Embed Size (px)
Citation preview

hf. 1. Radiation Oncology Biol. Phyx, 1977, Vol. 2. pp. 88S894. Pergamon Press. Printed in the U S.A.
??Original Contribution
THE ROLE OF RADIATION THERAPY IN CANCER OF THE EXTRA-HEPATIC BILIARY SYSTEM:
AN ANALYSIS OF THIRTEEN PATIENTS AND A REVIEW OF THE LITERATURE OF THE EFFECTIVENESS OF SURGERY,
CHEMOTHERAPY AND RADIOTHERAPY?
GENE KOPE:LSON, A.B.,S LEON HARISIADIS, M.D.,§ PATRICIA TRETTER, M.D.7 and CHU H. CHANG, M.D.11
Division of Raldiotherapy, Department of Radiology, College of Physicians and Surgeons, Columbia- Presbyterian Medical Center, New York, 10032, U.S.A.
An analysis of the role of radiotherapy in the management of gallbladder (GB) and extra-hepatic bile duct (EHBD) cancer iis based upon thirteen patients irradiated in our hospital and a review of the literature. These patients were treated as part of curative or palliative management in conjunction with surgery, after surgical failure or recurrence, and as the only palliative modality. Doses ranged from 3800 to 7225 rad.
Signillcant palliation was obtained in 92% of the patients; average total billrubin value decreased from 9.1 mg.% before to 1.7 mg.% after radiotherapy. The mean survival of all patients was 12.7 months after surgery (7.1 in (GB, 16.1 in EHBD), and was 7.3 months after initiation of radiotherapy (6.3 in GB, 8.0 in EHBD). Two patients were alive and well with no evidence of disease 12 and 16 months after radiotherapy, and local tumor control was achieved in two. Complications included possible biliary fibrosis.
Based upon a critical review of the surgical, chemotherapeutic, and radiotherapeutic literature, it is concluded that present surgical therapy fails because of extensive regional disease in which local recurrences follow various simple and radical surgical maneuvers; palliative surgery often fails. Survival rates have been poor following any therapy at present, although encouraging results are seen with carefully planned megavoltage radiotherapy.
A proposal iis made to evaluate the role of radiotherapy systematically: as part of curative therapy post-operatively to decrease local recurrences and to increase the length and quality of survival; to treat incfsional recurrences; as part of advanced disease management to increase the effectiveness and length of palliation; and i!n conjunction with chemotherapy to further consolidate therapeutic gains made with radio- therapy alone.
Radiotherapy, Gallbladder neoplasms -radiotherapy, Bile duct neoplasms-radiotherapy, Bile duct-radia- tion effects, Gallbladder-radiation effects, Radiation injuries.
INTRODUCTION
Survival figures are distressingly poor for gallbladder (GB) and extrahepati.c bile duct (EHBD) cancer. Recent studies give an overall 5-year survival rate of 6-7% in GB cancer4(‘,55,61,65,6 and less than 5% in EHBD cancer,22*72,99.109 although the prognosis is not so dismal in periampullary tumors.6*7~‘2~51~‘02*‘@j
We have studied our hospital records of 13 patients who received radiotherapy for GB and EHBD cancer, and have reviewed the literature with special re- ference to the cause of surgical failure and the role of radiotherapy and chemotherapy in the treatment of these tumors.
Although several textbooks”252.73 state that radiation METHODS AND MATERIALS therapy has no role in the management of these A review of the case registry at the Division of tumors, to our knowledge this has never been sub- Radiotherapy of the Columbia-Presbyterian Medical stantiated. Center revealed 15 patients with a diagnosis of GB or
tThis investigation was supported in part by United States Public Health Service Training Grant No. 5 TOl-CA 05181 from the National Cancer Institute.
*Senior Medical Student, College of Physicians and Sur- geons, Columbia University. After 20 June 1977: Associate Resident, Department of Radiation Medicine, Mas- sachusetts General Hospital, Boston, MA 02114, U.S.A.
OAssistant Professor of Clinical Radiology. TAssociate Professor of Clinical Radiology.
883
[/Professor of Radiology and Director, Division of Radiotherapy.
Reprint requests to: Leon Harisiadis, M.D., Division of Radiotherapy, Columbia-Presbyterian Medical Center, 622 West 168th Street, New York, NY 10032, U.S.A. Acknowledgements-The authors would like to thank Miss Susanne Thomasian and Mrs. Mindy Printz-Kopelson for their help in the preparation of this manuscript.
884 Radiation Oncology 0 Biology 0 Physics September-October 1977, Volume 2, No. 9 and No. 10
EHBD carcinoma who were treated with radio- therapy between January 1958 (the beginning of the installation of the Betatron) and December 1976, inclusive. Two patients were excluded from further analysis since they did not complete their planned courses of radiotherapy: one refused further therapy after receiving only 600 rad of a planned 4000 rad; in the other patient, therapy was terminated halfway through the course because the patient developed progressive respiratory failure because of pulmonary metastases, of which she died. The remaining 13 patients constitute this series.
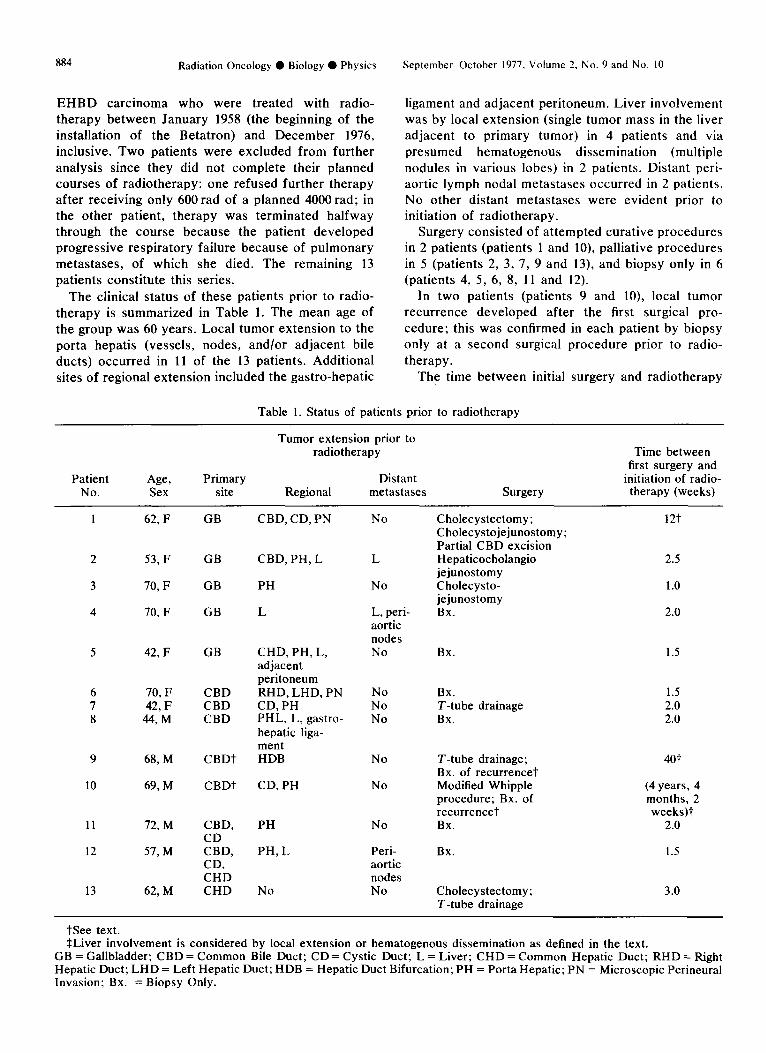
The clinical status of these patients prior to radio- therapy is summarized in Table 1. The mean age of the group was 60 years. Local tumor extension to the porta hepatis (vessels, nodes, and/or adjacent bile ducts) occurred in 11 of the 13 patients. Additional sites of regional extension included the gastro-hepatic
ligament and adjacent peritoneum. Liver involvement was by local extension (single tumor mass in the liver adjacent to primary tumor) in 4 patients and via presumed hematogenous dissemination (multiple nodules in various lobes) in 2 patients. Distant peri- aortic lymph nodal metastases occurred in 2 patients. No other distant metastases were evident prior to initiation of radiotherapy.
Surgery consisted of attempted curative procedures in 2 patients (patients 1 and lo), palliative procedures in 5 (patients 2, 3, 7, 9 and 13), and biopsy only in 6 (patients 4, 5, 6, 8, 11 and 12).
In two patients (patients 9 and lo), local tumor recurrence developed after the first surgical pro- cedure; this was confirmed in each patient by biopsy only at a second surgical procedure prior to radio- therapy.
The time between initial surgery and radiotherapy
Table 1. Status of patients prior to radiotherapy
Patient Age, Primary No. Sex site
Tumor extension prior to radiotherapy
Distant Regional metastases Surgery
Time between first surgery and
initiation of radio- therapy (weeks)
1 62, F GB CBD, CD, PN No
2 53, F
3 70, F
4 70, F
GB CBD, PH, L L
GB PH No
GB L
5 42, F GB
L, peri- aortic nodes No
6 70, F CBD 7 42, F CBD 8 44,M CBD
No Bx. No T-tube drainage No Bx.
9
10
11
12
13
68, M
69, M
CBDt
CHD, PH, L, adjacent peritoneum RHD, LHD, PN CD, PH PHL, L, gastro- hepatic liga- ment HDB No
CBDt CD, PH No
72, M
57, M
CBD, CD CBD, CD, CHD CHD
PH No
PH, L
62, M No
Peri- aortic nodes No
Cholecystectomy; Cholecystojejunostomy; Partial CBD excision Hepaticocholangio jejunostomy Cholecysto- jejunostomy Bx.
12t
2.5
1.0
2.0
Bx. 1.5
1.5 2.0 2.0
T-tube drainage; Bx. of recurrence-? Modified Whipple procedure; Bx. of recurrencet Bx.
401
(4 years, 4 months, 2 weeks)t
2.0
1.5 Bx.
Cholecystectomy; T-tube drainage
3.0
See text. SLiver involvement is considered by local extension or hematogenous dissemination as defined in the text.
GB = Gallbladder; CBD = Common Bile Duct; CD = Cystic Duct; L = Liver; CHD = Common Hepatic Duct; RHD = Right Hepatic Duct; LHD = Left Hepatic Duct; HDB = Hepatic Duct Bifurcation; PH = Porta Hepatic; PN = Microscopic Perineural Invasion; Bx. = Biopsy Only.
Biliary system radiotherapy ??G. KOPELSON et al. 885
usually was approxima.tely 2 weeks. In patient 1, a 4 month delay resulted from poor wound healing and pneumonia which was treated successfully with anti- biotics prior to radiotherapy. In patients 9 and 10, there were longer delays because radiotherapy was given only after the local recurrence had developed.
Indications for radiation therapy included: no im- provement in jaundice or worsening of jaundice after surgery (patients 2, 6 and 7), tumor was close to the surgical margin (patient l), tumor recurrence after surgery (patients 9 and lo), palliation since only a biopsy was done (patients 4, 5, 6, 8, 11 and 12), and hope to improve palliation with surgery and radio- therapy (patients 2 and 13).
Adjuvant chemotherapy was used in 6 patients, consisting of 5-fluoro-uracil (12.5-15.0 mg/kg), which
was given: prior to radiotherapy (patient 9), during the first 3 days of radiotherapy (patients 4, 5 and 8), or begun only after radiotherapy (patients 1 and 10). All patients who received the chemotherapy continued to receive it at monthly cycles after the completion of radiotherapy. Streptozotocin was used in 1 GB patient also.
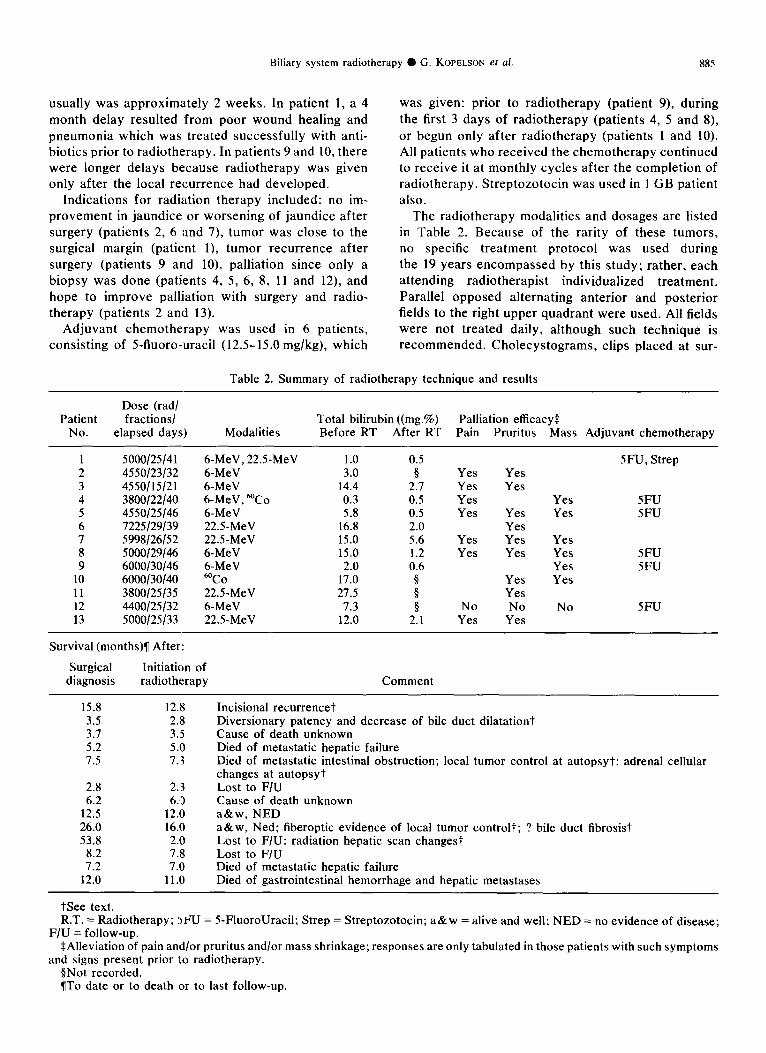
The radiotherapy modalities and dosages are listed in Table 2. Because of the rarity of these tumors, no specific treatment protocol was used during the 19 years encompassed by this study; rather, each attending radiotherapist individualized treatment. Parallel opposed alternating anterior and posterior fields to the right upper quadrant were used. All fields were not treated daily, although such technique is recommended. Cholecystograms, clips placed at sur-
Table 2. Summary of radiotherapy technique and results
Dose @ad/ Patient fractions/ Total bilirubin ((mg.%) Palliation efficacy*
No. elapsed days) Modalities Before RT After RT Pain Pruritus Mass Adjuvant chemotherapy
1 5000/25/41 6-MeV, 22.5-MeV 1.0 0.5 SFU, Strep 2 4550123132 6-MeV 3.0 0 Yes Yes 3 4550/15/21 6-MeV 14.4 2.1 Yes Yes 4 3800/22/40 6-MeV, @‘Co 0.3 0.5 Yes Yes 5FU 5 4550/25/46 6-MeV 5.8 0.5 Yes Yes Yes 5FU 6 7225129139 22.5-MeV 16.8 2.0 Yes 7 5998/26/52 22.5-MeV 15.0 5.6 Yes Yes Yes 8 5000/29/46 6-MeV 15.0 1.2 Yes Yes Yes 5FU 9 6000/30/46 6-MeV 2.0 0.6 Yes 5FU
10 6000/30/40 @co 17.0 Yes Yes 11 3800/25/35 22.5-MeV 21.5 1 Yes 12 4400/25/32 6-MeV 1.3 0 No No No SFU 13 5000/25/33 22.5-MeV 12.0 2.1 Yes Yes
Survival (months)7 After:
Surgical diagnosis
Initiation of radiotherapy Comment
15.8 12.8 3.5 2.8 3.7 3.5 5.2 5.0 7.5 7..3
2.8 2.3 6.2 6.0
12.5 12.10 26.0 16.10 53.8 2.10
8.2 7.8 7.2 7.10
12.0 11 .I0
Incisional recurrencet Diversionary patency and decrease of bile duct dilatationt Cause of death unknown Died of metastatic hepatic failure Died of metastatic intestinal obstruction; local tumor control at autopsyt; adrenal cellular changes at autopsyt Lost to F/U Cause of death unknown a&w, NED a&w, Ned; fiberoptic evidence of local tumor control?-; ? bile duct fibrosist Lost to F/U: radiation hepatic scan changest Lost to F/U Died of metastatic hepatic failure Died of gastrointestinal hemorrhage and hepatic metastases
tSee text. R.T. = Radiotherapy; :)FU = 5-FluoroUracil; Strep = Streptozotocin; a&w = alive and well; NED = no evidence of disease;
F/U = follow-up. *Alleviation of pain and/or pruritus and/or mass shrinkage; responses are only tabulated in those patients with such symptoms
and signs present prior to radiotherapy. PNot recorded. ITo date or to death or to last follow-up.
886 Radiation Oncology 0 Biology 0 Physics September-October 1977, Volume 2, No. 9 and No. 10
gery, and post-operative T-tube cholangiograms were used often to determine the treatment field. Portal size was approximately 10 X 10 to 16 X 16 cm. for the initial 2000-2500 rad; then field sizes usually were reduced for the remainder. Hepatic shields usually were added after 3000rad, although the tumor bed (determined by the procedures mentioned above) received the total dose.
RESULTS [TABLE 21 During the course of radiotherapy, successful pal-
liation (alleviation of jaundice and /or pain and/or pruritus and/or mass shrinkage) was obtained in 12 of 13 patients (92%). Symptoms and signs which were abnormal prior to radiotherapy were palliated successfully in 7 of 8 patients for pain (SS%), 9 of 10 patients for pruritus (90%), and 6 of 7 patients for mass shrinkage (86%). In 9 patients in whom labora- tory values were recorded both before and at the completion of radiotherapy, the average total biliru- bin value decreased from 9.1 mg.% before to 1.7 mg.% after. In patient 2, although no laboratory data was obtained after radiotherapy, there was cholangiographic evidence after radiotherapy that the surgical diversion was patent and that the previous bile duct dilatation had decreased. This documented relief of obstructive jaundice occurred both in those irradiated patients who did and who did not receive adjuvant chemotherapy. It also was achieved in those irradiated patients who were biopsied only and in those whose surgical palliative biliary diversion was failing. In fact, the only patient who did not respond to radiotherapy (patient 10) had both hepatic and distant metastases prior to radiotherapy, and he died of these.
The survival after diagnosis of all patients ranged from 2.8 to 53.8 months, had a mean of 12.7 months (7.1 in GB patients and 16.1 in EHBD patients), and had a median of 7.5 months (5.2 in GB patients and 10.1 in EHBD patients).
The survival after initiation of radiotherapy in all patients ranged from 2.0 to 16.0 months, had a mean of 7.3 months (6.3 in GB patients and 8.0 in EHBD patients), and had a median of 7.0 months (5.0 in GB patients and 7.4 in EHBD patients).
Analysis of the 10 patients with complete follow-up to date or to death (excluding patients 6, 10 and 11) revealed the mean survival after diagnosis was 10.0 months (7.1 in GB patients and 12.8 in EHBD patients), and the median was 7.4 months (5.2 in GB patients and 12.0 in EHBD patients). The mean sur- vival after initiation of radiotherapy was 8.3 months (6.3 in GB patients and 10.4 in EHBD patients), and the median was 7.2 months (5.0 in GB patients and 11.0 in EHBD patients).
In patients in whom the cause of death was known,
3 died of liver metastases (patients 4, 10 and 13); in 2 of these 3, both liver involvement and distant metas- tases were evident prior to radiotherapy. One patient (patient 5), died with widespread metastatic disease (ileal metastasis causing intestinal obstruction).
The two patients treated most recently (patients 8 and 9) were alive and well without evidence of disease after 12 and 16 months post-radiotherapy, respectively.
Aspects of local control and complications will be discussed later.
DISCUSSION FAILURE OF PRESENT THERAPY
Distant disease Patients do not usually present with distant disease
already evident on admission. In those series listing the general type of therapy used at presentation (i.e. curative, palliative, or inoperable), 500 of 1998 (25.0%) GB patients, 8.21,33.36,41.50.J6.61,65-67,72.76,87.94,98,l09
and 65 of 475 (13.7%) EHBD pa- tients 2,6.27.30,38,51,54,70.72.102.104.108.109 reviewed from the li- terature were judged “inoperable” at presentation. In many series, however, it often was unclear if “in- operable” meant that such extensive regional disease was present as to preclude curative resection or whether distant metastases were present. In addition, many surgical series have excluded such “inoperable” patients from study, and other studies provide insuffi- cient data. However, it can be concluded that most patients do not present with widely disseminated tumor.
Failure of curative surgery GB Cancer. After routine cholecystectomy many
patients are found to have occult carcinoma present in the resected gallbladder without further therapy being done; at surgery others are found to have apparent localized cancer which then is treated with curative intent by simple cholecystectomy. Several authors believe that simple cholecystectomy is cura- tive for localized disease because in their own series, the only “cures” (i.e. S-year survivors) were in this category.9*‘s”‘g’
However, a review of the literature of the known incidence of local recurrences in series giving specific follow-up of patients (Table 3) reveals that patients eventually failed because of such local recurrences.
In terms of early deaths, of 110 patients reviewed from seven series who died within 5 years after “curative” simple cholecystectomy, 95 (86%) died because of or with a local tumor recurrence (Table 3). This undoubtedly is why a recent review of eleven series could find only 30 reported 5-year survivors after “curative” simple cholecystectomy;’ 2 other cases have been reported recently.”
Biliary system radiotherapy 0 G. KOPELSON et al. 887
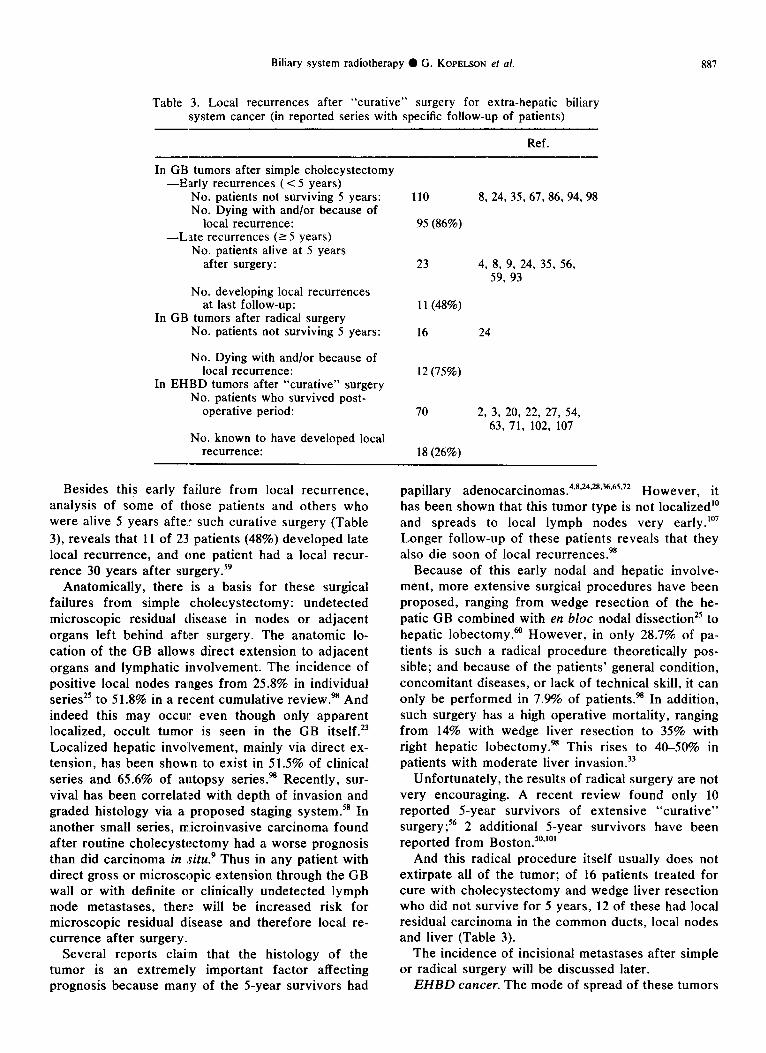
Table 3. Local recurrences after “curative” surgery for extra-hepatic biliary system cancer (in reported series with specific follow-up of patients)
Ref.
In GB tumors after simple cholecystectomy -Early recurrences (< 5 years)
No. patients not surviving 5 years: No. Dying with and/or because of
local recurrence: -L.ate recurrences (2 5 years)
No. patients alive at 5 years after surgery:
No. developing local recurrences at last follow-up:
In GB tumors after radical surgery No. patients not surviving 5 years:
No. Dying with and/or because of local recurrence:
In EHBD tumors after “curative” surgery No. patients who survived post-
operative period:
No. known to have developed local recurrence:
110 8, 24, 35, 67, 86, 94, 98
95 (86%)
23 4, 8, 9, 24, 35, 56, 59, 93
11(48%)
16 24
12 (75%)
70 2, 3, 20, 22, 27, 54, 63, 71, 102, 107
18 (26%)
Besides this early failure from local recurrence, analysis of some of those patients and others who were alive 5 years after such curative surgery (Table 3), reveals that 11 of 23 patients (48%) developed late local recurrence, and one patient had a local recur- rence 30 years after surgery.59
papillary adenocarcinomas.4~8~“~28~36~65~72 However, it has been shown that this tumor type is not localized” and spreads to local lymph nodes very early.“’ Longer follow-up of these patients reveals that they also die soon of local recurrences.98
Anatomically, there is a basis for these surgical failures from simple cholecystectomy: undetected microscopic residual disease in nodes or adjacent organs left behind after surgery. The anatomic lo- cation of the GB allows direct extension to adjacent organs and lymphatic involvement. The incidence of positive local nodes ranges from 25.8% in individual series” to 51.8% in a recent cumulative review.% And indeed this may occur even though only apparent localized, occult tumor is seen in the GB itself.23 Localized hepatic involvement, mainly via direct ex- tension, has been shown to exist in 51.5% of clinical series and 65.6% of autopsy series.% Recently, sur- vival has been correlated with depth of invasion and graded histology via a proposed staging system.” In another small series, microinvasive carcinoma found after routine cholecystectomy had a worse prognosis than did carcinoma in *situ.’ Thus in any patient with direct gross or microscopic extension through the GB wall or with definite or clinically undetected lymph node metastases, there will be increased risk for microscopic residual disease and therefore local re- currence after surgery.
Because of this early nodal and hepatic involve- ment, more extensive surgical procedures have been proposed, ranging from wedge resection of the he- patic GB combined with en bloc nodal dissection** to hepatic lobectomy.@’ However, in only 28.7% of pa- tients is such a radical procedure theoretically pos- sible; and because of the patients’ general condition, concomitant diseases, or lack of technical skill, it can only be performed in 7.9% of patients.% In addition, such surgery has a high operative mortality, ranging from 14% with wedge liver resection to 35% with right hepatic lobectomy.98 This rises to 40-50% in patients with moderate liver invasion.33
Unfortunately, the results of radical surgery are not very encouraging. A recent review found only 10 reported S-year survivors of extensive “curative” surgery? 2 additional 5-year survivors have been reported from Boston.“*“’
And this radical procedure itself usually does not extirpate all of the tumor; of 16 patients treated for cure with cholecystectomy and wedge liver resection who did not survive for 5 years, 12 of these had local residual carcinoma in the common ducts, local nodes and liver (Table 3).
Several reports claim that the histology of the The incidence of incisional metastases after simple tumor is an extremely important factor affecting or radical surgery will be discussed later. prognosis because many of the 5-year survivors had EHBD cancer. The mode of spread of these tumors
888 Radiation Oncology 0 Biology 0 Physics September-October 1977, Volume 2, No. 9 and No. IO
is through the bile duct wall early,** even with small tumors3’ causing extensive regional disease in 75% of patients even before the jaundice begins.” They also spread along the bile duct, and this may not be appreciated on gross examination.‘7*42 A litera- ture review of eleven surgical and autopsy series ~~**~~~~~~~~~~~~~~‘~80.~~.1~~~~~ shows that 155 patients of
376 (41%) had lymph node involvement and 133 patients of 371 (36%) had liver involvement, common in all types of tumor locations. Nodal metastases without apparent local extension also have been described.82 Perineural invasion occurs in more than 60% of patients,47,57.93 and this will be mentioned again later.
Curative procedures for EHBD tumors have varied with the tumor location. Hepatic ductal region tumors have been treated with tumor resection and hepatic- enteric anastamosis,70.92 hepatic lobectomy with in- trahepatic-cholangio-jejunostomy,27.64”os and total hepatectomy with liver transplantation.27 Mid-ductal region tumors (cystic duct and proximal common bile duct) have been treated with resection and end-to-end or biliary-enteric anastamosis5’,” and distal common bile duct tumors have been treated with pancreatico- duodenectomy.6.22.79~‘~~‘W
However, although occasional long-term survivors have been described,3,‘2*38*5’,a2~102 “curative” surgery generally is not highly curative. A literature review of 16 series 2,6.20,22,27,38,45,51,54,70.93.99,104,105,108.109 reveals a cu- mulative average survival in 94 patients treated with “curative” surgery was 16.9 months.
One reason for failure is the high surgical mortality (death within 1 month after surgery) after “curative” procedures. Of 368 patients in 13 series reviewed from the literature 2~6~7~12~20~22~27~49~63~70~93.102
post-operative mortality rate. there was an 18%
A second reason is that local recurrences occur after this “curative” surgery. A literature review of 10 series in which follow-up of patients with reason for failure was given (Table 3) shows that 26% of patients are known to have developed a local recur- rence.
This high rate of local recurrence is seen even when surgical margins are clear and nodes are nega- tive,** and has been related to the high incidence of perineural invasion,47,68 the difficulty in appreciating intraductal tumor infiltration,” the leaving behind of tumor cells at curative surgery,68V’04 and the recent finding that these tumors might be multicentric within the biliary system-thus making local curative resec- tion inadequate.”
This local recurrence rate must in fact be even higher, since there are so few long-term survivors and the average survival time is only 16.9 months (see above). In addition, patients die not from extensive distant nor hepatic metastatic disease but from local recurrence with extensive unrelieved biliary obstruc-
tion leading to hepatocellular failure.22~43~68~Y7~‘o’~‘02 Therefore, one must infer that localized disease is still present even after “curative” surgery to cause local recurrences in much greater numbers than the above 26% incidence would indicate.
Failure of palliative surgery Most patients with GB cancer have such extensive
regional disease that curative surgery is precluded and palliative biliary diversionary procedures alone must suffice.44.62*98 However, palliative surgery in GB cancer carries a fairly high surgical mortality of 13.7%.% It is successful only in 51% of patients, with an average survival after palliation of 4.6 months.%
Most patients with EHBD cancer can only receive surgical palliation for similar reasons as GB patients, 2.6,12.20,22.27.30,38,45,51.54.57,68.73,93,99,102.104,106.109 thus, these patients have known tumor left behind after surgery. This group also has a high surgical mortality and poor prognosis. A literature review reveals that of 149 patients from 9 series, there was 31% post- operative mortality;2~6~27*43~4s~49~93~102~’~ and of 157 pa- tients from 17 series, the average survival was only 9.3 months after surgery. 2,6,17,20,22,34,43,49,51,54,63,70,&1.106
Course of conservatively managed patients A recent review showed that patients who are only
biopsied at surgery or those untreated by surgery had a mean survival of. 1.1 months for GB tumors;98 and of 125 patients. reviewed from 11 series, the mean survival . was* 2.7 months for EHBD tumors 20,34.41.4~54,P3,76.80.93,,~~~109 This latter group also had
* an extremely .high su;gical morfality; of 64 patients reviewed from sixseries;th&post-operative mortality was 91%. 34X45V~93*‘?2;‘W Of &t&e; in this very advanced disease group’ the reason for death may very well have been the extent of tumor rather than operative factors.’ ’ ’ I ,’
Failure of chemotherapy Most authors concur that chemotherapy has had
little success in the palliative or curative management of GB or EHBD tumors,9~32~38~““‘~73~98.108~109 although some patients do show objective responses usually lasting a few months,‘9.52*53*85 but occasionally to years, 19*5499~‘02 to various agents, mainly Sfluorouracil. These variable results, from no response to apparent long-term successes, are seen because in some in- stances chemotherapy was added as part of curative treatment for local disease, and in other cases was only used after extensive regional and/or metastatic disease was present. In addition, in many patients radiotherapy was used in addition to
Biliary system radiotherapy 0 G. KOPILSON el al. 889
chemotherapy;38,56,%*99 the direct effects of the latter are thus difficult to distinguish. The possible value of such combination radiotherapy-chemotherapy will be discussed later.
RADICtTHERAPY
Radiation therapy has not been used often in the management of these tumors. Early workers sug- gested palliative radiothlerapy for squamous cell tu- mors but cited no cases;“‘*’ others achieved some palliation by infusions of “‘I-Rose Bengal.’ The re- ported use of radiotherapy for GB and EHBD cancer follows:
GB cancer. Lam@ treated three patients with radium implants but gave no follow-up. Ackerman and de1 Regato reported 1 patient who presented with invasion through and beyond the GB wall and ves- sels; the patient was griven intensive post-operative @‘Co and remained well for 5 years. Friedlands pal- liated 1 patient with locally recurrent leionmyosar- coma with a dose of 6000 rad (@‘Co) achieving both relief of pain and decrease in tumor mass; the patient died 5 months later. Moossa et a1.56 described 9 patients with apparently advanced disease who were treated with unspecified radiation doses: 3 with radio- therapy alone, 2 with combined surgery and radio- therapy, and 4 with combined chemotherapy and radiotherapy. The only follow-up was of the 2 treated by surgery and radiotherapy: 1 died of residual disease 2.5 years later; in the other patient (whose tumor was anaplastic and had extended to the subserosal fat with lymphatic and perineural invasion), the patient was alive and well ,without recurrence after 2 years at the time of the report. The author suggested that radiotherapy might improve the poor results of surgery. Krain& claimed that 2% of GB cancer patients in California were given radiotherapy only as the primary curative modality, and 22% were given combined surgery and radiotherapy; however, spe- cific survival statistics based upon modality were not given. Vaittener? found that 24 patients with lo- calized disease who were treated by “curative” sur- gery (most by simple cholecystectomy) had a median survival of 29 months; but those 7 patients who were given postoperative radiotherapy (unspecified dose) had a much longer me:dian survival of 63 months. However, the numbers were too few to be of statis- tical significance. Finally, Treadwell and Hardin% treated patients post-operatively by radiotherapy only (3 patients) and by radiotherapy and chemotherapy (6 patients). Doses ranged from 1000 to 4500r (dose not otherwise specified). Increased survival and better palliation was noted in patients receiving such ad- junctive therapy after surgery, although there was no distinction made in evaluating results as to which adjunctive therapies were used. The authors sug-
gested the use of such additional therapy in these patients.
EHBD cancer. Walters and Olson’00 described a patient with papillary adenocarcinoma of the duct bifurcation which was incompletely excised; the patient was given interstitial radium implants for 140 mg-hr, had a decrease in jaundice, and survived 2.5 months. Ariel and Pack’ described 2 patients who received 6000r (dose not otherwi‘se specified) external radiotherapy who survived 11.5 and 32 months after diagnosis. Van Heerden et a/.% described 2 patients who were given palliative radiotherapy with biliary diversion and chemotherapy for common bile duct and common hepatic duct lesions; the survived 5 and 24 months. Whelton et a!.‘@’ mentioned 5 patients who were given 5000 rad external radiotherapy (“Co) with palliative bypass surgery; they survived an average of 27 months after surgery and 18 months after initiation of radiotherapy. Green et al.” described 4 patients who were given palliative radiotherapy (2000- 5300 rad, @‘Co) for common hepatic duct tumors; they survived an average of 11.5 months after surgery. Terblanche et a1.88-w described 5 patients who were given radiotherapy (6000R: unspecified) in con- junction with palliative surgery for hepatic duct lesions. One patient died of the disease after 5 years; 1 patient was alive with recurrence after 2.5 years; but 3 patients were alive and well without recurrence after 2.5, 3.75 and 3.75 years. The author suggested that radiotherapy in conjunction with diversion might be curative.88 KrainM claimed that 19% of patients in California were given radiotherapy as part of initial management of this disease (2% radiotherapy only, 17% radiotherapy plus surgery); but no survival statistics according to modality were given. Finally, Hudgins and Meoz37 treated 3 patients with 5000 rad and obtained relief of obstructive jaundice for 6, 6 and 1 months after radiotherapy. They suggested that radiotherapy should be used in the palliative management of these tumors.
Some indications for radiation therapy in the management of these tumors include:
To increase survival. As seen earlier, the mean and median survivals after diagnosis in the GB group were 7.1 and 5.2 months, respectively; and after initiation of radiotherapy were 6.3 and 5.0 months, respectively. These figures appear to be higher than the previously-cited figures of 1.1 months for the no-treatment group and 4.6 months for the surgical palliation group.
In the EHBD group, the mean and median sur- vivals after diagnosis were 16.1 and 10.1 months, respectively, and after initiation of radiotherapy were 8.0 and 7.4 months, respectively. This appears to be higher than the previously-cited figures of : 2.7 months for the no-treatment group and 9.3 months for the
890 Radiation Oncology 0 Biology ??Physics September-October 1977, Volume 2. No. Y and No. IO
palliative surgery group. However these data appear not to be as good as the 16.9 months for the curative surgery group.
However, the 3 patients in our series who received radiotherapy with curative intent (patients 1, 9 and (lo), has an average survival of at least 31.9 months after diagnosis and 10.6 months after initiation of radiotherapy. Of course our series is retrospective and not randomized, and the number of patients discussed above is far too small to make a truly valid comparison; however, these data would suggest that post-operative radiotherapy can increase the length and quality of survival in both EHBD and GB cancer patients in comparison with surgery alone (curative or palliative), chemotherapy, or the conservatively managed group. Also, most patients in our series and those in the literature had fairly extensive regional disease and/or distant metastases when they were given radiotherapy; thus, increases in survival should be expected if patients with earlier disease receive radiotherapy. Finally, larger series of patients are needed in properly controlled and randomized series in order to completely evaluate the added survival provided by post-operative radiotherapy.
To achieve local tumor control. As seen from ear- lier discussion, most patients with these tumors who are treated with curative or palliative surgery develop and/or die because of locally recurrent tumor and not because of distant metastases. Thus control of tumor at the primary site is the major therapeutic objective in the management of this disease at present.
These tumors are not as radioresistant as was thought formerly. Green et al.” reported one patient in whom apparent local tumor control was achieved after 2000rad because at autopsy “there was no evidence of persistent cancer”, although serial sec- tions were not obtained. In our patient 9, a post- radiation (6000 rad) flexible fiberoptic-scope bile duct cannulation revealed that “no obvious tumor was seen. The bifurcation was sharp, and bile flowed from the right and left hepatic ducts”. In patient 5, the autopsy report read that after 4550 rad “the gallbladder received the highest dose of radiation, as a result of which, there are almost no malignant cells. The hepatic and common bile ducts were patent without evidence of tumor”, even though the tumor had been there at the biopsy only surgery which was performed prior to radiotherapy.
Thus there was no evidence of local tumor recur- rence in the primary site after radiotherapy, and local tumor control was achieved. A few histologically- intact cells that persist after radiotherapy do not necessarily indicate later local tumor growth.83
For palliation. As seen earlier, surgical palliation fails as often as it succeeds? indeed 3 patients in our
series (patients 3, 6 and 7), 1 in the series of Green et al.,3’ and 2 in the series of Hudgins and Meoz” were specifically given radiotherapy because surgery failed; 6 of our patients had no surgical palliation done at all. Yet in our series, radiotherapy achieved a 92% success rate with palliation, and this occurred even in patients who were not given palliative sur- gery. Thus radiotherapy can successfully palliate patients in combination with surgery, even when surgical palliation either was not attempted or had failed. And although the number of patients discussed is small, this 92% success rate in radiotherapeutic palliation appears to be much higher than the 51% with surgery.98
For suture line recurrences. Incisional recurrences after surgery have been described previously for GB 40,60,87.98 and EH~D2.43.63.89,‘~ tumors_
Radiotherapy has been of value in these patients, although Tanga and Ewing” described a suture-line recurrence that was unresponsive to an unspecified dose of radiation. But Pack et a1.60 described a patient who was treated with local radiotherapy (unspecified dose) and who survived 5 months, only to die of liver failure. Vaittinen% described a patient who was treated successfully with radiotherapy (unspecified dose) for such a lesion and who died 10 years later of generalized carcinomatosis; presumably this local radiotherapy succeeded in sterilizing the incisional recurrence. Kaplan4 described a patient with an incisional recurrence who was treated successfully with 800r (dose not otherwise specified) external radiotherapy and 3000 mg-hr of radium implantation.
Unfortunately, our patient 1 developed such a re- currence after radiotherapy. One of us (L.H.) has computed that the skin was in fact underdosed (ap- proximately 2000 rad) in this patient because 22 MeV X-rays were used. We suggest that a bolus on the skin be used in the incision area to prevent such incisional metastases whenever megavoltage radiotherapy is used.
In combination with chemotherapy. The combined use of radiotherapy-chemotherapy has been reported sporadically in the past.38,56*%*99 In our series, the mean and median survivals after diagnosis of the group (patients 1, 4, 5, 8, 9 and 12) receiving combined radiotherapy-chemotherapy (12.4 and 10.0 months, respectively) appears to be slightly higher than the remaining group receiving radiotherapy alone (11.5 and 6.2 months, respectively). Also, the two patients presently alive and well without evidence of disease (patients 8 and 9) did receive such combined therapy. It should be noted, however, that documented relief of obstructive jaundice in our series occurred after radiotherapy whether or not chemotherapy was used.
Larger series obviously are needed in order to
Biliary system radiotherapy 0 G. KOPELSON et al. 891
completely evaluate -the potentials of combined modality adjunctive therapy in these tumors.
COMPLICATIONS
Radiotherapy in this group of patients was tolerated quite well. In patient 1, a liver scan after 3000rad showed an area of decreased uptake about the porta hepatis that later resolved; such subclinical liver changes were expected. 39*78 Complaints which were unrelated to the primary disease but could be related to the irradiation of intestinal epithelium within the portals (proximal small bowel), such as diarrhea, often were not mentioned in the charts and thus are difficult to evaluate; most patients ex- perienced nausea and slight vomiting however. Also, patient 5 showed pyknotic adrenal cellular changes; adrenal and kidney changes can be expected if the entire kidney is included in the irradiated field. 74*7J*77
After receiving 600Orad, patient 9 was evaluated four months later via fiberoptic-scope for residual bile duct pathology. Although no tumor was found, there was “slight narrowing of the right hepatic duct for 1 cm with no proximal dilation. . . the bifurcation (of the hepatic ducts) was sharp, and bile flowed from the right and left hepatic ducts”; on cholangiogram, the “right hepatic duct seemed narrow”. Liver function tests all were normal, and the patient was asymp- tomatic.
The effects of radiotherapy on the human extra- hepatic biliary system are not well known. Case and Warthin14 found swollen bile duct walls and bile duct atrophy at autopsy of three patients who were given intensive abdominal radiotherapy. Warrenlo reviewed earlier work and found that heavy doses produced inflammation and necrosis of the GB. Ariel and Pack’ described one patient who had moderate cholangitis at autopsy 2 months after receiving 15 mCi of 13’1- Rose Bengal for GB cancer; this was thought to be the result of excretion of the radioactive dye in the bile. Recently, Green et ~1.~’ reported that 1 of 4 patients at autopsy had extensive fibrosis of the com- mon hepatic and common bile ducts after radio- therapy; however repeated T-tube manipulation was felt to be the cause.
Patient 9 was subjected to two surgical procedures plus chemotherapy and1 radiotherapy. He was asymp- tomatic when this fibrosis was seen, and there was no evidence of hindrance of bile flow nor proximal dilation. Thus even if radiation were the cause of this fibrosis, it caused no physiological problems.
Although part of the pancreas was within the radiation fields, there was no evidence in our patients that pancreatic fibrosis’b16*69*‘03 resulted.
CONCLUSIONS After a review of our series of 13 patients and an
extensive critical literature review of surgery, che- motherapy, and radiotherapy in the management of GB and EHBD tumors, we have drawn the following conclusions:
1. Most patients neither present with nor die of distant metastatic disease; thus, local and regional tumor control is at present the primary therapeutic objective. With increasing local control resulting from adjuvant radiotherapy, distant metastases may be- come more of a problem.
2. Curative surgery has a high post-operative mor- tality; most of these patients die eventually because of or with local recurrent tumor. Very few long-term survivors have been reported.
3. Palliative surgery has a high post-operative mortality, a low survival rate, and it fails as often as it succeeds.
4. Data presented here suggests that radiation therapy can increase the length and quality of sur- vival and be of definite palliative benefit in patients on whom curative surgery and palliative surgery has been performed. It also is a considerable benefit for patients in whom surgical recurrence has occurred, and for those patients in whom surgical palliation has failed or in whom biopsy only was done.
5. These tumors are not particularly radioresistant, and local tumor control can be achieved with radio- therapy.
6. Incisional recurrences can be eradicated suc- cessfully with radiotherapy.
7. Chemotherapy alone may be of some transient palliative benefit in some patients, although com- bination with radiotherapy may further improve results.
Post-operative radiotherapy has been shown to decrease local tumor recurrence in many types of tumors;‘* approximately 4500-5000rad in 4-5 weeks has been shown to sterilize small foci of adenocar- cinema in other sites;26 it seems reasonable that this will be true in extrahepatic biliary system tumors as well.
1. Post-operative radiotherapy be given after cura- tive surgery especially in those patients with inadequate surgical margins and/or locally aggressive tumors to increase the length and quality of survival by decreasing the incidence of local recurrences (and by decreasing incisional metastases).
We propose that the role of radiotherapy in the management of these tumors should be evaluated systemically as follows:
2. Post-operative radiotherapy be given as primary curative modality to sterilize tumors in those patients with occult GB tumors who refuse a second, more
892 Radiation Oncology ??Biology 0 Physics
radical procedure, and in those patients with known tumor left behind at curative surgery.
3. Post-operative radiotherapy be given after pal- liative or exploratory surgery; or when palliative surgery has failed, to increase the effectiveness of palliation and to increase local control.
4. Radiotherapy be used in patients needing relief
September-October 1977, Volume 2. No. 9 and No. 10
of obstructive jaundice and in whom surgery is re- fused and/or contraindicated.
5. Radiotherapy be used to treat incisional metas- tases.
6. Combination radiotherapy-chemotherapy be used to possibly further augment the gains achieved above.
REFERENCES
1. Ackerman, L.V., de1 Regato, J.A., Cancer, 4th Edn. St.
2. Aldrete, J.S.: Malignant neoplasms of the extra-hepa- Louis, Mosby, 1970, p. 591.
tic bile ducts. Am. Surg. 37: 613-621, 1971. 3. Altemeier, W.A., Gall, E.A., Culbertson, W.R., Inge,
W.W.: Sclerosing Carcinoma of the intrahepatic (hilar) bile ducts. Surgery 60: 191-200, 1966.
4. Appleman, R.M., Morlock, C.G., Dahlin, D., Adson, M.A.: Long term survival in carcinoma of the gall- bladder. Surg. Gynecol. & Obstet. 117: 459464, 1963.
5. Ariel, I.M., Pack, G.T.: The treatment of inoperable cancer of the biliary system with radioactive (I”‘) rose bengal. Am. _I. Roentgenol. 83: 474-490, 1960.
6. Aston, S.J., Longmire, Jr. W.P: Pancreaticoduodenal resection. Arch. Surg. 106: 813-817, 1973.
7. Beall, M.S., Dyer, G.A., Stephenson, H.E.: Disap- pointments in the management of, patients with malignancy of pancreas, duodenum and common bile duct. Arch. Surg. 101: 461-465, 1970.
8. Beltz, W.R., Condon, R.E.: Primary carcinoma of the gallbladder. Ann. Surg. 180: 180-184, 1974.
9. Bivins, B.A., Meeker, Jr., W.R., Weiss, D.L., Griffin, Jr., W.O.: Carcinoma in situ of the gallbladder: a dilemma. South Med. J. 68: 297-300, 1975.
10. Black, W.C., Key, C.R., Carmany, T.B., Herman, D.: Carcinoma of the gallbladder in a population of Southwestern American Indians. Cancer 39: 1267- 1279, 1977.
11. Bockus, H.L. ed., Gastroenterology, 2nd Edn. Philadelphia, Saunders, 1976, Vol. 3, p. 836.
12. Braasch, J.W., Warren, K.W., Kune, G.A.: Malignant neoplasms of the bile Ducts. Surg. Clin. N.A. 47: 627-638, 1%7.
13. Burdette, W.J.: Carcinoma of the gallbladder. Ann. Surg. 145: 832-847, 1957.
14. Case, J.T., Warthin, A.S.: The occurrence of hepatic lesions in patients treated by intensive deep roentgen irradiation. Am. J. Roentgenol. 12: 27-46, 1924.
15. Case Records of the Massachusetts General Hospital (Case 32-1%9). New Engl. J. Med. 281: 314-323, 1969.
16. Case Records of the Massachusetts General Hospital (Case 31-1970). New Eng. J. Med. 283: 191-201, 1970.
17. Case Records of the Massachusetts General Hospital (Case 35-1976). New Engl. J. Med. 295: 492499, 1976.
18. Committee for Radiation Oncology Studies: Radiation Therapy and Surgery. Cancer 37: 2084-2092, 1976.
19. Davis, H.L., Ramirez, G., Ansfield, F.J.: Adenocar- cinemas of stomach, pancreas, liver and biliary tracts. Cancer 33: 193-197, 1974.
20. Den Besten, L., Liechty, R.D.: Cancer of the biliary tree. Am. .I. Surg. 109: 587-589, 1965.
21. Donaldson, L.A., Busuttil, A.: A clinicopathological review of 68 carcinomas of the gallbladder. Br. J. Surg. 62: 26-32, 1975.
22. El-Domeiri, A.A., Brasfield, R.D., O’Quinn, J.L.: Car-
cinoma of the extrahepatic bile ducts. Ann. Surg. 169:
23. Fahim, R.B.: Carcinoma of the gallbladder: Analysis 525-532, 1969.
of an early case. Am. Surg. 30: 276-280, 1964. 24. Fahim, R.B., Ferris, D.O., McDonald , J.R.: Carcinoma
of the gallbladder. Arch. Surg. 86: 334-341, 1963. 25. Fahim, R.B., McDonald, J.R., Richards, J.C., Ferris,
D.0: Carcinoma of the gallbladder: a study of its mode of spread, Ann. Surg. 156: 114-124, 1962.
26. Fletcher, G.H.: Clinical dose-response curves of hu- man malignant epithelial tumors. Br. J. Radiol. 46: 1-12, 1973.
27. Fortner, J.G., Kallum, B.O., Kim, D.K.: Surgical management of carcinoma of the junction of the main hepatic ducts. Ann. Surg. 184: 68-73, 1976.
28. Frank, S.A., Spjut, H.J.: Inapparent carcinoma of the gallbladder. Am. Surg. 33: 367-372, 1967.
29. Friedland, H.M.: Leiomyosarcoma of the gallbaldder. J. Med. Sot. N.J. 68: 205-206, 1971.
30. Glenn, F., Hayes, D.M.: The scope of radical surgery in the treatment of malignant tumors of the extra- hepatic biliary tract. Surg. Gynecol. & Obstet. 99: 529-541, 1954.
31. Green, N., Mikkelsen, W.P., Kernen, J.A.: Cancer of the common hepatic bile ducts-palliative radio- therapy. Radiology 109: 687-689, 1973.
32. Greenspan, E.M: Clinical Cancer Chemotherapy, New York, Raven Press, 1975, p. 187.
33. HafstrSm, L., Zettergren, L., Akesson, L.A.: The natural history of primary and secondary malignant tumors of the Liver-IV. The prognosis for patients with carcinoma of the gallbladder, with special re- ference to the amount of tumor growth within the liver at the time of diagnosis. Acta Chir. Stand. 139: 264-269, 1973.
34. Ham, J.H., Mackenzie, D.C.: Primary carcinoma of the extra-hepatic bile ducts. Surg. Gynecol. 8z Qbstet. 118: 977-983, 1964.
35. Hardy, M.A., Volk, H.: Primary carcinoma of the gallbladder. Am. J. Surg. 120: 800-803, 1970.
36. Hart, J., Modan, B., Hashomer, T.: Factors affecting survival of patients with gallbladder neoplasms. Arch. Intern. Med. 129: 931-934, 1972.
37. Hudgins, P.T., Meoz, R.T.: Radiation therapy for obstructive jaundice secondary to tumor malignancy. Int. J. Radiat. Oncol. Biol. Phys. 1: 1195-1198, 1976.
38. Ingis, D.A., Farmer, R.G.: Adenocarcinoma of the bile ducts. Am. J. Dig. Dis. 20: 253-261, 1975.
39. Johnson, P.M., Grossman, F.M., Atkins, H.L.: Radia- tion induced hepatic injury. Am. J. Roentgenol. 99: 453-462, 1967.
40. Kaplan, 1.1.: Clinical Radiation Therapy, 2nd Edn. New York, Paul B. Hoeber, 1949, p. 495.
41. Keill, R.H., DeWeese, MS.: Primary carcinoma of the gallbladder. Am. J. Surg. 125: 726-729, 1973.
Biliary system radiotherapy 0 G. KOPELSON et al. 893
42. Kirschbaum, J.D., Kozoll, D.D.: Carcinoma of the gallbladder and extralhepatic bile ducts Surg. Gynecol. & Obstet. 73: 740-754, 1941.
43. Klatskin, G.: Adenocarcinoma of the hepatic duct at its bifurcation within the porta hepatis. Am. J. Med. 38: 241-256, 1965.
44. Klein, J.B., Finck, .J.M.: Primary carcinoma of the gallbladder. Arch. Surg. 104: 769-772, 1972.
45. Klippel, A.P., Shaw, R.B.: Carcinoma of the bile duct. Arch. Surg. 104: 102-103, 1972.
46. Krain, L.S.: Gallbladder and extra-hepatic bile duct carcinoma. Geriatrics 27: 11 l-l 17, 1972.
47. Kuwyati, K., Baggenstoss, A.H., Stauffer, M., Priest- ley, J.T.: Carcinoma of the major intra-hepatic and the extra-hepatic bile ducts exclusive of the papilla of vater. Surg. Gynecol. & Obstet. 104: 357-366, 1957.
48. Lam, C.R.: The present status of carcinoma of the gallbladder: a study of thirty-four cases. Ann. Surg. 111: 403-410, 1940.
49. Lippman, H.N., McDonald, L.C., Longmire, Jr. W.P.: Carcinoma of the extra-hepatic bile ducts. Am. Surg. 25: 819-826, 1959.
50. Litwin, M.S.: Primary carcinoma of the gallbladder. Arch. Surg. 95: 236-240, 1967.
51. Longmire, Jr. W.P., McArthur, MS., Bastounis, E.A., Hiatt, J.: Carcinoma of the extra-hepatic biliary tract. Ann. Surg. 178: 333-345. 1973.
52. Moertel, C.G., The IGallbladder. In Cancer Medicine, ed. by Holland, J.F., Frei, III, E. Philadelphia, Lea & Feibenger, 1974, p. l550.
53. Moertel, C.G., Reite:meier, R.J., Advanced Gastroin- testinal Cancer. New York, Harper & Row, 1969, p. 98.
54. Monge, J.J., Rudie, P.S.: Segmental resection of the common hepatic duct for carcinoma. Arch. Surg. 93: 1015-1018, 1966.
55. Moorhead, D.T., Warren, K.W.: Changing patterns of surgery of the gallbladder, bile ducts and liver. Surg. Clin. N.A. 56: 649-666, 1975.
56. Moossa, A.R., Anagnost, M., Hall, A.W., Moraldi, A., Skinner, D.B.: The continuing challenge of gallbladder cancer. Am. J. Surg. 130: 57-62, 1975.
57. Neibling, H.A., Dockerty, M.B., Waugh, J.W.: Car- cinoma of the extra-hepatic bile ducts. Surg. Gynecol. & Obstet. 89: 429-438, 1949.
58. Nevin, J.E., Moran, T.J., Kay, S., King, R.: Carcinoma of the gallbladder. Cancer 37: 141-148, 1976.
59. Orr, K.B.: Carcinoma of the gallbladder 24 years after cholecystostomy. Med. J. Aust. 1: 875, 1971
60. Pack, G.T., Miller, T.R., Brasfield, R.D.: Total right hepatic lobectomy for cancer for the gallbladder. Ann. Surg. 142: 6-16, 1955.
61. Pemberton, L., Beaty, D., Willis, F., Strohl, E.L.: The surgical significance of carcinoma of the gallbladder. Am. J. Surg. 122: 381-383, 1971.
62. Prakash, A.T.M., Sharma, L.K., Pandit, P.N.: Primary carcinoma of the gallbladder. Br. J. Surg. 62: 33-36, 1975.
63. Quattlebaum, J.K., ‘Quattlebaum, Jr. J.K.: Malignant obstruction of the major hepatic ducts. Ann. Surg. 161: 876-889, 1%4.
64. Ragins, H., Diamond, A., Meng, C-H.: Intra-hepatic cholangiojejunostomy in the management of malignant biliary obstruction. Surg. Gynecol. & Obstet. 136: 27- 32, 1973.
65. Ram, M.D.: Carcinoma of the gallbladder. Surg. Gynecol. & Obstet. 132: 1044-1048, 1971.
66. Richard, P.F., Cantin, J.: Primary carinoma of the gallbladder: a study of 108 cases. Can. J. Surg. 19: 27-32, 1976.
67. Robertson, W.A., Carlisle, B.B.: Primary carcinoma of the gallbladder. Am. J. Surg. 113: 738-742, 1967.
68. Ross, A.P., Braasch, J.W., Warren, K.W.: Carcinoma of the proximal bile ducts. Surg. Gynecol. 8z Obstet. 136: 923-928, 1973.
69. Rubin, P., Casarett, G.W., Clinical Radiation Pa- thology. Philadelphia, W.B. Saunders, 1968, p. 288.
70. Sako, K., Seitzinger, G.L., Garside, E.: Carcinoma of the extra-hepatic bile ducts. Surgery 41: 41ti37, 1957.
71. Salmon, P.A.: Carcinoma of the pancreas and extra- hepatic biliary system. Surgery 60: 554-565, 1966.
72. Shani, M., Hart, J., Modan, B.: Cancer of the biliary system: a study of 445 cases. Br. J. Surg. 61: 98-100, 1974.
73. Sleisenger, M.H., Fordtran, J.S., Gastrointestinal Disease. Philadelphia, W.B. Saunders, 1973, p. 1140.
74. Soanes, W.A., Cox, R.S., Maher, J.R.: The effects of roentgen irradiation on adrenal cortical function in man. Am. J. Roentgenol. 85: 133-144, l%l.
75. Soanes, W.A., Dodson, C.C.: The adrenal response to irradiation on patients with testicular tumors. J. Ural. 72: 705-711, 1954.
76. Solan, M.J., Jackson, B.T.: Carcinoma of the gall- bladder. Br. J. Surg. 58: 593-597, 1971.
77. Sommers, S.C., Carter, M.E.: Adrenocortical post- irradiation fibrosis. Arch. Pathol. 99: 421-423, 1975.
78. Spencer, R.P., Knowlton, A.H.: Redistribution of radiocolloid uptake after focal hepatic radiation. On- cology. 32: 266-268, 1975.
79. Stephenson, L.W., Blackstone, E.H., Aldrete, J.S.: Radical resection for periampullary carcinomas. Arch. Surg. 112: 245-249, 1977.
80. Steward, H.L., Liebner, M.M., Morgan, D.R.: Car- cinoma of the extra-hepatic bile ducts. Arch. Surg. 41: 662-713, 1940.
81. Strauch, G.O.: Primary carcinoma of the gallbladder. Surgery. 47: 368-383, 1960.
82. Strohl, E.L., Reed, W.H., Diffenbaugh, W.G., Ander- son, R.E.: Carcinoma of the bile ducts. Arch. Surg. 87: 567-577, 1963.
83. Suit, H.D., Gallager, H.S.: Inact tumor cells in ir- radiated tissue. Arch. Pathol. 78: 648-651, 1964.
84. Sullivan, R.C., Faris, T.D.: Hepaticojejunostomy. Am. J. Surg. 114: 722-725, 1967.
85. Sullivan, R.D., Oberfield, R.A.: Protracted ambulatory infusion cancer chemotherapy of the liver and biliary system. Prog. Liver Dis. 3: 481494, 1970.
85. Tanga, M.R.: Long term survival in gallbladder malignancy. Indian J. Cancer. 8: 61-63, 1971.
87. Tanga, M.R., Ewing, J.B.: Primary malignant tumors of the gallbladder: Report of 43 cases. Surgery. 67: 418-426, 1970.
88. Terblanche, J.: Is carcinoma of the main hepatic duct junction an indication for liver transplantation or pal- liative surgery? A plea for the U tube palliative procedure. Surgery. 79: 127-128, 1976.
89. Terblanche, J., Louw, J.H.: U Tube drainage in the palliative therapy of carcinoma of the main hepatic duct junction. Surg. C/in. N.A. 53: 1245-1256, 1973.
90. Terblanche, J., Saunders, S.J., Louw, J.H.: Prolonged palliation in carcinoma of the main hepatic duct junc- tion. Surgery 71: 720-731, 1972.
91. Thorbjarnarson, B.: Carcinoma of the biliary tree-I.
894 Biliary system radiotherapy 0 G. LOPEISON et al.
Carcinoma of the gallbladder. N. Y.S. Med. J. 75: 550-552, 1975.
92. Thorbjarnarson, B.: Carcinoma of the biliary tree--II. Carcinoma of the bile ducts. N.Y.S. Med. J. 75: 705- 707, 1975.
93. Thorbjarnarson, B.: Carcinoma of the bile ducts. Cancer 12: 708-713, 1959.
94. Thorbjarnarson, B.: Carcinoma of the gallbladder. Cancer 12: 1009-1015, 1959.
95. Tomkins, R.K., Johnson, J., Storm, F.K., Longmire, Jr. W.P.: Operative endoscopy in the management of biliary tract neoplasms. Am. J. Surg. 132: 174-182, 1976.
96. Treadwell, T.A., Hardin, W.J.: Primary carcinoma of the gallbladder. The role of adjunctive therapy in its treatment. Am. J. Surg. 132: 703-706, 1976.
97. Vaittinen, E.: Carcinoma of the cystic duct. Ann. Chir. Gyn. Fenn. 61: 190-194, 1972.
98. Vaittinen, E.: Carcinoma of the gallbladder: A study of 390 cases diagnosed in Finland 1953-1967. Ann. Chir. Gyn. Fenn. 168 (suppl.): 1-81, 1970.
99. Van Heerden, J.A., Judd, E.S., Dockerty, M.B.: Car- cinoma of the extra-hepatic bile ducts. Am. J. Surg. 113: 49-56, 1967.
100. Walters, W., Olson, P.F.: Papillary colloid adenocar- cinema of the extra-hepatic bile ducts. Minn. Med. 18:
460-462, 1935. 101. Warren, K.W., Hardy, K.J., O’Rourke, M.G.E.: Pri-
mary neoplasia of the gallbladder. Surg. Gynecol. & Obstet. 126: 1036-1040, 1968.
102. Warren, K.W., Mountain, J.C., Lloyd-Jones, W.: Malignant tumors of the bile ducts. Br. J. Surg. 59: 501-505, 1972.
103. Warren, S.: Effects of radiation on normal tissues- IV. Effects of radiation on the gastrointestinal tract, including the salivary glands, the liver and the pan- creas. Arch. Pathol. 34: 747-787, 1942.
104. Whelton, M.J., Petrelli, M., George, P., Young, W.B., Sherlock, S.: Carcinoma at the junction of the main hipatic ducts. Quart. J. Med. 38: 211-229, 1%9.
105. White, T.T.: Carcinoma of the hepatic ducts: Review of II cases. Am. Surg. 39: 445-447, 1973.
106. Wilson, S.M., Block, G.E.: Periampullary carcinoma. Arch. Surg. 108: 539-544, 1974.
107. Wolma, F.J., Lynch, J.B.: Papillary carcinoma of the gallbladder. Arch. Surg. 83: 657-660, 1961.
108. Yarborough, D.R.: Primary carcinoma of the extra- hepatic bile ducts. Am. J. Surg. 125: 723-725, 1973.
109. Yarborough, D.R.: Carcinoma of the extra-hepatic biliary tract. J. South Carolina Med. Assoc. 72: 80-83, 1976.