Embed Size (px)
Citation preview

The Study of a Unique Athletic Population: Health Concerns, Interventions, and Prevention in Elite Ballet Dancers
Ashley F. Doyle-Lucas
Dissertation submitted to the faculty of the Virginia Polytechnic Institute and State University in partial fulfillment of the requirements for the degree
of
Doctor of Philosophy In
Human Nutrition, Foods and Exercise
Brenda M. Davy, Chair Kevin P. Davy Billie Lepczyk
Janet W. Rankin Kerry J. Redican
February 1st, 2010 Blacksburg, Virginia
Keywords: Female Athlete Triad; Energetic Efficiency; Low Energy
Availability; Ballet Dancers; Nutrition Education
Copyright © 2010 by Ashley Doyle-Lucas

The Study of a Unique Athletic Population: Health Concerns, Interventions, and Prevention in Elite Ballet Dancers
Ashley F. Doyle-Lucas
ABSTRACT
Ballet dancers are a unique population of athletes in that, unlike other sports,
their success strictly depends on both physical capabilities and aesthetic factors 1-3.
While the physical demands of the performing sport are strenuous, ballet dancers
are often required to exhibit a thin physique, frequently resulting in weights 10-
12% below the ideal 4, 5. These low weights are commonly achieved by low energy
intakes 4, 6 which increase dancers’ susceptibility to the development of various
health conditions 7. Research investigating the health of dancers, however, is
limited and hampered by methodological limitations. To address these issues, we
tested the hypothesis that dancers would report a low habitual energy intake and,
therefore, be subject to conditions comprising the Female Athlete Triad, including
low energy availability, suboptimal bone density and menstrual irregularities. In
addition, we hypothesized that elite female dancers would have lower than
expected resting metabolic rate (RMR) based upon their fat-free mass, and thus
greater energetic efficiency as a result of chronic energy deficiency. As
hypothesized, dancers reported a significantly lower energy intake and exhibited a
lower RMR as compared to lean, pair-matched controls 8. Because treatment of

iii
these metabolic abnormalities is challenging, prevention of adverse health
outcomes among adolescent pre-professional dancers is key in promoting overall
health and optimal performance. Through our subsequent “formative work”, we
determined that the current availability of nutrition education offered to both
professional and pre-professional dancers is minimal and of questionable quality.
Thus, we developed, implemented, and evaluated a DVD-based educational
program, entitled “Nutrition for Optimal Performance”, aimed at improving health
knowledge and behaviors of pre-professional adolescent ballet dancers. Our
findings indicate that participants increased their knowledge of basic nutrition
principles and self-efficacy for adopting healthier dietary habits, as compared to
pre-program and control group scores, and that knowledge gains were sustained at
a six-week follow-up assessment. Collectively, these studies provide the field of
dance medicine with novel findings related to the characteristics and health
conditions of professional ballet dancers, and the effectiveness of a low-resource,
disseminable nutrition education program which promotes the health and optimal
performance of pre-professional adolescent ballet dancers.
References
1. Benson JE, Geiger CJ, Eiserman PA, et al. Relationship between nutrient intake, body mass index, menstrual function, and ballet injury. J Am Diet
Assoc. 1989;89(1):58-63.

iv
2. Cassill K. The bane of the ballerina. Life-threatening thinness. Science
Digest. 1980;87:52-55. 3. Micheli LJ, Gillespie WJ, Walaszek A. Physiologic profiles of female
professional ballerinas. Clin Sports Med. 1984;3(1):199-209. 4. Kaufman BA, Warren MP, Dominguez JE. Bone Density and amenorrhea in
ballet dancers are related to a decreased resting metabolic rate and lower leptin levels. J Cli Endo Met. 2002;87(6):2777-2783.
5. Shah S. Caring for the dancer: special considerations for the performer and
troupe. Curr Sports Med Rep. 2008;7(3):128-132. 6. Benson J, Gillien DM, Bourdet K, et al. Inadequate Nutrition and Chronic
Calorie Restriction in Adolescent Ballerinas. Phys Sportsmed. 1985;13(10):79-90.
7. Nattiv A, Loucks AB, Manore MM. The female athlete triad. Med Sci Sports
Exerc. 2007;39(10):1867-1882. 8. Doyle-Lucas AF, Akers JD, Davy BM. Energetic Efficiency, Menstrual
Irregularity, and Bone Mineral Density in Elite Professional Female Ballet Dancers. J Dance Med Sci, In Press.

v
Table of Contents Abstract Table of Contents List of Tables List of Figures Chapter 1: Chapter 2: Chapter 3:
Introduction References Energetic Efficiency, Menstrual Irregularity, and Bone Mineral Density in Elite Professional Female Ballet Dancers Abstract Introduction Materials and Methods Results Discussion Conclusion Acknowledgements References Dancers’ Health Services Survey: Current Practices among Professional
Ballet Companies Introduction Materials and Methods Results Conclusion References
ii v ix xii 1 5 6 8 11 16 18 22 23 24 36 37 38 39 41

vi
Chapter 4: Chapter 5: Chapter 6: Appendices:
Interests of the Target Audience: Young Dancers’ Nutrition Survey Purpose Materials and Methods Results Conclusion Development and Evaluation of an Educational Program for Pre-professional Adolescent Ballet Dancers: Nutrition for Optimal Performance
Abstract Introduction Materials and Methods Results Discussion Conclusion Acknowledgements References Conclusions Appendix A- Institutional Review Board Full Approval (Energetic Efficiency, Menstrual Irregularity, and Bone Mineral Density in Elite Professional Female Ballet Dancers) Appendix B- Institutional Review Board Amendment One Approval (Energetic Efficiency, Menstrual Irregularity, and Bone Mineral Density in Elite Professional Female Ballet Dancers) Appendix C- Institutional Review Board Continuation Approval (Energetic Efficiency, Menstrual Irregularity, and Bone Mineral Density in Elite Professional Female Ballet Dancers) Appendix D- Institutional Review Amendment Two Approval (Energetic Efficiency, Menstrual Irregularity, and Bone Mineral Density in Elite Professional Female Ballet Dancers)
44 44 44 46 48 49 53 59 62 65 65 66 82 85 86 87 88

vii
Appendix E- Institutional Review Board Approval (Dancers’ Health
Services Survey: Current Practices among Professional Ballet Companies) Appendix F- Survey Tool: Dancers’ Health Services Survey- Current Practices among Professional Ballet Companies Appendix G- Institutional Review Board Approval (Development and Evaluation of an Educational Program for Pre-professional Adolescent Ballet Dancers) Appendix H- Institutional Review Board Amendment One Approval (Development and Evaluation of an Educational Program for Pre-professional Adolescent Ballet Dancers) Appendix I- Institutional Review Board Amendment Two Approval (Development and Evaluation of an Educational Program for Pre-professional Adolescent Ballet Dancers) Appendix J- Institutional Review Board Continuation Approval (Development and Evaluation of an Educational Program for Pre-professional Adolescent Ballet Dancers) Appendix K- Sports Nutrition Knowledge and Behavior Questionnaire (Development and Evaluation of an Educational Program for Pre-professional Adolescent Ballet Dancers) Appendix L- Nutrition for Optimal Performance Script (Development and Evaluation of an Educational Program for Pre-professional Adolescent Ballet Dancers)
Class One: An Overview: Nutrition for Pre-professional
Dancers and the Importance of Health Behaviors Class Two: Nutrition Principles for Dancers
Class Three: Eating for Optimal Health and Performance Appendix M- Nutrition for Optimal Performance Handouts (Development and Evaluation of an Educational Program for Pre-professional Adolescent Ballet Dancers)
Class One: Healthy Behaviors and The Female Athlete Triad:
Being the Best You Can Be! Class Two: Nutrition Principles for Dancers: Learning the
Basics. Foods and Their Nutritional Benefits
Class Two: Worksheet: Application of Nutrition Principles Class Three: Eating for Optimal Health and Performance:
What Should I Eat?
89 90 93 94 95 96 97 102 107 118 127 128 129 130 132

viii
Appendix N- Nutrition for Optimal Performance Control Group Packet (Development and Evaluation of an Educational Program for Pre-professional Adolescent Ballet Dancers)
133

ix
LIST OF TABLES
Chapter 2:
Chapter 3:
Chapter 4:
Table 1. Demographic Characteristics of Pair-Matched Female Elite
Dancers and Lean Control Women
Table 2. Eating Behaviors in Pair-Matched Female Elite Dancers and
Lean Control Women
Table 3. Female Athlete Triad Characteristics in Pair-Matched Elite
Female Dancers and Lean Control Women
Table 4. Differences in Female Athlete Triad Characteristics and
Energetic Efficiency According to Menstrual Status Among
Pair-Matched Elite Female Dancers and Lean Control Women
Table 5. Dancers’ Health Services Survey: Questions and Responses
Table 6. Interests of the Target Audience: Young Dancers’ Nutrition
Survey
27
28
29
30
42
47

x
Chapter 5:
Table 7. Nutrition for Optimal Performance: Theoretical Constructs 69
Incorporated Into Program Content
Table 8. Nutrition for Optimal Performance: Class Titles and
Objectives
Table 9. Sports Nutrition Knowledge and Behavior Questionnaire:
Response Options and Associated Question Stems
Table 10. Comparison of Baseline Demographic Characteristics of
Intervention (I) and Control (C) Companies
Table 11. Baseline Demographic Characteristics of Enrolled
Participants
Table 12. Baseline and 6-Week Follow-Up Assessment Results for
Intervention and Control Participants for Nutrition
Knowledge, Theory-Based Behavioral Constructs and Self-
Reported Dietary Intake
69
70
71
73
74
75

xi
Table 13. Intervention Group Results of Participants Completing All
Baseline, Immediate Post-Program, and 6-Week Follow-Up
Assessments
78

xii
LIST OF FIGURES
Chapter 2:
Chapter 5:
Figure 1. Resting metabolic rate (kcal/day) in pair-matched elite
female dancers and lean control women.
Figure 2. Energetic efficiency: resting metabolic rate (kcal/kg
FFM/day) in pair-matched elite female dancers and lean
control women.
Figure 3. Observed versus predicted resting metabolic rate in elite
female ballet dancers.
Figure 4. Observed versus predicted resting metabolic rate in lean
control women.
Figure 5. Overview: Program Development, Implementation, and
Evaluation of Nutrition for Optimal Performance.
32
33
34
35
81

1
CHAPTER 1
Introduction
Female athletes who participate in sports or activities that emphasize low body weight are
at increased risk for the development of clinical conditions that may elicit significant health
concerns 1. Dancers comprise one athletic population that may be susceptible to the
development of various clinical conditions, as the “sport” often demands its athletes to be
extremely lean. Dancers are a unique group; their success depends on both physical capabilities
and aesthetic factors 2-4. Also, the strenuous training demands and performance schedules of
professional ballet dancers differ from those of other athletes, requiring dancers to perform at
their highest ability throughout a nine-month performance season.
The physical condition of female athletes may oscillate along a spectrum of health and
disease. Depending upon the athlete’s diet and exercise habits, her physical condition may shift
toward either the robust or pathological end of the health/disease spectrum. Three interrelated
conditions known to affect female athletes located along the pathological end of the spectrum
include low energy availability, amenorrhea/irregular menstrual function, and osteoporosis/ low
bone mineral density, which collectively have been termed the Female Athlete Triad (FT) 1.
Dancers represent an athletic population that often exhibits characteristics of the FT; they
chronically under-eat to achieve low body weight 5-7, which may in turn effect the proper
functioning of various metabolic processes 8 interfering with healthy menstruation and bone
growth.
Unlike other populations of athletes, research on the health of dancers is limited and
hampered by methodologic limitations 8. Therefore, the purpose of the following research was

2
to: 1) determine the characteristics of dancers which may lead to the development of the
conditions of the FT as well as increased energetic efficiency, 2) assess the availability of
nutrition education to professional and adolescent dancers and determine the health issues of
interest among adolescent dancers, and 3) develop, implement and evaluate a nutrition education
program for pre-professional adolescent ballet dancers aimed at preventing the development of
the FT and promoting optimal performance.
The specific aim of the first investigation was to compare the physical and behavioral
characteristics of female elite professional ballet dancers to sedentary/recreationally active non-
dancing control participants, including characteristics of the FT and energetic efficiency. We
hypothesized that the dancers would report a low habitual energy intake and, therefore, be
subject to conditions comprising the FT, including low energy availability, suboptimal bone
density and menstrual irregularities. Additionally, we hypothesized that elite female dancers
would have a lower than expected resting metabolic rate (RMR) based upon their fat-free mass
(FFM), and thus greater energetic efficiency as a result of chronic energy (caloric) deficiency.
Two preliminary studies were then conducted, one which assessed the nutritional
knowledge and beliefs of adolescent dancers, and a second which assessed the current
availability and type of nutritional education offered to professional ballet dancers and
adolescent dancers training in professional academies. These preliminary studies revealed the
typical nutrition knowledge, beliefs, and areas of interest among young dancers as well as the
need for a high-quality nutrition education program that could be feasibly delivered to pre-
professional adolescent dancers.

3
Dancers’ health and the “sport” of ballet are rarely investigated; to date, limited research
has been conducted on the effectiveness of nutrition education interventions which promote
dancers’ health. Research aimed at preventing the clinical conditions that often plague
professional dancers designed to educate the dancing youth, when health behaviors, habits, and
perceptions are forming, is clearly needed. Thus, we developed a nutrition education program
entitled “Nutrition for Optimal Performance” based upon the findings of our first laboratory-
based investigation, two “formative work” studies, and the theoretical constructs of the Health
Belief Model and Social Cognitive Theory. To allow for the possibility of large-scale
reproduction, ease of dissemination, and low delivery expense for ballet companies, this nutrition
education was produced in a DVD format. The development, implementation, and evaluation of
this DVD-based education program aimed at improving health knowledge and behaviors of pre-
professional adolescent dancers comprised the final investigation. Overall objectives of this
program were to: 1) inform young dancers of the conditions comprising the FT and increase their
awareness of risks associated with the disorder, 2) educate dancers on basic nutrition principles
that may promote overall health and performance, and 3) provide dancers with skills needed to
develop healthy lifestyle habits. Specifically, we aimed to increase knowledge of basic nutrition
principles, improve self-efficacy for adopting healthy dietary habits, and increase the
consumption of fruit, vegetable, and high-calcium foods while decreasing consumption of
nutrient-poor, high-fat and high-sugar foods among adolescent pre-professional ballet dancers.
Following completion of the DVD-program, we hypothesized that participants would
increase their knowledge of basic nutrition principles and self-efficacy for adopting healthier
dietary habits as compared to pre-program and control group scores, and that this knowledge
would be sustained post-program at a 6-week follow-up assessment. Additionally, we

4
hypothesized that intervention participants would demonstrate improvements in eating behaviors,
specifically increased consumption of fruits, vegetables, and calcium-rich foods, and reduced
consumption of high-fat and high-sugar foods.
Together, these investigations determined the common physical and behavioral
characteristics and health conditions associated with professional ballet dancers and established
an educational program for adolescent dancers to potentially aid in preventing the development
of such health conditions. These investigations may not only benefit a large yet understudied
population of athletes, but also provide novel findings concerning the sport and art of dance.

5
References
1. Nattiv A, Loucks AB, Manore MM. The female athlete triad. Med Sci Sports Exerc. 2007;39(10):1867-1882.
2. Braisted JR, Mellin L, Gong EJ, et al. The adolescent ballet dancer. Nutritional practices
and characteristics associated with anorexia nervosa. J Adolesc Health Care. 1985;6(5):365-371.
3. Benson JE, Geiger CJ, Eiserman PA, et al. Relationship between nutrient intake, body
mass index, menstrual function, and ballet injury. J Am Diet Assoc. 1989;89(1):58-63. 4. Micheli LJ, Gillespie WJ, Walaszek A. Physiologic profiles of female professional
ballerinas. Clin Sports Med. 1984;3(1):199-209. 5. Abraham S. Eating and weight controlling behaviours of young ballet dancers.
Psychopathology. 1996;29(4):218-222. 6. Kaufman BA, Warren MP, Dominguez JE. Bone Density and amenorrhea in ballet
dancers are related to a decreased resting metabolic rate and lower leptin levels. J Cli
Endo Met. 2002;87(6):2777-2783. 7. Cassill K. The bane of the ballerina. Life threatening thinness. Science Digest.
1980;87:52-55. 8. Doyle-Lucas AF, Akers JD, Davy BM. Energetic Efficiency, Menstrual Irregularity, and
Bone Mineral Density in Elite Professional Female Ballet Dancers. Journal of Dance
Medicine and Science, In Press.

6
CHAPTER 2
Energetic Efficiency, Menstrual Irregularity, and Bone Mineral Density in Elite Professional Female Ballet Dancers
Abstract
Sports which emphasize low body weight for optimal performance, such as ballet, are
associated with an increased prevalence of the Female Athlete Triad (FT). Previous work in this
area has been limited; the majority of studies have been performed on adolescents training in
classical ballet and not professional adult dancers. Our purpose is to compare the physical and
behavioral characteristics of female elite professional ballet dancers to sedentary/recreationally
active non-dancing control participants, including characteristics of the FT and energetic
efficiency. Women aged 18-35 years were recruited for this study. Elite female ballet dancers
(n=15) and sedentary to recreationally active, non-dancing female controls (n=15) were pair-
matched via age (dancers: 24.3+ 1.3 vs controls: 23.7+ 0.9 yrs), body mass index (dancers: 18.9
+ 0.2 vs controls: 19.4 + 0.2 kg/m2), and fat-free mass (dancers: 44.3+ 0.8 vs controls 44.1+ 0.9
kg). Assessments included habitual dietary intake using 4-day food records, self-reported
physical activity, psychometric measures of eating behaviors, health and menstrual history, body
composition and bone density (Dual Energy X-ray Absorptiometry), and resting metabolic rate
(RMR) assessed by indirect calorimetry. Characteristics of the FT specifically menstrual
irregularities (6/15 dancers reported irregular or no menses; 1/15 control women reported
irregular menses) and low energy availability were more prevalent in dancers than pair-matched
control women. Despite having a similar fat-free mass (FFM), dancers had a significantly lower
absolute RMR than pair-matched control women (dancers: 1367 + 27; controls: 1454 + 34,
kcal/d; P<0.05) and significantly lower RMR relative to FFM (dancers: 30.9 + 0.6; controls: 33.1
+ 0.8 kcal/kg fat-free mass/d; P<0.05). Energy intake between dancers (1577 + 89 kcal/d) and

7
pair-matched controls (2075 + 163, kcal/d; P<0.01) also differed significantly. Six of the 15
dancers met the criteria of FT (including low bone mineral density, menstrual irregularities, and
eating pathology accompanied by low energy availability) and, therefore, represent a population
of individuals afflicted with this disorder. These findings provide insight as to the metabolic
impact of chronic energy restriction, and suggest that alterations in RMR (i.e., energetic
efficiency) may be an indicator of low energy availability; future larger-scale studies are
warranted to address this possibility. Elite female ballet dancers appear prone to characteristics
of the FT, such as low energy availability, menstrual irregularities, and decreased bone density.
Interventions aimed at increasing energy availability in this unique population of athletes are
needed to promote optimal health status.
Keywords: Female Athlete Triad; Energetic Efficiency; Resting Metabolic Rate; Ballet Dancers

8
Introduction
Sports which emphasize low body weight for optimal performance are often associated
with an increased prevalence of the Female Athlete Triad (FT) 1. Low energy availability with
or without disordered eating, menstrual irregularity/amenorrhea, and bone loss/osteoporosis are
the three interrelated conditions that comprise the FT 1. Because the focus of ballet is on the
beauty of the body in its movement and shape, many dancers exhibit a preoccupation with their
body image which increases risk for disordered eating 2. Ballet dancers consistently weigh 10-
12% below ideal body weight, and these low weight ranges are commonly achieved by low
energy intakes (EI) 3. It has been observed that student and professional ballet dancers,
specifically females, consume 70-80% or below of the recommended daily allowance (RDA) for
total energy 4-7. However, an energy availability (dietary intake minus exercise energy
expenditure) of 30 kcal/kg fat-free mass (FFM)/day or less is associated with the development of
FT 1. In addition, a low EI relative to predicted energy expenditure may increase energetic
efficiency in endurance trained female athletes 8 and possibly also ballet dancers.
Female athletes who participate in sports where much importance is placed on lean
figures eat less than would be expected for their total energy expenditure 9. This hypometabolic
state induced by poor nutrition and/or chronic energy deficiency may lead to irregular
menstruation and/or osteoporotic development in female professional athletes 3. This in turn
gives rise to athletes susceptible of developing the conditions comprising the FT.
Low energy availability (EA) appears to be the key component responsible for the
development of the remaining two conditions of the FT 1. Research suggests that during
chronically decreased EA, processes that require energy such as reproduction, thermoregulation,
growth, and cellular maintenance are suppressed 1. Amenorrhea, the absence/loss of menstrual

9
periods, often results 9. Potential contributors to disruptions in the normal endocrine process
include exercise volume, low body weight, inadequate EA, low EI/nutritional restrictions, and
psychological stresses 10, 11. Most recent data, however, claims EA as the leading cause of
exercise-induced amenorrhea 12, 13.
Relative to other women participating in various sports, ballet dancers in particular have
poor bone density status, possibly due to the low EI and body weights reported in this
population 14. This may occur through reduced resting metabolic rate (RMR) and leptin
concentrations, a hormone that plays an important role in appetite regulation and metabolism,
which could lead to low bone density in female ballet dancers 3. Ballet dancers would be
expected to have slightly higher metabolic rates than weight-matched non-dancers, due to a
higher fat-free mass (FFM) 15. FFM is a primary determinant of RMR, which is composed
primarily of muscle, but also of bone, organ, and body water weight 16, 17. However, previous
work suggests that the metabolic rates of dancers may be less than would be predicted, based
upon weight and lean body mass (LBM) 3.
There is limited research investigating the health of professional ballet dancers; prior
work has focused primarily upon adolescent dancers training in classical ballet. Because body
composition, bone density, hormonal balance, and other aspects of metabolism greatly fluctuate
during this period of puberty/maturation, the observed “traits” of adolescent dancers may not be
indicative of those found in elite professional, adult ballet dancers. The effect of continuous,
rigorous demands throughout childhood into adulthood may result in more severe consequences,
resulting in specific characteristics found only in the professional population which has been
understudied.

10
Previous work in this area has also been limited, in that control groups are often not
included. Without the inclusion of control subjects pair-matched by age and body composition,
it is difficult to determine if low RMRs of dancers result from restrictive eating patterns,
amenorrhea, or differences in LBM. In comparing physically active dancers to
sedentary/recreationally active non-dancers of similar body composition, the primary
characteristics that lead to increased energetic efficiency may be determined.
With regard to assessment of FT, a challenge for both researchers and practitioners is that
there are currently no objective indicators of EA, thus making it difficult to assess due to reliance
on self-reported measures. Energetic efficiency as determined by comparison of measured to
predicted RMR may, therefore, be a surrogate indicator of low EA. This may be relevant to other
populations as well, including female endurance athletes and those who chronically diet to
control their body weight.
The purpose of this investigation was to compare the RMR of professional female ballet
dancers to non-dancing, healthy control women who were pair-matched by age, body mass
index, and FFM. The objectives of this study were as follows: 1) to describe the physical and
behavioral characteristics of female professional ballet dancers, including characteristics of the
FT, 2) to determine if there are differences in RMR between this population and control women
pair-matched by age, body mass index, and FFM, and 3) to determine associations between FT
characteristics and energetic efficiency (observed versus predicted RMR based upon body
composition). We hypothesized that the dancers would report a low habitual energy intake and,
therefore, be subject to conditions comprising the FT, including low EA, suboptimal bone
density and menstrual irregularities. We also hypothesized that elite female dancers would have

11
lower than expected RMR based upon their FFM, and thus greater energetic efficiency as a result
of chronic energy (caloric) deficiency.
Materials and Methods
Participants
Women aged 18-35 years (n=39) were recruited for participation. Group 1 (“dancers”;
n=15) consisted of elite (> 27 hours/week of dancing) female ballet dancers recruited from two
national professional ballet companies. Group 2 (“controls”; n=24) consisted of non-dancing
females who were sedentary to recreationally active (<150 min moderate to high-intensity
physical activity/week); control participants were oversampled in order to ensure adequate
matching with dancers on pair-matched variables. Data from control group participants not
included in the pair-matched sample was not used in subsequent analyses (n=9). The control
participants were representative of the typical “thin” woman, therefore, possible menstrual
irregularities were not inclusion criteria. These participants were recruited from the local
university community.
All 15 dancers were successfully pair-matched to 15 non-dancers via age, body mass
index (BMI), LBM, and FFM as these factors are the largest predictors of RMR 16, 17. Age was
matched +/- five years; this range is within that utilized by the Institute of Medicine in their
dietary intake recommendation ranges 18. BMI was matched +/- one unit, indicating similar
weight status between matches. LBM and FFM were matched +/- two kg to account for Dual
Energy X-ray Absorptiometry (DXA) measurement error 19. Three of the dancers were < 20
years of age, therefore, Z-scores (measurement system for bone density of individuals > 20
years) for these participants were determined as if they were 20 years of age.

12
All laboratory testing was conducted when participants were in the early-mid follicular
phase of their menstrual cycle (days 1-10); oligomenorrheic and amenorrheic subjects were
studied when convenient, as hormonal fluctuations were less predictable in these participants.
Women taking hormonal contraception were included. Three of the 15 dancers reported using
Oral Contraceptive Pills (OCP), and seven of the pair-matched controls reported using OCPs at
the time of the study. Participants were not pregnant, smokers, or suffering from major chronic
disease (e.g., diabetes, chronic obstructive pulmonary disease, renal disease, thyroid disease, or
cancer). Written informed consent was obtained from each participant following explanation of
the purpose, risks, and benefits of the study. The study protocol was approved by the
Institutional Review Board of Virginia Polytechnic and State University (Virginia Tech).
Protocol
The purpose and requirements of this study were explained to the dancers initially in the
building of their workplace due to the distance between the study laboratory and the professional
company (~250 miles). At that time, written informed consent was obtained from dancers
interested in participating. A health history questionnaire (HHQ), menstrual history
questionnaire, instructions for completing a four-day habitual dietary intake record, three-factor
eating questionnaire (TFEQ) 20, and eating attitudes test (EAT-26) 21 were distributed at this
meeting to participants immediately following the return of their signed informed consent
document. The HHQ includes questions related to current and previous medical conditions,
medication usage, changes in body weight, diet, and physical activity history. Current physical
activity levels of intensity were self-reported by use of a 1-10 range scale (1- 3 low intensity, 4-6
moderate intensity, 7-10 high intensity); the minutes per week subjects engaged in low,
moderate, and high intensity physical activity were recorded. The menstrual history

13
questionnaire assesses menstrual irregularities, patterns, and family menstrual history. The TFEQ
elicits information regarding three dimensions of eating behavior: 1) dietary restraint, or the
conscious, cognitive control of food intake, 2) disinhibition or lack of control in eating, and 3)
perceived hunger--the degree to which individuals feel that their eating is driven by feelings of
hunger 20. Each of the three factors of the TFEQ has been shown to be reliable and valid 20. A
score of > 11 for each individual factor indicates abnormal eating behaviors. Lastly, participants
completed the EAT-26 which is a 26-item, objective, self-report measure of symptoms of
disordered eating. Scoring of this tool is based on a six-point scale with answers ranging from
“never” to “always”. A score of ≥ 20 on the EAT-26 distinguishes individuals with disordered
eating 21.
To determine habitual dietary intake, four-day dietary intake records were obtained from
all participants. Participants were instructed in methods to accurately record their food and
beverage intake. Measuring spoons, cups, and food models were used to determine portion sizes.
All records were reviewed for accuracy and completeness prior to analysis using the NDS-R
nutritional analysis software program (Version 2006, University of Minnesota, Minneapolis,
MN). The food record and questionnaires were completed and returned on the day of scheduled
laboratory testing.
Control women visited the laboratory twice; they signed the written informed consent and
completed the same questionnaires as the dancers during their first laboratory visit. Their
completed food records were returned upon their second visit/assessment of RMR. All
participants visited the laboratory for assessment of RMR using indirect calorimetry, and body
composition and bone density using DXA (GE Lunar Prodigy; GE Healthcare, Madison, WI).
During the laboratory sessions, a laboratory technician performed the indirect calorimetry,

14
weight and height measurements, and DXA on a maximum of two subjects per morning. All
subjects arrived at the laboratory upon waking, one at a time, in hourly intervals beginning at
6:30am, in a fasted state (10-12 hours). The dancers traveled to the laboratory location the
evening before their testing day, and were transported to the laboratory for testing the following
morning. Participants were instructed not to engage in strenuous exercise within 24 hours of the
test. For three of the dancers this was not feasible due to their performance schedule and
menstrual cycle phase, however strenuous exercise was avoided for 12 hours prior to indirect
calorimetry for these participants. Participants were instructed to refrain from ingestion of
medication, nicotine, and/or caffeine on the morning of the test.
Laboratory Assessments
Height was measured in meters without shoes using a wall-mounted stadiometer. Body
weight was measured to the nearest 0.1 kg using a digital scale (Scale Tronix; Wheaton, IL).
Body mass index was calculated as weight (kg)/height(m)2. Waist circumference was measured
across the umbilicus without clothing. A Gulick tape measure (Gulick, Country Technology,
Inc; Gays Mill, WI) was used to obtain two measurements to the nearest 1.0 cm. The total fat,
fat-free (bone, muscle, and organs), and lean (muscle) body mass of all participants was
measured using DXA. Bone density at the posterior-anterior spine and left femur was also
measured using DXA, according to guidelines established by the International Society for
Clinical Densitometry (ISCD) 22. An ISCD-Certified Densitometry Technologist performed all
scans. Z-scores, comparing individuals' bone mineral density (BMD) to age and sex-matched
controls, were determined for each respective regional bone density area assessed. RMR was
determined by indirect calorimetry using a ventilated hood system (ParvoMedics; Sandy, UT).
Measurements were made in the early morning hours after a 10-12-hour fast. Participants rested

15
quietly for 10 minutes prior to the 45-minute test with a clear plastic ventilated hood over their
head, during which time inspired and expired gases were analyzed. The predicted RMR of each
individual was estimated via three calculation methods: the Cunningham equation (500 +
22FFM) which considers FFM (kg), the Mifflin equation (5 + 10W + 6.25H - 5A), and the
Harris-Benedict (HB) equation (655.09 + 9.56W + 1.84H- 4.67A), which both consider weight
(W; kg), height (H; cm), and age (A; yr) 23-25. Because the Cunningham equation includes FFM,
it is considered a better prediction equation for athletes 26, 27. The Mifflin equation has been
identified to produce a more accurate representation of RMR in obese and non-obese individuals
than the commonly used HB equation 26, 28; inclusion of the HB equation in this analysis is
important however, as it has been found to accurately predict RMR in eumenorrheic professional
ballet dancers 29. EA was calculated as dietary energy intake minus exercise energy expenditure
normalized to FFM in units of kcal/kg FFM/day 1. Exercise energy expenditure was calculated
from the equation: METS x kcal/hr (from RMR) x hrs exercising 30. The estimated rate of
energy expenditure for ballet used in calculations was 4.8 METS 31.
Statistical Analysis
Data analyses included descriptive characteristics, paired t-tests for group comparisons,
and simple correlation analyses to test for relationships between variables of interest, using SPSS
V.12.0. One-way Anova and post hoc (Tukey’s) tests were used when significant differences
were detected and to determine group differences according to menstrual status. Power
calculations on two of the key outcome variables, BMD and RMR, using preliminary data
(expected group differences, standard deviations, α =0.05) indicated that statistical power was
99.9% for BMD and 89.4% for RMR with our proposed sample size of 15 per group.

16
Results
A total of 24 control women and 15 dancers completed the study protocol. All dancers
were then pair-matched with 15 control women by age (dancers: 24.3+ 1.3 v. controls: 23.7 + 0.9
yrs), FFM (44.3+ 0.8 v. 44.1 + 0.9 kg), LBM (41.8 + 0.8 v. 41.5 + 0.8 kg), and BMI (18.9+ 0.2
v. 19.3+ 0.2 kg/m2). Body weight and body fat percentage were significantly lower in dancers
compared with control women (Table 1). As expected, physical activity (PA) levels were also
significantly lower in control women than dancers (Table 1), with dancers reporting habitual
moderate + high intensity PA of approximately 36 hours per week (> 5 hours/day). Controls
reported participating in low to high intensity PA including activities such as walking, running,
weight lifting, and biking.
As hypothesized, reported energy intake of dancers was significantly lower than control
women, as was EA (Tables 2 and 3). However, there were no group differences in self-reported
macro- and micronutrient intakes of dancers compared with control women (Table 2). Dancers
reported higher levels of dietary restraint and disinhibition than control women, and a higher
EAT-26 score, however these group differences were not significant (Table 2).
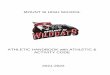
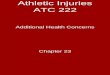
Despite having a similar FFM, dancers had a significantly lower absolute RMR than
matched controls (Figure 1) and lower RMR relative to FFM (Figure 2). The association
between RMR relative to FFM and EA, however, did not quite reach statistical significance
(r=0.34, P=0.067). No significant differences were found in total (whole body) BMD or total Z-
scores, although mean values were slightly lower in dancers. Regional Z-scores of the posterior-
anterior spine and left femur were higher compared to control women, although this difference
did not reach statistical significance.

17
Amenorrhea and irregular menses were more prevalent in dancers than matched controls.
Dancers experienced delayed menarche, on average beginning menses at the age of 15 years as
compared to control women beginning at the age of 13 years (Table 3). While only one control
woman reported irregular menses, six dancers reported either irregular or no menstrual cycles
(Table 4). As listed in Table 4, body fat, absolute RMR, RMR relative to FFM, total Z-score,
and EA decreased progressively from regularly menstruating control women, regularly
menstruating dancers, to irregularly menstruating and amenorrheic (“dysfunctional”) dancers.
“Dysfunctional” dancers were observed to have the lowest EA, energy intake, body fat
percentage, and total Z-score, and more abnormal eating behaviors (i.e., TFEQ dietary restraint,
EAT-26 score). This group of dancers (n=6) exhibited symptoms of the three conditions
comprising the Female Athlete Triad.
Observed versus predicted RMR among dancers varied significantly (Figure 3). Average
observed RMR (measured via indirect calorimetry) among all dancers was 1367 kcal/day, while
predicted RMR by the Cunningham equation was significantly higher at 1475 kcal/day (P<0.01).
RMR predicted from the Mifflin equation was significantly lower than both the Cunningham
equation and observed values (Figure 3). The HB equation most accurately predicted RMR in
dancers. When comparing RMR in eumenorrheic versus “dysfunctional” dancers, the HB
equation was most accurate for predicting RMR in the dysfunctional group with differences
(predicted minus observed RMR) at +4 kcals in dysfunctional dancers (P=0.94) and – 43 kcals in
eumenorrheic dancers (P=0.07). In contrast, observed versus predicted RMR among control
women was most similar with the Cunningham equation (Figure 4).

18
Discussion
This is the first investigation to pair-match elite professional female dancers to
sedentary/recreationally active control women in order to compare energetic efficiency,
menstrual irregularities, BMD and RMR, while accounting for age, FFM, and BMI. As
hypothesized, characteristics of the FT were more prevalent among dancers, specifically
menstrual irregularities and low EA. In general, dancers began menses at least one year later than
controls and were more likely to experience irregular or lack of menses. Bone density and Z-
scores among dancers and controls were not significantly different, however, when comparing
menstrual status to bone density, total Z-score and BMD continuously decreased from
eumenorrheic controls, eumenorrheic dancers, to “dysfunctional” (both irregularly menstruating
and amenorrheic) dancers. The mean posterior-anterior spine Z-score for “dysfunctional”
dancers was indicative of low bone density. Athletes participating in weight-bearing sports often
have 5-15% higher total BMD than nonathletes 1, 32, 33. Therefore, our findings suggest that
although not significantly lower than control women, the dancers’ BMD was not at a level of
optimal bone health.
Interestingly, energetic efficiency increased (and EA decreased) with dysfunctional
menstrual status. The ratio of kilocalories of food intake (i.e., energy intake) per day to kilogram
FFM decreased steadily from eumenorrheic controls to dysfunctionally menstruating dancers.
These results are similar to those reported by Drinkwater et al. and Marcus et al., who also
observed increased energetic efficiency in amenorrheic female runners 8, 34, 35. Our findings
indicate that the irregularly menstruating and amenorrheic dancers have the lowest energy
requirement to sustain a kilogram of body weight and the overall lowest calorie requirement
despite having the highest FFM.

19
Abnormal eating behaviors, indicated by a score of > 11 on the TFEQ, were prevalent
among the “dysfunctional” menstrual status dancers. This group scored a 12.6, indicating a high
level of dietary restraint and conscious cognitive control of food intake. The eumenorrheic
dancers and controls scored 6.1 and 5.8, respectively. The “dysfunctional” menstrual status
dancers also scored significantly higher on the EAT-26 than the other two groups. This group of
dancers meets the criteria of FT (including low BMD, menstrual irregularities, and eating
pathology accompanied by low EA) and is, therefore, a population representative of individuals
at high risk for this disorder.
Another main finding of this investigation is the significantly lower RMR as measured by
indirect calorimetry (both absolute and RMR relative to FFM) in dancers as compared to control
women, which suggests an increased energetic efficiency and decreased energy requirement in
these athletes. Energy intake was observed to be lower in dancers than control women,
providing evidence for low energy intake relative to predicted energy expenditure in the dancers.
Because the dancers were matched by FFM and age, our findings indicate that the low EA of the
dancers may be a primary contributor to their lower than expected RMR. Our results are similar
to those of Kaufman et al. who also observed a depressed absolute and RMR relative to FFM in
dancers as compared to controls and related this to energy (caloric) deficiency 3.
Unlike our findings and those of many other studies supporting depressed RMR in female
athletes, Horton et al. observed no significant differences in RMR or energy efficiency among
endurance-trained female cyclists versus untrained controls 36. This study, however, did not
account for a population of undereating female athletes. The subjects of this study were fed a
diet of fixed composition (30% fat, 15% protein, and 55% carbohydrates as a proportion of the
total energy they habitually consumed). Although no subjects gained weight during this five-day

20
diet period, the composition of their diet was likely altered and the average total energy
consumed per day was 2,300 kcal 36. Therefore, it is uncertain if chronic undereating was
characteristic of this study population. The dancers in our study exhibited energy restriction and,
therefore, may explain the differences between our results and those of Horton et al 36.
Horton et al. also suggested that previous reports of increased energetic efficiency in
female athletes may be due to underreporting on self-reported dietary intake records, undereating
by subjects during the measurement of energy intake, and/or over-reporting of exercise 36. The
calculation of EA is subject to inaccuracies due to a similar reliance on self-reported measures
and estimations. EA is now thought to be the central marker for development of the two
remaining conditions of the FT, therefore, the ability to measure it in female athletes is
important. With dependence on self-reported measures of energy intake and estimations of
exercise energy expenditure, this proves difficult, specifically for dancers whose exercise energy
expenditure varies greatly depending on their rehearsal schedule, their ranking in the ballet
company, and roles that they are required to perform. Therefore, a major challenge is the
assessment of EA in clinical practice.
A possible surrogate marker for EA is energetic efficiency (observed RMR versus
predicted RMR based upon FFM). If energetic efficiency is increased, or if the observed RMR is
less than the predicted RMR, this may indicate a low EA. Energetic efficiency relative to FFM
in dancers was 30.9 (+ 0.6) kcal/kgFFM which appears to be a reasonably accurate value for EA.
Calculated EA for the dancers (reported energy intake minus exercise energy expenditure) was
3.8 kcal/kgFFM, a potentially inaccurate value. By comparing observed RMR versus predicted
RMR based upon FFM, it may be possible to derive a value representative of EA that is not
dependent on self-reported measures. Although not statistically significant, our findings suggest

21
a trend for an association between RMR relative to FFM and EA. A depressed relative RMR
may therefore, be indicative of low EA and increased energetic efficiency.
In comparing observed to predicted RMR using the Cunningham, Mifflin, and HB
equations, we found, similar to Glace et al., that RMR in dancers is most accurately predicted by
the HB equation 29. However, in contrast to findings by Glace et al. who observed the HB
equation to better predict RMR in eumenorrheic than amenorrheic dancers 29, we found that the
HB only slightly overestimated amenorrheic dancers RMR (+4 kcal/day) yet notably
underestimated eumenorrheic dancers RMR (-43 kcal/day). Despite the variance in outcomes,
the HB equation appears to be the most accurate prediction equation in this athletic population.
We acknowledge several limitations of this investigation. First, the use of self-reported
physical activity habits may serve as a source of inaccuracy due to possible overestimation. In
future studies, objective measures such as accelerometry or doubly labeled water could be used
to assess physical activity energy expenditure. Second, self-reported dietary intake is also
subject to inaccuracies due to over- or underestimation. Specific to populations of lean female
athletes including dancers, a strong bias toward under-reporting energy intake has been
observed 29, 37, 38. To avoid this, prior to recording dietary intake, our participants were
individually instructed on how to complete an accurate food record, and were provided with
detailed instructions, food portion measurement aids, and were instructed not to alter their eating
habits on recorded days. Once completed, records were reviewed by the investigators for
completeness. These procedures should help to improve the accuracy of self-reported dietary
intake measures, but nevertheless we acknowledge these limitations. The extremely low
reported intakes of the dancers may be indicative of underreporting, resulting in lowered
corresponding EA values. Third, our sample size was limited which may have precluded the

22
detection of group differences in some outcome variables. However, we had adequate statistical
power to detect significant differences in several important physiological outcomes. Lastly, we
did not restrict eligibility to women not using OCP or to dancers with menstrual dysfunction.
Our intent was to recruit from the general population of both elite ballet dancers and
recreationally active, thin women. A more homogenous sample would have decreased
variability in some outcome variables, yet would not be a true representation of the general
population of elite ballet dancers or thin, recreationally active women. We recognize that not
controlling OCP may have affected outcome variables such as menstrual status, bone density,
and possibly RMR. We also recognize that self-reported menstrual histories may be a source if
inaccuracy which could affect findings related to menstrual status.
To overcome these limitations, future studies including larger sample sizes should assess
actual energy expended through physical activity and control for dietary intake of dancers to
avoid the reliance on self-reported measures, and include the direct measurement of relevant
hormones such as estrogen or leptin to determine their influence on conditions associated with
the FT. Future larger-scale studies are also warranted to better address the possibility that low
RMR may be a surrogate marker for low EA in female athletes.
Conclusion
There are no pharmacological agents that reverse the negative consequences of the
Female Athlete Triad; no treatment fully restores bone loss or corrects metabolic abnormalities
that impair the health and performance of amenorrheic, energy deficient athletes 1. By analyzing
the RMR, body composition, bone density, and energy intake of professional dancers as
compared to non-dancing control women, our findings provide insight to the potential metabolic
impact of chronic energy restriction as well as suggest possible alternative methods for

23
measuring energy availability in athletes. Proper eating behaviors of dancers and all athletes
begin during adolescence. Young dancers are rarely taught nutrition along with their classical
training, yet the ideal, thin, body type is continuously reinforced. Proper nutrition and eating
habits must be encouraged and implemented into the daily training of adolescent ballet dancers
to prevent the future development of amenorrhea, osteoporosis, and low energy availability.
Acknowledgements
We would like to thank the participants for their time and commitment to the study.

24
References
1. Nattiv A, Loucks AB, Manore MM. The female athlete triad. Med Sci Sports Exerc. 2007;39(10):1867-1882.
2. Abraham S. Eating and weight controlling behaviours of young ballet dancers.
Psychopathology. 1996;29(4):218-222. 3. Kaufman BA, Warren MP, Dominguez JE. Bone Density and amenorrhea in ballet
dancers are related to a decreased resting metabolic rate and lower leptin levels. J Cli
Endo Met. 2002;87(6):2777-2783. 4. Benson J, Gillien DM, Bourdet K, et al. Inadequate Nutrition and Chronic Calorie
Restriction in Adolescent Ballerinas. Phys Sportsmed. 1985;13(10):79-90. 5. Bonbright JM. The Nutritional Status of Female Ballet Dancers 15-18 Years of Age.
Dance Research Journal. 1989;21(2):9-14. 6. Dahlstrom M, Jansson E, Nordevang E, et al. Discrepancy between estimated energy
intake and requirement in female dancers. Clin Physiol. 1990;10(1):11-25. 7. Calabrese LH, Kirkendall DT, Floyd M. Menstrual abnormalities, nutritional patterns and
body composition in female classical ballet dancers. Phys Sportsmed. 1983;11:86-98. 8. Brownell KD, Steen SN, Wilmore JH. Weight regulation practices in athletes: analysis of
metabolic and health effects. Med Sci Sports Exerc. 1987;19(6):546-556. 9. Female Athlete Triad Coalition. The Triad. Available at:
http://www.femaleathletetriad.org/faq.html. Accessed August 17, 2007. 10. Warren MP, Perlroth NE. The effects of intense exercise on the female reproductive
system. J Endocrinol. 2001;170(1):3-11. 11. Loucks AB. Energy availability, not body fatness, regulates reproductive function in
women. Exerc Sport Sci Rev. 2003;31(3):144-148. 12. Loucks AB, Verdun M, Heath EM. Low energy availability, not stress of exercise, alters
LH pulsatility in exercising women. J Appl Physiol. 1998;84(1):37-46. 13. Torstveit MK, Sundgot-Borgen J. Participation in leanness sports but not training volume
is associated with menstrual dysfunction: a national survey of 1276 elite athletes and controls. Br J Sports Med. 2005;39(3):141-147.
14. Quintas ME, Ortega RM, Garrido G. Influence of dietetic and anthropometric factors and
of the type of sport practiced on bone density in different groups of women. Eur J Cli
Nutr. 2003;57(1):S58-S62.

25
15. Ravussin E, Lillioja S, Anderson TE, et al. Determinants of 24-hour energy expenditure
in man. Methods and results using a respiratory chamber. J Clin Invest. 1986;78(6):1568-1578
16. Gilliat-Wimberly M, Manore MM, Woolf K, et al. Effects of habitual physical activity on
the resting metabolic rates and body compositions of women aged 35 to 50 years. J Am
Diet Assoc. 2001;101(10):1181-1188. 17. Webb P. Energy expenditure and fat-free mass in men and women. Am J Clin Nutr.
1981;34(9):1816-1826. 18. Institute of Medicine; Dietary Reference Intakes. Washington, D.C.: National Academy
of Sciences 2006. 19. Haarbo J, Gotfredsen A, Hassager C, et al. Validation of body composition by dual
energy X-ray absorptiometry (DEXA). Clin Physiol. 1991;11(4):331-341. 20. Stunkard AJ, Messick S. The three-factor eating questionnaire to measure dietary
restraint. J Psychos Resear. 1985;29(71-83). 21. Garner DM, Olmsted MP, Bohr Y, et al. The eating attitudes test: psychometric features
and clinical correlates. Psych Med. 1982;12:871-979. 22. ISCD Official Positions. International Society for Clinical Densitometry. West Hartford,
CT 2007. Available at: www.ISCD.org. 23. Harris JA, Benedict FG. A Biometric Study of Basal Metabolism in Man. Washington,
DC: Carnegie Institute of Washington 1919. 24. Cunningham JJ. A reanalysis of the factors influencing basal metabolic rate in normal
adults. Am J Clin Nutr. 1980;33(11):2372-2374. 25. Mifflin MD, St Jeor ST, Hill LA, et al. A new predictive equation for resting energy
expenditure in healthy individuals. Am J Clin Nutr. 1990;51(2):241-247. 26. De Lorenzo A, Tagliabue A, Andreoli A, et al. Measured and predicted resting metabolic
rate in Italian males and females, aged 18-59 y. Eur J Clin Nutr. 2001;55(3):208-214. 27. Thompson J, Manore MM. Predicted and measured resting metabolic rate of male and
female endurance athletes. J Am Diet Assoc. 1996;96(1):30-34. 28. Frankenfield DC, Rowe WA, Smith JS, et al. Validation of several established equations
for resting metabolic rate in obese and nonobese people. J Am Diet Assoc. 2003;103:1152-1159.

26
29. Glace B, Kremenic I, Liederbach M. Energy Conservation in Amenorrheic Ballet Dancers. Med Probl Perform Art. 2006(21):97-104.
30. Ainsworth BE, Haskell WL, Leon AS, et al. Compendium of physical activities:
classification of energy costs of human physical activities. Med Sci Sports Exerc. 1993;25(1):71-80.
31. Ainsworth BE, Whitt MC, Irwin ML. Estimated rates of energy expenditure. Med Sci
Sports Exerc. 2000;32:S498-S516. 32. Fehling PC, Alekel L, Clasey J, et al. A comparison of bone mineral densities among
female athletes in impact loading and active loading sports. Bone. 1995;17(3):205-210. 33. Risser WL, Lee EJ, LeBlanc A, et al. Bone density in eumenorrheic female college
athletes. Med Sci Sports Exerc. 1990;22(5):570-574. 34. Marcus R, Cann C, Madvig P, et al. Menstrual function and bone mass in elite women
distance runners. Endocrine and metabolic features. Ann Intern Med. 1985;102(2):158-163.
35. Drinkwater BL, Nilson K, Chesnut CH, 3rd, et al. Bone mineral content of amenorrheic
and eumenorrheic athletes. N Engl J Med. 1984;311(5):277-281. 36. Horton TJ, Drougas HJ, Sharp TA. Energy balance in endurance-trained female cyclists
and untrained controls. J Appl Physiol. 1994;76(5):1937-1945. 37. Beidleman BA, Puhl JL, De Souza MJ. Energy balance in female distance runners. Am J
Clin Nutr. 1995;61(2):303-311. 38. Fogelholm GM, Kukkonen-Harjula TK, Taipale SA, et al. Resting metabolic rate and
energy intake in female gymnasts, figure-skaters and soccer players. Int J Sports Med. 1995;16(8):551-556.

27
Table 1. Demographic Characteristics of Pair-Matched Female Elite Dancers and Lean Control
Women
Dancers (n=15) Controls (n=15)
Mean (+ SEM) Mean (+ SEM)
Age, yrs 24.3(+ 1.3) 23.7 (+ 0.9)
Weight, kg 51.9 (+ 0.7) 56.5 (+ 0.9)*
Height, cm 166 (+ 1.0) 170 (+ 1.0)*
BMI, kg/m2 18.9 (+ 0.2) 19.4 (+ 0.2)
Fat-free mass, kg 44.3 (+ 0.8) 44.1 (+ 0.9)
Lean body mass, kg 41.8 (+ 0.8) 41.5 (+ 0.8)
Body fat, % 15.5 (+ 1.3) 22.6 (+ 1.0)*
Physical activity, low, min/wk 1 (+ 1) 33 (+ 17)
Physical activity, mod, min/wk 1118 (+ 32) 109 (+ 35)*
Physical activity, high, min/wk 1060 (+ 42) 165 (+ 88)*
*Significantly different from dancers (P<0.01).

28
Table 2. Eating Behaviors in Pair-Matched Female Elite Dancers and Lean Control Women Dancers (n=15) Controls (n=15)
Mean (+ SEM) Mean (+ SEM)
Energy Intake, kcal/d 1557 (+ 89) 2075 (+ 163)*
Macronutrients, % of total energy:
Carbohydrates
Protein
Fat
Alcohol
56 (+ 3)
17 (+ 1)
26 (+ 2)
4 (+ 1)
54 (+ 3)
16 (+ 1)
30 (+ 2)
3 (+ 1)
Micronutrients:
Calcium (mg)
Vitamin D (mcg)
Iron (mg)
851 (+ 80)
5 (+ 1)
13 (+ 1)
997 (+ 101)
4 (+ 1)
16 (+ 1)
Three Factor Eating Questionnaire (TFEQ), score:
Dietary Restraint
Disinhibition
Perceived Hunger
8.7 (+ 1.6)
5.8 (+ 1.1)
5.4 (+ 0.7)
5.7 (+ 1.1)
3.5 (+ 0.6)
6.5 (+ 0.8)
Eating Attitudes Test-26, score 7.9 (+ 2.0) 4.5 (+ 1.7)
*Significantly different from dancers (P<0.01).

29
Table 3. Female Athlete Triad Characteristics in Pair-Matched Elite Female Dancers and Lean
Control Women1
Dancers (n=15) Controls (n=15)
Mean (+ SEM) Mean (+ SEM)
RMR 1367 (+ 27) 1454 (+ 34)*
RQ 0.87 (+ 0.02) 0.85 (+ 0.01)
EA, kcal/kg FFM/d 3.75 (+ 2.2) 41.1 (+ 4.6)**
Onset of Menses, yr 14.9 (+ 0.4) 13.4 (+ 0.3)*
Menstrual Status, n
Normal
Irregular
Amenorrheic
9
3
3
14
1
0
Total Z-score 0.99 (+ 0.2) 1.20 (+ 0.3)
Total BMD, g/cm2 1.16 (+ 0.01) 1.19 (+ 0.02)
Left Femur Z-score 1.00 (+ 0.2) 0.64( + 0.3)
Posterior-Anterior Spine Z-score 0.23 (+ 0.2) 0.07 (+ 0.2)
*Significantly different from dancers (P<0.05).
**Significantly different from dancers (P<0.01).
1Abbreviations Used: RMR, Resting Metabolic Rate; RQ, Respiratory Quotient; EA, Energy
Availability; FFM, Fat Free Mass; BMD, Bone Mineral Density.

30
Table 4. Differences in Female Athlete Triad Characteristics and Energetic Efficiency
According to Menstrual Status among Pair-Matched Elite Female Dancers and Lean Control
Women1
Control, Dancer, Dancer, Eumenorrheic Eumenorrheic “Dysfunctional”
2 (n=14) (n=9) (n=6) Weight, kg 56.1a 51.9b 52.0b
Body fat, % 22.4a 17.4ab 12.5b
FFM, kg 44.0 43.4 45.6
RMR, kcal/d 1468 1376 1353
Energetic Efficiency, RMR kcal/kgFFM/d 33.5a 31.7ab 29.7b
EA, kcal/kgFFM/d 40.9a 5.8b 0.6b
Energy Intake, kcal/d 2073a 1685ab 1415b
BMD, g/cm2 1.19 1.17 1.14
Total Z-score 1.18 1.17 0.73
Posterior-Anterior Spine Z-score 0.05 0.56 -0.25
TFEQ, score:
Dietary Restraint
Disinhibition
Perceived Hunger
5.8a
3.6
6.7
6.1a
4.9
4.6
12.7b
7.2
6.7
Eating Attitudes Test-26, score 4.8a 4.1a 13.5b
1 Abbreviations Used: FFM, Fat Free Mass; RMR, Resting Metabolic Rate; EA, Energy
Availability; BMD, Bone Mineral Density; TFEQ, Three Factor Eating Questionnaire.
2 “Dysfunctional” group includes irregular menses and amenorrheic dancers.
a,b,cDifferent letters indicate significant mean differences after Tukey post hoc test.

31
Figure Legends
Figure 1. Resting Metabolic Rate (kcal/day) in Pair-Matched Elite Female Dancers and Lean
Control Women.
Figure 2. Energetic Efficiency: Resting Metabolic Rate (kcal/kg FFM/day) in Pair-Matched
Elite Female Dancers and Lean Control Women.
Figure 3. Observed versus Predicted Resting Metabolic Rate in Elite Female Ballet Dancers.
Figure 4. Observed versus Predicted Resting Metabolic Rate in Lean Control Women.

32
Figure 1. Resting Metabolic Rate (kcal/day) in Pair-Matched Elite Female Dancers and Lean
Control Women
*Significantly different from dancers (P<0.05).
*

33
Figure 2. Energetic Efficiency: Resting Metabolic Rate (kcal/kg FFM/day) in Pair-Matched
Elite Female Dancers and Lean Control Women
*Significantly different from dancers (P<0.05).
*

34
Figure 3. Observed versus Predicted Resting Metabolic Rate in Elite Female Ballet Dancers1
*Significantly different from observed RMR (P<0.01). 1Abbreviations Used: RMR, Resting Metabolic Rate.
*
*

35
Figure 4. Observed versus Predicted Resting Metabolic Rate in Lean Control Women1
*Significantly different from observed RMR (P<0.01). 1Abbreviations Used: RMR, Resting Metabolic Rate.
*

36
CHAPTER 3
Dancers’ Health Services Survey: Current Practices among Professional Ballet Companies
Introduction
The study “Energetic Efficiency, Menstrual Irregularity, and Bone Mineral Density in
Elite Professional Female Ballet Dancers,” investigated the physical and behavioral
characteristics of female professional ballet dancers and their association to the Female Athlete
Triad (FT) 1. The FT decreases optimal performance and poses significant health risks to female
athletes 2. Due to the emphasis placed on leanness, ballet dancers are often thought to exhibit
characteristics of the interrelated conditions comprising the FT. Our findings suggests that
conditions of the FT are more prevalent in dancers than the pair-matched non-dancing controls 1.
Recognition and treatment of the clinical conditions in all effected female ballet dancers should
be a priority.
Young dancers are rarely taught nutrition along with their classical training, yet the ideal,
thin, body type is continuously reinforced. Proper nutrition and eating habits must be
implemented into the training of adolescent ballet dancers to prevent the future development of
amenorrhea, osteoporosis, and low energy availability.
The purpose of this dancers’ health services survey, “Current Practices Among
Professional Ballet Companies”, is to obtain knowledge of the current nutritional practices of
professional ballet companies. This information will be used to guide the development of a
nutrition education program to be implemented into the academies of professional companies
aimed at teaching adolescent ballet dancers proper nutrition to optimize health and performance.
The effectivness of this educational program will be assessed pre, post, and 6-weeks following

37
program delivery through questionnaires evaluating knowledge gained and behavior changes. If
effective, this program may be reproduced and disseminated on a national basis.
Materials and Methods
This cross-sectional study asks survey respondents to complete one short online survey
(taking 5-10 minutes to answer). Professional ballet companies in the United States, defined as
those that provide the sole source of income and benefits to their dancers, were identified via the
internet; 58 companies met this criteria. Contact information of the company artistic, executive,
and school directors was collected from their website, and each was contacted individually by e-
mail. Because the company artistic, executive, and school directors make decisions regarding
implementation of educational programs and are, therefore, the most appropriate sources of
accurate information, they comprised the population of this study. Each individual was sent an
e-mail which described the purpose of the study and included a link to the survey (See Appendix
F: Survey Tool); the recipients of the e-mail were asked to complete the online survey
(administered using survey.vt.edu). A written paragraph describing the purpose of the study was
also provided at the beginning of the survey (see Table 5 for survey questions and results). After
each survey was completed, the investigator received an automatic e-mail notification of survey
completion. For recipients who had trouble accessing the survey online (n=3), a hard copy with
a stamped return envelope was sent via postal mail; all hard survey copies were successfully
completed.
To increase response rate from the companies, the survey was sent out a total of four
times over a five-month period. Once a company responded, they would no longer receive

38
additional e-mails. Participant responses remained anonymous and will be contacted for
additional follow-up as necessary only if they provided consent and contact information.
Results
With the knowledge gained from the survey responses, we were be able to determine the
current availability and type of nutritional education offered to professional and adolescent ballet
dancers. This survey concluded with a 50% response rate; 29 out of 58 companies replied.
Findings suggest that only 12 professional companies offer some type of nutrition education to
their professional dancers. Of the companies that do offer nutrition education to their
professional dancers, most (83%) offer only individual counseling on an as-needed basis.
Nutrition seminars are offered to dancers by 17% of the responding companies.
Nutrition education for adolescent dancers attending the professional company
academies during the school year is provided by 19 of the 28 companies. Students between 12
and18 years old are within the age range most commonly receiving the nutrition education. Of
this nutrition education offered to the students, 42% of companies offer seminars one to two
times per year while another 42% of companies offer both seminars one time per year and
individual counseling on as as-needed basis.
Many professional companies across the nation offer competitive pre-professional
summer intensive programs. These programs often last three to six weeks and only selected
dancers (auditions for these programs are held in the fall) are invited to attend. The programs are
often held in the building of the professional ballet company they represent and the selected
students train with the professional dancers and other respected artists such as choreographers

39
and musicians. These young dancers are often housed in dormitories, eat in cafeterias, and
dance six or more hours per day. A summer intensive program is offered by 27 of the
responding companies. Of these companies, 23 offer nutrition education programs as a part of
the curriculum. Eighty-two percent of these 23 companies offer a seminar-type program to the
dancers most commonly consisting of one lecture for one hour. Eight companies offer more than
one seminar for one hour during the summer intensive weeks. The quality and content of the
nutritional education offered, however, remains unclear. Five of these companies state that a
nutritionist offers the seminars, yet the education and training of these individuals is unknown.
Two companies specifically indicated a former dancer and instructor as the sole provider of their
nutrition seminars. Also, some companies include nutrition only as a small component of
lectures on topics such as physical therapy and stress management. Only three of the companies
indicated that the speaker was a registered dietitian or physician.
The primary reason for companies to not offer nutrition education during their summer
intensive program is due to lack of time within the summer schedule and/or financial reasons.
When asked if these companies would be interested in offering a nutrition workshop
emphasizing eating for optimal health and performance during their summer intensive program,
10 out of 12 companies that answered this question responded positively. These companies
indicated that one or more seminars of at least one hour in duration would be of optimal length
for such a program.
Conclusion
We did not receive a response from 29 companies, and it is possible that many of these
do not offer nutrition education to their dancers. Although the need for nutrition education in

40
conjunction with dancers’ training is slowly becoming recognized among professional
companies, the quality and content of the nutrition seminars offered should be addressed to
assure an effective learning experience which is specifically targeted toward the needs of this
unique population. Finally, programs should be developed which can overcome barriers stated
by companies not offering educational programs (e.g., time, personnel, cost).

41
References
1. Doyle-Lucas AF, Akers JD, Davy BM. Energetic Efficiency, Menstrual Irregularity, and Bone Mineral Density in Elite Professional Female Ballet Dancers. Journal of Dance
Medicine and Science, In Press. 2. Nattiv A, Loucks AB, Manore MM. The female athlete triad. Med Sci Sports Exerc.
2007;39(10):1867-1882.

42
Table 5. Dancers’ Health Services Survey: Questions and Responses
Question Answer Percent
(%) 1. Do you currently have
some type of nutrition
education program for
your professional dancers
(for example, programs
which address eating for
good health and
performance)?
If yes, what type of
program: workshops,
seminars, individual
counseling with a
nutritionist, other:
(describe)
Yes 12 No 15 No answer 2 Individual counseling on need basis 10 Pre-season evaluation 1 Both 1 Seminar and quiz 2
41 52 7
83 8 8
17
2. Do you currently have
some type of nutrition
education program for
your students attending
the academy during the
school year?
If yes, what are the ages
of these dancers receiving
education in nutrition?
If yes, what type of
program: workshops,
seminars, individual
counseling with a
nutritionist, other:
Yes 19 No 10 Age 9-18 4 Age 12-18 9 Age 12-14 1 Age 15-18 4 Age 16+ 1 Seminar 1-2 times per year 8 Individual counseling on need basis 2 Both 8 “How to cook” demonstration 1
66 34
42 11 42 5
3. Do you offer a summer
intensive program?
If yes, do you offer
nutrition education
programs as a part of the
curriculum?
If yes, what type of
program: workshops,
seminars, individual
Yes 27 No 1 No answer 1 Yes 23 No 5 No answer 1 Seminar 18 Individual counseling on need basis 4
93 3 3
79 17 3
82 18

43
counseling, other.
And, what is the duration
of the nutrition program?
(number of minutes,
hours, etc)
If a nutrition program is
not offered, what is the
primary reason for this:
1 hr/wk for 6 wk 4 2-3 seminars for 1 hr 4 1 seminar for 1 hr 7 1 seminar for 1.5 hr 5 Financial 2 Lack of person who could provide program 1 Lack of time within summer program 3 In progress 2
7 4
11 7
4. If you do not currently
provide a nutrition
program, would you be
interested in offering a
nutrition workshop to
your dancers during the
summer program that
would emphasize eating
well for optimal health
and performance?
What do you believe
would be the optimal
length of such a program,
if you were to offer one?
(minutes, hours, etc)
Yes 10 No 2 No answer 17 < 1 hr 1 > 1 hr 5 > 1 hr with lab 1
34 7
59
5. Would you permit us to
contact you for your
feedback on this topic in
the future?
Yes 23 No 3 No answer 3

44
CHAPTER 4
Interests of the Target Audience: Young Dancers’ Nutrition Survey
Purpose
The purpose of this survey was to obtain information on the interests regarding nutrition
education of the population (pre-professional ballet dancers) that will be targeted in the planned
nutrition education program, “Nutrition for Optimal Performance”. This survey briefly assessed
dancers’ basic knowledge and beliefs pertaining to nutrition and its influence on their dancing,
performance, and health.
Materials and Methods
Pre-professional ballet dancers (n=39), both male and female, participating in a pre-
professional summer dance program, were surveyed to assess their interests in nutrition
education, basic nutritional knowledge, and health beliefs. Group 1 (n= 21) consisted of dancers
aged 9-13 years and dancers comprising Group 2 (n=18) were between 14-17 years old. The
survey questions are listed in Table 6.
Results
Responses to the survey varied, however common themes could be identified. In
answering question one, 12 students of Group 1 wanted to learn how to “stay healthy and
strong”, “what bad foods do to you”, and what foods to eat to improve performance. A common
phrase from this group was, “what foods are good and what foods are bad?”. Group 2 was more
interested (72%) in learning how various foods effect the body, what foods are best for
performance, and what diets dancers should follow for weight loss. Half of the dancers in Group
2 wanted to learn how to lose weight, keep weight off, and build leaner muscles.

45
When asked what would make a nutrition lecture interesting, both Group 1 and 2
mentioned interactive activities, including games of identifying healthy versus unhealthy foods,
calorie guessing games, and worksheets to apply the learned information. Both groups were also
interested in having the lectures relate specifically to dancers, discussing nutrients found in
various foods and how they benefit the body to aid in performance.
Many dancers answered question three, what do you think happens if you don’t eat
enough calories and how do you think it effects your dancing, similarly. Twenty-one of the 39
dancers mentioned they would “get weak, dizzy, and lightheaded”. They also believed they
would “slow down” and not be able to dance to their full potential. Seventy-two percent of
Group 2 also stated they would become weak and lose muscle mass. Half of these dancers
mentioned that not eating sufficient calories would result in a reduction of their energy level,
which would not allow them to dance to their fullest abilities. However, many of these dancers
wrote of desired weight loss, indicating that if they did not eat enough calories they would be
weaker, yet, “skinnier”.
All dancers believed that what and when they eat effects their dancing. Dancers in
Group 1 commonly mentioned that eating a “healthy diet” would give them more energy for a
longer duration. They also stated that eating “junk food” would make them feel “tired and lazy”.
Three of the younger dancers mentioned protein-rich foods and pasta in particular as foods of
high importance for optimal performance.
Approximately 20% of all surveyed dancers realized that eating prior to dancing provided
them with more energy, and eating after rehearsals restored lost energy. A few dancers (n=5)
remarked on the importance of consuming carbohydrates for their overall energy level,

46
specifically mentioning fruit and granola bars. Nine of the older-aged dancers comprising
Group 2 stated that “junk food is bad” and eating too many fats and sugars “is not slimming”.
Conclusion
Young pre-professional dancers such as these surveyed, are keenly aware of a body
image they are often expected to exhibit. As seen by their survey responses pertaining more
often to weight loss and desired leanness, the older dancers (Group 2) are more conscious of this
issue. It is important for both younger and older dancers to have nutrition education incorporated
into their training to prevent any misinformation and/or misinterpretations of dancers’ nutritional
needs required for optimal performance and overall success.
Topics of focus in a nutrition education program for pre-professional, adolescent dancers
should include education on the risk factors associated with the Female Athlete Triad, eating and
training for injury prevention, maintaining hydration, and basic nutrition principles. Sample
meals, snacks, and ideas for “eating on the go” during rehearsal and performance days should be
included in the program as well as handouts and worksheets to provide interactive activities. As
suggested by the findings of this survey, it is clear that young dancers have significant interests
in improving their performance and maintaining a high energy level; program content should
include these aforementioned topics while being sensitive to the dance culture.

47
Table 6. Interests of the Target Audience: Young Dancers’ Nutrition Survey
Questions
1. What would you like to learn about nutrition and why?
2. What do you think would make a nutrition lecture for dancers interesting?
3. What do you think happens if you don’t eat enough calories and how do you think it effects
your dancing?
4. Do you think what you eat and when effects your dancing? How so?

48
CHAPTER 5
Development and Evaluation of an Educational Program for Pre-professional Adolescent Ballet Dancers: Nutrition for Optimal Performance
Abstract
The purpose of this study was to devise, implement, and evaluate a nutritional education
program based upon the theoretical approaches of the Social Cognitive Theory and Health Belief
Model through a DVD lecture series (three, 30-minute classes) into summer intensive programs
for pre-professional, adolescent ballet dancers. The objectives of this nutrition education
program, Nutrition for Optimal Performance, were to increase nutrition knowledge and self-
efficacy for adopting healthier dietary habits in this young athletic population. In addition, we
proposed to test the efficacy of the educational program pre and post delivery via questionnaires
assessing knowledge gained and changes in behavior, including dietary intake. Ballet dancers
aged 13-18 years attending summer intensive programs affiliated with professional ballet
companies were recruited. Group one (n=231) participated in the nutrition education program
while group two (n=90), wait-listed controls, did not participate in the program. Assessments
consisted of demographic characteristics, a Sports Nutrition Knowledge and Behavior
Questionnaire, and a Food Frequency Questionnaire. The intervention group was assessed at
baseline, immediate post-program, and at six weeks post-program. The control group was
assessed at baseline and at six weeks post-baseline. Overall, findings suggested that the program
significantly increased nutrition knowledge, perceived severity and self-efficacy constructs
among pre-professional adolescent dancers. Some improvements in dietary intake habits were
observed among intervention group participants, and some improvements were sustained at the
six-week follow-up assessment. To improve overall health and performance, nutrition education
should be incorporated into the training regimes of adolescent dancers.

49
Keywords: Adolescent Athletes, Dietary Intake, Nutrition Knowledge, Self-Efficacy, Ballet
Introduction
The physical demands placed on dancers are significant; the success of a dancer depends
not only on their athletic capabilities, but also on aesthetic factors 1-3. In order to achieve the
desired long, lean figure, ballet dancers often severely restrict dietary intake and/or engage in
abnormal eating behaviors 2, 4, 5. Student and professional ballet dancers, particularly females,
consume less than 70 to 80% of the recommended dietary allowance for total energy, and often
weigh 10 to 12% below ideal body weight 5-9. The intense training and physical expectations
placed upon dancers, particularly pubertal adolescents, requires significant energy consumption
for optimal performance and adequate nutrient intake 10, 11. Female athletes who participate in
sports where much importance is placed on low body weight are at increased risk for developing
the Female Athlete Triad (FT) 12. Low energy availability (with or without disordered eating),
menstrual irregularity/amenorrhea, and reduced bone density/osteoporosis are the three
interrelated conditions that comprise the disease spectrum of the FT 12. Due to the physical
demands and common dietary behaviors of adolescent dancers, this population is susceptible to
developing the FT.
Conditions of the FT, specifically menstrual irregularities and low energy availability, are
more prevalent in dancers than lean pair-matched non-dancing control women 13. Despite having
similar fat-free mass (FFM), body mass index (BMI), and age, dancers also demonstrate a
significantly lower resting metabolic rate (RMR) and lower energy intake compared to lean, non-
dancing women 13. Similar to these findings, Kaufman et al. also observed dancers to have a
depressed absolute and RMR relative to FFM as compared to non-dancers suggesting that this
phenomenon occurs due to chronic low energy intake 5. A low energy intake relative to

50
predicted energy expenditure may increase energetic efficiency in endurance trained female
athletes 14, which has been observed in female ballet dancers 13.
The FT decreases optimal performance levels and poses significant health risks to female
athletes 12. The negative consequences of the condition are not reversed by pharmacological
treatments 12. While recognition and treatment of the clinical conditions in all effected female
ballet dancers should be a priority, prevention via nutrition and health education aimed at
promoting healthy behaviors in the dancing youth is clearly needed 15. Previous work has
investigated health conditions often afflicting dancers and concluded that increased nutrition
knowledge and education is a necessity 1, 15-19. These investigations indicate that dancers want to
learn proper nutrition 15, and that nutrition education would benefit this athletic population 1, 15-17,
19. To date, only one research article has addressed nutrition education for dancers. Yannakoulia
et al. evaluated the effectiveness of a nutrition intervention that combined education and
prevention of disordered eating in a group of 32 dancers aged 19-25 years 20. Results indicated a
significant increase in nutrition knowledge and decrease in abnormal eating behaviors upon
completion of the 12-week program 20. These results are encouraging for the development of a
nutrition education program targeting adolescent ballet dancers who may be less educated about
healthy eating behaviors and vulnerable to misinformation. However, a larger study population
and the inclusion of a control group for comparison are necessary to evaluate the effectiveness of
a program which could be replicated and implemented on a large-scale basis by professional
dance academies.
Similar programs have been implemented into other populations of young athletes.
Chapman et al. evaluated the effectiveness of a sports nutrition education program (six, 45-
minute lectures) aimed at changing the nutrition behavior of female athletes involved in high

51
school varsity softball teams 21. Although a significant increase in nutrition knowledge was
reported, there was no change in dietary behaviors (food intake and/or food choices) 21. These
results are in agreement with others, suggesting that increased nutrition knowledge and positive
attitudes toward nutrition do not necessarily translate into healthier dietary behaviors 21-23.
Others have not demonstrated success in increasing nutrition knowledge, possibly due to limited
program contact time, and a large student-to-instructor ratio 24. Thus, to overcome limitations of
previous efforts aimed at developing an effective program, intervention content should aim to
increase nutrition knowledge as well as promote the adoption of healthy behaviors in adolescent
athletes. To achieve this objective, interventions should have a theoretical basis 25.
One example of a successful program aimed at teaching healthy nutrition and preventing
disordered eating among female high school students, entitled ATHENA (Athletes Targeting
Healthy Exercise and Nutrition Alternatives), consisted of eight, 45-minute sessions including
topics of healthy sport nutrition, effective training, and the effect of unhealthy behavior on sport
performance 26. This intervention succeeded in many of its health promotion and prevention
goals, perhaps due to its inclusion of lectures concerning behavior modification, demonstrating
that sports teams are effective “vehicles” for a curriculum that promotes healthy lifestyles among
young athletes 26. Summer intensive programs for adolescent ballerinas are similar to this “sport
team” environment and could support positive outcomes of an intervention focused on improving
nutrition knowledge and eating behaviors. However, the culture of professional dance
organizations, which may be at odds with promoting positive health behaviors due to their
emphasis on a dancer’s lean physique, must be considered in program development. Thus,
programs targeting this population must be tailored to the dancer’s need as well as the dance
culture 16, 19, 27.

52
The purpose of this investigation is to develop, implement, and evaluate the effectiveness
of a DVD-based nutrition education program, Nutrition for Optimal Performance, aimed at
improving health knowledge and behaviors of adolescent dancers aged 13-18 years. This
program incorporated theory-based approaches of the Health Belief Model (HBM) and Social
Cognitive Theory (SCT) to promote health and improve health behaviors while taking into
account the needs and interests of the target population and the culture of professional dance
organizations. Overall program objectives are to: 1) inform young dancers on the conditions
comprising the FT and increase their awareness of risks associated with the disorder, 2) educate
dancers on basic nutrition principles that may promote overall health and performance, and 3)
provide dancers with skills needed to develop healthy lifestyle habits. Specifically, this
intervention is designed to increase knowledge of basic nutrition principles, improve self-
efficacy for adopting healthy dietary habits, and increase the consumption of fruit, vegetable, and
high-calcium foods while decreasing consumption of nutrient-poor, high-fat and high-sugar
foods among adolescent pre-professional ballet dancers.
Following completion of the intervention, it is hypothesized that participants will have
increased their knowledge of basic nutrition principles and self-efficacy for adopting healthier
dietary habits as compared to pre-program and control group scores, and that this knowledge will
be sustained post-program at a 6-week follow-up assessment. It is also hypothesized that
intervention participants will demonstrate improvements in eating behaviors, specifically
increased consumption of fruits, vegetables, and calcium-rich foods, and reduced consumption of
high-fat and high-sugar foods.

53
Materials and Methods
Program Development
An overview of the study design is provided in Figure 5. Initial stages of program
development included two preliminary studies, one which assessed the nutritional knowledge
and beliefs of the target population, and a second which assessed the current availability and type
of nutrition education offered to professional ballet dancers and adolescent dancers training in
professional academies. Preliminary study one included 39 male and female adolescent ballet
dancers aged 9-17 years, participating in a pre-professional summer dance program. An open-
ended survey was administered to gauge their interests in nutrition education, and assess
nutritional knowledge and beliefs. Survey questions included: “What would you like to learn
about nutrition and why; What do you think would make a nutrition lecture interesting to
dancers; What do you think happens if you don’t eat enough calories and how do you think it
effects your dancing; Do you think what you eat and when effects your dancing and if so, how?”
Most dancers (> 50%) wanted to learn how to “build leaner muscles”, and “lose weight and keep
weight off”. Respondents indicated they desired weight loss, yet recognized that if they did not
eat enough calories they would “feel weak, yet, look skinnier”. All were interested in learning
nutrition principles that would benefit their performance and overall health. These preliminary
findings are consistent with prior work demonstrating the need for nutrition education focused on
informing young dancers of their nutritional needs and teaching skills for adopting healthier
dietary behaviors 18.
The second preliminary study assessed current practices among professional ballet
companies and the availability of nutrition programs for professional and adolescent dancers and

54
included the directors of professional national ballet companies. Survey questions included: “Do
you currently have some type of nutrition education program for your professional dancers (for
example, programs which address eating for good health and performance); If yes, list type of
program: workshops, seminars, or individual counseling with a nutritionist; Do you currently
have some type of nutrition education program for your students attending the academy during
the school year? If a nutrition program is not offered, what is the primary reason for this?; What
do you believe would be the optimal length of such a program, if you were to offer one?” Of 58
national companies indentified, 29 company directors completed the survey. According to this
survey, few (n=12) companies offer some type of nutrition education to their professional
dancers, which is often provided through individual counseling and only when deemed necessary
by the artistic directors. Many professional ballet companies offer competitive pre-professional
summer intensive programs: a 3 to 6-week, audition-required and acceptance permitting
“summer camp” where young dancers are often housed in dormitories, eat in cafeterias, and
dance six or more hours per day. Of the companies surveyed that offer summer intensive
programs, 85% indicated that they provide nutrition education for the training adolescent
dancers. The quality and content of the nutritional education offered, however, appeared
variable. For example, the education and training of program delivery personnel was often not
identified, and two companies specifically stated a former dancer/instructor delivered their
nutrition programs. Only three of 23 companies indicated that the education was delivered by a
health professional (e.g., registered dietitian, physician).
These preliminary studies demonstrated the typical nutrition knowledge, beliefs, and
areas of interest of the target population, as well as the need for a high-quality nutrition
education program that could be feasibly delivered to pre-professional adolescent dancers.

55
Based upon these preliminary findings and the theoretical components of the HBM and SCT
(Table 7), a program content outline and script was developed, entitled “Nutrition for Optimal
Performance” (See Appendix L). The script was revised following external review by two
registered dietitians (RDs) with expertise in sports nutrition and media communications, and by a
female professional ballet dancer. The script was then narrated and recorded in a DVD format
and edited to include video clips of professional and adolescent dancers, pictures, and text to
accompany the narrator. The DVD underwent multiple revisions and was finalized as three, 10
to 20-minute segments; a length believed to be optimal given the age of the targeted population
(Table 8).
Topics of the three DVD segments include information on the FT and associated health
risks, basic nutrition principles such as functions and sources of macronutrients and
micronutrients (vitamin D, vitamin C, Calcium, and Iron), the importance of adopting healthy
behaviors and healthy habits for dancers, maintaining/monitoring hydration, and
recommendations on eating for optimal health and performance with a focus on exemplary meals
and snacks (Table 8). Colorful handouts presenting the main objectives of each class were
developed, as well as “worksheets” to reinforce content related to macronutrient functions,
percentages, and food sources, and optimal pre-performance breakfast menus (See Appendix M).
Program Evaluation
Following DVD program development, seven elite national professional ballet companies
were contacted and expressed willingness to participate in the program evaluation. These
companies were sent packets of information containing a cover letter explaining the purpose,
benefits, and requirements of the study along with the informed consent (including both the

56
parental permission and child assent forms). The companies mailed this packet to dancers (aged
13-18 years old) who were accepted into their summer intensive program. The signed forms
were mailed back to the ballet company along with the company's own summer intensive
registration material, then forwarded to the study investigators.
All dancers attending the three summer intensives of the “intervention” companies
(n~445) attended the nutrition classes of educational program, however, only those who provided
prior consent completed pre- and post-program assessments. Teaching and administrative staff
of the ballet companies were encouraged to audit the lectures. The lead investigator (A.D-L.)
was present at all three of the DVD class segments during each summer intensive and
administered all handouts, worksheets, and assessments to the participants. A one-hour time
period for three consecutive days was allotted at each company; this allowed time for
participants to view the DVD program and complete worksheets and/or assessments.
Control participants received parental permission and child assent forms by the same
process. The lead investigator attended the control group summer intensive programs to
administer assessments during one, 30-minute time period. These dancers did not receive the
nutrition education program, however, they were provided with a printed educational packet of
nutrition information following the completion of their 6-week follow-up assessments (See
Appendix N). The “control group” companies were provided with copy of all program materials
(DVD lecture series and handouts) following the study, in the event they wished to include the
program in the following year’s summer intensive.
Participants

57
A total of 321 male and female dancers (aged 13-18 years) from seven summer intensive
programs affiliated with professional ballet companies were enrolled in this study. The
intervention group participants (n=231) received the “Nutrition for Optimal Performance”
program, while the control group participants (n=90) did not participate in the nutrition education
program. The study protocol and consent documents were approved by the Institutional Review
Board of Virginia Polytechnic and State University (Virginia Tech) prior to study initiation.
Assessments
Assessments included self-reported general demographic information (name, age,
ethnicity, weight, height, years dancing, previous nutrition education, and contact information), a
Sports Nutrition Knowledge and Behavior Questionnaire (SNKBQ) (developed by the
investigators; See Appendix K), and a Food Frequency Questionnaire (FFQ). As depicted in
Figure 5, intervention group participants completed assessments prior to the program,
immediately post-program, and at 6-weeks post-program, once they had returned home, to
determine longer term effectiveness and sustainability of targeted outcomes. Control group
participants were assessed at the beginning of the summer intensive program and again after six
weeks once returned home. All participants were instructed not to look for answers to SNKBQ
items once they returned home, to avoid external influence on the 6-week follow-up assessment
score. All questionnaires were administered by the lead investigator except for the 6-week
assessments, which were mailed to the participants in a packet including a stamped, addressed
return envelope. Participants were compensated $10 for their time following completion and
return of the 6-week assessments.

58
The SNKBQ was developed for this investigation after reviewing literature on adolescent
dancers’ health and nutrition misconceptions, and prior work done by this investigative team 13.
The SNKBQ consists of two parts: part one assesses sports nutrition knowledge while part two
(Table 9) assesses self-efficacy for adopting healthier dietary habits, perceived susceptibility to
the FT, and outcome expectations for the development of healthy dietary habits. Part two also
includes five questions from the Eating Attitudes Test-26 28 to assess abnormal eating behaviors
(AEB) allowing participants to score a maximum of 15 total points. The questions concerning
self-efficacy, perceived susceptibility and outcome expectations on the SNKBQ were scaled 1-5
to allow for consistency in answers and based on the nutrition self-efficacy scale developed by
Schwarzer and Renner, and Champion et al 29, 30. The SNKBQ was pilot-tested in 15 adolescent
dancers to ensure clear and understandable wording of questions/answers and to test reliability.
Pilot participants completed the SNKBQ on two occasions, one week apart. The Wilcoxon
Signed Rank Test was used to determine reliability of time one and time two for each question.
Responses were not different for 20 of 21 knowledge questions when comparing answers from
time one and time two. Three of 11 behavioral questions responses differed significantly from
time one and time two on the second occasion but in a favorable direction, suggesting that test
administration may have influenced responses during time two. The SNKBQ score on time one
and time two was not different (time one score: 64 +/- 5%; time two score: 64 +/- 4 % correct;
P=0.87).
The FFQ consisted of the Block dietary fat and fruit-vegetable-fiber screener 31, and
selected questions adapted from the Youth Risk Behavior Survey 32 and Youth/Adolescent Food
Frequency Questionnaire 33, 34. The FFQ assesses intake of adolescents by food groups including

59
fruits, juices, water, vegetables, cereals, protein sources, milk and cheese, soft drinks, sweets,
and high fat snacks, with outcomes measured in servings and frequency 31.
Statistical Analysis
Data analyses (SPSS for Windows, V.12.0.) included descriptive characteristics,
independent sample t-tests for between group comparisons (demographic characteristics and
baseline primary outcomes), and chi-square tests for frequency variables. One-way ANOVA
with Tukey post-hoc tests and repeated measures ANOVA were utilized for between-company
comparisons and to determine differences over the three time points among intervention group
participants. Where differences over time were found, paired t-tests were used to identify
significant differences between time points. Power calculations on the key outcome variable of
the SNKBQ score, using results from literature on nutrition intervention programs (expected
within group differences, standard deviations, α =0.05) indicated that within group statistical
power was 99% for SNKBQ scores with a sample size of 115 per group. Because results are
dependent on the number of returned 6-week follow up assessments, power calculations were
also performed on a within group sample size of 75 subjects, which estimated a 65% return rate
of follow up assessments. With a sample size of 75 per group, statistical power was 98% for
SNKBQ scores.
Results
Six professional companies and one youth professional company were recruited for this
study. Three of these companies (I1, I2, I3) comprised the intervention group, while four
companies (C4, C5, C6, C7) comprised the control group. Self-reported baseline demographic
characteristics of intervention and control companies are presented in Table 10. Baseline primary

60
outcomes including sports nutrition knowledge and eating behaviors were similar within groups.
Differences within control companies were found in age (C5) and years dancing (C6).
Differences within the intervention companies were found in age and height (I3), and in BMI
(I1). Although these significant differences were observed in some self-reported demographic
characteristics, the magnitude of these differences is not believed to be of practical significance
(e.g., most < 1 unit difference). Because demographic characteristic differences across company
type were minimal, baseline primary outcomes were not different, and all participating
companies were of comparable caliber and reputation, these companies were collapsed into two
groups, intervention and control (Table 11). The intervention group consisted of 231 participants.
Of these participants, 221 completed both baseline and post-program assessments, and 146
completed all three assessments (baseline, immediate post-program, and 6-week follow-up). The
control group consisted of 90 participants, 64 of whom completed both baseline and 6-week
follow up assessments (Figure 5). At baseline, primary outcomes of sports nutrition knowledge
and eating behavior scores were similar between groups (Table 11). Most participants were
female, Caucasian, and reported having some previous nutrition education. No differences in
baseline group demographic characteristics were noted with the exception of BMI and years
dancing, however these differences were minimal (< 1 unit for BMI and < 1 year for dancing
experience). To account for these differences, variables different at baseline were included as
covariates in subsequent analyses.
Analysis of baseline and 6-week follow-up assessment results between groups is
indicative of program effectiveness in increasing nutrition knowledge, perceived severity, and
self efficacy (Table 12). SNKBQ scores from baseline to follow-up within the intervention group
increased by 25%, yet only 8% within the control group. Perceived severity and self-efficacy

61
scores also increased over time in the intervention group (perceived severity score: intervention
group ∆=1.0, control group ∆=0.1; self-efficacy score: intervention group ∆=1.9, control group
∆=0.6). No changes were detected in AEB scores in either group.
Reported dietary fat, saturated fat, and diet soda intake decreased significantly over time
in both groups, while milk intake significantly increased within the intervention group by more
than 7%. Candy intake significantly declined by 33% among intervention group participants as
compared to an 11% decline among control group participants.
Significant improvements were observed within the intervention group from baseline to
immediate post-program assessments in nutrition knowledge (baseline: 66 + 1 v. post-program:
93 + 1 % correct, P<0.05), perceived self-efficacy (7.7 + 0.1 v. 8.9 + 0.1 score, P<0.05) and
perceived severity (15.5 + 0.2 v. 17.9 + 0.2 score, P<0.05) (Table 13). Although these scores
declined from post-program to the 6-week follow-up assessment, they remained significantly
improved from baseline. Reported AEB scores within program participants increased over the
three assessment periods. To further determine how the program influenced abnormal eating
behaviors, analysis was conducted on participants (n=30) who scored above the mean AEB
(score > 2.0) at baseline. Among those participants, AEB scores decreased from baseline to
post-program and remained unchanged in follow-up assessment results (baseline: 4.5 + 0.4; post-
program: 4.0 + 0.4; 6-week follow-up: 4.0 + 0.5).
Across the three time points, improvements were observed in dietary intake from baseline
to post-program (Table 13). Total fat (∆ = -6.4 g), saturated fat (∆ = -2.4 g), percent fat
(∆ = -1.7%) and candy intake (from >1 serving/wk to < 1 serving/wk) decreased from baseline
through follow-up assessments. Significant decreases were observed in fruit and vegetable
consumption from post-program to 6-week follow-up assessments, however, improvements in

62
fast food intake (i.e., 20% reduction) and milk consumption (i.e., 11% increase) were reported.
Lastly, water intake significantly increased from baseline to immediate post-program with
participants consuming water three times per day to almost four times per day, yet declined to
baseline levels by the 6-week follow-up assessment.
Discussion
These findings demonstrate that the nutrition education program, “Nutrition for Optimal
Performance”, improved nutrition knowledge, perceived severity, and self-efficacy for adopting
healthier dietary habits in pre-professional adolescent ballet dancers, and that changes were
sustained for at least six weeks following program participation. Significant increases in
nutrition knowledge and self-efficacy scores were detected from baseline to post-program
assessments within the intervention group. Although some 6-week follow-up scores decreased
from post-program scores within the intervention group, they remained significantly improved
from baseline as well as compared to the control group’s 6-week follow-up assessment.
The program was also associated with improving self-reported dietary intake habits such
as reducing candy, fast food, and soda consumption, while increasing milk consumption. Other
dietary variables were not improved, however. This could be attributed to several factors. First,
the tools used in the assessments of dietary intake may not have been adequate to detect the
changes in all dietary intake variables assessed. Second, participants completed the follow-up
assessment in a different environment than baseline and post-program assessments. During the
first two assessments, the majority of participants were eating away from home in a cafeteria
setting dependent on their own dietary choices (i.e., dormitory cafeteria). The final assessments
were completed in their usual home living environment, where participants likely depended on
others for purchasing and preparing meals. This factor may represent parental influence on the

63
participants’ eating habits and suggests that future interventions should consider including
families in educational programs. Lastly, because some dietary improvements were observed in
post-program but not in follow-up assessments, this may indicate the possibility of only short-
term program effectiveness regarding improvements in dietary intake habits.
Some studies have shown that increases in nutrition knowledge do not translate to
improvements in eating behavior and dietary intake 20-23. Yannakoulia et al. proposed that
detection of improvements in nutrition knowledge and perceptions may be immediate, however
changes in nutrient consumption are gradual and may not be detectable at a short-term (i.e., six
week) follow-up period 20. Thus, future studies could include a longer-term follow-up period.
A selection of questions from the EAT-26 was chosen to assess abnormal eating
behaviors and not to diagnose disordered eating (Table 9). Overall, AEB scores were very low
(i.e., < 2 of 15-point maximum). Also, there were no group by time differences in AEB scores;
the only significant increase in score was noted within the intervention group alone at the 6-week
follow-up assessment. Importantly, a reduction in scores within the population subset scoring
above the mean from baseline to post-program was observed. Also, follow-up scores for these
participants remained the same as post-program results. Program content included discussion of
the calorie content of food items to educate dancers on, for example, macronutrient composition
of food items. This information may have increased the dancers’ awareness of the caloric
content of specific foods causing them to answer AEB questions (e.g., question 8 in Table 9)
differently post-program; this may not necessarily indicate problems with abnormal eating
behaviors. This program did not directly address eating disorders, as the objective was to educate
adolescent dancers on skills to make healthy dietary choices. The overall increase in AEB scores
within the entire intervention group may, therefore, be due to an increased nutrition awareness.

64
Future studies may consider including more comprehensives assessments of AEB in this
population.
It is also important to note that at baseline, < 40% of study participants were able to
accurately answer questions on the SNKBQ related to the FT, or differentiate between aerobic
and anaerobic activities. Overall, participants’ knowledge was also poor (< 40% answered
correctly) in areas concerning functions and food sources of macronutrients and vitamins (i.e.,
vitamins C and D). It is, therefore, suggested that future nutrition education programs include
information on these specific topics.
The implementation of the program in several companies during summer intensives
serves as a strength of this investigation. Companies may vary in bias toward ideals on body
image/eating habits, thus demonstrating effectiveness in a large sample including multiple
companies demonstrates broad program effectiveness, and increases the generalizability of our
findings. Also, the DVD-format of the program increases ease of program delivery and
reproducibility, while minimizing cost. Lastly, the large sample size and relatively high follow-
up response rate (68%) were strengths. Nevertheless, we acknowledge several limitations. First,
the program was of short duration, however, both immediate and longer-term improvements in
primary outcomes were detected. A similar intervention consisting of a smaller group of older
dancers and longer in duration (i.e., 12 weekly two-hour classes) reported similar findings of
increased nutrition knowledge yet no difference in nutrient intake from baseline to post-
intervention to 6-month follow-up assessments 20. Also, reliance on self-reported measures is a
limitation. However, due to the large study sample size, available resources, and limited time for
program evaluation, other means of assessing outcomes were not feasible.

65
Conclusion
Ballet dancers are a high risk population of athletes susceptible to adverse health
outcomes such as the FT. Educating adolescent dancers in proper nutrition and improving skills
for adopting healthier dietary habits may be the key to preventing the development of such
conditions, however, current education promoting the health of dancers is minimal and of
questionable quality. The educational program “Nutrition for Optimal Performance”, was
associated with notable increases in adolescent dancers’ nutrition knowledge and self-efficacy,
while improving several key dietary intake behaviors. To date, no other intervention aimed at
educating adolescent dancers on nutrition and health has been conducted, thus these findings are
novel and have important implications for the field of dance medicine and the profession of
dance. Proper nutrition and eating habits are essential to the health and success of the dancer
athlete and should be incorporated into the training regimes of all pre-professional adolescent
dancers.
Acknowledgements
The authors would like to acknowledge the external reviewers for program content:
Roberta Anding, MS, RD; Heather Cox, MS, RD; Anne Mueller, dancer with Oregon Ballet
Theatre. The authors would also like to acknowledge the Virginia Tech Broadcast Center for
recording and editing the DVD: Nutrition for Optimal Performance. Lastly, authors would like to
acknowledge Elizabeth Thompson for creating program handouts and John Doyle for assistance
in aspects of program implementation and data collection.

66
References
1. Benson JE, Geiger CJ, Eiserman PA, et al. Relationship between nutrient intake, body mass index, menstrual function, and ballet injury. J Am Diet Assoc. 1989;89(1):58-63.
2. Cassill K. The bane of the ballerina. Life-threatening thinness. Science Digest.
1980;87:52-55. 3. Micheli LJ, Gillespie WJ, Walaszek A. Physiologic profiles of female professional
ballerinas. Clin Sports Med. 1984;3(1):199-209. 4. Abraham S. Eating and weight controlling behaviours of young ballet dancers.
Psychopathology. 1996;29(4):218-222. 5. Kaufman BA, Warren MP, Dominguez JE. Bone Density and amenorrhea in ballet
dancers are related to a decreased resting metabolic rate and lower leptin levels. J Cli
Endo Met. 2002;87(6):2777-2783. 6. Benson J, Gillien DM, Bourdet K, et al. Inadequate Nutrition and Chronic Calorie
Restriction in Adolescent Ballerinas. Phys Sportsmed. 1985;13(10):79-90. 7. Bonbright JM. The Nutritional Status of Female Ballet Dancers 15-18 Years of Age.
Dance Research Journal. 1989;21(2):9-14. 8. Dahlstrom M, Jansson E, Nordevang E, et al. Discrepancy between estimated energy
intake and requirement in female dancers. Clin Physiol. 1990;10(1):11-25. 9. Calabrese LH, Kirkendall DT, Floyd M. Menstrual abnormalities, nutritional patterns and
body composition in female classical ballet dancers. Phys Sportsmed. 1983;11:86-98. 10. Manore MM. Nutritional needs of the female athlete. Clin Sports Med. 1999;18(3):549-
563. 11. Thompson JL. Energy balance in young athletes. Int J Sport Nutr. 1998;8(2):160-174. 12. Nattiv A, Loucks AB, Manore MM. The female athlete triad. Med Sci Sports Exerc.
2007;39(10):1867-1882. 13. Doyle-Lucas AF, Akers JD, Davy BM. Energetic Efficiency, Menstrual Irregularity, and
Bone Mineral Density in Elite Professional Female Ballet Dancers. Journal of Dance
Medicine and Science, In Press. 14. Brownell KD, Steen SN, Wilmore JH. Weight regulation practices in athletes: analysis of
metabolic and health effects. Med Sci Sports Exerc. 1987;19(6):546-556.

67
15. Sawyer-Morse MK, Smolik T, Mobley C, et al. Nutrition beliefs, practices, and perceptions of young dancers. J Adolesc Health Care. 1989;10(3):200-202.
16. Maloney MJ. Anorexia nervosa and bulimia in dancers. Accurate diagnosis and treatment
planning. Clin Sports Med. 1983;2(3):549-555. 17. McCormick C. Development and Prevention of Disordered Eating in Young Dancers.
SCAN'S PULSE. 2006;25(1):15-16. 18. Braisted JR, Mellin L, Gong EJ, et al. The adolescent ballet dancer. Nutritional practices
and characteristics associated with anorexia nervosa. J Adolesc Health Care. 1985;6(5):365-371.
19. Calabrese LH, Kirkendall DT. Nutritional and medical considerations in dancers. Clin
Sports Med. 1983;2(3):539-548. 20. Yannakoulia M, Sitara M, Matalas AL. Reported eating behavior and attitudes
improvement after a nutrition intervention program in a group of young female dancers. Int J Sport Nutr Exerc Metab. 2002;12(1):24-32. 21. Chapman P, Toma RB, Tuveson RV, et al. Nutrition Knowledge among Adolescent High
School Female Athletes. Adolescence. 1997;32. 22. Story M, Resnick M. Adolescents' Views on Food and Nutrition. Journal of Nutrition
Education. 1986;18(4):188-192. 23. Perron M, Endres J. Knowledge, attitudes, and dietary practices of female athletes. J Am
Diet Assoc. 1985;85(5):573-576. 24. Reading KJ, McCargar LJ, Marriage BJ. Adolescent and Young Adult Male Hockey
Players: Nutrition Knowledge and Education. Can J Diet Pract Res. 1999;60(3):166-169. 25. National Cancer Institute. Theory at a Glance: A Guide for Health Promotion Practice.
Washington, DC: U.S. Department of Health and Human Services 2003. 26. Elliot DL, Goldberg L, Moe EL, et al. Preventing substance use and disordered eating:
initial outcomes of the ATHENA (athletes targeting healthy exercise and nutrition alternatives) program. Arch Pediatr Adolesc Med. 2004;158(11):1043-1049.
27. Stensland SH, Sobal J. Dietary practices of ballet, jazz, and modern dancers. J Am Diet
Assoc. 1992;92(3):319-324. 28. Garner DM, Olmsted MP, Bohr Y, et al. The eating attitudes test: psychometric features
and clinical correlates. Psych Med. 1982;12:871-979.

68
29. Schwarzer R, Renner B. Social-cognitive predictors of health behavior: action self-efficacy and coping self-efficacy. Health Psychol. 2000;19(5):487-495.
30. Champion VL. Instrument development for health belief model constructs. ANS Adv Nurs
Sci. 1984;6(3):73-85. 31. Block G, Gillespie C, Rosenbaum EH, et al. A rapid food screener to assess fat and fruit
and vegetable intake. Am J Prev Med. 2000;18(4):284-288. 32. CDC. Methodology of the Youth Risk Behavior Surveillance System 2004:1-13.
< www.cdc.gov/yrbss >.
33. Rockett HR, Breitenbach M, Frazier AL, et al. Validation of a youth/adolescent food f requency questionnaire. Prev Med. 1997;26(6):808-816. 34. Rockett HR, Wolf AM, Colditz GA. Development and reproducibility of a food
frequency questionnaire to assess diets of older children and adolescents. J Am Diet
Assoc. 1995;95(3):336-340.

69
Table 7. Nutrition for Optimal Performance: Theoretical Constructs Incorporated Into Program
Content
Theoretical Construct Program Content Perceived Susceptibility and Severity1
- Disease consequences and risks of the Female Athlete Triad (FT) in terms of health and dancing career - Facts on dancers’ susceptibility to the FT
Benefits and Barriers1
Outcome Expectations of Behavior Changes2
Personal Reinforcement2
- Eating properly increases health, energy level, and performance - Developing healthy habits is free, while doctors visits, medications, and physical therapy is costly and time consuming - Days taken to recover from injury decrease skills, days that should be used for training, and important performing opportunities. This may be prevented by the development of good eating habits. - Development of healthy habits may allow for intense training, an increase in skills, and better roles or promotion to higher training levels.
Cues to Action1
Observational Learning2
- Pictures of all food items and meals discussed - Pictures and video clips of adolescent, healthy dancers performing healthy activities - Pictures and video clips of healthy professional dancers
Perceived Self-Efficacy1,2
Goals2
- Information to help guide dancers to make healthier dietary choices - Skills on how to make a healthy breakfast, lunch, and dinner - Skills on how to monitor hydration status - Skills to prevent the development of the FT - Information on 10 healthy habits to include in a daily routine and how to adopt them
1Health Belief Model, 2Social Cognitive Theory.

70
Table 8. Nutrition for Optimal Performance: Class Titles and Objectives
CLASS TITLE CLASS OBJECTIVES Class One- An Overview: Nutrition for pre-
professional dancers and the importance of
healthy behaviors
(10 Minutes)
Participants will learn: • The difference between aerobic and
anaerobic exercise; • What the Female Athlete Triad is, the three
conditions comprising the Triad, and associated risks; and • The importance of adopting healthy eating habits. Handout: • “Healthy Behaviors and the Female Athlete
Triad: Being the Best You Can Be!” Class Two-Nutrition Principles for Dancers
(16 Minutes)
Participants will learn: • What a calorie is and how much dancers need
to consume in one day for good health; • The three primary macronutrients found in
food, what they provide the body, how much should be eaten daily and specific food sources of each; and • The roles of vitamin D, vitamin C, Calcium,
and Iron including the recommended daily allowance for adolescent athletes and specific food sources of each. Handout: • “Nutrition Principles for Dancers: Learning
the Basics” Worksheet: • “Application of Nutrition Principles”
Class Three-Eating for Optimal Health and
Performance
(16 Minutes)
Participants will: • Be able to name at least five healthy habits to
aim for daily; • Understand the importance of drinking water
and staying hydrated, and how to monitor their own hydration status (“WUT”); and • Be able to give an example of a dinner that should be eaten the evening before a performance. Handout: • “Eating for Optimal Performance: What
Should I Eat?”

71
Table 9. Sports Nutrition Knowledge and Behavior Questionnaire: Response Options and
Associated Question Stems
Section One: Female Athlete Triad Perceived Severity (2 questions)
Response Options Questions
Scale: 1-Strongly Disagree to 5-Strongly Agree
Total Score: 10 Maximum
1. I believe that the Female Athlete Triad is a
severe health problem affecting dancers.
2. If I had The Female Athlete Triad, my
dancing would suffer
Section Two: Healthy Habits Perceived Self-Efficacy (4 questions)
Scale: 1-Not Certain to 5- Very Certain
Total Score: 20 Maximum
3. How certain are you that you would know
what foods to choose for a healthy breakfast
meal?
4. I am certain that I know how to eat enough
calcium through food sources every day.
5. How likely are you to bring fruit to the
studio/theatre and eat it for a snack between
rehearsals every day?
6. How likely are you to consume a
carbohydrate-rich dinner the evening prior to a
performance?
Section Three: Abnormal Eating Behaviors (5 questions selected from EAT-261)
Responses: Always, Usually, Often, 7. I avoid eating when I am hungry.

72
Sometimes, Rarely, or Never
Total Score: Maximum 15
8. I am aware of the calorie content of foods
that I eat.
9. I particularly avoid foods with a high
carbohydrate content (i.e. bread, rice, potatoes,
etc).
10. I feel extremely guilty after eating.
11. I avoid foods with sugar in them.
1EAT-26, Eating Attitudes Test-26

73
Table 10. Comparison of Baseline Demographic Characteristics of Intervention (I) and Control
(C) Companies1
I1 I2 I3 C4 C5 C6 C7
(n=60) (n=91) (n=80) (n=28) (n=16) (n=23) (n=23)
SNKBQ,
% correct
65.3
+ 2.0
64.2
+ 1.5
66.4
+ 1.6
66.3
+ 3.0
64.3
+ 2.2
60.4
+ 3.3
60.2
+ 2.0
AEB, score 1.2
+ 0.2
1.6
+ 0.2
1.9
+ 0.2
1.4
+ 0.3
1.5
+ 0.5
1.3
+ 0.3
1.5
+ 0.3
Age, yrs 15.2
+ 0.2a
15.1
+ 0.1a
15.9
+ 0.1b
15.6
+ 0.3a,b
16.4
+ 0.2b
15.0
+ 0.3a
15.0
+ 0.3a
Weight, kg 51.7
+ 1.0
50.0
+ 0.8
51.6
+ 0.7
51.7
+ 1.3
53.7
+ 2.2
51.3
+ 1.3)
53.0
+ 1.5
Height, cm 165
+ 1.1a
165
+ 0.8a,b
168
+ 0.7b
164
+ 1.4
165
+ 2.3
163
+ 1.3)
166
+ 1.5
BMI, kg/m2 18.9
+ 0.2b
18.2
+ 0.2a
18.2
+ 0.1a
19.1
+ 0.3
19.6
+ 0.4
19.3
+ 0.4)
19.3
+ 0.4
Years Dancing, yrs 9.2
+ 0.3
9.3
+ 0.3
10.0
+ 0.3
10.2
+ 0.5a,b
10.9
+ 0.7a,b
11.1
+ 0.4b
8.9
+ 0.5a
1Values reported as Means + SEM. Abbreviations Used: BMI, Body Mass Index; SNKBQ,
Sports Nutrition Knowledge and Behavior Questionnaire; AEB, Abnormal Eating Behaviors
(score out of 15).
a,bDifferent letters indicate significant mean differences (P<0.05) within company type (I, C)
using a Tukey post hoc analysis.

74
Table 11. Baseline Demographic Characteristics of Enrolled Participants1
Intervention (n=231) Controls (n=90)
Mean + SEM (Range) Mean + SEM (Range)
SNKBQ, % correct 65.2 + 1.0 (24.0-90.0) 62.9 + 1.4 (29.0-95.0)
AEB, Score 1.6 + 0.1 (0.0-12.0) 1.4 + 0.2 (0.0-6.0)
Age, yrs 15.4 + 0.1 (13.0-18.0) 15.4 + 0.1 (13.0-18.0)
Weight, kg 51.0 + 0.5 (34.1-74.1) 52.3 + 0.7 (34.8-74.0)
Height, cm 166 + 0.5 (145-188) 164 + 0.8 (150-185)
BMI, kg/m2 18.4 + 0.1 (15.0-22.9) 19.3 + 0.2* (15.5-23.5)
Years Dancing, yrs 9.5 + 0.2 (3.0-15.0) 10.2 + 0.3* (2.0-15.0)
Sex, n
Male (M) / Female (F)
14 M / 217 F 6 M / 84 F
Previous Sports Nutrition
Counseling Received, n
Yes (Y) / No (N)
173 Y / 58 N 58 Y / 32 N
*Significantly different from Intervention participants (P<0.05). 1Abbreviations Used: BMI,
Body Mass Index; SNKBQ, Sports Nutrition Knowledge and Behavior Questionnaire; AEB,
Abnormal Eating Behaviors (score out of 15).

75
Table 12. Baseline and 6-Week Follow-Up Assessment Results for Intervention and Control
Participants for Nutrition Knowledge, Theory-Based Behavioral Constructs and Self-Reported
Dietary Intake1
Intervention Group
(n=146)
Control Group
(n=64)
Baseline Demographic
Characteristics:
Age, yrs 15.4 + 0.1 15.4 + 0.2
BMI, kg/m2 18.3 + 0.1 19.3 + 0.2*
Years Dancing, yrs 9.5 + 0.2 10.1 + 0.3
Baseline 6-week
follow-up
Baseline 6-week
follow-up
Nutrition Knowledge and
Related Behavioral Constructs:
SNKBQ2,3, % Correct 66.5 + 1.2 91.0 + 1.0 62.7 + 1.8 70.9 + 1.5
FT Perceived Severity3,
Total Score (Maximum 10)
7.7 + 0.1 8.7 + 0.1 7.6 + 0.2
7.7 + 0.2
HH Perceived Self-Efficacy3,
Total Score (Maximum 20)
15.5 + 0.2 17.4 + 0.2 15.4 + 0.4
16.0 + 0.3
AEB, Score (Maximum 15) 1.5 + 0.2 1.8 + 0.2 1.5 + 0.2 1.4 + 0.3

76
Self-Reported Dietary Intake:
Total Fat2, g 95.2 + 1.8 88.2 + 1.6 91.7 + 2.8 89.3 + 2.5
Saturated Fat2, g 25.1 + 0.7 22.5 + 0.6 23.1 + 1.1 22.2 + 1.0
Percent Fat2, % 34.9 + 0.5 33.2 + 0.4 34.0 + 0.7 33.4 + 0.6
Fruit and Vegetable, Servings 4.9 + 0.1 4.5 + 0.1 4.9 + 0.2 4.4 + 0.2
Vitamin C, mg 162 + 3 155 + 4 164 + 5 151 + 6
Magnesium, mg 400 + 6 387 + 7 399 + 9 377 + 10
Potassium, mg 3803 + 58 3681 + 65 3813 + 90 3595 + 100
Fiber, g 21.3 + 0.4 20.5 + 0.4 21.4 + 0.6 20.0 + 0.7
Low Fat Dairy, Scorea 2.4 + 0.1 2.2 + 0.1 2.3 + 0.1 2.1 + 0.2
Fried Fast Food, Scorea 0.5 + 0.1 0.4 + 0.1 0.6 + 0.1 0.7 + 0.1
Candy3, Scorea 1.2 + 0.1 0.8 + 0.1 0.9 + 0.1 0.8 + 0.1
Milk2,3, Scoreb 2.5 + 0.1 2.7 + 0.1 2.5 + 0.2 2.4 + 0.2
Soda, Scoreb 0.6 + 0.1 0.5 + 0.1 0.4 + 0.1 0.4 + 0.1
Diet Soda2, Scoreb 0.6 + 0.1 0.5 + 0.1 0.3 + 0.1 0.3 + 0.1
Water, Scoreb 5.1 + 0.1 5.0 + 0.1 5.0 + 0.2 4.5 + 0.2
1Mean+SEM. Abbreviations Used: SNKBQ, Sports Nutrition Knowledge and Behavior
Questionnaire; FT, Female Athlete Triad; HH, Healthy Habits; AEB, Abnormal Eating
Behaviors.
*Significantly different from Intervention participants (P<0.05).
2Significant main effect of time, P < 0.05.
3Significant group by time interaction, P < 0.05.

77
aScore: 0, never/less than 1 serving per week; 1, 1 serving during the past week; 2, 2-6 servings
during the past week; 3, 1 serving per day; 4, 2 + servings per day.
bScore: 0, none during the past week; 1, 1-3 times during the past week; 2, 4-6 times during the
past week; 3, 1 time per day; 4, 2 times per day; 5, 3 times per day; 6, 4 + times per day.

78
Table 13. Intervention Group Results of Participants Completing All Baseline, Immediate Post-
Program, and 6-Week Follow-Up Assessments (n=146)1
Variable Baseline Post-Program 6-Week Follow-Up
Nutrition Knowledge and
Related Behavioral Constructs:
SNKBQ, % correct
FT Perceived Severity,
Total Score (Maximum 10)
HH Perceived Self-Efficacy,
Total Score (Maximum 20)
AEB, Score (Maximum 15)
66.4 + 1.2
7.7 + 0.1
15.5 + 0.2
1.5 + 0.2
93.4 + 0.8*
8.9 + 0.1*
17.9 + 0.2*
1.5 + 0.2
91.0 + 0.8*a
8.7 + 0.1*
17.4 + 0.2*a
1.8 + 0.2*a
Self-Reported Dietary Intake:
Total Fat, g
Total Sat Fat, g
Percent Fat, %
Fruit and Vegetables, serving
Vitamin C, mg
Magnesium, mg
Potassium, mg
Fiber, g
Low Fat Dairy2, Score
Fried Fast Food2, Score
95.0 + 1.8
25.0 + 0.7
35.0 + 0.4
4.9 + 0.1
161 + 3
398 + 6
3795 + 58
21.2 + 0.4
2.3 + 0.1
0.5 + 0.1
93.0 + 1.7*
24.1 + 0.7*
34.3 + 0.4*
4.8 + 0.1
164 + 3
402 + 6
3834 + 58
21.5 + 0.4
2.5 + 0.1
0.4 + 0.1*
88.6 + 1.6*a
22.6 + 0.6*a
33.3 + 0.4*a
4.5 + 0.1*a
155 + 4a
387 + 7a
3678 + 65a
20.5 + 0.4a
2.2 + 0.1a
0.4 + 0.1*

79
Candy2, Score
Milk3, Score
Soda3, Score
Diet Soda3, Score
Water3, Score
1.2 + 0.1
2.4 + 0.1
0.6 + 0.1
0.6 + 0.1
5.1 + 0.1
1.0 + 0.1*
2.5 + 0.1
0.5 + 0.1
0.5 + 0.1
5.4 + 0.1*
0.8 + 0.1*a
2.7 + 0.1*a
0.5 + 0.1
0.5 + 0.1
5.0 + 0.1a
1Mean+SEM. Abbrevations Used: SNKBQ, Sports Nutrition Knowledge and Behavior
Questionnaire; FT, Female Athlete Triad; HH, Healthy Habits; AEB, Abnormal Eating
Behaviors.
2Score: 0, never/less than 1 serving per week; 1, 1 serving during the past week; 2, 2-6 servings
during the past week; 3, 1 serving per day; 4, 2 + servings per day.
3Score: 0, none during the past week; 1, 1-3 times during the past week; 2, 4-6 times during the
past week; 3, 1 time per day; 4, 2 times per day; 5, 3 times per day; 6, 4 + times per day.
*Significantly different from baseline scores, P<0.05.
aSignificantly different from post-program scores, P<0.05.

80
Figure Legends
Figure 5. Overview: Program Development, Implementation, and Evaluation of Nutrition for
Optimal Performance

81
PTER 6
Study One: Assessment of nutrition knowledge and beliefs of dancers aged 9-17 years (n=39)
Study Two: Assessment of current practices among professional ballet companies - the availability of nutrition programs for professional and adolescent dancers Contacted companies (n=58) Respondents (n=29)
Program Evaluation: Nutrition for Optimal Performance
Initial Company Recruitment (n=7) Total Participants Enrolled (n=321)
Intervention group (n=231) Completed baseline assessment
Received Nutrition for Optimal Performance program
Control group (n=90) Completed baseline assessment
Did not receive nutrition education program
Discontinued Intervention (n=10) Absent from one or more classes
Completed immediate post-program assessments (n=221)
6-Week follow-up Completed follow-up assessment (n=146) Did not return assessment (n=72) Returned, Inaccurate mailing address (n=2)
Included in analysis: Baseline, n=231; post-program, n=221; 6-week follow-up, n=146
6-Week follow-up Completed follow-up assessment (n=64) Incomplete assessment (n=25) Returned, Inaccurate mailing address (n=1)
Included in analysis: Baseline, n= 90; 6-week follow-up, n=64
Program Development: Preliminary Studies
Program Development: Program content outline, DVD script draft, and external review; DVD production
Program Implementation: 3 intervention companies, 4 control companies identified and recruited
Figure 5. Overview: Program Development, Implementation, and Evaluation of Nutrition for Optimal Performance

82
Chapter 6
Conclusions
Throughout history, ballet dancers have been predominantly viewed as artists which may
be reason for the lack of research on the health of dancers. Yet, these unique athletes are a high-
risk population susceptible to adverse health outcomes due to the professional dance culture. To
increase available research in this population, we conducted multiple investigations. In the first
study, our purpose was to determine the physical and behavioral characteristics of professional
female ballet dancers and their association to the Female Athlete Triad (FT). Our findings
supported our hypothesis that despite similar fat-free mass (FFM), resting metabolic rate (RMR)
was significantly lower in dancers as compared to pair-matched (by age, body mass index, and
FFM) non-dancing control women. Regardless of their higher total daily energy expenditure,
energy intake was also significantly lower in dancers. Additionally, we determined that
conditions of the FT were more prevalent in the dancer population than in control women,
suggesting that low energy availability may be the primary cause for low bone density, menstrual
irregularities, and a depressed RMR in these female athletes. The findings suggest the need for
programs aimed at the prevention of these adverse health outcomes commonly afflicting
professional ballet dancers.
Our subsequent investigation consisted of two “formative work” preliminary studies.
The objectives of these studies were to determine, 1) the availability of nutrition education
offered to professional dancers and, 2) the nutritional interests and needs of adolescent pre-
professional dancers. The findings suggest that nutrition education offered to professional
dancers is minimal and more commonly offered to adolescent pre-professional dancers. The
quality of programs available, however, is questionable. To address these issues, we conducted

83
our final investigation with the purpose of developing, implementing, and evaluating a nutrition
education program, entitled “Nutrition for Optimal Performance”. This program aimed to
increase sports nutrition knowledge and self-efficacy to adopt healthier dietary habits among
adolescent pre-professional dancers. In agreement with our hypothesis, the program was
effective in improving the primary outcomes. This program could, therefore, be reproduced and
disseminated on a larger scale basis in order to provide adolescent dancers with a high-quality
source of nutrition education pertinent to their needs and interests, while being sensitive to
limited resources ballet companies may have in delivering health education programs.
A common methodological limitation of prior work pertaining to the health of dancers is
the absence of control participants for comparison. There is also a lack of research investigating
interventions aimed at educating adolescent dancers, thus the findings of our investigations are
novel and have important implications for the field of dance medicine and the profession of
dance. Future studies should not only consider research investigating health issues among
professional dancers, but should also focus on advancing methods aimed at preventing the
development of adverse health conditions that plague dancers, such as the FT, through education
programs targeting dancing youth. Future interventions promoting adolescent dancers’ health
should consider including artistic directors, ballet instructors, and families in longer-term
educational programs. The social and environmental influence of these figures in adolescent
dancers’ dietary behaviors and perceptions of body image is considerable. The inclusion of these
authoritative individuals in longer-term (i.e., year-round) educational programs may be
associated with more significant, sustained positive effects in behavior change. These future
interventions should also consider incorporating interactive activities such as cooking classes,
food preparation demonstrations, and outings to grocery stores into the educational programs.

84
Both adolescent and professional dancers need to pragmatically integrate the learned nutrition
knowledge into their daily routines. Inclusion of the aforementioned activities may help to more
effectively translate the knowledge gained into behavioral aspects of a dancer’s lifestyle.
In conclusion, dancers are susceptible to the development of adverse health conditions,
including poor bone health, amenorrhea (absence/loss of a menstrual cycle), and low energy
availability (negative energy balance) which may have detrimental long-term effects on health,
performance, and well-being, similar to athletes participating in other sports that place
importance on maintaining a low body weight. Diagnosis and treatment of the conditions are
imperative, yet primary prevention among dancing youth may be the optimal way to improve
health among these “aesthetic” athletes.

V I R G I N I A P O L Y T E C H N I C I N S T I T U T E AND S T A T E U N I V E R S I T YAn equal opportunity, affirmative action i n s t i t u t i o n
Invent the Future
Office of Research ComplianceInstitutional Review Board1880 Pratt Drive (0497)Blacksburg, Virginia 24061540/231-4991 Fax: 540/231-0959E-mail: [email protected] www.irb.vt.edu
V I R G I N I A P O L Y T E C H N I C I N S T I T U T E U N I V E R S I T Y A N D S T A T E U N I V E R S I T Y
DATE: August 21, 2007
MEMORANDUM
TO: Brenda M. DavyAshley Lucas
FROM: David M. Moore
IRB Full IRB Approval: “Is Energy Efficiency Increased in Elite Female Ballet Dancers?” , IRB # 07-294
The above referenced protocol was submitted for full review and approval by the IRB at the June 11,2007, August 13, 2007 and August 13, 2007 meetings. The board had voted approval of this proposal contingent upon receipt of responses to questions raised during its deliberation. Following receipt and review of your responses, I, as Chair of the Virginia Tech Institutional Review Board, have,at the direction of the IRB, granted approval for this study for a period of 12 months, effective August 13, 2007.
Approval of your research by the IRB provides the appropriate review as required by federal and statelaws regarding human subject research. As an investigator of human subjects, your responsibilities include the following:
1. Report promptly proposed changes in previously approved human subject researchactivities to the IRB, including changes to your study forms, procedures and investigators, regardless of how minor. The proposed changes must not be initiatedwithout IRB review and approval, except where necessary to eliminate apparent immediate hazards to the subjects.
2. Report promptly to the IRB any injuries or other unanticipated or adverse events involving risks or harms to human research subjects or others.
3. Report promptly to the IRB of the study’s closing (i.e., data collecting and data analysis complete at Virginia Tech). If the study is to continue past the expiration date (listed above), investigators must submit a request for continuing review prior to the continuing review due date (listed above). It is the researcher’sresponsibility to obtained re-approval from the IRB before the study’s expiration date.
4. If re-approval is not obtained (unless the study has been reported to the IRB as closed) prior to the expiration date, all activities involving human subjects and data analysis must cease immediately, except where necessary to eliminate apparent immediate hazards to the subjects.
Important:If you are conducting federally funded non-exempt research, this approval letter must state that theIRB has compared the OSP grant application and IRB application and found the documents to be consistent. Otherwise, this approval letter is invalid for OSP to release funds. Visit our website at http://www.irb.vt.edu/pages/newstudy.htm#OSP for further information.
SUBJECT:
cc: File
Approval date:Continuing Review Due Date:Expiration Date:
8/13/2007
8/12/20087/28/2008
FWA00000572( expires 1/20/2010)IRB # is IRB00000667
Office of Research ComplianceInstitutional Review Board2000 Kraft Drive, Suite 2000 (0497)Blacksburg, Virginia 24061540/231-4991 Fax 540/231-0959e-mail [email protected]
85
Appendix A

V I R G I N I A P O L Y T E C H N I C I N S T I T U T E AND S T A T E U N I V E R S I T YAn equal opportunity, affirmative action i n s t i t u t i o n
Invent the Future
Office of Research ComplianceInstitutional Review Board1880 Pratt Drive (0497)Blacksburg, Virginia 24061540/231-4991 Fax: 540/231-0959E-mail: [email protected] www.irb.vt.edu
DATE: September 13, 2007
MEMORANDUM
TO: Brenda M. DavyAshley Lucas
FROM: David M. Moore
IRB Amendment 1 Approval: “Is Energy Efficiency Increased in Elite Female Ballet Dancers?” , IRB # 07-294
This memo is regarding the above referenced protocol which was previously granted approval by the IRB on August 13, 2007. You subsequently requested permission to amend your IRB application. Since the requested amendment is nonsubstantive in nature, I, as Chair of the Virginia Tech Institutional Review Board, have granted approval for requested protocol amendment, effective as ofSeptember 12, 2007. The anniversary date will remain the same as the original approval date.
As an investigator of human subjects, your responsibilities include the following:
1. Report promptly proposed changes in previously approved human subject researchactivities to the IRB, including changes to your study forms, procedures and investigators, regardless of how minor. The proposed changes must not be initiatedwithout IRB review and approval, except where necessary to eliminate apparent immediate hazards to the subjects.
2. Report promptly to the IRB any injuries or other unanticipated or adverse events involving risks or harms to human research subjects or others.
3. Report promptly to the IRB of the study’s closing (i.e., data collecting and data analysis complete at Virginia Tech). If the study is to continue past the expiration date (listed above), investigators must submit a request for continuing review prior to the continuing review due date (listed above). It is the researcher’sresponsibility to obtained re-approval from the IRB before the study’s expiration date.
4. If re-approval is not obtained (unless the study has been reported to the IRB as closed) prior to the expiration date, all activities involving human subjects and data analysis must cease immediately, except where necessary to eliminate apparent immediate hazards to the subjects.
Approval date:Continuing Review Due Date:Expiration Date:
8/13/2007
8/12/20087/28/2008
V I R G I N I A P O L Y T E C H N I C I N S T I T U T E U N I V E R S I T Y A N D S T A T E U N I V E R S I T Y
SUBJECT:
cc: File
FWA00000572( expires 1/20/2010)IRB # is IRB00000667
Office of Research ComplianceInstitutional Review Board2000 Kraft Drive, Suite 2000 (0497)Blacksburg, Virginia 24061540/231-4991 Fax 540/231-0959e-mail [email protected]
86
Appendix B

V I R G I N I A P O L Y T E C H N I C I N S T I T U T E AND S T A T E U N I V E R S I T YAn equal opportunity, affirmative action i n s t i t u t i o n
Invent the Future
Office of Research ComplianceInstitutional Review Board1880 Pratt Drive (0497)Blacksburg, Virginia 24061540/231-4991 Fax: 540/231-0959E-mail: [email protected] www.irb.vt.edu
DATE: August 14, 2008
MEMORANDUM
TO: Brenda M. DavyAshley Doyle
FROM: David M. Moore
IRB Full Review Continuation 1: “Is Energy Efficiency Increased in Elite Female Ballet Dancers?” , IRB # 07-294
This memo is regarding the above referenced protocol which was previously granted approval by the IRB. The proposed research, having been previously approved at a convened IRB meeting, required full IRB review prior to granting an extension of approval, according to the specifications authorized by45 CFR 46.110 and 21 CFR 56.110. The above referenced protocol was submitted for full review continuation and approval by the IRB at a recent meeting. Pursuant to your request, I, as Chair of theVirginia Tech Institutional Review Board, have, at the direction of the IRB, granted approval for this study for a period of 12 months, effective August 13, 2008.
Approval of your research by the IRB provides the appropriate review as required by federal and statelaws regarding human subject research. As an investigator of human subjects, your responsibilities include the following:
1. Report promptly proposed changes in previously approved human subject researchactivities to the IRB, including changes to your study forms, procedures and investigators, regardless of how minor. The proposed changes must not be initiatedwithout IRB review and approval, except where necessary to eliminate apparent immediate hazards to the subjects.
2. Report promptly to the IRB any injuries or other unanticipated or adverse events involving risks or harms to human research subjects or others.
3. Report promptly to the IRB of the study’s closing (i.e., data collecting and data analysis complete at Virginia Tech). If the study is to continue past the expiration date (listed above), investigators must submit a request for continuing review prior to the continuing review due date (listed above). It is the researcher’sresponsibility to obtain re-approval from the IRB before the study’s expiration date.
4. If re-approval is not obtained (unless the study has been reported to the IRB as closed) prior to the expiration date, all activities involving human subjects and data analysis must cease immediately, except where necessary to eliminate apparent immediate hazards to the subjects.
.
V I R G I N I A P O L Y T E C H N I C I N S T I T U T E U N I V E R S I T Y A N D S T A T E U N I V E R S I T Y
SUBJECT:
cc: File
Approval date:Continuing Review Due Date:Expiration Date:
8/13/2008
8/12/20097/27/2009
FWA00000572( expires 1/20/2010)IRB # is IRB00000667
Office of Research ComplianceInstitutional Review Board2000 Kraft Drive, Suite 2000 (0497)Blacksburg, Virginia 24061540/231-4991 Fax 540/231-0959e-mail [email protected]
Appendix C
87

V I R G I N I A P O L Y T E C H N I C I N S T I T U T E AND S T A T E U N I V E R S I T YAn equal opportunity, affirmative action i n s t i t u t i o n
Invent the Future
Office of Research ComplianceInstitutional Review Board1880 Pratt Drive (0497)Blacksburg, Virginia 24061540/231-4991 Fax: 540/231-0959E-mail: [email protected] www.irb.vt.edu
DATE: August 18, 2008
MEMORANDUM
TO: Brenda M. DavyAshley Doyle
FROM: David M. Moore
IRB Amendment 1 Approval: “Is Energy Efficiency Increased in Elite Female Ballet Dancers?” , IRB # 07-294
This memo is regarding the above referenced protocol which was previously granted approval by the IRB on August 13, 2008. You subsequently requested permission to amend your IRB application. Since the requested amendment is nonsubstantive in nature, I, as Chair of the Virginia Tech Institutional Review Board, have granted approval for requested protocol amendment, effective as ofAugust 18, 2008. The anniversary date will remain the same as the original approval date.
As an investigator of human subjects, your responsibilities include the following:
1. Report promptly proposed changes in previously approved human subject researchactivities to the IRB, including changes to your study forms, procedures and investigators, regardless of how minor. The proposed changes must not be initiatedwithout IRB review and approval, except where necessary to eliminate apparent immediate hazards to the subjects.
2. Report promptly to the IRB any injuries or other unanticipated or adverse events involving risks or harms to human research subjects or others.
3. Report promptly to the IRB of the study’s closing (i.e., data collecting and data analysis complete at Virginia Tech). If the study is to continue past the expiration date (listed above), investigators must submit a request for continuing review prior to the continuing review due date (listed above). It is the researcher’sresponsibility to obtain re-approval from the IRB before the study’s expiration date.
4. If re-approval is not obtained (unless the study has been reported to the IRB as closed) prior to the expiration date, all activities involving human subjects and data analysis must cease immediately, except where necessary to eliminate apparent immediate hazards to the subjects.
Approval date:Continuing Review Due Date:Expiration Date:
8/13/2008
8/12/20097/27/2009
V I R G I N I A P O L Y T E C H N I C I N S T I T U T E U N I V E R S I T Y A N D S T A T E U N I V E R S I T
SUBJECT:
cc: File
FWA00000572( expires 1/20/2010)IRB # is IRB00000667
Office of Research ComplianceInstitutional Review Board2000 Kraft Drive, Suite 2000 (0497)Blacksburg, Virginia 24061540/231-4991 Fax 540/231-0959e-mail [email protected]
Appendix D
88

An equal opportunity, affirmative action i n s t i t u t i o n
Invent the Future
Office of Research Compliance1880 Pratt Drive (0497)Blacksburg, Virginia 24061540/231-4358 Fax: 540/231-0959E-mail: [email protected] www.irb.vt.edu
cc: File
DATE: March 27, 2008
MEMORANDUM
TO: Brenda M. DavyAshley Doyle
FROM: Carmen Green
IRB Exempt Approval: “Current Practices Among Professional Ballet Companies: Availability of Nutrition Programs for Dancers” , IRB # 08-174
I have reviewed your request to the IRB for exemption for the above referenced project. I concur thatthe research falls within the exempt status. Approval is granted effective as of March 27, 2008.
As an investigator of human subjects, your responsibilities include the following:
1. Report promptly proposed changes in previously approved human subject researchactivities to the IRB, including changes to your study forms, procedures and investigators, regardless of how minor. The proposed changes must not be initiatedwithout IRB review and approval, except where necessary to eliminate apparent immediate hazards to the subjects.
2. Report promptly to the IRB any injuries or other unanticipated or adverse events involving risks or harms to human research subjects or others.
V I R G I N I A P O L Y T E C H N I C I N S T I T U T E U N I V E R S I T Y A N D S T A T E U N I V E R S I T Y
SUBJECT:
FWA00000572( expires 1/20/2010)IRB # is IRB00000667
Office of Research ComplianceCarmen T. Green, IRB Administrator2000 Kraft Drive, Suite 2000 (0497)Blacksburg, Virginia 24061540/231-4358 Fax 540/231-0959e-mail [email protected]
Appendix E
89

Survey Tool: Dancers’ Health Services Survey-
Current Practices among Professional Ballet Companies We are interested in learning about specific health and wellness services, particularly with respect to nutrition counseling, that are available to dancers in professional ballet companies. Your responses will be kept strictly anonymous; we will not identify any individuals responding to this survey by name or by organization. We appreciate your assistance in allowing us to learn more about what types of nutrition programs are currently available to professional dancers, as well as to those training in ballet. 1. Do you currently have some type of nutrition education program for your professional dancers (for example, programs which address eating for good health and performance)?
Yes
No If yes, what type of program: workshops, seminars, individual counseling with a nutritionist, other: (describe)
2. If yes, what type of program: workshops, seminars, individual counseling with a nutritionist, other: (describe)
Yes
No If yes, what are the ages of these dancers receiving education in nutrition? (Check all that apply)
Age 9-11
Age 12-14
Age 15-18
other:
Appendix F
90

If yes, what type of program: workshops, seminars, individual counseling with nutritionist, other: (describe)
3. Do you offer a summer intensive program?
Yes
No If yes, do you offer nutrition education programs as a part of the curriculum?
Yes
No If yes, what type of program: workshops, seminars, individual counseling with a nutritionist, other: (describe)
And, what is the duration of the nutrition program? (number of minutes, hours, etc)
If a nutrition program is not offered, what is the primary reason for this:
Financial
Lack of a person who could provide this type of program
Nutrition programs are low priority relative to other Program components
Lack of time within the summer schedule
other:
91

4. If you do not currently provide a nutrition program, would you be interested in offering a nutrition workshop to your dancers during the summer program that would emphasize eating well for optimal health and performance?
Yes
No What do you believe would be the optimal length of such a program, if you were to offer one? (minutes, hours, etc)
5. Would you permit us to contact you for your feedback on this topic in the future?
Yes
No 6. If you are willing, please provide your name and contact information in the space provided. Or, if you would like us to, with your permission, contact another individual in your organization for feedback, please include their contact information. Your responses to this survey will remain anonymous.
Thank you for taking the time to complete our survey. We appreciate your response! Ashley Doyle-Lucas Virginia Tech Graduate Student Brenda Davy PhD, RD, FACSM Assistant Professor Virginia Tech
92

V I R G I N I A P O L Y T E C H N I C I N S T I T U T E AND S T A T E U N I V E R S I T YAn equal opportunity, affirmative action i n s t i t u t i o n
Invent the Future
Office of Research ComplianceInstitutional Review Board1880 Pratt Drive (0497)Blacksburg, Virginia 24061540/231-4991 Fax: 540/231-0959E-mail: [email protected] www.irb.vt.edu
DATE: December 10, 2008
MEMORANDUM
TO: Brenda M. DavyAshley Doyle
FROM: David M. Moore
IRB Expedited Approval: “A Nutrition Education Program for Adolescent Pre-Professional Ballet Dancers: Nutrition for Optimal Health” , IRB # 08-757
This memo is regarding the above-mentioned protocol. The proposed research is eligible for expedited review according to the specifications authorized by 45 CFR 46.110 and 21 CFR 56.110. As Chair of the Virginia Tech Institutional Review Board, I have granted approval to the study for a period of 12 months, effective December 10, 2008.
As an investigator of human subjects, your responsibilities include the following:
1. Report promptly proposed changes in previously approved human subject researchactivities to the IRB, including changes to your study forms, procedures and investigators, regardless of how minor. The proposed changes must not be initiatedwithout IRB review and approval, except where necessary to eliminate apparent immediate hazards to the subjects.
2. Report promptly to the IRB any injuries or other unanticipated or adverse events involving risks or harms to human research subjects or others.
3. Report promptly to the IRB of the study’s closing (i.e., data collecting and data analysis complete at Virginia Tech). If the study is to continue past the expiration date (listed above), investigators must submit a request for continuing review prior to the continuing review due date (listed above). It is the researcher’sresponsibility to obtain re-approval from the IRB before the study’s expiration date.
4. If re-approval is not obtained (unless the study has been reported to the IRB as closed) prior to the expiration date, all activities involving human subjects and data analysis must cease immediately, except where necessary to eliminate apparent immediate hazards to the subjects.
Important:If you are conducting federally funded non-exempt research, please send the applicable OSP/grantproposal to the IRB office, once available. OSP funds may not be released until the IRB has compared and found consistent the proposal and related IRB applicaton.
V I R G I N I A P O L Y T E C H N I C I N S T I T U T E U N I V E R S I T Y A N D S T A T E U N I V E R S I T Y
SUBJECT:
cc: File
FWA00000572( expires 1/20/2010)IRB # is IRB00000667
Office of Research ComplianceInstitutional Review Board2000 Kraft Drive, Suite 2000 (0497)Blacksburg, Virginia 24061540/231-4991 Fax 540/231-0959e-mail [email protected]
Approval date:Continuing Review Due Date:Expiration Date:
12/10/2008
12/9/200911/25/2009
Appendix G
93

V I R G I N I A P O L Y T E C H N I C I N S T I T U T E AND S T A T E U N I V E R S I T YAn equal opportunity, affirmative action i n s t i t u t i o n
Invent the Future
Office of Research ComplianceInstitutional Review Board1880 Pratt Drive (0497)Blacksburg, Virginia 24061540/231-4991 Fax: 540/231-0959E-mail: [email protected] www.irb.vt.edu
DATE: April 8, 2009
MEMORANDUM
TO: Brenda M. DavyAshley Doyle
FROM: David M. Moore
IRB Amendment 1 Approval: “A Nutrition Education Program for Adolescent Pre-Professional Ballet Dancers: Nutrition for Optimal Health” , IRB # 08-757
This memo is regarding the above referenced protocol which was previously granted approval by the IRB on December 10, 2008. You subsequently requested permission to amend your IRB application.Since the requested amendment is nonsubstantive in nature, I, as Chair of the Virginia Tech Institutional Review Board, have granted approval for requested protocol amendment, effective as ofApril 7, 2009. The anniversary date will remain the same as the original approval date.
As an investigator of human subjects, your responsibilities include the following:
1. Report promptly proposed changes in previously approved human subject researchactivities to the IRB, including changes to your study forms, procedures and investigators, regardless of how minor. The proposed changes must not be initiatedwithout IRB review and approval, except where necessary to eliminate apparent immediate hazards to the subjects.
2. Report promptly to the IRB any injuries or other unanticipated or adverse events involving risks or harms to human research subjects or others.
3. Report promptly to the IRB of the study’s closing (i.e., data collecting and data analysis complete at Virginia Tech). If the study is to continue past the expiration date (listed above), investigators must submit a request for continuing review prior to the continuing review due date (listed above). It is the researcher’sresponsibility to obtain re-approval from the IRB before the study’s expiration date.
4. If re-approval is not obtained (unless the study has been reported to the IRB as closed) prior to the expiration date, all activities involving human subjects and data analysis must cease immediately, except where necessary to eliminate apparent immediate hazards to the subjects.
Approval date:Continuing Review Due Date:Expiration Date:
12/10/2008
12/9/200911/25/2009
V I R G I N I A P O L Y T E C H N I C I N S T I T U T E U N I V E R S I T Y A N D S T A T E U N I V E R S I T Y
SUBJECT:
cc: File
FWA00000572( expires 1/20/2010)IRB # is IRB00000667
Office of Research ComplianceInstitutional Review Board2000 Kraft Drive, Suite 2000 (0497)Blacksburg, Virginia 24061540/231-4991 Fax 540/231-0959e-mail [email protected]
Appendix H
94

V I R G I N I A P O L Y T E C H N I C I N S T I T U T E AND S T A T E U N I V E R S I T YAn equal opportunity, affirmative action i n s t i t u t i o n
Invent the Future
Office of Research ComplianceInstitutional Review Board1880 Pratt Drive (0497)Blacksburg, Virginia 24061540/231-4991 Fax: 540/231-0959E-mail: [email protected] www.irb.vt.edu
DATE: October 30, 2009
MEMORANDUM
TO: Brenda M. DavyAshley Doyle
FROM: David M. Moore
IRB Amendment 2 Approval: “A Nutrition Education Program for Adolescent Pre-Professional Ballet Dancers: Nutrition for Optimal Health” , IRB # 08-757
This memo is regarding the above referenced protocol which was previously granted approval by the IRB on December 10, 2008. You subsequently requested permission to amend your IRB application.Since the requested amendment is nonsubstantive in nature, I, as Chair of the Virginia Tech Institutional Review Board, have granted approval for requested protocol amendment, effective as ofOctober 30, 2009. The anniversary date will remain the same as the original approval date.
As an investigator of human subjects, your responsibilities include the following:
1. Report promptly proposed changes in previously approved human subject researchactivities to the IRB, including changes to your study forms, procedures and investigators, regardless of how minor. The proposed changes must not be initiatedwithout IRB review and approval, except where necessary to eliminate apparent immediate hazards to the subjects.
2. Report promptly to the IRB any injuries or other unanticipated or adverse events involving risks or harms to human research subjects or others.
3. Report promptly to the IRB of the study’s closing (i.e., data collecting and data analysis complete at Virginia Tech). If the study is to continue past the expiration date (listed above), investigators must submit a request for continuing review prior to the continuing review due date (listed above). It is the researcher’sresponsibility to obtain re-approval from the IRB before the study’s expiration date.
4. If re-approval is not obtained (unless the study has been reported to the IRB as closed) prior to the expiration date, all activities involving human subjects and data analysis must cease immediately, except where necessary to eliminate apparent immediate hazards to the subjects.
Approval date:Continuing Review Due Date:Expiration Date:
12/10/2008
12/9/200911/25/2009
V I R G I N I A P O L Y T E C H N I C I N S T I T U T E U N I V E R S I T Y A N D S T A T E U N I V E R S I T Y
SUBJECT:
cc: File
FWA00000572( expires 1/20/2010)IRB # is IRB00000667
Office of Research ComplianceInstitutional Review Board2000 Kraft Drive, Suite 2000 (0497)Blacksburg, Virginia 24061540/231-4991 Fax 540/231-0959e-mail [email protected]
Appendix I
95

FWA00000572( expires 1/20/2010)IRB # is IRB00000667
V I R G I N I A P O L Y T E C H N I C I N S T I T U T E AND S T A T E U N I V E R S I T YAn equal opportunity, affirmative action i n s t i t u t i o n
Invent the Future
Office of Research ComplianceInstitutional Review Board1880 Pratt Drive (0497)Blacksburg, Virginia 24061540/231-4991 Fax: 540/231-0959E-mail: [email protected] www.irb.vt.edu
V I R G I N I A P O L Y T E C H N I C I N S T I T U T E U N I V E R S I T Y A N D S T A T E U N I V E R S I T Y
SUBJECT:
cc: File
DATE: November 13, 2009
MEMORANDUM
TO: Brenda M. DavyAshley Doyle
FROM: David M. Moore
IRB Expedited Continuation 1: “A Nutrition Education Program for Adolescent Pre-Professional Ballet Dancers: Nutrition for Optimal Health” , IRB # 08-757
This memo is regarding the above referenced protocol which was previously granted expedited approval by the IRB. The proposed research is eligible for expedited review according to the specifications authorized by 45 CFR 46.110 and 21 CFR 56.110. Pursuant to your request, as Chairof the Virginia Tech Institutional Review Board, I have granted approval for extension of the study fora period of 12 months, effective as of December 10, 2009.
Approval of your research by the IRB provides the appropriate review as required by federal and statelaws regarding human subject research. As an investigator of human subjects, your responsibilities include the following:
1. Report promptly proposed changes in previously approved human subject researchactivities to the IRB, including changes to your study forms, procedures and investigators, regardless of how minor. The proposed changes must not be initiatedwithout IRB review and approval, except where necessary to eliminate apparent immediate hazards to the subjects.
2. Report promptly to the IRB any injuries or other unanticipated or adverse events involving risks or harms to human research subjects or others.
3. Report promptly to the IRB of the study’s closing (i.e., data collecting and data analysis complete at Virginia Tech). If the study is to continue past the expiration date (listed above), investigators must submit a request for continuing review prior to the continuing review due date (listed above). It is the researcher’sresponsibility to obtain re-approval from the IRB before the study’s expiration date.
4. If re-approval is not obtained (unless the study has been reported to the IRB as closed) prior to the expiration date, all activities involving human subjects and data analysis must cease immediately, except where necessary to eliminate apparent immediate hazards to the subjects.
Approval date:Continuing Review Due Date:Expiration Date:
12/10/2009
12/9/201011/25/2010
Office of Research ComplianceInstitutional Review Board2000 Kraft Drive, Suite 2000 (0497)Blacksburg, Virginia 24061540/231-4991 Fax 540/231-0959e-mail [email protected]
V I R G I N I A P O L Y T E C H N I C I N S T I T U T E U N I V E R S I T Y A N D S T A T E U N I V E R S I T Y
Appendix J
96

Date___________ ID#______________
Sports Nutrition Knowledge and Behavior Questionnaire, Part 1 Write your ID number as your “NAME” on the Scantron (ID number is found on the upper
right of this paper). *Please circle your answer on this form and shade in the corresponding bubble on the Scantron.
Use a Number 2 pencil only, fill in bubbles completely, and mark only ONE bubble per question.
1. Which of these conditions is NOT part of The Female Athlete Triad? a) Amenorrhea b) Osteoporosis c) Low energy availability d) Inflammation
2. Amenorrhea means:
a) That your period stops b) That your hair becomes thin c) That you bruise easily d) That your bones are weak
3. Osteoporosis means:
a) That your period stops b) That your hair becomes thin c) That you bruise easily d) That your bones are weak
4. You can reduce your risk of the Female Athlete Triad by eating a healthy diet with adequate calories.
a) True b) False
5. When a male dancer lifts a female dancer above his head, is this an example of an anaerobic or aerobic activity?
a) Anaerobic activity (without oxygen) b) Aerobic activity (with oxygen)
6. What do Calories measure?
a) Energy b) Weight c) Volume d) Height
7. Which of these macronutrients is the main source of energy/fuel for the body?
a) Protein b) Fat c) Carbohydrates d) Fiber
Appendix K
97

Date___________ ID#______________
8. Which macronutrient is important for maintaining muscle strength? a) Protein b) Fat c) Carbohydrates d) Fiber
9. Which macronutrient is important for proper brain, nerve, and reproductive function?
a) Protein b) Fat c) Carbohydrates d) Fiber
10. Which one of these food items is composed primarily of protein?
a) An orange b) A piece of bread c) Vegetable soup d) Tuna fish
11. What Vitamin is the Sunshine vitamin?
a) Vitamin C b) Vitamin A c) Vitamin B d) Vitamin D
12. Which of these food items is the best source of Vitamin C?
a) Apples b) Oranges c) Potatoes d) Bananas
13. To be used by the body, calcium needs the help of what vitamin?
a) Vitamin C b) Vitamin A c) Vitamin B d) Vitamin D
14. ______ is a good source of Vitamin C, which is needed for a healthy immune system.
a) Broccoli b) A Banana c) An Apple d) Salmon
15. This mineral helps carry oxygen to working muscles:
a) Calcium b) Iron c) Magnesium d) Zinc
98

Date___________ ID#______________
16. Having low amounts of _______ in your body can cause anemia, and ______ is a good food source to increase levels of this mineral.
a) Calcium, Yogurt b) Iron, Yogurt c) Iron, Red meat d) Zinc, Broccoli
17. In general, how many calories does a ballet dancer need in a day?
a) 1,000 to 1,500 b) 500 to 800 c) 2,200 to 3,000 d) 3,500 to 4,500
18. Good sources of carbohydrates include all of the following EXCEPT:
a) Whole grains b) Fruits c) Vegetables d) White bread
19. You can monitor your own hydration status by
a) Weight, Urine, Thirst b) Skin color, Urine, Thirst c) Weight, Urine, Saliva (spit) d) Skin color, Saliva (spit), Thirst
20. Low energy availability can be prevented by:
a) Taking daily vitamins b) Drinking more water c) Eating as many calories as you burn d) Sleeping more than 8 hours each night
21. An example of a meal to eat the evening before a performance, dress rehearsal, or long day of training is:
a) Fried chicken, French fries, ketchup, and soda b) A bowl of soup and water c) Steak, onion rings, and juice d) Spaghetti, broccoli, and milk
99

Date_________ ID#_______________
Sports Nutrition Knowledge and Behavior Questionnaire, Part 2 *Please circle your answer on this form. 1. I believe that the Female Athlete Triad is a severe health problem affecting dancers. (Scale: 1-Strongly Disagree 5-Strongly Agree)
a) 1 b) 2 c) 3 d) 4 e) 5
2. If I had The Female Athlete Triad, my dancing would suffer. (Scale: 1-Strongly Disagree 5-Strongly Agree)
a) 1 b) 2 c) 3 d) 4 e) 5
3. How certain are you that you would know what foods to choose for a healthy breakfast meal? (Scale: 1-Not Certain 5- Very Certain)
a) 1 b) 2 c) 3 d) 4 e) 5
4. I am certain that I know how to eat enough calcium through food sources every day. (Scale: 1-Not Certain 5-Very Certain)
a) 1 b) 2 c) 3 d) 4 e) 5
5. How likely are you to bring fruit to the studio/theatre and eat it for a snack between rehearsals every day? (Scale: 1-Not Likely 5-Very Likely)
a) 1 b) 2 c) 3 d) 4 e) 5
6. How likely are you to consume a carbohydrate rich dinner the evening prior to a performance? (Scale: 1-Not Likely 5- Very Likely)
a) 1 b) 2 c) 3 d) 4 e) 5
100

Date_________ ID#_______________
7. I avoid eating when I am hungry. a) Always b) Usually c) Often d) Sometimes e) Rarely f) Never
8. I am aware of the calorie content of foods that I eat.
a) Always b) Usually c) Often d) Sometimes e) Rarely f) Never
9. I particularly avoid foods with a high carbohydrate content (i.e. bread, rice, potatoes, etc).
a) Always b) Usually c) Often d) Sometimes e) Rarely f) Never
10. I feel extremely guilty after eating.
a) Always b) Usually c) Often d) Sometimes e) Rarely f) Never
11. I avoid foods with sugar in them.
a) Always b) Usually c) Often d) Sometimes e) Rarely f) Never
Office use only- PS: 1. _______ 2._______ Total: ________ SE: 3. _______ 4._______ 5.________ 6. ________ Total: _______ EAT Score: _______
101

102
Class One: An Overview: Nutrition for pre-professional
dancers and the importance of healthy behaviors
SLIDE 1:
This is a nutrition education program for pre-professional adolescent ballet dancers. This program is a series of three classes; each class will teach you knowledge and skills to help you be healthy and perform your best. You are a unique population of athletes and need to care for your bodies so you can train and perform at your highest abilities. SLIDE 2: Welcome to the first of our three classes: This class will focus on the importance of eating both for your health and for optimal performance. After this listening to this presentation, you should understand:
The difference between aerobic and anaerobic exercise What the Female athlete triad is and the three
conditions that comprise it, and The importance of adopting healthy eating habits
SLIDE 3: Dancers are athletes. Ballet requires great physical demands and athletic capabilities. Ballet is similar to other sports like gymnastics, figure skating, and even soccer which all use both aerobic and anaerobic pathways for supplying energy to working muscles. SLIDE 4: Aerobic- means with oxygen. Aerobic exercise is centered around endurance. This type of exercise overloads the heart and lungs and causes them to work harder than at rest. Aerobic exercise can be maintained for a long duration, for example similar to corps de ballet work in ballets like Swan Lake or Giselle. SLIDE 5: Anaerobic-means without oxygen. Anaerobic exercise is comprised of short, high intensity strength-based activities.
Display Objectives
Show pictures of other athletes and dancers Video Clip: Show corps de ballet Video Clip: Show man pressing woman
Appendix L: Nutrition for Optimal Performance Script

103
This type of exercise only last for short spurts. An example of anaerobic activity may be during a pas de deux when the man presses his partner above his head and holds her there for only four to eight counts. SLIDE 6: In a study comparing 60 different sports, ballet was ranked second only to football in terms of physical and mental demands required by, you, the athletes! Because of this intense exercise, ballet dancers like yourselves need to consume enough high-quality food to provide energy in order to perform well.
SLIDE 7: Injuries are prevalent among dancers. Research shows that ballet dancers get hurt as often and as seriously as athletes in contact sports. Certain injuries and conditions that plague dancers, however, can be avoided by proper training and eating well. The Female Athlete Triad is a condition that often effects ballet dancers. The consequences from developing the Female Athlete Triad are severe and can result in injuries, poor performances, and even the end of a dancing career. SLIDE 8: Three conditions comprise the Female Athlete Triad . They include Osteoporosis, Amenorrhea, and Low energy availability. These conditions often occur at the same time in elite female athletes. SLIDE 9: Osteoporosis (“weak bones”)- is a condition that effects the bone, making them extremely fragile and at an increased risk for fracture. Stress fractures that commonly afflict dancers may be an indicator of the beginnings of osteoporosis. Many people are unaware that osteoporosis is a condition that begins during adolescence. It is mistakenly thought of as an “old person’s”
disease, when in reality osteoporosis may begin as early as age 12 when bone growth is occurring. Peak bone mass and
Pictures of whole grains, fruits, vegetables, tuna fish, yogurt
Show picture of a brace, cast Display three conditions: triangle format Again show picture of a brace, cast Show picture of porous bone to normal bone Show young dancer pictures

104
strength is not reached until the age of about 20 in both males and females. SLIDE 10: Amenorrhea is the second condition of the Female Athlete Triad- it effects females and means your period stops. Specifically, it is the lack of having a period after turning 16 years old, or the disappearance of it for more than 90 days. Menstrual irregularities (meaning an irregular period), can sometimes develop into amenorrhea. Amenorrhea can interfere with proper growth of bones and may cause them to become fragile, weak, and prone to breaking. SLIDE 11: Low energy availability is the third condition of Female Athlete Triad- and it occurs when your food, or calorie, intake is much lower than what you “burn off” during a day. This
may be the root cause of both the development of osteoporosis and amenorrhea. Low energy availability is not a good situation for dancers in that it causes your energy levels to be low, and your training and performance ability will suffer.
SLIDE 12: Treating your body like the athlete it is, is important. Eating properly can increase your health, energy level, and performance ability. Ballet dancers are expected to have a lean, but strong body; most every dancer’s goal is to be
slender, strong, powerful, and energetic. Proper nutrition education and the development of good eating habits can help you achieve these goals. SLIDE 13: Injuries can happen quickly, yet take significant time to recover from. The days taken to heal from these injuries can decrease skills and physical condition, and days that should be used for training. These days taken for recovery can limit performance opportunities. No dancer wants to be sitting injured in the audience watching others perform their roles. Developing healthy eating habits will go a long way to help you avoid injuries.
Show picture of negative energy balance scale Video clip
Show injured dancer

105
SLIDE 14: How you treat your body now, when you are young, will determine the health of your body in the future. A career in ballet is extremely challenging both mentally and physically. Your body’s health will indeed effect the duration of your performing career, so it’s important to take good care of your
body now, so it’s healthy in the future. SLIDE 15: I’m sure all of you are wondering, “How do I stay healthy and
free from injury?” Moderation and balance is key. Consider these tips: 1- Eat a balanced diet, 2-Dance with proper technique 3-Rest between classes and rehearsals 4- Get enough sleep (at least 8 hours each night), and 5-Take good care of your body! We’ll talk more about how to eat well in the classes that follow. SLIDE 16: In Summary today you have learned:
The difference between aerobic (endurance) exercise and anaerobic (short, high intensity) exercise.
SLIDE 17:
That the Female Athlete Triad is a common condition effecting ballet dancers and may result in osteoporosis (weak bones), amenorrhea (the stopping of your period), or low energy availability (when you burn off more energy than you eat in food). But, by taking good care of yourself, you can prevent this from happening.
SLIDE 18:
And, that taking care of your body is very important as
a dancer. Injuries are common, but healthy eating habits can help you avoid many of them.
Another professional dancer photo
Show quick video clips of each from Slide 4 and Slide 5
Same picture of porous bone, and negative energy balance scale

106
SLIDE 19: In the next two classes you will learn: Basic nutrition principles and food sources of nutrients. This information will help guide you to make healthier choices and avoid developing the female athlete triad. You will also learn how to eat for optimal performance, how to maintain hydration, and will be given examples of meals and snacks specifically useful to ballet dancers. SLIDE 20:
"If dancing were any easier it would be called football." –anonymous
Oregon Ballet Theatre picture and picture of young happy dancer

107
Class Two: Nutrition Principles for Dancers
SLIDE 1:
Welcome to the second class: Nutrition principles for Dancers
By the end of this class you should understand: What a calorie is and how many you need to consume
in one day for good health The three primary nutrients found in food and what
they provide the body, and The roles of vitamin D, vitamin C, Calcium, and Iron
We are going to begin by defining some basic nutrition terms that we will use:
SLIDE 2: 1- Calorie: A calorie is a unit of measurement for energy. The amount of food you eat and need in a day is measured in calories. The amount of calories (food) that people need in a day varies from person to person. For example, a young woman who is very active, such as a runner or a ballet dancer would need more calories than a young woman who sits all day working on a computer.
SLIDE 3:
Female dancers your age usually need to eat at least 2000 to 2500 calories each day and male dancers often need to consume even more than that, like 2500-3300 calories per day. Calories provide energy for your body-for both its normal daily functions like thinking and talking, as well as for exercise.
SLIDE 4: 2- Metabolism: The complete set of chemical reactions that occur in cells of your body which convert food to energy. This is the rate at which we burn or “use up” calories. Your
metabolism, or metabolic rate, is slower when you are doing things like sitting, and faster when you are moving a lot, like dancing or running. Because your body “uses up” more
Display objectives
Picture of someone sitting versus someone running/dancing w/ calories needed underneath
Show healthy food pictures Same picture as above with each titled w/ slow versus fast metabolism

108
calories when you are exercising, you need to eat more to give your muscles energy to function. SLIDE 5: 3- Macronutrients: There are three primary nutrients found in foods. These are called Macronutrients and include, Carbohydrates, Proteins, and Lipids (also known as Fats). Each of these macronutrients provide your body with energy, and have specific jobs to do.
SLIDE 6:
Carbohydrates are the major sources of energy and fuel for your body to dance. They can be found in grains, fruits, vegetables, and sugars, and are digested rather quickly. Carbohydrates also provide the body with fiber. If you eat too few carbohydrates your body will use its stored protein for energy. Stored protein is found in your muscles, so if you don’t eat enough carbohydrates, your muscle mass and/or strength will decline. You will lose strength and feel weak, and your performance will suffer. This means that you will not be able to dance to the best of your abilities.
SLIDE 7:
Carbohydrates will be the macronutrient that you eat the most of during the day. Let’s say that you are eating about 2200
calories a day. Carbohydrates should make up at least half of those calories!
This means that you should eat about 1100 calories or 275 grams of carbohydrates each day. Usually we count macronutrients (carbohydrates, proteins, and fats) in grams. To calculate the number of carbohydrate grams, divide calories by 4. Here is an example of sources of carbohydrates you could eat to reach 275 grams:
- One cup of granola (64 g CHO) with one cup of skim milk (12 g CHO)
- ½ cup trail mix (45 g CHO) and ½ cup fruit yogurt (25 g CHO)
List Macronutrients
Show picture of whole grains, fruits, vegetables Show nutrition label with carbohydrates circled Show this list of foods with carbohydrate content

109
- A peanut butter and Jelly sandwich (50 g CHO) and one apple (20 g CHO)
- One cup of spaghetti with sauce (45 g CHO), ½ cup broccoli (4 g CHO), and ½ piece of garlic bread (12)
- Totals (277 g CHO)
SLIDE 8: Proteins are important for maintaining your muscle mass as well as for maintaining healthy hair and nails. You can get protein from meat, fish, dairy, beans and nuts. Proteins take longer to digest, therefore, eating meals with protein in them will make you feel fuller longer. If you do not consume enough protein, recovery from injuries and muscle soreness can become major problems. Also, your muscle strength will greatly decline.
SLIDE 9:
How can you find out how much protein you need? Well, there is a simple formula:
Take your own body weight and multiply it by the number 0.8. This will give you the grams of protein you should eat in one day.
For example let’s say we have a female dancer, 16 years old,
who weighs 120 pounds. To find the amount of protein she needs to eat each day we take:
Her weight of 120 pounds x 0.8 to get 96 grams of protein that she should eat daily. (see here again we are measuring protein in grams, just like we did with carbohydrates).
For protein sources, this dancer could eat:
- One bagel with one tablespoon of peanut butter (14 g protein) and ½ cup milk (4 g protein)
- A tuna fish sandwich (22g protein) with ½ cup cottage cheese (14 g protein)
Show calculations while speaking through this Show pictures of meat, dairy, beans, nuts Show calculations 120lb x 0.8 = 96 grams protein Show nutrition label with protein circled Show list of food with protein content

110
- A Cliff bar (12 gram protein)
- And, a chicken breast the size of a deck of cards (26 g protein) with a baked potato (4 g protein)
SLIDE 10: Fats act to protect organs from injury, and are vital for healthy skin, reproductive, brain, and nerve function. Fats also help you feel fuller longer after eating. Eating fat is an important part of your diet. Healthy fats come from foods such as, avocados, nuts, fatty fish, and oils (like olive oil and vegetable oil). These types of fats contain many helpful nutrients including vitamins. If fat intake is too low, your energy level will drop and you may not grow properly. SLIDE 11: Many people avoid eating fat as they think it will cause them to become overweight, however healthy fats are an important part of a good diet. It is true that some high-fat foods are not full of good nutrients, for example French fries and potato chips contain the less healthy types of fat.
SLIDE 12: So, how much fat should you eat in one day? Again let’s say you are eating about 2200 calories each day. About one third of these calories should come from fat. This would be about 660 calories or 73 grams. To calculate the number of grams, divide calories by 9.
Here is what a dancer could eat for healthy fat sources to reach 73 grams:
- One whole egg cooked with olive oil (about 10 g fat)
- 10 almonds (6 g fat)
- 4 walnuts (6g fat)
- Salad topped with 1/3 avocado and olive oil/vinegar dressing (15 g fat)
Show nutrition label with fat circled
Show avocado, nuts, salmon, bottle of olive oil
Show “good fat” items
from above to French fries and potato chips
Show food label with sat/trans fat circled “unhealthy”
Show calculations:
2200/3 =660 calories 660/9 = 73 gram fat
Show list of foods with fat content

111
- A low fat yogurt with ½ cup trail mix (19 g fat)
- A piece of Salmon the size of a deck of cards (7g fat)
- One cup of low fat milk (2.5 g fat)
- 2 squares of dark chocolate (8 g fat)
If you ate these foods, your fat intake would be 73.5 g.
SLIDE 13: If you are consuming too few carbohydrates, proteins, or fats you may experience a decrease in skills or difficulty in performing skills that you may usually be able to do. This can be detrimental to your dance training and performance.
SLIDE 14:
Now we will discuss a few key vitamins and minerals that are important to the health of dancers. Vitamins and mineralsthemselves do not provide your body with energy, only carbohydrates, fats, and proteins can do that. But, vitamins and minerals are important for many other body functions.
SLIDE 15:
1. Vitamin D is important to dancers because along with many other health benefits (perhaps preventing some cancers) it supports good bone health. Vitamin D comes from two sources: Sunlight and your diet. Spending time in the sun allows your body to make vitamin D. Also, drinking milk and eating fish like Cod, salmon, and tuna can increase your levels of vitamin D. Eggs also contain vitamin D, but you have to be sure to eat the whole egg, because the vitamin is found in the orange-colored yolk.
SLIDE 16:
2. Vitamin C is important for helping you fight colds and other illnesses. Because dancers are working so hard training every day, maintaining a strong immune system is essential for staying healthy throughout the year. Vitamin C comes
Show in text to emphasize point
Picture of sun, fish, egg
Picture of oranges, grapefruits, strawberries, broccoli, peppers

112
from your diet and can be found in citrus fruits like oranges, grapefruits, and strawberries, and also in vegetables like broccoli and bell peppers.
SLIDE 17:
3. Calcium is a mineral that is essential to the health of dancers. Adequate calcium intake can help prevent the development of osteoporosis (fragile bones). Vitamin D and calcium work together to help proper bone growth. In order to absorb calcium, vitamin D is needed. Without vitamin D, your body cannot use the calcium you eat. Calcium comes from your diet and is found in dairy products like milk, yogurt, cheese, and ice cream and also in some vegetables like kale, asparagus, and cabbage. If you can’t tolerate dairy
products, some foods are fortified with calcium, such as orange juice.
SLIDE 18:
4. Iron is the last mineral we will discuss today. Iron helps carry oxygen in your blood. It is important for athletes who need to bring oxygen to their working muscles. Many athletes are low in iron which can lead to a condition called anemia. Anemia causes people to be very tired, weak, pale, and bruise easily. Young female athletes and vegans (people who do not eat meat, fish, or dairy) often have low levels of iron. Iron can be found in red meat, turkey, oysters, spinach, beans, and fortified cereals.
SLIDE 19:
Take a few minutes to look over your handout entitled “Foods
and their Benefits”. Pay attention to the types of food and
what nutrients they provide.
We will end today’s class by discussing some foods for health:
SLIDE 20: 1. Remember you need Vitamin D to absorb calcium. Spend some time in the sun and add fish to your diet.
Pictures of milk, yogurt, cheese and vitamin D
Picture/display red meat, spinach, beans

113
You need to eat about 5µg of vitamin D each day. You could get this by spending about 5 - 10 minutes in the sun without sun screen 3 times weekly if you are light-skinned. If you are darker-skinned increase it to 10-15 minutes. Or you could eat 3 ounces of grilled salmon (the size of a checkbook) which would give you more than enough vitamin D for the entire day.
SLIDE 21:
2. Vitamin C is important for helping you fight illnesses especially when you are dancing a lot.
You need to eat 45 mg per day of vitamin C if you are aged 9 to 13 years old. If you are 14 to 18 years old and a boy, you should eat 75 mg per day and if you are a girl in this age group, 65 mg per day. Take a look at this chart:
So, a boy or girl 9 to 13 years old could drink ½ cup of orange juice, or eat ½ cup of strawberries.
A boy 14-18 years old could eat one large grapefruit. And a girl of the same age, a medium orange.
SLIDE 22:
3. Again Calcium is important to the dancer’s diet. Try to
add low fat dairy products like yogurt and cheese to your diet. It is always best to obtain nutrients from foods rather than vitamins and minerals. Many vitamin and mineral supplements are not easily digested and absorbed in your body. If you have problems eating enough dairy foods, you should ask your doctor or a registered dietitian about vitamin and/or mineral supplements.
SLIDE 23: You should aim to eat about 1300 mg of calcium per day. Here is what you could eat to get this much calcium:
1. One cup of milk (300mg)
2. One cup of broccoli (90mg)
Picture of sun, and three ounces of salmon Chart: see attached at end of lecture Show foods and chart on slide Show list of food with calcium contents, and pictures of some items

114
3. A container of yogurt (300mg)
4. A cup of fortified orange juice (300mg)
5. A small frozen yogurt (110mg)
6. And a piece of cheese (200mg)
If you ate all of this you would have eaten 1300 mg of calcium.
SLIDE 24:
4. And, do you remember what Iron does for the body? Iron helps carry oxygen in your blood to your working muscles.
If you are a boy or girl aged 9-13 years old you need to eat 8 mg of Iron each day. If you are 14-18 years old and a boy, you should eat 11 mg per day and a girl of this age should eat even more, like 15 mg per day. Take a look at this chart:
SLIDE 25:
It’s important to note that food sources of nutrients are the
best. Sometimes vitamin supplements do not digest and/or absorb fully. To be sure your body is actually getting the vitamins, be sure to eat them through foods in your diet.
SLIDE 26:
In summary today you have learned:
That a calorie is a unit of measurement for energy and, therefore, the amount of food you eat. Active young women need a minimum of 2000-2500 calories per day, and active men of the same age need a minimum of 2500-3300 calories per day.
SLIDE 27:
The three primary nutrients in food are Carbohydrates, Proteins, and Fats. Carbohydrate is the major source of fuel and energy for your body. Proteins are important for maintaining your muscle mass and strength. Fats protect your organs and are essential for
Chart: see attached at end of lecture Show one item for each nutrient from earlier in lecture

115
healthy skin, and proper nerve, brain, and reproductive function.
SLIDE 28:
And, Vitamin D comes from the sun and works with Calcium to make your bones strong. Vitamin C is found in citrus fruits and helps you fight colds. Calcium comes from dairy foods and is essential for strong bones and preventing stress fractures. Iron is found in red meat, beans and spinach and carries oxygen to your working muscles. And, Anemia is a condition that effects athletes with a low iron intake and can make you very weak, pale, and tired.
SLIDE 29:
In the final class you will learn:
-how to eat for optimal performance, how to maintain hydration, and will be given examples of meals and snacks specifically useful to ballet dancers. SLIDE 30: “Dancing is a sweat job.”- Fred Astaire
Show one item for each nutrient from earlier in lecture
Happy dancer photo

116
Class Two Charts: See slides 21 and 24 Vitamin C- Recommended Amounts and Food Sources
Sex Age (year) Amount Vitamin C What to eat to get this amount
Male 9-13 45 mg/day About ½ cup of Orange Juice
Female 9-13 45 mg/day About ½ cup of Strawberries
Male 14-18 75 mg/day One Large Grapefruit
Female 14-18 65 mg/day One Medium Orange
Iron-Recommended Amounts and Food Sources
Sex Age (year) Amount Iron What to eat to get this amount
Male 9-13 8 mg/day One packet of Instant oatmeal [8mg]
Female 9-13 8 mg/day One bowl of lentil soup
[4 mg]
+
One bowl of cheerios [4.5 mg]
Male 14-18 11 mg/day One hamburger patty ( the size of a deck of cards) [2.5 mg]
+
One a bowl of cheerios [4.5 mg]

117
+
One bowl of Split Pea Soup [4 mg]
Female 14-18 15 mg/day ½ packet of Instant Oatmeal [4 mg]
+
One bowl of lentil soup [4mg]
+
½ cup of Total cereal
[6 mg]

118
Class Three: Eating for Optimal Health and Performance
SLIDE 1:
Welcome the third and final class: eating for optimal health and performance After listening to this presentation, you should
Be able to name at least five healthy habits dancers should aim for
Understand the importance of drinking water and staying hydrated and how to monitor your hydration status (“WUT”)
Be able to give an example of a dinner that should be eaten the evening before a performance
SLIDE 2: As you may know from personal experience and have learned from the first class of this program, injury is common among dancers. Dancers like yourselves train intensely and place demands on your bodies that not many people outside of the “ballet world” understand. You are a unique population of athletes and need to care for your bodies so you can train and perform at your highest abilities. Proper technique, resting when appropriate, being able to cope with stress, and eating right can help you achieve your goals.
SLIDE 3: We are going to begin today’s class by discussing 10 healthy goals for dancers to aim for. Sometimes it’s difficult to make
a lot of changes at one time, so try to pick two or three of these goals to master during this summer intensive program. Once you get home try to pick up a few more. This way you will be on the right path to achieving good health.
SLIDE 4:
1- Eat breakfast every day: Everyone here should begin their day with a healthy breakfast. Individuals who eat breakfast have healthier body weight, an increased metabolism, and suffer less illness. If you are someone who doesn’t like eating a lot in the morning, try something small like a yogurt and/or apple. Ideally, you should eat some source of carbohydrates
Display Objectives Picture from Oregon Ballet Theatre
Show picture of example breakfast

119
like cereal, oatmeal or fruit, some fat and protein from yogurt or milk, or maybe an egg.
SLIDE 5:
2-Add fish and omega-3 fatty acids to your diet: Omega-3 fatty acids decrease inflammation and are good for your heart and blood vessels. Try to eat salmon, halibut, and/or walnuts once or twice a week. These foods also provide other important nutrients that we’ve mentioned such as vitamin D and calcium.
SLIDE 6:
3- Eat a diet high in vegetables, fruit, whole grains, lean meat, and low fat dairy foods: A balanced diet is great for a dancer. If at each meal you have a variety of colors on your plate, you are on your way to eating a balanced diet.
Let’s go over the amount of each of these foods that you should aim for eating in a day:
SLIDE 7:
Grains- You should try to eat about 6-11 servings of grains each day. Grains are found in foods like pasta, cereal, bread, and rice. Whole grains are the best sources of grain. You can tell if something is made from whole grains if it is marked with this symbol (show whole grain stamp) or if you search the ingredient list and make sure the first word is “whole” like
“whole wheat”. An example of one serving of whole grains is
½ cup of cooked oatmeal or ½ cup of whole wheat pasta.
SLIDE 8:
Vegetables- you should try to eat about 3-5 servings (equal to about 2.5 cups) of vegetables every day. Try to choose colorful vegetables because they are high in many nutrients. Examples of one vegetable serving includes ½ of a sweet potato or 10 baby carrots.
SLIDE 9:
Fruits- You should try to eat about 2-3 servings (1.5 cups) of fruit each day. Try to eat the actual fruit rather than drinking
Show picture of salmon from lecture two
Show balanced, colorful meal versus “brown” meal
Show whole grain stamp
Show list of examples, with pictures
Show items: sweet potato, carrots, broccoli
Show fruit pictures

120
it in its juice form since you’ll get more fiber from whole, fresh fruit. Examples of one fruit serving includes one banana, or one apple, or 15 grapes.
SLIDE 10:
As for “junk foods” we usually eat these because they taste
good. They are okay to eat every once in a while, but do not provide your body with the nutrients it needs for optimal performance.
SLIDE 11:
4-Choose lower fat varieties of dairy foods such as milk, yogurt, and cheeses: Dairy foods are very important for dancers. Remember why? From the second class you learned that dairy foods provide calcium which helps your body build strong bones, and many people do not consume adequate amounts of calcium in their diets. Aim for three servings of low fat dairy per day. An example of one serving would be one cup of milk or one cup of yogurt. If you are allergic or intolerant to dairy foods, ask your doctor or a registered dietitian for advice on other non-dairy sources of calcium.
SLIDE 12:
5-Limit your intake of unhealthy fast food: Sometimes fast food is the only option, but you can still make healthy food choices even when eating at a fast food restaurant. Try choosing healthy options like salads with low fat dressings, or grilled chicken rather than fried, bean or chicken burritos, fruit and yogurt cups, or even sushi!
SIDE 13:
6- Eat regularly scheduled meals: Dancers use a lot of energy during the day. To keep your body fueled and your metabolism up eat small meals throughout the day. Rather than eating three huge meals, try eating small meals every three hours.
Pictures of chips, soda, candy bars
Show picture of three servings from lecture two
Show pictures of health fast food options
Show clock with three hour time intervals

121
SLIDE 14:
7-Drink adequate amounts of water: Water is the most essential nutrient to humans and composes more than 50% of the human body. We cannot live over one week without water. If athletes do not consume enough water, their performance suffers. Dancers should drink water before, during, and after classes, rehearsals, and performances. We will discuss more about water later in this lecture, and you can learn how to tell if you are drinking enough.
SLIDE 15:
8-Get enough sleep: Doctors recommend people to sleep eight hours each night. Athletes need to get even more than this! You should try for nine to ten hours. Sleep effects your mental alertness and your day’s performance so be sure to get
to bed early enough to get these hours in!
SLIDE 16:
9-Cross train to prevent injury. All dancers should consider cross training. Cross training is exercising in different ways to improve overall performance. Good sources of exercise for dancers include cycling, swimming, lifting weights, jogging, yoga, and Pilates. These exercises strengthen muscles that aren’t used much in your dance training. To make your body balanced and prevent injuries, participate in some different exercises occasionally.
SLIDE 17:
10-Have Fun! Be sure to enjoy yourself and take good care of your body- dancing is a wonderful form of sport and art. You are lucky to have the skills and opportunity to be here today.
SLIDE 18:
Hydration-
Now we are going to focus our attention on Healthy Habit #7-drinking enough water. Water needs vary depending upon how much you sweat, your body size, the climate you live in,
Picture of re-usable water bottle
Picture of sleeping adolescent
Picture of cycling bike, Pilates mat, running shoes, free weights
Picture of adolescent dancer

122
and how much exercise you do. A common recommendation is to aim for drinking at least eight cups of water per day.
Researchers know that performance is optimal when athletes maintain fluid balance, or in other words, stay hydrated. If you do not drink water throughout the day, especially when you are training you will become dehydrated (this happens when there is not enough water in your body). When this happens, your performance level will decrease and you may develop muscle cramps or become dizzy or nauseous. Dehydration also increases your risk for serious life-threatening injuries like heat stroke.
SLIDE 19:
Here are some tips about staying hydrated:
1. Drink water when you wake up. Try for two cups.
2. Drink water before your first class or rehearsal.
3. Try to take sips of water throughout class, rehearsal, and especially during performances, at least every 20 minutes.
4. Drink at least two to three cups of fluid after rehearsal and performance to replace fluid loss through sweat. This is especially important if it’s hot in the studio or theatre.
5. If you wait until you’re thirsty to drink, you are already dehydrated!
6. If you are only dancing for one to two hours, drinking just water is fine. If you are dancing intensely for more than one to two hours, you could mix sports drinks like Gatorade with your water. Sports drinks have important minerals in them to help hydrate you and may help prevent muscle cramps.
SLIDE 20:
You can monitor your own day to day hydration status by remembering the acronym “WUT”
“W” stands for weight. If you lose more than 1 pound in one day this is from water loss and is a sign of dehydration.
Display tips
Display acronym with definition

123
“U” stands for urine. If you are well-hydrated, you should go to the bathroom often and have pale or colorless urine, like the color of lemonade. If you are dehydrated, less urine will be produced and it will be darker in color, and stronger smelling.
“T” stands for Thirst. If you are thirsty you are probably
already dehydrated and you need to drink!
If you have two of these markers, it’s likely you are
dehydrated. If you have three, it is very likely!
Remember, keeping your body hydrated is essential for being a successful dancer. Always carry a refillable water bottle with you, so that you can drink frequently.
SLIDE 21:
When and what to eat
What and when you eat is also important to your performance. Does anyone here think about what they eat for dinner the evening before a performance? What about breakfast the day of the performance? If you do, you are on the right track to optimizing your performance. If not, it’s
time to start!
SLIDE 22:
1. The evening of-
What you eat the evening before a performance, a dress rehearsal, or a long day of training will determine your energy levels for the next day. As you learned in class two, carbohydrates are the primary sources of fuel for your body. So, these dinners should consist of healthy carbohydrates, such as fruits, vegetables, and whole grains like we discussed earlier.
Choose a meal high in complex carbohydrate to optimize energy storage. This way you’ll have fuel stored in your
muscles for the next day’s dancing.
Here is an example of how to prepare an appropriate dinner.
Show lemonade
MEAL PREPARATION VIDEO CLIP: Show potatoes, whole grain bread, brown rice with salmon/chicken, broccoli, milk in clip

124
SLIDE 23:
Here are some more examples: Please refer to your handout to follow along
1: Spaghetti with low fat meat sauce, whole wheat bread, steamed broccoli, and low fat milk 2: Turkey and cheese sandwich on whole wheat bread, vegetable soup, low fat milk, and a piece of fruit 3: Grilled chicken breast (without skin) with a baked potato, green beans, applesauce, and some low-fat milk 4: Fish or tofu with brown rice, vegetables, and orange juice or low fat milk These are some examples of dinners that will prepare your body for the next day. SLIDE 24: 2. Breakfast
Breakfast is important for beginning every day, especially prior to a performance, dress rehearsal, or long training day. Again you want to include carbohydrates for energy, but also protein for your muscles, and fat to help you stay full longer. SLIDE 25: Here are some examples: 1: Oatmeal with blueberries, low fat milk and/or orange juice, and yogurt 2: Whole wheat bagel with peanut butter, an orange, and apple juice or low fat milk 3: Scrambled eggs with whole wheat bread, a banana, and orange juice or low fat milk SLIDE 26: 3- Snacks between shows and hours rehearsing to be eaten
throughout the day
Show example breakfast

125
Throughout a day of dancing you need to keep your body fueled with small, healthy snacks. Also, if you have more than one performance during one day, you need to eat between them to have energy to perform well in the evening. Choose a snack that has carbohydrates, protein, and is low in fat. Here are some examples: Cereal bar, apple with peanut butter, fig bars, string cheese, bananas, grapes, oranges, yogurt, soy nuts, a turkey sandwich on whole wheat bread And finally, after that long day of dancing remember to refuel, rest, and relax! Eating after a performance is crucial for recovery, particularly when you are performing for many days in a row. Also, remember to drink plenty of water. SLIDE 27:
Today you have learned a lot of important information. Let’s summarize some key points here:
Now you know some healthy habits you can try to include in your daily routine. Here they are again: eat breakfast every day, add fish and/or omega-3 fatty acids to your diet, eat a balanced diet, choose lower fat varieties of dairy food, limit your intake of unhealthy fast food items, eat regularly scheduled meals, drink adequate amounts of water, get enough sleep, cross train, and have fun!
SLIDE 28:
Now you understand that drinking fluids and staying hydrated is important to your performance. Remember that if you are thirsty you are already dehydrated! And you can monitor your own status by “WUT” Weight (one pound per day is water weight that needs to be replenished), urine (dark color equals dehydration), and thirst. Remember to try to mix sports drinks with your water if dancing intensely for more than one to two hours.
Show pictures of appropriate foods

126
SLIDE 29:
And finally: you were given some examples of meals to eat at specific times during the day. Remember your evening meals before a performance, dress rehearsal, or long day training should consist of good quality carbohydrates such as fruits, vegetables, and whole grains to fuel your muscles for the next day’s
work!
SLIDE 30:
“Set yourself up for success and anything is possible."
Show “healthy habits” in
bullet points to follow voice
Picture of adolescent dancer to older dancer

Healthy Behaviors and the Female Athlete Triad:
Being the Best You Can Be! Class One
Consuming high-quality foods like fruits, vegetables, whole grains, and lean meats will provide your body with the huge amount of energy required by the physical demands of ballet. In addition, eating a variety of these foods regularly will provide essential nutrients to prevent injury, prevent the risks of the female athlete triad, and keep you performing at your best!
Do I need to worry about energy demands?
Yes! Ballet is one of the most physically and mentally challenging sports, and has even been compared to football. It uses both aerobic and anaerobic pathways to provide energy to your
muscles.
Aerobic exercise requires oxygen and is endurance exercise
Anaerobic exercise doesn’t require constant oxygen and is shorter, high intensity exercise
In ballets like Swan Lake, the corps uses aerobic pathways.
When a man lifts his partner in the air, the short burst of
energy he uses comes from anaerobic pathways.
Always dance with
proper technique.
Rest between classes &
rehearsals.
Eat a
balanced diet.
Take good
care of your body!
Get at least 8 hours of
sleep a night.
KEY POINTS
1. Amenorrhea
- you no longer have
your monthly
Period; may lead to
poor bone health/fractures
3. Low Energy
Availability - eating fewer calories than
you burn; may lead
to feeling weak, tired, unable to perform
2. Osteoporosis
- weakening of the
bones; may cause stress fractures
3 CONDITIONS CONTRIBUTE TO
THE FEMALE
ATHLETE TRIAD
Why eat healthy anyway?
Appendix M: Nutrition for Optimal Performance Handouts
127

Nutrition Principles for Dancers:
Learning the Basics Class Two
Common Questions I know I eat them, but what exactly are calories?
A calorie is a unit of measurement for energy. The amount of food you eat and
need in a day is measured in calories. How many calories do I need if I’m a female dancer?
Female dancers your age usually need to eat at least 2000 to 2500 calories
each day.
What is metabolism and how fast is mine? Metabolism is the complete set of chemical reactions that occur in cells of your
body which convert food to energy. This is the rate at which we burn or “use
up” calories. Your metabolism, or metabolic rate, is slower when you are doing
things like sitting, and faster when you are moving a lot, like dancing or running
What are the 3 macronutrients and which one should I get the most of? The three macronutrients are carbohydrates, protein, and lipids (or fats), and as
a dancer, about half of your calories should come from carbohydrates. These 3
macronutrients provide your body with all of its energy.
Important
Vitamins & Minerals Vitamin D – supports good bone health
Sources: salmon, tuna, eggs, or even just 15
minutes/week in the sun without sunscreen!
Vitamin C – helps you fight colds and illness
Sources: oranges, strawberries, or broccoli
Calcium –with the help of vitamin D it aids in
bone health
Sources: milk, yogurt, cheese, or ice cream
Iron – carries oxygen in your blood; without it,
you could develop anemia (muscle weakness,
feeling tired and bruising easily)
Sources: red meat, turkey, or spinach
FUNCTIONS OF THE 3 MACRONUTRIENTS
CARBOHYDRATES Supply most of the energy your
body needs for dancing; you also
get fiber from carbohydrates.
Sources: whole grains, vegetables,
or fruits
PROTEIN Helps maintain your muscle mass
and keeps your hair and nails
healthy.
Sources: lean meat, fish, or beans
FAT Protects your organs from injury
and helps you have healthy skin; it
also aids in reproductive, nerve,
and brain function.
Sources: nuts, fish, or oils
128

FO
OD
S A
ND
TH
EIR
NU
TRIT
ION
AL
BEN
EFI
TS
Typ
e o
f Fo
od
N
utr
ien
ts P
rovid
ed
B
en
efits
Wh
ole
Gra
ins
(bre
ad
s, c
ere
als
, ric
e,
pa
sta
)
Co
mp
lex c
arb
oh
yd
rate
s, f
ibe
r, B
vita
min
s, ir
on
, sm
all
am
ou
nt
of
pro
tein
Imm
ed
iate
en
erg
y,
bo
we
l re
gu
larity
,
en
erg
y f
or
exe
rcis
ing
mu
scle
s
Ve
ge
tab
les
(de
pe
nd
s o
n t
he
ir c
olo
r)
*All v
eg
eta
ble
s h
av
e fib
er*
1. Y
ello
w a
nd
Ora
ng
e (
Sq
ua
sh, C
arr
ot)
Vita
min
A, b
eta
ca
rote
ne
, vita
min
C
2. G
ree
n (
Sp
ina
ch
, G
ree
n p
ep
pe
r)
Vita
min
A, v
ita
min
C,
iro
n, so
me
ha
ve
ca
lciu
m
3. R
ed
(To
ma
to, R
ed
pe
pp
er)
Vita
min
A, ly
co
pe
ne
, v
ita
min
C
4.
Wh
ite
(P
ota
to, C
au
liflo
we
r)
Hig
h c
arb
oh
yd
rate
s, p
ota
ssiu
m
1. Y
ello
w a
nd
Ora
ng
e
Go
od
skin
, h
air, n
ails
, v
isio
n, m
ay
pre
ve
nt
som
e c
an
ce
rs
2. G
ree
n
He
alth
y g
um
s a
nd
imm
un
e s
yst
em
fun
ctio
n
3. R
ed
Ma
y lo
we
r risk
s o
f d
eve
lop
ing
ma
ny
typ
es
of
ca
nc
er
4.
Wh
ite
Qu
ick e
ne
rgy a
nd
mu
scu
lar
fun
ctio
n
Fru
its
*Mo
st f
ruits
ha
ve
fib
er*
V
ita
min
A, v
ita
min
C, p
ota
ssiu
m,
low
in f
at,
hig
h in
fib
er
Qu
ick e
ne
rgy, h
elp
ma
inta
in b
od
y
flu
ids
an
d e
lec
tro
lyte
ba
lan
ce
, b
ow
el
reg
ula
rity
Da
iry
(milk
, c
he
ese
, ic
e c
rea
m, y
og
urt
)
Pro
tein
, c
alc
ium
, p
ho
sph
oru
s,
vita
min
s A
, D
, a
nd
rib
ofla
vin
(B
vita
min
)
Bo
ne
/ske
leta
l d
eve
lop
me
nt,
lo
we
r risk
for
ost
eo
po
rosi
s a
nd
str
ess
fra
ctu
res,
he
alth
y s
kin
, n
ails
, a
nd
ha
ir
Pro
tein
(me
at,
fis
h, p
ou
ltry
, e
gg
s, b
ea
ns,
soy
, n
uts
)
Pro
tein
, iro
n, B
vita
min
s, a
nd
fa
t
Mu
scle
de
ve
lop
me
nt
an
d
ma
inte
na
nc
e, so
urc
es
of
iro
n t
o h
elp
ca
rry o
xyg
en
th
rou
gh
blo
od
fo
r u
se b
y
ce
lls a
nd
mu
scle
s
Fats
(ve
ge
tab
le o
ils,
nu
ts,
ma
rga
rin
e,
av
oc
ad
os)
Ess
en
tia
l fo
r g
oo
d h
ea
lth
, O
me
ga
-3
fatt
y a
cid
s, a
nd
mo
no
-
po
lyu
nsa
tura
ted
fa
ts
Gro
wth
an
d b
od
y d
eve
lop
me
nt,
he
alth
y s
kin
, d
ec
rea
se in
fla
mm
atio
n,
inc
rea
se h
ea
ling
pro
ce
sse
s
129

About how many calories should you eat in a day, if you are a dancer aged 13-18? Circle the correct choices.
Male: 1200-1600 Male: 2500-3300 Female: 800-1200 Female: 2000 – 2200
Look at the food pictures below, and:
Draw a X around the food item highest in unhealthy fat
Draw an through the food item highest in carbohydrates
Draw a around the food item highest in protein
Look at the pie chart below which represents the percent of each macronutrient you should consume in one day.
Shade in the section representing carbohydrates
With lines, color in the section representing fat
With dots, color in the section representing protein
Macronutrient Percentages
Class Two Worksheet: Application of Nutrition Principles
130

Match the correct vitamin or mineral to its food source below:
1. Cod (fish), eggs, the sun ______
2. Strawberries, bell peppers, oranges, broccoli ______
3. Red meat, spinach, beans, fortified cereals ______
4. Cheese, yogurt, milk, asparagus ______
In the space below, write a menu for a healthy breakfast that you might eat the day of a performance. Make sure your meal includes protein, carbohydrates, and fat.
Your Breakfast Menu:
Item #1____________________________
Item #2____________________________
Item #3____________________________
Item #4____________________________
Word Bank
A = Iron
B = Calcium
C = Vitamin C
D = Vitamin D
131

2. For breakfast… Include carbohydrates for energy,
protein for your muscles, and fat to
keep you feeling satisfied.
Examples:
- Oatmeal with blueberries,
yogurt, low fat milk and/or
orange juice
- Scrambled eggs with whole
wheat bread, a banana, and
orange juice or low fat milk
3. Snacks for during the day… Choose a snack with carbohydrates,
protein, and low in fat to keep your
energy up between classes/rehearsals.
Examples:
- Cereal bar
- Apple with peanut butter
- String cheese
WHEN and
WHAT to
eat
Eating for Optimal Health and Performance:
What Should I Eat? Class Three
STAYING HYDRATED
“W” = weight. If you lose more than 1 pound in one day this is from water loss,
a sign of dehydration.
“U” = urine. If you are well-hydrated, you should have pale or colorless urine. If
you are dehydrated, your urine will be darker in color, and stronger smelling.
“T” = thirst. If you are thirsty you are probably already dehydrated!
*2 or more of these symptoms means you are probably dehydrated!*
5 TIPS FOR DRINKING MORE WATER
1. Aim for 2 cups when you wake up.
2. Grab some before class or rehearsal.
3. Take sips throughout class or rehearsal, at least every 20 minutes.
4. Aim for 2-3 cups after class or rehearsal, even more if it’s hot.
5. If you are dancing intensely, you could mix sports drinks with your water.
What to Aim for Daily: Grains 6-11 servings
Vegetables 3-5 servings
Fruits 2-3 servings
Dairy 3 servings
“Junk foods” are ok every once in a
while but try to limit them. They may
not provide you with all the nutrients
your body needs for optimal
performance.
If fast food is your only option, try the
following:
Salad with low fat dressing
Grilled chicken rather than fried
Fruit or yogurt cups
1. The evening of a performance… Eat plenty of carbohydrates from fruits, vegetables, and whole
grains.
Examples:
- Spaghetti with low fat meat sauce, whole wheat
bread, steamed broccoli, and low fat milk
- Grilled chicken breast with a baked potato, green
beans, applesauce, and low fat milk
10 Tips for
Overall Healthy Habits
1. Eat breakfast everyday.
2. Add fish to your diet to
increase omega-3 fatty
acids. Great sources are
salmon, halibut, and
walnuts.
3. Eat a wide variety of
foods for a healthy diet.
4. Aim for 3 low fat dairy
servings per day. They are a
great source of calcium!
5. Limit fast food.
6. Eat small meals
throughout the day to keep
your energy up.
7. Aim to get at least 8
hours of sleep a night.
8. Drink plenty of water.
9. Cross train: Bike, swim,
jog, do yoga or pilates to
prevent injury.
10. HAVE FUN! 132

Nutrition for Optimal Performance: The Needs of Pre-professional Adolescent Ballet
Dancers
________
Healthy Behaviors and the Female Athlete Triad: Being the Best You Can Be!
Why should I eat healthy?
High quality foods like fruits, vegetables, whole grains, and lean meats will provide your body with the huge amount of energy required by the physical demands of ballet.
Eating a variety of these healthy foods regularly will also help prevent injury and prevent you from developing the conditions that comprise the female athlete triad (discussed below).
Do I need to worry about energy demands?
YES! Ballet is extremely challenging and has even been compared to football. To be successful as a dancer, you must supply your body with the energy it needs to dance by adopting proper eating habits.
So, how many calories per day should you aim for?
Female dancers should aim for eating 2000 - 2500 calories per day
Male dancers should aim for eating 2500 - 3000 calories per day
The Female Athlete Triad: the female athlete triad has 3 components
1. Amenorrhea: when you no longer have your monthly period; this condition may cause osteoporosis.
2. Osteoporosis: the weakening of your bones; this condition can cause stress fractures.
3. Low Energy Availability: when you eat fewer calories than you burn during a day; this condition can cause both amenorrhea and osteoporosis.
KEY POINTS Eat a balanced diet.
Always dance with proper technique.
Rest between classes and rehearsals.
Get at least 8 hours of sleep a night.
Take good care of your body.
Appendix N: Nutrition for Optimal Performance Control Group Packet
133

_________
Nutrition Principles for Dancers: Learning the Basics
Calories and Energy Balance
Calorie: A unit of measurement for energy; the food you eat is measured in calories.
Female dancers usually need 2000-2500 calories/day.
Metabolism: The complete set of chemical reactions that occur in cells of your body that convert food to energy; your metabolism, or metabolic rate, is slower when you are doing things like sitting, and faster when you are doing things like running or dancing.
Macronutrients
Macronutrients are sources of calories, or energy, for your body.
There are 3 primary macronutrients:
Protein helps maintain your muscle mass and keeps your hair and
nails healthy. Food Sources: lean meat, fish, and beans
Carbohydrates provide your body with most of its energy; Some
carbohydrates also provide fiber. Food Sources: whole grains, vegetables, and fruits
Fat protects your organs from injury, helps you maintain healthy
skin, and aids in reproductive, nerve, and brain function. Food Sources: nuts, fish, and oils
Important Vitamins and Minerals Vitamin/Mineral Vitamin D Vitamin C Calcium Iron
Function Supports
bone growth with calcium
Helps you fight colds and
illnesses
Supports bone growth with the help of vitamin D
Carries oxygen to your blood; without it, you can develop anemia (symptoms
include muscle weakness and bruising easily)
Sources
Salmon, tuna, eggs, 15-20
minutes/week in the sun
without sunscreen
Oranges, strawberries,
broccoli
Milk, yogurt, cheese, ice
cream
Read meat, turkey, spinach
134

__________
Eating for Optimal Health and Performance: What Should I Eat?
When and What to Eat The evening before a performance – eat plenty of carbohydrates from fruits, vegetables, and whole grains.
Example Meal #1: Spaghetti with low fat meat sauce, whole wheat bread, steamed broccoli, and low fat milk Example Meal #2: Grilled chicken breast with a baked potato, green beans, applesauce, and low fat milk
For breakfast – include carbohydrates for energy, protein for your muscles, and healthy fat to keep you feeling satisfied.
Example Meal #1: Oatmeal with blueberries, low fat milk or orange juice, and yogurt Example Meal #2: Scrambled eggs with whole wheat bread, a banana, and low fat milk or orange juice
Snacks throughout the day – choose snacks with plenty of carbohydrates and protein that are low in fat to keep your energy up
Example Snacks: Cereal bars, apples with peanut butter, string cheese, fig bars
Staying Hydrated Remember the acronym “WUT”!
W = weight; if you lose more than one pound in one day, this may be
from water loss and is a sign of dehydration.
U = urine; if you are well-hydrated, your urine will be pale or colorless; if
you are dehydrated, your urine will be darker in color and stronger smelling.
T = thirst; if you are thirsty, you are probably dehydrated and need to
drink!
Some tips for staying hydrated: Aim for 2 cups of fluid in the morning Drink water before class or rehearsal Take sips throughout class or rehearsal, at least every 20 minutes Aim for 2-3 cups of fluid after class or rehearsal If you are dancing intensely for multiple hours, you could mix sports
drinks into your water
135

10 Tips for Optimal Health and Performance
1. Start each day with a healthy breakfast.
2. Add healthy fats to your diet, such as fish and nuts to increase your intake of Omega-3 fatty acids (examples: salmon, halibut, and walnuts).
3. Eat a wide variety of foods; variety is the key to a healthy diet.
4. Aim for 3 low fat dairy servings per day; they are a great source of calcium.
5. Limit your intake of “fast food”; fast foods may not provide your body with the proper nutrients it needs to perform at its best.
6. Eat small meals throughout the day to keep your energy level up.
7. Aim to get 9 or 10 hours of sleep a night; 8 hours should be the minimum!
8. Drink plenty of water.
9. Cross train: bike, swim, jog, or try yoga and/or Pilates; this is a great way to prevent injury and keep the muscles you don’t use as often in shape.
10. HAVE FUN!
136