Embed Size (px)
Citation preview

1
Provided by Integrity Continuing Education, Inc.Supported by an educational grant from Sanofi Genzyme and Regeneron Pharmaceuticals.
The Role of the Physician Assistant in Achieving Optimal Outcomes in Moderate to Severe
Atopic Dermatitis

2
Faculty and Affiliation
Anthony J. Mancini, MD, FAAP, FAADHead, Division of Dermatology
Ann & Robert H. Lurie Children’s Hospital of Chicago Professor of Pediatrics and Dermatology
Northwestern University Feinberg School of MedicineChicago, Illinois

3
Faculty Disclosures
Anthony J. Mancini, MD, FAAP, FAAD
Consulting Fees:Pfizer Pharmaceuticals

4
Learning Objectives
Utilize updated criteria and guidelines to accurately diagnose atopic dermatitis (AD)
Assess and document disease severity in individual patients
Review updated guidelines and evaluate available clinical data for therapies utilized in the treatment of AD
Describe indications for specialist referral of patients with AD and review best practices for co-management of moderate to severe disease with specialist physicians

5
Burden of AD and Unmet Needs

6
Prevalence of AD
AD in almost 32 million
Affects ~31.9 million in the US1
– 11%–20% of children2
– 7% of adults1,3
• 29% with moderate disease; 11% with severe disease3
AD often the first sign of long-term disease continuum4
– 60% eventually develop asthma or allergic rhinitis
– 30% develop food allergies
1 in 4 adults with AD report adult onset5
– 30% of childhood cases persist into adult years6
1. Silverberg JI. Dermatol Clin. 2017;35:283-289. 2. Shaw TE, et al. J Invest Dermatol. 2011;131:67-73. 3. Chiesa Fuxench ZC, et al. J Invest Dermatol. 2019;139:583-590. 4. NIH Genetics Home Reference. Atopic dermatitis. https://ghr.nlm.nih.gov/condition/atopic-dermatitis. 5. Lee HH, et al. J Am Acad Dermatol. 2019;80:1526-1532. 6. Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018;120:10-22.

7
AD: Psychosocial/Health-Related Burden
HRQOL, health-related quality of life; QOL, quality of life.
1. Simpson EL. J Am Acad Dermatol. 2016;74:491-498. 2. Silverberg JI, et al. Ann Allergy Asthma Immunol. 2018;121:340-347. 3. Drucker AM. J Invest Dermatol. 2017;137:26-30. 4. Paller A, et al. Am J Clin Dermatol. 2018;19:821-838. 5. Patel KR, et al. J Am Acad Dermatol.2019;80:402-410. 6. Chang Y-S, Chiang B-L. Int J Mol Sci. 2016;174:462. 7. Simpson EL, et al. J Am Acad Dermatol. 2016;74:491-498. 8. Mollanazar NK, et al. Clin Rev Allergy Immunol. 2016;51:263-292.
Detrimental to QOL1-4
Heavy psychosocial impact– Due to stigma, embarrassment, isolation, unpredictability
of flares Associated with anxiety, depression, and suicidal ideation5
Negative impact on academic and job-related performance
Negative effect on sleep (mostly due to pruritus)6-8
87% experience itching daily Itching lasts ≥18 hours in ~42% of patients Leads to excessive daytime sleepiness, fatigue, and
reduced HRQOL

8
AD: Psychosocial/Health-Related Burden (cont.)
1. Ong PY. Immunol Allergy Clin North Am. 2017;37:75-93. 2. Drucker AM, et al. J Invest Derm. 2017;137:26-30. 3. National Eczema Association 2016 Caregiver Survey. https://nationaleczema.org/in-your-words-survey-series/. 4. Zuberbier T. J Allergy Clin Immunol. 2006;118:226-232. 5. Ricci G, et al. J Pediatr Health Care. 2006;20:311-315.
Infection Increased risk of cutaneous and systemic
infections contribute to overuse of antibiotics1
Heavy care/financial burden for parents, caregivers2
Interrupted sleep >3×/week due to AD3
Patients average 9 flares/year, each lasting ~15 days4
Out-of-pocket expenses for families estimated to total ~10% of annual income5
AD superinfected with toxin-secreting S. aureus
Photo courtesy of Mark Boguniewicz, MD

9
More Than Skin Deep: AD Comorbidities
Atopic
Allergic rhinitis
Asthma
Conjunctivitis
Food allergies
Eosinophilic esophagitis
Nonatopic
Cardiometabolic– Obesity– Diabetes– Hypertension
Autoimmune disease Neuropsychiatric
– ADHD– Anxiety– Depression
“Atopic march” concept says that for many, AD will start early and develop into extracutaneous nonatopic comorbidities
More recent understanding is that more-severe skin disease will manifest in a higher burden of multiple atopic and nonatopic comorbidities
Brunner PM, et al. J Invest Dermatol. 2017;137:18-25. Davidson WF, et al. J Allergy Clin Immunol. 2019;143:894-913. Paller A, et al. J Allergy Clin Immunol. 2019;143:46-55. Silverberg JI, et al. Ann Allergy Asthma Immunol. 201;121:604-612.
ADHD, attention deficit hyperactivity disorder.

10
Unmet Needs in AD
Effective treatments that relieve symptoms
and improve long-term outcomes
Reliable biomarkers to guide treatment selection
Consistent guideline implementation
Effective strategies to ensure/encourage
medication adherence
Leung DYM. J Allergy Clin Immunol. 2017;139(4)(suppl):S47-S48. Patel N, Feldman SR. Adv Exp Med Biol. 2017;1027:139-159. Silverberg JI. Allergy Asthma Proc. 2017;38:243-249.

11
Diagnosis, Severity Assessment & Available Guidelines

12
Diagnostic Criteria for AD from the AAD
AD currently diagnosed based on history and clinical presentation (biomarkers not yet specific enough to confirm diagnosis or assess severity)
Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018;120:10-22. Eichenfield LF, et al. J Allergy Clin Immunol. 2017;139:S49-S57. Eichenfield LF, et al. J Am Acad Dermatol. 2014;70:338-351.
Essential (must be present)
• Pruritus• Eczema (acute, subacute,
chronic)• Morphology: typical or
atypical?• Age-specific patterns:
– Infants and children: facial, neck, extensor involvement
– Any age: current or previous flexural lesions; sparing of groin and axillary regions
• History: chronic or relapsing
Important(supports diagnosis)
• Early age of onset• Atopy• Personal and/or
family history• IgE reactivity• Xerosis
Differential/Exclusion Diagnoses
(alternate or concomitant)• Seborrheic dermatitis• Contact dermatitis
(allergic or irritant)• Scabies• Immunodeficiencies• Ichthyoses• Psoriasis• Photosensitivity dermatoses• Cutaneous T-cell lymphoma• Erythroderma of other causes
AAD, American Academy of Dermatology; IgE, immunoglobin E.

13
Other Diseases Can Look Like AD
Contact Dermatitis (both photos) Scabies
AD
Photos courtesy of Sheila F. Friedlander, MD.

14
Clinical Features in Darker Skin Types
Erythema may be difficult to see
Follicular accentuation
Hypopigmentation
Grayish-white skin discoloration (“ashy skin”)
Siegfried EC, et al. J Clin Med. 2015;4:884-917.

15
Distribution Patterns Vary with Age
InfantsForehead, cheeks,
and chin; trunk (except diaper area);
extensor surfaces
Young ChildrenFace, neck, antecubital/popliteal
fossae, wrists, ankles
Adolescents/AdultsPeriorbital area, neck, extensor
surfaces, antecubital/popliteal fossae, wrists, hands, ankles, feet
Simpson EL, et al. Semin Cutan Med Surg. 2016;35:S84-S88.

16
Guidelines
1. Schneider L, et al. J Allergy Clin Immunol. 2013;131:295-299. 2. Eichenfield LF, et al. Pediatrics. 2015;136:554-565. 3. Eichenfield LF, et al. J Am Acad Dermatol. 2014;70:338-351. 4. Eichenfield LF, et al. J Am Acad Dermatol. 2014;71:116-132. 5. Sidbury R, et al. J Am Acad Dermatol. 2014;71:327-349. 6. Sidbury R, et al. J Am Acad Dermatol. 2014;71:1218-1233. 7. Eichenfield LF, et al. J Allergy Clin Immunol. 2017;139:S49-S57.
Guidelines for assessing and treating AD come from divergent clinical perspectives
AAAAI, American Academy of Allergy, Asthma, and Immunology; ACAAI, American College of Allergy, Asthma, and Immunology; PCPs, primary care providers.
2013
2014
2015
2017

17
“Yardstick” Guidelines Published in 2018*
Developed to merge and reconcile differing recommendations from multidisciplinary specialist guidelines
Incorporates many of the recommendations from the 4-part AAD guidelines
Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018;120:10-22.
*Yardstick guidelines available as open-access PDF at https://www.annallergy.org/article/S1081-1206(17)31260-7/pdf
17
Emphasis is on practical, step-by-step, “how-to” strategies to ensure clear or almost-clear skin from all levels of severity

18
Don’t test for:
Testing Options
Do test for:
Secondary bacterial infections with disease
exacerbations
Food allergies for patients <5 years with refractory AD despite optimal treatment and/or clinical history of
allergic reaction to certain foods
Contact dermatitis for refractory AD despite optimal treatment, especially if involving the face
and/or feet
Food allergies on a routine basis
Testing recommendations from integrated guidelines1
1. Eichenfield LF, et al. J Allergy Clin Immunol. 2017;139:S49-S57. 2. Totte JE, et al. Br J Dermatol. 2016;175:687-695.
Serum IgE, patch testing, and/or genetic testing should be done if necessary, to rule out
differential diagnoses.
~70% of patients with AD will show
Staphylococcus aureus colonization with swab testing2

19
Determining Clinically Relevant Infections
Systemic antibiotics are recommended only when there is clear evidence of infection (presence of purulent exudate and pustules)3
Some guidelines recommend dilute bleach baths for bacterial control; however, a systematic review of 5 published articles concluded bleach baths are no more effective than water baths, alone4
1. Totte JE, et al. Br J Dermatol. 2016;175:687-695. 2. Eichenfield LF, et al. J Am Acad Dermatol. 2014;71:116-132. 3. Sidbury R, et al. J Am Acad Dermatol. 2014;71:327-349. 4. Chopra R, et al. Ann Allergy Asthma Immunol. 2017;119:435-440.
S. aureus is resident on the skin of ≥70% of AD patients1
– This colonization does not indicate infection– However, S. aureus can exacerbate AD
AAD guidelines do not support the use of antimicrobial solutions nor topical antibiotics—even when infection is present2
– These do not improve outcomes or disease severity and are associated with contact dermatitis and antimicrobial drug resistance
S. aureus infectionPhoto courtesy of Eric L. Simpson, MD

20
Severity Assessments
Accurate assessment of disease severity is important for optimal treatment
Nonspecialists can quickly and easily use the vIGA and NRS for itch
To use the NRS, ask your patient: “What’s your worst itch intensity over the last 24 hours on a scale of 0 to 10?” (0 = no itch; 10 = worst itch imaginable)
NRS, numerical rating scale.Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018;120:10-22.
Validated Investigator Global Assessment (vIGA)
Score Description
0 – Clear No inflammatory signs of AD (erythema, induration/papulation, lichenification, nor oozing/ crusting). Postinflammatory hyperpigmentation and/or hypopigmentation may be present.
1 – Almost Clear
Barely perceptible erythema, barely perceptible induration/papulation, and/or minimal lichenification. No oozing or crusting.
2 – Mild Slight but definite erythema (pink), slight but definite induration/papulation, and/or slight but definite lichenification. No oozing or crusting.
3 – Moderate Clearly perceptible erythema (dull red), clearly perceptible induration/papulation, and/or clearly perceptible lichenification. Oozing and crusting may be present.
4 – Severe Marked erythema (deep or bright red), marked induration/papulation, and/or marked lichenification. Disease is widespread in extent. Oozing or crusting may be present.

21
AD Severity: Mild
Photos courtesy of Eric L. Simpson, MD

22
AD Severity: Moderate
Photos courtesy of Eric L. Simpson, MD

23
AD Severity: Severe
Photo courtesy of Eric L. Simpson, MD

24
Severity Assessment in Clinical Practice
At each visit, ask about impact of AD on:
Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018;120:10-22. Eichenfield LF, et al. J Allergy Clin Immunol. 2017;139:S49-S57.
Itch
Sleep
Daily Life

25
Case Study 1, Part 1

26
Case Study 1: Nicholas, 17-Year-Old Male
Presents to family physician with eczema that has been present over past 6 months on flexural area of elbows, neck, and face
History of episodic eczema in early adolescence and childhood
Comorbidity of mild asthma Has had multiple allergy tests (all
negative) Has tried diets (gluten-free, probiotics) Now experiences stigma and
embarrassment in school Skin itch and appearance now
interrupting sleep, activities, and sports
Photo courtesy of Eric L. Simpson, MD

28
Pathophysiology and Treatment Approaches

29
AD Pathophysiology: Altered Epidermal Barrier + Immune Dysregulation
CLA, cutaneous lymphocyte-associated; IDEC, inflammatory dendritic epidermal cells; IFN, interferon; IL, Interleukin; LC, Langerhans cells; MC, mast cell; MØ, macrophage; Th2, T helper type 2 cell; ThO, native T cell; TSLP, thymic stromal lymphopoietin.
Adapted from: Boguniewicz M, et al. Immunol Rev. 2011;242:233-246.

30
Treatment Goals
Control itch Control skin inflammation Restore barrier integrity Decrease xerosis Treat secondary infection Recognize and prevent triggers Reduce frequency of flares Improve and maintain QOL

31
Step-Care Management: Non-Lesional/Basic
1. Skin Care• Moisturizer, liberal and frequent• Warm baths or showers using non-soap
cleansers, usually 1×/day followed by moisturizer (even on clear areas)
2. Trigger Avoidance• Common allergens and irritants
Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018:120:10-22. van Zuuren EJ, et al. Cochrane Database Syst Rev. 2017 Feb 6:CD012119. Weber TM, et al. J Drugs Dermatol. 2015;14:478-485
Daily moisturizing can reduce incidence of flare and overall disease severity

32
Step-Care Management: Mild Disease
Topical OTC hydrocortisone can temporarily relieve pruritus and inflammation due to mild AD
– Medical attention should be sought if symptoms worsen or last >7 days
– Not to be used on children <2 years
– OTC treatments should not contain ingredients known to be AD irritants
• eg, soaps, detergents, perfumes
Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018:120:10-22. Weber TM, et al. J Drugs Dermatol. 2015;14:478-485.
1. Skin Care• Moisturizer, liberal and frequent • Warm baths or showers using non-
soap cleansers, usually 1×/day followed by moisturizer (even on clear areas)
2. Antiseptic Measures• Dilute bleach bath (or equivalent)
≤2×/week according to severity (especially with recurrent infections)
3. Trigger Avoidance • Patient-specific proven allergens
and irritants• Consider comorbidities
OTC, over the counter.

33
Topicals: TCS
Available TCS Agents in Various Potencies and Vehicles
Potency Drugs
Least Potent • Hydrocortisone • Hydrocortisone acetate
Mild • Alclometasone dipropionate• Desonide
• Fluocinolone acetonide
Lower Mid-Strength
• Hydrocortisone butyrate• Hydrocortisone probutate
• Hydrocortisone valerate• Prednicarbate
Mid-Strength
• Betamethasone valerate• Clocortolone pivalate• Desoximetasone• Fluocinolone acetonide
• Flurandrenolide• Fluticasone propionate• Mometasone furoate• Triamcinolone acetonide
Potent
• Amcinonide• Betamethasone dipropionate• Desoximetasone• Diflorasone diacetate
• Fluocinonide• Halcinonide• Mometasone furoate• Triamcinolone acetonide
Most Potent • Betamethasone dipropionate• Clobetasol propionate
• Diflorasone diacetate• Halobetasol propionate
TCS usually the first line of treatment to reduce local inflammation Available in a wide variety of formulations (eg, cream, lotion, ointment, foam) Can cause skin
atrophy and thinning if used inappropriately (eg, long-term use of high-potency TCS)
No consensus regarding optimal dosing or frequency
Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018:120:10-22. Eichenfield LF, et al. J Am Acad Dermatol. 2014;71:116-132. Paller AS, et al. J Allergy Clin Immunol. 2017;140:633-643.
TCS, topical corticosteroids.

34
Topicals: TCIs
Nonsteroidal, can be applied to face, extremities, and genital area Stinging/burning at application site most frequent adverse event Inhibits calcineurin-dependent T-cell activation Not indicated for:
– Children <2 years of age
– Long-term, continuous treatment
Sun protection should be used as a precaution
Eichenfield LF, et al. J Am Acad Dermatol. 2014;71:116-132. Siegfried EC, et al. Am J Clin Dermatol. 2013;14:163-178. Stein SL, et al. JAMA. 2016;315:1510-1511.
Currently Available TCIs
TCI Vehicle Indications
Pimecrolimus (1%) cream Mild to moderate AD (2 years and older)
Tacrolimus (0.03% and 0.1%) ointment Moderate to severe AD (2 years and older: 0.03%; 15 years and older: 0.1%)
Note: Despite black-box warnings, postmarketing registry studies have shown virtually no risk for malignancy.
TCIs, topical calcineurin inhibitors.

35
Topical: PDE4 Inhibitor
PDE4 is a key regulator of inflammatory cytokines
Crisaborole 2% ointment, only PDE4 inhibitor approved for AD
– Approved for mild to moderate AD in adults and children ≥2 years
Efficacy proven in two phase 3 studies (N=1,522 patients >2 years) with mild to moderate AD randomized 2:1 to crisaborole or placebo
In both studies, crisaborole shown to be more effective than placebo at achieving clear or almost-clear skin
Stinging/burning at application site most frequent adverse event
Positive long-term data on safety recently published, but no long-term data on efficacy*
*Eichenfield LF, et al. J Am Acad Dermatol. 2017;77:641-649. Ahmed A, et al. Br J Dermatol. 2018;178:659-662. Paller AS, et al. J Am Acad Dermatol. 2016;75:494-503.
PDE4, phosphodiesterase 4.

36
Case Study 1, Part 2

37
Nicholas, Part 2
The family physician recommended that Nicholas avoid triggers and apply topical anti-inflammatory– Prescribed 2×/day for 2 weeks, then 2×/weekly as needed
Within a few weeks, patient reports dissatisfaction with this treatment– Complains that the treatment “never worked”
After careful questioning, Nicholas reveals he didn’t use it as instructed– Couldn’t remember to apply 2×/day
– Didn’t like the “greasy” feel

39
Moderate to Severe Disease and Systemic Treatments

40
Step-Care Management: Moderate Disease
Maintenance TCS• Low potency 1×-2×/day (including face)• Medium potency 1×-2×/day (except face)
OR Maintenance TCI• 1×-2×/day • 2×-3×/week (not an indicated dose)
OR PDE4 Inhibitor*• 2×/day
Inflamed Skin• Medium to high potency TCS 2x/day for 3–7
days beyond clearance (can consider TCI or PDE4 inhibitor)
Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018:120:10-22.
*Indicated for patients at least 2 years old.

41
When to Use Systemic Treatment
Many patients
effectively managed
with topical medications
If condition worsens despite
topicals, consider alternate or concomitant
diagnoses
If adherence is good, the treatment may have failed
—not the patient!Consider systemic
treatment
Simpson EL, et al. J Am Acad Dermatol. 2017;4:623-633.
Determine if adherence and
patient education has been optimal

42
• Dupilumab, only targeted biologic approved for moderate to severe AD in patients ≥12 years
Limitation:• No data for optimal ways to step down or discontinue after clear skin is achieved
• Azathioprine*
• Corticosteroids†
• Cyclosporine*
• Methotrexate*
• Mycophenolate*
Limitation:• Not usable long-term because of multiple systemic adverse events
Types of Treatments for Moderate to Severe Disease
Systemic Immunosuppression
*Not approved by FDA to treat AD. †Not recommended for long-term maintenance.
Biologic

43
Pros and Cons of 5 Most Frequently Used Oral Systemics
Agent Advantages Disadvantages
AZA • Demonstrated efficacy in 3 RCTs• Can be used as monotherapy in
refractory AD
• Nausea and other GI system AEs common• Delayed efficacy (may need ≥12 weeks)• Can cause myelosuppression• Increased risk for cutaneous cancer and lymphoma
CSA • Modest efficacy demonstrated in 14 RCTs• Rapid efficacy (2–6 weeks)
• Long-term use (≥1 year) associated with renal toxicity• Risk for cutaneous cancer and lymphoma
MMF • Modest effect in refractory AD• Generally well tolerated
• Efficacy inconsistent• Nausea most common AE (reduced with enteric-coated
formulation)
MTX • Can show efficacy in low doses• Can be taken long term• Risk for toxicities reduced with folic acid
supplementation
• Nausea and other GI system AEs common• Delayed efficacy (~10 weeks)• Chronic use increases risk for liver toxicity
SCS • Provides rapid response• Only systemic approved for AD
• High rates of toxicity/poor drug survival• Use discouraged by all guidelines because of unfavorable
risk-benefit profile
Drucker AM, et al. Br J Dermatol. 2018;178:768-775. Sidbury R, et al. J Am Acad Dermatol. 2014;71:327-349.
AE(s), adverse event(s); AZA, azathioprine; CSA, cyclosporine A; GI, gastrointestinal; MMF, mycophenolate mofetil; MTX, methotrexate; RCTs, randomized clinical trials; SCS, systemic corticosteroids.

44
Step-Care Management: Severe Disease
Systemic Immunosuppressants• Cyclosporine A‡
• Methotrexate‡
• Mycophenolate mofetil‡• Azathioprine§
Dupilumab†
• Approved for ages ≥12 years
If not resolved in 7 days, consider• Nonadherence, misdiagnosis, referral
Consider acute treatment for some patients• Wet-wrap therapy or hospitalization
Adapted from: Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018:120:10-22.
†Indicated for patients at least 12 years old. ‡Not approved by FDA to treat AD. §Not recommended for long-term maintenance.
Rarely used in children

45
Case Study 2, Part 1

46
Case Study 2, Brianna, 21-Year-Old Female
Presents to primary care physician with complaints of eczema and severe itching– Reports life-long history of mild to moderate disease that has
worsened over the past 2 years
Lesions recently appear on forehead and cheeks– Brianna contends that topical steroids “don’t help” and the lesions go
away only when she takes oral corticosteroids
– Has involvement of 15% of body surface area
Brianna is a newly licensed real estate agent– Complains that it’s difficult at her age to gain credibility in this field;
believes facial involvement worsens this
– Has difficulty sleeping, which makes her more anxious

48
Approved Biologic

49
AD Etiology: Interrelated Dysfunction Between Immune System and Skin
Immune System Skin
Dry skin and Eczematous Lesions
Cycle of Itching/Scratching
Epidermal Barrier Breakdown
Cellular Damage and Secondary Infections
Immune Dysregulation
Activated Inflammatory
Cascade
Overproduction of Cytokines
IL-4, IL-13, IL-31
Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018;120:10-22. Irvine AD, et al. N Engl J Med. 2011;365:1315-1327.

50
One Approved Biologic Agent for AD
Dupilumab
Approved as second-line treatment for moderate to severe AD not controlled
by topical treatments
Anti-IL-4Rα targets IL-4 and IL-13 receptors
Subcutaneous injectable given every other
week after initial dose
Approved March 2019 for ages 12–17
with moderate to severe AD
mAb, monoclonal antibody. Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018:120:10-22. Dupilumab (Dupixent®) PI 03/2019.

51
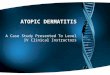
IGA Reduction at Week 16
12% (n=315)
8% (n=236)
10% (n=224)
39% (n=319)
36% (n=233)
38% (n=224)
39% (n=106)
36% (n=239)
37% (n=223)
0 5 10 15 20 25 30 35 40 45
LIBERTY AD CHRONOS (N=740)*
SOLO 2 (N=708)
SOLO 1 (N=671)
% Achieving IGA Endpoint from Baseline
Patients Achieving IGA Score of 0/1 and Reduction of ≥2 Points at Week 16 in SOLO 1, SOLO 2, and CHRONOS Trials
Dupilumab 300 mg QW Dupilumab 300 mg Q2W Placebo
*CHRONOS combined dupilumab with concomitant topical corticosteroid.IGA, Investigator’s Global Assessment; Q2W, every other week; QW, every week.
Simpson EL, et al. N Engl J Med. 2016;375:2335-2348.

52
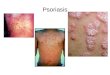
EASI Reduction at Week 16 and 52
Adapted from: Blauvelt A, et al. Lancet. 2017;389:2287-2303.
CHRONOS Trial Reduction in EASI Scores Over Time*
*Least squares mean percent change in EASI score over time. EASI, Eczema Area and Severity Index.
-10
-20
-30
-40
-50
-60
-70
-80
-90
-100% M
ean
Chan
ge in
EAS
ISco
re fr
om B
asel
ine* Placebo + TCS
Dupilumab 300 mg QW + TCS
Dupilumab 300 mg Q2W + TCS
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52Study Week
-43%
-77%
-77%
-46%
-78%
-80%

53
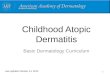
Pruritus NRS Reduction at Week 16 and 52
-29 (n=315)
-27 (n=264)
-55 (n=319)
-55 (n=270)
-56 (n=106)
-56 (n=89)
-60
-50
-40
-30
-20
-10
0
% R
educ
tion
in P
rurit
us N
RS
Placebo + TCS Dupilumab 300 mg QW + TCS Dupilumab 300 Q2W + TCS
Week 16 Week 52
CHRONOS Trial Reductions in Pruritus*
Blauvelt A, et al. Lancet. 2017;389:2287-2303.
*Percentages are rounded.

54
Common AEs and Other Effects of Dupilumab
Incr
ease
d Ri
sk
Redu
ced
Risk Skin infection
(RR 0.54; 95% CI 0.42–0.69)
AD exacerbation (RR 0.44; 95% CI 0.34–0.59)
Injection-site reaction (RR 2.24; 95% CI 1.68–2.99)
Headache (RR 1.47; 95% CI 1.05–2.06)
Conjunctivitis (RR 2.64; 95% CI 1.79–3.89)
A meta-analysis of 8 dupilumab RCTs assessed common drug-related AEs in adults with moderate to severe AD
Ou Z, et al. Int Immunopharmacol. 2018;54:303-310.
CI, confidence interval; RR, risk ratio.

55
Phase 3 Trial of Dupilumab in Adolescents
First biologic study of AD in ages 12–17 years (NCT03054428)– 251 patients with moderate to severe disease randomized to dosing
every 4 weeks, every 2 weeks, or placebo– Coprimary endpoints EASI response and IGA score of 0 (clear) or
1 (almost clear)– Secondary endpoint reduction in pruritus NRS
Preliminary phase 3 results presented September 2018 at EADV showed statistically significant improvement in skin, pruritus, and QOL by week 16– Approval granted for use in ages 12–17 in March 2019
Clinicaltrials.gov. NCT03054428 https://clinicaltrials.gov/ct2/show/NCT03054428. Simpson EL, et al. EADV abstract D3T01.1L. Presented September 15, 2018.
EADV, European Academy of Dermatology and Venereology.

56
Phase 3 Dupilumab Trial in Adolescents
18
38
46
24
4248
2.4 8.2
19
0
10
20
30
40
50
60
IGA EASI-75 Pruritus NRS
Perc
enta
ge
16 Weeks
Dupilumab 300 mg Q4W Dupilumab 200/300 Q2W Placebo
Simpson EL, et al. EADV abstract D3T01.1L. Presented September 15, 2018.
Patients Achieving Trial Endpoints of IGA 0/1,Improvement of ≥75% and Reductions in Pruritus*
*Percentages are rounded. Q4W, every 4 weeks.

57
Phase 3 Dupilumab Trial in Adolescents: Safety
1311
6
11 10 9
20
5 5
0
5
10
15
20
25
Skin Infections Conjunctivitis Injection-Site Reactions
Perc
enta
ge
16 Weeks
Dupilumab 300 mg Q4W Dupilumab 200/300 Q2W Placebo
Most Common Adverse Events*
Simpson EL, et al. EADV abstract D3T01.1L. Presented September 15, 2018.*Percentages are rounded.

58
Case Study 2, Part 2

59
Brianna, Part 2
Brianna was prescribed a mid-strength topical corticosteroid– Instructed to apply once daily for 2 weeks
Begins to flare upon topical corticosteroid taper and daily TCI
Brianna reports struggling with anxiety and depression because of itching and appearance
It’s important to employ shared decision-making regarding treatment for this patient– Patient says she’s too busy to undergo phototherapy
– She says she wants a course of oral corticosteroids because they have always worked before

61
Considerations in Managing AD

62
Identifying Treatment Failure
No validated biomarkers to assess treatment response
No standard definition for treatment failure
Boguniewicz M, et al. J Allergy Clin Immunol Pract. 2017;5:1519-1531. Spergel JM. UpToDate. Last Updated: August 15, 2018.
Definitions Proposed by
Expert Panel in 2017
No relief from impairment
(particularly in QOL)
Unacceptable AEs leading to treatment
discontinuation
Lack of stable, long-term control (flares continue)
Inadequate clinical
improvement

63
Causes for Treatment Failure
Poor understanding of disease– Clinicians, caregivers, patients unaware AD is systemic,
inflammatory disorder
Poor adherence/incorrect medication use– TCS phobia affects up to 80% of patients and
caregivers1
Exacerbating factors/environmental triggers Secondary infection
– Bacterial, viral, dermatophyte
Hypersensitivity reactions to treatments Incorrect diagnosis
1. Li AW, et al. JAMA Dermatol. 2017;153:1036-1042. 2. Simpson EL, J Am Acad Dermatol. 2016;74:491-498.
“Misdiagnosis of atopic dermatitis is a
concern … it can contribute to making the disease worse.”2
–Dirk M. Elson, MD Past President, AAD
2013–2014

64
Considerations for Dupilumab
Cost and coverage are important considerations Method of administration
– Subcutaneous injection may be difficult for some
Patients with moderate to severe AD have increased risk for infection– Dupilumab reduces risk for infection vs placebo
Insurance requires prior authorization for immunomodulators or biologics– Forms and requirements different for each company
For insurance to cover, clinicians must document– Diagnosis of AD (not just “eczema”)– Condition severity– Prior treatments and failures
• Specify the type of failure: inadequate response to medium- or high-potency TCS, suboptimal improvement, failure to achieve long-term control, unacceptable AEs
Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018;120:10-22. Eichenfield LF, et al. Am J Clin Dermatol. 2019;20:443-456. Kuznik A, et al. Dermatol Ther (Heidelb). 2017;7:493-505. Ou Z, et al. Int Immunopharmacol. 2018;54:303-310.

65
Who Should Be Referred to Specialists?
Phototherapy‡
Stepping up from Moderate to Severe AD: If patient is still symptomatic* despite optimal
therapy and conservative management, options include the following†
Dupilumab§ Systemic immunosuppressantsǁ
*Poorly or inadequately controlled signs and symptoms of AD. †Before stepping up therapy, patient should be assessed for nonadherence, comorbidities, other factors that could mitigate against treatment response. ‡Patient should be willing and able to commit to phototherapy’s cost and understand its limited access. §Indicated for patients ≥12 years with moderate to severe AD. ǁNone are approved for AD, except for systemic corticosteroids, which are not typically recommended.
For some, consider acute treatment:• Wet-wrap
therapy• Hospitalization
Boguniewicz M, et al. Ann Allergy Asthma Immunol. 2018:120:10-22. Eichenfield LF, et al. J Allergy Clin Immunol. 2017;139:S49-S57.

66
Multidisciplinary Collaboration
AD specialists are usually dermatologists or allergists Patients with moderate to severe AD are good
candidates for multidisciplinary management which can include immunosuppressive or biologic therapy as well as additional specialist care
PCPs (family medicine, pediatricians, NPs, PAs) are the center of this team
Comorbid atopic diseases, sleep problems and mental health impacts should be addressed and appropriate specialists used if needed
Utilizing this multi-disciplinary team ensures that patients with AD get a more global approach to care to achieve optimal outcomes and give patients back their life
NPs, nurse practitioners; PAs, physician assistants.LeBovidge JS, et al. J Allergy Clin Immunol. 2016;138:325-334.

67
Strategies for Adherence and Patient Education
Written eczema “action plans”
Nurse-led eczema workshops
Providing psychological support
Caring for comorbidities (eg, asthma, cardiovascular, allergies, obesity)
Multidisciplinary patient education
Discussing patients’ fears about treatment
Asking patients to choose preferred treatment vehicle (especially with topicals)
Bass AM, et al. J Clin Med. 2015;4:231-242. Borok J. Dermatology News. June 27, 2017. Patel NU, et al. Am J Clin Dermatol. 2017;18:323-332. Snyder, et al. Cutis. 2015;96:397-401.

68
Summary
AD is an inflammatory disease involving immune dysregulation and epidermal barrier breakdown
Disease negatively affects QOL of children and adults, as well as their family members
Diagnosis based on clinical presentation
AD associated with multiple comorbidities—even later in life
Severity assessments are necessary to determine treatment

69
Summary (cont)
Multiple treatments available depending on disease severity
Systemic immunosuppression not suitable for long-term maintenance and none approved in children
Dupilumab the only biologic thus far available
– Trials show long-term efficacy
– Recent phase 3 trial in adolescents yielded positive results
– Approved by FDA in March 2019 for adolescents 12–17 with moderate to severe AD

70
Thank You!