Embed Size (px)
Citation preview

The use of antiretroviral agents during pregnancy in Canada and compliance with North-American guidelines
I. Boucoiran, T. Lee, K. Tulloch, L. Sauve, L. Samson, J. Brophy,
M. Boucher and D. Money
For and members of the Canadian Pediatric HIV Surveillance Program (CPHSP)
CONFLICT OF INTEREST DISCLOSURE
The authors declare no conflicts of interest
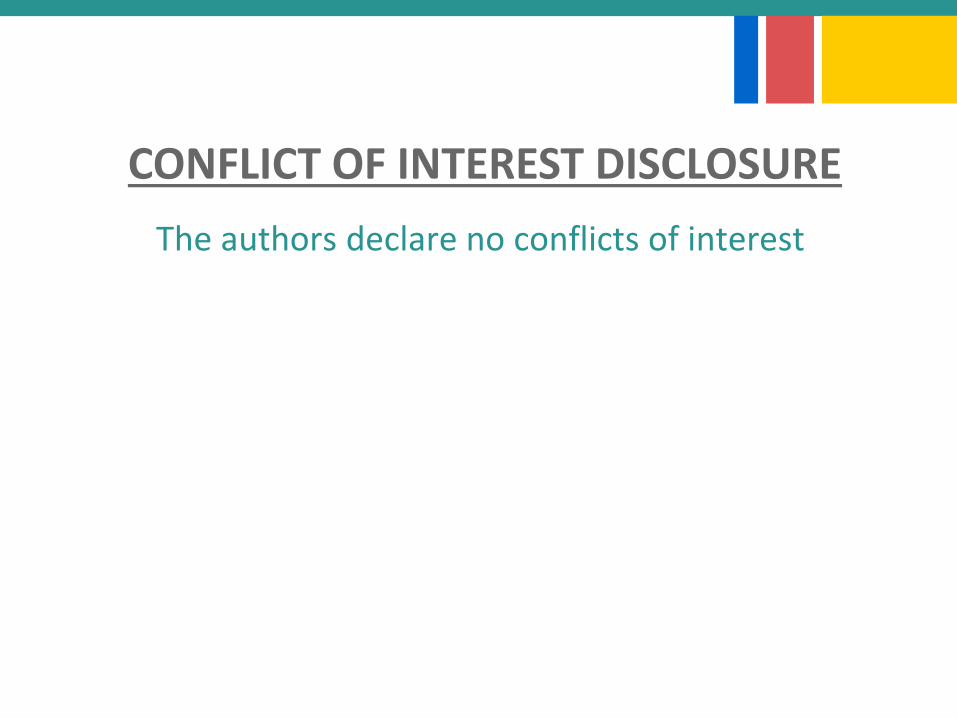
Current Antiretroviral medications
August 20153
NRTI
Abacavir (ABC)
Didanosine (ddI)
Emtricitabine (FTC)
Lamivudine (3TC)
Stavudine (d4T)
Tenofovir DF (TDF)
Zidovudine (AZT, ZDV)
NNRTI
Efavirenz (EFV)
Etravirine (ETR)
Nevirapine (NVP)
Rilpivirine (RPV)
PI
Atazanavir (ATV)
Darunavir (DRV)
Fosamprenavir (FPV)
Indinavir (IDV)
Lopinavir (LPV)
Nelfinavir (NFV)
Saquinavir (SQV)
Tipranavir (TPV)
Pharmacokinetic
Enhancers
Ritonavir (RTV, /r)
Cobicistat (COBI)
Entry Inhibitor
Enfuvirtide (ENF, T-20)
Maraviroc (MVC)
INSTI
Raltegravir (RAL)
Elvitegravir (EVG)
Dolutegravir (DTG)
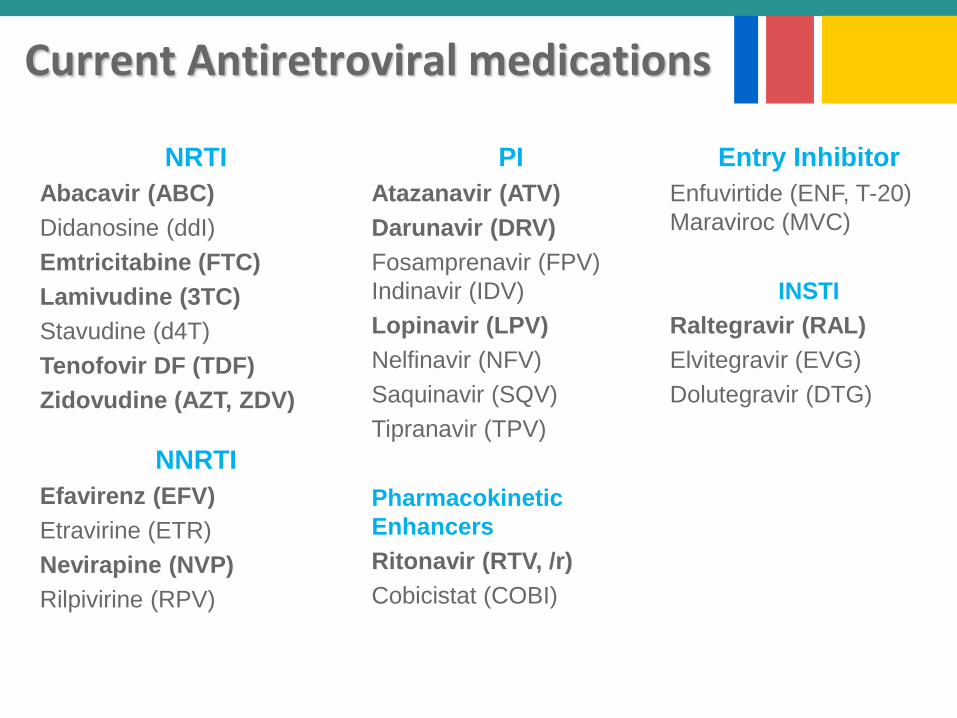
North American HIV Perinatal Guidelines
HHS US 2004
HHS US 2005
HHS US 2006
HHS US 2006
HHS US 2007
HHS US 2009
HHS US 2011
HHS US 2013
HHS US 2015
+ Canada: CMAJ (2003), SOGC (2013)
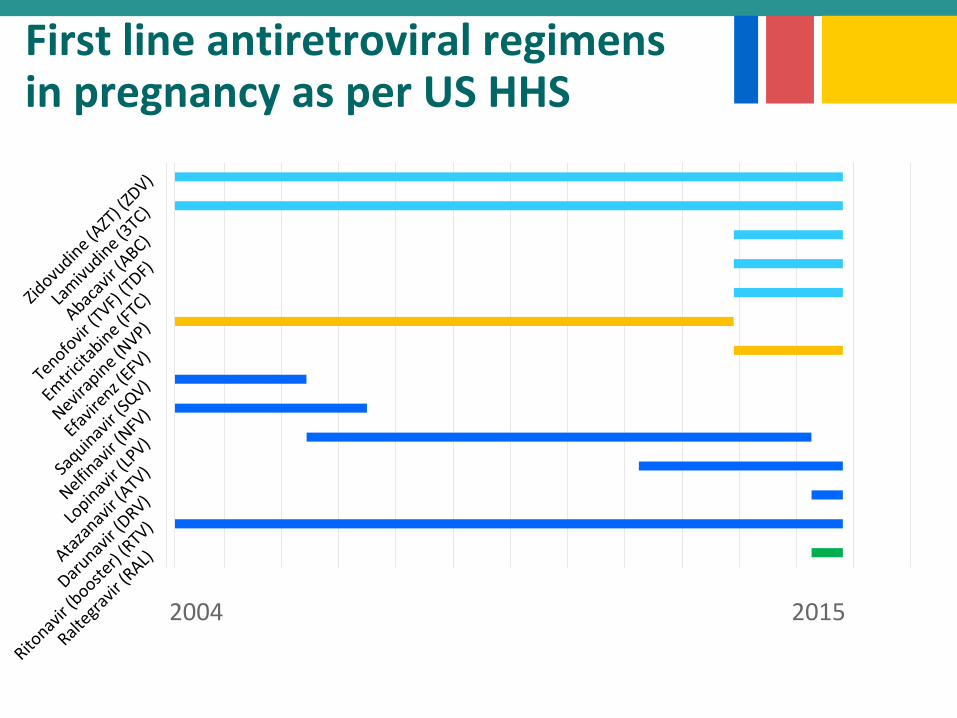
First line antiretroviral regimens in pregnancy as per US HHS
2004 2015
Treatment as prevention
►How the use of antiretroviral therapy (ART) in pregnancy is influenced by evolution of perinatal and adult guidelines in Canada?
►Objectives: – To describe trends in Canada for the use of
ART in pregnancy– To compare ART received at conception/1st
trimester or initiated in pregnancy with North-American guidelines.
Research question
► Since 1984
► 22 sites in Canada
► Collected data: demographics, antiretroviralexposure, HIV testingoutcome of the infant.
► Data management and analysis provided by the Canadian Institutes of HealthResearch – Canadian HIV Trials Network (CTN)
CPHSP: the Canadian Perinatal HIV Surveillance Program
Methods
►ARV categorization according to: – Available guidelines at the time of conception– 2015 guidelines
►Mother infant pairs included between 2004 and 2015
n = 2355 pregnancies(1839 women)
Exclusion criteria:
• No ARV in pregnancy (n=157)
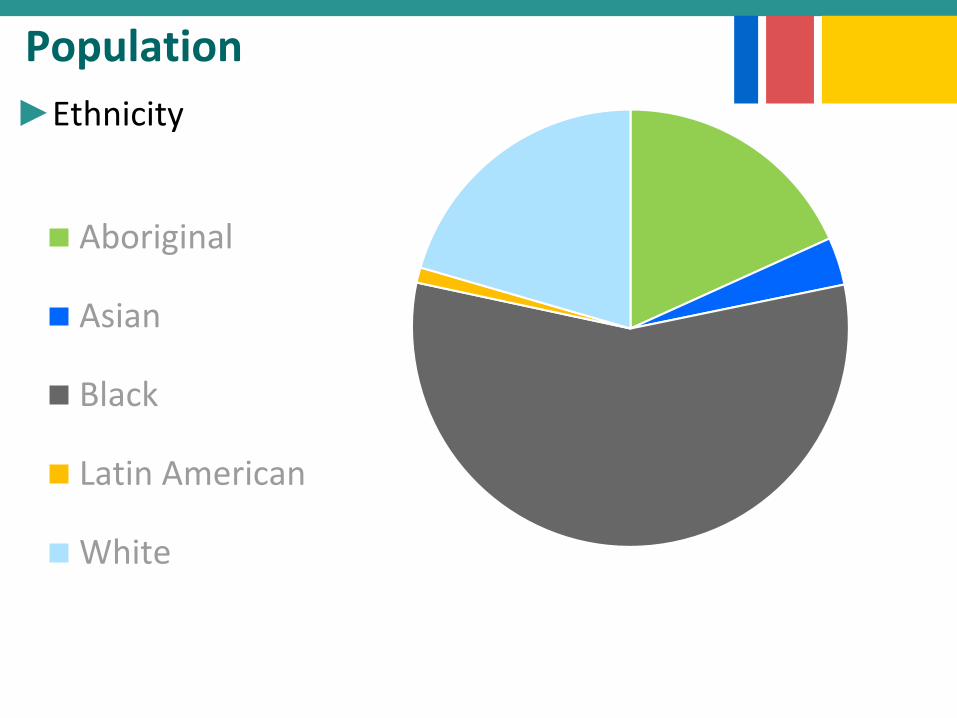
Population
►Ethnicity
Aboriginal
Asian
Black
Latin American
White
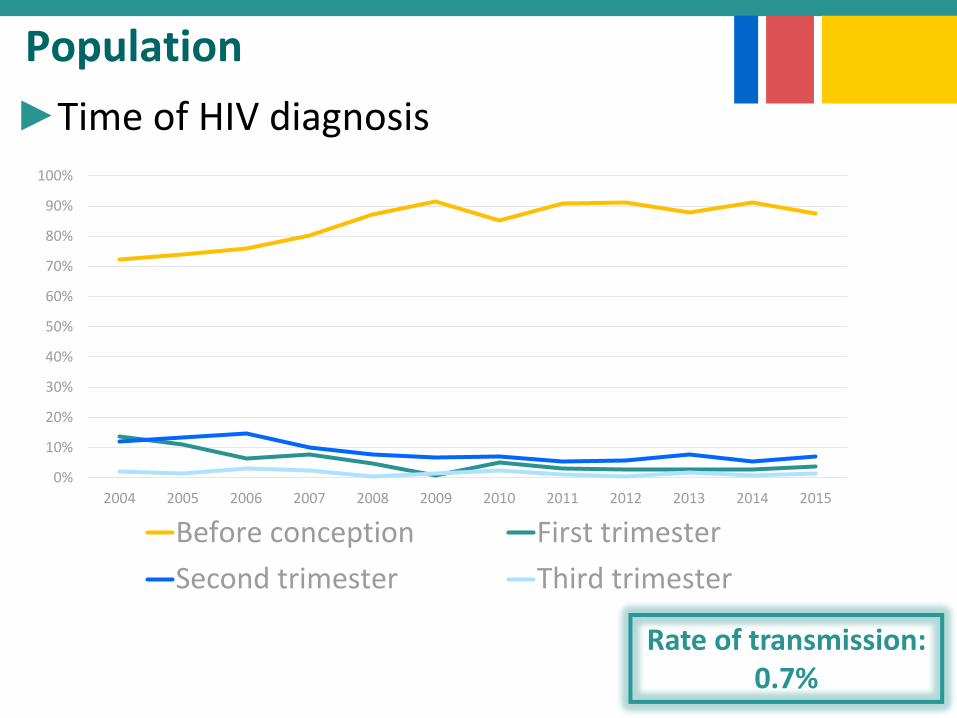
Population
►Time of HIV diagnosis
Rate of transmission: 0.7%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Before conception First trimester
Second trimester Third trimester
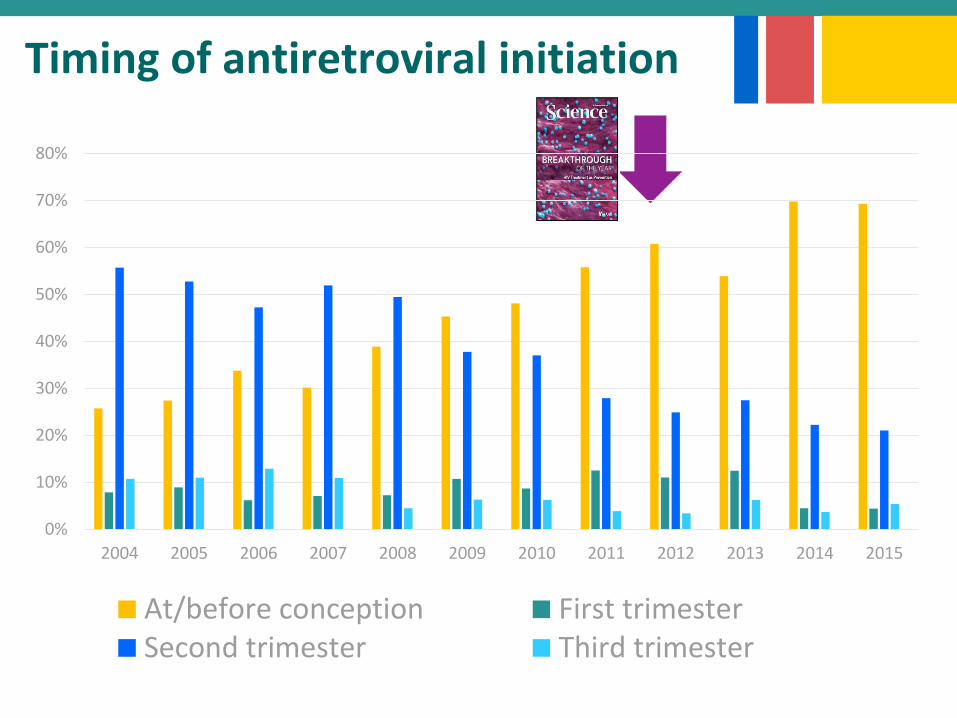
Timing of antiretroviral initiation
0%
10%
20%
30%
40%
50%
60%
70%
80%
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
At/before conception First trimesterSecond trimester Third trimesterDetectable VL at delivery
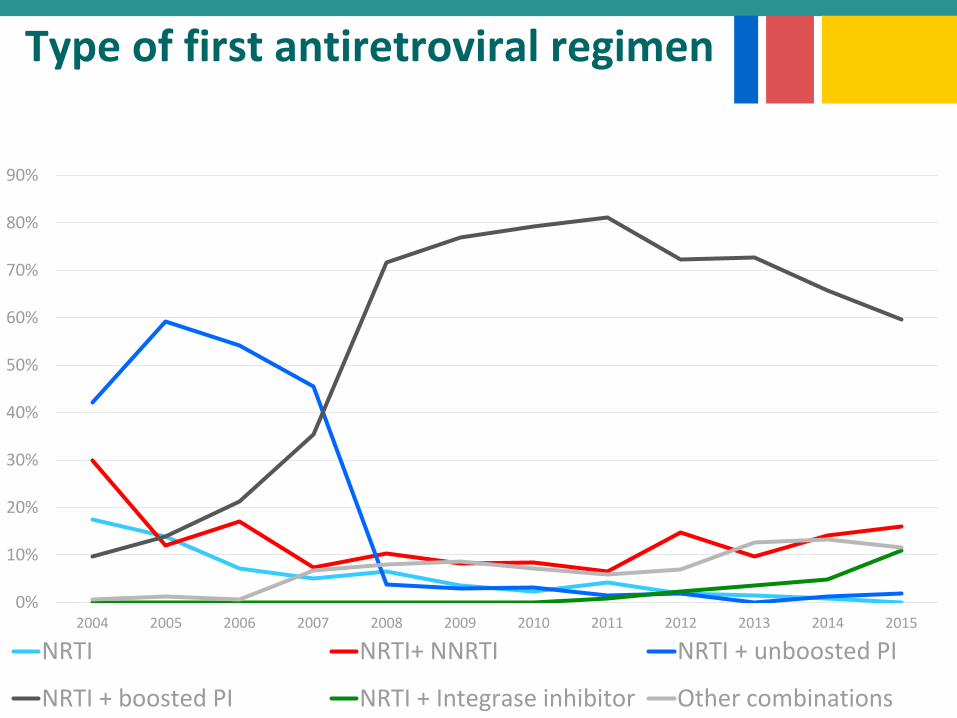
Type of first antiretroviral regimen
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
NRTI NRTI+ NNRTI NRTI + unboosted PI
NRTI + boosted PI NRTI + Integrase inhibitor Other combinations
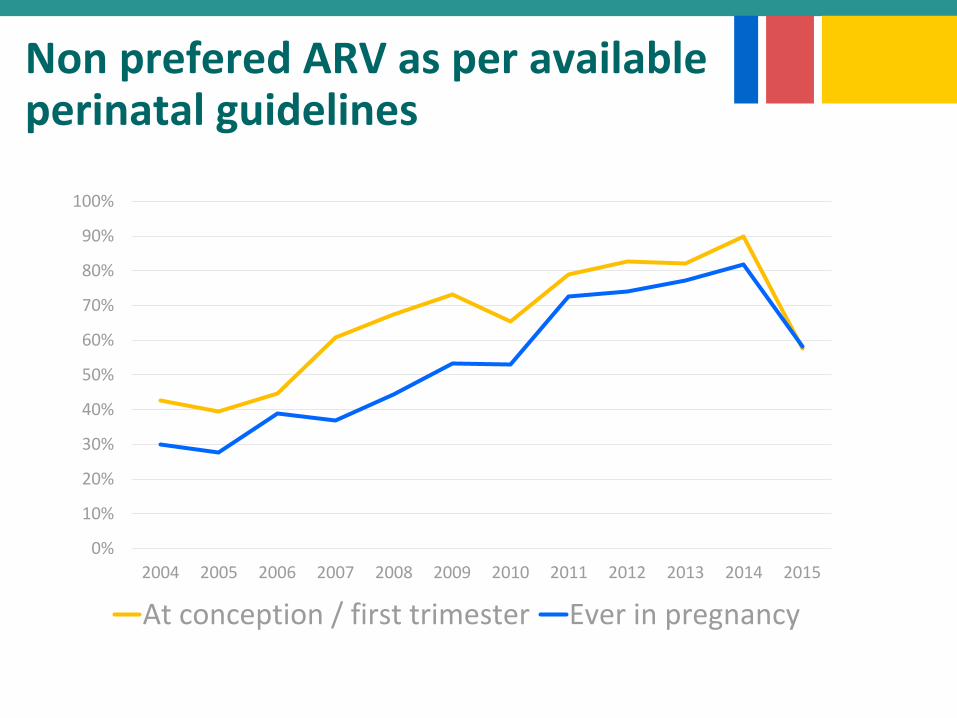
Non prefered ARV as per availableperinatal guidelines
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
At conception / first trimester Ever in pregnancy
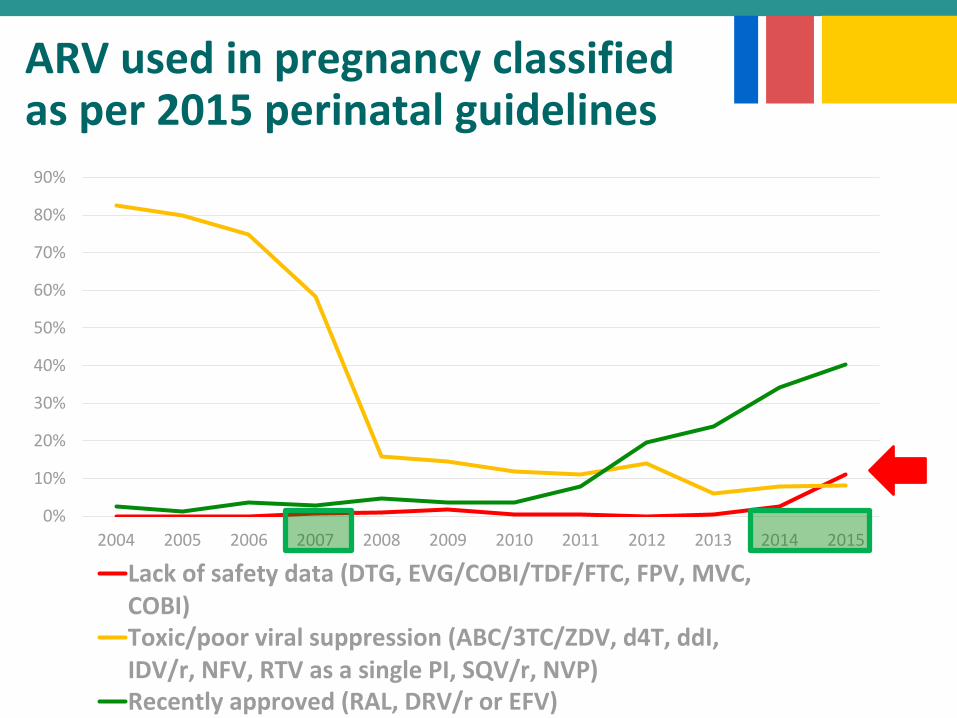
ARV used in pregnancy classifiedas per 2015 perinatal guidelines
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015
Lack of safety data (DTG, EVG/COBI/TDF/FTC, FPV, MVC,COBI)Toxic/poor viral suppression (ABC/3TC/ZDV, d4T, ddI,IDV/r, NFV, RTV as a single PI, SQV/r, NVP)Recently approved (RAL, DRV/r or EFV)
Comments
►Moving practice
►Clinical practice advancing ahead of perinatal guidelines
►Limits– No data on congenital anomalies and spontaneous
abortion– No genotype data
Conclusions
►A high number of HIV-infected women receiving ART at the time of conception tend to be treated with not preferred ART as per North-American perinatal guidelines.
►Concern in the context of the licensure of new ART medication: Principles of antiretrovirals selection in pregnancy should be considered when prescribing ART to women in reproductive age

Thank you
General Principles of AntiretroviralsSelection in Pregnancy
►Consider and discuss the benefits vs. risks of each ARV
– Concerns about specific ARVs during pregnancy
– Limited experience during pregnancy with newer ARVs
– ARV drug-resistance
– Gestational age at ARV initiation
– Increased volume of distribution / pharmacokinetics
– Adherence – hyperemesis and substance use
– Interactions with other medications
►Ensure that at least 1 NRTI with high placental transferis included in cART regimen for sufficient infant preexposure prophylaxis.
►Coordinate between HIV and OB specialists.
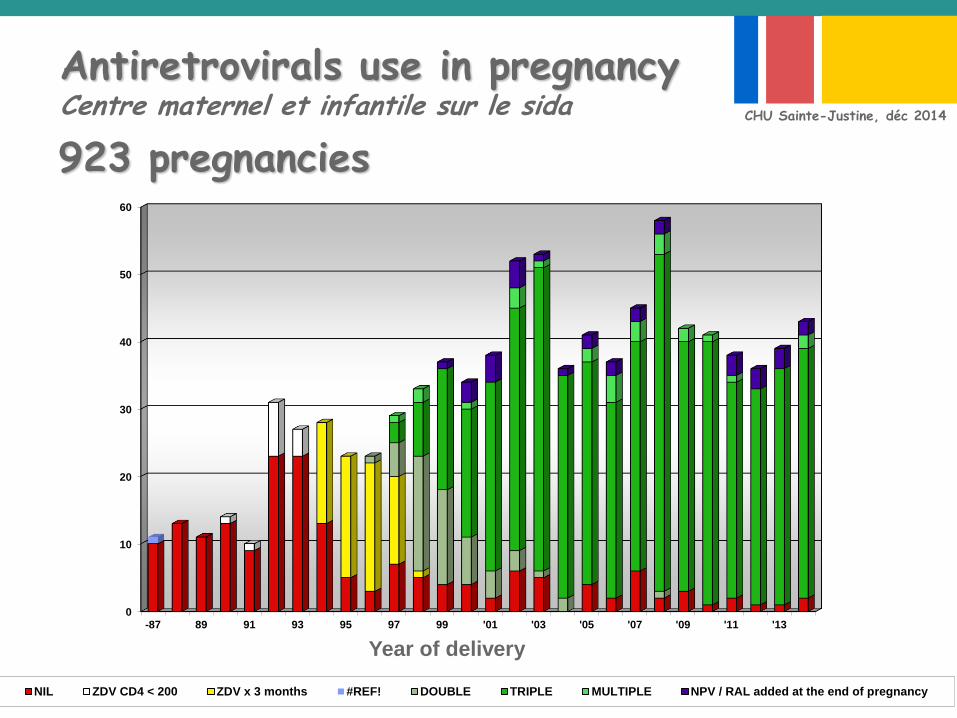
Antiretrovirals use in pregnancy Centre maternel et infantile sur le sida
0
10
20
30
40
50
60
-87 89 91 93 95 97 99 '01 '03 '05 '07 '09 '11 '13
NIL ZDV CD4 < 200 ZDV x 3 months #REF! DOUBLE TRIPLE MULTIPLE NPV / RAL added at the end of pregnancy
Year of delivery
CHU Sainte-Justine, déc 2014
923 pregnancies
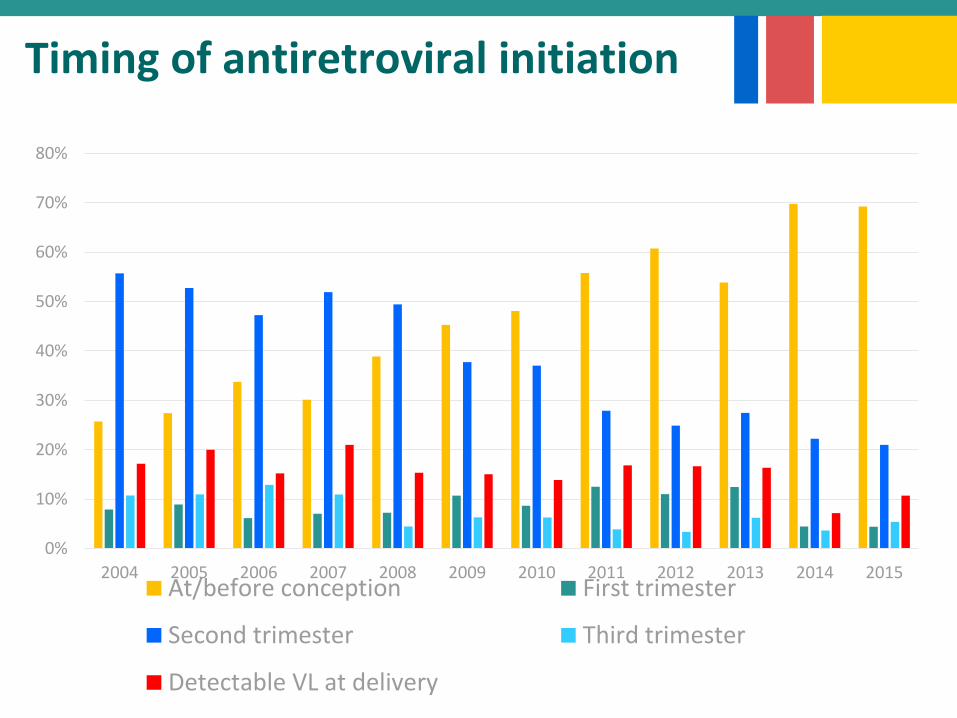
Timing of antiretroviral initiation
0%
10%
20%
30%
40%
50%
60%
70%
80%
2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015At/before conception First trimester
Second trimester Third trimester
Detectable VL at delivery