Embed Size (px)
Citation preview

The Sri Lanka Journal of Haematology
Volume 10 Issue 1 September 2018
THE OFFICIAL JOURNAL OF THE SRI LANKA COLLEGE OF HAEMATOLOGISTS
ISSN 1391-7919
In this issue
EDITORIAL Direct oral ancoagulants Are we aware
of their efficacy and safety
LEADING ARTICLE Predictors of bleeding in acute
dengue virus infecon
PERSPECTIVE Current issues in the management of
thalassaemia major
CASE REPORT 1 An early presentaon of classical
Hodgkin lymphoma with atypical pneumonia
CASE REPORT 2 Paroxysmal cold haemoglobinuria
A case series in children
IMAGES IN HAEMATOLOGY A case of
haemophagocyc lymphohisocytosis
RESEARCH ARTICLE A study of mean cell
volume (MCV) in paents who are treated at
Colombo South Teaching Hospital
CME Theme ndash Neutropenia in infants and children
The Sri Lanka College of HaematologistsThe Sri Lanka College of Haematologists
No 6 Wijerama House
Wijerama Mawatha
Colombo 7
No 6 Wijerama House
Wijerama Mawatha
Colombo 7
Phone 0112685088
Fax 0112685088
E-mail slcohaemgmailcom
Website wwwslchaemlk
Phone 0112685088
Fax 0112685088
E-mail slcohaemgmailcom
Website wwwslchaemlk
Editor Dr H W Chandima K KulathilakeMBBS DipPath MD(Haematology)
Editorial Committee Dr Senani WilliamsMBBS DipPath MD(Haematology) FRCPath(Haematology)
Dr Manal RathnayakeMBBS DipPath MD(Haematology)
Dr Durga MoratuwagamaMBBS DipPath MD(Haematology) FRCPath(Haematology)
The Sri Lanka Journal of Haematology
The Sri Lanka College of Haematologists
No 6 Wijerama House Phone 0112685088
Wijerama Mawatha Fax 0112685088
Colombo 7 E-mail slcohaemgmailcom
Printed by
Ananda Press277 Hokandara RoadThalawathugoda
E-mail anandapress65gmailcom
Volume 10 Issue 1 September 2018
ISSN 1391-7919
The Sri Lanka Journal of Haematology 1
HWCK Kulathilake SLJH 2018 10(1) 1-4
The only oral anticoagulant available in clinicalpractice for more than five decades has beenwarfarin a vitamin K antagonist (VKA) Despite itseffectiveness and feasibility for long term use ithas several short comings Warfarin has a variabledose response a narrow therapeutic index andnumerous drug and dietary interactions thatrequire frequent monitoring by the internationalnormalized ratio (INR) to ensure an adequate yetsafe dose1
These shortcomings have prompted the develop-ment of direct acting oral anticoagulants (DOACs)that directly act on coagulation factors such asfactors Xa and IIa (thrombin) From 2008 regulatoryagencies in EU and US have approved severalDOACs for specific indications based on the resultsobtained in clinical trials demonstrating efficacyand safety that are at least non-inferior if notsuperior compared to warfarin and heparins forstroke prevention in atrial fibrillation (AF) as wellas for treatment and prophylaxis of venous throm-boembolism (VTE)2
DOACs used in clinical practice at present includedabigatran rivaroxaban apixaban and edoxabanThese agents offer major pharmacological advan-tages over warfarin such as rapid onset of actionminimal drug or dietary interactions and predic-table pharmacokinetics which eliminates therequirement for regular coagulation monitoring12
DOACs can be divided into two broad classes (i)Direct thrombin inhibitors (dabigatran) which
Direct oral anticoagulants Are we aware of their efficacy and safety
Editorial
HWCK Kulathilake1
1Senior LecturerConsultant HaematologistDepartment of Pathology Faculty of MedicalSciences University of Sri Jayewardenepura SriLanka
Correspondence chandimawarawitayahoocouk
SLJH 2018 10(1) 1-4
inhibit thrombin (Factor IIa) and (ii) Factor Xainhibitors (rivaroxaban apixaban edoxaban)which inhibit factor Xa Apixaban rivaroxaban anddabigatran will be discussed in this review
Apixaban is approved for use in the prevention ofstroke and systemic embolism in adult patientswith nonvalvular AF and in the primary preventionof VTE in adult patients who have undergoneelective total hip arthroplasty (THA) or total kneearthroplasty (TKA)3
The efficacy and safety of apixaban have beenevaluated in phase 3 clinical trials The use ofapixaban in postoperative VTE Prophylaxis for TKAwas evaluated in (ADVANCE)-14 and ADVANCE-25
trials All the treatments in either arm of the 2trials (apixaban vs enoxaparin) were continued for10 to 14 days In ADVANCE-3 trial6 both drugs werecontinued for 35 days after THA Primary efficacy(symptomatic or asymptomatic VTE non fatal PEdeath) was similar in both drugs in ADVANCE-1and apixaban was superior to enoxaparin inADVANCE-2 and 3 trails The combined incidenceof major bleeding and clinically relevant non majorbleeding was less with apixaban use comparedwith enoxaparin use in ADVANCE-1 but equivalentin ADVANCE-2 and 3 trials
Apixaban was evaluated in the prevention ofstroke and systemic embolism in nonvalvular AFin 2 large randomized controlled trials apixabanversus aspirin to prevent stroke in atrial fibril-lation patients who have failed or are unsuitablefor Vitamink Antagonist Treatment (AVERROES)trial 7 and the Apixaban for Reduction in Strokeand Other Thromboembolic Events in AtrialFibrillation (ARISTOTLE)8
In both trials the primary efficacy outcome (strokeor systemic embolism) was superior with apixabanThe rate of major bleeding per year was less withapixaban compared with warfarin in ARISTOTLE
Key words warfarin direct oral anticoagulants clinical trials
The Sri Lanka Journal of Haematology2
HWCK Kulathilake SLJH 2018 10(1) 1-4
Rivaroxaban is approved for use in the primaryprevention of VTE in adult patients who haveundergone elective THA or TKA in nonvalvular AFin the treatment of DVT and PE and to reduce therisk of recurrent DVT and PE after initial treatment3
The efficacy and safety of rivaroxaban have beenevaluated in phase 3 clinical trials in differentclinical situations The Regulation of Coagulationin Orthopedic Surgery to Prevent Deep VenousThrombosis and Pulmonary Embolism (RECORD)1234 trials9101112 compared rivaroxaban withenoxaparin in Postoperative VTE Prophylaxis forjoint replacement surgery (THA and TKA) Riva-roxaban significantly reduced the total event ratecompared with enoxaparin in all four trials andthere was no difference in the incidence of majorbleeding between the rivoroxaban and enoxa-parin arms On the basis of these results riva-roxaban was approved in Europe and Canada forthe prevention of VTE in patients undergoingelective hip or knee arthroplasty
The EINSTEIN study 13 compared oral rivaroxabanwith enoxaparin followed by a VKA for 3 6 or 12months in patients with acute symptomatic DVT(initial treatment study) A parallel double blindrandomized study compared rivaroxaban withplacebo for an additional 6 or 12 months in patientswho had completed 6 to 12 months of treatment forVTE (continued-treatment study) The EINSTEIN-PE14 was a similar study that evaluated the samedose of rivaroxaban vs enoxaparinVKA in patientswith an acute symptomatic PE with or without DVT
In EINSTEIN rivaroxaban therapy was noninferiorto enoxaparinVKA therapy with regard to recurrentVTE (21 vs 30 Plt001) In the continued-treatment study rivaroxaban therapy was superiorto placebo use with regard to recurrent VTE (13vs 71 Plt001) The rates of symptomatic recur-rent VTE in the EINSTEIN-PE study were similarbetween the rivaroxaban and enoxaparinVKAgroups In both EINSTEIN and EINSTEIN-PE thesafety outcome of major or clinically relevant nonmajor bleeding were similar in both treatmentarms
The Rivaroxaban Once Daily Oral Direct Factor XaInhibition Compared with Vitamin K Antagonismfor Prevention of Stroke and Embolism Trial in AtrialFibril lation (ROCKET AF) study1516 evaluated
rivaroxaban for prevention of stroke or systemicembolization in patients with nonvalvular AF(intermediate to high risk of stroke) Patients wererandomly divided to receive either rivaroxaban 20mgday or warfarin (target INR 20-30) and thepatients were monitored for 24 months Riva-roxaban was non inferior to warfarin (21 vs 24per year Plt001 for noninferiority) in the primaryefficacy outcome of stroke and systemic embolismThere was no difference between patients takingrivaroxaban and those taking warfarin in terms ofall bleeding events
Dabigatran is approved for use in nonvalvular atrialfibrillation and in the primary prevention of venousthromboembolic events (VTEs) in adult patients withelective total hip (THA) or knee (TKA) arthroplastyDabigatran has been evaluated in several phase 3clinical trials to assess its safety and efficacy indifferent clinical situations
The RE-LY (Randomized Evaluation of Long-termAnticoagulant Therapy Warfarin compared withDabigatran) study1718 evaluated the efficacy andsafety of dabigatran at 110 or 150 mg twice dailycompared with dose-adjusted warfarin targetingan INR of 2 to 3 in patients with nonvalvular AF andan intermediate risk of thromboembolism Bothdoses of dabigatran were non-inferior to warfarinwhile the higher dose proved to be superior forthe primary outcome The major bleeding occurredat a rate of 311 271 and 336 year for thepatients treated with dabigatran 150 mg dabi-gatran 110 mg and warfarin respectively Thedifferences in both the efficacy and safety out-comes were statistically significant
The RE-COVER study19 evaluated patients withacute VTE for a period of 06 months The 6-monthincidence of recurrent symptomatic VTE andrelated deaths was 24 in patients treated withdabigatran vs 21 in those treated with warfarin(Plt001 for noninferiority) The rates of majorbleeding episodes were similar in both groups
Dabigatran in postoperative VTE prophylaxis forjoint replacement sugery was evaluated in theEuropean RE-MODEL study North American RE-MOBILIZE study the European RE-NOVATE (I) andthe North American RE-NOVATE (II) studies Therewere conflicting results between the first 2 trialsin postop TKA In RE-MODEL20 the incidence of VTE
The Sri Lanka Journal of Haematology 3
HWCK Kulathilake SLJH 2018 10(1) 1-4
or mortality was 377 in the enoxaparin armcompared with 364 in the dabigatran 220-mgarm (P=0003 for noninferiority) and 405 in thedabigatran 150-mg arm (P=017 for non-inferio-rity) However in RE-MOBILIZE21 the compositeof VTE and death occurred in 253 of those in theenoxaparin arm compared with 311 of those inthe dabigatran 220-mg arm (P=02) and 337 ofthose in the dabigatran 150-mg arm (Plt001) Thedifferences in efficacy between the 2 trials maybe due to the different dosing schedules ofenoxaparin So dabigatran may not be an equallyefficacious prophylaxis option in this settingAmong the 3 arms the incidence of major bleedingdid not differ significantly in the 02 trials
The RE-NOVATE I and II studies2223 evaluateddabigatran in preventing VTE after THA comparedwith enoxaparin In RE-NOVATE I the findingsconfirmed noninferiority for dabigatran (Plt0001for noninferiority) Furthermore RE-NOVATE IIdetected total VTE and death in 77 in thedabigatran 220-mg arm vs 88 in the enoxaparinarm (P=43) In both RE-NOVATE studies there wasno difference in major bleeding rates with eitherdose of dabigatran compared with enoxaparin
Since the introduction of DOACs in 2008 the globalanticoagulant market shows that warfarin use hasdeclined from 875 to 72 through 2008 to 2014while DOACs have shown an upward trend with amarket share of 155 as of 20142 The questionof whether these agents will replace warfarin andheparins which have been accepted as the goldstandard during all these years is one that needsto be answered after a thorough evaluation ofseveral aspects including high cost of DOACs lackof specific antidotes and lack of long-term safetydata
References
1 Galanis T Thomson L Palladino M et al J ThrombThrombolysis 2011 31 310 httpsdoiorg101007s11239-011-0559-8 PMid21327511
2 Oktay E Will NOACs become the new standard ofcare in anticoagulation therapy InternationalJournal of the Cardiovascular Academy 1 2015 1-4httpsdoiorg101016jijcac201506007
3 Wilson I Gonsalves Rajiv K Pruthi Mrinal MPatnaik The New Oral Anticoagulants in ClinicalPractice Mayo Clin Proc 2013 88(5) 495-511
httpsdoiorg101016jmayocp201303006PMid23639500
4 Lassen MR Raskob GE Gallus A Pineo G Chen DPortman RJ Apixaban or enoxaparin for thrombo-prophylaxis after knee replacement N Engl J Med2009 361(6) 594-604 httpsdoiorg101056NEJMoa0810773 PMid19657123
5 Lassen MR Raskob GE Gallus A Pineo G Chen DHornick P Apixaban versus enoxaparin for thrombo-prophylaxis after knee replacement (ADVANCE-2) arandomised double-blind trial Lancet 2010375(9717) 807-15 httpsdoiorg101016S0140-6736(09)62125-5
6 Lassen MR Gallus A Raskob GE Pineo G Chen DRamirez LM Apixaban versus enoxaparin forthromboprophylaxis after hip replacement N Engl JMed 2010 363(26) 2487-98 httpsdoiorg101056NEJMoa1006885 PMid21175312
7 Connolly SJ Eikelboom J Joyner C et al Apixaban inpatients with atrial fibrillation N Engl J Med 2011364(9) 806-17 httpsdoiorg101056NEJMoa1007432 PMid21309657
8 Granger CB Alexander JH McMurray JJ et alApixaban versus warfarin in patients with atrialfibrillation N Engl J Med 2011 365(11) 981-92h tt p s d o i o rg 10 1056 N E JM o a 1107039PMid21870978
9 Eriksson BI Borris LC Friedman RJ et alRivaroxaban versus enoxaparin for thrombo-prophylaxis after hip arthroplasty N Engl J Med2008 358(26) 2765-75 httpsdoiorg101056NEJMoa0800374 PMid18579811
10 Kakkar AK Brenner B Dahl OE et al Extended durationrivaroxaban versus short-term enoxaparin for theprevention of venous thromboembolism after totalhip arthroplasty a double-blind randomisedcontrolled trial Lancet 2008 372(9632) 31-9 httpsdoiorg101016S0140-6736(08)60880-6
11 Lassen MR Ageno W Borris LC et al Rivaroxabanversus enoxaparin for thromboprophylaxis aftertotal knee arthroplasty N Engl J Med 2008 358(26)2776-86 httpsdoiorg101056NEJMoa076016PMid18579812
12 Turpie AGG Lassen MR Davidson BL et al Riva-roxaban versus enoxaparin for thromboprophylaxisafter total knee arthroplasty (RECORD4) arandomised trial Lancet 2009 373(9676) 1673-80httpsdoiorg101016S0140-6736(09)60734-0
13 Bauersachs R Berkowitz SD Brenner B et al Oralrivaroxaban for symptomatic venous thrombo-embolism N Engl J Med 2010 363(26) 2499-510h tt p s d o i o rg 10 1056 N E JM o a 1007903PMid21128814
The Sri Lanka Journal of Haematology4
HWCK Kulathilake SLJH 2018 10(1) 1-4
14 Buller HR Prins MH Lensin AW et al Oral riva-roxaban for the treatment of symptomatic pulmonaryembolism N Engl J Med 2012 366(14) 1287-97httpsdoiorg101056NEJMoa1113572PMid22449293
15 Patel MR Mahaffey KW Garg J et al Rivaroxabanversus warfarin in nonvalvular atrial fibrillation NEngl J Med 2011 365(10) 883-891 httpsdoiorg101056NEJMoa1009638 PMid21830957
16 Fox KA Piccini JP Wojdyla D et al Prevention ofstroke and systemic embolism with rivaroxabancompared with warfarin in patients with nonvalvularatrial fibrillation and moderate renal impairmentEur Heart J 2011 32(19) 2387-94 httpsdoiorg101093eurheartjehr342 PMid21873708
17 Connolly SJ Ezekowitz MD Yusuf S et al Dabigatranversus warfarin in patients with atrial fibrillationN Engl J Med 2009 361(12) 1139-51 httpsdoiorg101056NEJMoa0905561 PMid19717844
18 Wallentin L Yusuf S Ezekowitz MD et al Efficacyand safety of dabigatran compared with warfarin atdifferent levels of international normalised ratiocontrol for stroke prevention in atrial fibrillationan analysis of the RE-LY trial Lancet 2010 376(9745)975-83httpsdoi org101016S0140-6736(10)61194-4
19 Schulman S Kearon C Kakkar AK et al Dabigatranversus warfarin in the treatment of acute venous
thromboembolism N Engl J Med 2009 361(24)2342-52 httpsdoiorg101056NEJMoa0906598PMid19966341
20 Eriksson BI Dahl OE Rosencher N et al Oraldabigatran etexilate vs subcutaneous enoxaparinfor the prevention of venous thromboembolism aftertotal knee replacement the REMODEL randomizedtrial J Thromb Haemost 2007 5(11) 2178-85httpsdoiorg101111j1538-7836200702748xPMid 17764540
21 Ginsberg JS Davidson BL Comp PC et al Oralthrombin inhibitor dabigatran etexilate vs NorthAmerican enoxaparin regimen for prevention ofvenous thromboembolism after knee arthroplastysurgery J Arthroplast 2009 24(1) 1-9 httpsdoiorg101016jarth200801132 PMid18534438
22 Eriksson BI Dahl OE Rosencher N et al Dabigatranetexilate versus enoxaparin for prevention of venousthromboembolism after total hip replacement arandomised double-blind non inferiority trialLancet 2007 370(9591) 949-56 httpsdoiorg101016S0140-6736(07)61445-7
23 Eriksson BI Dahl OE Huo MH et al Oral dabigatranversus enoxaparin for thromboprophylaxis afterprimary total hip arthroplasty (RE-NOVATE II) arandomised double blind non nferiority trialThromb Haemost 2011 105(4)721-9 httpsdoiorg101160TH10-10-0679 PMid21225098
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 5
1Professor Centre for Dengue Research Universityof Sri Jayewardenepura Nugegoda Sri Lanka2Weatherall Institute of Molecular Medicine JohnRadcliffe Hospital Oxford OX3 9DS UK
Introduction
Dengue viral infections represent one of the mostrapidly emerging mosquito borne infections in theworld which causes 100 million apparent dengueinfections each year1 From 2005 to 2015 althoughthe mortality rates due to many infectious diseasesdecreased the deaths due to dengue increasedby 487 resulting in an estimated 18400 deathsin 20152 Although there is a dengue vaccine licensedto be used in children over the age of 9 years thevaccine manufacturer and other authorities havesuggested that this vaccine should be avoided inindividuals who have not been infected with thedengue virus (DENV) due to the likelihood ofdisease enhancement3
Although the majority of those who are infectedwith the DENV develop asymptomatic or milddisease 478 to 5072 of individuals have shownto develop severe dengue depending on the epi-demic serostatus and circulating DENV serotypesduring that epidemic4 Severe dengue is charac-terized by clinically detectable vascular leakagethat manifest in the form of pleural effusions andascites which can lead to haemodynamic insta-bility and shock5 In addition patients may alsodevelop complications such as bleeding mani-festations liver and renal dysfunction Althoughmild forms of bleeding manifestations such aspetechiae and bleeding from sites of venipunctureare seen in many patients with dengue haemor-rhagic fever (DHF) significant bleeding such as pervaginal bleeding haematuria haematemesis and
Predictors of bleeding in acute dengue virus infection
Gathsaurie Neelika Malavige12
Leading article
Key words dengue viral infection bleeding plasma leakage
malena can lead to haemodynamic instability andshock Development of significant bleeding wasshown to be an independent risk factor associatedwith fatalities in patients with DHF6 Gastrointestinalbleeding alone was shown to strongly associatewith the occurrence of death7
Association of plasma leakage and bleeding
While bleeding manifestations are sometimesseen in patients with dengue fever (DF) significantbleeding is usually seen in those who have severeplasma leakage prolonged shock or organ dys-function89 Severe vascular leakage leading to poorperfusion of the intestinal mucosa and organdysfunction are thought to be the predominantcauses of intestinal bleeding10 Our data has shownthat bleeding manifestations were more frequentamong dengue patients in Sri Lanka in the pastcompared to recent epidemics possibly due tobetter fluid management and reduction in thedevelopment of shock For instance in a study doneby us in year 2004 in adult patients 42108 (389)patients developed bleeding manifestations11whereas the only 26179 (145) developedbleeding manifestations in a patient cohortstudied in years 2016 and 201712 Therefore bettermanagement of fluid leakage appears to indirectlyreduce the incidence of bleeding in dengue
Thrombocytopenia and occurrence of bleeding
Although severe thrombocytopenia was found tobe a predictor of significant bleeding in denguethrombocytopenia alone in the absence of a highhematocrit or liver dysfunction was not associatedwith significant bleeding13 Direct infection ofplatelets by the DENV destruction of platelets dueto immune complexes and bone marrow sup-pression have shown to be the predominant factorsleading to thrombocytopenia (Figure 1)14 Apartfrom the reduction of platelet counts platelet
SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
6
function has also shown to be significantlyimpaired in patients with DHF including impairedplatelet aggregation in response to ADP9 This wasshown to be accompanied by an increase in plasma-thrombomodulin and platelet factor-4 whichindicate an increased secretory activity9 Impairedplatelet function and destruction has also beenobserved in transfused platelets which have ledto a marked reduction in survival rates of trans-fused platelets especially in those with DHF1415
Due to the presence of severe degrees of throm-bocytopenia in the past many centres have pro-phylactically transfused platelets in order toprevent development of any bleeding Howeverseveral retrospective studies had shown thatprophylactic platelet transfusions were associatedwith fluid overload and prolonged hospital staywithout any reduction in bleeding manifestationsor improved platelet recovery1617 In order toaddress this controversy a multi centre rando-mized controlled trial carried out in several centresin Singapore and Malaysia in patients with plateletcounts 20000 plateletsmicroL showed that pro-phylactic platelet transfusions did not reduce theoccurrence of bleeding18 Instead platelet trans-fusions were associated with an increase incidenceof adverse effects including those of seriousnature such as anaphylaxis and transfusion relatedacute lung injury18 Therefore both the WHOguidelines and the National dengue managementguidelines do not recommend platelet trans-fusions but have advocated blood transfusions inthose who are suspected to have developedsignificant bleeding
The effect of many herbal preparations such as theleave extract of Carica papaya in improving plateletcounts have been studied and in vitro evidencehave shown that this leaf extract reduces plateletaggregation19 Two multi-centre randomizeddouble blind placebo controlled trials using Caricapapaya in India showed that this leaf extract doessignificantly increase platelet counts initiallyalthough there was no significant difference inplatelet counts 48 hours after administration ofthe leaf extract20 However these trials had notassessed the efficacy of this leaf extract onreducing plasma leakage organ dysfunction and
mortality and have not reported any adverseeffects as is indicated in the standard reporting ofclinical trials20 Therefore as it is difficult toascertain the other possible benefits or adverseeffects of this drug it would be important toconduct proper clinical trials according to theinternationally recommended guidelines
Coagulation abnormalities leading to bleeding
Apart from the presence of prolonged shocksevere liver dysfunction is suggested as one the mostimportant predictors of severe bleeding21 Manyclotting factors such as factor V VII VIII IX and Xfibrinogen protein C and S and antithrombin aresynthesized by the liver and low levels of theseproteins are seen in patients with acute dengueAlthough thromboelastographic studies have alsodemonstrated deficiency of coagulation factorsand abnormalities in platelet function the levelswere not associated with the degree of thrombo-cytopenia or liver dysfunction22
Many patients with DHF have a prolongedprothrombin time prolonged INR and activatedpartial thromboplastin time (aPTT) It is thoughtthat these abnormalities possibly occur due to thereduced production of these factors and alsoleakage of these proteins into extravascular spacesacross the dysfunctional endothelium92123 Prolon-gation of the prothrombin time has been shownto be an important predictor of occurrence ofbleeding in patients with severe plasma leakage21Although many studies have reported an increasein partial thromboplastin times and reduction infibrinogen concentrations9 change in these para-meters correlated with the extent of vascularleakage and not with bleeding24 More detailedstudies which have assessed changes of theseproteins at different stages of the illness haveshown that protein C S and antithrombin III levelswere significantly lower in patients with moresevere degrees of shock during the leakagephase However as these proteins returned tonormal levels following the leakage phase it hasbeen suggested that leakage of these proteinsinto extravascular tissues could be the mainfactor leading to low levels in patients with DHF(Figure 1)9
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 7
Endothelial activation and bleeding in dengue
Patients with more severe forms of dengue arealso shown to have high levels of tissue factorthrombomodulin and plasminogen activatorinhibitor type 1 (PAI-1) which have been attri-buted to endothelial platelet and monocyteactivation9 Endothelial activation and injury is alsoreflected by high levels of von Willebrand factor(vWF) especially in patients with severe shock23It was also shown that the number of circulatingendothelial cells and soluble thrombomodulinlevels were significantly higher in patients withprofound shock further supporting that endo-thelial injury occurs in severe dengue23 Thromo-bomodulin which is an integral membrane proteinexpressed on endothelial cells monocytes andcertain dendritic cells is cofactor in activation of
protein C Although soluble thrombomodulinlevels were markedly high in those with severeforms plasma leakage as protein C levels are lowthe contribution to these pathways in causingsevere dengue and bleeding is not certain
Despite significant derangements in prothrom-botic antithrombotic and fibrinolytic pathways asmost patients do not develop bleeding it issuggested that the combinations of many factorssuch tissue hypoxia acidosis along with thrombo-cytopenia are important co-factors Howeverplasma leakage secondary endothelial dysfunctionappears to be the most important factor leading toshock poor organ perfusion organ dysfunctionderangement of many coagulation pathways andbleeding510 We have identified that plateletactivating factor (PAF) significantly contributed to
Bleeding manifestations are thought to occur due to the complex interplay of many factors such asendothelial dysfunction liver dysfunction and thrombocytopenia Endothelial dysfunction leads to plasmaleakage and when severe leads to shock poor organ perfusion and tissue hypoxia Tissue hypoxia in thegastrointestinal and possibly the lung epithelium is thought to be the main contributing factors forbleeding from these sites Many clotting factors and antithrombic factors are also thought to extravasatein to the tissues leading to low levels of these in the plasma In addition liver dysfunction may also leadto reduction in the production of these factors
Figure 1 Factors that contribute to bleeding in acute dengue infection
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
8
vascular leakage in dengue25 In addition lipidmediators that oppose the action of PAF andprotect the endothelial barrier integrity such assphingosine-1-phosphate was found to bemarkedly low in patients with DHF especiallyduring the critical phase26
As plasma leakage appears to be the most impor-tant factor leading to all complications of dengueit would be reasonable to use drugs that preventor reduce vascular leakage as a suitable option toreduce severe dengue and associated compli-cations We have concluded a phase 2 randomizedplacebo controlled clinical trial in 183 patients atthe National Institute of Infectious Diseases SriLanka using a PAF receptor blocker known asrupatadine27 In this clinical trial we found thatrupatadine up to 40mg daily appeared safe andwell-tolerated in patients with acute dengue Inaddition patients given rupatadine had higherplatelet counts and lower aspartate-aminotrans-ferase levels during the critical phase and signifi-cantly smaller pleural effusions27 The develop-ment of significant bleeding manifestations suchas per vaginal bleeding and gastrointestinalbleeding was also lower in the group who receivedtreatment As the beneficial effects of this drugappeared to be greater when given early in theillness we are currently conducting another trialwhich is double blind randomized placebocontrolled trial in a larger cohort of patientsAlthough the initial trial showed promising resultsthese results should be interpreted with cautionuntil the same beneficial effects are seen in largertrials that we are currently carrying out
Summary
Endothelial dysfunction leading to plasma leakageappears to be the most important predictor ofoccurrence of bleeding in acute dengue Althoughthrombocytopenia is a risk factor of bleeding indengue thrombocytopenia alone was notassociated with bleeding in the absence of plasmaleakage Many abnormalities in the coagulationpathways are seen in severe dengue which appearto return to normal during the recovery phaseThese coagulation abnormalities have beenassociated with the degree of plasma leakage As
References
1 Bhatt S Gething PW Brady OJ Messina JP FarlowAW Moyes CL et al The global distribution andburden of dengue Nature 2013 496(7446) 504-7Epub 20130409 doi 101038nature12060 PubMedPMID 23563266 PubMed Central PMCIDPMC3651993
2 Mortality GBD Causes of Death C Global regionaland national life expectancy all-cause mortality andcause-specific mortality for 249 causes of death1980-2015 a systematic analysis for the GlobalBurden of Disease Study 2015 Lancet 2016388(10053) 1459-544 doi 101016S0140-6736(16)31012-1 PubMed PMID 27733281
3 Rouvinski A Guardado-Calvo P Barba-Spaeth GDuquerroy S Vaney MC Kikuti CM et al Recognitiondeterminants of broadly neutralizing humanantibodies against dengue viruses Nature 2015520(7545) 109-13 doi 101038nature14130PubMed PMID 25581790
4 Soo KM Khalid B Ching SM Chee HY Meta-Analysisof Dengue Severity during Infection by DifferentDengue Virus Serotypes in Primary and SecondaryInfections PloS one 2016 11(5) e0154760doi 101371journalpone02154760 PubMed PMID27213782 PubMed Central PMCID PMCPMC4877104
5 Malavige GN Ogg GS Pathogenesis of vascular leakin dengue virus infection Immunology 2017 151(3)261-9 doi 101111imm12748 PubMed PMID28437586 PubMed Central PMCID PMCPMC5461104
Authorship
Contribution This is the sole work of ProfGathsaurie Neelika Malavige
Conflict-of-interest disclosure The author declaresno conflict of interest
Correspondence Prof Gathsaurie Neelika MalavigeDPhil FRCP (Lond) FRCPath (UK)Centre for Dengue Research Faculty of MedicalSciences University of Sri Jayawardanapura SriLanka
E-mail gathsauriemalavigendmoxacuk
bleeding manifestations appear to best correlatewith the degree of leakage proper and meticulousfluid management would be the most importantmeasure in preventing bleeding manifestations
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 9
6 Md-Sani SS Md-Noor J Han WH Gan SP Rani NS TanHL et al Prediction of mortality in severe denguecases BMC infectious diseases 2018 18(1) 232 doi101186s12879-018-3141-6 PubMed PMID29783955
7 Pinto RC Castro DB Albuquerque BC Sampaio Vde SPassos RA Costa CF et al Mortality Predictors inPatients with Severe Dengue in the State of AmazonasBrazil PloS one 2016 11(8)e0161884 doi 101371journalpone0161884 PubMed PMID 27564084PubMed Central PMCID PMCPMC5001629
8 Sam SS Omar SF Teoh BT Abd-Jamil J AbuBakar SReview of Dengue hemorrhagic fever fatal cases seenamong adults a retrospective study PLoS neglectedtropical diseases 2013 7(5)e2194 doi 101371journalpntd0002194 PubMed PMID 23658849PubMed Central PMCID PMCPMC3642057
9 Wills BA Oragui EE Stephens AC Daramola OA DungNM Loan HT et al Coagulation abnormalities indengue hemorrhagic Fever serial investigations in167 Vietnamese children with Dengue shocksyndrome Clin Infect Dis 2002 35(3) 277-85 Epub20020713 doi 101086341410 PubMed PMID12115093
10 WHO editor Comprehensive guidelines forprevention and control of dengue fever and denguehaemorrhagic fever SEARO New Delhi India WorldHealth Organization 2011
11 Malavige GN Velathanthiri VG Wijewickrama ESFernando S Jayaratne SD Aaskov J et al Patterns ofdisease among adults hospitalized with dengueinfections Qjm 2006 99(5) 299-305 PubMed PMID16603571
12 Wijewickrama A FS Jayerathne PGSB Perera MAPAAbeynaike SA Gomes L Jeewandara C Malavige GNEffect of change in serotype on clinical severity ofdengue infections In SLMA editor Annual Con-ference of the Sri Lanka Medical AssociationColombo SLMA 2017
13 Wong JG Thein TL Leo YS Pang J Lye DC IdentifyingAdult Dengue Patients at Low Risk for ClinicallySignificant Bleeding PloS one 2016 11(2) e0148579doi 101371journalpone0148579 PubMed PMID26849556 PubMed Central PMCID PMCPMC4743958
14 Ojha A Nandi D Batra H Singhal R Annarapu GKBhattacharyya S et al Platelet activation determinesthe severity of thrombocytopenia in dengue infectionSci Rep 2017 7 41697 doi 101038srep41697PubMed PMID 28139770 PubMed Central PMCIDPMCPMC5282509
15 Isarangkura P Tuchinda S The behavior of transfused
platelets in dengue hemorrhagic fever The SoutheastAsian Journal of Tropical Medicine and Public Health1993 24 Suppl 1 222-4 PubMed PMID 7886581
16 Lum LC Abdel-Latif Mel A Goh AY Chan PW Lam SKPreventive transfusion in Dengue shock syndrome-is it necessary The Journal of Pediatrics 2003143(5) 682-4 PubMed PMID 14615749
17 Lye DC Lee VJ Sun Y Leo YS Lack of efficacy ofprophylactic platelet transfusion for severethrombocytopenia in adults with acute uncom-plicated dengue infection Clin Infect Dis 2009 48(9)1262-5 PubMed PMID 19292665
18 Lye DC Archuleta S Syed-Omar SF Low JG Oh HMWei Y et al Prophylactic platelet transfusion plussupportive care versus supportive care alone inadults with dengue and thrombocytopenia amulticentre open-label randomised superioritytrial Lancet 2017 389(10079) 1611-8 doi 101016S0140-6736(17)30269-6 PubMed PMID 28283286
19 Chinnappan S Ramachandrappa VS Tamilarasu KKrishnan UM Pillai AK Rajendiran S Inhibition ofPlatelet Aggregation by the Leaf Extract of Caricapapaya During Dengue Infection An In Vitro StudyViral immunology 2016 29(3) 164-8 doi 101089vim20150083 PubMed PMID 26910599
20 Charan J Saxena D Goyal JP Yasobant S Efficacyand safety of Carica papaya leaf extract in thedengue A systematic review and meta-analysis Int JAppl Basic Med Res 2016 6(4)249-54 doi 1041032229-516X192596 PubMed PMID 27857891PubMed Central PMCID PMCPMC5108100
21 Laoprasopwattana K Binsaai J Pruekprasert PGeater A Prothrombin Time Prolongation was theMost Important Indicator of Severe Bleeding inChildren with Severe Dengue Viral Infection Journalof Tropical Pediatrics 2017 63(4)314-20 doi101093tropejfmw097 PubMed PMID 28177091
22 Sureshkumar VK Vijayan D Kunhu S Mohamed ZThomas S Raman M Thromboelastographic Analysisof Hemostatic Abnormalities in Dengue PatientsAdmitted in a Multidisciplinary Intensive Care UnitA Cross-sectional Study Indian J Crit Care Med 201822(4)238-42 doi 104103ijccmIJCCM_486_17PubMed PMID 29743762 PubMed Central PMCIDPMCPMC5930527
23 Chuansumrit A Chaiyaratana W Hemostaticderangement in dengue hemorrhagic feverThrombosis Research 2014 133(1)10-6 doi101016jthromres201309028 PubMed PMID24120237
24 Wills B Tran VN Nguyen TH Truong TT Tran TN
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
Editor Dr H W Chandima K KulathilakeMBBS DipPath MD(Haematology)
Editorial Committee Dr Senani WilliamsMBBS DipPath MD(Haematology) FRCPath(Haematology)
Dr Manal RathnayakeMBBS DipPath MD(Haematology)
Dr Durga MoratuwagamaMBBS DipPath MD(Haematology) FRCPath(Haematology)
The Sri Lanka Journal of Haematology
The Sri Lanka College of Haematologists
No 6 Wijerama House Phone 0112685088
Wijerama Mawatha Fax 0112685088
Colombo 7 E-mail slcohaemgmailcom
Printed by
Ananda Press277 Hokandara RoadThalawathugoda
E-mail anandapress65gmailcom
Volume 10 Issue 1 September 2018
ISSN 1391-7919
The Sri Lanka Journal of Haematology 1
HWCK Kulathilake SLJH 2018 10(1) 1-4
The only oral anticoagulant available in clinicalpractice for more than five decades has beenwarfarin a vitamin K antagonist (VKA) Despite itseffectiveness and feasibility for long term use ithas several short comings Warfarin has a variabledose response a narrow therapeutic index andnumerous drug and dietary interactions thatrequire frequent monitoring by the internationalnormalized ratio (INR) to ensure an adequate yetsafe dose1
These shortcomings have prompted the develop-ment of direct acting oral anticoagulants (DOACs)that directly act on coagulation factors such asfactors Xa and IIa (thrombin) From 2008 regulatoryagencies in EU and US have approved severalDOACs for specific indications based on the resultsobtained in clinical trials demonstrating efficacyand safety that are at least non-inferior if notsuperior compared to warfarin and heparins forstroke prevention in atrial fibrillation (AF) as wellas for treatment and prophylaxis of venous throm-boembolism (VTE)2
DOACs used in clinical practice at present includedabigatran rivaroxaban apixaban and edoxabanThese agents offer major pharmacological advan-tages over warfarin such as rapid onset of actionminimal drug or dietary interactions and predic-table pharmacokinetics which eliminates therequirement for regular coagulation monitoring12
DOACs can be divided into two broad classes (i)Direct thrombin inhibitors (dabigatran) which
Direct oral anticoagulants Are we aware of their efficacy and safety
Editorial
HWCK Kulathilake1
1Senior LecturerConsultant HaematologistDepartment of Pathology Faculty of MedicalSciences University of Sri Jayewardenepura SriLanka
Correspondence chandimawarawitayahoocouk
SLJH 2018 10(1) 1-4
inhibit thrombin (Factor IIa) and (ii) Factor Xainhibitors (rivaroxaban apixaban edoxaban)which inhibit factor Xa Apixaban rivaroxaban anddabigatran will be discussed in this review
Apixaban is approved for use in the prevention ofstroke and systemic embolism in adult patientswith nonvalvular AF and in the primary preventionof VTE in adult patients who have undergoneelective total hip arthroplasty (THA) or total kneearthroplasty (TKA)3
The efficacy and safety of apixaban have beenevaluated in phase 3 clinical trials The use ofapixaban in postoperative VTE Prophylaxis for TKAwas evaluated in (ADVANCE)-14 and ADVANCE-25
trials All the treatments in either arm of the 2trials (apixaban vs enoxaparin) were continued for10 to 14 days In ADVANCE-3 trial6 both drugs werecontinued for 35 days after THA Primary efficacy(symptomatic or asymptomatic VTE non fatal PEdeath) was similar in both drugs in ADVANCE-1and apixaban was superior to enoxaparin inADVANCE-2 and 3 trails The combined incidenceof major bleeding and clinically relevant non majorbleeding was less with apixaban use comparedwith enoxaparin use in ADVANCE-1 but equivalentin ADVANCE-2 and 3 trials
Apixaban was evaluated in the prevention ofstroke and systemic embolism in nonvalvular AFin 2 large randomized controlled trials apixabanversus aspirin to prevent stroke in atrial fibril-lation patients who have failed or are unsuitablefor Vitamink Antagonist Treatment (AVERROES)trial 7 and the Apixaban for Reduction in Strokeand Other Thromboembolic Events in AtrialFibrillation (ARISTOTLE)8
In both trials the primary efficacy outcome (strokeor systemic embolism) was superior with apixabanThe rate of major bleeding per year was less withapixaban compared with warfarin in ARISTOTLE
Key words warfarin direct oral anticoagulants clinical trials
The Sri Lanka Journal of Haematology2
HWCK Kulathilake SLJH 2018 10(1) 1-4
Rivaroxaban is approved for use in the primaryprevention of VTE in adult patients who haveundergone elective THA or TKA in nonvalvular AFin the treatment of DVT and PE and to reduce therisk of recurrent DVT and PE after initial treatment3
The efficacy and safety of rivaroxaban have beenevaluated in phase 3 clinical trials in differentclinical situations The Regulation of Coagulationin Orthopedic Surgery to Prevent Deep VenousThrombosis and Pulmonary Embolism (RECORD)1234 trials9101112 compared rivaroxaban withenoxaparin in Postoperative VTE Prophylaxis forjoint replacement surgery (THA and TKA) Riva-roxaban significantly reduced the total event ratecompared with enoxaparin in all four trials andthere was no difference in the incidence of majorbleeding between the rivoroxaban and enoxa-parin arms On the basis of these results riva-roxaban was approved in Europe and Canada forthe prevention of VTE in patients undergoingelective hip or knee arthroplasty
The EINSTEIN study 13 compared oral rivaroxabanwith enoxaparin followed by a VKA for 3 6 or 12months in patients with acute symptomatic DVT(initial treatment study) A parallel double blindrandomized study compared rivaroxaban withplacebo for an additional 6 or 12 months in patientswho had completed 6 to 12 months of treatment forVTE (continued-treatment study) The EINSTEIN-PE14 was a similar study that evaluated the samedose of rivaroxaban vs enoxaparinVKA in patientswith an acute symptomatic PE with or without DVT
In EINSTEIN rivaroxaban therapy was noninferiorto enoxaparinVKA therapy with regard to recurrentVTE (21 vs 30 Plt001) In the continued-treatment study rivaroxaban therapy was superiorto placebo use with regard to recurrent VTE (13vs 71 Plt001) The rates of symptomatic recur-rent VTE in the EINSTEIN-PE study were similarbetween the rivaroxaban and enoxaparinVKAgroups In both EINSTEIN and EINSTEIN-PE thesafety outcome of major or clinically relevant nonmajor bleeding were similar in both treatmentarms
The Rivaroxaban Once Daily Oral Direct Factor XaInhibition Compared with Vitamin K Antagonismfor Prevention of Stroke and Embolism Trial in AtrialFibril lation (ROCKET AF) study1516 evaluated
rivaroxaban for prevention of stroke or systemicembolization in patients with nonvalvular AF(intermediate to high risk of stroke) Patients wererandomly divided to receive either rivaroxaban 20mgday or warfarin (target INR 20-30) and thepatients were monitored for 24 months Riva-roxaban was non inferior to warfarin (21 vs 24per year Plt001 for noninferiority) in the primaryefficacy outcome of stroke and systemic embolismThere was no difference between patients takingrivaroxaban and those taking warfarin in terms ofall bleeding events
Dabigatran is approved for use in nonvalvular atrialfibrillation and in the primary prevention of venousthromboembolic events (VTEs) in adult patients withelective total hip (THA) or knee (TKA) arthroplastyDabigatran has been evaluated in several phase 3clinical trials to assess its safety and efficacy indifferent clinical situations
The RE-LY (Randomized Evaluation of Long-termAnticoagulant Therapy Warfarin compared withDabigatran) study1718 evaluated the efficacy andsafety of dabigatran at 110 or 150 mg twice dailycompared with dose-adjusted warfarin targetingan INR of 2 to 3 in patients with nonvalvular AF andan intermediate risk of thromboembolism Bothdoses of dabigatran were non-inferior to warfarinwhile the higher dose proved to be superior forthe primary outcome The major bleeding occurredat a rate of 311 271 and 336 year for thepatients treated with dabigatran 150 mg dabi-gatran 110 mg and warfarin respectively Thedifferences in both the efficacy and safety out-comes were statistically significant
The RE-COVER study19 evaluated patients withacute VTE for a period of 06 months The 6-monthincidence of recurrent symptomatic VTE andrelated deaths was 24 in patients treated withdabigatran vs 21 in those treated with warfarin(Plt001 for noninferiority) The rates of majorbleeding episodes were similar in both groups
Dabigatran in postoperative VTE prophylaxis forjoint replacement sugery was evaluated in theEuropean RE-MODEL study North American RE-MOBILIZE study the European RE-NOVATE (I) andthe North American RE-NOVATE (II) studies Therewere conflicting results between the first 2 trialsin postop TKA In RE-MODEL20 the incidence of VTE
The Sri Lanka Journal of Haematology 3
HWCK Kulathilake SLJH 2018 10(1) 1-4
or mortality was 377 in the enoxaparin armcompared with 364 in the dabigatran 220-mgarm (P=0003 for noninferiority) and 405 in thedabigatran 150-mg arm (P=017 for non-inferio-rity) However in RE-MOBILIZE21 the compositeof VTE and death occurred in 253 of those in theenoxaparin arm compared with 311 of those inthe dabigatran 220-mg arm (P=02) and 337 ofthose in the dabigatran 150-mg arm (Plt001) Thedifferences in efficacy between the 2 trials maybe due to the different dosing schedules ofenoxaparin So dabigatran may not be an equallyefficacious prophylaxis option in this settingAmong the 3 arms the incidence of major bleedingdid not differ significantly in the 02 trials
The RE-NOVATE I and II studies2223 evaluateddabigatran in preventing VTE after THA comparedwith enoxaparin In RE-NOVATE I the findingsconfirmed noninferiority for dabigatran (Plt0001for noninferiority) Furthermore RE-NOVATE IIdetected total VTE and death in 77 in thedabigatran 220-mg arm vs 88 in the enoxaparinarm (P=43) In both RE-NOVATE studies there wasno difference in major bleeding rates with eitherdose of dabigatran compared with enoxaparin
Since the introduction of DOACs in 2008 the globalanticoagulant market shows that warfarin use hasdeclined from 875 to 72 through 2008 to 2014while DOACs have shown an upward trend with amarket share of 155 as of 20142 The questionof whether these agents will replace warfarin andheparins which have been accepted as the goldstandard during all these years is one that needsto be answered after a thorough evaluation ofseveral aspects including high cost of DOACs lackof specific antidotes and lack of long-term safetydata
References
1 Galanis T Thomson L Palladino M et al J ThrombThrombolysis 2011 31 310 httpsdoiorg101007s11239-011-0559-8 PMid21327511
2 Oktay E Will NOACs become the new standard ofcare in anticoagulation therapy InternationalJournal of the Cardiovascular Academy 1 2015 1-4httpsdoiorg101016jijcac201506007
3 Wilson I Gonsalves Rajiv K Pruthi Mrinal MPatnaik The New Oral Anticoagulants in ClinicalPractice Mayo Clin Proc 2013 88(5) 495-511
httpsdoiorg101016jmayocp201303006PMid23639500
4 Lassen MR Raskob GE Gallus A Pineo G Chen DPortman RJ Apixaban or enoxaparin for thrombo-prophylaxis after knee replacement N Engl J Med2009 361(6) 594-604 httpsdoiorg101056NEJMoa0810773 PMid19657123
5 Lassen MR Raskob GE Gallus A Pineo G Chen DHornick P Apixaban versus enoxaparin for thrombo-prophylaxis after knee replacement (ADVANCE-2) arandomised double-blind trial Lancet 2010375(9717) 807-15 httpsdoiorg101016S0140-6736(09)62125-5
6 Lassen MR Gallus A Raskob GE Pineo G Chen DRamirez LM Apixaban versus enoxaparin forthromboprophylaxis after hip replacement N Engl JMed 2010 363(26) 2487-98 httpsdoiorg101056NEJMoa1006885 PMid21175312
7 Connolly SJ Eikelboom J Joyner C et al Apixaban inpatients with atrial fibrillation N Engl J Med 2011364(9) 806-17 httpsdoiorg101056NEJMoa1007432 PMid21309657
8 Granger CB Alexander JH McMurray JJ et alApixaban versus warfarin in patients with atrialfibrillation N Engl J Med 2011 365(11) 981-92h tt p s d o i o rg 10 1056 N E JM o a 1107039PMid21870978
9 Eriksson BI Borris LC Friedman RJ et alRivaroxaban versus enoxaparin for thrombo-prophylaxis after hip arthroplasty N Engl J Med2008 358(26) 2765-75 httpsdoiorg101056NEJMoa0800374 PMid18579811
10 Kakkar AK Brenner B Dahl OE et al Extended durationrivaroxaban versus short-term enoxaparin for theprevention of venous thromboembolism after totalhip arthroplasty a double-blind randomisedcontrolled trial Lancet 2008 372(9632) 31-9 httpsdoiorg101016S0140-6736(08)60880-6
11 Lassen MR Ageno W Borris LC et al Rivaroxabanversus enoxaparin for thromboprophylaxis aftertotal knee arthroplasty N Engl J Med 2008 358(26)2776-86 httpsdoiorg101056NEJMoa076016PMid18579812
12 Turpie AGG Lassen MR Davidson BL et al Riva-roxaban versus enoxaparin for thromboprophylaxisafter total knee arthroplasty (RECORD4) arandomised trial Lancet 2009 373(9676) 1673-80httpsdoiorg101016S0140-6736(09)60734-0
13 Bauersachs R Berkowitz SD Brenner B et al Oralrivaroxaban for symptomatic venous thrombo-embolism N Engl J Med 2010 363(26) 2499-510h tt p s d o i o rg 10 1056 N E JM o a 1007903PMid21128814
The Sri Lanka Journal of Haematology4
HWCK Kulathilake SLJH 2018 10(1) 1-4
14 Buller HR Prins MH Lensin AW et al Oral riva-roxaban for the treatment of symptomatic pulmonaryembolism N Engl J Med 2012 366(14) 1287-97httpsdoiorg101056NEJMoa1113572PMid22449293
15 Patel MR Mahaffey KW Garg J et al Rivaroxabanversus warfarin in nonvalvular atrial fibrillation NEngl J Med 2011 365(10) 883-891 httpsdoiorg101056NEJMoa1009638 PMid21830957
16 Fox KA Piccini JP Wojdyla D et al Prevention ofstroke and systemic embolism with rivaroxabancompared with warfarin in patients with nonvalvularatrial fibrillation and moderate renal impairmentEur Heart J 2011 32(19) 2387-94 httpsdoiorg101093eurheartjehr342 PMid21873708
17 Connolly SJ Ezekowitz MD Yusuf S et al Dabigatranversus warfarin in patients with atrial fibrillationN Engl J Med 2009 361(12) 1139-51 httpsdoiorg101056NEJMoa0905561 PMid19717844
18 Wallentin L Yusuf S Ezekowitz MD et al Efficacyand safety of dabigatran compared with warfarin atdifferent levels of international normalised ratiocontrol for stroke prevention in atrial fibrillationan analysis of the RE-LY trial Lancet 2010 376(9745)975-83httpsdoi org101016S0140-6736(10)61194-4
19 Schulman S Kearon C Kakkar AK et al Dabigatranversus warfarin in the treatment of acute venous
thromboembolism N Engl J Med 2009 361(24)2342-52 httpsdoiorg101056NEJMoa0906598PMid19966341
20 Eriksson BI Dahl OE Rosencher N et al Oraldabigatran etexilate vs subcutaneous enoxaparinfor the prevention of venous thromboembolism aftertotal knee replacement the REMODEL randomizedtrial J Thromb Haemost 2007 5(11) 2178-85httpsdoiorg101111j1538-7836200702748xPMid 17764540
21 Ginsberg JS Davidson BL Comp PC et al Oralthrombin inhibitor dabigatran etexilate vs NorthAmerican enoxaparin regimen for prevention ofvenous thromboembolism after knee arthroplastysurgery J Arthroplast 2009 24(1) 1-9 httpsdoiorg101016jarth200801132 PMid18534438
22 Eriksson BI Dahl OE Rosencher N et al Dabigatranetexilate versus enoxaparin for prevention of venousthromboembolism after total hip replacement arandomised double-blind non inferiority trialLancet 2007 370(9591) 949-56 httpsdoiorg101016S0140-6736(07)61445-7
23 Eriksson BI Dahl OE Huo MH et al Oral dabigatranversus enoxaparin for thromboprophylaxis afterprimary total hip arthroplasty (RE-NOVATE II) arandomised double blind non nferiority trialThromb Haemost 2011 105(4)721-9 httpsdoiorg101160TH10-10-0679 PMid21225098
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 5
1Professor Centre for Dengue Research Universityof Sri Jayewardenepura Nugegoda Sri Lanka2Weatherall Institute of Molecular Medicine JohnRadcliffe Hospital Oxford OX3 9DS UK
Introduction
Dengue viral infections represent one of the mostrapidly emerging mosquito borne infections in theworld which causes 100 million apparent dengueinfections each year1 From 2005 to 2015 althoughthe mortality rates due to many infectious diseasesdecreased the deaths due to dengue increasedby 487 resulting in an estimated 18400 deathsin 20152 Although there is a dengue vaccine licensedto be used in children over the age of 9 years thevaccine manufacturer and other authorities havesuggested that this vaccine should be avoided inindividuals who have not been infected with thedengue virus (DENV) due to the likelihood ofdisease enhancement3
Although the majority of those who are infectedwith the DENV develop asymptomatic or milddisease 478 to 5072 of individuals have shownto develop severe dengue depending on the epi-demic serostatus and circulating DENV serotypesduring that epidemic4 Severe dengue is charac-terized by clinically detectable vascular leakagethat manifest in the form of pleural effusions andascites which can lead to haemodynamic insta-bility and shock5 In addition patients may alsodevelop complications such as bleeding mani-festations liver and renal dysfunction Althoughmild forms of bleeding manifestations such aspetechiae and bleeding from sites of venipunctureare seen in many patients with dengue haemor-rhagic fever (DHF) significant bleeding such as pervaginal bleeding haematuria haematemesis and
Predictors of bleeding in acute dengue virus infection
Gathsaurie Neelika Malavige12
Leading article
Key words dengue viral infection bleeding plasma leakage
malena can lead to haemodynamic instability andshock Development of significant bleeding wasshown to be an independent risk factor associatedwith fatalities in patients with DHF6 Gastrointestinalbleeding alone was shown to strongly associatewith the occurrence of death7
Association of plasma leakage and bleeding
While bleeding manifestations are sometimesseen in patients with dengue fever (DF) significantbleeding is usually seen in those who have severeplasma leakage prolonged shock or organ dys-function89 Severe vascular leakage leading to poorperfusion of the intestinal mucosa and organdysfunction are thought to be the predominantcauses of intestinal bleeding10 Our data has shownthat bleeding manifestations were more frequentamong dengue patients in Sri Lanka in the pastcompared to recent epidemics possibly due tobetter fluid management and reduction in thedevelopment of shock For instance in a study doneby us in year 2004 in adult patients 42108 (389)patients developed bleeding manifestations11whereas the only 26179 (145) developedbleeding manifestations in a patient cohortstudied in years 2016 and 201712 Therefore bettermanagement of fluid leakage appears to indirectlyreduce the incidence of bleeding in dengue
Thrombocytopenia and occurrence of bleeding
Although severe thrombocytopenia was found tobe a predictor of significant bleeding in denguethrombocytopenia alone in the absence of a highhematocrit or liver dysfunction was not associatedwith significant bleeding13 Direct infection ofplatelets by the DENV destruction of platelets dueto immune complexes and bone marrow sup-pression have shown to be the predominant factorsleading to thrombocytopenia (Figure 1)14 Apartfrom the reduction of platelet counts platelet
SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
6
function has also shown to be significantlyimpaired in patients with DHF including impairedplatelet aggregation in response to ADP9 This wasshown to be accompanied by an increase in plasma-thrombomodulin and platelet factor-4 whichindicate an increased secretory activity9 Impairedplatelet function and destruction has also beenobserved in transfused platelets which have ledto a marked reduction in survival rates of trans-fused platelets especially in those with DHF1415
Due to the presence of severe degrees of throm-bocytopenia in the past many centres have pro-phylactically transfused platelets in order toprevent development of any bleeding Howeverseveral retrospective studies had shown thatprophylactic platelet transfusions were associatedwith fluid overload and prolonged hospital staywithout any reduction in bleeding manifestationsor improved platelet recovery1617 In order toaddress this controversy a multi centre rando-mized controlled trial carried out in several centresin Singapore and Malaysia in patients with plateletcounts 20000 plateletsmicroL showed that pro-phylactic platelet transfusions did not reduce theoccurrence of bleeding18 Instead platelet trans-fusions were associated with an increase incidenceof adverse effects including those of seriousnature such as anaphylaxis and transfusion relatedacute lung injury18 Therefore both the WHOguidelines and the National dengue managementguidelines do not recommend platelet trans-fusions but have advocated blood transfusions inthose who are suspected to have developedsignificant bleeding
The effect of many herbal preparations such as theleave extract of Carica papaya in improving plateletcounts have been studied and in vitro evidencehave shown that this leaf extract reduces plateletaggregation19 Two multi-centre randomizeddouble blind placebo controlled trials using Caricapapaya in India showed that this leaf extract doessignificantly increase platelet counts initiallyalthough there was no significant difference inplatelet counts 48 hours after administration ofthe leaf extract20 However these trials had notassessed the efficacy of this leaf extract onreducing plasma leakage organ dysfunction and
mortality and have not reported any adverseeffects as is indicated in the standard reporting ofclinical trials20 Therefore as it is difficult toascertain the other possible benefits or adverseeffects of this drug it would be important toconduct proper clinical trials according to theinternationally recommended guidelines
Coagulation abnormalities leading to bleeding
Apart from the presence of prolonged shocksevere liver dysfunction is suggested as one the mostimportant predictors of severe bleeding21 Manyclotting factors such as factor V VII VIII IX and Xfibrinogen protein C and S and antithrombin aresynthesized by the liver and low levels of theseproteins are seen in patients with acute dengueAlthough thromboelastographic studies have alsodemonstrated deficiency of coagulation factorsand abnormalities in platelet function the levelswere not associated with the degree of thrombo-cytopenia or liver dysfunction22
Many patients with DHF have a prolongedprothrombin time prolonged INR and activatedpartial thromboplastin time (aPTT) It is thoughtthat these abnormalities possibly occur due to thereduced production of these factors and alsoleakage of these proteins into extravascular spacesacross the dysfunctional endothelium92123 Prolon-gation of the prothrombin time has been shownto be an important predictor of occurrence ofbleeding in patients with severe plasma leakage21Although many studies have reported an increasein partial thromboplastin times and reduction infibrinogen concentrations9 change in these para-meters correlated with the extent of vascularleakage and not with bleeding24 More detailedstudies which have assessed changes of theseproteins at different stages of the illness haveshown that protein C S and antithrombin III levelswere significantly lower in patients with moresevere degrees of shock during the leakagephase However as these proteins returned tonormal levels following the leakage phase it hasbeen suggested that leakage of these proteinsinto extravascular tissues could be the mainfactor leading to low levels in patients with DHF(Figure 1)9
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 7
Endothelial activation and bleeding in dengue
Patients with more severe forms of dengue arealso shown to have high levels of tissue factorthrombomodulin and plasminogen activatorinhibitor type 1 (PAI-1) which have been attri-buted to endothelial platelet and monocyteactivation9 Endothelial activation and injury is alsoreflected by high levels of von Willebrand factor(vWF) especially in patients with severe shock23It was also shown that the number of circulatingendothelial cells and soluble thrombomodulinlevels were significantly higher in patients withprofound shock further supporting that endo-thelial injury occurs in severe dengue23 Thromo-bomodulin which is an integral membrane proteinexpressed on endothelial cells monocytes andcertain dendritic cells is cofactor in activation of
protein C Although soluble thrombomodulinlevels were markedly high in those with severeforms plasma leakage as protein C levels are lowthe contribution to these pathways in causingsevere dengue and bleeding is not certain
Despite significant derangements in prothrom-botic antithrombotic and fibrinolytic pathways asmost patients do not develop bleeding it issuggested that the combinations of many factorssuch tissue hypoxia acidosis along with thrombo-cytopenia are important co-factors Howeverplasma leakage secondary endothelial dysfunctionappears to be the most important factor leading toshock poor organ perfusion organ dysfunctionderangement of many coagulation pathways andbleeding510 We have identified that plateletactivating factor (PAF) significantly contributed to
Bleeding manifestations are thought to occur due to the complex interplay of many factors such asendothelial dysfunction liver dysfunction and thrombocytopenia Endothelial dysfunction leads to plasmaleakage and when severe leads to shock poor organ perfusion and tissue hypoxia Tissue hypoxia in thegastrointestinal and possibly the lung epithelium is thought to be the main contributing factors forbleeding from these sites Many clotting factors and antithrombic factors are also thought to extravasatein to the tissues leading to low levels of these in the plasma In addition liver dysfunction may also leadto reduction in the production of these factors
Figure 1 Factors that contribute to bleeding in acute dengue infection
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
8
vascular leakage in dengue25 In addition lipidmediators that oppose the action of PAF andprotect the endothelial barrier integrity such assphingosine-1-phosphate was found to bemarkedly low in patients with DHF especiallyduring the critical phase26
As plasma leakage appears to be the most impor-tant factor leading to all complications of dengueit would be reasonable to use drugs that preventor reduce vascular leakage as a suitable option toreduce severe dengue and associated compli-cations We have concluded a phase 2 randomizedplacebo controlled clinical trial in 183 patients atthe National Institute of Infectious Diseases SriLanka using a PAF receptor blocker known asrupatadine27 In this clinical trial we found thatrupatadine up to 40mg daily appeared safe andwell-tolerated in patients with acute dengue Inaddition patients given rupatadine had higherplatelet counts and lower aspartate-aminotrans-ferase levels during the critical phase and signifi-cantly smaller pleural effusions27 The develop-ment of significant bleeding manifestations suchas per vaginal bleeding and gastrointestinalbleeding was also lower in the group who receivedtreatment As the beneficial effects of this drugappeared to be greater when given early in theillness we are currently conducting another trialwhich is double blind randomized placebocontrolled trial in a larger cohort of patientsAlthough the initial trial showed promising resultsthese results should be interpreted with cautionuntil the same beneficial effects are seen in largertrials that we are currently carrying out
Summary
Endothelial dysfunction leading to plasma leakageappears to be the most important predictor ofoccurrence of bleeding in acute dengue Althoughthrombocytopenia is a risk factor of bleeding indengue thrombocytopenia alone was notassociated with bleeding in the absence of plasmaleakage Many abnormalities in the coagulationpathways are seen in severe dengue which appearto return to normal during the recovery phaseThese coagulation abnormalities have beenassociated with the degree of plasma leakage As
References
1 Bhatt S Gething PW Brady OJ Messina JP FarlowAW Moyes CL et al The global distribution andburden of dengue Nature 2013 496(7446) 504-7Epub 20130409 doi 101038nature12060 PubMedPMID 23563266 PubMed Central PMCIDPMC3651993
2 Mortality GBD Causes of Death C Global regionaland national life expectancy all-cause mortality andcause-specific mortality for 249 causes of death1980-2015 a systematic analysis for the GlobalBurden of Disease Study 2015 Lancet 2016388(10053) 1459-544 doi 101016S0140-6736(16)31012-1 PubMed PMID 27733281
3 Rouvinski A Guardado-Calvo P Barba-Spaeth GDuquerroy S Vaney MC Kikuti CM et al Recognitiondeterminants of broadly neutralizing humanantibodies against dengue viruses Nature 2015520(7545) 109-13 doi 101038nature14130PubMed PMID 25581790
4 Soo KM Khalid B Ching SM Chee HY Meta-Analysisof Dengue Severity during Infection by DifferentDengue Virus Serotypes in Primary and SecondaryInfections PloS one 2016 11(5) e0154760doi 101371journalpone02154760 PubMed PMID27213782 PubMed Central PMCID PMCPMC4877104
5 Malavige GN Ogg GS Pathogenesis of vascular leakin dengue virus infection Immunology 2017 151(3)261-9 doi 101111imm12748 PubMed PMID28437586 PubMed Central PMCID PMCPMC5461104
Authorship
Contribution This is the sole work of ProfGathsaurie Neelika Malavige
Conflict-of-interest disclosure The author declaresno conflict of interest
Correspondence Prof Gathsaurie Neelika MalavigeDPhil FRCP (Lond) FRCPath (UK)Centre for Dengue Research Faculty of MedicalSciences University of Sri Jayawardanapura SriLanka
E-mail gathsauriemalavigendmoxacuk
bleeding manifestations appear to best correlatewith the degree of leakage proper and meticulousfluid management would be the most importantmeasure in preventing bleeding manifestations
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 9
6 Md-Sani SS Md-Noor J Han WH Gan SP Rani NS TanHL et al Prediction of mortality in severe denguecases BMC infectious diseases 2018 18(1) 232 doi101186s12879-018-3141-6 PubMed PMID29783955
7 Pinto RC Castro DB Albuquerque BC Sampaio Vde SPassos RA Costa CF et al Mortality Predictors inPatients with Severe Dengue in the State of AmazonasBrazil PloS one 2016 11(8)e0161884 doi 101371journalpone0161884 PubMed PMID 27564084PubMed Central PMCID PMCPMC5001629
8 Sam SS Omar SF Teoh BT Abd-Jamil J AbuBakar SReview of Dengue hemorrhagic fever fatal cases seenamong adults a retrospective study PLoS neglectedtropical diseases 2013 7(5)e2194 doi 101371journalpntd0002194 PubMed PMID 23658849PubMed Central PMCID PMCPMC3642057
9 Wills BA Oragui EE Stephens AC Daramola OA DungNM Loan HT et al Coagulation abnormalities indengue hemorrhagic Fever serial investigations in167 Vietnamese children with Dengue shocksyndrome Clin Infect Dis 2002 35(3) 277-85 Epub20020713 doi 101086341410 PubMed PMID12115093
10 WHO editor Comprehensive guidelines forprevention and control of dengue fever and denguehaemorrhagic fever SEARO New Delhi India WorldHealth Organization 2011
11 Malavige GN Velathanthiri VG Wijewickrama ESFernando S Jayaratne SD Aaskov J et al Patterns ofdisease among adults hospitalized with dengueinfections Qjm 2006 99(5) 299-305 PubMed PMID16603571
12 Wijewickrama A FS Jayerathne PGSB Perera MAPAAbeynaike SA Gomes L Jeewandara C Malavige GNEffect of change in serotype on clinical severity ofdengue infections In SLMA editor Annual Con-ference of the Sri Lanka Medical AssociationColombo SLMA 2017
13 Wong JG Thein TL Leo YS Pang J Lye DC IdentifyingAdult Dengue Patients at Low Risk for ClinicallySignificant Bleeding PloS one 2016 11(2) e0148579doi 101371journalpone0148579 PubMed PMID26849556 PubMed Central PMCID PMCPMC4743958
14 Ojha A Nandi D Batra H Singhal R Annarapu GKBhattacharyya S et al Platelet activation determinesthe severity of thrombocytopenia in dengue infectionSci Rep 2017 7 41697 doi 101038srep41697PubMed PMID 28139770 PubMed Central PMCIDPMCPMC5282509
15 Isarangkura P Tuchinda S The behavior of transfused
platelets in dengue hemorrhagic fever The SoutheastAsian Journal of Tropical Medicine and Public Health1993 24 Suppl 1 222-4 PubMed PMID 7886581
16 Lum LC Abdel-Latif Mel A Goh AY Chan PW Lam SKPreventive transfusion in Dengue shock syndrome-is it necessary The Journal of Pediatrics 2003143(5) 682-4 PubMed PMID 14615749
17 Lye DC Lee VJ Sun Y Leo YS Lack of efficacy ofprophylactic platelet transfusion for severethrombocytopenia in adults with acute uncom-plicated dengue infection Clin Infect Dis 2009 48(9)1262-5 PubMed PMID 19292665
18 Lye DC Archuleta S Syed-Omar SF Low JG Oh HMWei Y et al Prophylactic platelet transfusion plussupportive care versus supportive care alone inadults with dengue and thrombocytopenia amulticentre open-label randomised superioritytrial Lancet 2017 389(10079) 1611-8 doi 101016S0140-6736(17)30269-6 PubMed PMID 28283286
19 Chinnappan S Ramachandrappa VS Tamilarasu KKrishnan UM Pillai AK Rajendiran S Inhibition ofPlatelet Aggregation by the Leaf Extract of Caricapapaya During Dengue Infection An In Vitro StudyViral immunology 2016 29(3) 164-8 doi 101089vim20150083 PubMed PMID 26910599
20 Charan J Saxena D Goyal JP Yasobant S Efficacyand safety of Carica papaya leaf extract in thedengue A systematic review and meta-analysis Int JAppl Basic Med Res 2016 6(4)249-54 doi 1041032229-516X192596 PubMed PMID 27857891PubMed Central PMCID PMCPMC5108100
21 Laoprasopwattana K Binsaai J Pruekprasert PGeater A Prothrombin Time Prolongation was theMost Important Indicator of Severe Bleeding inChildren with Severe Dengue Viral Infection Journalof Tropical Pediatrics 2017 63(4)314-20 doi101093tropejfmw097 PubMed PMID 28177091
22 Sureshkumar VK Vijayan D Kunhu S Mohamed ZThomas S Raman M Thromboelastographic Analysisof Hemostatic Abnormalities in Dengue PatientsAdmitted in a Multidisciplinary Intensive Care UnitA Cross-sectional Study Indian J Crit Care Med 201822(4)238-42 doi 104103ijccmIJCCM_486_17PubMed PMID 29743762 PubMed Central PMCIDPMCPMC5930527
23 Chuansumrit A Chaiyaratana W Hemostaticderangement in dengue hemorrhagic feverThrombosis Research 2014 133(1)10-6 doi101016jthromres201309028 PubMed PMID24120237
24 Wills B Tran VN Nguyen TH Truong TT Tran TN
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

The Sri Lanka Journal of Haematology 1
HWCK Kulathilake SLJH 2018 10(1) 1-4
The only oral anticoagulant available in clinicalpractice for more than five decades has beenwarfarin a vitamin K antagonist (VKA) Despite itseffectiveness and feasibility for long term use ithas several short comings Warfarin has a variabledose response a narrow therapeutic index andnumerous drug and dietary interactions thatrequire frequent monitoring by the internationalnormalized ratio (INR) to ensure an adequate yetsafe dose1
These shortcomings have prompted the develop-ment of direct acting oral anticoagulants (DOACs)that directly act on coagulation factors such asfactors Xa and IIa (thrombin) From 2008 regulatoryagencies in EU and US have approved severalDOACs for specific indications based on the resultsobtained in clinical trials demonstrating efficacyand safety that are at least non-inferior if notsuperior compared to warfarin and heparins forstroke prevention in atrial fibrillation (AF) as wellas for treatment and prophylaxis of venous throm-boembolism (VTE)2
DOACs used in clinical practice at present includedabigatran rivaroxaban apixaban and edoxabanThese agents offer major pharmacological advan-tages over warfarin such as rapid onset of actionminimal drug or dietary interactions and predic-table pharmacokinetics which eliminates therequirement for regular coagulation monitoring12
DOACs can be divided into two broad classes (i)Direct thrombin inhibitors (dabigatran) which
Direct oral anticoagulants Are we aware of their efficacy and safety
Editorial
HWCK Kulathilake1
1Senior LecturerConsultant HaematologistDepartment of Pathology Faculty of MedicalSciences University of Sri Jayewardenepura SriLanka
Correspondence chandimawarawitayahoocouk
SLJH 2018 10(1) 1-4
inhibit thrombin (Factor IIa) and (ii) Factor Xainhibitors (rivaroxaban apixaban edoxaban)which inhibit factor Xa Apixaban rivaroxaban anddabigatran will be discussed in this review
Apixaban is approved for use in the prevention ofstroke and systemic embolism in adult patientswith nonvalvular AF and in the primary preventionof VTE in adult patients who have undergoneelective total hip arthroplasty (THA) or total kneearthroplasty (TKA)3
The efficacy and safety of apixaban have beenevaluated in phase 3 clinical trials The use ofapixaban in postoperative VTE Prophylaxis for TKAwas evaluated in (ADVANCE)-14 and ADVANCE-25
trials All the treatments in either arm of the 2trials (apixaban vs enoxaparin) were continued for10 to 14 days In ADVANCE-3 trial6 both drugs werecontinued for 35 days after THA Primary efficacy(symptomatic or asymptomatic VTE non fatal PEdeath) was similar in both drugs in ADVANCE-1and apixaban was superior to enoxaparin inADVANCE-2 and 3 trails The combined incidenceof major bleeding and clinically relevant non majorbleeding was less with apixaban use comparedwith enoxaparin use in ADVANCE-1 but equivalentin ADVANCE-2 and 3 trials
Apixaban was evaluated in the prevention ofstroke and systemic embolism in nonvalvular AFin 2 large randomized controlled trials apixabanversus aspirin to prevent stroke in atrial fibril-lation patients who have failed or are unsuitablefor Vitamink Antagonist Treatment (AVERROES)trial 7 and the Apixaban for Reduction in Strokeand Other Thromboembolic Events in AtrialFibrillation (ARISTOTLE)8
In both trials the primary efficacy outcome (strokeor systemic embolism) was superior with apixabanThe rate of major bleeding per year was less withapixaban compared with warfarin in ARISTOTLE
Key words warfarin direct oral anticoagulants clinical trials
The Sri Lanka Journal of Haematology2
HWCK Kulathilake SLJH 2018 10(1) 1-4
Rivaroxaban is approved for use in the primaryprevention of VTE in adult patients who haveundergone elective THA or TKA in nonvalvular AFin the treatment of DVT and PE and to reduce therisk of recurrent DVT and PE after initial treatment3
The efficacy and safety of rivaroxaban have beenevaluated in phase 3 clinical trials in differentclinical situations The Regulation of Coagulationin Orthopedic Surgery to Prevent Deep VenousThrombosis and Pulmonary Embolism (RECORD)1234 trials9101112 compared rivaroxaban withenoxaparin in Postoperative VTE Prophylaxis forjoint replacement surgery (THA and TKA) Riva-roxaban significantly reduced the total event ratecompared with enoxaparin in all four trials andthere was no difference in the incidence of majorbleeding between the rivoroxaban and enoxa-parin arms On the basis of these results riva-roxaban was approved in Europe and Canada forthe prevention of VTE in patients undergoingelective hip or knee arthroplasty
The EINSTEIN study 13 compared oral rivaroxabanwith enoxaparin followed by a VKA for 3 6 or 12months in patients with acute symptomatic DVT(initial treatment study) A parallel double blindrandomized study compared rivaroxaban withplacebo for an additional 6 or 12 months in patientswho had completed 6 to 12 months of treatment forVTE (continued-treatment study) The EINSTEIN-PE14 was a similar study that evaluated the samedose of rivaroxaban vs enoxaparinVKA in patientswith an acute symptomatic PE with or without DVT
In EINSTEIN rivaroxaban therapy was noninferiorto enoxaparinVKA therapy with regard to recurrentVTE (21 vs 30 Plt001) In the continued-treatment study rivaroxaban therapy was superiorto placebo use with regard to recurrent VTE (13vs 71 Plt001) The rates of symptomatic recur-rent VTE in the EINSTEIN-PE study were similarbetween the rivaroxaban and enoxaparinVKAgroups In both EINSTEIN and EINSTEIN-PE thesafety outcome of major or clinically relevant nonmajor bleeding were similar in both treatmentarms
The Rivaroxaban Once Daily Oral Direct Factor XaInhibition Compared with Vitamin K Antagonismfor Prevention of Stroke and Embolism Trial in AtrialFibril lation (ROCKET AF) study1516 evaluated
rivaroxaban for prevention of stroke or systemicembolization in patients with nonvalvular AF(intermediate to high risk of stroke) Patients wererandomly divided to receive either rivaroxaban 20mgday or warfarin (target INR 20-30) and thepatients were monitored for 24 months Riva-roxaban was non inferior to warfarin (21 vs 24per year Plt001 for noninferiority) in the primaryefficacy outcome of stroke and systemic embolismThere was no difference between patients takingrivaroxaban and those taking warfarin in terms ofall bleeding events
Dabigatran is approved for use in nonvalvular atrialfibrillation and in the primary prevention of venousthromboembolic events (VTEs) in adult patients withelective total hip (THA) or knee (TKA) arthroplastyDabigatran has been evaluated in several phase 3clinical trials to assess its safety and efficacy indifferent clinical situations
The RE-LY (Randomized Evaluation of Long-termAnticoagulant Therapy Warfarin compared withDabigatran) study1718 evaluated the efficacy andsafety of dabigatran at 110 or 150 mg twice dailycompared with dose-adjusted warfarin targetingan INR of 2 to 3 in patients with nonvalvular AF andan intermediate risk of thromboembolism Bothdoses of dabigatran were non-inferior to warfarinwhile the higher dose proved to be superior forthe primary outcome The major bleeding occurredat a rate of 311 271 and 336 year for thepatients treated with dabigatran 150 mg dabi-gatran 110 mg and warfarin respectively Thedifferences in both the efficacy and safety out-comes were statistically significant
The RE-COVER study19 evaluated patients withacute VTE for a period of 06 months The 6-monthincidence of recurrent symptomatic VTE andrelated deaths was 24 in patients treated withdabigatran vs 21 in those treated with warfarin(Plt001 for noninferiority) The rates of majorbleeding episodes were similar in both groups
Dabigatran in postoperative VTE prophylaxis forjoint replacement sugery was evaluated in theEuropean RE-MODEL study North American RE-MOBILIZE study the European RE-NOVATE (I) andthe North American RE-NOVATE (II) studies Therewere conflicting results between the first 2 trialsin postop TKA In RE-MODEL20 the incidence of VTE
The Sri Lanka Journal of Haematology 3
HWCK Kulathilake SLJH 2018 10(1) 1-4
or mortality was 377 in the enoxaparin armcompared with 364 in the dabigatran 220-mgarm (P=0003 for noninferiority) and 405 in thedabigatran 150-mg arm (P=017 for non-inferio-rity) However in RE-MOBILIZE21 the compositeof VTE and death occurred in 253 of those in theenoxaparin arm compared with 311 of those inthe dabigatran 220-mg arm (P=02) and 337 ofthose in the dabigatran 150-mg arm (Plt001) Thedifferences in efficacy between the 2 trials maybe due to the different dosing schedules ofenoxaparin So dabigatran may not be an equallyefficacious prophylaxis option in this settingAmong the 3 arms the incidence of major bleedingdid not differ significantly in the 02 trials
The RE-NOVATE I and II studies2223 evaluateddabigatran in preventing VTE after THA comparedwith enoxaparin In RE-NOVATE I the findingsconfirmed noninferiority for dabigatran (Plt0001for noninferiority) Furthermore RE-NOVATE IIdetected total VTE and death in 77 in thedabigatran 220-mg arm vs 88 in the enoxaparinarm (P=43) In both RE-NOVATE studies there wasno difference in major bleeding rates with eitherdose of dabigatran compared with enoxaparin
Since the introduction of DOACs in 2008 the globalanticoagulant market shows that warfarin use hasdeclined from 875 to 72 through 2008 to 2014while DOACs have shown an upward trend with amarket share of 155 as of 20142 The questionof whether these agents will replace warfarin andheparins which have been accepted as the goldstandard during all these years is one that needsto be answered after a thorough evaluation ofseveral aspects including high cost of DOACs lackof specific antidotes and lack of long-term safetydata
References
1 Galanis T Thomson L Palladino M et al J ThrombThrombolysis 2011 31 310 httpsdoiorg101007s11239-011-0559-8 PMid21327511
2 Oktay E Will NOACs become the new standard ofcare in anticoagulation therapy InternationalJournal of the Cardiovascular Academy 1 2015 1-4httpsdoiorg101016jijcac201506007
3 Wilson I Gonsalves Rajiv K Pruthi Mrinal MPatnaik The New Oral Anticoagulants in ClinicalPractice Mayo Clin Proc 2013 88(5) 495-511
httpsdoiorg101016jmayocp201303006PMid23639500
4 Lassen MR Raskob GE Gallus A Pineo G Chen DPortman RJ Apixaban or enoxaparin for thrombo-prophylaxis after knee replacement N Engl J Med2009 361(6) 594-604 httpsdoiorg101056NEJMoa0810773 PMid19657123
5 Lassen MR Raskob GE Gallus A Pineo G Chen DHornick P Apixaban versus enoxaparin for thrombo-prophylaxis after knee replacement (ADVANCE-2) arandomised double-blind trial Lancet 2010375(9717) 807-15 httpsdoiorg101016S0140-6736(09)62125-5
6 Lassen MR Gallus A Raskob GE Pineo G Chen DRamirez LM Apixaban versus enoxaparin forthromboprophylaxis after hip replacement N Engl JMed 2010 363(26) 2487-98 httpsdoiorg101056NEJMoa1006885 PMid21175312
7 Connolly SJ Eikelboom J Joyner C et al Apixaban inpatients with atrial fibrillation N Engl J Med 2011364(9) 806-17 httpsdoiorg101056NEJMoa1007432 PMid21309657
8 Granger CB Alexander JH McMurray JJ et alApixaban versus warfarin in patients with atrialfibrillation N Engl J Med 2011 365(11) 981-92h tt p s d o i o rg 10 1056 N E JM o a 1107039PMid21870978
9 Eriksson BI Borris LC Friedman RJ et alRivaroxaban versus enoxaparin for thrombo-prophylaxis after hip arthroplasty N Engl J Med2008 358(26) 2765-75 httpsdoiorg101056NEJMoa0800374 PMid18579811
10 Kakkar AK Brenner B Dahl OE et al Extended durationrivaroxaban versus short-term enoxaparin for theprevention of venous thromboembolism after totalhip arthroplasty a double-blind randomisedcontrolled trial Lancet 2008 372(9632) 31-9 httpsdoiorg101016S0140-6736(08)60880-6
11 Lassen MR Ageno W Borris LC et al Rivaroxabanversus enoxaparin for thromboprophylaxis aftertotal knee arthroplasty N Engl J Med 2008 358(26)2776-86 httpsdoiorg101056NEJMoa076016PMid18579812
12 Turpie AGG Lassen MR Davidson BL et al Riva-roxaban versus enoxaparin for thromboprophylaxisafter total knee arthroplasty (RECORD4) arandomised trial Lancet 2009 373(9676) 1673-80httpsdoiorg101016S0140-6736(09)60734-0
13 Bauersachs R Berkowitz SD Brenner B et al Oralrivaroxaban for symptomatic venous thrombo-embolism N Engl J Med 2010 363(26) 2499-510h tt p s d o i o rg 10 1056 N E JM o a 1007903PMid21128814
The Sri Lanka Journal of Haematology4
HWCK Kulathilake SLJH 2018 10(1) 1-4
14 Buller HR Prins MH Lensin AW et al Oral riva-roxaban for the treatment of symptomatic pulmonaryembolism N Engl J Med 2012 366(14) 1287-97httpsdoiorg101056NEJMoa1113572PMid22449293
15 Patel MR Mahaffey KW Garg J et al Rivaroxabanversus warfarin in nonvalvular atrial fibrillation NEngl J Med 2011 365(10) 883-891 httpsdoiorg101056NEJMoa1009638 PMid21830957
16 Fox KA Piccini JP Wojdyla D et al Prevention ofstroke and systemic embolism with rivaroxabancompared with warfarin in patients with nonvalvularatrial fibrillation and moderate renal impairmentEur Heart J 2011 32(19) 2387-94 httpsdoiorg101093eurheartjehr342 PMid21873708
17 Connolly SJ Ezekowitz MD Yusuf S et al Dabigatranversus warfarin in patients with atrial fibrillationN Engl J Med 2009 361(12) 1139-51 httpsdoiorg101056NEJMoa0905561 PMid19717844
18 Wallentin L Yusuf S Ezekowitz MD et al Efficacyand safety of dabigatran compared with warfarin atdifferent levels of international normalised ratiocontrol for stroke prevention in atrial fibrillationan analysis of the RE-LY trial Lancet 2010 376(9745)975-83httpsdoi org101016S0140-6736(10)61194-4
19 Schulman S Kearon C Kakkar AK et al Dabigatranversus warfarin in the treatment of acute venous
thromboembolism N Engl J Med 2009 361(24)2342-52 httpsdoiorg101056NEJMoa0906598PMid19966341
20 Eriksson BI Dahl OE Rosencher N et al Oraldabigatran etexilate vs subcutaneous enoxaparinfor the prevention of venous thromboembolism aftertotal knee replacement the REMODEL randomizedtrial J Thromb Haemost 2007 5(11) 2178-85httpsdoiorg101111j1538-7836200702748xPMid 17764540
21 Ginsberg JS Davidson BL Comp PC et al Oralthrombin inhibitor dabigatran etexilate vs NorthAmerican enoxaparin regimen for prevention ofvenous thromboembolism after knee arthroplastysurgery J Arthroplast 2009 24(1) 1-9 httpsdoiorg101016jarth200801132 PMid18534438
22 Eriksson BI Dahl OE Rosencher N et al Dabigatranetexilate versus enoxaparin for prevention of venousthromboembolism after total hip replacement arandomised double-blind non inferiority trialLancet 2007 370(9591) 949-56 httpsdoiorg101016S0140-6736(07)61445-7
23 Eriksson BI Dahl OE Huo MH et al Oral dabigatranversus enoxaparin for thromboprophylaxis afterprimary total hip arthroplasty (RE-NOVATE II) arandomised double blind non nferiority trialThromb Haemost 2011 105(4)721-9 httpsdoiorg101160TH10-10-0679 PMid21225098
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 5
1Professor Centre for Dengue Research Universityof Sri Jayewardenepura Nugegoda Sri Lanka2Weatherall Institute of Molecular Medicine JohnRadcliffe Hospital Oxford OX3 9DS UK
Introduction
Dengue viral infections represent one of the mostrapidly emerging mosquito borne infections in theworld which causes 100 million apparent dengueinfections each year1 From 2005 to 2015 althoughthe mortality rates due to many infectious diseasesdecreased the deaths due to dengue increasedby 487 resulting in an estimated 18400 deathsin 20152 Although there is a dengue vaccine licensedto be used in children over the age of 9 years thevaccine manufacturer and other authorities havesuggested that this vaccine should be avoided inindividuals who have not been infected with thedengue virus (DENV) due to the likelihood ofdisease enhancement3
Although the majority of those who are infectedwith the DENV develop asymptomatic or milddisease 478 to 5072 of individuals have shownto develop severe dengue depending on the epi-demic serostatus and circulating DENV serotypesduring that epidemic4 Severe dengue is charac-terized by clinically detectable vascular leakagethat manifest in the form of pleural effusions andascites which can lead to haemodynamic insta-bility and shock5 In addition patients may alsodevelop complications such as bleeding mani-festations liver and renal dysfunction Althoughmild forms of bleeding manifestations such aspetechiae and bleeding from sites of venipunctureare seen in many patients with dengue haemor-rhagic fever (DHF) significant bleeding such as pervaginal bleeding haematuria haematemesis and
Predictors of bleeding in acute dengue virus infection
Gathsaurie Neelika Malavige12
Leading article
Key words dengue viral infection bleeding plasma leakage
malena can lead to haemodynamic instability andshock Development of significant bleeding wasshown to be an independent risk factor associatedwith fatalities in patients with DHF6 Gastrointestinalbleeding alone was shown to strongly associatewith the occurrence of death7
Association of plasma leakage and bleeding
While bleeding manifestations are sometimesseen in patients with dengue fever (DF) significantbleeding is usually seen in those who have severeplasma leakage prolonged shock or organ dys-function89 Severe vascular leakage leading to poorperfusion of the intestinal mucosa and organdysfunction are thought to be the predominantcauses of intestinal bleeding10 Our data has shownthat bleeding manifestations were more frequentamong dengue patients in Sri Lanka in the pastcompared to recent epidemics possibly due tobetter fluid management and reduction in thedevelopment of shock For instance in a study doneby us in year 2004 in adult patients 42108 (389)patients developed bleeding manifestations11whereas the only 26179 (145) developedbleeding manifestations in a patient cohortstudied in years 2016 and 201712 Therefore bettermanagement of fluid leakage appears to indirectlyreduce the incidence of bleeding in dengue
Thrombocytopenia and occurrence of bleeding
Although severe thrombocytopenia was found tobe a predictor of significant bleeding in denguethrombocytopenia alone in the absence of a highhematocrit or liver dysfunction was not associatedwith significant bleeding13 Direct infection ofplatelets by the DENV destruction of platelets dueto immune complexes and bone marrow sup-pression have shown to be the predominant factorsleading to thrombocytopenia (Figure 1)14 Apartfrom the reduction of platelet counts platelet
SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
6
function has also shown to be significantlyimpaired in patients with DHF including impairedplatelet aggregation in response to ADP9 This wasshown to be accompanied by an increase in plasma-thrombomodulin and platelet factor-4 whichindicate an increased secretory activity9 Impairedplatelet function and destruction has also beenobserved in transfused platelets which have ledto a marked reduction in survival rates of trans-fused platelets especially in those with DHF1415
Due to the presence of severe degrees of throm-bocytopenia in the past many centres have pro-phylactically transfused platelets in order toprevent development of any bleeding Howeverseveral retrospective studies had shown thatprophylactic platelet transfusions were associatedwith fluid overload and prolonged hospital staywithout any reduction in bleeding manifestationsor improved platelet recovery1617 In order toaddress this controversy a multi centre rando-mized controlled trial carried out in several centresin Singapore and Malaysia in patients with plateletcounts 20000 plateletsmicroL showed that pro-phylactic platelet transfusions did not reduce theoccurrence of bleeding18 Instead platelet trans-fusions were associated with an increase incidenceof adverse effects including those of seriousnature such as anaphylaxis and transfusion relatedacute lung injury18 Therefore both the WHOguidelines and the National dengue managementguidelines do not recommend platelet trans-fusions but have advocated blood transfusions inthose who are suspected to have developedsignificant bleeding
The effect of many herbal preparations such as theleave extract of Carica papaya in improving plateletcounts have been studied and in vitro evidencehave shown that this leaf extract reduces plateletaggregation19 Two multi-centre randomizeddouble blind placebo controlled trials using Caricapapaya in India showed that this leaf extract doessignificantly increase platelet counts initiallyalthough there was no significant difference inplatelet counts 48 hours after administration ofthe leaf extract20 However these trials had notassessed the efficacy of this leaf extract onreducing plasma leakage organ dysfunction and
mortality and have not reported any adverseeffects as is indicated in the standard reporting ofclinical trials20 Therefore as it is difficult toascertain the other possible benefits or adverseeffects of this drug it would be important toconduct proper clinical trials according to theinternationally recommended guidelines
Coagulation abnormalities leading to bleeding
Apart from the presence of prolonged shocksevere liver dysfunction is suggested as one the mostimportant predictors of severe bleeding21 Manyclotting factors such as factor V VII VIII IX and Xfibrinogen protein C and S and antithrombin aresynthesized by the liver and low levels of theseproteins are seen in patients with acute dengueAlthough thromboelastographic studies have alsodemonstrated deficiency of coagulation factorsand abnormalities in platelet function the levelswere not associated with the degree of thrombo-cytopenia or liver dysfunction22
Many patients with DHF have a prolongedprothrombin time prolonged INR and activatedpartial thromboplastin time (aPTT) It is thoughtthat these abnormalities possibly occur due to thereduced production of these factors and alsoleakage of these proteins into extravascular spacesacross the dysfunctional endothelium92123 Prolon-gation of the prothrombin time has been shownto be an important predictor of occurrence ofbleeding in patients with severe plasma leakage21Although many studies have reported an increasein partial thromboplastin times and reduction infibrinogen concentrations9 change in these para-meters correlated with the extent of vascularleakage and not with bleeding24 More detailedstudies which have assessed changes of theseproteins at different stages of the illness haveshown that protein C S and antithrombin III levelswere significantly lower in patients with moresevere degrees of shock during the leakagephase However as these proteins returned tonormal levels following the leakage phase it hasbeen suggested that leakage of these proteinsinto extravascular tissues could be the mainfactor leading to low levels in patients with DHF(Figure 1)9
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 7
Endothelial activation and bleeding in dengue
Patients with more severe forms of dengue arealso shown to have high levels of tissue factorthrombomodulin and plasminogen activatorinhibitor type 1 (PAI-1) which have been attri-buted to endothelial platelet and monocyteactivation9 Endothelial activation and injury is alsoreflected by high levels of von Willebrand factor(vWF) especially in patients with severe shock23It was also shown that the number of circulatingendothelial cells and soluble thrombomodulinlevels were significantly higher in patients withprofound shock further supporting that endo-thelial injury occurs in severe dengue23 Thromo-bomodulin which is an integral membrane proteinexpressed on endothelial cells monocytes andcertain dendritic cells is cofactor in activation of
protein C Although soluble thrombomodulinlevels were markedly high in those with severeforms plasma leakage as protein C levels are lowthe contribution to these pathways in causingsevere dengue and bleeding is not certain
Despite significant derangements in prothrom-botic antithrombotic and fibrinolytic pathways asmost patients do not develop bleeding it issuggested that the combinations of many factorssuch tissue hypoxia acidosis along with thrombo-cytopenia are important co-factors Howeverplasma leakage secondary endothelial dysfunctionappears to be the most important factor leading toshock poor organ perfusion organ dysfunctionderangement of many coagulation pathways andbleeding510 We have identified that plateletactivating factor (PAF) significantly contributed to
Bleeding manifestations are thought to occur due to the complex interplay of many factors such asendothelial dysfunction liver dysfunction and thrombocytopenia Endothelial dysfunction leads to plasmaleakage and when severe leads to shock poor organ perfusion and tissue hypoxia Tissue hypoxia in thegastrointestinal and possibly the lung epithelium is thought to be the main contributing factors forbleeding from these sites Many clotting factors and antithrombic factors are also thought to extravasatein to the tissues leading to low levels of these in the plasma In addition liver dysfunction may also leadto reduction in the production of these factors
Figure 1 Factors that contribute to bleeding in acute dengue infection
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
8
vascular leakage in dengue25 In addition lipidmediators that oppose the action of PAF andprotect the endothelial barrier integrity such assphingosine-1-phosphate was found to bemarkedly low in patients with DHF especiallyduring the critical phase26
As plasma leakage appears to be the most impor-tant factor leading to all complications of dengueit would be reasonable to use drugs that preventor reduce vascular leakage as a suitable option toreduce severe dengue and associated compli-cations We have concluded a phase 2 randomizedplacebo controlled clinical trial in 183 patients atthe National Institute of Infectious Diseases SriLanka using a PAF receptor blocker known asrupatadine27 In this clinical trial we found thatrupatadine up to 40mg daily appeared safe andwell-tolerated in patients with acute dengue Inaddition patients given rupatadine had higherplatelet counts and lower aspartate-aminotrans-ferase levels during the critical phase and signifi-cantly smaller pleural effusions27 The develop-ment of significant bleeding manifestations suchas per vaginal bleeding and gastrointestinalbleeding was also lower in the group who receivedtreatment As the beneficial effects of this drugappeared to be greater when given early in theillness we are currently conducting another trialwhich is double blind randomized placebocontrolled trial in a larger cohort of patientsAlthough the initial trial showed promising resultsthese results should be interpreted with cautionuntil the same beneficial effects are seen in largertrials that we are currently carrying out
Summary
Endothelial dysfunction leading to plasma leakageappears to be the most important predictor ofoccurrence of bleeding in acute dengue Althoughthrombocytopenia is a risk factor of bleeding indengue thrombocytopenia alone was notassociated with bleeding in the absence of plasmaleakage Many abnormalities in the coagulationpathways are seen in severe dengue which appearto return to normal during the recovery phaseThese coagulation abnormalities have beenassociated with the degree of plasma leakage As
References
1 Bhatt S Gething PW Brady OJ Messina JP FarlowAW Moyes CL et al The global distribution andburden of dengue Nature 2013 496(7446) 504-7Epub 20130409 doi 101038nature12060 PubMedPMID 23563266 PubMed Central PMCIDPMC3651993
2 Mortality GBD Causes of Death C Global regionaland national life expectancy all-cause mortality andcause-specific mortality for 249 causes of death1980-2015 a systematic analysis for the GlobalBurden of Disease Study 2015 Lancet 2016388(10053) 1459-544 doi 101016S0140-6736(16)31012-1 PubMed PMID 27733281
3 Rouvinski A Guardado-Calvo P Barba-Spaeth GDuquerroy S Vaney MC Kikuti CM et al Recognitiondeterminants of broadly neutralizing humanantibodies against dengue viruses Nature 2015520(7545) 109-13 doi 101038nature14130PubMed PMID 25581790
4 Soo KM Khalid B Ching SM Chee HY Meta-Analysisof Dengue Severity during Infection by DifferentDengue Virus Serotypes in Primary and SecondaryInfections PloS one 2016 11(5) e0154760doi 101371journalpone02154760 PubMed PMID27213782 PubMed Central PMCID PMCPMC4877104
5 Malavige GN Ogg GS Pathogenesis of vascular leakin dengue virus infection Immunology 2017 151(3)261-9 doi 101111imm12748 PubMed PMID28437586 PubMed Central PMCID PMCPMC5461104
Authorship
Contribution This is the sole work of ProfGathsaurie Neelika Malavige
Conflict-of-interest disclosure The author declaresno conflict of interest
Correspondence Prof Gathsaurie Neelika MalavigeDPhil FRCP (Lond) FRCPath (UK)Centre for Dengue Research Faculty of MedicalSciences University of Sri Jayawardanapura SriLanka
E-mail gathsauriemalavigendmoxacuk
bleeding manifestations appear to best correlatewith the degree of leakage proper and meticulousfluid management would be the most importantmeasure in preventing bleeding manifestations
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 9
6 Md-Sani SS Md-Noor J Han WH Gan SP Rani NS TanHL et al Prediction of mortality in severe denguecases BMC infectious diseases 2018 18(1) 232 doi101186s12879-018-3141-6 PubMed PMID29783955
7 Pinto RC Castro DB Albuquerque BC Sampaio Vde SPassos RA Costa CF et al Mortality Predictors inPatients with Severe Dengue in the State of AmazonasBrazil PloS one 2016 11(8)e0161884 doi 101371journalpone0161884 PubMed PMID 27564084PubMed Central PMCID PMCPMC5001629
8 Sam SS Omar SF Teoh BT Abd-Jamil J AbuBakar SReview of Dengue hemorrhagic fever fatal cases seenamong adults a retrospective study PLoS neglectedtropical diseases 2013 7(5)e2194 doi 101371journalpntd0002194 PubMed PMID 23658849PubMed Central PMCID PMCPMC3642057
9 Wills BA Oragui EE Stephens AC Daramola OA DungNM Loan HT et al Coagulation abnormalities indengue hemorrhagic Fever serial investigations in167 Vietnamese children with Dengue shocksyndrome Clin Infect Dis 2002 35(3) 277-85 Epub20020713 doi 101086341410 PubMed PMID12115093
10 WHO editor Comprehensive guidelines forprevention and control of dengue fever and denguehaemorrhagic fever SEARO New Delhi India WorldHealth Organization 2011
11 Malavige GN Velathanthiri VG Wijewickrama ESFernando S Jayaratne SD Aaskov J et al Patterns ofdisease among adults hospitalized with dengueinfections Qjm 2006 99(5) 299-305 PubMed PMID16603571
12 Wijewickrama A FS Jayerathne PGSB Perera MAPAAbeynaike SA Gomes L Jeewandara C Malavige GNEffect of change in serotype on clinical severity ofdengue infections In SLMA editor Annual Con-ference of the Sri Lanka Medical AssociationColombo SLMA 2017
13 Wong JG Thein TL Leo YS Pang J Lye DC IdentifyingAdult Dengue Patients at Low Risk for ClinicallySignificant Bleeding PloS one 2016 11(2) e0148579doi 101371journalpone0148579 PubMed PMID26849556 PubMed Central PMCID PMCPMC4743958
14 Ojha A Nandi D Batra H Singhal R Annarapu GKBhattacharyya S et al Platelet activation determinesthe severity of thrombocytopenia in dengue infectionSci Rep 2017 7 41697 doi 101038srep41697PubMed PMID 28139770 PubMed Central PMCIDPMCPMC5282509
15 Isarangkura P Tuchinda S The behavior of transfused
platelets in dengue hemorrhagic fever The SoutheastAsian Journal of Tropical Medicine and Public Health1993 24 Suppl 1 222-4 PubMed PMID 7886581
16 Lum LC Abdel-Latif Mel A Goh AY Chan PW Lam SKPreventive transfusion in Dengue shock syndrome-is it necessary The Journal of Pediatrics 2003143(5) 682-4 PubMed PMID 14615749
17 Lye DC Lee VJ Sun Y Leo YS Lack of efficacy ofprophylactic platelet transfusion for severethrombocytopenia in adults with acute uncom-plicated dengue infection Clin Infect Dis 2009 48(9)1262-5 PubMed PMID 19292665
18 Lye DC Archuleta S Syed-Omar SF Low JG Oh HMWei Y et al Prophylactic platelet transfusion plussupportive care versus supportive care alone inadults with dengue and thrombocytopenia amulticentre open-label randomised superioritytrial Lancet 2017 389(10079) 1611-8 doi 101016S0140-6736(17)30269-6 PubMed PMID 28283286
19 Chinnappan S Ramachandrappa VS Tamilarasu KKrishnan UM Pillai AK Rajendiran S Inhibition ofPlatelet Aggregation by the Leaf Extract of Caricapapaya During Dengue Infection An In Vitro StudyViral immunology 2016 29(3) 164-8 doi 101089vim20150083 PubMed PMID 26910599
20 Charan J Saxena D Goyal JP Yasobant S Efficacyand safety of Carica papaya leaf extract in thedengue A systematic review and meta-analysis Int JAppl Basic Med Res 2016 6(4)249-54 doi 1041032229-516X192596 PubMed PMID 27857891PubMed Central PMCID PMCPMC5108100
21 Laoprasopwattana K Binsaai J Pruekprasert PGeater A Prothrombin Time Prolongation was theMost Important Indicator of Severe Bleeding inChildren with Severe Dengue Viral Infection Journalof Tropical Pediatrics 2017 63(4)314-20 doi101093tropejfmw097 PubMed PMID 28177091
22 Sureshkumar VK Vijayan D Kunhu S Mohamed ZThomas S Raman M Thromboelastographic Analysisof Hemostatic Abnormalities in Dengue PatientsAdmitted in a Multidisciplinary Intensive Care UnitA Cross-sectional Study Indian J Crit Care Med 201822(4)238-42 doi 104103ijccmIJCCM_486_17PubMed PMID 29743762 PubMed Central PMCIDPMCPMC5930527
23 Chuansumrit A Chaiyaratana W Hemostaticderangement in dengue hemorrhagic feverThrombosis Research 2014 133(1)10-6 doi101016jthromres201309028 PubMed PMID24120237
24 Wills B Tran VN Nguyen TH Truong TT Tran TN
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

The Sri Lanka Journal of Haematology2
HWCK Kulathilake SLJH 2018 10(1) 1-4
Rivaroxaban is approved for use in the primaryprevention of VTE in adult patients who haveundergone elective THA or TKA in nonvalvular AFin the treatment of DVT and PE and to reduce therisk of recurrent DVT and PE after initial treatment3
The efficacy and safety of rivaroxaban have beenevaluated in phase 3 clinical trials in differentclinical situations The Regulation of Coagulationin Orthopedic Surgery to Prevent Deep VenousThrombosis and Pulmonary Embolism (RECORD)1234 trials9101112 compared rivaroxaban withenoxaparin in Postoperative VTE Prophylaxis forjoint replacement surgery (THA and TKA) Riva-roxaban significantly reduced the total event ratecompared with enoxaparin in all four trials andthere was no difference in the incidence of majorbleeding between the rivoroxaban and enoxa-parin arms On the basis of these results riva-roxaban was approved in Europe and Canada forthe prevention of VTE in patients undergoingelective hip or knee arthroplasty
The EINSTEIN study 13 compared oral rivaroxabanwith enoxaparin followed by a VKA for 3 6 or 12months in patients with acute symptomatic DVT(initial treatment study) A parallel double blindrandomized study compared rivaroxaban withplacebo for an additional 6 or 12 months in patientswho had completed 6 to 12 months of treatment forVTE (continued-treatment study) The EINSTEIN-PE14 was a similar study that evaluated the samedose of rivaroxaban vs enoxaparinVKA in patientswith an acute symptomatic PE with or without DVT
In EINSTEIN rivaroxaban therapy was noninferiorto enoxaparinVKA therapy with regard to recurrentVTE (21 vs 30 Plt001) In the continued-treatment study rivaroxaban therapy was superiorto placebo use with regard to recurrent VTE (13vs 71 Plt001) The rates of symptomatic recur-rent VTE in the EINSTEIN-PE study were similarbetween the rivaroxaban and enoxaparinVKAgroups In both EINSTEIN and EINSTEIN-PE thesafety outcome of major or clinically relevant nonmajor bleeding were similar in both treatmentarms
The Rivaroxaban Once Daily Oral Direct Factor XaInhibition Compared with Vitamin K Antagonismfor Prevention of Stroke and Embolism Trial in AtrialFibril lation (ROCKET AF) study1516 evaluated
rivaroxaban for prevention of stroke or systemicembolization in patients with nonvalvular AF(intermediate to high risk of stroke) Patients wererandomly divided to receive either rivaroxaban 20mgday or warfarin (target INR 20-30) and thepatients were monitored for 24 months Riva-roxaban was non inferior to warfarin (21 vs 24per year Plt001 for noninferiority) in the primaryefficacy outcome of stroke and systemic embolismThere was no difference between patients takingrivaroxaban and those taking warfarin in terms ofall bleeding events
Dabigatran is approved for use in nonvalvular atrialfibrillation and in the primary prevention of venousthromboembolic events (VTEs) in adult patients withelective total hip (THA) or knee (TKA) arthroplastyDabigatran has been evaluated in several phase 3clinical trials to assess its safety and efficacy indifferent clinical situations
The RE-LY (Randomized Evaluation of Long-termAnticoagulant Therapy Warfarin compared withDabigatran) study1718 evaluated the efficacy andsafety of dabigatran at 110 or 150 mg twice dailycompared with dose-adjusted warfarin targetingan INR of 2 to 3 in patients with nonvalvular AF andan intermediate risk of thromboembolism Bothdoses of dabigatran were non-inferior to warfarinwhile the higher dose proved to be superior forthe primary outcome The major bleeding occurredat a rate of 311 271 and 336 year for thepatients treated with dabigatran 150 mg dabi-gatran 110 mg and warfarin respectively Thedifferences in both the efficacy and safety out-comes were statistically significant
The RE-COVER study19 evaluated patients withacute VTE for a period of 06 months The 6-monthincidence of recurrent symptomatic VTE andrelated deaths was 24 in patients treated withdabigatran vs 21 in those treated with warfarin(Plt001 for noninferiority) The rates of majorbleeding episodes were similar in both groups
Dabigatran in postoperative VTE prophylaxis forjoint replacement sugery was evaluated in theEuropean RE-MODEL study North American RE-MOBILIZE study the European RE-NOVATE (I) andthe North American RE-NOVATE (II) studies Therewere conflicting results between the first 2 trialsin postop TKA In RE-MODEL20 the incidence of VTE
The Sri Lanka Journal of Haematology 3
HWCK Kulathilake SLJH 2018 10(1) 1-4
or mortality was 377 in the enoxaparin armcompared with 364 in the dabigatran 220-mgarm (P=0003 for noninferiority) and 405 in thedabigatran 150-mg arm (P=017 for non-inferio-rity) However in RE-MOBILIZE21 the compositeof VTE and death occurred in 253 of those in theenoxaparin arm compared with 311 of those inthe dabigatran 220-mg arm (P=02) and 337 ofthose in the dabigatran 150-mg arm (Plt001) Thedifferences in efficacy between the 2 trials maybe due to the different dosing schedules ofenoxaparin So dabigatran may not be an equallyefficacious prophylaxis option in this settingAmong the 3 arms the incidence of major bleedingdid not differ significantly in the 02 trials
The RE-NOVATE I and II studies2223 evaluateddabigatran in preventing VTE after THA comparedwith enoxaparin In RE-NOVATE I the findingsconfirmed noninferiority for dabigatran (Plt0001for noninferiority) Furthermore RE-NOVATE IIdetected total VTE and death in 77 in thedabigatran 220-mg arm vs 88 in the enoxaparinarm (P=43) In both RE-NOVATE studies there wasno difference in major bleeding rates with eitherdose of dabigatran compared with enoxaparin
Since the introduction of DOACs in 2008 the globalanticoagulant market shows that warfarin use hasdeclined from 875 to 72 through 2008 to 2014while DOACs have shown an upward trend with amarket share of 155 as of 20142 The questionof whether these agents will replace warfarin andheparins which have been accepted as the goldstandard during all these years is one that needsto be answered after a thorough evaluation ofseveral aspects including high cost of DOACs lackof specific antidotes and lack of long-term safetydata
References
1 Galanis T Thomson L Palladino M et al J ThrombThrombolysis 2011 31 310 httpsdoiorg101007s11239-011-0559-8 PMid21327511
2 Oktay E Will NOACs become the new standard ofcare in anticoagulation therapy InternationalJournal of the Cardiovascular Academy 1 2015 1-4httpsdoiorg101016jijcac201506007
3 Wilson I Gonsalves Rajiv K Pruthi Mrinal MPatnaik The New Oral Anticoagulants in ClinicalPractice Mayo Clin Proc 2013 88(5) 495-511
httpsdoiorg101016jmayocp201303006PMid23639500
4 Lassen MR Raskob GE Gallus A Pineo G Chen DPortman RJ Apixaban or enoxaparin for thrombo-prophylaxis after knee replacement N Engl J Med2009 361(6) 594-604 httpsdoiorg101056NEJMoa0810773 PMid19657123
5 Lassen MR Raskob GE Gallus A Pineo G Chen DHornick P Apixaban versus enoxaparin for thrombo-prophylaxis after knee replacement (ADVANCE-2) arandomised double-blind trial Lancet 2010375(9717) 807-15 httpsdoiorg101016S0140-6736(09)62125-5
6 Lassen MR Gallus A Raskob GE Pineo G Chen DRamirez LM Apixaban versus enoxaparin forthromboprophylaxis after hip replacement N Engl JMed 2010 363(26) 2487-98 httpsdoiorg101056NEJMoa1006885 PMid21175312
7 Connolly SJ Eikelboom J Joyner C et al Apixaban inpatients with atrial fibrillation N Engl J Med 2011364(9) 806-17 httpsdoiorg101056NEJMoa1007432 PMid21309657
8 Granger CB Alexander JH McMurray JJ et alApixaban versus warfarin in patients with atrialfibrillation N Engl J Med 2011 365(11) 981-92h tt p s d o i o rg 10 1056 N E JM o a 1107039PMid21870978
9 Eriksson BI Borris LC Friedman RJ et alRivaroxaban versus enoxaparin for thrombo-prophylaxis after hip arthroplasty N Engl J Med2008 358(26) 2765-75 httpsdoiorg101056NEJMoa0800374 PMid18579811
10 Kakkar AK Brenner B Dahl OE et al Extended durationrivaroxaban versus short-term enoxaparin for theprevention of venous thromboembolism after totalhip arthroplasty a double-blind randomisedcontrolled trial Lancet 2008 372(9632) 31-9 httpsdoiorg101016S0140-6736(08)60880-6
11 Lassen MR Ageno W Borris LC et al Rivaroxabanversus enoxaparin for thromboprophylaxis aftertotal knee arthroplasty N Engl J Med 2008 358(26)2776-86 httpsdoiorg101056NEJMoa076016PMid18579812
12 Turpie AGG Lassen MR Davidson BL et al Riva-roxaban versus enoxaparin for thromboprophylaxisafter total knee arthroplasty (RECORD4) arandomised trial Lancet 2009 373(9676) 1673-80httpsdoiorg101016S0140-6736(09)60734-0
13 Bauersachs R Berkowitz SD Brenner B et al Oralrivaroxaban for symptomatic venous thrombo-embolism N Engl J Med 2010 363(26) 2499-510h tt p s d o i o rg 10 1056 N E JM o a 1007903PMid21128814
The Sri Lanka Journal of Haematology4
HWCK Kulathilake SLJH 2018 10(1) 1-4
14 Buller HR Prins MH Lensin AW et al Oral riva-roxaban for the treatment of symptomatic pulmonaryembolism N Engl J Med 2012 366(14) 1287-97httpsdoiorg101056NEJMoa1113572PMid22449293
15 Patel MR Mahaffey KW Garg J et al Rivaroxabanversus warfarin in nonvalvular atrial fibrillation NEngl J Med 2011 365(10) 883-891 httpsdoiorg101056NEJMoa1009638 PMid21830957
16 Fox KA Piccini JP Wojdyla D et al Prevention ofstroke and systemic embolism with rivaroxabancompared with warfarin in patients with nonvalvularatrial fibrillation and moderate renal impairmentEur Heart J 2011 32(19) 2387-94 httpsdoiorg101093eurheartjehr342 PMid21873708
17 Connolly SJ Ezekowitz MD Yusuf S et al Dabigatranversus warfarin in patients with atrial fibrillationN Engl J Med 2009 361(12) 1139-51 httpsdoiorg101056NEJMoa0905561 PMid19717844
18 Wallentin L Yusuf S Ezekowitz MD et al Efficacyand safety of dabigatran compared with warfarin atdifferent levels of international normalised ratiocontrol for stroke prevention in atrial fibrillationan analysis of the RE-LY trial Lancet 2010 376(9745)975-83httpsdoi org101016S0140-6736(10)61194-4
19 Schulman S Kearon C Kakkar AK et al Dabigatranversus warfarin in the treatment of acute venous
thromboembolism N Engl J Med 2009 361(24)2342-52 httpsdoiorg101056NEJMoa0906598PMid19966341
20 Eriksson BI Dahl OE Rosencher N et al Oraldabigatran etexilate vs subcutaneous enoxaparinfor the prevention of venous thromboembolism aftertotal knee replacement the REMODEL randomizedtrial J Thromb Haemost 2007 5(11) 2178-85httpsdoiorg101111j1538-7836200702748xPMid 17764540
21 Ginsberg JS Davidson BL Comp PC et al Oralthrombin inhibitor dabigatran etexilate vs NorthAmerican enoxaparin regimen for prevention ofvenous thromboembolism after knee arthroplastysurgery J Arthroplast 2009 24(1) 1-9 httpsdoiorg101016jarth200801132 PMid18534438
22 Eriksson BI Dahl OE Rosencher N et al Dabigatranetexilate versus enoxaparin for prevention of venousthromboembolism after total hip replacement arandomised double-blind non inferiority trialLancet 2007 370(9591) 949-56 httpsdoiorg101016S0140-6736(07)61445-7
23 Eriksson BI Dahl OE Huo MH et al Oral dabigatranversus enoxaparin for thromboprophylaxis afterprimary total hip arthroplasty (RE-NOVATE II) arandomised double blind non nferiority trialThromb Haemost 2011 105(4)721-9 httpsdoiorg101160TH10-10-0679 PMid21225098
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 5
1Professor Centre for Dengue Research Universityof Sri Jayewardenepura Nugegoda Sri Lanka2Weatherall Institute of Molecular Medicine JohnRadcliffe Hospital Oxford OX3 9DS UK
Introduction
Dengue viral infections represent one of the mostrapidly emerging mosquito borne infections in theworld which causes 100 million apparent dengueinfections each year1 From 2005 to 2015 althoughthe mortality rates due to many infectious diseasesdecreased the deaths due to dengue increasedby 487 resulting in an estimated 18400 deathsin 20152 Although there is a dengue vaccine licensedto be used in children over the age of 9 years thevaccine manufacturer and other authorities havesuggested that this vaccine should be avoided inindividuals who have not been infected with thedengue virus (DENV) due to the likelihood ofdisease enhancement3
Although the majority of those who are infectedwith the DENV develop asymptomatic or milddisease 478 to 5072 of individuals have shownto develop severe dengue depending on the epi-demic serostatus and circulating DENV serotypesduring that epidemic4 Severe dengue is charac-terized by clinically detectable vascular leakagethat manifest in the form of pleural effusions andascites which can lead to haemodynamic insta-bility and shock5 In addition patients may alsodevelop complications such as bleeding mani-festations liver and renal dysfunction Althoughmild forms of bleeding manifestations such aspetechiae and bleeding from sites of venipunctureare seen in many patients with dengue haemor-rhagic fever (DHF) significant bleeding such as pervaginal bleeding haematuria haematemesis and
Predictors of bleeding in acute dengue virus infection
Gathsaurie Neelika Malavige12
Leading article
Key words dengue viral infection bleeding plasma leakage
malena can lead to haemodynamic instability andshock Development of significant bleeding wasshown to be an independent risk factor associatedwith fatalities in patients with DHF6 Gastrointestinalbleeding alone was shown to strongly associatewith the occurrence of death7
Association of plasma leakage and bleeding
While bleeding manifestations are sometimesseen in patients with dengue fever (DF) significantbleeding is usually seen in those who have severeplasma leakage prolonged shock or organ dys-function89 Severe vascular leakage leading to poorperfusion of the intestinal mucosa and organdysfunction are thought to be the predominantcauses of intestinal bleeding10 Our data has shownthat bleeding manifestations were more frequentamong dengue patients in Sri Lanka in the pastcompared to recent epidemics possibly due tobetter fluid management and reduction in thedevelopment of shock For instance in a study doneby us in year 2004 in adult patients 42108 (389)patients developed bleeding manifestations11whereas the only 26179 (145) developedbleeding manifestations in a patient cohortstudied in years 2016 and 201712 Therefore bettermanagement of fluid leakage appears to indirectlyreduce the incidence of bleeding in dengue
Thrombocytopenia and occurrence of bleeding
Although severe thrombocytopenia was found tobe a predictor of significant bleeding in denguethrombocytopenia alone in the absence of a highhematocrit or liver dysfunction was not associatedwith significant bleeding13 Direct infection ofplatelets by the DENV destruction of platelets dueto immune complexes and bone marrow sup-pression have shown to be the predominant factorsleading to thrombocytopenia (Figure 1)14 Apartfrom the reduction of platelet counts platelet
SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
6
function has also shown to be significantlyimpaired in patients with DHF including impairedplatelet aggregation in response to ADP9 This wasshown to be accompanied by an increase in plasma-thrombomodulin and platelet factor-4 whichindicate an increased secretory activity9 Impairedplatelet function and destruction has also beenobserved in transfused platelets which have ledto a marked reduction in survival rates of trans-fused platelets especially in those with DHF1415
Due to the presence of severe degrees of throm-bocytopenia in the past many centres have pro-phylactically transfused platelets in order toprevent development of any bleeding Howeverseveral retrospective studies had shown thatprophylactic platelet transfusions were associatedwith fluid overload and prolonged hospital staywithout any reduction in bleeding manifestationsor improved platelet recovery1617 In order toaddress this controversy a multi centre rando-mized controlled trial carried out in several centresin Singapore and Malaysia in patients with plateletcounts 20000 plateletsmicroL showed that pro-phylactic platelet transfusions did not reduce theoccurrence of bleeding18 Instead platelet trans-fusions were associated with an increase incidenceof adverse effects including those of seriousnature such as anaphylaxis and transfusion relatedacute lung injury18 Therefore both the WHOguidelines and the National dengue managementguidelines do not recommend platelet trans-fusions but have advocated blood transfusions inthose who are suspected to have developedsignificant bleeding
The effect of many herbal preparations such as theleave extract of Carica papaya in improving plateletcounts have been studied and in vitro evidencehave shown that this leaf extract reduces plateletaggregation19 Two multi-centre randomizeddouble blind placebo controlled trials using Caricapapaya in India showed that this leaf extract doessignificantly increase platelet counts initiallyalthough there was no significant difference inplatelet counts 48 hours after administration ofthe leaf extract20 However these trials had notassessed the efficacy of this leaf extract onreducing plasma leakage organ dysfunction and
mortality and have not reported any adverseeffects as is indicated in the standard reporting ofclinical trials20 Therefore as it is difficult toascertain the other possible benefits or adverseeffects of this drug it would be important toconduct proper clinical trials according to theinternationally recommended guidelines
Coagulation abnormalities leading to bleeding
Apart from the presence of prolonged shocksevere liver dysfunction is suggested as one the mostimportant predictors of severe bleeding21 Manyclotting factors such as factor V VII VIII IX and Xfibrinogen protein C and S and antithrombin aresynthesized by the liver and low levels of theseproteins are seen in patients with acute dengueAlthough thromboelastographic studies have alsodemonstrated deficiency of coagulation factorsand abnormalities in platelet function the levelswere not associated with the degree of thrombo-cytopenia or liver dysfunction22
Many patients with DHF have a prolongedprothrombin time prolonged INR and activatedpartial thromboplastin time (aPTT) It is thoughtthat these abnormalities possibly occur due to thereduced production of these factors and alsoleakage of these proteins into extravascular spacesacross the dysfunctional endothelium92123 Prolon-gation of the prothrombin time has been shownto be an important predictor of occurrence ofbleeding in patients with severe plasma leakage21Although many studies have reported an increasein partial thromboplastin times and reduction infibrinogen concentrations9 change in these para-meters correlated with the extent of vascularleakage and not with bleeding24 More detailedstudies which have assessed changes of theseproteins at different stages of the illness haveshown that protein C S and antithrombin III levelswere significantly lower in patients with moresevere degrees of shock during the leakagephase However as these proteins returned tonormal levels following the leakage phase it hasbeen suggested that leakage of these proteinsinto extravascular tissues could be the mainfactor leading to low levels in patients with DHF(Figure 1)9
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 7
Endothelial activation and bleeding in dengue
Patients with more severe forms of dengue arealso shown to have high levels of tissue factorthrombomodulin and plasminogen activatorinhibitor type 1 (PAI-1) which have been attri-buted to endothelial platelet and monocyteactivation9 Endothelial activation and injury is alsoreflected by high levels of von Willebrand factor(vWF) especially in patients with severe shock23It was also shown that the number of circulatingendothelial cells and soluble thrombomodulinlevels were significantly higher in patients withprofound shock further supporting that endo-thelial injury occurs in severe dengue23 Thromo-bomodulin which is an integral membrane proteinexpressed on endothelial cells monocytes andcertain dendritic cells is cofactor in activation of
protein C Although soluble thrombomodulinlevels were markedly high in those with severeforms plasma leakage as protein C levels are lowthe contribution to these pathways in causingsevere dengue and bleeding is not certain
Despite significant derangements in prothrom-botic antithrombotic and fibrinolytic pathways asmost patients do not develop bleeding it issuggested that the combinations of many factorssuch tissue hypoxia acidosis along with thrombo-cytopenia are important co-factors Howeverplasma leakage secondary endothelial dysfunctionappears to be the most important factor leading toshock poor organ perfusion organ dysfunctionderangement of many coagulation pathways andbleeding510 We have identified that plateletactivating factor (PAF) significantly contributed to
Bleeding manifestations are thought to occur due to the complex interplay of many factors such asendothelial dysfunction liver dysfunction and thrombocytopenia Endothelial dysfunction leads to plasmaleakage and when severe leads to shock poor organ perfusion and tissue hypoxia Tissue hypoxia in thegastrointestinal and possibly the lung epithelium is thought to be the main contributing factors forbleeding from these sites Many clotting factors and antithrombic factors are also thought to extravasatein to the tissues leading to low levels of these in the plasma In addition liver dysfunction may also leadto reduction in the production of these factors
Figure 1 Factors that contribute to bleeding in acute dengue infection
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
8
vascular leakage in dengue25 In addition lipidmediators that oppose the action of PAF andprotect the endothelial barrier integrity such assphingosine-1-phosphate was found to bemarkedly low in patients with DHF especiallyduring the critical phase26
As plasma leakage appears to be the most impor-tant factor leading to all complications of dengueit would be reasonable to use drugs that preventor reduce vascular leakage as a suitable option toreduce severe dengue and associated compli-cations We have concluded a phase 2 randomizedplacebo controlled clinical trial in 183 patients atthe National Institute of Infectious Diseases SriLanka using a PAF receptor blocker known asrupatadine27 In this clinical trial we found thatrupatadine up to 40mg daily appeared safe andwell-tolerated in patients with acute dengue Inaddition patients given rupatadine had higherplatelet counts and lower aspartate-aminotrans-ferase levels during the critical phase and signifi-cantly smaller pleural effusions27 The develop-ment of significant bleeding manifestations suchas per vaginal bleeding and gastrointestinalbleeding was also lower in the group who receivedtreatment As the beneficial effects of this drugappeared to be greater when given early in theillness we are currently conducting another trialwhich is double blind randomized placebocontrolled trial in a larger cohort of patientsAlthough the initial trial showed promising resultsthese results should be interpreted with cautionuntil the same beneficial effects are seen in largertrials that we are currently carrying out
Summary
Endothelial dysfunction leading to plasma leakageappears to be the most important predictor ofoccurrence of bleeding in acute dengue Althoughthrombocytopenia is a risk factor of bleeding indengue thrombocytopenia alone was notassociated with bleeding in the absence of plasmaleakage Many abnormalities in the coagulationpathways are seen in severe dengue which appearto return to normal during the recovery phaseThese coagulation abnormalities have beenassociated with the degree of plasma leakage As
References
1 Bhatt S Gething PW Brady OJ Messina JP FarlowAW Moyes CL et al The global distribution andburden of dengue Nature 2013 496(7446) 504-7Epub 20130409 doi 101038nature12060 PubMedPMID 23563266 PubMed Central PMCIDPMC3651993
2 Mortality GBD Causes of Death C Global regionaland national life expectancy all-cause mortality andcause-specific mortality for 249 causes of death1980-2015 a systematic analysis for the GlobalBurden of Disease Study 2015 Lancet 2016388(10053) 1459-544 doi 101016S0140-6736(16)31012-1 PubMed PMID 27733281
3 Rouvinski A Guardado-Calvo P Barba-Spaeth GDuquerroy S Vaney MC Kikuti CM et al Recognitiondeterminants of broadly neutralizing humanantibodies against dengue viruses Nature 2015520(7545) 109-13 doi 101038nature14130PubMed PMID 25581790
4 Soo KM Khalid B Ching SM Chee HY Meta-Analysisof Dengue Severity during Infection by DifferentDengue Virus Serotypes in Primary and SecondaryInfections PloS one 2016 11(5) e0154760doi 101371journalpone02154760 PubMed PMID27213782 PubMed Central PMCID PMCPMC4877104
5 Malavige GN Ogg GS Pathogenesis of vascular leakin dengue virus infection Immunology 2017 151(3)261-9 doi 101111imm12748 PubMed PMID28437586 PubMed Central PMCID PMCPMC5461104
Authorship
Contribution This is the sole work of ProfGathsaurie Neelika Malavige
Conflict-of-interest disclosure The author declaresno conflict of interest
Correspondence Prof Gathsaurie Neelika MalavigeDPhil FRCP (Lond) FRCPath (UK)Centre for Dengue Research Faculty of MedicalSciences University of Sri Jayawardanapura SriLanka
E-mail gathsauriemalavigendmoxacuk
bleeding manifestations appear to best correlatewith the degree of leakage proper and meticulousfluid management would be the most importantmeasure in preventing bleeding manifestations
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 9
6 Md-Sani SS Md-Noor J Han WH Gan SP Rani NS TanHL et al Prediction of mortality in severe denguecases BMC infectious diseases 2018 18(1) 232 doi101186s12879-018-3141-6 PubMed PMID29783955
7 Pinto RC Castro DB Albuquerque BC Sampaio Vde SPassos RA Costa CF et al Mortality Predictors inPatients with Severe Dengue in the State of AmazonasBrazil PloS one 2016 11(8)e0161884 doi 101371journalpone0161884 PubMed PMID 27564084PubMed Central PMCID PMCPMC5001629
8 Sam SS Omar SF Teoh BT Abd-Jamil J AbuBakar SReview of Dengue hemorrhagic fever fatal cases seenamong adults a retrospective study PLoS neglectedtropical diseases 2013 7(5)e2194 doi 101371journalpntd0002194 PubMed PMID 23658849PubMed Central PMCID PMCPMC3642057
9 Wills BA Oragui EE Stephens AC Daramola OA DungNM Loan HT et al Coagulation abnormalities indengue hemorrhagic Fever serial investigations in167 Vietnamese children with Dengue shocksyndrome Clin Infect Dis 2002 35(3) 277-85 Epub20020713 doi 101086341410 PubMed PMID12115093
10 WHO editor Comprehensive guidelines forprevention and control of dengue fever and denguehaemorrhagic fever SEARO New Delhi India WorldHealth Organization 2011
11 Malavige GN Velathanthiri VG Wijewickrama ESFernando S Jayaratne SD Aaskov J et al Patterns ofdisease among adults hospitalized with dengueinfections Qjm 2006 99(5) 299-305 PubMed PMID16603571
12 Wijewickrama A FS Jayerathne PGSB Perera MAPAAbeynaike SA Gomes L Jeewandara C Malavige GNEffect of change in serotype on clinical severity ofdengue infections In SLMA editor Annual Con-ference of the Sri Lanka Medical AssociationColombo SLMA 2017
13 Wong JG Thein TL Leo YS Pang J Lye DC IdentifyingAdult Dengue Patients at Low Risk for ClinicallySignificant Bleeding PloS one 2016 11(2) e0148579doi 101371journalpone0148579 PubMed PMID26849556 PubMed Central PMCID PMCPMC4743958
14 Ojha A Nandi D Batra H Singhal R Annarapu GKBhattacharyya S et al Platelet activation determinesthe severity of thrombocytopenia in dengue infectionSci Rep 2017 7 41697 doi 101038srep41697PubMed PMID 28139770 PubMed Central PMCIDPMCPMC5282509
15 Isarangkura P Tuchinda S The behavior of transfused
platelets in dengue hemorrhagic fever The SoutheastAsian Journal of Tropical Medicine and Public Health1993 24 Suppl 1 222-4 PubMed PMID 7886581
16 Lum LC Abdel-Latif Mel A Goh AY Chan PW Lam SKPreventive transfusion in Dengue shock syndrome-is it necessary The Journal of Pediatrics 2003143(5) 682-4 PubMed PMID 14615749
17 Lye DC Lee VJ Sun Y Leo YS Lack of efficacy ofprophylactic platelet transfusion for severethrombocytopenia in adults with acute uncom-plicated dengue infection Clin Infect Dis 2009 48(9)1262-5 PubMed PMID 19292665
18 Lye DC Archuleta S Syed-Omar SF Low JG Oh HMWei Y et al Prophylactic platelet transfusion plussupportive care versus supportive care alone inadults with dengue and thrombocytopenia amulticentre open-label randomised superioritytrial Lancet 2017 389(10079) 1611-8 doi 101016S0140-6736(17)30269-6 PubMed PMID 28283286
19 Chinnappan S Ramachandrappa VS Tamilarasu KKrishnan UM Pillai AK Rajendiran S Inhibition ofPlatelet Aggregation by the Leaf Extract of Caricapapaya During Dengue Infection An In Vitro StudyViral immunology 2016 29(3) 164-8 doi 101089vim20150083 PubMed PMID 26910599
20 Charan J Saxena D Goyal JP Yasobant S Efficacyand safety of Carica papaya leaf extract in thedengue A systematic review and meta-analysis Int JAppl Basic Med Res 2016 6(4)249-54 doi 1041032229-516X192596 PubMed PMID 27857891PubMed Central PMCID PMCPMC5108100
21 Laoprasopwattana K Binsaai J Pruekprasert PGeater A Prothrombin Time Prolongation was theMost Important Indicator of Severe Bleeding inChildren with Severe Dengue Viral Infection Journalof Tropical Pediatrics 2017 63(4)314-20 doi101093tropejfmw097 PubMed PMID 28177091
22 Sureshkumar VK Vijayan D Kunhu S Mohamed ZThomas S Raman M Thromboelastographic Analysisof Hemostatic Abnormalities in Dengue PatientsAdmitted in a Multidisciplinary Intensive Care UnitA Cross-sectional Study Indian J Crit Care Med 201822(4)238-42 doi 104103ijccmIJCCM_486_17PubMed PMID 29743762 PubMed Central PMCIDPMCPMC5930527
23 Chuansumrit A Chaiyaratana W Hemostaticderangement in dengue hemorrhagic feverThrombosis Research 2014 133(1)10-6 doi101016jthromres201309028 PubMed PMID24120237
24 Wills B Tran VN Nguyen TH Truong TT Tran TN
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
The Sri Lanka Journal of Haematology 3
HWCK Kulathilake SLJH 2018 10(1) 1-4
or mortality was 377 in the enoxaparin armcompared with 364 in the dabigatran 220-mgarm (P=0003 for noninferiority) and 405 in thedabigatran 150-mg arm (P=017 for non-inferio-rity) However in RE-MOBILIZE21 the compositeof VTE and death occurred in 253 of those in theenoxaparin arm compared with 311 of those inthe dabigatran 220-mg arm (P=02) and 337 ofthose in the dabigatran 150-mg arm (Plt001) Thedifferences in efficacy between the 2 trials maybe due to the different dosing schedules ofenoxaparin So dabigatran may not be an equallyefficacious prophylaxis option in this settingAmong the 3 arms the incidence of major bleedingdid not differ significantly in the 02 trials
The RE-NOVATE I and II studies2223 evaluateddabigatran in preventing VTE after THA comparedwith enoxaparin In RE-NOVATE I the findingsconfirmed noninferiority for dabigatran (Plt0001for noninferiority) Furthermore RE-NOVATE IIdetected total VTE and death in 77 in thedabigatran 220-mg arm vs 88 in the enoxaparinarm (P=43) In both RE-NOVATE studies there wasno difference in major bleeding rates with eitherdose of dabigatran compared with enoxaparin
Since the introduction of DOACs in 2008 the globalanticoagulant market shows that warfarin use hasdeclined from 875 to 72 through 2008 to 2014while DOACs have shown an upward trend with amarket share of 155 as of 20142 The questionof whether these agents will replace warfarin andheparins which have been accepted as the goldstandard during all these years is one that needsto be answered after a thorough evaluation ofseveral aspects including high cost of DOACs lackof specific antidotes and lack of long-term safetydata
References
1 Galanis T Thomson L Palladino M et al J ThrombThrombolysis 2011 31 310 httpsdoiorg101007s11239-011-0559-8 PMid21327511
2 Oktay E Will NOACs become the new standard ofcare in anticoagulation therapy InternationalJournal of the Cardiovascular Academy 1 2015 1-4httpsdoiorg101016jijcac201506007
3 Wilson I Gonsalves Rajiv K Pruthi Mrinal MPatnaik The New Oral Anticoagulants in ClinicalPractice Mayo Clin Proc 2013 88(5) 495-511
httpsdoiorg101016jmayocp201303006PMid23639500
4 Lassen MR Raskob GE Gallus A Pineo G Chen DPortman RJ Apixaban or enoxaparin for thrombo-prophylaxis after knee replacement N Engl J Med2009 361(6) 594-604 httpsdoiorg101056NEJMoa0810773 PMid19657123
5 Lassen MR Raskob GE Gallus A Pineo G Chen DHornick P Apixaban versus enoxaparin for thrombo-prophylaxis after knee replacement (ADVANCE-2) arandomised double-blind trial Lancet 2010375(9717) 807-15 httpsdoiorg101016S0140-6736(09)62125-5
6 Lassen MR Gallus A Raskob GE Pineo G Chen DRamirez LM Apixaban versus enoxaparin forthromboprophylaxis after hip replacement N Engl JMed 2010 363(26) 2487-98 httpsdoiorg101056NEJMoa1006885 PMid21175312
7 Connolly SJ Eikelboom J Joyner C et al Apixaban inpatients with atrial fibrillation N Engl J Med 2011364(9) 806-17 httpsdoiorg101056NEJMoa1007432 PMid21309657
8 Granger CB Alexander JH McMurray JJ et alApixaban versus warfarin in patients with atrialfibrillation N Engl J Med 2011 365(11) 981-92h tt p s d o i o rg 10 1056 N E JM o a 1107039PMid21870978
9 Eriksson BI Borris LC Friedman RJ et alRivaroxaban versus enoxaparin for thrombo-prophylaxis after hip arthroplasty N Engl J Med2008 358(26) 2765-75 httpsdoiorg101056NEJMoa0800374 PMid18579811
10 Kakkar AK Brenner B Dahl OE et al Extended durationrivaroxaban versus short-term enoxaparin for theprevention of venous thromboembolism after totalhip arthroplasty a double-blind randomisedcontrolled trial Lancet 2008 372(9632) 31-9 httpsdoiorg101016S0140-6736(08)60880-6
11 Lassen MR Ageno W Borris LC et al Rivaroxabanversus enoxaparin for thromboprophylaxis aftertotal knee arthroplasty N Engl J Med 2008 358(26)2776-86 httpsdoiorg101056NEJMoa076016PMid18579812
12 Turpie AGG Lassen MR Davidson BL et al Riva-roxaban versus enoxaparin for thromboprophylaxisafter total knee arthroplasty (RECORD4) arandomised trial Lancet 2009 373(9676) 1673-80httpsdoiorg101016S0140-6736(09)60734-0
13 Bauersachs R Berkowitz SD Brenner B et al Oralrivaroxaban for symptomatic venous thrombo-embolism N Engl J Med 2010 363(26) 2499-510h tt p s d o i o rg 10 1056 N E JM o a 1007903PMid21128814
The Sri Lanka Journal of Haematology4
HWCK Kulathilake SLJH 2018 10(1) 1-4
14 Buller HR Prins MH Lensin AW et al Oral riva-roxaban for the treatment of symptomatic pulmonaryembolism N Engl J Med 2012 366(14) 1287-97httpsdoiorg101056NEJMoa1113572PMid22449293
15 Patel MR Mahaffey KW Garg J et al Rivaroxabanversus warfarin in nonvalvular atrial fibrillation NEngl J Med 2011 365(10) 883-891 httpsdoiorg101056NEJMoa1009638 PMid21830957
16 Fox KA Piccini JP Wojdyla D et al Prevention ofstroke and systemic embolism with rivaroxabancompared with warfarin in patients with nonvalvularatrial fibrillation and moderate renal impairmentEur Heart J 2011 32(19) 2387-94 httpsdoiorg101093eurheartjehr342 PMid21873708
17 Connolly SJ Ezekowitz MD Yusuf S et al Dabigatranversus warfarin in patients with atrial fibrillationN Engl J Med 2009 361(12) 1139-51 httpsdoiorg101056NEJMoa0905561 PMid19717844
18 Wallentin L Yusuf S Ezekowitz MD et al Efficacyand safety of dabigatran compared with warfarin atdifferent levels of international normalised ratiocontrol for stroke prevention in atrial fibrillationan analysis of the RE-LY trial Lancet 2010 376(9745)975-83httpsdoi org101016S0140-6736(10)61194-4
19 Schulman S Kearon C Kakkar AK et al Dabigatranversus warfarin in the treatment of acute venous
thromboembolism N Engl J Med 2009 361(24)2342-52 httpsdoiorg101056NEJMoa0906598PMid19966341
20 Eriksson BI Dahl OE Rosencher N et al Oraldabigatran etexilate vs subcutaneous enoxaparinfor the prevention of venous thromboembolism aftertotal knee replacement the REMODEL randomizedtrial J Thromb Haemost 2007 5(11) 2178-85httpsdoiorg101111j1538-7836200702748xPMid 17764540
21 Ginsberg JS Davidson BL Comp PC et al Oralthrombin inhibitor dabigatran etexilate vs NorthAmerican enoxaparin regimen for prevention ofvenous thromboembolism after knee arthroplastysurgery J Arthroplast 2009 24(1) 1-9 httpsdoiorg101016jarth200801132 PMid18534438
22 Eriksson BI Dahl OE Rosencher N et al Dabigatranetexilate versus enoxaparin for prevention of venousthromboembolism after total hip replacement arandomised double-blind non inferiority trialLancet 2007 370(9591) 949-56 httpsdoiorg101016S0140-6736(07)61445-7
23 Eriksson BI Dahl OE Huo MH et al Oral dabigatranversus enoxaparin for thromboprophylaxis afterprimary total hip arthroplasty (RE-NOVATE II) arandomised double blind non nferiority trialThromb Haemost 2011 105(4)721-9 httpsdoiorg101160TH10-10-0679 PMid21225098
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 5
1Professor Centre for Dengue Research Universityof Sri Jayewardenepura Nugegoda Sri Lanka2Weatherall Institute of Molecular Medicine JohnRadcliffe Hospital Oxford OX3 9DS UK
Introduction
Dengue viral infections represent one of the mostrapidly emerging mosquito borne infections in theworld which causes 100 million apparent dengueinfections each year1 From 2005 to 2015 althoughthe mortality rates due to many infectious diseasesdecreased the deaths due to dengue increasedby 487 resulting in an estimated 18400 deathsin 20152 Although there is a dengue vaccine licensedto be used in children over the age of 9 years thevaccine manufacturer and other authorities havesuggested that this vaccine should be avoided inindividuals who have not been infected with thedengue virus (DENV) due to the likelihood ofdisease enhancement3
Although the majority of those who are infectedwith the DENV develop asymptomatic or milddisease 478 to 5072 of individuals have shownto develop severe dengue depending on the epi-demic serostatus and circulating DENV serotypesduring that epidemic4 Severe dengue is charac-terized by clinically detectable vascular leakagethat manifest in the form of pleural effusions andascites which can lead to haemodynamic insta-bility and shock5 In addition patients may alsodevelop complications such as bleeding mani-festations liver and renal dysfunction Althoughmild forms of bleeding manifestations such aspetechiae and bleeding from sites of venipunctureare seen in many patients with dengue haemor-rhagic fever (DHF) significant bleeding such as pervaginal bleeding haematuria haematemesis and
Predictors of bleeding in acute dengue virus infection
Gathsaurie Neelika Malavige12
Leading article
Key words dengue viral infection bleeding plasma leakage
malena can lead to haemodynamic instability andshock Development of significant bleeding wasshown to be an independent risk factor associatedwith fatalities in patients with DHF6 Gastrointestinalbleeding alone was shown to strongly associatewith the occurrence of death7
Association of plasma leakage and bleeding
While bleeding manifestations are sometimesseen in patients with dengue fever (DF) significantbleeding is usually seen in those who have severeplasma leakage prolonged shock or organ dys-function89 Severe vascular leakage leading to poorperfusion of the intestinal mucosa and organdysfunction are thought to be the predominantcauses of intestinal bleeding10 Our data has shownthat bleeding manifestations were more frequentamong dengue patients in Sri Lanka in the pastcompared to recent epidemics possibly due tobetter fluid management and reduction in thedevelopment of shock For instance in a study doneby us in year 2004 in adult patients 42108 (389)patients developed bleeding manifestations11whereas the only 26179 (145) developedbleeding manifestations in a patient cohortstudied in years 2016 and 201712 Therefore bettermanagement of fluid leakage appears to indirectlyreduce the incidence of bleeding in dengue
Thrombocytopenia and occurrence of bleeding
Although severe thrombocytopenia was found tobe a predictor of significant bleeding in denguethrombocytopenia alone in the absence of a highhematocrit or liver dysfunction was not associatedwith significant bleeding13 Direct infection ofplatelets by the DENV destruction of platelets dueto immune complexes and bone marrow sup-pression have shown to be the predominant factorsleading to thrombocytopenia (Figure 1)14 Apartfrom the reduction of platelet counts platelet
SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
6
function has also shown to be significantlyimpaired in patients with DHF including impairedplatelet aggregation in response to ADP9 This wasshown to be accompanied by an increase in plasma-thrombomodulin and platelet factor-4 whichindicate an increased secretory activity9 Impairedplatelet function and destruction has also beenobserved in transfused platelets which have ledto a marked reduction in survival rates of trans-fused platelets especially in those with DHF1415
Due to the presence of severe degrees of throm-bocytopenia in the past many centres have pro-phylactically transfused platelets in order toprevent development of any bleeding Howeverseveral retrospective studies had shown thatprophylactic platelet transfusions were associatedwith fluid overload and prolonged hospital staywithout any reduction in bleeding manifestationsor improved platelet recovery1617 In order toaddress this controversy a multi centre rando-mized controlled trial carried out in several centresin Singapore and Malaysia in patients with plateletcounts 20000 plateletsmicroL showed that pro-phylactic platelet transfusions did not reduce theoccurrence of bleeding18 Instead platelet trans-fusions were associated with an increase incidenceof adverse effects including those of seriousnature such as anaphylaxis and transfusion relatedacute lung injury18 Therefore both the WHOguidelines and the National dengue managementguidelines do not recommend platelet trans-fusions but have advocated blood transfusions inthose who are suspected to have developedsignificant bleeding
The effect of many herbal preparations such as theleave extract of Carica papaya in improving plateletcounts have been studied and in vitro evidencehave shown that this leaf extract reduces plateletaggregation19 Two multi-centre randomizeddouble blind placebo controlled trials using Caricapapaya in India showed that this leaf extract doessignificantly increase platelet counts initiallyalthough there was no significant difference inplatelet counts 48 hours after administration ofthe leaf extract20 However these trials had notassessed the efficacy of this leaf extract onreducing plasma leakage organ dysfunction and
mortality and have not reported any adverseeffects as is indicated in the standard reporting ofclinical trials20 Therefore as it is difficult toascertain the other possible benefits or adverseeffects of this drug it would be important toconduct proper clinical trials according to theinternationally recommended guidelines
Coagulation abnormalities leading to bleeding
Apart from the presence of prolonged shocksevere liver dysfunction is suggested as one the mostimportant predictors of severe bleeding21 Manyclotting factors such as factor V VII VIII IX and Xfibrinogen protein C and S and antithrombin aresynthesized by the liver and low levels of theseproteins are seen in patients with acute dengueAlthough thromboelastographic studies have alsodemonstrated deficiency of coagulation factorsand abnormalities in platelet function the levelswere not associated with the degree of thrombo-cytopenia or liver dysfunction22
Many patients with DHF have a prolongedprothrombin time prolonged INR and activatedpartial thromboplastin time (aPTT) It is thoughtthat these abnormalities possibly occur due to thereduced production of these factors and alsoleakage of these proteins into extravascular spacesacross the dysfunctional endothelium92123 Prolon-gation of the prothrombin time has been shownto be an important predictor of occurrence ofbleeding in patients with severe plasma leakage21Although many studies have reported an increasein partial thromboplastin times and reduction infibrinogen concentrations9 change in these para-meters correlated with the extent of vascularleakage and not with bleeding24 More detailedstudies which have assessed changes of theseproteins at different stages of the illness haveshown that protein C S and antithrombin III levelswere significantly lower in patients with moresevere degrees of shock during the leakagephase However as these proteins returned tonormal levels following the leakage phase it hasbeen suggested that leakage of these proteinsinto extravascular tissues could be the mainfactor leading to low levels in patients with DHF(Figure 1)9
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 7
Endothelial activation and bleeding in dengue
Patients with more severe forms of dengue arealso shown to have high levels of tissue factorthrombomodulin and plasminogen activatorinhibitor type 1 (PAI-1) which have been attri-buted to endothelial platelet and monocyteactivation9 Endothelial activation and injury is alsoreflected by high levels of von Willebrand factor(vWF) especially in patients with severe shock23It was also shown that the number of circulatingendothelial cells and soluble thrombomodulinlevels were significantly higher in patients withprofound shock further supporting that endo-thelial injury occurs in severe dengue23 Thromo-bomodulin which is an integral membrane proteinexpressed on endothelial cells monocytes andcertain dendritic cells is cofactor in activation of
protein C Although soluble thrombomodulinlevels were markedly high in those with severeforms plasma leakage as protein C levels are lowthe contribution to these pathways in causingsevere dengue and bleeding is not certain
Despite significant derangements in prothrom-botic antithrombotic and fibrinolytic pathways asmost patients do not develop bleeding it issuggested that the combinations of many factorssuch tissue hypoxia acidosis along with thrombo-cytopenia are important co-factors Howeverplasma leakage secondary endothelial dysfunctionappears to be the most important factor leading toshock poor organ perfusion organ dysfunctionderangement of many coagulation pathways andbleeding510 We have identified that plateletactivating factor (PAF) significantly contributed to
Bleeding manifestations are thought to occur due to the complex interplay of many factors such asendothelial dysfunction liver dysfunction and thrombocytopenia Endothelial dysfunction leads to plasmaleakage and when severe leads to shock poor organ perfusion and tissue hypoxia Tissue hypoxia in thegastrointestinal and possibly the lung epithelium is thought to be the main contributing factors forbleeding from these sites Many clotting factors and antithrombic factors are also thought to extravasatein to the tissues leading to low levels of these in the plasma In addition liver dysfunction may also leadto reduction in the production of these factors
Figure 1 Factors that contribute to bleeding in acute dengue infection
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
8
vascular leakage in dengue25 In addition lipidmediators that oppose the action of PAF andprotect the endothelial barrier integrity such assphingosine-1-phosphate was found to bemarkedly low in patients with DHF especiallyduring the critical phase26
As plasma leakage appears to be the most impor-tant factor leading to all complications of dengueit would be reasonable to use drugs that preventor reduce vascular leakage as a suitable option toreduce severe dengue and associated compli-cations We have concluded a phase 2 randomizedplacebo controlled clinical trial in 183 patients atthe National Institute of Infectious Diseases SriLanka using a PAF receptor blocker known asrupatadine27 In this clinical trial we found thatrupatadine up to 40mg daily appeared safe andwell-tolerated in patients with acute dengue Inaddition patients given rupatadine had higherplatelet counts and lower aspartate-aminotrans-ferase levels during the critical phase and signifi-cantly smaller pleural effusions27 The develop-ment of significant bleeding manifestations suchas per vaginal bleeding and gastrointestinalbleeding was also lower in the group who receivedtreatment As the beneficial effects of this drugappeared to be greater when given early in theillness we are currently conducting another trialwhich is double blind randomized placebocontrolled trial in a larger cohort of patientsAlthough the initial trial showed promising resultsthese results should be interpreted with cautionuntil the same beneficial effects are seen in largertrials that we are currently carrying out
Summary
Endothelial dysfunction leading to plasma leakageappears to be the most important predictor ofoccurrence of bleeding in acute dengue Althoughthrombocytopenia is a risk factor of bleeding indengue thrombocytopenia alone was notassociated with bleeding in the absence of plasmaleakage Many abnormalities in the coagulationpathways are seen in severe dengue which appearto return to normal during the recovery phaseThese coagulation abnormalities have beenassociated with the degree of plasma leakage As
References
1 Bhatt S Gething PW Brady OJ Messina JP FarlowAW Moyes CL et al The global distribution andburden of dengue Nature 2013 496(7446) 504-7Epub 20130409 doi 101038nature12060 PubMedPMID 23563266 PubMed Central PMCIDPMC3651993
2 Mortality GBD Causes of Death C Global regionaland national life expectancy all-cause mortality andcause-specific mortality for 249 causes of death1980-2015 a systematic analysis for the GlobalBurden of Disease Study 2015 Lancet 2016388(10053) 1459-544 doi 101016S0140-6736(16)31012-1 PubMed PMID 27733281
3 Rouvinski A Guardado-Calvo P Barba-Spaeth GDuquerroy S Vaney MC Kikuti CM et al Recognitiondeterminants of broadly neutralizing humanantibodies against dengue viruses Nature 2015520(7545) 109-13 doi 101038nature14130PubMed PMID 25581790
4 Soo KM Khalid B Ching SM Chee HY Meta-Analysisof Dengue Severity during Infection by DifferentDengue Virus Serotypes in Primary and SecondaryInfections PloS one 2016 11(5) e0154760doi 101371journalpone02154760 PubMed PMID27213782 PubMed Central PMCID PMCPMC4877104
5 Malavige GN Ogg GS Pathogenesis of vascular leakin dengue virus infection Immunology 2017 151(3)261-9 doi 101111imm12748 PubMed PMID28437586 PubMed Central PMCID PMCPMC5461104
Authorship
Contribution This is the sole work of ProfGathsaurie Neelika Malavige
Conflict-of-interest disclosure The author declaresno conflict of interest
Correspondence Prof Gathsaurie Neelika MalavigeDPhil FRCP (Lond) FRCPath (UK)Centre for Dengue Research Faculty of MedicalSciences University of Sri Jayawardanapura SriLanka
E-mail gathsauriemalavigendmoxacuk
bleeding manifestations appear to best correlatewith the degree of leakage proper and meticulousfluid management would be the most importantmeasure in preventing bleeding manifestations
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 9
6 Md-Sani SS Md-Noor J Han WH Gan SP Rani NS TanHL et al Prediction of mortality in severe denguecases BMC infectious diseases 2018 18(1) 232 doi101186s12879-018-3141-6 PubMed PMID29783955
7 Pinto RC Castro DB Albuquerque BC Sampaio Vde SPassos RA Costa CF et al Mortality Predictors inPatients with Severe Dengue in the State of AmazonasBrazil PloS one 2016 11(8)e0161884 doi 101371journalpone0161884 PubMed PMID 27564084PubMed Central PMCID PMCPMC5001629
8 Sam SS Omar SF Teoh BT Abd-Jamil J AbuBakar SReview of Dengue hemorrhagic fever fatal cases seenamong adults a retrospective study PLoS neglectedtropical diseases 2013 7(5)e2194 doi 101371journalpntd0002194 PubMed PMID 23658849PubMed Central PMCID PMCPMC3642057
9 Wills BA Oragui EE Stephens AC Daramola OA DungNM Loan HT et al Coagulation abnormalities indengue hemorrhagic Fever serial investigations in167 Vietnamese children with Dengue shocksyndrome Clin Infect Dis 2002 35(3) 277-85 Epub20020713 doi 101086341410 PubMed PMID12115093
10 WHO editor Comprehensive guidelines forprevention and control of dengue fever and denguehaemorrhagic fever SEARO New Delhi India WorldHealth Organization 2011
11 Malavige GN Velathanthiri VG Wijewickrama ESFernando S Jayaratne SD Aaskov J et al Patterns ofdisease among adults hospitalized with dengueinfections Qjm 2006 99(5) 299-305 PubMed PMID16603571
12 Wijewickrama A FS Jayerathne PGSB Perera MAPAAbeynaike SA Gomes L Jeewandara C Malavige GNEffect of change in serotype on clinical severity ofdengue infections In SLMA editor Annual Con-ference of the Sri Lanka Medical AssociationColombo SLMA 2017
13 Wong JG Thein TL Leo YS Pang J Lye DC IdentifyingAdult Dengue Patients at Low Risk for ClinicallySignificant Bleeding PloS one 2016 11(2) e0148579doi 101371journalpone0148579 PubMed PMID26849556 PubMed Central PMCID PMCPMC4743958
14 Ojha A Nandi D Batra H Singhal R Annarapu GKBhattacharyya S et al Platelet activation determinesthe severity of thrombocytopenia in dengue infectionSci Rep 2017 7 41697 doi 101038srep41697PubMed PMID 28139770 PubMed Central PMCIDPMCPMC5282509
15 Isarangkura P Tuchinda S The behavior of transfused
platelets in dengue hemorrhagic fever The SoutheastAsian Journal of Tropical Medicine and Public Health1993 24 Suppl 1 222-4 PubMed PMID 7886581
16 Lum LC Abdel-Latif Mel A Goh AY Chan PW Lam SKPreventive transfusion in Dengue shock syndrome-is it necessary The Journal of Pediatrics 2003143(5) 682-4 PubMed PMID 14615749
17 Lye DC Lee VJ Sun Y Leo YS Lack of efficacy ofprophylactic platelet transfusion for severethrombocytopenia in adults with acute uncom-plicated dengue infection Clin Infect Dis 2009 48(9)1262-5 PubMed PMID 19292665
18 Lye DC Archuleta S Syed-Omar SF Low JG Oh HMWei Y et al Prophylactic platelet transfusion plussupportive care versus supportive care alone inadults with dengue and thrombocytopenia amulticentre open-label randomised superioritytrial Lancet 2017 389(10079) 1611-8 doi 101016S0140-6736(17)30269-6 PubMed PMID 28283286
19 Chinnappan S Ramachandrappa VS Tamilarasu KKrishnan UM Pillai AK Rajendiran S Inhibition ofPlatelet Aggregation by the Leaf Extract of Caricapapaya During Dengue Infection An In Vitro StudyViral immunology 2016 29(3) 164-8 doi 101089vim20150083 PubMed PMID 26910599
20 Charan J Saxena D Goyal JP Yasobant S Efficacyand safety of Carica papaya leaf extract in thedengue A systematic review and meta-analysis Int JAppl Basic Med Res 2016 6(4)249-54 doi 1041032229-516X192596 PubMed PMID 27857891PubMed Central PMCID PMCPMC5108100
21 Laoprasopwattana K Binsaai J Pruekprasert PGeater A Prothrombin Time Prolongation was theMost Important Indicator of Severe Bleeding inChildren with Severe Dengue Viral Infection Journalof Tropical Pediatrics 2017 63(4)314-20 doi101093tropejfmw097 PubMed PMID 28177091
22 Sureshkumar VK Vijayan D Kunhu S Mohamed ZThomas S Raman M Thromboelastographic Analysisof Hemostatic Abnormalities in Dengue PatientsAdmitted in a Multidisciplinary Intensive Care UnitA Cross-sectional Study Indian J Crit Care Med 201822(4)238-42 doi 104103ijccmIJCCM_486_17PubMed PMID 29743762 PubMed Central PMCIDPMCPMC5930527
23 Chuansumrit A Chaiyaratana W Hemostaticderangement in dengue hemorrhagic feverThrombosis Research 2014 133(1)10-6 doi101016jthromres201309028 PubMed PMID24120237
24 Wills B Tran VN Nguyen TH Truong TT Tran TN
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
The Sri Lanka Journal of Haematology4
HWCK Kulathilake SLJH 2018 10(1) 1-4
14 Buller HR Prins MH Lensin AW et al Oral riva-roxaban for the treatment of symptomatic pulmonaryembolism N Engl J Med 2012 366(14) 1287-97httpsdoiorg101056NEJMoa1113572PMid22449293
15 Patel MR Mahaffey KW Garg J et al Rivaroxabanversus warfarin in nonvalvular atrial fibrillation NEngl J Med 2011 365(10) 883-891 httpsdoiorg101056NEJMoa1009638 PMid21830957
16 Fox KA Piccini JP Wojdyla D et al Prevention ofstroke and systemic embolism with rivaroxabancompared with warfarin in patients with nonvalvularatrial fibrillation and moderate renal impairmentEur Heart J 2011 32(19) 2387-94 httpsdoiorg101093eurheartjehr342 PMid21873708
17 Connolly SJ Ezekowitz MD Yusuf S et al Dabigatranversus warfarin in patients with atrial fibrillationN Engl J Med 2009 361(12) 1139-51 httpsdoiorg101056NEJMoa0905561 PMid19717844
18 Wallentin L Yusuf S Ezekowitz MD et al Efficacyand safety of dabigatran compared with warfarin atdifferent levels of international normalised ratiocontrol for stroke prevention in atrial fibrillationan analysis of the RE-LY trial Lancet 2010 376(9745)975-83httpsdoi org101016S0140-6736(10)61194-4
19 Schulman S Kearon C Kakkar AK et al Dabigatranversus warfarin in the treatment of acute venous
thromboembolism N Engl J Med 2009 361(24)2342-52 httpsdoiorg101056NEJMoa0906598PMid19966341
20 Eriksson BI Dahl OE Rosencher N et al Oraldabigatran etexilate vs subcutaneous enoxaparinfor the prevention of venous thromboembolism aftertotal knee replacement the REMODEL randomizedtrial J Thromb Haemost 2007 5(11) 2178-85httpsdoiorg101111j1538-7836200702748xPMid 17764540
21 Ginsberg JS Davidson BL Comp PC et al Oralthrombin inhibitor dabigatran etexilate vs NorthAmerican enoxaparin regimen for prevention ofvenous thromboembolism after knee arthroplastysurgery J Arthroplast 2009 24(1) 1-9 httpsdoiorg101016jarth200801132 PMid18534438
22 Eriksson BI Dahl OE Rosencher N et al Dabigatranetexilate versus enoxaparin for prevention of venousthromboembolism after total hip replacement arandomised double-blind non inferiority trialLancet 2007 370(9591) 949-56 httpsdoiorg101016S0140-6736(07)61445-7
23 Eriksson BI Dahl OE Huo MH et al Oral dabigatranversus enoxaparin for thromboprophylaxis afterprimary total hip arthroplasty (RE-NOVATE II) arandomised double blind non nferiority trialThromb Haemost 2011 105(4)721-9 httpsdoiorg101160TH10-10-0679 PMid21225098
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 5
1Professor Centre for Dengue Research Universityof Sri Jayewardenepura Nugegoda Sri Lanka2Weatherall Institute of Molecular Medicine JohnRadcliffe Hospital Oxford OX3 9DS UK
Introduction
Dengue viral infections represent one of the mostrapidly emerging mosquito borne infections in theworld which causes 100 million apparent dengueinfections each year1 From 2005 to 2015 althoughthe mortality rates due to many infectious diseasesdecreased the deaths due to dengue increasedby 487 resulting in an estimated 18400 deathsin 20152 Although there is a dengue vaccine licensedto be used in children over the age of 9 years thevaccine manufacturer and other authorities havesuggested that this vaccine should be avoided inindividuals who have not been infected with thedengue virus (DENV) due to the likelihood ofdisease enhancement3
Although the majority of those who are infectedwith the DENV develop asymptomatic or milddisease 478 to 5072 of individuals have shownto develop severe dengue depending on the epi-demic serostatus and circulating DENV serotypesduring that epidemic4 Severe dengue is charac-terized by clinically detectable vascular leakagethat manifest in the form of pleural effusions andascites which can lead to haemodynamic insta-bility and shock5 In addition patients may alsodevelop complications such as bleeding mani-festations liver and renal dysfunction Althoughmild forms of bleeding manifestations such aspetechiae and bleeding from sites of venipunctureare seen in many patients with dengue haemor-rhagic fever (DHF) significant bleeding such as pervaginal bleeding haematuria haematemesis and
Predictors of bleeding in acute dengue virus infection
Gathsaurie Neelika Malavige12
Leading article
Key words dengue viral infection bleeding plasma leakage
malena can lead to haemodynamic instability andshock Development of significant bleeding wasshown to be an independent risk factor associatedwith fatalities in patients with DHF6 Gastrointestinalbleeding alone was shown to strongly associatewith the occurrence of death7
Association of plasma leakage and bleeding
While bleeding manifestations are sometimesseen in patients with dengue fever (DF) significantbleeding is usually seen in those who have severeplasma leakage prolonged shock or organ dys-function89 Severe vascular leakage leading to poorperfusion of the intestinal mucosa and organdysfunction are thought to be the predominantcauses of intestinal bleeding10 Our data has shownthat bleeding manifestations were more frequentamong dengue patients in Sri Lanka in the pastcompared to recent epidemics possibly due tobetter fluid management and reduction in thedevelopment of shock For instance in a study doneby us in year 2004 in adult patients 42108 (389)patients developed bleeding manifestations11whereas the only 26179 (145) developedbleeding manifestations in a patient cohortstudied in years 2016 and 201712 Therefore bettermanagement of fluid leakage appears to indirectlyreduce the incidence of bleeding in dengue
Thrombocytopenia and occurrence of bleeding
Although severe thrombocytopenia was found tobe a predictor of significant bleeding in denguethrombocytopenia alone in the absence of a highhematocrit or liver dysfunction was not associatedwith significant bleeding13 Direct infection ofplatelets by the DENV destruction of platelets dueto immune complexes and bone marrow sup-pression have shown to be the predominant factorsleading to thrombocytopenia (Figure 1)14 Apartfrom the reduction of platelet counts platelet
SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
6
function has also shown to be significantlyimpaired in patients with DHF including impairedplatelet aggregation in response to ADP9 This wasshown to be accompanied by an increase in plasma-thrombomodulin and platelet factor-4 whichindicate an increased secretory activity9 Impairedplatelet function and destruction has also beenobserved in transfused platelets which have ledto a marked reduction in survival rates of trans-fused platelets especially in those with DHF1415
Due to the presence of severe degrees of throm-bocytopenia in the past many centres have pro-phylactically transfused platelets in order toprevent development of any bleeding Howeverseveral retrospective studies had shown thatprophylactic platelet transfusions were associatedwith fluid overload and prolonged hospital staywithout any reduction in bleeding manifestationsor improved platelet recovery1617 In order toaddress this controversy a multi centre rando-mized controlled trial carried out in several centresin Singapore and Malaysia in patients with plateletcounts 20000 plateletsmicroL showed that pro-phylactic platelet transfusions did not reduce theoccurrence of bleeding18 Instead platelet trans-fusions were associated with an increase incidenceof adverse effects including those of seriousnature such as anaphylaxis and transfusion relatedacute lung injury18 Therefore both the WHOguidelines and the National dengue managementguidelines do not recommend platelet trans-fusions but have advocated blood transfusions inthose who are suspected to have developedsignificant bleeding
The effect of many herbal preparations such as theleave extract of Carica papaya in improving plateletcounts have been studied and in vitro evidencehave shown that this leaf extract reduces plateletaggregation19 Two multi-centre randomizeddouble blind placebo controlled trials using Caricapapaya in India showed that this leaf extract doessignificantly increase platelet counts initiallyalthough there was no significant difference inplatelet counts 48 hours after administration ofthe leaf extract20 However these trials had notassessed the efficacy of this leaf extract onreducing plasma leakage organ dysfunction and
mortality and have not reported any adverseeffects as is indicated in the standard reporting ofclinical trials20 Therefore as it is difficult toascertain the other possible benefits or adverseeffects of this drug it would be important toconduct proper clinical trials according to theinternationally recommended guidelines
Coagulation abnormalities leading to bleeding
Apart from the presence of prolonged shocksevere liver dysfunction is suggested as one the mostimportant predictors of severe bleeding21 Manyclotting factors such as factor V VII VIII IX and Xfibrinogen protein C and S and antithrombin aresynthesized by the liver and low levels of theseproteins are seen in patients with acute dengueAlthough thromboelastographic studies have alsodemonstrated deficiency of coagulation factorsand abnormalities in platelet function the levelswere not associated with the degree of thrombo-cytopenia or liver dysfunction22
Many patients with DHF have a prolongedprothrombin time prolonged INR and activatedpartial thromboplastin time (aPTT) It is thoughtthat these abnormalities possibly occur due to thereduced production of these factors and alsoleakage of these proteins into extravascular spacesacross the dysfunctional endothelium92123 Prolon-gation of the prothrombin time has been shownto be an important predictor of occurrence ofbleeding in patients with severe plasma leakage21Although many studies have reported an increasein partial thromboplastin times and reduction infibrinogen concentrations9 change in these para-meters correlated with the extent of vascularleakage and not with bleeding24 More detailedstudies which have assessed changes of theseproteins at different stages of the illness haveshown that protein C S and antithrombin III levelswere significantly lower in patients with moresevere degrees of shock during the leakagephase However as these proteins returned tonormal levels following the leakage phase it hasbeen suggested that leakage of these proteinsinto extravascular tissues could be the mainfactor leading to low levels in patients with DHF(Figure 1)9
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 7
Endothelial activation and bleeding in dengue
Patients with more severe forms of dengue arealso shown to have high levels of tissue factorthrombomodulin and plasminogen activatorinhibitor type 1 (PAI-1) which have been attri-buted to endothelial platelet and monocyteactivation9 Endothelial activation and injury is alsoreflected by high levels of von Willebrand factor(vWF) especially in patients with severe shock23It was also shown that the number of circulatingendothelial cells and soluble thrombomodulinlevels were significantly higher in patients withprofound shock further supporting that endo-thelial injury occurs in severe dengue23 Thromo-bomodulin which is an integral membrane proteinexpressed on endothelial cells monocytes andcertain dendritic cells is cofactor in activation of
protein C Although soluble thrombomodulinlevels were markedly high in those with severeforms plasma leakage as protein C levels are lowthe contribution to these pathways in causingsevere dengue and bleeding is not certain
Despite significant derangements in prothrom-botic antithrombotic and fibrinolytic pathways asmost patients do not develop bleeding it issuggested that the combinations of many factorssuch tissue hypoxia acidosis along with thrombo-cytopenia are important co-factors Howeverplasma leakage secondary endothelial dysfunctionappears to be the most important factor leading toshock poor organ perfusion organ dysfunctionderangement of many coagulation pathways andbleeding510 We have identified that plateletactivating factor (PAF) significantly contributed to
Bleeding manifestations are thought to occur due to the complex interplay of many factors such asendothelial dysfunction liver dysfunction and thrombocytopenia Endothelial dysfunction leads to plasmaleakage and when severe leads to shock poor organ perfusion and tissue hypoxia Tissue hypoxia in thegastrointestinal and possibly the lung epithelium is thought to be the main contributing factors forbleeding from these sites Many clotting factors and antithrombic factors are also thought to extravasatein to the tissues leading to low levels of these in the plasma In addition liver dysfunction may also leadto reduction in the production of these factors
Figure 1 Factors that contribute to bleeding in acute dengue infection
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
8
vascular leakage in dengue25 In addition lipidmediators that oppose the action of PAF andprotect the endothelial barrier integrity such assphingosine-1-phosphate was found to bemarkedly low in patients with DHF especiallyduring the critical phase26
As plasma leakage appears to be the most impor-tant factor leading to all complications of dengueit would be reasonable to use drugs that preventor reduce vascular leakage as a suitable option toreduce severe dengue and associated compli-cations We have concluded a phase 2 randomizedplacebo controlled clinical trial in 183 patients atthe National Institute of Infectious Diseases SriLanka using a PAF receptor blocker known asrupatadine27 In this clinical trial we found thatrupatadine up to 40mg daily appeared safe andwell-tolerated in patients with acute dengue Inaddition patients given rupatadine had higherplatelet counts and lower aspartate-aminotrans-ferase levels during the critical phase and signifi-cantly smaller pleural effusions27 The develop-ment of significant bleeding manifestations suchas per vaginal bleeding and gastrointestinalbleeding was also lower in the group who receivedtreatment As the beneficial effects of this drugappeared to be greater when given early in theillness we are currently conducting another trialwhich is double blind randomized placebocontrolled trial in a larger cohort of patientsAlthough the initial trial showed promising resultsthese results should be interpreted with cautionuntil the same beneficial effects are seen in largertrials that we are currently carrying out
Summary
Endothelial dysfunction leading to plasma leakageappears to be the most important predictor ofoccurrence of bleeding in acute dengue Althoughthrombocytopenia is a risk factor of bleeding indengue thrombocytopenia alone was notassociated with bleeding in the absence of plasmaleakage Many abnormalities in the coagulationpathways are seen in severe dengue which appearto return to normal during the recovery phaseThese coagulation abnormalities have beenassociated with the degree of plasma leakage As
References
1 Bhatt S Gething PW Brady OJ Messina JP FarlowAW Moyes CL et al The global distribution andburden of dengue Nature 2013 496(7446) 504-7Epub 20130409 doi 101038nature12060 PubMedPMID 23563266 PubMed Central PMCIDPMC3651993
2 Mortality GBD Causes of Death C Global regionaland national life expectancy all-cause mortality andcause-specific mortality for 249 causes of death1980-2015 a systematic analysis for the GlobalBurden of Disease Study 2015 Lancet 2016388(10053) 1459-544 doi 101016S0140-6736(16)31012-1 PubMed PMID 27733281
3 Rouvinski A Guardado-Calvo P Barba-Spaeth GDuquerroy S Vaney MC Kikuti CM et al Recognitiondeterminants of broadly neutralizing humanantibodies against dengue viruses Nature 2015520(7545) 109-13 doi 101038nature14130PubMed PMID 25581790
4 Soo KM Khalid B Ching SM Chee HY Meta-Analysisof Dengue Severity during Infection by DifferentDengue Virus Serotypes in Primary and SecondaryInfections PloS one 2016 11(5) e0154760doi 101371journalpone02154760 PubMed PMID27213782 PubMed Central PMCID PMCPMC4877104
5 Malavige GN Ogg GS Pathogenesis of vascular leakin dengue virus infection Immunology 2017 151(3)261-9 doi 101111imm12748 PubMed PMID28437586 PubMed Central PMCID PMCPMC5461104
Authorship
Contribution This is the sole work of ProfGathsaurie Neelika Malavige
Conflict-of-interest disclosure The author declaresno conflict of interest
Correspondence Prof Gathsaurie Neelika MalavigeDPhil FRCP (Lond) FRCPath (UK)Centre for Dengue Research Faculty of MedicalSciences University of Sri Jayawardanapura SriLanka
E-mail gathsauriemalavigendmoxacuk
bleeding manifestations appear to best correlatewith the degree of leakage proper and meticulousfluid management would be the most importantmeasure in preventing bleeding manifestations
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 9
6 Md-Sani SS Md-Noor J Han WH Gan SP Rani NS TanHL et al Prediction of mortality in severe denguecases BMC infectious diseases 2018 18(1) 232 doi101186s12879-018-3141-6 PubMed PMID29783955
7 Pinto RC Castro DB Albuquerque BC Sampaio Vde SPassos RA Costa CF et al Mortality Predictors inPatients with Severe Dengue in the State of AmazonasBrazil PloS one 2016 11(8)e0161884 doi 101371journalpone0161884 PubMed PMID 27564084PubMed Central PMCID PMCPMC5001629
8 Sam SS Omar SF Teoh BT Abd-Jamil J AbuBakar SReview of Dengue hemorrhagic fever fatal cases seenamong adults a retrospective study PLoS neglectedtropical diseases 2013 7(5)e2194 doi 101371journalpntd0002194 PubMed PMID 23658849PubMed Central PMCID PMCPMC3642057
9 Wills BA Oragui EE Stephens AC Daramola OA DungNM Loan HT et al Coagulation abnormalities indengue hemorrhagic Fever serial investigations in167 Vietnamese children with Dengue shocksyndrome Clin Infect Dis 2002 35(3) 277-85 Epub20020713 doi 101086341410 PubMed PMID12115093
10 WHO editor Comprehensive guidelines forprevention and control of dengue fever and denguehaemorrhagic fever SEARO New Delhi India WorldHealth Organization 2011
11 Malavige GN Velathanthiri VG Wijewickrama ESFernando S Jayaratne SD Aaskov J et al Patterns ofdisease among adults hospitalized with dengueinfections Qjm 2006 99(5) 299-305 PubMed PMID16603571
12 Wijewickrama A FS Jayerathne PGSB Perera MAPAAbeynaike SA Gomes L Jeewandara C Malavige GNEffect of change in serotype on clinical severity ofdengue infections In SLMA editor Annual Con-ference of the Sri Lanka Medical AssociationColombo SLMA 2017
13 Wong JG Thein TL Leo YS Pang J Lye DC IdentifyingAdult Dengue Patients at Low Risk for ClinicallySignificant Bleeding PloS one 2016 11(2) e0148579doi 101371journalpone0148579 PubMed PMID26849556 PubMed Central PMCID PMCPMC4743958
14 Ojha A Nandi D Batra H Singhal R Annarapu GKBhattacharyya S et al Platelet activation determinesthe severity of thrombocytopenia in dengue infectionSci Rep 2017 7 41697 doi 101038srep41697PubMed PMID 28139770 PubMed Central PMCIDPMCPMC5282509
15 Isarangkura P Tuchinda S The behavior of transfused
platelets in dengue hemorrhagic fever The SoutheastAsian Journal of Tropical Medicine and Public Health1993 24 Suppl 1 222-4 PubMed PMID 7886581
16 Lum LC Abdel-Latif Mel A Goh AY Chan PW Lam SKPreventive transfusion in Dengue shock syndrome-is it necessary The Journal of Pediatrics 2003143(5) 682-4 PubMed PMID 14615749
17 Lye DC Lee VJ Sun Y Leo YS Lack of efficacy ofprophylactic platelet transfusion for severethrombocytopenia in adults with acute uncom-plicated dengue infection Clin Infect Dis 2009 48(9)1262-5 PubMed PMID 19292665
18 Lye DC Archuleta S Syed-Omar SF Low JG Oh HMWei Y et al Prophylactic platelet transfusion plussupportive care versus supportive care alone inadults with dengue and thrombocytopenia amulticentre open-label randomised superioritytrial Lancet 2017 389(10079) 1611-8 doi 101016S0140-6736(17)30269-6 PubMed PMID 28283286
19 Chinnappan S Ramachandrappa VS Tamilarasu KKrishnan UM Pillai AK Rajendiran S Inhibition ofPlatelet Aggregation by the Leaf Extract of Caricapapaya During Dengue Infection An In Vitro StudyViral immunology 2016 29(3) 164-8 doi 101089vim20150083 PubMed PMID 26910599
20 Charan J Saxena D Goyal JP Yasobant S Efficacyand safety of Carica papaya leaf extract in thedengue A systematic review and meta-analysis Int JAppl Basic Med Res 2016 6(4)249-54 doi 1041032229-516X192596 PubMed PMID 27857891PubMed Central PMCID PMCPMC5108100
21 Laoprasopwattana K Binsaai J Pruekprasert PGeater A Prothrombin Time Prolongation was theMost Important Indicator of Severe Bleeding inChildren with Severe Dengue Viral Infection Journalof Tropical Pediatrics 2017 63(4)314-20 doi101093tropejfmw097 PubMed PMID 28177091
22 Sureshkumar VK Vijayan D Kunhu S Mohamed ZThomas S Raman M Thromboelastographic Analysisof Hemostatic Abnormalities in Dengue PatientsAdmitted in a Multidisciplinary Intensive Care UnitA Cross-sectional Study Indian J Crit Care Med 201822(4)238-42 doi 104103ijccmIJCCM_486_17PubMed PMID 29743762 PubMed Central PMCIDPMCPMC5930527
23 Chuansumrit A Chaiyaratana W Hemostaticderangement in dengue hemorrhagic feverThrombosis Research 2014 133(1)10-6 doi101016jthromres201309028 PubMed PMID24120237
24 Wills B Tran VN Nguyen TH Truong TT Tran TN
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 5
1Professor Centre for Dengue Research Universityof Sri Jayewardenepura Nugegoda Sri Lanka2Weatherall Institute of Molecular Medicine JohnRadcliffe Hospital Oxford OX3 9DS UK
Introduction
Dengue viral infections represent one of the mostrapidly emerging mosquito borne infections in theworld which causes 100 million apparent dengueinfections each year1 From 2005 to 2015 althoughthe mortality rates due to many infectious diseasesdecreased the deaths due to dengue increasedby 487 resulting in an estimated 18400 deathsin 20152 Although there is a dengue vaccine licensedto be used in children over the age of 9 years thevaccine manufacturer and other authorities havesuggested that this vaccine should be avoided inindividuals who have not been infected with thedengue virus (DENV) due to the likelihood ofdisease enhancement3
Although the majority of those who are infectedwith the DENV develop asymptomatic or milddisease 478 to 5072 of individuals have shownto develop severe dengue depending on the epi-demic serostatus and circulating DENV serotypesduring that epidemic4 Severe dengue is charac-terized by clinically detectable vascular leakagethat manifest in the form of pleural effusions andascites which can lead to haemodynamic insta-bility and shock5 In addition patients may alsodevelop complications such as bleeding mani-festations liver and renal dysfunction Althoughmild forms of bleeding manifestations such aspetechiae and bleeding from sites of venipunctureare seen in many patients with dengue haemor-rhagic fever (DHF) significant bleeding such as pervaginal bleeding haematuria haematemesis and
Predictors of bleeding in acute dengue virus infection
Gathsaurie Neelika Malavige12
Leading article
Key words dengue viral infection bleeding plasma leakage
malena can lead to haemodynamic instability andshock Development of significant bleeding wasshown to be an independent risk factor associatedwith fatalities in patients with DHF6 Gastrointestinalbleeding alone was shown to strongly associatewith the occurrence of death7
Association of plasma leakage and bleeding
While bleeding manifestations are sometimesseen in patients with dengue fever (DF) significantbleeding is usually seen in those who have severeplasma leakage prolonged shock or organ dys-function89 Severe vascular leakage leading to poorperfusion of the intestinal mucosa and organdysfunction are thought to be the predominantcauses of intestinal bleeding10 Our data has shownthat bleeding manifestations were more frequentamong dengue patients in Sri Lanka in the pastcompared to recent epidemics possibly due tobetter fluid management and reduction in thedevelopment of shock For instance in a study doneby us in year 2004 in adult patients 42108 (389)patients developed bleeding manifestations11whereas the only 26179 (145) developedbleeding manifestations in a patient cohortstudied in years 2016 and 201712 Therefore bettermanagement of fluid leakage appears to indirectlyreduce the incidence of bleeding in dengue
Thrombocytopenia and occurrence of bleeding
Although severe thrombocytopenia was found tobe a predictor of significant bleeding in denguethrombocytopenia alone in the absence of a highhematocrit or liver dysfunction was not associatedwith significant bleeding13 Direct infection ofplatelets by the DENV destruction of platelets dueto immune complexes and bone marrow sup-pression have shown to be the predominant factorsleading to thrombocytopenia (Figure 1)14 Apartfrom the reduction of platelet counts platelet
SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
6
function has also shown to be significantlyimpaired in patients with DHF including impairedplatelet aggregation in response to ADP9 This wasshown to be accompanied by an increase in plasma-thrombomodulin and platelet factor-4 whichindicate an increased secretory activity9 Impairedplatelet function and destruction has also beenobserved in transfused platelets which have ledto a marked reduction in survival rates of trans-fused platelets especially in those with DHF1415
Due to the presence of severe degrees of throm-bocytopenia in the past many centres have pro-phylactically transfused platelets in order toprevent development of any bleeding Howeverseveral retrospective studies had shown thatprophylactic platelet transfusions were associatedwith fluid overload and prolonged hospital staywithout any reduction in bleeding manifestationsor improved platelet recovery1617 In order toaddress this controversy a multi centre rando-mized controlled trial carried out in several centresin Singapore and Malaysia in patients with plateletcounts 20000 plateletsmicroL showed that pro-phylactic platelet transfusions did not reduce theoccurrence of bleeding18 Instead platelet trans-fusions were associated with an increase incidenceof adverse effects including those of seriousnature such as anaphylaxis and transfusion relatedacute lung injury18 Therefore both the WHOguidelines and the National dengue managementguidelines do not recommend platelet trans-fusions but have advocated blood transfusions inthose who are suspected to have developedsignificant bleeding
The effect of many herbal preparations such as theleave extract of Carica papaya in improving plateletcounts have been studied and in vitro evidencehave shown that this leaf extract reduces plateletaggregation19 Two multi-centre randomizeddouble blind placebo controlled trials using Caricapapaya in India showed that this leaf extract doessignificantly increase platelet counts initiallyalthough there was no significant difference inplatelet counts 48 hours after administration ofthe leaf extract20 However these trials had notassessed the efficacy of this leaf extract onreducing plasma leakage organ dysfunction and
mortality and have not reported any adverseeffects as is indicated in the standard reporting ofclinical trials20 Therefore as it is difficult toascertain the other possible benefits or adverseeffects of this drug it would be important toconduct proper clinical trials according to theinternationally recommended guidelines
Coagulation abnormalities leading to bleeding
Apart from the presence of prolonged shocksevere liver dysfunction is suggested as one the mostimportant predictors of severe bleeding21 Manyclotting factors such as factor V VII VIII IX and Xfibrinogen protein C and S and antithrombin aresynthesized by the liver and low levels of theseproteins are seen in patients with acute dengueAlthough thromboelastographic studies have alsodemonstrated deficiency of coagulation factorsand abnormalities in platelet function the levelswere not associated with the degree of thrombo-cytopenia or liver dysfunction22
Many patients with DHF have a prolongedprothrombin time prolonged INR and activatedpartial thromboplastin time (aPTT) It is thoughtthat these abnormalities possibly occur due to thereduced production of these factors and alsoleakage of these proteins into extravascular spacesacross the dysfunctional endothelium92123 Prolon-gation of the prothrombin time has been shownto be an important predictor of occurrence ofbleeding in patients with severe plasma leakage21Although many studies have reported an increasein partial thromboplastin times and reduction infibrinogen concentrations9 change in these para-meters correlated with the extent of vascularleakage and not with bleeding24 More detailedstudies which have assessed changes of theseproteins at different stages of the illness haveshown that protein C S and antithrombin III levelswere significantly lower in patients with moresevere degrees of shock during the leakagephase However as these proteins returned tonormal levels following the leakage phase it hasbeen suggested that leakage of these proteinsinto extravascular tissues could be the mainfactor leading to low levels in patients with DHF(Figure 1)9
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 7
Endothelial activation and bleeding in dengue
Patients with more severe forms of dengue arealso shown to have high levels of tissue factorthrombomodulin and plasminogen activatorinhibitor type 1 (PAI-1) which have been attri-buted to endothelial platelet and monocyteactivation9 Endothelial activation and injury is alsoreflected by high levels of von Willebrand factor(vWF) especially in patients with severe shock23It was also shown that the number of circulatingendothelial cells and soluble thrombomodulinlevels were significantly higher in patients withprofound shock further supporting that endo-thelial injury occurs in severe dengue23 Thromo-bomodulin which is an integral membrane proteinexpressed on endothelial cells monocytes andcertain dendritic cells is cofactor in activation of
protein C Although soluble thrombomodulinlevels were markedly high in those with severeforms plasma leakage as protein C levels are lowthe contribution to these pathways in causingsevere dengue and bleeding is not certain
Despite significant derangements in prothrom-botic antithrombotic and fibrinolytic pathways asmost patients do not develop bleeding it issuggested that the combinations of many factorssuch tissue hypoxia acidosis along with thrombo-cytopenia are important co-factors Howeverplasma leakage secondary endothelial dysfunctionappears to be the most important factor leading toshock poor organ perfusion organ dysfunctionderangement of many coagulation pathways andbleeding510 We have identified that plateletactivating factor (PAF) significantly contributed to
Bleeding manifestations are thought to occur due to the complex interplay of many factors such asendothelial dysfunction liver dysfunction and thrombocytopenia Endothelial dysfunction leads to plasmaleakage and when severe leads to shock poor organ perfusion and tissue hypoxia Tissue hypoxia in thegastrointestinal and possibly the lung epithelium is thought to be the main contributing factors forbleeding from these sites Many clotting factors and antithrombic factors are also thought to extravasatein to the tissues leading to low levels of these in the plasma In addition liver dysfunction may also leadto reduction in the production of these factors
Figure 1 Factors that contribute to bleeding in acute dengue infection
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
8
vascular leakage in dengue25 In addition lipidmediators that oppose the action of PAF andprotect the endothelial barrier integrity such assphingosine-1-phosphate was found to bemarkedly low in patients with DHF especiallyduring the critical phase26
As plasma leakage appears to be the most impor-tant factor leading to all complications of dengueit would be reasonable to use drugs that preventor reduce vascular leakage as a suitable option toreduce severe dengue and associated compli-cations We have concluded a phase 2 randomizedplacebo controlled clinical trial in 183 patients atthe National Institute of Infectious Diseases SriLanka using a PAF receptor blocker known asrupatadine27 In this clinical trial we found thatrupatadine up to 40mg daily appeared safe andwell-tolerated in patients with acute dengue Inaddition patients given rupatadine had higherplatelet counts and lower aspartate-aminotrans-ferase levels during the critical phase and signifi-cantly smaller pleural effusions27 The develop-ment of significant bleeding manifestations suchas per vaginal bleeding and gastrointestinalbleeding was also lower in the group who receivedtreatment As the beneficial effects of this drugappeared to be greater when given early in theillness we are currently conducting another trialwhich is double blind randomized placebocontrolled trial in a larger cohort of patientsAlthough the initial trial showed promising resultsthese results should be interpreted with cautionuntil the same beneficial effects are seen in largertrials that we are currently carrying out
Summary
Endothelial dysfunction leading to plasma leakageappears to be the most important predictor ofoccurrence of bleeding in acute dengue Althoughthrombocytopenia is a risk factor of bleeding indengue thrombocytopenia alone was notassociated with bleeding in the absence of plasmaleakage Many abnormalities in the coagulationpathways are seen in severe dengue which appearto return to normal during the recovery phaseThese coagulation abnormalities have beenassociated with the degree of plasma leakage As
References
1 Bhatt S Gething PW Brady OJ Messina JP FarlowAW Moyes CL et al The global distribution andburden of dengue Nature 2013 496(7446) 504-7Epub 20130409 doi 101038nature12060 PubMedPMID 23563266 PubMed Central PMCIDPMC3651993
2 Mortality GBD Causes of Death C Global regionaland national life expectancy all-cause mortality andcause-specific mortality for 249 causes of death1980-2015 a systematic analysis for the GlobalBurden of Disease Study 2015 Lancet 2016388(10053) 1459-544 doi 101016S0140-6736(16)31012-1 PubMed PMID 27733281
3 Rouvinski A Guardado-Calvo P Barba-Spaeth GDuquerroy S Vaney MC Kikuti CM et al Recognitiondeterminants of broadly neutralizing humanantibodies against dengue viruses Nature 2015520(7545) 109-13 doi 101038nature14130PubMed PMID 25581790
4 Soo KM Khalid B Ching SM Chee HY Meta-Analysisof Dengue Severity during Infection by DifferentDengue Virus Serotypes in Primary and SecondaryInfections PloS one 2016 11(5) e0154760doi 101371journalpone02154760 PubMed PMID27213782 PubMed Central PMCID PMCPMC4877104
5 Malavige GN Ogg GS Pathogenesis of vascular leakin dengue virus infection Immunology 2017 151(3)261-9 doi 101111imm12748 PubMed PMID28437586 PubMed Central PMCID PMCPMC5461104
Authorship
Contribution This is the sole work of ProfGathsaurie Neelika Malavige
Conflict-of-interest disclosure The author declaresno conflict of interest
Correspondence Prof Gathsaurie Neelika MalavigeDPhil FRCP (Lond) FRCPath (UK)Centre for Dengue Research Faculty of MedicalSciences University of Sri Jayawardanapura SriLanka
E-mail gathsauriemalavigendmoxacuk
bleeding manifestations appear to best correlatewith the degree of leakage proper and meticulousfluid management would be the most importantmeasure in preventing bleeding manifestations
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 9
6 Md-Sani SS Md-Noor J Han WH Gan SP Rani NS TanHL et al Prediction of mortality in severe denguecases BMC infectious diseases 2018 18(1) 232 doi101186s12879-018-3141-6 PubMed PMID29783955
7 Pinto RC Castro DB Albuquerque BC Sampaio Vde SPassos RA Costa CF et al Mortality Predictors inPatients with Severe Dengue in the State of AmazonasBrazil PloS one 2016 11(8)e0161884 doi 101371journalpone0161884 PubMed PMID 27564084PubMed Central PMCID PMCPMC5001629
8 Sam SS Omar SF Teoh BT Abd-Jamil J AbuBakar SReview of Dengue hemorrhagic fever fatal cases seenamong adults a retrospective study PLoS neglectedtropical diseases 2013 7(5)e2194 doi 101371journalpntd0002194 PubMed PMID 23658849PubMed Central PMCID PMCPMC3642057
9 Wills BA Oragui EE Stephens AC Daramola OA DungNM Loan HT et al Coagulation abnormalities indengue hemorrhagic Fever serial investigations in167 Vietnamese children with Dengue shocksyndrome Clin Infect Dis 2002 35(3) 277-85 Epub20020713 doi 101086341410 PubMed PMID12115093
10 WHO editor Comprehensive guidelines forprevention and control of dengue fever and denguehaemorrhagic fever SEARO New Delhi India WorldHealth Organization 2011
11 Malavige GN Velathanthiri VG Wijewickrama ESFernando S Jayaratne SD Aaskov J et al Patterns ofdisease among adults hospitalized with dengueinfections Qjm 2006 99(5) 299-305 PubMed PMID16603571
12 Wijewickrama A FS Jayerathne PGSB Perera MAPAAbeynaike SA Gomes L Jeewandara C Malavige GNEffect of change in serotype on clinical severity ofdengue infections In SLMA editor Annual Con-ference of the Sri Lanka Medical AssociationColombo SLMA 2017
13 Wong JG Thein TL Leo YS Pang J Lye DC IdentifyingAdult Dengue Patients at Low Risk for ClinicallySignificant Bleeding PloS one 2016 11(2) e0148579doi 101371journalpone0148579 PubMed PMID26849556 PubMed Central PMCID PMCPMC4743958
14 Ojha A Nandi D Batra H Singhal R Annarapu GKBhattacharyya S et al Platelet activation determinesthe severity of thrombocytopenia in dengue infectionSci Rep 2017 7 41697 doi 101038srep41697PubMed PMID 28139770 PubMed Central PMCIDPMCPMC5282509
15 Isarangkura P Tuchinda S The behavior of transfused
platelets in dengue hemorrhagic fever The SoutheastAsian Journal of Tropical Medicine and Public Health1993 24 Suppl 1 222-4 PubMed PMID 7886581
16 Lum LC Abdel-Latif Mel A Goh AY Chan PW Lam SKPreventive transfusion in Dengue shock syndrome-is it necessary The Journal of Pediatrics 2003143(5) 682-4 PubMed PMID 14615749
17 Lye DC Lee VJ Sun Y Leo YS Lack of efficacy ofprophylactic platelet transfusion for severethrombocytopenia in adults with acute uncom-plicated dengue infection Clin Infect Dis 2009 48(9)1262-5 PubMed PMID 19292665
18 Lye DC Archuleta S Syed-Omar SF Low JG Oh HMWei Y et al Prophylactic platelet transfusion plussupportive care versus supportive care alone inadults with dengue and thrombocytopenia amulticentre open-label randomised superioritytrial Lancet 2017 389(10079) 1611-8 doi 101016S0140-6736(17)30269-6 PubMed PMID 28283286
19 Chinnappan S Ramachandrappa VS Tamilarasu KKrishnan UM Pillai AK Rajendiran S Inhibition ofPlatelet Aggregation by the Leaf Extract of Caricapapaya During Dengue Infection An In Vitro StudyViral immunology 2016 29(3) 164-8 doi 101089vim20150083 PubMed PMID 26910599
20 Charan J Saxena D Goyal JP Yasobant S Efficacyand safety of Carica papaya leaf extract in thedengue A systematic review and meta-analysis Int JAppl Basic Med Res 2016 6(4)249-54 doi 1041032229-516X192596 PubMed PMID 27857891PubMed Central PMCID PMCPMC5108100
21 Laoprasopwattana K Binsaai J Pruekprasert PGeater A Prothrombin Time Prolongation was theMost Important Indicator of Severe Bleeding inChildren with Severe Dengue Viral Infection Journalof Tropical Pediatrics 2017 63(4)314-20 doi101093tropejfmw097 PubMed PMID 28177091
22 Sureshkumar VK Vijayan D Kunhu S Mohamed ZThomas S Raman M Thromboelastographic Analysisof Hemostatic Abnormalities in Dengue PatientsAdmitted in a Multidisciplinary Intensive Care UnitA Cross-sectional Study Indian J Crit Care Med 201822(4)238-42 doi 104103ijccmIJCCM_486_17PubMed PMID 29743762 PubMed Central PMCIDPMCPMC5930527
23 Chuansumrit A Chaiyaratana W Hemostaticderangement in dengue hemorrhagic feverThrombosis Research 2014 133(1)10-6 doi101016jthromres201309028 PubMed PMID24120237
24 Wills B Tran VN Nguyen TH Truong TT Tran TN
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
6
function has also shown to be significantlyimpaired in patients with DHF including impairedplatelet aggregation in response to ADP9 This wasshown to be accompanied by an increase in plasma-thrombomodulin and platelet factor-4 whichindicate an increased secretory activity9 Impairedplatelet function and destruction has also beenobserved in transfused platelets which have ledto a marked reduction in survival rates of trans-fused platelets especially in those with DHF1415
Due to the presence of severe degrees of throm-bocytopenia in the past many centres have pro-phylactically transfused platelets in order toprevent development of any bleeding Howeverseveral retrospective studies had shown thatprophylactic platelet transfusions were associatedwith fluid overload and prolonged hospital staywithout any reduction in bleeding manifestationsor improved platelet recovery1617 In order toaddress this controversy a multi centre rando-mized controlled trial carried out in several centresin Singapore and Malaysia in patients with plateletcounts 20000 plateletsmicroL showed that pro-phylactic platelet transfusions did not reduce theoccurrence of bleeding18 Instead platelet trans-fusions were associated with an increase incidenceof adverse effects including those of seriousnature such as anaphylaxis and transfusion relatedacute lung injury18 Therefore both the WHOguidelines and the National dengue managementguidelines do not recommend platelet trans-fusions but have advocated blood transfusions inthose who are suspected to have developedsignificant bleeding
The effect of many herbal preparations such as theleave extract of Carica papaya in improving plateletcounts have been studied and in vitro evidencehave shown that this leaf extract reduces plateletaggregation19 Two multi-centre randomizeddouble blind placebo controlled trials using Caricapapaya in India showed that this leaf extract doessignificantly increase platelet counts initiallyalthough there was no significant difference inplatelet counts 48 hours after administration ofthe leaf extract20 However these trials had notassessed the efficacy of this leaf extract onreducing plasma leakage organ dysfunction and
mortality and have not reported any adverseeffects as is indicated in the standard reporting ofclinical trials20 Therefore as it is difficult toascertain the other possible benefits or adverseeffects of this drug it would be important toconduct proper clinical trials according to theinternationally recommended guidelines
Coagulation abnormalities leading to bleeding
Apart from the presence of prolonged shocksevere liver dysfunction is suggested as one the mostimportant predictors of severe bleeding21 Manyclotting factors such as factor V VII VIII IX and Xfibrinogen protein C and S and antithrombin aresynthesized by the liver and low levels of theseproteins are seen in patients with acute dengueAlthough thromboelastographic studies have alsodemonstrated deficiency of coagulation factorsand abnormalities in platelet function the levelswere not associated with the degree of thrombo-cytopenia or liver dysfunction22
Many patients with DHF have a prolongedprothrombin time prolonged INR and activatedpartial thromboplastin time (aPTT) It is thoughtthat these abnormalities possibly occur due to thereduced production of these factors and alsoleakage of these proteins into extravascular spacesacross the dysfunctional endothelium92123 Prolon-gation of the prothrombin time has been shownto be an important predictor of occurrence ofbleeding in patients with severe plasma leakage21Although many studies have reported an increasein partial thromboplastin times and reduction infibrinogen concentrations9 change in these para-meters correlated with the extent of vascularleakage and not with bleeding24 More detailedstudies which have assessed changes of theseproteins at different stages of the illness haveshown that protein C S and antithrombin III levelswere significantly lower in patients with moresevere degrees of shock during the leakagephase However as these proteins returned tonormal levels following the leakage phase it hasbeen suggested that leakage of these proteinsinto extravascular tissues could be the mainfactor leading to low levels in patients with DHF(Figure 1)9
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 7
Endothelial activation and bleeding in dengue
Patients with more severe forms of dengue arealso shown to have high levels of tissue factorthrombomodulin and plasminogen activatorinhibitor type 1 (PAI-1) which have been attri-buted to endothelial platelet and monocyteactivation9 Endothelial activation and injury is alsoreflected by high levels of von Willebrand factor(vWF) especially in patients with severe shock23It was also shown that the number of circulatingendothelial cells and soluble thrombomodulinlevels were significantly higher in patients withprofound shock further supporting that endo-thelial injury occurs in severe dengue23 Thromo-bomodulin which is an integral membrane proteinexpressed on endothelial cells monocytes andcertain dendritic cells is cofactor in activation of
protein C Although soluble thrombomodulinlevels were markedly high in those with severeforms plasma leakage as protein C levels are lowthe contribution to these pathways in causingsevere dengue and bleeding is not certain
Despite significant derangements in prothrom-botic antithrombotic and fibrinolytic pathways asmost patients do not develop bleeding it issuggested that the combinations of many factorssuch tissue hypoxia acidosis along with thrombo-cytopenia are important co-factors Howeverplasma leakage secondary endothelial dysfunctionappears to be the most important factor leading toshock poor organ perfusion organ dysfunctionderangement of many coagulation pathways andbleeding510 We have identified that plateletactivating factor (PAF) significantly contributed to
Bleeding manifestations are thought to occur due to the complex interplay of many factors such asendothelial dysfunction liver dysfunction and thrombocytopenia Endothelial dysfunction leads to plasmaleakage and when severe leads to shock poor organ perfusion and tissue hypoxia Tissue hypoxia in thegastrointestinal and possibly the lung epithelium is thought to be the main contributing factors forbleeding from these sites Many clotting factors and antithrombic factors are also thought to extravasatein to the tissues leading to low levels of these in the plasma In addition liver dysfunction may also leadto reduction in the production of these factors
Figure 1 Factors that contribute to bleeding in acute dengue infection
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
8
vascular leakage in dengue25 In addition lipidmediators that oppose the action of PAF andprotect the endothelial barrier integrity such assphingosine-1-phosphate was found to bemarkedly low in patients with DHF especiallyduring the critical phase26
As plasma leakage appears to be the most impor-tant factor leading to all complications of dengueit would be reasonable to use drugs that preventor reduce vascular leakage as a suitable option toreduce severe dengue and associated compli-cations We have concluded a phase 2 randomizedplacebo controlled clinical trial in 183 patients atthe National Institute of Infectious Diseases SriLanka using a PAF receptor blocker known asrupatadine27 In this clinical trial we found thatrupatadine up to 40mg daily appeared safe andwell-tolerated in patients with acute dengue Inaddition patients given rupatadine had higherplatelet counts and lower aspartate-aminotrans-ferase levels during the critical phase and signifi-cantly smaller pleural effusions27 The develop-ment of significant bleeding manifestations suchas per vaginal bleeding and gastrointestinalbleeding was also lower in the group who receivedtreatment As the beneficial effects of this drugappeared to be greater when given early in theillness we are currently conducting another trialwhich is double blind randomized placebocontrolled trial in a larger cohort of patientsAlthough the initial trial showed promising resultsthese results should be interpreted with cautionuntil the same beneficial effects are seen in largertrials that we are currently carrying out
Summary
Endothelial dysfunction leading to plasma leakageappears to be the most important predictor ofoccurrence of bleeding in acute dengue Althoughthrombocytopenia is a risk factor of bleeding indengue thrombocytopenia alone was notassociated with bleeding in the absence of plasmaleakage Many abnormalities in the coagulationpathways are seen in severe dengue which appearto return to normal during the recovery phaseThese coagulation abnormalities have beenassociated with the degree of plasma leakage As
References
1 Bhatt S Gething PW Brady OJ Messina JP FarlowAW Moyes CL et al The global distribution andburden of dengue Nature 2013 496(7446) 504-7Epub 20130409 doi 101038nature12060 PubMedPMID 23563266 PubMed Central PMCIDPMC3651993
2 Mortality GBD Causes of Death C Global regionaland national life expectancy all-cause mortality andcause-specific mortality for 249 causes of death1980-2015 a systematic analysis for the GlobalBurden of Disease Study 2015 Lancet 2016388(10053) 1459-544 doi 101016S0140-6736(16)31012-1 PubMed PMID 27733281
3 Rouvinski A Guardado-Calvo P Barba-Spaeth GDuquerroy S Vaney MC Kikuti CM et al Recognitiondeterminants of broadly neutralizing humanantibodies against dengue viruses Nature 2015520(7545) 109-13 doi 101038nature14130PubMed PMID 25581790
4 Soo KM Khalid B Ching SM Chee HY Meta-Analysisof Dengue Severity during Infection by DifferentDengue Virus Serotypes in Primary and SecondaryInfections PloS one 2016 11(5) e0154760doi 101371journalpone02154760 PubMed PMID27213782 PubMed Central PMCID PMCPMC4877104
5 Malavige GN Ogg GS Pathogenesis of vascular leakin dengue virus infection Immunology 2017 151(3)261-9 doi 101111imm12748 PubMed PMID28437586 PubMed Central PMCID PMCPMC5461104
Authorship
Contribution This is the sole work of ProfGathsaurie Neelika Malavige
Conflict-of-interest disclosure The author declaresno conflict of interest
Correspondence Prof Gathsaurie Neelika MalavigeDPhil FRCP (Lond) FRCPath (UK)Centre for Dengue Research Faculty of MedicalSciences University of Sri Jayawardanapura SriLanka
E-mail gathsauriemalavigendmoxacuk
bleeding manifestations appear to best correlatewith the degree of leakage proper and meticulousfluid management would be the most importantmeasure in preventing bleeding manifestations
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 9
6 Md-Sani SS Md-Noor J Han WH Gan SP Rani NS TanHL et al Prediction of mortality in severe denguecases BMC infectious diseases 2018 18(1) 232 doi101186s12879-018-3141-6 PubMed PMID29783955
7 Pinto RC Castro DB Albuquerque BC Sampaio Vde SPassos RA Costa CF et al Mortality Predictors inPatients with Severe Dengue in the State of AmazonasBrazil PloS one 2016 11(8)e0161884 doi 101371journalpone0161884 PubMed PMID 27564084PubMed Central PMCID PMCPMC5001629
8 Sam SS Omar SF Teoh BT Abd-Jamil J AbuBakar SReview of Dengue hemorrhagic fever fatal cases seenamong adults a retrospective study PLoS neglectedtropical diseases 2013 7(5)e2194 doi 101371journalpntd0002194 PubMed PMID 23658849PubMed Central PMCID PMCPMC3642057
9 Wills BA Oragui EE Stephens AC Daramola OA DungNM Loan HT et al Coagulation abnormalities indengue hemorrhagic Fever serial investigations in167 Vietnamese children with Dengue shocksyndrome Clin Infect Dis 2002 35(3) 277-85 Epub20020713 doi 101086341410 PubMed PMID12115093
10 WHO editor Comprehensive guidelines forprevention and control of dengue fever and denguehaemorrhagic fever SEARO New Delhi India WorldHealth Organization 2011
11 Malavige GN Velathanthiri VG Wijewickrama ESFernando S Jayaratne SD Aaskov J et al Patterns ofdisease among adults hospitalized with dengueinfections Qjm 2006 99(5) 299-305 PubMed PMID16603571
12 Wijewickrama A FS Jayerathne PGSB Perera MAPAAbeynaike SA Gomes L Jeewandara C Malavige GNEffect of change in serotype on clinical severity ofdengue infections In SLMA editor Annual Con-ference of the Sri Lanka Medical AssociationColombo SLMA 2017
13 Wong JG Thein TL Leo YS Pang J Lye DC IdentifyingAdult Dengue Patients at Low Risk for ClinicallySignificant Bleeding PloS one 2016 11(2) e0148579doi 101371journalpone0148579 PubMed PMID26849556 PubMed Central PMCID PMCPMC4743958
14 Ojha A Nandi D Batra H Singhal R Annarapu GKBhattacharyya S et al Platelet activation determinesthe severity of thrombocytopenia in dengue infectionSci Rep 2017 7 41697 doi 101038srep41697PubMed PMID 28139770 PubMed Central PMCIDPMCPMC5282509
15 Isarangkura P Tuchinda S The behavior of transfused
platelets in dengue hemorrhagic fever The SoutheastAsian Journal of Tropical Medicine and Public Health1993 24 Suppl 1 222-4 PubMed PMID 7886581
16 Lum LC Abdel-Latif Mel A Goh AY Chan PW Lam SKPreventive transfusion in Dengue shock syndrome-is it necessary The Journal of Pediatrics 2003143(5) 682-4 PubMed PMID 14615749
17 Lye DC Lee VJ Sun Y Leo YS Lack of efficacy ofprophylactic platelet transfusion for severethrombocytopenia in adults with acute uncom-plicated dengue infection Clin Infect Dis 2009 48(9)1262-5 PubMed PMID 19292665
18 Lye DC Archuleta S Syed-Omar SF Low JG Oh HMWei Y et al Prophylactic platelet transfusion plussupportive care versus supportive care alone inadults with dengue and thrombocytopenia amulticentre open-label randomised superioritytrial Lancet 2017 389(10079) 1611-8 doi 101016S0140-6736(17)30269-6 PubMed PMID 28283286
19 Chinnappan S Ramachandrappa VS Tamilarasu KKrishnan UM Pillai AK Rajendiran S Inhibition ofPlatelet Aggregation by the Leaf Extract of Caricapapaya During Dengue Infection An In Vitro StudyViral immunology 2016 29(3) 164-8 doi 101089vim20150083 PubMed PMID 26910599
20 Charan J Saxena D Goyal JP Yasobant S Efficacyand safety of Carica papaya leaf extract in thedengue A systematic review and meta-analysis Int JAppl Basic Med Res 2016 6(4)249-54 doi 1041032229-516X192596 PubMed PMID 27857891PubMed Central PMCID PMCPMC5108100
21 Laoprasopwattana K Binsaai J Pruekprasert PGeater A Prothrombin Time Prolongation was theMost Important Indicator of Severe Bleeding inChildren with Severe Dengue Viral Infection Journalof Tropical Pediatrics 2017 63(4)314-20 doi101093tropejfmw097 PubMed PMID 28177091
22 Sureshkumar VK Vijayan D Kunhu S Mohamed ZThomas S Raman M Thromboelastographic Analysisof Hemostatic Abnormalities in Dengue PatientsAdmitted in a Multidisciplinary Intensive Care UnitA Cross-sectional Study Indian J Crit Care Med 201822(4)238-42 doi 104103ijccmIJCCM_486_17PubMed PMID 29743762 PubMed Central PMCIDPMCPMC5930527
23 Chuansumrit A Chaiyaratana W Hemostaticderangement in dengue hemorrhagic feverThrombosis Research 2014 133(1)10-6 doi101016jthromres201309028 PubMed PMID24120237
24 Wills B Tran VN Nguyen TH Truong TT Tran TN
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
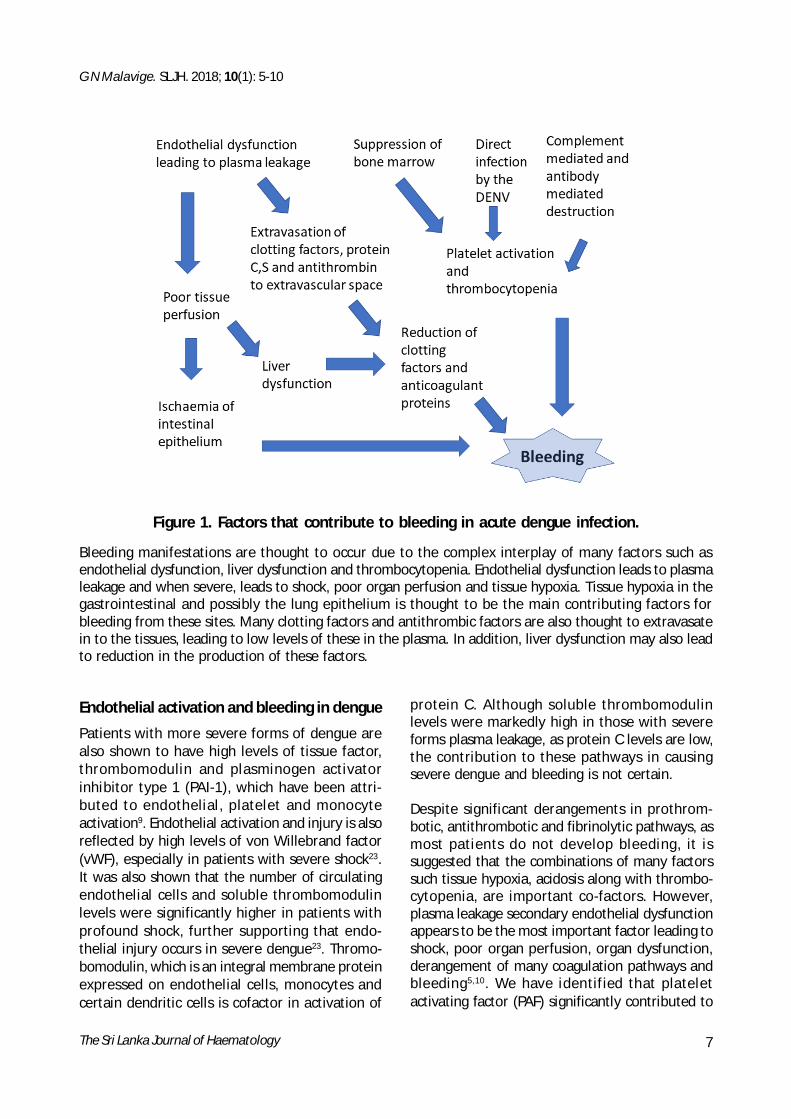
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 7
Endothelial activation and bleeding in dengue
Patients with more severe forms of dengue arealso shown to have high levels of tissue factorthrombomodulin and plasminogen activatorinhibitor type 1 (PAI-1) which have been attri-buted to endothelial platelet and monocyteactivation9 Endothelial activation and injury is alsoreflected by high levels of von Willebrand factor(vWF) especially in patients with severe shock23It was also shown that the number of circulatingendothelial cells and soluble thrombomodulinlevels were significantly higher in patients withprofound shock further supporting that endo-thelial injury occurs in severe dengue23 Thromo-bomodulin which is an integral membrane proteinexpressed on endothelial cells monocytes andcertain dendritic cells is cofactor in activation of
protein C Although soluble thrombomodulinlevels were markedly high in those with severeforms plasma leakage as protein C levels are lowthe contribution to these pathways in causingsevere dengue and bleeding is not certain
Despite significant derangements in prothrom-botic antithrombotic and fibrinolytic pathways asmost patients do not develop bleeding it issuggested that the combinations of many factorssuch tissue hypoxia acidosis along with thrombo-cytopenia are important co-factors Howeverplasma leakage secondary endothelial dysfunctionappears to be the most important factor leading toshock poor organ perfusion organ dysfunctionderangement of many coagulation pathways andbleeding510 We have identified that plateletactivating factor (PAF) significantly contributed to
Bleeding manifestations are thought to occur due to the complex interplay of many factors such asendothelial dysfunction liver dysfunction and thrombocytopenia Endothelial dysfunction leads to plasmaleakage and when severe leads to shock poor organ perfusion and tissue hypoxia Tissue hypoxia in thegastrointestinal and possibly the lung epithelium is thought to be the main contributing factors forbleeding from these sites Many clotting factors and antithrombic factors are also thought to extravasatein to the tissues leading to low levels of these in the plasma In addition liver dysfunction may also leadto reduction in the production of these factors
Figure 1 Factors that contribute to bleeding in acute dengue infection
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
8
vascular leakage in dengue25 In addition lipidmediators that oppose the action of PAF andprotect the endothelial barrier integrity such assphingosine-1-phosphate was found to bemarkedly low in patients with DHF especiallyduring the critical phase26
As plasma leakage appears to be the most impor-tant factor leading to all complications of dengueit would be reasonable to use drugs that preventor reduce vascular leakage as a suitable option toreduce severe dengue and associated compli-cations We have concluded a phase 2 randomizedplacebo controlled clinical trial in 183 patients atthe National Institute of Infectious Diseases SriLanka using a PAF receptor blocker known asrupatadine27 In this clinical trial we found thatrupatadine up to 40mg daily appeared safe andwell-tolerated in patients with acute dengue Inaddition patients given rupatadine had higherplatelet counts and lower aspartate-aminotrans-ferase levels during the critical phase and signifi-cantly smaller pleural effusions27 The develop-ment of significant bleeding manifestations suchas per vaginal bleeding and gastrointestinalbleeding was also lower in the group who receivedtreatment As the beneficial effects of this drugappeared to be greater when given early in theillness we are currently conducting another trialwhich is double blind randomized placebocontrolled trial in a larger cohort of patientsAlthough the initial trial showed promising resultsthese results should be interpreted with cautionuntil the same beneficial effects are seen in largertrials that we are currently carrying out
Summary
Endothelial dysfunction leading to plasma leakageappears to be the most important predictor ofoccurrence of bleeding in acute dengue Althoughthrombocytopenia is a risk factor of bleeding indengue thrombocytopenia alone was notassociated with bleeding in the absence of plasmaleakage Many abnormalities in the coagulationpathways are seen in severe dengue which appearto return to normal during the recovery phaseThese coagulation abnormalities have beenassociated with the degree of plasma leakage As
References
1 Bhatt S Gething PW Brady OJ Messina JP FarlowAW Moyes CL et al The global distribution andburden of dengue Nature 2013 496(7446) 504-7Epub 20130409 doi 101038nature12060 PubMedPMID 23563266 PubMed Central PMCIDPMC3651993
2 Mortality GBD Causes of Death C Global regionaland national life expectancy all-cause mortality andcause-specific mortality for 249 causes of death1980-2015 a systematic analysis for the GlobalBurden of Disease Study 2015 Lancet 2016388(10053) 1459-544 doi 101016S0140-6736(16)31012-1 PubMed PMID 27733281
3 Rouvinski A Guardado-Calvo P Barba-Spaeth GDuquerroy S Vaney MC Kikuti CM et al Recognitiondeterminants of broadly neutralizing humanantibodies against dengue viruses Nature 2015520(7545) 109-13 doi 101038nature14130PubMed PMID 25581790
4 Soo KM Khalid B Ching SM Chee HY Meta-Analysisof Dengue Severity during Infection by DifferentDengue Virus Serotypes in Primary and SecondaryInfections PloS one 2016 11(5) e0154760doi 101371journalpone02154760 PubMed PMID27213782 PubMed Central PMCID PMCPMC4877104
5 Malavige GN Ogg GS Pathogenesis of vascular leakin dengue virus infection Immunology 2017 151(3)261-9 doi 101111imm12748 PubMed PMID28437586 PubMed Central PMCID PMCPMC5461104
Authorship
Contribution This is the sole work of ProfGathsaurie Neelika Malavige
Conflict-of-interest disclosure The author declaresno conflict of interest
Correspondence Prof Gathsaurie Neelika MalavigeDPhil FRCP (Lond) FRCPath (UK)Centre for Dengue Research Faculty of MedicalSciences University of Sri Jayawardanapura SriLanka
E-mail gathsauriemalavigendmoxacuk
bleeding manifestations appear to best correlatewith the degree of leakage proper and meticulousfluid management would be the most importantmeasure in preventing bleeding manifestations
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 9
6 Md-Sani SS Md-Noor J Han WH Gan SP Rani NS TanHL et al Prediction of mortality in severe denguecases BMC infectious diseases 2018 18(1) 232 doi101186s12879-018-3141-6 PubMed PMID29783955
7 Pinto RC Castro DB Albuquerque BC Sampaio Vde SPassos RA Costa CF et al Mortality Predictors inPatients with Severe Dengue in the State of AmazonasBrazil PloS one 2016 11(8)e0161884 doi 101371journalpone0161884 PubMed PMID 27564084PubMed Central PMCID PMCPMC5001629
8 Sam SS Omar SF Teoh BT Abd-Jamil J AbuBakar SReview of Dengue hemorrhagic fever fatal cases seenamong adults a retrospective study PLoS neglectedtropical diseases 2013 7(5)e2194 doi 101371journalpntd0002194 PubMed PMID 23658849PubMed Central PMCID PMCPMC3642057
9 Wills BA Oragui EE Stephens AC Daramola OA DungNM Loan HT et al Coagulation abnormalities indengue hemorrhagic Fever serial investigations in167 Vietnamese children with Dengue shocksyndrome Clin Infect Dis 2002 35(3) 277-85 Epub20020713 doi 101086341410 PubMed PMID12115093
10 WHO editor Comprehensive guidelines forprevention and control of dengue fever and denguehaemorrhagic fever SEARO New Delhi India WorldHealth Organization 2011
11 Malavige GN Velathanthiri VG Wijewickrama ESFernando S Jayaratne SD Aaskov J et al Patterns ofdisease among adults hospitalized with dengueinfections Qjm 2006 99(5) 299-305 PubMed PMID16603571
12 Wijewickrama A FS Jayerathne PGSB Perera MAPAAbeynaike SA Gomes L Jeewandara C Malavige GNEffect of change in serotype on clinical severity ofdengue infections In SLMA editor Annual Con-ference of the Sri Lanka Medical AssociationColombo SLMA 2017
13 Wong JG Thein TL Leo YS Pang J Lye DC IdentifyingAdult Dengue Patients at Low Risk for ClinicallySignificant Bleeding PloS one 2016 11(2) e0148579doi 101371journalpone0148579 PubMed PMID26849556 PubMed Central PMCID PMCPMC4743958
14 Ojha A Nandi D Batra H Singhal R Annarapu GKBhattacharyya S et al Platelet activation determinesthe severity of thrombocytopenia in dengue infectionSci Rep 2017 7 41697 doi 101038srep41697PubMed PMID 28139770 PubMed Central PMCIDPMCPMC5282509
15 Isarangkura P Tuchinda S The behavior of transfused
platelets in dengue hemorrhagic fever The SoutheastAsian Journal of Tropical Medicine and Public Health1993 24 Suppl 1 222-4 PubMed PMID 7886581
16 Lum LC Abdel-Latif Mel A Goh AY Chan PW Lam SKPreventive transfusion in Dengue shock syndrome-is it necessary The Journal of Pediatrics 2003143(5) 682-4 PubMed PMID 14615749
17 Lye DC Lee VJ Sun Y Leo YS Lack of efficacy ofprophylactic platelet transfusion for severethrombocytopenia in adults with acute uncom-plicated dengue infection Clin Infect Dis 2009 48(9)1262-5 PubMed PMID 19292665
18 Lye DC Archuleta S Syed-Omar SF Low JG Oh HMWei Y et al Prophylactic platelet transfusion plussupportive care versus supportive care alone inadults with dengue and thrombocytopenia amulticentre open-label randomised superioritytrial Lancet 2017 389(10079) 1611-8 doi 101016S0140-6736(17)30269-6 PubMed PMID 28283286
19 Chinnappan S Ramachandrappa VS Tamilarasu KKrishnan UM Pillai AK Rajendiran S Inhibition ofPlatelet Aggregation by the Leaf Extract of Caricapapaya During Dengue Infection An In Vitro StudyViral immunology 2016 29(3) 164-8 doi 101089vim20150083 PubMed PMID 26910599
20 Charan J Saxena D Goyal JP Yasobant S Efficacyand safety of Carica papaya leaf extract in thedengue A systematic review and meta-analysis Int JAppl Basic Med Res 2016 6(4)249-54 doi 1041032229-516X192596 PubMed PMID 27857891PubMed Central PMCID PMCPMC5108100
21 Laoprasopwattana K Binsaai J Pruekprasert PGeater A Prothrombin Time Prolongation was theMost Important Indicator of Severe Bleeding inChildren with Severe Dengue Viral Infection Journalof Tropical Pediatrics 2017 63(4)314-20 doi101093tropejfmw097 PubMed PMID 28177091
22 Sureshkumar VK Vijayan D Kunhu S Mohamed ZThomas S Raman M Thromboelastographic Analysisof Hemostatic Abnormalities in Dengue PatientsAdmitted in a Multidisciplinary Intensive Care UnitA Cross-sectional Study Indian J Crit Care Med 201822(4)238-42 doi 104103ijccmIJCCM_486_17PubMed PMID 29743762 PubMed Central PMCIDPMCPMC5930527
23 Chuansumrit A Chaiyaratana W Hemostaticderangement in dengue hemorrhagic feverThrombosis Research 2014 133(1)10-6 doi101016jthromres201309028 PubMed PMID24120237
24 Wills B Tran VN Nguyen TH Truong TT Tran TN
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
8
vascular leakage in dengue25 In addition lipidmediators that oppose the action of PAF andprotect the endothelial barrier integrity such assphingosine-1-phosphate was found to bemarkedly low in patients with DHF especiallyduring the critical phase26
As plasma leakage appears to be the most impor-tant factor leading to all complications of dengueit would be reasonable to use drugs that preventor reduce vascular leakage as a suitable option toreduce severe dengue and associated compli-cations We have concluded a phase 2 randomizedplacebo controlled clinical trial in 183 patients atthe National Institute of Infectious Diseases SriLanka using a PAF receptor blocker known asrupatadine27 In this clinical trial we found thatrupatadine up to 40mg daily appeared safe andwell-tolerated in patients with acute dengue Inaddition patients given rupatadine had higherplatelet counts and lower aspartate-aminotrans-ferase levels during the critical phase and signifi-cantly smaller pleural effusions27 The develop-ment of significant bleeding manifestations suchas per vaginal bleeding and gastrointestinalbleeding was also lower in the group who receivedtreatment As the beneficial effects of this drugappeared to be greater when given early in theillness we are currently conducting another trialwhich is double blind randomized placebocontrolled trial in a larger cohort of patientsAlthough the initial trial showed promising resultsthese results should be interpreted with cautionuntil the same beneficial effects are seen in largertrials that we are currently carrying out
Summary
Endothelial dysfunction leading to plasma leakageappears to be the most important predictor ofoccurrence of bleeding in acute dengue Althoughthrombocytopenia is a risk factor of bleeding indengue thrombocytopenia alone was notassociated with bleeding in the absence of plasmaleakage Many abnormalities in the coagulationpathways are seen in severe dengue which appearto return to normal during the recovery phaseThese coagulation abnormalities have beenassociated with the degree of plasma leakage As
References
1 Bhatt S Gething PW Brady OJ Messina JP FarlowAW Moyes CL et al The global distribution andburden of dengue Nature 2013 496(7446) 504-7Epub 20130409 doi 101038nature12060 PubMedPMID 23563266 PubMed Central PMCIDPMC3651993
2 Mortality GBD Causes of Death C Global regionaland national life expectancy all-cause mortality andcause-specific mortality for 249 causes of death1980-2015 a systematic analysis for the GlobalBurden of Disease Study 2015 Lancet 2016388(10053) 1459-544 doi 101016S0140-6736(16)31012-1 PubMed PMID 27733281
3 Rouvinski A Guardado-Calvo P Barba-Spaeth GDuquerroy S Vaney MC Kikuti CM et al Recognitiondeterminants of broadly neutralizing humanantibodies against dengue viruses Nature 2015520(7545) 109-13 doi 101038nature14130PubMed PMID 25581790
4 Soo KM Khalid B Ching SM Chee HY Meta-Analysisof Dengue Severity during Infection by DifferentDengue Virus Serotypes in Primary and SecondaryInfections PloS one 2016 11(5) e0154760doi 101371journalpone02154760 PubMed PMID27213782 PubMed Central PMCID PMCPMC4877104
5 Malavige GN Ogg GS Pathogenesis of vascular leakin dengue virus infection Immunology 2017 151(3)261-9 doi 101111imm12748 PubMed PMID28437586 PubMed Central PMCID PMCPMC5461104
Authorship
Contribution This is the sole work of ProfGathsaurie Neelika Malavige
Conflict-of-interest disclosure The author declaresno conflict of interest
Correspondence Prof Gathsaurie Neelika MalavigeDPhil FRCP (Lond) FRCPath (UK)Centre for Dengue Research Faculty of MedicalSciences University of Sri Jayawardanapura SriLanka
E-mail gathsauriemalavigendmoxacuk
bleeding manifestations appear to best correlatewith the degree of leakage proper and meticulousfluid management would be the most importantmeasure in preventing bleeding manifestations
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 9
6 Md-Sani SS Md-Noor J Han WH Gan SP Rani NS TanHL et al Prediction of mortality in severe denguecases BMC infectious diseases 2018 18(1) 232 doi101186s12879-018-3141-6 PubMed PMID29783955
7 Pinto RC Castro DB Albuquerque BC Sampaio Vde SPassos RA Costa CF et al Mortality Predictors inPatients with Severe Dengue in the State of AmazonasBrazil PloS one 2016 11(8)e0161884 doi 101371journalpone0161884 PubMed PMID 27564084PubMed Central PMCID PMCPMC5001629
8 Sam SS Omar SF Teoh BT Abd-Jamil J AbuBakar SReview of Dengue hemorrhagic fever fatal cases seenamong adults a retrospective study PLoS neglectedtropical diseases 2013 7(5)e2194 doi 101371journalpntd0002194 PubMed PMID 23658849PubMed Central PMCID PMCPMC3642057
9 Wills BA Oragui EE Stephens AC Daramola OA DungNM Loan HT et al Coagulation abnormalities indengue hemorrhagic Fever serial investigations in167 Vietnamese children with Dengue shocksyndrome Clin Infect Dis 2002 35(3) 277-85 Epub20020713 doi 101086341410 PubMed PMID12115093
10 WHO editor Comprehensive guidelines forprevention and control of dengue fever and denguehaemorrhagic fever SEARO New Delhi India WorldHealth Organization 2011
11 Malavige GN Velathanthiri VG Wijewickrama ESFernando S Jayaratne SD Aaskov J et al Patterns ofdisease among adults hospitalized with dengueinfections Qjm 2006 99(5) 299-305 PubMed PMID16603571
12 Wijewickrama A FS Jayerathne PGSB Perera MAPAAbeynaike SA Gomes L Jeewandara C Malavige GNEffect of change in serotype on clinical severity ofdengue infections In SLMA editor Annual Con-ference of the Sri Lanka Medical AssociationColombo SLMA 2017
13 Wong JG Thein TL Leo YS Pang J Lye DC IdentifyingAdult Dengue Patients at Low Risk for ClinicallySignificant Bleeding PloS one 2016 11(2) e0148579doi 101371journalpone0148579 PubMed PMID26849556 PubMed Central PMCID PMCPMC4743958
14 Ojha A Nandi D Batra H Singhal R Annarapu GKBhattacharyya S et al Platelet activation determinesthe severity of thrombocytopenia in dengue infectionSci Rep 2017 7 41697 doi 101038srep41697PubMed PMID 28139770 PubMed Central PMCIDPMCPMC5282509
15 Isarangkura P Tuchinda S The behavior of transfused
platelets in dengue hemorrhagic fever The SoutheastAsian Journal of Tropical Medicine and Public Health1993 24 Suppl 1 222-4 PubMed PMID 7886581
16 Lum LC Abdel-Latif Mel A Goh AY Chan PW Lam SKPreventive transfusion in Dengue shock syndrome-is it necessary The Journal of Pediatrics 2003143(5) 682-4 PubMed PMID 14615749
17 Lye DC Lee VJ Sun Y Leo YS Lack of efficacy ofprophylactic platelet transfusion for severethrombocytopenia in adults with acute uncom-plicated dengue infection Clin Infect Dis 2009 48(9)1262-5 PubMed PMID 19292665
18 Lye DC Archuleta S Syed-Omar SF Low JG Oh HMWei Y et al Prophylactic platelet transfusion plussupportive care versus supportive care alone inadults with dengue and thrombocytopenia amulticentre open-label randomised superioritytrial Lancet 2017 389(10079) 1611-8 doi 101016S0140-6736(17)30269-6 PubMed PMID 28283286
19 Chinnappan S Ramachandrappa VS Tamilarasu KKrishnan UM Pillai AK Rajendiran S Inhibition ofPlatelet Aggregation by the Leaf Extract of Caricapapaya During Dengue Infection An In Vitro StudyViral immunology 2016 29(3) 164-8 doi 101089vim20150083 PubMed PMID 26910599
20 Charan J Saxena D Goyal JP Yasobant S Efficacyand safety of Carica papaya leaf extract in thedengue A systematic review and meta-analysis Int JAppl Basic Med Res 2016 6(4)249-54 doi 1041032229-516X192596 PubMed PMID 27857891PubMed Central PMCID PMCPMC5108100
21 Laoprasopwattana K Binsaai J Pruekprasert PGeater A Prothrombin Time Prolongation was theMost Important Indicator of Severe Bleeding inChildren with Severe Dengue Viral Infection Journalof Tropical Pediatrics 2017 63(4)314-20 doi101093tropejfmw097 PubMed PMID 28177091
22 Sureshkumar VK Vijayan D Kunhu S Mohamed ZThomas S Raman M Thromboelastographic Analysisof Hemostatic Abnormalities in Dengue PatientsAdmitted in a Multidisciplinary Intensive Care UnitA Cross-sectional Study Indian J Crit Care Med 201822(4)238-42 doi 104103ijccmIJCCM_486_17PubMed PMID 29743762 PubMed Central PMCIDPMCPMC5930527
23 Chuansumrit A Chaiyaratana W Hemostaticderangement in dengue hemorrhagic feverThrombosis Research 2014 133(1)10-6 doi101016jthromres201309028 PubMed PMID24120237
24 Wills B Tran VN Nguyen TH Truong TT Tran TN
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
G N Malavige SLJH 2018 10(1) 5-10
The Sri Lanka Journal of Haematology 9
6 Md-Sani SS Md-Noor J Han WH Gan SP Rani NS TanHL et al Prediction of mortality in severe denguecases BMC infectious diseases 2018 18(1) 232 doi101186s12879-018-3141-6 PubMed PMID29783955
7 Pinto RC Castro DB Albuquerque BC Sampaio Vde SPassos RA Costa CF et al Mortality Predictors inPatients with Severe Dengue in the State of AmazonasBrazil PloS one 2016 11(8)e0161884 doi 101371journalpone0161884 PubMed PMID 27564084PubMed Central PMCID PMCPMC5001629
8 Sam SS Omar SF Teoh BT Abd-Jamil J AbuBakar SReview of Dengue hemorrhagic fever fatal cases seenamong adults a retrospective study PLoS neglectedtropical diseases 2013 7(5)e2194 doi 101371journalpntd0002194 PubMed PMID 23658849PubMed Central PMCID PMCPMC3642057
9 Wills BA Oragui EE Stephens AC Daramola OA DungNM Loan HT et al Coagulation abnormalities indengue hemorrhagic Fever serial investigations in167 Vietnamese children with Dengue shocksyndrome Clin Infect Dis 2002 35(3) 277-85 Epub20020713 doi 101086341410 PubMed PMID12115093
10 WHO editor Comprehensive guidelines forprevention and control of dengue fever and denguehaemorrhagic fever SEARO New Delhi India WorldHealth Organization 2011
11 Malavige GN Velathanthiri VG Wijewickrama ESFernando S Jayaratne SD Aaskov J et al Patterns ofdisease among adults hospitalized with dengueinfections Qjm 2006 99(5) 299-305 PubMed PMID16603571
12 Wijewickrama A FS Jayerathne PGSB Perera MAPAAbeynaike SA Gomes L Jeewandara C Malavige GNEffect of change in serotype on clinical severity ofdengue infections In SLMA editor Annual Con-ference of the Sri Lanka Medical AssociationColombo SLMA 2017
13 Wong JG Thein TL Leo YS Pang J Lye DC IdentifyingAdult Dengue Patients at Low Risk for ClinicallySignificant Bleeding PloS one 2016 11(2) e0148579doi 101371journalpone0148579 PubMed PMID26849556 PubMed Central PMCID PMCPMC4743958
14 Ojha A Nandi D Batra H Singhal R Annarapu GKBhattacharyya S et al Platelet activation determinesthe severity of thrombocytopenia in dengue infectionSci Rep 2017 7 41697 doi 101038srep41697PubMed PMID 28139770 PubMed Central PMCIDPMCPMC5282509
15 Isarangkura P Tuchinda S The behavior of transfused
platelets in dengue hemorrhagic fever The SoutheastAsian Journal of Tropical Medicine and Public Health1993 24 Suppl 1 222-4 PubMed PMID 7886581
16 Lum LC Abdel-Latif Mel A Goh AY Chan PW Lam SKPreventive transfusion in Dengue shock syndrome-is it necessary The Journal of Pediatrics 2003143(5) 682-4 PubMed PMID 14615749
17 Lye DC Lee VJ Sun Y Leo YS Lack of efficacy ofprophylactic platelet transfusion for severethrombocytopenia in adults with acute uncom-plicated dengue infection Clin Infect Dis 2009 48(9)1262-5 PubMed PMID 19292665
18 Lye DC Archuleta S Syed-Omar SF Low JG Oh HMWei Y et al Prophylactic platelet transfusion plussupportive care versus supportive care alone inadults with dengue and thrombocytopenia amulticentre open-label randomised superioritytrial Lancet 2017 389(10079) 1611-8 doi 101016S0140-6736(17)30269-6 PubMed PMID 28283286
19 Chinnappan S Ramachandrappa VS Tamilarasu KKrishnan UM Pillai AK Rajendiran S Inhibition ofPlatelet Aggregation by the Leaf Extract of Caricapapaya During Dengue Infection An In Vitro StudyViral immunology 2016 29(3) 164-8 doi 101089vim20150083 PubMed PMID 26910599
20 Charan J Saxena D Goyal JP Yasobant S Efficacyand safety of Carica papaya leaf extract in thedengue A systematic review and meta-analysis Int JAppl Basic Med Res 2016 6(4)249-54 doi 1041032229-516X192596 PubMed PMID 27857891PubMed Central PMCID PMCPMC5108100
21 Laoprasopwattana K Binsaai J Pruekprasert PGeater A Prothrombin Time Prolongation was theMost Important Indicator of Severe Bleeding inChildren with Severe Dengue Viral Infection Journalof Tropical Pediatrics 2017 63(4)314-20 doi101093tropejfmw097 PubMed PMID 28177091
22 Sureshkumar VK Vijayan D Kunhu S Mohamed ZThomas S Raman M Thromboelastographic Analysisof Hemostatic Abnormalities in Dengue PatientsAdmitted in a Multidisciplinary Intensive Care UnitA Cross-sectional Study Indian J Crit Care Med 201822(4)238-42 doi 104103ijccmIJCCM_486_17PubMed PMID 29743762 PubMed Central PMCIDPMCPMC5930527
23 Chuansumrit A Chaiyaratana W Hemostaticderangement in dengue hemorrhagic feverThrombosis Research 2014 133(1)10-6 doi101016jthromres201309028 PubMed PMID24120237
24 Wills B Tran VN Nguyen TH Truong TT Tran TN
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
The Sri Lanka Journal of Haematology
G N Malavige SLJH 2018 10(1) 5-10
10
Nguyen MD et al Hemostatic changes in Vietnamesechildren with mild dengue correlate with the severityof vascular leakage rather than bleeding TheAmerican Journal of Tropical Medicine and Hygiene2009 81(4)638-44 Epub 20091010 doi 104269ajtmh200908-0008 PubMed PMID 19815879
25 Jeewandara C Gomes L Wickramasinghe NGutowska-Owsiak D Waithe D Paranavitane SA etal Platelet activating factor contributes to vascularleak in acute dengue infection PLoS Neglected TropicalDiseases 2015 9(2) e0003459 Epub 20150204doi 101371journalpntd0003459 PubMed PMID25646838 PubMed Central PMCID PMC4315531
26 Gomes L Fernando S Fernando RH WickramasingheN Shyamali NL Ogg GS et al Sphingosine 1-phosphate in acute dengue infection PloS one 20149(11) e113394 Epub 20141120 doi 101371journalpone0113394 PubMed PMID 25409037PubMed Central PMCID PMC4237441
27 Malavige GN Wijewickrama A Fernando SJeewandara C Ginneliya A Samarasekara S et al Apreliminary study on efficacy of rupatadine for thetreatment of acute dengue infection Sci Rep 20188(1) 3857 doi 101038s41598-018-22285-xPubMed PMID 29497121 PubMed Central PMCIDPMCPMC5832788
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 11
1Senior Staff Specialist 2Staff Specialist Departmentof Haematology Prince of Wales Hospital and NSWHealth Pathology Randwick NSW 2031 Australia
Thalassaemia major is the commonest monogenicdisorder with several thousand affected indi-viduals born each year predominantly in under-developed countries Beta thalassaemia majorresults from the inheritance of mutations in theβ globin gene from both parents resulting in life-long dependence on blood transfusions Indi-viduals with thalassaemia intermedia generallyhave inherited β globin gene mutations that allowthe production of some β globin with a subsequentless severe phenotype often without the needfor regular or intermittent transfusions Patientswith Haemoglobin H disease most commonly havedeletions of three of four α globin genes and havea variable phenotype most similar to thalassaemiaintermedia
The globin genes are present in clusters on chromo-somes 11 (β globin-like cluster) and 16 (α globin-like cluster) Normal haemoglobin comprises twoα-like and two β-like proteins bound to a hemecore Patients with thalassaemia major fail toproduce β globin generally due to the presence ofpoint mutations in both β globin genes with failureof switching from fetal (α2 γ2) to adult (α2 β2) haemo-globin production in early childhood Disorderederythropoiesis is exacerbated by the precipitationof α globin tetramers that form in the absence ofβ globin with extramedullary expansion causingcharacteristic skeletal manifestations and spleno-megaly Ineffective erythropoiesis results in ironoverload because of suppression of hepcidin themaster regulator of iron metabolism This increasesiron absorption and release of iron from macro-phages with increased free iron (non-transferrinbound iron) in the circulation promoting the for-mation of reactive oxygen species that lead totissue damage
Current issues in the management of thalassaemia major
Robert Lindeman1 Annmarie Bosco2 Giselle Kidson-Gerber1
Perspective
SLJH 2018 10(1) 11-16
Untreated thalassaemia major is therefore charac-terised by severe anaemia extramedullary haemo-poiesis (including splenomegaly and characteristicbony deformities) and iron overload
A Supportive treatment and its complications
The mainstay of treatment is blood transfusion atfrequent intervals to manage anaemia and tosuppress ineffective erythropoiesis Much of themorbidity associated with thalassaemia majorrelates to complications of transfusions
i Bloodborne infection
Prior to the introduction of screening for hepatitisC many regularly transfused patients wereinfected with this agent Treatment for hepatitis Cwith interferon and ribavirin was associated witha 40 eradication but more recently short coursesof combinations of direct antiviral agents achievecure in 95 of patients Nevertheless the com-bination of cirrhosis as a legacy of past hepatitis Cinfection and iron overload creates a residual riskof hepatoma in patients necessitating lifelongscreening in selected patients Screening of theblood supply for hepatitis B and HIV commencedin the early 1990s in most countries
Current recommendations are that patients withcirrhosis undergo six monthly ultrasound exami-nations to assist in the early detection of hepatomaas outcomes have been demonstrated to beimproved in patients with cirrhosis as a result ofearly intervention The identification of patientsrequiring screening is however problematic sincepatients no longer undergo liver biopsies to assessiron overload
Patients with thalassaemia major are at increasedrisk of severe infection with siderophilic bacteria(particularly but not exclusively Yersinia entero-colitica) Because chelating agents liberate ironfrom tissue macrophages this risk is exacerbated
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
12
by chelation therapy and it is recommended thatpatients suspend chelation therapy during bac-terial infections
ii Iron overload
Iron homeostasis is focused on the retention ofiron which is essential for many cellular functionsbut which in excess causes tissue damage Thereare no effective mechanisms for the active elimi-nation of excess iron Each transfused unit containsapproximately 250 mg of iron and in the absenceof iron chelation therapy severe iron overloadquickly develops during childhood
Until iron chelators became available mostpatients died in childhood of congestive cardiacfailure and arrhythmias resulting from iron over-load but iron overload also contributes to cirrhosisand causes damage to endocrine organs with conse-quent growth retardation failure of secondarysexual development and infertility hypothyroi-dism hypoparathyroidism and diabetes mellitus
Three iron chelators are available Desferrioxaminewas approved by the Food and Drug Administration(FDA) in 1982 and is administered by slow sub-cutaneous infusion over at least eight hours eachnight at least five times weekly with consequentpoor adherence to therapy particularly in youngadults Deferiprone is effective and administeredorally three times daily with evidence of synergyin removal of cardiac iron when combined withDesferrioxamine therapy (administered less fre-quently) but is associated with idiosyncraticneutropenia and rarely agranulocytosis necessi-tating regular blood count monitoring Deferasirox(approved in 2005 and 2006 in the United Statesand Europe respectively) is administered orallyonce daily and induces urinary and faecal excretionof iron Deferasirox is associated with gastro-intestinal toxicity and produces a non-progressiveincrease in the creatinine in a significant minorityof patients Deferasirox is generally available onlyas dispersible tablets however a newer film-coated formulation is becoming available which isassociated with improved patient acceptance
Deferasirox is expensive limiting its accessibilityin many countries
Since the introduction of effective iron chelatorsthe incidence of early cardiac deaths has reduceddramatically although older patients still have thelegacy of endocrine dysfunction and cirrhosis fromiron overload in early life
Adherence to therapy remains problematic butthe availability of cardiac and hepatic iron moni-toring (replacing liver biopsies) using T2 MRIexamination provides feedback to patients andclinicians and assists in guiding chelation therapy
iii Endocrine complications of iron overload
The management of patients with thalassaemiamajor includes screening for and treatment ofendocrine complications of iron overload Pituitarydysfunction is common in patients in whom ade-quate chelation was not commenced in earlychildhood Cyclical hormone supplementation (anoral contraceptive) is recommended in post-pubertal females to minimise the risk of osteo-porosis Patients are screened regularly for hypo-thyroidism hypoparathyroidism and diabetesmellitus (although use of the HbA1c is invalidatedby regular transfusions) and treated accordinglyBecause diabetes is due to pancreatic iron loadingmost diabetic patients are insulin dependentPatients may require induction of ovulationspermatogenesis for successful conception
iv Post-splenectomy complications
Splenectomy may be performed to reduce or avoidregular transfusions Patients in whom splenec-tomy has been performed are at increased risk ofpost-splenectomy infection Patients are vac-cinated against pneumococcus meningococcusand haemophilus influenza prior to splenectomywith follow-up vaccination at regular intervals1Evidence of benefit from long term prophylacticantibiotics in adults is scanty but patients shouldhave ready access to and commence antibiotictherapy promptly with infection and should havea low threshold for seeking medical attention
It has become apparent that the underlyingthromboembolic is exacerbated followingsplenectomy particularly in patients with thalas-saemia intermedia No specific interventions arerecommended although patients (particularly with
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 13
thalassaemia intermedia) should have echo-cardiograms to screen for pulmonary hyper-tension the incidence of which is increased inthese patients
v Osteoporosis
Patients with thalassaemia major commonly haveosteoporosis associated with expanded erythro-poiesis (in poorly transfused patients) hypo-thyroidism hypoparathyroidism hypogonadismreduced growth hormone-insulin like growthfactor-I (GH-IGF-I) and vitamin D deficiency whilea variety of genetic factors including mutations incollagen type 1 A1 (COLIA1) vitamin D receptorand transforming growth factor-beta (TFG-β)genes may be contributory Iron chelators mayhave a negative impact on bone density2
Regular (annual or second yearly) dual energy x-rayabsorptiometry (DEXA) screening is appropriate toensure early intervention Biochemical turnovermarkers can be used for the clinical follow-up ofosteoporotic patients ndash bone alkaline phosphataseosteocalcin and pro-peptide of type 1 procollagen(P1NP) are sensitive markers of bone formationwhile N-telopeptide cross-linked collagen type 1(NTx) is a sensitive marker of bone resorption
Treatment of hypogonadism with hormone replace-ment therapy in female patients improves bonedensity parameters but has not yet been demons-trated to reduce the risk of fractures2
The administration of potent osteoclast inhibitorsbisphosphonates (alendronate pamidronate andzoledronic acid) is associated with improvementin bone mineral density and a reduction in bonecomplications and pain There is less experience withTeriparatide (recombinant parathyroid hormone)and Denosumab (a RANKL monoclonal antibody)in patients with thalassaemia major
Curative options
A Allogeneic transplantation
Allogeneic haemopoietic stem cell transplantationis currently the only generally available curativetherapy for thalassaemia and has been mostsuccessful in children without complications of ironoverload with cure rates approaching 90 in
developed countries Availability of a matchedsibling donor limits the possibility of transplan-tation to the minority of patients but haplo-identical transplants (36 HLA locus matches) arebeing explored to increase donor availabilityReduced intensity transplantation may also reducethe morbidity and mortality associated withmyeloablative conditioning
B Gene therapy
Gene therapy offers the hope of an alternative cura-tive option Gene therapy using modified auto-logous haemopoietic stem cells (HSCs) obviatesthe need for a matched donor and mitigates someof the risks associated with allogeneic trans-plantation Cells are harvested for gene modifi-cation and reinfused or injected Gene therapyprotocols for haemoglobinopathies have requiredthat the patient receive cytoreductive conditioningtherapy
The successful use of gene replacement therapyin a patient with thalassaemia was reported in 2010A recent publication3 described two phase 1-2studies in which autologous CD34+ cells in 22patients were transduced ex vivo with a lentiviralvector encoding an extended β globin gene structureand reinfused after myeloablative therapy withbusulfan Twelve of 13 patients with a non- β0β0
genotype and three of nine patients with a β0β0
genotype (with a 73 reduction in transfusion re-quirements among those nine patients) achievedtransfusion independence at a median of 26 monthsTreatment-related side effects were related to theautologous transplant with no serious adverseevents related to the vector
The feasibility of disrupting specific DNA seq-uences is being explored in vitro as an approach tocorrecting or inactivating deleterious with geneediting approaches
C Novel agents
i Activin receptor ligand traps
Activin receptors are shared by multiple TGF-βfamily ligands including bone morphogenicproteins (BMPs) myostatin growth differentiationfactor-11 (GDF11) and GDF15 Activins GDFs andBMPs are regulators of human haematopoiesis and
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
14
activation promotes proliferation and reducesdifferentiation via the Smad 23 pathway Elevatedlevels of GDF15 are found in patients with β thalass-aemia and are associated with ineffective erythro-poiesis4 while blocking of GDF11 which is over-expressed in thalassaemia erythroblasts pro-moted terminal differentiation and induced apo-ptosis of immature erythroblasts reducing reactiveoxygen species and the formation of a globinaggregations
A trap ligand (sotatercept ACE-011) was manu-factured by fusing the extracellular domain ofactivin Receptor IIA and IIB to the Fc domain ofhuman IgG1 in order to trap endogenous ligandsand reduce downstream signalling that contributesto osteoporosis Another molecule in this class(luspatercept ACE-536) reduced anaemia in mousemodels of myelodysplasia and β thalassaemia bytrapping GDF11 A dose dependent and sustainableincrease in haemoglobin was demonstrated forluspatercept and sotatercept in normal volunteers5
A phase 2 open-label dose-ranging study inpatients with β thalassaemia has been completedand a two year extension study is underway ndashpatients receive luspatercept at doses of 02 to 125mgkg subcutaneously every three weeks Lus-patercept was generally well tolerated andassociated with reduced transfusion requirements(83 at least 33 lower transfusion requirementsand 67 at least 50 compared to baseline)reduced liver iron concentration in transfusion-dependent patients increased haemoglobinlevels (78 and 56 ge 10 and 15 gL respectively)and improved patient-reported outcomes in non-transfusion-dependent patients6 Similar resultshave been seen with Sotatercept7
A phase III double-blind randomised placebo-controlled multicentre study (BELIEVE) is currentlyunderway in transfusion-dependent patients withβ thalassaemia to determine the efficacy andsafety of luspatercept8
ii Janus kinase inhibitors
Jak2 is a cytoplasmic tyrosine kinase that mediatessignalling from cell surface receptors including theerythropoietin receptor (Epo-R) Binding of theEpo-R activates pathways critical to erythropoiesisincluding Signal Transducer and Activator of Trans-
cription 5 (Stat5) Down regulation of erythro-poiesis would be expected to reduce ineffectiveand extra-medullary erythropoiesis
Ruxolitinib is Janus kinase (Jak) oral inhibitor thatis approved for the treatment of myeloprolife-rative disorders A phase II single arm multicentrestudy has been performed to explore the efficacyand safety of this drug in regularly transfusedpatients with β thalassaemia with oral treatmentescalating over a 30 week period There was a trendto a reduction in transfusion requirements and aslight improvement in pre-transfusion haemoglobinwith a reduction in spleen volume over time9Similar studies have been performed with Febra-tinib but it remains to be seen whether this classof agents will find a role in the treatment ofpatients with thalassaemia
iii Hepcidin analogues
Hepcidin is a 25 amino acid peptide that regulatesiron homeostasis Hepcidin is produced in the liverin proportion to plasma iron concentrations andiron stores and binding causes internalisation anddegradation of the cellular iron exporter ferro-portin-1 (FPN-1) which is expressed on the surfaceof cells involved in iron absorption recycling andstorage Thalassaemia is associated with chronicsuppression of hepcidin
Transgenic overexpression of hepcidin in a mousemodel of thalassaemia has been demonstrated toprevent iron overload and augment erythro-poiesis while disruption using antisense oligonu-cleotide and RNA interference of Tmprss6 ahepcidin regulator has been demonstrated toproduce similar effects10 suggesting the possi-bility that increasing hepcidin levels might beclinically beneficial Minihepcidins (short peptides)have beneficial consequences in mouse modelssuggesting potential efficacy in patients withthalassaemia
D Management of fertility and pregnancy
Many women with thalassaemia major haveprimary or secondary amenorrhoea as a result ofiron-induced damage to the anterior pituitarygland during the first and second decades of lifeDespite this ovarian function is generally pre-served in these women and pregnancy can be
R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

R Lindeman et al SLJH 2018 10(1) 11-16
The Sri Lanka Journal of Haematology 15
achieved with hormonal stimulation Luteinisinghormone (LH) follicle-stimulating hormone (FSH)and oestradiol levels can be used to identifyhypogonadism in thalassaemia but have poorpredictive value with regard to reproductivepotential Antimuumlllerian hormone (AMH) has beensuggested as a better biomarker and declines morerapidly than in normal age-matched women
Induction of ovulation using a variety of regimensis commonly successful but some patients requireassisted reproductive technology involving themanipulation of oocytes or embryos in vitro Sper-matogenesis in impaired in heavily iron loadedmales with thalassaemia major but micromani-pulation techniques such as intracytoplasmic sperminjection (ICSI) have improved conception rates
A pre-pregnancy assessment including an echo-cardiogram review by a cardiologist and cardiacand hepatic T2 MRI is recommended particularlyas women with a T2 MRI of le 10 msec or withevidence of cardiac dysfunction are at higher riskThalassaemia or sickle trait should be excluded inthe partner in the context of genetic counsellingManagement of a pregnancy with a fetus at risk fora major haemoglobinopathy may involve preim-plantation embryo diagnosis or chorionic villussampling while some couples may elect to usedonor sperm
Pregnancy management requires a multidisci-plinary team including a haematologist repro-ductive medicine specialist high-risk obstetricianand cardiologist Cardiac risk in patients withthalassaemia major is due to iron deposition andreduced cardiac reserve and left ventriculardysfunction and pulmonary hypertension due tochronic anaemia Arrhythmias right ventriculardysfunction and cardiac failure have been reportedin 11 to 156 of pregnancies in patients withthalassaemia major11 major contributors to themorbidity and mortality in pregnancy in thesewomen
Women who have undergone splenectomy andwho are not transfusion dependent are atincreased risk of thrombosis Thromboprophylaxisshould be considered during pregnancy and thepostpartum period Other considerations include
an abdominal ultrasound and management ofgallstones prior to pregnancy screening forrelevant infectious agents (and treatment of hepa-titis C prior to pregnancy) and screening for signifi-cant red cell antibodies
Echocardiograms are recommended during eachtrimester with regular ferritin monitoring thyroidfunction tests and screening for diabetes Trans-fusion requirements increase and ensuring ahaemoglobin over 100 gL with more frequent lowvolume transfusions is recommended
Chelation therapy is withheld during pregnancy(usually when pregnancy is confirmed) because ofconcerns regarding teratogenicity and cardiac andliver iron deposition (detected by T2 MRI exami-nation) may increase as a result In the absence ofreports of teratogenicity in later pregnancy someclinicians recommend resuming chelation withdesferrioxamine in the second and third trimestersto reduce the cardiac risks associated with aprolonged period without chelation Adminis-tration of intravenous Desferrioxamine (2 g over24 hours) during labour to minimise the concen-tration of non-transferrin-bound iron in the serumand the risk of cardiac arrhythmias could beconsidered in high risk women12 Spontaneouscommencement of labour with vaginal delivery ispreferred except in women with cephalopelvicdisproportion cardiac dysfunction or significantiron overload when caesarean section is generallyrecommended
Conclusion
The landscape of thalassaemia management indeveloped countries is changing with greateremphasis on the management of endocrine andhepatic complications of iron overload and theunresolved problem of osteopenia and osteo-porosis in a population with a greatly increasedlife expectancy Safer allogeneic transplantationand the prospect of the availability of gene therapyrepresent potentially curative options whilefertility and pregnancy management are relevantfor populations of well-chelated patients Despitethese advances the majority of patients withthalassaemia major are managed in a setting wherethe foremost goals are reliable access to safe bloodproducts and the availability of suitable chelationtherapy
The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

The Sri Lanka Journal of Haematology
R Lindeman et al SLJH 2018 10(1) 11-16
16
References
1 Australian Technical Advisory Group on Immuni-sation (ATAGI) The Australian immunisationhandbook 10th ed [2017 update] CanberraAustralian Government Department of Health 2017(available online)
2 De Sanctis V et al Bone disease in beta thalassemiapatients past present and future perspectivesMetabolism 2018 80 66-79
3 Thompson AA et al Gene Therapy in Patients withTransfusion-Dependent beta- Thalassemia N Engl JMed 2018 378(16) 1479-93
4 Ronzoni LSL Duca L et al Growth differentiationfactor 15 expression and regulation during erythroiddifferentiation in non-transfusion dependentthalassemia Blood Cells Mol Dis 2015 54(1) 26-28
5 Attie KM AM McClure T et al A phase 1 study ofACE-536 a regulator of erythroid differentiation inhealthy volunteers Am J Hematol 2014 89(7)766-70
6 Piga AG PI Gamberini R et al Luspatercept increaseshemoglobin decreases transfusion burden andimproves iron overload in adults with beta-thalassemia Blood 2016 128 851
7 Cappellini MD PJ Origa R et al Interim results froma phase 2A open-label dose-finding study ofsotatercept (ACE-011) in adult patients (PTS) withbeta-thalssemia [abstract] Haematologica 2015100(s1) 17-18
8 An efficacy and safety study of luspatercept (ACE-536) versus placebo in adults who require regularred blood cell transfuisons due to beta (b)thalassemia (BELIEVE) Clinicaltrialsgov 2017 Jan 23httpsclinicaltrialsgovct2showNCT02604433
9 Aydinok Y KZ Cassinerio E et al Efficacy and safetyof ruxolitinib in regularly transfused patients withthalassemia results from single-arm multicenterphase 2a truth study [abstract] Blood 2016 128(22)852
10 Casu C Nemeth E Rivella S Hepcidin agonists astherapeutic tools Blood 2018 131(16) 1790-4
11 Carlberg KT Singer ST Vichinsky EP Fertility andPregnancy in Women with Transfusion-DependentThalassemia Hematol Oncol Clin North Am 201832(2) 297-315
12 Petrakos G AP Tsironi M Pregnancy in women withthalssemia challenges and solutions InternationalJournal of Womenrsquos Health 2016 8 441-51
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Conjoint Professor RobertLindeman MBBS FRACP FRCPA PhDSenior Staff Specialist Department of Haemato-logy Prince of Wales Hospital and NSW HealthPathology Randwick NSW 2031 Australia
E-mail robertlindemanhealthnswgovau
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 17
1Consultant Haematologist DGH Trincomalee SriLanka 2Consultant Haematologist Colombo SouthTeaching Hospital Sri Lanka
Abstract
Mean cell volume (MCV) is an important para-meter in diagnosing anaemia and also presence ofit without anaemia provides important informationregarding underlying disease to the clinician Werely on reference ranges of Caucasian populationeven though Sri Lanka has different environmentalconditions and habits compared to westernpopulation The study was carried out at ColomboSouth Teaching Hospital 525 consecutive FBCsamples with MCV gt80fL were analyzed Pregnantmothers pediatric samples (lt12 years) OPDsamples and samples with any features suggestiveof iron deficiency were excluded All underwentblood picture examination and intervieweradministered questionnaire Further testing toidentify at least one reason for macrocytosis wasdone in patients who have a single positive findingin blood picture or questionnaireOur study included 582 male and 418 femalepatients 904 were Sinhalese 6 Tamil 19Muslims and 17 others Age varied from 13-91years Significant association was demonstratedbetween macrocytosis and age (plt005)In our study prevalence of macrocytosis in FBC was162 and prevalence of blood picture macro-cytosis was 379 Appearance of macrocytes inthe blood picture was significant when MCVincreases (lt0001)
A study of mean cell volume (MCV) in patients who are treated at ColomboSouth Teaching Hospital
PLSP Vitharana1 N Ranasinghe2
Research paper
Key words mean cell volume macrocytes
SLJH 2018 10(1) 17-22
Presence of a reason for macrocytosis was signifi-cantly high when MCV was gt90fL (gt0001) with amean MCV value of 942fL Having macrocytes inblood picture was a significant indicator for anunderlying reason for macrocytosis (lt0001) In 27of patients with normal MCV macrocytosis wouldhave been missed if blood picture examinationwas not performed
There was an significant association betweenmacrocytosis and alcohol intake (plt0001) macro-cytosis and smoking (ltplt0001) macrocytosis andvegetarians (plt005) macrocytosis and hydroxyureatreatment (lt005) and macrocytosis and CLCD(plt0001) There was also an association betweenmacrocytosis and reticulocytosis (plt005) macro-cytosis and roulaeux formation (lt005) macro-cytosis and elevated RDW (lt0001) and macro-cytosis and anaemia in female patients (lt005)
Introduction
FBC report provides various parameters which arenecessary in diagnosing various diseases MeanCell Volume (MCV) is one of the important para-meters in diagnosing anaemia MCV can be definedas the average volume of a red cell When manualtests are performed MCV is calculated usingPacked Cell Volume (PCV) and Red Cell Count(RCC) Results are given in femtoliters (fL)Automated analyzers measure MCV directly basedon the actual measurement of the volume as itpasses through a laser or an electronic beam Sinceit is directly measured few internal factors play arole in fastidious increase in MCV
MCV vary depending on the technology used andthe method of instrument calibration Thereforenormal range for MCV has inter-laboratory variation1It is given as 80-95fL in Essential Haematology byVictor Hoffbrand and Wintrobersquos Clinical Haema-
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
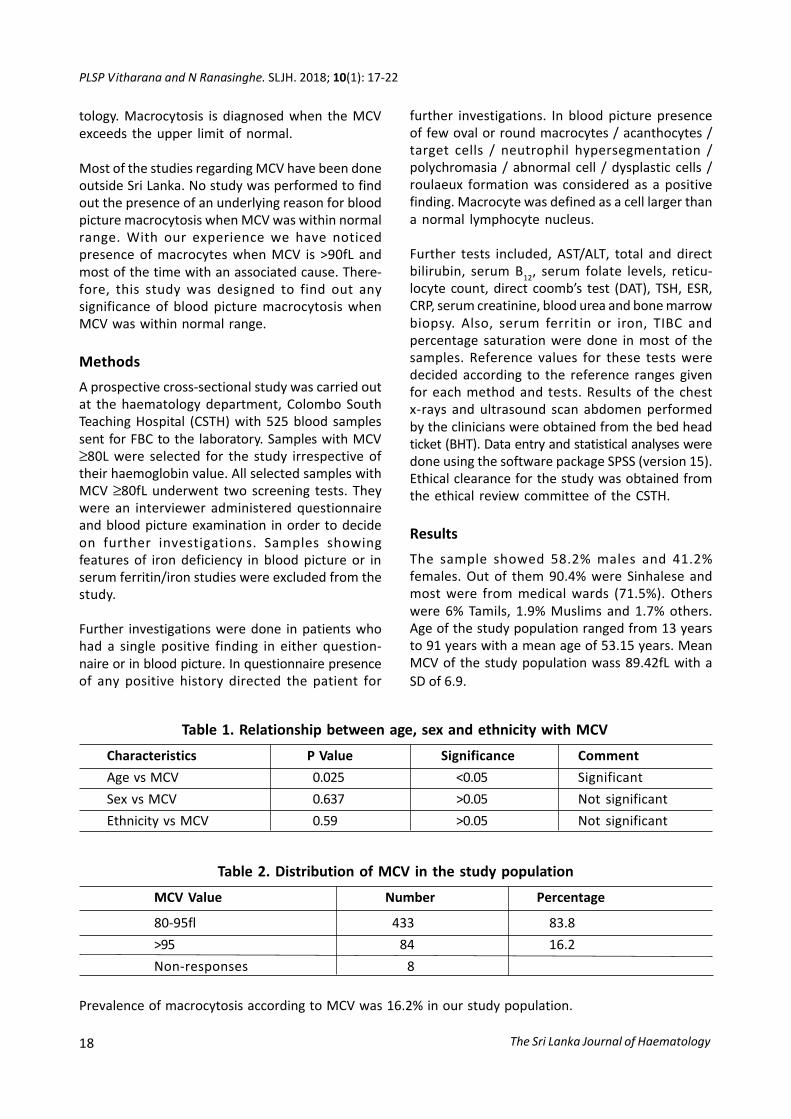
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
18
tology Macrocytosis is diagnosed when the MCVexceeds the upper limit of normal
Most of the studies regarding MCV have been doneoutside Sri Lanka No study was performed to findout the presence of an underlying reason for bloodpicture macrocytosis when MCV was within normalrange With our experience we have noticedpresence of macrocytes when MCV is gt90fL andmost of the time with an associated cause There-fore this study was designed to find out anysignificance of blood picture macrocytosis whenMCV was within normal range
Methods
A prospective cross-sectional study was carried outat the haematology department Colombo SouthTeaching Hospital (CSTH) with 525 blood samplessent for FBC to the laboratory Samples with MCVge80L were selected for the study irrespective oftheir haemoglobin value All selected samples withMCV ge80fL underwent two screening tests Theywere an interviewer administered questionnaireand blood picture examination in order to decideon further investigations Samples showingfeatures of iron deficiency in blood picture or inserum ferritiniron studies were excluded from thestudy
Further investigations were done in patients whohad a single positive finding in either question-naire or in blood picture In questionnaire presenceof any positive history directed the patient for
further investigations In blood picture presenceof few oval or round macrocytes acanthocytes target cells neutrophil hypersegmentation polychromasia abnormal cell dysplastic cells roulaeux formation was considered as a positivefinding Macrocyte was defined as a cell larger thana normal lymphocyte nucleus
Further tests included ASTALT total and directbilirubin serum B12 serum folate levels reticu-locyte count direct coombrsquos test (DAT) TSH ESRCRP serum creatinine blood urea and bone marrowbiopsy Also serum ferritin or iron TIBC andpercentage saturation were done in most of thesamples Reference values for these tests weredecided according to the reference ranges givenfor each method and tests Results of the chestx-rays and ultrasound scan abdomen performedby the clinicians were obtained from the bed headticket (BHT) Data entry and statistical analyses weredone using the software package SPSS (version 15)Ethical clearance for the study was obtained fromthe ethical review committee of the CSTH
Results
The sample showed 582 males and 412females Out of them 904 were Sinhalese andmost were from medical wards (715) Otherswere 6 Tamils 19 Muslims and 17 othersAge of the study population ranged from 13 yearsto 91 years with a mean age of 5315 years MeanMCV of the study population wass 8942fL with aSD of 69
Table 1 Relationship between age sex and ethnicity with MCV
Characteristics P Value Significance Comment
Age vs MCV 0025 lt005 Significant
Sex vs MCV 0637 gt005 Not significant
Ethnicity vs MCV 059 gt005 Not significant
Table 2 Distribution of MCV in the study population
MCV Value Number Percentage
80-95fl 433 838
gt95 84 162
Non-responses 8
Prevalence of macrocytosis according to MCV was 162 in our study population
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
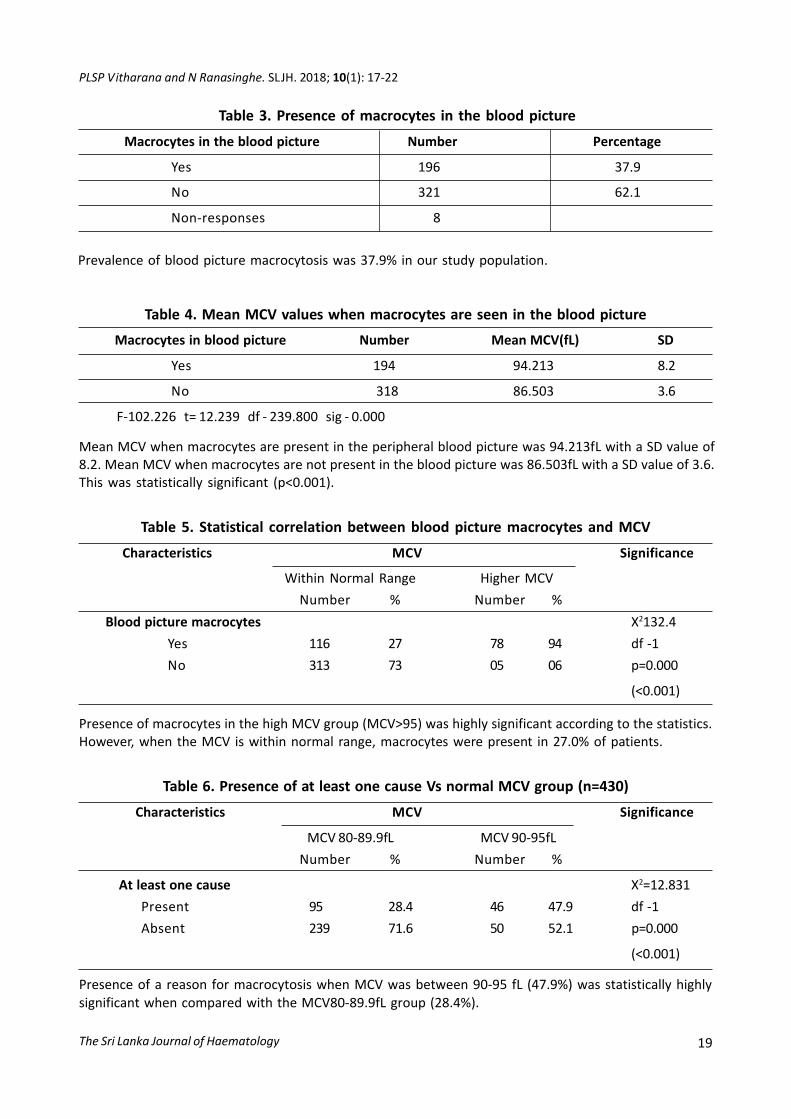
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 19
Table 3 Presence of macrocytes in the blood picture
Macrocytes in the blood picture Number Percentage
Yes 196 379
No 321 621
Non-responses 8
Prevalence of blood picture macrocytosis was 379 in our study population
Table 4 Mean MCV values when macrocytes are seen in the blood picture
Macrocytes in blood picture Number Mean MCV(fL) SD
Yes 194 94213 82
No 318 86503 36
F-102226 t= 12239 df - 239800 sig - 0000
Mean MCV when macrocytes are present in the peripheral blood picture was 94213fL with a SD value of82 Mean MCV when macrocytes are not present in the blood picture was 86503fL with a SD value of 36This was statistically significant (plt0001)
Table 5 Statistical correlation between blood picture macrocytes and MCV
Characteristics MCV Significance
Within Normal Range Higher MCV
Number Number
Blood picture macrocytes X21324
Yes 116 27 78 94 df -1
No 313 73 05 06 p=0000
(lt0001)
Table 6 Presence of at least one cause Vs normal MCV group (n=430)
Characteristics MCV Significance
MCV 80-899fL MCV 90-95fL
Number Number
At least one cause X2=12831
Present 95 284 46 479 df -1
Absent 239 716 50 521 p=0000
(lt0001)
Presence of macrocytes in the high MCV group (MCVgt95) was highly significant according to the statisticsHowever when the MCV is within normal range macrocytes were present in 270 of patients
Presence of a reason for macrocytosis when MCV was between 90-95 fL (479) was statistically highlysignificant when compared with the MCV80-899fL group (284)
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
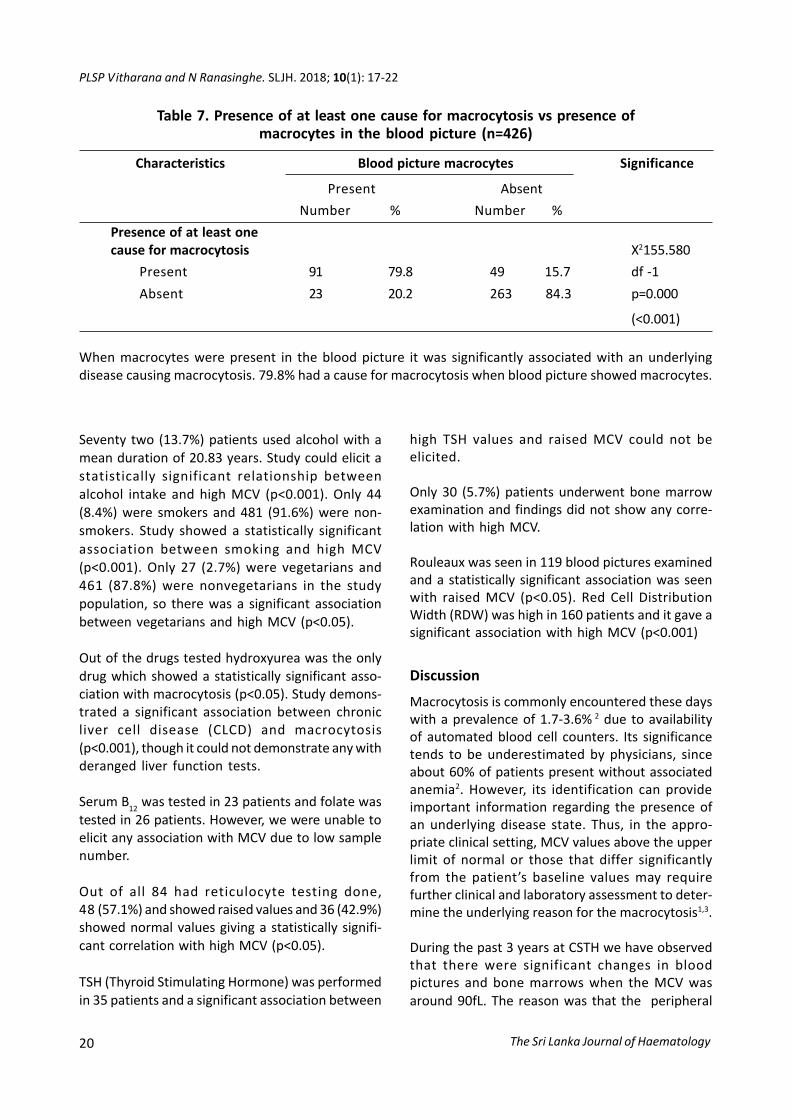
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
20
Seventy two (137) patients used alcohol with amean duration of 2083 years Study could elicit astatistically significant relationship betweenalcohol intake and high MCV (plt0001) Only 44(84) were smokers and 481 (916) were non-smokers Study showed a statistically significantassociation between smoking and high MCV(plt0001) Only 27 (27) were vegetarians and461 (878) were nonvegetarians in the studypopulation so there was a significant associationbetween vegetarians and high MCV (plt005)
Out of the drugs tested hydroxyurea was the onlydrug which showed a statistically significant asso-ciation with macrocytosis (plt005) Study demons-trated a significant association between chronicliver cell disease (CLCD) and macrocytosis(plt0001) though it could not demonstrate any withderanged liver function tests
Serum B12
was tested in 23 patients and folate wastested in 26 patients However we were unable toelicit any association with MCV due to low samplenumber
Out of all 84 had reticulocyte testing done48 (571) and showed raised values and 36 (429)showed normal values giving a statistically signifi-cant correlation with high MCV (plt005)
TSH (Thyroid Stimulating Hormone) was performedin 35 patients and a significant association between
Table 7 Presence of at least one cause for macrocytosis vs presence ofmacrocytes in the blood picture (n=426)
Characteristics Blood picture macrocytes Significance
Present Absent
Number Number
Presence of at least onecause for macrocytosis X2155580
Present 91 798 49 157 df -1
Absent 23 202 263 843 p=0000
(lt0001)
When macrocytes were present in the blood picture it was significantly associated with an underlyingdisease causing macrocytosis 798 had a cause for macrocytosis when blood picture showed macrocytes
high TSH values and raised MCV could not beelicited
Only 30 (57) patients underwent bone marrowexamination and findings did not show any corre-lation with high MCV
Rouleaux was seen in 119 blood pictures examinedand a statistically significant association was seenwith raised MCV (plt005) Red Cell DistributionWidth (RDW) was high in 160 patients and it gave asignificant association with high MCV (plt0001)
Discussion
Macrocytosis is commonly encountered these dayswith a prevalence of 17-36 2 due to availabilityof automated blood cell counters Its significancetends to be underestimated by physicians sinceabout 60 of patients present without associatedanemia2 However its identification can provideimportant information regarding the presence ofan underlying disease state Thus in the appro-priate clinical setting MCV values above the upperlimit of normal or those that differ significantlyfrom the patientrsquos baseline values may requirefurther clinical and laboratory assessment to deter-mine the underlying reason for the macrocytosis13
During the past 3 years at CSTH we have observedthat there were significant changes in bloodpictures and bone marrows when the MCV wasaround 90fL The reason was that the peripheral
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
The Sri Lanka Journal of Haematology 21
blood smear was more sensitive than RBC indicesfor identifying early macrocytic changes as MCVrepresents the mean of the distribution curve andis insensitive to the presence of small numbers ofmacrocytes4 When compared with the peripheralblood smear a normal MCV may miss macrocytosisin over 30 of cases5
We have shown a significant association ofmacrocytosis with increase in age (plt005) (Table 1)Similar findings were shown in a study done in 1996at Whipps Cross Hospital6
We demonstrated a highly significant associationbetween macrocytosis and smoking (plt0001)Similar results were shown in a study done indepartment of Haematology Cork UniversityHospital and University College Cork Ireland7
Our study showed a significant association bet-ween vegetarians and macrocytosis (plt005)which was a well-known fact that vegetarians couldhave B12 deficiency leading to macrocytosisHowever a study done in USA vegetarian popu-lation showed B
12 deficiency in a significant
number of participants but macrocytosis amongthem was minimal8
Prevalence of macrocytosis in FBC was 162(Table 2) Prevalence of macrocytes in peripheralblood picture was 379 in our study group (Table 3)This was much higher than the prevalence describedin literature2
Our study showed a highly significant associationbetween increasing MCV and presence of macro-cytes in the peripheral blood (plt0001) Mean MCVvalue for the study population when macrocytesappear in peripheral blood picture was 94213fLwith a SD value of 82 (Table 4) This mean waswithin the normal reference range of MCV andstatistically highly significant (plt0001) Thereforewe can conclude that peripheral blood macrocytesmay be present even with normal MCV valuesMean MCV value when macrocytes were not in theblood picture was 86503fL This was alsostatistically significant (plt0001)
Furthermore 27 patients who were withinnormal MCV range have shown peripheral bloodmacrocytes during blood picture examination
(Table 5) It clearly indicates that we can easily missthe presence of macrocytes in peripheral blood ifwe do not examine the blood picture
When whole study group is further analyzed wefound 216 (411) has at least one identifiablecause for macrocytosis Out of that 141 (6527)was in 80-95fL MCV group
Since our mean MCV when macrocytes werepresent in blood picture was 94213fL and in routinepractice we see causes of macrocytosis when MCVgt90 we arbitrary divide normal MCV group in to 2subgroups (MCV ndash 80-899 and 90-95fL) Table 6shows the difference between the 02 groups(plt0001)
798 of participants who has macrocytes in theblood picture had a reason behind for its presenceOnly 202 participants did not show an esta-blished reason for its presence Therefore pre-sence of macrocytes in the blood picture wassignificantly associated (Table 7) with an underlyingcause for macrocytosis (plt0001)
Conclusions and Recommendations
Appearance of macrocytes in the blood picture issignificant when MCV is high When blood pictureshows macrocytes there is a significantly highchance of it being associated with an establishedunderlying reason for macrocytosis Thereforeblood picture examination is an importantscreening tool in individuals with a MCV gt90fL todecide on further investigations and follow up inorder to look for a cause for macrocytosis
However we need further studies in healthypopulation to assess the significance of thesefindings
Authorship
Contribution Both the authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr PLSP Vitharana ConsultantHaematologist General Hospital Trincomalee SriLanka
E-mail shaniv23yahoocom
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
The Sri Lanka Journal of Haematology
PLSP Vitharana and N Ranasinghe SLJH 2018 10(1) 17-22
22
Acknowledgements
The authors would like to acknowledge the Directorof Colombo South Teaching Hospital Kalubowilafor giving permission to carry out this study Theyalso gratefully acknowledge the cooperation of allstaff and patients involved in this study
References
1 Bain BJ Morphology of blood cells Blood cells Apractical Guide 4th edition 2006
2 Colon-Otero G Menke D Hook CC A practicalapproach to the differential diagnosis andevaluation of the adult patient with macrocyticanemia Med Clin North Am 1992 76 581-97
3 Savage DG Ogundipe A Allen RH Stabler SP
Lindenbaum J Etiology and diagnostic evaluation ofmacrocytosis Am J Med Sci 2000 319 343-52
4 Kasper DL Braunwald E Fauci A Hauser S Longo DJameson JL Harrisonrsquos principles of internalmedicine 16th ed New York McGraw-Hill MedicalPublishing Division 2005
5 Davidson RJ Hamilton PJ High mean red cell volumeits incidence and significance in routinehaematology J Clin Pathol 1978 31 493-8
6 Mahmoud MY Lugon M Anderson CC UnexplainedMacrocytosis in elderly Age and Ageing 1996 25(4)310-12
7 OrsquoReilly MA Buckley CM Harrington JM OrsquoShea SPerry IJ Cahill MR Cigarette smoking is an underrecognised cause of macrocytosis Blood 2013122(21) 4660
8 Dong A Scott SC Serum B12 and blood cell values invegetarians Ann Nutr Metab 1982 26(4) 209-16
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
KHBP Fernandopulle SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology 23
1Senior Lecturer Consultant Haematologist Department of Pathology Faculty of Medical SciencesUniversity of Sri Jayewardenepura Sri Lanka
Correspondence Dr KHBP Fernandopulle
E-mail shivifgmailcom
Neutropenia in children specially the chronic neutropenias have diverse causes Some are inheritedwhile others are acquired some need monitoring only while others need active management Themultiple choice questions given below are designed to refresh you of some causes of childhoodneutropenia how to investigate and manage
1 Which of the following support a diagnosis of Kostmann syndrome in a 5-month-old girl presentingwith recurrent lung infections severe neutropenia normal haemoglobin and platelet count
a) Maturation arrest of neutrophils at the myelocyte stage seen in the bone marrow
b) Autosomal recessive inheritance
c) Normal neutrophil counts in between the septic episodes
d) Hepatosplenomegaly
e) Clinical presentation before six months of age
2 Which of the following statements regarding other neutropenias in childhood are true
a) Acute transient neutropenia occurs after viral and bacterial infections
b) Complete blood count is performed 2-3 times a week for six weeks to diagnose cyclicneutropenia
c) Drug related neutropenia is not seen in the paediatric age group
d) Demonstration of neutrophil specific autoantibodies is the gold standard in diagnosingprimary auto immune neutropenia
e) Some metabolic diseases are associated with neutropenia
3 Which of the following statements regarding treatment of neutropenias in childhood are correct
a) Bone marrow transplantation (BMT) has been accepted as the preferred treatment in Kostmannsyndrome
b) The factors which determine the risk of leukemia transformation in congenital neutropeniainclude the neutrophil count mutation type and intensity of G-CSF treatment
Theme Neutropenia in infants and children
KHBP Fernandopulle1
CME Article (Series VI)
SLJH 2018 10(1) 23-24
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
The Sri Lanka Journal of Haematology
KHBP Fernandopulle SLJH 2018 10(1) 23-24
24
c) No treatment is indicated in benign familial neutropenia
d) G-CSF is initiated at a dose of 5 μgkg in children with severe neutropenic sepsis
e) Immunosuppressive drugs are beneficial in primary autoimmune neutropenia
Answer Grid
Q1 a b c d e Q2 a b c d e Q3 a b c d e
T T T T T T T T T T T T T T T
F F F F F F F F F F F F F F F
CME points 01
The answers and the discussion are given in page 34
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 25
1Registrar in Haematology 3Consultant Histo-pathologist 4Consultant Haematologist TeachingHospital Kandy Sri Lanka 2Registrar in Haemato-logy Teaching Hospital Peradeniya Sri Lanka
Abstract
Classical Hodgkin lymphoma (HL) is one of the fewadult malignancies that most frequently presentswith progressive painless enlargement of theperipheral lymph nodes Hodgkin lymphoma (HL)is a clinicopathologically unique an aggressive B-celllymphoma which is one of the most curable of allhaematological malignancies The excellent out-comes that are seen in HL is due to the treatmentcombination of multi-agent chemotherapy andradiotherapy A 19-year-old boy presented with feverand cervical lymphadenopathy was diagnosed ashaving mycoplasma infection and treated Sincelymphadenopathy and fever were persisting despiteatypical antibiotic coverage lymph node biopsywas done which revealed presence of classicalHodgkin lymphoma He was staged and his pro-gnostic assessment revealed that he was in stageIIA with favourable prognosis He was started on 4cycles of ABVD chemotherapy without radio-therapy
Introduction
Classical HL is defined as a proliferative neoplasmof the lymph nodes which show mono-nuclearHodgkin cells and multi nucleated Reed Sternberg(RS) cells in variable proportions along withneutrophils eosinophils histiocytes fibro-blastscollagen fibers non neoplastic lymphocytes andplasma cells
Hodgkin lymphoma (HL) is a clinicopathologicallyunique an aggressive B-cell lymphoma which is
An early presentation of classical Hodgkin lymphoma with atypical pneumonia
WAON Wickramasinghe1 DMHMK Dassanayake2 A Vithanage3 VC Panditha Gunawardena4
Case report I
Key words Hodgkin lymphoma mycoplasma infection
SLJH 2018 10(1) 25-27
one of the most curable of all hematological mali-gnancies The excellent outcomes that are seen inHL is due to the combination treatment regimesusing multi-agent chemotherapy and radiotherapy
Case report
A 19-year-old previously healthy boy presentedwith fever frontal headache dry cough non specificgastro intestinal symptoms for two weeks andgeneralized erythematous skin rash for 2 days Rashappeared on day 4 of fever and was first noticed inthe upper extremities and trunk which thengeneralized within few hours Rash was a genera-lized erythematous maculopapular blanchingnon itchy rash with few desquamating regionsaround neck and axilla but palms and soles werespared There were no arthralgia myalgia orconstitutional symptoms He did not have anysignificant medical problems in the past
On clinical examination he was febrile not pale oricteric with bilateral mildly enlarged tonsils andbilateral cervical lymphadenopathy involvingsuperficial deep cervical and posterior auricularregions each node measuring 05-1cm in diameternon tender discrete and firm in consistency Therewere no other clinically palpable lymph nodes Nofacial or ankle oedema was noted
Cardiovascular system examination was normalexcept for a mild tachycardia there were no lungsigns and abdominal examination was normal withno evidence of organomegaly There were no otherfocal neurological signs
Investigations revealed WBC 1732times109L withneutrophils 125times109L lymphocytes 38times109Leosinophils 09times109L and monocytes 01times109LHeamoglobin was 112gdL and Platelet count was
The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

The Sri Lanka Journal of Haematology
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
26
220times109L Blood picture revealed evidence ofsecondary bacterial infection and mild eosino-phillia ESR of 45mmhr CRP of 307mgL which roseupto 42mgL in 3 days Procalcitonin of 896 mgmLproved that sepsis was likely Blood culture wasnegative Chest radiograph revealed bilateralperibroncheolar and perivascular infiltrativeshadows in lower zones Mantoux was negativeand throat swab for culture and ABST was negativeLiver function test revealed AST of 444UL and ALTof 348UL with normal ALP GGT and total serumbilirubin Renal function tests and electrolyteswere normal
Serum LDH was 324UL ANA was negative and viralserology for HIV1 amp 2 Hep BC EBV and CMV werenegative With the finding of bilateral chestinfiltrates mycoplasma Ab Ig M was performedand found to have positive in two occasions andthe titres were 132UL amp 151 UL) Directantiglobulin test (DAT) was negative and reticcount was 22 ECG was normal and 2D Echorevealed no cardiac vegetations with EF of 60USS abdomen revealed no hepatosplenomagaly orabdominal lympha-denopathy
The patientrsquos mycoplasma infection was treatedwith oral Clarythromycin The rash and respiratorysymptoms responded but fever and lymphadeno-pathy persisted Therefore a lymph node biopsywas performed Histology revealed effaced nodalarchitecture expanded para cortical areas with amixed infiltrate composed of eosinophils lympho-cytes and plasma cells many scattered mono-nuclear Hodgkinrsquos and Reed Sternberg cells Mitoticactivity was increased and many apoptotic cellswere present Immunohistochemistry revealedmembranous positivity for CD15 amp CD 30 in largecells and scattered CD3 positivity CD 20 amp ALK werenegative Those features confirmed the diagnosisof mixed cellularity type Hodgkin Lymphoma
The CECT neck chest abdomen amp pelvis togetherwith bone marrow aspiration and trephine biopsywere done for staging CECT revealed bilateraldeep cervical supraclavicular and anterior andmiddle mediastinal adenopathy 21 cm in AP
diameter with no para aortic portal or mesentericlymph nodes or hepatosplenomegaly Bone marrowtrephine biopsy revealed normal trilineagehaemophoesis with no evidence of infiltration byHL According to Ann Arbor staging with cots-wolds modification and EROCT prognostic criteriahe was in stage II A (early stage) with favourableprognosis
He was started treatment with on 4 cycles of ABVD(doxorubicin (adriamycin) bleomycin vinblastinand dacarbazine) supportive care and concurrentmedications after improvement of transaminasesand CXR features without any complications
Discussion
This is a patient presented with mycoplasmainfection an early presentation of classical Hodgkinlymphoma which was diagnosed due to presen-tation with an atypical pneumonia Skin mani-festation of Hodgkin lymphoma could be due topara neoplastic syndrome or skin infiltration in laterstages But in this patient the cutaneous rash wasbe attributed to the mycoplasma infectionPossibility of DRESS mobiliform rash of EBVinfection treated with amoxicillin and Sweetsyndrome was excluded by the absence of facialoedema negative EBV serology and absence oftender plaques respectively
Due to early stage and involvement of cervicalregion radiotherapy was omitted from manage-ment plan to prevent unwanted side effects Sincethis was a young patient with early stage andfavourable prognostic markers we expect a goodprognosis
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr VC Panditha GunawardenaConsultant Haematologist Teaching HospitalKandy Sri Lanka
E-mail drvishchanyahoocom
WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

WAON Wickramasinghe et al SLJH 2018 10(1) 25-27
The Sri Lanka Journal of Haematology 27
References
1 Blombery P Linch D et al Hodgkin lymphomaPostgraduate Haematology 7th Edition Jan 2016
2 Follows GA Ardeshna KM Barrington SF CulliganDJ Hoskin PJ Linch D et al Guidelines for the firstline management of classical Hodgkin lymphomaBr J Haematol 2014 166(1) 34-49 doi 101111bjh12878
3 Collins GP Parker AN Pocock C Kayani I Sureda AIllidge T et al Guideline on the management ofprimary resistant and relapsed classical Hodgkin
lymphoma Br J Haematol 2014 164(1) 39-52 doi101111bjh12582
4 Eichenauer DA Engert A Andreacute M Federico M IllidgeT Hutchings M et al Hodgkinrsquos lymphoma ESMOClinical Practice Guidelines for diagnosis treatmentand follow-up Ann Oncol 2014 25 Suppl 3 iii70-5doi 101093annoncmdu181
5 Hoppe RT Advani RH Ai WZ Ambinder RF Aoun PArmand P et al NCCN Guidelines Insights HodgkinLymphoma Version 12018 J Natl Compr Canc Netw2018 16(3) 245-254 doi 106004jnccn20180013
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
28
1Registrar in Clinical Haematology 2Postgraduatetrainee in Clinical Haematology 3ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
Abstract
Paroxysmal cold haemoglobinuria (PCH) is anacquired autoimmune haemolytic anaemia whichcauses intravascular haemolysis and anaemia It isa rare disease and commonly described amongpaediatric patients This case series describes fourpatients admitted to Lady Ridgeway hospital forchildren within a period of three months Theywere successfully managed with blood trans-fusions and steroid therapy Donath Landsteinertest which is the confirmatory test was not helpfulin confirming the diagnosis in two out of the fourpatients Therefore clinical diagnosis is of para-mount importance for early initiation of appro-priate treatment to control haemolysis andminimize disease related complications
Introduction
Paroxysmal cold hemoglobinuria (PCH) is a rareacquired autoimmune hemolytic anemia causedby immunoglobulin G (IgG) antibodies that bindsto P antigens in red cells in cold temperatures andcause complement mediated haemolysis at warmtemperatures PCH usually affects young childrenand they present with high fever chills abdominalpain passage of red-brown coloured urine yello-wish discolouration of eyes and commonly upperrespiratory tract symptoms The diagnostic test forPCH is the Donath-Landsteiner test an in vitroassay for biphasic hemolysis12 We report 4 casesof PCH presenting within 3 months during a coldrainy season in 2018
Paroxysmal cold haemoglobinuria A case series in children
DP Ranasinghe1 MS Buddhadasa2 AN Hettiarachchi2 C Thevarapperuma3 N Senadheera3
Case report II
Key words paroxysmal cold haemoglobinuria steroids leukocytosis
SLJH 2018 10(1) 28-32
Most literature describes this disease to be lsquoself-limitingrsquo but in our experience all patients re-quired blood transfusions and three out of fourcases needed steroid therapy to control the haemo-lysis The timely recognition of this entity by physi-cians and haematologists will allow promptmanagement and will help resolution of hemolysiswithout complications
Case 1
A previously healthy one year and four months oldmale child was transferred from Ratnapura GeneralHospital with anaemia jaundice and passage ofdark coloured urine
He had cough and cold for 3 weeks and fever forthe last 3 days He had passed dark red colouredurine after admission to hospital The initiallaboratory findings included a hemoglobin of98 gdL which dropped to 55 gdL despite redcell transfusions Reticulocyte count graduallyincreased from 6 to 24
Donath-Landsteiner test was done twice and wasnegative Initially they could not interpret it dueto marked haemolysis This test was repeatedwhen the haemoglobinuria resolved but wasnegative again It was done both times by the directmethod The indirect DL test was not available
As the child developed features of heart failureintravenous methyl prednisolone 30mgkg dailywas given for 3 days followed by oral prednisolone1 mgkgdaily He was also given folic acid 5 mgdaily and intravenous antibiotics During hishospital stay the patient received transfusions ofleuko-reduced red cell concentrates
After 9 days of illness haemoglobin was stable andurine colour became normal He was discharged10 days after admission in a stable conditionSteroids were tailed off and stopped during clinicfollow-up
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
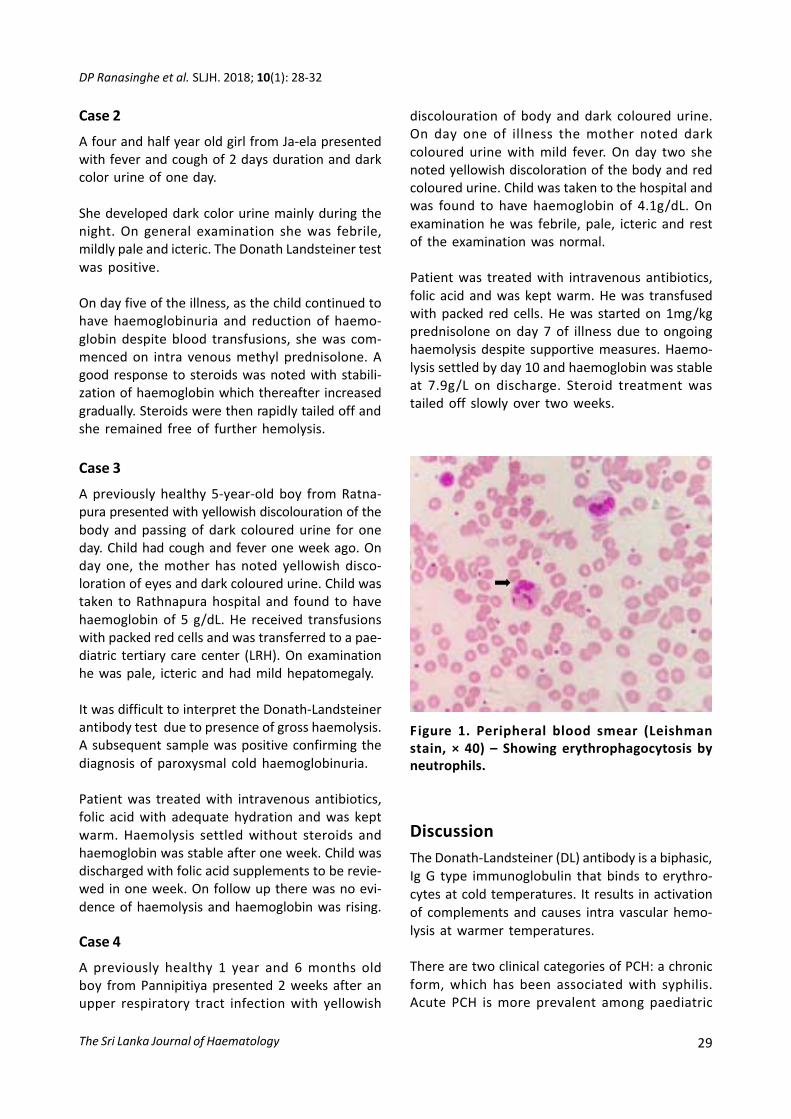
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 29
Case 2
A four and half year old girl from Ja-ela presentedwith fever and cough of 2 days duration and darkcolor urine of one day
She developed dark color urine mainly during thenight On general examination she was febrilemildly pale and icteric The Donath Landsteiner testwas positive
On day five of the illness as the child continued tohave haemoglobinuria and reduction of haemo-globin despite blood transfusions she was com-menced on intra venous methyl prednisolone Agood response to steroids was noted with stabili-zation of haemoglobin which thereafter increasedgradually Steroids were then rapidly tailed off andshe remained free of further hemolysis
Case 3
A previously healthy 5-year-old boy from Ratna-pura presented with yellowish discolouration of thebody and passing of dark coloured urine for oneday Child had cough and fever one week ago Onday one the mother has noted yellowish disco-loration of eyes and dark coloured urine Child wastaken to Rathnapura hospital and found to havehaemoglobin of 5 gdL He received transfusionswith packed red cells and was transferred to a pae-diatric tertiary care center (LRH) On examinationhe was pale icteric and had mild hepatomegaly
It was difficult to interpret the Donath-Landsteinerantibody test due to presence of gross haemolysisA subsequent sample was positive confirming thediagnosis of paroxysmal cold haemoglobinuria
Patient was treated with intravenous antibioticsfolic acid with adequate hydration and was keptwarm Haemolysis settled without steroids andhaemoglobin was stable after one week Child wasdischarged with folic acid supplements to be revie-wed in one week On follow up there was no evi-dence of haemolysis and haemoglobin was rising
Case 4
A previously healthy 1 year and 6 months oldboy from Pannipitiya presented 2 weeks after anupper respiratory tract infection with yellowish
discolouration of body and dark coloured urineOn day one of illness the mother noted darkcoloured urine with mild fever On day two shenoted yellowish discoloration of the body and redcoloured urine Child was taken to the hospital andwas found to have haemoglobin of 41gdL Onexamination he was febrile pale icteric and restof the examination was normal
Patient was treated with intravenous antibioticsfolic acid and was kept warm He was transfusedwith packed red cells He was started on 1mgkgprednisolone on day 7 of illness due to ongoinghaemolysis despite supportive measures Haemo-lysis settled by day 10 and haemoglobin was stableat 79gL on discharge Steroid treatment wastailed off slowly over two weeks
DiscussionThe Donath-Landsteiner (DL) antibody is a biphasicIg G type immunoglobulin that binds to erythro-cytes at cold temperatures It results in activationof complements and causes intra vascular hemo-lysis at warmer temperatures
There are two clinical categories of PCH a chronicform which has been associated with syphilisAcute PCH is more prevalent among paediatric
Figure 1 Peripheral blood smear (Leishmanstain times 40) ndash Showing erythrophagocytosis byneutrophils
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
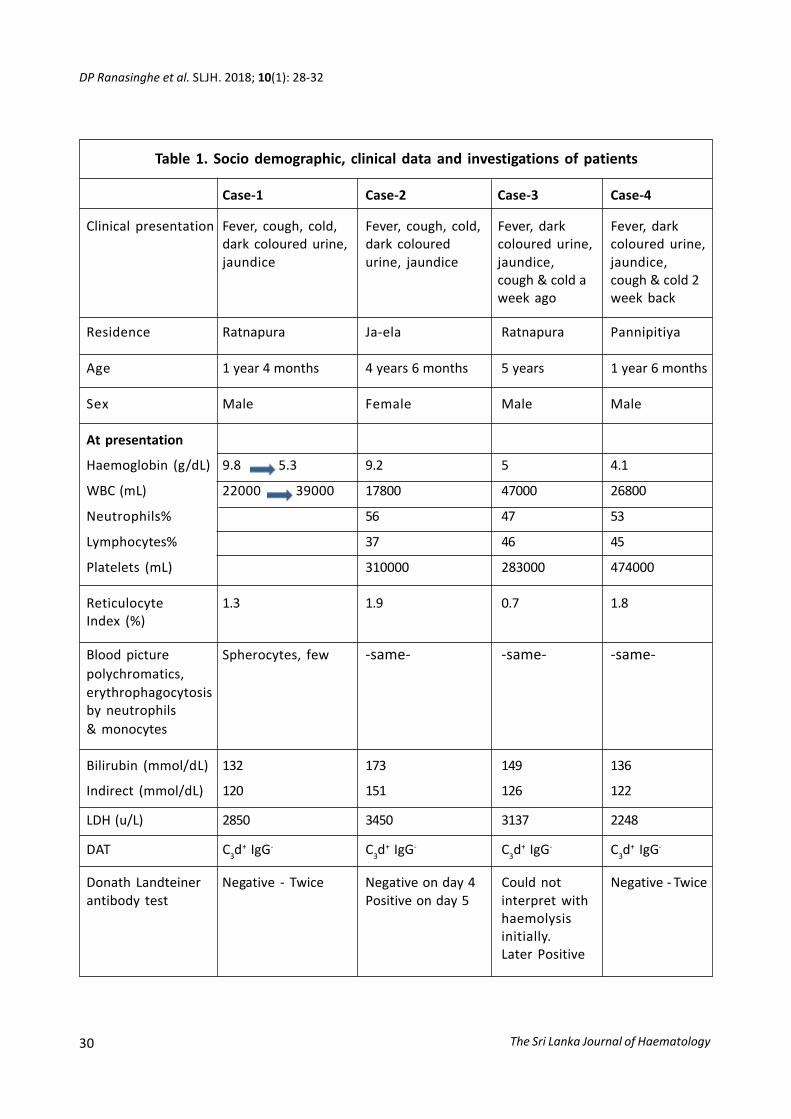
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
30
Clinical presentation Fever cough cold Fever cough cold Fever dark Fever darkdark coloured urine dark coloured coloured urine coloured urinejaundice urine jaundice jaundice jaundice
cough amp cold a cough amp cold 2week ago week back
Table 1 Socio demographic clinical data and investigations of patients
Case-1 Case-2 Case-3 Case-4
Residence Ratnapura Ja-ela Ratnapura Pannipitiya
Age 1 year 4 months 4 years 6 months 5 years 1 year 6 months
Sex Male Female Male Male
At presentation
Haemoglobin (gdL) 98 53 92 5 41
WBC (mL) 22000 39000 17800 47000 26800
Neutrophils 56 47 53
Lymphocytes 37 46 45
Platelets (mL) 310000 283000 474000
Reticulocyte 13 19 07 18Index ()
Blood picture Spherocytes few -same- -same- -same-polychromaticserythrophagocytosisby neutrophilsamp monocytes
Bilirubin (mmoldL) 132 173 149 136
Indirect (mmoldL) 120 151 126 122
LDH (uL) 2850 3450 3137 2248
DAT C3d+ IgG- C3d
+ IgG- C3d+ IgG- C3d
+ IgG-
Donath Landteiner Negative - Twice Negative on day 4 Could not Negative - Twiceantibody test Positive on day 5 interpret with
haemolysisinitiallyLater Positive
DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

DP Ranasinghe et al SLJH 2018 10(1) 28-32
The Sri Lanka Journal of Haematology 31
patients and is usually associated with upperrespiratory tract infections Chronic PCH is notcommonly seen now due to the development ofpotent antibiotics and proper management ofsyphilis12
The causative agent is often not identified in acutePCH However several infectious agents have beenimplicated including measles mumps EBV cyto-megalovirus varicella zoster virus adenovirusinfluenza and rarely bacterial infections likeMycoplasma pneumoniae Haemophilus influenzaeand Escherichia coli3 Some cases are reportedfollowing immunization too Rarely an associationwith lympho-proliferative disorders and collagenvascular diseases has been described All ourpatients presented with symptoms and signs ofupper respiratory tract infection which is a commonassociation
PCH is not a commonly encountered entity butthese 4 cases were reported within a 3 monthperiod from April to June 2018 During that timethe climate was cold with frequent heavy showersand an epidemic of upper respiratory tractinfections were reported in various parts of thecountry which were the causative factors that leadto these cases
As described earlier acute PCH is typically occursin children younger than 5 years which wasconsistent with our cases although it can affectpatients of all ages Acute PCH frequently causesevere haemolytic anaemia but the illness resolvesspontaneously within a few days to several weeksafter the onset
Pallor jaundice and haemoglobinuria are the mostcommon clinical findings Rapidly worseninganaemia with relative reticulocytopenia is knownto occur at the time of presentation followed byreticulocytosis Reticulocytopenia represents anineffective marrow response either to viral haemo-poietic suppression or preferential destruction ofred cells by DL antibodies4 All these childreninitially had reticulocytopaenia followed by reti-culocytosis
According to literature spherocytosis is particularlycommon in peripheral blood which was seen in all
our patients Other features are fragmented redcells polychromasia red cell agglutination erythro-phagocytosis and nucleated red cells Erythro-phagocytosis by neutrophils is strongly associatedwith PCH Erythrophagocytosis by monocytes occurin autoimmune haemolytic anaemia of variousaetiologies5
In our patients positivity of haemoglobinuriaconfirmed intravascular haemolysis and the DATpositivity with C3d specificity supported immune-mediated haemolysis The autoantibody associatedwith PCH is termed a biphasic hemolysin as itsensitizes red blood cells in the cold but haemo-lyses when red cells reach 37degC DL antibodies arevery potent even with low titers that they cancause significant haemolysis Disease is usuallyself-limiting and resolves within few weeks as theperiod of antibody production is relatively briefIn the first and fourth patients DL antibody wasnegative but the clinical and the rest of thehaematological and immunological test resultswere supportive of the diagnosis of PCH
As the DL antibody like the cold agglutinin bindsat lower temperatures keeping the patient warmis a mainstay of therapy These children weremanaged with blood transfusions through awarmer and were given folic acid6 It is essentialto maintain a good hydration as free haemoglobinformed due the intra vascular haemolysis can resultin acute renal damage
Leukopenia may also be seen early in the coursebut this is frequently followed by a markedleukocytosis (10-80 times 109L) which was common toall our patients Clinical assessment is of utmostimportance and CRP is very helpful when takingmanagement decisions especially regardingantibiotics in patients with rising and elevatedwhite cell counts
The severity of anaemia reticulocytopenia andfeatures of heart failure lead to the initiation ofsteroids in our patients resulting in a goodresponse Corticosteroids are often given althoughtheir effectiveness is difficult to evaluate becauseof the transient nature of haemolysis7 Cortico-steroids may depress antibody production anddecrease complement receptor-mediated phago-
The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

The Sri Lanka Journal of Haematology
DP Ranasinghe et al SLJH 2018 10(1) 28-32
32
cytosis in the liver and spleen According toavailable data corticosteroids do not provide muchclinical benefit in PCH However quite contrary tothese reports three of our patients experiencedsevere ongoing haemolysis despite supportivecare and they showed a dramatic response tocommencement of steroids
References
1 Sokol RJ Booker DJ Stamps R Paroxysmal coldhemoglobinuria and the elusive Donath-Landsteinerantibody Immunohematology 1998 14(3) 109-12
Authorship
Contribution All authors contributed equally
Conflict-of-interest disclosure The authors declareno conflict of interest
Correspondence Dr N Senadheera ConsultantHaematologist Lady Ridgeway Hospital forChildren Colombo Sri Lanka
E-mail nipunikasenadheeragmailcom
2 Sanford KW Roseff SD Detection and significance ofDonath-Landsteiner Antibodies in a 5-year-oldFemale Presenting with Hemolytic Anemia Lab Med2010 41(4) 209-12
3 Wolach B Heddle N Barr RD Zipursky A Pai KRBlajchman MA Transient Donath-Landsteinerhaemolytic anaemia Br J Haematol 1981 48(3)425-34
4 Sokol RJ Booker DJ Stamps R ErythropoiesisParoxysmal Cold Haemoglobinuria A Clinico-Pathological Study of Patients with a Positive Donath-Landsteiner Test Hematology 1999 4(2) 137-64
5 Mukhopadhyay S Keating L Souid AK Erythro-phagocytosisin Paroxysmal Cold HemoglobinuriaAm J Hematol 2003 74(3) 196-7
6 Asfir EL Senadheera N Jayasinghe S Liyanage HParoxysmal cold haemoglobinuria in a pregnantwoman leading to severe anaemia and fetal loss SriLanka Journal of Haematology 2015 7(1) 25
7 Gunawardena D Velu M Senaviratne SN Case reporton a child with paroxysmal cold haemoglobinuriaIndian J Hematol Blood Transfus 2012 28(2) 112-3doi 101007s12288-011-0094-y
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
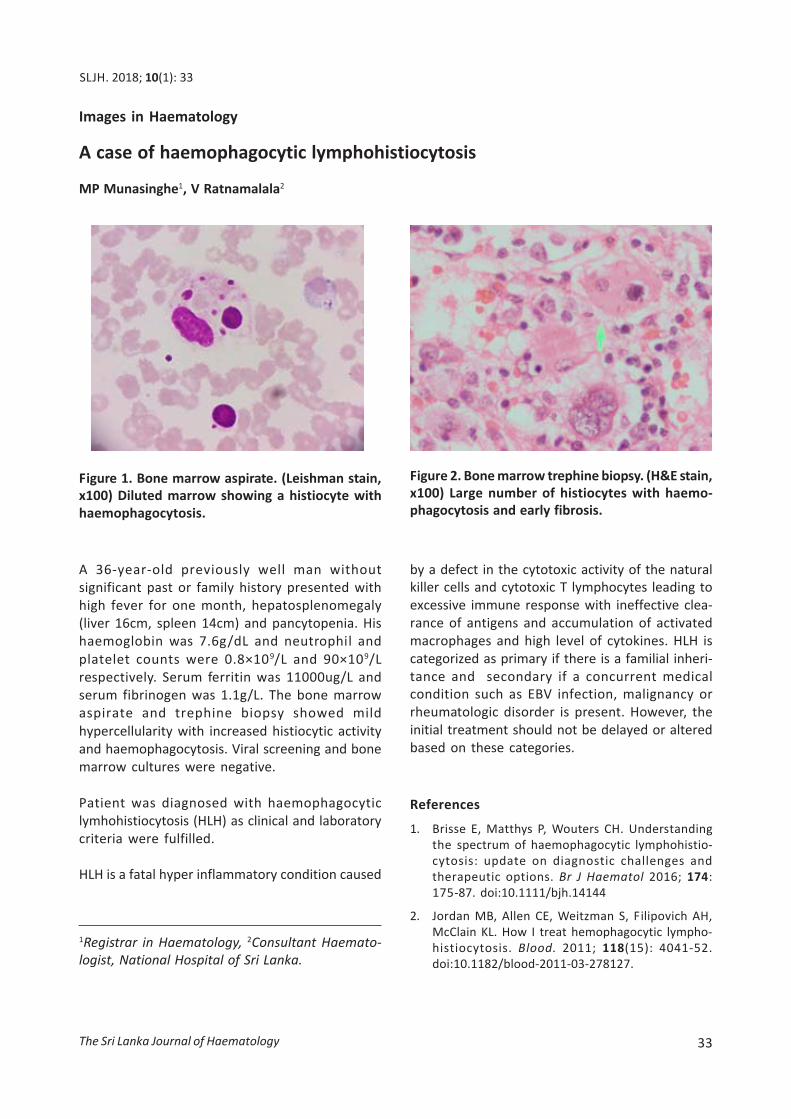
MN Dilhani et al SLJH 2015 7 32
The Sri Lanka Journal of Haematology 33
A 36-year-old previously well man withoutsignificant past or family history presented withhigh fever for one month hepatosplenomegaly(liver 16cm spleen 14cm) and pancytopenia Hishaemoglobin was 76gdL and neutrophil andplatelet counts were 08times109L and 90times109Lrespectively Serum ferritin was 11000ugL andserum fibrinogen was 11gL The bone marrowaspirate and trephine biopsy showed mildhypercellularity with increased histiocytic activityand haemophagocytosis Viral screening and bonemarrow cultures were negative
Patient was diagnosed with haemophagocyticlymhohistiocytosis (HLH) as clinical and laboratorycriteria were fulfilled
HLH is a fatal hyper inflammatory condition caused
A case of haemophagocytic lymphohistiocytosis
MP Munasinghe1 V Ratnamalala2
Images in Haematology
SLJH 2018 10(1) 33
Figure 1 Bone marrow aspirate (Leishman stainx100) Diluted marrow showing a histiocyte withhaemophagocytosis
Figure 2 Bone marrow trephine biopsy (HampE stainx100) Large number of histiocytes with haemo-phagocytosis and early fibrosis
by a defect in the cytotoxic activity of the naturalkiller cells and cytotoxic T lymphocytes leading toexcessive immune response with ineffective clea-rance of antigens and accumulation of activatedmacrophages and high level of cytokines HLH iscategorized as primary if there is a familial inheri-tance and secondary if a concurrent medicalcondition such as EBV infection malignancy orrheumatologic disorder is present However theinitial treatment should not be delayed or alteredbased on these categories
References
1 Brisse E Matthys P Wouters CH Understandingthe spectrum of haemophagocytic lymphohistio-cytosis update on diagnostic challenges andtherapeutic options Br J Haematol 2016 174175-87 doi101111bjh14144
2 Jordan MB Allen CE Weitzman S Filipovich AHMcClain KL How I treat hemophagocytic lympho-histiocytosis Blood 2011 118(15) 4041-52doi101182blood-2011-03-278127
1Registrar in Haematology 2Consultant Haemato-logist National Hospital of Sri Lanka
The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

The Sri Lanka Journal of Haematology34
1) TTFFT
2) TTFTT
3) TTTTF
Discussion (MCQ points are highlighted in bold)
Many hereditary and acquired causes areresponsible for neutropenia in children Chronicneutropenia is defined as neutropenia lasting forgt 6 months1
Kostmann syndrome causes a severe neutropeniawith neutrophil counts below 200mm3 Althoughit has an autosomal recessive inheritance it mayalso occur as a result of autosomal dominantinheritance or spontaneous mutations Thesemutations in the neutrophil elastase gene haltmaturation in the promyelocyte myelocyte stagein the bone marrow Clinically severe bacterialinfections including otitis media pneumoniasepsis and cutaneous and hepatic abscesses areseen The disease becomes symptomatic in thefirst month in 50 of the cases and in 100 by sixmonths of age2 Granulocyte colony stimulatingfactor (at a dose of 5 μμμμμgkg) increases maturationof myelocytes Bone marrow trasnplantationoffers a definitive cure In the presence of cyto-genetic changes these patients carry a risk ofmalignant transformation to myelodysplasticsyndrome (MDS) and acute myeloid leukemia(AML) The factors which determine the risk oftransformation to leukemia include the neutrophilcount mutation type and intensity of G-CSFtreatment1
Infection-related neutropenia is the mostcommon cause of neutropenia in children Acutetransient neutropenia most commonly occursafter viral infections such as varicella measlesrubella hepatitis A and B influenza cytomega-lovirus Ebstein-Barr virus parvovirus B19adenovirus and coxsackie Neutropenia may alsobe observed in bacterial infections includingStaphylococcus aureus brucella rickettsia andtuberculosis Usually neutropenia recovers withrecovery of the infection Rarely however neutro-
Answers for the CME Neutropenia in infants and children
penias which develop secondary to infection lastsfor longer than eight weeks and may persist for upto even one year1
Neutropenia is observed in congenital metabolicdiseases including hyperglycinuria oroticaciduriametylmalonicaciduria hypergly cinemia and morecommonly glucogen storage disease (GSD) type1b patients
Cyclic neutropenia is characterized with recurrentinfections which develop in relation to severeneutropenia every 21 days (14-42 days) withregular frequency The attacks generally last for 3-6 days and most patients benefit from low dose Gndash CSF The patients are asymptomatic during theintervals and the neutrophil counts are normalComplete blood count is performed 2-3 times aweek for six weeks to differentiate cyclicneutropenia from severe chronic neutropenia
Many medications lead to neutropenia in child-hood too Some associated drugs are pheno-thiazines semi-synthetic penicillins non-steroidanti-inflammatory drugs aminopyrine derivativesbarbiturates antithyroid drugs Neutropeniadevelops in 2-3 months with use of medicationsand usually improves within 10 days of discon-tinuation of the drug but sometimes this durationmay be longer
Primary autoimmune neutropenia is rare and isobserved mostly in girls and in children below theage of two years Recurrent mild cutaneous andupper respiratory tract infections are seen Thegold standard in the diagnosis is demonstration ofneutrophil specific autoantibodies1 The diseasehas a good prognosis and neutropenia generallyimproves spontaneously Most patients are givenprophylactic antibiotics but immunosupressivedrugs are not used In severe infection high doseintravenous immunoglobulin and G-CSF are used
Benign familial neutropenia is observed morecommonly in some ethnic groups Since neutro-penia is mild there are no infections Bone marrowis normal It has an autosomal dominant inheri-tance and blood counts of the parents and siblings
The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena

The Sri Lanka Journal of Haematology 35
will help in the diagnosis Chronic benignneutropenia also follows a benign course ofdisease Although the absolute neutrophil countranges between 200 and 500 mm3 G ndash CSF is notrecommended unless there are repetitiveinfections1 The bone marrow is either normal orincrease in the myeloid precursors is observedwith maturation paused in the late stage
References
1 Celkan T Koc BS Approach to the patient withneutropenia in childhood Turk Pediatri Ars 201550 136-44 doi105152TurkPediatriArs20152295
2 Soylu H Cunuvar A Ustun N Congenital Agranulo-cytosis (Kostmannrsquos Syndrome) and G-CSF Therapyin an Infant Turk J Haematol 1999 16(4) 171-5
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena
The Sri Lanka Journal of Haematology is the official publication of the Sri Lanka College of HaematologistsAll views expressed in the Journal are those of the individual authorscontributors and the publisherdoes not take any responsibility for the views expressed or the material submitted by the authorscontributors
Information and copies could be obtained from the Editors Sri Lanka Journal of Haematology No 06Wijerama Mawatha Colombo 07
The Journal will publish original articles perspectives case reports and images in haematology Lettersto the Editor are also welcome Review articles and leading articles will be solicited by the EditorsAuthor Guidelines are available in the College website httpwwwslchaemlk
Publications by the Sri Lanka College of Haematologists
Thalassaemia ndash M Nanada Prematileke
Anticoagulation with unfractionated heparin ndash Arundathi P Kurukulasuriya
Warfarin ndash Mala Tudawe
Guidelines for the treatment of bleeding in Haemophilia ndash Sudharma Vidyatilake
What you should know about Haemophilia (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) ndash Sudharma Vidyatilake
What you should know about ITP (in Sri Lanka) (English Sinhala and Tamil translations)
ndash Dammika Gunawardena