Embed Size (px)
Citation preview
The Role of the Cytology Laboratory
Irene Samphier
Cytology Department
Pathology
East Surrey Hospital
Liquid Based Cytology
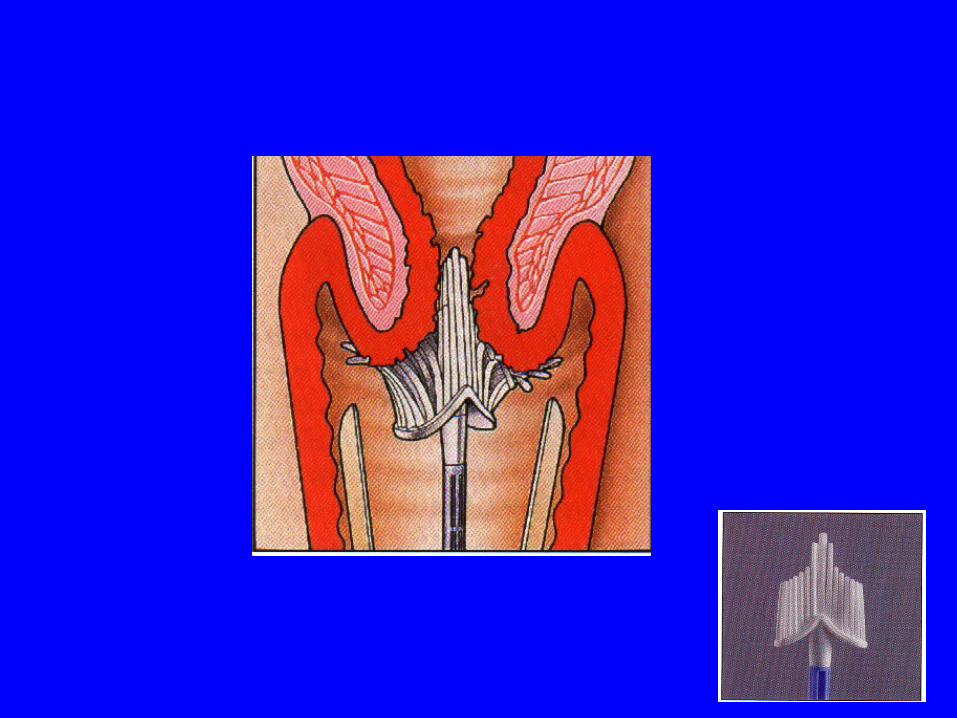
• Randomised cells presented as a thin layer preparation on slide
• Cells collected with plastic broom• Transported in liquid medium• Smaller area to screen• Better cell preservation• ThinPrep and SurePath
Beware the difference
• Different technologies have slightly different requirements (brush head in or out)
• If you move areas, check technology being used
• Will need a short conversion course if move to a Surepath area
• PIN number from this training valid for all of Kent, Surrey, Sussex
Advantages of LBC
• Almost mono-layer of cells, therefore each cell is easy to view
• Cells are well preserved
• Facilitates 14 day turnaround
• Subsequent HPV typing possible

HPV testing
• Not available on NHS yet, being introduced by March 2012
1) Testing as a low grade cytology triage test
at initial diagnosis stage
2) Test of cure: negative cytology, negative HPV test, routine recall.
14 DAY Turnaround time
• 14 day turnaround from sample taking to the lady receiving her result
• Every aspect of the cervical screening has to play its part to achieve this vital sign
• Target is 98% 14 day TAT including time for HPV testing
PreservCyt fluid
• Methanol based collection fluid –
health and safety considerations (toxic – keep out of reach)
Wash splashes off the skin thoroughly with soap and water
Eye contact: Irrigate thoroughly for at least 10 mins. If discomfort persists seek medical attention.
Use by date on pot
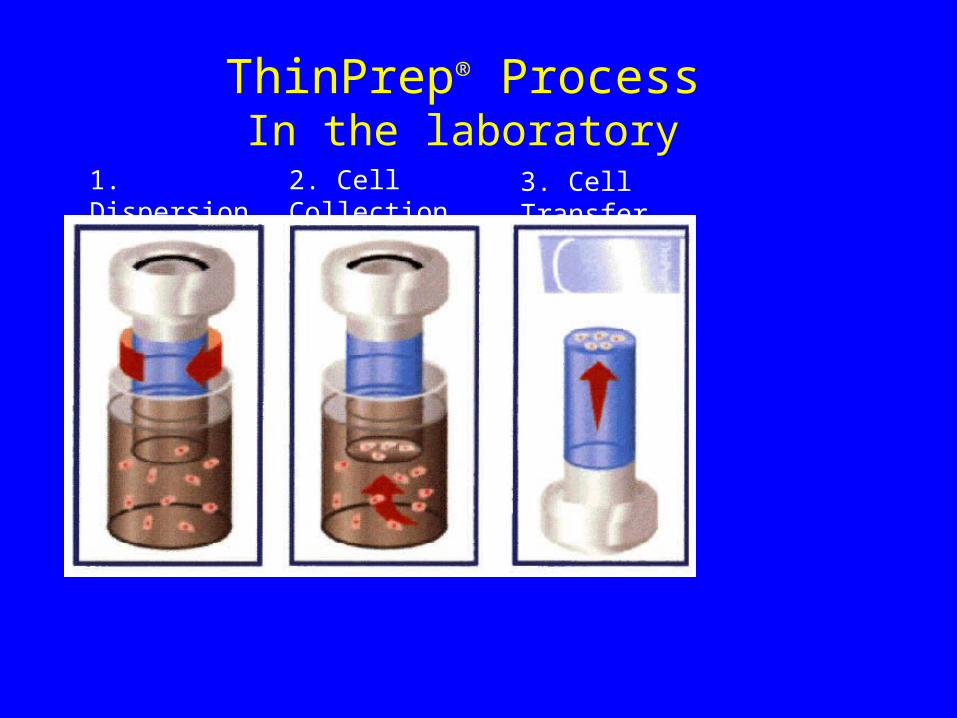
ThinPrep® ProcessIn the laboratory
1. Dispersion 2. Cell Collection 3. Cell Transfer

Liquid Based Cytology
• THINPREP™
T3000 main processor
• Processes up to 60,000 specimens per year• Automated process• Racks of 80 vials take approx 2 hours to
process.• Vials are bar coded• T3000 reads each barcode and transfers the
information to an LBC slide for that specimen
ThinPrep® 3000 Processor
Staining and Coverslipping
Papanicolaou stain
• Originator of the cervical smear
• Stain designed to be gentle on the eye and be able to see through layers of cells to the cells below
• Nuclear stain: Haematoxylin
• Cytoplasmic stains (Papanicolaou stains): EA50 and OG 6
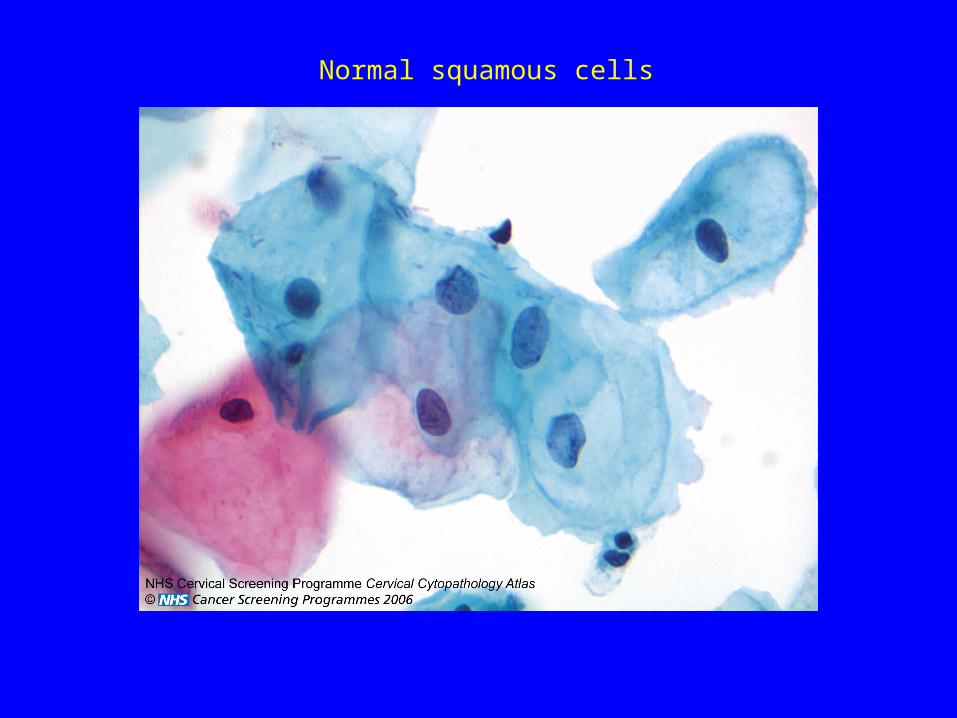
Normal squamous cells
Coverslipping• Slides are stained and then to protect the
cells, a very thin glass coverslip is placed over them
• Stuck in place with mountant with same refractive index as glass
• Therefore down microscope all you see are the cells
• Slides are stored for 10 years for audit
Processing chain
• Samples and request forms checked and verified and then bar coded at original Laboratory
• Racks of vials sent to HUB each day for processing and staining
• The prepared LBC slides (and vials) next day• Original Laboratory screen and report the
specimens
Interpretation of reports
• The report will have the cytological pattern eg negative, mild dyskaryosis etc
• The report will be graded as the highest abnormality seen
• A specimen will not be called inadequate (even if very few cells present or technically inadequate) if any abnormal cells are seen.
Mild, Moderate, Severe Dyskaryosis.
• Cytological grading used to predict underlying histology.
• Mild dyskaryosis predicts CIN I
• Moderate dyskaryosis predicts CIN II
• Severe dyskaryosis predicts CIN III
• Borderline change – uncertain significance
• The report should also have a management recommendation
eg normal recall, repeat in x months,
gynaecological referral etc
• This laboratory operates direct referral for colposcopy for GP and community clinic samples– the result should be stamped to say this has happened if require.
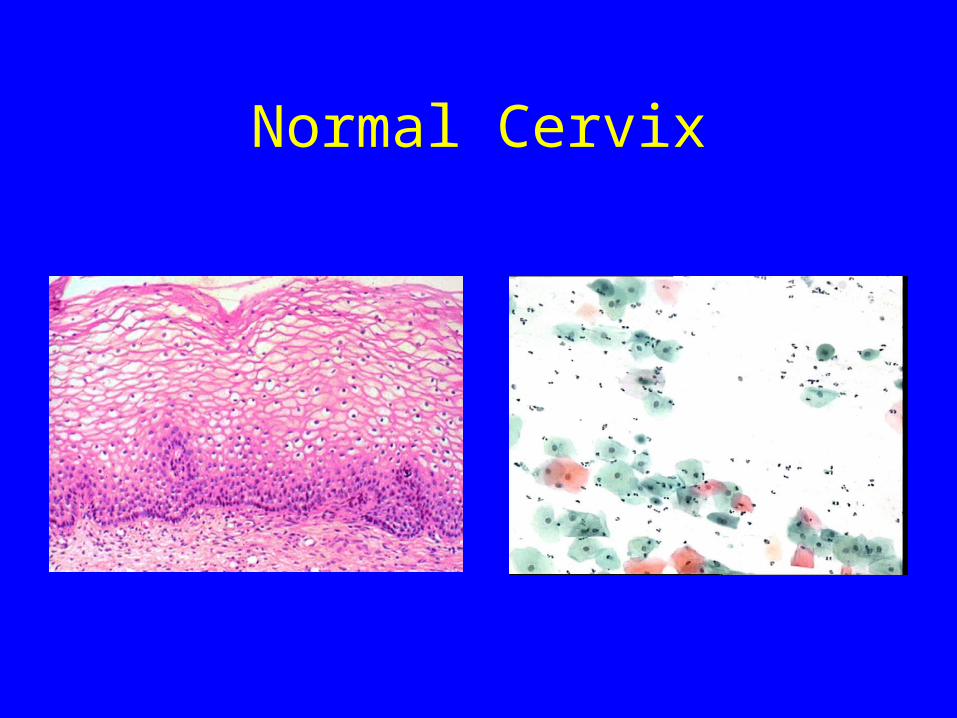
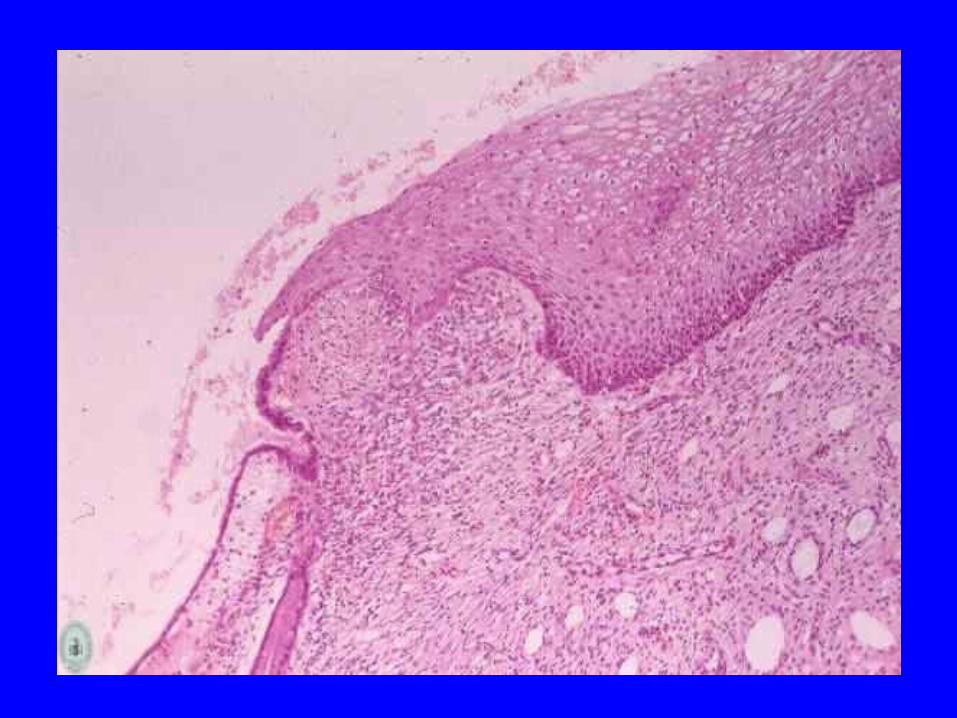
Normal Cervix
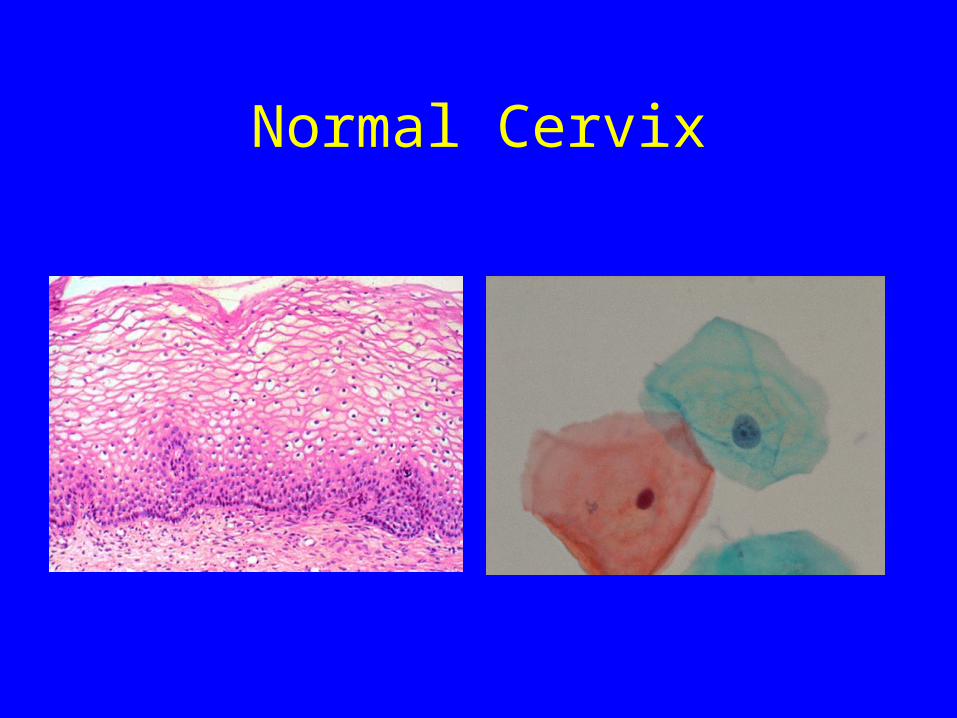
Normal Cervix
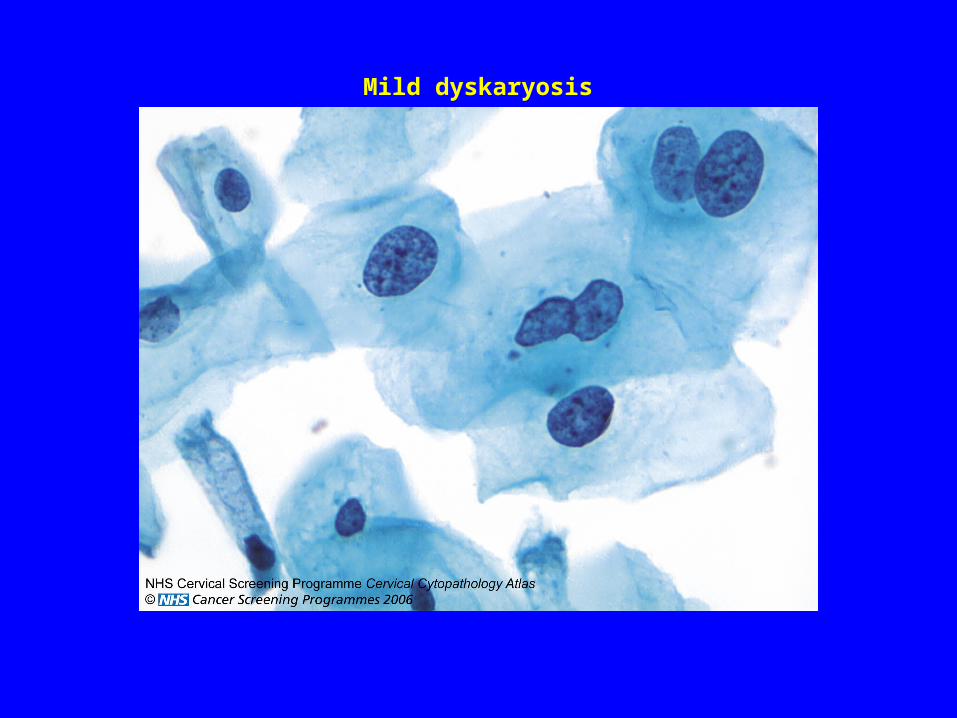
Mild dyskaryosis
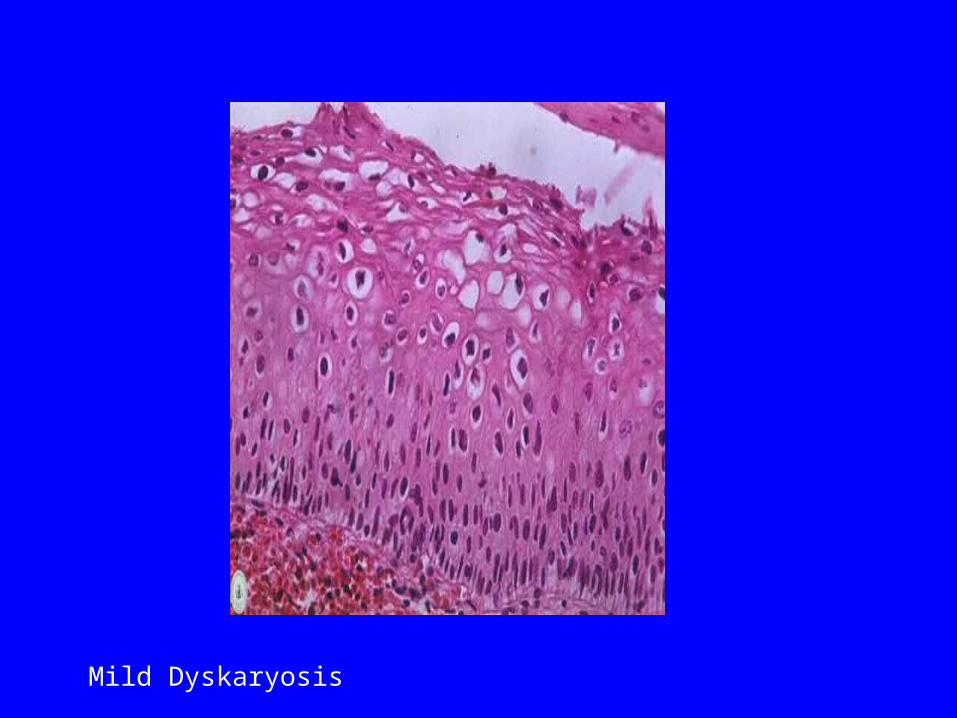
Mild Dyskaryosis
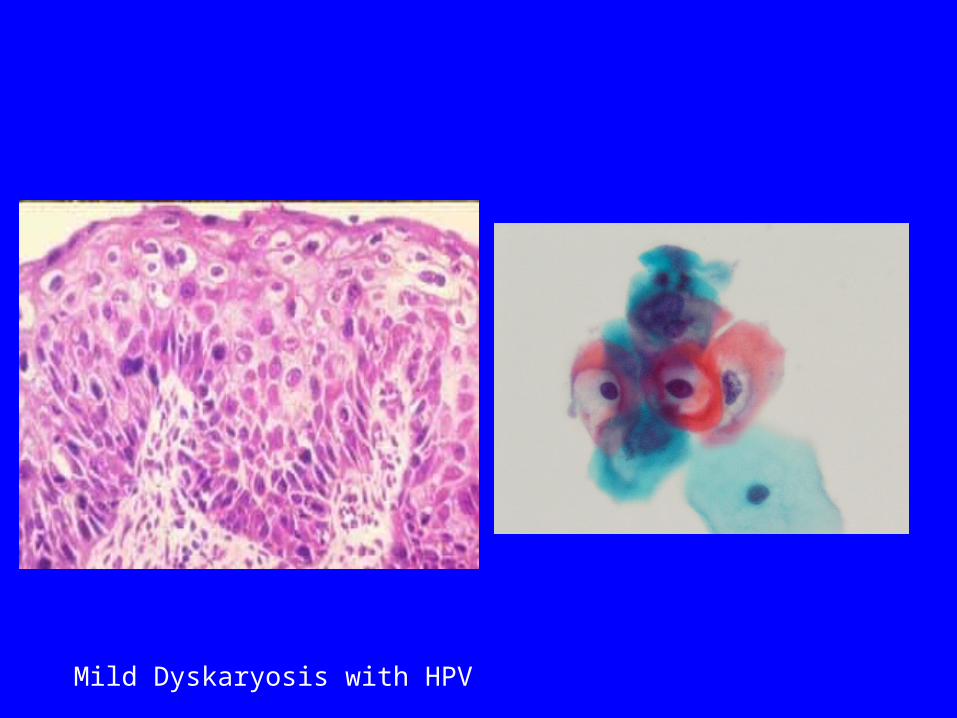
Mild Dyskaryosis with HPV
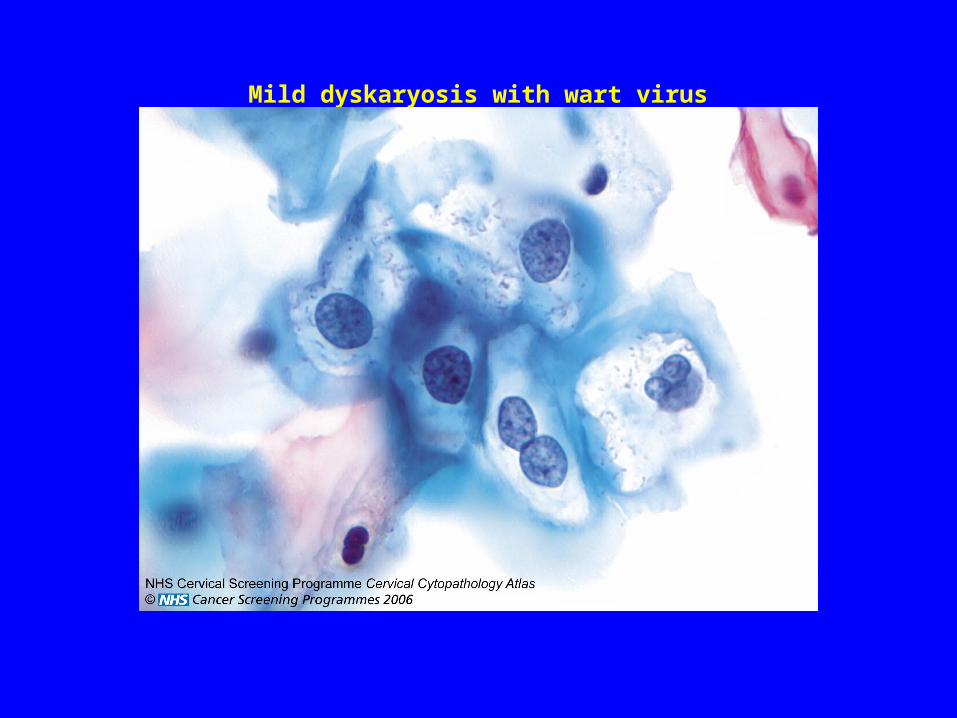
Mild dyskaryosis with wart virus
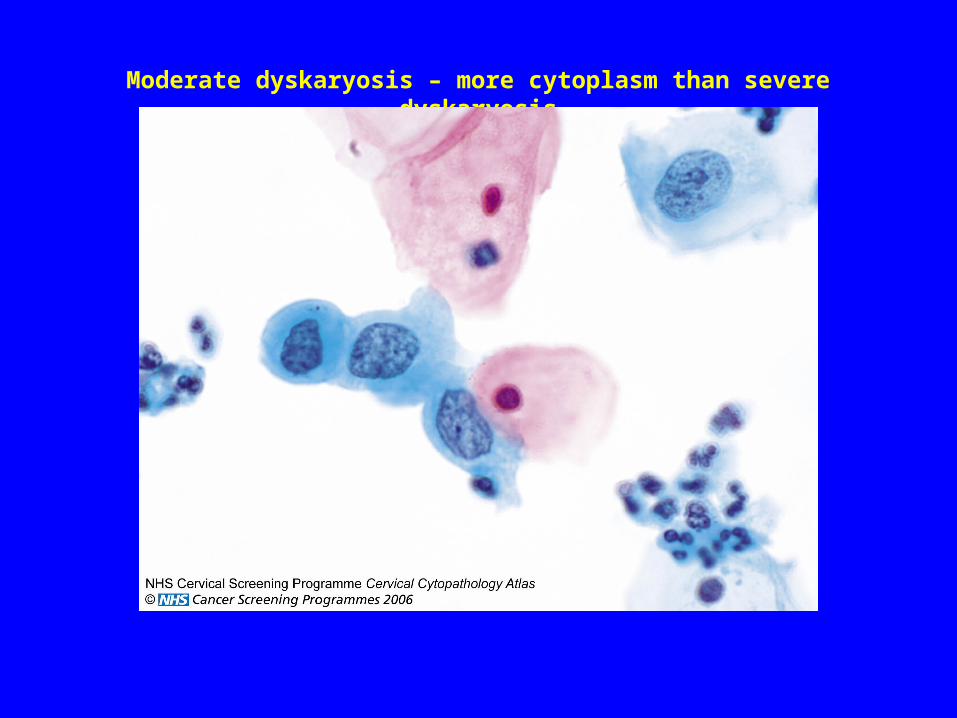
Moderate dyskaryosis – more cytoplasm than severe dyskaryosis
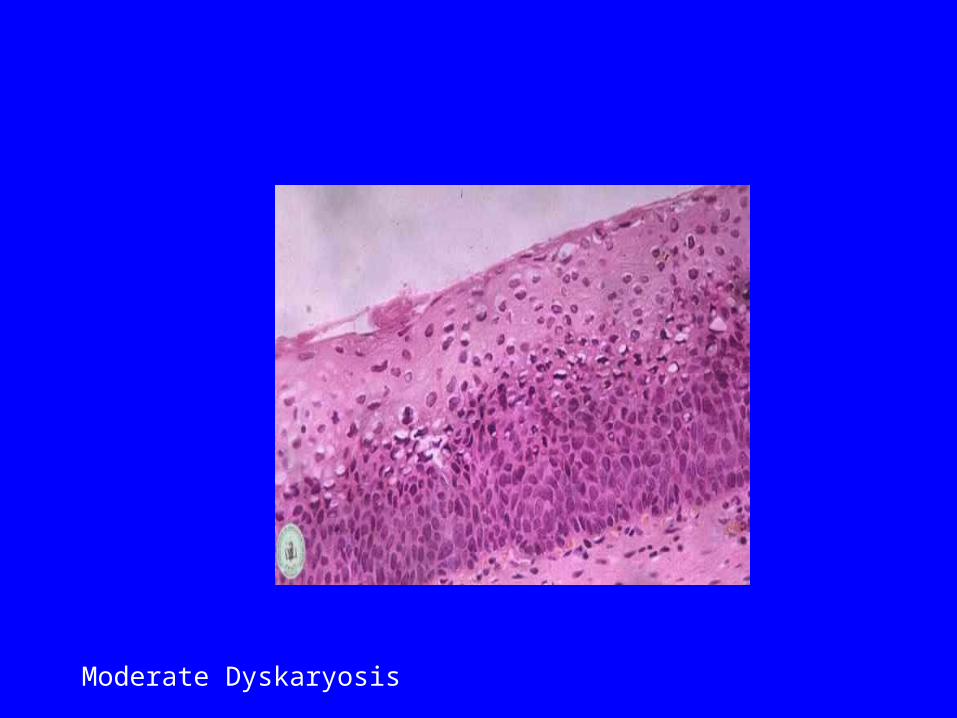
Moderate Dyskaryosis
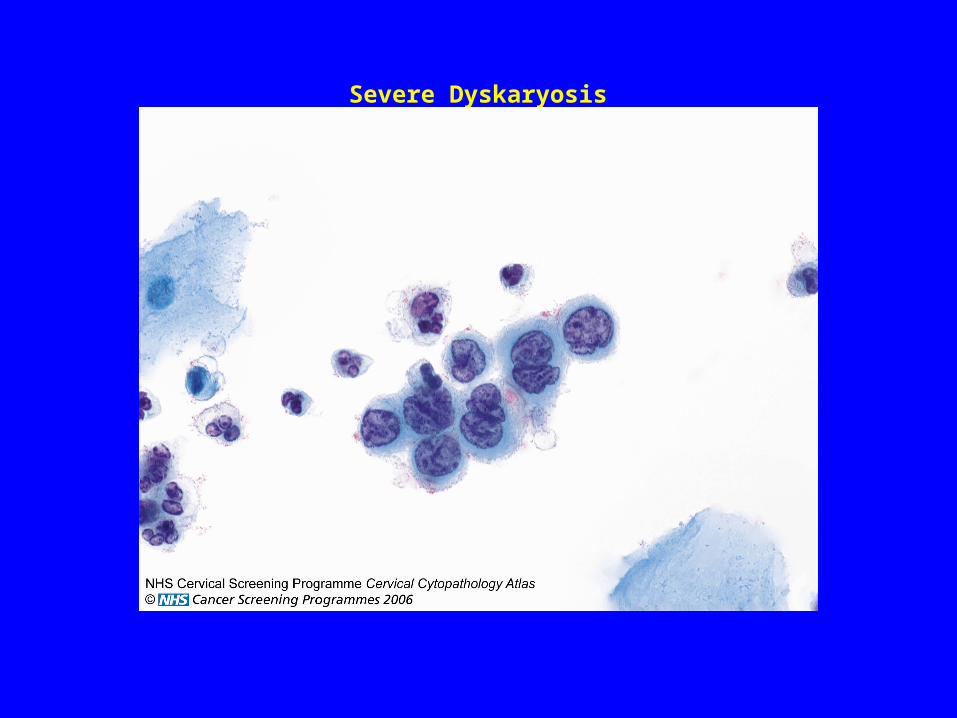
Severe Dyskaryosis
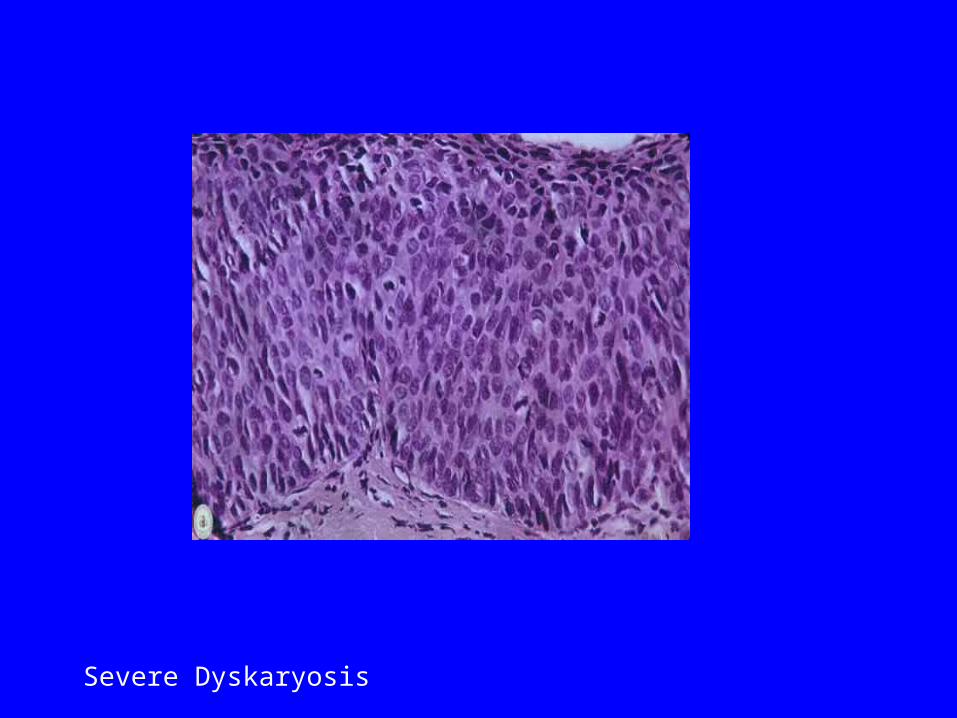
Severe Dyskaryosis
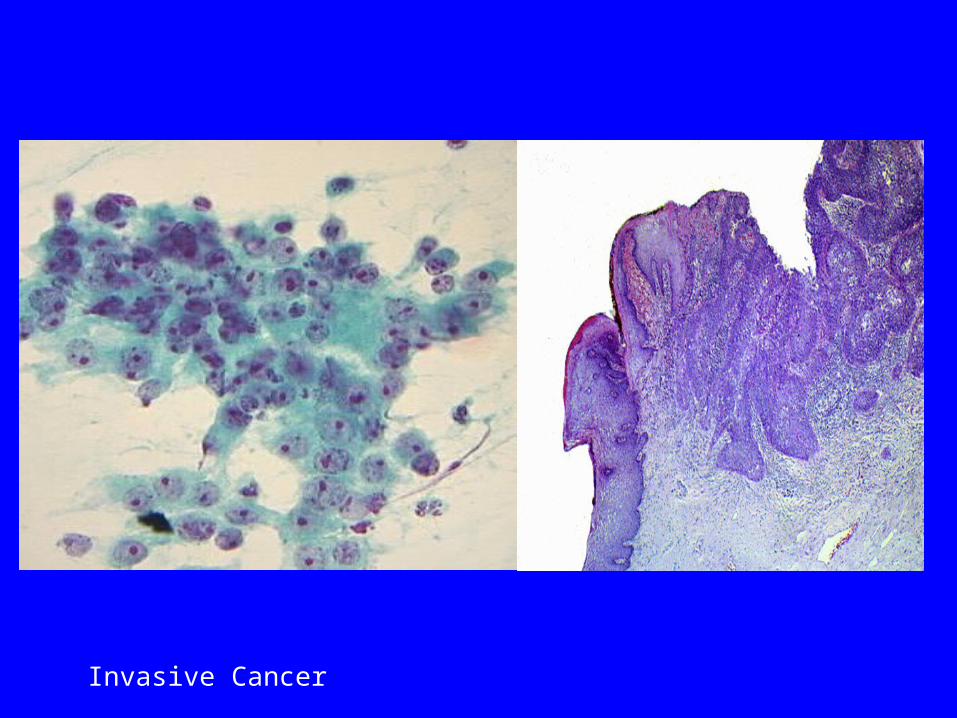
Invasive Cancer
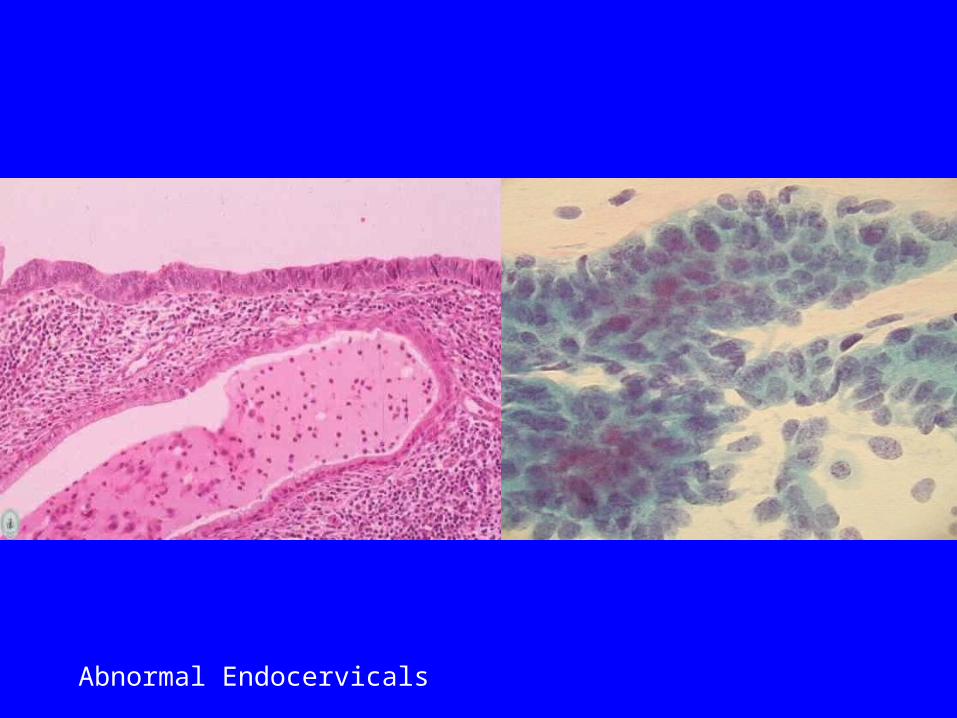
Abnormal Endocervicals
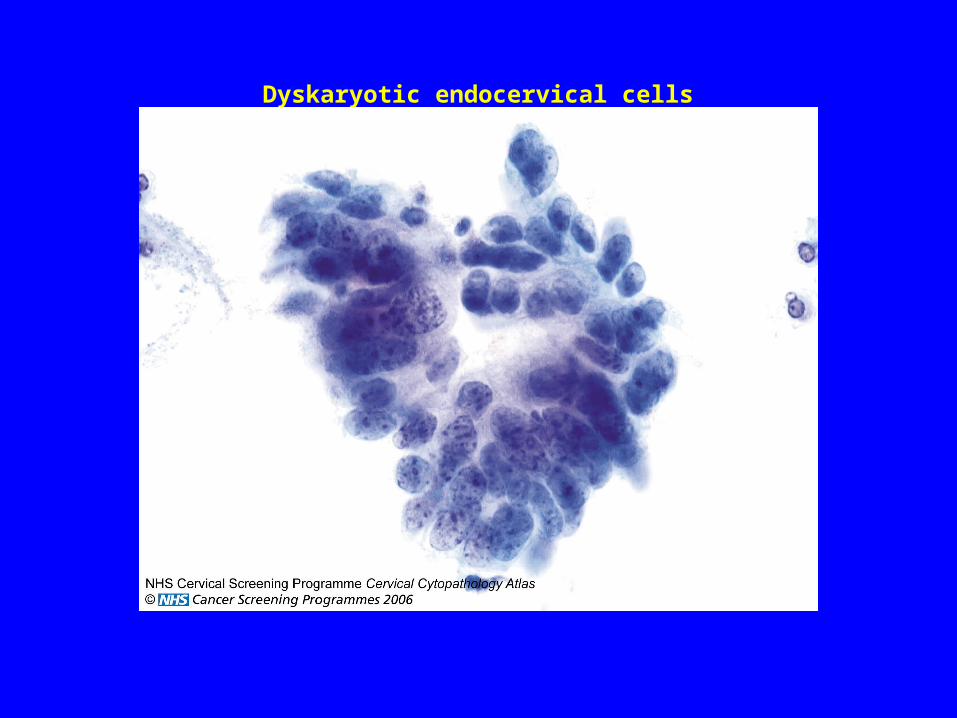
Dyskaryotic endocervical cells
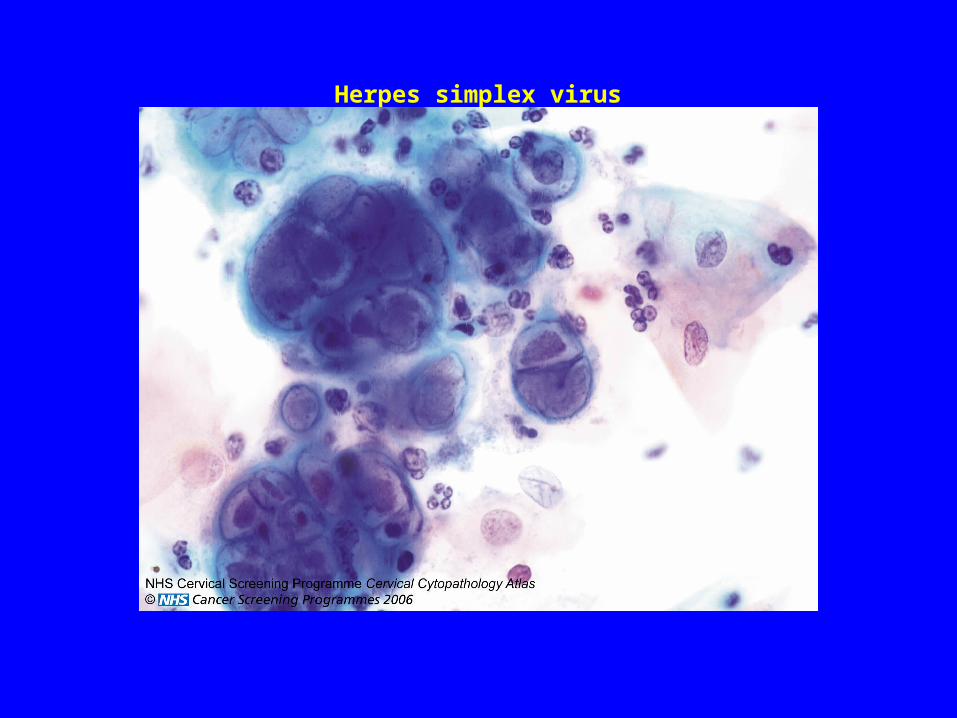
Herpes simplex virus
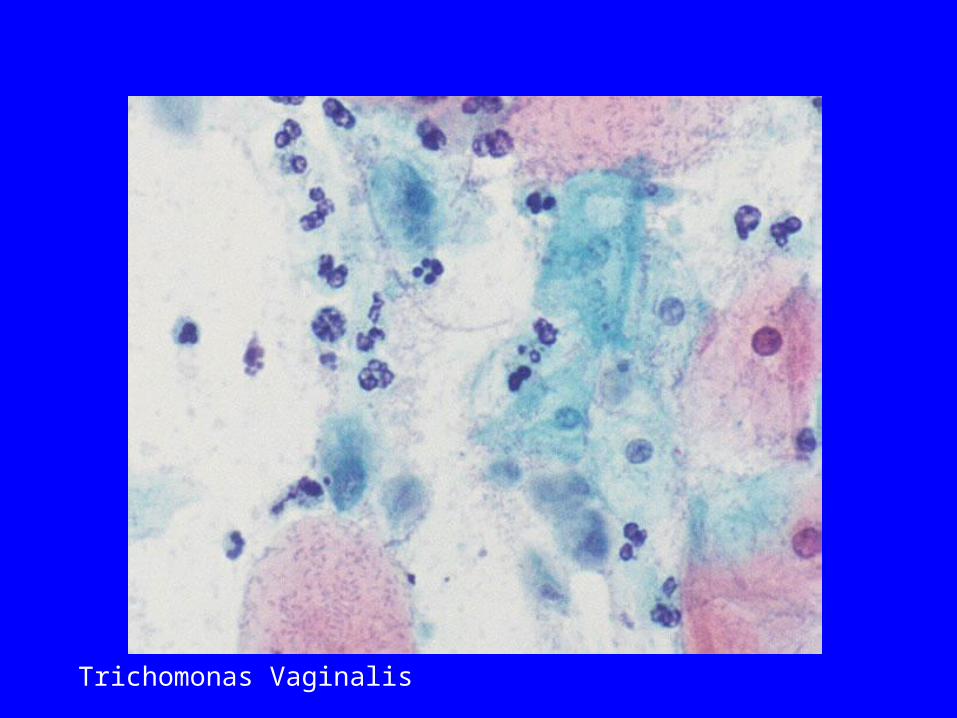
Trichomonas Vaginalis
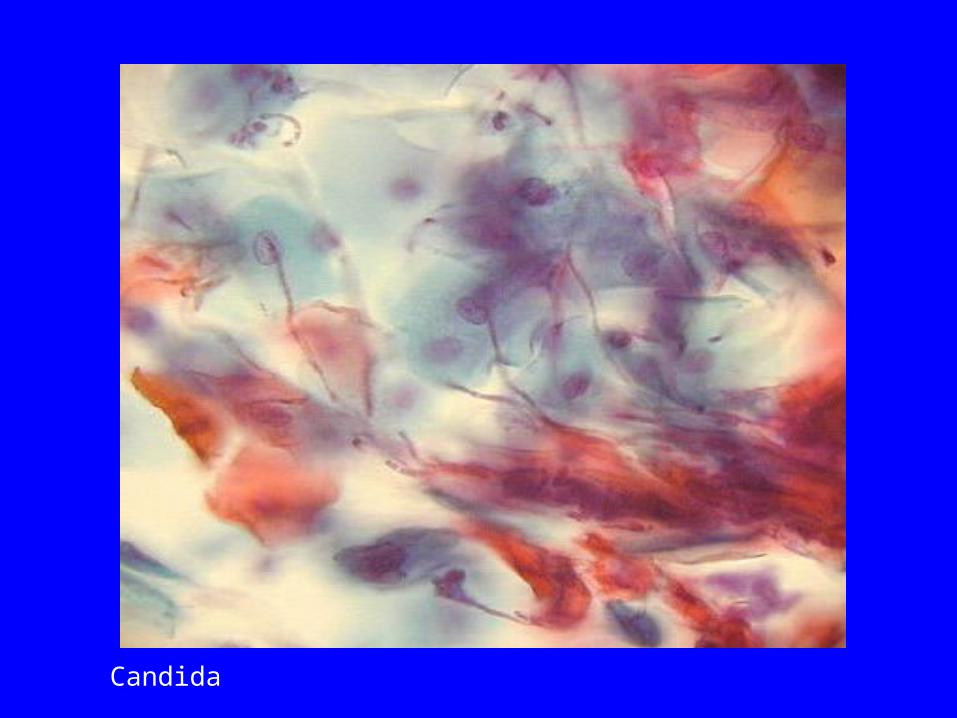
Candida
Inadequate samples due to cellularity
• Heavily blood stained
• Contamination with lubricant
• Insufficient cells present
• Cells obscured by polymorphs
• No endocervical cells when following up endocervical lesions
• Thin prep can cope with a small amount of blood, but large quantities make the specimens inadequate
• Before we report a specimen as inadequate due to blood we will have reprocessed it to remove some of the blood
Inadequate samples due to paperwork/technical:
• Unlabelled vial
• Incorrectly labelled/partially incorrect
• Sample taken more than 6 weeks prior to receipt in lab
• Leaked so insufficient specimen for processing
• No PIN number/not recognised
• Look easy?
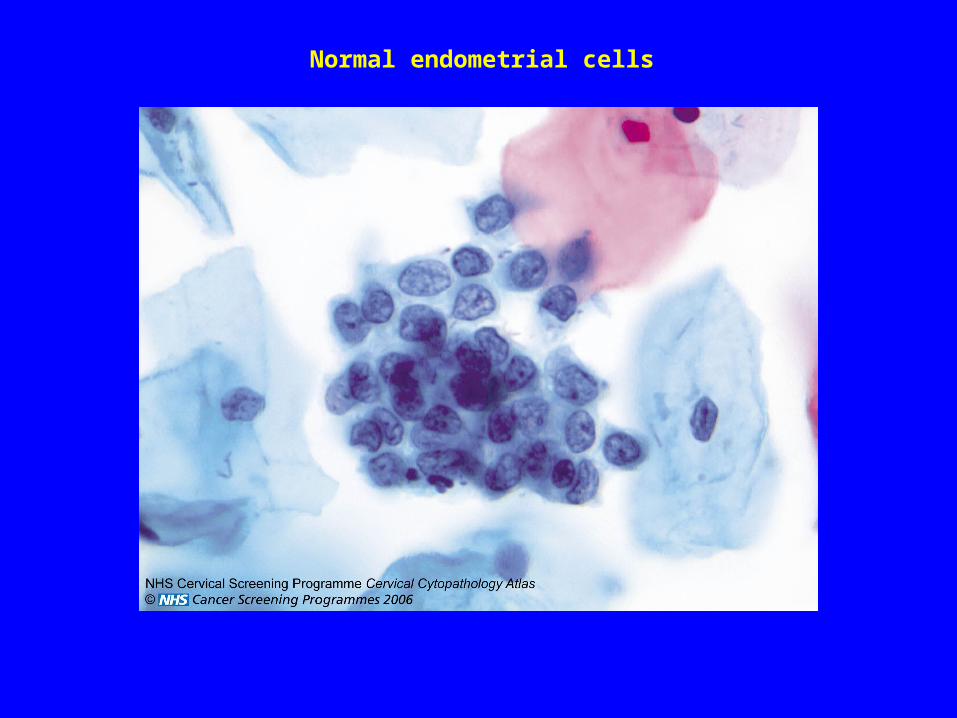
Normal endometrial cells
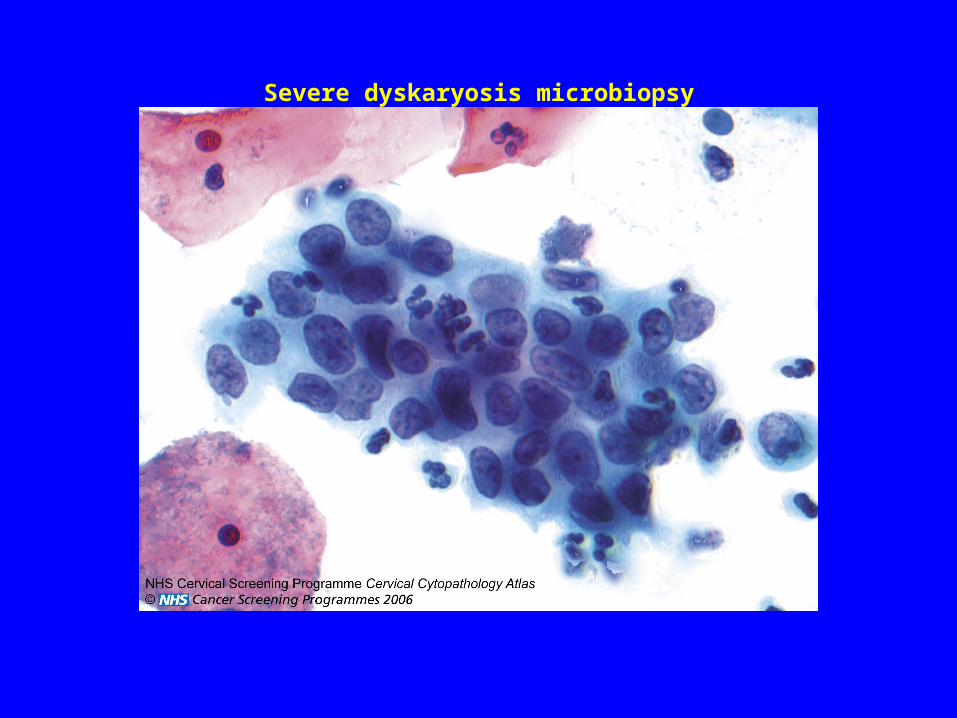
Severe dyskaryosis microbiopsy
Quality assurance in the laboratory
• Each person reporting cervical samples (Screeners and Pathologists) participates in an interpretive EQA
• Quarterly statistics are performed on all the screeners work to ensure that they are competent
• Have to be within national detection rates - Especially important for the high grade dyskaryosis 0.8- 1.4%•
• KC61 Department of Health statistics –published every
autumn
• Clinical Pathology Accreditation (CPA)
• QARC visits