Embed Size (px)
Citation preview

The role of surgery in mRCC
Thomas PowlesBarts Cancer Institute
St Bartholomew’s Hospital London

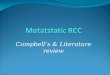
SWOG trial of nephrectomy plus interferon versus interferon alone
20 % of patients who underwent surgery died within the first 4 months !

Surgery in metastatic disease has significant complications
Multi-Institutional retrospective analysis of 141 patients after CN
Systemic therapy 70% (98/141)
No Systemic therapy 31% (43/141)
– Rapid PD 30% (13/43)– Decision for surveillance 21% (9/43)– Patient refusal 23% (10/43)– Perioperative death 19% (8/43)– Unknown reasons 7% (3/43)
Kutikov et al, 2010.
15 % do either progress rapidly or die after surgery

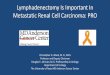
CN: IMT Planned CN: Targeted Therapy
Metastatic Burden Metastatic Burden
Symptomatic Primary Limited Extensive Limited Extensive
Good Risk Yes
No
Poor Risk Yes
No
AppropriateAppropriateAppropriateAppropriate
UncertainUncertain
UncertainUncertainUncertainUncertain
InappropriateInappropriate
RAND Appropriateness Panel on cytoreductive nephrectomy
RAND = Research and Development; IMT = immunotherapy.Halbert et al, 2006.

Association of percentage of tumour burden removed with nephrectomy and PFS in
patients with mRCC treated with targeted therapy
n=46
Barbastefano et al., BJUI 106:1266-1269, 2010

Complete remission with TKI in RCC only reported in those with previous
nephrectomy
n=64 with previous nephrectomy in all cases
61 % in CR after median FUP of 255d 48 % in CR after median FUP of 322d
Albiges et al., JCO 2012

Surgery for isolated brain metastasis with isolated PD?
Whole brain RTSystemic therapy

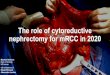
CN in mRCC patients treated with VEGF-targeted therapy
(n = 314 patients; n = 201 with CN vs. n = 113 without CN)
Prior to sunitinib After 2 cycles of sunitinib
Kaplan-Meier curve of OS from initiation of VEGF targeted therapy by CN, and KPS 80 or > (A) or KPS < 80 (B)
VEGF = vascular endothelial growth factor; KPS = Karnofsky performance status.Choueiri et al, 2011.

Better survival in patients with mRCC after nephrectomy: A population based study in
the Netherlands
RCC = renal cell carcinoma.Aben KK et al., Eur J Cancer 2011
N=328 patients, 37.5 % underwent nephrectomy; after adjustment for prognostic factors nephrectomy remained significantly associated with better survival (hazard ratio: 0.52, 95% CI: 0.37-0.73)

Why should there be a survival benefit by removal of the primary tumor ?
-VEGF, PDGF, FGF, TGF-β-Inhibitory molecules CTLA-4, B7-H1 (PD-L1),B7-H3, B7-H4-intratumoral regulatory T-cells-MDSC-anaerobic metabolism of hypoxia (Cori-cycle) and cachexia
-VEGF, PDGF, FGF, TGF-β-Inhibitory molecules CTLA-4, B7-H1 (PD-L1),B7-H3, B7-H4-intratumoral regulatory T-cells-MDSC, STAT 3 and 5 crosstalk-anaerobic metabolism of hypoxia (Cori-cycle) and cachexia
Gajewski et al., Immunol Rev 213:131-145, 2006Thompson et al., Cancer Res 66:3381-85, 2006Krambeck et al., PNAS 103:10391-96, 2006Finke et al., Clin Canc Res 14:6674-82, 2008Ko et al., Cancer Res 70:3526-36, 2010Griffioen et al., Thromb Haemost 101:1025-31, 2009Lindenberg et al., Immunother 3:77-96, 2011Dosquet et al., Clin Canc Res 3:2451-58, 1997Jacobsen et al., J Urol 163:343-47, 2000
The influence of microenvironment

4 weeks 4 weeks 4 weeks2 weeks
2 weeks
At least2 weeks
2 weeks
biopsysurgery
Interval nephrectomy as an alternative to upfront nephrectomy in mRCC

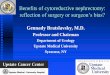
Effect of sunitinib on primary tumour.

Prior to Sunitinib After 2 Cycles of Sunitinib
SD = stable disease; PR = partial response.Thomas, Rini, Lane, et al, 2009; Powles et al, 2011, Abel et al.2011
Progression of primary tumor during TKI treatment
Retrospective study (n = 19) to downsize primary tumor– Local primary tumor progression (RECIST); n = 9 (47%)
Presurgical phase II trial (n = 22) – n = 2; local progression with SD and PR at metastatic sites
Retrospective analysis of 168 tumors: increase >10%In +/- 5 %

Surgical complications associated with up front sunitinib therapy

Surgical complications associated with up front sunitinib therapy

Arguments in Favor of Nephrectomy
Palliate local symptoms
Primary tumor has not responded to systemic therapy and progresses
Long interval between progression and death with potential progression of the primary tumor if left in situ
Possibility of CR more likely in combination with nephrectomy
Benefit of pivotal phase III trials of targeted agents largely demonstrated in nephrectomised patients
Adequate histology can be obtained
Removal of the source of metastases, growth factors, cytokines, etc…
Combined analysis of 66 patients with clear cell mRCC treated with presurgical sunitinib in 2 independent phase II trials
Combined analysis of 66 patients with clear cell mRCC treated with presurgical sunitinib in 2 independent phase II trials
Powles et al, European Urology 2011

Delayed nephrectomy in RCC
Advantages• Starts systemic
therapy quickly• Select out patients
with primary refractory disease
• Down staging of primary tumour
Disadvantages• More complex surgery• Increased tumour bulk
may inhibit response to therapy
• Period off therapy for surgery may result in tumour rebound

Tumour heterogeneity in terms of protein expression hampering
biomarker research.
Stewart et al GU ASCO 2012

Choice between sunitinib and pazopanib in the UK
• 2 pivotal trials will direct us.
Single institution audit of 78 patients
%

PANTHER: Upfront pazopanib followed by nephrectomy in
metastatic disease.

Phase III nephrectomy trials in mRCC

Cytoreductive nephrectomy in metastatic disease
• There is a lack of randomised surgical data in the TKI era
• The retrospective data remains compelling especially those with low volume metastatic disease and MSKCC good risk disease.
• Targeted therapy prior to nephrectomy appears attractive in selected individuals although the reduction in the size of the primary tumour appears modest.