Embed Size (px)
Citation preview

1
The Swan Song of the Country Doctor: Flexner and the Economics of the Practice of Medicine
Carolyn M. Moehling, Rutgers University and NBER Melissa A. Thomasson, Miami University and NBER
Jaret Treber, Kenyon College
March 2015
Abstract
During the first few decades of the twentieth century, the number of doctors setting up practice in rural areas dropped dramatically. Many contemporaries attributed this decline to Abraham Flexner's 1910 report and the accompanying reforms in medical education that resulted in many medical schools closing or merging with each other or with major research universities. Others argued that it reflected the falling income of country doctors due to increasing competition brought about by the automobile and decline in the population in rural areas. We use data from the American Medical Directories (AMD) for 1909, 1914, 1918, and 1920 to examine the location decisions of physicians and determine the factors leading to the shift of medical practice out of rural areas. We find that much of the movement out of rural areas was due to changes in where recent medical school graduates chose to set up practice. Although the rural share of all physicians in the AMD sample fell from 27 percent in 1909 to 22 percent in 1920, the rural share for recent medical school graduates fell from 29 to 15 percent over the same period. In addition, the location choices of both established and new physicians were strongly influenced by the quality of the medical schools they attended. Graduates of schools receiving favorable reviews from Flexner were about 8 percent more likely to locate in rural areas than graduates of other schools. For a subset of the AMD data, we have information on city or county of birth. These data reveal that the physicians most likely to set up practice in rural areas were those who were born in rural areas. Rural-born doctors were also less likely to attend medical schools Flexner had reviewed favorably in his report. As the lower quality schools closed or merged with more prestigious institutions, the supply of physicians to rural areas declined.
* Results are preliminary. Please do not cite without permission of the authors.

2
I. Introduction
One of the persistent characteristics of the U.S. health care system is the relative lack of
physicians in rural areas compared to urban regions, a fact that concerns policymakers who worry that
this geographic “maldistribution” limits the ability of rural people to access health care.1 (Rosenblatt
2010; Rosenblatt and Hart 2000). These concerns are not new; as early as the 1920s, alarms were being
sounded about the medical care crisis in rural America. A.F. van Bibber, M.D. offered a particularly
dramatic statement of this problem in an article published in the North American Review in 1929:
the agricultural population cannot and will not carry on without any medical care; and when the farmer quits there will ensue an epidemic disease that not even the Specialists can cope with --- Starvation (p. 94).
While rural areas and small towns were likely always underserved by physicians relative to large cities,
this gap grew substantially in the first few decades of the twentieth century. In 1924, Lewis Mayers and
Leonard Harrison used data from the American Medical Directories to examine the changing geographic
distribution of doctors between 1906 and 1923. While the nationwide population to physician ratio
increased by 13 percent (from 670 to 759) over this period, the ratio increased by 21 percent (from 775 to
939) for places with populations of 25,000 or less (Mayers and Harrison 1924: 168).
Many contemporary observers, Dr. van Bibber among them, linked the growing scarcity of
physicians in rural areas to changes in medical education that occurred during the period (van Bibber
1929: 93). The seeds of change were planted in the 1890s when some prominent medical schools raised
their admission standards, lengthened their period of instruction, and added basic science and clinical
studies to their curricula. Even though standards in medical education were improving even before 1910,
the watershed event was the publication in 1910 of Abraham Flexner’s report, Medical Education in the
United States and Canada. Flexner painted a grim picture of American medical education. He reviewed
each school, dissecting its curriculum, physical facilities, faculty, and standards of admission. His most
scathing attacks were on proprietary schools -- schools owned by the faculty and supported solely by
1 This view that the relative difference in the numbers of rural v. urban physicians reflects a “maldistribution” is not universal. For example, Newhouse et al (1982) argue that this view needs “rethinking.”

3
student fees -- some of which he accused of outright fraud (Ludmerer 1985: 167). Flexner believed that
the only acceptable type of medical school was that associated with a university and having a large, full-
time faculty engaged in research (ibid: 167).
Flexner’s report accelerated the movement towards higher admission standards and more rigorous
curricula in American medical education. The American Medical Association (AMA) added to the
momentum by incorporating some of Flexner’s criteria into its own medical school rating scheme
(Ludmerer 1985: 241). As a result, low quality and proprietary schools were driven out of the market
and the total number of medical schools in the U.S. fell from over 150 in 1900 to around 80 by 1923
(Mayers and Harrison 1924: 16). Contemporaries perceived these changes as increasing the costs of
going to medical school, thus influencing the types of people who were willing and able to enter the
medical profession, and also the locations and types of positions they were willing to accept after
graduation. Graduates of the prestigious medical schools were believed to be more likely to want to live
in large urban centers where their expected incomes would be higher and where they would have access
to hospitals and the latest medical technologies. As Dr. van Bibber argued:
It is not fair to blame the graduates of today for their choice of an urban career. Bear in mind, first, what they have invested, of time and money both, in their license to practice; second, the fact that their diminishing numbers, the populations of the cities in the mean time increasing enormously, seem to assure them all a good prospect of pleasant and profitable careers in an ideal environment, convenient to hospitals, clinics, libraries, laboratories and professional societies, with the most eminent consultants always available and the stimulating association with able colleagues. (van Bibber 1929: 93)
Raising the bar for admission to medical school was further thought to prevent the “poor boy” or “country
boy” from entering the profession, and such individuals were believed to be more willing to set up
practice in rural areas (Mayers and Harrison, 1924: 138). The historian Kenneth Ludmerer makes an even
more direct connection between medical education reform and the shrinking supply of physicians in rural
areas. He lays blame on the closing of the proprietary schools claiming that, “graduates of these schools
tended to migrate to rural areas and small towns, where there was less competition from graduates of
prestigious schools” (1985: 248-9). Ludmerer criticizes Flexner for being naïve for thinking that the

4
“graduates of strong schools would just as readily disperse to rural as to urban areas” (Ludmerer
1985: 249).
Interestingly, Mayers and Harrison came to a very different conclusion in their study of the
geographical distribution of physicians in the 1920s. They argued that the reforms of medical education
in the 1910s could have been no “more than a secondary influence in leading recent graduates to avoid
rural locations.” They observe that the even physicians who had “received their medical education under
a regime far removed from that of today” were moving away from rural areas during this period, and
conclude that the primary factors leading doctors to more urban areas were “the increasingly superior
financial, social, and professional advantages of the larger places” (1924: 149). Mayers and Harrison
argue that the growing appeal of urban areas was at least in part due to the deteriorating prospects in rural
areas. Key to this change was the advent of the automobile and the growing competition village doctors
faced from doctors in surrounding villages, towns, and even nearby cities (1924: 10-14).
Our paper examines the location choices of physicians in the first couple of decades of the
twentieth century to better understand the factors leading to the decline of the rural doctor and the
increasing urbanization of medical practice. We look in particular at whether the shifting geographic
distribution can be linked to the changes in medical education during the period. Were new graduates
more likely than more established physicians to choose large urban areas? Were graduates of stronger
programs more likely to avoid rural practice? We also consider factors that were changing the ways
physicians, both rural and urban, practiced medicine during the period: the development of road networks
and the building and expansion of hospitals. Understanding the forces driving the decline in the rural
doctor will help us assess the impact of this process on the welfare of the rural population. It may also
suggest policies that could increase the provision of physician services to rural areas.

5
II. Flexner’s Bulletin No. 4 and Changes in Medical Education
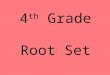
The number of medical schools increased at a rapid pace throughout the 19th century, as shown in
Figure 1. Originally, these schools had opened to supplement the apprenticeship system that produced
physicians during the colonial period, but eventually they came to supplant it. Medical schools were
inexpensive to operate, and profitable for faculty. Would-be physicians faced virtually no entrance
standards, including literacy (Ludmerer 1985: 12-13). Although states gave medical licensing powers to
state and local medical societies, they also viewed medical school diplomas to be equivalent to licenses,
and by the Civil War, most state licensing laws had been repealed or abandoned (Rothstein 1972: 108).
As the number of medical schools increased, they competed heavily for students. Competition
among medical schools led to shorter terms and more lax requirements for graduation (Rothstein 1972:
97). At the time Charles Eliot took over as President of Harvard in 1869, Harvard Medical School
admitted any fee-paying student. Only 20 percent of the students held undergraduate degrees, and one
faculty member suggested that over half the students could not write. Harvard’s curriculum consisted of
two, four-month terms of lectures. Students did not engage in laboratory or clinical work, and needed to
pass only five of nine five minute oral quizzes to pass their studies (Ludmerer 1985:49-50). Eliot
succeeded in implementing a series of reforms at the medical school, which included changes in both
administration and curriculum. The university took over the finances of the medical school, and no
longer allowed professors to divide fees among themselves. The program was extended to three years,
with nine-month terms, and the curriculum emphasized science, laboratory work, and clinical
instruction. By 1880, the University of Pennsylvania had followed Harvard’s lead, as did the University
of Michigan. Johns Hopkins opened in 1893 with the strictest requirements of all: students had to have a
bachelor’s degree, and received rigorous training in the sciences, laboratory work, and two years of
clinical instruction (Ludmerer 1985: 50-51).
Despite outright reforms at these schools, and improved curricula at others, some medical schools
were slow to upgrade their standards, if at all, partially because state licensing laws remained weak.
Most state licensing boards were ineffective; as late as 1906, 13 states granted medical licenses even to

6
nongraduates (Ludmerer 1985: 235). Thus, even by 1904, only four out of 162 schools even required two
years of college work; most required a high school diploma or less (Biennial Survey of Education, 1916-
1918: 72). In 1906, the Council on Medical Education of the American Medical Association (AMA)
conducted a survey of the nation’s medical schools. Given that its members were mainly academic
physicians, the Council used the most rigorous university model as the yardstick against which it
compared all schools. Not surprisingly, the Council drew largely the same conclusions as Abraham
Flexner ultimately would in 1910: that most medical schools did not even come close to meeting the
standards of the rigorous model (Ludmerer 1985, p. 170). Since the AMA could not be openly critical of
medical schools, it invited the Carnegie Foundation for the Advancement of Teaching – and Abraham
Flexner – to perform a similar study.
Although the 1910 publication of Abraham Flexner’s “Medical Education in the United States
and Canada” is often credited with ushering in a new era of standards in medical education, it is clear
that these changes were well underway before its publication. Nevertheless, Flexner’s report may have
accelerated the changes. The AMA incorporated Flexner’s criteria into their rating system. Schools rated
“A” were acceptable, schools rated “B” were in need of improvement, but redeemable, and schools rated
“C” were in need of complete reorganization . After 1910, state licensing boards decided whether to
recognize a school’s diploma based on its AMA rating. As early as 1914, medical schools with a “C”
rating were denied recognition in 31 states (Ludmerer 1985: 241). These changes had a pronounced
impact on where physicians earned their degrees. In 1910, just over half (54 percent) of medical school
graduates earned their degrees from schools reviewed unfavorably by Flexner; by 1920, most (88
percent) new graduates earned their degrees at reputable institutions that were rated “A” by the
American Medical Association (AMA). The question we want to examine in this paper is whether these
changes differentially led new physicians to choose to practice in urban areas over rural areas.

7
III. American Medical Directory Data
In order to examine the relationship between the changes in medical education and the geographic
distribution of physicians, we use data from the 1909, 1914, 1918, and 1920 American Medical
Directories (AMDs).2 The AMDs provide information (by location) on all practicing physicians, the
medical schools they attended, their graduation dates, and for the later years, their specialties, if any. We
supplement the AMD data with data on medical school characteristics from the Flexner report and AMA
publications. We use data from four states: California, Mississippi, New York, and North Carolina.
California and New York both contain major metropolitan areas, as well as sizable rural populations.
California is also of interest because of the high level of in-migration during this period and the dramatic
growth of Los Angeles and other metropolitan areas. Mississippi and North Carolina offer the
opportunity to look at states with predominantly rural populations. Both New York and North Carolina
are of additional interest because they had received particular attention in Mayers and Harrison’s
analysis as well: New York because the shortage of doctors in rural areas in the state had received much
public discussion and North Carolina because it had, together with South Carolina, a lower ratio of
physicians to population than any other state (Mayers and Harrison 1924: ix).
The lure to cities may have been greater for physicians than the population at large. Mayers and
Harrison (1924) note that the growth of roads and the rise of specialty practice increased incomes for
physicians in urban areas at the expense of rural practitioners:
The larger financial possibilities of the successful town practitioner have of course always been a feature in favor of town location; but the possibilities of the successful town specialist rise much higher still, creating in reality a wholly new level of medical earnings, and holding out to the rural practitioner a lure to the town far more powerful than formerly existed (Mayers and Harrison 1924: 27).
2 The AMA published the first AMD in 1906 with the subtitle, “A Register of the Legally Qualified Physicians of the United States and Canada.” The AMA compiled this first listing by consulting the records of state licensing boards, medical colleges, and medical societies. The foreword notes that the goal was to include only “legally qualified” physicians.

8
Moreover, metropolitan areas usually provided physicians with access to hospitals and laboratories,
facilities that were becoming increasingly important in medical practice, especially for more recently
trained graduates of medical school (Mayers and Harrison 1924: 32-3).
Despite the changes in medical technology that were occurring over this period, urban areas with
paved roads and social amenities attracted all types of people. To get a sense of whether urbanization
differed from the population as a whole compared to physicians, we use data from the published reports
of the U. S. Census and the IPUMS. Rather than using city size to examine population movements, we
use a county-based classification scheme based on the concept of metropolitan areas. A metropolitan area
is defined as a county or group of counties which has a large city as its economic center. We use the
IPUMS definitions of metropolitan counties in 1900, 1910 and 1920 and divide rural (non-metropolitan)
counties into those adjacent to metropolitan areas and those not adjacent to metropolitan areas.3 Besides
being more similar in spirit to the classification schemes used to examine the geographic distribution of
medical professionals today, this scheme better captures the population movements we are trying to
describe. The process of urbanization was not just about the growing numbers of people in central cities;
it was also about the growing influence of those central cities on their surrounding areas. The rapid
diffusion of automobiles and the expansion of road networks meant that a physician’s pool of potential
patients extended beyond a town’s borders.
As shown in Table 1, the U.S. population was moving out of rural areas into metropolitan areas
fairly rapidly between 1900 and 1920. In 1900, 57 percent of the population lived in rural counties not
adjacent to metropolitan areas. By 1920, that percentage had fallen to 43 percent, and almost all of that
decline was accounted for by the increase in the fraction of the population in metropolitan areas.
Professional workers were already more urban than the population at large in 1900 but they also were
3 The IPUMs defines a metropolitan area to be a county or group of contiguous counties that contained at least one city of 50,000 or more residents. For a county to be included in a metropolitan area, it had either to contain the central city or be “metropolitan in character,” meaning that it contained a sizable non-agricultural workforce.

9
moving out of rural areas at a somewhat more rapid rate; the percentage of professional workers living in
remote rural counties fell from 47 to 32 percent between 1900 and 1920 while the percentage living in
metropolitan areas increased from 41 to 55 percent.
The bottom panel of Table 1 shows the geographic distributions of physicians and surgeons and
some of the other so-called “learned professions”, dentists, and lawyers and judges. What is striking
about the data for physicians is just how rural the profession was at the turn of the century; half of all
physicians in 1900 were located in rural counties not adjacent to rural areas. Between 1900 and 1920, the
percentage of physicians living in such places, though, fell by 14 percentage points, or almost 30 percent.
Dentists and legal professionals experienced similar drops in the fraction in rural areas over this period,
but they started from much lower levels in 1900. Much more so than other professional workers,
physicians had a significant presence in rural areas at the turn of the twentieth century.
The AMD data allow us to consider how the geographic distribution of physicians varied by
where and when they went to medical school. Table 2 presents the distribution by location for our four-
state sample of AMD listings. The top panel presents the data for all physicians and the bottom panel, for
recent medical school graduates (five or fewer years since graduation). Since our sample includes New
York and California, two populous states with several large cities, it has a much higher fraction in
metropolitan areas than found in the census data. Nonetheless, the AMD data show the same overall
pattern of a movement of physicians from remote rural counties to metropolitan areas. The comparison of
the two panels, however, reveals that this movement was much more pronounced for newly minted
physicians. In 1909, about 30 percent of recent graduates had set up practice in rural counties not adjacent
to metropolitan areas, compared to only 15 percent by 1920. At the same time, the percent locating in
metropolitan areas rose from 62 to 77 percent. More recently educated physicians may have preferred
greater access to medical technologies found in hospitals in major cities.
Table 3 shows the distribution of newly minted physicians who graduated from a school receiving
a “favorable” review in Abraham Flexner’s 1910 report, compared to those who graduated from
unfavorably reviewed schools. The trend towards urbanization is clear for both groups. But, in the first

10
three years of the data, the graduates from schools that Flexner had viewed as unfavorable were about
twice as likely as graduates of favorably reviewed schools to locate in rural counties not adjacent to
metropolitan areas. This corroborates Ludmerer’s (1985) claim that graduates of less prestigious medical
schools were much more likely than graduates of other schools to locate in rural areas. By 1920, these
differences had largely dissipated, most likely because following Flexner's report, most substandard
schools either improved or closed. Supporting evidence on this comes in Panel C which shows the
distribution for graduates of medical schools with low (less than 75 percent) pass rates on state board
exams. In 1909, 67 percent of the graduates of such schools set up practice in remote rural counties.
Over the years, this fraction dropped to be in line with recent graduates from higher quality schools. But
the most notable pattern in Panel C is the precipitous drop in the number of graduates of such schools in
the sample – from 513 in 1909 to only 305 in 1920 – even as the total number of recent medical school
graduates increased. The lower quality schools were being driven out of the market, and the evidence in
Table 3 is that such schools were more likely to produce physicians willing to set up practice in rural
areas.
IV. Possible Explanations for the Urbanization of Medical Practice
The contrasts between the geographic distributions of new and established physicians and
between recent graduates of highly rated and poorly rated medical schools clearly suggest links between
the demise of the country doctor and the changes in medical education. However, the precise
mechanisms underlying these links are still unclear. Contemporary observers offered two competing, but
not mutually exclusive, explanations. The first was that the rising academic standards and tuition costs of
medical school were preventing the “country boy” from entering the profession. If country-born
physicians were more likely to set up their practices in rural areas, then as these individuals faced greater
and greater hurdles to going to medical school, the numbers of country doctors would decline. The
second explanation was that more rigorously trained doctors were more likely to be attracted to places
where there were more hospitals and laboratories and potentially larger markets for their services.

11
The AMD data do not provide data on birthplace. However, we do know whether a physician
attended medical school in a rural area. If most medical students chose schools close to home, attending a
medical school in a rural area could be a proxy for being from a rural area. Table 4 shows that between
1909 and 1920 the geographic distribution of medical schools changed very little. In both years, over 80
percent of all medical school students were in metropolitan areas. However, Table 5 shows that 12
percent of the students in schools given poor reviews by Flexner were in remote rural counties, compared
to only 5 percent of the students in favorably reviewed schools. Table 6 presents the distribution of
physicians in 1909 by the location of medical school. Almost 60 percent of the graduates of rural medical
schools set up practice in remote rural counties.
To try to tease out more from the AMD data on what was driving the urbanization of medical
practice, we estimate multinomial models of location choice. We consider how the characteristics of a
physician’s medical school, including its rating by Flexner and its geographic location, as well as his
years in practice and race affected the likelihood he located in a metropolitan area, a rural country
adjacent to a rural area, or a rural county not adjacent to a metropolitan area. Of particular interest is
whether the factors influencing the location choices of new physicians varied over time, so we also
include indicator variables for year and interact them with medical school characteristics. We also use a
subsample of the AMD data for recent medical school graduates in North Carolina in 1918 for whom we
have data on place of birth to more directly determine if rural nativity influenced location choice.
To determine what place characteristics attracted or repelled physicians choosing where to locate
their practices, we also estimate conditional logit models. In these models, we include factors thought to
influence the general population movements of the period such as the extent of the road network, as well
as factors expected to have particular influence on new physicians such as the numbers of hospital beds
and established doctors per capita. In order to further probe the hypothesis that the urbanization of
medical practice resulted from changes in medical education during the period, we also examine whether
graduates of different quality medical schools and physicians of different vintages responded differently
to location characteristics.

12
V. Multinomial Logit Models of Location Choice
Using the AMD data, we estimate multinomial logit models of location choice first for all
practicing physicians and then for recent (5 or fewer years) graduates of medical school. We include as
explanatory variables indicators for attending a medical school that received a favorable review in the
Flexner report, attending a medical school located in a rural county not adjacent to a metropolitan area,
attending a foreign medical school, and having self-reported being “colored” in the AMD. For the model
including all physicians, we include the number of years a physician had been in practice – defined as the
number of years since he had graduated from medical school – and its square. For recent graduates, we
also include an indicator for attending a school with a low pass rate (less than 75 percent) on state board
exams. We include state fixed effects to capture the persistent differences across states in the sizes of
their rural population and year effects to capture the secular decline in the rural presence of doctors
common to all states. To gauge whether the effects of medical school characteristics were changing over
time, we also estimate models interacting the medical school variables with the year effects.
Table 7 presents the marginal effects from the multinomial logit models estimated using all
physicians in the AMD sample. The largest marginal effects are for physicians who self-reported being
“colored” in the AMD listings. Such physicians were 28 percentage points more likely to have practices
in metropolitan areas and 16 and 13 percentage points less likely to be in the two categories of rural
counties. These results may speak more to the incentives of reporting one’s race in the AMD than to the
impact of race on physician location choices. In rural areas, it was likely unnecessary to report one’s race
as it was likely common knowledge among the potential patient base. However, in metropolitan areas,
physicians of color may have wanted to advertise their race to attract patients of color.
Even after controlling for years in practice and allowing for changes in location choices over
time, we still see strong differences in location choices by medical school characteristics. Graduates of
schools that received favorable ratings from Abraham Flexner in 1909 were much more likely (9
percentage points) than graduates of other schools to locate in metropolitan areas. Graduates of foreign

13
medical schools were also more likely to locate in metropolitan areas. Many of these graduates of foreign
medical schools were foreign nationals, but some were Americans who had traveled abroad to receive
more rigorous training at the European medical schools that served as the models for many of the reforms
proposed by Flexner and the AMA for American medical education. The effects of the years in practice
variables confirm what we surmised from Table 2: the draw of metropolitan areas was strongest for
younger doctors.
A particularly striking finding is that even after controlling for medical school quality as
evaluated by Flexner, graduates of medical schools located in remote rural counties were more likely to
set up practice in such counties. A straightforward interpretation of this result is that physicians preferred
to set up practice near where they went to medical school (a hypothesis we will test directly in the
conditional logit models we present later in the paper). An alternative, albeit more speculative,
interpretation is that this effect captures the “country boy” story. If attending a rural medical school is a
proxy for being from a rural area, then the greater probability of graduates of these schools of setting up
practice in rural areas can be interpreted as supporting the idea that country doctors were mostly country
boys returning home to serve their community.
The model in the right-hand panel shows that the differences in location choices by medical
school characteristics persist through the sample period. Although some of the interactions of these
characteristics with the year fixed effects are statistically different from zero, they are for the most part
small and suggest only slight narrowing of the gaps in location choices of doctors from different types of
medical schools.
The differences by years in practice, however, increased in size over the period. The preference
of more recent medical school graduates for metropolitan areas meant a growing age gap between country
and city physicians. Given the dramatic changes in medical education during this period, this growing
age gap likely meant a growing knowledge gap as well.

14
Both models in Table 7, though, reveal the strong, secular trend out of rural areas into
metropolitan areas. The year effects indicate that regardless of medical school background and years in
practice, the probability of practicing in a metropolitan area was increasing over the period.
Table 8 presents the marginal effects for the multinomial models for recent medical school
graduates. These models also reveal significant differences in location choices by medical school
characteristics. However, unlike the results for all physicians, these differences do not persist over the
sample period. The interactions between year and the indicators for attending a school Flexner rated
favorably or a school in a rural area reveal that although there were sizable differences in the location
choices of new graduates along these dimensions in 1909, these differences eroded over time. By 1920,
new graduates, regardless of where they went to medical school, were avoiding rural counties and
establishing practices in metropolitan areas.
The narrowing of the differences in location choices of recent medical school graduates most
likely reflects the convergence in medical school training during the 1910s. Schools that received
unfavorable reviews by Flexner yet remained open made drastic changes to their admission standards,
curricula, and facilities. That the graduates of such schools in 1920 made location choices similar to the
graduates of schools which had been more highly rated in 1909 indicates that the these schools now
attracted a similar pool of students and/or produced physicians with similar preferences for the amenities,
both professional and personal, afforded by metropolitan areas.
VI. Effect of Birthplace on Location Choice: North Carolina, 1918
The results from the multinomial logit estimations suggest that even when controlling for school
quality, physicians who attended a rural medical school were less likely to settle in metropolitan areas and
more likely to settle in rural areas than physicians who attended medical school in non-rural settings.
Although we hypothesize that the “rural medical school” variable captures the effect of rural nativity, we
can only speculate without more information on birthplace. We match a subsample of recent medical
school graduates from the 1918 AMD listings for North Carolina to their World War I draft cards which

15
contain their cities or counties of birth. We use this subsample of the AMD data to probe the “country
boy” story further by examining the impact of rural birth on the decision to set up a practice in a rural
area. Since North Carolina contained no metropolitan areas in this period, we use the Census definition
of rural – population less than 2,500 – for this investigation.
Table 9 provides summary statistics of recent medical school graduates residing in North
Carolina in 1918. Clearly, those born in a rural area are more likely to practice within a rural area, with 74
percent of physicians born in a rural area continuing to practice in a rural area, compared to only 24
percent of physicians who were born in an urban area in the state. Rural born physicians were far less
likely to have attended a medical school that received a favorable review from Flexner; only 28 percent of
those who were rural born attended a school that received a favorable rating, compared to 50 percent of
those who were born in an urban area. In the same vein, rural born physicians were also much more likely
to go to proprietary schools (that were typically of lower quality) than urban-born physicians; with 61
percent of rural-born doctors having attended a proprietary school compared to only 44 percent of urban-
born physicians.
In order to examine this issue more carefully, we use the North Carolina data to run a probit
model that looks at the likelihood of practicing in a rural area, controlling for rural nativity, medical
school location and quality, and whether the physician is black. These results, reported in table 10,
highlight the fact that a physician born in a rural area is 44 percent more likely to settle in a rural area
following graduation than a physician who was not, regardless of the quality of the medical school
attended. But, the results also indicate that physicians who went to a higher quality medical school (a
school with a favorable rating from Flexner) were 28 percent less likely to settle in rural areas than those
who did not, even after controlling for rural birthplace and having attended a rural medical school.4 Thus,
although these results do reinforce the fact that rural born physicians are more likely to practice in rural
4 Perhaps surprisingly, physicians who attended a rural medical school were less likely to settle in a rural area, but this probably stems from the fact that of the three medical schools in North Carolina at the time, two had favorable Flexner reviews (UNC and Wake Forest) and only the only one that did not (Leonard Medical School) was in an urban area.

16
areas, they also suggest that physicians who attended higher-rated schools were less likely to settle in
rural areas, even if they were originally born in one. Although these results are from a single year and do
not allow us to examine the impact of changing medical education over time, they suggest that if these
reforms did reduce the supply of physicians to rural areas by limiting the opportunities of the “country
boys” to attend medical school, then they did so by reducing the supply of poorly trained physicians.
VII. Conditional Logit Models for Physicians’ Location Choices
An important element of most explanations connecting the demise of the country doctor with the
medical education reforms of the 1910s is that the more science and technology based curricula – and
their much higher costs -- made doctors trained in such programs more likely to be attracted to places
with larger patient bases and more professional amenities such as hospitals and laboratories. We use
McFadden’s conditional logit model to look at the factors influencing where physicians decide to practice
(McFadden 1974). This model assumes each individual faces a set of J unordered alternatives and
chooses the alternative that provides him with the highest level of utility. We assume that the choice set
faced by a recent medical school graduate is the set of counties in the state in which he takes the medical
board examinations. In essence, this assumes a sequential decision-making process in which a physician
first chooses the state in which to locate and then at the next step, chooses the county within that state.
This assumption is necessitated by the nature of the data, but it does accord with the fact that to practice
medicine, a medical school graduate first had to be licensed, and licensing was done by the states.
We include county characteristics that likely influenced the movements of the general population
during this period such as whether the county was in a metropolitan area or adjacent to a metropolitan
area and the log of the number of miles of improved roads. The mileage in improved roads generally
excludes town and city streets and therefore captures the extent of the road network in the unincorporated,
or rural area, of a county. This measure is intended to capture differences in transportation costs across
counties, but it may also capture differences in economic activity. Recent research has found that the
agricultural productivity was increasing in the number of miles of improved roads in a county (Lee

17
2012). 5 We also include characteristics that we would expect particularly to influence physicians’
location choices: the number of hospital beds and the number of established physicians (having
graduated from medical school more than five years earlier) per 1,000 persons in the population, and the
log of the number of miles from the physician’s medical school to the county seat.
Given the findings above, we also want to examine how physicians' location choices were
influenced by the characteristics of their medical schools and years in practice. In the conditional logit
framework, the characteristics of the individual decision-maker are incorporated through interactions with
the characteristics of the elements of the choice sets. In other words, an individual trait like the type of
medical school one attended is allowed to affect the degree to which that individual is drawn to, or
repelled by, certain county characteristics. We use the measure of medical school quality used above – an
indicator for attending a medical school favorably reviewed by Flexner and, in the models for all
physicians, we also include an indicator for having been in practice ten or more years.6
We estimate conditional logit models separately by year and state. This modeling choice is
driven by the practical concern that some of the county characteristics vary dramatically across these two
dimensions. At least some of this variation is due to differences in the method of measurement, a case in
point being the improved road mileage variable. However, estimating separate models also allows us to
consider whether new physician’s location decisions varied over time and across states. North Carolina
and Mississippi contained no metropolitan areas in the sample period. By choosing to set up practice in
those states, physicians were limiting their choice set to rural counties. Since we are interested in the
decisions to choose metropolitan versus rural counties, we present only the models for New York and
California. We also limit our samples to graduates trained in American medical schools to allow us to
look at how distance from medical school affected location choices.
5 The Bureau of Public Roads conducted surveys and published data by county on total road mileage and improved road mileage county roads in 1904, 1909, and 1914. The Bureau also conducted a survey in 1921, but never published the county-level data. Lee (2012) was able to track down in the National Archives the 1921 county-level data for some states, including New York and Mississippi. We thank Dr. Lee for sharing these data with us. 6 This methodology is similar to that used by Wozniak (2010), Gottlieb and Joseph (2006), and Polsky et al. (2002).

18
Table 11 presents the estimated odds ratios from the conditional logit models for all doctors in
New York and California in 1909 and 1920. Odds ratios indicate how one-unit changes in the county
characteristics affect the odds a physician chooses to locate in a particular county. An odds ratio greater
than one indicates that an increase in that characteristic increases the probability a physician chooses a
county whereas an odds ratio less than one indicates that an increase in that characteristic decreases the
probability.
Not surprisingly, physicians were drawn to counties in metropolitan areas and, to a lesser extent,
counties adjacent to metropolitan areas. In both states, physicians had a preference of being closer to
where they went to medical school. The odds of locating in a county were decreasing as the distance
from that county to a physician’s medical school increased. For California in 1909, the mileage in
improved county roads increased the odds of a physician setting up practice there. However, for both
years, greater county road mileage reduced the odds of location choice for New York doctors. This may
reflect the differences in how the road mileage data was constructed for the different states or it may just
indicate that more mileage in county roads was a signal for being a less populous area. The models for
both states indicate agglomeration effects. New York physicians were attracted to counties with more
hospital beds per capita while California physicians were attracted to counties with more established
physicians per capita.
More significant for the research agenda of this paper, though, are the differences in the effects of
location characteristics on the location choices of doctors of different types. To interpret the impact of an
interaction term, we have to multiply the odds ratio of the interaction term with the main effect. So for
instance, the effect of being a metropolitan county on graduates of favorably reviewed schools for New
York in 1909 is 5.487*2.346= 12.873. For both states both in 1909 and 1920, physicians trained at the
higher ranked schools were more strongly drawn to metropolitan areas than graduates of other programs.
They were also more likely to choose counties with larger medical communities as represented by the
number of established doctors per capita, and were also more willing or able to move further after
graduation to set up practice.

19
Table 11 also reveals clear differences in location preferences by years in practice for physicians.
Physicians in practice 10 or more years were much less likely than their more recently minted peers to
have practices in metropolitan areas. More experienced doctors were also more likely to be in practice
further from where they went to medical school than were younger doctors.
Table 12 presents the odds ratios for the conditional logit models for recent medical school
graduates only versus the results for all physicians reported in Table 11. Once again, we observe the
strong and growing pull of metropolitan areas. By 1920, the odds a new doctor settled in a metropolitan
county rather than a remote rural county was 4 to 1 in New York and 12 to 1 in California. We also see
the evidence of agglomeration effects with the attraction of new doctors in both states to counties with
more hospital beds and in California to counties with more established doctors per capita. The interaction
terms indicate that these agglomeration effects were stronger for the graduates of the schools Flexner
rated highly. In addition, as for the results for all physicians, the graduates of more highly rated medical
schools were more likely to travel further to set up their practice.
In California, the attraction to metropolitan areas did not differ by medical school type by 1920.
These results once again suggest the growing convergence in the location choices of recent medical
school graduates. The geographic distribution of older physicians reflected strong differences in location
choices by medical school characteristics. Graduates of highly rated medical schools were drawn to
places with more hospital beds or larger medical communities and were much more likely than their
colleagues from less prestigious schools to set up practice in metropolitan areas. But the changes in
medical education led to greater uniformity in medical school admission standards and curricula and, in
the process, eroded the differences in the practice location choices for new graduates.
Interestingly, in New York, even in 1920, the graduates from the more prestigious medical
schools were more strongly attracted to metropolitan areas. This likely reflects the very strong pull in this
state of New York City and its surrounding areas.

20
VIII. Conclusions
In 1900, about half of the physicians and surgeons in the United States were located in rural
counties not adjacent to metropolitan areas. By 1920, that fraction had fallen to less than a third. The
analysis of the AMD data indicates that the changes in medical education in the wake of the Flexner
report contributed to the demise of the rural doctor. Traditionally, graduates of the weaker schools were
more likely to set up practice in rural areas and, as those schools closed or improved their standards, the
supply of physicians to rural areas fell. Attracted to the more extensive medical infrastructure of cities
and perhaps the greater income opportunities, new medical school graduates, regardless of where they
went to medical school, were increasingly likely to set up practice in metropolitan areas.
We do find some evidence supporting the idea that the physicians most likely to set up practice in
rural areas were those that were born in rural areas. However, even controlling for birthplace, we find
that physicians trained in more modern medical programs were more likely to shy away from rural
practice and locate in urban areas. These findings imply that to a great extent the doctors being “lost” to
the countryside were doctors trained in lower quality medical schools. The question is: was a doctor from
a low quality medical school better than no doctor at all? In some respects, the practice of medicine had
changed very little between the 1890s and the 1920s. General practitioners spent most of their time
seeing patients in their office or making house calls, and very little time at hospitals. Most of their patient
visits were for minor surgeries, obstetrics, and respiratory and contagious diseases (Rothstein 1987: 122).
The apprenticeship training common in the nineteenth century most likely adequately prepared doctors
for this type of practice. It may not, however, have prepared them to adapt to the changes in medical
technology that were on the horizon.

21
References
Flexner, Abraham. 1910. Medical Education in the United States and Canada. New York: Carnegie Foundation for the Advancement of Teaching.
Gottlieb, Daniel S. and George Joseph. 2006. “College-to-Work Migration of Technology Graduates and
Holders of Doctorates within the United States.” Journal of Regional Science 46 (4): 627-659. Lee, Jason. 2012. “The Road to Development: Empirical Evidence of the Effect of Roads on the U.S.
Economy, 1904-1921.” PhD. Dissertation, University of California, Davis. Ludmerer, Kenneth M. 1985. Learning to Heal: The Development of American Medical Education.
New York: Basic Books, Inc.
Mayers, Lewis and Leonard V. Harrison. 1924. The Distribution of Physicians in the United States. New York: General Education Board.
McFadden, Daniel. 1974. “Analysis of Qualitative Choice Behavior.” In Frontiers in Econometrics, ed. Paul Zarembka. New York: Academic Press.
Polsky, Daniel, Philip R. Kletke, Gregory D. Wozniak, and José J. Escarce. (2002). “Initial Practice
Locations of International Medical Graduates.” Health Services Research 37:4 (August): 907-928.
Rosenblatt, Roger A. 2010. “Commentary: Do Medical Schools Have a Responsibility to Train
Physicians to Meet the Needs of the Public? The Case of Persistent Rural Physician Shortages.” Academic Medicine 85 (4): 572-574.
Rosenblatt, Roger A. and L. Gary Hart. 2000. “Physician Shortages in Rural America.” Western Journal of Medicine 173: 348-351.
Rothstein, William G. 1987. American Medical Schools and the Practice of Medicine: A History. New York: Oxford University Press.
Ruggles, Steven, J. Trent Alexander, Katie Genadek, Ronald Goeken, Matthew B. Schroeder, and
Matthew Sobek. Integrated Public Use Microdata Series: Version 5.0 [Machine-readable database]. Minneapolis: University of Minnesota, 2010.
van Bibber, A.F. 1929. “The Swan Song of the Country Doctor.” The North American Review 227(1): 89-
94.
Wozniak, Abigail. (2010). “Are College Graduates More Responsive to Distant Labor Market Opportunities?” Journal of Human Resources 45 (4): 944-970.

22
Figure 1: Number of Medical Schools, 1760-1920

23
Table 1.—Distribution of the Population, Professional Workers, and Learned Professions by Location, 1900-1920
Total population All professional workers Size of place 1900 1910 1920 1900 1910 1920
Metropolitan area 31.1% 36.9% 42.9% 41.0% 48.7% 55.4% Rural county, adjacent to
metro area 12.3 14.2 14.5 12.3 12.9 12.7
Rural county, not adjacent to
metro area 56.7 48.8 42.5 46.8 38.4 31.9
Physicians and surgeons Dentists Lawyers 1900 1910 1920 1900 1910 1920 1900 1910 1920 Metropolitan area 37.7 45.2 51.2 46.1 53.9 57.4 43.9 49.8 61.6 Rural county, adjacent to
metro area 12.0 13.5 12.6 10.9 9.2 14.9 10.7 11.7 8.9 Rural county, not adjacent to
metro area 50.3 41.3 36.3 43.0 36.9 27.7 45.5 38.5 29.5
Sources: US population data calculated from ICPSR dataset #2896; data on professional workers calculated from IPUMS datafiles

24
Table 2.—Distribution of American Medical Directory Samples by Location, All Doctors and Recent Medical School Graduates
Note: Recent medical school graduates defined as those who graduated within 5 years of the American Medical Directory publication date.
All Doctors 1909 1914 1918 1920 Metropolitan area 59.9% 61.2% 64.8% 66.6% Rural county, adjacent to metro area 13.0 12.3 12.5 11.9 Rural county, not adjacent to metro area 27.1 26.5 22.6 21.5 Number of observations 22,273 24,449 25,937 27,064 Recent Medical School Graduates 1909 1914 1918 1920 Metropolitan area 61.6 65.7 73.4 77.3 Rural county, adjacent to metro area 9.8 7.5 8.1 7.3 Rural county, not adjacent to metro area 28.6 26.8 18.5 15.4 Number of observations 3,491 3,418 3,551 3,737

25
Table 3.—Distribution of Recent Medical School Graduates by Location, By Flexner Report Review of Medical School
Panel A: Graduates of Schools Receiving Favorable
Reviews 1909 1914 1918 1920 Metropolitan area 74.6% 77.0% 81.4% 81.4% Rural county, adjacent to metro area 6.6 4.9 6.2 5.6 Rural county, not adjacent to metro area 18.8 18.1 12.4 13.0 Number of observations 1,535 1,625 1,858 2,097
Panel B: Graduates of Schools Receiving Unfavorable
Reviews 1909 1914 1918 1920 Metropolitan area 51.2 54.5 66.8 74.0 Rural county, adjacent to metro area 12.4 10.3 9.9 8.8 Rural county, not adjacent to metro area 36.4 35.2 23.3 17.2 Number of observations 1,587 1,579 1,505 1,308 Panel C: Graduates of Schools with Pass Rates < 0.75 1909 1914 1918 1920 Metropolitan area 25.7 47.6 76.8 85.6 Rural county, adjacent to metro area 7.6 7.7 10.6 5.6 Rural county, not adjacent to metro area 66.7 44.7 12.6 8.9 Number of observations 513 532 531 305

26
Table 4.—Distribution of Medical Students by Location, 1909 and 1920 1909 1920 Metropolitan area 87.0 % 84.7 % Rural county, adjacent to metro area 4.1 8.7 Rural county, not adjacent to metro area 8.9 6.7 Number of observations 21,721 13,949 Table 5.—Distribution of Medical Students by Location and Flexner Review, 1909 Favorable Review Unfavorable Review Metropolitan area 89.0 % 86.0 % Rural county, adjacent to metro area 6.3 2.4 Rural county, not adjacent to metro area 4.6 11.6 Number of observations 9,819 11,467

27
Table 6.—Physicians in 1909, Practice Location versus Medical School Location
Medical School Location Practice location Metropolitan area Rural – adjacent Rural – not adjacent Metropolitan area 62.3% 38.6% 31.8% Rural –adjacent 13.3 24.0 9.6 Rural – not adjacent 24.4 37.5 58.6 Number of observations 18,883 526 1,037

28
Table 7. – Marginal Effects from Multinomial Logit Models of Location Choice, All Physicians
Metro area
Rural –adjacent
Rural – not adj.
Metro area
Rural –adjacent
Rural – not adj.
Flexner--favorable 0.09 -0.05 -0.03 0.09 -0.06 -0.04 (32.60) (-23.68) (-16.43) (17.02) (-11.77) (-9.62) * 1914 -0.01 0.00 0.01 (-0.76) (-0.27) (1.44) * 1918 -0.01 0.01 0.00 (-1.13) (0.86) (0.55) * 1920 -0.02 0.01 0.01 (-2.33) (1.08) (1.93) Rural medical school -0.05 0.00 0.06 -0.07 -0.01 0.07 (-8.49) (-0.27) (14.87) (-4.91) (-0.70) (10.56) * 1914 0.03 -0.01 -0.02 (1.46) (-0.68) (-1.60) * 1918 0.01 0.02 -0.03 (0.51) (1.12) (-2.55) * 1920 0.02 0.02 -0.04 (0.99) (1.19) (-3.44) Years in practice -4.5E-03 2.5E-03 2.0E-03 -3.4E-03 2.3E-03 1.1E-03 (-15.02) (10.25) (8.78) (-5.67) (4.50) (2.80) * 1914 -8.4E-04 3.7E-04 4.7E-04 (-0.97) (0.50) (0.80) * 1918 -1.1E-03 -1.5E-04 1.3E-03 (-1.26) (-0.21) (1.96) * 1920 -2.4E-03 4.7E-04 1.9E-03 (-2.80) (0.69) (2.95) Years in practice—sqrd. 2.5E-05 -8.3E-05 -1.7E-05 4.5E-06 -5.4E-06 9.4E-07 (4.63) (-1.91) (-4.12) (0.39) (-0.58) (0.12) * 1914 1.8E-05 -4.7E-06 -1.3E-05 (1.06) (-0.34) (-1.16) * 1918 2.2E-05 5.0E-06 -2.7E-05 (1.29) (0.37) (-2.19) * 1920 4.2E-05 -6.6E-06 -3.6E-05 (2.77) (-0.55) (-3.10)

29
Table 7. – Continued.
Metro area
Rural –adjacent
Rural – not adj.
Metro area
Rural –adjacent
Rural – not adj.
Foreign medical school 0.12 -0.10 -0.02 0.12 -0.10 -0.02 (18.32) (-15.90) (-4.96) (9.45) (-8.32) (-2.30) * 1914 0.00 -0.01 0.01 (-0.11) (-0.32) (0.68) * 1918 0.00 0.01 -0.01 (-0.10) (0.77) (-0.89) * 1920 -0.02 0.03 -0.01 (-0.82) (1.72) (-1.07) Reported as “colored” 0.28 -0.16 -0.13 0.28 -0.16 -0.13 (1.87) (-1.71) (-1.98) (1.86) (-1.71) (-1.96) 1914 0.01 -0.01 -0.01 0.02 -0.01 -0.01 (3.93) (-2.75) (-2.29) (2.06) (-1.38) (-1.27) 1918 0.05 -0.01 -0.04 0.06 -0.01 -0.05 (14.34) (-2.32) (-17.13) (5.92) (-1.11) (-6.76) 1920 0.07 -0.02 -0.05 0.10 -0.03 -0.07 (20.39) (-6.76) (-20.21) (9.08) (-3.26) (-8.35) Number of observations 97,376 97,376 Log likelihood -57,864.65 -57,841.679
Notes: Numbers in parentheses z-statistics. Both models include state fixed effects.

30
Table 8.—Marginal Effects from Multinomial Logit Models of Location Choice, Recent Medical School Graduates
Metro area
Rural –adjacent
Rural – not adj.
Metro area
Rural –adjacent
Rural – not adj.
Flexner--favorable 0.07 -0.05 -0.02 0.08 -0.06 -0.02 (12.87) (-10.67) (-5.09) (7.48) (-6.81) (-2.39) * 1914 0.01 -0.01 0.00 (0.52) (-0.43) (-0.22) * 1918 -0.02 0.02 0.00 (-1.18) (1.57) (-0.18) * 1920 -0.03 0.03 0.00 (-1.91) (2.18) (0.09) Low pass rate 0.00 0.01 0.00 0.02 -0.02 0.00 (-0.37) (1.09) (-0.74) (1.27) (-1.69) (0.27) * 1914 -0.02 0.03 -0.01 (-0.89) (1.38) (-0.40) * 1918 -0.04 0.06 -0.02 (-1.64) (3.01) (-1.03) * 1920 0.01 0.03 -0.04 (0.30) (1.13) (-1.41) Rural medical school -0.08 0.04 0.04 -0.15 0.07 0.08 (-4.93) (3.27) (3.71) (-4.89) (2.86) (4.90) * 1914 0.12 -0.06 -0.06 (2.73) (-1.68) (-2.44) * 1918 0.06 -0.03 -0.03 (1.31) (-0.88) (-0.99) * 1920 0.13 -0.01 -0.12 (2.65) (-0.42) (-3.51) Foreign -0.01 -0.03 0.03 0.03 -0.05 0.02 (-0.29) (-1.62) (3.12) (0.79) (-1.45) (0.97) * 1914 0.02 -0.04 0.02 (0.38) (-0.73) (0.65) * 1918 -0.09 0.04 0.05 (-1.71) (0.74) (1.89) * 1920 -0.06 0.08 -0.02 (-1.10) (1.88) (-0.58)

31
Table 8. – Continued.
Metro area
Rural –adjacent
Rural – not adj.
Metro area
Rural –adjacent
Rural – not adj.
Reported as “colored” 1.26 -0.76 -0.50 1.27 -0.78 -0.49 (0.02) (-0.02) (-0.02) (0.02) (-0.02) (-0.02) 1914 0.03 -0.02 -0.01 0.02 -0.02 0.00 (3.69) (-3.36) (-1.23) (2.01) (-2.23) (-0.23) 1918 0.05 -0.02 -0.04 0.07 -0.03 -0.03 (7.19) (-2.81) (-6.78) (6.15) (-3.78) (-4.25) 1920 0.07 -0.03 -0.04 0.08 -0.04 -0.04 (9.32) (-4.22) (-7.98) (7.57) (-4.97) (-4.83) Number of observations 14,057 14,057 Log likelihood -6075.79 -6051.41
Notes: Numbers in parentheses z-statistics. Both models include state fixed effects.

32
Table 9.—Characteristics of Recent Medical School Graduates by Birthplace, North Carolina, 1918
Born in rural area in
North Carolina Born in urban area in
North Carolina
No. obs. Percent No. obs. Percent Practice in rural area 241 73.9 % 62 24.2 % Black 241 1.7 62 24.2 Medical school characteristics: Favorable review from Flexner 241 28.2 62 50.0 Low pass rate on state boards 240 3.8 62 21.0 Located in rural county, not
adjacent to metro area 241 26.6 62 22.6
Proprietary school 214 61.2 59 40.7 Closed by 1924 241 36.5 62 27.4
Notes: Sample consists of male physicians born between 1886 and 1896 found in the AMD listings for North Carolina in 1918 and linked to World War I draft registration cards.

33
Table 10.—Marginal Effects from Probit Model of Practice in Rural Area, North Carolina 1918
North Carolina 1918 Born in rural area 0.44 (5.46) Favorable review from Flexner -0.20 (-2.75) Rural medical school -0.20 (-2.63) Black -0.26 (-1.79) Number of Observations 303 Log likelihood -166.42

34
Table 11.—Odds Ratios from Conditional Logit Models of Physicians’ Choices of Counties
New York California 1909 1920 1909 1920 Metropolitan area 5.487 6.271 7.055 9.831 (19.79) (12.80) (17.73) (16.46) Rural – adj. to metro 1.357 1.327 1.932 2.279 (3.36) (1.88) (5.15) (5.38) Ln(miles to medical school attended) 0.376 0.350 0.552 0.461 (-51.36) (-49.15) (-18.14) (-23.63) Ln(miles improved roads) 0.506 0.586 1.109 (-33.59) (-44.24) (5.05) Hospital beds per 1000 1.007 1.007 1.005 1.000 (4.03) (3.00) (1.75) (-0.14) Est. doctors per 1000 0.584 1.713 2.140 3.169 (-4.57) (3.05) (8.46) (11.00) Favorable Flexner rating * Metro 2.346 2.566 1.920 1.378 (9.64) (9.56) (6.87) (3.57) * Rural – adj. to metro 1.267 1.236 1.609 1.202 (2.56) (2.15) (3.84) (1.78) * Ln(miles to med school) 1.226 1.702 1.273 1.325 (8.93) (26.03) (6.12) (9.21) * Ln(miles imp. roads) 1.046 0.958 0.949 (1.86) (-3.66) (-2.59) * Hospital beds 0.999 1.005 1.004 1.001 (-0.30) (3.49) (1.42) (0.45) * Est. doctors 1.698 1.968 1.465 1.532 (4.48) (5.22) (4.50) (6.25) Years in practice > 9 * Metro 0.730 0.574 1.466 1.110 (-3.35) (-3.78) (3.45) (0.76) * Rural – adj. to metro 0.930 0.975 1.043 0.989 (-0.73) (-0.17) (0.31) (-0.07) * Ln(miles to med school) 1.090 1.093 1.040 1.172 (4.21) (4.12) (1.02) (4.49) * Ln(miles imp. roads) 1.165 1.118 1.052 (7.21) (9.45) (2.32) * Hospital beds 0.997 1.000 1.002 0.998 (-1.56) (0.04) (0.76) (-0.77) * Est. doctors 1.597 1.134 1.107 0.823 (3.76) (0.69) (1.09) (-1.91) Number of Physicians 10,320 13,278 3,275 5,371

35
Table 12.—Odds Ratios from Conditional Logit Models of Recent Medical School Graduates’ Choices of Counties
New York California 1909 1920 1909 1920 Metropolitan area 5.714 4.386 4.431 11.972 (12.90) (7.76) (6.34) (10.37) Rural – adj. to metro 1.684 0.992 1.440 2.072 (3.69) (-0.04) (1.59) (2.85) Ln(miles to medical school attended) 0.347 0.336 0.498 0.426 (-33.89) (-32.25) (-11.26) (-19.67) Ln(miles improved roads) 0.485 0.558 1.055 (-20.95) (-26.47) (1.47) Hospital beds per 1000 1.013 1.007 1.008 1.008 (4.88) (2.15) (1.73) (1.75) Est. doctors per 1000 0.369 0.971 1.946 2.159 (-5.07) (-0.12) (3.98) (4.36) Favorable Flexner rating * Metro 2.236 4.637 2.558 1.097 (3.36) (4.63) (3.01) (0.30) * Rural – adj. to metro 0.975 2.517 1.919 1.410 (-0.10) (2.70) (1.90) (1.03) * Ln(miles to med school) 1.208 2.000 1.337 1.570 (3.31) (13.71) (2.86) (6.05) * Ln(miles imp. roads) 1.223 0.968 1.026 (3.38) (-1.03) (0.46) * Hospital beds 0.991 1.005 1.000 0.990 (-1.96) (0.99) (-0.03) (-1.63) * Est. doctors 4.298 3.921 1.576 3.102 (4.77) (3.50) (1.90) (5.01) Numbers of Physicians 2,119 2,463 449 626