Embed Size (px)
Citation preview
The search for new ways of treating Alzheimer’s disease
Written by: M.N. de BruinStudentnumber: 3007936Examiner: R.S. Oosting
Introduction
In 1906 the first case of a peculiar dementia was reported by Alois Alzheimer, a dementia that therefore later would be known as Alzheimer’s disease (AD) [1]. Alzheimer found “miliary foci” and neurofibrillary changes in the cerebral cortex of this female patient after death and correlated these findings with the cognitive and behavioral features the patient displayed during her life [1]. In the last couple of decades, more advanced scientific techniques and better genetic insights have given a better understanding of which pathological processes take place when patients suffer from AD. Biomarkers to detect AD pathology can nowadays be identified more easily, and among others have led to the finding that pathological changes in patients with AD can be seen 10 to 20 years before the onset of dementia [2]. However, more than a century later there is still no treatment for AD, be it delaying its onset or improving cognitive functioning. With the increasing knowledge about AD, more possibilities of finding a treatment will arise as well. Since the number of patients suffering from AD (already having an estimated prevalence of 30 million worldwide) is expected to quadruple in the next 40 years, many studies are currently being done in the hopes of finding this urgently needed treatment [2].
To gain a better understanding of the working mechanisms of drugs being researched for Alzheimer’s disease, the pathological progress of the disease will first be reviewed.
Amyloid-β
When looked at the brain of a patient suffering from Alzheimer’s disease at microscopic level, amyloid plaques, neurofibrillary tangles (NFTs) and extensive neuronal loss can be seen [3]. Amyloid plaques are accumulated molecules, residing in the extracellular spaces of the brain. The plaques mainly consist of the Amyloid-β (Aβ) peptide, a peptide derived from the much larger amyloid precursor protein (APP) [4,5]. Within these plaques the Aβ-peptide is present in aggregated forms such as fibrils and oligomers [6,7]. The Aβ plaques are surrounded by swollen and degenerating neurites. In the same areas gliosis occurs. This inflammatory response might contribute to the brain injury seen in AD patients [8,9].
Within APP, three major sites appear where proteolysis occurs [2]. The three proteases responsible for this proteolysis are α-, β- and γ-secretase. The most dangerous form of AB is the Aβ(1-42) peptide, formed by cleavage of APP at a γ-secretase action site. Although the Aβ(1-42) peptide is not the most present form of Aβ in tissues and body fluids, it is more hydrophobic and likely to aggregate, and therefore appears to play an important part in initiating Aβ-aggregation [2,10,11]. Missense mutations in APP at the action site of β- and γ-secretase lead to familiar AD (FAD) or a disease with cerebrovascular plaques and cerebral hemorrhage [12-19]. When mutations occur adjacent at the γ-secretase action site, near the C-terminal of the Aβ -peptide, it leads to an increased amount of Aβ42 compared to Aβ40, without having an influence on the overall amount of Aβ [20,21]. Another mutation, discovered in a Swedish family in which development of AD was hereditary, occurring near
the β-secretase action site of APP leads to an increase of all forms of Aβ [22]. This mutation likely leads to cerebrovascular plaques as well as AD [23,24]. Individuals with Down syndrome (which have an extra chromosome 21) and from families having a duplication of part of chromosome 21 (one which must contain the APP gene) also develop AD, supporting the idea that increased production of Aβ leads to the disease [25]. Some mutations of APP occur in the Aβ-peptide itself. Different mutations reside at the C-terminal to the α-cleavage site and are responsible for making the Aβ more likely to oligomerize, fibrillize or be cleared less effective [18,19,26]. Another mutation is responsible for deletion the amino acid in place 22 in the Aβ-peptide, making the peptide highly fibrillogenic [27,28]. The exact function of APP is still unclear, but evidence suggests it plays a role in axonal pruning and neuronal migration during nervous system development and contributes in cognitive functions such as learning and memory [29-31]. Other evidence shows that Aβ production is regulated by neuronal activity itself [32,33]. Some experimental models show that some forms of Aβ even suppress neuronal activity by interacting with glutamate receptors [34]. When it is clear that APP and Aβ are needed for the brain to normally function, targeting one or both therapeutically would be a major challenge [2].
FAD is not only caused by mutation in the gene coding for APP, but also by mutations in two other genes, namely presenilin-1 (PSEN-1) and presenilin-2 (PSEN-2). Both presenilins are involved in forming γ-secretase and thus important for the generation of Aβ [35-38]. Since APP is not the only protein cleaved by γ-secretase, research with γ-secretase inhibitors has failed to show that these inhibitors can be used as a safe way to inhibit Aβ generation as a treatment for AD [39-42].
Tau
NFTs, neuritic dystrophy and neuropil threads are developed by nerve cell bodies, as by their processes [43]. The NFTs and neuropil threads are mainly composed of a protein called tau, which in AD is present as a hyperphosphorylated aggregated form [44-47]. Tau normally functions as a microtubule-binding protein which is produced in all neurons and is also present in glia. When tau becomes hyperphosphorylated, like when happens with AD, it self-aggregates and dissociates from the microtubules, leading to the NFTs and dystrophic neuritis seen in patients suffering from AD. The aggregates, due to their high B-sheet conformation, ultra-structurally appear as paired helical filaments [48].
It is likely that the aggregation, conformation change and buildup of different kinds of Aβ play a central role in starting the pathogenesis of AD and directly damage the brain. Evidence however suggests that the pathology of tau is important for the clinical progression of AD. This may partly be due pathways downstream of the Aβ -protein pathway, although evidence has also been found supporting the idea tau can cause brain damage independently of Aβ [49]. The cognitive dysfunction seen in patients with AD comes from disruptions of networks connections between specific brain areas of the limbic system and areas of the neocortex [50]. For the main part, Aβ and tau pathology reside at different places in the brain, nonetheless there is clear evidence both pathways have an influence on each other. Tau and Aβ aggregates seem to be able to spread from one brain region to other brain regions, and from cell to cell, in
a way such as prions do [51-54]. If the spreading of these proteins plays a role in the progression of AD, new drugs targeting this mechanism may be researched as a treatment for the disease [2].
Neurotransmission
Apart from the forming of plaques and NFTs there is loss of synapses and selective neuronal cell death, accompanied by a decrease in markers for certain neurotransmitters [55]. The neurons that are most affected by AD are neurons that use glutamate as a neurotransmitter. Patients suffering from AD show (little) symptomatic improvements when given memantine. Memantine modulates the NMDA receptor, which is a subtype of glutamate receptors [56]. Noradrenergic and cholinergic neurons are also affected by AD. Cholinergic neurons are believed to be involved in attention and memory, and therefore are the reason centrally active drugs inhibiting cholinesterase (the enzyme responsible for breaking down acetylcholine) have been developed [57,58]. However, these drugs also only show symptomatic improvements in patients suffering from AD [59].
Genetics
Mutations in genes other than earlier specified can lead to a greater risk of developing non-familiar AD [60-65]. The biggest risk comes from a mutation in the gene coding for Apolipoprotein E (Apo-ε). People carrying the ε3 allele of Apo-ε have a decreased chance of developing AD, whereas people carrying the ε4 allele have a threefold higher chance of developing AD [66,67]. Some of the risk alleles discovered play a role in lipid biology, where Apo-ε also mainly exhibits it’s function, although it’s exact function in normal and disease conditions remains unknown [68-70]. Other risk alleles are involved with immune responses or processes in the cell membrane, such as endocytosis [2]. These findings may suggest that a broader spectrum of causes is involved with the development of AD, than Aβ and tau pathophysiology.
Insulin
A novel theory is that AD might be caused by defects in insulin signaling in the brain. AD is associated with a decreased level of insulin in the cerebrospinal fluid and a decline in insulin receptor expression, which indicates an impaired transport of insulin into the brain [71-73]. The impaired transport might then ultimately lead to decreased activation of glucose transporters and therefore lead to glucose hypometabolism, decrements in mitochondrial metabolism and ATP production [74]. Higher glucose levels in the brain might lead to an increase of advanced glycation end products and the toxic effects that come with them [75]. Defects in insulin signaling could lead to an increase of GSK-3β activity, a kinase responsible for the phosphorylation of tau [73,75]. GSK-3β might also enhance γ-secretase activity, leading to higher intracellular levels of Aβ [76,77]. Another way in which insulin might have influence on the pathophysiology of AD is by a decreased activity of insulin-degrading enzyme (IDE). IDE is responsible for breaking down extracellular substrates such as insulin and Aβ [78,79]. It has been made clear that IDE activity is indeed negatively correlated with Aβ(1-42) peptide levels [80]. Since most of these features are also present in patients
suffering from diabetes mellitus, it is no wonder AD is now also called diabetes mellitus type 3 [81].
Inflammation
In patients suffering from AD gliosis is a common feature. Many activated microglia and astrocytes are found near Aβ plaques and neurons, together with increased expression of several pro-inflammatory cytokines [82-86]. This inflammatory reaction probably is due to the presence of Aβ and NFTs and leads to necrosis of neurons in the vicinity [87.88]. Aβ might induce a positive feedback loop by interacting with cytokines. The secretion of IL-8 and IL-6 can for instance be potentiated by Aβ [89]. By interacting with astrocytes, Aβ can mediate the release of several chemokines and cytokines [90]. Although activation of microglia contributes to the pro-inflammatory reactions seen in AD, in some situations the activation of microglia is beneficial. Activation of microglia leads to neuronal growth factors and enhances phagocytosis of Aβ-plaques [91,92].
Influencing Aβ generation and damage
“Notch-sparing” γ-secretase inhibitors
Although inhibition of γ-secretase seems like a viable method to stop Aβ-generation, most clinical trials looking at inhibition of γ-secretase have failed to show satisfactory results in trying to treat AD this way. Problems mainly arise because γ-secretase inhibitors also prevent γ-secretase from cleaving Notch, which is another transmembrane protein. Skin tumor progression and worsening of cognitive tasks was the result when Notch could not be cleaved in animal models [93,94]. This led to the development of “Notch-sparing” γ-secretase inhibitors such as BMS-708163 (avagacestat) and EVP-0962 [95,96]. BMS-708163’s selectivity for APP over Notch was assessed in each of the 4 human Notch proteins. The Notch2 protein showed the lowest ratio of 1:33, showing BMS-708163 is much more selective for APP [97]. Tests in healthy human volunteers, together with toxicity studies in rats and dogs, showed that a dose of BMS-708163 between 25mg and 50mg could be administered to decrease Aβ generation dependent on dose, without causing too many serious side effects [97].
Additionally, when different doses of BMS-708163 were given as a single dose in other clinical trials, only the highest dose (800mg) showed some inhibition of Notch-related plasma biomarkers [98]. Higher discontinuation rates were however seen at doses of 100mg or higher because of adverse effects, that could likely be the result of the cleaving of Notch [99]. It therefore remains to be seen if the biomarkers used to screen for Notch-related adverse effect are suitable. Furthermore, BMS-708163 might not be as selective as was thought. BMS-708,163 binds directly to the presenilin-1 N-terminal fragment. Other pan-γ-secretase inhibitors are able to challenge this binding, whereas γ-secretase modulators can’t. The binding of four different active site-directed γ-secretase photo-affinity probes was blocked by

BMS-708163, making it possible that this compound is an allosteric non-selective γ-secretase inhibitor having the same adverse effects as other γ-secretase inhibitors [100].
EVP-0962 is currently being investigated in a Phase II clinical trial, after successful preclinical and Phase I studies [101]. During this study, four doses of EVP-0962 administered once daily for 14 days will be researched. Safety, tolerability, pharmacokinetics and cerebral Aβ levels will be evaluated in either healthy volunteers, patients suffering from mild cognitive impairment or patients suffering from early AD. EVP-0962 lowered Aβ(1-42) levels, reduced Aβ-plaque formation, attenuated memory deficits and was well tolerated in a transgenic mouse model [96]. However, data from the Phase I clinical trial remains unpublished so far.
BACE-inhibitors
Because of the many side effects seen in trials with γ-secretase inhibitors, other ways to reduce the amount of Aβ generated were explored. An attractive method to do this is by inhibiting another secretase: the β-secretase. The gene coding for this enzyme (BACE1) has been cloned, and mice lacking this enzyme produce very low levels of Aβ [102,103]. β-secretase has fewer known substrates than γ-secretase, which supports the idea that use of β-secretase will lead to fewer side effects. Although BACE1 knockout mice did have defects in peripheral nerve myelination, β-secretase inhibitors still remain attractive drugs to treat AD therapeutically [104].
A clinical Phase I study was performed with AZD3839, which is such a novel BACE1 inhibitor small molecule. The structure of AZD3839 was found using fragment-based screening and structure based design. In biochemical fluorescence energy transfer assays AZD3839 showed to inhibit BACE1 activity, with a 14-fold higher selectivity for BACE1 than BACE2 and with over a thousandfold higher selectivity for the aspartic protease cathepsin D. Furthermore, soluble APP and Aβ(1-40) release was tested in SH-SY5Y cells. Aβ(1-40) release was also tested in N2A cells and primary neurons from both mouse and guinea pig. All releases were inhibited by AZD3839 in a concentration dependent matter. Further testing in vivo (mouse, guinea pig and non-human primate) revealed AB-levels in plasma, brain and cerebrospinal fluid were lowered after administration of AZD3839 in a dose- and time-dependent matter after. Pharmacokinetic and –dynamic analyses of the results obtained with primary cortical neurons and the results obtained with in vivo- testing showed a good correlation between the potency of AZD3839 in the primary cortical neurons and brain effects seen in vivo [105]. These results combined make AZD3839 a promising candidate for treating AD. However, results from the clinical trial have yet to be published.
Another compound, AZD3293, which is also a BACE1 inhibitor, is currently being studied in several clinical trials (preclinical data is not published). A phase I study looking at safety and efficacy of AZD3293 has been set up wherein healthy elderly volunteers receive ascending doses of AZD3293 starting with 5mg. Patients suffering from mild to moderate Alzheimer’s disease then receive 1 or up to 3 dosage levels of AZD3293 [106]. The second Phase I trial that is being commenced uses both young and elderly healthy Japanese volunteers. In the first part of the study young volunteers will receive a single dose of 15, 50 or 150mg of AZD3293. If the safety and tolerability is confirmed in this part of the study, the study moves onto the
second part. In this part elderly volunteers either receive a single dose of 15 or 50mg of AZD3293, or multiple ascending doses. Next to safety and tolerability pharmacokinetics and pharmacodynamics will also be evaluated [107]. The last study currently being performed with AZD3293 is another Phase I clinical trial and looks at the effects of AZD3293 on CYP3A4 metabolism [108]. This study consists of three groups, testing effects of AZD3293 together with either itraconazole, diltiazem (which are both known for their CYP3A4 inhibiting activity) or midazolam (which is a CYP3A4 substrate)[109-111] . The first group of volunteers participating in this study will receive a fixed dose of AZD3293 on the first day. From day 5 on itraconazole will be administered twice daily for 9 consecutive days. On the 8 th
day, AZD3293 will be administered as one single dose. With this dosing regimen the effect of CYP3A4 inhibition on AZD3293 metabolism can be assessed. The second group of this study will receive diltiazem instead of itraconazole, with the same dosing regimen. The third group of volunteers participating in this study will receive a fixed dose of midazolam on the first day. From day 5 on AZD3293 will be administered twice daily for 9 consecutive days. On the 8th day, midazolam will be administered as one single dose. With this dosing regimen the effect of AZD3293inhibition on CYP3A4 metabolism can be assessed.
A third BACE inhibitor being studied in clinical trials is MK-8931. Although preclinical and clinical data has not yet been published, two clinical trials have currently been set to study safety and effects of MK-8931 in larger patient groups. The first clinical trials is a Phase II/III clinical trials wherein patients suffering from mild to moderate AD receive a tablet of MK-8931 once daily for 78 weeks (12, 40 or 60 mg) [112]. The other clinical trial looks at efficacy and safety of 12 or 40mg administered once daily for 104 weeks in patients with prodromal AD [113].
Immunotherapy
Another way in which the damaging Aβ might be cleared from the brain is with immunotherapy [114]. This can be done by direct immunization, active immunization or passive or passive immunization. With direct immunization, synthetic Aβ(1-42) peptides are directly delivered to the patients. Preclinical research in mice showed that Aβ levels indeed can be reduced via this way, with a decrease in Aβ neuropathology and cognitive improvement [115]. Active immunization can be achieved by conjugating synthetic Aβ fragments to a carrier protein and delivering this to the patients. With passive immunization the patient receives monoclonal antibodies against Aβ [114]. Preclinical research showed that a humoral response alone can reduce amyloid burden, and improve cognitive functioning without a cellular response, making passive immunization a promising way to clear Aβ from the brain [116].
The first drug developed as an active immunization to treat AD was AN1792. The Phase II clinical trial was however terminated after 6% of the patients suffered from meningoencephalitis due to a high T-cell response [114,117]. CAD106 was hereafter developed, consisting of a short N-terminal fragment of Aβ(1-6) combined with a virus-like particle. Phase I studies showed a smaller T-cell response with CAD106 treatment than with AN1792 treatment [118]. Phase II studies with CAD106 have been completed, but data has so
far not yet been published. ACC-001 was developed with the same idea as CAD106, but uses a protein carrier as conjugate that is injected intramuscular instead of a virus-like particle. Like CAD106, treatment with ACC-001 did not lead to a harmful T-cell response at preclinical stages [119]. There are currently three clinical trials ongoing investigating ACC-001, all being Phase II studies. One study is a long term extensions study looking to the effects of ACC-001, alone or in combination with QS-21, which enhances the ability of the immune system to respond to antigens, on safety tolerability and immunogenicity in patients suffering from mild to moderate AD [120]. The second study is comparing two doses of ACC-001(3 or 10 µg), both administered with QS-21 also in patients suffering from mild to moderate AD. Safety and efficacy of both doses will be assessed in this study [121]. The third study has the same set up as the second, with the only difference being that patients suffer from early AD, instead of mild to moderate [122].
Phase III clinical trials with bapineuzumab, which was the first passive immunization drug developed to treat AD, were terminated after bapineuzumab failed to improve cognitive functioning [123]. Another monoclonal antibody developed as a treatment for AD is solanezumab. Solanezumab (being a humanized monoclonal IgG1 antibody) binds to soluble Aβ(13-28), where bapineuzumab was more selective for fibrillar Aβ-plaques. The Phase I clinical trial with solanezumab showed treatment with solanezumab had fewer side effects than treatment with bapineuzumab, something that was confirmed in the Phase II clinical trial [124,125]. After Aβ(1-42) plasma levels were increased after treatment with solanezumab in the Phase II clinical trial, two Phase III trials were set up [125,126]. Both trials didn’t meet their endpoint when they were analyzed separately. However, when data from both trials were pooled together, and patients were categorized in Apo-ε4 carriers or non-carriers, a reduction in cognitive decline was seen [126]. With the first two Phase III clinical trials being only mildly encouraging, a third Phase III clinical trial has been set up in order to see if treatment with solanezumab will slow the cognitive and functional decline compared with placebo in patients suffering from mild AD [127]. At the same time patients from the earlier Phase III clinical trials will still be monitored for any safety effects [128].
BAN2401 is also a humanized monoclonal antibody, but differs from solanezumab by selectively binding to Aβ protofibrils. A Phase II clinical trial has been set up to study the safety, efficacy and tolerability of BAN2401 in patients suffering from early AD. Patients will receive 2,5mg, 5mg or 10mg twice a week for 18 months or 5mg or 10mg monthly for 18 months administered as a 60-minute intravenously infusion [129]. Data from earlier studies has not yet been published.
Another monoclonal IgG1 antibody currently being investigated in clinical trials is BIIB037 and is fully human. BIIB037 is selective for fibrillar Aβ and reduced Aβ-levels in animal brains (data not published). One Phase I study is looking at the safety and tolerability of a range of doses of BIIB037 intravenously administered as single doses in patients suffering from mild to moderate AD [130]. The other Phase I study is investigating the pharmacodynamics, pharmacokinetics, safety and tolerability of BIIB037 when administered intravenously in a multiple dose regimen [131].

Gantenerumab is yet another IgG1 antibody developed to treat AD that is fully human. Gantenerumab binds to fibrillar Aβ, whereby the initial contact of gantenerumab with Aβ is with its N-terminal, followed with the binding of adjacent central Aβ. At the preclinical stage of development, gantenerumab reduced Aβ-plaque load in mice. In these mice it only targeted Aβ in the brain without interfering with Aβ from the plasma. As another benefit, no antibodies against the drug itself were present after treatment with gantenerumab for five months [132]. The Phase I clinical trial showed gantenerumab indeed reduced Aβ-burden in patients suffering from mild to moderate AD. Due to the small population of patients in this trial, effects on cognitive functioning could however not be studied efficiently [133]. Three clinical trials with gantenerumab are therefore currently being performed. The first is a Phase I clinical trials where multiple doses of gantenerumab are given to Japanese patients suffering from mild to moderate AD. Three different doses are hereby tested every 4 weeks during 24 weeks. Safety, tolerability, pharmacokinetics and preliminary pharmacodynamics will be assessed [134]. The second clinical trial is to compare the effects of gantenerumab to solanezumab treatment in patients with an autosomal dominant AD. The primary outcome of this Phase II/III clinical study is fibrillar Aβ deposition at baseline and after two years of treatment [135]. The third clinical trial is a Phase III study looking at the effects of gantenerumab on cognition and functioning, together with pharmacokinetics and safety, in patients suffering from prodromal AD, wherein patients receive 105mg or 225mg of gantenerumab subcutaneously every 4 weeks for 104 weeks [136].
Crenezumab is a monoclonal antibody against Aβ with an IgG4 backbone. The idea is to limit the release of inflammatory cytokines while stimulating amyloid phagocytosis to reduce side effects such as vasogenic edema. Crenezumab recognizes aggregated Aβ (oligomeric and fibrillar) as well as Aβ-plaques [137]. A Phase II extension study has been set up, in which patients suffering from mild to moderate AD that enrolled in Phase I clinical trials, are given crenezumab to assess its long-term safety and tolerability [138]. Another Phase II clinical trial looks at the effects of crenezumab in patients carrying the PSEN1 autosomal mutation on safety and efficacy compared to placebo [139].
With TTP4000, a fusion was created between the ligand binding domains of IgG and RAGE (a receptor for advanced glycation end products). As mentioned earlier advanced glycation end products can lead to neuronal damage. Since Aβ also binds to RAGE, and via this way can be removed together with glycation end products, this method of passive immunotherapy is very promising. Animals treated with TTP4000 did indeed have a smaller amyloid burden in the brains which was associated with cognitive improvement [140]. A Phase I clinical trial is being performed to assess the safety, tolerability, pharmacokinetics and immunogenicity of two doses of TTP4000 (1mg/kg or 3mg/kg administered subcutaneously) in patients suffering from mild to moderate AD [141].
Influencing PPARγ and RXR
In cell cultures peroxisome proliferator-activated receptor γ (PPARγ) agonists have been seen to reduce the amount of Aβ production. They do so in several ways. Firstly, APP expression will be down-regulated [142]. Secondly, the effect of certain cytokines on β-secretase
expression is diminished by PPARγ activation [143,144]. Thirdly, PPARγ induces Apo-ε expression together with the retinoid X receptor (RXR), which in turn leads to a higher breakdown of Aβ [145,146]. Genistein has been shown to increase the promotor activity of PPARγ and is therefore being investigated in a clinical trial where it is given as a dietary supplement for 180 days to patients suffering from AD [147]. In preclinical studies, genistein was indeed able to improve cognitive functioning in rats [148]. Genistein will be compared with placebo, with Aβ as primary outcome [149]. Bexarotene, on the market as an anticancer drug, is an RXR agonist and in one study showed promising effects on Aβ clearance from the brains of mice and their cognitive functioning [150]. This led to the Phase II clinical trial that is currently being performed wherein patients suffering from mild to moderate AD are given bexarotene to assess its safety and efficacy [151]. Several research groups have however tried to replicate the findings found in the earlier preclinical, but found different results. Two of the studies did see a decrease in soluble Aβ and an improvement of cognitive functioning, but none of the studies did see a reduction of Aβ plaques [152-155].
Inhibiting Fyn
Aβ in the brain can active the kinase Fyn [156]. When Fyn gets activated, it is able to phosphorylate the NR2B-subunit of the NMDA receptor. This in turn leads to enhanced signaling of this receptor, possibly leading to excitotoxicity and the neuronal damage seen in AD patients [157]. Being a substrate for Fyn as well, deficits in tau phosphorylation might be caused by this very kinase [156]. For this reason a Phase I clinical trial investigating safety and tolerability of AZD0530, which inhibits Fyn, in AD patients has been set up [158].
Blocking calcium channels
In a preclinical study nilvadipine enhanced Aβ clearance from the brain and restored cortical perfusion in an AD mice model [159]. In a female patient suffering from early AD both global and regional cerebral blood flow increased after three months of treatment with nilvadipine. Cognitive functioning was hereby also slightly increased [160]. Because nilvadipine is normally used as a treatment for hypertension which might be a safety risk in AD patients, a study has been carried out in which 56 AD patients received nilvadipine to assess safety and tolerability with blood pressure as an outcome [161]. Since nilvadipine was well tolerated in this study, a Phase III clinical trial has been set up to see if 18 months of treatment with nilvadipine can improve cognitive functioning in a larger patient group suffering from mild to moderate AD [162].
Blocking β-adrenergic transmission
Carvedilol, which is already on the market as a treatment for hypertension, was able to improve cognitive functioning and reduce Aβ levels in the brain in two independent AD mouse models. Neuronal transmission was hereby significantly improved [163]. For this reason, a Phase IV clinical trial has been set up, to see if six months of treatment with carvedilol will improve cognitive functioning of AD patients when compared to placebo. As a second outcome CSF Aβ levels will be measured at the beginning, halfway during and at the end of the study [164].
Influencing tau
Inhibiting aggregation
Since treatment with drugs influencing Aβ generation and damage has not been as effective as was hoped, research groups have turned to other possible ways to treat AD [165]. One such way is by inhibiting the aggregation of tau proteins. Two Phase III studies are being performed in which the safety and efficacy profile of TRx0237 (leuco-methylthioninium: a tau-aggregation inhibitor) is being investigated. One study investigates the drug profile in patients suffering from mild Alzheimer’s disease; the other investigates the drug profile in patients suffering from mild to moderate Alzheimer’s disease [166,167]. Success was already seen in a Phase II trial where methylioninium was shown to have beneficial effects on the progression of mild to moderate Alzheimer’s disease. However, there were problems with the bioavailability of methylioninium. TRx0237 is the reformulated form of methylioninium to increase this bioavailability [168].
Immunotherapy
Like with Aβ, immunotherapy has been proposed as a method to remove misfolded tau proteins from the brain. AADvac1 is such a vaccine targeted at pathologically misfolded tau-proteins that is currently being studied in a 3-month long Phase I trial to assess its safety and tolerability profile [169]. The vaccine consists of a genetic determinant which is a synthetic peptide derived from a tau protein sequence, coupled to keyhole limpet homecyanin to induce an immune response, with aluminum hydroxide as an adjuvant. After completion of this study participants will be monitored for 18 months to assess long-term safety [170].
Inhibiting microtubules
Although not directly targeted at tau, TPI-287 is currently being studied for its effects and safety in patients with mild to moderate Alzheimer’s disease. It exerts its action by inhibiting microtubules [171]. Since tau binds these microtubules an effect will likely be seen.
Influencing neurotransmission
Influencing cholinergic transmissions
Nicotine and nicotinic agonists improve learning and cognitive functioning. Recent study showed both α4β2 and α7 nicotinic receptors are important for memory function [172]. This is the reason agonists for these receptors have been developed in the hopes of treating diseases like AD. Currently, the effects, safety and tolerability of AZD3480 (also called ispronicline) are being investigated in patients suffering from mild to moderate Alzheimer’s disease. AZD3480 is a selective agonist of the central α4β2 and α2β2 neuronal nicotinic cholinergic receptors [173]. Earlier study showed however that AZD3480 did not improve ADAS-Cog score of Alzheimer’s disease patients compared to placebo [174]. It therefore remains

controversial if AZD3480 would provide benefits when used as a treatment for Alzheimer’s disease.
EVP-6124 is an α7 selective nicotinic cholinergic receptor partial agonist currently being investigated in a Phase III clinical trial [175]. The theory behind the treatment is that when EVP-61242 and acetylcholine bind with the α7 receptor it cognition of the patient will be enhanced. By sensitizing the α7 receptor with EVP-6124, less acetylcholine will be needed at a later stadium for the same cognitive effect [176]. Preclinical and clinical data are very promising with a significant improvement on cognitive function [176]. The safety and efficacy of EVP-6124 is being evaluated in a Phase II clinical trial as well [177]. In this study patients suffering from mild to moderate Alzheimer’s disease are treated with either a high or low dose of EVP-6124. The efficacy is assessed by looking at the ADAS-Cog-13 scale.
In another phase II study, ABT-126, having the same working mechanism as EVP-6124, is being studied for safety and efficacy in patients suffering from mild moderate AD and already receive stable doses of acetylcholinesterase inhibitor treatment [178].
Inhibiting cholinesterase
Cholinesterase inhibitors were among the first of treatments for AD. Although cholinesterase inhibitors were not as effective as was hoped; they are still being improved and researched. Bisnorcymserine is a butynylcholinesterase inhibitor that is currently being tested in adult healthy volunteers for safety and efficacy at Phase I [179]. The theory is that when acetylcholinesterase inhibitors stop working, bisnorcymserine might increase acetylcholine in the brain, leading to improved cognitive functioning [180].
Influencing monoamine oxidation
Monoamine oxidase is a mitochondrial enzyme catalyzing the oxidation of monoamines such a dopamine, serotonin and norepinephrine. Two different types of these enzymes are present in the brain: MAO-A and MAO-B. Although monoamine oxidation is essential for correct functioning of neurotransmission, neurotoxic chemical species are byproducts of this oxidation [181]. Excessive activation of MAO might therefore lead to neuronal damage. Because many side effects were seen in patients receiving a-selective MAO-inhibitors, attention was directed to the development of selective MAO-inhibitors [182,183]. MAO-A inhibitors tend to have antidepressant effects, whereas MAO-B inhibitors are more neuroprotective. The Mayflower Road study is studying RO4602522, which is a novel orally active MAO-B selective inhibitor currently being investigated in patients suffering from moderate AD. Patients getting background therapy of acetylcholinesterase inhibitors, alone or in combination with at least 4 months of memantine treatment will either receive one of two possible doses of RO4602522 or placebo to evaluate the efficacy and safety of RO4602522 in this Phase II clinical trial [184].
Low dose administration of ladostigil is currently being evaluated in a Phase III clinical trial in patients with mild cognitive impairment [185]. Ladostigil combines the mechanism of action older drugs such as rasagiline and rivastigmine in the hopes of being a better treatment
for Alzheimer’s disease [186]. It acts as a cholinesterase and butynylcholinesterase, and after chronic treatment also MAO-A and MAO-B. Ladostigil may induce neurogenesis and reverse some of the damage seen in Alzheimer’s disease, making it more of a cure than most other treatments seen that are mostly symptomatic [187]. Early memory loss in patients suffering from mild cognitive impairment might be averted, thus not leading to more serious cognitive dysfunction.
Glutamate-induced excitotoxicity
Since glutamate-induced excitotoxicity is thought to be one of the causes of brain damage in Alzheimer’s disease, riluzole is currently being investigated in a Phase II clinical trial for beneficial cognitive effects [188]. Riluzole is a glutamate-modulating agent reducing excitotoxicity and has already proved to be safe in the treatment for amyothrophic lateral sclerosis (ALS) [189].
Serotonergic transmission
Lu AE58054, a potent 5-HT6-receptor antagonist, is being studied as an adjunctive therapy to donezapil in order to improve the cognitive function of patients suffering from mild to moderate Alzheimer’s disease in two Phase II clinical trials [190,191]. In a preclinical study, Lu AE58054 attenuated the effects of phencyclidine and in this way cognitive functioning in a schizophrenia rat model [192]. Another Phase II clinical trials studies Lu AE58054 as adjunctive therapy next to acetylcholine esterase inhibitors [193].
Gene therapy
One Phase II study is currently being carried out using gene therapy. An adeno-associated virus delivery of Nerve growth factor (NGF) is being injected in the brain in the hopes of protecting nerve cells from damage and dying. This treatment is called CERE-110 with the study being carried out in mild to moderate Alzheimer’s disease patients [194]. Preclinical studies showed that NGF deficits can indeed lead to the abnormalities in tau and Aβ physiology seen in AD patients [195,196].
Attenuating insulin signaling
When insulin is present in the brain at optimal levels, it enhances memory, facilitates plasticity and is protective. When insulin levels are too low or when there’s a shortage of insulin activity cognitive impairment arises. Insulin modulates the level of Aβ and protects neuronal synapses from the negative effects of Aβ oligomers. Patients suffering from diabetes type 2 have a 2-fold risk of developing AD compared to healthy people. These factors show insulin is important in AD progression [71].
Resensitizing the brain to insulin
Improving cognitive function or slowing cognitive decline might be done by resensitizing the brain for insulin. A new class of drugs, glucagon-like peptide-1 receptor agonists, might be beneficial. These drugs act by mimicking the GLP-1 hormone, which helps to produce insulin [197]. A couple of drugs have been looked at for beneficial effect in AD. Liraglutide has been shown to have neuroprotective potential in preclinical studies and does so by ameliorating tau hyperphosphorylation and insulin signaling [198-200]. A Phase II clinical trial is being carried out wherein patients receiving liraglutide are being evaluated for its safety and efficacy [201].
Another drug in this class, exendin-4, also improved cognitive function in mice, as well as normalized insulin signaling [202].The efficacy and safety of exendin-4 is also being studied in a Phase II clinical trial in patients with early AD [203].
NIC5-15, which is already being investigated as a treatment for diabetes, is another insulin-sensitizing agent, but one of which the working mechanism is still unknown [204]. Preclinical studies showed NIC5-15 is also a Notch-sparing g-secretase inhibitor, but that doses needed to stop accumulation of Aβ were too high compared to the doses used in studies investigating the effects of NIC5-15 in diabetes patients (data not published) [205]. A Phase II study has therefore been set up to investigate the effects of on mild to moderate Alzheimer’s disease and to find the right therapeutic dose to block Aβ accumulation [205].
Delivering insulin to the brain
Instead of resensitizing the brain to insulin, insulin could also be directly delivered to the brain nasally. In the brain, insulin improves cognition, daily functioning and memory [206]. Several clinical trials are however still being carried out assessing the safety and efficacy of this method.
The SNIFF study is a Phase II/III clinical trial where patients suffering from AD or mild cognitive impairment receive intranasal insulin or placebo for 12 months [207]. In yet another Phase II clinical study the effects of insulin detemir on cognitive functioning are compared to insulin. The hypothesis is that insulin detemir might work even better than insulin due to its albumin binding properties [208]. Glulisine, which is a rapidly acting insulin analog, is also being studied as an intranasal treatment in a Phase II clinical trial carried out in patients suffering from mild to moderate AD [209].
Anti-inflammatory solutions
Mast cells
Mast cells play a big role in sustaining inflammatory reaction in the central nervous system by releasing pro-inflammatory mediators when activated [210]. Via these mediators they can also regulate the permeability of the blood brain barrier and deficits in the blood brain barrier is something which is commonly seen in neurodegenerative diseases such as AD [211,212].

Masitinib, which is a tyrosine kinase inhibitor, is able to control the survival, degranulation and differentiation of mast cells, and in this way able to regulate the release of pro-inflammatory mediators [213]. A Phase II clinical trial has been carried out wherein patients suffering from mild to moderate AD treated with memantine of cholinesterase-inhibitors were given masitinib as well. Cognitive decline was less in patients treated with masitinib compared to patients treated with placebo and masinitib was well tolerated in these patients [214]. For this reason, a Phase III clinical trial in mild to moderate AD patients has been set up, investigating the safety and efficacy of masitinib, again together with memantine or cholinesterase-inhibitor treatment [215].
TNF-α
One cytokine thought to play a role in AD progression is TNF-α. Not only is it a pro-inflammatory mediator, it also influences glutamate neurotransmission and amyloid pathways [216]. Etanercept, a TNF-α inhibitor already used to treat arthritis, was able to rapidly improve cognitive functioning within minutes after perispinal administration in patients suffering from mild to moderate AD in a Phase I clinical trial [217]. Another Phase I trial has been set up to test the short term safety and efficacy of Etanercept when given together with dietary supplements [218].
Lp PLA2
GSK2647544 is a selective lipoprotein-associated phospholipase A2 (an enzyme produced by inflammatory cells to hydrolyze oxidized phospholipids) inhibitor currently being studied for its effects on Alzheimer’s disease. So far it is only being studies in young and elderly volunteers for its safety, tolerability and pharmacokinetics. Drug-drug interaction between GSK2647544 and simvastatine is studied as well to check for CYP3A4 inhibition by GSK2647544 [219].
Influencing Apo-ε3
Since the majority of AD patients carries the Apo-ε4 allele and Apo-ε3 seems to have a protective effect, efforts are being made to mimic the effects of Apo-ε3. COG133, a biotechnically derived Apo-ε3 mimicker, reduced inflammatory responses ex vivo in human blood. This compound did the same in the central nervous system and periphery of mice treated with lipopolysaccharide. In transgenic animals, compounds of the same sort, administration of COG112 and COG1410 lead to fewer lost neurons, reduced the production of neurofibrillary tangles and plaques and made less IL-6, a proinflammatory cytokine. Compared to untreated mice, an improvement in learning and memory was also observed. Being both neuroprotective and anti-inflammatory, this group of drugs might be very helpful when treating AD [220]. However, no clinical trials have yet been set up to test the safety of Apo-mimickers.

Changes in diet
As has been made clear in recent years, glucose and lipid metabolism both play a role in the pathogenesis of AD. The attention of current research is therefore more and more directed at changing diets of patients suffering from AD, or at people at risk of developing AD. By changing eating patterns, neuronal damage might be averted and the onset of AD might be delayed in this way.
Vitamin E, together with selenium, are currently being studied in the PREADVISE study. It is investigated how vitamin E and selenium can help prevent Alzheimer’s disease by reducing oxidative stress since less oxidative stress is thought to lead to less neuronal damage seen in Alzheimer’s disease [221]. Although selenium is an important trace element for the body, a lot of controversy remains on the part it might play in AD pathophysiology [222-224]. Vitamin E has been shown to reduce neuronal damage due to Aβ in cortical neurons and hippocampal cells, but correlations between AD pathophysiology and vitamin E intake in patients remain much harder to prove [225-227]. Anatabloc is another supplement that is being studied for positive effects on Alzheimer’s disease treatment in a Phase II clinical trial [228]. Containing anatabine (a MAO-inhibitor), vitamin A and vitamin D3, it is hoped Anatabloc also reduces the inflammatory reactions and damage seen in Alzheimer’s disease [229]. The study is performed in patients suffering from mild to moderate Alzheimer’s disease.
Omega-3 fatty acids have shown to be beneficial in AD pathophysiology. In elderly healthy patients a higher intake of Omega-3 fatty acids led to a decrease in Aβ40 and Aβ42 [230]. Dietary intake of these fatty acids, used for the viscosity of cell membranes and inflammatory responses in the body, might therefore lead to a reduced risk of developing AD [230]. To assess if changes in diet can slow the progress of Alzheimer’s disease, a Phase I/II clinical trials has been set up wherein patients receive lipoic acid and fish-oil concentrate, both high in Omega-3 fatty acids. This study looks at memory changes and changes in daily activities of participants during this study [231]. Another study looks at the effects of lipoic acid with omega-3 fatty acids when preventing Alzheimer’s disease [232].
A caprylic triglyceride momentarily being studied in a Phase II/III clinical trial is AC-1204. Regional cerebral hypometabolism has been pointed out as a prominent feature of Alzheimer's disease and AC-1204 induces chronic ketosis which improves mitochondrial metabolism [233]. Correcting cellular metabolism with AC-1204 might therefore be beneficial in AD patients. Via the citric cycle, endogenous ketone bodies can be converted to acetyl-CoA in order to produce the needed energy [234].
Chromatin modifying compounds
Recent study showed DNA methylation and in particular histone acetylation plays a role in the etiology of AD [235]. Histone acetylation is hereby done by histone acetyltransferases (HATS) and histone deacetylation is done by histone deacetylases (HDACs). The acetylation of histone is important for gene transcription and regulating chromatin condensation. HDACs regulate this acetylation and via this way gene expression. Two families of HDAC enzymes exist. The first family consists of metal-dependent enzymes (HDAC-I and HDAC-II). The second family (HDAC-III) is composed of seven mammalian sirtuins (SIRTs) [236].
The most researched SIRT is the nicotinamide adenine dinucleotide dependent (NAD+) SIRT1. SIRT1, which is localized in the nucleus and cytoplasm, appears to play a role in AD [237]. Firstly, the production of α-secretase is increased by SIRT1 as it deacetylates and activates the retinoic acid receptor-β protein. This stimulates the transcription of the ADAM10 gene [238,239]. After transcription of ADAM10, more α-secretase cleavage of APP occurs within the amyloid peptide region. These actions lead to a reduction of the Aβ protein and plaques seen in AD [239,240]. Secondly, SIRT1 seems able to deacetylate tau proteins, after which destabilization and proteolysis occurs, ultimately leading to a reduction in NFTs in neurons [241]. Thirdly, SIRT1 inhibits NFκB signaling which leads to a decrease of released neurotoxic chemokines, cytokines and nitric oxide by microglia, induced by Aβ [242]. Lastly, activation of SIRT1 has an anti-apoptotic effect by interacting with p53 and an antioxidant effect by activating FOXO3 and regulating PGC-1α [243].
The actions of SIRT1 make it an attractive therapeutic target. Resveratrol, a natural SIRT1 activator, seems have protective effects on Aβ-induced toxicity in cultured rat hippocampal cells. For this reason, supplemental forms of resveratrol are being investigated in a Phase II clinical trial [244]. Even as a lot is clear, the precise mechanism of SIRT1 still needs to be clarified and the bioavailability of resveratrol remains controversial [237]. Studies must be done to find the concentrations clinically relevant to influence the SIRT-pathways.
In contrast, nicotinamide (which is a competitive SIRT inhibitor) was also found to have beneficial effects in an animal model of AD. This was probably due to a reduction of phosphorylation at threonine-231 of the tau protein [245]. To understand how SIRTs might be therapeutically helpful, more research has to be done to find the precise mechanisms of their involvement in AD.
Of the metal-dependent HDACs, HDAC2 and HDAC6 are involved with the pathophysiology of AD [235]. Over-expressing HDAC2 leads to a reduction in synaptic plasticity and memory formation. Deficiency of HDAC2 leads to an increase of synaptic plasticity and memory formation. Modifying the effects of HDAC2 might be a beneficial way of treating AD. HDAC6 is over-expressed in AD patients. When HDAC6 is inhibited by tubacin, a selective HDAC6 inhibitor, a reduction of phosphorylation is seen at threonine-231 of the tau protein [246]. Inhibiting HDAC6 might be beneficial for decreasing the neurofibrillary tangles seen in AD, as threonine-231 phosphorylation is important for the regulation and stability of the cytoskeleton.
When looked at the known HDAC inhibitors, many of them have shown to have benefits in models of AD. Trichostatin A increases H4 acetylation and improves contextual performance in a mouse model [247]. SAHA rescues contextual memory in a transgenic mouse model of AD [248]. Valproic acid inhibits the production of Aβ in cells transfected with the Swedish APP-isoform. It does the same in a PDAPP transgenic mouse model [249]. In the APP23 transgenic mouse model, valproic acid not only decreases Aβ production, but reduces behavioral deficits as well [250]. A recent clinical trial showed however, although valproic acid has a long history of clinical use, contraindications in AD [251].
Phenylbutyrate, another HDAC inhibitor, shows no signs of toxicity in transgenic AD mouse models, and does show beneficial effects on pathology and memory performance [248]. Firstly, phenylbutyrate represses apoptosis in stressed neuronal regions [252]. Additionally, it restores the acetylation of histone H4 and clears intraneuronal Aβ accumulation leading to increased synaptic plasticity, improved learning and memory and reduction of spatial memory deficits [253].
HDAC inhibitors seem a potent treatment for AD, however most studies investigating the effects of HDAC inhibitors as a treatment for AD used broad-spectrum HADC inhibitors. The use of broad-spectrum HDAC inhibitors in neurodegeneration therefore remains controversial. To counter unwanted effects when treating AD, more specific HDACs have to be found and evaluated [237].
Other possible treatments
Caspase
In a preclinical study Aβ led to the activation of caspase 3, which is a protein involved in apoptosis. Pramipexol was able to attenuate this effect in human neuroblastoma cells [254]. Due to this neuroprotective effects R-pramipexol is now being studied in a Phase II clinical trial as treatment for early Alzheimer’s disease [255].
Immunotherapy
Sargramostim is being investigated in a Phase II clinical trial for its safety and effects in patients suffering from mild to moderate Alzheimer’s disease [256]. Sargramostim is a recombinant granulocyte macrophage colony-stimulating factor, making it an immunostimulator. Sargramostim normally is used for bone marrow stimulation and could help to improve memory in Alzheimer’s disease patients by clearing Aβ from the brain [257].
PDE5-inhibition
Udenafil, belonging to the class of PDE5-inhibtors, is being investigated for any positive effects on cognitive function in patients suffering from Alzheimer’s disease [258]. PDE5 inhibition leads to higher levels of cAMP and cGMP, increasing neuronal strength and synaptic strength [259,260]. Earlier administration of udenafil in a small group of patients
with erectile dysfunction showed an increase in cognitive functioning, possibly making udenafil a treatment for AD without targeting Aβ [261].
Fixing neuronal damage
RPh201 is a botanical extract that has been shown to reverse neurological damage in preclinical trials (data not published). A duel-centre Phase I/IIa study has been set up to study the safety and tolerability of RPh201, combined with its cognitive and behavioral effects. The Phase I part of the study was completed in October 2012, with RPh201 considered safe and tolerated enough at all tested doses. The Phase IIa part of the study is currently being done in patients suffering from moderate to severe Alzheimer’s disease [262].
Stem-cell therapy
A follow-up study is being executed wherein patients that participated in a Phase I study, are tested for long-term safety and efficacy of NEUROSTEM-AD. NEUROSTEM-AD are human umbilical cord blood-derived mesenchymal stem cells delivered directly into the brain in the hopes of promoting proliferation and differentiation of neuroprogenitor cells, leading to a restored functionality of brain tissue [263].
Figure 1: Clinical trials studying AD therapies momentarily being carried out
Drug Class/Mechanism of action
Phase Start of study Severity of Alzheimer’s disease
Status
EVP-0962 Y-secretase modulator II August 2012 Early stage ActiveAZD3293 BACE-1 inhibitor I February
2013Mild-moderate/
healthy volunteersRecruiting participants
AZD3293 BACE-1 inhibitor I December 2013
Healthy volunteers Recruiting participants
AZD3293 BACE-1 inhibitor I December 2013
Healthy volunteers Recruiting participants
MK-8931 BACE inhibitor II/III November 2012
Mild-moderate Recruiting participants
MK-8931 BACE inhibitor III September 2012
Prodromal Recruiting participants
Solanezumab Monoclonal IgG1 antibody against Ab
III July 2013 mild Recruiting participants
Solanezumab Monoclonal IgG1 antibody against Ab
III May 20120 All Active
BIIB037 Monoclonal IgG1 antibody against Ab-
plaques
I June 2011 Mild-moderate Active
BIIB037 Monoclonal IgG1 antibody against Ab-
plaques
I August 2012 Mild Recruiting participants
Gantenerumab Monoclonal antibody against Ab40/42
I June 2012 Mild-moderate Recruiting participants
BAN2401 Monoclonal antibody against AB protofibrils
II January 2013 Early Recruiting participants
AZD0530 Fyn-blocker I May 2013 All Recruiting participantsNilvadipine Calcium channel
blockerIII October 2012 Mild-moderate Recruiting participants
ACC-001 multiple short Aβ fragments linked to a
carrier
II January 2011 Mild-moderate Active
ACC-001 multiple short Aβ fragments linked to a
II October 2010 Early Active
carrierACC-001 multiple short Aβ
fragments linked to a carrier
II August 2009 Mild-moderate Active
ACC-001 multiple short Aβ fragments linked to a
carrier
II August 2009 Mild-moderate Active
Crenezumab Monoclonal IgG4 antibody against aggregated Ab
II November 2012
Mild-moderate Recruiting participants
Crenezumab Monoclonal IgG4 antibody against aggregated Ab
II November 2013
None Recruiting participants
Genistein Retinoid X receptor agonist
- October 2013 All Recruiting participants
Bexarotene Retinoid X receptor agonist
II January 2013 Mild-moderate Active
Carvedilol B-blocker IV May 2011 Early Recruiting participantsTPP4000 Combination of RAGE
and IgG ligand domains
I February 2012
Mild Active
Masitinib Tyrosine-kinase inhibitor
III June 2013 Mild-moderate Recruiting Participants
Etanercept Biological dietary supplement
I October 2012 Mild-moderate Recruiting participants
Vitamin E + selenium
Dietary supplement III June 2002 All Active
GSK2647544 Lp-PLA2 inhibitor I October 2013 Healthy volunteers Recruiting participantsLiraglutide GLP-1 agonst II April 2013 Mild Not yet recruiting
participantsExendin-4 GLP-1 agonist II December
2010Early Recruiting participants
Nasal insulin Peptide hormone II/III January 2013 Mild Not yet recruiting participants
Insulin LISPRO Peptide hormone - July 2012 Mild Not yet recruiting participants
Insulin glulisine Peptide hormone II September 2011
Mild-moderate Active
Insulin detemir Peptide hormone II May 2012 Mild-moderate ActiveResveratrol SIRT activator II December
2011Mild-moderate Active
NIC5-15 a-secretase inhibitor II August 2012 All Recruiting participantsCERE-110 NGF-delivery II April 2009 Mild-moderate ActiveTRx0237 Tau aggregation
inhibitorIII September
2012Mild Recruiting participants
TRx0237 Tau aggregation inhibitor
III September 2012
Mild-moderate Recruiting participants
AADvac1 Vaccine against misfolded tau
I May 2013 All Recruiting participants
AADvac1 Vaccine against misfolded tau
I January 2014 All Recruiting participants
TPI-287 Microtubule stabilizer I October 2013 Mild-moderate Not yet recruiting participants
RO4602522 MAO-B inhibitor II August 2012 Moderate-severe Recruiting participantsLadostigil Cholinesterase
inhibitor/MAO-B inhibitor
II September 2011
Early Active
AZD3480 NACh receptor agonist II November 2011
Mild-moderate Active
EVP-6124 A7 NACh receptor agonist
III October 2013 Mild-moderate Recruiting participants
EVP-6124 A7 NACh receptor agonist
III November 2013
Mild-moderate Recruiting participants
ABT-126 A7 NACh receptor agonist
II September 2012
Mild-moderate Active
Bisnorcymserine Butynylcholinesterase inhibitor
I December 2012
Healthy volunteers Recruiting participants
Lipioic acid + omega-3 fatty acids
Dietary supplement I/II January 2010 Probable AD Active
Lipioic acid + omega-3 fatty acids
Dietary supplement I/II January 2013 No AD Recruiting participants
AC-1204 Caprylic triclyceride II/III November 2012
Mild-moderate Recruiting participants
Anatabloc Dietary supplement II August 2012 Mild-moderate Recruiting participantsRiluzole Glutamate modulator II October 2012 Mild Recruiting participants
R-pramipexol Caspase inhibitor II June 2011 Early ActiveSargramostim Bone marrow
stimulatorII August 2011 Mild-moderate Recruiting participants
Udenafil PDE5 inhibitor III September 2013
Probable AD Not yet recruiting participants
Lu AE58054 5HT6 receptor agonist III December 2013
Mild-moderate Not yet recruiting participants
Lu AE58054 5HT6 receptor agonist III September 2013
Mild-moderate Recruiting participants
Lu AE58054 5HT6 receptor agonist III December 2013
Mild-moderate Not yet recruiting participants
rPh201 Neuroprotective botanical extract
I/II January 2012 Moderate-severe Recruiting participants
NEUROSTEM-AD Stemcell therapy - September 2012
All Recruiting participants
Discussion
As Aβ generation is a prominent feature of AD, for many years researchers focused on clearing the brain of Aβ-plaques. Although Aβ still remains a target for many newly developed drugs to treat AD, earlier research did not lead to any new treatments for AD [2]. The small molecules that were developed were either too dangerous or simply not effective enough. This goes next to the fact that new insights are that Aβ might even be necessary for the brain to normally function [2]. However, innovative tools and new gained knowledge led new possibilities (such as immunotherapy and PPARγ inhibition) of clearing the brain from these Aβ-plaques [114,142].
Many factors are involved in the generation of Aβ(1-42) and Aβ(1-40), which are thought to be the proteins that are leading to the harmful effects seen in patients suffering from AD. With many pathways influencing the generation of Aβ-plaques, influencing just one pathway therapeutically will not be beneficial for slowing the disease progress. Stopping inflammation caused by Aβ-plaques will for instance not stop the generation Aβ-plaques in the brain. Neurogeneration will only work as a cure, when nerve damaging factors can be removed from the brain at the same time [263,214].
Enhancing cholinergic transmission, either by butynyltransferase inhibitors or nicotinic cholinergic partial agonists, might increase cognitive functioning of patients and solve a bit of the problems arising when patients suffer from AD [175,179]. Treatment with such drugs is however only symptomatic.
Evidence is emerging that changes in lifestyle might prevent the onset of AD. Insulin has shown to play a huge role in AD pathogenesis [71]. Intake of Omega-3 fatty acids is very likely to be of benefit in slowing AD progression [230]. Vitamins and other anti-oxidants
might all have positive influences on delaying AD onset and reducing inflammation [221]. This shows that food intake is a big factor in developing AD, and changes in diet can possibly help to prevent patients from developing AD. With changing the diets of patients before they develop AD more targets influencing Aβ generation can be reached at once, making changes in diet a more synergistical method of treating/preventing AD.
Genetic screening of people might be a useful method of discovering which treatment will be beneficial in which patients. A person carrying the Apo-ε4 allele will find more use for Apo-ε3 mimickers than a person already carrying the Apo-ε3 allele [220].
With many aspects of the AD pathophysiology still unclear, finding a cure will be nearly next to impossible. However, with the many known factors influencing AD progression, finding methods to prevent AD will be more likely in the near future.

References
[1] A. Alzheimer, Über eine eigenartige Erkrankung der Hirnrinde. 1907 Allg. Z. Psychiatr. 64, 146–148[2] D.M. Holtzman, J.C. Morris, A.M. Goate. Alzheimer’s Disease: The Challenge of the Second Century. 2011. Sci Transl Med. Apr 6;3(77):77sr1[3] J.L. Price, D.W. McKeel, V.D. Buckles, C.M. Roe, C. Xiong. Neuropathology of nondemented aging: presumptive evidence for preclinical Alzheimer disease. 2009. Neurobiol Aging. Jul;30(7):1026-36[4] T.E. Golde, C.B. Eckman, S.G. Younkin. Biochemical detection of Aβ isoforms: implications for pathogenesis, diagnosis, and treatment of Alzheimer’s disease. 2000 Biochim Biophys Acta. Jul 26;1502(1):172-87[5] J. Hardy, D.J. Selkoe. The amyloid hypothesis of Alzheimer's disease: progress and problems on the road to therapeutics. 2002 Science. Jul 19;297(5580):353-6[6] R. Kayed, E. Head, J.L. Thompson, T.M. Mclntire, S.C. Milton. Common structure of soluble amyloid oligomers implies common mechanism of pathogenesis. 2003 Science. Apr 18;300(5618):486-9[7] R.M. Koffie, M. Meyer-Luehmann, T. Hashimoto, K.W. Adams, M.L. Mielke. Oligomeric amyloid beta associates with postsynaptic densities and correlates with excitatory synapse loss near senile plaques. 2009 Proc Natl Acad Sci U S A. Mar 10;106(10):4012-7[8] K.M. Lucin, T. Wyss-Coray. Immune activation in brain aging and neurodegeneration: too much or too little? 2009 Neuron. Oct 15;64(1):110-22. doi: 10.1016/j.neuron.2009.08.039[9] P.L. McGeer, E.G. McGeer. The inflammatory response system of brain: implications for therapy of Alzheimer and other neurodegenerative diseases. 1995 Brain Res Brain Res Rev. Sep;21(2):195-218[10] J.T. Jarrett, E.P. Berger, P.T. Lansbury. The carboxy terminus of the beta amyloid protein is critical for the seeding of amyloid formation: implications for the pathogenesis of Alzheimer's disease. 1993 Biochemistry. May 11;32(18):4693-7 [11] T. Iwatsubo, A. Odaka, N. Suzuki, H. Mizusawa, N. Nukina. Visualization of A beta 42(43) and A beta 40 in senile plaques with end-specific A beta monoclonals: evidence that an initially deposited species is A beta 42(43). 1994 Neuron. Jul;13(1):45-53[12] A. Goate, M.C. Chartier-Harlin, M. Mullan, J. Brown, F. Crawford. Segregation of a missense mutation in the amyloid precursor protein gene with familial Alzheimer's disease. 1991 Nature. Feb 21;349(6311):704-6[13] E. Levy, M.D. Carman, I.J. Fernandez-Madrid, M.D. Power, I. Lieberburg. Mutation of the Alzheimer's disease amyloid gene in hereditary cerebral hemorrhage, Dutch type. 1990 Science. Jun 1;248(4959):1124-6[14] C. van Broeckhoven, J. Haan, E. Bakker, J.A. Hardy, W. van Hul. Amyloid beta protein precursor gene and hereditary cerebral hemorrhage with amyloidosis (Dutch). 1990 Science. Jun 1;248(4959):1120-2[15] M.C. Chartier-Harlin, F. Crawfordm H. Houlden, A. Warren, D Hughes. Early-onset Alzheimer's disease caused by mutations at codon 717 of the beta-amyloid precursor protein gene. 1991 Nature. Oct 31;353(6347):844-6[16] J. Murrell, M. Farlow, B. Ghetti, M.D. Benson. A mutation in the amyloid precursor protein associated with hereditary Alzheimer's disease. 1991 Science. Oct 4;254(5028):97-9[17] J. Davis, W.E. van Nostrand. Enhanced pathologic properties of Dutch-type mutant amyloid beta-protein. 1996 Proc Natl Acad Sci U S A. Apr 2;93(7):2996-3000[18] T.J. Grabowski, H.S. Cho, J.P. Vonsattel, G.W. Rebeck, S.M. Greenberg. Novel amyloid precursor protein mutation in an Iowa family with dementia and severe cerebral amyloid angiopathy. 2001 Ann Neurol. Jun;49(6):697-705[19] W.E. van Nostrand, J.P. Melchor, H.S. Cho, S.M. Greenberg, G.W. Rebeck. Pathogenic effects of D23N Iowa mutant amyloid beta -protein. 2001 J Biol Chem. Aug 31;276(35):32860-6[20] C. Haass, A.Y. Hung, D.J. Selkoe, D.B. Teplow. Mutations associated with a locus for familial Alzheimer's disease result in alternative processing of amyloid beta-protein precursor. 1994 J Biol Chem. Jul 1;269(26):17741-8[21] N. Suzuki, T.T. Cheung, X.D. Cai, A. Odaka, L. Otvos. An increased percentage of long amyloid beta protein secreted by familial amyloid beta protein precursor (beta APP717) mutants. 1994 Science. May 27;264(5163):1336-40[22] M . Mullan, F. Crawford, K. Axelman, H. Houlden, L. Lilius. A pathogenic mutation for probable Alzheimer's disease in the APP gene at the N-terminus of beta-amyloid. 1992 Nat Genet. Aug;1(5):345-7[23] X.D. Cai, T.E. Golde, S.G. Youkin. Release of excess amyloid beta protein from a mutant amyloid beta protein precursor. 1993 Science. Jan 22;259(5094):514-6
[24] M. Citron, T. Oltersdorf, C. Haass, L. McConlogue, A.Y. Hung. Mutation of the beta-amyloid precursor protein in familial Alzheimer's disease increases beta-protein production. 1992 Nature. Dec 17;360(6405):672-4[25] A. Rovelet-Lecrux, D. Hannequin, G. Raux, N. Le Meur, A. Laquerrière. APP locus duplication causes autosomal dominant early-onset Alzheimer disease with cerebral amyloid angiopathy. 2006 Nat Genet. Jan;38(1):24-6[26] C. Nilsberth, A. Westlind-Danielsson, C.B. Eckman, M.M. Condron, K. Axelman. The 'Arctic' APP mutation (E693G) causes Alzheimer's disease by enhanced Abeta protofibril formation. 2001 Nat Neurosci. Sep;4(9):887-93[27] T. Tomiyama, T. Nagata, H. Shimada, R. Teraoka, A. Fukushima. A new amyloid beta variant favoring oligomerization in Alzheimer's-type dementia. 2008 Ann Neurol. Mar;63(3):377-87[28] A.L. Cloe, J.P. Orgel, J.R. Sachleben, R. Tycko, S.C. Meredith. The Japanese mutant Aβ (ΔE22-Aβ(1-39)) forms fibrils instantaneously, with low-thioflavin T fluorescence: seeding of wild-type Aβ(1-40) into atypical fibrils by ΔE22-Aβ(1-39). 2011 Biochemistry. Mar 29;50(12):2026-39[29] A. Nikolaev, T. McLaughlin, D.D. O’Leary, M. Tessier-Lavigne. APP binds DR6 to trigger axon pruning and neuron death via distinct caspases. 2009 Nature. Feb 19;457(7232):981-9[30] T.L Young-Pearse, S. Suth, E.S. Luth, A. Sawa. D.J. Selkoe. Biochemical and functional interaction of disrupted-in-schizophrenia 1 and amyloid precursor protein regulates neuronal migration during mammalian cortical development. 2010 J Neurosci. Aug 4;30(31):10431-40[31] S. Ring, S.W. Weyer, S.B. Kilian, E. Waldron, C.U. Pietrzik. The secreted beta-amyloid precursor protein ectodomain APPs alpha is sufficient to rescue the anatomical, behavioral, and electrophysiological abnormalities of APP-deficient mice. 2007 J Neurosci. Jul 18;27(29):7817-2[32] J.R. Cirrito, K.A. Yamada, M.B. Finn, R.S. Sloviter, K.R. Bales. Synaptic activity regulates interstitial fluid amyloid-beta levels in vivo. 2005 Neuron. Dec 22;48(6):913-22[33] F. Kamenetz, T. Tomita, J. Hsieh, G. Seabrook, D. Borchelt. APP processing and synaptic function. 2003 Neuron. Mar 27;37(6):925-37[34] W. Wei, L.N. Nguyen, H.W. Kessels, H.Hagiwara, S. Sisodia. Amyloid beta from axons and dendrites reduces local spine number and plasticity. 2010 Nat Neurosci. Feb;13(2):190-6[35] N. Takasugi, T. Tomita, I. Hayashi, M. Tsuruoka, M. Niimura. The role of presenilin cofactors in the gamma-secretase complex. 2003 Nature. Mar 27;422(6930):438-41[36] D. Edbauer, E. Winkler, J.T. Regula, B. Pesold, H. Steiner. Reconstitution of gamma-secretase activity. 2003 Nat Cell Biol. May;5(5):486-8[37] L. Serneels, J. van Biervliet, K. Craessaerts, T. Dejaegere, Horré K. gamma-Secretase heterogeneity in the Aph1 subunit: relevance for Alzheimer's disease. 2009 Science. May 1;324(5927):639-42[38] G. Yu, M. Nishimura, S. Arawaka, D. Levitan, L. Zhang. Nicastrin modulates presenilin-mediated notch/glp-1 signal transduction and betaAPP processing. 2000 Nature. Sep 7;407(6800):48-54[39] Y.M. Li, M. Xu, MT. Lai, Q. Huang, J.L. Castro. Photoactivated gamma-secretase inhibitors directed to the active site covalently label presenilin 1. 2000 Nature. Jun 8;405(6787):689-94[40] M.S. Wolfe, W. Xia, B.L. Ostaszweski, T.S. Diehl, W.T. Kimberly. Two transmembrane aspartates in presenilin-1 required for presenilin endoproteolysis and gamma-secretase activity. 1999 Nature. Apr 8;398(6727):513-7[41] Z. Liu, A. Turkoz, E.N. Jackson, J.C. Corbo, J.A. Engelbach. Notch1 loss of heterozygosity causes vascular tumors and lethal hemorrhage in mice. 2011 J Clin Invest. Feb;121(2):800-8[42] N.F. Schor. What the halted phase III γ-secretase inhibitor trial may (or may not) be telling us. 2011 Ann Neurol. Feb;69(2):237-9[43] H. Braak, E. Braak. Frequency of stages of Alzheimer-related lesions in different age categories. 1997 Neurobiol Aging. Jul-Aug;18(4):351-7[44] I. Grundke-Iqbal, K. Iqbal, Y.C. Tung, M. Quinlan, H.M. Wisniewski. Abnormal phosphorylation of the microtubule-associated protein tau (tau) in Alzheimer cytoskeletal pathology. 1986 Proc Natl Acad Sci U S A. Jul;83(13):4913-7[45] C.M. Wischik, M. Novak, P.C. Edwards, A. Klug, W. Tichelaar. Structural characterization of the core of the paired helical filament of Alzheimer disease. 1988 Proc Natl Acad Sci U S A. Jul;85(13):4884-8[46] C.M. Wischik, M. Novak, H.C. Thøgersen, P.C. Edwards, M.J. Runswick. 1988 Proc Natl Acad Sci U S A.
Jun;85(12):4506-10[47] M. Goedert, C.M. Wischik, R.A. Crowther, J.E. Walker, A. Klug. Cloning and sequencing of the cDNA encoding a core protein of the paired helical filament of Alzheimer disease: identification as the microtubule-associated protein tau. 1988 Proc Natl Acad Sci U S A. Jun;85(11):4051-5[48] V.M. Lee, B.J. Balin, L. Otvos, J.Q. Trojanowski. A68: a major subunit of paired helical filaments and derivatized forms of normal Tau. 1991 Science. Feb 8;251(4994):675-8[49] S.A. Small, K. Duff. Linking Abeta and tau in late-onset Alzheimer's disease: a dual pathway hypothesis. 2008 Neuron. Nov 26;60(4):534-42[50] R.L. Buckner, A.Z. Snyder, B.J. Shannon, G. LaRossa, R. Sachs. Molecular, structural, and functional characterization of Alzheimer's disease: evidence for a relationship between default activity, amyloid, and memory. 2005 J Neurosci. Aug 24;25(34):7709-17[51] B. Frost, M.I. Diamond, Prion-like mechanisms in neurodegenerative diseases. 2010 Nat Rev Neurosci. Mar;11(3):155-9[52] M. Meyer-Luehmann, J. Coomaraswamy, T. Bolmont, S. Kaeser, C. Schaefer. Exogenous induction of cerebral beta-amyloidogenesis is governed by agent and host. 2006 Science. Sep 22;313(5794):1781-4[53] Y.S. Eisele, U. Obermüller, G. Heilbronner, F. Baumann, S.A. Kaeser. Peripherally applied Abeta-containing inoculates induce cerebral beta-amyloidosis. 2010 Science. Nov 12;330(6006):980-2[54] F. Clavaguera, T. Bolmont, R.A. Crowther, D. Abramowski, S. Frank. Transmission and spreading of tauopathy in transgenic mouse brain. 2009 Nat Cell Biol. Jul;11(7):909-13[55] R.J. Perrin, A.M. Fagan, D.M. Holtzman. Multimodal techniques for diagnosis and prognosis of Alzheimer's disease. 2009 Nature. Oct 15;461(7266):916-22[56] S.A. Areosa, F. Sherriff, R. McShane. Memantine for dementia. 2005 Cochrane Database Syst Rev. Apr 18[57] J.T. Coyle, D.L. Price, M.R. DeLong. Alzheimer's disease: a disorder of cortical cholinergic innervation. 1983 Science. Mar 11;219(4589):1184-90[58] P. Davies, A.J. Maloney. Selective loss of central cholinergic neurons in Alzheimer's disease. 1976 Lancet. Dec 25;2(8000):1403[59] M.R. Farlow, M.L. Miller, V. Pejovic. Treatment options in Alzheimer's disease: maximizing benefit, managing expectations. 2008 Dement Geriatr Cogn Disord.;25(5):408-22[60] L. Bertram, C. Lange, K. Mullin, M. Parkinson, M. Hsiao. Genome-wide association analysis reveals putative Alzheimer's disease susceptibility loci in addition to APOE. 2008 Am J Hum Genet. Nov;83(5):623-32[61] D. Harold, R. Abraham, P. Hollingworth, R. Sims, A. Gerrish. Genome-wide association study identifies variants at CLU and PICALM associated with Alzheimer's disease. 2009 Nat Genet. Oct;41(10):1088-93[62] J.C. Lambert, S. Heath, G. Even, D. Campion, K. Sleegers. Genome-wide association study identifies variants at CLU and CR1 associated with Alzheimer's disease. 2009 Nat Genet. Oct;41(10):1094-9[63] S. Seshadri, A.L. Fitzpatrick, M.A. Ikram, A.L. DeStefano, V. Gudnason. Genome-wide analysis of genetic loci associated with Alzheimer disease. 2010 JAMA. May 12;303(18):1832-40[64] A.C. Naj, G. Jun, G.W. Beecham, L.S. Wang, B.N. Vardarajan. Common variants at MS4A4/MS4A6E, CD2AP, CD33 and EPHA1 are associated with late-onset Alzheimer's disease. 2011 Nat Genet. May;43(5):436-41[65] P. Hollingworth, D. Harold, R. Sims, A. Gerrish, J.C. Lambert. Common variants at ABCA7, MS4A6A/MS4A4E, EPHA1, CD33 and CD2AP are associated with Alzheimer's disease. 2011 Nat Genet. May;43(5):429-35[66] E.H. Corder, A.M. Saunders, W.J. Strittmatter, D.E. Schmechel, P.C. Gaskell. Gene dose of apolipoprotein E type 4 allele and the risk of Alzheimer's disease in late onset families. 1993 Science. Aug 13;261(5123):921-3[67] W.J. Strittmatter, A.M. Saunders, D. Schmechel, M. Pericak-Vance, J.Enghild. Apolipoprotein E: high-avidity binding to beta-amyloid and increased frequency of type 4 allele in late-onset familial Alzheimer disease. 1993 Proc Natl Acad Sci U S A. Mar 1;90(5):1977-81[68] J. Kim, J.M. Basak, D.M. Holtzman. The role of apolipoprotein E in Alzheimer's disease. 2009 Neuron. Aug 13;63(3):287-303[69] R.W. Mahley, Apolipoprotein E: cholesterol transport protein with expanding role in cell biology. 1988 Science. Apr 29;240(4852):622-30.[70] A.S. Plump, J.L. Breslow, Apolipoprotein E and the apolipoprotein E-deficient mouse. 1995Annu Rev
Nutr.15:495-518[71] A.M. Maloney, R.J. Griffin, S. Timmons, R. O’Conner, R. Ravid. Defects in IGF-1 receptor, insulin receptor and IRS-1/2 in Alzheimer's disease indicate possible resistance to IGF-1 and insulin signaling. 2010 Neurobiol Aging. Feb;31(2):224-43[72] A.I. Duarte, P.I. Moreira, C.R. Oliveira. Insulin in central nervous system: more than just a peripheral hormone. 2012 J Aging Res. 2012:384017[73] S.M. de la Monte. Insulin resistance and Alzheimer's disease. 2009 BMB Rep. Aug 31;42(8):475-81[74] D. Bosco, A. Fava, M. Plastino, T. Montalcini, A. Pujia. Possible implications of insulin resistance and glucose metabolism in Alzheimer's disease pathogenesis. 2011 J Cell Mol Med. Sep;15(9):1807-21[75] S.C. Correia, R.X. Santos, G. Perry, X. Zhu, P.I Moreira. Insulin-resistant brain state: the culprit in sporadic Alzheimer's disease? 2011 Ageing Res Rev. Apr;10(2):264-73[76] P.I. Moreira, A.I. Duarte, M.S. Santos, A.C. Rego, C.R. Oliveira. An integrative view of the role of oxidative stress, mitochondria and insulin in Alzheimer's disease. 2009 J Alzheimers Dis. 16(4):741-61[77] B. Kim, E.L. Feldman. Insulin resistance in the nervous system. 2012 Trends Endocrinol Metab. Mar;23(3):133-41[78] A.R. Cole, A. Astell, C. Green, C. Sutherland. Molecular connexions between dementia and diabetes. 2007 Neurosci Biobehav Rev. 31(7):1046-63[79] L.P. van de Heide, B.M. Ramakers, M.P. Smidt. Insulin signaling in the central nervous system: learning to survive. 2006 Prog Neurobiol. Jul;79(4):205-21[80] Z. Zhao. Z. Xiang. V. Haroutunian, J.D. Buxbaum, Stetka B. Insulin degrading enzyme activity selectively decreases in the hippocampal formation of cases at high risk to develop Alzheimer's disease. 2007 Neurobiol Aging. Jun;28(6):824-30[81] E. Candeias, A.I. Duarte, C. Carvalho, S.C. Correia, S. Cardoso. The impairment of insulin signaling in Alzheimer's disease. 2012 IUBMB Life. Dec;64(12):951-7[82] A. Fuster-Matanzo, M. Llorens-Martín , F. Hernández, J. Avila. Role of neuroinflammation in adult neurogenesis and Alzheimer disease: therapeutic approaches. 2013 Mediators Inflamm. 2013:260925[83] W.S. Griffin, R.E. Mrak. Interleukin-1 in the genesis and progression of and risk for development of neuronal degeneration in Alzheimer's disease 2002 J Leukoc Biol. Aug;72(2):233-8.[84] C.E. Finch, T.E. Morgan. Systemic inflammation, infection, ApoE alleles, and Alzheimer disease: a position paper. 2007 Curr Alzheimer Res. Apr;4(2):185-9[85] R.E. Mrak, W.S. Griffin. Glia and their cytokines in progression of neurodegeneration. 2005 Neurobiol Aging. Mar;26(3):349-54[86] M. Cacquevel. N. Lebeurrier, S. Chéenne, D. Vivien. Cytokines in neuroinflammation and Alzheimer's disease. 2004 Curr Drug Targets. Aug;5(6):529-34[87] G. Halliday, S.R. Robinson, C. Shepherd, J. Kril. Alzheimer's disease and inflammation: a review of cellular and therapeutic mechanisms. 2000 Clin Exp Pharmacol Physiol. Jan-Feb;27(1-2):1-8[88] T. Town, V. Nikolic, J. Tan. The microglial "activation" continuum: from innate to adaptive responses. 2005 J Neuroinflammation. Oct 31;2:24[89] G. Forloni, F. Mangiarotti, N. Angeretti, E. Lucca, M.G. De Simoni. Beta-amyloid fragment potentiates IL-6 and TNF-alpha secretion by LPS in astrocytes but not in microglia. 1997 Cytokine. Oct;9(10):759-62[90] D.A. DeWitt, G. Perry, M. Cohen, C. Doller, J. Silver. Astrocytes regulate microglial phagocytosis of senile plaque cores of Alzheimer's disease. 1998 Exp Neurol. Feb;149(2):329-40[91] B. Liu, J.S. Hong. Role of microglia in inflammation-mediated neurodegenerative diseases: mechanisms and strategies for therapeutic intervention. 2003 J Pharmacol Exp Ther. Jan;304(1):1-7[92] S.A. Frautschy, F. Yang, M. Irrizarry, B. Hyman, T.C. Saido. Microglial response to amyloid plaques in APPsw transgenic mice. 1998 Am J Pathol. Jan;152(1):307-17[93] X. Xia, S. Qian, S. Soriano, Y. Wu, A.M. Fletcher. Loss of presenilin 1 is associated with enhanced beta-catenin signaling and skin tumorigenesis. 2001 Proc Natl Acad Sci U S A. Sep 11;98(19):10863-8[94] M. Nicolas, A. Wolfer, K. Raj, J.A. Kummer, P. Mill. Notch1 functions as a tumor suppressor in mouse skin. 2003 Nat Genet. Mar;33(3):416-21[95] C.R. Hopkins. ACS chemical neuroscience molecule spotlight on BMS-708163. ACS Chem Neurosci. 2012 Mar 21;3(3):149-50

[96] K. Rogers, K.M. Felsentein, L. Hrdlicka, Z. Tu, F. Albayya. Modulation of γ-secretase by EVP-0015962 reduces amyloid deposition and behavioral deficits in Tg2576 mice. 2012 Mol Neurodegener. Dec 18;7:6[97] C.F. Albright, R.C. Dockens, J.E. Meredith, R.E. Olson, R. Slemmon. Pharmacodynamics of selective inhibition of γ-secretase by avagacestat. 2013J Pharmacol Exp Ther. Mar 344(3):686-95[98] G. Tong, L. Castaneda, J.S. Wang, O. Sverdlov, S.P. Huang. Effects of single doses of avagacestat (BMS-708163) on cerebrospinal fluid Aβ levels in healthy young men. 2012 Clin Drug Investig. Nov;32(11):761-9[99] V. Coric, C.H. van Dyck, S. Salloway, N. Andreasen, M. Brody. Safety and tolerability of the γ-secretase inhibitor avagacestat in a phase 2 study of mild to moderate Alzheimer disease. 2012 Arch Neurol. Nov;69(11)[100] C.J. Crump, S.V. Castro, F. Wang, N. Podznyakov, T.E. Ballard. BMS-708,163 targets presenilin and lacks notch-sparing activity. 2012 Biochemistry. Sep 18;51(37):7209-1[101] Clinicaltrials.gov. Safety, Tolerability, Pharmacokinetics of EVP-0962 and Effects of EVP-0962 on Cerebral Spinal Fluid Amyloid Concentrations in Healthy Subjects and in Subjects With Mild Cognitive Impairment or Early Alzheimer's Disease. http://clinicaltrials.gov/ct2/show/NCT01661673. Last visited on 03-01-2014[102] R. Vassar, B.D. Bennett, S. Babu-Khan, S. Kahn, E.A. Mendiaz. Beta-secretase cleavage of Alzheimer's amyloid precursor protein by the transmembrane aspartic protease BACE. 1999 Science. Oct 22;286(5440):735-41[103] H. Cai, Y. Wang, D. McCarthy, H. Wen, D.R. Borchelt. BACE1 is the major beta-secretase for generation of Abeta peptides by neurons. 2001 Nat Neurosci. Mar;4(3):233-4[104] M. Willem, S. Lammich, C. Haass. Function, regulation and therapeutic properties of beta-secretase (BACE1). 2009 Semin Cell Dev Biol. Apr;20(2):175-82[105] F. Jeppsson, S. Eketjäll, J. Janson, S. Karlström, S. Gustavsson. Discovery of AZD3839, a potent and selective BACE1 inhibitor clinical candidate for the treatment of Alzheimer disease. 2012 J Biol Chem. Nov 30;287(49):41245-57[106] Clinicaltrials.gov. A Two-part Multiple Dose Study to Assess the Safety and Effects of AZD3293 in Healthy Elderly and Alzheimer's Patients. http://clinicaltrials.gov/ct2/show/NCT01795339. Last visited on 03-01-2014[107] Clinicaltrials.gov. A Two-part Single and Multiple Dose Study to Assess the Safety , Pharmacokinetics and Effects of AZD3293 in Healthy Japanese Young and Elderly Volunteers. http://clinicaltrials.gov/ct2/show/NCT02005211. Last visited on 03-01-2014[108] Clinicaltrials.gov A Phase I Study in Healthy Volunteers to Assess the Effect of Cytochrome3A4 (CYP3A4) Inhibitors (Diltiazem and Itraconazole) on the Pharmacokinetics (PK) of AZD3293 and the Effects of AZD3293 on the Pharmacokinetics of Midazolam, a Cytochrome 3A4 and Cytochrome 3A5 (CYP3A4/CYP3A5) Substrate. http://clinicaltrials.gov/ct2/show/NCT02010970. Last visited on 23-01-2014[109] I. Templeton, C.C. Peng, K.E. Thummel, C. Davis, K.L Kunze. Accurate prediction of dose-dependent CYP3A4 inhibition by itraconazole and its metabolites from in vitro inhibition data. 2010 Clin Pharmacol Ther. Oct;88(4):499-505[110] X. Zhang, D.R. Jones, S.D. Hall. Prediction of the effect of erythromycin, diltiazem, and their metabolites, alone and in combination, on CYP3A4 inhibition. Drug Metab Dispos. 2009 Jan;37(1):150-60[111] C. Emoto, K. Iwasaki. Relative roles of CYP2C19 and CYP3A4/5 in midazolam 1'-hydroxylation. 2007 Xenobiotica. Jun;37(6):592-603[112] Clinicaltrials.gov An Efficacy and Safety Trial of MK-8931 in Mild to Moderate Alzheimer's Disease (P07738), http://clinicaltrials.gov/ct2/show/NCT01739348. Last visited on 03-01-2014 [113] Clinicaltrials.gov Efficacy and Safety Trial of MK-8931 in Participants With Prodromal Alzheimer's Disease (MK-8931-019). http://clinicaltrials.gov/ct2/show/NCT01953601 Last visited on 23-01-2014Immunotherapy[114] J. Delrieu, P.J. Ousset, C. Caillaud, B. Vellas. 'Clinical trials in Alzheimer's disease': immunotherapy approaches. 2012 J Neurochem. Jan;120 Suppl 1:186-93[115] D. Schenk, R. Barbour, W. Dunn, G. Gordon, H. Grajeda. Immunization with amyloid-beta attenuates Alzheimer-disease-like pathology in the PDAPP mouse. 1999 Nature. Jul 8;400(6740):173-7[116] B.J. Bacskai, S.T. Kaidasz, R.H. Christie, C. Carter, D. Games. Imaging of amyloid-beta deposits in brains of living mice permits direct observation of clearance of plaques with immunotherapy. 2001 Nat Med.
Mar;7(3):369-72[117] Clinicaltrials.gov. Randomized Safety, Tolerability and Pilot Efficacy of AN-1792 in Alzheimer's Disease http://clinicaltrials.gov/ct2/show/NCT00021723. Last visited on 13-01-2014[118] B. Winblad, N. Andreasen, L. Minthon, A. Floesser, G. Imbert. Safety, tolerability, and antibody response of active Aβ immunotherapy with CAD106 in patients with Alzheimer's disease: randomised, double-blind, placebo-controlled, first-in-human study. 2012 Lancet Neurol. Jul;11(7):597-604[119] M. Pride, P. Seubert, M. Grundman, M. Hagen, J. Eldridge. Progress in the active immunotherapeutic approach to Alzheimer's disease: clinical investigations into AN1792-associated meningoencephalitis. 2008 Neurodegener Dis. 5(3-4):194-6[120] Clinicaltrials.gov. A Long Term Extension Study Evaluating ACC-001 With QS-21 in Subjects With Mild to Moderate Alzheimer's Disease http://clinicaltrials.gov/ct2/show/NCT00960531. Last visited on 23-01-2014[121] Clinicaltrials.gov. Amyloid Imaging And Safety Study Of ACC-001 In Subjects With Mild to Moderate Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01284387. Last visited on 04-01-2014[122] Clinicaltrials.gov. Amyloid Imaging And Safety Study Of ACC-001 In Subjects With Early Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01227564. Last visited on 04-01-2014[123] Clinicaltrials.gov. A Long-Term Safety And Tolerability Study Of Bapineuzumab In Alzheimer Disease Patients. http://clinicaltrials.gov/ct2/show/NCT00996918. Last visited on 13-01-2014[124] E.R. Siemens, S. Friedrich, R.A. Dean, C.R. Gonzales, M.R. Farlow. Safety and changes in plasma and cerebrospinal fluid amyloid beta after a single administration of an amyloid beta monoclonal antibody in subjects with Alzheimer disease. . 2010 Clin NeuropharmacolMar-Apr;33(2):67-73[125] M. Farlow, S.E. Arnold, C.H. van Dyck, P.S. Aisen, B.J. Snider. Safety and biomarker effects of solanezumab in patients with Alzheimer's disease. 2012 Alzheimers Dement. Jul;8(4):261-71[126] H.O. Tayeb, E.D. Murray, B.H. Price, F.I. Tarazi. Bapineuzumab and solanezumab for Alzheimer's disease: is the 'amyloid cascade hypothesis' still alive? 2013 Expert Opin Biol Ther. Jul;13(7):1075-84[127] Clinicaltrials.gov. Progress of Mild Alzheimer's Disease in Participants on Solanezumab Versus Placebo, http://clinicaltrials.gov/ct2/show/NCT01900665. Last visited on 03-01-2014[128] Clinicaltrials.gov. Continued Safety Monitoring of Solanezumab in Alzheimer's Disease http://clinicaltrials.gov/ct2/show/NCT01127633. Last visited on 23-01-2013[129] Clinicaltrials.gov. A Study to Evaluate Safety, Tolerability, and Efficacy of BAN2401 in Subjects With Early Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01767311. Last visited on 03-01-2014[130] Clinicaltrials.gov. Single Ascending Dose Study of BIIB037 in Subjects With Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01397539. Last visited 03-01-2014[131] Clinicaltrials.gov. Multiple Dose Study of BIIB037 in Subjects With Prodromal or Mild Alzheimer's Disease. http://clinicaltrials.gov/ct2/show/NCT01677572. Last visited on 03-01-2014[132] B. Bohrmann, K. Baumann, J. Benz, F. Gerber, W. Huber. Gantenerumab: a novel human anti-Aβ antibody demonstrates sustained cerebral amyloid-β binding and elicits cell-mediated removal of human amyloid-β. 2012 J Alzheimers Dis. 28(1):49-69[133] S. Ostrowitzki, D. Deptula, L. Thurfjell, F. Barkhoff, B. Bohrmann. Mechanism of amyloid removal in patients with Alzheimer disease treated with gantenerumab. 2012 Arch Neurol. Feb;69(2):198-207[134] Clinicaltrials.gov. A Multiple-dose Study of Gantenerumab in Japanese Alzheimer's Disease Patients, http://clinicaltrials.gov/ct2/show/NCT01656525. Last visited on 03-01-2014[135] Clinicaltrials.gov. Dominantly Inherited Alzheimer Network Trial: An Opportunity to Prevent Dementia. A Study of Potential Disease Modifying Treatments in Individuals at Risk for or With a Type of Early Onset Alzheimer's Disease Caused by a Genetic Mutation. http://clinicaltrials.gov/ct2/show/NCT01760005. Last visited on 23-01-2014[136] Clinicaltrials.gov. A Study of Gantenerumab in Patients With Prodromal Alzheimer's Disease http://clinicaltrials.gov/ct2/show/NCT01224106. Last visited on 23-01-2014[137] K. Garber. Genentech's Alzheimer's antibody trial to study disease prevention. 2012 Nat Biotechnol. Aug;30(8):731-2.[138] Clinicaltrials.gov. A Long-Term Safety Extension Study of Studies ABE4869g And ABE4955g in Patients With Mild To Moderate Alzheimer's Disease Treated With Crenezumab, http://clinicaltrials.gov/ct2/show/NCT01723826. Last visited on 04-01-2014
[139] Clinicaltrials.gov. A Study of Crenezumab Versus Placebo in Preclinical PSEN1 E280A Mutation Carriers to Evaluate Efficacy and Safety in the Treatment of Autosomal-Dominant Alzheimer Disease, Including a Placebo-Treated Noncarrier Cohort. http://clinicaltrials.gov/ct2/show/NCT01998841. Last visited on 23-01-2014[140] Transtech Pharma. TTP4000 http://www.ttpharma.com/TherapeuticAreas/AlzheimersDisease/TTP4000/tabid/124/Default.aspx. Last visited on 14-01-2014[141] Clinicaltrials.gov. A Safety Study of TTP4000 in Subjects With Alzheimer's Disease , http://clinicaltrials.gov/ct2/show/NCT01548430. Last visited on 04-01-2014[142] C. d’Abramo, S. Massone, J.M. Zingg, A. Pizzuti, P. Marambaud. Role of peroxisome proliferator-activated receptor gamma in amyloid precursor protein processing and amyloid beta-mediated cell death. Biochem J. 2005 Nov 1;391(Pt 3):693-8[143] M. Sastre, I. Dewachter, G.E. Landreth, T.M. Wilson, T. Klockgether. Nonsteroidal anti-inflammatory drugs and peroxisome proliferator-activated receptor-gamma agonists modulate immunostimulated processing of amyloid precursor protein through regulation of beta-secretase. 2003 J Neurosci. Oct 29;23(30):9796-804[144] M. Sastre, I. Dewachter, S. Rossner, N. Bogdanovic, E. Rosen. Nonsteroidal anti-inflammatory drugs repress beta-secretase gene promoter activity by the activation of PPARgamma. Proc Natl Acad Sci U S A. 2006 Jan 10;103(2):443-8 [145] Q. Jiang, C.Y. Lee, S. Mandrekar, B. Wilkinson, P. Cramer. ApoE promotes the proteolytic degradation of Abeta. 2008 Neuron. Jun 12;58(5):681-93[146] P. Lefebvre, Y. Benomar, B. Staels. Retinoid X receptors: common heterodimerization partners with distinct functions. 2010 Trends Endocrinol Metab. Nov;21(11):676-83[147] T. Zhang, F. Wang, H.X. Xu, L. Yi, Y. Qin. Activation of nuclear factor erythroid 2-related factor 2 and PPARγ plays a role in the genistein-mediated attenuation of oxidative stress-induced endothelial cell injury. 2013 Br J Nutr. Jan 28;109(2):223-35[148] M. Bagheri, M.T. Joghataei, S. Mohseni, M. Roghani. Genistein ameliorates learning and memory deficits in amyloid β(1-40) rat model of Alzheimer's disease. Neurobiol Learn Mem. 2011 Mar;95(3):270-[149] Clinicaltrials.gov. Genistein as a Possible Treatment for Alzheimer's Disease. , http://clinicaltrials.gov/ct2/show/NCT01982578. Last visited on 04-01-2014[150]. P.E. Cramer, J.R. Cirrito, D.W. Wesson, C.Y. Lee, J.C. Karlo. ApoE-directed therapeutics rapidly clear β-amyloid and reverse deficits in AD mouse models. 2012 Science. Mar 23;335(6075):1503-6[151] Clinicaltrials.gov. Bexarotene Amyloid Treatment for Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01782742. Last visited on 04-01-2014[152] N.F. Fitz, A.A. Cronican, I. Lefterov, R. Koldamova. Comment on "ApoE-directed therapeutics rapidly clear β-amyloid and reverse deficits in AD mouse models". 2013 Science. May 24;340(6135):924-c[153] A.R. Price, G. Xu, Z.B. Ziemienski, L.A. Smithson, D.R. Borchelt, T.E. Golde. Comment on "ApoE-directed therapeutics rapidly clear β-amyloid and reverse deficits in AD mouse models". 2013 Science. May 24;340(6135):924-d[154] I. Tesseur, A.C. Lo, A. Roberfroid, S. Dietvorst, B. van Broeck. Comment on "ApoE-directed therapeutics rapidly clear β-amyloid and reverse deficits in AD mouse models". 2013 Science. May 24;340(6135):924-e[155] K. Veeraraghavalu, C. Zhang, S. Miller, J.K. Hefendehl, T.W. Rajapaksha. Comment on "ApoE-directed therapeutics rapidly clear β-amyloid and reverse deficits in AD mouse models". 2013 Science. May 24;340(6135):924-f[156] M.E. Larson, S.E. Lesné. Soluble Aβ oligomer production and toxicity. 2012 J Neurochem. Jan;120 Suppl 1:125-39[157] J.W. Um, H.B. Nygaard, J.K. Heiss, M.A. Kostylev, M. Stagi. Alzheimer amyloid-β oligomer bound to postsynaptic prion protein activates Fyn to impair neurons. 2012 Nat Neurosci. Sep;15(9):1227-3[158] Clinicaltrials.gov. Safety and Tolerability of AZD0530 (Saracatinib) in Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01864655. Last visited on 03-01-2014[159] D. Paris, A. Quadros, J. Humphrey, N. Patel, R. Crescentini. Nilvadipine antagonizes both Abeta vasoactivity in isolated arteries, and the reduced cerebral blood flow in APPsw transgenic mice. 2004 Brain Res. Feb 27;999(1):53-61[160] H. Matsuda, N. Araki, I. Kuji, T. Ohkubo. E. Imabayashi. Effect of nilvadipine on regional cerebral blood flow in a patient with early Alzheimer disease. 2008 Clin Nucl Med. Jan;33(1):34-5
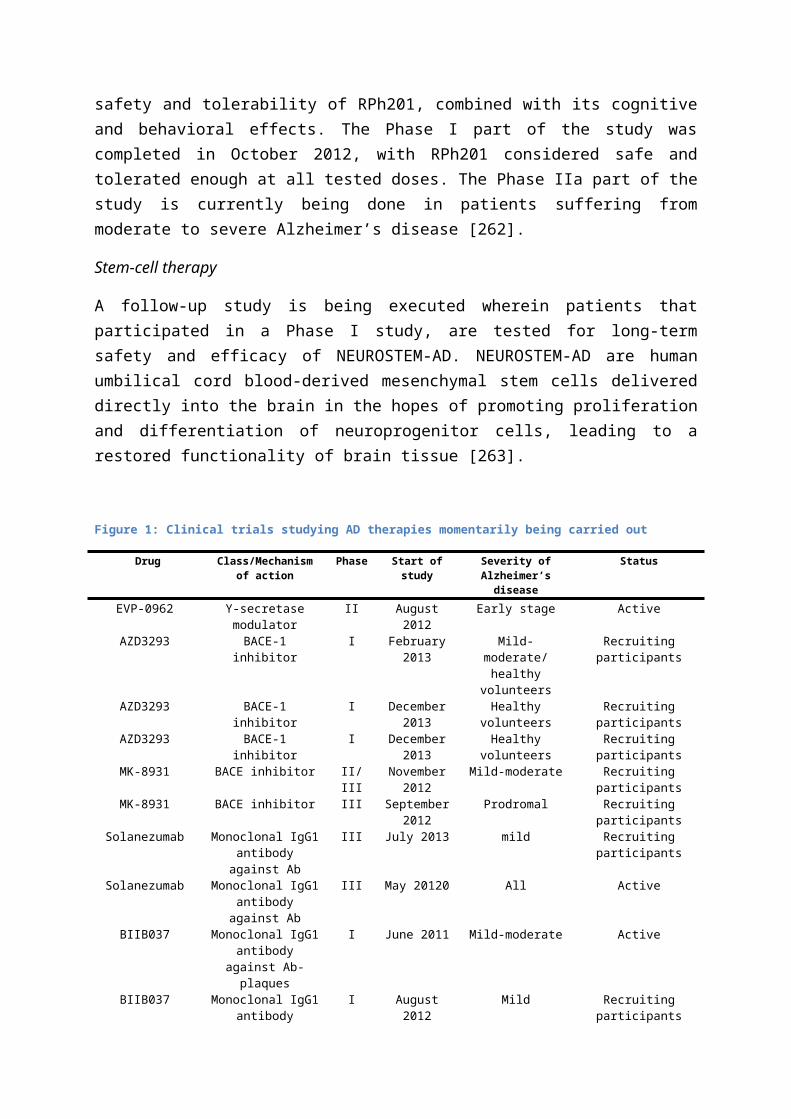
[161] S.P. Kennelly, L. Abdullah, D. Paris, J. Parish, V. Mathura. Demonstration of safety in Alzheimer's patients for intervention with an anti-hypertensive drug Nilvadipine: results from a 6-week open label study. Int J Geriatr Psychiatry. 2011 Oct;26(10):1038-45[162] Clinicaltrials.gov. A Phase III Trial of Nilvadipine to Treat Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT02017340. Last visited on 03-01-2014[163] J. Wang, K. Ono, D.L. Dickstein, I. Arrieta-Cruz, W. Zhao. Carvedilol as a potential novel agent for the treatment of Alzheimer's disease. 2011 Neurobiol Aging. Dec;32(12):2321.e1-12[164] Clinicaltrials.gov. Trial of Carvedilol in Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01354444. Last visited on 04-01-2014[165] C.M. Wischik, C.R. Harrington, J.M. Storey. Tau-aggregation inhibitor therapy for Alzheimer's disease. 2013 Biochem Pharmacol. Dec 19[166] Clinicaltrials.gov. Safety and Efficacy Study Evaluating TRx0237 in Subjects With Mild Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01689233. Last visited on 05-01-2014[167] Clinicaltrials.gov. Safety and Efficacy Study Evaluating TRx0237 in Subjects With Mild to Moderate Alzheimer's Disease , http://clinicaltrials.gov/ct2/show/NCT01689246. Last visited on 05-01-2014[168] Alzheimer forum. TrX0237. http://www.alzforum.org/therapeutics/trx0237. Last visited on 15-01-2014[169] Clinicaltrials.gov. Safety Study of AADvac1, a Tau Peptide-KLH-Conjugate Active Vaccine to Treat Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01850238. Last visited on 05-01-2014[170] Clinicaltrials.gov. 18-months Safety Follow-up Study of AADvac1, an Active Tau Vaccine for Alzheimer's Disease. http://clinicaltrials.gov/ct2/show/NCT02031198. Last visited on 23-01-2014[171] Clinicaltrials.gov. A Safety, Tolerability, Pharmacokinetics, Pharmacodynamics and Preliminary Efficacy Study of TPI-287 in Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01966666. Last visited on 05-01-2014[172] E.D. Levin, F.J. McClernon, A.H. Rezvani. Nicotinic effects on cognitive function: behavioral characterization, pharmacological specification, and anatomic localization. 2006 Psychopharmacology (Berl). Mar;184(3-4):523-39 [173] Clinicaltrials.gov. Efficacy, Safety, & Tolerability of AZD3480 Patients With Mild to Moderate Dementia of the Alzheimer's Type (AD), http://clinicaltrials.gov/ct2/show/NCT01466088. Last visited on 05-01-2014[174] L. Frölich, T. Ashwood, J. Nilsson, G. Eckerwall. Effects of AZD3480 on cognition in patients with mild-to-moderate Alzheimer's disease: a phase IIb dose-finding study. 2011 J Alzheimers Dis. 24(2):363-74[175] Clinicaltrials.gov. Study of the Safety and Clinical Effects of 2 Doses of EVP-6124 in Subjects With Alzheimer's Disease Who Complete Study EVP-6124-024 or EVP-6124-025, http://clinicaltrials.gov/ct2/show/NCT02004392. Last visited on 05-01-2014[176] J. Prickaerts, N.P. van Goethem, R. Chesworth, G. Shapiro, F.G. Boess. EVP-6124, a novel and selective α7 nicotinic acetylcholine receptor partial agonist, improves memory performance by potentiating the acetylcholine response of α7 nicotinic acetylcholine receptors. 2012 Neuropharmacology. Feb;62(2):1099-110[177] Clinicaltrials.gov. Study of the Safety and Effectiveness of Two Doses of Investigational Study Drug EVP-6124 in Subjects With Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01969136 last visited on 05-01-2014[178] Clinicaltrials.gov. Safety and Tolerability Study Evaluating a New Treatment for Subjects With Mild to Moderate Alzheimer's Disease http://clinicaltrials.gov/ct2/show/NCT01690195. Last visited on 23-01-2014[179] Clinicaltrials.gov. Bisnorcymserine in Healthy Adult Volunteers. http://clinicaltrials.gov/ct2/show/NCT01747213. Last visited on 23-01-2014[180] M.A. Kamal, P. Klein, Q.S. Yu, D. Tweedie, Y. Li. Kinetics of human serum butyrylcholinesterase and its inhibition by a novel experimental Alzheimer therapeutic, bisnorcymserine. 2006 J Alzheimers Dis. Sep;10(1):43-51[181] C.S. Brown, T.A. Kent, S.G. Bryant, R.M. Gevedon, J.L. Campbell. Blood platelet uptake of serotonin in episodic aggression. 1989 Psychiatry Res. Jan;27(1):5-12[182] J.P. Johnston, Some observations upon a new inhibitor of monoamine oxidase in brain tissue. Biochem Pharmacol. 1968 Jul;17(7):1285-97[183] J. Birks, L. Flicker. Selegiline for Alzheimer's disease. 2003Cochrane Database Syst Rev. (1):CD000442[184] Clinicaltrials.gov. MAyflOwer RoAD Study: A Study of RO4602522 in Patients With Moderate Severity

Alzheimer Disease on Background Alzheimer Disease Therapy, http://clinicaltrials.gov/ct2/show/NCT01677754. Last visited on 05-01-2014[185] Clinicaltrials.gov. A 3 Year Study to Evaluate the Safety and Efficacy of Low Dose Ladostigil in Patients With Mild Cognitive Impairment (MCI), http://clinicaltrials.gov/ct2/show/NCT01429623[186] M.B. Youdim. Multi target neuroprotective and neurorestorative anti-Parkinson and anti-Alzheimer drugs ladostigil and m30 derived from rasagiline. 2013 Exp Neurobiol. Mar;22(1):1-10[187] O. Weinreb, T. Amit, O. Bar-am, M.N. Youdim. Ladostigil: a novel multimodal neuroprotective drug with cholinesterase and brain-selective monoamine oxidase inhibitory activities for Alzheimer's disease treatment. 2012 Curr Drug Targets. Apr;13(4):483-94[188] Clinicaltrials.gov. Riluzole in Mild Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01703117. Last visited on 05-01-2014[189] R.G. Miller, J.D. Mitchell, D.H. Moore. Riluzole for amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND). 2012 Cochrane Database Syst Rev. Mar 14;3:CD001447[190] Clinicaltrials.gov Study of Lu AE58054 in Patients With Mild - Moderate Alzheimer's Disease Treated With Donepezil, http://clinicaltrials.gov/ct2/show/NCT01955161. Last visited on 05-01-2014[191] Clinicaltrials.gov. Lu AE58054 in Patients With Mild-moderate Alzheimer's Disease Treated With Donepezil, http://clinicaltrials.gov/ct2/show/NCT02006641. Last visited on 05-01-2014[192] J. Arnt, B. Bang-Andersen, B. Grayson, F.P. Bymaster, M.P. Cohen. Lu AE58054, a 5-HT6 antagonist, reverses cognitive impairment induced by subchronic phencyclidine in a novel object recognition test in rats. 2010 Int J Neuropsychopharmacol. Sep 13(8):1021-33[193] Clinicaltrials.gov. Lu AE58054 in Patients With Mild to Moderate Alzheimer's Disease Treated With an Acetylcholinesterase Inhibitor, http://clinicaltrials.gov/ct2/show/NCT02006654. Last visited on 05-01-2014[194] Clinicaltrials.gov. Randomized, Controlled Study Evaluating CERE-110 in Subjects With Mild to Moderate Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT00876863. Last visited on 05-01-2014[195] L. Tian, R. Guo, X. Yue, Q. Lv, X. Ye. Intranasal administration of nerve growth factor ameliorate β-amyloid deposition after traumatic brain injury in rats. 2012 Brain Res. Feb 27;1440:47-55[196] R. Nuydens, G. Dispersyn, M. de Jong, G. van den Kieboom, M. Borgers. Aberrant tau phosphorylation and neurite retraction during NGF deprivation in PC12 cells. 1997 Biochem Biophys Res Commun. Nov 26;240(3):687-91[197] V. Parthsarathy, C. Hölscher. Chronic treatment with the GLP1 analogue liraglutide increases cell proliferation and differentiation into neurons in an AD mouse model. 2013 PLoS One. 8(3):e58784[198] M.K. Sharma, J. Jalewa, C. Hölscher. Neuroprotective and anti-apoptotic effects of Liraglutide on SH-SY5Y cells exposed to Methylglyoxal stress. 2013 J Neurochem. Oct 1. doi: 10.1111/jnc.12469[199] H. Xiong, C. Zheng, J. Wang. J. Song, G. Zhao. The neuroprotection of liraglutide on Alzheimer-like learning and memory impairment by modulating the hyperphosphorylation of tau and neurofilament proteins and insulin signaling pathways in mice. 2013 J Alzheimers Dis. 37(3):623-35[200] Y. Yang, J. Zhang, D. Ma, M. Zhang, S. Hu. Subcutaneous administration of liraglutide ameliorates Alzheimer-associated tau hyperphosphorylation in rats with type 2 diabetes. 2013 J Alzheimers Dis. 37(3):637-48[201] Clinicaltrials.gov. Evaluating Liraglutide in Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01843075, 04-01-2014[202] T.R. Bonfirm, L. Forny-Germano, L.B. Sathler, J. Brito-Moreira, J.C. Houzel. An anti-diabetes agent protects the mouse brain from defective insulin signaling caused by Alzheimer's disease- associated Aβ oligomers. 2012 J Clin Invest. Apr 2;122(4):1339-53[203] Clinicaltrials.gov. A Clinical Trial of Exendin-4 for the Treatment of Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01255163. Last visited on 04-01-2014[204] H.J. Kim, K.S. Park, S.K. Lee, K.W. Min, K.A. Han. Effects of pinitol on glycemic control, insulin resistance and adipocytokine levels in patients with type 2 diabetes mellitus. 2012 Ann Nutr Metab. 60(1):1-5[205] Clinicaltrials.gov. A Single Site, Randomized, Double-blind, Placebo Controlled Trial of NIC5-15 in Subjects With Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01928420. Last visited on 05-01-2014[206] S. Craft, L.D. Baker, T.J. Montine, S. Minoshima, G.S. Watson, A. Claxton. Intranasal insulin therapy for Alzheimer disease and amnestic mild cognitive impairment: a pilot clinical trial. 2012 Arch Neurol.

Jan;69(1):29-38[207] Clinicaltrials.gov. The Study of Nasal Insulin in the Fight Against Forgetfulness (SNIFF), http://clinicaltrials.gov/ct2/show/NCT01767909. Last visited on 05-01-2014[208] Clinicaltrials.gov. Study of Nasal Insulin to Fight Forgetfulness - Long-acting Insulin Detemir - 120 Days (SL120) http://clinicaltrials.gov/ct2/show/NCT01595646. Last visited on 05-01-2014[209] Clinicaltrials.gov. Safety and Effectiveness Study of Intranasal Insulin Glulisine on Cognitive and Memory in Mild-Mod AD Patients. http://clinicaltrials.gov/ct2/show/NCT01436045. Last visited on 05-01-2014
Anti-inflammatory solutions[210] J.P. Kinet. The essential role of mast cells in orchestrating inflammation. 2007 Immunol Rev. Jun;217:5-7[211] T.C. Theoharides, D.E. Cochrane. Critical role of mast cells in inflammatory diseases and the effect of acute stress. 2004 J Neuroimmunol. Jan;146(1-2):1-12[212] G.L. Bowman, J.A. Kaye, M. Moore, D. Waichunas, N.E. Carlson. Blood-brain barrier impairment in Alzheimer disease: stability and functional significance. 2007 Neurology. May 22;68(21):1809-14[213] P. Dubreuil, S. Letard, M. Ciufolini, L. Gros, M. Humbert. Masitinib (AB1010), a potent and selective tyrosine kinase inhibitor targeting KIT. PLoS One. 2009 Sep 30;4(9):e7258[214] F. Piette, J. Belmin, H. Vincent, N. Schmidt, S. Pariel. Masitinib as an adjunct therapy for mild-to-moderate Alzheimer's disease: a randomised, placebo-controlled phase 2 trial. 2011 Alzheimers Res Ther. Apr 19;3(2):16[215] Clinicaltrials.gov. A Phase 3 Study to Evaluate the Safety and Efficacy of Masitinib in Patients With Mild to Moderate Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01872598. Last visited on 04-01-2014[216] E. Tobinick. Perispinal etanercept for treatment of Alzheimer's disease. 2007 Curr Alzheimer Res. Dec;4(5):550-2[217] E.L. Tobinick, H. Gross. Rapid cognitive improvement in Alzheimer's disease following perispinal etanercept administration. 2008 J Neuroinflammation. Jan 9;5:2[218] Clinicaltrials.gov. Short Term Efficacy and Safety of Perispinal Administration of Etanercept in Mild to Moderate Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01716637. Last visited on 04-01-2014[219] Clinicaltrials.gov GSK2647544 RD, DDI in Healthy Young and Elderly Volunteers, http://clinicaltrials.gov/ct2/show/NCT01978327. Last visited on 04-01-2013[220] M.P. Vitek, D.J. Christensen, D. Wilcock, J. Davis, W.E. van Nostrand. APOE-mimetic peptides reduce behavioral deficits, plaques and tangles in Alzheimer's disease transgenics. 2012 Neurodegener Dis.10(1-4):122-6
DIET[221] Clinicaltrials.gov. Prevention of Alzheimer's Disease by Vitamin E and Selenium (PREADVISE), http://clinicaltrials.gov/ct2/show/NCT00040378. Last visited on 04-01-2014[222] B.R. Cardoso, C. Cominetti, S.M. Cozzolini. Importance and management of micronutrient deficiencies in patients with Alzheimer's disease. 2013 Clin Interv Aging. 8:531-42[223] H. Vural, H. Demirin, Y. Kara, I. Eren, N. Delibas. Alterations of plasma magnesium, copper, zinc, iron and selenium concentrations and some related erythrocyte antioxidant enzyme activities in patients with Alzheimer's disease. 2010 J Trace Elem Med Biol. Jul 24(3):169-73[224] C. Smorgon, E. Mari, A.R. Atti, E. Dalla Nora, P.F. Zamboni. Trace elements and cognitive impairment: an elderly cohort study. 2004 Arch Gerontol Geriatr Suppl. (9):393-402[225] L.A. Boothby, P.L. Doering. Vitamin C and vitamin E for Alzheimer's disease. 2005 Ann Pharmacother. Dec;39(12):2073-80[226] J. Machado, C.L. Caram, A.A. Frank, A. Eede Soares, J. Laks. Nutritional status in Alzheimer's disease. 2009 Rev Assoc Med Bras. Mar-Apr;55(2):188-91[227] J.A. Luchsinger, R. Mayeux. Dietary factors and Alzheimer's disease. 2004 Lancet Neurol. Oct;3(10):579-87[228] Clinicaltrials.gov. Study to Evaluate Dietary Supplementation With a Version of Anatabloc(R) in Subjects With Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01669876. Last visited on 05-01-2014[229] K. Castagnoli, J.B. Petzer, S.J. Steyn, C.J. van der Schyf, N. Castagnoli. Inhibition of human MAO-A and MAO-B by a compound isolated from flue-cured tobacco leaves and its neuroprotective properties in the MPTP mouse model of neurodegeneration. 2003Inflammopharmacology. 11(2):183-8 [230] Y. Gu. N. Schupf, S.A. Cosentino, J.A. Luchsinger, N. Scarmeas. Nutrient intake and plasma β-amyloid. 2012 Neurology.Jun 5;78(23):1832-40[231] Clinicaltrials.gov. Lipoic Acid and Omega-3 Fatty Acids for Alzheimer's Disease. http://clinicaltrials.gov/ct2/show/NCT01058941. Last visited on 05-01-2014

[232] Clinicaltrials.gov. Pilot Study: Lipoic Acid and Omega-3 Fatty Acids for Alzheimer's Prevention. http://clinicaltrials.gov/ct2/show/NCT01780974. Last visited on 05-01-2014[233] E.M. Reiman, K. Chen, G.E. Alexander, R.J. Caselli, D. Bandy. Functional brain abnormalities in young adults at genetic risk for late-onset Alzheimer's dementia. 2004 Proc Natl Acad Sci U S A. Jan 6;101(1):284-9[234] Clinicaltrials.gov AC-1204 26-Week Long Term Efficacy Response Trial With Optional Open-label Ext, http://clinicaltrials.gov/ct2/show/NCT01741194. Last visited on 05-01-2014[235] K. Xu, X.L. Dai, H.C. Huang, Z.F. Jiang. Targeting HDACs: a promising therapy for Alzheimer's disease. 2011 Oxid Med Cell Longev. 2011:143269[236] S. Michan, D. Sinclair. Sirtuins in mammals: insights into their biological function. 2007 Biochem J. May 15;404(1):1-13[237] T.C. Karagiannis, K. Ververis. Potential of chromatin modifying compounds for the treatment of Alzheimer's disease. 2012 Pathobiol Aging Age Relat Dis. 2[238] F. Tippmann, J. Hundt, A. Schneider, K. Endres, F. Fahrenholz. Up-regulation of the alpha-secretase ADAM10 by retinoic acid receptors and acitretin. 2009 FASEB J. Jun;23(6):1643-54[239] G. Donmez, D. Wang, D.E. Cohen, L. Guarente. SIRT1 suppresses beta-amyloid production by activating the alpha-secretase gene ADAM10. 2010 Cell. Jul 23;142(2):320-32[240] V. Vingtdeux, P. Marambaud. Identification and biology of α-secretase. 2012 J Neurochem. Jan;120 Suppl 1:34-45[241] S.W. Min, S.H. Cho, Y. Zhou, S. Schroeder, V. Haroutunian. Acetylation of tau inhibits its degradation and contributes to tauopathy. 2010 Neuron. Sep 23;67(6):953-66[242] M.T. Heneka, M.K. O’Banion, D. Terwel, M.P. Kummer. Neuroinflammatory processes in Alzheimer's disease. 2010 J Neural Transm. Aug;117(8):919-47 [243] T.S. Anekonda. Resveratrol--a boon for treating Alzheimer's disease? 2006 Brain Res Rev. Sep;52(2):316-26[244] Clinicaltrials.gov. Resveratrol for Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01504854. Last visited on 05-01-2014[245] K.N. Green, J.S. Steffan, H. Martinez-Coria, X. Sun, S.S. Schreiber. Nicotinamide restores cognition in Alzheimer's disease transgenic mice via a mechanism involving sirtuin inhibition and selective reduction of Thr231-phosphotau. 2008 J Neurosci. Nov 5;28(45):11500-10[246] H. Ding, P.J. Dolan, G.V. Johnson. Histone deacetylase 6 interacts with the microtubule-associated protein tau. 2008 J Neurochem. Sep;106(5):2119-30[247] Y.I. Francis, M. Fà, H. Ashraf, H. Zhang, A. Staniszewski. Dysregulation of histone acetylation in the APP/PS1 mouse model of Alzheimer's disease. 2009 J Alzheimers Dis.18(1):131-9 [248] M. Kilgore, C.A. Miller, D.M. Fass, K.M. Hennig, S.J. Haggarty. Inhibitors of class 1 histone deacetylases reverse contextual memory deficits in a mouse model of Alzheimer's disease. 2010 Neuropsychopharmacology. Mar;35(4):870-80[249] Y. Su, J. Ryder, B. Li, X. Wu, N. Fox. Lithium, a common drug for bipolar disorder treatment, regulates amyloid-beta precursor protein processing. 2004 Biochemistry. Jun 8;43(22):6899-908[250] H. Qing, G. He, P.T. Ly, C.J. Fox, M. Staufenbiel. Valproic acid inhibits Abeta production, neuritic plaque formation, and behavioral deficits in Alzheimer's disease mouse models. 2008 J Exp Med. Nov 24;205(12):2781-9[251] A.S. Fleischer, D. Truran, J.T. Mai, J.B. Langbaum, P.S. Aisen. Chronic divalproex sodium use and brain atrophy in Alzheimer disease. 2011 Neurology. Sep 27;77(13):1263-71[252] H. Ryu, K. Smith, S.I. Camelo, I. Carreras, J. Lee. Sodium phenylbutyrate prolongs survival and regulates expression of anti-apoptotic genes in transgenic amyotrophic lateral sclerosis mice. 2005 J Neurochem. Jun;93(5):1087-98[253] A. Ricobaraza, M. Cuadrado-Tejedor, A. Pérez-Mediavilla, D. Frechilla, J. Del Río. Phenylbutyrate ameliorates cognitive deficit and reduces tau pathology in an Alzheimer's disease mouse model. 2009 Neuropsychopharmacology. Jun;34(7):1721-32[254] N.A. Abramova, D.S. Cassarino, S.M. Khan, T.W. Painter, J.P. Bennett. Inhibition by R(+) or S(-) pramipexole of caspase activation and cell death induced by methylpyridinium ion or beta amyloid peptide in SH-SY5Y neuroblastoma. 2002 J Neurosci Res. Feb 15;67(4):494-500[255] Clinicaltrials.gov. Safety Study of R(+)Pramipexole to Treat Early Alzheimer's Disease. http://clinicaltrials.gov/ct2/show/NCT01388478. Last visiteid on 23-01-2014[256] Clinicaltrials.gov. Study of the Safety & Efficacy of Granulocyte-Macrophage Colony-Simulating Factor (Leukine) in the Treatment of Alzheimer's Disease. http://clinicaltrials.gov/ct2/show/NCT01409915. Last visited on 23-01-2014[257] T.D. Boyd, S.P. Bennett, T. Mori, M. Runfeldt, M. Norden. GM-CSF upregulated in rheumatoid arthritis reverses cognitive impairment and amyloidosis in Alzheimer mice. 2010 J Alzheimers Dis. 21(2):507-18[258] Clinicaltrials.gov. Zydena on Cognitive Function of Alzheimer's Disease Patients,

http://clinicaltrials.gov/ct2/show/NCT01940952. Last visited on 05-01-2014[259] T. Tully. Regulation of gene expression and its role in long-term memory and synaptic plasticity. 1997 Proc Natl Acad Sci U S A. Apr 29;94(9):4239-41[260] J.C. Yin, T. Tully. CREB and the formation of long-term memory. 1996 Curr Opin Neurobiol. Apr;6(2):264-8[261] A. García-Osta, M. Cuadrado-Tejedor, C. García-Barroso, J. Oyarzábal, R. Franco. Phosphodiesterases as therapeutic targets for Alzheimer's disease. ACS 2012 Chem Neurosci. Nov 21;3(11):832-44[262] Clinicaltrials.gov. A Randomized SAD and MAD Study Evaluating the Safety and Tolerability of RPh201 in Healthy Subjects and in Adults With Alzheimer's Disease, http://clinicaltrials.gov/ct2/show/NCT01513967. Last visited on 05-01-2014[263] Clinicaltrials.gov. The Long-Term Safety and Efficacy Follow-Up Study of Subjects Who Completed the Phase I Clinical Trial of Neurostem®-AD, http://clinicaltrials.gov/ct2/show/NCT01696591. Last visited on 05-01-2014





























