Embed Size (px)
DESCRIPTION
The Role of Thought Believability in the Relationship Between Depression, Diabetes, and Stress. Eric Schmidt, Kate Ward, Jennifer Gregg, Jesse Tarango, and Tommy VanVeghel. San José State University. The Diabetes Epidemic. In U.S. alone, 24+ million (CDC, 2007/2008) - PowerPoint PPT Presentation
Citation preview

The Role of Thought Believability in the Relationship Between
Depression, Diabetes, and Stress.
Eric Schmidt, Kate Ward, Jennifer Gregg, Jesse Tarango, and
Tommy VanVeghel
San José State University

The Diabetes Epidemic
• In U.S. alone, 24+ million (CDC, 2007/2008)
– Diagnosable diabetes > 8% of U.S. population– Another 57 million with pre-diabetes
• 250+ million worldwide (WHO, 2009)
– 7 million/year increase in cases– Causes 5% of deaths globally – Number of deaths to double by 2030
• Still uncertain etiology in Type 2 Diabetes– Population rates related to obesity

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
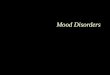
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
1994

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
1995

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
1996

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
1997

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
1998

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
1999

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
2000

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
2001

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
2002

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
2003

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
2004

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
2005

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
2006

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
2007

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
2008

CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
Obesity (BMI≥30 kg/m2) Diabetes
<4.5%Missing data4.5 - 5.9% 6.0 - 7.4%7.5 - 8.9% ≥9.0%
18.0 -21.9%<14.0%Missing Data
14.0 - 17.9%22.0 - 25.9% ≥26.0%
Age-adjusted Percentage of U.S. Adults Who Were Obese or Who Had Diagnosed Diabetes
2008

Depression and Diabetes
Those with comorbid Diabetes and Depression• Show less adherence to prescription regimen• Tend to partake in fewer self-management activities• Are at increased risk for undesirable and preventable
medical outcomes and mortality(Gonzalez et al., 2007; Ciechanowski et al., 2000; Lin et al., 2004; Kalsekar et al., 2006; Katon et al., 2005; Katon et
al., 2009)
• People with Diabetes at 1.6-2.0x risk for Depression (Anderson et al., 2001; Ali et al., 2006)
• No difference has been reported (Téllez-Zenteno et al., 2002)
• People with Depression at 23-37% increased risk for developing Diabetes (Knol et al., 2006; Brown et al., 2005)

Depression, Stress, & Diabetes
• Stress – “Perceived Stress” – Acute stressors and Allostatic Load
• Depression and Stress correlated– Stress also important in chronic disease– Self-Management & Adherence linked with blood
sugar control– Blood sugar control linked with medical
outcomes and mortality in diabetes

Cortisol, Diabetes, & Depression
• Stress biomedically related to diabetes in a way we don’t often see with psychological disorders– Affects behavior (self-management, etc.)– But *also* matters biologically
• Cortisol related to “Fight or Flight”– Related to both Stress and Depression– Activation of HPA Axis, inhibits insulin action– Increased blood sugar levels– Increased risk for undesirable medical outcomes

Previous ResearchSacco et al. (2005, 2007) • Self-Efficacy mediates adherence and depression
Doesn’t give us a way to intervene within the model• “…enhancing adherence in people with diabetes should
enhance their physical and mental health by reducing depressive symptoms.”
• Recommend emphasis on diet and exercise adherence
Adherence Depression-0.35* -0.38*
2005 2007 * p < .01 † p = n.s.
Self-Efficacy
Adherence Depression
0.74*0.74*
-0.41*-0.38*
† †

But From an ACT PerspectiveSacco et al. (2005, 2007) • Self-Efficacy mediates adherence and depression
Doesn’t give us a way to intervene within the model• “…enhancing adherence in people with diabetes should
enhance their physical and mental health by reducing depressive symptoms.”
• Recommend emphasis on diet and exercise adherence
Adherence Depression-0.35* -0.38*
2005 2007 * p < .01 † p = n.s.
Self-Efficacy
Adherence Depression
0.74*0.74*
-0.41*-0.38*
† †

But From an ACT PerspectiveSacco et al. (2005, 2007) • Self-Efficacy mediates adherence and depression
Doesn’t give us a way to intervene within the model• Adherence is still the problem!!• We already know that adherence efforts don’t work consistently
Adherence Depression
Believability
Adherence DepressionDepression Adherence
?
? ?

BelievabilityAn Intervention for Adherence• Varied levels of depression symptoms related to high
levels of non-adherence (Fisher et al., 2007; Gonzalez et al., 2007)
– Some patients “distressed,” not depressed
• Conflicting support for Depression as predictor in mediation, and relationship remains complicated (McKellar et al., 2004; Gregg et al., 2010)
– Insulin vs. medication adherence (Aikens et al., 2008)
– Gender differences (Nau et al., 2007)
Need interventions that provide patients with behavioral tools delivered within the diabetes self-management and depression relationship.

Research Questions
1. Does Believability of Negative Thoughts mediate relationship between Adherence to diabetes self-management and Depression?
2. Does Believability of Negative Thoughts mediate the relationship between Adherence to diabetes self-management and Stress?

Methods
• Cross-sectional internet-based survey• Participants with Type 2 Diabetes Mellitus
(N=171)◦ Diabetes-specific discussion boards, websites, and forums◦ $5 Amazon.com gift card
• Depression, Stress, Diabetes Self-Care• Exclusions: Duplicate IP address,
International, Entries not referring to Diabetes, Pregnant, Eating Disorder (N=34)

Methods - Measures
• Automatic Thoughts Questionnaire (ATQ-B)– “Believability” or Cognitive Fusion
• Beck Depression Inventory (BDI)
• Perceived Stress Scale (PSS)
• Summary of Diabetes Self-Care Activities – “Adherence”– Diet and exercise focus– E.g., “On how many of the last 7 days did you eat your
recommended number of vegetables?”

Methods: Mediation Analysis
1. Adherence predicts Stress
2. Believability predicts Stress
3. Adherence predicts Believability
4. Statistically significant reduction of the predictive power of Adherence on Stress when Believability is controlled
Believability
Adherence Stress
Proposed Model

Research Question 1
Depression Model• Believability of Negative Thoughts mediates
Adherence and Depression (Gregg et al., 2010)– Model not significant with Depression as predictor
Believability
Adherence Depression
-0.24** 0.48***
-0.37***
* p < .01 ** p < .001

Research Question 1
Depression Model• Believability of Negative Thoughts mediates
Adherence and Depression (Gregg et al., 2010)– Model not significant with Depression as predictor
Believability
Adherence Depression
-0.24** 0.48***
-0.37***
Believability
Adherence Depression
-0.24** 0.42***
-0.27**
* p < .01 ** p < .001

Research Question 1
Depression Model• Believability of Negative Thoughts mediates
Adherence and Depression (Gregg et al., 2010)– Model not significant with Depression as predictor
Believability
Adherence Depression
-0.24** 0.48***
-0.37***
Believability
Adherence Depression
-0.24** 0.42***
-0.27**
β = −.270, t (121) = -3.428, p < .01Sobel = 2.43, p = .015* p < .01 ** p < .001

Results: Stress Model
Believability
Adherence Stress
Proposed Model
Adherence Stress
Believability Stress
β = −.279, t (119) = -3.182, p = .002
Adherence Believability
β = .306, t (119) = 3.574, p = .001
β = −.240, t (119) = -2.711, p = .008
Depression Stressr = .219 p = .01
MeasuresStress: Perceived Stress ScaleBelievability: Automatic Thoughts Questionnaire - BAdherence: Summary of Diabetes Self-Care ActivitiesDepression: Beck Depression Inventory

Results: Stress Model
Believability
Adherence Stress
-0.24** 0.31***
-0.28**
*p<.05 **p<.01 ***p<.001
• Believability of Negative Thoughts mediated Adherence and Perceived Stress– Partial mediation with Believability for Stress, Depression, and
Adherence

Results: Stress Model
Believability
Adherence Stress
-0.24** 0.31***
-0.28**
Believability
Adherence Stress
-0.24** 0.33***
-0.20*
*p<.05 **p<.01 ***p<.001
• Believability of Negative Thoughts mediated Adherence and Perceived Stress– Partial mediation with Believability for Stress, Depression, and
Adherence

Results: Stress Model
Believability
Adherence Stress
-0.24** 0.31***
-0.28**
Believability
Adherence Stress
-0.24** 0.33***
-0.20*
β = −.200, t (119) = -2.337, p = .021Sobel = 2.184, p = .029*p<.05 **p<.01 ***p<.001
• Believability of Negative Thoughts mediated Adherence and Perceived Stress– Partial mediation with Believability for Stress, Depression, and
Adherence

Discussion• Depression and Stress related to Adherence• Believability mediated both relationships
– Adherence → Depression– Adherence → Stress– Depression and Stress correlated
• Contributes to the viability of Believability as a clinical target in this population– ACT for Clinically Depressed patients with Diabetes– Principles of ACT incorporated into Diabetes Education
• Gregg et al. (2007) reported more desirable blood sugar and self-management at 3 months in group receiving 1-day ACT with Diabetes Education

Future Research
• Limitations– Cross-Sectional Data– Internet-Based (benefit?)– Self-Report– Strength of Relationships
• Future Research– Are these models bi-directional? Causation?– Do these models represent distinct sub-populations?– Can ACT principles lead to benefits in Diabetes self-
management at various stages of diabetes and psychological flexibility?
ATQ-Frequency
ATQ-Believability
r = .569***
For more information, contact Eric Schmidt at [email protected]

ReferencesAli, S., Stone, M.A., Peters, J.L., Davies, M.J., & Kunti, K. (2006). The prevalence of co-morbid
depression in adults with Type 2 diabetes: A systematic review and meta-analysis. Diabetic Medicine, 23, 1165-1173.
Anderson, R.J., Feedland, K.E., Clouse, R.E., & Lustman, P.J. (2001). The prevalence of comorbid depression in adults with diabetes. Diabetes Care, 24, 1069-1078.
Brown, L.C., Majumdar, S.R., Newman, S.C., & Johnson, J.A. (2005). History of depression increases risk of type 2 diabetes in younger adults. Diabetes Care, 28, 1063-1067.
Centers for Disease Control and Prevention (2007). National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2007. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2008.
Ciechanowski, P.S., Katon, W.J., & Russo, J.E. (2000). Depression and diabetes: Impact of depressive symptoms on adherence, function, and costs. Archives of Internal Medicine, 160, 3278-3285.
Fisher, L., Skaff, M.M., Mullan, J.T., Arean, P., Mohr, D., Masharani, U., et al. (2007). Clinical depression versus distress among patients with type 2 diabetes. Not just a question of semantics. Diabetes Care, 30, 542-548.
Gonzalez, J.S., Safren, S.A., Cagliero, E., Wexler, D.J., Delahanty, L., Wittenberg, E. et al. (2007). Depression, self-care, and medication adherence in type 2 diabetes. Diabetes Care, 30, 2222-2227.
For more information, contact Eric Schmidt at [email protected]

ReferencesGregg, J.A., Callaghan, G.M., Hayes, S.C., & Glenn-Lawson, J.L. (2007). Improving diabetes
self-management through acceptance, mindfulness, and values: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 75, 336-343.
Gregg, J.A., Schmidt, E.S., Ward, K.C., Almada, P., & Knezevich, P. (2010). An alternative model for understanding the diabetes-depression relationship: The mediational role of thought believability. Journal of Behavioral Health and Medicine, 1 (1), 15-23.
Kalsekar, I.D., Madhavan, S.S., Amonkar, M.M., Makela, E.H., Scott, V.G., Douglas, S.M., et al. (2006). Depression in patients with type 2 diabetes: Impact on adherence to oral hypoglycemic agents. The Annals of Pharmacotherapy, 40, 605-611.
Katon, W.J., Rutter, C., Simon, G., Lin, E.H.B., Ludman, E., Ciechanowski, P. et al. (2005). The association of comorbid depression with mortality in patients with type 2 diabetes. Diabetes Care, 28, 2668-2672.
Katon, W., Russo, J., Lin, E.H.G., Heckbert, S.R., Karter, A.J., Williams, L.H., et al. (2009). Diabetes and poor disease control: Is comorbid depression associated with poor medication adherence or lack of treatment intensification? Psychosomatic Medicine, 71, 965-972.
Knol, M.J., Twisk, J.W.R, Beekman, A.T.F., Heine, R.J. Snoek, F.J., & Pouwer, F. (2006). Depression as a risk factor for the onset of type 2 diabetes mellitus. A meta-analysis. Diabetologia, 49, 837-845.
For more information, contact Eric Schmidt at [email protected]

ReferencesLin, E.H.B., Katon, W., Von Korff, M., Rutter, C., Simon, G.E., Oliver, M., et al. (2004).
Relationship of depression and diabetes self-care, medication adherence, and preventive care. Diabetes Care, 27, 2154-2160.
Nau, D.P., Aikens, J.E., & Pacholski, A.M. (2007). Effects of gender and depression on oral medication adherence in persons with type 2 diabetes mellitus. Gender Medicine, 4, 205-213.
Sacco, W.P., Wells, K.J., Vaughan, C.A., Friedman, A., Perez, S., & Matthew, R. (2005). Depression in adults with type 2 diabetes: The role of adherence, body mass index, and self-efficacy. Health Psychology, 24, 630-634.
Sacco, W.P., Wells, K.J., Friedman, A., Matthew, R., Perez, S., & Vaughan, C.A. (2007). Adherence, body mass index, and depression in type 2 diabetes: The mediational role of diabetes symptoms and self-efficacy. Health Psychology, 26, 693-700.
Téllez-Zenteno, J.F., & Cardiel, M.H. (2002). Risk factors associated with depression in patients with type 2 diabetes mellitus. Archives of Medical Research, 33 (1), 53-60.
World Health Organization (2009). Diabetes fact sheet. No 312. WHO Statistical Information System, Global Burden of Disease Project. Available at http://www.who.int/diabetes/facts/en/index.html, downloaded May 15, 2010.
For more information, contact Eric Schmidt at [email protected]

ReferencesAli, S., Stone, M.A., Peters, J.L., Davies, M.J., & Kunti, K. (2006). The prevalence of co-morbid
depression in adults with Type 2 diabetes: A systematic review and meta-analysis. Diabetic Medicine, 23, 1165-1173.
Anderson, R.J., Feedland, K.E., Clouse, R.E., & Lustman, P.J. (2001). The prevalence of comorbid depression in adults with diabetes. Diabetes Care, 24, 1069-1078.
Brown, L.C., Majumdar, S.R., Newman, S.C., & Johnson, J.A. (2005). History of depression increases risk of type 2 diabetes in younger adults. Diabetes Care, 28, 1063-1067.
Centers for Disease Control and Prevention (2007). National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2007. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2008.
Ciechanowski, P.S., Katon, W.J., & Russo, J.E. (2000). Depression and diabetes: Impact of depressive symptoms on adherence, function, and costs. Archives of Internal Medicine, 160, 3278-3285.
Fisher, L., Skaff, M.M., Mullan, J.T., Arean, P., Mohr, D., Masharani, U., et al. (2007). Clinical depression versus distress among patients with type 2 diabetes. Not just a question of semantics. Diabetes Care, 30, 542-548.
Gonzalez, J.S., Safren, S.A., Cagliero, E., Wexler, D.J., Delahanty, L., Wittenberg, E. et al. (2007). Depression, self-care, and medication adherence in type 2 diabetes. Diabetes Care, 30, 2222-2227.
For more information, contact Eric Schmidt at [email protected]

ReferencesGregg, J.A., Callaghan, G.M., Hayes, S.C., & Glenn-Lawson, J.L. (2007). Improving diabetes
self-management through acceptance, mindfulness, and values: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 75, 336-343.
Gregg, J.A., Schmidt, E.S., Ward, K.C., Almada, P., & Knezevich, P. (2010). An alternative model for understanding the diabetes-depression relationship: The mediational role of thought believability. Journal of Behavioral Health and Medicine, 1 (1), 15-23.
Kalsekar, I.D., Madhavan, S.S., Amonkar, M.M., Makela, E.H., Scott, V.G., Douglas, S.M., et al. (2006). Depression in patients with type 2 diabetes: Impact on adherence to oral hypoglycemic agents. The Annals of Pharmacotherapy, 40, 605-611.
Katon, W.J., Rutter, C., Simon, G., Lin, E.H.B., Ludman, E., Ciechanowski, P. et al. (2005). The association of comorbid depression with mortality in patients with type 2 diabetes. Diabetes Care, 28, 2668-2672.
Katon, W., Russo, J., Lin, E.H.G., Heckbert, S.R., Karter, A.J., Williams, L.H., et al. (2009). Diabetes and poor disease control: Is comorbid depression associated with poor medication adherence or lack of treatment intensification? Psychosomatic Medicine, 71, 965-972.
Knol, M.J., Twisk, J.W.R, Beekman, A.T.F., Heine, R.J. Snoek, F.J., & Pouwer, F. (2006). Depression as a risk factor for the onset of type 2 diabetes mellitus. A meta-analysis. Diabetologia, 49, 837-845.
For more information, contact Eric Schmidt at [email protected]

ReferencesLin, E.H.B., Katon, W., Von Korff, M., Rutter, C., Simon, G.E., Oliver, M., et al. (2004).
Relationship of depression and diabetes self-care, medication adherence, and preventive care. Diabetes Care, 27, 2154-2160.
Nau, D.P., Aikens, J.E., & Pacholski, A.M. (2007). Effects of gender and depression on oral medication adherence in persons with type 2 diabetes mellitus. Gender Medicine, 4, 205-213.
Sacco, W.P., Wells, K.J., Vaughan, C.A., Friedman, A., Perez, S., & Matthew, R. (2005). Depression in adults with type 2 diabetes: The role of adherence, body mass index, and self-efficacy. Health Psychology, 24, 630-634.
Sacco, W.P., Wells, K.J., Friedman, A., Matthew, R., Perez, S., & Vaughan, C.A. (2007). Adherence, body mass index, and depression in type 2 diabetes: The mediational role of diabetes symptoms and self-efficacy. Health Psychology, 26, 693-700.
Téllez-Zenteno, J.F., & Cardiel, M.H. (2002). Risk factors associated with depression in patients with type 2 diabetes mellitus. Archives of Medical Research, 33 (1), 53-60.
World Health Organization (2009). Diabetes fact sheet. No 312. WHO Statistical Information System, Global Burden of Disease Project. Available at http://www.who.int/diabetes/facts/en/index.html, downloaded May 15, 2010.
For more information, contact Eric Schmidt at [email protected]