fever. The risk and severity of radiation pneumonitis are related to the volume of lung irradiated and the doses used. In a study of 1624 patients by Lingos et al," 17 patients developed symptomatic radiation pneumonitis. In all cases, the symptoms were transient. The risk of pneumonitis increased with the use of a third field and with the use of adjuvant chemotherapy. In patients treated by three fields and adjuvant chemotherapy, the risk of radiation pneumonitis was 1.3% for patients treated with sequential chemotherapy and 8.8% for patients treated with concomitant Chemotherapy. The use of radiation therapy to treat the supraclavicular and axillary areas is usually associated with subsequent radiographic changes in the irradiated lungs without translation into clinical These changes can be confused with lung metastasis in the form of lymphangitis, if the radiologist is not familiar with them.
Injury to the heart is a possible complication of radiation therapy. The risk seems to be mostly related to the radiation technique used. In their updated meta-analysis, Cuzick et alZo showed an increased number of cardiac deaths in

1108 TAGHIAN &I POWELL
both early and recent trials, which was offset by a reduced number of deaths from breast cancer in patients who received postmastectomy radiation therapy. In the Stockholm the increased mortality from ischemic heart disease was associated with the use of an old technique in which a large volume of heart was irradiated, suggesting that the increase in cardiac mortality could be avoided by the use of appropriate techniques, namely three-dimensional plan- ning in cancer on the left side. An Italian study'** found that the combination of doxorubicin (Adriamycin) and breast irradiation on the left side given concur- rently increased the risk of cardiomyopathy.
Radiation-induced sarcoma of the soft tissue or bone and angiosarcoma of the intact breast has been rep0rted.9~. 135 In a series from Gustave-Roussy Institute, Taghian et aP9 reported that 9 of 7620 patients treated for breast cancer developed sarcoma within the irradiated fields. The mean latency period was approximately 10 years. The cumulative frequency was 0.2%, 0.43%, and 0.78% at 10,20, and 30 years, respectively. Angiosarcomas induced by breast irradiation usually present as reddish, bluish, and purple nodules or discoloration of the skin that are usually multiple, but the incidence is very
SUMMARY
Radiation therapy for breast cancer has gone through two revolutions in the last two decades: the routine use of radiation therapy in conjunction with breast-conserving surgery as an equivalent treatment to mastectomy, and the use of radiation therapy following mastectomy in advanced or node-positive disease. Indeed, the perception of postmastectomy radiation has gone full circle: from having no benefit when used for all cases, to being detrimental because of cardiac irradiation, to the present in which the selective use of irradiation in high-risk patients provides both an improvement in local control and an improvement of 8% to 10% in the survival rate. Improvements in radiation technique have reduced complications, in particular late cardiac deaths. The major issues still to be resolved are the targets for postmastectomy irradiation, determining which patients do not need radiation therapy for DCIS and for node-negative disease, and the efficacy of delivering radiation to just the affected quadrant rather than to the whole breast. At present, most patients approach radiation therapy for breast cancer with the knowledge that it has a very high probability of being successful.
References
1. Abdel-Wahab M, Wolfson A, Raub W, et al: The importance of postoperative radiation therapy in multimodality management of locally advanced breast cancer: A phase I1 trial of neoadjuvant MVAC, surgery and irradiation. Int J Radiat Oncol Biol Phys 40:875-880, 1998
2. Anscher M, Jones P, Prosnitz L, et al: Local failure and margin status in early-stage breast carcinoma treated with conservative surgery and radiation therapy. Ann Surg
3. Arriagada R, Le MG, Rochard F, et al: Conservative treatment versus mastectomy in early breast cancer: Patterns of failure with fifteen years of follow-up. J Clin Oncol
4. Arriagada R, Le M, Mouriesse H, et al: Long-term effect of the internal mammary chain treatment. Results of a multivariate analysis of 1195 patients with operable breast cancer and positive axillary nodes. Radiother Oncol 11:213-222, 1988
218~22-27, 1993
141558-1564, 1996

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1109
5. Auquier A, Rutqvist L, Host H, et al: Post-mastectomy megavoltage radiotherapy: The Oslo and Stockholm trials. Eur J Cancer 28:433437, 1992
6. Baker L: Breast cancer detection demonstration project: Five-year summary report. CA Cancer J Clin 32:194-225, 1982
7. Bartelink H, Border J, van Dongen J, et al: The impact of tumor size and histology on local control after breast conserving therapy. Radiother Oncol 11:297-303, 1988
8. Blichert-Toft M, Rose C, Anderson JA, et al: Danish randomized trial comparing breast conservation therapy with mastectomy: Six years of life table analysis. J Natl Cancer Inst Monogr 11:19-26, 1992
9. Bonadonna G, Valagussa P: Primary chemotherapy in operable breast cancer. Semin Oncol23:464-474, 1996
10. Bonadonna G, Valagussa P, Brambilla C, et al: Primary chemotherapy in operable breast cancer: Eight-year experience at the Milan Cancer Institute. J Clin Oncol
11. Boyages J, Recht A, Connolly J, et al: Early breast cancer: Predictors of breast recur- rence for patients treated with conservative surgery and radiation therapy. Radiother Oncol 19:29-35, 1990
12. Brain E, Garrino C, Misset J, et al: Long-term prognostic and predictive factors in 107 stage II/III breast cancer patients treated with anthracycline-based neoadjuvant chemotherapy. Br J Cancer 79:1360-1367, 1997
13. Bretton R, Nelson R Causes and treatment of postmastectomy lymphedema of the arm. JAMA 180:95-101, 1962
14. Burke M, Allison R, Tripcony L: Conservative therapy of breast cancer in Queensland. Int J Radiat Oncol Biol Phys 31:295-303, 1995
15. Buzdar A, Kau S, Smith T, et al: The order of administration of chemotherapy and radiation and its effect on the local control of operable breast cancer. Cancer 71:3680-3685, 1993
16. Calais G, Berger CH, Descamps PH, et al: Conservative treatment feasibility with induction chemotherapy, surgery, and radiotherapy for patients with breast carcinoma larger than 3 cm. Cancer 74:1283-1288, 1994
17. Clark R, McCulloch P, Levine M, et al: Randomized clinical trial to assess the effectiveness of breast irradiation following lumpectomy and axillary dissection for node-negative breast cancer. J Natl Cancer Inst 84:683-688, 1992
18. Clarke D, Le M, Sarrazin D, et al: Analysis of local-regional relapses in patients with early breast cancers treated by excision and radiotherapy: Experience of the Institut Gustave-Roussy Int J Radiat Oncol Biol Phys 11:137-142, 1985
19. Cowen D, Largillier R, Bardou VJ, et al: Positive margins after conservative treatments impacts local control and possibly survival in node-negative breast cancer [abstract #3]. Int J Radiat Oncol Biol Phys 42(suppl):126, 1998
20. Cuzick J, Stewart H, Rutqvist L, et al: Cause-specific mortality in long-term survivors of breast cancer who participated in trials of radiotherapy. J Clin Oncol 12:447453, 1994
21. Danforth D, Zujewski J, O'Shaughnessy J, et al: Selection of local therapy after neoadjuvant chemotherapy in patients with stage IIIA, B breast cancer. AM Surg Oncol5:150-158, 1998
22. de la Rochefordiere A, Asselain B, Campana F, et al: Age as a prognostic factor in premenopausal breast carcinoma. Lancet 341:1039-1043, 1993
23. de la Rochefordiere A, Mouret-Fourme E, Ricke Y, et al: Local and distant relapses in relation to age following breast-conserving surgery and irradiation in premeno- pausal patients with breast cancer [abstract #111]. Int J Radiat Oncol Biol Phys 42(suppl):180, 1998
24. Donegan W, Stine S, Samter T Implications of extracapsular nodal metastasis for treatment and prognosis of breast cancer. Cancer 72:778-782, 1993
25. Eltahir A, Heys S, Hutcheon A, et al: Treatment of large and locally advanced breast cancers using neoadjuvant Chemotherapy. Am J Surg 175:127-132, 1998
26. Farrow J: Current concepts in the detection and the treatment of the earliest of the early breast cancers. Cancer 25:468-477, 1970
27. Fisher B, Anderson S, Redmond CK, et al: Reanalysis and results after 12 years of
16~93-100, 1998

1110 TAGHIAN & POWELL
follow up in a randomized clinical trial comparing total mastectomy with lumpec- tomy with or without irradiation in the treatment of breast cancer. N Engl J Med 333:1456-1461, 1995
28. Fisher B, Costantino J, Redmond C, et al: Lumpectomy compared with lumpectomy and radiation therapy for the treatment of intraductal breast cancer. N Engl J Med
29. Fisher B, Redmond C, Fisher E, et a1 Lumpectomy for breast cancer: An update of the NSABP experience. J Natl Cancer Inst Monogr 11:7-12, 1992
30. Fisher B, Redmond C, Fisher E, et al: Ten year result of a randomized clinical trial comparing radical mastectomy and total mastectomy with or without irradiation in the treatment of breast cancer. N Engl J Med 312674-679, 1985
31. Fisher B, Redmond C, Poisson R, et al: Eight year results of a randomized clinical trial comparing mastectomy and lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med 320:822-828, 1989
32. Fisher 8, Wickerham D, Deutsch M, et al: Breast tumor recurrence following lumpec- tomy with and without breast irradiation: An overview of recent NSABP findings. Semin Surg Oncol8:153-160, 1992
33. Fisher B, Dignam J, Wolmark N, et al: Lumpectomy and radiation therapy for the treatment of intraductal breast cancer: Findings from the National Surgical Adjuvant Breast and Bowel Project B-17. J Clin Oncol 16:441452, 1998
34. Fisher B, Wolmark N, Redmond C, et al: Findings from NSABP Protocol B-04: Comparison of radical mastectomy with alternative treatments, the clinical and bio- logic significance of medial-central breast cancers. Cancer 48:1863-1872, 1981
35. Fisher B, Bryant J, Wolmark N, et al: Effect of preoperative chemotherapy on the outcome of women with operable breast cancer. J Clin Oncol 169672-2685, 1998
36. Fisher E, Costantino J, Fisher B, e al: Pathologic findings from the National Surgical Adjuvant Breast and Bowel Project (NSABP) Protocol 8-17: Intraductal carcinoma (ductal carcinoma in situ). Cancer 75:1310-1319, 1995
37. Fisher E, Costantino J, Fisher B, et al: Response: Blunting the counterpoint. Cancer
38. Fleck R, McNeese M, Ellerbroek N, et al: Consequences of breast irradiation in
328:1581-1586, 1993
15:1223-1227, 1995
patients with preexisting collagen vascular disease. Int J Radiat Oncol Biol Phys 17829-835, 1989
39. Forrest P, Stewart H, Everington D, et al: Randomized controlled trial of conservation therapy for breast cancer: 6-year analysis of the Scottish trial. Lancet 348:708-713,1996
40. Fourquet A, Campana F, Mosseri V, et al: Iridium-192 versus cobalt-60 boost in 3-7 cm breast cancer treated by irradiation alone: Final results of a randomized trial. Radiother Oncol 34114-120, 1995
41. Fourquet A, Campana F, Zafrani B, et al: Prognostic factors of breast recurrence in the conservative management of early breast cancer: A 25-year follow-up. Int J Radiat Oncol Biol Phys 17719-724, 1989
42. Fowble 8: Intraductal noninvasive breast cancer: A comparison of three local treat- ments. Oncology 3:5140, 1989
43. Fowble B, Gray R, Gilchrist K, et al: Identification of a subgroup of patients with breast cancer and histologically positive axillary nodes receiving chemotherapy who may benefit from post-operative radiotherapy. J Clin Oncol 6:1107-1117, 1988
44. Fowble B, Schultz D, Overmoyer 8, et al: The influence of young age on outcome in early stage breast cancer. Int T Radiat Oncol Biol Phvs 30:23-69. 1994
45.
46.
47.
Freidma; G, Fowble B, Hanlon A, et al: Patient; with close or positive margins treated with conservative surgery and radiation have an increased risk of breast recurrence that is delayed by adjuvant systemic therapy [abstract #4]. Int J Radiat Oncol Biol Phys 42(suppl):126, 1998 Gage I, Schnitt S, Nixon A, et al: Pathologic margin involvement and the risk of recurrence in patients treated with breast-conserving therapy. Cancer 78:1921-1928, 1996 Gallagher E, Buchsel P: Breast cancer and fatigue: How to help women with breast cancer live with treatment-related fatigue. Am J Nurs (suppl) 17-20, 1998

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1111
48. Early Breast Cancer Trialists’ Collaborative Group: Systemic treatment of early breast cancer by hormonal, cytotoxic or immune therapy. Lancet 339:l-15, 71-85, 1992
49. Early Breast Cancer Trialists’ Collaborative Group: Effects of radiotherapy and sur- gery in early breast cancer. N Engl J Med 333:1444-1455, 1995
50. Halverson K, Taylor M, Perez C, et al: Regional nodal management and patterns of failure following conservative surgery and radiation therapy for stage I and I1 breast cancer. Int J Radiat Oncol Biol Phys 26:593-599, 1993
51. Harris J, Morrow M: Treatment of early-stage breast cancer. In Harris J, Morrow M, Hellman S (eds): Diseases of the Breast. Philadelphia, Lippincott-Raven, 1996
52. Harris J, Sawicka J, Gelman R, et al: Management of locally advanced carcinoma of the breast by primary radiation therapy. Int J Radiat Oncol Biol Phys 9:345-351, 1983
53. Hartsell W, Recine D, Griem K, et al: Delaying the initiation of intact breast irradiation for patients with lymph node positive breast cancer increases the risk of local recur- rence. Cancer 76:2497-2503, 1995
54. Holland R, Connolly J, Gelman R, et al: The presence of an extensive intraductal component following a limited excision correlates with prominent residual disease in the remainder of the breast. J Clin Oncol 8:113-118, 1990
55. Hortobagyi G, Ames F, Buzdar U, et al: Management of stage 111 primary breast cancer with primary chemotherapy, surgery, and radiation therapy. Cancer 62:2507- 2516, 1988
56. Hortobagyi G, Blumenschein G, Spanos W, et al: Multimodal treatment of locoregio- nally advanced breast cancer. Cancer 51:763-768, 1983
57. Host H, Brennhovd I, Loeb M: Postoperative radiotherapy in breast cancer: Long- term results from the Oslo study. Int J Radiat Oncol Biol Phys 12:727-732, 1986
58. Jacobson J, Danforth D, Cowan K, et al: Ten-year results of the National Cancer Institute’s randomized trial of breast conservation versus mastectomy for stage I and I1 breast cancer. N Engl J Med 332:907-911, 1995
59. Jacquemier J, Kurtz J, Amalric R, et al: An assessment of extensive intraductal component as a risk factor for local recurrence after breast conserving therapy. Br J Cancer 61:873-876, 1990
60. Jaquillat C, Baillet F, Weil M, et al: Results of conservative treatment combining induction (neoadjuvant) and consolidation chemotherapy, hormonotherapy, and ex- ternal and interstitial irradiation in 98 patients with locally advanced breast cancer (IIIA-IIIB). Cancer 61:1977-1982, 1988
61. Kinne D, Petrek J, Osborne M, et al: Breast carcinoma in situ. Arch Surg 124:33-36, 1989
62. Kling K, Ostrzega N, Schmit P: Breast conservation after induction chemotherapy for locally advanced breast cancer. Am Surg 63:861-864, 1997
63. Krag D, Weaver D, Ashikaga T, et al: The sentinel node in breast cancer. A multicenter validation study. N Engl J Med 330:941-946, 1998
64. Kuerer H, Newman L, Smith T, et al: Clinical course of breast cancer patients with complete pathologic primary tumor and axillary node response to doxorubicin-based neoadjuvant chemotherapy. J Clin Oncol 1:460469, 1999
65. Kurtz J, Jacquemier J, Amalric R, et al: Why are local recurrences after breast- conserving therapy more frequent in younger patients? J Clin Oncol 8:591-596, 1990
66. Lagios M: Ductal carcinoma in situ: Controversies in diagnosis, biology, and treat- ment. Breast Journal 1:68-78, 1995
67. Lagios M, Margolin F, Westdahl P, et al: Mammographically detected duct carcinoma in situ: Frequency of local recurrence following tylectomy and prognostic effect of nuclear grade on local recurrence. Cancer 63:619-624, 1989
68. Lagios M, Westdahl P, Margolin F, et al: Duct carcinoma in situ: Relationship of occult invasion, multicentricity, lymph node metastasis and short term treatment failures. Cancer 50:1309-1314, 1982
69. Lara-Jimenez P, Garcia Puche J, Pedraza V Adjuvant combined modality treatment in high risk breast cancer patients: Ten-year results [abstract] Proceedings of the 5th EORTC Breast Cancer Working Conference, 1991
70. Larson D, Weinstein M, Goldberg I, et al: Edema of the arm as a function of the

1112 TAGHIAN & POWELL
extent of axillary surgery in patients with stage I and I1 carcinoma of the breast treated with primary radiotherapy. Int J Radiat Oncol Biol Phys 122377-882, 1986
71. Le M, Arriagada R, de Vathaire F, et al: Can internal mammary chain treatment decrease the risk of death for patients with medial breast cancers and positive axillary lymph nodes? Cancer 66:2313-2318, 1990
72. Levine M, Bramwell V, Abu-Zahra H, et a1 The effect of systemic adjuvant chemother- apy on local breast recurrence in node positive breast cancer patients treated by lumpectomy without radiation. Br J Cancer 65:13&132, 1992
73. Lichter A, Fraass B, Yanke 8: Treatment techniques in the conservative management of breast cancer. Semin Radiat Oncol2:94-99, 1992
74. Liljegren G, Holmberg L, Adami HO, et a1 Sector resection with or without postopera- tive radiotherapy for stage I breast cancer: Five-year results of a randomized trial. J Natl Cancer Inst 86717-722, 1994
75. Lin P, Allison D, Wainstock J, et a1 Impact of axillary lymph node dissection on the therapy of breast cancer patients. J Clin Oncol 11:1536-1541, 1993
76. Lingos T, Recht A, Vincini F, et al: Radiation pneumonitis in breast cancer patients treated with conservative surgery and radiation therapy. Int J Radiat Oncol Biol Phys 21:355-360, 1991
77. Mansfield C, Komanicky L, Scwartz G, et al: Ten-year results in 1070 patients with stages I and I1 breast cancer treated by conservatke surgery and radiation therapy. Cancer 75:2328-2336, 1995
78. Margolin F, Lagios M: Mammographic detection of early breast cancer. West J Med 144:46-48, 1986
79. Mauriac L, Durand M, Avril A, et al: Effects of primary chemotherapy in conservative treatment of breast cancer patients with operable tumors larger than 3 cm. Ann Oncol
80. McCready D, Hortobagyi G, Kau S, et a1 The prognostic significance of lymph node metastasis after preoperative chemotherapy for locally advanced breast cancer. Arch Surg 124:21-25, 1989
81. Morris A, Morris R, Wilson J, et a1 Breast-conserving therapy versus mastectomy in early-stage breast cancer: A meta-analysis of 10 year survival. Cancer Journal Scientific American 36-12, 1997
82. Morris M, Powell S: Irradiation in the setting of collagen vascular disease: Acute and late complications. J Clin Oncol 15:2728-2735, 1997
83. National Institutes of Health Consensus Development Panel Consensus Statement: Treatment of early-stage breast cancer. J Natl Cancer Inst Monogr 11:ll-15, 1992
84. Nemoto T, Pate1 J, Rosner D, et al: Factors affecting recurrence in lumpectomy without irradiation for breast cancer. Cancer 672079-2083, 1991
85. Olivotto I, Rose M, Osteen R, et a1 Late cosmetic outcome after conservative surgery and radiotherapy: Analysis of causes of cosmetic failure. Int J Radiat Oncol Biol Phys
86. Overgaard M, Hansen P, Overgaard J, et a1 Postoperative radiotherapy in high-risk premenopausal women with breast cancer who receive adjuvant chemotherapy. N Engl J Med 337949-955, 1997
87. Overmoyer B, Fowble B, Solin L, et a1 The long term results of conservative surgery and radiation with concurrent chemotherapy for early breast cancer [abstract]. Pro- ceedings of the American Society of Clinical Oncology 11:90, 1992
88. Page D, Lagios M: Pathologic analysis of the NSABP-B17 trial: Unanswered questions remaining unanswered considering current concept of ductal carcinoma in situ. Cancer 75:1219-1222, 1995
89. Palmer M, Ribeiro G: Thirty-four year follow up of patients with breast cancer in clinical trial of postoperative radiotherapy. British Medical Journal Clinical Research Edition 291:1088-1091, 1985
90. Park C, Mitsumori M, Recht A, et a1 The relationship between pathologic margin status and outcome after breast-conserving therapy [abstract #1]. Int J Radiat Oncol Biol Phys 42(supp):125, 1998
91. Patchevsky A, Scwartz G, Finkelstein S, et al: Heterogeneity of intraductal carcinoma of the breast. Cancer 63:731-741, 1989
2347-354, 1991
17747-753, 1989

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1113
92. Perez C, Taylor M, Halverson K, et al: Brachytherapy or electron beam boost in conservation therapy of carcinoma of the breast: A nonrandomized comparison. Int J Radiat Oncol Biol Phys 34:995-1007, 1996
93. Pierce S, Recht A, Lingos T, et al: Long term radiation complications following conservative surgery and radiation therapy in early-stage breast cancer. Int J Radiat Oncol Biol Phys 23:915-923, 1992
94. Powell S, Cooke J, Parsons C: Radiation-induced brachial plexus injury: Follow-up of two different fractionation schedules. Radiother Oncol 18:213-218, 1990
95. Powles T, Hickish T, Makris A, et al: Randomized trial of chemoendocrine therapy started before or after surgery for treatment of primary breast cancer. J Clin Oncol
96. Ragaz J, Jackson S, Le N, et al: Adjuvant radiotherapy and chemotherapy in node- positive premenopausal women with breast cancer. N Engl J Med 337:956-962, 1997
97. Recht A, Pierce S, Abner A, et al: Regional node failure after conservative surgery and radiotherapy for early-stage breast cancer. J Clin Oncol 9:988-993, 1991
98. Recht A, Come S, Henderson I, et al: The sequencing of chemotherapy and radiation therapy after conservative surgery for early-stage breast cancer. N Engl J Med
99. Roberson P, Lichter A, Bodner A, et al: Dose to the lung in primary breast irradiation. Int J Radiat Oncol Biol Phys 9:97-102, 1982
100. Robertson J, Clarke D, Pevzner M, et al: Breast conservation therapy: Severe breast fibrosis after radiation therapy in patients with collagen vascular disease. Cancer
101. Romestaing P, Lehinge Y, Carrie C, et al: Role of 10 Gy boost in the conservative treatment of early breast cancer: Results of a randomized clinical trial in Lyon, France. J Clin Oncol 15:963-968, 1997
102. Rose M, Henderson I, Gelman R, et al: Premenopausal breast cancer patients treated with conservative surgery, radiotherapy and adjuvant chemotherapy have a low risk of local failure. Int J Radiat Oncol Biol Phys 17711-715, 1989
103. Ross J, Hussey D, Mayr N, et al: Acute and late reactions to radiation therapy in patients with collagen vascular diseases. Cancer 71:3744-3750, 1993
104. Rothwell R, Kelly S, Joslin C: Radiation pneumonitis in patients treated for breast cancer. Radiother Oncol 4:9-14, 1985
105. Rutqvist L, Lax I, Fornander T, et al: Cardiovascular mortality in a randomized trial of adjuvant therapy versus surgery alone in primary breast cancer. Int Radiat Oncol Biol Phys 22:887-892, 1992
106. Rutqvist L, Petterson D, Johansson H: Adjuvant radiation therapy versus surgery alone in operable breast cancer: Long-term follow-up of a randomized clinical trial. Radiother Oncol26:104-110, 1993
107. Salner A, Botnik L, Herzog A, et al: Reversible brachial plexopathy following primary radiation therapy for breast cancer. Cancer Treatment Reports 65:915-920, 1981
108. Salvadori 8: Local recurrences after breast-conserving treatment: An open problem. Semin Surg Oncol 12:46-52, 1996
109. Schnitt S, Abner A, Gelman R, et al: The relationship between microscopic margins of resection and the risk of local recurrence in breast cancer patients treated with conservative surgery and radiation therapy. Cancer 74:1746-1751, 1994
110. Schnitt S, Hayman J, Gelman R, et al: A prospective study of conservative surgery alone in the treatment of selected patients with stage I breast cancer. Cancer 771094- 1100, 1996
111. Scholl S, Fourquet A, Asselain B, et al: Neoadjuvant versus adjuvant chemotherapy in premenopausal patients with tumours considered too large for breast conserving surgery: Preliminary results of a randomized trial: S6. Eur J Can 30A:645-652, 1994
112. Schwartz G, Birchansky C, Kormarnicky L, et al: Induction chemotherapy followed by breast conservation for locally advanced carcinoma of the breast. Cancer 73:362- 369, 1994
113. Schwartz G: The role of excision and surveillance alone in subclinical DCIS of the breast. Oncology 8:21-26, 1994
13~547-552, 1995
3341356-1361, 1996
68:502-509, 1991

1114 TAGHIAN & POWELL
114. Silverstein M, Lagios M, Groshen S, et al: The influence of margin width on local control of ductal carcinoma in situ of the breast. N Engl J Med 340:1455-1461, 1999
115. Smitt M, Nowels K, Zdeblick M, et al: The importance of the lumpectomy surgical margin status in long term results of breast conservation. Cancer 76:259-264, 1995
116. Solin L, Fowble B, Schultz D, et a1 The significance of pathology margins of the tumor excision on the outcome of patients treated with definitive irradiation for early-stage breast cancer. Int J Radiat Oncol Biol Phys 21:279-287, 1991
117. Solin L, Kurtz J, Fourquet A, et a1 Fifteen year results of breast conserving surgery and definitive breast irradiation for the treatment of ductal carcinoma in situ (intra- ductal carcinoma) of the breast. J Clin Oncol 14:754-759, 1996
118. Swain S, Sorace R, Bagley C, et a1 Neoadjuvant chemotherapy in the combined modality approach of locally advanced breast cancer. Cancer Res 473889-3894, 1987
119. Taghian A, de Vathaire F, Terrier P, et al: Long-term risk of sarcoma following radiation treatment for breast cancer. Int J Radiat Oncol Biol Phys 21:361-368, 1991
120. Touboul E, Belkacemi Y, Lefranc J, et a1 Early breast cancer: Influence of type of boost (electrons vs Iridium-192 implant) on local control and cosmesis after conserva- tive surgery and radiation therapy. Radiother Oncol34:105-113, 1995
121. Touboul E, Buffat L, Lefranc J, et al: Possibility of conservative local treatment after combined chemotherapy and preoperative irradiation for locally advanced nonin- flammatory breast cancer. Int J Radiat Oncol Biol Phys 34:1019-1028, 1996
122. Valagussa P, Zambetti M, Biasi S, et a1 Cardiac effects following adjuvant chemother- apy and breast irradiation in operable breast cancer. AM Oncol5:209-214, 1994
123. van Dongen J, Bartelink H, Fentiman I, et al: Randomized clinical trial to assess the value of breast-conserving therapy in stage I and I1 breast cancer, EORTC 10801 trial. J Natl Cancer Inst Monogr 11:15-18, 1992
124. Van Limbergen E, Van der Bogaert W, Van der Schueren E, Rijnders A: Tumor excisions and radiotherapy as primary treatment of breast cancer: Analysis of patient and treatment parameters and local control. Radiother Oncol8:l-9, 1987
125. Veronesi U, Banfi A, Salvadori B Breast conservation is the treatment of choice in small breast cancer: Long-term results of a randomized trial. Eur J Cancer 26:668- 670, 1990
126. Veronisi U, Bonadonna G, Zurrida S, et al: Conservation surgery after chemotherapy in large carcinomas of the breast. Ann Surg 222:612-618, 1995
127. Veronisi U, Luini A, Del Vecchio M, et al: Radiotherapy after breast-preserving surgery in women with localized cancer of the breast. N Engl J Med 328:487-491,1993
128. Veronisi U, Luini A, Galimberti V, Zurrida S Conservation approaches for the man- agement of stage 1/11 carcinoma of the breast: Milan Cancer Institute trials. World J Surg 18:70-75, 1994
129. Veronisi U, Salvadori B, Luini A, et al: Breast conservation is a safe method in patients with small cancer of the breast: Long-term results of these randomized trials of 1,973 patients. Eur J Cancer 31A:1574-1581, 1995
130. Veronisi U, Salvadori B, Luini A, et al: Conservative treatment of early breast cancer: Long-term results of 1232 cases treated with quadrantectomy, axillary dissection, and radiotherapy. Ann Surg 211:250-256, 1990
131. Vicini F, Recht A, Abner A, et al: Recurrence in the breast following conservative surgery and radiation therapy for early-stage breast cancer. J Natl Cancer Inst Monogr 11:33-39, 1992
132. Vrieling C, Collette L, Fourquet A, et a1 for the EORTC Radiotherapy and Breast Cancer Cooperative Group: The higher local recurrence rate after breast conserving therapy in young patients explained by larger tumor size and incomplete excision at first attempt? [abstract 21. Int J Radiat Oncol Biol Phys 42(suppl):125, 1998
133. Werner R, McCormick B, Petrek J, et al: Arm edema in conservatively managed breast cancer: Obesity is a major predictive factor. Radiology 180177-192, 1991
134. Winchester D, Cox J: Standard for breast conservation treatment. CA Cancer J Clin 134-137, 1992
135. Zucali R, Merson M, Placuci M, et al: Soft tissue sarcoma of the breast after conserva- tive surgery and irradiation for early mammary cancer. Radiother Oncol 30271-276, 1994

THE ROLE OF RADIATION THERAPY FOR PRIMARY BREAST CANCER 1115
136. Zucali R, Uslenghi C, Kenda R, et al: Natural history and survival of inoperable breast cancer treated with radiotherapy and radiotherapy followed by radical mastec- tomy. Cancer 371422-1427, 1976
137. Zucali R, Mariani L, Marubini E, et al: Early breast cancer: Evaluation of the prognos- tic role of the site of the primary tumor. J Clin Oncol 16:1363-1366, 1998
Address reprint requests to Alphonse G. Taghian MD, PhD
Breast Cancer Unit Department of Radiation Oncology, Box 3
Massachusetts General Hospital Boston, MA 02114
e-mail: [email protected]




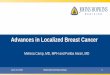













![Case Report Primary MALT Lymphoma of the Breast Treated ... · radiation therapy, such as involved eld radiation therapy, and a moderate dose of Gy are recommended [,]. Treatment](https://img.pdfslide.net/doc/110x75/6136877c0ad5d20676481606/case-report-primary-malt-lymphoma-of-the-breast-treated-radiation-therapy-such.jpg)










