Embed Size (px)
Citation preview

The sequential estimation of plasma catecholamines
and whole blood histamine in myocardial infarction
John Gri’ths, B.Sc., M.B., B.Ch., F.C.S.C.C., F.I.M.L.T. Fred Leung, Ph.D.
Vancouver, B. C., Canada
G azes, Richardson, and Woods,’ using the ethylenediamine fluorometric
method of Weil-Malherbe, examined the plasma of 13 patients with myocardial in- farction. Levels were taken at random within the first 36 hours and again after 72 hours. Initially, mean elevations of norepi- nephrine approximately twice the normal levels were found, with mean epinephrine elevations of approximately three times normal. At the end of 72 hours, norepineph- rine levels had returned to the quoted normal for their method, but epinephrine had remained approximately double the normal. There was no attempt to correlate cardiac dysrhythmias with raised catechol- amine levels in this study.
Although several workers2e3 have re- ported increased urinary catecholamine levels after myocardial infarction, a decade appears to have passed before McDonald and associates,4 using the trihydroxyindole fluorometric method of Anton and Sayre, further investigated plasma catechola- mines. In a series of 50 patients with myo- cardial infarction they noted a significant increase in the mean plasma level of nor- epinephrine compared with that of normal control patients. The level of epinephrine in both groups of patients, however, was similar. Further correlation with respect
to cardiac dysrhythmias was made; it indi- cated that patients with atria1 or ventricu- lar dysrhythmias in the first five days fol- lowing infarction had higher norepineph- rine concentrations than those patients without dysrhythmias or with ventricular dysrhythmias occurring after five days from the onset of infarction.
In relating whole blood histamine levels to myocardial infarction, there appears to be a single paper by Kipshidze and Bari- ghyan5 These authors, using a biological assay with guinea pig small intestine, studied levels in man following myocardial infarction. They noted elevations up to ten times normal and related these in- creased levels to the development of both chest pain and hypotension.
The present study endeavored to assess sequential changes for 24 hours in plasma catecholamines and whole blood histamine in patients with myocardial infarction.
Methodology
Subjects. Twenty-five men aged 29 to 68 (mean 56) years, who had been admitted to cardiac intensive care units in the hos- pitals in the Vancouver area with recent myocardial infarction, were investigated.
The presence of myocardial infarction was substantiated in all cases by electro-
From the Division of Clinical Chemistry, Vancouver General Hospital, Vancouver, B. C., Canada. Received for publication Oct. 8, 1970. Reprint requests to: Dr. J. Griffith% Head, Division of Clinical Chemistry. Vancouver General Hospital, Vancouver 9,
B. C., Canada.
Vol. 82, No. 2, pp. 171-179 August, 1971 American Heart Journal 171

140
130
120
110
100
80
70
60
50 1
20
IO 1
110
100
90
80
70
60 1
110
100
90
80
70 1
20
10 1
IbO-
150-
140-
130-
120-
110-
ioo-
90-
80-
70-
60-
20-
10-
Systolic Blood Pressure m m m Hg
T
Syrlol~c Blood Pressure in m m Hg
1
Hew! Rate m BealrlMin.
I T T
I
Central Venous Pressure ,n cm H20
I I I 0 6 12
TIME IN HOURS
7
24
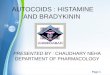
Fig. 1. Relation of central venous pressure, heart rate, and systolic blood pressure to time in the three clinically defined groups.
cardiograph (W.H.O. designation) and the characteristic pattern of evolution of the three serum enzymes, ATP :creatine phos- photransferase (2.7.3.2), L-aspartate:2-oxo- glutarate aminotransferase (2.6.1.1), and L-1actate:NAD oxidoreductase (1.1.1.27).
Group A comprised nine patients who were considered to be in clinical shock. The mean systolic pressure recorded on initial examination was 64 mm. Hg, with a range extending from 53 to 7.5 mm. Hg. The mean heart rate on initial examination was found to be 110 beats per minute, with a range extending from 104 to 116 beats per minute. The central venous pressure measured at the initial examination was found to be 15 cm. HZO, with a range ex- tending from 13 to 17 cm. HaO. The subse- quent mean and range for systolic blood pressure, heart rate, and central venous pressure are recorded in Fig. 1. The mean urine output over the first 24 hours of observation was 16.5 ml. per hour. During the 24 hour period of study, eight patients showed atria1 or ventricular dysrhythmias, and it was also noted that all patients showed evidence of skin vasoconstriction with cold, sweating extremities. Eight of the nine patients in this group received doses of morphine varying from 30 to 90 mg. in the 24 hour period of study. Seven of the nine patients in this group died.
Normal control sribjects were SO indi- Group B comprised 8 patients, but these viduals in the resling state, who were con- could not I)e considered to I)e irk clinical sidered to be average healthy persons, all shock on the basis of the criteria previousl) with a normal heart rate and blood pres- selected. The mean systolic pressure re- sure. Twenty-five persons admitted with a corded on initial examination was found to
suspicion of myocardial infarction and treated in the same cardiac intensive care units as those patients with proved infarc- tion were also studied.
Blood samples from the patients with electrocardiographically confirmed infarc- tions were taken on admission to the in- tensive care unit and at approxitnately 6, 12, and 24 hours thereafter.
These patients were divided retrospec- tively into three groups on the basis of their clinical presentation and progress. Blood samples from the patients with suspected myocardial infarction were taken approximately 24 hours after admission to the intensive care unit. Clinical shock was defined by the measurements available: a systolic blood pressure of less than 100 mm. Hg, a heart rate greater than 100 beats per minute, a urinary output of less than 20 ml. per hour, a central venous pressure greater than 15 cm. HzO, and, finally, cold, sweating extremities.

Estimation of plasma cntecholamines and histamine 173
be 86 mm. Hg, with a range extending from 72 to 100 mm. Hg. The mean heart rate on initial examination was found to be 90 beats per minute, with a range extending from 80 to 100 beats per minute. The cen- tral venous pressure measured at the initial examination was found to be 12 cm. HzO, with a range extending from 9 to 15 cm. H,O. Subsequent measurements of the sys- tolic blood pressure, heart rate, and central venous pressure are illustrated in Fig. 1. The mean urine output was 34 ml. per hour in the 24 hour period of study. During the period of study, four patients showed atria1 or ventricular dysrhythmias. Skin vasocon- striction or sweating was not noted in the eight patients. Morphine was given in doses ranging from 30 to 75 mg. in the 24 hour period of study. Two of the eight patients in this group died.
Group C comprised eight patients. The mean systolic blood pressure recorded on initial examination was found to be 124 mm. Hg, with a range extending from 114 to 134 mm. Hg. The mean heart rate on initial examination was found to be 84 beats per minute, with a range extending from 77 to 91 beats per minute. The central venous pressure measured at initial exami- nation was found to be 8 cm. HzO, with a range extending from 5 to 11 cm. H,O. Subsequent measurements of systolic blood pressure, heart rate, and central venous pressure for this group are recorded in Fig. 1. The mean urine output in the 24 hour period of study was greater than 60 ml. per hour. During the period of study one patient showed atria1 dysrhythmia. Morphine was administered to six of the eight patients in doses varying from 15 to 60 mg. over the 24 hour period. One patient in this group died.
Laboratory technique. Plasma levels of norepinephrine and epinephrine were esti- mated by a modified trihydroxyindole method which has been evaluated by studies of 50 normal subjects.6
Blood from the antecubital vein was collected in a polypropylene tube contain- ing ethylene diamine tetra-acetic acid (EDTA), the protein precipitated by per- chloric acid, and after centrifugation the catecholamines adsorbed onto aluminum oxide. Elution from the aluminum oxide
was performed with perchloric acid and the eluate centrifuged at high speed to remove the fine particles of aluminum oxide which may interfere with subsequent fluorescence. Differential analysis of norepinephrine and epinephrine was effected through the use of their optimum pH levels of 6.5 and 4.0, respectively, and by their different excita- tion and emission wavelength bands. The activation wavelengths of 380 and 425 nm. and fluorescence wavelengths of 480 and 500 nm. for norepinephrine and epineph- rine, respectively, were used. The fluores- cence of the samples was determined by the use of an Aminco-Bowman spectro- photofluorometer (American Instrument Co.), which is equipped with a xenon lamp in an off-axis ellipsoidal condensing system.
Whole blood histamine was determined by a modification of the ffuorometric pro- cedure of Anton and Sayre.’ An aliquot of the blood drawn for catecholamine estima- tion was transferred into an iced test tube. This was treated with concentrated per- chloric acid and histamine extracted from the supernatant fluid by the stated proce- dure. Fluorophor formation with orthoph- thaldialdehyde (OPT) and citric acid sta- bilization of the fluorescence intensity was performed. The fluorescence intensity of the histamine-OPT complex was measured in the Aminco-Bowman spectrophotofluo- rometer in the same manner as the catechol- amines. An activation wavelength of 358 nm. and an emission wavelength of 4.50 nm. were used.
Results
The mean levels of plasma catechol- amines established in 50 healthy subjects taken in the resting fasting state were as follows: norepinephrine, 0.24 ng. per milli- liter, with a range of 0.15 to 0.33 ng. per milliliter; epinephrine, 0.04 ng. per milli- liter, with a range of 0.00 to 0.08 ng. per milliliter. The mean level of whole blood histamine established in the same group of healthy subjects was 0.052 fig per milli- liter, with a range of 0.015 to 0.089 pg per milliliter. The levels of norepinephrine in 25 patients who had been 24 hours in the coro- nary monitor unit but did not have a clinically proven infarction were 0.29 ng. per milliliter, with a range of 0.23 to 0.35

Clinical group Epinephrine Histamirfe
(ng./nd.) 6dnll.j
A B C
Patients without myo- cardial infarction
4.1 *0.6 O.lf * 0. 10 0, 064 * 0.020 1.5 * 0.41 0, 12 + 0.06 0.056 * 0.030 0.61 * IJ ‘2 0.09 * 0.04 0, (145 * 0 035 0. 29 * 0 06 0.08 * 0.04 0.054 * 0.030
*See legend under Fig. 2 for normal resting levels.
ng. per milliliter. The mean level for epinephrine was 0.08 ng. per milliliter, with a range of 0.04 to 0.12 ng. per milli- liter. The mean level for xvhole blood hista- mine in these patients was 0.054 pg per milliliter, with a range of 0.024 to 0.084 pg per milliliter (see Table I).
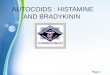
Figs. 2, 3, and 4 indicate graphically the mean plasma levels of norepinephrine, cpi- nephrine, and whole blood histamine over the 24 hour period of study for the three clinically defined groups, A, B, and C. In all groups there appears to be initial eIeva- tion at the first point of assay, but subse- quent assays indicate a progressive fall in norepinephrine and epinephrine levels over the time period studied. The whole blood histamine levels appear unchanged both on initial assay and during further assays during the period studied.
In Group A, carrving the highest mor- tality rate, there w\:js significant elevation of norepinephrine (1’ < 0.001) and also of epinephrine (P < O.OOl), but no significant elevation of whole blood histamine xvhen compared to the normal resting values. This significant elevation of norepinephrine and of epinephrine also occurs when the values are compared to the control group of patients in the cardiac monitor unit without myocardial infarction.
In Group B, with a lower mortality rate, the elevations of norepinephrine and epi- nephrine, although considerably less, were still statistically significant (I’ < 0.001) when compared to normal resting values and to the control group of patients in the intensive care unit I\-ithout myocardial
infarction. Again there was no change in whole blood histamine.
In Group C, with the lowest mortality rate, there was a progressive reduction in the mean initial plasma levels of norepi- nephrine and epinephrine, but both are statistically significant elevations (P < 0.001) when compared to normal resting values. The mean initial plasma levels of norepinephrine when compared to those of the patients without myocardial infarction show a statistically significant elevation (P < 0.001). The mean initial levels of epinephrine, however, are comparable (P < 0.01) to the elevated levels of epinephrine in the patients without myocardial infarc- tion. There was no change in the whole blood histamine in this group.
If norepinephrine levels are compared within the three clinical groups, it is found statistically (P < 0.001) that each group shows a significant elevation when com- pared to one another, and to the group of patients without myocardial infarction. For epinephrine levels, however, when the clini- cal groups are compared to one another, Group A shows a statistically significant elevation when compared to Groups R and c, whereas the recorded elevations in (Groups B and C are comparable (I’ < 0.01). If epinephrine levels in Groups R and C: are also compared with epinephrine levels in the group of patient controls in the in- tensive care unit L\-ithout myocardial in- farction, then the levels are found to be comparably elevated (I? < 0.01).
Table II relates the type of arrhythmias to tile initial mean plasn~ levels and indi-

Estimation of plasma cntecholnmines and histamine 175
i
0.5
(
- Norspinephrine .--.a Epinephrina e-4 Histamine
Ratio Ratio Ratio Ratio 5
NE-E NE-E NE-E NE-E y
15:l 18:l 15:l 13:l I
I--__ f - - c - ~----++
l - - - - - . . . . . . . . . . . . . . . . . . j . . . . . . . . . . . . . . . . . . . . . . . . . . . . . f . . . . . . . . . . . . . . . . . . . . . . : _ . . . . . . . . . . . _ . . . . _ . _ {
1 I I 0 6 12
>b4
TIME IN HOURS
Fig. 2. Group A, relation of levels of catecholamines and histamine to time over the first 24 hours. Normal resting NE, 0.24 =t 0.09 ng. per milliliter; normal resting E, 0.04 * 0.04 ng. per milliliter; normal resting hista- mine, 0.052 f 0.037 pg per milliliter.
cates the striking relationship of cardiac arrhythmias to elevations predominantly of norepinephrine but, to a lesser extent, epinephrine. In 12 of the 25 patients no significant dysrhythmias were found; atria1 dysrhythmias occurred in five, and ven- tricular dysrhythmias in eight. The five patients with atria1 dysrhythmia showed a mean initial norepinephrine level of 3.74 ng. per milliliter, with a range of 3.22 to 4.26 ng. per milliliter. The eight patients with ventricular dysrhythmia showed a mean initial norepinephrine level of 3.94 ng. per milliliter, with a range of 3.42 to 4.46 ng. per milliliter.
Discussion
Plasma levels of norepinephrine were found to be significantly elevated in the first 24 hours following myocardial infarc-
tion, the degree of elevation appearing to have prognostic significance. There was a smaller but significant increase in epineph- rine levels. There was no statistically sig- nificant increase in whole blood histamine levels. This study, therefore, reports the preferential release of norepinephrine over epinephrine in myocardial infarction, both in patients with clinical shock and in those in whom clinical shock was not defined. The degree of elevation of the catechol- amines, particularly norepinephrine, ap- pears to be related to the development of the clinical shock.
An increase in plasma catecholamine levels has been noted in many forms of shock. There have been many experimental studies (in animals) in septic shock, in hypovolemic shock, and in anaphylactoid shock. These have been fully surveyed by

Ratio Ratio Ratio Ratic NE-E NE-E NE-E NE-E 12.5:l 12.5:1 13:l 1O:l
- Norepinephrine l ...-.“* Epinephrine l ---* Histamine
TIME IN HOURS
Fig. 3. Group B, relation of levels of catecholamines and histamine to time over the Iirs;t 21 hours. See legend under I;ig. 2 for normal resting Icvels.
2 0 - Norepinsphrine
f s....--.-.. Epinephrine l/J
2 l ----* Histamine $
Z
5 Ratio Ratio Ratio Ratio 5 NE-E NE-E NE-E
Z_:
$5 6:l 7:l 6:l
NE-E fL 6:l
t:
;F 1 g?
1’ o.5: jyw@ %’
5 E--- . . . . . . . . . . . . . . . . . . . . . . . * . . . . . . . . . . . . . . . . . . . . . . . . . . . . . * . . . . . . . . . . . . . . . . . . . d,! . . . . . . . . . . . . . . . . . . . . . . f
o- I I I 0 6 12 24
TIME IN HOURS
Fig. 4. Group C, relation of levels of catecholamines and histamine to time over the first 2-L hours. See legend under Fig. 2 for normal resting levels.
Richardson8 In such studies, a definite, evolving differential release pattern of catecholamines has been noted, but this tends to vary with the species and the results obtained are difficult to compare with those obtained in man, in whom there is limited information regarding plasma catecholamines in myocardial infarction. The paper of Gazes suggests that epineph- rine is the dominant catecholamine during the period of assay extending over 72 hours, whereas McDonald suggests in single as- says that norepinephrine solely is released with no detectable elevation of epinephrine. With regard to blood histamine, the single paper of Kipshidze and Barighyan5 suggests that histamine is released and is related to the decrease of arterial blood pressure. We
have been unable to confirm the results reported by these authors. A basic differ- ence in methodology exists, in that hista- mine was assayed in the paper of Kipshidze and Barighyan5 by a biological method. In spite of reputed selective extraction of the histamine, there is reason to believe that the method may not be as specific as the fluorometric technique used in our study.
Norepinephrine and epinephrine are de- rived from phenylalanine and tyrosine in a well-defined anabolic pathway, the rate- limiting enzyme being tyrosine hydroxyl- ase.g The adrenal medulla is the major site for epinephrine biosynthesis but produces some norepinephrine also. Following forma- tion, epinephrine is stored in identifiable granules distinct from other intracellular

Volume 82 Number 2 Estimation of plasma catecholamines and histamine 177
Table II. Relation of mean initial amine concentrations with dysrhythmias
No. of fatients
Mean initial amine levels*
Norepinephrine
I
Epinephrine (W./ml.) (w/ml.)
No significant dysrhythmias 12 0.96 * 0.12 0.07 * 0.05 Atria1 dysrhythmias 5 3.74 * 0.52 0.26 * 0.11 Ventricular dysrhythmias 8 3.94 * 0.52 0.27 * 0.09
*See legend under Fig. 2 for normal resting levels.
constituents, and containing large quanti- ties of ATP in a molar ratio of about 1:4 with the catecholamines.10 It is estimated in man that cells of the adrenal medulla contain about 80 per cent epinephrine and 20 per cent norepinephrine.” Norepineph- rine biosynthesis occurs within the post- ganglionic sympathetic neurone, the amine being also stored within the cell as an identifiable granule. The ATP combina- tion, however, may not be as firm as with epinephrine, and there may be considerable norepinephrine in the cytoplasmic sap.12 Apart from the adrenal medulla, the cat- echolamine content of tissues varies greatly, with norepinephrine the predomi- nant amine.13
The reasons for the preferential release of norepinephrine reported in this study are unknown, and any comment on the mecha- nism of release must at this stage be specu- lative. A possible concept for the release of the catecholamines is discussed by Douglas.14 He suggests that following the quanta1 discharge of acetylcholine by neuro- genie impulses, a sequence of events begin- ning with the increased permeability of the outer membrane of the chromaffin cell or sympathetic neurone to calcium is initiated. The inward movement of calcium, accel- erated by a similar inward movement of potassium, activates adenosine triphospha- tase (ATPase) and releases the contents of the granule. The process of granular release requires a high energy potential, whereas the catecholamine release from the cyto- plasmic sap is probably achieved by simple diffusion with little or no energy require- ment. Euler’” has shown that the release of catecholamines is much faster from the nerve granule than from the granule of
adrenal origin. In vitro, at 37” C., nerve granules release half their norepinephrine in six to eight minutes, while those from the adrenal medulla take about 100 minutes for similar quanta1 release. Euler further showed that local acidosis would consider- ably enhance the rate of release. Another possible source of the predominantly nor- epinephrine elevation, at least in the initial phase, is the myocardium with its rich sympathetic innervation. It is calculated that each gram of myocardium contains 0.64 pg of norepinephrine. The release of norepinephrine is presumably initiated by acute tissue hypoxia.
The emotional response to the stress of myocardial infarction and subsequent treat- ment in an intensive care unit may be con- sidered to be responsible for some of the catecholamine release. That noted in those patients without myocardial infarction but subjected to the stress of hospitalization in the intensive care unit appears to be one of epinephrine rather than norepinephrine. McDonald4 noted a similar epinephrine re- lease phenomena in six patients undergoing cardiac catheterization, and Levi16 has shown in studies with subjects undergoing stress with emotional disturbances the re- lease, as reflected in urinary catecholamines, to be predominantly epinephrine.
A major mechanism of removal from the plasma is reuptake by the granule. Iversen17 has shown that uptake by the medullary granule is slow compared with that of the nerve granule, but there may be also two different uptake mechanisms for exogenous norepinephrine dependent on the circu- lating norepinephrine concentration. Mc- Donald4 has suggested that epinephrine release is short lived, possibly inferring that

the useful half-life of epinephrine may l)e less than that of norepinephrine, yielding more readily to catabolism by monoamine oxidase and catechol-@methyl transferase enzyme system.
The effect of morphine given to the majority of patients in this study must also be considered. Cairnie and colleagues’” sug- gested by indirect experiments that mor- phine prevented the release of norepineph- rine from the postganglionic neurones. However, Gunnel@ administered increasing doses of morphine to rats, then estimated their catecholamine secretion in urine. There was a prompt increase in both cate- cholamines, the rise maintaining the normal ratio of norepinephrine to epinephrine-. norepinephrine being the dominant amine if the dose of morphine were small. With large doses of morphine the epinephrine levels showed a marked rise, exceeding those of norepinephrine.
The relationship of elevated catechol- amine levels to atria1 and ventricular dys- rhythmias is of particular significance, al- though the mechanism of action is not clear. Oppenheimer2O induced experimental myo- cardial infarction in dogs. He noted that in the group previously given reserpine there was an almost complete absence of ven- tricular fibrillation when compared to the control group, the members of which had not been given reserpine. This observation suggests that catecholamines play an im- portant role in the production of the ventricular arrhythmias.
The mechanism for the fall in both catecholamines in the 24 hour study period is unknown. In the more severe cases it may be due to initial degranulation of the nor- epinephrine-epinephrine stores without re- synthesis of the amines in unfavorable cel- lular conditions such as marked acidosis. This could cause inhibition of the rate- limiting enzyme. In those with response to treatment, stabilization of the factors caus- ing release may be an effective reason for the decline in amine levels.
Our findings in respect to the catechol- amines confirm in part the recent work of McDonald,4 particularly with norepineph- rine levels. The levels of epinephrine found in our series did not exceed 0.29 ng. per milliliter and are comparable to those
quoted by McDonald who, however, (quotes the normal mean epinephrine at 0.25 ng. per milliliter. This is approximately five times that quoted by other authors \vho have determined plasma levels.6,21-“R
Considering the inconsistent and unpre- dictable alterations in the hemodynamics of the macrocirculation following myocar- dial infarction, these studies are but pre- liminary communications. It is obvious that there are many complex changes occurring, of which epinephrine and norepinephrine are but part. The relationships between plasma or tissue kinins and catechola- mines,24 and between kinins, catechola- mines, and 5hydroxytryptaminez5 require further considerable investigation.
Summary
Plasma norepinephrine and epinephrine, together with whole blood histamine, were measured at six-hour intervals for a total period of 24 hours after proved myocardial infarction.
The values obtained were compared to resting levels in 50 healthy subjects with a mean heart rate of 72.4 beats per minute and a mean systolic blood pressure of 114 mm. Hg, and to 25 patients with a mean heart rate of 76.2 beats per minute and a mean systolic pressure of 122 mm. Hg. These were patients who were in the cardiac intensive care unit but in whom a diagnosis of myocardial infarction was not sub- stantiated.
Norepinephrine levels were significantly higher in the patients with proved myo- cardial infarction, the mean initial reading being up to sixteen times the matched rest- ing levels, whereas epinephrine levels showed a relatively smaller increase initially --up to five times the matched resting levels. A similar elevation was noted in the patients with proved myocardial infarction when compared to those patients in the cardiac intensive care unit in whom a diag- nosis of myocardial infarction was not con- firmed. The degree of initial elevation appears to have prognostic significance in spite of a gradual decrease in the 24 hour period of study. The degree of initial ele- vation also appears to be associated with atria1 or ventricular dysrhythmias. The levels of \vhole blood histamine remained

volume 82 Number 2 Estimation of plasma catecholamines and histamine 179
within normal limits irrespective of clinical status. It is concluded that the response of the three vasoactive compounds studied to confirmed myocardial infarction was pre- dominantly the release of norepinephrine.
The considerable technical assistance from Miss Po-Hing Leung is acknowledged, and grateful thanks are expressed to Dr. John A. Osborne, Director of Cardiology at Vancouver General Hospital, and to Dr. Henry S. Ballon for their advice and encourage- ment during the period of this study.
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
REFERENCES
Gazes, P. C., Richardson, J. A., and Woods, E. F.: Plasma catecholamine concentrations in myocardial infarction and angina pectoris, Circulation 19:657, 1959. Forssman, O., Hansson, G., and Jensen, C. C.: The adrenal function in coronary thrombosis, Acta Med. Stand. 142:441. 1952. Valori, C., Thomas, M., and Shillingford, J. P.: Free noradrenaline and adrenaline excretion in relation to clinical syndromes following myocardial infarction, Amer. J. Cardiol. 20:605, 1967. McDonald, L., et al.: Plasma catecholamines after cardiac infarction, Lancet 2:1021, 1969. Kipshidze, H. H., and Barighyan, H. K.: Blood histamine in acute myocardial infarction, Ter. Arkh. 39~78, 1967. Griffiths, J., and Leung, F.: The fluorometric determination of plasma catecholamines in the normal human, Clin. Chim. Acta 30:2, 1970. Anton, A. M., and Sayre, D. F.: A modified fluorometric procedure for tissue histamine and its distribution in various animals, J. Pharma- col. Exp. Ther. 166:285, 1969. Richardson, J. A.: Catecholamines in shock, in Mills, L. C., and Moyer, J. H., editors: Shock and hypotension, New York, 1965, Grune & Stratton, Inc. Levitt, M., et al.: Elucidation of the rate limiting step in norepinephrine biosynthesis in the perfused guinea pig heart, J. Pharmacol. Exp. Ther. 148:1, 1965. Hillarp, N.-A., Hogberg, B., and Wilson, B.: Adenosine triphosphate in the adrenal medulla, Nature 176:1032, 1955. Callingham, B. A.: in Gray, C. H., and Bach-
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
arach, A. L., editors: Hormones in blood, New York, 1967, Academic Press, Inc., vol. 2. Euler, U. S., and Lishajko, F.: Noradrenaline re- lease from isolated nerve granules, Acta Physiol. Stand. 51:193, 1961. Iversen, L. L.: Uptake and storage of norepi- nephrine in sympathetic nerves, London, 1967, Cambridge University Press. Douglas, W. W.: The mechanism of release of catecholamines on the adrenal medulla, Phar- macol. Rev. 18:471, 1966. Euler, U. S.: Some facts affecting catecholamine uptake, storage and release in adrenergic nerve granules, Circ. Res. 20, 21 (Suppl. III):S, 1967. Levi, L.: Emotional stress and biochemical re- actions, Excerpta Medica International Con- gress Series, No. 182, 1968. Iversen, 1~. L.: Uptake of norepinephrine by the isolated perfused rat heart, Brit. J. Pharmacol. 21523, 1963. Cairnie, A. B., Kostalitz, H. W., and Taylor, D. S.: The effect of morphine on some svmoa- thetically innervated effkctors, Brit. J. ‘Phar- macol. 17:539, 1961. Gunne, L.-M.: The excretion of noradrenaline and adrenaline in the urine of rats during chronic morphine administration, Psycho- pharmacologica 2:214, 1961. Oppenheimer, M. J., et al.: Useof reserpine in the analysis of the mechanism of cardiogenic shock, in Mills, L. C., and Moyer, J. H., editors: Shock and hypotension, New York, 1965, Grune & Stratton, Inc. Haggendal, J.: The presence of conjugated adrenaline and noradrenaline in human blood plasma, Acta Physiol. Stand. 59:242, 1963. Price, H. L.: Estimation of epinephrine and norepinephrine concentrations in human plasma by the trihydroxyindole method, Pharmacol. Rev. 11:273, 1959.
Klensch, H.: Studies on adrenaline and nor- adrenaline in human plasma, Pflueger Arch. Physiol. 290:218, 1966. Feldberg, W., and Lewis, G. P.: The action of peptides on the adrenal medulla. Release of adrenaline by bradykinin, J. Physiol. 171:98, 1964. Peltona, P.: Release of serotonin during brady- kinin infusion, Stand. J. Clin. Lab. Invest. 24(Suppl.): 107, 1969.