Embed Size (px)
Citation preview
830
slow-infusion pump or intermittently every one totwo hours,21-23 the mean induction/abortion intervalof approximately fifteen hours is shorter than that
resulting from hypertonic saline. The addition ofintravenous oxytocin increases the success-rate ofabortion resulting within a specific time and reducesthe amount of drug required. The intra-amnioticroute has been more popular for clinical trials in theU.S.A., and in one study using high doses a mean timeto abortion similar to that with extramembraneousadministration was reported.24 Intra-amniotic prosta-glandins in combination with another abortifacient-urea-have been reported to have advantages, withabortion resulting in a mean time of 10 hours.25 Thepotential complications of intrauterine injection in-clude sepsis, coagulation defects, and injury to thecervix. Other side-effects, including episodes of
vomiting and diarrhoea, have in general been found tobe tolerable, but the possible complications of prosta-glandin therapy in asthmatic patients have beenstressed. 26
For labour induction, intravenous prostaglandin E2and F2C( 27,28 are not used widely in routine obstetricpractice despite their freedom from the antidiureticproperties possessed by oxytocin 29 and their lack ofsignificant effects on placental function 30,31 and fetalwellbeing. 32 This is because they seem to have fewadvantages over oxytocin, except possibly for the
management of fetal death, in patients with severepre-eclampsia or cardiac disease, and for missed abor-tion and hydatidiform mole; in these last situationsthey are preferable to oxytocin because of therelative insensitivity of the uterus to oxytocin shortof term. There is little to suggest that the outcomeof labour at term is likely to be significantly differentwhen each of these substances is infused at an opti-mal concentration. Although sequential oxytocintherapy should be monitored with particular care,simultaneous administration may have some
advantages. 33If, then, intravenous usage has some limitations for
labour induction, what is the place of alternativeroutes ? ? The efficacy of vaginal administration re-mains uncertain because of the unpredictability of
21. Embrey, M. P., Hillier, K., Mahendran, P. ibid. 1972, iii, 146.22. Midwinter, A., Bowen, M., Shepherd, A. J. Obstet. Gynœc. Br.
Commonw. 1972, 79, 807.23. Miller, A. W. S., Calder, A. A., MacNaughton, M. C. Lancet,
1972, ii, 5.24. Craft, I. L. J. Obstet. Gynœc. Br. Commonw. 1973, 80, 46.25. Craft, I. L. Lancet, 1973, i, 1344.26. Smith, A. P. ibid. 1972, ii, 655.27. Karim, S. M. M., Trussell, R. R., Hillier, K., Patel, R. C. J. Obstet.
Gynœc. Br. Commonw. 1969, 76, 769.28. Karim, S. M. M., Hillier, K., Trussell, R. R., Patel, R. C., Tamu-
sange, S. ibid. 1970, 77, 200.29. Roberts, G., McGarry, J., Turnbull, A. C. Br. med. J. 1970, ii, 152.30. Keller, P. J., Ruppen, M., Gerber, C., Schmid, J. J. Obstet. Gynœc.
Br. Commonw. 1972, 79, 804.31. Thiery, M., Willighagen, R. G. J. I.R.C.S. Med. Sci. (73-9)
10-26-2.32. Thiery, M., Vroman, S., van Kets, H., Derom, R. Eur. J. Obstet.
Gynec. 1972, 4, 125.33. Naismith, W. C. M. K., Barr, W., MacVicar, J. Br. med. J. 1972,
iv, 461.
absorption, especially when the membranes are
ruptured. Intrauterine application is still a research
procedure. Oral administration, following the initialstudy by KARIM and SHARMA,34 has proved a con-venient and acceptable method of inducing labour forboth patient and midwife, particularly in multi-
gravidae and in primigravidae with favourable inductionfeatures,35,36 since doses are required only every oneor two hours. Concomitant amniotomy is important.37In patients with unfavourable induction features
larger doses may be necessary to induce optimaluterine activity, and with such doses gastrointestinalside-effects are likelier. In this group, in whichlabour will probably be prolonged, an intravenousoxytocic is preferable since an infusion may be
required to limit ketosis in any event. Buccal oxy-tocin is a possible alternative, but oral prostaglandinsare more convenient 38 and with these the risks of
mismanagement are smaller. On the other hand,buccal oxytocin is free from gastrointestinal side-effects.
Since some labours induced with oral prosta-glandins may last only a few hours,38 not all patientswill require an intravenous infusion. Accordingly,several departments are now assessing the outcomeof induction by means of pre-labour inducibilityscoring systems designed to determine the favour-ability of such features as the state of the cervix anddescent of the head. Amniotomy, associated with anintravenous oxytocic (either prostaglandin or
oxytocin), may be the most rational policy for mostpatients with unfavourable induction features. Forthe remainder more convenient oxytocics such as
oral prostaglandin may have advantages, especiallyin busy obstetric departments.
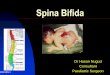
The Spinal Cord in Spina BifidaA WELL-KNOWN sculptured group in Athens is
that of a beautiful woman playing with a half-humangoatlike figure. This dwarf has cloven (club) feet,a projection in the mid-lumbar region surmounted bya tuft of hair (the most common site of a meningo-myelocele), a short body, relatively normal arms, anda somewhat unintelligent though very happy-lookingface and head. The sculptor depicts the end stageof the severest form of meningomyelocele likely tosurvive at that time-one with a covered back lesion,partial paralysis of the legs, talipes, and the absenceof urinary-tract lesions or gross hydrocephalus.With the development of antisepsis, some of the
more severe forms of meningomyelocele survivedand were to be found in long-stay hospitals as grossly34. Karim, S. M. M., Sharma, S. D. ibid. 1971, i, 260.35. Barr, W., Naismith, W. C. M. K. ibid. 1972, ii, 188.36. Craft, I. ibid. p. 191.37. Craft, I. ibid. p. 653.38. Craft, I. Proceedings of Upjohn Prostaglandin Symposium, Royal
College of Physicians, September, 1972, p. 25.
831
crippled and deformed children with severe scoliosis,paralysed legs, and varying degrees of hydrocephalus.The development of an effective ventricular shuntsystem, of new antibiotics, and of muscle transplantschanged all this and led to the formation of units
dealing with these children and the concentrationof material for study, previously not possible. Soon itbecame obvious that a large number of these childrenhad unsuspected spinal-cord deformities. In oneunit-Sheffield-a systematic necropsy study hasbeen carried out on the whole of the spinal cords of100 such children. 1
The most striking finding was that a high propor-tion of the cords showed duplication of the centralcanal and varying degrees of diplomyelia. Over 50%of the cords showed such an abnormality caudal tothe plaque and, of these, half were completely dividedinto two. In the plaque area a great variety of de-formities was found, only about half of them appearingto be lesions of a single whole cord. In 9% the spinalcord was completely divided into two parts, only oneof which was exposed-a condition that DUCKWORTHand his co-workers 2 call hemimyelocele. At the
plaque level, defined here as the whole exposedarea of the cord, varying amounts of nervous tissuewere absent; here much of the deficit was apparentlydue to recent trauma or exposure rather than to
non-development. The parts most destroyed werethe dorsal horns and the columns of the cords. Theventral horns often seemed to have an almost normal
complement of nerve cells, as did the dorsal-root
ganglia. 31% had complete division in the cordcranial to the plaque and in 50% the cord abnormalitycontinued up to the upper cervical region. In only14° did the cord cranial to the plaque appear normal.Hydromyelia, sometimes very gross, affected 29%of the cords proximal to the plaque. Only a smallproportion of cords with diplomyelia showed tra-versing bony spurs and connective tissue, and thesetraversing bands did not usually seem to be restrictingthe cord or compressing nerves. Likewise, the cer-vical cord in these children showed extensive changes.There was gross distortion and compression in thefirst two to three segments related to the prolapseof the medulla and to the Chiari II deformity, but,apart from this, almost half the cords showed varyingdegrees of hydromyelia and 20% showed syringo-myelia.3 In addition, there were often small necroticareas and evidence of old haemorrhages. Soft-tissuelesions of the cord membranes commonly accom-panied the nervous-tissue lesions.4 In 19% fibro-lipomas of the filum were detected; most of thesewere small and probably not of clinical importance,but 16% of these children showed dural fibrolipomasthese can distort the cord at a higher level), and 6%
Emery, J. L., Lendon, R. G. J. Path. 1973, 110, 83.Duckworth, T., Sharrard, W. J. W., Lister, J., Seymour, N.Deal Med. Chld Neurol. 1968, suppl. 22, p. 33.
MacKenzie, N. G., Emery, J. L. ibid. 1971, suppl. 25, p. 58.Emery, J. L., Lendon, R. G. ibid. 1969, suppl. 20, p. 62.
showed hamartomas related to diastematomyelia.Fat and squamous implants were common-beingperhaps accidental rather than congenital.A first reaction is to wonder that these children
survived at all. Only in recent years have childrenwith gross lesions reached adolescence, and only noware some of the nervous defects coming to light inthese children. At the meeting of the Society forResearch into Spina Bifida and Hydrocephalus inCardiff in June this year, participants were worriedabout previously unsuspected coordination defects inthe arms of these children-features that will inter-fere greatly with their earning capacity. The histo-
pathological findings listed here indicate that a largenumber can be expected to show signs of deficiencyin intercommisural activity. Their nerve defects are
likely to be extremely mixed ones, hence they cannotbe equated with a partial traumatic spinal-cordlesion or a spinal tumour. The gross number ofnerve-cells in the cords is often not greatly reduced 6
and, indeed, the number of cells in the dorsal rootganglia is probably normal.’ 7 Nerve-cell loss, in-
cidentally, possibly has to exceed 50% to producesymptoms in children. 8
The split spinal cord in these children is of geneticinterest. Almost 50% of apparently normal childrenhave minor degrees of splitting and forking of thecentral canal in the equinal cord,9 suggesting a
genetic tendency in this direction in a high proportionof the population. Probably it is the penetration ofthis effect that causes isolated diastematomyelia, andthis genetic factor apparently becomes increased ifassociated with dysrhaphism. Incidentally, of themany teratogenic agents that produce meningo-myelocele in mice and rats, none produce the splittingof the cord seen in man.The study of necropsy material from children is
inevitably biased to the more severe lesions, andthus the morbid anatomical findings reported fromSheffield are most relevant to the type of child whosesurvival is due to very active treatment. The findingsindicate problems likely to arise when efforts are
made to prolong the life of some of these children,and they also explain why results have, in many cases,been unexpectedly disappointing. In the treatment ofmeningomyelocele and hydrocephalus we have gonethrough a period of overoptimism, but there is now adanger of going to the opposite extreme. Precise
knowledge of the pathophysiology of these children isonly now emerging. Therapy has so far been largelyempirical. There is a need to start again; beforedecisions are made about treatment, these children
clearly require much more refined neurologicalassessment than seemed necessary in the past.5. Emery, J. L. Symposium on Myelomeningocele, American Academy
of Orthopedic Surgeons. St. Louis, 1972.6. Lendon, R. G., PH.D. thesis, University of Sheffield, 1968.7. Emery, J. L., Nunn, H., Singhal, R. Devl Med. Chld Neurol. 1973,
15, 467.8. Sharrard, W. J. W. J. Bone Jt Surg. 1955, 37B, 540.9. Lendon, R. G., Emery, J. L. J. Anat. 1970, 106, 499.