Embed Size (px)
Citation preview

The Role & Overlap of Brain Injury in
Victims & Offenders
Liz Gerdeman, MA, CBIS-T
Director of Professional Programs, BIAC
303.562.3298
© 2019 Brain Injury Alliance of Colorado

Acquired Brain Injury
Traumatic Brain Injury
External Forcesex: assault, fall,
blast injury, motor vehicle accident
Non Traumatic Brain Injury
Internal Event ex: stroke, tumor, lack of oxygen,
infection
© 2019 Brain Injury Alliance of Colorado

Mechanism of Injury
Bony ridges Anoxia:
A loss of oxygen to the brain caused by
an airway obstruction due to choking,
strangulation, near drowning or drug
reactions.
Stroke:
Traumatic Brain Injury Non Traumatic Brain Injury
© 2019 Brain Injury Alliance of Colorado

© 2019 Brain Injury Alliance of Colorado

Classification of TBI Severity
Mild – Loss of consciousness 0-30 minutes
(Concussion)
Moderate – Loss of consciousness 30 minutes to 24hrs
Severe – Loss of consciousness for over 24 hours
© 2019 Brain Injury Alliance of Colorado

• Children 0 to 4 years, older adolescents aged 15 to 19 years,
and adults 65 years+ are most at risk
• Males are almost twice as likely to sustain a TBI as females
• Falls are the leading cause of TBIs in the United States
(globally, motor vehicle accidents are #1)
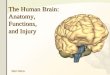
TBI Statistics
In 2013, 2.8 million TBIs
occurred in the U.S.
47%
14%
11%
13%
15%
Falls
Motor Vehicle Traffic
Assault
Unknown/Other
Struck By/Against
© 2019 Brain Injury Alliance of Colorado

Over 500,000 adults in Colorado have sustained a brain injury
• Colorado ranks 9th in the nation of fatalities and 13th in the nation of hospitalizations due to a TBI
• Almost 5,000 individuals are hospitalized and nearly 1,000 die due to a TBI in Colorado each year
• 23,500 emergency room visits each year are due to a TBI
• Males are twice as likely to sustain a TBI in Colorado as females
• The age groups with the highest risk of sustaining a TBI in Colorado are 15-24 and 65+
• Each year, 2,200 individuals continue to experience disability one year after hospitalization for a
TBI
The number of people with TBI who are not seen in an emergency department or who receive no care is
unknown.
Traumatic Brain Injury National Data Center
Colorado Data
© 2019 Brain Injury Alliance of Colorado

“Mild” TBI: Complications
>75% of TBIs are mild. MTBI symptoms may appear mild, but can lead to significant,
life-long impairment affecting an individual’s ability to function physically, cognitively, and
psychologically
• Symptoms may be subtle
– 90% of concussions are not associated with a loss of consciousness
– Concussive symptoms may develop over days or even months later
• Treated in non-hospital setting, not in ED, or not treated at all
– 90% of mTBI may go unreported
– Often not visible on CT scan or MRI
• Brain Injury can mirror other disabilities
• Individuals with a history of concussion are at an increased risk of sustaining a subsequent concussion
© 2019 Brain Injury Alliance of Colorado

Signs & Symptoms
Thinking/
Remembering
Difficulty thinking
clearly
Feeling slowed
down
Difficulty
concentrating
Difficulty
remember new
information
Physical Headache
Fuzzy or blurry
vision
Nausea or
vomiting (early
on)
Dizziness
Sensitivity to noise
or light
Balance problems
Feeling tired,
having no energy
Emotional/
Mood
Irritability Sadness More emotional Nervousness or
anxiety
Sleep Sleeping more than
usual
Sleeping less than
usual
Trouble falling
asleep
Difficulty
maintaining deep
sleep
© 2019 Brain Injury Alliance of Colorado

• Rehabilitation– Physical Therapy
– Occupational Therapy
– Speech/Language Pathologist: Cognitive Therapy
• Independent Living Skills
• Medication– Pain management
– Physical symptoms (e.g., headaches, seizures, attention, fatigue)
– Mental health
• Complimentary and Alternative Modalities
How is brain injury “treated”?
© 2019 Brain Injury Alliance of Colorado

• Functional abilities (physical, cognitive)
• Neurological changes: self awareness, cognition, communication, emotional regulation,
cognitive fatigue, hypersensitivity, executive functioning
• Life roles as worker, spouse, lover, friend, parent, sibling, authority figure, student…
• Responsibilities as bread winner, role model, support to others (emotional, work, home,
parenting, etc.), driving
• Social network of friends/family
• Self-esteem
• Intimacy
A Multitude of Loss
risk for homelessness
risk for substance abuse
risk for criminal activity
risk for mental health issues
© 2019 Brain Injury Alliance of Colorado

Almost half of adults with TBI who have no pre-injury history of mental health problems develop
mental health problems after the TBI (Gould, Ponsford, Johnston, & Schonberger, 2011. Psychological Medicine, 41, 2099-2109.)
1/3 of TBI survivors experience emotional problems between 6 months and a year post injury
Patients who reported:
• Hopelessness 35%
• Suicidal ideation 23%
• Suicide attempts 18%
85% of survivor families report that emotional or behavioral problems have an impact on their function
Suicidal ideation can be 7x higher in people with TBI than in those without
• Attempts of suicide post-TBI can be at rates close to 17%
• Increased suicide risk persists up to 15 years post-injuryFazel, et al. 2014. JAMA Psychiatry, 71(3), 326-33.; Mackelprang et al., 2014. Am J Public Health, 104(7), e100; Simpson & Tate, 2007. Brain Inj., 21(13-14), 1335-51.
Mental Health Fallout
© 2019 Brain Injury Alliance of Colorado

Brain Injury & Substance Use/Abuse
Why would TBI be association with substance abuse disorders?
1. Intoxication causes TBI
2. Early life TBI predispose to substance abuse
3. Structural damage from TBI changes behavioral control
© 2019 Brain Injury Alliance of Colorado

Brain Injury & Violence
Violence is one of the leading causes of brain injury in the United States
• The CDC estimates that at least 150,000 brain injury deaths, hospitalizations,
and ED visits are related to assault annually.
• Of women reporting to emergency rooms for injuries associated with
domestic violence:
– 30% reported a loss of consciousness at least once
– 67% reported residual problems that were likely brain injury related (Corrigan, 2003)
• Another study polled 99 battered women:
– 75% reported sustaining at least 1 partner-related brain injury
– 50% sustained multiple (Valera, 2003)
© 2019 Brain Injury Alliance of Colorado

Brain Injury & Violence
• Women experience about 4.8 million intimate partner-
related physical assaults and rapes every year
• Less than 20 percent of battered women sought
medical treatment following an injury
• Leaving an abuser: economic, emotional barriers and
BI can reduce planning, organizing, and memory skills
needed to leave
© 2019 Brain Injury Alliance of Colorado

Brain Injury & Victimization
✓ Difficulty with anger management, which may prompt others to use undue physical
force or inappropriate medication
✓ Misperceptions may lead to treatment that is demeaning or abusive
✓ TBI outcomes affect others’ perceptions of a person’s ability to honestly and
accurately report an incident of victimization
✓ Persons with TBI or other disabilities may experience physical and sexual violence,
emotional abuse, or neglect by a caregiver
✓ A TBI can cause cognitive problems that reduce one’s ability to perceive,
remember, or understand risky situations that could lead to an incident of physical
or sexual violence
✓ May engage in at-risk drinking or drug use that place them in situations or
relationships that lead to episodes of victimization
✓ Uninhibited behaviors that lead to risky sexual engagement
© 2019 Brain Injury Alliance of Colorado

Specific Challenges
Skills that may be needed
• Identifying that a plan to leave is needed
• Planning/remembering a sequence of actions
• Contacting community resources
• Finding a new place to stay
• Getting money needed
• Packing in secret
• Keeping plan a secret
• Making sure new place is safe
• Anticipating consequences
Skill deficits that are common
• Generativity can be impaired
• Ability to imagine other options
• Initiating and planning action sequences is impaired
• Initiating contact with resources
• Organization, prioritizing tasks
• Remembering details
• Impulse control
• Tendency to “blurt things out”
• Keeping secrets difficult
• Ability to infer others’ intentions
• Social judgment to assess safety
• Weighing benefits/risks impaired
• Depression and/or anxiety may immobilize the individual
• Difficulty with self initiation may prevent action steps needed
• Poor self awareness may limit the individual’s ability to change approach taken
• Cognitive difficulties serve to maintain depression/anxiety
© 2019 Brain Injury Alliance of Colorado

Brain Injury & PTSD
• Brain injuries are often sustained during traumatic
experiences
• Range of co-morbidity that exist with both TBI and PTSD
(depression, chronic pain, etc.)
• Evidence that people can develop PTSD following severe
brain injury even when traumatic event can not be recalled
“The period of greatest psychological exposure is in reality the period of
greatest traumatic exposure” – Judith Herman
© 2019 Brain Injury Alliance of Colorado

Brain Injury & Offenders
• Recent meta-analytic review found the prevalence of TBI in
the offender population to be 60.25% (Shiroma, Ferguson, &
Pickelsimer, 2010) vs. 8.5% general population report a history of
TBI (Wald, Helgeson, & Langlois, 2008)
• One meta-analysis found that approximately 30% of
juvenile offenders have sustained a previous brain injury (Vaughn, Salas-Wright, Delisi, & Perron, 2014)
• TBI is associated with higher impulsivity, aggressive
behavior and negative emotion ratings (Farrer, Frost, & Hedges,
2013)
© 2019 Brain Injury Alliance of Colorado

Colorado Data
Childhood
Violence
Adult
Victimization
Suicide
Attempts
School
Suspensions
Substance
Abuse
Mental Health
60% 62% 39% 54% 93% 75%
• 4-year federal grant; screened over a thousand of offenders across 18
judicial sites
• Those that screened positive for history of brain injury & cognitive
impairment also had co-occurring diagnoses:
© 2019 Brain Injury Alliance of Colorado

Encounters with authority can be made worse by…
• An invisible injury
• Stress
• Flooding
• Confabulation
• Symptoms that mirror intoxication
© 2019 Brain Injury Alliance of Colorado


Sensory-
Motor
Attention

What does brain injury “look” like?
Impaired AttentionThe ability to sustain focus on the information
necessary for learning or completing a task.
• Fidgets, squirms in seat, can’t sit
still
• Interrupts conversation
• Low frustration tolerance
• Talks Excessively
• Off topic
• Impulsivity
(inability
to inhibit)Memory
Sensory-
MotorInhibitionAttention
Processing
Speed
Language
Processes
Learning
Processes
Visual-
Spatial
Processes
Social
Emotional
Competency
Executive
Functions
Achievement/
Cognitive
Ability/
Reasoning

Accommodations for Impaired Attention
• Check to make sure there is good eye contact
• Be okay with redirecting
• Work on only one task at a time – check in regularly
• Keep instructions brief, simple, & to the point
• Have client participate in discussion & development of plan
• Reduce distractions, meet in quiet environment
• Use cue words to alert the client to pay attention (“look”,
“listen”)
• Establish nonverbal cueing system (eye contact, touch)

What does brain injury “look” like?
Delayed Processing SpeedHow quickly information is received, processed, and/or
outputted.
• Slow to respond to questions
• Appears to not be paying attention
• Looks confused
• Doesn’t follow instructions
MemorySensory-
MotorInhibitionAttention
Processing
Speed
Language
Processes
Learning
Processes
Visual-
Spatial
Processes
Social
Emotional
Competency
Executive
Functions
Achievement/
Cognitive
Ability/
Reasoning

Accommodations for Delayed Processing Speed
• Provide additional time to review information
• Speak slowly, making sure client understands – ask them to
rephrase back to you what they heard
• Offer assistance with completing forms
• Utilize checklists and a written schedule of routines
• Provide written cues for organizing (“first do this, then do
this”)

What does brain injury “look” like?
Short Term Memory LossThe mental ability to store and retrieve words, facts,
procedures, skills, concepts and experiences.
• Can’t remember more than one
thing at a time
• Can’t remember details
• Appears disorganized
• Appears to have an “attitude”
problem
• Appears
manipulative
MemorySensory-
MotorInhibitionAttention
Processing
Speed
Language
Processes
Learning
Processes
Visual-
Spatial
Processes
Social
Emotional
Competency
Executive
Functions
Achievement/
Cognitive
Ability/
Reasoning

Accommodations for Short Term Memory Loss
• Repeat information and summarize
• Provide written summary – cue them to record important
information (dates, action items)
• Review new information frequently
• Teach client to use reminder system like planner
• Teach “chunking” as a way to aid in retention
• Stick to routine as much as possible
• Keep information tangible and relevant
• Practice & reinforce strategies until they become automatic

What does brain injury “look” like?
Impaired Sensory Motor SkillsPerceiving and responding to what is seen, heard,
smelled, tasted, felt and touched.
• Appear overwhelmed
• Emotionally melt down
• Irritable, short fused
• May appear oppositional
• Shuts down
MemorySensory-
MotorInhibitionAttention
Processing
Speed
Language
Processes
Learning
Processes
Visual-
Spatial
Processes
Social
Emotional
Competency
Executive
Functions
Achievement/
Cognitive
Ability/
Reasoning

Accommodations for Impaired Sensory Motor
• Keep environment quiet
• Keep noise and lights to a minimum
• Keep sessions short to minimize onset of headaches and
fatigue
• Schedule rest periods and breaks from planned activities
• Consider time of day (mornings are often better)
• Ask client where in the room they’d prefer to sit or what
other accommodations they might need

What does brain injury “look” like?
Language (social pragmatics)Verbal and nonverbal rules of social language and
interactions.
• Do not interpret body language
• Use inappropriate eye contact
• May get in your space
• May either say too little or too
much
• Have little insight or
awareness of how their
behavior may
be inappropriateMemory
Sensory-
MotorInhibitionAttention
Processing
Speed
Language
Processes
Learning
Processes
Visual-
Spatial
Processes
Social
Emotional
Competency
Executive
Functions
Achievement/
Cognitive
Ability/
Reasoning

Accommodations for Social Pragmatics
• Provide direct, structured and concrete feedback
• Do not rely on body language to convey a message
• Role play
• Videotaping interactions

What does brain injury “look” like?
Language (Receptive)Ability to understand what is being said.
• Confused
• May say “huh” frequently
• Followers
• Struggle with abstract
language/sarcasm
• May withdraw
MemorySensory-
MotorInhibitionAttention
Processing
Speed
Language
Processes
Learning
Processes
Visual-
Spatial
Processes
Social
Emotional
Competency
Executive
Functions
Achievement/
Cognitive
Ability/
Reasoning

Accommodations for Receptive Language
• Be direct
• Avoid abstract humor, sarcasm, metaphors, colloquialisms,
etc.
• Allow wait time for person to process what has been said
• Provide instructions/directions slowly and one at a time
• Ask if it would be helpful to repeat or rephrase your
message
• Let the individual know that you value their input, thoughts,
and feelings

What does brain injury “look” like?
Language (Expressive)Ability to be understood.
• Poor grammar or immature speech
• Difficult to follow in conversation
• Difficulty staying on topic
• Difficulties navigating
social rules
• May withdraw
MemorySensory-
MotorInhibitionAttention
Processing
Speed
Language
Processes
Learning
Processes
Visual-
Spatial
Processes
Social
Emotional
Competency
Executive
Functions
Achievement/
Cognitive
Ability/
Reasoning

Accommodations for Expressive Language
• Redirect if the individual is off topic
• Provide opportunities to practice expression
• Role play common real life conversations
• Teach individual to rehearse silently before replying
• Be patient and allow person time to respond

What does brain injury “look” like?
Executive Function: InitiationAbility to start an action or activity
• Appears lazy or spacey
• Appears unmotivated
• Follower
• Needs constant cuing
• Lags in independent
living skills
MemorySensory-
MotorInhibitionAttention
Processing
Speed
Language
Processes
Learning
Processes
Visual-
Spatial
Processes
Social
Emotional
Competency
Executive
Functions
Achievement/
Cognitive
Ability/
Reasoning

Accommodations for Initiation Deficits
• Encourage client to focus on one step at a time
• Ask client to repeat instructions to ensure comprehension
• Use underlining and highlighting for significant parts of
directions. Checklists & calendars can help organize.
• Break complex directions into simple steps and assign
action items
• Utilize color-coding
• Help the person get started
• Repeat instructions or interventions multiple times in
different ways

What does brain injury “look” like?
Executive Function: Mental
FlexibilityAbility to easily shift from one idea, train of thought,
activity or way of looking at things to another.
• Perseverate
• Difficulties taking feedback
• Resistant
• Can appear stubborn or
argumentative
• May appear to
lack empathy
MemorySensory-
MotorInhibitionAttention
Processing
Speed
Language
Processes
Learning
Processes
Visual-
Spatial
Processes
Social
Emotional
Competency
Executive
Functions
Achievement/
Cognitive
Ability/
Reasoning

Accommodations for Mental Flexibility Deficits
• Suggest arriving at appointments/meetings early
• Develop and practice routines & plan ahead for changes in
routines
• Prepare for transitions
• Help develop alternative plans
• Assist in prioritizing goals, breaking them down into
smaller tangible tasks
• Provide respectful feedback to potential or obvious problem
areas

What does brain injury “look” like?
Executive Function: ReasoningDeliberate and controlled mental operations to solve
novel and on the spot problems.
• Concrete thinkers
• Can’t think of alternative solutions
• Difficulties answering open ended
questions
• Difficulties learning from
experience, cause and effect
MemorySensory-
MotorInhibitionAttention
Processing
Speed
Language
Processes
Learning
Processes
Visual-
Spatial
Processes
Social
Emotional
Competency
Executive
Functions
Achievement/
Cognitive
Ability/
Reasoning

Accommodations for Reasoning Deficits
• Point out possible consequences of decisions, short- & long-
term (“Is this a good idea? What might happen? Is this
consistent with your goals?”)
• Teach step by step approach to problem solving
• Avoid open-ended questions
• Speak concretely
• Be clear on expectations and consequences of risk taking
behaviors
• Be supportive and continually identify strengths

What does brain injury “look” like?
Emotional/BehavioralThe awareness of social, emotional and behavioral self-
regulation, control and monitoring.
• Over/under reaction
• Difficulties with anger management
• Melt down
• Can appear emotionally “flat”
• Difficulties making friends
• Can appear
argumentative
MemorySensory-
MotorInhibitionAttention
Processing
Speed
Language
Processes
Learning
Processes
Visual-
Spatial
Processes
Social
Emotional
Competency
Executive
Functions
Achievement/
Cognitive
Ability/
Reasoning

Accommodations for Emotional/Behavioral
Challenges
• Minimize anxiety with reassurance, education, and structure.
• Avoid focusing only on individual’s deficits
• Promote self awareness by stopping and addressing
undesired behavior immediately
• Don’t interpret lack of emotion as a sign of lack of interest.
• Suggest breaks if the individual becomes irritable or
agitated.
• Mindfulness exercises to aid clients in accurately identify
internal emotional states: progressive relaxation, body scans,
deep breathing exercises
• Practice positive social interactions. Provide alternative
comments or choices that could have been made

BIAColorado.org • (303) 355-9969
Skill vs. Will

Key Concepts
• Brain injury may present medically, but often, and more
importantly, behaviorally
• Accommodate and create simple strategies for the
behaviors (do not feel like you need to “treat” the injury)
• Consider first if the individual is capable of doing
something, as opposed questioning their willfulness
© 2019 Brain Injury Alliance of Colorado

Screening and Identification

Importance of Screening for Brain Injury
One study found that 42% of persons who indicated they had incurred a TBI as defined by
the CDC did not seek medical attention (Corrigan & Bogner, 2007)
• Brain injury increases risk for problem behaviors & re-offending (Williams, Mewse, Tonks,
Mills, Burgess & Cordan, 2010)
• Clients may be eligible for support services (BIAC)
• Psychotherapies can be adapted for neurocognitive deficits. Examples:
• Minimize environmental distractions
• Educational therapies (e.g. CBT, DBT) should emphasize pacing, provide frequent
opportunities for clients to respond, generate feedback, and provide reinforcement to
maintain client engagement
• Written material/handouts where possible
• Repetition of key points
• Non-electronic devices might include checklists, pictures or icons, photograph cues, post-
it-notes, calendars, planners, and journals
• Therapies should be introduced with a simple rationale
© 2019 Brain Injury Alliance of Colorado

Components of Screening
• Education / awareness
• Training regarding the sequelae of brain injury
• Important to have a foundational knowledge of brain injury
• Training should be provided to anyone conducting intake/screening
• Medical documentation
• Best practice
• Important to note that medical documentation only indicates an injury not impact
• Documentation should be from a clinician trained in diagnosing TBI
• Establishing credible history
• Assessing impact
• Modifying/generating novel interventions
© 2019 Brain Injury Alliance of Colorado

Screening Tools
• Screening tools must be:
– Valid and reliable
– Sensitive to the population
– Appropriate to the setting
• Resources– Brain Check Survey (http://www.lobi.chhs.colostate.edu/survey.aspx)
– Brain Injury Screening Questionnaire
– OSU TBI-ID
(www.ohiovalley.org/informationeducation/screening/)
© 2019 Brain Injury Alliance of Colorado



Resources
• BIAColorado.org
• CraigHospital.org
• TBI Toolkit: http://www.mirecc.va.gov/visn19/tbi_toolkit/
• Brainline.org
© 2019 Brain Injury Alliance of Colorado

Funds from surcharges on convictions of speeding tickets,
DUI, DWAI, & the children’s helmet law
Community
Grants
Research
GrantsServices
CO Department of Human Services
• Resource navigation for youth & adults with brain injury
• Specialized support & consultation about school-related
issues for children/youth with brain injury
• Brain injury specific classes and workshops
• Trainings to community providers about brain injury and
resources © 2019 Brain Injury Alliance of Colorado

Brain Injury Alliance of ColoradoThe go-to resource for help and services for survivors of an injury to the brain, their
families, and providers.
BIAC is a statewide nonprofit dedicated to helping all persons with a brain injury thrive in their community
– Core service is resource navigation for all ages – this is free, with no income or insurance eligibility criteria
– Brain injury specific conferences & workshops
– Online educational materials for survivors, family, & professionals
– Statewide brain injury professional networking groups
– Adaptive recreation programs, music & art therapy classes
– Emergency utility assistance through Energy Outreach Colorado
– Online resource directory specific to brain injury providers
– Statewide support groups
– Member of United States Brain Injury Alliance
© 2019 Brain Injury Alliance of Colorado

Resource Navigation
Resource Navigation is our foundational support program
for survivors, family members, and caregivers. It is
intended to be quick and easy to access.
All ages can access this free support.
Examples of support:
•Finding medical providers
•Understanding brain injury
•Filling out paperwork
•Connecting to community-based resources
•Problem-solving
How to connect:
•Online Referral Form: https://biacolorado.org/referral/
•Email: [email protected]
•Phone: 303.355.9969, toll-free 1.800.955.2443
© 2019 Brain Injury Alliance of Colorado

Self-management/Skill-building• Designed for survivors who want to invest time in improving their
skills in specific areas that can be challenging after a brain injury.
• BIAC Advisors work one-on-one with each participant to assess their
strengths & weaknesses, identify natural supports in their life, &
develop strategies for building specific skills with the goal of greater
self-sufficiency.
• Six-month program, average of 4 hours per month
• Participants will have regular homework outside of meetings with
their Advisor which will be reviewed each time they meet.
Areas of focus for Self-management:
• Communication
• Scheduling/Planning
• Prioritization/Organization
How to apply:
If you are a survivor interested in participating in the Self-management Program, please contact BIAC
to request an application: [email protected] or 303.355.9969, toll-free 1.800.955.2443© 2019 Brain Injury Alliance of Colorado

BIAC has a Youth Education Liaison specialist on staff who
provides free, statewide consultation and support services to
children and youth, aged 0-21, with a documented brain injury.
Examples of support:
• Providing parent/guardian education of services and
programming options available in schools
• Assisting in the partnership between parents and schools
• Educating parents and school teams on how a student has been
impacted by their brain injury
• Collaborating with schools on intervention planning
• Attending transition, IEP, MTSS, and other planning meetings
• Partnering with hospitals to help with transition to school
• Any other student specific educational
needs/concerns/questions
Education Consultation
How to apply:
If you are a parent or professional working with a child or youth with brain injury, please contact BIAC to request an
application for education consultation: [email protected] or 303.355.9969, toll-free 1.800.955.2443
© 2019 Brain Injury Alliance of Colorado

The Power of Peer!
Have you ever been inspired to give back to other brain injury
survivors as someone who “has been there?” Have you ever
thought your life could improve by talking to someone that “really
understands because they know what it is like to have a brain
injury?”
The Peer Mentorship Program is looking for volunteers!
The program will span up to a year in duration, with weekly
phone or video conference contacts, and if possible a monthly
community activity (dependent upon proximity, transportation and
personal budgets). The program is designed to support survivors
explore resiliency, define what it means to thrive, and then to take
steps in this direction.
Peer Mentorship Program
If you are interested or would like to learn more, please contact:
Seija Curtin at [email protected] or 303-223-0731
© 2019 Brain Injury Alliance of Colorado

https://biacolorado.org/referral/
© 2019 Brain Injury Alliance of Colorado

Classes & WorkshopsThese activities are free, however space is limited and registration is required.
Clients in services with BIAC have priority access.
Classes
Art
Music Therapy
Adaptive Yoga
Cooking
Balance (fall prevention)
Workshops
Financial Health
Brain Injury Basics
Mindfulness
© 2019 Brain Injury Alliance of Colorado

Recreation & Social Programs
Our camps are an opportunity to build friendships; gain confidence, accomplish physical feats you
did not think possible, earn field work credits and have more fun than you thought imaginable! Partial scholarship funding awarded based on needs and availability of funds.
Contact: Linda Heesch
303-562-0401
Multi Day Opportunities:
Winter Sports: March/April
Summer Camps: June through
August
Canoe Trip: September
Creative Activities September
Day Programs:
Obstacle Course – April
Rock Climbing – May
Paddle Sports – July
Zip Line – October
Social Activities:
Movies
Sporting events
Cultural activities
© 2019 Brain Injury Alliance of Colorado

© 2019 Brain Injury Alliance of Colorado


http://cokidswithbraininjury.com

Please see our website for more information:
BIAColorado.org
Thank you for your time!
Questions? Comments?
Feedback?
BIAColorado.org • (303) 355-9969
© 2019 Brain Injury Alliance of Colorado