Embed Size (px)
Citation preview
Department of Health
PO Box 2060, Cape Town, 8000
Mobile:
For more information contact: Michele Twomey (SATS Implementation Advisor)
+27 850 3281 email: [email protected]
The South AfricanTriage Scale
(SATS)
Training manual 2012
Departmental Website: www.health.gov.za
Provincial Website: www.westerncape.gov.za

ISATS TRAINING MANUAL 2012
Table of Contents
TABLE OF COnTEnTs
Table of Contents IAcknowledgements II1. Introduction 1 1.1 ThebenefitsofimplementingSATS 1 1.2 Triagerequirements 2 1.3 Whoshouldbethetriageprovider? 2 1.4 Terminologyandkeyconcepts 3 AssessmentQuestions 5
2. TheSATSprocessflowchart 6 2.1 Thefivestepapproach 6 2.2 TheSATSprocessflowchart 6 2.3 SATSprioritylevels 6 2.4 Terminologyandkeyconcepts 7 AssessmentQuestions 7 AdultSATSChart 8 PaediatricSATSChart 10
3. Adult Clinical signs 12 3.1 Emergency signs 12 3.2 Very urgent signs 12 3.3 Urgent signs 13 AssessmentQuestions 13
4. Paediatric Clinical signs 14 4.1 Emergency signs: the abc-c-c-do approach 14 4.1.1 Abairwayandbreathingareusuallyassessedtogether 14 4.1.2 Ccirculationassessment 16 4.1.3 C-ccomaandconvulsionsassessment 16 4.1.4 Dseveredehydrationassessment 17 4.1.5 Ootheremergencysigns 18 4.2 Very urgent signs 18 4.3 Urgent signs 21 AssessmentQuestions 24
5. Triage Early Warning score TEWs 25 5.1Observationsattriage 26 5.2Terminologyandkeyconcepts 26 AssessmentQuestions 27
6. AdditionalInvestigations 28 AssessmentQuestions 29
7. Additional Tasks 30 AssessmentQuestions 32
8. Triage in Context 33 8.1 Pre-Hospital 33 8.2 Patientstreaming 33 8.3 Infrastructure 33 8.4 Alignmentofstafftotemporalflowofpatients 33
9. summary 3410. References 34
1SATS TRAINING MANUAL 2012II SATS TRAINING MANUAL 2012
Introduction
InTRODUCTIOn
LearningObjectives:
• UnderstandthepurposeoftriageandthebenefitsofimplementingtheSATS• Befamiliarwiththerequirementsforstandardisedtriageimplementation• Understandtheterminologyandkeyconceptsaroundtriage
Anine-montholdbabyboyiscarriedintothechildren’ssectionoftheoutpatientdepartmentinhismother’sarms.Heappearstobeasleep.Atthetriagedeskheisseenbyanurseandfoundtohavelipsandtonguethataregrey/blueincolour,andheistakenstraightintotheresuscitationroomasanemergency.Intheresuscitationroomheisgivenoxygenat15litres/minutebyfacemaskwithanon-rebreatherreservoirbag.Heisnotedtobegruntingandbreathingveryfast.Hishandsarecoldtotouchandthecapillaryrefilltimeisprolongedtofourseconds.Anintravenouscannulaisplaced.Abloodsampleistakenatthesametimeforbloodglucose,fullbloodcountandbloodculture.Anintravenousinfusionofnormalsalineiscommencedat20ml/kgtorunasfastasitcango.Othertreatmentsaregiven,dependingontheresultoftheinvestigationsandtheresponsetothetreatmenthereceives.Itisnow18minutessincethebabycamethroughtheoutpatientdepartment’sdoor,andhissituationisstable.Itisnowtimetotakeafullhistoryandcarryoutafullexaminationtomakeadefinitivediagnosis.Heisdiagnosedashavingveryseverepneumonia,andreceivesspecifictreatmentforthis.However,beforecomingtothisdiagnosis,notimewaswasted,hisstatuswasstabilized,basedonafewleadingsignsandsymptoms,evenwhenthemedicalstaffdidnotknowexactlywhatwaswrongwithhim.Thiswasgoodtriageandemergencymanagement.Wouldithavehappenedlikethisinyourhospital?Inthistrainingcourse,youaregoingtoacquirethenecessaryknowledgeforthecorrecttriageofsickchildrenandadults.Manydeathsinhospitaloccurwithin24hoursofadmission.Someofthesedeathscanbepreventedifverysickpatients(especiallychildren)arequicklyidentifiedontheirarrivalandtreatmentisstartedwithoutdelay.Inmanyhospitalsaroundtheworld,childrenarenotcheckedbeforeaseniorhealthworkerexaminesthem;asaresult,someseriouslyillpatientshavetowaitaverylongtimebeforetheyareseenandtreated.Childrenareknowntohavediedofatreatableconditionwhenwaitinginthequeuefortheirturn.Theideaoftriageistopreventthisfromhappening.Thepurposeoftriageistoprioritisepatientsbasedonmedicalurgencyincontextswherethereisamismatchbetweendemandandcapacity(i.e.patientloadoverwhelmstheavailableresources).
1.1ThebenefitsofimplementingSATS1. expeditethedeliveryoftime-criticaltreatmentforpatientswithlife-threateningconditions.2. ensurethatallpatientsareappropriatelyprioritisedaccordingtotheirmedicalurgency.3. improvepatientflow.4. improvepatientsatisfaction.5. decreasethepatient’soveralllengthofstay.6. facilitatestreamingoflessurgentpatients.7. provideauser-friendlytoolforalllevelsofhealthcareprofessionals.
ByintroducingtheSATSatapublicurbanhospitalinCapeTown,meanwaitingtimeswerereducedsignificantlyforallprioritylevelsexceptthenon-urgentgreencategory.Themostdramaticreductioninwaitingtimeswasseeninpatientscodedasred(82%).1
1
Acknowledgements
ACKnOWLEDGEMEnTs
TheSouthAfricanTriageGroup(SATG)wouldliketothankthePaediatricTriageWorkingGroup(PTWG)oftheWesternCapeGovernment(WCG)ofSouthAfrica(SA)(undertheauspicesofthePaediatricProvincialCo-ordinatingCommittee&theEmergencyMedicineProvincialCo-ordinatingCommittee)fortheireffortsandhardworkindevelopingpaediatrictriagebasedontwoexistingtriagetools:theEmergencyTriageAssessmentandTreatment(ETAT)oftheWorldHealthOrganization(WHO)andtheSouthAfricanTriageScale(SATS).
TheSATGandPTWGwishestoacknowledgetheWHODepartmentofChildandAdolescentHealthandDevelopmentandProfessorElizabethMolyneux,whodevelopedtheETATtrainingcourseonwhichthesecoursematerialsarebased.WearealsogratefultotheETAT-SouthAfrica(ETAT-SA)workinggroupforalltheireffortsandhardworkinadaptinganddevelopingthegenericETATmaterialsintotheETAT-SAmaterialsspecificallyfortheSouthAfricansetting.
AllreasonableprecautionshavebeentakenbythePTWG,theETAT-SAworkinggroup,WHOandSATSgrouptoverifytheinformationcontainedinthispublication.However,thepublishedmaterialisbeingdistributedwithoutwarrantyofanykind,eitherexpressorimplied.Theresponsibilityfortheinterpretationanduseofthemateriallieswiththereader.InnoeventshallthePTWG,theETAT-SAworkinggroup,WHOortheSATGbeliablefordamagesarisingfromitsuse.
Dr Baljit Cheema and Dr Michèle Twomey
On behalf of the Paediatric Triage Working Groupand thesouth African Triage Group
Paediatric TriageWorking Group AnthonyWestwoodBaljitCheemaHeloiseBuysJeanAugustynHeatherTuffinMichaelLeeAndrewArgentShaheemdeVriesLeeWallisZaneleNxumaloLouiseCookePeterLeschMajedahIsmailLieslStraussAngeladeSáJacoSlabbertWendyRosenthalMichèleTwomey
ETAT-sAWorking Group
LesleyBamfordGerryBoonHeloiseBuysBaljitCheemaSueHarrisMarkPatrickCindyStephenChrisSutton

3SATS TRAINING MANUAL 20122 SATS TRAINING MANUAL 2012
1.4 Terminology and key concepts1. Triage,fromtheFrenchword“trier”,literallymeans:“tosort”.Theaimistobring“thegreatest
goodtothegreatestnumberofpeople”–thisisachievedthroughprioritisinglimitedresourcestoachievethegreatestpossiblebenefit.Patientsaresortedwithascientifictriagescaleinorderofurgency-theendresultisthatthepatientwiththegreatestneedishelpedfirst.
2. Patient to triage:forthehospitalorcliniccontextthisreferstoapatientthatappearsrelativelystableandisabletomobilisehim/herselftothedesignatedtriagearea.Thiswillbethetypeoftriageusedformosthospitalandcliniccases.
3. Triage to patient:herethepatientisusuallyunstable.Thepatientisunabletomobilisehim/herselftothedesignatedtriageareaandwillneedtobetriagedwheretheyarefound.Theymayneedtobereferreddirectlytotheresuscitation(resus)areaiftheyareatahealthfacility.Triagemayalsobeperformedatthebedsideanddocumentedinretrospect.Thistypeoftriagewillbeusedlessofteninthehospitalcontextandpredominantlyinthepre-hospitalcontext.
4. Physiology(i.e.vitalsigns):referstothenormalfunctioningofthedifferentbodysystems.Someofthephysiologycanbereadilymeasured(e.g.pulse,bloodpressure,respiratoryrate,temperature).
5. TEWs: Triage Early Warning score.Thisisacompositescoreofthepatient’sphysiology.Thescoreisderivedbyassigninganumberbetween0and2foreachofthepatient’svitalsigns.Thehigherthescorethegreatertheurgency.
6. streaming:theuseofdedicatedhealthcareresourcesforeachprioritygroupofpatients.Forgreenpatients,thismaybeadoctorornursepractitioner:thispersonneedstheirownspacetoseethesepatients.
7. Pain:Severepainisunbearable,theworstpainthepatienthaseverfelt.Itmaybeassociatedwithsweatiness,paleness,andalteredlevelofconsciousness.Moderatepainisintense,butbearable.Mildpainisanyotherpain.Remembertodoapainassessmentoneverypatientthatyousee.
8.
!AdditionalInvestigation:Youwillfindthisexclamationiconinlaterchapters. Itrepresentsanadditionalinvestigationwhichmayleadtoachangeinthepatient’striageprioritylevel.Checkingthebloodglucoseconcentrationormeasuringtheoxygensaturationlevelareexamplesofadditionalinvestigations.Sectionsixoutlinesallkeyadditionalinvestigationsimportantattriage.TheycanalsobefoundontheSATScharts.
9. Warning: Thelightbulbiconindicatesawarningthatusuallyfollowsimmediatelyafteranadditionalinvestigation,implyingthatsomeimmediateactionisrequired(e.g.achildwhoseoxygensaturationlevelsarefoundtobe80%requiresoxygenadministrationandshouldbetakentotheresuscitationarea).
10. Additional tasks: Theiconwitharedcrossrepresentsadditionaltasksthatarebeneficialtothepatientifinitiatedattriage.Theseadditionaltasksdonotchangethepatient’striageprioritylevel.Examplesincludestartingoralrehydrationtherapyforachildthatisdehydrated,coolingaburnthatoccurredwithin3hoursorapplyingdirectpressuretoanuncontrolledhaemorrhage.
1.2 Triage requirements Triageissimpletodo,butinordertostandardisetheprocessandcomprehensivelyimplementtheSATSasavalidatedtoolcertainrequirementsneedtobemet.Table1showstheequipmentneededfortheprocessandAppendixAonpage4includesadetailedchecklistofrequirements.
Location Equipment Additional equipment
Privacy:Screen,partitionorseparateroom.
Gloves,facemasks&otherbarrierprotectivedevices
Pulseoximeterwithpaediatricprobes
Safety:Security/protected Wallclock ECG
Sizeofarea:pushchairs,wheelchairs,stretchers
Lowreadingelectronic/mercurythermometer
Fingerprickmachine,haemoglobinandglucometermeasurement
Accessibility VitalsignsmonitorORbauma-nometerwithpaediatriccuffs
Urinecollectioncontainers,urinedipsticks&urinepregnancytests
Baby-changingfacilities Drydressings/bandages
Table 1: Requirements for adequate / efficient triage
1.3Whoshouldbethetriageprovider?Nurse-basedtriagehasbeensuccessfullyimplementedworldwideinthecountriesofNorthAmerica,Europe,theMiddleEastandAustralasiasincethedevelopmentofEmergencyMedicineasaspecialityabout30yearsago.Table2showsthenumberofmedicalpractitionersandnursesperunitofpopulationinSouthAfrica,comparedtosome“developed”countries.Giventhesignificantlylowerdoctor:nurseratioinSouthAfricacomparedtocountrieswherenursetriageiswidelypracticed,itisapparentthatthedevelopmentofnurse-basedtriageshouldbeapriorityinoursetting.
Country Rate per 100,000 population/ year
Doctors nurses Doctor: nurse ratio
SouthAfrica 56.3 471.2 1:8.0
Canada 229 897 1:4.0
Australia 240 830 1:3.4
Israel 385 613 1:1.6
UK 164 479 1:3.0
Table 2: Doctor and nurse rates per 100,000 population per annum for selected countries
NursesarethefirstmedicalcontactforthepatientsattendingtheEmergencyCentreinmostinstances.InSouthAfricanstudies,adequatelytrainedEnrolledNursingAssistants(ENAs)havebeenshowntobeaccuratetoadegreecomparablewithinternationalstandardsofnursingtriage.2 3 TheSouthAfricanTriageScaleshouldbeknownandappliedbyallhealthcareprofessionalsinvolvedintheEmergencyCentre.Thetriageprovidercanbethemedicalofficer,theregisterednurse,enrollednurseortheENA.Thepurposeofthistrainingprogramistoempowertheindividualwhoparticipateswiththeknowledgetotriage.Itwillonlybethroughpracticeandrepetitionthataproviderwillbecomeskilledwithtriage.Successfulprovidersarethereforeencouragedtoparticipateintriagingasfrequentlyaspossibleinordertostayinpracticeanduptodate.
IntroductionIntroduction

5SATS TRAINING MANUAL 20124 SATS TRAINING MANUAL 2012
APPEnDIX A: Checklist of triage emergency centre requirements
structural Requirements
Doesthetriageareameetthefollowingcriteria: Yes No
1 Isthetriageareaadedicatedspace?
2 Isthetriageareawellsigned?
3 Isthetriageareasecure(i.e.behindthesecuritygate,orineasyviewofsecuritystaff)?
4 Isthetriageareaatleast10squaremetersinsize(i.e.shouldbeabletoaccommodateanurse,patientinawheelchairandrelativeorcarer)?
Checklist of triage Infrastructure Requirements
Content Requirements
Doesthetriageareacontainthefollowing: Yes No
1 Adeskandchair?
2 Triagepaperworkforadult,childrenandinfants?
3 Awallclockwithasecondhand?
4 Astethoscope?
5 Alowreadingthermometer?
6 Drydressingsandbandages?
7 Gloves?
8 Sphygmomanometer(manual,digitalorelectronic)?
9 Bloodglucosemonitor?
10 AmeasuringtapeORmarksdisplayedonwallintriageareatomeasurechildren(i.eonemarkat95cmandoneat150cm)?
11 2xdifferentSATSpostersprominentlydisplayedintriagearea?
12 SATSmanualreadilyavailablefortriageofficeasasourceofinfo?
13 SATSpatientinfoleafletprominentlydisplayedinthewaitingarea?
14 Triageregisterorcomputerwithregister?
15 Whiteboardtotrackandcommunicatetootherstaffacuityofthosetriaged?
Assessment QuestionsClearlyindicatewhetherthefollowingstatementsaretrueorfalse:
1. Thepurposeoftriageistopreventdeteriorationordeathofapatientwhilewaitinginthequeuefortheirturn.
True False
2. Thetriagemethodshouldbeknownandappliedbyclinicalnursepractitionersonly.
True False
3. Streamingistheprocessofgettingpatientstowaitforaslongaspossible.
True False
Choosethecorrectanswer:4. Thebenefitsoftriageare: (a) Tofacilitatestreamingofgreenpatients (b) Todecreasethewaitingtimeoflife-threateningconditions (c) Toensurethatpatientsareappropriatelyprioritizedbyurgency (d) Topreventchildrenfromdyinginthewaitingroom (e) Alloftheabove
5. TEWSisshortfor: (a) TriageEarlyWarningSystem (b) TraumaEarlyWarningScale (c) TriageEmergencyWarningSystem (d) TriageEarlyWarningScore (e) TraumaEmergencyWaitingScore
IntroductionIntroduction

7SATS TRAINING MANUAL 20126 SATS TRAINING MANUAL 2012
TheSATSprocessflowchart
ThE sATs PROCEss FLOWChART
LearningObjectives:
• UnderstandthefivestepapproachandSATSprocessflowchart• BefamiliarwiththetwoversionsoftheSATSchart• BefamiliarwiththeprioritylevelsofSATS
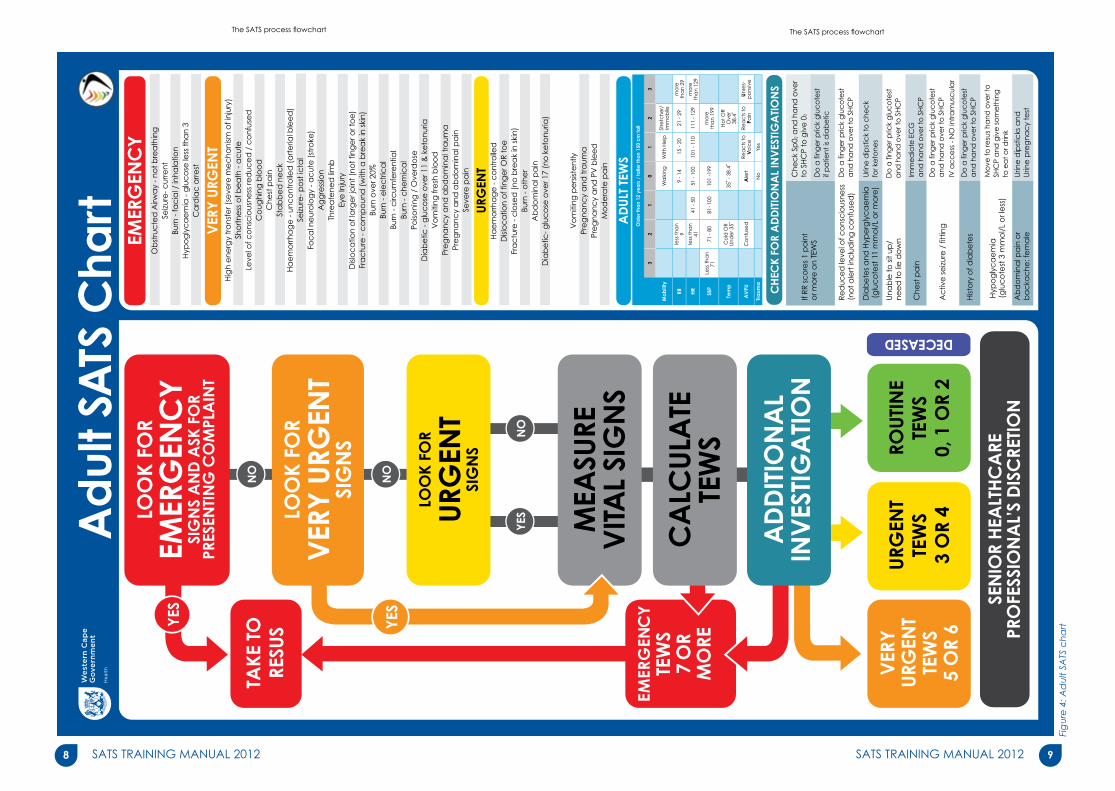
2.1Thefivestepapproachstep 1: Look for emergency signs and ask for the presenting complaintStep2: LookforveryurgentORurgentsignsStep3: MeasurethevitalsignsandcalculatetheTEWSStep4: CheckkeyadditionalinvestigationsStep5: Assignfinaltriageprioritylevel
Figure 1: SATS five step approach
Theprocessoftriagestartswithaquestiontothemother/carer/patientastothereasonforcomingtotheemergencycentre.AsthisquestionisbeingaskedandansweredthetriageprocessalreadycommenceswiththetriagepractitionerrapidlyassessingthepatientforanyEmergency clinical signs.TheAirway,Breathing,Circulation,Coma,Convulsion,Dehydration,Other(ABC-c-c-DO)approachisusedforpaediatricpatients.Ifemergencyclinicalsignsarefound,thepatientisassignedaRedprioritylevelandtakenstraighttotheresuscitationareawithoutdelay.IfnoEmergencyclinicalsignsarepresentthencheckforanyVery Urgent or Urgentclinicalsigns.Whetherthesearepresentornot,vitalsignsaremeasured,theTEWSiscalculated,keyadditionalinvestigationsarecheckedandthetriagepriorityadjustedasshowninFigure2.ItisimportanttonotethatifapatienthasanyemergencysignsthenaTEWSdoesNOTneedtobecalculatedattriage.Thereshouldbenodelayintakingthepatienttotheresuscitationarea.Finallytheseniorhealthcareprofessional’s(SHCP)discretionasseeninFigure2,allowstheclinicalnursepractitionerorseniordoctortooverridethefinaltriagepriorityassigned.
2.2TheSATSprocessflowchartTherearetwoversionsoftheSATSchartasseeninFigure4and5.ThepaediatricversionoftheSATSchartisusedtotriageallpatientsyoungerthan12yearsandsmallerthan150cm.TheadultversionoftheSATSchartisusedtotriagepatientsolderthan12yearsortallerthan150cm.BothagespecificversionshavetheexactsameSATSprocessflowchartasdepictedinFigure2.ThefivestepsinFigure1areintegratedintothisprocessflowchart.ThedifferencesarefoundintheirrespectiveclinicalsignsandtheirageappropriateTEWS.Thenexttwosectionsdescribeindetailtheadultandpaediatricclinicalsignsrespectively.
2.3SATSprioritylevelsTheSouthAfricanTriageScalehasfourprioritylevelsasshowninTable3.Eachprioritylevelshouldideallybemanagedwithinthetargettimetotreatment.
2
YES NO
NO
NO
LOOK FOREMERGENCY
SIGNS AND ASK FORPRESENTING COMPLAINT
VERYURGENT
TEWS5 OR 6
EMERGENCYTEWS7 OR
MORE
TAKE TORESUS
URGENTTEWS
3 OR 4
ROUTINETEWS
0, 1 OR 2 DEC
EASE
D
LOOK FOR
URGENTSIGNS
CALCULATETEWS
SENIOR HEALTHCAREPROFESSIONAL’S DISCRETION
ADDITIONALINVESTIGATION
MEASUREVITAL SIGNS
YES
LOOK FORVERY URGENT
SIGNS
YES
Figure 2: The SATS process flowchart
TheSATSprocessflowchart
2.4 Terminology and key concepts1. RedvsResus:PatientsmaybetriagedRedonthebasisoftheirpresentation,butnot
necessarilybeafullresuscitationcase.Conversely,ifapatientpresentstoyouasaresusyoudonotneedatriagetooltotellyouthattheyareaRedcase.Forthosepatientswhopresentlikethis(e.gCardiacarrest),triagebeforetreatmentisnotnecessary–ifapatientisaresus,theyareRedbydefinition.
2. MajorsvsMinors:Themajorsareainahospitalisstaffedbyappropriatelytrainedpersonnelandadvancedequipmenttodealwithemergency,veryurgentandurgentpatients.Theminorsareaisstaffedbyappropriatelytrainedpersonnelandtherespectiveequipmentandresourcestodealwithroutineornon-urgentpatients.
Priority COLOUR Target time Management
RED IMMEDIATE Taketotheresuscitationroomforemergencymanagement
ORAnGE < 10 mins Refertomajorsforveryurgentmanagement
YELLOW < 1 hour Refertomajorsforurgentmanagement
GREEn < 4 hours Refertodesignatedareafornon-urgentcases
BLUE < 2 hours Refertodoctorforcertification
Table 3: SATS priority levels and target times to be seen with-in
Assessment QuestionsClearlyindicatewhetherthefollowingstatementsaretrueorfalse:
1. TherearetwoSATScharts–oneforpaediatricpatientsandoneforadultpatients.
True False
2. Ifanemergencysignisidentifiedinthefirststep,thepatientistakentotheresuscitationareaimmediately.
True False
3. Ifnoemergencysignsareidentifiedinstepone,butanurgentsignisidentifiedinsteptwo,thepatientisimmediatelytriagedyellowandaskedtowait.
True False
Choosethecorrectanswer:4. TheSATSprioritylevelOrangeisdefinedas: (a)Emergencyrequiringimmediateintervention (b) VeryUrgentrequiringinterventionwithin10minutes (c) Urgentrequiresinterventionwithin60minutes (d) Routinerequiringinterventionwithin240minutes (e) Lifethreateningbutnotrequiringanyintervention
5. Theseniorhealthcareprofessional’sdiscretionrefersto: (a) Thejuniornurseoverridingthefinaltriagedecision (b) Theclinicalnursepractitioneroverridingthefinaltriagedecision (c) Themedicalstudentoverridingthefinaltriagedecision (d) Themedicalofficeroverridingthefinaltriagedecision (e) banddabove
9SATS TRAINING MANUAL 20128 SATS TRAINING MANUAL 2012
TheSATSprocessflowchart TheSATSprocessflowchart
Figu
re 4
: Ad
ult S
ATS
cha
rt
Ad
ult S
ATS
Cha
rt
YES
NO
NO
NO
LOO
K FO
REM
ERG
ENC
YSI
GN
S A
ND
ASK
FO
RPR
ESEN
TIN
G C
OM
PLA
INT
VER
YU
RGEN
TTE
WS
5 O
R 6
EMER
GEN
CY
TEW
S7
OR
MO
RE
TAKE
TO
RESU
S
URG
ENT
TEW
S3
OR
4
ROU
TIN
ETE
WS
0, 1
OR
2
DECEASEDLO
OK
FOR
URG
ENT
SIG
NS
CA
LCU
LATE
TEW
S
SEN
IOR
HEA
LTH
CA
REPR
OFE
SSIO
NA
L’S
DIS
CRE
TIO
N
AD
DIT
ION
AL
INV
ESTI
GA
TIO
N
MEA
SURE
VIT
AL
SIG
NS
YES
LOO
K FO
RV
ERY
URG
ENT
SIG
NS
YES
EMER
GEN
CY
Ob
stru
cte
d A
irwa
y - n
ot b
rea
thin
gSe
izure
- cur
rent
Burn
- fa
cia
l / in
hala
tion
Hyp
og
lyc
ae
mia
- g
luc
ose
less
tha
n 3
Ca
rdia
c a
rrest
VER
Y U
RGEN
T
URG
ENT
AD
ULT
TEW
S
Vo
miti
ng p
ers
iste
ntly
Pre
gna
ncy
and
tra
uma
Pre
gna
ncy
and
PV
ble
ed
Mo
de
rate
pa
in
Ha
em
orrh
ag
e -
co
ntro
lled
Disl
oc
atio
n o
f fin
ge
r OR
toe
Fra
ctu
re -
clo
sed
(no
bre
ak
in s
kin)
Burn
- o
the
rA
bd
om
ina
l pa
inD
iab
etic
- glu
co
se o
ver 1
7 (n
o k
eto
nuria
)
If RR
sc
ore
s 1
po
int
or m
ore
on
TEW
S
Che
ck
Sp02
and
ha
nd o
ver
to S
HC
P to
giv
e 0
2
Do
a fi
nge
r pric
k g
luc
ote
sta
nd h
and
ove
r to
SH
CP
Do
a fi
nge
r pric
k g
luc
ote
stif
pa
tient
is d
iab
etic
Do
a fi
nge
r pric
k g
luc
ote
sta
nd h
and
ove
r to
SH
CP
Do
a fi
nge
r pric
k g
luc
ote
sta
nd h
and
ove
r to
SH
CP
Do
a fi
nge
r pric
k g
luc
ote
sta
nd h
and
ove
r to
SH
CP
Mo
ve to
resu
s ha
nd o
ver t
o
SHC
P a
nd g
ive
so
me
thin
gto
ea
t or d
rink
Urin
e d
ipst
icks
and
Urin
e p
reg
nac
y te
st
IV a
cc
ess
- N
O in
tra
mus
cul
ar
Imm
ed
iate
EC
Ga
nd h
and
ove
r to
SH
CP
Red
uce
d le
vel o
f co
nsc
ious
ness
(no
t ale
rt in
clu
din
g c
onf
use
d)
Che
st p
ain
Hist
ory
of d
iab
ete
s
Urin
e d
ipst
ick
to c
hec
kfo
r ke
tone
s
Una
ble
to s
it up
/ne
ed
to li
e d
ow
n
Hyp
og
lyc
ae
mia
(glu
co
test
3 m
mo
l/L
or l
ess
)
Ab
do
min
al p
ain
or
ba
cka
che
: fe
ma
le
Ac
tive
se
izure
/ fi
ttin
g
Old
er t
han
12 y
ea
rs /
talle
r tha
n 15
0 c
m ta
ll
32
10
12
3
Mo
bili
ty
Wa
lkin
gW
ith H
elp
Stre
tch
er/
Im
mo
bile
RR
less
th
an
9
9
- 14
15
- 20
21 -
29
mo
re
tha
n 2
9
HR
less
th
an
41
41 -
50
51 -
100
101
- 11
011
1 -
129
mo
re
tha
n 1
29
SBP
Less
th
an
71
71
- 8
081
-100
101
-199
mo
re
tha
n 1
99
Tem
p
Co
ld O
R U
nd
er 3
5˚35
˚ -
38.4
˚H
ot
OR
Ove
r 38
.4˚
AV
PUC
on
fuse
dA
lert
Rea
cts
to
V
oic
eRe
ac
ts t
o
Pain
Un
res-
po
nsiv
e
Tra
uma
No
Yes
Dia
be
tes
and
Hyp
erg
lyc
ae
mia
(g
luc
ote
st 1
1 m
mo
l/L
or m
ore
)
Hig
h e
nerg
y tr
ans
fer (
seve
re m
ec
hani
sm o
f inj
ury)
Sho
rtne
ss o
f be
ath
- a
cut
eLe
vel o
f co
nsc
ious
ness
red
uce
d /
co
nfus
ed
Co
ughi
ng b
loo
dC
hest
pa
inSt
ab
be
d n
ec
kH
ae
mo
rrha
ge
- un
co
ntro
lled
(a
rte
rial b
lee
d)
Seizu
re- p
ost
icta
lFo
ca
l ne
uro
log
y - a
cut
e (
stro
ke)
Ag
gre
ssio
nTh
rea
tene
d li
mb
Eye
Inju
ryD
islo
ca
tion
of l
arg
er j
oin
t (no
t fin
ge
r or t
oe
)Fr
ac
ture
- c
om
po
und
(w
ith a
bre
ak
in s
kin)
Burn
ove
r 20%
Burn
- e
lec
tric
al
Burn
- c
ircum
fere
ntia
lBu
rn -
che
mic
al
Poiso
ning
/ O
verd
ose
Dia
be
tic -
glu
co
se o
ver 1
1 &
ke
tonu
riaV
om
iting
fre
sh b
loo
dPr
eg
nanc
y a
nd a
bd
om
ina
l tra
uma
Pre
gna
ncy
and
ab
do
min
al p
ain
Seve
re p
ain
CH
ECK
FOR
AD
DIT
ION
AL
INV
ESTI
GA
TIO
NS

11SATS TRAINING MANUAL 201210 SATS TRAINING MANUAL 2012
Figu
re 5
: Pae
dia
tric
SATS
cha
rt
TheSATSprocessflowchart TheSATSprocessflowchart
YES
NO
NO
NO
LOO
K FO
REM
ERG
ENC
YSI
GN
S A
ND
ASK
FO
RPR
ESEN
TING
CO
MPL
AIN
T
VERY
URG
ENT
TEW
S5
OR
6
EMER
GEN
CY
TEW
S7
OR
MO
RE
TAKE
TORE
SUS
URG
ENT
TEW
S3
OR
4
ROUT
INE
TEW
S0,
1 O
R 2
DECEASEDLO
OK
FOR
URG
ENT
SIG
NS
CA
LCUL
ATE
TEW
S
SEN
IOR
HEA
LTHC
ARE
PRO
FESS
ION
AL’S
DIS
CRE
TION
ADD
ITIO
NA
LIN
VEST
IGA
TION
MEA
SURE
VITA
L SIG
NS
YES
LOO
K FO
RVE
RY U
RGEN
TSI
GN
S
YES
AVP
U: R
espo
nds o
nly
to P
ain
(P) O
R Un
resp
onsiv
e (U
)C
onfu
sion
Paed
iatri
c SA
TS C
hart
EMER
GEN
CY
OLD
ER C
HILD
TEW
S
YOUN
GER
CHI
LD TE
WS
If RR
scor
es 1
poi
ntor
mor
e on
TEW
SC
heck
Sp0
2 -
if be
low
92%
gi
ve 0
2 a
nd m
ove
to re
sus
Do
a fin
ger p
rick
gluc
ose
test
and
hand
ove
r to
Seni
or H
ealth
C
are
Prof
essio
nal (
SHC
P)
Do
a fin
ger p
rick
gluc
ose
test
Hand
ove
r to
SHC
P
Do
a fin
ger p
rick
gluc
ose
test
Do
a fin
ger p
rick
gluc
ose
test
Do
a fin
ger p
rick
gluc
ose
test
If be
low
3 m
mol
/L m
ove
to re
sus
If “H
I” ch
eck
with
SHC
P
Finge
r pric
k ha
emog
lobi
n if
8 or
less
che
ck w
ith S
HCP
Star
t ORT
Redu
ced
leve
l of c
onsc
ious
ness
(not
ale
rt, in
clud
ing
mor
e sle
epy
than
nor
mal
)
Dia
rrhoe
a
Mal
nutri
tion
-vi
sible
seve
re w
astin
g
Mal
nutri
tion
- with
pitt
ing
oede
ma
of B
OTH
feet
Unab
le to
sit o
r mov
e as
nor
mal
fo
r the
chi
ld
Hist
ory
of d
iabe
tes
Hist
ory
of b
leed
ing:
Ble
edin
g PR
, PO
or f
rom
the
site
of tr
aum
a
Vom
iting
onl
y an
d de
hydr
atio
n
VERY
URG
ENT
URG
ENT
Tiny
baby
- yo
unge
r tha
n
2
mon
ths
Inco
lsola
ble
cryi
ng /s
ever
e pa
inPr
esen
ting
com
plai
nt -
mor
e sle
epy
than
nor
mal
Poiso
ning
or o
verd
ose
Foca
l neu
rolo
gy a
cute
Seve
re m
echa
nism
of i
njur
yBu
rns 1
0% o
r mor
e (c
ircum
fere
ntia
l, el
ectri
cal,
chem
ical
)Ey
e in
jury
Frac
ture
- op
en o
r thr
eate
ned
limb
Dislo
catio
n of
larg
er jo
int
(not
fing
er o
r toe
)
Circ
ulat
ion
Con
vulsi
ons
Com
a
Dehy
drat
ion
Oth
er
Som
e re
spira
tory
dist
ress
Som
e De
hydr
atio
n - D
iarrh
oea
or
Diar
rhoe
a an
d vo
miti
ng+1
or m
ore
of th
e fo
llow
ing:
•
sunk
en e
yes
•
restl
ess /
irrit
able
•
thirs
ty /
decr
ease
d ur
ine
outp
ut
• dr
y m
outh
•
cryi
ng w
ithou
t tea
rs
• sk
in p
inch
slow
- le
ss th
an 2
sec
Unab
le to
drin
k / f
eed
OR
vom
its e
very
thin
gM
alnu
tritio
n (v
isibl
e se
vere
was
ting)
Mal
nutri
tion
Oed
ema
(pitt
ing
oede
ma
of B
OTH
feet
)Un
wel
l chi
ld w
ith k
now
n di
abet
esA
ny o
ther
bur
n le
ss th
an 1
0%C
lose
d fra
ctur
eDi
sloca
tion
of fi
nger
or t
oe
Not
bre
athi
ng o
r rep
orte
d ap
noea
Obs
truct
ed b
reat
hing
Cen
tral c
yano
sis o
r SpO
² les
s tha
n 92
%Re
spira
tory
dist
ress
(sev
ere)
Diar
rhoe
a +2
or m
ore
of th
e fo
llow
ing:
• Le
thar
gy /
flopp
y in
fant
• Ve
ry su
nken
eye
s•
Skin
pin
ch v
ery
slow
- 2
sec
or m
ore
Faci
al /
inha
latio
n bu
rnHy
pogl
ycae
mia
reco
rded
at a
ny ti
me
Glu
cose
less
than
3 m
mol
/LPu
rpur
ic ra
sh
Col
d ha
nds +
2 or
mor
e of
the
follo
win
g:•
pulse
wea
k an
d fa
st•
capi
llary
refil
l tim
e 3
sec
or m
ore
• le
thar
gic
Unco
ntro
lled
blee
ding
(not
nos
e bl
eed)
Con
vulsi
ng o
r im
med
iate
ly p
ost-i
ctal
and
not
ale
rt
Airw
ay a
nd
Brea
thin
g
YOUN
GER
THA
N 3
YEA
RS /
SM
ALL
ER TH
AN
95
cm
32
10
12
3
Mob
ility
N
orm
al
for a
ge
Unab
le to
m
ove
as
norm
al
RRle
ss th
an
2020
- 25
26
- 39
40
- 49
50 o
r m
ore
HRle
ss th
an
7070
- 79
80
- 13
0
131
- 159
160
or
mor
e
Tem
p
Feel
s C
old
Unde
r 35˚
35˚ -
38.
4˚Fe
els H
ot
Ove
r 38
.4˚
AV
PUA
lert
Reac
ts to
Vo
ice
Reac
ts to
Pa
inUn
res-
pons
ive
Trau
ma
No
Yes
3 to
12
YEA
RS O
LD /
95
to 1
50 c
m ta
ll
32
10
12
3
Mob
ility
N
orm
al
for a
ge
Unab
le to
w
alk
as
norm
al
RRle
ss th
an
1515
-16
17
- 21
22
- 26
27 o
r m
ore
HRle
ss th
an
6060
- 79
80
- 99
100
- 129
130
or
mor
e
Tem
p
Feel
s C
old
Unde
r 35˚
35˚ -
38.
4˚Fe
els H
ot
Ove
r 38
.4˚
AV
PUC
onfu
sed
Ale
rtRe
acts
to
Voic
eRe
acts
to
Pain
Unre
s-po
nsiv
e
Trau
ma
No
Yes
CHE
CK
FOR
ADD
ITIO
NA
L IN
VEST
IGA
TION
S

13SATS TRAINING MANUAL 201212 SATS TRAINING MANUAL 2012
AdultClinicalSigns
3
It is important to note that if a patient has any emergency signs then a TEWs does nOT need to be calculated to categorise them as RED. There should be no delay in taking the patient to the resuscitation area. Thefirstsetofvitalsmaybeobtainedintheresuscitation area or in the ambulance.
ADULT CLInICAL sIGns
LearningObjectives:
• Befamiliarwiththeadultemergencysigns• Befamiliarwiththeadultveryurgentandurgentsigns
3.1 EMERGEnCY sIGns
EMERGEnCYObstructed airway – not breathing
seizures - current
Burn – facial /inhalationhypoglycaemia – glucose less than 3 mmol/L
Cardiac arrest
Burn - facial inhalationAnypatientinwhomtheairwayhaspotentiallybeenexposedtoheat(e.g.trappedinahousefire,hotwaterburntofacewithpossiblesteaminhalationorchemicalburntofaceormouth)maygetrapidswellingoftheairway.Adultspresentingwiththisemergencysignmayhavesingedfacialhairs(eyelashes,eyebrows),carbonaceousmaterialinandaroundtheirnose/mouthandshouldbetriagedRed.Otheremergencysignsforadultsincludeanobstructedairway(patientnotbreathing),apatientconvulsing,andhypoglycaemiawithaglucoselessthan3mmol/Lorcardiacarrest.
3.2 VERY URGEnT sIGns
Highenergytransfer(severemechanismofinjury)Inourcontextthisreferstohighspeedinjuries.Examplesoftheseincludeamotorvehicleaccidentof40km/hormore,pedestrianvehicleaccident,afallfromarooforahighvelocitygunshotwound.
AdultClinicalSigns
Levelofconsciousnessreduced/confusedAnypatientthatisnotfullyalert(i.e.confused, onlyrespondingtoaverbalstimulus,painfulstimulusorunresponsive).
Threatened limbApatientpresentingwith apainful,pale,pulseless, weak,numblimb.
3.3 URGEnT sIGns
haemorrhage - controlled Thisreferstoasituationwhereapatientpresentswithanactivebleedandyouasthetriageproviderapplydirectpressurewithadrydressingandareabletocontrolthebleed. Thisdoesnotrefertoapatientpresentingwithdryblood.
Abdominal painInallfemalesofchild-bearingageadditionalinvestigations(i.e.urinedipstickandurinepregnancytest)shouldbeperformedtopickupapossibleectopicpregnancy.
Assessment QuestionsClearlyindicatewhetherthefollowingstatements aretrueorfalse:
1. Singedfacialhairsandsootaroundthenoseandmouthareanindicationofinhalationburninapatientthathasbeentrappedinaburninghouse.
True False
2. Haemorrhagecontrolledreferstoapatientwhoseactivebleedwascontrolledbythetriageproviderbyapplyingdirectpressurewithadrydressing.
True False
3. ApatientincardiacarrestisimmediatelycategorisedRed.
True False
Choosethecorrectanswer:4. Examplesofhighenergytransfersinclude: (a) Motorvehicleaccidentat60km/h (b) Fallfromaheightoftenmeters (c) Pedestrianvehicleaccidentat50km/h (d) Highvelocitygunshotwound (e) Alloftheabove
5. Athreatenedlimbmaypresentas: (a) Painintheaffectedlimb (b) Apale,pulselessaffectedlimb (c) Aweakornumbaffectedlimb (d) Theaffectedlimbiscoldandhaspoorperfusion (e) Alloftheabove
A threatened limb presents as:P Pain P Pulselessness P CapillaryRefillDelayP Pallor P Paralysisorpins&needles PTemperature
A Isthepatient Alert?Ifnot,V IsthepatientrespondingtoVoice?Ifnot,P IsthepatientrespondingtoPain?U ThepatientwhoisUnresponsivetovoice
AnDtopainisUnconscious.
URGEnT
haemorrhage - controlledDislocationoffingerORtoe
Fracture–closed(nobreakintheskin)Burn - other
Abdominal painDiabetic–glucoseover17(noketonuria)
Vomiting persistentlyPregnancy & trauma
Pregnancy & PV bleed Moderate pain
VERY URGEnT
high energy transfer (severemechanismofinjury)
Focal neurology – acute (stroke)
Burn – circumferential
shortness of breath - acute Aggression Burn – chemical
Levelofconsciousnessreduced / confused
Threatened limb Poisoning/Overdose
Coughing blood Eye injury Diabetic–glucoseover 11 and ketonuria
Chest pain Dislocation of larger joint (notfingerortoe)
Vomiting fresh blood
stabbed neck Fracture - compound (withabreakinskin)
Pregnancy and abdominal trauma
haemorrhage – uncontrolled (arterialbleed)
Burnover20% Pregnancy and abdominal pain
seizure – post ictal Burn – electrical SeverePain

15SATS TRAINING MANUAL 201214 SATS TRAINING MANUAL 2012
PaediatricClinicalSigns
PAEDIATRIC CLInICAL sIGns
LearningObjectives:
• Befamiliarwiththepaediatricemergencysigns• UnderstandtheABC-c-c-DOapproachforemergencysigns• Befamiliarwiththepaediatricveryurgentandurgentsigns
4.1 EMERGEnCY sIGns: The ABC-c-c-DO approachTriageofpatientsinvolveslookingforsignsofseriousillnessorinjury.TheseemergencysignsrelatetotheAirway-Breathing-Circulation/Coma/Convulsion-Dehydration-Otherandareeasilyrememberedas“ABC-c-c-DO”.Eachletterreferstoanemergencysignwhich,whenidentified,shouldalertyoutoapatientwhoisseriouslyillandneedsimmediateintervention.ItisimportanttonotethatifapatienthasanyemergencysignsthenaTEWSdoesNOTneedtobecalculated.Thereshouldbenodelayintakingthepatienttotheresuscitationarea.Thefirstsetofvitalsmaybetakenintheresuscitationareaorintheambulanceonthewaytothehospital.
EMERGEnCY
Airway and Breathing not breathing or reported apnoeaObstructed breathingCentral cyanosis or spO2lessthan92%Respiratorydistress(severe)
Circulation Cold hands + 2 or more of the following:(i)pulseweakandfast(ii)capillaryrefilltime3secormore(iii)lethargicUncontrolledbleeding(notnosebleed)
Coma AVPU:RespondsonlytoPain(P)ORUnresponsive(U)Confusion
Convulsions Convulsingorimmediatelypost-ictalandnotalert
Dehydration Diarrhoeaorvomiting+2ormoreofthefollowing:(i)Lethargy/floppyinfant(ii)Verysunkeneyes(iii)Skinpinchveryslow-2secormore
Other Facial /inhalation burnhypoglycaemia recorded at any time - glucose less than 3 mmol/LPurpuric rash
HOWTOTriage?KeepinmindtheABC-c-c-DOsteps: Airway,Breathing,Circulation,Coma,Convulsion,DehydrationandOther.
4.1.1 AB AIRWAY AnD BREAThInG ARE UsUALLY AssEssED TOGEThERThe letters AandBin “ABC-c-c-DO”represent“airway and breathing”. Itisevidentthatanopen(patent)airwayisneededforbreathing.Anairway orbreathingproblemislife-threateningandmustreceiveyourattentionbeforeyoumoveontoothersystems.Itisthereforeconvenientthatthefirsttwolettersofthealphabetrepresentthetwomostimportantareastolookforemergencyorprioritysigns.Ifthereisnoproblemwiththeairwayorbreathing,youshouldlookforsignsintheareasrepresentedbyC.
4
Toassessifthechildhasairwayorbreathingproblemsyouneedtoknow:• Isthechildbreathing?• Istheairwayobstructed?• Isthechildblue(centrallycyanosed)?
ISTHECHILDBREATHING? Ifactive,talking,orcrying,thechildisobviouslybreathing.IfinanydoubtyoumustAssEssthreethingstocheckifthechildisbreathing(seeFigure6):
• LOOK-toseeifthechestismoving.• LIsTEn-foranybreathingsounds.
Aretheynormal?• FEEL-Canyoufeelthebreathatthenoseor
mouthofthechild?Ifthechildisnotbreathing(oryouarenotsureifthereisbreathing),youneedtotakethechildtotheresuscitationareawherethebreathingneedstobeartificiallysupportedbyventilatingthechildwithabagvalvemask(BVM)devicewhilstthechildisfurtherassessedandmanagedappropriately.
ISTHEBREATHINGOBSTRUCTED?Noisybreathingcanbeasignthattheairwaymaybethreatenedorpartiallyobstructed.Thisismostcommoninpatientswithadecreasedlevelofconsciousness,upperrespiratorytractinfectionsoraspirationofforeignbodies.Obstructedbreathingcanalsobeduetoblockagebythetongueorthepatient’sownsecretionsifthesearenotbeingswallowed.
ARETHEREABNORMALRESPIRATORYNOISES?Arethereanynoisesheardwhenbreathingin?Aharshnoiseonbreathinginiscalledstridor,ashortnoisewhenbreathingoutinyounginfantsiscalledgrunting.Bothnoisesaresignsofsevererespiratoryproblems.
NB:Ablockednoseisanextremelycommoncauseofnoisybreathing,butitisNOTlife-threatening.
DOESTHECHILDSHOWCENTRALCYANOSIS? DEFInITIOn: Cyanosisoccurswhenthereisanabnormallylowlevelofoxygenintheblood. Thisproducesabluishorpurplishdiscolorationofthetongue,theinsideofthemouthandtheskin.Thissignmaybeabsentinachildwhohassevereanaemia.To AssEssforcentralcyanosis:LOOK-atthemouthandtongue.Abluishorpurplishdiscolorationofthetongueandtheinsideofthemouthindicatescentralcyanosis.MEAsURE-Ifoxygensaturationmonitoringisavailableyoucancheckthechild’soxygenlevels. Firstensurethattheprobeiscorrectlysitedandthatagoodregulartraceisshowingonthemonitor.Ifoxygensaturationis<92%inroomairthechildhaslowoxygenlevelsandthisisanemergency.
DOESTHECHILDHAVESEVERERESPIRATORYDISTRESS?To AssEsswhetherthechildhassevererespiratorydistresscheckforthefollowingsigns:
• Isthechildhavingtroublegettingbreathsothatitisdifficulttotalk,eatorbreastfeed?
• Isthechildbreathingveryfast?• Doesthechildhaveseverechestindrawing?Thiscan
beintercostal(betweentheribs),subcostal(belowtheribcage),suprasternal(abovethesternum)orsternalindrawing(thebreastboneissuckedinoninspiration).
• Doesthechildhavenasalflaringoragruntingnoiseonexpiration?• Isthechildusingtheaccessorymusclesoftheneckforbreathing?Thiscancausetheheadto
nodorbobwitheverybreath.Thisisparticularlyseeninyoungbabies.• Exhaustion:Ifthechild’sbreathingisverylaboured,especiallyifithasbeenlikethisforsome
time,thens/hemaybecomeexhausted?Ifthishappensthenthesignsofincreasedworkofbreathingcanactuallydecreaseasthechildistotired-thisisaverydangeroussign.
Ifyouseethesesignsthenitislikelythatthechildhassevererespiratorydistress.
PaediatricClinicalSigns
Figure 6: Look, listen and feel
Signsofsevererespiratorydistress:• Veryfastbreathing• Severelowerchestwallindrawing• Useofauxiliarymuscles• Headnodding• Inabilitytofeedbecauseof
respiratoryproblems• Gruntingandflaring

17SATS TRAINING MANUAL 201216 SATS TRAINING MANUAL 2012
MEAsURE:Inanychildwithrespiratorydistress,youshouldcheckoxygensaturationlevelsifyouhaveanoxygensaturationmonitor.Firstensurethattheprobeiswellsitedandthatyouhaveagoodtraceonthemonitor–iftheoxygensaturationislessthan92%inroomair,thischildhasanemergencysignandneedsoxygentherapy.Howeverifachildisobviouslyinsevererespiratorydistress,oxygensaturationlevelsdonotneedtobecheckedattriagetoconfirmthisemergencysign,rathertakethechild to the resuscitation area immediately.Ifthechildisbreathingadequately,gotothenextsectiontoquicklycontinuetheassessmentforemergencysigns.Ifthechildhasanairwayorbreathingproblem,youshouldinitiateappropriatetreatmentandthenquicklyresumetheassessment.
4.1.2 C CIRCULATIOn AssEssMEnTFIRsT FEEL ThE ChILDs hAnDs – IF ThEY ARE WARM YOU DO nOT nEED TO ChECK ThE CIRCULATIOn AnY FURThER. MOVE On TO ThE nEXT EMERGEnCY sIGn.IF ThE hAnDs ARE COLD OR COOL – YOU nEED TO RAPIDLY AssEss FOR OThER sIGns OF CIRCULATORY shOCK: PULsE VOLUME AnD RATE; CAPILLARY REFILL TIME AnD LEThARGY.
ISTHEPULSEWEAKANDFAST?Theradialpulse(thepulseatthewrist)shouldbefelt.Ifthisisstrongandnotobviouslyfast,thepulseisadequate;nofurtherassessmentisneeded.Theradialpulseisusedasaninitialscreenbecauseitiseasytoaccesswithoutundressingthepatient.Iftheradialpulseisdifficulttofind,youneedtolookforamorecentralpulse(apulsenearertotheheart).Inaninfant(lessthanoneyearofage)thebestplacetolookisatthemiddleoftheupperarm,thebrachialpulse.Ifthechildislyingdownyoucouldlookforthefemoralpulseinthegroin.Thepulseshouldbestrong.Ifthemorecentralpulsefeelsweak,decideifitalsoseemsfast.Thisisasubjectivejudgementandanexactcountisnottaken.Ifthecentralpulseisweakandfast,thechildneedsfurtherassessmentandpossibletreatmentforshock.Alltheseprocedurescanandshouldbepractisedonyourself,yourfriends,yourchildrenandfamily,andfinallyonrealpatients.Practiceisthebestwaytoimproveonfindingpulsesandmeasuringcapillaryrefill.
Notethatwedonotrecommendbloodpressuretoassessforshockattriagebecauseoftworeasons: 1)Lowbloodpressureisalatesignofshockinchildrenandtheywillalreadyhaveotherobvioussignsand2)thebloodpressureinchildrenislesspredictiveattriagethaninadults.
4.1.3 C-C COMA AnD COnVULsIOns AssEssMEnT
ISTHECHILDINACOMA? Achildwhoisawakeisobviouslyconsciousandyoucanmovetothenextcomponentoftheassessment.Ifthechildisasleep,askthemotherifthechildisjustsleeping.Ifthereisanydoubt,youneedtoassessthelevelofconsciousness.Trytowakethechildbytalkingtohim/her,e.g.callhis/hernameloudly.Achildwhodoesnotrespondtothisshouldbegentlyshaken.Alittleshaketothearmorlegshouldbeenoughtowakeasleepingchild.Ifthisisunsuccessful,applyafirmsqueezetothenail
bed,enoughtocausesomepain.Achildwhodoesnotwaketovoiceorbeingshakenortopainisunconscious.Tohelpyouassesstheconsciousnesslevelofachild,asimplescale(AVPU)isused:Achildwhoisnotalert,butrespondstovoice,islethargic.Anunconsciouschildmayormaynotrespondtopain.Any child with a coma scale of “P” or “U” is an emergency and needs to be taken to the resuscitation area immediately.
PaediatricClinicalSigns
Toassessforcomaandconvulsionsyouneedtoknow:(i) Isthechild’slevelofconsciousness
disturbed?(ii) Isthechildconvulsingnow?
A IsthechildAlert?Ifnot,V IsthechildrespondingtoVoice?
Ifnot,P IsthechildrespondingtoPain?U ThechildwhoisUnresponsive
tovoice(orbeingshaken) ANDtopainisUnconscious.
Toassessifthechildhascirculationproblemsyou needtoknow:•Doesthechildhavecoolorcoldhands?IF YEs -Isthecapillaryrefilltime(CRT)3secondsormore? -IftheCRTisprolongedisthepulseweakandfast? -Isthechildlethargic
ISTHECHILDCONVULSINGNOWORPOST-ICTAL? Thisassessmentdependsonyourobservationofthechildandonthehistoryfromtheparent.Childrenwhohaveahistoryofconvulsion,butarealertduringtriage,willneedacompleteclinicalhistoryandinvestigationbyaclinician,butattriagetheyarenotassignedanemergencyclinicalsign,astheydonotusuallyrequireanyresuscitationimmediately.Thechildmaybeseentohaveaconvulsionduringthetriageprocessorwhilewaitingintheoutpatientdepartment.Youcanrecognizeaconvulsionbythesuddenlossofconsciousnessassociatedwithuncontrolledjerkymovementsofthelimbsand/ortheface.Thereisstiffeningofthechild’sarmsandlegsanduncontrolledmovementsofthelimbs.Thechildmaylosecontrolofthebladder,andisunconsciousduringtheconvulsionanddrowsyafterwards.Sometimes,insmallinfants,thejerkylimbmovementsmaybeabsent,buttheremaybemoresubtletwitchingmovementsoftheface,mouth,eyes,handsorfeet.Youhavetoobservetheinfantcarefully.
4.1.4 D sEVERE DEhYDRATIOn AssEssMEnTInthissectionwewilllookattheassessmentofseveredehydrationinthechildwithdiarrhoeaorvomiting.Ifthechildisseverelymalnourishedthesignsofdehydrationarenotasreliable.
DOESTHECHILDHAVEDIARRHOEAORVOMITING? Thisinformationcomesfromtheparentorguardian. Ifthechildhasnodiarrhoeaorvomiting,donotcheckfordehydration.Movetothenextassessment.Ifthechildhasdiarrhoeaorvomitingassessforseveredehydration.Ahistoryofdiarrhoeaorvomitingandthepresenceoftwoormoreofthesignsintheboxabovemeansthechildhasseveredehydrationandneedstobetakentotheresuscitationareaimmediately.
ISTHECHILDLETHARGIC?Intheolderchildlethargyisquiteeasytoassess.YouhavealreadyassessedthestateofconsciousnessofthechildusingtheAVPUscale.Nowobserveifthechildappearsdrowsyanddoesnotshowinterestinwhatishappeningaroundhim/her.Alethargicchildmaynotlookatthemotherorwatchyourfacewhenyoutalk.Thechildmaystareblanklyandappearnottonoticewhatisgoingonaroundhim/her.Doesthechildknowhis/hernameandanswerquestionssensibly?Ifthechildrespondstovoicebutremainsdrowsy,he/sheislethargic.Intheyoungerchild,signsoflethargyarehardertoassess.
DOEs ThE ChILD hAVE VERYSUNKENEYES?Lookatthechild’seyestodetermineiftheyappearunusuallysunkenintheirsockets(seeFigure8).Askthemotherifthechild’seyesaremoresunkenthanusual.
DOESASKINPINCHGOBACKVERYSLOWLY(2SECONDSORMORE)?Thisisasimpletesttolookathowelastictheskinis.Ifthechildisnotdehydrated,theskinwillbeelasticand,whenpinchedandreleased,willreturntonormalstraightaway.Trythisonyourself. Thedehydratedchildwillhavelostfluid.Thebodymovesfluidfromlessimportantplaces,suchastheskin,tomaintainthecirculation.Theskinbecomeslesselasticand,whenpinched,isslowtoreturn.Locatetheareaonthechild’sabdomenhalfwaybetween
PaediatricClinicalSigns
Toassessifthechildisseverelydehydratedyouneedtoknow:• Isthechildlethargic?• Doesthechildhavevery
sunkeneyes?• Doesaskinpinchtake2seconds
ormoretogoback?
Figure 8: Sunken eyes
Figure 9: Skin pinch
Figure 7:Feeling the brachial pulse in an infant

19SATS TRAINING MANUAL 201218 SATS TRAINING MANUAL 2012
PaediatricClinicalSigns
theumbilicusandthesideoftheabdomen.Avoidingusingyourfingertips,asthisispainful.Pinchtheskininavertical(headtofoot)directionandnotacrossthechild’sbody.Youshouldpickupallthelayersoftheskinandthefattissueunderneath.Pinchforonesecondandthenrelease.Seewhethertheskingoesbackveryslowly(2secondsormore).Severedehydrationispresentifthechildhasahistoryofdiarrhoeaplusanytwoofthefollowingsigns:lethargy,sunkeneyesorveryslowskinpinch(2secondsormore).
4.1.5 O OThER EMERGEnCY sIGns
Facial inhalational burnsAnychildinwhomtheairwayhaspotentiallybeenexposedtoheat(e.g.trappedinahousefire,hotwaterburntofacewithpossiblesteaminhalationorchemicalburntofaceormouth)maygetrapidswellingoftheairway.ChildrenpresentingwiththisemergencysignshouldbetriagedRed.
Glucose <3mmol/L at any timeChildrenwithalowbloodsugarareoftenverysickandneedtobeseenimmediately.TheyshouldbetriagedRediffoundtohaveabloodglucoseconcentrationoflessthan3mmol/L.
Purpuric RashChildrenwhopresentwithacomplaintofarash-shouldbeassessedtoseeifthespotsblanchwithpressurefromfingertiporglasstest(i.e.turnswhitewhenpressureisapplied).Ifthespotsarenon-blanching(i.e.doesnotturnwhitewhenpressureisapplied)-thenthereisariskofmeningococcaldisease.ChildrenpresentingwiththisemergencysignshouldbetriagedRed.Ifyouareunsureaboutachildpresentingwitharashasktheseniorhealthcareprofessional.Youhavenowlearnedhowtorecognizetheobviousemergencysignsinpaediatricpatients.Thenextsectionwillcovertheveryurgentandurgentsignsrespectively.ItisimportanttonotethatifapatienthasanyemergencysignsthenaTEWSdoesNOTneedtobecalculated.Thereshouldbenodelayintakingthepatienttotheresuscitationarea.Thefirstsetofvitalsmaybetakenintheresuscitationareaorintheambulanceonthewaytothehospital.
• IfanyEMERGENCYsignshavebeenfoundtheTEWSshouldNOTbecalculatedattriage,thechild is within the RED category and should be taken to the resuscitation area.
• ChildrenwithintheRED category need emergency care and should be seen immediately.• AlwaysensurethatthechildwithemergencysignsishandedoverdirectlytoaSHCP.
• If there are no EMERGEnCY signs, check to see whether the child has any VERY URGEnT signs.
4.2 VERY URGEnT sIGnsIfthechilddoesnothaveanyoftheemergency ABC-c-c-DOsigns,thetriageproviderproceedstoassessthechildontheveryurgentsigns.Thisshouldnottakemorethanafewseconds.SomeofthesesignswillhavebeennoticedduringtheABCDtriagediscussedsofar,andothersneedtobere-checked.Followthelistofveryurgentsignstoquicklycompletethissectiontodecidewhetherthechildhasanyveryurgentorurgentsignsthatneedpromptmanagement.
Thefrequencywithwhichchildrenshowingtheseveryurgentsignsappearinyouremergencycentredependsonthelocalepidemiology.
Performafingerprickglucotestinthefollowingcases:• Reducedlevelofconsciousness• Unabletositormoveasusual• Currentorrecentseizure• Knownwithdiabetes• Severemalnutrition
Thepresenceofobviousveryurgentsignsdoesnotautomatically make the child’s triage priority ORAnGE. Always calculate the TEWs and check key additional investigationstoensurethatthechilddoesnotneedtobeassigned to the RED category and taken for emergency care
VERY URGEnTTiny baby - younger than
2 monthsInconsolable crying /
severepainPresenting complaint -
More sleepy than normalPoisoningoroverdoseFocal neurology acute
SeveremechanismofinjuryBurns (circumferential, electrical, chemical,
10%ormore)Eye Injury
Fracture – open or threatened limb
Dislocation of larger joint (notfingerortoe)
Tinybaby(lessthantwomonthsofage) Ifthechildappearsveryyoung,askthemotherhisage.Ifthechildisobviouslynotayoungbaby,youdonotneedtoaskthisquestion.Smallbabiesaremoredifficulttoassessproperly,morepronetogettinginfections(fromotherpatients),andmorelikelytodeterioratequicklyifunwell.Alltinybabiesofundertwomonthsofageshouldthereforebeseenveryurgently.
Inconsolablycrying/severepainTheinconsolablecryingchildisconsciousbutcriesconstantlyandwillnotsettle.Asktheparentofcaregiverifthechildisupset/frightenedbytheunfamiliarenvironmentorwhetherthisisthepresentingcomplaint.Ifachildhasseverepainandisinagony,s/heshouldbeprioritizedtoreceiveveryurgentassessmentandpainrelief.Severepainmaybeduetosevereconditionssuchasacuteabdomen,meningitis,etc.Youarenotrequiredtodoaformalpainscaleassessment,butforyourinformationtherearesomeexamplesofpainscalesappendedattheendofpartfour.
Presenting complaint - ‘more sleepy than normal’ When the mothercomplainsthatherchildthatismoresleepythannormal(NOTjustinnaturalsleep),thechildmaybeintheearlystagesofseriousconditionssuchasmeningitis,hypoglycaemia,septicaemiaetc,andwillneedtobeidentifiedandmanagedveryurgently.EvenifthechildappearsalertattriagestillassignaVeryUrgentclinicalsignaswehavetotakeseriouslythemothersconcern.
PoisoningorOverdoseAchildwithahistoryofswallowingdrugsorotherdangeroussubstancesneedstobeassessedveryurgently,ass/hecandeterioraterapidlyandmightneedspecifictreatmentdependingonthesubstancetaken.Themotherwilltellyouifshehasbroughtthechildbecauseofpossibleintoxication.ConsultSHCPforadviceregardingveryurgentmanagement.
Focal neurology acuteAchildwhoisfullyconsciousbuthasnewfocalneurologicalsignswillneedveryurgentassessment.Inthiscase,thechilddoesnotrequireemergencytreatmentbecausetheydonothaveanyABCDemergencysigns,butmayneedurgentimagingandintervention.Examplesoffocalneurologicalsignsincludecranialnervepalsiesandacutelyparalysedlimbs-theirpresencemayindicateaformofvascularstrokeandmanagementmaybetimedependent.Thechildmayhaveaweaknessononesideofthebodyandmaynotbeabletomoveasnormal.Theparentmayalsocomplainthattheirchildhasanewonsetofasquintoraparalysedface.
SevereTrauma–severemechanismofinjuryUsuallythisisanobviouscase,butoneneedstothinkofmotorvehicleaccidentinjuries,fallsfromaheightgreaterthanonemetreinheight,gunshotwoundsandothertraumaticmechanismsofinjuryinthiscategory.Rememberthe ABC-c-c-DOassessmentwouldalreadyhaveidentifiedanylife-threateningproblemsrequiringimmediateresuscitation.
Burns Theseinclude:Circumferential,Electrical,Chemicalandanyburninvolving10%ormore of body surface area.Burnsareextremelypainfulandchildrenwhoseemquitewellcandeterioraterapidly.
PaediatricClinicalSigns
WARnInGAny major burn take to resuscitation area
ADDITIOnAL TAsKPain check with shCP for analgesia initiation
ADDITIOnAL TAsKPoisoning/Overdose Refer to shCP
ADDITIOnAL TAsKBleeding apply pressure to the site of trauma and coveropenwounds
Pain check with shCP for analgesia initiation
ADDITIOnAL TAsKPain check with shCP for analgesia initiation
ADDITIOnAL TAsKTiny baby Refer to shCP
!ADDITIOnAL InVEsTIGATIOnReducedlevelofconsciousness dofingerprickglucosetest
WARnInGIf glucose less than 3 mmol/L take to resuscitation area

21SATS TRAINING MANUAL 201220 SATS TRAINING MANUAL 2012
ThesizeoftheburnneedstobedeterminedusingtheRuleofNinesmethod(thepalmarmethodismoresuitableforsmallerburns-seepage23).Foranychildwithamajorburnresuscitationmustbecommenced.Followtheprovincialburnsmanagementguidelines2011includinganalgesia.
Theexampleleftisofaoneyear-oldchild.RefertoTableintheprovincialEmergencyManagementofSevereBurnsmanualfordifferentages.
Fracture – open Anopenfracturemaybeassociatedwithalargevolumeofbloodlossthatmaybeveryobvious(external)ormaybeconcealed(internal)–perhapsonlyrecognisablebyswellingaroundthefracturearea.Thisneedsveryurgentattention.
Threatened limb
Dislocationoflargejoint(notfingerortoe)Apartfrombeingverypainful,alargejointdislocationmaycompromisebloodandnervesupplytothelimbdistaltotheaffectedjoint.Damagetotheneurovascularbundleimpliesseriousinjuryandneedsveryurgentattention.
• If any VERY URGEnTsignshavebeenfoundtheTEWSshouldbecalculatedandkeyadditionalinvestigationsshouldbecheckedtoensurethatthechilddoesnotneedtobeassigned to the RED category and taken for emergency care.
• Children within the ORAnGE category should be seen within 10 minutes.• HandoverallORAnGE category children personally to the health worker in the Orange area,• Always check for additional tasks that should be done.
• If there are no VERY URGEnT signs, check to see whether the child has any URGEnT signs.
PaediatricClinicalSigns
ADDITIOnAL TAsKIftheburnoccurredrecently(within3hrs) it is still worthwhile to cool the burnt area with water, for example, by running cool tap water
overtheburntareafor30minutes.Thechildshouldthenbedriedandwrappedinacleansheetorblankettoavoidhypothermia.Theburncanbecoveredinclingwrapifavailable,oracleandrysheetortowelwillalsobesuitable.
A threatened limb presents as:P PainP PallorP PulselessnessP Paralysisorpins&needlesP CapillaryRefillDelayP Temperature
Figure 10: Rule of Nines for burn surface area estimation in a one year old child
ADDITIOnAL TAsKPain check with shCP for analgesia initiation
ADDITIOnAL TAsKPain check with shCP for analgesia initiation
ADDITIOnAL TAsKDislocation of large joint HandovertoSHCP.
Pain check with shCP for analgesia initiation
APPEnDIX B: Examples of different pain scales Behavioral Observation Pain Rating Scale
Categories scoring0 1 2
Face Noparticularexpressionorsmile;disinterested
Occasionalgrimaceorfrown,withdrawn
Frequenttoconstantfrown,clenchedjaw,quiveringchin
Legs Nopositionorrelaxed Uneasy,restless,tense Kicking,orlegsdrawnup
Activity Lyingquietly,normalposition,moveseasily
Squirming,shiftingbackandforth,tense
Arched,rigidorjerking
Cry Nocrying (awakeorasleep)
Moansorwhimpers, occasionalcomplaint
Cryingsteadily,screamsorsobs,frequentcomplaints
Consolability Content,relaxed Reassuredbyoccasionaltouching,hugging,ortalkingto.Distractable
Difficulttoconsoleorcomfort
Eachofthefivecategories:(F)Face;(L)Legs;(A)Activity;(C)Cry;(C)Consolability isscoredfrom0-2,whichresultsinatotalscorebetween0and10.
Observethechildandscorethechild’spainaccordingtothe‘FLACC’scale.
‘Faces’ Pain Rating Scale
4.3 URGEnT sIGns ThesechildrendonothaveanyoftheemergencyABC-c-c-DOsignsnordotheyhaveanyoftheveryurgentsigns.Thetriageprovidershouldproceedtoassessthechildontheurgentsigns.Thisshouldnottakemorethanafewseconds.
some respiratory distressWhenyouassessedtheairwayandbreathing,didyouobserveanyrespiratorydistress?Ifthechildhassevererespiratorydistress,thisisanemergency.Theremayhowever,besignspresentthatyoudonotthinkaresevere,e.g.somelowerchestwallindrawing(butnotsevere),orslightincrease
PaediatricClinicalSigns
!ADDITIOnAL InVEsTIGATIOnRR scoring 1 point or more measure oxygen saturation
0nO hURT
1hURTs
LITTLE BIT
2hURTs
LITTLE MORE
3hURTs
EVEn MORE
4hURTs
WhOLE LOT
5hURTsWORsT
Asktheolderchildtopointtothefacethatbestdescribeshows/hefeels.
Evenifthereareobviousurgentsigns–calculate the TEWs and carry out additional investigationstoensurethatthepatientisnotpossibly within the RED or ORAnGE category.
WORsT POssIBLE PAIn
nO PAIn
10-
9-
8-
7-
6-
5-
4-
3-
2-
1-
0-
URGEnT
some respiratory distress
some Dehydration - Diarrhoea or diarrhoeaandvomiting+1ormore
of the following: (i)sunkeneyes(ii) restless/irritable(iii) thirsty/decreasedurineoutput(iv)drymouth(v)cryingwithouttears(vi)skinpinchslow-lessthan2sec
some Dehydration - Unable to drink/feed ORvomitseverything+1ormoreofsigns
(i)–(vi)above
Malnutrition(visibleseverewasting)
Malnutrition Oedema (pitting oedema ofBOTHfeet)
Unwell child with known diabetes
Anyotherburnlessthan10%
Closed fracture
Dislocationoffingerortoe
23SATS TRAINING MANUAL 201222 SATS TRAINING MANUAL 2012
inbreathingrate.Inthiscase,thechilddoesnotrequireemergencytreatmentbutwillneedurgentassessment.Understandingthelevelofseverityofrespiratorydistresscomewithpracticeandexperience.Ifyouhaveanydoubts,consultaseniorhealthcareprofessionalimmediately.
SomeDehydration-Diarrhoeaordiarrhoeaandvomiting+1ormoresignsofdehydrationInfantsandchildrenwithdiarrhoeaorvomitingmayhavelostenoughfluidtoshowoneormoreofthefollowingsignsofdehydration:
Becausethesechildrenhavelossesthatareongoinganddifficulttoquantify,theyneedtocommenceoralrehydrationtherapyassoonaspossibletoavoidbecomingseverelydehydratedorshockedi.e.signsthatwouldnowplacethemintotheREDcategory.MostofthemarethirstyandtheirmothersneedtoofferthemextrafluidsaccordingtotheOralRehydrationCornerguidelines.Infantsandyoungchildrenthatarebreast-fedshouldbeencouragedtocontinuetodosowhilstawaitingfurtherurgentassessment.
Unabletodrink/feedORvomitseverythingInfantsandchildrenthatarenotwellenoughtofeedorarevomitingeverythingmayhaveseriousmedicalorsurgicalconditionsaffectinganyofthebodysystems.Examplesincludesepticaemia,
meningitis,heartconditions,acutesurgicalabdomen,pneumoniaetc.
Malnutrition withvisibleseverewastingSeverewastingisaformofseveremalnutrition.Thesechildrenareeasytopickupbecausetheirmusclesareverywastedandtheyhavelooseskinfoldsparticularlynoticeablearoundtheirupperthighs,buttocksandupperarms.Ifyouareconcernedthatachildmightbemalnourishedlookrapidlyatthesebodyareas.Severelymalnourishedchildrenarepronetohypothermia,hypoglycaemiaandinfectionsandneedtobemanagedurgentlyaccordingtotheWHOseveremalnutritionguidelinestopreventcomplications.
Malnutrition with pitting oedema of both feetThisisanotherformofseveremalnutrition.Itisasdangerousastheonedescribedaboveandisrecognisedbythepittingoedemaofbothfeet;theymayalsopresentwithgeneralbodyswelling.Ifyouareconcernedthatachildmightbemalnourishedlookrapidlyatthechild’sfeetandcheckforoedemaofbothfeet.Thesechildrenoftenappearlistlessandapatheticandhaveskinandhairchanges.Theyarealsopronetohypothermia,hypoglycaemiaandinfectionsandneedtobemanagedurgentlyaccordingtotheWHOseveremalnutritionguidelinestopreventcomplications.
PaediatricClinicalSigns
WARnInGIf oxygen saturation below 92% giveoxygenandmovetoresuscitationarea
(i) sunkeneyes-askthemother(ii) restless/irritable(iii) thirsty/decreasedurineoutput
(iv) drymouth(v) cryingwithouttears(vi) skinpinchslow-lessthan2seconds
Vomitingonlyanddehydration:• bewarethechildmayhaveanacutesurgical
bowelproblem• oralfluidsmaybecontraindicated• seekadvicefromaseniorhealthprofessional
!ADDITIOnAL InVEsTIGATIOnMalnutritionwithvisibleseverewasting doafingerprickglucosetest and check with shCP
ADDITIOnAL TAsKVomiting only and dehydration consult with shCP
!ADDITIOnAL InVEsTIGATIOnMalnutritionwithvisibleseverewasting doafingerprickglucosetest and check with shCP
ADDITIOnAL TAsKDiarrhoe start oral rehydrationtherapy(ORT)
WARnInG If glucose is below 3 mmol/L move
to resuscitation
Unwell child with known diabetesChildrenwithdiabetesoftenlosecontroloftheirsugarlevelswhentheyareunwellfromacuteillnessandinfectionse.g.acuterespiratoryinfections, (upperorlower)urinarytractinfectionsordiarrhoea. Theyoftendevelophighorlowbloodglucoselevelsbecausetheirinsulinneedsmayincreaseordecreasewhilsttheyareunwellandtheyarenoteatingasusualbecauseoflossofappetite,nauseaorvomiting.
Burnlessthan10%ofbodysurfaceareaThesizeoftheburnneedstobedeterminedusingthepalmarmethod(patient’soutstretchedopenpalmincludingthefingersis≈to1%ofthebodysurfacearea).
Closedfracture(nobreakintheskin)Thesechildrenoftenpresentwithpainonmovingorrefusaltomovetheaffectedlimb.Theremaybedeformityofthelimbevident.
DislocationoffingerortoeThisoftencausesanobviousdeformity;thedislocateddigitwillneedtobereducedundersomeformofanaesthesia.
PaediatricClinicalSigns
WARnInG If glucose is below 3 mmol/L moveto resuscitation
WARnInGIf glucose result is ‘hI’ check with shCP
Figure 11: Palmor method illustrating 1% of the body
ADDITIOnAL TAsKBurnlessthan10% followtheprovincialburns management guidelines. If the burn occurred recently, within the last 3 hours, it is still worthwhile to cool the burnt area with
water, for example, with cool tap water for at least 30minutes.Theburnshouldthenbedriedandcoveredwith cling wrap or a clean dry sheet. The child should also be wrapped in a blanket and kept warm
ADDITIOnAL TAsKPain check with shCP for analgesia initiation
ADDITIOnAL TAsKPain check with shCP for analgesia initiation
ADDITIOnAL TAsKClosed fracture If required get a wheelchair or stretcher and immobilise the affected limb with a simple splint e.g. a padded wire splint or triangular bandage that does not interfere with thebloodsupplyornervebundle,andprovideanalgesiaaccordingyoursite’sguidelines.
!ADDITIOnAL InVEsTIGATIOnhistory of diabetes do a fingerprickglucosetest
ADDITIOnAL TAsKPain check with shCP for analgesia initiation
WARnInG If glucose is less than 3 mmol/L move
to resuscitation
25SATS TRAINING MANUAL 201224 SATS TRAINING MANUAL 2012
Assessment QuestionsClearlyindicatewhetherthefollowingstatementsaretrueorfalse:
1. Gruntingandnasalflaringaresignsofsevererespiratorydistress.
True False
2. Oxygensaturationlevelsshouldalwaysbecheckedinachildthatlooksblue.
True False
3. Ifnoemergencysignisidentifiedinstepone,butanurgentsignisidentifiedinsteptwo,thepatientisimmediatelytakentothemajorsareaforurgentmanagement.
True False
Choosethecorrectanswer:4. IntheABC-c-c-DOapproachABCstandsforairway,breathing,circulation.
Whatdoesc-c-Dstandfor? (a) convulsions,chestpain,dehydration (b) coma,cancer,disabilities (c) coma,convulsions,dehydration (d) coma,craniopharyngioma,dehydration (e) chronicpain,constipation,dehydration
5. Thefollowingareemergencysigns (a) oxygensaturationlevelsmorethan92% (b) facialorinhalationburn (c) stridor,snoringandsecretions (d) closedfracture (e) bandcabove
PaediatricClinicalSigns
• IfanyURGENTsignshavebeenfoundtheTEWSshouldbecalculatedandadditionalinvestigationscheckedtoensurethatthechilddoesnotneedtobeassignedtothe RED or ORAnGEcategoryandtakenforemergencyorveryurgentcare.
• ChildrenwithintheYellowcategoryshouldbeseenwithin60minutes.• Always check for additional tasks that should be done.• IftherearenoURGENTsigns,calculatetheTEWSandcheckforadditionalinvestigationsto
determinewhatthechild’sfinaltriagecolouris.
TRIAGE EARLY WARnInG sCORE TEWs
LearningObjectives:
• BefamiliarwiththedifferentageappropriateversionsoftheTEWS• UnderstandhowtocalculatetheTEWSinpaediatricandadultpatients
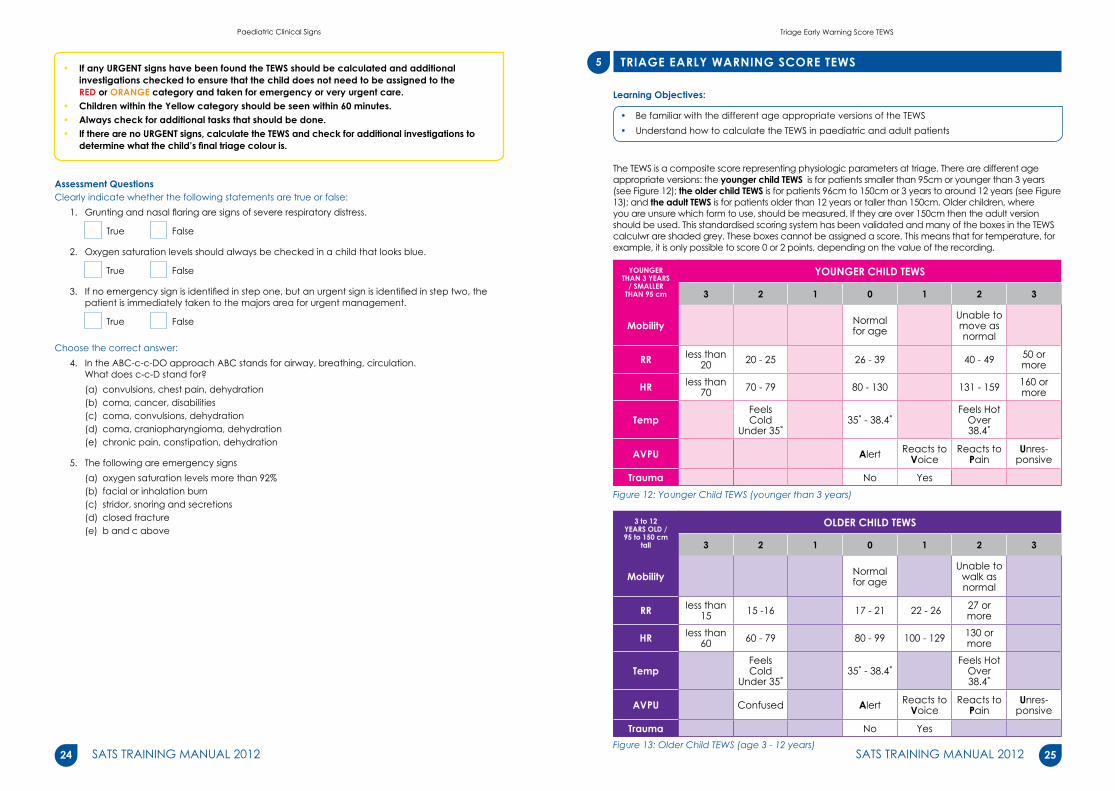
TheTEWSisacompositescorerepresentingphysiologicparametersattriage.Therearedifferentageappropriateversions:theyounger child TEWsisforpatientssmallerthan95cmoryoungerthan3years(seeFigure12);the older child TEWsisforpatients96cmto150cmor3yearstoaround12years(seeFigure13);andthe adult TEWsisforpatientsolderthan12yearsortallerthan150cm.Olderchildren,whereyouareunsurewhichformtouse,shouldbemeasured.Iftheyareover150cmthentheadultversionshouldbeused.ThisstandardisedscoringsystemhasbeenvalidatedandmanyoftheboxesintheTEWScalculwrareshadedgrey.Theseboxescannotbeassignedascore.Thismeansthatfortemperature,forexample,itisonlypossibletoscore0or2points,dependingonthevalueoftherecording.
YOUnGER ThAn 3 YEARs
/ sMALLER ThAn 95 cm
YOUnGER ChILD TEWs
3 2 1 0 1 2 3
Mobility Normalforage
Unable to moveasnormal
RR less than 20 20-25 26-39 40-49 50or
more
hR less than 70 70-79 80-130 131-159 160or
more
Temp FeelsCold
Under35˚35˚-38.4˚
FeelsHot Over38.4˚
AVPU Alert ReactstoVoice
ReactstoPain
Unres-ponsive
Trauma No YesFigure 12: Younger Child TEWS (younger than 3 years)
3 to 12 YEARs OLD / 95 to 150 cm
tall
OLDER ChILD TEWs
3 2 1 0 1 2 3
Mobility Normalforage
Unable to walkasnormal
RR less than 15 15-16 17-21 22-26 27or
more
hR less than 60 60-79 80-99 100-129 130 or
more
Temp FeelsCold
Under35˚35˚-38.4˚
FeelsHot Over38.4˚
AVPU Confused Alert ReactstoVoice
ReactstoPain
Unres-ponsive
Trauma No YesFigure 13: Older Child TEWS (age 3 - 12 years)
5
TriageEarlyWarningScoreTEWS

27SATS TRAINING MANUAL 201226 SATS TRAINING MANUAL 2012
OLDER ThAn 12 YEARs /
TALLER ThAn 150cmtall)
ADULT TEWs
3 2 1 0 1 2 3
Mobility Walking WithHelp Stretcher/Immobile
RR less than 9 9-14 15-20 21-29 more
than29
hR less than 41 41-50 51-100 101 - 110 111-129 more
than129
sBP Less than 71 71-80 81-100 101-199 more
than199
Temp ColdOR Under35˚ 35˚-38.4˚
HotOR Over38.4˚
AVPU Confused Alert ReactstoVoice
ReactstoPain
Unres-ponsive
Trauma No YesFigure 14: Adult TEWS (older than 12 years)
5.1ObservationsattriageTocalculatetheTEWSthefirststepistoperformtheobservationsrequiredbytheTEWS.
REsPIRATORY RATEThepatient’srespiratoryrateiscalculatedbycountingthebreathsfor30secondsandthenmultiplyingbytwo.Thisshouldbedoneatthefirstopportunitywhenthechildisquiet.Ifthechildissmallitisbesttoleavehim/herinthemother’slap.Donotundressthechildtocounttherespiratoryrateasdoingthismayupsethim/her.Countthebreathingratebyobservingratherthantouchingthechild.
hEART RATETomeasuretheheartrate,thetriageprovidercanmanuallycounttheheartratebyfeelingthepulsefor30secondsandthenmultiplyingbytwo.Alternativelyaheartratemonitorcanbeused(ideallynotfromasaturationmonitor–astheheartrateonthesemonitorscanbeunrelaibleandcanchangefrequentlyifthechildmoves).
TEMPERATUREThetemperatureismeasuredusingeitheranelectronicormercurythermometer(preferablyalow-readingthermometer).RectaltemperatureshouldNOTbetakenroutinely.
AVPU AVPUisdonebyseeingifthechildisalert.Ifnotobviouslyalertthenthetriageproviderneedstoobservethechild’sresponsetotheir(ortheparent’s)voice.Ifthechildrespondstovoiceandisthenalert–heisan‘A’–butifheremainsdrowsythenheisa‘V’’.Ifhemakesnoresponsetovoicethenthetriageproviderneedtoassesstheresponsetoapainfulstimulus(e.g.nailbedpressureorsternalrub)–ifthechildrespondstothiss/heisa ‘P’.Ifthereisnoresponsetoeitherverbalorpainstimulithepatientislabelledasunresponsive.
TriageEarlyWarningScoreTEWS
DO nOT UPsET ThE ChILD thisaffectsyourobservationsforTEWS
V meansthepatientisnotfullyalertandREsPOnDs OnLY TO YOUR VOICE. Another way of describing this = ‘lethargic’
P meansthepatientisnotalert anddoesnotrespondtoyourvoicebutREsPOnDs OnLY TO A PAInFUL sTIMULUs
MOBILITY Mobilityisobservedbynotingthemodeinwhichthepatienthastobemobilised.Asmallbabyiscarriedbythecarer–asmightasmallinfantorchild.Youneedtoassessifthelevelofmovementisnormalforthatparticularchild.Intheeventthatthechildoradultisinawheelchairduetopermanentparalysis2pointsaregivenformobilityasthechildinawheelchairismoreatrisk.
TRAUMATraumaispresentifthereisANYinjurytothepatientwithinthepast48hours.
5.2 Terminology and key concepts1. Confusion:Anolderchildmaybereportedtohaveconfusedbehaviourorthismaybe
discoveredattriage.Aconfusedchildappearsdisorientated,s/hemaynotbeinteractingnormallywiththecarerortheenvironment,s/hemaybedeliriousorhallucinating.Aconfusedchildmaybetalkingalotandaggressiveors/hemaybequietandfearfullooking.Thissignisdifficulttodetectinyoungerchildrenwhoareusuallypre-verbal-soitisonlyincludedontheTEWSfortheolderchild.
2. AcutevsChronic:ManypatientsinSouthAfricaarechronicallyunwellwithseriousconditionssuchasTBorHIV/AIDS.Inthesepatients,dailyrestingphysiologysuchasrespiratoryratemaybeabnormal.Thisisimportanttobearinmind,astheirTEWSwillbehighandtheywillbegivenanoverlyhightriagecode(theymaybeovertriaged).Itisnotfortheinexperiencedtriageprovidertodecidewhetherthisisthecaseornot,assickpatientsmaybemissed.However,itisappropriatetoaskaseniordoctororsistertoreviewthepatient’striagecode.
3. The younger and older child:Youngerandolderchildrenhavedifferentrestingvitalsignstoadults.Theseareoftendifficulttoobtain,andthepatientsoftencry,whichpushesuptheirrespiratoryandheartrate.Thevaluesstillneedtoberecordedasyoumeasurethem,sothatacorrectscorecanbegivenintheTEWS,buttelltheseniordoctororsisterthatthechildwascryingwhentheywererecorded.Thesestaffmemberscanthendecidewhetherthechildhasbeenovertriagedornot.
Assessment QuestionsClearlyindicatewhetherthefollowingstatementsaretrueorfalse:
1. IfachildisnineyearsoldweusetheolderchildTEWS.
True False
2. Alwaysundressachildandweighthemsothatitiseasiertoobtaintheirvitalsigns.
True False
3. Toaccuratelyobtainarespiratoryratealwaysstartwhenthepatientisatrest,countrespirationsfor30secondsandmultiplybytwo.
True False
Choosethecorrectanswer:4. TheadultTEWSconsistsofthefollowingparameters: (a) Mobility,respiratoryrate,heartrate,temperatureandbloodpressure (b) Mobility,capillaryrefilltime,heartrate,temperatureandbloodpressure (c) Mobility,respiratoryrate,heartrate,temperature,systolicbloodpressure,AVPUandtrauma (d) Mobility,respiratoryrate,heartrate,temperature,AVPUandtrauma (e) Mobility,respiratoryrate,oxygensaturationlevelandbloodglucoseconcentration
5. TheolderchildTEWSconsistsofthefollowingparameters: (a)Mobility,respiratoryrate,heartrate,temperatureandbloodpressure (b) Mobility,capillaryrefilltime,heartrate,temperatureandbloodpressure (c) Mobility,respiratoryrate,heartrate,temperatureandtrauma (d) Mobility,respiratoryrate,heartrate,temperature,AVPUandtrauma (e) Mobility,respiratoryrate,oxygensaturationlevelandbloodglucoseconcentration
TriageEarlyWarningScoreTEWS

29SATS TRAINING MANUAL 201228 SATS TRAINING MANUAL 2012
ADDITIOnAL InVEsTIGATIOns
LearningObjectives:
• Befamiliarwiththeadditionalinvestigationsandwhentoperformthem• Knowhowadditionalinvestigationsmaychangethetriageprioritylevel
Forallpatients(especiallychildren)immediateadditionalinvestigationsmaybeindicatedtoidentifypotentiallyseriouscomplicationsoftheirpresentingconditions.Checkifthepatienthasanyoftheconditionslistedbelowandactaccordingly.
RESPIRATORYRATE(RR)SCORESMORETHAN 1 POInT On TEWs:
AraisedRRforagemayindicateseriousunderlyingpathologysuchaschestinfectionrequiringsupplementaloxygen
REDUCED LEVEL OF COnsCIOUsnEssAllpatientsthatarenotfullyalert(i.e.confusedoronlyrespondingtoverbalorpainfulstimulus)needtohaveafingerprickglucotestdoneandshouldbehandedovertotheseniorhealthcareprofessional.Ifthechildisnotalert,orthecaregivervolunteersthatthechildismoresleepythannormal,thismayindicateaseriousevolvingmedicalconditionsuchasmeningitisorifassociatedwithahistoryoftraumatherecouldbeatraumaticbraininjury.Anysickchildwhohasnotbeenfeedingwellorhasbeenvomitingmaybecomedrowsybecauseofalowbloodsugarlevel.Tinybabiesandmalnourishedchildrenareparticularlyatriskofhypoglycaemia.
UnABLE TO sIT OR MOVE As nORMAL Ifthepatientisunabletowalkormoveasnormalorthecaregiverreportsthatthechildislethargicorunabletomoveasusual,thismayalsobeasignofseriousillnessorofalowbloodsugarlevel.
RECEnT sEIZURE/FITThepatientwhoisactivelyfittingwillhavebeentakentotheresuscitationarea.Inanychildwithahistoryofrecentseizuretherecouldbeeasilyidentifiableandtreatablecauses,includinghypoglycaemia,pyrexia(febrileseizure)orhighbloodpressure.
hIsTORY OF DIABETEsAllpatientswithdiabetesareatriskofeitherbecominghypoglyacaemic(usuallydrowsyorconfused)orhyperglycaemicwithdiabeticketoacidosis(DKA).Allthereforeneedaglucotestdoneatpresentation.
AdditionalInvestigations
6
WARnInGIf glucose is below 3 mmol/L movetoresuscitationand handovertoSHCPIf glucose is hi handovertoSHCP
WARnInGFor children if oxygen saturation isbelow92%onroomair Movetoresuscitationareaandadminister nasal prong or facemask oxygen
!ADDITIOnAL InVEsTIGATIOnMeasure oxygen saturation (for childrenonfinger,toe,handorearlobe,dependingonavailable
saturationprobeandco-operation)
WARnInG If glucose is below 3 mmol/L movetoresuscitationand handovertoSHCP
!ADDITIOnAL InVEsTIGATIOnPerformafingerprickglucotest immediately to exclude hypoglycaemia
WARnInG If glucose is below 3 mmol/L movetoresuscitationand handovertoSHCP
!ADDITIOnAL InVEsTIGATIOnPerformafingerprickglucotest immediately to exclude hypoglycaemia
!ADDITIOnAL InVEsTIGATIOnPerformafingerprickglucotestimmediately to exclude hypoglycaemia
DIABETEs AnD hYPERGLYCAEMIA (GLUCOTEST11ORMORE)
Allpatientswithaglucoseconcentrationof11mmol/Lormorerequireaurinedipsticktocheckforketones.
ChILD hAs MALnUTRITIOn WITh sEVERE VIsIBLE WAsTInG or WITh PITTInG OEDEMA OF BOTh FEETThischildisatriskofhypoglycaemia,aswellashypothermia
ABDOMInAL PAIn OR BACKAChE In FEMALEsTheadultfemalewithabdominalpainmayhaveanectopicpregnancyleadingtoseverepainanddiscomfortastimeprogresses.Shemaybeatriskforarupturedectopicorothercomplicationsinpregnancyrequiringemergencysurgery.Theseadditionalinvestigationsmayrapidlyidentifyveryillpatientsandchangetheircategory.Theyalsopreventand/oridentifyseriouscomplications.
Assessment QuestionsClearlyindicatewhetherthefollowingstatementsaretrueorfalse:
1. Apatientwithaglucoseof11mmol/Lneedstohaveaurinedipstickdonetocheckforketonesintheurine.
True False
2. Checkthefingerprickhaemoglobinonallpatientsthathaveahistoryofdiabetes.
True False
3. Doaurinedipstickandurinepregnancytestonalladultfemalespresentingwithabdominalpain.
True False
Choosethecorrectanswer:4. Performafingerprickglucotestonthefollowingcases: (a)Currentorrecentseizure (b) Facialburn (c) Reducedlevelofconsciousness (d) Historyofdiabetes (e) a,candd
5. ThefollowingtwoadditionalinvestigationsmayupgradeapatienttotheRedcategory: (a) Oxygensaturationlevelsinchildrenandfingerprickhaemoglobin (b) Fingerprickhaemoglobinlevelsandurinedipstick (c)Urinedipsticktestandoxygensaturationlevels (d) Fingerprickglucotestandoxygensaturationlevels (e) Fingerprickglucotestandfingerprickhaemoglobin
!ADDITIOnAL InVEsTIGATIOnPerform a urine dipstick to check for ketones
WARnInG If glucose is below 3 mmol/L movetoresuscitationand handovertoSHCP! ADDITIOnAL InVEsTIGATIOn
Performafingerprickglucotest immediately to exclude hypoglycaemia
PERFORM A FInGER PRICK GLUCOTEsT In ThE FOLLOWInG CAsEs:
• Reducedlevelofconsciousness
• Unabletositormoveasusual• Currentorrecentseizure• Knownwithdiabetes• Severemalnutrition !
ADDITIOnAL InVEsTIGATIOnPerform a urine dipstick and urine pregnancy test
AdditionalInvestigations

31SATS TRAINING MANUAL 201230 SATS TRAINING MANUAL 2012
ADDITIOnAL TAsKs
LearningObjectives:
• Befamiliarwiththeadditionaltasks• Knowwhentoperformadditionaltasks
TInY BABY UnDER 2 MOnThs Smallbabiesunder2monthsaremoredifficulttoassess,theirsymptomsareoftennon-specific,theyhavelowerimmunitythanotherchildrensoaremorepronetoinfections,andtheydeterioratemorequickly.Theythereforeneedtobeassessedasapriority.
POIsOnInG OR OVERDOsEToddlersareinquisitiveandliketoexploretheirenvironments.Theymayaccidentallyingestavarietyofhouseholdsubstances,pesticidesormedications.Achildwhohasingestedapoisoncandeterioratequickly.Theymayrequireaspecificantidoteandifapoisonormedicationhasbeeningestedrecentlyimmediateinterventionmaybeneeded(e.g.activatedcharcoal).ItisthereforeimportanttoconsultaSHCPforchildrenandadultsevenifthepatientappearsstable.
IF ChILD APPEARs TO BE In PAIn or Is InCOnsOLABLY CRYInGThismaybeduetoamedicalcauselikeanearinfectionorfromsevereheadacheduetomeningitis.Ortheremaybeanobviouscausesuchasafractureorlaceration.Painisobviouslyunpleasantforboththechildandcarer.Itisgoodpracticetoinitiateanalgesiaassoonaspossibleforchildrenandadults.
BURnThepatientwillbeexperiencingpainandespeciallychildrenhavethepotentialtodeterioraterapidlyfromsignificantfluidlossesandmaydevelophypothermia.Iftheburnisrecent(<3hrs)immediateinterventionmaylimittheextentoftissuedamage.
TEMPERATURE38.5˚CORMOREAveryhightemperaturewillresultinphysiologicalchangesthatmayaffecttheTEWS,andmakethepatientfeeluncomfortableandinsomechildrenmaybeassociatedwithafebrileseizure.
TEMPERATURE35.5˚CORLESSHypothermiamightbeasignofseveresepsiswithverysmallbabies,ex-prematurebabiesandseverelymalnourishedchildrenbeingthemostatrisk.
DIARRhOEA & VOMITInGEvenifthechildhasnoorsomedehydration,thechildisatriskofbecomingdehydratedwhilstwaitingtobeseenandshouldreceiveoralrehydrationtotreatand/orpreventfurtherdehydration
ADDITIOnAL TAsKTiny baby under 2 months refer to shCP
ADDITIOnAL TAsKPoisoning/overdose refer to shCP
ADDITIOnAL TAsKPain or inconsolable crying check with shCP for initiation of analgesiaandreview
ADDITIOnAL TAsKPain check with shCP for initiationofanalgesiaandreview
ADDITIOnAL TAsKIftheburnoccurredrecently(within3hrs) it is still worthwhile to cool the burnt area with water,forexample,byrunningcooltapwaterovertheburntareafor30minutes.Thechildshouldthenbedriedandwrappedinacleansheetorblankettoavoidhypothermia.
Theburncanbecoveredinclingwrapifavailable,oracleandrysheetortowelwillalsobesuitable.
ADDITIOnAL TAsKhigh temperature removeexcessiveclothing and check with shCP for initiationofanalgesiaandreview
7
ADDITIOnAL TAsKLow temperature warm the patient with additional blankets for children with a
capifavailableandhandovertoSHCP
Forallpatients(especiallychildren)whethertriagedRED, ORAnGE, YELLOW OR GREEnimmediateadditional tasksmaybeindicatedtostabilisethepatientand/oridentifyorpreventpotentiallyseriouscomplications.Checkifthechildhasanyoftheconditionslistedbelowandactaccordingly.
ADDITIOnAL TAsKDiarrhoea&vomiting take child toORTcornerandadvisecaregiverto start ORT by cup and spoon
AdditionalTasks
VOMITInG WIThOUT DIARRhOEA AnD ThE ChILD Is DEhYDRATEDVomitingalonewhichissevereenoughtoresultindehydrationmayindicateadiagnosisotherthansimplegastroenteritise.g.urinarytractinfection;asurgicalproblemwithbowelobstruction,;diabeticketoacidosisorevenmeningitisoranothersevereinfection.Itmaynotbeappropriatetoautomaticallycommencethischildonatrialoforalrehydration–andsosenioradviceshouldbesought.
IF ThE ChILD hAs A CLOsED FRACTUREThesechildrenwillbeexperiencingsignificantpain-bothmedicationandimmobilizationoftheaffectedlimbwillprovidesomerelieffromthepainandshouldbeinitiatedpriortoformalassessment
ChEsT PAInPatientswithchestpainmaybehavinganacutemyocardialinfarct(AMI).AnimmediateECGisrequiredtoruleoutapotentialAMI.
ACTIVE OnGOInG BLEEDInG Childrenhaveasmallcirculatingbloodvolume,andareatriskofbecomingshockedquicklyifthereisongoingbleedingfromatraumasite
hIsTORY OF RECEnT BLEEDInG - EIThER RECTAL, ORAL OR FROM A sITE OF TRAUMAThispatientmaybeanaemicfrombloodloss
PREsEnTInG COMPLAInT Is ABDOMInAL PAInAbdominalpainisacommoncomplaintinchildrenandithasawidevarietyofpossiblecausesincludingurinarytractinfection,diabeticketoacidosis,hepatitisorothercauses.Aurinedipstickforchildrenandadultswillassistinexcludingordiagnosingthese.Theseadditionaltasksmayassisttorapidlyidentifyveryillpatientsandpreventandidentifyseriouscomplications.Theyalsoimprovequalityofcarebyprovidingrelieffrompain.
Additional Tasks at triageADULT PATIEnTs
PROBLEM IMMEDIATE TAsKs1.Temperature38.5°ormore Paracetamol1gorallystat(documentinthenotes)
2.Temperature35°orless Warmthepatientwithblanketsifavailable3.Diabetesandhyperglycaemia
(glucotest11mmol/Lormore)Urinedipsticktocheckforketones
4.Historyofbleeding Fingerprickhaemoglobin5.BleedingPR,POorfromthesiteoftrauma Fingerprickhaemoglobin6.Abdominalpainorbackacheinmales Urinedipsticks7.PVbleeding Urinedipsticks,Urinepreganancytest
Fingerprickhaemoglobin
ADDITIOnAL TAsKVomiting without diarrhoea refer to shCP for assessment
ADDITIOnAL TAsKPain checkwithSHCPforinitiationofanalgesiaandreviewClosed fracture immobilise affected limb with simple padded splint or a triangular bandage sling and get a wheelchair or stretcher if required
ADDITIOnAL TAsKActivebleed apply direct pressure to the site of trauma with a dry dressing andperformfingerprickhaemoglobinto
obtainabaselineandhandovertoSHCP
ADDITIOnAL TAsKhistory of bleeding checkfingerprickhaemoglobin.Iflessthan8g/dlthenhandovertoSHCP
ADDITIOnAL TAsKChest Pain perform an ECG to rule out potential AMIandhandovertoSHCP
ADDITIOnAL TAsKFor a younger child Place a urine bag, ifolderchild,givecontainer
AdditionalTasks
A senior healthcare professional should be alerted in the following cases:• Tinybabyyoungerthan2monthsold•Reducedlevelofconsciousness• Achildinpainincludingfracturesandburns•Poisoningestionoroverdose
•Veryhighorverylowtemperatures•Vomitingonlywithdehydration• Theseverelymalnourishedchild•Achildwithactivebleeding
33SATS TRAINING MANUAL 201232 SATS TRAINING MANUAL 2012
PAEDIATRIC PATIEnTsPROBLEM IMMEDIATE TAsKs
1.PoisoningORoverdose RefertoSeniorHealthcareProfessional(SHCP)2.ChildinpainORinconsolablecrying CheckwithSHCPforanalgesiainitiation3.Childwithaburn CheckwithSHCPforanalgesiainitiation
Ifburnoccurredwithin3hours,cooltheburntareaCoverburninclingwraporcleandrysheet
4.Temperature38.5°ormore Removeexcessiveclothing&discusswithSHCP5.Temperature35°orless Warmthechildwithblanketsifavailable.RefertoSHCP
6.Diarrhoea TaketoORTcornerandadvisecaregivertogiveORTbycupandspoon
7.Vomitingwithoutdiarrhoeabutwithdehydration RefertoSHCPforassessment
8.Presentingcomplaint-abdominalpain youngerchild-urinebag/olderchild-urinecontainer9.Closedfracture CheckwithSHCPforanalgesiainitiation
Immobilizeaffectedlimbwithasimplepaddedsplintortriagularbandage
10.Activeongoingbleeding ApplypressuretothesiteoftraumaPerformfingerprickhaemoglobintoobtainabaselineRefertoSHCP
11.Historyofrecentbleeding PerformfingerprickhaemoglobinIflessthan8g/dlthenrefertoSHCP
Assessment QuestionsClearlyindicatewhetherthefollowingstatementsaretrueorfalse:
1. AtinybabyundertwomonthsshouldalwaysbereferredtotheSHCPoncetheyhavebeencomprehensivelytriaged.
True False
2. Apatientwithanactiveongoingbleedshouldplacethebleedingareaunderrunningwater.
True False
3. AchildthatisvomitingonlywithnodiarrhoeashouldfirstbereferredtotheSHCPforfurtherassessmentbeforecommencingthechildonatrialoralrehydration.
True False
Choosethecorrectanswer:4. Inachildwithaburninjuryfromboilingoilthatoccurred20minutesago: (a) Theburntareamaybecoveredinclingwrapifavailable (b) Coolrunningtapwaterovertheburntareafor30minutesmay
limittheextentoftissuedamage (c) Theburntareashouldbewrappedinacleansheettopreventhypothermia (d) aandb (e) a,bandc
5. Theseniorhealthcareprofessionalshouldbeconsultedinthefollowingcases: (a) Poisoningestionandoverdose (b) Aseverelymalnourishedchild (c) Vomitingonlywithdehydration (d) aandc (e) a,bandc
AdditionalTasks
TRIAGE In COnTEXT
8.1 Pre-hospitalTheuseoftriagewithinapre-hospitalsettingisgenerallywellacceptedandunderstooduniversally.Whilstthisneedisquiteobvious(evencritical)duringmajorincidents,it’sthedailyapplicationoftriageprinciplesinthedespatchofambulanceresourceswhereithasthemostbenefit.Inthesescenarios,triagepermitstheEMSdespatchertoapplyrulesbaseddecisionmakingtowhatisanotherwiseimpossiblechoice.Thepre-hospitaluseoftriageinthefieldvariesfromregiontoregion,butisgenerallycategorisedintofourpriorities(representedbythecoloursred,yellow,greenandblue).Suchtriagetypicallyusesinstabilityofvitalsignstodifferentiatehighfromlowprioritypatients.Discrepanciesintriageappearwhenpersonnelofdifferinglevelsofmedicalexperienceandqualificationsneedtoassesspatientsastherearenocleardefinitionsof‘unstable’physiology.Theterms‘stable’and‘unstable’arepoorlyunderstoodandfailtoaccuratelyreflectthepatient’sclinicalcondition.Accuratepre-hospitaltriageisessentialforappropriatecalloutofsecondaryresources;,accuratenotificationofreceivinghospitals,andqualityassessmentandauditoftheambulanceservice.Thisisparticularlypertinentinaeromedicalcalloutrequestsanduseofthisspecialisedresource.Forthesereasonstriagetoolsbasedonobjectivephysiologicaldiscriminatorsareessential.
8.2 Patient streamingTriageassignsthepatienttoanacuitylevel,whichthendictatestheamountoftimethepatientcanwaitsafelybeforebeingseen:Redimmediate,Orangewithin10minutes,YellowwithinanhourandGreenwithinfourhours.Itistherecommendedpracticeto“stream”thesepatientcategoriestodifferentareasand/orhealthcareproviderswithinthefacility.ThenormalstreamingpatternwouldbeRedstoresus,OrangesandYellowstoMajorsandGreenstoMinors,whichwouldbemannedbystaffdedicatedtotheseareas.Forthemostpart,streamingpatientsaccordingtoacuitywillalsostreamthemaccordingtoresourceuse:fullmonitoring,accesstohigh-powereddrugsandinterventionswithfullteamresponseisnecessarytoeffectivelytreattheRedpatient,whilearoomwithachairandasinglepractitionermaybeallthatisnecessarytoseeandtreatthepatientsintheGreenstream.Howandwherepatientsarestreameddependsontheload,manningandinfrastructureoftheEmergencyCentreorHealthFacility.Itisimportantinanysystemthatprioritisesorder-to-be-seenbyanythingotherthan“first-come-first-served”tohaveaplantoseethelowerprioritypatients.Streamingisapossiblemechanismtoachievethis.Withoutstreaming,theGreenpatientwillkeepbeingpushedtothebackofthequeuebythepatientofhigheracuity,whobynecessityshouldbeseenfirst.Withstreaming,thehigheracuitypatientsareseenbeforetheydiewhiletheloweracuitypatientsareseeninanotherareabeforetheyleave!
8.3 InfrastructureTriageisaprocess,notaplace,butforthemostpartwillneedanareafortriageofthosepatientsnotsentdirectlythroughtoresusormajors.ThisareashouldallowforprivacyandbesetupinordertoperformthevitalsignsfortheTEWS,additionalinvestigationsandtasks.Theroomshouldpreferablyallowforone-wayflowofpatientsfromthewaitingroomintoasubwaitingareaintheareatowhichtheyhavebeenstreamed.Ifnotpossible,somesortofdemarcationoftheareaorpatientsshouldbemadeinordertoseparatethosealreadytriagedfromthosewhohavenotbeenassessedbythetriageofficer.
8.4AlignmentofstafftotemporalflowofpatientsItisimportantthattriage,thetooltoensurethatpatientsareassessedtimeously,doesnotbecomethebottleneckinthesystem.Importantly,ifthedoctorisreadyforthenextpatient,butcannotseethemastheyare“firstgettingtriaged”,theobjectisbeingdefeated!Moreoftenthebottleneckoccursduetofailuretoalignstaffwiththeflowofpatients.Forthemostpart,itispossibletopredictthetimesofdaywhentheflowofpatientsintotheECisheavier(typical“saddle-shaped”curve).Staffingfortriageneedstoreflectthisflow.Thereshouldalsobesomesortofplaninplacetodealwithunexpectedinfluxofpatients:eachfacilityshouldhaveanupperlimitofpatientsthattheyarewillingtohavewaitingfortriage,overwhichacontingencyplanneedstobeactivated:egaregionalhospitalhasanagreementthatiftherearefiveormorepatientsneedingtriage,anurseiscalledfrommajorstohelptriagethepatientsuntilthelevelisbackdowntolessthanfivewaiting.
8
TriageinContext

34 SATS TRAINING MANUAL 2012
sUMMARY
Triageisanessentialfirststepinefficientandeffectiveemergencycare–whetherontheroadsideorinthepublicorprivatehospitalarena.Arobusttriagetoolwillhelptosavelivesandreducemorbidity.TheSouthAfricanTriageScalehasbeenderivedbyapanelofexpertsinEmergencyMedicine(doctors,nursesandparamedics),andisscientificallyproven.Ithasbeenshowntoimprovewaitingtimesandmaketheemergencycentrerunmoresmoothly.However,attentionneedstobepaidtothosepatientstriagedGreen,especiallyinpeaktimes,andtheSATGrecommendstheuseofstreamingwithaclinicalnursepractitionerordoctortoseethisgroup.TheSATShasbeenvalidatedaspartofaMastersinPhilosophy(MPhil)with700publicsectorpatients,anMPhilwith2000privatesectorpatientsandaPhD.Feedbackfollowingpublicationinfourmajorjournalshascontributedtotheprocess.ThisisEdition3andweacceptthatthetoolmaynotbeperfect,thatiswhyyourfeedbackissoimportant.Inaddition,therewillbeongoingresearchaimedatkeepingthetoolaccurateandappropriate.Ifnecessary,subsequenteditionswillfollow.
Online resources:
Forfurtherinformationpleasevisit
www.emssa.org.za/sats
Contact details:
MicheleTwomey
SATSImplementationAdvisor
0828503281
REFEREnCEs
1. BruijnsSR,WallisLA,BurchVC.EffectofintroductionofnursetriageonwaitingtimesinaSouthAfricanemergencydepartment.EmergMedJ2008;25:395-397.
2. TwomeyM,WallisLA,ThompsonML,MyersJE.TheSouthAfricanTriageScale(adultversion)providesreliableacuityratings.IntEmergNurs.PublishedOnlineFirst:19September2011.doi:10.1016/j.ienj.2011.08.002.
3. TwomeyM,WallisLA,ThompsonML,MyersJE.TheSouthAfricanTriageScale(adultversion)providesvalidacuityratingswhenusedbydoctorsandenrollednursingassistants.AfricanJEmergMed2012;2:3-12.
4. BruijnsSR,WallisLA,BurchVC.AprospectiveevaluationoftheCapetriagescoreintheemergencydepartmentofanurbanpublichospitalinSouthAfrica.EmergMedJ.2008;25:398-402.
5. PolicyforimplementationofthetriageofpatientsinWesternCapeemergencyunits.CircularH7of2006.DepartmentofHealth,ProvincialGovernment,update2012.
6. GottschalkS,WoodD,DeVriesS,WallisL,BruijnsS,OnbehalfoftheCapeTriageGroup.Thecapetriagescore:anewtriagesystemSouthAfrica.ProposalfromtheCapetriagegroup.EmergMedJ2006;23:149-153.
7. AugustynJ.TheSouthAfricanTriageScale:atoolforemergencynurses.ProfNursToday2011;15:24–29.8. IsaacsAA,HellenbergD.Implementingastructuredtriagesystematacommunityhealthcentre(CHC)using
Kaizen.SAFamPract.2009;519. GoudgeJ,CornellJ,McIntyreD,etal.Privatesectorfinancing.In:NtuliA,SulemanF,BarronP,McCoyD:editors.
SouthAfricanHealthReview2001.Durban:HealthSystemsTrust;2001.10.BradshawD,GroenewaldP,LaubscherR,NannanN,NojilanaB,NormanR,PieterseDandSchneiderM.Initial
BurdenofDiseaseEstimatesforSouthAfrica,2000.CapeTown:SouthAfricanMedicalResearchCouncil,2003.11.IsersonKV,MoskopJC.TriageinMedicine,PartI:Concept,History,andTypes.AnnEmergMed.2007;49:275-281.12.FitzGeraldG,JelinekGA,ScottD,GerdtzMF.EmergencydepartmentTriagerevisited.EmergMedJ2010;27:86-92.13.MollHA.ChallengesinthevalidationofTriagesystemsatemergencydepartments.JClinEpi2010;63:384-88.14.TwomeyM,deSaA,WallisLA,MyersJE.Inter-raterreliabilityoftheSouthAfricanTriageScale:Assessingtwo
differentcadresofhealthcareworkersinarealtimeenvironment.AfricanJEmergMed2011;1:113-118.
9
10
SummaryandReferences

Department of Health
PO Box 2060, Cape Town, 8000
Mobile:
For more information contact: Michele Twomey (SATS Implementation Advisor)
+27 850 3281 email: [email protected]
The South AfricanTriage Scale
(SATS)
Training manual 2012
Departmental Website: www.health.gov.za
Provincial Website: www.westerncape.gov.za