Embed Size (px)
Citation preview

EDITORIALThe Role of Vitrectomy in the Treatment of
Diabetic Macular Edema
HILEL LEWIS, MD
D IABETIC MACULAR EDEMA DEVELOPS IN INDIVIDU-
als with diabetes when macromolecules and fluidaccumulate in the extracellular space. The condi-
tion affects an estimated 75,000 new patients in theUnited States every year and is the most common cause ofdecreased visual acuity among diabetics.1 A population-based study has shown that over a 10-year period the
See also pp. 44–49
incidence of diabetic macular edema among individualswith diabetes was between 13.9% and 25.4%.2 It has beenpredicted that 42% of individuals with type I diabetes willdevelop macular edema in their lifetime,3 so diabeticmacular edema is an important public health problem anda major cause of suffering, disability, and lost productivity.
Causes of diabetic macular edema include increasedvasopermeability and damage to the retinal capillaries andthe barrier provided by the retinal pigment epithelium.Our understanding of the mechanisms responsible for thebreakdown of the blood-retinal barrier and the develop-ment of macular edema in diabetics has increased in recentyears. Aiello and colleagues demonstrated that vascularendothelial growth factor induces retinal vascular perme-ability and that this effect is mediated primarily by theactivation of the beta-isoform of protein kinase C.4 Theloss of the barrier function of the blood-retinal barrier canbe explained by damage in the structure of the retinalendothelial junction. Antonetti and colleagues showedthat increased levels of vascular endothelial growth factorin the vitreous decrease levels of occludin, a membrane-spanning tight junction protein, which could account forthe increased vasopermeability in patients with diabeticmacular edema.5 Histamine can also increase the perme-ability of the blood–retinal barrier by reducing the expres-
sion of the tight junction/adherens junction protein, ZO-1.6
Although diabetic macular edema can spontaneouslyresolve,7–8 the Early Treatment Diabetic RetinopathyStudy demonstrated that most eyes with diabetic macularedema, whether treated by photocoagulation or not, de-velop progressive loss of vision.8
The treatment for diabetic macular edema includesmedical control of metabolic abnormalities. Patientsshould achieve excellent glycemic control, normalizeblood pressure, improve cardiac and renal status, andreduce serum lipids; photocoagulation therapy also isbeneficial. The Early Treatment Diabetic RetinopathyStudy showed that focal macular photocoagulation forclinically significant diabetic macular edema reduced theincidence of moderate vision loss by 50%; however, only3% of patients in the study had improvement of 3 or morelines of visions.8 As a result, focal laser treatment is likelyto reduce the rate of vision loss only, not to improvevision, and patients are frequently disappointed with theresults of treatment. The high and increasing prevalence ofdiabetic macular edema and the absence of a fully success-ful treatment have resulted in the search for alternativetherapies.
Since our publication in 1992 (Ophthalmology 99:753–759, ● 2000), which described a subset of patients withdiabetic macular traction and edema associated with pos-terior hyaloidal thickening, there has been an interest invitreous surgery as a potential treatment for diabeticmacular edema.9
What evidence exists that the vitreous plays a role inthe development or exacerbation of macular edema indiabetic patients and that removing it is beneficial?
The prevalence of posterior vitreous detachment inpatients with diabetic macular edema is significantlyhigher than in diabetic patients without macular edema.10
Moreover, a small prospective study by Hikichi and col-leagues strongly suggested that vitreomacular separationmay cause spontaneous resolution of diabetic macularedema.7
Several groups have confirmed our initial observationthat vitrectomy seems to be beneficial for patients with
Accepted for publication Jul 14, 2000.From the Cole Eye Institute, The Cleveland Clinic Foundation,
Cleveland, OhioReprint requests to Hilel Lewis, MD, Cole Eye Institute and the
Division of Ophthalmology (i30), The Cleveland Clinic Foundation,9500 Euclid Ave, Cleveland, OH 44195; fax: (216) 445-7654; e-mail:[email protected]
© 2001 BY ELSEVIER SCIENCE INC. ALL RIGHTS RESERVED.0002-9394/01/$20.00 123PII S0002-9394(00)00660-7
macular edema and traction that are associated withposterior hyaloidal thickening.11–13 Others have found thateven among patients whose diabetic macular edema is notaccompanied by visible evidence of posterior hyaloidalthickening or traction some respond to vitrectomy withresolved macular edema and improved vision.14–17 In theseries reported in the literature, from 38% to 100% of eyesthat underwent vitrectomy for diabetic macular edemashowed improved visual acuity.9,11–15,17 One possible ex-planation for this high rate of improvement is chance.Most of these studies were retrospective and nonrandom-ized, they included only small numbers of patients, andvisual acuity was not measured by masked observers usinga specific protocol. An additional explanation might bethat the patients had a short duration of macular edema.
However, these studies may instead support our hypoth-esis that the tractional forces exerted by the posteriorhyaloid produce a shallow macular detachment that can-not be discerned ophthalmoscopically or even intraopera-tively. Removing these tractional forces by vitrectomy mayresult in spontaneous macular reattachment, which couldexplain the improvement in visual function seen in thesepatients.9 If this theory were not true, the percentage ofeyes with improved vision after resolution of macularedema would be expected to be the same, whether vitrec-tomy or focal macular photocoagulation had been per-formed.
Kaiser and associates report the use of optical coherencetomography to confirm our hypothesis in this issue of THE
JOURNAL. Using such tomography, we showed that patientswith diabetic macular edema and posterior hyaloidal thick-ening had a shallow macular traction detachment from theposterior hyaloid in addition to macular thickening.18 Ashallow macular tractional detachment would allow thefluorescein to pool under the detached neurosensory ret-ina, which would explain the characteristic angiographicfinding of deep, diffuse, late leakage in these eyes. Spon-taneous macular reattachment after vitrectomy would alsoexplain the subsequent improvement in visual function.Future studies should determine whether a shallow maculardetachment is also present in some eyes with diabeticmacular edema that do not have evident posterior hyaloi-dal thickening or traction.
Current evidence suggests that the vitreous could beimplicated in the development or exacerbation of diabeticmacular edema through several mechanical or physiologicmechanisms, all of which stem from the increased retinalvascular permeability caused by vascular endothelialgrowth factor.
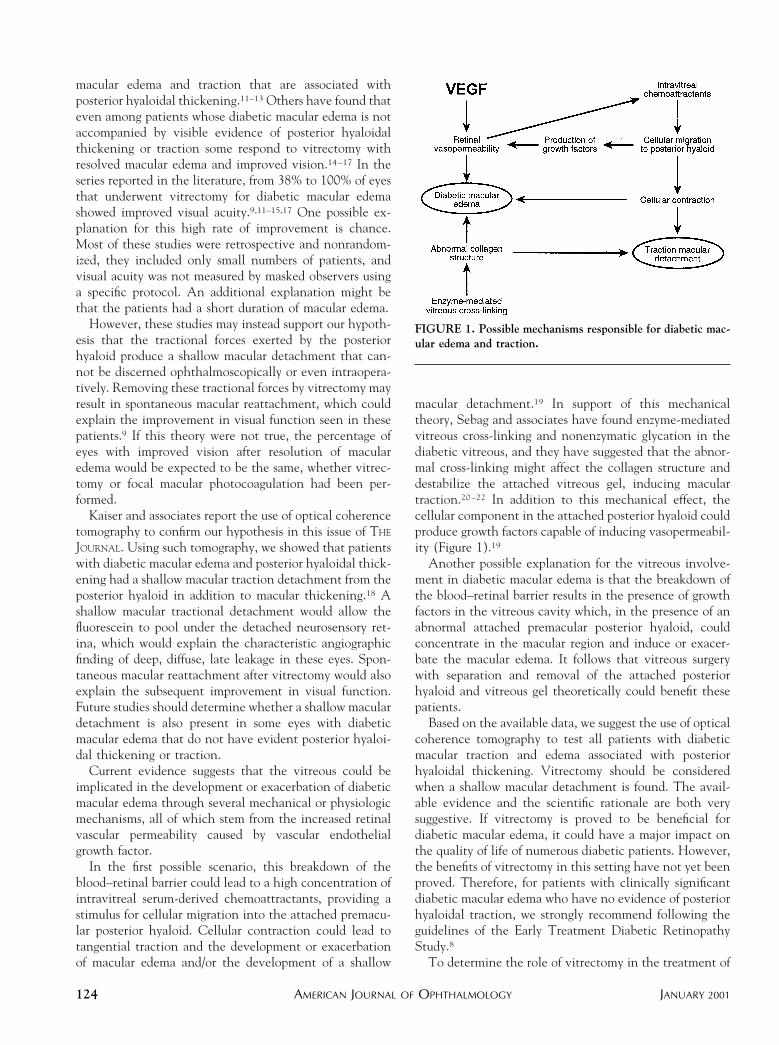
In the first possible scenario, this breakdown of theblood–retinal barrier could lead to a high concentration ofintravitreal serum-derived chemoattractants, providing astimulus for cellular migration into the attached premacu-lar posterior hyaloid. Cellular contraction could lead totangential traction and the development or exacerbationof macular edema and/or the development of a shallow
macular detachment.19 In support of this mechanicaltheory, Sebag and associates have found enzyme-mediatedvitreous cross-linking and nonenzymatic glycation in thediabetic vitreous, and they have suggested that the abnor-mal cross-linking might affect the collagen structure anddestabilize the attached vitreous gel, inducing maculartraction.20–22 In addition to this mechanical effect, thecellular component in the attached posterior hyaloid couldproduce growth factors capable of inducing vasopermeabil-ity (Figure 1).19
Another possible explanation for the vitreous involve-ment in diabetic macular edema is that the breakdown ofthe blood–retinal barrier results in the presence of growthfactors in the vitreous cavity which, in the presence of anabnormal attached premacular posterior hyaloid, couldconcentrate in the macular region and induce or exacer-bate the macular edema. It follows that vitreous surgerywith separation and removal of the attached posteriorhyaloid and vitreous gel theoretically could benefit thesepatients.
Based on the available data, we suggest the use of opticalcoherence tomography to test all patients with diabeticmacular traction and edema associated with posteriorhyaloidal thickening. Vitrectomy should be consideredwhen a shallow macular detachment is found. The avail-able evidence and the scientific rationale are both verysuggestive. If vitrectomy is proved to be beneficial fordiabetic macular edema, it could have a major impact onthe quality of life of numerous diabetic patients. However,the benefits of vitrectomy in this setting have not yet beenproved. Therefore, for patients with clinically significantdiabetic macular edema who have no evidence of posteriorhyaloidal traction, we strongly recommend following theguidelines of the Early Treatment Diabetic RetinopathyStudy.8
To determine the role of vitrectomy in the treatment of
FIGURE 1. Possible mechanisms responsible for diabetic mac-ular edema and traction.
AMERICAN JOURNAL OF OPHTHALMOLOGY124 JANUARY 2001

patients with diabetic macular edema, a randomized clin-ical trial should be conducted. Fortunately, we can alsoanticipate a time when diabetic macular edema will be lessprevalent. Eventually, nonsurgical methods of creating aposterior vitreous separation and pharmacologic interven-tion, such as the use of protein kinase C beta inhibitors, arelikely to decrease the incidence of clinically significantdiabetic macular edema.
REFERENCES
1. Klein R, Klein BEK, Moss SE. The epidemiology of ocularproblems in diabetes mellitus. In: Feman SS, editor. Ocularproblems in diabetes mellitus. Boston: Blackwell ScientificPublications, 1991:1–51.
2. Klein R, Klein BE, Moss SE, Cruickshanks KJ. The Wiscon-sin epidemiologic study of diabetic retinopathy XV: thelong-term incidence of macular edema. Ophthalmology1995;102:7–16.
3. Javitt JC, Canner JK, Sommer A. Cost effectiveness ofcurrent approaches to the control of retinopathy in type Idiabetes. Ophthalmology 1989;96:255–264.
4. Aiello LP, Bursell SE, Clermont A, et al. Diabetes 1997;46:1473–1480.
5. Antonetti DA, Barber AJ, Khin S, Lieth E, Tarbell JM,Gardner TW, and the Penn State Retina Research Group.Vascular permeability in experimental diabetes associatedwith reduced endothelial occludin content. Diabetes 1998;47:1953–1959.
6. Gardner TW, Lesher T, Khin S, Vu C, Barber AJ, BrennanWA. Histamine reduces ZO-1 tight junction protein expres-sion cultured retinal microvascular endothelial cells. Bio-chem J 1996;320:717–721.
7. Hikichi T, Fujio N, Akiba J, Azuma Y, Takahashi M,Yoshida A. Association between the short-term naturalhistory of diabetic macular edema and the vitreomacularrelationship in type II diabetes mellitus. Ophthalmology1997;104:473–478.
8. Early Treatment Diabetic Retinopathy Study ResearchGroup. Photocoagulation for diabetic macular edema. EarlyTreatment Diabetic Retinopathy Study Report No. 1. ArchOphthalmol 1985;103:1796–1806.
9. Lewis H, Abrams GW, Blumenkranz MS, Campo R. Vitrec-tomy for diabetic macular traction and edema associated with
posterior hyaloidal traction. Ophthalmology 1992;99:753–759.
10. Nasrallah FP, Jalkh AE, Van Coppenolle F, et al. The role ofthe vitreous in diabetic macular edema. Ophthalmology1988;95:1335–1339.
11. Harbour JW, Smiddy WE, Flynn HW, Rubsamen PE. Vit-rectomy for diabetic macular edema associated with a thick-ened and taut posterior hyaloid membrane. Am JOphthalmol 1996;121:405–413.
12. Yang CM. Surgical treatment for severe diabetic macularedema with massive hard exudates. Retina 2000;20:121–125.
13. Gandorfer A, Messmer EM, Ulbig MW, Kampik A. Resolu-tion of diabetic macular edema after surgical removal of theposterior hyaloid and the inner limiting membrane. Retina2000;20:126–133.
14. Tachi N, Ogino N. Vitrectomy for diffuse macular edema incases of diabetic retinopathy. Am J Ophthalmol 1996;122:258–260.
15. Ikeda T, Sato K, Katano T, Hayashi Y. Vitrectomy forcystoid macular edema with attached posterior hyaloid mem-brane in patients with diabetes. Br J Ophthalmol 1999;83:12–14.
16. Ikeda T, Sato K, Katano T, Hayashi Y. Attached posteriorhyaloid membrane and the pathogenesis of honeycombedcystoid macular edema in patients with diabetes. Am JOphthalmol 1999;127:478–479.
17. Otani T, Kishi S. Tomographic assessment of vitreous surgeryfor diabetic macular edema. Am J Ophthalmol 2000;129:487–494.
18. Kaiser PK, Riemann CD, Sears JE, Lewis H. Macular tractiondetachment secondary to posterior hyaloidal traction is thecause of syndrome: diabetic macular traction and edemaassociated with posterior hyaloidal traction. Am J Ophthal-mol 2000.
19. Jumper MJ, Embabi SN, Toth CA, McCuen BW, HatchellDL. Electron immunocytochemical analysis of posterior hy-aloid associated with diabetic macular edema. Retina 2000;20:63–68.
20. Sebag J, Buckingham B, Charles MA, Reiser K. Biochemicalabnormalities in vitreous of humans with proliferative dia-betic retinopathy. Arch Ophthalmol 1992;110:1472–1476.
21. Sebag J, Nie S, Reiser K, et al. Raman spectroscopy of humanvitreous in proliferative diabetic retinopathy. Invest Oph-thalmol Vis Sci 1994;35:2976–2980.
22. Sebag J, Balazs EA. Pathogenesis of CME: Anatomic consid-erations of vitreoretinal adhesions. Surv Ophthalmol 1984;29(suppl):493–498.
EDITORIALVOL. 131, NO. 1 125





























