Embed Size (px)
DESCRIPTION
The toxicology of NMP (What adverse effects might we expect from exposure to NMP). Professor Ken Donaldson ELEGI Colt Laboratory Centre for Inflammation Research, Edinburgh University, Medical School, Edinburgh , Scotland. What diseases do particle cause or worsen?. - PowerPoint PPT Presentation
Citation preview

The toxicology of NMP
(What adverse effects might we expect from exposure to NMP)
Professor Ken Donaldson
ELEGI Colt Laboratory
Centre for Inflammation Research,
Edinburgh University, Medical School,
Edinburgh , Scotland

Site Setting Disease Exemplar particlesAirways Occ/Env Bronchitis Coalmine dust, organic dust, PM10
Occ Small airways disease Coalmine dust, quartz
Occ Sensitisation/asthma Metals, organic dusts
Occ/Env Lung cancer Quartz, metals, asbestos, PM10
Env Exacerbations of airways disease – COPD and asthma
PM2.5
Parenchyma Occ Emphysema Coalmine dust, quartzOcc Silicosis (pneumoconiosis)-
nodular fibrosisQuartz, coalmine dust
Occ Asbestosis (pneumoconiosis)- interstitial fibrosis
Fibres
Occ Progressive massive fibrosis Silicosis (pneumoconiosis)- nodular fibrosis
coalmine dust
Pleura, peritoneum Occ Mesothelioma FibresCardiovascular system Env Atherothrombosis PM2.5
What diseases do particle cause or worsen?
Parenchyma – pink alveoli
Airways – white bronchial tubes
Pleura – outside surface lung surface and chest wall surface
Cardiovascular system – blood vessels and heart

Typical particles - Silica, asbestos, welding fume, nuisance dusts
Exposure – High (mg/m3 analogous to workplace) –peaks during shifts , zero at other times
Exposed population - Predominantly healthy males <65 years old – no susceptibles due to healthy worker effect
Typical responses - Pneumoconiosis, COPD, cancer, asthma
If NMP have effects based on the occupational paradigm?

If NMP had effects based on the environmental (PM10) paradigm?
Exposure to - urban PM10 containing combustion-derived nanoparticles
Exposed population - Everyone but acute effects are only seen in susceptible and aged, ill populations with pre-existing oxidative stress and inflammation = susceptibility
Exposure - Low (tens of ug/m3 as per urban environment) constant with peaks
Typical responses – In susceptible populations - Exacerbations of COPD/asthma, exacerbations of cardiovascular disease, cancer
In normals – very little except likely contribution to chronic disease

Factors contributing to toxic response to particles in the lungs
Intrinsic toxicity of the material i.e. hazard
Exposure concentration
Length of exposure
Contribute to dose
Variable but low for NMP??
For NMP could be chronic or brief
Generally low for NMP but exceptions e.g. quartz, metals

General scheme for what happens when harmful particles deposit in the lungs
Total deposited
doseBiologically
effective dose
Normal tissue
Exposure
Tissue stress
Clearance
Inflammation oxidative damage genotoxicity etc
DiseaseThreshold not
exceededThreshold exceeded
Defences induced
Macrophage clearance
Muco-ciliary and macrophage clearance
Tissue injury
Total deposited
doseBiologically
effective dose
Normal tissue
Exposure
Tissue stress
Clearance
Inflammation oxidative damage genotoxicity etc
DiseaseThreshold not
exceededThreshold exceeded
Defences induced
Macrophage clearance
Muco-ciliary and macrophage clearance
Tissue injury
That fraction of the total dose that actually
delivers toxicity

Current metricBiologically effective doseParticle
Nuisance dust standard of respirable mass
Surface areaCarbon black (NP)
Respirable mass Area of reactive (unblocked or unpassivated) surface
Quartz
Fibres longer then 5m, >3m diameter and Aspect Ratio>3
Biopersistent fibres longer than ~ 20m
Asbestos
Respirable massSoluble transition metals Welding fume (NP)
Contained in PM10Organics/metals/surfacesDiesel soot
Mass by PM10 conventionOrganics/metals/surfacesPM10
We are not good at measuring the BED in our metrics

The central hypothetical role of inflammation in the occupational paradigm
Inflammation
Occupational particles
COPD,
Airways inflammation
Pneumoconiosis,
Stimulation of fibroblast growth
and ECM secretion
Cancer
Oxidative adducts of DNA
Asthma
Airways inflammation/ adjuvant effect

Inflammation
PM10
Superimposed on Airways inflammation of Asthma, COPD
Exacerbation Hospitalisation
Death (COPD)
Increased inflammatory activity in plaques
Atheromatous plaque formation is an inflammatory process
Plaque rupture
Myocardial infarction
thrombosis
Mortality
The central hypothetical role of inflammation in the environmental paradigm
Endothelial dysfunction
Pro-thrombotic state

Toxicology testing approaches
Approach depends on aim - screening, mechanisms, regulatory
NMP studies will be screening and mechanisms
1) Characterising the physico-chemistry – surface area, size etc, metals – aiming towards a structure:activity paradigm?
2) In vitro cell-free – e,g detecting free radical –generation, complement activation etc
3) In vitro cells – huge number of endpoints but should be pathophysiologically-relevant i.e. tells us about something we already understand as having a role in disease e.g. ability to cause a pro-inflammatory effect
4) In vivo- particle are instilled into or inhaled by rodents - lungs are then examined for effects (huge number of potential endpoints)

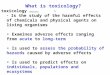
Example of an inhalation study with a NMP – Montserrat ash
The importance of using controls to contextualise the response
0
5
10
15
20
25
0 20 40 60
Lung burden (mg)
PM
N (
mill
ion
s)
Ash
TiO2
0
5
10
15
20
25
0 20 40 60
Lung burden (mg)
PM
N (
mill
ion
s)
Ash
TiO2
Rats inhaled ash along with a control dust TiO2 that is low in toxicity – at the same mass burden the ash was more inflammogenic as shown by more PMN in the lavage
0
25
50
75
100
125
0 10 20 30 40 50Mass burden (mg)
PM
N (
x106
)
volcanic ashTiO2
coalmine dusts L and A
quartz
0
25
50
75
100
125
0 10 20 30 40 50Mass burden (mg)
PM
N (
x106
)
volcanic ashTiO2
coalmine dusts L and A
quartz
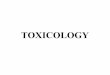
However, when plotted alongside particles of known toxicity, the ash was less than coalmine dust and quartz (see vertical axes).

PM2.5AtherothrombosisEnvCardiovascular systemFibresMesotheliomaOccPleura, peritoneum
coalmine dustProgressive massive fibrosis Silicosis (pneumoconiosis)-nodular fibrosis
Occ
FibresAsbestosis (pneumoconiosis)-interstitial fibrosis
Occ
Quartz, coalmine dustSilicosis (pneumoconiosis)-nodular fibrosis
OccCoalmine dust, quartzEmphysemaOccParenchyma
PM2.5Exacerbations of airways disease – COPD and asthma
EnvQuartz, metals, asbestos, PM10Lung cancerOcc/EnvMetals, organic dustsSensitisation/asthmaOccCoalmine dust, quartzSmall airways diseaseOccCoalmine dust, organic dust, PM10BronchitisOcc/EnvAirwaysExemplar particlesDiseaseSetting Site
PM2.5AtherothrombosisEnvCardiovascular systemFibresMesotheliomaOccPleura, peritoneum
coalmine dustProgressive massive fibrosis Silicosis (pneumoconiosis)-nodular fibrosis
Occ
FibresAsbestosis (pneumoconiosis)-interstitial fibrosis
Occ
Quartz, coalmine dustSilicosis (pneumoconiosis)-nodular fibrosis
OccCoalmine dust, quartzEmphysemaOccParenchyma
PM2.5Exacerbations of airways disease – COPD and asthma
EnvQuartz, metals, asbestos, PM10Lung cancerOcc/EnvMetals, organic dustsSensitisation/asthmaOccCoalmine dust, quartzSmall airways diseaseOccCoalmine dust, organic dust, PM10BronchitisOcc/EnvAirwaysExemplar particlesDiseaseSetting Site
Summing up- toxicology of NMP
•Particle toxicology is a mature science- we know what to do …but…
•Does NMP as a grouping make sense?
•Coalmine dust, quartz and asbestos are NMP but they are looked on as occupational diseases
•Do we have a disease from environmental exposures to NMP?
•How many people are at risk – in UK?, in Europe? In the world?
•What is the documented burden of ill-health due to environmental exposures to NMP?
•Only if there is a recognition that environmental exposures to NMP constitute a substantial health risk will funding be diverted from other known substantial heath risks
…….Discuss