Embed Size (px)
Citation preview

H U M A N G E N E T H E R A P Y 6:927-939 (July 1995) Mary Ann Liebert, Inc.
Clinical Protocol
The Treatment of Ovarian Cancer with a Gene Modified
Cancer Vaccine: A Phase I Study
INVESTIGATORS: Scott M. Freeman, M.D. (P.I.) Craig McCune, M.D. William Robinson, M.D. Camille N. Abboud, M.D. George N. Abraham, M.D. Cynthia Angel, M.D. Aizen Marrogi, M.D.
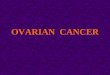
THE TREATMENT OF OVARIAN CANCER WITH A
DAYl GENE-MODIFIED CANCER VACCINE:
A PHASE I STUDY
Eligible
Stage I, n, or m. Ovarian Cancer
Patients Who Have Completed E DAY 2 Surgery and Chemotherapy
Evidence of Residual Disease By Tumor Marker or Imaging Must be Present
Goals
E
N
T
E
R
~*"
I. To evaluate the safety and side effects of treatment with a gene-modified Ovarian Cancer Vaccine which is adminstered inttaperitoneally and activated by ganciclovir
2. To determine a maximum cell dose of the vaccine which can safely be administered inttaperitoneaUy.
3. To evaluate the immunologic response to this vaccine program.
4. To observe for clinical effects on the residual ovarian cancer.
Intraperitoneal Infusion of Gene-Modified Ovarian Cancer Cells
Ganciclovir, 5 mg/kg, BID, IV for 7 day
D A Y 22
R E P E A T
C Y C L E
— •
D A Y 43
R E P E A T
C Y C L E
Gene-Modifled Ovarian Cancer Vaccine
The Ovarian Carcinoma CeU Line, PA-1, has been transduced to express the Herpes Simplex Virus Thymidine Kinase, PA-1-STK.
Vaccine Dosage and Administration: A cell dose escalation plan will be followed with each patient such that a higher dose is given with repeat cycles. The assigned dose of cells will be prepared, radiated and administered through an inttaperitoneal catheter in 1000 cc of normal saline.
3.0 Introduction
3.1 Overall status of treatment of ovarian cancer There are approximately 19,000 new cases of and 12,000
deaths from ovarian cancer each year (I). Mortality from ovarian cancer accounts for 6% of cancer deaths in females, and ap
proximately 5 0 % of gynecological maUgnancies (I). Ovarian cancer is staged into foitt categories: Stage I—growth Unuted to ovaries. Stage n—growth involving one or more ovaries with pelvic extension. Stage HI—tomor extending outside die pelvis and/or rettoperitoneal or inguinal node involvement, and Stage IV—distant metastasis outside the peritoneal cavity. The fu-st
Tulane University Medical Center, University of Rochester Medical Center
927

928 CLINICAL P R O T O C O L
three stages can be divided into three substages of more progressive disease (a-b-c).
Patient survival can be evaluated based on the stage of the disease at diagnosis. Higher stage disease conelates with a worse prognosis. Treatment of ovarian cancer is based on the stage of the disease. Higher stages of disease are tteated more aggressively. Stage I disease can be tteated with either surgery or siu-gery and chemotherapy. Stage II, HI, and IV patients are initially surgically debulked of tumor before receiving chemotherapy and/or radiation therapy. The tteatment is based on the ability to surgically remove the tomor and the location of the remaining tumor. The initial chemotherapy usually includes the drug cisplatin in the regimen as it is highly active against this tomor, and this protocol requttes that patients have previously received either cisplatin or carboplatin. Following the iiutial chemotherapy patients may be treated with inttaperitoneal chemotherapy. Therefore, the technology allowing the insertion of fluid into the peritoneal cavity for tteatment of ovarian cancer is estabUshed (I), and tiiese methods are used in this investigation.
Ovarian cancer cure is approximately the following: Stage 1—80-100%, Stage H to Stage Hla—30-40%, Stage Illb— 20%, and Stage HIc to IV—5-10%. An ovarian cancer patient's prognosis can also be estimated by either: (1) size of largest tumor lesion at the time of diagnosis, or (2) diameter of the largest remaining metastatic lesion after surgical reduction. Patients presenting with a > 10 cm tumor mass exhibited a 0 % three year survival and a 9 month mean survival (2). Patients with a >1.5 cm tomor mass post-surgical reduction exhibited a 0 % three year survival with a 6 month mean survival (2). In addition, patients who relapse following the initial chemotherapy only have a 10-20% response to second line therapy which has not been shown to prolong patient survival (3).
The C A 125 marker has been useful in determining microscopic disease recunence if the patient presented with a positive titer which decreased with treatment. C A 125 is a cell surface glycoprotein found on ovarian tumor ceUs. In a patient with ovarian cancer, a C A 125 titer of >35 IU/ml is almost always associated with disease. A negative titer is a poor indicator for lack of disease (4). The rising or falling of the C A 125 titer can be used to follow the success or failure of tteatment. Thus, persistentiy elevated titers during tteatment usually indicates tteatment failure (4).
3.2 Progress in the investigation of vaccines for active-specific immunotherapy
The clinical trials of vaccines for active-specific immunotherapy have had some success with three types of malignancy; renal carcinoma, colon carcinoma, and maUgnant melanoma. The methodologic requttements for cancer vaccines have gradually been worked out in animal models in the last 15 years. Many cUiucal trials in this field were iiutiated before this information was available, or did not adhere to the methodologic requttements that had been found in the animal studies. As a consequence, there are several cUnical investigations of active immunotherapy that failed due to study design or preparation of the tumor vaccine. These studies may have failed due to one of the following factors: (A) The tumor cells should be preserved in a viable form in those vaccines where whole tu
mor cells are used. (B) Each procedure toward a subcellular product must be carefuUy evaluated as the immunogenicity can be easily desttoyed. (C) The cryopreservation procedure for storing tamor cells for a later use in the vaccine must be carefully evaluated and shown not to desttoy the inununogeiucity of the vaccine. (D) The use of an adjuvant is essential, but the adjuvant must be given at a predetemiined optimal concenttation. Tumor cell vaccines are considered to be weakly antigenic and the use of an effective adjuvant is critical to success, but selection of the wrong dose can negate the adjuvant's role. (E) The dose of tumor cells or quantity of antigenic material is a critical factor and when an inadequate dose is given, the immunologic effect wiU be lost. (F) The animal studies had predicted that the use ofthe patient's own tumor ceUs (autologous) would have the highest Ukelihood of success, while allogenic cells were often unsatisfactory. However, the use of allogeneic cell lines would have great practical advantages of standardization, avaUabiUty, and ease of vaccine preparation.
W e have been conducting trials based on the concept of active-specific immunotherapy, for metastatic kidney carcinomas using autologous tamor cells and C. parvum as an adjuvant. The vaccine was administered weekly for six weeks, 3 of 14 patients underwent objective regressions in the initial study (9), and 5 of 20 patients responded in a second trial (10,11). Several of the responding patients had remissions lasting from 2-5 years and some remain in remission.
CUnical investigators have had some success with vaccines for advanced maUgnant melanoma. Berd, Magutte, and Mastrangelo (12) used autologous melanoma tumor cells for their vaccine with B C G as the adjuvant and have reported responses in melanoma patients in the 16-20% range with some responses being complete remissions which were long-lasting. Mitchell and associates (5) have been evaluating an allogeneic vaccine derived from two cultured melanoma Unes and tiien prepared as a subcellular lysate. As an adjuvant they employed the agent Detox. They have observed responses in 20-30% of the patients in the Phase I and Phase II studies. Morton and associates have used a 3-Une aUogeneic melanoma vaccine and have obtained responses in 19% of thett patients (6). Preliminary but non-randomized stadies for early melanoma have shown promise (7,8).
In colon cancer, Hanna and Hoover (13,14) have conducted a prospective randomized stady comparing surgical tteatment only versus surgery followed by a vaccine of autologous tamor cells witil B C G as the adjuvant. The survival outcome in these patients favored those receiving the vaccine at an early point when only 20 patients had been entered in each arm. The full study with about 75 patients participating continues to demonstrate a significant recunence-free survival and overaU survival for those patients tteated with vaccines following surgery.
One group has begun investigations with active immunotherapy for ovarian cancer. Freedman and associates (29) prepared a vttal oncolysate from allogeneic ovarian cancer cell lines. This vaccine was administered IP or intrapleurally. In thett Phase I stady of 40 patients, they noted decreased ascites in 7 and partial remissions in 2.
Two recent developments have added exciting prospects for improving active immunization tteatments. Fttst came the finding that some of the new cytokines were very effective as systemic adjuvants when given with vaccines. IL-2 dramatically

CLINICAL PROTOCOL 929
improves the effect of a rabies vaccine (15), and a herpes vaccine (16) in animal stodies, and improved the response to a hepatitis vaccine (26) in humans. W e are curtentiy testing these observations in a clinical study for renal carcinoma and melanoma patients in which they receive an autologous tumor vaccine with IL-2.
W e found that another cytokine, IL-I, was the most powerful adjuvant with a tumor vaccine that w e have seen in experimental models (27), and we are currentiy investigating this cytokine with vaccines in the tteatment of colon cancer.
The second major development has been the success in gene modifications of tumor cells such that they become better vaccines. The approaches have included enzyme expression (as in this protocol), M H C class I expression, or cytokine expression (IFN, IL-2, IL-4).
3.3 Gene transfer clinical studies
Gene Transfer and Therapy protocols have been approved for human tiials in the past few years (17). The initial Gene Transfer stody was a gene marking study by Rosenberg and colleagues to mark tumor infilttating lymphocytes (TIL) in vitto with the neo"* gene. These marked TIL were injected back into the patient in order to determine the in vivo fate of these ceUs. This was accompUshed by using the polymerase chain reaction (PCR) technique to analyze cells isolated from the patient over time. These cultured TIL frequently demonsttate in vitto cytotoxicity to the tomor from which the cells were isolated, and cause necrosis of tamor deposits when injected into the patient (18). Wlule melanoma patients have had up to a 1 0 % complete response, the lack of significant response in the majority of tteated patients has raised questions about the fate of infused TIL. Stodies to determine cell survival have been Umited by the instabiUty of the radionucleotide used to label TIL. To avoid this Umitation TIL were permanently marked with the LNL-6 rettovttal vector, which contains the neomycin resistance gene as a marker (17). TIL ttansduced in vitro with the LNL-6 rettovttal vector have been infused into patients and, subsequently, polymerase chain reaction (PCR) was used to detect the neo** D N A sequence within tissues (17). Rettovttally marked cells from 4 of 5 evaluable patients could be reisolated and grown in cultare in the presence of G4I8, the neomycin analog toxic to mammalian ceUs. Using PCR, neo** TIL could be consistently detected in the circulation for three to eight weeks postinfusion. The neoR D N A could be detected by P C R in biopsies of patient tamor deposits for up to 64 days (17).
As of this writing there have been two gene therapy protocols approved (19,20). One protocol by Blaese and colleagues has genetically altered lymphocytes from adenosine deaminase deficiency patients. They have inserted the gene for adenosine deaminase ( A D A ) , the defective gene in this disease, into these patients' lymphocytes. The ttansduced cells are grown to large numbers and then infused into the patient. The hope is that these cells with a normal A D A gene will also function normally and citte the immunodeficiency found in these patients.
The second gene therapy protocol also involves the use of TIL. Clinical stadies using recombinant T N F to infuse into patients have been unsuccessful, possibly due to the toxic side effects of TNF. T N F producing TIL may be a more effective method to deliver the T N F to the tumor deposits. The TIL are
genetically modified with a gene encoding the tumor necrosis factor (TNF) protein. These T N F producing TIL when injected into the patient may migrate to the tumor, thus theoretically producing high local T N F levels while potentially avoiding the systemic side effects.
In addition, recently three human gene ttansfer protocols are being reviewed which serve to mark tamor cells in the bone martow of patients undergoing autologous bone m a n o w transplantation ( A B M T ) (21). They will attempt to determine the role of these tumor cells on cancer relapse in these patients after A B M T . These protocols are the first to propose using rettovttal stock on cells which will be immediately removed from the vttal stock and injected into a patient, rather than first monitoring the cells in vitro for adverse side effects (i.e., repUcation competent virus production or tomor formation due to an oncogenic event). However, assays to detect repUcation competent virus will allow this procedure to be performed safely since these assays can detect repUcation competent vttus in the vttal stock.
The ability to transfer genes to non-transformed cells has become possible over the past decade. The most common method for gene ttansfer into non-ttansformed cells is by rettovttal-mediated methods (22). Rettovttal vectors, most commonly generated from the Moloney murine leukemia virus ( M - M u L V ) , will efficiently ttansduce, stably insert into, and generate high levels of recombinant protein in host cells (23). The receptor for murine leukemia viruses is ubiquitous in mammalian species. A number of potential hazards exist when using the M -M u L V retroviral vector. First, the M - M u L V wild type rettovirus is a leukemia virus in some murine species. It can cause leukemia, in part, through protooncogene activation in the infected cell by the retrovttal long terminal repeat (LTR). Second, though rettovttal vectors are "crippled" rettoviruses and thus are replication incompetent, they possess the ability to recombine with retroviruses within a packaging cell line to form a repUcation competent virus.
Though the M - M u L V rettoviral vector still possesses its LTR, the frequency with which oncogenesis occurs in the ttansduced cells appears to be very low. The overwhelming majority of reported experiments performed over the past decade with rettovkal vectors demonsttate no association with ttansformed cells. These studies include experiments in mouse, dog, monkey, and sheep models to name a few.
The abiUty of rettoviral vectors to undergo recombination events to produce replication competent virus can be detected by sensitive assays which have been estabUshed over the past decade. These assays are termed S"'"/L"" and Helper Rescue Assay (24). If a recombination event occurs, it wiU almost always occur in the producer cell. The producer ceU line contains both a helper virus and the retrovkal vector. The producer cell line generates the viral particles used for ttansduction. Therefore, the producer cell Une can be continually momtored for the appearance of repUcation competent virus. CeUs ttansduced with replication incompetent viral stock, as measured by the above assays, are very unlikely to generate replication competent virus themselves. However, as described in this protocol below, these transduced cells can also be monitored for a few weeks after transduction, a period sufficient to detect repUcation competent virus by the above assays. Thus monitoring ttansduced cells for a few weeks in vitto before injection into

930 CLINICAL PROTOCOL
a patient will greatly reduce the risk of generating repUcation competent virus. This proposal will be designed such that the transduced ovarian tumor cells will be monitored for at least four weeks post-ttansduction before these cells are injected into a patient.
3.4 Gene-modified tumor cells: preclinical studies relevant to this protocol
A. In vitro studies Tumor cells expressing the herpes simplex virus gene for
thymidine kinase (HSV-TK, or T K ) are killed in vitto and in vivo by the drug ganciclovtt (GCV) as has been demonsttated by Moolten and coUeagues. W h e n the H S V - T K expressing tomor cells die after exposure to G C V , the nearby tumor cells are also killed even though they are H S V - T K negative. These nearby tomor cells appear to die by two contributing mechanisms: I) ttansfer of the H S V - T K phenotype from tiie HSVT K positive cells to the H S V - T K negative cells, thus rendering the H S V - T K cells susceptible to ganciclovtt therapy and 2) generation of host immunity against the killed tomor cells. The stodies presented in this section will illusttate both mechanisms with the main focus being on the former.
The initial studies analyzed the ability of H S V - T K ttansduced tumor cells to respond to G C V in vitto. A murine fibroblast cell line, N I H 3T3, was transduced with either the S T K or u T K vector. Both are neo"^ and H S V - T K containing rettoviral vectors (25). These ttansduced ceUs were selected in G4I8, a neomycin analog toxic to mammaUan cells. The cells were then placed in varying concenttations of G C V for 10-14 days at which time live cells (colonies) were counted. G C V is a nucleotide analog which is phosphorylated by H S V - T K with a 1000 times more efficiency as compared to the cellular thymidine kinase. The phosphorylated compound can then be di- and triphospborylated by cellular enzymes. The-triphosphate form of G C V is toxic to the cell by either functioning as a D N A polymerase inhibitor or a D N A chain terminator or both. W e showed that G C V was highly effective in kilUng either tiie S T K or /xTK transduced cells, while control L N L cells were not affected by GCV.
W e next transduced a murine fibrosarcoma cell line, Kbalb, with the STK, yu-TK, and L N L rettovttal vectors. Almost all H S V - T K positive cells were killed by 0.5 p U G C V , while the unttansduced or L N L transduced Kbalb cells were virtually unaffected at G C V concenttations of 50 p M .
These studies were repeated with human tomor cell Unes, S K - N - M C and H C T (neuroblastoma and colon carcinoma), with the same results. Of note is the evidence of smaU numbers of G C V resistant colonies observed even at high G C V concentrations. From this we can anticipate that G C V wiU not completely eliminate tumors expressing S T K when the tomor cells are given as in vivo challenges. In fact, an immunologic response also occurs in vivo as demonsttated below.
T w o human ovarian carcinoma cell lines, SKOV-3 and PA-1, were ttansduced with the S T K retrovttal vector and exposed to varying concenttations of ganciclovtt. W e demonstrated a similar sensitivity to the drug in these ovarian tumor lines. The PA-l-STK has been selected for use in the vaccine of this clinical stady.
W e next studied the time kinetics of cell kill of T K positive
cells by ganciclovtt. Using either 10 p M or I p M G C V , the approximate peak and ttough levels achieved in vivo, respectively, Kbalb-STK cells were exposed over varying time periods to these G C V concenttations. W e observed that exposure of Kbalb-STK cells to even 1 p M G C V for only three hours resulted in marked kilUng of the cell population with even more complete cell death after 24-28 hours as shown. In designing the cUnical protocol we have planned for patients to receive G C V for 7 days to provide a prolonged exposure for kilUng S T K cells.
B. In vivo experiments The initial observations described above also demonsttated
that some S T K ttansduced ceUs were resistant to G C V therapy in vitto. It was therefore, surprising to find when we began in vivo experiments that an H S V - T K positive cell population could be entttely eradicated in vivo. This occvured even when a sufficiently large number of tumor cells had been injected such that enough resistant cells were present to allow tumor growth.
Kbalb-STK and conttol Kbalb-LNL transduced cells were injected subcutaneously (2 X 10^ cells per mouse) in syngeneic mice. The tomor bearing mice were tteated with ganciclovir (150 mg/kg/dose X 5-10 doses) beginning on day 0 or day 5 relative to the time of tumor inoculation. Some animals received Kbalb-STK or Kbalb-LNL cells without G C V therapy. Mice which received S T K ttansduced tomor cells and G C V therapy rejected thett tomors, while the control groups did not.
A second murine tumor, SA-1, a fibrosarcoma, was ttansduced and studied in a similar manner. The results again showed complete prevention of tamor growth. To analyze the stabtiity of the H S V - T K gene expression in vivo, we sequentially passaged S T K ttansduced Kbalb murine fibrosarcoma cells in syngeneic mice. O n day 42 and 80 of passage, additional mice were inoculated subcutaneously with the passaged ceUs. These nuce were then tteated with G C V . All T K positive tumors passaged on both day 42 and day 80 regressed if the mice were exposed to G C V , while conttol L N L transduced passaged tumor cetis grew.
C. GCV effects on nearby TK negative tumor cells Based on the above experiments which demonsttated the
ability to eradicate S T K transduced population in vivo, questions about tiie effects of T K positive ceUs on nearby T K negative cells arose. In vitto mixing experiments were performed using the Kbalb-tamor cell Une. Tumor cell preparations were made in which Kbalb-LNL and Kbalb-STK were mixed. These nuxed ceUs were plated at 2 X 10^ per 100 m m tissue culture plate. G C V at 50 p W m l was added. The percent of Kbalb-STK was varied from 0 to 100%. Plates were stained with a 1 % metii-ylene blue solution 10-14 days later and Uve colonies were counted. This experiment was designed to determine die effect of T K positive cells on neighboring T K negative cells in vitto. A population of cells containing as few as 1 0 % S T K positive cells could eradicate vtttually all cells in the plate. Therefore, T K positive ceUs can affect nearby T K negative cells in vitto. These studies were repeated and confttmed wifli another murine tomor.
Studies on the possible mechanism for the effect of T K positive cells on T K negative cells were begun by analyzing tiie

CLINICAL P R O T O C O L 931
mechanism of cell death when T K positive cells are exposed to GCV. CeUs die by two mechanisms, necrosis and apoptosis. Necrotic cell death is characterized by cell swelUng, cell membrane disintegration, and nuclear flocculation. Apoptotic cell death is characterized by cell shrinkage, vesicle fonnation, and chromatin condensation. Cells dying by apoptosis break up into vesicles which can be phagocytized by nearby cells. Tumor cells have the abiUty to phagocytize apoptotic vesicles. T K negative cells may be affected by T K positive cells due to the ability of T K negative cells to phagocytize toxic metabolites contained in T K positive apoptotic vesicles. W e have seen by Ught microscopy of normal and T K positive ceUs exposed to G C V that the T K positive ceUs show the characteristic signs of apoptosis: cell shrinkage, vesicle formation, and chromatin condensation.
W e next analyzed the effects of T K positive cells on T K negative cells in vivo. Using the Kbalb tumor model, mice were inoculated with varying ratios of Kbalb tumor cells which were ttansduced with either tiie STK or conttol LNL rettovttal vectors. Mice received 2 X 10^ tamor ceUs subcutaneously on day 0. These tamor ceU challenges contained from 0 to 100% Kbalb-STK ceUs while the remainder in each mixture were Kbalb-LNL ceUs. The mice were tteated with G C V on day 3 when the tumor diameters were approximately 2 mm. The dose of G C V was 150 mg/kg given LP., twice each day for 5 days. Groups of mice receiving eiflier 50%, 90%, or 100% Kbalb-STK cells demonsttated tamor regression (Table I). These studies were repeated with two other murine tumor lines. The same pattem of results occuned with aU 3 tumors: in groups receiving tamor challenges containing only 1% or 0 % STK ceUs all developed progressive tamors, those groups receiving 10% STK cells had some mice where the tumors regressed, and in those groups receiving 5 0 % or more STK ceUs, all had complete tamor regression.
D. Immunologic responses are a requirement The abiUty of immunodeficient mice to reject STK ttans
duced cells was also studied. Nude and non-lethally inadiated mice were inoculated subcutaneously with 205-STK or 207-STK tamor ceUs at varying ratios as described above and tteated with GCV. The immunodeficiency mice were poor at rejecting the tamors even when 100% of the tumor cells contained the HSV-TK gene (Table 2). This indicates that an intact immune response is a necessary component in the rejection of these tamors. It appears that both the local effects of G C V and the systemic immunity contribute to the rejection mechanism.
Table 2
Table I
Tumor rejected/ % STK" # mice challenged
100% 90% 50%
5/5 5/5 5/5 0/5
% STK"
100 50 10 0
Syngenei(l° mice
5/5 5/5 3/4 0/5
Nude^ mice
1/4 0/3
0/3
Radiated" syngeneic
mice
1/4 0/4
0/3
^The ratio of Kbalb-STK/Kbalb-LNL
''The ratio of Kbalb-STK/Kbalb-LNL. 'Tumors rejected/number of nuce challenged.
E. An intraperitoneal cancer model W e next evaluated the effect of Kbalb-STK positive tumor
cells on T K negative cells using an intraperitoneal tumor model. The previous experiments demonsttated that in a relatively confined subcutaneous space, as few as 5 0 % T K positive ceUs within a tumor could cause regression of the tomor. W e injected IP varying ratios of Kbalb-STK/Kbalb-LNL cells into the syngeneic Balb/c mice. They were tteated with G C V (150 mg/kg LP., b.i.d., X5 doses) beginning five days post tumor inoculation. Survival studies were then performed. Groups of mice receiving either 5 0 % or 100% STK transduced tumor ceUs had prolonged survival with most animals having no evidence of tumor for more than 80 days as seen in Table 3. Control mice, receiving Kbalb-LNL ceUs or Kbalb-STK witiiout G C V all developed progressive abdominal tumor. Groups receiving 1% or 10% STK ttansduced ceUs contained no long term survivors but had a ttend towards surviving longer than the conttols. Therefore, the ability of T K positive tumor cells to affect T K negative tumor cells can be demonsttated in a large enclosed body cavity.
W e next analyzed whether T K positive tomor ceUs could affect a preexisting inttaperitoneal tomor. The Kbalb tomor model was used to address this question. Mice were inoculated I.P. with 2 X 10 Kbalb-LNL. As seen in Table 4, those groups receiving treatment with Kbalb-STK cells and G C V had a distinctly prolonged survival, even when the tteatment was begun 5 days following the challenge; however, none of these mice remained tamor-free long term.
The above experiment which demonsttated the effect of Kbalb-STK ttansduced tumor cells on preexisting inttaperitoneal tumor was repeated using a human ovarian tamor Une SKOV-3 in the tteatment step. This Une was ttansfected to express the STK gene. The results are shown in Table 5. Of interest was the finding that 3/8 mice tteated with SKOV-3-STK, remained tamor free for the total observation period of over 150 days.
F. Studies using radiated cells The abUity of G C V to kill ttradiated HSV-TK expressing ta
mor cells was analyzed. The Kbalb-LNL or Kbalb-STK tumor ceUs were exposed to 3,000 rads and then cultitted in vitto. The cells were exposed to 50 p M G C V at varying times post-inadiation. The irtadiated Kbalb-LNL tumor ceUs exposed to G C V continued to remain metaboUcally active as evidenced by their abUity to remain attached to a tissue cultare dish up to 28 days post inadiation. W e determined that G C V had virtoally no ef-

932 CLINICAL PROTOCOL
Table 3
Group
I 2 3 4 5 6
# of Mice
4 9 5 5 6 7
Challenge IP
0 % Kbalb-STK/ 0 % Kbalb-STK/ 1% Kbalb-STK/
10% Kbalb-STK/ 5 0 % Kbalb-STK/ 100% Kbalb-STK/
100% Kbalb-LNL 100% Kbalb-LNL 9 9 % Kbalb-LNL 9 0 % Kbalb-LNL 5 0 % Kbalb-LNL 0 % Kbalb-LNL
Ganciclovir treatment"
— -\--\--1-4--1-
Mean survival
(days ± SE)^
18.0 ± 0.0 18.2 ± 2.1 25.4 ± 1.7 29.8 ± 1.4"= 82.0 ± 13.6'̂ 87.1 ± 8.3'
''Given IP for 3 days, beginning 5 days after chaUenge. ''Statistical comparisons with group 2 are using Student's T test. '!)> O.OOI.
feet on inadiated T K negative cells. Inadiated T K positive cells exposed to G C V on day 0 died within a week, while cells exposed to G C V after day 0 died after approximately one month.
In vitto nuxing experiments were set up using inadiated T K positive cells (HCT-STK, human colon carcinoma) and non-irradiated T K negative cells (Kbalb-LNL). Cells were plated at varying ratios of inadiated T K positive to T K negative cells with a total of 2 X 10^ ceUs plated in a 100 m m cultore dish and G C V (50 p M ) was immediately added. The results approximate those seen in the above experiments using non-irta-diated T K positive tumor cells. When the T K positive cells made up as few as 10% of the cells virtually all the ttradiated HCT-STK and non-inadiated Kbalb-LNL cells were killed by GCV, while inadiated H C T tomor cells had no effect on the Kbalb-LNL cells.
W e next evaluated the effect of radiating the T K positive cells with in vivo studies. The mice were challenged with IP injected Kbalb-LNL syngeneic tomor cells. Two human tumor lines which had been ttansduced to express TK, and were radiated with 3000 rads, were used as the therapeutic agents. The results are shown in Table 6 and demonstrate that both the human colon Une (HCT-STK) and the human ovarian line (PAl-STK) were effective agents under the additional condition of radiation prior to use. Long term survival (>70 days) was seen in 2 5 % of the mice.
G. Immunization studies To begin to stody the immunologic effect of kiUing STK
ttansduced cells in vivo, the syngeneic mice were subcutaneously inoculated with either Kbalb-STK tumor cells or 205-STK tomor cells and tteated with GCV. Three to eight weeks post G C V therapy the rruce were rechallenged with either Kbalb or 205 tumor cells. Conttol (untteated) mice were also challenged with tumor. The results are shown in Table 7 and indicate an immunoprotective effect. This effect is typical of tomor vaccine stodies and requttes additional experiments to determine whether cell death by the TK/GCV mechanism is more immunogenic than injection of radiated tumor ceUs. However, the experiment does indicate the potential of the TK/GCV approach to kill tumor ceUs by 2 complementary mechanisms: the local effect on nearby tumor cells and a subsequent longer lasting immunologic response.
3.S Safety Issues
3.51 Testing of cultured cell lines. The PA-l-STK cell line used for the vaccine, and the cul
tared cell Unes used for skin testing are all tested to exclude contaminating agents. They are steriUty tested for freedom from bacteria and fungi in our lab, tested by cultivation methods to exclude the presence of vims through our medical center's clin-
Table4
Group" Treatment Mean survival'̂ (days ± SE)
None I0« Kbalb-STK dl, no G C V G C V d 5-7 10^ Kbalb-STK dl, G C V d5-7 106-10^ Kbalb-STK d5, G C V d9-II
18.0 ± 0.0 13.3 ± 0.5 18.2 ± 2.1 31.6 ± 4.3*̂ 31.8 ±9.6=
^AU mice were challenged day 0 with 2 X 10^ Kbalb-LNL IP. ''Both agents were administered IP. '̂ Statistical comparisons with group 3 are given using the Student's T Test <'p<.001. "tx.ooi.

CLINICAL PROTOCOL 933
Group"
I 2
Table 5
Treatment^
2 X 10^ SKOV-3 day 1 plus G C V days 4-7 2 X 10« SKOV-3-STK day 1 plus G C V days 4-7
Mean survivaF (days ± SE)
17.1 ± 4.7 58.2 ± 28.6
''Challenged with 2 X 10^ Kbalb-LNL day 0, I.P. ''Both agents were administered I.P. "Statistical comparison by the Generalized Savage (Mantel Cox) p •• 0.0093.
ical virology lab, and tested for mycoplasma and rettovimses (by reverse ttanscriptase) by commercial laboratories.
3.52 Testing for retroviral effects. One concem in the use of rettovttal vectors for gene ther
apy is thett oncogenic effect on the host cells. This is particularly a concem when ceUs expected to have a long survival are given to the host, such as with somatic cells secreting genetically absent molecules. However, for our purposes, the gene-modified tamor ceUs used are lethally radiated prior to administtation and thett survival is expected to be only a few days.
A second concem is the potential for replication competent virus being produced and released by the tamor ceUs used in the tteatment. The vector and helper virus used in the ttansduction are both designed to be unable to form replication competent vims. However, to provide evidence that no recombination event has occuned, the supematant from both the packaging cell line and the PA- I-STK cell line used for tteatment have been tested by our collaborator. Dr. James Zwiebel, at Georgetown University, using the S"'"/L~ assay, and found to be free of vims.
3.53 Other human studies with gene-modified cells. To date, approximately one dozen patients have received ge
netically engineered cells with no adverse effects (17, 19, and 20). The initial stadies by Rosenberg et al. injected genetically marked TIL cells into cancer patients. These ceUs were transduced with replication incompetent vkal stock. The vttal stock was momtored for the presence of repUcation competent vims, a byproduct of a recombination event, by the sensitive S"''/L~ assay or helper rescue assay. In addition, once ttansduced, the TTL cells were grown in vitto for almost a month and tested for
repUcation competent vttus in the event that a repUcation competent vttal particle went undetected in the viral stock. Growing the cells in culture for a few weeks prior to reinfusion also allows the opportunity to analyze the cells for an oncogenic event produced by the insertion of the rettoviral vector near a protooncogene. The next two human gene ttansfer cUnical protocols followed similar procedures.
Recently, clinical protocols have been submitted which ttansduce and infuse bone martow cells into a patient within a few days of the transduction process (21). These protocols which for technical reasons caimot monitor the ttansduced cells for replication competent virus or an oncogenic event before reinjection are still considered safe since the vttal stack is tested by sensitive techniques (Helper Rescue Assay). In addition, the frequency of oncogenesis using murine rettovkal vectors is very low. These factors are considered before an approval of the protocol in the context of the risk-benefit to the cancer patient. In the advanced cancer patients used in the last studies, the inability to monitor ttansduced cells long term before reinfusion was deemed as acceptable risk.
Our protocol also is for advanced cancer patients, but we will be able to monitor the transduced cells for at least four weeks post ttansduction and assay for the presence of repUcation competent vims before infusion of the cells into the patients. In addition, we plan to inadiate the cells prior to injection and thus will not assay for oncogenic events.
3.54 Retroviral In Vivo Studies The following experimental data does not relate to the STK
rettoviral vector, it does relate to the effects of retrovkal ttansduction on oncogenesis and therefore wUl be presented in this context. Studies were undertaken to analyze the effects of in
Table 6
Group" Treatment^ Mean survival (days ± SE)
2 X IO'' P A I-STK day I, G C V days 2-5 2 X 10'' P A I day I, G C V days 2-5 2 X 10'' HCT-STK day 3, G C V days 3-6 2 X 10'' H C T day 3, G C V days 3-6
55.4 ± 24.7'' 29.1 ± 4.9 68.3 ± 54.6= 24.3 ± 15.6
'<:hallenged with 2 X 10= Kbalb-LNL day 0, I.P. ''Both agents were administered I.P. "Statistical comparisons with control groups were made with the Generahzed Savage
(Mantel Cos). •"Group 2 vs. Group I, p = 0.0182. "Group 4 vs. Group 3, p = 0.0481.

934 CLINICAL PROTOCOL
Table 7
Immunizing tumor cells"
Challenge tumor cells°
Tumor free/no. challenged
None Kbalb-STK
None 205-STK
Kbalb Kbalb
205 205
0/4 4/8
0/4 13/28
"I X 10^ unirtadiated cells given s.c. followed by G C V on days.
''1 X 10^ ceUs given s.c.
vivo passage on rettovttally ttansduced cells. Rat skin fibroblasts were isolated from a Fischer 344 rat and expanded in tissue culture. The non-immortalized cell line was designated PRSF and transduced with the p G 2 N rettoviral vector. This vector is an N 2 based vector with an L T R (long tenninal repeat) promoted growth hormone c D N A and a SV40 promoted neomycin resistance gene (neoR). The transduced PRSF cells were selected in G418 for 14 days and subsequently single clones were isolated. One clone, C2, producing approximately 600 ng/10* cells/24° was isolated. The C 2 population of cells was used for implantation into hypophysectomized Fischer 344 rats. Alginate, a mucopolysaccharide, was used to encapsulate the C 2 cells prior to implantation and the cell alginate mixture was implanted inttaperitoneally (I.P.). W e had previously demonsttated that encapsulated cells survived and when s e m m growth hormone levels were undetectable, one rat was sacrificed and the I.P. contents, consisting of a slurry mixture, were isolated and grown in tissue culture in the presence of G4I8. T w o cell populations were isolated as distinguished by morphology. Plate A shows the original pre-implantation C 2 ceUs as compared to plate B, which was one isolated cell population (7078) exciting normal morphology, and plate C, a second population (7078T) which was spindly in appearance and grows in low semm. The C 2 7078, and 7078T cells were all G4I8 resistant and produced growth hormone at approximately 600 ng/10* cells/24°. The four cell populations, PRSF, C2, 7078, and 7078T, were plated in soft agar to assay for ttansformation. Virtoally no colonies formed in agar from any of the cell populations except the 7078T cells, which had a plating efficiency of 2.8%. In addition, colony formation of the 7078T cells demonsttated a larger colony size than the colorues formed by the non-transformed lines. These cell lines were also inoculated into nude mice with only the 7078T cells forming tomors. Therefore, the morphology and ability to grow in low semm, as well as, anchorage independent growth and tomor formation in nude mice were indications of transformation.
W e next performed Southern blot analysis and showed that the p G 2 N retroviral vector was present in the C2, 7078, and 7078T cell Unes. The clonality of C 2 and 7078 can also be demonstrated by Bgl II restriction enzyme digests, an enzyme that digests within the retroviral vector, by the presence of a single identical band in the C 2 and 7078 cell lines. FinaUy, w e can show not only the reanangement of the growth hormone gene in the 7078T cells but also the reanangement the c-myc oncogene. Since the G 2 N rettoviral vector did not insert near the c-myc oncogene, it may be possible that the G 2 N vector
produces a trans activating factor which effected the c-myc oncogene. This represent the fkst reported association of a retroviral vector and a transformed cell.
4.0 Objectives of the Study
4.1 To evaluate the safety and side effects of tteatment with a Gene-Modified Ovarian Cancer Vaccine which is adnunistered inttaperitoneally and activated with ganciclovir. 4.2 To determine a maximum treatment dose ( M T D ) of the vaccine and the dose limiting side effects of tteatment. 4.3 To evaluate the immunologic response to this vaccine program. 4.4 To observe for clinical effects on the residual ovarian can-
5.0 Patient Selection
5.1 A diagnosis of epithelial ovarian carcinoma must be established histologically. 5.2 Patients may initially have been Stage I, II, or RI. Stage TV patients initially or at present are not eUgible. 5.3 Patients must have completed the initial surgery and chemotherapy and have been off tteatment for at least 6 weeks. Previous chemotherapy must have included cisplatin or carboplatin containing regimens. 5.4 Patients must have clinical evidence of recunent, progressive or residual disease by laparoscopy, laparotomy, imaging, surgery, or successive elevation of the C A 125 marker. If possible, resistance or progression should be documented by histology/cytology. If C A 125 is used as evidence of residual disease, then the level must be greater than 35 IU/ml and increasing on two successive detemunations, greater than 1 month apart, and the patient must not have had a laparotomy within the preceding 3 months. 5.5 The patient's performance status must be 0 or 1 by E C O G standards. 5.6 Any tomor masses found by imaging must be 2.0 c m or less to be eligible for this stody. 5.7 Adequate bone martow, kidney and liver function must be shown by: Hct > 30, W B C > 4,000, platelets > 100,000, creatinine < 1.5 m g % , Creat. Cl > 50, normal biUmbin, S G O T and alkaline phosphatase < 1.5 X normal. 5.8 Patients must not have a significant history of heart disease (frequent angina, M I within the past 6 mos., congestive heart failure requiring daily tteatment). 5.9 A patient is not eligible if there is a history of a previous malignancy, other than squamous or basal cell carcinoma ofthe skin. Patients with childbearing potential are not eligible. 5.10 Patients with extensive abdominal adhesions and lack of free flow of fluid within the peritoneal cavity are not eUgible. 5.11 Patients with evidence of moderate to severe pulmonary disease (COPD) will not be eUgible. 5.12 Patients requtting steroid treatment are not eligible. 5.13 Patients with a negative Epstein Bart antibody test are not eUgible.

CLINICAL PROTOCOL 935
6.0 Study Design
This is a phase I study in which a primary goal is to deternune the toxicity and safety of administering PA-l-STK modified ovarian tumor cells I.P. with subsequent ganciclovir therapy. The maximum tolerated dose (MTD) (up to I X I0'° ceUs per dose) of genetically modified tumor cells will be determined. If the M T D has not been detemuned by four groups of patients, an additional group could be added at an appropriately higher dose. Four patients will initiaUy receive 3 X 10'' HSVT K positive tumor ceUs I.P. on day 1. Patients wiU begin a 7 day course of Ganciclovtt starting within 24 hours of receiving the I.P. infusion. Two weeks after the tennination of ganciclovk tiierapy the patient will be reevaluated in terms of side effects from tteatment and disease state. If no adverse toxicity occuned from the previous I.P. tumor injection and ganciclovir therapy and there appears to be no evidence of progressing tumor which would requtte chemotherapy, then flie patient wiU be eUgible for the next dose. This schedule will continue for doses of I X 10*, 3 X 10* for Group I. If no adverse side effects wartanting the stoppage of therapy are reported in Group I then Group 2 patients wUI begin at one dose level higher as shown in sec. 8.2 and this pattem will continue through the 4 groups. If a patient has to drop out of the stady for reasons other than toxicity, then another patient may be added to die group and will begin therapy at the lowest dose for that group. By entering patients at each dose level, we shall attempt to address the question of the maximum tolerated dose (MTD).
7.0 Patient Registration
Patients may enter this stady by completing a consent form. Thek eUgibiUty will be confirmed by the data manager at the University of Rochester Cancer Center. Patients will be assigned to Groups by the data manager. Participation or non-participation in this cUnical study will not affect other therapy for which the patient is eUgible.
8.0 Treatment Plan
8.1 The patients wiU be admitted to the hospital for the first eight days of each cycle. The vaccine is given on day I and ganciclovk is given for seven days, beginning on day I. The tteatment is repeated at 3 week intervals for a total of 3 cycles of tteatment. At the completion of tteatment, patients will be followed regularly until there is progression of disease. 8.2 Vaccine and administtation. Patients wUl be assigned in order of enttance on study to one of the four tteatment schedules below. The dose escalates with each treatment unless any toxicity or grade II or higher level has occuned (Appendix B). For Grade II toxicity (except for neuttopeiua or thrombocytopenia) the dose is repeated but physician discretion could lower the dose if overall toxicity is of concem. For Grade III or TV toxicity, the dose is lowered one level. If these Grade III/IV toxicities do not resolve within 1 week, the patient will be taken off the study.
Patients
l ^ 5-8 9-12 13-16
First dose
3 X 10^ I X 10* 3X 10* I X 10'
Second dose
I X 10* 3X 10* I X 109 3 X 105
Third dose
3 X 10* 1 X 10* 3 X 105 1 X lO'o
The vaccine is prepared in 1000 cc of normal saline and administered through a smaU intraperitoneal catheter which may be placed on the day of treatment and then removed after the infusion, or surgically implanted prior to the treatment on a semi-permanent basis. Catheter placement and diffusion of fluid will be checked by a technetium flow study prior to the vaccine.
8.3 Vaccine side effects. Inadiated tamor cells have been administered as vaccines at intradermal sites in previous studies. At inttadermal sites, the local side effects are usually only a ttansient non-tender bump and even this side effect is largely detemiined by the adjuvant used rather than the tomor cells. The side effects from inttaperitoneal vaccine administration are largely unknown. In a study by Freedman, a lysate of tumor cells was given IP with no apparent side effects. The ganciclovir activation of the tumoricidal effect could lead to some local inflammatory response which may be a beneficial antitumor effect. However, whether symptoms will occur is unknown. For this reason the study is designed with an escalating dose plan and the patients wiU be hospitalized and monitored daily for side effects. 8.4 Ganciclovir is a nucleoside analog. It's an F D A approved dmg for the treatment of cytomegalovims infection. It is excreted by the Iddney and a creatinine clearance is a required pretteatment test. Granulocytopenia and thrombocytopenia are common side effects during the 2 to 3 week course for C M V infections. W e will only be giving a 7 day course but mild cy-topenias can be expected. Pain and phlebitis at the site of administration may occur. Anemia, fever, rash, and abnormal Uver enzymes have also been reported.
Reconstitotion and administtation. It is suppUed as a sterile powder and is reconstituted with sterile water. It is not compatible with bacteriostatic water. For I.V. administration it is prepared in 100 cc of normal saline or 5 % Dexttose and water and infused over one hour.
Dosage and adjustments. The dosage is determined per manufactarer's instmctions. The standard dose is 5 mg/kg b.i.d. when patients have a creatinine clearance > 80. If the CrCL is 50-79, the dose is 2.5 mg/kg b.i.d. Daily C B C and platelet counts will be obtained during tteatment. The dmg should be stopped if the absolute granulocyte count falls below 750 or the platelets are less than 50,000.
Storage requirements and stability. The original sterile powder suppUed in 10 ml sterile vials, 25 in a carton should be stored at room temperatare avoiding heat above 40 C (104 F). Reconstituted solution in the vial should be stored at room temperature. It should not be refrigerated. When stored accordingly it wiU be stable for 12 hours. Final diluted infusion solution (admixture preparation) should be refrigerated but freezing is not recommended. The solution must be used within 24 hours of dilution to reduce the risk of bacterial contamination. 8.5 Grading of side effects and toxicity will be detennined by the NCI's "Common toxicity criteria" (Appendix B).

936 CLINICAL P R O T O C O L
8.6 To document the patient reported incidence and severity of side effects
Each diary lists 23 possible side effects and includes space for patients to write in additional side effects. Patients also rate the efficacy of self-care activities in alleviating treatment side effects. In addition patients are asked to give an overall rating of how upsetting and dismpting are the side effects. The diary takes approximately 15 minutes to complete. The diary has been shown to have adequate variance and is acceptable to patients (28). It is curtentiy being used with patients receiving ttaditional chemotherapy as well as inpatients receiving IL-2. The diary will be completed daily for the 8 day hospital stay for each tteatment and at I week and 2 weeks following discharge (Appendix F). 8.7 Reporting of Adverse Reactions. For known reactions, toxicities of Grade I-III will be reported as part of the stody results. Grade TV toxicities, fatal events, and fkst occurtence of any toxicity (regardless of grade) must be reported by phone (301-496-7957) within 24 hours and require a written report to IDB within 10 workings days. 8.8 Retrovkally ttansduced PA-l-STK cells. PA-l-STK cells will be monitored before vaccine freezing for the presence of repUcation competent murine retrovims using the helper rescue assay. In addition, at the time of freezing an aliquot of cells will be taken from the batch and grown in culture for at least two additional months and then assayed for the presence of replication competent vims.
of cytotoxic lymphocytes is produced by the immunizing procedure. The methods are described in Appendix C. 9.3 Immune responses directed at M H C antigens on the allogeneic ovarian tomor ceUs of the vaccine. It may be difficuh to detect immune responses directed at autologous tomor antigens (sec. 9.2). However, responses to the M H C antigens should definitely occur and be measurable. Although this is a Phase I stody and the patient numbers are necessarily smaU, we will be observing for T cell and B cell responses and comparing low levels of vaccine cell dose with higher levels.
A. Cytotoxic assays. These will be performed concurtentiy with the autologous
tumor ceU assay but the target ceU line will be the PA-1-STK used in the vaccine.
B. Anti-HLA antibodies. The H L A antigens exposed on the PA-1 STK line will be de
termined through the tissue typing laboratory. Semm specimens wiU be serially obtained from each patient to determine an antibody titer dkected at the H L A molecule. 9.4 The C A 125 marker level will be detemiined prior to beginning therapy and prior to each vaccine cycle. 9.5 Imaging studies will be obtained following the second tteatment. Another imaging stody wiU be performed following completion of the tteatment. 9.6 Laparotomy or laparoscopy. A laparoscopy or laparotomy wiU be performed within 45 days of beginning this study to document the presence and size of tomor.
9.0 Measurement of Effects 10.0 Administrative Aspects
9.1 Pretreatment immunologic evaluation. Active specific immunotherapy treatments are dependent upon an intact immune system in the host in order to respond to the vaccine. Patients with an impaired immune status due to advanced cancer, nutritional deficiency, or immunosuppressive agents are less likely to respond. The eUgibility criteria help to avoid this problem but in addition the statos of each patient's immune system may be evaluated as below. Participation is not dependent on the outcome of these tests, but they will be used in analyzing the immunologic and climcal parameters.
Recall skin tests. This tests immune responsiveness to challenge with antigens to which virtually all individuals have been exposed previously: Candida albicans, stteptokinase/stteptodor-nase, and mumps. 9.2 Immune response directed at autologous tumor cells. The precUnical work suggests that the inttaperitoneal vaccine procedure may achieve a systemic immunity. W e wOl evaluate this aspect of the response in two ways.
A. Autologous tumor cell skin tests. Prior to tteatment and subsequent to each vaccine adminis
tration, the patients may be challenged with 10* radiated autologous tomor cells (if available) given as an intradermal injection. The tomor tissue will have been obtained from the patient's initial surgical resection. W e have previously used this skin testing in studies with renal carcinoma. The procedure is described in Appendix A.
B. Lymphocyte cytotoxic assay. Using the patient's lymphocytes as effector cells and autol
ogous tamor cells as targets, we will determine if a population
All institutional. State, and Federal regulations regarding informed consent and peer judgment will be fulfiUed. See attached consent form.
11.0 Records to be Kept
12.0 Criteria for Measurement of Response (from G O G Protocols)
Refer to Appendix E.
REFERENCES
1. Cancer Treatment, ed. Haskell, CM., W.B. Saunders Company (Philadelphia), p. 295, 1990.
2. Berek, J.S. and Hacker, N.F. Practical Gynecologic Oncology. Baltimore, Williams & Wilkins, p. 342, 1989.
3. Thigpen, J.T. Ovarian Cancer. Boston, Martinus Nijhoff, p. 115, 1985.
4. Berek, J.S. Obstet. Gynecol. 67:685, 1988. 5. Mitchell, M.S., Kan-Mitchell, J., Kempf, R.A., Harel, W., Shau,
H., Lind, S. Active specific immunotherapy for melanoma: Phase I ttial of allogeneic lysates and a novel adjuvant. Cancer Res. 48:5883-5893, 1988.
6. Morton, D., Nizze, A., Foshag, L., Hoon, D., Famatiga, E., Gupta, R., kie, R. Proc. Am. Asso. Con. Res. 31:281, 1990.

CLINICAL PROTOCOL 937
7. Wallack, M.K., Bash, J.A., Leftheriotis, E., Seigler, H., Bland, K., Wanebo, H., Blach, C, Bartolucci, A.A. Positive relationship of clinical and serologic responses to vaccinia melanoma oncolysate. Arch. Surg. 122:1460-1463, 1987.
8. Bysteyn, J.C, Oratz, R., Harris, M.N., Roses, D.F., Golomb, F.M., Speyer, J.L. Immunogenicity of a polyvalent melanoma antigen vaccine in humans. Cancer 61:1065-1070, 1988.
9. McCune, C.S., Schapka, D.V., Henshaw, E.C. Specific immunotherapy of advanced renal carcinoma: evidence for the polyclonality of metastases. Cancer, 47:1984-1987, 1981.
10. Sahasrabudhe, D.M., deKemion, J.B., Pontes, I.E., Ryan, D.M., O'Donnell, R.W., Marquis, D.M., Mudholkar, G.S., McCune, CS. Specific immunotherapy with suppressor function inhibition for metastatic renal cell carcinoma. J. Biol. Resp. Mod., 5:581-594, 1986.
II. McCune, C, O'Donnell, R., Marquis, D., Sahasrabudhe, D. Renal cell carcinoma tteated by vaccines for active specific immunotherapy: Correlation of survival with skin testing by autologous tumor ceUs. In Press.
12. Berd, D., Maguke, H.C, Mas'trangelo, M.J. Induction of cell-mediated immunity to autologous melanoma cells and regression of metastases after tteatment with a melanoma cell vaccine preceded by cyclophosphamide. Cancer Res. 46:2572-2577, 1986.
13. Hoover, H.C, Surdyke, M., Dangel, R.B., Peters, L.C, Hanna, M.G. Delayed cutaneous hypersensitivity to autologous tumor cells in colorectal cancer patients immunized with an autologous tumor cell: Bacillus Calmette-Guerin vaccine. Cancer Res. 44:1671-1676, 1984.
14. Hoover, H.C, Surdyke, M., Dangel, R.B., Peters, L.C, Hanna, M.G. Prospectively randomized trial of adjuvant active-specific immunotherapy for human colorectal cancer. Cancer 55:1236-1243, 1985.
15. Nunberg, J.H., Ooyle, M.V., Newell, A.D., Anderson, G.A., York, CJ. Interleukin-2 as an adjuvant to vaccination. J. Cell Biochem., Suppl. 128:12, 1988.
16. Weinberg, A., Merigan, T.C. Recombinant interleukin 2 as an adjuvant forvaccine-induced protection. J. Immunol. 140:294-299, 1988.
17. Rosenberg, S.A., Abersold, P., Cometta, K., Kasid, A., Morgan, R., Moen, R., et al. Gene ttansfer into humans—Immunotherapy of patients with advanced carcinoma. NEJM 232:570-578, 1990.
18. Rosenberg, S.A., Packard, B.S., Aebersold, P.M., Solomon, D., Topalian, S.L., Toy, S.T., Simon, P., Lotze, M.T., Yang, J.C, Seipp, C, Simpson, C, Carter, C, Bock, S., Schwartzentruber, D., Wei, J.P., White, D.E. Use of tumorinfilttating lymphocytes and interleukin-2 in the immunotherapy of patients with metastatic melanoma. N. Engl. J. Med. 319:1676-1680, 1988.
19. Federal Register, vol. 55, No. 177, p. 37567, Sept. 12, 1990. 20. Federal Register, vol. 55, No. 177, p. 37566, Sept. 12, 1990. 21. Federal Register, (in press). 22. Joyner, A., Keller, G., Phillips, R.A., and Bemstein, A. Rettovirus
ttansfer of a bacterial gene into mouse hematopoietic progenitor cells. Nature 305:556-558, 1983.
23. EgUtis, M.A., Kantoff, P., Gilboa, E., and Anderson, W.F., Gene expression in mice after high efficiency rettovkal mediated gene ttansfer. Science 230:1395-1398, 1985.
24. Aaronson, S.A., Bassin, R.H., and Weaver, C Comparison of the murine sarcoma viruses in non-producer and S-I-/L— transformed cells. J. Vkol. 9:701-704, 1972.
25. Moolten, F. and Wells, J.M., J. Nati. Cancer Inst. Curability of tumor bearing herpes simplex virus thymidine kinase genes ttansferred by rettovkal vectors. 82:297-300, 1990.
26. Meuer, S.C, Dumann, H., Meyer zum Buschenfelde, K.H., Kohler, H. Low-dose interleukin-2 induces systemic immune responses against HBsAg in immunodeficient non-responders to Hepatitis B vaccination. The Lancet, p. 1518, January 7, 1989.
27. McCune, C, Marquis, D. Interleukin-1 as an adjuvant for active specific immunotherapy in a murine tumor model. Cancer Res. 50:1212-1215, 1990.
28. Nail, L.M., Jones, L.S., Greene, D., Schipper, D.L., and Jensen, R. Use and perceived efficacy of self care activities in patients receiving chemotherapy. Oncology Nursing Forum 18(5): 883-887, 1991.
29. Freedman, R.S., Edwards, C.L., Bowen, J.M., Lotzova, E., Katz, R., Lewis, E., Atkinson, N., and Carsetti, R. Vkal oncolysates in patients with advanced ovarian cancer. Gynecologic Oncology 29:337-347, 1988.
12.0 Appendices
APPENDIX A
SKIN TESTING WITH ALLOGENEIC AND AUTOLOGOUS TUMOR CELLS
I. For allogeneic tumor cell skin tests, PA-1 STK, the gene-modified ovarian carcinoma cell Une used in the vaccine, wiU be used here, and in addition, another ovarian carcinoma ceU Une, S K OV-3, and the human renal carcinoma cell Une, Caki 2, to test for specificity. They are grown in semm free medium if possible, otherwise in medium containing human semm albumin (HSA), tested in the same way as for vaccine use, but frozen in aUquots of 3 X 10* cells/vial in freezing medium of 1 % H S A and 7.5% D M S O in M199 (HSA-FM).
O n the day of use a vial of each cell line is thawed, inadiated, and washed as for vaccine use. After the final wash, each ceU Une is suspended in M199 at 10* cells/0.3 ml and kept on ice until needed. Immediately before use, the cells are mixed well and 0.3 ml drawn into a I cc T B syringe with 25gX 1/2 inch needle for administtation i.d. in the patient's forearm.
2. For autologous tumor cell skin tests, a portion of the patient's tumor is taken for dissociation after surgical resection. In a laminar flow hood the tomor is trimmed, minced into 2-3 m m ^ pieces, and washed in Ml99 plus gentamicin (Gm) before being placed in a trypsinization flask (Bellco #1989, 125 ml) containing an enzyme solution made up of 0.002% deoxyribonuclease Type I, 0.1% coUagenase Type I, 0.05% hyaluronidase Type I, and G m in MI99. The flask is rocked ovemight at RT. The resulting cell suspension is diluted with M199, filtered through stainless steel mesh, centrifuged, and washed twice with MI99. The washed ceUs are resuspended in Ml99, layered over ficoll hypaque and centrifuged for recovery of the ceUs at the interface. These cells are drawn off, washed further in M199 and sampled for count and viability check before cryopreservation at 3 X 10* ceUs/vial in H S A . F M for use as autologous skin test and cytotoxicity test targets.
One of these vials wiU later be thawed and prepared as for a skin test, to be sterility tested and sent to an independent testing laboratory for the standard F D A d m g safety test.
O n the day of use a vial of autologous tumor cells is

938 CLINICAL P R O T O C O L
thawed, counted, inadiated, washed, resuspended at 10* cells/0.3 ml in MI99, and administered like the allogeneic tumor cells.
APPENDIX C
CYTOTOXICITY ASSAYS
For the cytotoxicity assays, the patient's lymphocytes will be used as effector cells, and K562 (NK sensitive), Daudi (NK resistant, L A K sensitive), PA-l-STK (the vaccine cells), autologous tumor cells (prepared and stored as described in Appendix A ) , and C R L 1579 (melanoma, a negative conttol) will be used as target cells, in a standard 4 hour "Chromium release assay.
O n the day of each skin test, 2 green tops will be taken from the patient, the contents diluted in buffer solution, layered over Ficoll Hypaque, spun down, the cells in the buffy layer washed in the standard manner, and frozen for use as effector cells. O n the day of the assay a flask of each target cell line is harvested, washed, counted, and viabiUty checked in trypan blue, and 2 X 10* cells of each line resuspended in 0.4 ml complete medium ( C M ) to be labeled with .08 mci "Cr (Na "Chromate) for I hr. at 37°C with gentie mixing every 10 min. The labeled cells are then washed 3 X in C M and resuspended in C M for a final count. To serve as targets at 5 X 10^ cells/well, they are diluted to 5 X lO'̂ /ml, in assay medium (AM).
By this time all the effector cells have been thawed, washed, counted, and, if possible, diluted in A M to 5 X 10* cells/ml to provide the highest effector: target (E:T) ratio of 100:1 in the assay plate. The assays are performed in 96-well u-bottom T C plates. Six two-fold dilutions of each batch of effector cells are made in the plates, 3 wells/dilution for each target, leaving 0.1 ml final effector cell volume/well, and allowing for target cell conttols, lysed and normal, on each plate. Then 0.1 ml target cells is added to each well, the plates are centrifuged Ughtly and incubated at 37°C -I- 6 % C O 2 and 9 0 % humidity for 4 hrs, centrifuged again, then harvested using Skatton, Inc. harvesting frames and filters (cat. no. 87076), and a harvesting press (cat. no. 87090) and the filters placed in 12 X 75 tubes for counts on a gamma counter. The percent lysis at each E:T ratio can then be calculated using the following formula:
effector -I- target cell count — spontaneous target cell count
maximum (lysed) target cell count — spontaneous target ceU count
% lysis = X 100
From the resulting dose response curves lytic units and the lytic index of the patient's lymphocytes can be calculated if desired.
CM = RPMI 1640 + 10% ABS A M = RPMI -1640-1- 10% ABS, HEPES-tricine,
L-glutamine and gentamicin
Assay of Precursor Cytotoxic Cells
The frequency of cytolytic lymphocyte (CTL) precursors will be measured by Mitchell's adaptation'* of the method of Vose.'5 Heparinized whole blood from a patient is passed through a nylon wool column to remove adherent cells and platelets. Peripheral blood lymphocytes (PBLs) are removed from the column-tteated blood by Ficoll-Hypaque gradient centrifugation, resuspended in RPMI-1640 -I- 1 0 % human A B s e m m (CM), washed, and frozen for use in the precursor assay at a later date, to allow all the assays to be m n simultaneously. Autologous feeder cells, used at 2 X IO''/well will be prepared from inadiated peripheral blood mononuclear (PRM) cells. Recombinant human IL-2 at 10 U/well is used as a growth factor.
For the assay 1.25 X 10^ to 2 X IO'' responder cells/well, 32 wells/dilution for statistical accuracy, are plated in 96 well round bottom plates, O.I ml/well in C M . A mixed lymphocyte-tumor ceU ( M L T C ) reaction is set up in wells to which 5 X 1 0 ^ irtadiated tumor cells are added. IL-2-induced cytotoxicity is measured in wells containing IL-2, lymphocytes, and 2 X 10^ feeder cells. To determine the frequency of cytotoxic cells, plates are incubated 9-10 days at 37°C, and fed on the 6th day with additional IL-2. Wells containing feeder cells only, or feeder cells plus tumor cells and IL-2, are used for background measurements.
For the cytotoxicity test, 5 X IO-' allogeneic ovarian carcinoma cells, PA-I STK, labeled with ("Cr) sodium chromate are added in C M to each weU. After the plates are incubated 6 hrs at 37°C, wells are harvested using the Skatton setup and their radioactivity measured in a g a m m a counter.
Positive wells are those whose counts measure more than 2 standard deviations over the mean conttol values of wells containing autologous feeder cells and stimulator cells. The number of cells plated conesponding with 37°C negative wells on a plate provides an estimate of frequency indicating one cytotoxic cell in that population according to the Poisson distribution.
This method of calculation, an iterative method based on minimization of variance, is described by Fazekas de St. Groth.^" It also permits calculation of 9 5 % confidence intervals for frequency and the chi square value of differences between 2 groups.
To check for the specificity of these C T L precursors, the ability of several unlabeled (cold) target cell lines to inhibk lysis ofthe "Cr-labeled allogeneic ovarian carcinoma line (from the vaccine) by effector lymphocytes is tested twice during patient tteatment: on day 20, 2 weeks after cycle I, and on day 62, 2 weeks after cycle 3.
Cytotoxic cells are generated in M L T C cultures, contaimng 2 X 1 0 * P M B s and 10' inadiated tumor cells in C M plus 5 U/ml IL-2. After 9-10 days in culture the effector cells are harvested and cold target competition assays set up in 96 well plates. Each well contains 5 X 10^ "Cr-labeled tumor cells of the Une used above, 2 X 10' effector cells and various numbers of "cold" target cell Unes: another ovarian carcinoma line (SK OV-3), a renal carcinoma Une (Caki 2) or a myeloid leukemia line (K562). After the plates are centiifuged lightiy and incubated 6 hrs at 37°C, wells are harvested using the Skatton setup and

CLINICAL PROTOCOL 939
counted in a g a m m a counter. Percent cytotoxicity is calculated as 100 X [cpm test wells - spontaneous release/maximum release — spontaneous release]. Percent inhibition is calculated as 100 X [I - a/b] where a = cytotoxicity in the presence of "cold" targets, and b = cytotoxicity against labeled target cells only.
APPENDIX D
PREPARATION AND ADMINISTRATION OF THE VACCINE
For the allogeneic ovarian carcinoma cell vaccine, the cell line PA-I has been selected and obtained from the American Type Culture Collection. This Une was ttansduced with a rettovttal vector to express the herpes simplex vims gene for thymidine kinase (HSV-TK) and selected in G4I8.
This gene-modified line PA-I S T K was grown as a primary (1°) seed lot in medium containing 1 0 % calf semm, trypsinized, washed, and frozen in 30 to 40 vials at 10' cells/vial in a freezing medium (CS-FM) of 2 0 % calf s e m m and 7.5% D M S O in MI99, at — 80°C ovemight in an insulated container, then stored in liquid luttogen.
From the 1° seed lot a vial of cells was thawed, washed, and used to grow a similarly sized secondary (2°) seed lot from which the cells for patient tteatment will be grown, also frozen away as above. Single lot numbers of medium, seram, and other reagents used in growing these cells have been obtained in sufficient quantity to be used for the production of aU patient tteatments from the 2° seed lot.
Vials of ceUs from the 2° seed lot will first be pretested for bacteria and fungi, and then sent to independent testing laboratories for the F D A general safety test in guinea pigs and mice, and tests for mycoplasma, reverse ttanscriptase (RT), and common human vimses (adenovkus, cytomegalovims, herpes simplex vkus, influenza vkus, parainfluenza vkus, respkatory syncytial vims, enterovkus, rhinovkus, and varicella zoster vims).
A few days before a patient tteatment is scheduled, a vial of cells from the 2° seed lot will be thawed, washed, and seeded in the requisite number of flasks needed for die vaccine treatment. O n flie day of use the cells will be harvested, washed, counted, kradiated with 10,000 rads from a cesium source, washed again, and suspended in 1000 ml normal saline for administtation of the vaccine.
APPENDIX E
CRITERIA FOR MEASUREMENT OF RESPONSE
Response shall be documented in all patients entered into the trial in accordance with standard definitions employed by the Gynecologic Oncology Group (GOG). Objective response is assessed in terms of the size of lesions measurable in at least two dimensions (Table I). Ca-125 levels should also be monitored and recorded in addition to lesion size and location. Response should be documented each time the vaccine is administered and within 6 weeks of the conclusion of the trial.
Patients who do not have cUnicaUy-assessable disease will be followed with serial Ca-125 detemunations and an imaging study, either C T scan or M R I at the conclusion of the trial. Plain films, ulttasound, or other imaging modalities may be included in the evaluation of response at the discretion of the physician, and may substitote for CT/MRI if disease progression can be documented.
Table I. Definitions of the Objective Response Employed by the Gynecologic Oncology Group
Response Definition
Complete response (CR) Complete disappearance of aU evidence of disease for at least I month
Partial response (PR) Reduction of the product of the greatest diameter of a lesion and ks perpendicular by at least 5 0 % for at least I month; these criteria must be exhibited by each measurable lesion
Stable disease (SD) Maintenance for each lesion of criteria less than those required for either a partial response or increasing disease
Increasing disease (ID) Increase of the product of the greatest diameter of a lesion and its perpendicular by at least 5 0 % or the appearance of a new lesion within I month