Embed Size (px)
Citation preview

THE SUPPLY CHAIN EXECUTIVE’S ROLE IN
MANAGING RISING PHARMACY EXPENSE
Marv Feldman, MS, RPh
Pharmacy Executive, Retired
OBJECTIVES
Overview the current trends in pharmacy supply expense with a focus on
the health-system environment (acute care and ambulatory clinics)
Discuss many of the contributing factors for this change including drug
pricing, medication utilization and availability of new products
Present the strategies being used to manage pharmacy supply cost
including the associated impediments to full implementation
Provide suggestions for the Supply Chain Executive to position their expertise
in helping to control overall pharmacy supply expense increase

LET’S START BY GETTING TO KNOW YOU…
How many of you work in a health-care provider setting and at an
executive level in supply chain leadership?
How many of you work in the health-care supplier industry and
have some interest in the changing pharmaceutical field?
How many of you are now (have been) close to the pharmacy
leadership in a hospital or health-system?
Who has actively participated in organized cost management?
Who here has the complete solution to rising drug expense?

Hospital formularies are open and getting more lax
Closing an “open formulary” will save significant dollars
Prescriptive patterns cannot be changed (“black box”)
Clinicians don’t pay attention to supply cost
The most costly product always works better
There is always an alternative product
We spend more for drugs when our census rises
We spend more for drugs…so we can save more in drugs
CEO MISCONCEPTIONS ABOUT COST MANAGEMENT

Brand Interchange
Generic Interchange
Therapeutic Interchange
EDUCATE STAKEHOLDERS TO GAIN THEIR SUPPORT
Specialty Drugs
and Biosimilars

• Formulary Stages
• Non Formulary Status
• Restricted Formulary
• Prescriptive Guidelines
Launch & Acceptance
• Therapeutic Substitution
• Utilization Management
• Formulary Interchange
• Dosing and Frequency
Maturation
• Generic Substitution
• AutoSub
• Over the Counter (“OTC”)
Generics
Limited
Competition &
Minimal Discounts
if Contracted
Competition of non-chemically
equivalent drugs
Marketshare and committed
volume drive pricing Firm pricing and deep
discounting
Shortages
SAVINGS STRATEGIES MUST CONSIDER THE LIFE CYCLE

CAN UNDERSTANDING DRUG COST BE THIS SIMPLE?
PriceQuantity
UsedExtended ExpenseX
…probably not

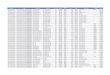
TOP 20 DRUGS BY SPEND VARIANCE (SIX HOSPITAL HEALTH SYSTEM)
EXAMPLE OF PRICE AND UTILIZATION RELATIONSHIP

Impacted by contracting (GPO, sole-source, aggregated, etc.)
Formulary considerations (preferred product, one-of-many)
Clinician preference (bias, unusual clinic/patient need)
Third party payers (restrictive and preferential coverage)
Access to specialty and limited distribution medications
Price

UNPRECEDENTED PRICE INCREASES >100% CY14/15CALCITONINSALMONSYNTHETIC VIAL MIACALCIN MIACALCIN 1255%
CEFAZOLIN SODIUM VIAL GENERIC CEFAZOLIN SODIUM 850%
MIDDRINE HCL MIDODRINE HCL 718%
HYDROCORTISONE CREAM PROCTOZONE-HC PROCTOZONE-HC 711%
AMIODARONE TABS PACERONE PACERONE 468%
ALLOPURINOL SODIUM VIAL ALOPRIM ALOPRIM 371%
PAPAVERINE HCL PAPAVERINE HCL 305%
CHLORPROMAZINE HCL TABLET CHLORPROMAZINE HCL 250%
FLUCYTOSINE GENERIC FLUCYTOSINE 248%
LEUPROLIDE ACETATE ELIGARD ELIGARD 214%
MITOMYCIN MITOMYCIN 200%
LIDOCAINE HCL SOLUTION LIDOCAINE HCL 153%
CEFEPIME HCL MAXIPIME MAXIPIME 151%
NYSTATIN NYSTOP NYSTOP 139%
TOLTERODINE TARTRATE DETROL LA DETROL LA 129%
PHYTONADIONE AMPUL VITAMIN K1 128%
NEOSTIGMINE METHYLSULFATE VIAL BLOXIVERZ BLOXIVERZ 127%
NALOXONE HCL SYRINGE NALOXONE HCL 120%
PHENOBARB/HYOSCY/ATROPINE/SCOP DONNATAL 112%
ALBENDAZOLE ALBENZA 105%
AMINOCAPROIC ACID VIAL AMINOCAPROIC ACID 100%
CEFTAROLINE FOSAMIL ACETATE TEFLARO 100%
FENOLDOPAM MESYLATE CORLOPAM CORLOPAM 100%
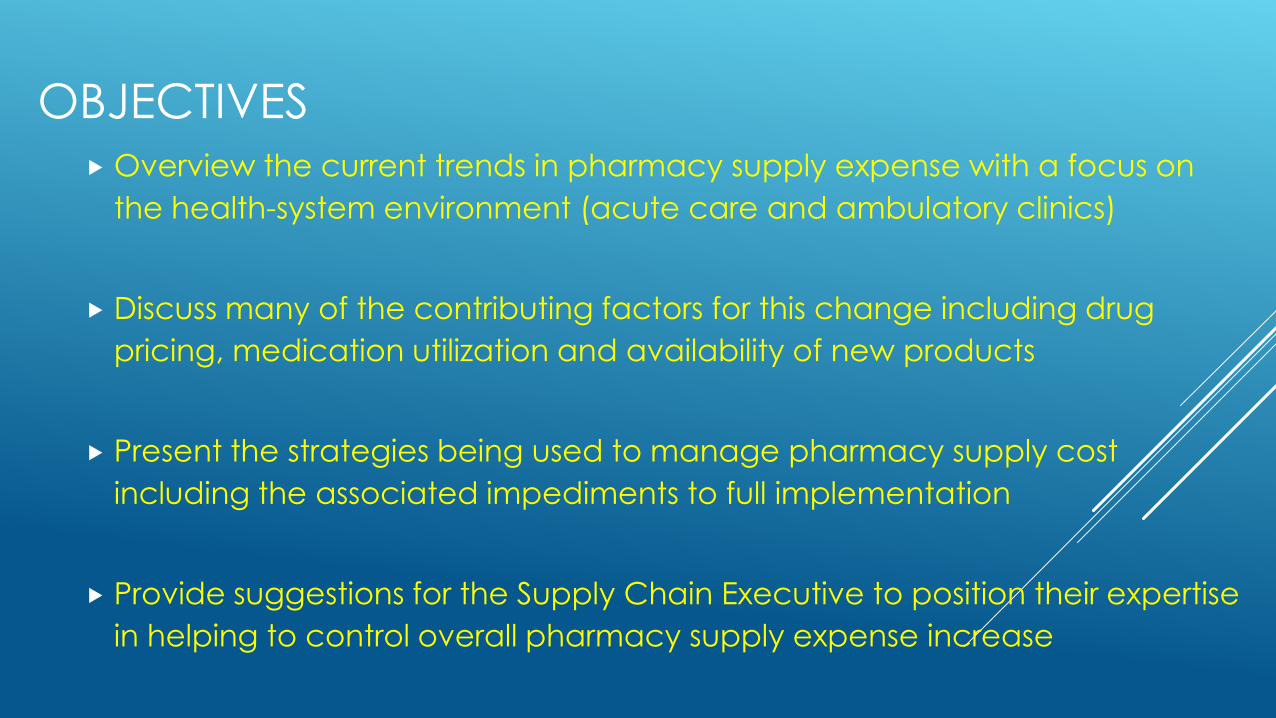
WHO WANTS TO LEARN MORE ABOUT THIS?
NEJM

Selection of most appropriate therapy (right drug therapy-right patient)
Accurate and timely comparison of the “cost to treat” (source of truth)
Drug shortages may impact selection (more expense option)
Deployment of clinical pharmacists to influence “smart shopping”
Adherence to Formulary and prescribing guidelines (evidence based)
Quantity Used

Visible Savings
Invisible Savings
Drug A costs $45 per dose. The price drops by
$5 through a new contract. Utilization remains
constant. Annualized savings (based on 1,000
doses given) total $5,000.
Pharmacy target program educates
physicians to prescribe this drug once
daily instead of twice. Consumption
then drops to 500 doses annually with
no change in price. Annualized savings
of $22,500 without any change in price.
CHANGING PRESCRIPTIVE GUIDELINE GIVES SAVINGS

WHAT ADDITIONAL SITUATIONS IMPACT YOUR COST?
Expansion of your ambulatory care foot print (oncology practices, retail)
DESI (Drug Efficacy Study Implementation) review
Drug expiry and discard (Fact or Fiction?)
Value-based Pharmaceutical Contracting
Predatory Corporate pricing (Acthar, Isoproterenol, IV Acetaminophen)
Regulatory changes (Chapter 797 and 800; 503B Compounding; 340B)
Washington DC environment and changes in ACA?

Inpatient Pharmacy Budget Drug costs are often capitated.
Focus on reducing cost.
Increase in Cost of Goods Sold is
compressing operating margin.
Overall trend has been flat lined
through recent flurry of generics.
Pharmacists impact utilization and
expense through Formulary.
Ambulatory Pharmacy Budget Drug costs are not fully capitated.
Focus on revenue margin.
Increase in Cost of Goods Sold is
likely producing revenue.
Overall trend is seeing proliferative
year over year growth.
Finance should optimize revenue
cycle processes and billing.
HEALTH SYSTEMS OPERATE TWO DIFFERENT BUSINESSES
HOW CAN THE SUPPLY CHAIN EXECUTIVE HELP?
Understand the challenges (meet regularly with Pharmacy Leadership)
Provide analytic support to compare contracts (do not usurp the process)
Empower the pharmacy to own daily on-site inventory replenishment
Enable “C-Suite” visibility for the pharmacy leader to explain expense trends
Help pharmacy document specific facts of extraordinary budget busters
Help negotiate “true business agreements” (prime vendor, capital)
Monitor and forward important articles from WSJ, Modern Healthcare, etc
ASSUME YOUR PHARMACY LEADER WON’T SEE THESE
“What is driving up my health care costs?” (WSJ July 12, 2017)
“Novartis Defends Therapy’s Price” (WSJ August 31, 2017)
“Pfizer Files Antitrust Lawsuit Against J&J” (WSJ September 21, 2017)
“This State Is Taking On Drug Makers” (WSJ September 29, 2017)
“Abb Avie, Amgen Settle Humira Patent Fight” (WSJ September 29, 2017)
“Drug Prices Expected to Rise nearly 8% Next Year” (MH July 25, 2017)
“Providers Reduce Waste to Work Around Ballooning Drug Prices” (MH Sept 11, 2017)

QUESTIONS AND CONCLUDING THOUGHTS?