Embed Size (px)
Citation preview

The Swiss IMRT dosimetry intercomparison using a thorax phantom
H. Schiefer1, A. Fogliata2, G. Nicolini2, L. Cozzi2, W.W. Seelentag1, E. Born3, F. Hasenbalg3, J. Roth4, B. Schnekenburger4, K. Münch-Berndl5, V. Vallet6, M. Pachoud6, B. Reiner7,
G. Dipasquale8, B. Krusche9, and M.K. Fix3
1 Klinik für Radio-Onkologie, Kantonsspital St.Gallen, St.Gallen, Switzerland, 2 Oncology Institute of Southern Switzerland, Medical Physics Unit, Bellinzona, Switzerland, 3Division of Medical Radiation Physics, Inselspital, Bern University Hospital, and University of Bern, Switzerland, 4 Institut für Radio-Onkologie, Universitätsspital Basel, Switzerland, 5: Radio-Onkologie, Lindenhofspital, Bern, Switzerland, 6 University Institute for Applied Radiophysics, Grand-Pré 1, CH-1007 Lausanne, Switzerland, 7 Radiation Oncology, University Hospital, Zurich, Switzerland, 8Service de Radio-Oncologie, Hôpitaux Universitaires de Genève, Geneva, Switzerland, 9Institut für Physik, Universität Basel, CH-4056, Basel, Switzerland
Corresponding Author:
Hans Schiefer
Klinik für Radio-Onkologie
Kantonsspital
CH-9007 St.Gallen
Switzerland
Tel: +41 71 494 2239
FAX: +41 71 494 2893
Email: [email protected]

The Swiss IMRT dosimetry intercomparison using a thorax phantom
Abstract
Purpose: In 2008, a national Intensity Modulated Radiation Therapy (IMRT) dosimetry
intercomparison was carried out for all 23 radiation oncology institutions in Switzerland. It
was the aim to check the treatment chain, focused on the planning, dose calculation and
irradiation process.
Methods: A thorax phantom with inhomogeneities was used, in which thermoluminescence
dosimeter (TLD), and ionization chamber measurements were performed. Additionally,
absolute dosimetry of the applied beams has been checked. Altogether, 30 plan-measurement
combinations have been used in the comparison study. The results have been grouped
according to dose calculation algorithms, classified as “type a” or “type b”, as proposed by
Knöös et al.1.
Results: Absolute dosimetry check under standard conditions: The mean ratio between the
dose derived from the single field measurement and the stated dose, calculated with the
treatment planning system, was 1.007 ± 0.010 for the ionisation chamber and 1.002 ± 0.014
(mean ± standard deviation) for the TLD measurements.
IMRT plan check: In the lung tissue of the planning target volume (PTV) a significantly better
agreement between measurements (TLD, ionisation chamber) and calculations is shown for
“type b” algorithms than for “type a” (p < 0.001). In regions outside the lungs the absolute
differences between TLD measured and stated dose values, relative to the prescribed dose,
(Dm-Ds)/Dprescribed , are 1.9 ± 0.4% and 1.4 ± 0.3%, respectively. These data show the same
degree of accuracy between the two algorithm types if low density medium is not present.
Conclusion: Our results demonstrate that the performed intercomparison is feasible and
confirm the calculation accuracies of “type a” and “type b” algorithms in a water equivalent
and low-density environment. It is now planned to offer the intercomparison on a regular basis
to all Swiss institutions using IMRT techniques.
Key words: dose comparison, radiotherapy, Intensity-Modulated, heterogeneity,
thermoluminescence dosimetry
2

The Swiss IMRT dosimetry intercomparison using a thorax phantom
I. INTRODUCTION
A few years ago, IMRT (Intensity Modulated Radiation Therapy) was described as “a revolution in
the treatment of cancer”.2 Now, IMRT is practiced in most radiotherapy centers and is accepted as an
improvement on existing treatment techniques for several disease sites3-5.
Due to its complexity, IMRT is associated with a variety of uncertainties.6, 7 Uncertainties leading to
inaccurate dose delivery have implications on tumor control, treatment morbidity and toxicity. 8, 9 Thus,
comprehensive quality assurance (QA) procedures are essential to check calculation and delivery. 10 For
patient related QA, the validation of at least the data transfer and the intended dose to be delivered is
important.11
In addition to the patient and machine related QA procedures performed by the institutions
themselves, an audit organized by an independent external body is a fundamental step in any dosimetry
QA program.6 The audits provided by the European Society for Therapeutic Radiology and Oncology
(ESTRO), the Radiological Physics Center (RPC) and other institutions comprise not only basic tests of
the machine calibration, but they also check a substantial amount of the total therapy chain.12-14 Ebert et al.
presented a comprehensive view on national and international studies and intercomparisons.8
An intercomparison based on a standard patient represented by an anthropomorphic phantom enables
an end to end test, i.e. all technical steps in the treatment chain can be checked. 8 In the hierarchical
structure defined by Kron et al.15 such kind of test is classified as Level III, while an intercomparison
measuring the linear accelerator output under reference conditions in a regular phantom is referred to as
Level I.
An issue often discussed is the ability of the dose calculation algorithms to properly take into account
inhomogeneities, especially in low-density regions. Additionally, it is well known that dose calculation
errors can be enhanced due to very small fields (< 4 cm edge length) which are typical for the IMRT
technique.1, 16-21
This paper deals with the first such national intercomparison study held in Switzerland. All Swiss
radiotherapy institutions participated in the study. Dose distributions in an anthropomorphous phantom
with inhomogeneities were investigated. Calculations using different treatment planning systems were
compared with measurements using different detectors.
Since an intercomparison was considered of general interest, the SSRMP (Swiss Society of
Radiobiology and Medical Physics) decided to organize a national IMRT dosimetry intercomparison and
offer it to all Swiss radio-oncology centers. The aim was to check multiple components of IMRT
treatments using a thorax phantom provided with inhomogeneities. The intercomparison was organized
by the physics team of the Cantonal Hospital St.Gallen which is responsible for all national dosimetric
intercomparisons that have been performed in Switzerland since 2001.
3

The Swiss IMRT dosimetry intercomparison using a thorax phantom
II. MATERIALS AND METHODS
All 23 radiation oncology institutions in Switzerland participated in the Swiss IMRT intercomparison
between July 2008 and February 2009. A thorax phantom together with TLDs and ionization chamber
inserts were sent to each participating center with a pre-defined time schedule. Two phantoms were used
in a two week cycle. Detailed information on how to perform plans, calculations and measurements were
also included. Each center had the possibility to perform ionization chamber measurements using their
own equipment. It is legally required in Switzerland that all ionisation chamber calibrations have to be
traceable to the National Primary Dosimetry Laboratory (METAS; Bundesamt für Metrologie und
Akkreditierung). The 95% confidence interval of the METAS calibration for photon beams is 1.4% (at
the date of the intercomparison). All errors are stated at one standard deviation of the mean of the
quantity of interest.
II.A. Detectors
TLD-100 discs (4.5 mm Ø x 0.9 mm; Harshaw Inc.) were used together with a TLD reader model
“5500” (Harshaw Inc.). The TLDs were tempered in a PTW-TLDO oven (PTW Freiburg). Reference
irradiations were performed using a “Theratron 60” cobalt unit (AECL of Canada). An evaluation of
consecutive reference irradiations has shown that the measurement reproducibility of one single TLD is
better than 0.5% (1 SD). The measurement uncertainty for a detector consisting of five discs has been
determined in the course of a preliminary study, which is described below.
Ionization chamber measurements were conducted by the individual centers using their own
equipment.
II.B. Phantom
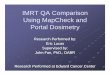
For the IMRT intercomparison, the thorax phantom 002LFC (CIRS Inc.) has been selected. The
phantom is shown in figure 1. It consists basically of a 15 cm thick slice (slice 01, on the right side of the
picture) and 15 standard slices (each 1cm thick, on the left side). They are composed of water equivalent
material with inhomogeneities mimicking lungs (density 0.21 g/cm3) and a bony vertebra (density 1.6
g/cm3), with invariant geometry and density distribution in the longitudinal direction. Slice 01 can
accommodate different ionization chambers (using appropriate inserts allowing the usage of different ion
chamber types) in pre-defined positions.
4

The Swiss IMRT dosimetry intercomparison using a thorax phantom
Figure 1. Schematic view of the CIRS thorax phantom. Right: Ionization chamber measurements
are performed in the 15 cm slice. Left: Standard slice. Sketch provided with courtesy by CIRS Inc.
A 1 cm slice has been modified with 54 holes to accommodate two TLDs each. The TLD positions
are grouped as shown in figure 2, where also different anatomical structures are overlaid: Planning Target
Volume (PTV), located both in soft tissue (11 TLD positions), and in lung tissue (11 TLD positions), lung
tissue (16 TLD positions), soft tissue (11 TLD positions, 5 of them in the ‘heart’ structure), bone (5 TLD
positions). Four TLD positions coincide with ionization chamber measurement points (Pos1: PTV in soft
tissue, Pos2: PTV in lung tissue, Pos3: bone, and Pos4: lung outside the PTV).
Figure 2. TLD and ionisation chamber (Pos1 to Pos4) measurement points.
The aim was to check the applied dose on one single transversal plane with TLDs and ionisation
chambers. This allows cross checking the measurements. In order to avoid perturbations of the dose
distribution in the measurement plane induced by the measurement equipment, measurements have been
performed in a plane outside the beam divergence, 5 cm off axis to the isocenter. In this way both the
influence of the small air gap between slices and the “shadowing” of TLD detectors are eliminated.
5

The Swiss IMRT dosimetry intercomparison using a thorax phantom
II.C. Preliminary study
Dose calculations of a single 6 MV photon field laterally crossing both lungs (gantry angle: 90°; field
length: 20 cm, field width: 10 cm, dose to the isocentre position: 1.8 Gy) have been carried out by the
Division of Medical Radiation Physics, Inselspital and University of Bern. The “Voxel Monte Carlo”
(VMC++) code within the Swiss Monte Carlo Plan environment has been applied.22 The code was
explicitly commissioned for the Linac used in Berne.
Six institutions participated in the preliminary study. The tissue phantom ratios (TPR20, 10) of the
used linacs showed a very similar beam quality within 0.8%. Thus the commissioning of each individual
linac was not necessary for the purpose of this study. 24 TLD positions in a transversal plane have been
aligned on two paths, longitudinal and transverse to the field axis. Each position contained five TLDs.
II.D. Intercomparison
II.D.I. Linac calibration check
A correct machine calibration is the basis of every successful irradiation treatment. Kron et al. 15
highlighted the usefulness of undertaking simultaneous Levels I and III measurements. Following Kron et
al., a single field irradiation with 2 Gy in a water equivalent portion of the phantom was used as machine
calibration check (a special insert with 8 TLD at 10 cm depth was included for this purpose). The field
setup was: field size 10 x 10 cm2, source to surface distance SSD = 90 cm, gantry angle 0°, i.e. reference
geometry as recommended by the Swiss protocol for high energy photon beams.23 A measurement under
the same conditions was performed with an ionization chamber (“Pos 1” in figure 2). The institutions
were asked to calculate the dose with the same algorithm as used for the plan. Additionally, the
institutions stated the expected dose in water in 10 cm depth, for the same field setup and the identical
number of monitor units (MU).
From this field irradiation, factors (converting the dose in the phantom to the dose expected in water
when applying the same number of monitor units) for both TLD and ion chamber measurements are
determined. They are used to derive the expected dose in water under the same conditions (results see
table 2).
II.D.II. IMRT treatment
The computer tomography (CT) scans of the phantom were carried out by the individual institutions.
Since the phantom was already filled with TLDs when sent to the testing institutions, the applied CT dose
also had to be measured.
Preparatory measurements confirmed that the dose within the phantom can be approximated with
sufficient accuracy by the dose of the surface. Similar to the RPC (Radiological Physics Center)
procedure11, surface dose was determined by strips of three TLDs each.
Furthermore one additional strip was provided in order to measure the background contribution
6

The Swiss IMRT dosimetry intercomparison using a thorax phantom
during transport and storage. Doses accumulated by the TLD in those strips were subtracted from the total
dose read from TLDs prior to analysis.
Two Perspex slices with cutouts for PTV and “heart” at the phantom longitudinal edges permitted an
easy delineation of the PTV and the heart structures for the treatment planning (otherwise not visible).
The PTV and the heart are 8 cm long, while the lung and spinal cord structures cover the entire phantom
length.
Centers were asked to prepare an IMRT plan fulfilling the following constraints:
• PTV: dose prescription (100%) to median PTV Dose = 2.00 Gy.
• Spinal cord: Maximum dose Dmax < 75% of the prescribed dose.
• Both lungs outside PTV: Less than 20% of each lung should receive more than 35% of the prescribed dose (D20% < 35%)
• Heart: Dmax < 55% of the prescribed dose.
The institutions were asked to irradiate the phantom hosting TLDs and ionization chamber according to
this plan. The dose calculated by the treatment planning system (called Ds, stated dose) at each TLD and
ion chamber measuring point were provided to the coordinating center in St.Gallen, along with the results
of the ionization chamber measurements.
IMRT was the suggested technique, but other techniques have also been accepted. Some institutions
carried out the calculation with two different calculation algorithms (five centers) or participated twice in
the intercomparison by testing different machines (one center) or irradiation techniques (one center using
IMRT or RapidArc). All plans used 6 MV beams.
Altogether 30 plan-measurement combinations were evaluated, and each is considered as independent
in the present study. Twelve evaluations related to static IMRT (using static field segments), eleven to
dynamic IMRT (using dynamic sliding window method or Rapid Arc), one to Tomotherapy and six to
3D-CRT irradiation techniques. A total of 24 machines have been tested.
For data analysis the percentage dose difference between stated and measured dose was reported:
(Dm-Ds)/Dprescribed, where Dm is the measured dose, Ds the stated dose and Dprescribed is the dose prescription
of 2 Gy (median PTV dose). The “absolute difference” is defined by the expression (Dm-Ds)/Dprescribed .
For the evaluation, the algorithms used by the institutions have been classified as “type a” and “type
b” algorithms, as defined by Knöös et al.1 and Fogliata et al.18: “Type a” algorithms are primarily based
on equivalent path length for inhomogeneity correction. “Type b” algorithms account for electron
transport in an approximate way as well as the secondary photon transport in the medium, thus
accounting for density changes along all dimensions. The treatment planning systems (TPS), calculation
algorithms and irradiation techniques used in the intercomparison are summarized in table 1. No
institution performed the dose calculation with a MC algorithm.
7

The Swiss IMRT dosimetry intercomparison using a thorax phantom
Table 1. Applied TPS, calculation algorithms and irradiation techniques.
TPS calculation algorithm and version3D-CRT
dyn. IMRT
static IMRT all
type
a (
12) Eclipse PBC + mod.Batho 7.5,7.6,8.0,8.1,8.2,8.5 7 2 9
KonRad PBC 2.2 1 1
Precise Plan Clarkson 2.12 1 1
Eclipse PBC + eqTAR 8.1 1 1
type
b (
18) Pinnacle CCC 8.0 2 4 6
Eclipse AAA 7.5 / 8.1 / 8.2 / 8.5 4 1 5
Oncentra MasterPlan CCC 3.0 3 1 4
XiO multigrid conv./superp. 4.3 / 4.34 2 2
Hi-Art (Tomo) conv./superp. 3.1 1 1
all 6 12 12 30
III. RESULTS
III.A. Preliminary study
Apart from measurements close to the field edges, the absolute dose difference between MC dose
calculations and TLD measurements is 0.9±0.6% in the normal tissue and 1.1±1.2% in lung, respectively
(1 SD). These values are in the same range as the measurement uncertainty of 0.6% to 0.9% observed in
previous dosimetry intercomparisons in a water tank.24
III.B. IMRT dosimetry intercomparison
III.B.I. Linac calibration check
Table 2 shows the ratio between the dose derived from the phantom measurement, Dm, and the stated
dose under standard conditions, Ds. It is a measure of the linac calibration.
Table 2. Results of the absolute dosimetry measurements (28 evaluations)
Dm/Ds ion. chamber Dm/Ds TLD
“type a” 1.005 ± 0.006 1.000 ± 0.014
“type b” 1.008 ± 0.012 1.004 ± 0.014
All 1.007 ± 0.010 1.002 ± 0.014
The maximum deviation of the TLD measured dose to the stated dose is 3.2%. 24 of 28 TLD
measurements (85%) agree better than 2% with the stated doses, which is an excellent result. No relevant
differences between ionization chamber and TLD measurements have been found (p = 0.19) although a
0.5% higher measured value (on average) for ion chamber is present with respect to TLD. The TLD
8

The Swiss IMRT dosimetry intercomparison using a thorax phantom
measurements show a larger standard deviation than the ionization chamber measurements. This is likely
to be due to the lower precision of the TLD measurements compared to ionisation chamber measurements
and due to linac calibration by the institutions, where the ionisation chamber system used for calibration
can correspond to the one used in the IMRT intercomparison. No information about the uncertainty of the
ionisation chamber measurements is available.
III.B.II. IMRT planning and treatment
A visual example of the results in terms of percentage dose differences is shown in figure 3, for a
“type a” (Eclipse, PBC) and a “type b” (Eclipse, AAA) algorithm for the same unit. Differences occur
especially in the lung region with high doses (PTV), and in particular for the “type a” algorithm, as is to
be expected.
Figure 3. Graphical representation of the dose difference values for an IMRT case, planned with 7
fields (gantry angles of 40, 90, 125, 180, 235, 285 and 345 degree). Deviations larger than 5% are
highlighted in dark gray (Electronic version: Overdosed points in comparison with the calculation in dark
red, underdosed points in dark blue). Deviations within 1% are colored in white. Left: “Type a” algorithm
(Eclipse PBC), right: “Type b” algorithm (Eclipse AAA), for the same treatment unit and measurement
set.
To show the accuracy of different dose calculation algorithms, especially related to the calculations in
low density media, the relative difference between the (Dm-Ds)/Dprescribed values in the lung and the soft
tissue regions within the PTV are calculated. Since the dose level is comparable in the lung and normal
tissue regions of the PTV, differences between these media are independent of systematic deviations
originating from the planning process or machine calibration, but depend on the dose calculation
algorithm. Averaged values derived from ionization chamber and TLD measurements for 30 plan-
measurement combinations are shown in table 3. TLD values are averaged over 11 single positions
whereas the ionization chamber value is based on a single measurement point.
9

The Swiss IMRT dosimetry intercomparison using a thorax phantom
Table 3. Ion chamber and TLD measurements in the soft tissue and lung region within the PTV: Mean
(Dm-Ds)/Dprescribed values and associated uncertainties in %. The number of cases per algorithm is added in
parentheses. For the Tomotherapy machine, the ionization chamber measurements are missing.
PTV soft PTV lung difference
Ion ch. TLD Ion ch. TLD Ion ch. TLD
type
a
Eclipse PBC (9) -1.8 ± 1.2 -1.4 ± 2.3 -3.3 ± 2.8 -5.4 ± 2.1 -1.5 ± 2.3 -4.0 ± 1.4
KonRad PB (1) -2.3 -0.4 -10.7 -8.7 -8.5 -8.3
PrecisePlan Clarkson (1) 0.0 -0.5 -6.5 -4.9 -6.6 -4.4
Eclipse PBC eTAR (1) 0.5 0.5 -2.3 -3.8 -2.7 -4.3
type
b
Pinnacle CCC (6) 0.4 ± 0.9 0.6 ± 0.6 0.2 ± 0.8 -0.5 ± 1.0 -0.1 ± 0.4 -1.1 ± 0.8
Eclipse AAA (5) -1.8 ± 0.9 -1.8 ± 1.6 -1.0 ± 1.3 -1.5 ± 1.3 0.7 ± 0.9 0.4 ± 0.8
MasterPlan CCC (4) 0.2 ± 0.9 2.1 ± 0.6 1.6 ± 3.6 2.1 ± 2.8 1.4 ± 3.1 -0.1 ± 2.5
XiO-CMS (2) -2.2 ± 0.7 0.0 ± 1.5 0.0 ± 1.4 -0.2 ± 1.4 2.2 ± 0.8 -0.1 ± 0.1
Tomotherapy CS (1) - -1.3 - -4.2 - -2.9
Mann-Whitney-tests for both TLD and ionization chamber measurements in the PTV prove that
“type b” algorithms are superior to “type a” in calculating the dose in the lung region within the PTV,
with p < 0.001.
10

The Swiss IMRT dosimetry intercomparison using a thorax phantom
Table 4 shows the percentage dose difference in regions outside the PTV: left and right lungs, normal
soft tissue, heart and spinal cord (embedded in the bony-like structure).
Table 4. Mean percentage (Dm-Ds)/Dprescribed values in the regions outside the PTV
Considering all TLD measurements (all points) and institutions, the mean absolute difference
between measured and stated dose values, relative to the prescribed dose, (Dm-Ds)/Dprescribed , is 2.5 ±
2.0% for the “type a” and 1.4 ± 1.1% for the “type b” algorithms. In regions outside the lungs the values
are 1.9 ± 0.4% and 1.4 ± 0.3%, respectively, while for points inside lung densities the figures are 3.3 ±
1.7% and 1.4 ± 0.3%, respectively. The data show the same degree of accuracy between the two
algorithm types as long as no low density medium is present.
Figure 4 shows the mean of the (Dm-Ds)/Dprescr. absolute values for the PTV lung and normal tissue
regions, categorized by the algorithm type and the irradiation technique. The data give no hint about an
influence of the irradiation technique.
11
mean TLD measurement: (Dm-Ds)/Dprescribed [%]
Algorithm left lung right lung normal tissue heart spinal cord
type
a
Eclipse PBC -1.7 ± 2.5 -0.7 ± 1.3 -0.3 ± 2.1 -0.8 ± 1.7 -2.3 ± 2.4
KonRad PB -4.7 -2.4 -1.4 -3.5 -2.3
PrecisePlan integr.
alg.
-4.5 -3.3 -1.5 -0.4 1.7
Eclipse PBC eTAR 1.2 -1.5 1.0 1.6 0.4
mean “type a” -1.9 ± 2.6 -1.1 ± 1.4 -0.4 ± 1.9 -0.8 ± 1.8 -1.7 ± 2.4
type
b
Pinnacle CCC 0.8 ± 1.3 0.1 ± 1.0 0.7 ± 1.2 0.5 ± 0.9 -0.2 ± 2.1
Eclipse AAA -0.9 ± 2.1 -0.5 ± 0.6 -0.5 ± 1.1 -0.4 ± 1.1 -1.4 ± 1.9
MasterPlan CCC 0.0 ± 1.7 1.2 ± 0.6 0.7 ± 0.8 0.4 ± 0.6 1.5 ± 1.1
XiO-MSC 1.1 ± 0.4 0.4 ± 2.1 -0.6 ± 2.5 -1.7 ± 2.4 2.9 ± 2.7
Tomotherapy CS 0.8 -1.2 -0.6 0.4 -0.7
mean „type b“ 0.2 ± 1.7 0.2 ± 1.2 0.2 ± 1.5 0.0 ± 1.4 0.1 ± 2.3

The Swiss IMRT dosimetry intercomparison using a thorax phantom
Figure 4. Mean absolute (Dm-Ds)/Dprescr. values (error bars for 1 SD) grouped according to the
irradiation technique and the applied algorithm type. The number of comparisons is quoted in
parentheses.
Figure 5 shows the graded (Dm-Ds)/Dprescr. absolute values for the PTV normal and lung tissue (30
evaluations), derived from the TLD measurements. For the normal tissue, all values except one (97%) are
smaller than 5%. 24 values (80%) are smaller than 3%. The corresponding values for the lung are 77%
and 50%. As stated earlier, it can be observed that “type b” algorithms show a better agreement with the
measurements in the lung region than “type a” algorithms. This statement is not valid for the normal
tissue region. An influence of the irradiation technique cannot be observed.
Figure 5. Graded (Dm-Ds)/Dprescr. values for PTV lung and normal tissue. Black symbols: “type a”
algorithms, white symbols: “type b” algorithms. Irradiation techniques are indicated with different
12

The Swiss IMRT dosimetry intercomparison using a thorax phantom
symbols.
Criteria for failure rates have not been defined. But these results underline again the highly satisfying
dosimetry performed by the institutions in Switzerland.
IV. DISCUSSION
A first IMRT plan intercomparison project was held in Switzerland in 2008-2009, aiming to check
dose distributions mainly from IMRT plans, as calculated by treatment planning systems and as measured
(with TLD and ion chamber) in an anthropomorphic thorax phantom.
The preliminary study, checking one single field against Monte Carlo simulations, proved the
accuracy of the TLD measurements both in water and lung equivalent media to be sufficient. They were
reliable and therefore suitable for the intercomparisons.
Additionally, ionisation chamber measurements were performed by the individual institutions, giving
further and immediate information supporting the TLD results.
The specific check of the plan dose calculation and delivery chain gave valuable information to the
participating centers. Additionally, the results from the intercomparison showed some interesting features,
mainly differences between “type a” and “type b” dose calculation algorithms: With a multicenter
intercomparison, where several and different TPS were used as well as different techniques, we
confirmed that “type b” algorithms take inhomogeneities into account better than “type a”. This finding
coincides with other groups25.
Some “type a” algorithms show deviations between calculations and measurements of more than 5%
in the PTV region located in the lung area, with both TLDs and ionization chamber. The same pattern is
detected in lung regions outside the PTV. A useful additional outcome of this dosimetry intercomparison,
is that it gives the participating centers the opportunity to evaluate the degree of accuracy of their dose
calculation algorithm when used in near clinical conditions. In particular two main points could be
addressed. The first point concerns the cases where the target partially includes a low density medium: in
this case a center running a “type a” algorithm is informed that the dose delivered to the PTV in the lung
tissue could be about 5% lower than planned (and expected), with possible issues in terms of treatment
outcome. The second point relates to the dose delivered to healthy lung tissue: the user needs to consider
the issue of the tolerance dose level stipulated for the lung and the dose computed by their TPS,
depending on whether the algorithm is a type “a” or “b”. These dosimetric tests permit users a better
understanding of their algorithm response in certain conditions and the possible consequences.
Within soft tissue, both “type a” and “b” algorithms present dose calculations which agree with the
measurements within 2% of the prescribed dose, with no significant difference between the two types.
This finding coincides with other published results.1,18,26. The irradiation technique (3D-CRT, static or
dynamic IMRT) has no influence on the agreement between measurements and calculations.
No information is available on the time needed for planning, irradiation and documentation of the
13

The Swiss IMRT dosimetry intercomparison using a thorax phantom
intercomparison. But our own experiences show that the effort has been about three times larger than for
a clinical IMRT plan.
The intercomparison focused on the currently available dose calculation algorithms. In 2008, MC was
not available for routine planning in the institutions. Due to the rapid adoption of MC algorithm in the
community with the increasingly powerful computing, the inclusion of MC will be an issue for future
dosimetric intercomparisons.
Finally, it can be stated that all the treatment plans carried out by the Swiss radiotherapy centers
fulfilled the requirements in terms of planning objectives. However, it has to be pointed out that relevant
parts of the overall treatment chain cannot be checked in the frame of a dosimetry intercomparison. For
this a more general intercomparison would be necessary including e.g. the diagnosis and the therapy
concept, the delineation of the planning structures, the positioning of the patient and treated volume, etc.
It is the responsibility of the institutions to arrange and participate in advanced education and QA
concepts including such tasks. These elements are subjects of ongoing investigations.27-30
V. CONCLUSION
The intercomparison procedure has turned out to be feasible and yields valuable convincing results.
In the future, the IMRT intercomparison will be repeated on a three years regular interval with modified
objectives adapted to the current demands.
VI. ACKNOWLEDGMENTS
The persons responsible for the IMRT intercomparison - Hans Schiefer and Wolf W. Seelentag -
thank all the participants for the excellent cooperation in the planning process of the intercomparison and
in the intercomparison itself. They express their sincere thanks especially to the participants of the pilot
study which served additionally as co-authors of this article. A special thank due to the members of the
AMS team of the University of Berne, above all to Michael Fix, Federico Hasenbalg and Ernst Born for
the MC calculation which confirmed the accuracy of the TLD measurements. A thank goes to Nicci
Lomax for the final article review.
Tables:
See text
Figure Captions:
See text
Author to whom correspondence should be addressed: Electronic address: [email protected];
Telephone: (0041) +71 494 2239; Fax: (0041) +71 494 289.3
14

The Swiss IMRT dosimetry intercomparison using a thorax phantom
References1T. Knöös, E. Wieslander, L. Cozzi, C. Brink, A. Fogliata, D. Albers, H. Nyström, and S. Lassen,
“Comparison of dose calculation algorithms for treatment planning in external photon beam therapy for
clinical situations,” Phys. Med. Biol. 51, 5785-5807 (2006).
2J. Mundt, and J.C. Roeske, “Can Intensity-modulated Radiation Therapy Replace Brachytherapy in the
Management of Cervical Cancer? Counterpoint,” Brachytherapy 1, 192-194 (2002).
3M.J. Zelefsky, Z. Fuks, L. Happersett, H.J. Lee, C.C. Ling, C.M. Burman, M. Hunt, T. Wolfe, E.S.
Venkatraman, A. Jackson, M. Skwarchuk, S.A. Leibel, “Clinical experience with intensity modulated
radiation therapy (IMRT) in prostate cancer,” Radiother. Oncol. 55, 241-249 (2000).
4A. Lin, H.M. Kim, J.E. Terrell, L.A. Dawson, J.A. Ship, and A. Eisbruch, “Quality of Life After Parotid-
sparing IMRT for Head-and-Neck Cancer: A Prospective Longitudinal Study,” Int. J. Radiat. Oncol.
Biol. Phys. 57, 673-682 (2003).
5H.H. Liu, X. Wang, L. Dong, Q. Wu, Z. Liao, C.W. Stevens, T.M. Guerrero, R. Komaki, J.D. Cox, R.
Mohan, “Feasibility of sparing lung and other thoracic structures with intensity-modulated radiotherapy
for non-small-cell lung cancer,” Int. J. Radiat. Oncol. Biol. Phys. 58, 1268-1279 (2004).
6A. Swinnen, J. Verstraete and D. P. Huyskens, “The use of a multipurpose phantom for mailed dosimetry
checks of therapeutic photon beams: ‘OPERA’ (operational phantom for external radiotherapy audit),”
Radiother. Oncol. 64, 317-326 (2002).
7G.A. Ezzell, J.M. Galvin, D. Low, J.R. Palta, I. Rosen, M.B. Sjarpe, P. Xia, Y. Xiao, L. Xing, and C.X.
Yu, “Guidance document on delivery, treatment planning, and clinical implementation of IMRT: Report
of the IMRT subcommittee of the AAPM radiation therapy committee,” Med. Phys. 30, 2089–2115
(2003).
8M.A. Ebert, K.M. Harrison, D. Cornes, S.J. Howlett, D.J. Joseph, T. Kron, C.S. Hamilton, and J.W.
Denham, “Comprehensive Australasian multicentre dosimetric intercomparison: Issues, logistics and
recommendations,” J. Med. Imaging Radiat. Oncol. 53, 119–131, (2009).
9P. Dixon, and B. O'Sullivan, “Radiotherapy quality assurance: time for everyone to take it seriously,”
Eur. J. Cancer 39, 423-429 (2003).
10A.L. Boyer, E. Mok, and G. Luxton “Quality assurance for treatment planning dose delivery by 3DRTP
and IMRT,” in: A. S. Shiu, D. E. Mellenberg, editors. “General practice of radiation oncology physics in
the 21st centry,” Madison, WI: Medical Physics Publishing, 187-230 (2000).
15

The Swiss IMRT dosimetry intercomparison using a thorax phantom
11A Molineu, D.S. Followill, P.A. Balter, W. Hanson, M.T. Gillin, M.S. Huq, A. Eisbruch, and G.S.
Ibbott, “Design and implementation of an anthropomorphic quality assurance phantom for intensity-
modulated radiation therapy for the radiation therapy oncology group,” Int. J. Radiat. Oncol. Biol. Phys.
63, 577-583 (2005).
12AAPM, “Quality Assurance for Clinical Trials: A Primer for Physicists,” AAPM Report No. 86,
Madison, WI: Medical Physics Publishing (2004).
13G.S. Ibbott, D.S. Followill, A. Molineu, J.R. Lowenstein, P.E. Alvarez, and J.E. Roll, “Challenges in
credentialing institutions and participants in advanced technology multi-institutional clinical trials,” Int. J.
Radiat. Oncol. Biol. Phys. 71(1), S71-S75 (2008).
14A. Swinnen, “Quality assurance in radiotherapy: development and validation of a mailed dosimetry
procedure for external audits using a multipurpose phantom and in vivo dosimetry,” Thesis submitted to
the Katholieke Universiteit Leuven, (2005).
15T. Kron, C. Hamilton, M. Roff, and J. Denham, “Dosimetric intercomparison for two Australasian
clinical trials using an anthropomorphic phantom,” Int. J. Radiat. Oncol. Biol. Phys. 52, 566-579 (2002).
16R. Capote, F. Sanchez-Doblado, A. Leal, J.I. Lagares, R. Arrans, and G.H. Hartmann, “An EGSnrc
Monte Carlo study of the microionization chamber for reference dosimetry of narrow irregular IMRT
beamlets,” Med. Phys. 31, 2416 (2004).
17P. Carrasco, N. Jornet, M.A. Duch, L. Weber, M. Ginjaume, T. Eudaldo, D. Jurado, A. Ruiz, and M.
Ribas, “Comparison of dose calculation algorithms in phantoms with lung equivalent heterogeneities
under conditions of lateral electronic disequilibrium,” Med Phys. 31(10), 2899-2911 (2004).
18A. Fogliata, E. Vanetti, D. Albers, C. Brink, A. Clivio, T. Knöös, G. Nicolini, and L. Cozzi, “On the
dosimetric behavior of photon dose calculation algorithms in the presence of simple geometric
heterogeneities: comparison with Monte Carlo calculations,” Phys. Med. Biol. 52, 1363-1385 (2007).
19P. Carrasco, N. Jornet, M. A. Duch, V. Panettieri, L. Weber, T. Eudaldo, M. Ginjaume, and M. Ribas,
“Comparison of dose calculation algorithms in slab phantoms with cortical bone equivalent
heterogeneities,” Med. Phys. 34(8), 3323-3333 (2007).
20L. Cozzi, G. Nicolini, E. Vanetti, A. Clivio, M. Glashörster, H. Schiefer, and A. Fogliata, “Basic
dosimetric verification in water of the anisotropic analytical algorithm for Varian, Elekta and Siemens
linacs,” Zeitschr. f. Med. Physik 18(2), 128-135 (2008).
21J.C. Chow, M.K. Leung, and J. Van Dyk, “Variations of lung density and geometry on inhomogeneity
correction algorithms: a Monte Carlo dosimetric evaluation,” Med. Phys. 36(8), 3619-3630 (2009).
16

The Swiss IMRT dosimetry intercomparison using a thorax phantom
22M.K. Fix, P. Manser, D. Frei, W Volken, R. Mini, and E. J. Born, “An efficient framework for photon
Monte Carlo treatment planning,” Phys. Med. Biol. 52, N425-N437 (2007).
23SGSMP, “Recommendations No 8: High-Energy Photon Beam Therapy Dosimetry with Ionisation
Chambers, “ISBN 3 908 125 25-1, (2000).
24H. Schiefer, and W.W. Seelentag, “Results of the Pilot study to the IMRT dose intercomparison 2008,”
SGSMP Bulletin 2/2008 66, 14-16 (2008).
Online: http://sgsmp.ch/bullA82.pdf
25S.A. Davidson, R.A. Popple, G.S. Ibbott, D.S. Followill, “Technical note: Heterogeneity dose
calculation accuracy in IMRT: study of five commercial treatment planning systems using an
anthropomorphic thorax phantom,” Med Phys. 35, 5434-5439 (2008).
26F. Hasenbalg, H. Neuenschwander, R. Mini and E.J. Born, “Collapsed cone convolution and analytical
anisotropic algorithm dose calculations compared to VMC++ Monte Carlo simulations in clinical cases,“
Phys. Med. Biol. 52, 3679-3691 (2007).
27S. Baxi, E. Park, V. Chong, H.T. Chung, “Temporal changes in IMRT contouring of organs at risk for
nasopharyngeal carcinoma - the learning curve blues and a tool that could help,” Technol. Cancer Res.
Treat. 8(2), 131-140 (2009).
28L.K. Schubert, D.C. Westerly, W.A. Tomé, M.P. Mehta, E.T. Soisson, T.R. Mackie, M.A. Ritter, D.
Khuntia, P.M. Harari, and B. R. Paliwal, “A comprehensive assessment by tumor site of patient setup
using daily MVCT imaging from more than 3,800 helical tomotherapy treatments,” Int. J. Radiat. Oncol.
Biol. Phys. 73(4), 1260-1269 (2009).
29A. Brahme, P. Nyman, and B. Skatt, „4D laser camera for accurate patient positioning, collision
avoidance, image fusion and adaptive approaches during diagnostic and therapeutic procedures,” Med.
Phys. 35(5), 1670-1681 (2008).
30H. Schiefer, F. von Toggenburg, W.W. Seelentag, L. Plasswilm, G. Ries, H.P. Schmid, T. Leippold, B.
Krusche, J. Roth, and D. Engeler, “Topological methods for the comparison of structures using LDR-
brachytherapy of the prostate as an example,” Phys. Med. Biol. 54, 4959-4970 (2009).
17








![Clinical Implementation of a 3D Dosimeter for Accurate IMRT and … · [10] for multi-institutional comparison of IMRT dosimetry were used for this investigation. Gamma pass rates](https://img.pdfslide.net/doc/110x75/5f55fbeabba14e48d36a07e7/clinical-implementation-of-a-3d-dosimeter-for-accurate-imrt-and-10-for-multi-institutional.jpg)