Embed Size (px)
Citation preview

The Trouble with Spectroscopy Papers’
Paul A. Bottomley, PhD
344
Writing a critique and guide for au-thors of clinical spectroscopy re-
search papers is a likely way of en-suring that one never sees another ofone’s own papers published in thisfield. Nevertheless, it is disappoint-ing, though perhaps predictable, thatdespite its historical foundations in
quantitative spectroscopy, the fieldhas its fair share of findings that arenot so obviously reconciled. Here isthe view of one author, one referee,and one spectroscopy protagonistabout what might be expected of aclinical spectroscopy paper. In addi-tion to novelty, the fundamental cii-teria for acceptance should be thatthe conclusions are supported byproperly and objectively quantifiedresults, and that sufficient experi-mental detail is provided so that oneskilled in the art could reproduce thestudy and its findings.
Index terms: Editorials #{149}Magnetic resonance(MR), spectroscopy
Radiology 1991; 181:344-350
1 From the GE Research and Development
Center, NMR Bldg. Rm 130, River Rd. P0 Box 8,Schenectady, NY 12309. Received July 22, 1991;
accepted July 23. Address reprint requests tothe author.
C RSNA, 1991
A decade ago, and a year after
magnetic resonance (MR) imag-
ing became practical in the body, areport of a phosphorus-31 MR spec-
troscopy study of a patient withMcArdle syndrome (1) heralded theage of clinical spectroscopy research.
It put substance to the hope that thebrands of chemistry to which thetechnology provides unique access
might now provide new insight into
disease, its clinical diagnosis, andtreatment. Like early MR imaging,initial spectroscopy studies were,
however, often of limited or heteroge-
neous patient populations and char-
acterized by poor spatial resolution.
Criticisms of the statistical rigor of
early imaging studies in establishing
clinical efficacy (2), as just or unjust asthey might be (3,4), might have been
leveled at much of the early clinical
spectroscopy work, too, if it were not
for the fact that, unlike MR imaging
(which appeared to be efficacious
anyway), MR spectroscopy has yet to
find an everyday efficacious clinical
application.
Like an author who at first dis-agrees with a reviewer’s comments,
then revises his paper to address
them, and later concedes that the re-
sulting compromise is a major im-provement over the original, we, asclinical spectroscopy researchers,
must now strive for robust, quantita-
tive documentation of our clinical
findings if we are to expect them to be
taken seriously in a medical environ-
ment where requirements for demon-
strating efficacy, or even establishingfact, grow ever more sophisticatedand onerous.
The problems with the introduction
of spectroscopy as a new medicaltechnology differ so fundamentally
from those of its sister technology,
MR imaging, to which it is inextrica-
bly linked, that its failure to material-
ize clinically with the same speed that
MR imaging arrived should be of little
surprise (5). Whereas MR imaging
provided anatomical pictures in thecontext of a long history of clinical
imaging modalities, from x rays to
ultrasound (US) and computed to-
mography, the biochemical informa-tion provided by means of spectros-copy has no real clinical antecedentsand we must look to the biochemistryresearch literature for its interpreta-
tion. Clinical MR spectroscopy and
spectroscopy papers thus fall into rel-atively uncharted territory in the fieldof radiology and in this and otherclinical journals.
LOUD AND SOFTCONTROVERSIES
That reproducibility is the key to the
successful application of spectroscopyto clinical medicine, just as it is the keyto scientific research in general, goeswithout saying. It is also easier said thandone. The Table notes a few examplesof different findings from different labo-ratories, starting with the controversyover the proton (H-i) spectroscopy
blood test for cancer (6-21). In general,discrepencies are attributable to differ-ent systematic error components in themeasurements, which include the use ofdifferent MR techniques, timing param-eters, patient protocol, and disease sta-tus. Because there are often more thanone source of systematic error and eacherror may add or subtract from the mea-sured quantities, a complete objectiveaccounting of the sources of differencesis rarely feasible on the basis of whatone finds, at least in the bodies of pres-
ent published articles. The onus is onauthors to acknowledge and providesome attempt at a feasible explanationfor any differences between their valuesand previously published quantitativevalues when they occur.
This is why the exact protocol andmethods employed for each study mustbe meticulously documented. Thingsleft unstated tend to be misstated. In myown case, a seemingly unimportantomission of stating in print between1982 and 1984 that the time required to
switch our MR imaging instrumentfrom H-i imaging to P-3i spectroscopywas typically less than 90 seconds (22)led to the misrepresentation that theswitchover time was 2-14 hours in anargument against the technology(Kaufman L, Crooks L, Margulis H. MRIat the threshold. Diagnostic Imaging
1984;[Jan]:36-43).

Reproducibility in Clinical Applications of MR Spectroscopy
Volume 181 #{149}Number 2 Radiology #{149}345
Reference Claims and Counterclaims Evidence Comments and Problems
6 Claim: cancer detection by using plasma No overlap in values between patientslipid H-i line widths with malignant tumor and healthy
subjects
7,8 Counterclaim: plasma line widths unreli- Much overlap between patients and Problems: Variable plasma triglyceride 1ev-
able for cancer detection healthy subjects els cause excessive false-positive andfalse-negative detections. Sample treat-ment
9 Claim: clinical detection of heart trans-plant rejection by using plasma lipid H-I
90% predictive value for detecting rejec-tion: normal widths in patients indicate
Comment: Can patients with rejection ofsufficient severity to require augmented
line widths rejection, but abnormal widths mean norejection
therapy be distinguished from thosewho do not? Why do normal widths sig-rtify rejection and abnormal widths sig-nify no rejection?
10 Claim: correlation between plasma glyco- Useful correlations between echocardio- Problem: reliability for predicting rejectionsylated residues and heart transplant graphic data and MR imaging in only on an individual basisrejection eight of 13 patients
11
12
Claim: brain T1(PCr) = 4.8 ± 0.2 sec,T1(-y-ATP) = 1.0 sec
Counterclaim: brain T1(PCr) = 3.1 ± 0.5sec (1.5 T), Ti(PCr) = 2.7 ± 0.2 sec (2.0
Topical MR spectroscopy in subjects at1.9 T
ISIS in seven subjects at 15 T, three sub-jects at 2.0 T
Comment: differences probably due tosystematic error. Absolute values vary-ing this much may affect quantitation ifused for correction, depending on repe-
T), T1(’y-ATP) 0.6 ± 0.1 sec (1.5-2 1) tition time. What are the correct values?13 Counterclaim: brain Ti(PCr) = 3.1 ± 0.5 ISIS at 1.5 T
sec, Ti (-y-ATP) = 1.36 ± 0.3 sec
14 Claim: normal heart PCr/ATP = 1.6 ± 0.4 DRESS, six subjects Problems: possible chest muscle contami-1516
Claim: normal heart PCr/ATP = 1.6 ± 0.2Claim: normal heart PCr/ATP = 1.72 ±
Rotating frame, six subjectsOne-dimensional phase encoding, ii sub-
nation (increases PCr/ATP); acquisition
delay (decreases PCr/ATP); partial satu-
170.15
Claim: normal heart PCr/ATP = 1.93 ±
jectsOne-dimensional phase encoding, 19 sub-
ration (usually decreases PCr/ATP, espe-cially with ISIS); cardiac motion in ISIS;
0.21 jects blood ATP contamination (decreases18 Claim: normal heart PCr/ATP = 1.7 ± 0.2 Three-dimensional spectroscopic imaging,
four adultsPCr/ATP)
19 Counterdaim: normal heart PCr/ATP = ISIS, 10 subjects1.33 ± 0.19
20 Counterclaim: normal heart PCr/ATP = ISIS, 10 subjects1.37 ± 0.09
21 Counterclaim: normal heart PCr/ATP =
0.89 ± 0.08Three-dimensional phase encoding, 14
subjects
Note.-ATP = adenosine triphosphate, DRESS = depth-resolved surface coil spectroscopy, ISIS = image-selected in vivo spectroscopy, PCr = phosphocrea-tine.
PICTURES, PEAKS, AND NUMBERS
From the outset, primary findingswith spectroscopy were displayed asgraphs of the absorption-mode intensityversus chemical shift in parts per mil-
lion and quantified numerically as me-tabolite ratios, pH units, or concentra-tions, not pictures. This mode ofquantification suits spectroscopy well tostatistical validation techniques andeven blinded studies, but at least quan-titative numerical comparisons. It is in-deed a technology well suited to the
types of quantitative analysis embraced
for scientifically rigorous clinical re-search (2).
Reformatting localized spectroscopicinformation into anatomic-style imageswhose intensities or hues are propor-tional to a metabolite or the ratio of twodoes not of itself, without additionalquantification, contribute to the estab-lishment of a robust scientific finding,which might then be found to be of din-ical value. Such displays alone do not
address the problem of interpretationposed by the unique character of theinformation, nor do they necessarily
facilitate acceptance of the technology
in radiology. Their generally poor spa-tial resolution and vulnerability to arti-
fact seldom render them usable as ana-tomic images in their own right, whichis why their interpretation in conjunc-
tion with another imaging modality,
such as MR imaging or US, has becomea virtual necessity. There is a dangerthat if spectroscopy is proffered only as
an anatomic imaging modality, it will bejudged as one. As such, it would almost
certainly fail because millirnole-per-litertissue metabolites cannot be imagedwith MR with the same quality as 100-mole-per-liter tissue water protons (5).
There is no objection to the inclusionof intensity or color-coded spectroscopic
images in a clinical paper as an aid tolocating or visualizing certain results(this may well be their forte), but thequantitative analysis of the metabolicinformation that establishes the basicfindings should be a primary consider-
ation. If we are then to change from anumerically based to an image-basedquantification in spectroscopy, a basisfor reliable and reproducible presenta-
tion and interpretation of spectroscopic
images must be established; otherwise
we will be moving backward.Thus, if spectroscopy findings are to
be evaluated by means of images alone,
there must be a proper accounting of allthe artifacts and abnormalities mani-fested in images obtained from patients,
as well as from healthy control subjects,throughout the field of view, not just
those abnormalities or artifacts that hap-pen to coincide with, say, the location ofa known pathologic condition as deter-mined with MR imaging. It must be as-sumed, until proved otherwise, that themetabolic information at the millimole-per-liter level is independent of the MRimaging information to which adipose
and tissue water are the overwhelmingcontributing moieties. Indeed, manyexamples already exist in which meta-bolic abnormalities demonstrated bymeans of spectroscopy have no obviouscorrelation with the anatomic character-istics of a pathologic condition as seen
with MR imaging: the dementia corn-plex associated with acquired immuno-
deficiency syndrome (23,24); tumors

346 #{149}Radiology November 1991
(25); and myocardial ischemia (16), to
name a few. The standard deviation ofthe noise in a spectroscopic imageshould be less than the magnitude of
the change being claimed for the metab-olite signal intensity in a particularvoxel, and this noise should not be ob-fuscated by careful windowing in “rep-resentative” examples. A reading ofspectroscopic images by multipleblinded observers would do much toallay these concerns.
NUMBERS FROM PEAKS
What should the numbers measure,
or if one must display a spectroscopicimage, what should its intensity or hue
reflect? If all spectral peaks werenonoverlapping singlets acquired underconditions in which neither the instru-ment nor the subject contributed signifi-cant inhomogeneous broadening to thespectral widths in all data sets constitut-ing a given study, the peak heights
might provide an acceptable measure oftheir source moieties. This is rarely trueor achievable in today’s clinical spec-troscopy examinations, however, and
such a claim would be difficult to vali-date and just as difficult to reproduce byothers.
Unlike peak heights, the integratedarea of an absorption-mode resonance isrelatively immune from instrument-and subject-induced line broadeningand from the complication of multipletline structure. It should therefore form
the basis of all measurements of metab-olite levels used for interexaminationcomparisons. Magnitude spectra, calcu-lated from the root of the sum of thesquares of the absorption and disper-sion modes, contain broader peaks andsignal artifacts when any broad baselinecomponents are present, as is often thecase in vivo, and are therefore usuallyunacceptable, except perhaps whenthey are derived from spin echoes. Peakheights of absorption spectra are suit-able for intraexamination comparisons
when nothing is changed that couldconceivably alter the line widths, whichincludes moving the patient.
Perversely, the areas of the peaks ofmost interest most often overlap others,
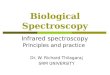
which means that the traditional run-ning integral used by chemical MRspectroscopists is unacceptable, as illus-trated in Figure 1. Area measurementsof overlapping peaks that are delimitedby saddle points are also generally lessreliable if either of the adjacent peaksvaries independently. This is because
the relative location of the saddle pointwill change as the peaks vary in ampli-tude, and most of the signal in a peakresides near its base, not its summit.Therefore, the individual peaks must bedeconvolved when they overlap.
Such deconvolution typically in-volves curve fitting a spectrum with
Lorentzian, Gaussian, or a Lorentzian-
Gaussian mixture of line shapes-whichever fits best-so that the differ-ence between the original and the fittedspectra are less than or equal to thenoise. The number used to characterize
each component resonance is then theintegral of its corresponding fitted
curve. Before curve fitting, spectra must
usually be conditioned so that they arein fact in the absorption mode, whichmay involve zero and first-order (vary-ing linear with frequency in parts per
million) phase corrections. Any broad
baseline signal components must be ac-counted for, usually by fitting or sub-traction, to avoid significant contamina-tion of the peaks of interest withspurious baseline area contributions.
Overlap is especially problematic forthe quantification of Pi in P-3i heartspectra, where it falls but a few tenths of1 ppm from one of the blood 2,3 diphos-phoglycerate (DPG) resonances in thePM region, and for the quantification oflactate in H-i spectra, which falls in aregion of the spectrum prone to containa broad lipid peak. Since lipids are ubiq-uitous in the body, conclusions aboutlactate detection in pathologic condi-tions and the assignment of signals in
the lactate region of a H-i spectrumwholly to lactate require evidence:“It isn’t lactate ‘til the fat peak is dis-counted” should be the maxim adoptedfor quantitative studies. When pH mea-surements are derived from measure-ments of the chemical shift of a curve-
fitted Pi peak in the presence of over-lapping PM in a P-31 spectrum, expectto see baseline, calibration, and sam-
pling uncertainties of about 0.04 to 0.1pH unit when the signal-to-noise ratio(S/N) is 3 or more, and up to 0.i4 pHunit or more with a S/N of i-3, even fornarrow line widths (26).
Spectral processing is automatable(27,28) if appropriate care is taken toensure that the algorithms are robust tospectra of variable quality and with spu-rious artifacts. There are also valid spec-
tral processing techniques that can beperformed on the raw time-domaindata (29,30). These techniques are analo-gous to those noted above in that theyinvolve curve fitting of the free-induc-tion-decay signal with a decaying func-tion such as the inverse Fourier trans-form of a Lorentzian (that is, an expo-nential) or a Gaussian function for eachresonance. In each case, it is importantto obtain an estimate of the noise or theS/N as an index to cross-check reliabil-ity. Since processing will vary amongstudies and sites, details of the condi-tioning applied should be fully docu-mented if that hypothetically skilled-in-the-art reader is to have a chance atreproducing the findings.
The widespread use of ratios of themetabolite integrals, as opposed to the
Figure 1. How do you quantify a P-31 brain
spectrum? A = conventional running lineintegral. Inflection points are unresolved, butintegration of the signal between the saddle
points of the respective peaks, including the
contaminating phosphodiester (PD), yields
PCr/�3-ATP of 3.4 and PCr/inorganic phos-
phate (Pi) of 2.0. B = spectrum from a 3-cm-thick axial section through the brain of a pa-
tient with suspected Alzheimer dementia inwhom a large pituitary tumor and infarctionwere seen at MR imaging during the spec-troscopy examination (brain area, 135 cm2;tumor and infarct area, 25 cm2; acquisitionmade at 1.5 T with a repetition time of 15 sec-onds, a one-dimensional ISIS sequence, auniform P-31 head coil, and a 0.5-msec acqui-sition delay) (23). Phosphomonoester (PM),
Pi, and PCr peaks overlap that of PD. By us-
ing peak heights, PCr/�3-ATP = 3.8, andPCr/Pi = 2.1. Curve fitting the spectrum (C)
to resolve the resonances (D) yields PCr/ATP
of 3.4 and PCr/Pi of 3.5 if the heights of the
component peaks are used, or PCr/ATP of2.3 and PCr/Pi of 4.1 by using the integrals of
the component peaks.
reporting of integrated areas in arbi-trary units, appropriately accounts forthe latter generally varying from studyto study with spectrometer gain, voxelsize, and other systematic differences.Accordingly, tables of arbitrary peakareas are of little use without normaliza-tion. A recent odd practice of norrnaliz-ing peak areas by dividing them by thetotal integrated area of the spectrum,however, should be acceptable only ifall of that area is fully assigned and ac-counted for (lest there be changes in
unidentified components) and if thereare no artifacts present in the total spec-trum that vary over the course of astudy (lest they systematically or ran-domly affect the findings).
Measurements of the absolute con-centrations of metabolites, rather thantheir ratios, have become increasingly

�“\
a.
-2 -1 0 1 2
Offset frequency (kHz)
-5Time (ms) Offset frequency (KI-IZ)
Volume 181 #{149}Number 2 Radiology #{149}347
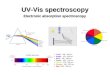
b.Figure 2. Selective excitation bandwidths
(a) of i-�-3-T (solid curve) and i-�-io-T�-s-T(dashed curve) solvent suppression 90#{176}corn-posite pulses with interpulse delays of 0.5msec (adapted, with permission, from refer-
ence 35) and (b, at right) of a single i0-mseccosine-windowed 90#{176}chemical-selective sincpulse (at left) at a 1-kHz offset frequency (36).M,5 = transverse nuclear magnetization, B1 =transverse excitation field amplitude.
important in characterizing which me-tabolites are and are not altered in vari-
ous disease states. These measurementsare performed by comparing the peakintegrals with that of a concentrationreference, but an accurate accounting ofthe voxel volume contributing to thespectrum being quantified, the transmit-ter and receiver radio-frequency fieldhomogeneity, signal loss or distortionthrough partial saturation, T2 relax-ation, j modulation, water suppression,and any Overhauser effect must be in-
cluded (3i,32). It is too easy to see howsmall systematic errors in each correc-tion required to derive a concentrationcould accumulate to produce significantor large discrepancies over and abovethe claimed random errors in concentra-tions reported from different sites orstudies (31).
Finally, one expects to see randomscatter in measurements of metaboliteconcentrations or ratios that is commen-
surate with the particular S/N of themoieties in question. Because the per-centage of uncertainty in the ratio oftwo metabolites is equal to the sum ofthe percentages of uncertainty in each,the choice of a metabolite with a lowS/N for the quotient will provide mea-surernents with larger scatter than nor-malization with a large peak. Low S/Nmay thus dictate that the error or stan-dard deviation in measurements of, say,Pi and lactate in normal P-3i and H-iMR spectra exceeds 50%. This does not
necessarily mean that the results areuseless or dismissable. If the error istruly random, a careful statistical analy-
sis of many such measurements fromdifferent study groups (preferablyblinded) can reveal a significant scien-tific or even clinically useful finding,
: � depending on whether the difference:/ between the means of each group is
I’! large enough and on the extent to
which individual data overlap. More-over, since each datum in the overlap-ping region corresponds to a patientwhose spectroscopy findings are equiv-
ocal, the question of the everyday clini-
cal utility of any spectroscopy test tendsto pivot on the proportion of cases thatexhibit such overlap.
DISTORTED SPECTRA
Distorted spectra and measurementsderived therefrom pervade in vivo spec-troscopy and are probably the majorsource of disparity among findings fromdifferent laboratories. The most corn-mon sources of distortion are Ti and T2relaxation processes, the spatial localiza-
tion technique employed, and watersuppression techniques used in H-ispectroscopy.
Different metabolites have differentrelaxation times (32,33), which results in
differential partial saturation and/orsignal decay when the repetition time is
too short or echo time too long. If repe-tition time or echo time are not speci-fled, the quantitative findings of a studymay not be reproducible. The same istrue of the flip angle of the excitationpulse that affects partial saturation.
If a surface coil is used to excite an
MR signal with a nonuniform flip angleover the field of view, authors shouldexplain their standardized protocol foradjusting the flip angle so that it is sub-stantially the same in the region of in-
terest for each of the examinations thatcomprise a clinical study. Alternatively,they should develop and validate a pro-tocol for correcting the measurementsfor partial saturation, which is prefera-ble. With such a diversity in repetition-time values and dubious flip-angle ad-justments in P-3i studies especially,why should not investigators be respon-sible for somehow correcting their ownmetabolite values for partial saturationso that others might use them for corn-parison?
Examples of distortions caused by the
localization technique used to acquire aspectrum are the baseline “wiggles” or“holes,” sometimes resembling the
wings of sinc functions, that surroundresonances that are localized by meansof methods employing imaging gradi-ent magnetic fields like DRESS andphase-encoded gradient spectroscopy.These result from the small acquisition
delay during which the gradients mustbe applied (34). Missing or attenuated
peaks such as that of 13-ATP in rotatingframe techniques (15) are apparently
due to bandwidth limitations. It may betoo much to ask that measurements becorrected for such distortions as well,but authors must provide enough of therelevant information about sequencetiming that skilled readers might gaugetheir affect on the results, if not performthe experiment themselves.
The famous “1-3-3-i” water-suppres-sion pulse often employed for H-i spec-troscopy possesses frequency responsecharacteristics with the capacity forenormous chemical shift-dependentspectral distortion (35), as illustrated inFigure 2. Chemical-selective pulses (36)
offer inherently less distortion, but theadvantage is easily lost if their widths
are too narrow. The point here is thatthe absolute ratio of, say, N-acetyl as-partate or lactate to the total creatine
pool or to choline could depend on howthe water-suppression pulse was ad-
justed. Differences between studygroups could arise from changes in theadjustment parameters or protocol.
VOLUMINOUS VOXELS
Less obvious and therefore more sin-
ister are the effects of contamination of
spectra from signals whose sources lieoutside a declared voxel, which alsohinge on how one defines voxel size
(37). If the voxel is defined only by theamplitude of a sensitivity profile and
it represents a small fraction of thevolume of a sample, it can easily beswamped by the integrated signal fromthe bulk of that sample even if the am-plitude of the signal at any point out-side the voxel is tiny (5,37). For example,motion (37,38) and partial saturation
when repetition time is less than Ti inISIS (39) are potentially overwhelmingsources of contamination, yet who per-forms ISIS with a repetition time equalto or greater than Ti? Those who do notmust describe their solutions to theseproblems.
In rotating frame and phase-encodedgradient spectroscopy, there is voxel“bleed” of signal intensity from adja-cent voxels that depends on how muchthe signal sources vary within a voxel(37), but at least all of the artifact is dis-tributed over a large expanse of thespectroscopic imaging array (as it is inMR imaging) and cannot easily find itsway into a single “localized” spectrum.The point is that a spectrum claimed tobe derived from, say, a 27-cm3 voxel in abrain tumor cannot really be said to bederived from that tumor if 80% of thesignal intensity in the spectrum is con-tamination from the rest of the brain(39).
It is also important to recognize thatbecause even the smallest spectroscopyvoxel of perhaps 1 cm3 is manifoldlarger than those of MR imaging, it will

348 #{149}Radiology November 1991
be the exception, not the rule, that vox-els are contaminated by contributionsfrom normal tissue and/or heteroge-neous pathologic conditions identifiablewith MR imaging. Conclusions, there-fore, should either be bullet-proofed ortempered by the potentially confound-ing effects of tissue heterogeneity. In
cases in which the spectral characteris-tics of one or possibly more of the tissue
components that can be identified in avoxel are well defined, it may be possi-ble to apply a correction to each spec-trum to account for and substantiallyeliminate that contamination source.
For example, blood contamination ofP-3i heart spectra in voxels intersecting
the ventricular chamber can alter theobserved PCr-to-ATP ratio, since bloodcontains AlP but no PCr. Since blood
exhibits a characteristic DPG doubletwith DPG/ATP � 30%, its affect on themyocardial PCr/ATP measurement maybe substantially compensated for bysubtracting i5% of the total integratedDPG signal from the ATP integral forthat voxel (40).
In a similar way, since liver and kid-ney contain no PCr, liver and kidneyP-3i spectra that are contaminated by
muscle signals might be corrected bysubtracting from each resonance an
amount of muscle signal contributionthat is derived from the product of theknown muscle metabolite ratios to PCr,with the measured amount of PCr con-taminating the spectrum. Care in ensur-ing that the muscle spectra are in factnormal or at least do not vary betweenstudy groups, and that metabolite ratiosassumed for the corrections are valid forthe saturation conditions present dur-ing spectral acquisition (which may ne-
cessitate use of a uniform excitation
field or a repetition time much greaterthan Ti[PCr]), would be essential in
avoiding other systematic errors in casesin which the corrections are large.
LOCALIZATION WARS
If spectroscopy were another ana-tomic imaging modality, only volume,section-selective, or “inner-volume”techniques of multivoxel spectroscopicimage localization would probably nowbe acceptable. Adoption of this posturewould dismiss the bulk of clinical re-
search findings in spectroscopy to datethat were discovered by other means(5). It would also ignore the fact that
some pathologic conditions are bettersuited to particular localization strate-
gies.It would make little sense, for exam-
pie, to employ spectroscopic imagingfor a clinical examination of a muscularmetabolic disease that globally affectedthe leg, when a simple surface receivercoil will do the trick (1,5). It would benice to have a full three-dimensional
phase-encoded P-3i spectroscopic irn-age of the heart during stress testing ofpatients with coronary disease (16), butthis presently cannot quite be accom-plished in the 5 minutes or so allotted
for spectroscopy acquisition during ex-ercise on the basis of patient tolerance.Thus, a one-dimensional or some other
three-dimensional hybrid (41) surfacecoil sequence is employed. If MR imag-ing precisely delimits a tumor, what iswrong with tailoring a single spectros-copy voxel to fit inside it and omittingacquisition of spectra from the remain-ing regions not of interest?
Witnesses to spectroscopy confer-ences still report duels between champi-
ons of localization techniques in searchof that which is unflawed or at least lessflawed, or that which is universal, yet agaggle of different strategies remainsproductive. In light of the outstandingopportunities for voxel contaminationand distortion in most in vivo situationsas noted above, we might do well toparaphrase a parable: “Let he whosevoxel is without contamination cast thefirst stone” when evaluating alternativelocalization approaches. What mattersof course, is that the artifacts are undercontrol and not overwhelming and thatthe experiment and its findings are re-producible and quantitative. The local-ization technique should be chosen tosuit the pathologic condition and thepatient limitations.
N
Studies composed of small patient pop-ulations, or larger ones that are so hetero-geneous that only one or two pathologicconditions of any single type are repre-sented, are problematic because whetherthe conclusions are characteristic of thepathologic condition in question remainsunknown. Authors of papers about one ortwo patients who conclude little morethan that one or two patients can be stud-ied with a particular technology have notadded significantly to the literature unlessthe innovation is found elsewhere in thepaper. Papers that introduce and demon-strate a substantially new technology or aparticularly unusual patient history orpathologic condition are examples ofthose in which small patient numbersmight initially be acceptable. Otherwise,study populations should be sufficientlylarge to reflect the usual range of biologicheterogeneity in each group that is care-fully defined in the Subjects section of thepaper, and large enough to establishwhether any statistically significant differ-ences exist among the groups. This usuallymeans performing identical measure-ments with a comparably sized controlpopulation.
Magnetic Resonance in Medicine now rec-ommends in its information to authors ofsubmissions that measurements from atleast four subjects for communications,and 10 subjects for full papers, be included
to establish significant biologic or medicalconclusions. While I am opposed to jour-nals setting rigid limits on the reporting ofresearch, which is supposed to be innova-tive but not rigid, and although there is
occasionally something to be said in awell-documented case study, it would not
hurt to adopt these numbers as guidelinesfor those clinical spectroscopy researchpapers that possess few other novel fea-tures and are submitted to appear in Radi-ology.
APPENDIX
Suggested Guidelines for Descriptionof Experimental Parameters in ClinicalMR Spectroscopy and Chemical ShiftSpectroscopic Imaging Studies
The following experimental parametersrepresent the consensus of a 1990-1991Spectroscopy Advisory Subcommittee ofthe Society of Magnetic Resonance Imag-ing with respect to the parameters thatdescribe in vivo spectroscopy and chemi-cal shift imaging examinations. The sub-committee members were Cecil Charles,PhD, Kamil Ugurbil, PhD, Paul Bottomley,PhD, Truman Brown, PhD, Robert Lenkin-ski, PhD, Ian Young, PhD, Wolfhard Sem-mler, MD, PhD, and Michael Weiner, MD(chairman).
I. Equipment ParametersA. Magnet
1. Static field strengthThe field strength is expressedin tesla.
2. Homogeneity adjustmentThe means of homogeneity ad-justment (shimming), includingany localization technique,should be specified, and the ho-mogeneity obtained in the givenexperiment should be reportedas frequency width half maxi-
mum in parts per million orhertz for the observed tissue.
B. Radio-Frequency Field (B1)1. Frequency of observed nucleus2. Radio-frequency coil character-
istics
a) physical/electrical/MR char-acteristics
b) size and shapec) special designs (eg, coplanar
arrays, other arrays, volume!surface coil combinations,conformal coils, and packag-ing where appropriate, as ininsertable coils)
C. Gradient FieldsDescribe the relevant gradientwaveform(s) and strength.
II. Acquisition TechniqueA. Localization Technique
I. Reference or description of lo-calization technique
2. Image reference (if appropriate)3. Solvent suppression for hydro-
gen studies: The technique andthe water-suppression factorachieved in the experimentshould be stated.

Volume 181 #{149}Number 2 Radiology #{149}349
B. Sampling TechniqueIf nonlinear techniques are used,they should be described or refer-enced and the sampling criterionnoted.
C. Artifact Reduction MethodsMethods used to minimize arti-facts, such as cardiac gating andgradient reordering, should be de-scribed or referenced.
D. Scan Parameters (underlined pa-rameters strongly recommended)
1. Repetition time
2. Echo time (if applicable)3. Inversion time (if applicable)4. Mixing period (in a two-dimen-
sional spectroscopy experi-ment, if applicable)
5. Flip angle: The procedurefor set-tingflip angle should be described.
6. Width of nonselective pulses7. Selective pulses
a) pulse widthb) bandwidthc) additional descriptors: shape
(mathematical description!graphic description), windowfunctions (eg, Hanning),number of data points inwaveform
8. Spectral width9. Field of view
10. Number of acquired points1 1 . Number of reconstructed
points (see below)12. Whetherfree induction decay, half
echo, or whole echo is acquired13. Receiver dead time delay (op-
tional)14. Additional delays in free-induc-
tion-decay acquisitions due tohardware limitations
15. Number of excitations/encod-ings/etc
16. Total imaging time (includingany dummy acquisitions)
17. Total examination time (includ-ing coil placement/shimming!data acquisition)
III. Data Reconstruction, Display, andAnalysis
A. Reconstruction1. Fourier transform or other algo-
rithm2. Zero padding or other interpo-
lation3. Filter functions used in the spa-
tial and/or chemical shift do-mains
4. Phase correctiona) orders of correction used
(zero, first, higher)b) whether manual or auto-
matic (algorithm should benoted)
5. Baseline correction: For all base-line corrections involving ad-justment of selected points tozero, the means of selectingthese points should be ex-plained.a) manual (eg, linear tilts)b) automatic: Algorithm (eg,
cubic spline) should benoted.
B. Display1. Spectra
a) Chemical shift scale shouldbe present with a chemicalshift reference identified.
b) The means of peak identifica-tion should be indicated (eg,from literature reference ortitration with standard).
c) Stack plots/contour plots:The additional dimension(time, space, etc) should beclearly labeled with appro-priate scalars, and for con-tour plots, the contour scaleshould be displayed with thedata.
2. Metabolic images (chemical shiftimaging/spectroscopic imaging)a) Images of specific chemical
shift resonances should havespatial labels (right/left, ante-rior/posterior, superior/infe-nor) for coordination with ahigh-resolution image; la-
bel(s) of the species (eg, lac-tate, Pi); any interpolationtechnique used for the im-age; the image depth (fre-quency width) in the chemi-cal shift dimension; thespectral mode displayed (eg,real, imaginary, or magni-tude component) and an in-tensity scale.
b) Images that are generatedfrom curve-fitted data ratherthan raw data should be solabeled.
C. Analysis1. Curve fitting (time or frequency)
a) Fitting algorithm should bedescribed or referenced.
b) An error analysis should beincluded.
2. A signal-to-noise analysis ofspectra should be included. #{149}
ADDENDUM
The question of the correct value
for the PCr/ATP ratio in normal hu-man heart tissue raised in the Table
was addressed at a discussion forumheld at the 10th Annual Society of
Magnetic Resonance in Medicine
Meeting in San Francisco, August iO-16, 1991. Panelists J. S. Ingwall, PhD,P. Styles, PhD, S. Schaefer, MD, P. R.
Luyten, PhD, P. M. L. Robitaille, PhD,
and I evaluated existing evidence and
reached a consensus of opinion that
the true value likely falls in the range
of 1.6-2.0. As some issues resolve,however, new ones breed at the fron-tier, such as the consistency with
which lactate detected with H-i spec-
troscopy can be induced in the hu-man visual cortex by means of visual
stimulation (42,43): Analogous experi-
ments with positron emission tomog-
raphy show increased uptake of fluo-
rodeoxygiucose with visual stim-
ulation.
References1. Ross BD, Radda GK, Gadian DC, Rocker G,
Esiri M, Falconer-Smith J. Examination ofa case of suspected McArdles syndrome by31P nuclear magnetic resonance. N EnglMed 1981; 304:1338-1342.
2. Cooper LS, Chalmers TC, McCally M, Ber-rierJ, Sacks HS. The poor quality of earlyevaluations of magnetic resonance imag-
ing. JAMA 1988; 259:3277-3280.3. Margulis AR. About articles of judgment.
Radiology 1988; 169:576-577.4. Shuman WP, Hillman BJ, Friedman PJ,
Rosenquist CJ, Stark DD. Early evalua-tions of MR imaging: worthless or worth-while? AJR 1988; 15:857-864.
5. Bottomley PA. Human in vivo NMR spec-troscopy in diagnostic medicine: clinicaltool or research probe? Radiology 1989;170:1-15.
6. Fossel ET, Carr JM, McDonagh J. Detec-tion of malignant tumors: water sup-
pressed proton nuclear magnetic reso-
nance spectroscopy of plasma. N EngI
Med 1986; 315:1369-1376.7. Engan T, Krane J, Klepp 0, Kvinnsland S.
Proton magnetic resonance spectroscopy
of plasma from healthy subjects and pa-tients with cancer. N EnglJ Med 1990; 322:949-953.
8. Okunieff P, Zietman A, Kahn J, et al. Lackof efficacy of water-suppressed proton nu-clear magnetic resonance spectroscopy ofplasma for the detection of malignant tu-mors. N EnglJ Med 1990; 322:953-958.
9. Eugene M, Le Moyec L, de Certaines J, et
al. Lipoproteins in heart transplantation:
proton magnetic resonance spectroscopyof plasma. Magn Reson Med 1991; 18:93-101.
10. Pont H, Vion-Dury J, Kriat M, et al. NMRspectroscopy of plasma during acute rejec-
tion of transplanted hearts. Lancet 1991;337:792-793.
11. Oberhaensli RD. Galloway GJ, Hilton-Jones
D, et al. The study of human organs byphosphorus-31 topical magnetic resonancespectroscopy. BrJ Radiol 1987; 60:367-373.
12. Hubesch B, Sappey-Marinier D, Roth K,Meyerhoff DJ, Matson GB, Weiner MW.P-31 MR spectroscopy of normal humanbrain and brain tumors. Radiology 1990;174:401-409.
13. Luyten PR, Groen JP, Vermeulen JWAH,den HollanderJA. Experimental ap-proaches to image localized human “PNMR spectroscopy. Magn Reson Med 1989;11: 1-21.
14. Bottomley PA, Herfkens RJ, Smith LS,Bashore TM. Altered phosphate metabo-
lism in myocardial infarction: P-31 MRspectroscopy. Radiology 1987; 165:703-707.
15. Blackledge MJ, Rajagopalan B, OberhaensliRD, Bolas NM, Styles P, Radda GK.Quantitative studies of human cardiac me-tabolism by P-31 rotating frame NMR. ProcNatl Acad Sci USA 1987; 84:4283-4287.
16. Weiss RG, Bottomley PA, Hardy CJ, Ger-stenblith G. Regional myocardial metabo-lism of high-energy phosphates during
isometric exercise in patients with coronaryartery disease. N Engl J Med 1990; 323:1593-1600.
17. Bottomley PA, Weiss RG, Hardy CJ, Baum-gartner WA. Myocardial high-energyphosphate metabolism and allograft rejec-
tion in patients with heart transplants. Ra-diology 1991; 181:67-75.

350 #{149}Radiology November 1991
18. Bottomley PA, Hardy CJ, Roemer PB.Phosphate metabolite imaging and concen-tration measurements in human heart bynuclear magnetic resonance. Magn ResonMed i990; 14:425-434.
19. Schaefer S, GoberJ, Valenza M, et al. Nu-clear magnetic resonance imaging-guidedphosphorus-3i spectroscopy of the humanheart. J Am Coil Cardiol 1988; 12:i449-1455.
20. Luyten PR, Bruntink C, Sloff FM, et al.Broadband proton decoupling in human“P NMR spectroscopy. NMR Biomed i989;1:177-183.
21. Schaefer S. GoberJR, Schwartz GG, TwiegDB, Weiner MW, Massie B. In vivo phos-phorus-31 spectroscopic imaging in pa-tients with global myocardial disease. AmJCardiol 1990; 65:1154-1161.
22. Bottomley PA, Hart HR. Edelstein WA, etal. Anatomy and metabolism of the nor-mal human brain studied by magnetic res-onance at 1.5 Tesla. Radiology 1984; 150:441-446.
23. Bottomley PA, Hardy CJ, CousinsJP, Arm-strong M, Wagle WA. AIDS dementiacomplex: brain high-energy phosphate me-tabolite deficits. Radiology 1990; 176:407-411.
24. Menon DK, Baudouin CJ, Tomlinson D,Hoyle C. Proton MR spectroscopy andimaging of the brain in AIDS: evidence ofneuronal loss in regions that appear nor-mal with imaging. J Comput Assist Tomogr1990; 14:882-885.
25. Luyten PR, Marien AJH, Heindel W, et al.Metabolic imaging of patients with intra-cranial tumors: H-i MR spectroscopic im-aging and PET. Radiology 1990; 176:791-799.
26. Madden A, Leach MO, SharpJC, CollinsDJ, Easton D. A quantitative analysis of
the accuracy of in vivo pH measurementswith 31P NMR spectroscopy: assessment ofpH measurement methodology. NMRBiomed 1991; 4:1-11.
27. Dumoulin C. Automatic peak assign-ments for in vivo 31P NMR spectra. Comput
Enhanced Spectroscopy 1984; 2:61-67.28. Nelson SJ, Brown TR. The accuracy of
quantification from 1D NMR spectra usingthe PIQABLE algorithm. J Magn Reson1989; 84:95-109.
29. Spielman D, Webb P. Macovski A. A sta-tistical framework for in vivo spectroscopicimaging. J Magn Reson 1988; 79:66-77.
30. van der Veen JWC, de Beer R, Luyten PR,van Ormondt D. Accurate quantificationof in vivo 31P NMR signals using the van-able projection method and prior knowl-edge. Magn Reson Med 1988; 6:92-98.
31. Bottomley PA, Hardy CJ. Rapid, reliablein vivo assays of human phosphate metab-olites by nuclear magnetic resonance. ClinChem 1989; 35:392-395.
32. Roth K, Hubesch B, Meyerhoff DJ, et al.Noninvasive quantitation of phosphorusmetabolites in human tissue by NMR spec-troscopy. J Magn Reson 1989; 81:299-311.
33. Merboldt KD, Chien D, Hanicke W, Gyn-geil ML, Bruhn H, Frahm J. Localized 3PNMR spectroscopy of the adult humanbrain in vivo using stimulated-echo(STEAM) sequences. J Magn Reson 1990;89:343-361.
34. Ailman T, Holland GA, Lenkinski RE,Charles HC. A simple method for pro-cessing NMR spectra in which acquisitionis delayed: applications to in vivo localized31P NMR spectra acquired using the DRESStechnique. Magn Reson Med 1988; 7:88-94.
35. Morris GA, Smith KI, Waterton JC. Pulsesequences for solvent suppression withminimal spectral distortion. J Magn Reson1986; 68:526-532.
36. Bottomley PA, Edelstein WA, Foster TH,Adams WA. In vivo solvent-suppressedlocalized hydrogen nuclear magnetic reso-
nance spectroscopy: a window to metabo-lism? Proc Natl Acad Sci USA 1985; 82:2148-2152.
37. Bottomley PA, Hardy CJ, Roemer PB, WeissRG. Problems and expediencies in hu-man 31P spectroscopy: the definition of lo-calized volumes, dealing with saturationand the technique-dependence of quantifi-cation. NMR Biomed 1989; 2:284-289.
38. Bottomley PA, Hardy CJ. PROGRESS inefficient three-dimensional spatially local-ized in vivo “P NMR spectroscopy usingmultidimensional spatially selective (p)pulses. J Magn Reson 1987; 74:550-556.
39. Lawry TJ, Karczmar GS, Weiner MW, Mat-son GB. Computer simulation of MRSlocalization techniques: an analysis of ISIS.Magn Reson Med 1989; 9:299-314.
40. Hardy CJ, Weiss RG, Bottomley PA, Ger-stenblith G. Altered myocardial high-en-ergy phosphate metabolites in patientswith dilated cardiomyopathy. Am HeartJ1991; 122:795-801.
41. Hardy CJ, Bottomley PA. “P spectro-scopic localization using pinwheel NMRexcitation pulses. Magn Reson Med 1991;
17:315-327.42. Pnchard J, Rothman D, Novotny E, et al.
Lactate rise detected by ‘H NMR in humanvisual cortex during physiologic stimula-tion. Proc NatI Acad Sci USA 1991; 88:5829-
5831.43. Merboldt KD, Bruhn H, Gyngell ML, Han-
icke W, Michaelis T, FrahmJ. Variabilityof lactate in normal human brain in vivo:localized proton MRS during rest andphotic stimulation (abstr). In: Book of ab-
stracts: Society of Magnetic Resonance inMedicine 1991. Berkeley, Calif: Society ofMagnetic Resonance in Medicine, 1991;
392.