Embed Size (px)
Citation preview

PA55CH05-Cohen ARI 29 November 2014 10:39
The Use of Biomarkersin Human Pharmacology(Phase I) StudiesA.F. Cohen,1,2 J. Burggraaf,1,3 J.M.A. van Gerven,1,2
M. Moerland,1 and G.J. Groeneveld1,4
1Centre for Human Drug Research, 2333 CL Leiden, The Netherlands; email: [email protected] University Medical Center, 2333 ZA Leiden, The Netherlands3Leiden Academic Centre for Drug Research, Leiden University, 2333 CC Leiden, TheNetherlands4VU University Medical Center, 1081 HZ Amsterdam, The Netherlands
Annu. Rev. Pharmacol. Toxicol. 2015. 55:55–74
First published online as a Review in Advance onOctober 6, 2014
The Annual Review of Pharmacology and Toxicologyis online at pharmtox.annualreviews.org
This article’s doi:10.1146/annurev-pharmtox-011613-135918
Copyright c© 2015 by Annual Reviews.All rights reserved
Keywords
question-based drug development, surrogate endpoints, clinical trials,precision medicine, prediction in pharmacology
Abstract
The development of a new medicine is a risky and costly undertaking thatrequires careful planning. This planning is largely applied to the opera-tional aspects of the development and less so to the scientific objectives andmethodology. The drugs that will be developed in the future will increas-ingly affect pathophysiological pathways that have been largely unexplored.Such drug prototypes cannot be immediately introduced in large clinicaltrials. The effects of the drug on normal physiology, pathophysiology, andeventually the desired clinical effects will need to be evaluated in a structuredapproach, based on the definition of drug development as providing answersto important questions by appropriate clinical studies. This review describesthe selection process for biomarkers that are fit-for-purpose for the stageof drug development in which they are used. This structured and practicalapproach is widely applicable and particularly useful for the early stages ofinnovative drug development.
55
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
INTRODUCTION
In the 1960s, Black et al. (1) discovered propranolol, the first successful antagonist to the β
adrenoreceptor. Techniques for testing the pharmacology of the novel drug in humans werealready available (2, 3), and before the drug was tested in patients (4), the effects of the β-blockeron the actions of epinephrine (5) were tested in healthy volunteers after infusions in the brachialartery. Thus, progression of a receptor blocker from molecular pharmacology through animalpharmacological models to human tests using pharmacological challenges to clinical trials in adiseased population is not a new approach.
In the half century following these landmark studies, as drug development progressed andincreased in size and complexity, this logical scientific approach was largely abandoned ratherthan expanded. In an earlier paper, we showed that in the Netherlands, most early studies withnew medicines in humans had clinical tolerability as the primary objective rather than an indicationof the human pharmacology of the compound (6). The puzzling question that arises is why earlystudies are not designed to be more informative. The answer may be that most medicines arenow developed for chronic diseases including cancer, diabetes, or inflammatory conditions such asatherosclerosis. The discovery of a new drug candidate is based on presumed effects on biochemicalor immunological mechanisms, but the important clinical effects can only be discovered over thelong term using outcome measures such as improvement in function or survival. Early knowledgeof precise, quantitative, pharmacological effects is often not seen as predictive of later clinicalevents.
An example is the cholesteryl ester transfer protein (CETP) inhibitor torcetrapib (7). Exten-sive validated evidence that increased high-density lipoprotein (HDL) cholesterol was associatedwith beneficial effects on survival from atherosclerosis existed when the drug was discoveredand developed. Researchers knew that inhibition of CETP would increase HDL (the short-termpharmacological effect), implying that it therefore would reduce mortality in patients with vas-cular disease (the clinical effect). Initial studies in healthy subjects demonstrated the quantitativerelationship between the blood concentration of the CETP inhibitor and CETP inhibition andincreases in HDL cholesterol (8). Unfortunately, clinical trials with this compound demonstratedno beneficial clinical effects (7, 9) and had negative effects on cardiovascular events. The develop-ment of the drug continued until the definitive clinical studies demonstrated these adverse effectsconvincingly, and development was stopped at a cost of about $800 million. The reason why anapparently beneficial improvement in a well-known and apparently validated marker of vasculardisease (HDL cholesterol) did not lead to clinical improvement has not been fully elucidated butmay have been caused by other effects of torcetrapib, notably increases in blood pressure and ef-fects on aldosterone secretion. These effects were potentially detectable in animals (10) and wereseen in earlier studies (11) and even in late clinical studies (9, 12).
This therapeutic failure may have added to existing skepticism about the usefulness of collectingearly pharmacological data in human studies (13). However, integration of the available data fromearly human pharmacology could arguably have prevented this mishap. Examples such as thisshould probably lead to collecting and above all connecting more, rather than less, data on thepharmacological effect profile.
There are several other examples similar to this, such as the CD28 agonist TGN 1412 thatcaused severe immunological damage (14) and the polymer RheothRx that produced renal damageand excess death (15) in human trials despite earlier available data that indicated this possibility(16, 17). The question of why such obviously negative information obtained in the early stagesof research was not adequately investigated will probably never be answered (16) but can be seenas an important motive for a more integrated form of knowledge management in the clinical
56 Cohen et al.
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
INVESTIGATIONAL MEDICINAL PRODUCT
An investigational medicinal product is a pharmaceutical form of an active substance or placebo being tested or usedas a reference in a clinical trial. This includes products that already have a marketing authorization but are used orassembled (formulated or packaged) differently from the authorized form, used for an unauthorized indication, orused to gain further information about the authorized form.
development of new medicines. Here we present a comprehensive approach that is applicable toa wide range of new interventions and can be implemented relatively easily. In this review, weuse the words drug, medicine, and compound for brevity as synonyms for the term investigativemedicinal product used in the regulatory directive (18) (see the sidebar entitled InvestigationalMedicinal Product).
PHASE I STUDIES AND BEYOND
Traditionally, the process of developing a new medicine is divided into four distinct and consecu-tive phases, which are described clearly in many textbooks (19). Phase I studies commonly have thesimple aim of providing information about tolerability (evaluated by the incidence of subjectiveside effects), safety (measured by side effects and laboratory values), and the pharmacokinetics ofthe drug. In many cases, researchers make an attempt to find the maximally tolerated dose. Thestudies are often done in healthy male subjects, unless inherent toxicity of the compound precludesthis, as for the traditional cytotoxic drugs. In Phase II, the diseased subject is studied, and the dose ofthe drug is titrated against a measure of disease activity. Phase III is for the performance of the con-trolled trials that lead to registration, and Phase IV trials are those done after marketing approval.
The US Food and Drug Administration (FDA) and the European Medicines Agency (EMA)issued a guideline on general aspects of clinical trials in 1998 that made the clear point that a linearapproach to drug development is not recommended (20). The regulatory guidance starts withthe statement that “The essence of rational drug development is to ask important questions andanswer them with appropriate studies” and subsequently gives the rationale for using a system ofclassification based on objectives rather than the passage of time (20). The regulatory authoritiesdescribe drug development as an adaptable series of studies in which, as in all scientific evaluation,previous experiments determine the nature of the subsequent experiments. Such an approach isincompatible with the phased approach, in essence a linear time series of experiments. In fact,a Phase III trial may easily generate further preclinical or even (traditional) Phase I trials; theCETP inhibitor torcetrapib, mentioned above, is a case in point, as the findings in late-stage trialsprompted further preclinical work to elucidate the mechanism of the off-target effects on bloodpressure. The choice between a phased approach and a more cyclical form of project managementin innovation has been the subject of much work in the management literature (21, 22). It isgenerally accepted that a phased approach is appropriate for the standard development of incre-mentally innovative projects, in which the expected end result is known and few unknown findingsare expected. In the 1998 guideline, the EMA had already stipulated that new drug developmentrequired a more cyclical approach than the hitherto-accepted phased one (20).
This guideline is generally ignored, even by the regulatory agencies themselves, who haveadhered to classifying research according to the passage of time rather than objectives and haveadded more subphases (0, IIa, and IIb). We have argued earlier that, in early phases of development,this classification is uninformative and that the objectives of tolerability and safety in human
www.annualreviews.org • Use of Biomarkers in Human Pharmacology 57
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
pharmacology studies cannot be attained because of the small number of subjects exposed in theseearly trials, unless unexpected severe toxicity occurs (23). In this review, we use the preferredterms from the EMA guideline, based on the objective of the studies (human pharmacology,therapeutic exploratory, and use studies), rather than Phases I–IV. Our focus is the establishmentof a logical and practical system for the selection and use of biomarkers in human pharmacologyand therapeutic exploratory studies.
THE DRUG PROTOTYPE
The rational development of new medicines, as an adaptable series of studies designed to answerimportant questions (20), is most applicable to a subset of innovative products with a novel mech-anism of action. In these situations, the uncertainty about the different aspects of the drug is thegreatest, and flexibility in the drug development program and innovative methods are the mosturgently required.
The definition of this subset of projects is important for research organizations because theproject management is radically different depending on the type of compound. The innovativenature of a compound depends on two continuous variables (6). One is the level of certainty aboutthe link between the pharmacological/physiological mechanism and the intended clinical effect.The other is the level of validation of a measurement or set of measurements that indicates thestrength of this link. When both are at a high level, as in the case of a generic version of an existingeffective drug from a well-established class, there are a limited number of unknown areas that canbe managed easily during development. Such compounds can be developed in a highly organized,time-phased fashion and are not the subject of this review. The project management of innovative,high-uncertainty projects requires different management, staff competences, and systems that arelargely related to the integration of information rather than the purely operational requirementsof a generic development program (22).
OVERVIEW OF DEVELOPMENT MODELS
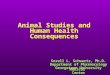
Many models for drug development have been described (see Figure 1). By the time the FDAguideline was released, Sheiner (24) had already introduced a cyclical model of development thatrecommended cycles of learning and confirming research. He emphasized that much can be learnedfrom existing data by applying mathematical models that still assume a time-phased approach withall measurement techniques to attain the goals already in place. In a paper on mechanism-basedmodeling, Danhof et al. (25) proposed seven classes of measurements that could be used in clinicaldevelopment and recommended that these be used in mathematical models to assist in decisionmaking in the development process. This classification is conceptually interesting but has thedrawback that the classes are not mutually exclusive and are represented in a linear manner, as ifone would always follow the other.
Lalonde et al. (26) and Milligan et al. (27) described an integrated, model-based drug develop-ment paradigm in which all aspects of the development program, from modulation of a biological
−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−−→Figure 1Models of development and biomarker classification. (a) The learn-and-confirm paradigm from Sheiner, adapted from Reference 26with permission. (b) The mechanism-based biomarker classification by Danhof et al. (25). (c) Model-based drug development byLalonde et al. (26) and Milligan et al. (27). Abbreviations: M&S, modeling and simulation; PD, pharmacodynamics; PK,pharmacokinetics. Panel b adapted from Reference 25 with permission. Panel c adapted from References 26 and 27 with permission.
58 Cohen et al.
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
Drug development and model buildinga
b
c
Learning and confirming
Continuum of learn/confirm/predict at each decision point
M&S
Preclinical Phase I Phase IIa Phase IIb Phase III Registrationlabeling
Phase IV
EfficacyToxicologyPK/PD
TolerationHuman PK/PD
Efficacy and safetyDose or exposure-responseDose adjustments
Therapeutic indexCovariate effects
Results relative to competitors,regional differences, and therapeutic index
UncertaintyConfidence in drug and disease
Type 0Phenotype/
genotype
Type 1Drug
concentration
Type 2Target
occupancy
Type 3Target
activation
Type 4Physiological
response
Type 5Pathophysiological
response
Type 6Clinical
response
Trial performance
metrics
Quantitative
decision criteria
Data
analysis model
PK/PD and
disease models
Model-based
drug developmentCompetitor information
and meta-analysis
Design and trial
execution models
Systemsbiology
Pathway
Systemspharmacology
Target
Translationalsciences
Drug
Exposureresponse
Benefit/risk
PD
PKConcentration Time
PK/PD
Effect
Optimizedmedicines
Right pathway Right target Right molecule
Impact
Right dose Right patients
Rationale #1 Rationale #2 Rationale #3 Rationale #4 Rationale #5
Effectiveness and
reimbursement
www.annualreviews.org • Use of Biomarkers in Human Pharmacology 59
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
pathway to financial reimbursement on the basis of cost effectiveness, can be included. Theydemonstrated that a quantitative approach, using mathematical models that allow simulation ofresearch steps, can lead to increased efficiency.
All these models are conceptually elegant and statistically and mathematically complex, butthey depend fully on what is measured and how well such measurements reflect the objectivesof the research or, in the words of the FDA guideline, how well they address certain questions.Therefore, applying the inappropriate measurement to a particular question can result in anunsuccessful development trajectory.
In the 1990s, a generally accepted measure for cardiac arrhythmia—the number of ventricularextrasystoles during continuous ECG recording—was reduced effectively by several drugs, but allincreased mortality (28). This was an excellent demonstration of how a pharmacological mech-anism (interference with Na+ channels in the cardiomyocyte) affected a measurement of organfunction (number of extrasystoles) but did not correlate with the clinical endpoint (improvementof survival). Although it has often been stated that this result invalidates the measurement of ex-trasystoles, this is only true in the sense that they are not a valid surrogate for the effect of thedrug on survival. However, they are a very good measure for the drug’s effect on Na+ channels. Inthe majority of subjects, there is no direct association between extrasystoles and survival. Anotherexample of pharmacological effects being used erroneously as a surrogate was the dopaminergicdrug ibopamine. Introduced in the 1980s with positive effects on renal and cardiac hemodynamicsin heart failure (29, 30), it was marketed for a long time between 1991 and 1995 before trialsof mortality and morbidity first raised doubts (31). Subsequent trials with mortality as the end-point demonstrated that the drug was actually deleterious (32), and ibopamine was withdrawnfrom the market. Clearly, the short-term improvement of heart function was not a surrogate forimprovement of the mortality rate (33). This demonstrates the importance of using a model thatindicates what questions have to be asked, what methodology is used for providing the answers,and how the progression to establishing the efficacy and safety of a medicine is mapped andcommunicated.
A NEW, PRACTICAL, CONCEPTUAL MODEL FOR EARLYPROTOTYPE DEVELOPMENT
Any proposed conceptual approach to the development of new medicines is a method of communi-cation within a project team, from the project team to management and funders and to authoritieswho judge the value of a new treatment. Moreover, there is an increasing need for communicationto the patients or their representatives, who will rightly want to play a role in the development.Any model should therefore be relatively simple and provide continuous opportunities for trackingprogress.
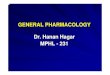
Our proposed approach starts with the determination of the prototypical nature of the drugcandidate (Figure 2). In practice, this means that the validation of the target must be judgedagainst the validation of the available measurement systems. This model was introduced as aconceptual model of development (6), indicating the need for validation of the targets as well asthe biomarkers. This model is supplemented by the model of Danhof et al. (25), which describesa logical nomenclature of biomarker types linked to their purpose for biomarkers of drug activity,and the model-based drug development approach described by Milligan et al. (27) and Lalondeet al. (26). The synthesis of models we now describe may be a useful tool to plan developmentand track progress. Moreover, this synthesis makes clear that drug development is not a directtrajectory from a prototype to a drug in practical use. We have reported earlier that in a set ofhuman pharmacology (Phase I) studies submitted to the Netherlands Clinical Trial Competent
60 Cohen et al.
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
0. Assays to identify
and validate targets
1. Drug concentration
2. Target occupancy
3. Target activation
4. Physiological response
5. Pathophysiological response
6. Clinical response
Pathway Target Drug Benefit/
risk
Efficacy/
reimbursement
LSF
CASTi
ii
iii
iv
Figure 2Identification of prototypical projects. This model incorporates the drug development models of Danhofet al. (25), Milligan et al. (27), and Cohen (6). The thick white line indicates a perceived ideal drugdevelopment trajectory in which, after identification of a suitable drug molecule, trials are performed thatshow clinical utility. Unfortunately, the situation is often more like that of the antiarrhythmics in the CardiacArrhythmia Suppression Trial (CAST, red circle) (28), in which a target was chosen (Na+ channels in themyocyte) and an inhibitor (flecainide) and a physiological biomarker (extrasystole on the ECG) wereestablished. The final trial incorrectly assumed that this was a clinical biomarker, and the trajectory (thinwhite line) turned toward a late-stage failure (LSF, yellow circle), causing doubts about whether the pathwayand target were correct for the clinical endpoint (mortality). The blue line indicates a hypothetical programwith learn-and-confirm cycles at many points, biomarkers that are tuned to the objective of the developmentstage, and a longer, but in this case successful, development program with reduced risks. Note that in theearlier phases, a loop (dashed line) back to the prototypical state—in that case, often for a differentindication—is possible. Figure adapted from References 6, 25, and 27 with permission.
Authority, the use of early quantitative markers of drug action was still very low in 2009 (6).Many examples from the past, as presented in this review, do not support this fast-lane approachfor prototypes. The model presented in Figure 2 allows investigators to make the prototypicalstate of a new drug explicit. If the link between the biological mechanism and a disease is alreadystrongly established and good biomarkers are available for all stages, development can be standard.In other cases, the nonstandard approach must be determined on a case-by-case basis. The nextsection presents a practical approach to this.
DEFINITIONS OF BIOMARKERS
Beginning around 1990, drug development scientists were increasingly interested in quantitativemarkers of disease activity, perhaps influenced by the need to obtain rapid quantitative indications
www.annualreviews.org • Use of Biomarkers in Human Pharmacology 61
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
Biomarkerqualification:evidentiary andstatistical processlinking biological,pathological, andclinical endpoints tothe drug effect orlinking a biomarker tobiological and clinicalendpoints
of drug action (34) to speed the development of new anti-HIV agents. The importance of thesequantitative markers increased rapidly. The number of publications with biomarker as a searchterm went up about 6-fold between 1985 and 2010, while the total number of publications onlydoubled.
The most useful definitions of the terms currently available are the result of a report by theNational Institutes of Health Biomarkers Definitions Working Group in 2001 (35):
� Biological marker (biomarker): a characteristic that is objectively measured and evaluatedas an indicator of normal biological processes, pathogenic processes, or pharmacologicalresponses to a therapeutic intervention;
� Clinical endpoint: a characteristic or variable that reflects how a patient feels, functions, orsurvives; and
� Surrogate endpoint: a biomarker that is intended to substitute for a clinical endpoint. Asurrogate endpoint is expected to predict clinical benefit (or harm or lack of benefit) basedon epidemiological, therapeutic, pathophysiological, or other scientific evidence.
These definitions have provided considerable clarity to the field. A biomarker is just a quanti-tative indicator of a biological process. In drug development and pharmacology, influencing sucha process is done only with the goal of attaining a clinical endpoint, which is an improvement ofthe functioning, feelings, or survival of a patient. Clinical measurement of these effects tends tobe variable and is often related to prevention of delayed but serious events, such as mortality, ordisease manifestations, such as stroke or infarction. This means that meaningful effects on suchmeasurements require very large and/or long trials (36). Therefore, a parametric and accuratemarker of the pharmacological influence of a critical pathophysiological process should be able toreflect the clinical effect to such an extent that this measurement could replace the clinical outcomemeasurement. Such a measure is then called a surrogate endpoint. This ultimate, elevated stateof a biomarker is reached rarely. Perhaps the best examples are the serum viral load in HIV orhepatitis C. The state of surrogacy for a biomarker can only be assured when the clinical programfor a drug has been completed, and the earlier surrogate biomarker is only useful for the fasterdevelopment of similar medicines.
The need for more advanced measurement tool kits in clinical research was highlighted in a2004 report by the FDA (37), which issued subsequent guidance on the validation of biomarkersin both genomics and biochemistry (38, 39). Lee et al. (40) provided useful clarifications aboutvalidation, which is usually defined as assessing the performance characteristics of a biochemicalassay. For a biomarker to have utility in drug development and for acceptance for registrationpurposes, the traditional requirements for sensitivity, specificity, and precision are just as importantas for any laboratory test. The clinical validation of biomarkers as surrogate markers involves aprocess for which the FDA introduced biomarker qualification as the preferred term (35).
BIOMARKERS PROVIDE THE ANSWERS TO SCIENTIFIC QUESTIONS
The definition above does not specify what question a particular measurement is intended toaddress. The catalogue of potential measurements in biology is virtually unlimited; therefore, thechoice of biomarkers requires guidance. The basis for this can be found in the EMA guidelineabout clinical trials (20), which states that rational drug development asks important questionsand answers them with appropriate studies. We now expand this definition as follows:
The essence of rational drug development is to ask important questions and answer them with appropriate studiesusing fit-for-purpose, qualified biomarkers.
62 Cohen et al.
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
Table 1 An approach to classifying clinical studies according to objectivea
Type of study Objective of study Study examplesHumanpharmacology
Assess tolerance; define/describe PK and PDExplore drug metabolism and interactionsEstimate activity
Dose-tolerance studiesSingle- and multiple-dose PK and PD studiesDrug interaction studies
Therapeuticexploratory
Explore use for targeted indicationEstimate dosage for subsequent studiesProvide basis for confirmatory study design,endpoints, and methodologies
Earliest trials of relatively short duration in well-defined,narrow patient populations, using surrogate orpharmacological endpoints or clinical measures
Dose-response exploration studiesTherapeuticconfirmatory
Demonstrate and confirm efficacyEstablish safety profileProvide an adequate basis for assessing thebenefit-risk relationship to support licensing
Establish dose-response relationship
Adequate, well-controlled studies to establish efficacyRandomized parallel dose–response studiesClinical safety studiesStudies of mortality/morbidity outcomesLarge, simple trialsComparative studies
Therapeutic use Refine understanding of benefit-risk relationshipin general or special populations and/orenvironments
Identify less common adverse reactionsRefine dosing recommendation
Comparative effectiveness studiesStudies of mortality/morbidity outcomesStudies of additional endpointsLarge, simple trialsPharmacoeconomic studies
Abbreviations: PD, pharmacodynamic; PK, pharmacokinetic.aData from Reference 20.
QUESTION-BASED DRUG DEVELOPMENT
The next step in every drug development program is to determine what these important questionsare. The objectives from the guidance are presented in a manner that appears generally applicable(see Table 1), and it is therefore attractive to use this approach for a drug with a known mechanismof action and a development trajectory that has been explored previously. Such nonprototypicaldevelopment is relatively low risk.
However, for prototypical compounds with new proposed mechanisms, standard developmentmay lead to serious oversight of essential problems. The most well-known example is TGN 1412, adrug with an entirely new immunological mechanism, for which questions about the pharmacologyof the drug in humans were obvious before the trial. Such questions could have been answeredby simple biomarkers obtainable ex vivo and by calculations of receptor density that would haverevealed that this drug was overdosed 100–1,000-fold during the first administration to humansand consequently caused serious harm to the subjects (14, 41).
Another example is the 5-hydroxytryptamine4 (5-HT4) receptor agonist tegaserod, which wasintroduced for the treatment of irritable bowel syndrome in 2001 and was taken off the marketin 2007, when a meta-analysis of adverse events showed a small but significant increase in car-diovascular events. The drug was found to be well tolerated in healthy volunteers (42), and thecompound underwent extensive research that was all directed toward the effects on the colon.When the drug was withdrawn, several small studies were published (43–45) that raised doubtabout the presence of any cardiovascular effects of the drug. However, investigators knew thattegaserod was pharmacologically nonselective and its effects on 5-HT4 receptors on platelets mayhave contributed to the cardiovascular events (46). It is tempting to speculate what would havehappened if the question about 5-HT4 antagonism had been asked at the start of developmentand if adequate studies to address the cardiovascular risks had been carried out properly.
www.annualreviews.org • Use of Biomarkers in Human Pharmacology 63
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
Does the drugreach the site of action?
Administration formAbsorptionDistribution to action siteMetabolism/elimination
Dissolution testsPlasma concentrationReceptor occupancy by PETCSF concentration
QuestionsQuestions Biomarkers (examples)Biomarkers (examples)
In vitro method validationValidate in plasma and CSFDevelop and test PET ligand
Qualification planQualification plan
Is the on-targetpharmacologicaleffect present?
PD effect on action siteResting-state MRIPlasma prolactinCSF metabolite
Studies with other compoundsAssay for metabolites
Are there off-targetpharmacologicaleffects?
PD effect on off-target siteSedation measurement Polysomnography
Test with other sedatives
Technical qualification
Are there on-targetpathophysiologicaleffects?
Etiological effectPathophysiologyDisease modification
Clinical scaleMortality
Tests are qualified
What is thetherapeutic window?
Balance between efficacyand safety
PharmacoeconomicsPharmacoeconomic and
PK/PD modeling
Are there off-targetpathophysiologicaleffects?
Etiology of side effectPathophysiologyCollateral side effect
Side-effect incidenceMortality
Tests are qualified
Examples of questions
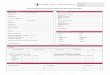
Figure 3Example of the structure of a question-based drug development plan. The double-headed arrows signify the development of aPK/PD model to relate the effects on biomarkers with clinical effects. All questions are answered in a certain population with regard to,for example, age, genetics, and genomics, and the methods to stratify the population (especially genomic or biochemical methods)also require validation and fit-to-purpose qualification. Abbreviations: CSF, cerebrospinal fluid; MRI, magnetic resonance imaging;PD, pharmacodynamic; PET, positron emission tomography; PK, pharmacokinetic. Adapted from Reference 6 withpermission.
The question-based drug development approach shown in Figure 3 has been described indetail by de Visser (47). When a new project is initiated, this approach allows a project leader orteam to develop an initial outline of the important questions. The figure shows a hypotheticalexample for a central nervous system (CNS) drug, but the questions have to be adapted to theactual therapeutic situation. The questions are arranged in six domains that follow the logicalprogression of a drug through the body, from absorption to excretion and the pharmacologi-cal, (patho)physiological, and eventually clinical effects that may occur. In an important study,researchers at a major pharmaceutical company found that in 43% of projects, the mechanisticaspects of new compounds were not tested adequately. They called knowledge about (a) exposureat the site of action, (b) target binding, and (c) the establishment of functional pharmacolog-ical activity the three pillars of survival of a new compound (48). Drug development withoutthis knowledge had a considerable chance of failure. These pillars were built into the question-based scheme. This model can be used for individual studies, for programs and projects, orboth.
64 Cohen et al.
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
From Questions to Answers
After the questions have been defined, generally in a process that involves several meetings, thenext step is to determine which biomarkers are available for obtaining the answers. Additionally,the qualification and validation status of the biomarkers has to be assessed. This is importantbecause many measurements are unsuitable for use in a particular type of trial, even though theyare adequately described in the literature. Often, a considerable amount of work is required tomake them fit-for-purpose (answering the important question).
Conversion of Questions to Studies and Real Options Project Planning
The set of questions defined above now needs to be translated into a series of studies or a singlestudy. The advantage of this approach is that the objectives of the studies can be derived easilyfrom the questions. The order in which the questions are answered is often apparent but canalso be determined more formally by decision analysis based on the real options method. Thisform of decision analysis optimizes the balance between cost and reduction of uncertainty andprovides a rational method for the design of a development program (47, 49, 50). The details of thisapproach are beyond the scope of this review; briefly, they require a priori assessment of the costof answering a certain question and the probability that useful information about this questionwill be obtained. A real options decision analysis then provides a logical order that optimizesinformation content and cost. Quantitative methods for project planning have been underused inpharmaceutical research. The main advantage of the real options method is that it makes the valueof scientific information explicit rather than just expressing it as a cost.
The development trajectory has now been turned into a question-based plan supported by aseries of studies and the possibility of tracking the progress through real milestones rather thananonymous phases in time. All that remains is for researchers to choose the right biomarkers.
SAFETY BIOMARKERS
We do not make a special case for biomarkers of adverse effects or safety. Aronson & Ferner(51) have proposed the term off-target pharmacology, recognizing that adverse events are alsoreflections of the pharmacology of the compound. This is even true for rare but serious eventssuch as anaphylaxis or severe liver damage induced by drugs, although sometimes the mechanism isnot known. The development of a prototypical compound is always based on some balance betweentarget and off-target effects, and the question-based scheme makes that explicit. Especially in earlydevelopment, the same biomarkers can reflect, in some cases, an off-target effect and, in othercases, the desired pharmacology of a drug. An example is the centrally acting antihypertensiverilmenidine, for which the speed of horizontal eye saccades was used to demonstrate off-targetsedative effects on the CNS (52). For the orexin antagonist almorexant (53), the same biomarkerwas used to quantify the intended (on-target) pharmacological effect on sleepiness.
Another aspect of the fit-for-purpose approach to biomarkers for off-target effects is thatfrequent measurement can enhance their usefulness. Supplemental Figure 1 shows the effectof a new antisense compound (54) on renal biomarkers as an example (follow the SupplementalMaterial link from the Annual Reviews home page at http://www.annualreviews.org).
QUALIFICATION OF BIOMARKERS BY PHARMACOLOGY
In its early phase, drug development research is conceptually no different than late-phase research.However, in the early phases of research with prototypical drugs, the biomarker plan will include a
www.annualreviews.org • Use of Biomarkers in Human Pharmacology 65
Supplemental Material
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
much greater proportion of biomarkers that are not yet qualified, as the need for measurements ofcertain variables only arises because a prototypical drug affects a hitherto-unaffected mechanism.The measurements are therefore just as unknown as the new mechanism and their relevance stilluncertain. This is probably one of the reasons investigators are reluctant to use biomarkers inearly-phase studies. However, obtaining the most detailed information about the pharmacologyof a new drug in humans is obviously also of the utmost importance. For the less innovativecompounds, a course of action can readily be found in the relevant literature and regulatorydocuments and, if necessary, adapted. The incorporation of biomarkers in early development ofprototypes sometimes requires the development of unqualified biomarkers to quantify an unknownmechanism, and this is not possible. In principle, the biomarker must be established as useful beforethe drug can be evaluated in its different aspects. This is clear from Figure 2, in which the trajectoryproceeds upward (develop the biomarker) before moving to the right (develop the drug).
Mechanism-Specific Biomarkers
Mechanism-specific biomarkers are also sometimes called proximal (55) and reflect the actionof a drug on pharmacology or pathophysiology (types 0–3 in Figure 2). The requirements forvalidation and qualification are well established and described for biomarkers that are collectedfrom biological fluids and measured in a biochemical or genetic laboratory (sometimes calledwet biomarkers) (40, 55). Most of the criteria can also be applied to biomarkers obtained fromimaging with positron emission tomography, which measures in vivo binding of a drug to aparticular receptor. The requirements for such measurements are also relatively easily derivedfrom the mechanism of action and the off-target effects of the new medicine. This can be doneon the basis of the question-based plan. Additionally, these biomarkers can often be tested afteranimal experiments, and experimental drugs can be added to human blood and examined in thelaboratory before any trials in human subjects begin. Perhaps the most widely used biomarker isthe concentration of the drug and its metabolites in biological fluids, for which the availability ofa reliable and rapid assay during early stages of development in human trials is essential. In thetraditional approach, this would be just a marker for pharmacokinetics. However, as a measurethat is obtained after each dosing step, it provides an immediate link to the toxicological andpharmacological experiments in animals and can be used for mathematical modeling of the drug-target interaction (27, 56).
An example of this is the development of a low-molecular-weight inhibitor of mitogen-activatedprotein kinase (Supplemental Figure 2). Such an approach could be a typical one for question-based development with built-in learn-and-confirm cycles. Any biomarker qualification requirestime, and this adds strong support for a question-based biomarker plan that is carried out as earlyas possible in development and well before first-in-human studies.
Clinical Biomarkers
Validation and qualification are less obvious for clinical biomarkers than for biomarkers demon-strating the pharmacology of a drug. Clinical biomarkers (also termed distal; types 4–6 inFigure 2) are thought to reflect disease activity and pathophysiology (55). Some clinical biomark-ers are clearly validated, but many of these relate to the delayed occurrence of events, such asmortality or the incidence of certain adverse events.
Selection of clinical biomarkers. Although it is possible that, for some effects, a whole newtest must be constructed, functional tests of most organs and physiological systems are generally
66 Cohen et al.
Supplemental Material
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
available. Rather, there is often an embarrassment of choices, and their usefulness has generallybeen determined in clinical practice, where they are used as markers for disease progression. Forexample, plasma creatinine concentration is a widely used marker for disease progression in renaldisease, but it lacks utility for the detection of potential, small changes in renal function inducedby new medicines (54, 57). Simply collecting such functional biomarkers from the literature doesnot provide a useful basis for selection because there is no indication of the performance ofsuch a biomarker in drug studies. We have published several meta-analyses of biomarkers basedon the assumption that, when a biomarker is sensitive to the effects of compounds from a certainmechanistic class, this will also hold for subsequent new compounds from that class. These analyseswere mainly done in the CNS area for benzodiazepines (58), antipsychotics (59), cannabinoid drugs(60), selective serotonin reuptake inhibitors (61), and alcohol (62). In the CNS area, the choiceof potential biomarkers of CNS function is virtually unlimited, and hundreds of tests and testvariants have been published. The selection process used in this area can also be transferred toother areas, such as cardiovascular or pulmonary functional testing, where the number of tests isgenerally smaller and the problem easier to handle.
Selection process. A useful biomarker in any class has to comply with the following generalcriteria (58):
� There must be a consistent response of the biomarker across studies (preferably from dif-ferent research groups) and drugs from the same mechanistic class.
� The biomarker must respond clearly to therapeutic (not supratherapeutic) doses.� There must be a clear dose- or concentration-response relationship.� There must a plausible relationship between the biomarker, pharmacology of the drug class,
and disease pathophysiology.
An example of how the selection process takes place can be found in several meta-analyses specif-ically performed for this purpose (58, 60, 61, 63).
Validation. The meta-analysis technique is very useful for the selection of biomarkers that al-ready exist and can be used to highlight a certain type of test. However, this does not meanthat an identified test is immediately usable. Even when the four criteria indicated above apply,qualification of a test in real-life circumstances is indicated. For a laboratory-based biomarker, awell-described validation plan is available using quality control samples, calibration, and tests ofaccuracy and precision (40). In principle, such tests could be performed with a biomarker mea-suring clinical function, but in practice, this is not practical; each step requires a clinical trial, andmultiple positive and negative controls would have to be tested. Despite this, at least some stepshave to be taken, including determining the sensitivity of a test.
The sensitivity of a test can vary considerably. For instance, the well-known sedative benzo-diazepine temazepam produced significant negative results on a particular eye-hand coordinationtest, the pursuit rotor, only after a dose of 40 mg (64), whereas the effects of a dose of 5 mg wereeasily detectable by a reduction of the speed of saccadic eye movements (65). If temazepam hadbeen an experimental drug and the insensitive test was used during early development, the activedose would have been grossly overestimated. Although the most sensitive tests will generally revealmore consistent significant effects in a literature overview or meta-analysis, sensitivity studies withrelevant comparator drugs can greatly increase the confidence in a biomarker, even though suchstudies are time-consuming. The selectivity of a test can be determined by using it on a range ofdrugs affecting a certain function but acting through different mechanisms. This is particularlyrelevant for CNS medicines, where the functions to be measured are fairly generic and related to
www.annualreviews.org • Use of Biomarkers in Human Pharmacology 67
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
activation or depression of brain function, but the mechanisms from which these effects originatevary considerably. A practical approach is to evaluate several known drugs and perform a range oftests to see which ones respond. For instance, this was done with a new magnetic resonance imag-ing measure (resting-state network analysis) by comparing alcohol and morphine—both have aknown sedative potential but also act through diverse mechanisms (66). Such a clinical biomarkervalidation program would reveal if tests that were described as useful do not in fact meet thecriteria for a biomarker (67).
Practical validation. Investigators must also pay attention to the practical aspects of a clinicalbiomarker. A test usually has to be administered multiple times to follow the effect of a drug andmust not be too long or too burdensome for the subjects, who might lose motivation to participate.Evaluation of the test results generally must be fast, and automated and secure data collection istherefore important. The ability to study several subjects at the same time requires test instrumentsthat are well characterized and technically standardized so that multiplication of instruments doesnot become unduly expensive and, when necessary, the test system can be transferred to otherstudy sites. In addition, attention must be given to the reliability of a biomarker in clinical trialsin which the circumstances and patient populations may require adaptations of the tests.
Use for new medicines with an untested mechanism of action. The indicated approach maylead to the best possible clinical biomarker set. However, for a medicine with an entirely novelmechanism of action, it is not certain that these biomarkers will actually give the desired response.
The biomarker could be unresponsive to the effect of the drug because another pathway orfunction is affected. For instance, cannabinoid agonists do not affect the speed of saccadic eyemovements at all, but they have a pronounced effect on subjective alertness and body stability (68).Selective γ-aminobutyric acid (GABA) agonists have little effect on alertness and body stability,whereas the decrease in the speed of saccadic eye movements is similar to that of the nonselectiveGABA agonist lorazepam (69).
Such differences cannot be immediately predicted unless a drug with a similar mechanism ofaction has already been tested. Evidence has now been gathered that firmly relates peak saccadicvelocity to the pharmacological activity of partial subtype-selective GABAA agonists (70). Forfirst-in-class drugs, the only practical solution is to apply a range of tests broadly encompassingthe functional domains. Preferably, such tests should evaluate drugs with as much overlap withunderlying mechanisms as possible.
Another possibility is that a compound does not produce any functional effects by itself. Thisis most likely the case for agonists or antagonists of a phasic rather than tonic physiologicalsystem or systems with low intrinsic activity. These can only be detected by challenging thesystem with an agonist. Examples are scopolamine for the cholinergic system in the brain (71),tetrahydrocannabinol for testing cannabinoid antagonists (72, 73), vasopressin for antagonists ofthe vasopressinergic system (74, 75), and 5-HT for the serotinergic system in the brain (76). Inaddition, serotonin-induced arterial constriction (77) and the use of 5-HT (78) for the study of drugeffects on platelet reactivity are good examples of the use of challenges in vascular pharmacology.
The development and selection of a challenge agent have to comply with the same rules as adirect functional biomarker. The development of such tests for a new compound generally requirestime and an early biomarker plan.
In-trial pharmacological qualification. The measures described above help to develop abiomarker that is maximally useful and well qualified for the purpose that is predefined in thequestion-based plan. Yet much depends on the decisions taken in early development, and these
68 Cohen et al.
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
need to be supported by robust data. Biomarkers of function may lose reliability in a trial for manytechnical reasons or through changes in motivation of subjects or staff. In any early trial, a positivecontrol group treated with a relevant drug of which the performance of the biomarker is knownis essential and provides considerable comfort about the findings obtained for a new drug (53,79). Positive controls can be easily added, even to a first-in-human design, either as a crossovertreatment or as a separate group. The positive control group also provides immediate relevanceto the size of the functional biomarker’s effect.
Pharmacokinetic-pharmacodynamic qualification. When a measurement with a functional ormechanistic biomarker can be related closely to the plasma concentrations of the drug througha plausible pharmacokinetic-pharmacodynamic model, this implies that the marker is relevantfor evaluation of target engagement of the drug. Researchers must still make explicit for whichpurpose the use of the biomarker is intended. For instance, for the experimental CETP inhibitorBAY 60–5521, investigators elegantly showed that inhibition of the target protein was related toplasma concentration in a pharmacological model. They could also predict how this would affectHDL cholesterol (80, 81). The biomarkers indicate that the drug affects a physiological responsebut obviously do not provide direct information about the clinical effect. In view of the knownproblems with blood pressure increases caused by these drugs, it is interesting that blood pressurewas used as a safety biomarker and not reported in relation to the plasma concentrations (as anoff-target functional marker).
Use of qualified biomarkers in confirmatory clinical trials. The use of biomarkers for targetengagement in early-phase trials has important implications for the later-phase drug development.When used in these later-phase trials, researchers can show that target engagement has also oc-curred in the relevant patient population under more realistic conditions. Biomarker use can lead toenrichment of a patient population by using target engagement as a covariate in the cases in whichthis is variable for pharmacokinetic or pharmacodynamic reasons. Finally, the use of biomarkersin these trials will contribute to the development of early biomarkers with relevance for clinicaleffects.
CONCLUSIONS
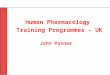
A summary of the steps that have to be taken before a biomarker can be used in early drugdevelopment is given in Figure 4. Quantitative evaluation of the dose-response relationship is thebasis of pharmacology and therefore of the scientific development of new investigational medicalproducts in humans. Researchers can quantify the drug response with a multitude of measurementsthat have to be selected, evaluated, validated, and qualified before a new drug development programis started. Lack of attention to this methodological support for a development program can beexpensive and dangerous. We propose a rational and transparent approach to the involvement ofimportant biomarkers in the development of new medicines. Biomarkers should be fit-for-purposeto show essential drug properties and effects. The subsequent application of qualified biomarkersin confirmatory clinical trials may demonstrate whether the underlying pharmacological effectsare indeed maintained throughout the development. The FDA succinctly stated the essence ofrational drug development as asking important questions and answering them with appropriatestudies (20). In this review, we have provided a conceptual approach to populate these studies withappropriate biomarkers.
www.annualreviews.org • Use of Biomarkers in Human Pharmacology 69
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
New potential medicine
Question-based planBiomarker plan
with validation status
Mechanisticbiomarkers
Clinicalbiomarkers
Full analytical validationQualification
SensitivityPracticalPositive controls
Biomarkermeta-analysis
No fit-to-purposebiomarkers
Fit-to-purposebiomarkers
Question-basedbiomarker set
Start biomarkerdevelopment
Figure 4Overview of biomarker development. The development of a question-based plan and a provisionalbiomarker plan with a known validation status allows investigators to subdivide the plan into mechanisticbiomarkers (generally requiring traditional laboratory validation) and clinical biomarkers (requiringfit-to-purpose qualification). A meta-analysis of available biomarkers needs to be done to seek availableknowledge about sensitivity and specificity. On the basis of this analysis, researchers can design furtherstudies to attain a question-based and fit-to-purpose biomarker set. This analysis will also reveal the need forfull biomarker development, with implications for the timing of development.
DISCLOSURE STATEMENT
The authors are not aware of any affiliations, memberships, funding, or financial holdings thatmight be perceived as affecting the objectivity of this review. All authors are full-time employees ofthe Foundation Centre for Human Drug Research. The terms of employment of this organizationprohibit shareholdings in health-care-related companies. Fees for lectures and other compensa-tion are charged through the Foundation and not directly reflected in the compensation of theemployees.
LITERATURE CITED
1. Black JW, Crowther AF, Shanks RG, Belf MD, Smith LH, et al. 1964. A new adrenergic: beta-receptorantagonist. Lancet 283:1080–81
2. Pilkington TRE, Lowe RD, Robinson BF, Titterington E. 1962. Effect of adrenergic blockade on glucoseand fatty-acid mobilisation in man. Lancet 280:316–17
70 Cohen et al.
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
3. Dornhorst AC, Robinson BF. 1962. Clinical pharmacology of a beta-adrenergic-blocking agent(nethalide). Lancet 280:314–16
4. Prichard BNC, Gillam PMS. 1969. Treatment of hypertension with propranolol. BMJ 1:7–165. Harris WS, Schoenfeld CD, Brooks RH, Weissler AM. 1966. Effect of beta adrenergic blockers on the
hemodynamic responses to epinephrine in man. Am. J. Cardiol. 17:484–926. Cohen AF. 2010. Developing drug prototypes: pharmacology replaces safety and tolerability? Nat. Rev.
Drug Discov. 9(11):856–657. Nissen SE, Tardif J-C, Nicholls SJ, Revkin JH, Shear CL, et al. 2007. Effect of torcetrapib on the
progression of coronary atherosclerosis. N. Engl. J. Med. 356:1304–168. Clark RW, Sutfin TA, Ruggeri RB, Willauer AT, Sugarman ED, et al. 2004. Raising high-density lipopro-
tein in humans through inhibition of cholesteryl ester transfer protein: an initial multidose study of torce-trapib. Arterioscler. Thromb. Vasc. Biol. 24:490–97
9. Bots ML, Visseren FL, Evans GW, Riley WA, Revkin JH, et al. 2007. Torcetrapib and carotid intima-media thickness in mixed dyslipidaemia (RADIANCE 2 study): a randomised, double-blind trial. Lancet370:153–60
10. Forrest MJ, Bloomfield D, Briscoe RJ, Brown PN, Cumiskey A-M, et al. 2008. Torcetrapib-induced bloodpressure elevation is independent of CETP inhibition and is accompanied by increased circulating levelsof aldosterone. Br. J. Pharmacol. 154(7):1465–73
11. McKenney JM, Davidson MH, Shear CL, Revkin JH. 2006. Efficacy and safety of torcetrapib, a novelcholesteryl ester transfer protein inhibitor, in individuals with below-average high-density lipoproteincholesterol levels on a background of atorvastatin. J. Am. Coll. Cardiol. 48(9):1774–81
12. Barter P, Caulfield M. 2007. Effects of torcetrapib in patients at high risk for coronary events. N. Engl. J.Med. 357(21):2109–22
13. Zhao L, Jin W, Rader D, Packard C, Feuerstein. 2009. A translational medicine perspective of the devel-opment of torcetrapib: Does the failure of torcetrapib development cast a shadow on future development oflipid modifying agents, HDL elevation strategies or CETP as a viable molecular target for atherosclerosis?Biochem. Pharmacol. 78:315–25
14. Kenter MJH, Cohen AF. 2006. Establishing risk of human experimentation with drugs: lessons fromTGN1412. Lancet 368(9544):1387–91
15. Yusuf S, Flather M, Gent M. 1997. Effects of RheothRx on mortality, morbidity, left ventricular function,and infarct size in patients with acute myocardial infarction. Circulation 96(1):192–201
16. Schaer GL, Spaccavento LJ, Browne KF, Krueger KA, Krichbaum D, et al. 1996. Beneficial effects ofRheothRx injection in patients receiving thrombolytic therapy for acute myocardial infarction: results ofa randomized, double-blind, placebo-controlled trial. Circulation 94(3):298–307
17. Jewell RC, Khor SP, Kisor DF, LaCroix KA, Wargin WA. 1997. Pharmacokinetics of RheothRx injectionin healthy male volunteers. J. Pharm. Sci. 86(7):808–12
18. Eur. Parliam. Counc. 2001. Directive 2001/20/EC of the European Parliament and of the Council. Off.J. Eur. Communities L121:34–44
19. Ng R. 2009. Drugs: From Discovery to Approval. Hoboken, NJ: Wiley. 2nd ed.20. Eur. Med. Agency. 1998. Note for guidance on general considerations for clinical trials (CPMP/ICH/291/95).
Rep., London21. Lenfle S, Loch C. 2009. Lost roots: how project management settled on the phased approach (and compromised its
ability to lead change in modern enterprises). INSEAD Work. Pap., Fontainebleau, France22. De Meyer A, Loch CH, Pich MT. 2002. Managing project uncertainty: from variation to chaos. IEEE
Eng. Manag. Rev. 30:91–9823. Cohen A. 2007. Should we tolerate tolerability as an objective in early drug development? Br. J. Clin.
Pharmacol. 64(3):249–5224. Sheiner L. 1997. Learning versus confirming in clinical drug development. Clin. Pharmacol. Ther.
61(3):275–9125. Danhof M, Alvan G, Dahl SG, Kuhlmann J, Paintaud G. 2005. Mechanism-based pharmacokinetic-
pharmacodynamic modeling—a new classification of biomarkers. Pharm. Res. 22(9):1432–3726. Lalonde RL, Kowalski KG, Hutmacher MM, Ewy W, Nichols DJ, et al. 2007. Model-based drug devel-
opment. Clin. Pharmacol. Ther. 82(1):21–32
www.annualreviews.org • Use of Biomarkers in Human Pharmacology 71
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
27. Milligan PA, Brown MJ, Marchant B, Martin SW, van der Graaf PH, et al. 2013. Model-based drug devel-opment: a rational approach to efficiently accelerate drug development. Clin. Pharmacol. Ther. 93(6):502–14
28. Echt DS, Liebson PR, Mitchell LB, Peters RW, Obias-Manno D, et al. 2014. Mortality and morbidity inpatients receiving encainide, flecainide or placebo—the Cardiac Arrhythmia Suppression Trial. N. Engl.J. Med. 324:781–88
29. Dei Cas L, Manca C, Bernardini B, Vasini G, Visioli O. 1982. Noninvasive evaluation of the effects of oralibopamine (SB 7505) on cardiac and renal function in patients with congestive heart failure. J. Cardiovasc.Pharmacol. 4:436–40
30. Col J, Mievis E, Reynaert M. 1983. Ibopamine in very severe congestive heart failure: pilot haemodynamicinvasive assessment. Eur. J. Clin. Pharmacol. 24(3):297–300
31. van Veldhuisen DJ, Man in’t Veld AJ, Dunselman PHJM, Lok DJA, Dohmen HJM, et al. 1993. Double-blind placebo-controlled study of ibopamine and digoxin in patients with mild to moderate heart failure:results of the Dutch Ibopamine Multicenter Trial (DIMT). J. Am. Coll. Cardiol. 22(6):1564–73
32. Hampton JR, van Veldhuisen DJ, Kleber FX, Cowley AJ, Ardia A, et al. 1997. Randomised study of effectof ibopamine on survival in patients with advanced severe heart failure. Lancet 349:971–77
33. Yee KM, Struthers A. 1997. Can drug effects on mortality in heart failure be predicted by any surrogatemeasure? Eur. Heart J. 18(12):1860–64
34. Ho D, Moudgil T, Alam M. 1989. Quantitation of human immunodeficiency virus type 1 in the blood ofinfected persons. N. Engl. J. Med. 321(24):1621–25
35. Atkinson AJ Jr, Colburn WA, DeGruttola VG, DeMets DL, Downing GJ, et al. 2001. Biomarkers andsurrogate endpoints: preferred definitions and conceptual framework. Clin. Pharmacol. Ther. 69(3):89–95
36. Peto R, Pike M, Armitage P, Breslow N, Cox D, et al. 1976. Design and analysis of randomized clinicaltrials requiring prolonged observation of each patient. Br. J. Cancer 34:585–612
37. U.S. Food Drug Adm. 2004. Innovation or stagnation: challenge and opportunity on the critical path to newmedical products. Chall. Oppor. Rep., U.S. Dep. Health Hum. Serv., Rockville, MD
38. U.S. Food Drug Adm. 2011. Guidance for industry: E16 biomarkers related to drug or biotechnology productdevelopment: context, structure and format of qualification submissions. Rep., U.S. Dep. Health Hum. Serv.,Rockville, MD
39. U.S. Food Drug Adm. 2005. Guidance for industry: pharmacogenomic data submissions. Proced. Rep., U.S.Dep. Health Hum. Serv., Rockville, MD
40. Lee JW, Devanarayan V, Barrett YC, Weiner R, Allinson J, et al. 2006. Fit-for-purpose method devel-opment and validation for successful biomarker measurement. Pharm. Res. 23(2):312–28
41. Expert Sci. Group. 2006. Expert scientific group on phase one clinical trials. Final Rep., Nov. 3042. Appel S, Kumle A, Hubert M, Duvauchelle T. 1997. First pharmacokinetic—pharmacodynamic study in
humans with a selective 5-hydroxytryptamine4 receptor agonist. J. Clin. Pharmacol. 37:229–3743. Wood P. 2012. Tegaserod in the treatment of constipation-predominant irritable bowel syndrome. Do
the risks outweigh the benefits? Naunyn-Schmiedeberg’s Arch. Pharmacol. 385(1):1–344. Al-Judaibi B, Chande N, Gregor J. 2010. Safety and efficacy of tegaserod therapy in patients with irritable
bowel syndrome or chronic constipation. Can. J. Clin. Pharmacol. 17(1):e194–20045. Chan KY, de Vries R, Leijten FPJ, Pfannkuche H-J, van den Bogaerdt AJ, et al. 2009. Functional char-
acterization of contractions to tegaserod in human isolated proximal and distal coronary arteries. Eur. J.Pharmacol. 619(1–3):61–67
46. Tack J, Camilleri M, Chang L, Chey WD, Galligan JJ, et al. 2012. Systematic review: cardiovascular safetyprofile of 5-HT4 agonists developed for gastrointestinal disorders. Aliment. Pharmacol. Ther. 35(7):745–67
47. de Visser S. 2003. A question based approach to drug development. PhD Thesis, Leiden Univ., Leiden, Neth.48. Morgan P, Van Der Graaf PH, Arrowsmith J, Feltner DE, Drummond KS, et al. 2012. Can the flow of
medicines be improved? Fundamental pharmacokinetic and pharmacological principles toward improvingPhase II survival. Drug Discov. Today 17(9–10):419–24
49. Copeland TE, Keenan PT. 1998. Making real options real. McKinsey Q. 3:128–4250. D’Souza F. 2002. Putting real options to work to improve project planning. Harvard Manag. Update
7(8):3–651. Aronson JK, Ferner RE. 2003. Joining the DoTS: new approach to classifying adverse drug reactions.
BMJ 327:1222–25
72 Cohen et al.
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
52. van der Post JP, de Visser SJ, Schoemaker RC, Cohen AF, van Gerven JMA. 2004. Pharmacokinetic/pharmacodynamic assessment of tolerance to central nervous system effects of a 3 mg sustained releasetablet of rilmenidine in hypertensive patients. J. Psychopharmacol. 18(2):221–27
53. Hoever P, Hay J, Rad M, Cavallaro M, van Gerven JM, Dingemanse J. 2013. Tolerability, pharmacoki-netics, and pharmacodynamics of single-dose almorexant, an orexin receptor antagonist, in healthy elderlysubjects. J. Clin. Psychopharmacol. 33(3):363–70
54. Van Poelgeest EP, Swart RM, Betjes MGH, Moerland M, Weening JJ, et al. 2013. Acute kidney injuryduring therapy with an antisense oligonucleotide directed against PCSK9. Am. J. Kidney Dis. 62(4):796–800
55. Lee JW, Weiner RS, Sailstad JM, Bowsher RR, Knuth DW, et al. 2005. Method validation and measure-ment of biomarkers in nonclinical and clinical samples in drug development: a conference report. Pharm.Res. 22(4):499–511
56. van der Graaf PH. 2012. CPT: pharmacometrics and systems pharmacology. CPT Pharmacometrics Syst.Pharmacol. 1:e8
57. van Meer L, Moerland M, Cohen AF, Burggraaf J. 2013. Urinary kidney biomarkers for early detectionof nephrotoxicity in clinical drug development. Br. J. Clin. Pharmacol. 77:947–57
58. de Visser SJ, van der Post JP, de Waal PP, Cornet F, Cohen AF, van Gerven JMA. 2003. Biomarkers forthe effects of benzodiazepines in healthy volunteers. Br. J. Clin. Pharmacol. 55(1):39–50
59. de Visser SJ, van der Post JP, Pieters MSM, Cohen AF, van Gerven JMA. 2001. Biomarkers for the effectsof antipsychotic drugs in healthy volunteers. Br. J. Clin. Pharmacol. 51:119–32
60. Zuurman L, Ippel AE, Moin E, van Gerven JMA. 2009. Biomarkers for the effects of cannabis and THCin healthy volunteers. Br. J. Clin. Pharmacol. 67(1):5–21
61. Dumont GJH, de Visser SJ, Cohen AF, van Gerven JMA. 2005. Biomarkers for the effects of selectiveserotonin reuptake inhibitors (SSRIs) in healthy subjects. Br. J. Clin. Pharmacol. 59(5):495–510
62. Zoethout RWM, Delgado WL, Ippel AE, Dahan A, van Gerven JMA. 2011. Functional biomarkers forthe acute effects of alcohol on the central nervous system in healthy volunteers. Br. J. Clin. Pharmacol.71(3):331–50
63. Rijnbeek B, de Visser SJ, Franson KL, Cohen AF, van Gerven JMA. 2003. REM sleep effects as a biomarkerfor the effects of antidepressants in healthy volunteers. J. Psychopharmacol. 17(2):196–203
64. Pleuvry BJ, Maddison SE, Odeh RB, Dodson ME. 1980. Respiratory and psychological effects of oraltemazepam in volunteers. Br. J. Anaesth. 52(9):901–6
65. van Steveninck AL, Schoemaker HC, Pieters MSM, Kroon R, Breimer DD, Cohen AF. 1991. A compar-ison of the sensitivities of adaptive tracking, eye movement analysis and visual analog lines to the effectsof incremental doses of temazepam in healthy volunteers. Clin. Pharmacol. Ther. 50(2):172–80
66. Khalili-Mahani N, van Osch MJP, Baerends E, Soeter RP, de Kam M, et al. 2011. Pseudocontinuousarterial spin labeling reveals dissociable effects of morphine and alcohol on regional cerebral blood flow.J. Cereb. Blood Flow Metab. 31(5):1321–33
67. van der Post J, de Waal PP, de Kam ML, Cohen AF, van Gerven JMA. 2004. No evidence of the usefulnessof eye blinking as a marker for central dopaminergic activity. J. Psychopharmacol. 18(1):109–14
68. Strougo A, Zuurman L, Roy C, Pinquier JL, van Gerven JMA, et al. 2008. Modelling of the concentration–effect relationship of THC on central nervous system parameters and heart rate—insight into its mech-anisms of action and a tool for clinical research and development of cannabinoids. J. Psychopharmacol.22(7):717–26
69. de Haas SL, de Visser SJ, van der Post JP, de Smet M, Schoemaker RC, et al. 2007. Pharmacodynamicand pharmacokinetic effects of TPA023, a GABAA α2,3 subtype-selective agonist, compared to lorazepamand placebo in healthy volunteers. J. Psychopharmacol. 21(4):374–83
70. Chen X, de Haas S, de Kam M, van Gerven J. 2012. An overview of the CNS-pharmacodynamic profilesof nonselective and selective GABA agonists. Adv. Pharmacol. Sci. 2012:134523
71. Liem-Moolenaar M, Zoethout RWM, de Boer P, Schmidt M, de Kam ML, et al. 2010. The effectsof the glycine reuptake inhibitor R213129 on the central nervous system and on scopolamine-inducedimpairments in psychomotor and cognitive function in healthy subjects. J. Psychopharmacol. 24(11):1671–79
www.annualreviews.org • Use of Biomarkers in Human Pharmacology 73
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55CH05-Cohen ARI 29 November 2014 10:39
72. Klumpers LE, Fridberg M, de Kam ML, Little PB, Jensen NO, et al. 2013. Peripheral selectivity of thenovel cannabinoid receptor antagonist TM38837 in healthy subjects. Br. J. Clin. Pharmacol. 76(6):846–57
73. Zuurman L, Roy C, Schoemaker RC, Amatsaleh A, Guimaeres L, et al. 2010. Inhibition of THC-inducedeffects on the central nervous system and heart rate by a novel CB1 receptor antagonist AVE1625.J. Psychopharmacol. 24(3):363–71
74. Jacobs GE, van Gerven JMA, de Kam ML, Elassaiss-Schaap J, Ruigt G, et al. 2011. A pharmacologicaltool to assess vasopressinergic co-activation of the hypothalamus–pituitary–adrenal axis more integrallyin healthy volunteers. J. Psychopharmacol. 25(3):361–69
75. Jacobs GE, Hulskotte EGJ, van Gerven JMA, Zuurman L, de Kam ML, et al. 2011. Desmopressin asa pharmacological tool in vasopressinergic hypothalamus–pituitary–adrenal axis modulation: neuroen-docrine, cardiovascular and coagulatory effects. J. Psychopharmacol. 25(3):353–60
76. Smarius LJCA, Jacobs GE, Hoeberechts-Lefrandt DHM, de Kam ML, van der Post JP, et al. 2008.Pharmacology of rising oral doses of 5-hydroxytryptophan with carbidopa. J. Psychopharmacol. 22(4):426–33
77. Kemme MJB, Burggraaf J, Schoemaker RC, Cohen AF, Blauw GJ. 2000. No evidence for functionalinvolvement of 5-HT2B receptors in serotonin-induced vasodilatation in the human forearm. 36:699–703
78. Moerland M, Kemme M, Dijkmans A, Bergougnan L, Burggraaf J. 2011. Modulation of vasoactivity andplatelet aggregation by selective 5-HT receptor antagonism in humans. 58:575–80
79. van Gerven JMA, Roncari G, Schoemaker RC, Massarella J, Keesmaat P, et al. 1997. Integrated pharma-cokinetics and pharmacodynamics of Ro 48–8684, a new benzodiazepine, in comparison with midazolamduring first administration to healthy male subjects. Br. J. Clin. Pharmacol. 44(5):487–93
80. Weber O, Willmann S, Bischoff H, Li V, Vakalopoulos A, et al. 2012. Prediction of a potentially effectivedose in humans for BAY 60–5521, a potent inhibitor of cholesteryl ester transfer protein (CETP) byallometric species scaling and combined pharmacodynamic and physiologically-based pharmacokineticmodelling. Br. J. Clin. Pharmacol. 73(2):219–31
81. Boettcher M-F, Heinig R, Schmeck C, Kohlsdorfer C, Ludwig M, et al. 2012. Single dose pharmacoki-netics, pharmacodynamics, tolerability and safety of BAY 60–5521, a potent inhibitor of cholesteryl estertransfer protein. Br. J. Clin. Pharmacol. 73(2):210–18
74 Cohen et al.
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55-FrontMatter ARI 1 December 2014 15:8
Annual Review ofPharmacology andToxicology
Volume 55, 2015Contents
A Conversation with Susan Band HorwitzSusan Band Horwitz and I. David Goldman � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 1
Introduction to the Theme “Precision Medicine and Predictionin Pharmacology”Paul A. Insel, Susan G. Amara, and Terrence F. Blaschke � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �11
Identifying Predictive Features in Drug Response Using MachineLearning: Opportunities and ChallengesMathukumalli Vidyasagar � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �15
Predicting Toxicities of Reactive Metabolite–Positive Drug CandidatesAmit S. Kalgutkar and Deepak Dalvie � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �35
The Use of Biomarkers in Human Pharmacology (Phase I) StudiesA.F. Cohen, J. Burggraaf, J.M.A. van Gerven, M. Moerland,
and G.J. Groeneveld � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �55
Improving Postapproval Drug Safety Surveillance: Getting BetterInformation SoonerSean Hennessy and Brian L. Strom � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �75
Preemptive Clinical Pharmacogenetics Implementation: CurrentPrograms in Five US Medical CentersHenry M. Dunnenberger, Kristine R. Crews, James M. Hoffman, Kelly E. Caudle,
Ulrich Broeckel, Scott C. Howard, Robert J. Hunkler, Teri E. Klein,William E. Evans, and Mary V. Relling � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � �89
A Personalized Medicine Approach for Asian Americans with theAldehyde Dehydrogenase 2*2 VariantEric R. Gross, Vanessa O. Zambelli, Bryce A. Small, Julio C.B. Ferreira,
Che-Hong Chen, and Daria Mochly-Rosen � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 107
Pharmacogenomics in Asthma Therapy: Where Are We and WhereDo We Go?Heung-Woo Park, Kelan G. Tantisira, and Scott T. Weiss � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 129
v
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55-FrontMatter ARI 1 December 2014 15:8
Drug Disposition in Obesity: Toward Evidence-Based DosingCatherijne A.J. Knibbe, Margreke J.E. Brill, Anne van Rongen, Jeroen Diepstraten,
Piet Hein van der Graaf, and Meindert Danhof � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 149
How Good Is “Evidence” from Clinical Studies of Drug Effects andWhy Might Such Evidence Fail in the Prediction of the ClinicalUtility of Drugs?Huseyin Naci and John P.A. Ioannidis � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 169
The Ethics and Economics of Pharmaceutical PricingSara Parker-Lue, Michael Santoro, and Greg Koski � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 191
Brown, Beige, and White: The New Color Code of Fat and ItsPharmacological ImplicationsAlexander Pfeifer and Linda S. Hoffmann � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 207
Candidate Drug Targets for Prevention or Modification of EpilepsyNicholas H. Varvel, Jianxiong Jiang, and Raymond Dingledine � � � � � � � � � � � � � � � � � � � � � � � � � 229
The Design of Covalent Allosteric DrugsRuth Nussinov and Chung-Jung Tsai � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 249
Therapeutic Modulation of Urinary Bladder Function: MultipleTargets at Multiple LevelsMartin C. Michel � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 269
Mineralocorticoids in the Heart and Vasculature: New Insightsfor Old HormonesAchim Lother, Martin Moser, Christoph Bode, Ross D. Feldman, and Lutz Hein � � � � � � 289
Unraveling the Physiological Complexities of Antibiotic LethalityDaniel J. Dwyer, James J. Collins, and Graham C. Walker � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 313
Intraclass Differences Among Antihypertensive DrugsR.D. Feldman, Y. Hussain, L.M. Kuyper, F.A. McAlister, R.S. Padwal,
and S.W. Tobe � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 333
Targeting Hsp90/Hsp70-Based Protein Quality Control forTreatment of Adult Onset Neurodegenerative DiseasesWilliam B. Pratt, Jason E. Gestwicki, Yoichi Osawa, and Andrew P. Lieberman � � � � � � 353
New Approaches to Inhibiting Platelets and CoagulationJeremiah P. Depta and Deepak L. Bhatt � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 373
DREADDs (Designer Receptors Exclusively Activated by DesignerDrugs): Chemogenetic Tools with Therapeutic UtilityDaniel J. Urban and Bryan L. Roth � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 399
Learning by Failing: Ideas and Concepts to Tackle γ-Secretases inAlzheimer’s Disease and BeyondBart De Strooper and Lucıa Chavez Gutierrez � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 419
vi Contents
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.

PA55-FrontMatter ARI 1 December 2014 15:8
Therapeutic Applications of Extracellular Vesicles: Clinical Promiseand Open QuestionsBence Gyorgy, Michelle E. Hung, Xandra O. Breakefield, and Joshua N. Leonard � � � � � 439
Eph Receptors and Ephrins: Therapeutic OpportunitiesAntonio Barquilla and Elena B. Pasquale � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 465
Designed Ankyrin Repeat Proteins (DARPins): Binding Proteins forResearch, Diagnostics, and TherapyAndreas Pluckthun � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 489
Synthetic Lethal Vulnerabilities of CancerFerran Fece de la Cruz, Bianca V. Gapp, and Sebastian M.B. Nijman � � � � � � � � � � � � � � � � � 513
Calcitonin Gene-Related Peptide (CGRP): A New Target for MigraineAndrew F. Russo � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 533
Activation and Regulation of Caspase-6 and Its Rolein Neurodegenerative DiseasesXiao-Jun Wang, Qin Cao, Yan Zhang, and Xiao-Dong Su � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 553
Constellation Pharmacology: A New Paradigm for Drug DiscoveryRussell W. Teichert, Eric W. Schmidt, and Baldomero M. Olivera � � � � � � � � � � � � � � � � � � � � � � 573
DNA Methylation and Its Implications and Accessibilityfor Neuropsychiatric TherapeuticsJeremy J. Day, Andrew J. Kennedy, and J. David Sweatt � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 591
Targeting Receptor-Mediated Transport for Delivery of BiologicsAcross the Blood-Brain BarrierJason M. Lajoie and Eric V. Shusta � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 613
Novel Targeted Therapies for Eosinophil-Associated Diseasesand AllergySusanne Radonjic-Hoesli, Peter Valent, Amy D. Klion, Michael E. Wechsler,
and Hans-Uwe Simon � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 633
Indexes
Cumulative Index of Contributing Authors, Volumes 51–55 � � � � � � � � � � � � � � � � � � � � � � � � � � � 657
Cumulative Index of Article Titles, Volumes 51–55 � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � � 661
Errata
An online log of corrections to Annual Review of Pharmacology and Toxicology articlesmay be found at http://www.annualreviews.org/errata/pharmtox
Contents vii
Ann
u. R
ev. P
harm
acol
. Tox
icol
. 201
5.55
:55-
74. D
ownl
oade
d fr
om w
ww
.ann
ualr
evie
ws.
org
Acc
ess
prov
ided
by
Uni
vers
ity o
f L
eide
n -
Facu
lteit
Soci
ale
Wet
ensc
happ
e on
01/
28/1
9. F
or p
erso
nal u
se o
nly.