Embed Size (px)
Citation preview

Climcal Radtology (1985) 36, 553-559 © 1985 Royal College of Radiologists
The Technology of Magnetic Resonance Imaging M. A. SMITH
NMR Imaging Unit, University of Edinburgh, Royal Infirmary, Edinburgh
000%9260/85/569553502 O0
In the clinical use of magnetic resonance imaging (MRI) it may be more important to understand some of the technical aspects of the imaging technique, rather than the fundamental physical principles. This review, therefore, sets out to present the essential aspects of the technique, including T~ and T2 relaxation times in rela- tion to biological tissue, MRI equipment, pulse sequences, factors affecting image quality and patient throughput.
The application of nuclear magnetic resonance (NMR) in medicine has been hailed as a major innovation. Although NMR is relatively new in the field of medicine, the technique itself has been in use for nearly 40 years. However, it was not until the early 70s that NMR was considered as an imaging technique. Nuclear magnetic resonance imaging, or magnetic resonance imaging (MRI) as it has more recently become known, was developed over the subsequent 10 years by research groups and commercial companies until the first com- mercial MRI systems became available in the early 1980s.
The fundamental physical principles of NMR and the methods of image production have been described pre- viously in several publications (Fullerton, 1982; Pykett, 1982; Smith, 1984) and will not be dealt with in this article. Instead, a more 'black box' approach is adopted which recognises the school of thought that may be summarised by the phrase 'you don't need to know how a carburettor works in order to drive a car'. This article describes the essential scientific and technical aspects of MRI which should be understood by the clinician using the technique.
SUMMARY OF THE PHYSICAL PRINCIPLES
The term nuclear magnetic resonance gives an indica- tion of the basis of the technique. It is the nucleus of the atom and its ability to resonate under certain conditions in the presence of a magnetic field with which we are concerned. There are two quite separate stages in the NMR process.
1 The patient is placed in a strong magnetic field and is then exposed to an oscillating magnetic field in the radio-frequency (RF) region of the electromagnetic spectrum, which causes the nuclei in the subject to resonate about their equilibrium position.
2 The RF radiation is then switched off but the nuclei continue to resonate, resulting in the second stage, the emission of RF radiation from the resonating nuclei within the subject which can be detected as an
NMR signal. The nuclei eventually return to their original equilibrium position.
There is, therefore, a philosophical difference between NMR and other radiographic techniques. In the latter, the body interacts with a beam of X-rays, attenuating the beam. This is not so with NMR. The RF radiation transmitted through the patient is not attenu- ated; it stimulates the tissue itself to produce a signal. The frequency at which nuclei resonate is directly pro- portional to the magnetic field strength and is referred to as the resonant frequency or Larmor frequency.
The resonance of the nuclei within a sample is a complex phenomenon with two principal components, characterised by T I and T 2 relaxation times. These are time constants relating to the exponential decay of two components of resonance. Alternative names for T1 and T 2 are spin-lattice and spin-spin, respectively. There are a number of nuclei whose properties enable them to be measured by NMR, but it is the combined sensitivity and abundance of hydrogen which makes MRI possible. For a fixed volume within the human subject, the NMR signal from hydrogen will be in the region of 105 times stronger than from 3~p. As the hydrogen nucleus con- tains a single proton, the term proton density is used to describe the distribution of resonating nuclei within the patient.
T 1 AND T 2 RELAXATION TIMES
Although some tissues may have a high T 1 and T~ or a low T~ and T2, there is no direct relationship between the two relaxation times. The following, however, is always true:
TI>T2 Both T 1 and T 2 are measured in milliseconds (ms), with T 2 around an order of magnitude smaller than T~ in most tissues.
Despite the fact that the NMR signal detected in MR1 comes from protons within the body, not all protons produce a signal. Protons giving rise to an NMR signal are mainly those in lipid and cellular water, the latter constituting by far the greatest proportion of protons in the body. The protons in macromolecules, such as pro- teins, DNA and solid structures such as bone, do not usually contribute to the NMR signal. As the majority of the NMR signal will come from water within the tissues, it is largely the behaviour of this water which determines the values of T~ and T 2 in MRI.
The biological mechanisms which influence T~ and T 2 relaxation times are not yet fully understood; however, it is generally accepted that the concept of free and bound water gives the best understanding of variations

554 CLINICAL RADIOLOGY
in T 1 and T2, although it may be, to some extent, an oversimplified model. A proportion of the water in tissue is bound to the surface of proteins and, in conse- quence, its motion is slowed by proximity to the large molecules. This results in a lowering of the T~ value, Other water in the tissue will not be bound to protein and is considered to be free, resulting in a higher T~. The T; of pure water, equivalent to free water in the tissue, is of the order of 3 s. T~ in tissue is much lower than this and will depend on the relative proportions of free and bound water within the tissue: the larger the proportion of free water, the higher the T1; the larger the propor- tion of bound water, the lower the T~. It is generally assumed that the increase in T~ in tumour tissue com- pared with normal tissue is due to a release of bound water, resulting in an increase in free water.
The effect of magnetic field strength on the two relax- ation parameters is different. As the strength of the magnet used for MRI is increased, the resonant fre- quency also increases. As the resonant frequency increases, so T~ increases. It is, therefore, not possible to quote the T; value for a particular tissue without stipulating the frequency at which it was measured. This causes considerable difficulties in comparing in vivo tissue measurements on patients using different MRI systems, as different field strengths are often used. Grey matter, for example, will have a T; of around 400 ms in a low-strength magnetic field increasing to over 800 ms in a high-strength magnetic field.
Compared with the large variation in T, with field strength, there is little variation in T 2 and most biological tissues have a T 2 value in the range of about 50-150 ms. T 2 in free water is also longer than that in bound water, resulting in an increase in T 2 in lesions which have more free water than normal tissue.
A great deal of work, particularly in vitro, has been done on the quantitation of T~ and T2, which has been reviewed recently (Mathur-De Vr6, 1984). The clinical value of obtaining an accurate estimate of the T~ or T 2 value of a particular tissue is a subject of debate. Many MRI systems do not obtain a quantitative value of the relaxation parameters but rely on a qualitative assess- ment of the relative differences between the tissues.
MAGNETIC RESONANCE IMAGING EQUIPMENT
Magnet
The largest item of hardware in the MRI system is the magnet which produces the constant magnetic field. The choice of magnet is dependent on a variety of considera- tions, but all must produce a stable, uniform magnetic field throughout a slice or volume large enough to con- tain the appropriate region of the human body. The strength of magnetic field used for MR1 varies from 0.02 T up to 2.0 T (1 T = I Tesla=10 000 gauss). There are three types of magnets: resistive, permanent and superconducting.
A resistive magnet usually consists of four ring mag- nets. Electricity is continually applied to these magnets, which generate a magnetic field perpendicular to the plane of the ring magnets. The electrical energy used to create the magnetic field is dissipated as heat and so resistive magnets must be continually cooled, usually with circulating water. A magnet with a field strength of
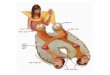
0.1 T uses approximately 30 kW of electricity. The orientation-of the ring magnets used in resistive MRI systems can be either vertical, so that the patient enters through the centre of the rings (Fig. 1), or horizontal, so that the patient enters between, and parallel to, the central pair of ring magnets.
Rmg Gradlent mQ, oet co~[ RF co~k
I Fig. 1 - Line diagram of a horizontal field resistive lmager with four vertical ring magnets The RF saddle coil fits closely round the pahcnt The gradient coils are at tached around the outside of the cylinder which forms the bore of the imager.
Field strengths above 0.2 T are impractical when using resistive magnets because of the problems of heat dis- sipation and thermal instability. For field strengths above 0.2 T superconducting magnets must be used. Superconducting (or cryogenic) magnets utilise the pro- perty that at very low temperatures electrical resistance is reduced to zero. In a resistive magnet heat is gener- ated in overcoming the resistance of the conducting material within the coils: if the resistance is zero it therefore follows that heat dissipation will also be zero. The ring magnets of a cryogenic magnet are maintained at 4 K using liquid helium, the low temperature being maintained by an additional layer of liquid nitrogen. At the temperature of liquid helium the windings of the coils have zero resistance and so if an electric current is applied, it continues to circulate within the coils after the source is removed. Thus, once an electric field is gener- ated and the low temperature maintained, a constant stable magnetic field is maintained without the need for a continual supply of electricity. The savings in electricity costs, however, are more than balanced by the cost of liquid helium and liquid nitrogen (referred to as cryogens) which boil off continually and must be replenished at regular intervals. If the resistance of a coil rises above zero the circulating electric current will immediately be dissipated as heat, causing some of the cryogens to boil off rapidly and the magnetic field to disappear. This process is known as quenching.
A permanent magnet is an attractive proposition for MRI because of the absence of the costs for electricity and cryogens. Permanent magnets are constructed on site from small blocks of magnetic material. Details of the three different types of magnet systems used in MRI are listed in Table 1.

THE TECHNOLOGY OF MAGNETIC RESONANCE IMAGING 555
Table 1 - Magnets used for MRI
Magnet type FwId ~trength (T)
Resistive 0.02-0.15 (low)
Permanent 0.3 (medium)
Cryogenic 0 15-0.6 (medium)
Cryogenic >1.5 (high)
Advantages
Lower capital, installation and running costs than cryogemc systems. Better T 1 contrast at lower field strength. Can be installed in sites with difficult access
Very low fringe field Low running costs
Spatial resolution increases as field strength increases. Intrinsically stable magnetic field Easier to shim than resistive magnet
As above but further increase in spatial resolution. 31p spectroscopy
D&advantages
Feedback systems often required to maintain magnetic field stability
Weight
Z l contrast decreases as field strength increases. Cost increases as field strength increases
Further decrease in T~ contrast and increase in cost. Biological effects of MRI, such as RF heating, become a consideration
Radio-frequency coils
Radio-frequency coils are an arrangement of a loop or loops, not necessarily circular, of copper ribbon or pipe which transmit the RF radiation to induce resonance within the patient and also detect the emitted RF radia- tion from the resonating nuclei. Separate RF coils can be used as an RF transmitter and receiver but, because the events occur separately, the same coil can be used for both.
There are two main types of RF coil. In MRI systems with a superconducting magnet or a resistive magnet with a horizontal field, saddle coils are used (Fig. 1). As the name suggests, they arc saddle-shaped and fit closely around the contours of the patient. Magnetic resonance imaging systems using a permanent magnet or a resistive magnet with a vertical field often use a solenoid RF coil, which surrounds the patient. At lower magnetic field values a solenoid RF coil has the advantage over a saddle coil of a higher signal-to-noise ratio.
The third type of RF coil is a surface coil, which is simply a circular loop, the diameter of which is deter- mined by the region of the body to be imaged. The surface coil is placed on the surface of the region of interest, perhaps the eye or over the spine, and a limited
retrigeration : unit
t Power supp!y ~,
'- I I I N M R I
I i probe. I I
' m a g n e t I I
~ J gradient L ~ X , Y and Z 1 J '1 I gradients ] ~_J - lamplifiers
CO~uter
L . -~ ~ ,,91
Fig. 2 - Block diagram of an MRI system The dotted boxes indicate equipment present only in resistive systems and the dashed box indi- cates the equipment present in the lmager around the pahent .
region may be imaged with fairly high spatial resolution. However, the body can only be imaged to a limited depth which is directly related to the size of the RF coil.
Magnetic Gradients
Images are produced in MRI by varying the magnetic field experienced by the patient in a controlled manner. This is done by maintaining the main magnetic field at a fixed level and applying a much smaller magnetic field, the magnitude of which can be changed rapidly. The direction of the gradient field is always parallel to the main field, the two fields adding together. The variation in magnetic field produced by a magnetic gradient is approximately 1% of the main magnetic field. Magnetic field gradients are generated in the three orthogonal co-ordinate directions by electrical windings which sur- round the central bore of the MRI system. The sound that can be heard from an MRI system comes from the movement of the gradient coils as they are switched on and off during image acquisition.
Imaging System
A block diagram of an MRI system is shown in Fig. 2 and an illustration of a system in Fig. 1. The RF pulses are applied and the gradients switched on and off so that a number of different NMR signals are produced, usually 64, 128 or 256, and recorded in a computer. Generally, spatial information is stored in the phase and frequency of each signal and a two-dimensional Fourier transform (2DFT) of all the signals produces an image. The image is stored in a matrix of 128× 128,256×256 or 512×512 pixels.
Environment
The presence of a strong magnetic field in MRI results in environmental problems which are quite different from those of other radiological techniques. The magne- tic field can pose a hazard to patients with a cardiac pacemaker or recent aneurysm clips and can cause small items like scissors or screwdrivers to become projectiles which travel into the bore of the magnet at a high velocity. It can also result in the loss of magnetically stored information on items such as credit cards. Because MRI systems rely on a stable, uniform magne- tic field, the presence of moving ferromagnetic material

556 CLINICAL RADIOLOGY
within its environment can degrade the image quality. The effect of moving ferromagnetic objects will be rel- ated to their size and distance from the magnet. During the planning of an MRI installation the distance of items such as lifts and cars would be taken into consideration.
PULSE SEQUENCES
In MRI a sequence of RF pulses is used to produce the data from which an image can be constructed. The value of each pixel in the image will be influenced by the following:
1 proton density, 2 TI relaxation, 3 T 2 relaxation, 4 movement (flowing blood) and 5 timing of pulse sequence used.
In static tissue with a particular pulse sequence the pixel value will be determined by the proton density, T~ and T 2 of the tissue. The choice and timing of the pulse sequences is often under the operator's control and can be chosen to increase or decrease the proton density, T1 or T= contribution to the image in order to obtain the maximum difference in signal intensities between nor- mal and abnormal tissue on the image, i.e. to optimise the tissue contrast.
The two types of RF pulses used in MRI are called 90 ° and 180 ° pulses. The angle refers to the change in direction of the magnetic moment of the individual nuclei following the RF pulse. When used, it is the position and timing of the 180 ° pulse with respect to the 90 ° pulses which determines the amount of T~ or T 2 in the signal. There are three main pulse sequences used in MRI: saturation-recovery (sometimes referred to as partial saturation or repeated FID), inversion-recovery and spin-echo.
Saturation recovery
This is the simplest pulse sequence; 90 ° RF pulses are repeatedly applied to the patient and the NMR signal is measured after each pulse. The repetition time or time between the pulses is referred to as TR (Fig. 3). If TR is relatively long, perhaps 3 or 4 times the T 1 of the sample, then all the nuclei have sufficient time to return to equilibrium before the next RF pulse. The amplitude of the NMR signal after each pulse, therefore, contains only proton density information. If, however, the pulse repetition time TR is much shorter, for example, approximately equal to the T 1 of the sample, then the nuclei do not have sufficient time to return to their equilibrium position before the next RF pulse. The amount by which they have failed to return to equilibrium will depend on the T~ of the sample. Thus, the intensity of the image will contain information about the T 1 of the sample as well as the proton density, provided TR is short compared with T~.
The amplitude of the NMR signal in the saturation- recovery sequence will be a function of proton density, TR and T~. TR is the only variable in this sequence and it can be altered so that more or less T 1 information is contained in the signal. The faster the repetition time, i.e. the shorter the TR, the smaller the NMR signal becomes and the more T1 information it contains. If, however, the pulse repetition time is reduced too much the signal becomes so small that the quality of the final image is severely degraded.
Inversion-recovery
The principle of inversion-recovery is very similar to that of saturation-recovery with a short TR. In both sequences the nuclei are not allowed sufficient time to return to equilibrium before the 90 ° pulse is applied. The difference in inversion-recovery is that the nuclei are
9o., TR {
Saturation recovery
i BO* I 90*1/~
I. TR
1Bo° I 90.1/~ Inversion recovery
,80.1 90* 90" I H Uv"'~
'TR I
",v yv ' - Spin echo
Fig, 3 - RF pulses, NMR signals and corresponding timing intervals in the three standard pulse sequences. TR is the repeti t ion time for each pulse or pair of pulses in all three sequences. TI is the time from inversion m the inversion-recovery sequence and TE is the time to echo in the spin-echo sequence.

THE TECHNOLOGY OF MAGNETIC RESONANCE IMAGING 557
caused to resonate by a 180 ° pulse prior to the 90 ° pulse so that the nuclei are not at equilibrium when the 90 ° pulse is applied. Again, the extent by which the nuclei have failed to return to equilibrium is reflected in the amplitude of the signal and will depend on the T 1 of the tissue in that region. The time delay between the 180 ° and the 90 ° pulses determines the amount of T~ informa- tion contained in the amplitude of the NMR signal, just as the time between successive 90 ° pulses does in the saturation recovery sequence. The time between the 180 ° and the 90 ° pulse is referred to as TI (time from inversion) or sometimes as r (tau).
The amplitude of the NMR signal is a function of the proton density, T 1, TR and TI. Although both of the last two variables influence the T~ contribution in the final signal, it is generally only TI which is changed. T 1 contrast in a clinical image is demonstrated much better by the inversion-recovery sequence than with the satura- tion-recovery sequence.
Spin-echo
The spin-echo pulse sequence produces a signal in which both T 1 and T 2 contribute to the signal amplitude. Athough it contains information about T1 and T 2 it is principally to obtain T 2 information that it is used in clinical investigation. A typical spin-echo sequence used for clinical imaging is illustrated in Fig. 3. The time between the 90 °, 180 ° pulse combination is TR and determines the T~ contribution in the signal. The time between the 90 ° and the signal is designated as TE (time
short T 1 tong T 1
short TR
to echo) and the larger this value, the greater the T 2 contribution in the signal.
The intensity of the image is, therefore, influenced by the variables proton density, T 1, T2, TR and TE. The length of the delay TE is slightly less than an order of magnitude smaller than the delay TI in the inversion- recovery pulse sequence.
Effect of Pulse Sequence Timing on Image
It is important to understand how the timing values TR, TE and TI can affect the relative contributions of proton density, T 1 or T 2 in the NMR image. Some MRI systems use a fixed pulse sequence and obtain a T 1 image. Most systems, however, give the operator the option of choosing the timing values TR, TE and TI, depending on the pulse sequences used, so that the maximum contrast between the particular tissues of interest is obtained. This presupposes that the T 1 and T 2 value of the tissues may be anticipated so that the timing can be chosen to produce optimum contrast. Values of TR vary from 200 ms to 3000 ms, with the majority of scans being performed with values between 1000 ms and 2000 ms. Values of T! vary from 200 ms to 1200 ms and values of TE vary from 10 ms to 80 ms.
The amplitude of the NMR signal and, hence, the intensity of any region of an image will contain different amounts of proton density, T~ and T 2 information, depending not only on their respective values but also on the timing of the pulse sequence used. The relative contributions of these three parameters can be repre- sented using a pie diagram in which the respective sizes of the segments represent the relative contributions to the intensity of the image. Pie diagrams are illustrated in Fig. 4 for short and long Tj and T 2 and short and long TR, TE and TI in the three main pulse sequences.
It is common to quote the sequence timing for any clinical image as an abbreviation indicating the pulse
(ong TR
Soturahon Recover K
short T 1
proton density [] T1 •
long T 1
/~-~shorf T 1 ~.~ (f~long q ~ short T 2 long T 2 short T 2 long T 2
short TR
® short TI
(ongTl ~ ~
[nversmn Recover~ proton density []
T 1 •
~ s h o r f T E ~ ~ ~ ~
~ong Y#
LI°ngTE ~ ~ ~ ~
Spin Echo proton denstty [] T 1 • T 2 [] Fig. 4 - Pie diagrams showing the relative contributions to the image plxel value from proton density, T1 and T2. The proton density remains constant and the effect of short and long TR, TI or TE on tissue with a long or short T1 or T2 is shown. For example, the image pixel value will contain mainly Tz information if the tissue has a short T2 in a spin-echo sequence with a long TR and TE. However, the pixel value will contain mainly T1 information if the tissue has a long T1 in an inversion-recovery sequence with a short T1. The pixel value will contain almost all proton density information if the tissue has a short T~ in both a saturation-recovery sequence with a long TR and a spin-echo sequence with a long TR and short TE.

55g CLINICAL RADIOLOGY
sequence followed by two or three numbers, the timing always being quoted in milliseconds and, generally, in a specific order. Examples and explanations of this con- vention are given below.
SRl400 Saturation-recovery sequence: TR= 1400 ms SE16oo,% Spin-echo sequence: TR=1600 ms,
TE=56 ms IRlsoO4oo Inversion-recovery sequence: TR=1500 ms,
TI=400 ms IR2ooo,soo,~ o Inversion-recovery sequence with a further
180 ° pulse soon after the 90 ° pulse to produce an echo: TR=2000 ms, TI=500 ms, TE=30 ms
FACTORS AFFECTING MAGNETIC RESONANCE IMAGE
Signal-to-noise Ratio
In all imaging techniques there is an element of ran- dom noise, which degrades the information available from the signal in which we are interested. The signal- to-noise (S/N) ratio of MRI significantly influences the spatial resolution of the image. The spatial resolution determines the amount of fine detail that can be observed. To obtain good spatial resolution it must be possible to detect very small differences in the frequency of the NMR signal. Any noise which is present in the signal is at relatively high frequencies, which makes the detection of small frequency differences within the sig- nal more difficult and, hence, the spatial resolution is degraded. Although many aspects of the S/N ratio of an MRI system are a function of the system itself and are outwith the operator 's control, there are a number of factors which can be influenced.
(a) Section Thickness
When a section is acquired the noise detected is con- stant and the signal will be influenced by the thickness of the section; the wider the thickness, the larger the sig- nal. Consequently, signal-to-noise ratio can be reduced to an unacceptable level if the slice thickness chosen is too narrow.
(b) Signal Averaging
A magnetic resonance image is constructed from a number ot different NMR signals. If the number of signals is increased, for example, whereas a single signal may have been acquired, four signals are now acquired and an average taken; the signal-to-noise ratio is increased by a factor of two. The penalty, however, for the higher spatial resolution would be, m thts example, a four-fold increase in acquisition time for a single section.
Contrast
The contrast of an NMR image refers to the difference in signal intensity between different tissues in the image. The contrast between different tissues in MRI is much greater than is present in X-ray computed tomography (CT). Most MRI systems will have inferior spatial resolution to X-ray CT scanners but much better tissue contrast. The ability to perceive an abnormality is always a function of both spatial resolution and contrast but it is important to remember that, in MR1, contrast is as important, possibly more so, than spatial resolution.
Magnetic Field Strength
One question which has been frequently debated in the last couple of years is that of the optimum field strength for MRI. The inherent spatial resolution of the system will improve as the field strength of the magnet is increased due to improved S/N ratio. This fact and the possibility of phosphorus spectroscopy have been important factors in the decision to pursue high-field- strength MRI systems. Set against this is the fact that T~ increases as the field strength increases and the separa- tion between T~ values of different tissues decreases, resulting in a reduction in contrast. Thus, low-field- strength systems have superior contrast in addition to being cheaper to purchase, install and run. However, the ability to detect abnormal pathology is a combina- tion of both the contrast betwen the lesion and the surrounding tissue and the noise which is present in the
A A
sI(ces
A B C 0 A B C
ABCD
Fig. 5 - In smgle shce imaging, sufficient time is left between the NMR sxgnals to allow the nuclei to return to eqmhbrmm In simultaneous shce acquisition the delay between the signals from Slice A is used to produce resonance in other shces (B, C and D). Using this techmque It is possible to ~magc many slices in the same time as had previously been taken to tmage just one.

THE TECHNOLOGY OF MAGNETIC RESONANCE IMAGING 559
image. Thus, in MR1 the contrast/noise ratio is often considered when comparing systems of different field strengths.
The underlying problem in trying to find the opt imum field strength for M R I is the fact that it may not even exist. There may, in fact, be no opt imum field for MRI. In some clinical applications it may be more important to have high spatial resolution without tissue contrast, whereas in others it may be more important to have acceptable spatial resolution but with higher tissue contrast. There may, therefore, be as many 'op t imum fields' as there are clinical applications for MRI.
Movement
As with all radiological techniques, patient movement will degrade the image. The mathematical technique of two-dimensional Fourier transform used for image pro- duction in M R I can tolerate a larger degree of patient movement than the back-projection method used in X-ray CT. Patient movemen t does not simply blur the image but produces faint multiple superimposed images (aliasing) in one dimension.
PATIENT THROUGHPUT
The imaging time taken to acquire a single section is a function of the pulse sequence, the resolution required and possibly the number of different pulse sequences
used. Scan times vary from about 15 s for a low-resolu- tion saturat ion-recovery image, which contains suffi- cient information for patient positioning, to 30-40 min for a high-resolution inversion-recovery image with a number of signal averages. Patient throughput can be increased using simultaneous slice acquisition, often called multiple slice acquisition (Fig. 5). In this tech- nique, during the time that the nuclei in one section are returning to equilibrium, resonance is induced in a num- ber of other sections, Thus, though the imaging time per section is not increased, as many as 16 sections can be imaged in the same time that it had previously taken to image a single section.
Acknowledgements. I would like to thank Professor Jonathan Best for comments during the preparanon of this article. I am grateful to Mrs C. N. Rowan for secretarial servmes and to Mtss J. Dyer for preparing the illustrations. Parts of this article appear courtesy oi Hememann Medical Books, London Fundmg from the MRC is acknowledged
REFERENCES
Fullerton, G D. (1982). Basic concepts |or nuclear magnetic reso- nance imaging. Magnetic Resonance lmagmg, 1, 39-55
Mathur-DeVrd,R. (1084) Reviewartlcle. Blomedicalimphcationsof the relaxation behaviour of water related to NMR tmaglng British Journal of Radzology, 57, 955-976.
Pykett, I L. (1982). NMR imaging in medicine. Sctentzfic American, 246, 78-88.
Smtth, M A. (1984). NMR imaging in medminc: an introduction to the physical principles Parts I and II. Ra&ology Now, 1(2), 4-6; 1(3), 3-5.
49