Embed Size (px)
Citation preview
THE VALIDITY AND RELIABILITY OF A RANGE OF MOTION ASSESSMEM' OF SMILE FOR CHiL,DREN WITH FACIAL PALSY
Shawna Elise Wade
A thesis submitted in conformity with the requirements for the degree of Masters of Science
Graduate Department of the Institute of Medical Science University of Toronto
Q Copyright by Shawna Elise Wade, 2000
National Library of Canada
Bibliothèque nationale du Canada
Acquisitions and Acquisitions et Bibliographie Services services bibliographiques
395 Wellington Street 395, nie Wellington Ottawa ON K1A ON4 Ottawa ON K1 A ON4 Canada Canada
The author has granted a non- L'auteur a accordé une licence non exclusive Licence allowing the exclusive permettant à la National Library of Canada to Bibliothèque nationale du Canada de reproduce, Ioan, distribute or sel1 reproduire, prêter, distribuer ou copies of this thesis in microform, vendre des copies de cette thèse sous paper or electronic formats. la fome de microfiche/film, de
reproduction sur papier ou sur format électronique.
The author retains ownership of the L'auteur conserve la propriété du copyright in this thesis. Neither the droit d'auteur qui protége cette thèse. thesis nor substantid extracts fiom it Ni la thèse ni des extraits substantiels may be printed or otherwise de celle-ci ne doivent être imprimés reproduced without the author's ou autrement reproduits sans son permission. autorisation.
TEE VALiDITY AND RELIABILITY OF A RANGE OF MOTION ASSESSMENT OF SMDLE FOR CHILDREN WITH FACIAL PALSY
Shawna Wade Masters of Science
lnstitute of Medical Science University of Toronto
2000
Injury to the VI1 craaial nerve may resuit in a condition know as facial palsy, paralysis of the
muscles of facial expression. For children with long-standing paralysis, re-animation surgery
has provided them with the ability to smile. In order to assess the child's progress, the
efficacy of therapeutic interventions and the long-term outcomes, it is important to estabiish a
range of motion (ROM) assessment that is valid and reliable. The important amibutes to
rneasiue in the ROM assessment of srnile were identified and the content vdidity established.
The inter-rater reliability of the clinically derived measures of smile was determined using
three measurement tools: the modified hand held caliper (MCT), the d e r and the
goniorneter. The most clinically appropriate of the three tools was selected to cornpiete each
facial measurement. For clinicd activities the MCT appeared to be reasonably consistent in
the documentation of distance measutements in the assessment of smile. The d e r and
goniorneter were not found to be as reliable although the rneasurements of, lip droop and
direction of srnile are important in the assessment of smile. The results of this investigation
have produced a ROM assessment that will reliably measure most of the gross motor
components of srnile deemed important in the clinical setting: cornmisure movement, upper
lip movement, symmetry of the upper and lower Iips and symaietry of the philtnim. To
capture the smaller facial movements the community of researchers need to continue to
perfect the cornputer d y s i s of facial movement.
Appreciation and thanks are extended to my Master's Degree s u p e ~ s o r y cornmittee, Dr. R.
Manktelow, Dr. R Zuker, Dr. L. Mainwaring and Dr. C. Graveline. 1 am grateful to Dr.
Manktelow for consenting to provide me with passage into the graduate program of The
Institute of Medical Science and his ongoing mentorship throughout my graduate expenence.
1 continualiy admire the vision and slcili of both Dr. Manktelow and Dr. Zuker in their
treatment of children with facial palsy and the devotion they have in improving the quality of
Iife for this group of individuals. Dr. Mainwaring has been my lighthouse. 1 appreciate her
astuteness, her sense of clarïty, and sensitivity to my growth as a young researcher. Causaiity
is afforded to Dr. Graveline for daring me to begin this venture. I am indebted to her for
recognizing my potentiai.
Thank you to all the staff of Rehabilitation Services who supported me and the development
of this project. Special recognition is given to the Academic and Clinical Research
Committee for their insightfbi critique of this proposai and to Tara Muir, the second rater in
this study. 1 would also like to thank an exceptional group of individuals at Sick Kid's for
providing the polish to this project: Andrew Baziw - Medicai Engineering, Derek Stephens -
Biostatictics, Rob Tetemck, Eimer Cruz and Bili Fox - Graphic' s Department and Frank
Ferrari and Sam Mendolia - Audio-Visual Department In addition, 1 would aiso like to
acknowledge The Hospital for Sick Chiidren's Seed Grant Comrnittee for funcihg this
research study.
A profound thank you to the extraordinary children and families who participated in the
research study. Their interest and devotion to improve the outcornes for children undergohg
facial re-animation procedures needs to be commended.
A heartfelt thanks is also owed to my biends and family for their support, encouragement
and perseverance. In particular, my parents Murray and Chns Wade for al1 that they have
done for me in making this possible.
1 would now finaily thank rny husband Morgan Robinson for his never falling support and
patience with my graduate work and this research project. He is an excellent editor and 1 his
number one fan.
Appendix A Table Al : The Houe Brackmann Facial Nerve Grading Scale From: Facial nerve grading system by J.W. House and D E Brackmann. 1985, Oto lameolo~ Head and Neck Sur~ew, 93 (2), 146. (permission pending)
Table A 2 The Fisch Detailed Evaluation of Facial Symmetry From: Comparative value of facial nerve grading systems by Rickenmann, J., Jaquenod, C., Cerenko, D., Fisch, U. 1997, Otolamgolog~ Head and Neck Sur~ery, 1 17(4), 323. (permission pending)
Figure Al The Suonybrook Facial Grading System From: Development of a sensitive clinicd facial grading system by Ross, B.G., Fradet, G., & Nedzelski, J.M. 1996, Otolamaolo~ Head and Neck Surperv, 114(3), 382. (permission pending)
Appendix B
Figure B 1 : Landmarks for The Maximal Static Response Assay (Figure 1) From: Simultaneous quantification of facial movements: The maximal static response assay of facial nerve function. Johnson, P.C., Brown, H., Kuzon, W.M., Balliet, R, Ganison, J.L., & Campbell, J., 1994. Annals of Plastic Sureerv, 32(2), 1 72. (permission pending)
Figure B2: Landmarks for The Three Dimensional Tracking S ystem in Sensitivity of a method for the analysis of facial mobility: vector displacement. Trotman, C., Faraway, J.J., Silverster, KT., Greedee, G.M., & Johnston, L.E.
Reprinted with pennission from m e American Cleft Palate-Craniofacial Association &iginaily pubrished in The CZe fi PaZute-Cranio facial JoutnuI, 1998; 35(2), 133. bending author permission)
Figure B3: Interlandmark Separation for The Three Dimensional Tracking System in Sensitivity of a rnethod for the analysis of facial rnobility: Landmark separation. Trotman, C., Faraway , J. J.
Reprinted with permission from The Americun CIeft Palate-Craniofacial Association OriginaZZy published in The Clef? PaZate-Cranidacial Joum~Z, 2000; 35(2), 1 43. @ending author permission)
TABLE OF CONTlENTS
TABLE OP CONTENTS ...aa...a.a.a............................................................................................... vi
LIST OF FIGURES AND TABLES ........................................................................................... i~
................................................................................................... LIST OF SREVL4TIONS * . s s ~
S ~ E C T I E ASSESSMENTS ............................................................................................................................................ 6 ENtXFtEn OBECTNE GRADING SYSTEMS ...................................................................................................................... 8
........................................................................................... Hotue- Brackrnann Facial Grading Scaie (HBFGS) - 9 ...................................................................................... Fisch Detaifed Evafuation @Facial Symmetry (DEFS) 13
................................................................................................ The Sunnybrook Facial Grading System (SFGS) 15 .................................................................... .............................. Critical Anaiysis of Indirect Grading Sysrems ,.. 17
CHARACTERISTICS OF ïHE WICAL S m .................................~~..~.......................................................................... 1 8 OBJEC~~VE MEASUREMMT SYSTEMS ......................................................................................................................... -22
Liner Memurement Index (LM?) ......................................................................................................................... -25 Faciorneter by Frey ................................................................................................................ ,... ................... .., 27
..................................................... Cornputeriked Quantitative Assessrnent ofRynamic Facial Motion (QAFM 29 ................................................................................................... The Maimal Static Rtsponse Assay (UTR4) 3 1 ...................................................................................................... Three Dimensional Tracking System (TDTS) 34
....................................................................................... Critical Analysis of Objective Meanrtement Systems ... 35 SUMMARY OF LITERATURE REVIEW ............................................................................................................................. 36
......................................................................... RATIONALE FOR THE CURRENT STUDY 38
............................................................................................................................ OBJECTIVES .*40
....................................... PHASE ONE: DEVELOPMEElT OF THE ROM ASSESS MENT ..41
DESIGN .....................................................................................~..............~.......~.....................~...................................... 42
............................................................. PHASE TMrO: PRIMARY RELlABILITY STllDY *43
S ~ J E ~ S E L E ~ O N ........... .. ..................................................................................................................................... 43 RATERS ....................................................................................................................................................................... -44 -mmNG pROCEDURES ................................................................................................................................................. 44 THE MEASUREMENTT00I.S ....................................................................................................................................... 45 DESIGN .................................................~...............~.............................~.............~.................~.......................................~~ 46 POWERAND SAMPLE SIZE ............................ ,., .......................................................................................................... 47 ANALYSES .................................................................................................................................................................... 47
................................................... PHASE: ONE: DEYELOPMENT OF THE .4 SSESSMENT 53
................................................... PHASE THREE: FOLLOW-UP RELIABILITY STZTDY ..66
DEVELOPMENT OF m ASSESSMENT ........................................................................................................................... 70 INTER-RATER RELLABIL~~Y .......................................................................................................................................... 71
Hypothesrlr One ................................,................................................................................................................. 73 Hypothesis Two ................................................................................................................................................... 75 HypothesrS Three ................................................................................................................................................ 76 Hypothests Four .................................................................................................................................................. 77
CONTRI~U~ONS OF ms -1s ................................................... .............................................................................. 79 Lwrr~no~s ................................................................................................................................................................ 80 F m D B C ~ ~ O N ................................................................................................................................................ 8 1
CONCLUSIONS ....................................................................................................... 0........0.0.....0083
APPENDICES
APPENDDC A: IND~RECT O B E ~ FACIAL GRADMG SYS- .................................................................................. I Table A l . The Howe B r o c h m Facial Nerve Grading Scale Table A2 . The Ftsch Detailed Evdurrtion of Facial Symmetry Figue A I . The Swi.ybrook Facial Grading &stem
APPENDK B: Dmcr OB JE^ FACIAL GRADING S Y S ~ .................................................................................... IV Figure 81 . Facial Landmmks for the Maximal Static Respome As* Figure B2 . Facial Landmarks for the Three Dimensional Tracking System Jector Displucement Figure B3 . Facial Lcrndmorksfor the Three Dimensional Tracking System Sepuration of
Lu.MharRF
vii
APPMDR C: MEAS- TOOLS... ..................................................................................................................... VU Figure CI. The Modified Hand Held Coliper Tool with Coronal Plane Level Figure C2. The Transparent Goniorneter
&PENDE D: INFORMATION SENT TO FAMILLES ........-............-................................................................................... IX Recruitment Letter Infiormation for Familier Letter of Responre
APPENDIX E: CONSENT FORMS ........................................-....................................................................................... XI Corsent form for partic@ants I6 years and older Consent-fbrm f i r participants Zms than 16 years of age Assent form
APPENDE F: ASsESSMENT PROCEDURES ......~................-.......................................................................................... XX Standard Protocol for the Administration of the Assesment Tobie FI. Data Base: ROM Assessmeni ofSrnile
LIST OF TABLES AND FIGURES
Table 1:
Figure 1:
Table 2:
Figure 2:
Figure 3:
Figure 4:
Table 3:
Table 4:
Figure 5:
Figure 6:
Table 5:
Table 6:
Table 7:
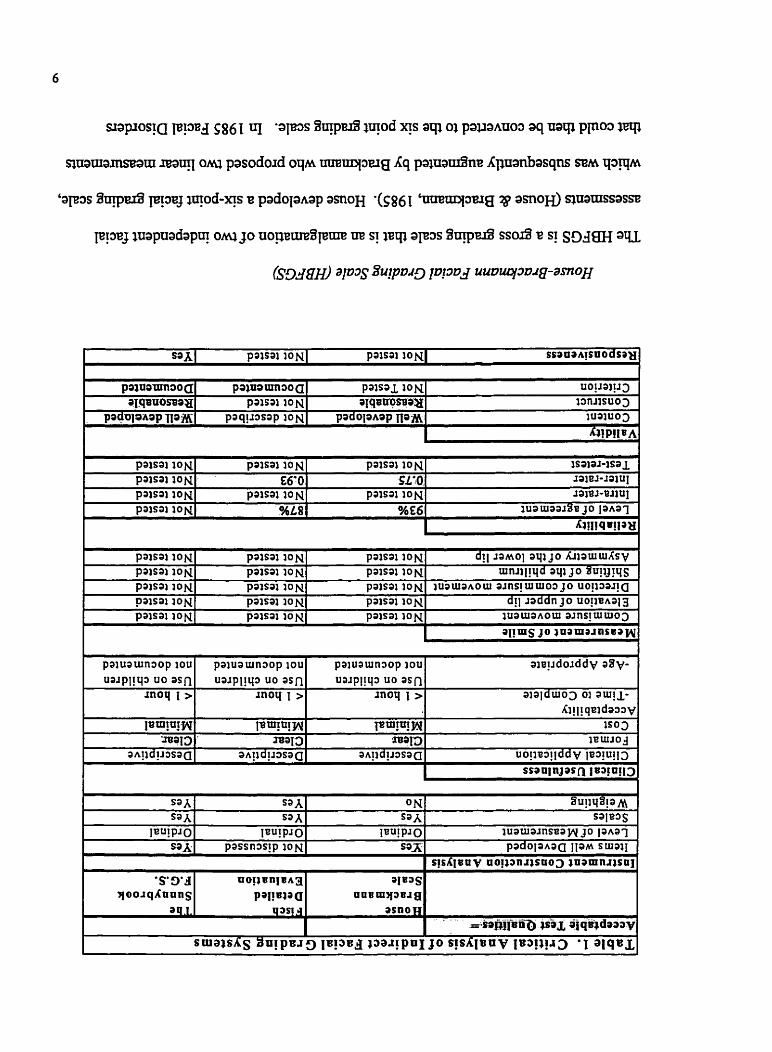
Critical Analysis of Indirect Facial Grading Systems: H o u e Brackmann Scale, Fisch Detailed Evaluation, The Sunnybrook Facial Grading System
Facial Landmarks based on the investigations by Burres (1985); Paletz, Manktelow & Chaban (1 994); Frey, MY, Giovanoli & Stussi (1 994)
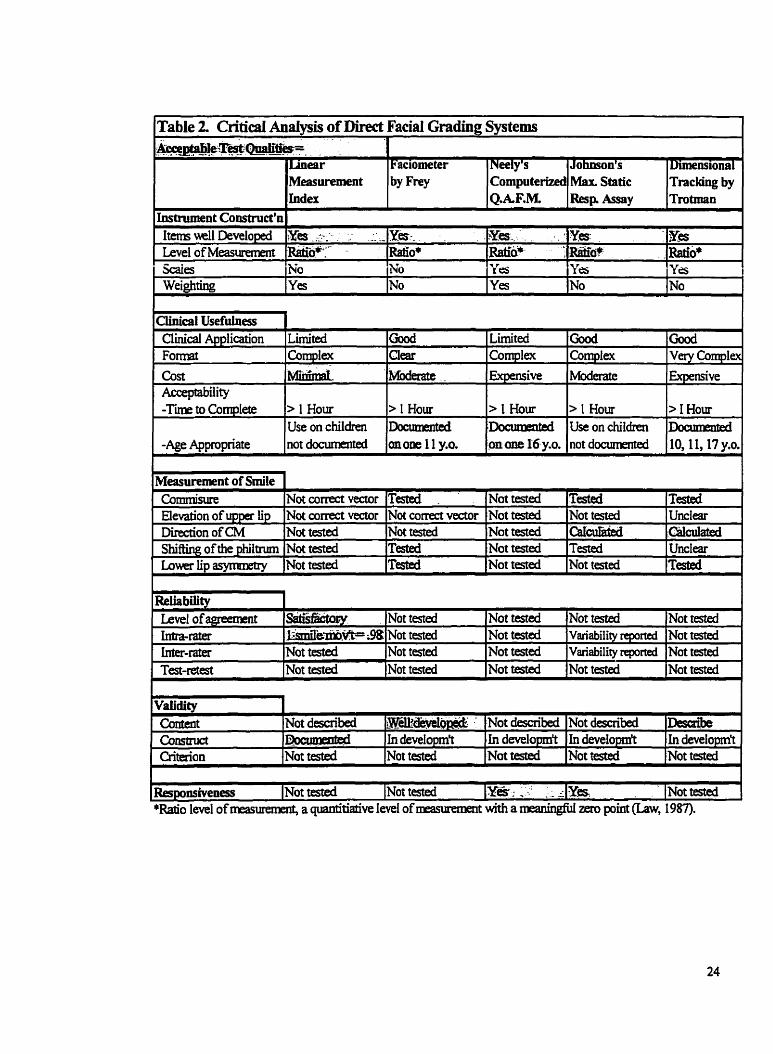
Cntical Analysis of Direct Facial Grading Systems: Linear Measurement Index, Faciorneter, Cornputerized Quantitative Assessment of Dynamic Facial Motion, The Maximal Static Response Assay, Three Dimension Trac king
Facial Landmarks -primary study
Range of Motion Assessment of Smile -pnmary study
Direction of Cornmisure Movement
Inter-rater Reliability of Facial ROM Measurement -primary study (distance measurements and direction of cornmisure movement)
Inter-rater Reliability of Facial Range of Motion Measurement -primary shidy (depth measurement)
Follow-up Study: Shifting of the Philtrum Revised
Follow-up Study: Depth of the Nasolabid Fold Revised
Inter-rater Reliability of Facial Range of Motion Measurement -follow-up study (distance measurement)
Inter-rater Reliability of Facial Range of Motion Measurement -follow-up shidy (direction of cornmisure movement and depth measurement)
Proposed Facial Assessment Data Base
Page 9
Page 20
Page 24
Page 56
Page 60,6 1,62
Page 63
Page 65
Page 65
Page 67
Page 68
Page 69
Page 69
Page 84
LIST OF ABBREVLATIONS
ROM
MCT
B F G S
DEFS
SFGS
LM
QAFM
MSRA
TDTS
HSC
ICC
ANOVA
ROM
Modified hand held caliper tool
House-Brackmann Facial Grading Scale
Fisch Detailed Evaluation of Facial Symmetry
The Sunnybrook Facial Grading System
Linear Measurement Index
Computerized Quantitative Assessrnent of Dynamic Facial Motion
The Maximal Static Response Assay
Three Dimensional Tracking S ystem
The Hospital for Sick Children
Interclass Correlation Coefficient
Analysis of Variance
LNTRODUCTION
Injury to the W cranial neme can result in a condition bown as facial palsy. This is
rnanifested by a unilateral or bilateral paralysis of the muscles of facial expression. Ln
children, facial nerve palsy can be classified into three major groups. The first group,
congenital or developmental facial nerve palsy presents at bkth and is a result of an error
intrinsic to embryogenesis; for example, Moebius Syndrome. The second category, prenatai
acquired facial nerve palsy, occurs as a result of extrinsic factors during fetai development;
for exarnple, pressure and infections. The third group, postnatal acquired facial nerve
paralysis, is the most diverse group of disorden, wbich includes inflammation, infection,
trauma, and diseases of the sM1 as well as intracranial and extracranial causes (Orobello,
199 1).
The incidence of facial paralysis in children has not been adequately reported. However, two
large studies with divergent results have docurnented the incidence of facial palsy in the
newbom. Hepner (1 95 1) reported a rate of occurrence of 7% where as McHugh, Sowden
and Levitt (1 969) ascertained a kequency of 0.23%. The reasons for this incongruity are
unclear, yet one can conclude the incidence of facial palsy in the newbom is a rare event
(OrobeiIo, 1 99 1). Nevertheless, as a tertiary center, the Hospital for Sick Children (HSC)
evaluates over 100 children with facial nerve p d y s i s through the plastic surgery clinic each
year (Dr. R Zuker, personal communication, 2000).
Paralysis of the facial muscles can have a significant impact on a child's physical, social and
psychologicaf developrnent Physicaily, children with facial newe palsy can present with
facial asymmetries and motor difficulties in tasks such as eating, drinking and speaking.
Socially these children will have the challenge of conveying emotions through facial
expression; for exarnple, happiness, sadness and surprise. The social effects of coping with
facial paralysis may lead to problerns in school and leisure activities. These children often
have to contend with cruel teasing from their peers and this can have a devastating impact on
their seit-esteem. Al1 of these factors can have consequences in the psychosociai adjutment
of the child.
To date, there has been no published research on the psychosocial adjustment of children
who present with facial pdsy. A few researchers have d e d the social psychology in
children who present with facial differences. These investigations typically included a small
sample group of children with a variety of craniofacial diagnoses that may or may not
include facial palsy. The results indicated children with craniofacial anomalies, when
evaluated against match cornparison groups, present with a number of psychosocial
limitations: the children were more introverted, have a poorer self-concept and experience
more negative social interaction (Pope & Wood, 1 997; Padwa, Evans, & Pillemer.F.C., 199 1 ;
Pertschuk & Whitaker, 1985).
Occupational Therapy is involved in the assessrnent and follow-up of children who present
with long-standing facial palsy. The majority of these children have undergone facial re-
animation surgery at HSC. In these chiIdren there is often a functional or anatomical absence
of the facial nerve and muscles (Dr. R Zuker, personal communication, 1999). This
population of children would be classified pre-operatively as having grade IV or grade V
facial function using the House-Brackmann facial grading scale. Grade IV ninction is
defined as obvious weakness andor facial disfigurement indicating moderate to severe
dysfunction. Grade V function is defined as only barely perceptible motion demonstrating
severe dysfunction (House & Brackmann, 1985).
For ciiildren who present with a uniiaterai faciai paisy, facial re-animation surgery is a two-
part procedure. The first stage involves a cross-face sural nerve gr& in which the unaffected
facial neme is evaluated and three to five fascicles from the zygomatic and buccal branches
are selected for repair with the nerve graft. The sural nerve graft is then placed in a
previously dissect tunnel across the face and the end is anchored close to the ear on the
paralyzed side. This technique allows for facial nerve input from the non-paralyzed side of
the face yet leaves adequate innervation of the musculature on the normal side.
Once the nerve graft has regenerated to the paralyzed side (6 to 12 months later) the surgeon
can proceed with the second phase; the muscle =fer. A section of the gracilis muscle with
its neurovascular bundle is transferred to the recipient side of the face. The origin of the
muscle is attached to the temporal fascia as well as the area in fiont of the tragus of the ear
and the insertion of the muscle to the commissure of the mouth and upper lip. The
neurovascular repairs then foilow. The goals of this procedure are: to have the mouth in
balance at rest, to assist in oral cornpetence, to improve speech patterns, to facilitate
voluntary and spontaneous active elevation of the corner of the mouth, and hal ly, to mate a
symmetrical d e (Dr. R Zuker, personal communication, 1 999; Frey, Jenny, Giovmoli, &
Stüssi, 1994; Zuker t Manktelow, 1993). Occupational Therapy interventions in children
with facial paisy address severai areas. In terms of motor function, the children may need an
exercise program to skengthen the transferred muscle andor re-training to gain a
symmetrical smile.
The assessment and treatment of children with facial palsy does present a significant
challenge to the multidisciplinary team. The clinical changes as a result of therapeutic
intervention can be significant but when measued objectively the changes are small. For
example, Goldberg & Zuker (in press) investigated the fiuictional outcomes of facial re-
animation surgery in children who presented with Moebius Syndrome (bilateral facial
paralysis of the VI and VI1 cranial nerves). Ln regards to facial motion these investigators
estimated the movement at the cornmisure corner of the mouth improved on average 15 mm
with a range of 6 mm - 28 mm. Elevation of the upper lip improved on average 7 mm with a
range of 4 mm - 13 mm. With the advances made in the surgical treatment of facial palsy
the curent measurement systems are either not sensitive enough to document the detailed
functional changes or too complex to be usefùl in the clinical setting. It is important to
establish a reüable and valid outcome assessment to quantify srnile in order to assess the
chid's progress, the efficacy of therapeutic interventions, and the long-tem functional
outcornes. The reliabiliq of an assessment refers to the consistency and stability of a
meanirement whereas validity refers to the assessments ability to measure what it is designed
to meastue (Law, 1987). The overall objective of this study is to develop a valid and reliable
assessment that will mûasure the range of movement for s d e in children with facial palsy
and is suitable for &y to day clinicai use.
LITERATW REVIEW
The intent of this review is to examine the accumulated empiricai evidence to determine if
there is a reliable, valid and clinically usefil assessment that wouid evaluate modest yet
signincant changes in the ROM of a child's smile. Several assessments currently used in
clinical practice are critiqued. Emphasis is placed on the scientific ngor and clinicai utility of
these instruments. The overd construction of the assessment is considered with particular
importance placed on the ROM evaluation of smile. Operational issues such as clhical
usefulness, scoring, cost and acceptability are reviewed. As well, the reliability, vaiidity and
responsiveness of the test are reported. Responsiveness is a fonn of vaiidity that it refers to
the tests ability to document changes within an individual over time (Law, 1987). The
review concludes with an evaluation of the existing rneasurement systems, followed by a
discussion of the specific research questions and hypotheses suggested by the review and
exsunined in this thesis.
Facial nerve palsy is a cornplex phenornenon to characterize. The multiple variables that can
be evaluated and how these variables are prioritized make it difficult to document findings.
As a result, there is a myriad of facial grading scales available and each scaie presents its
own hadequacies (House, 1983; Smith, Murray, Cd, & Slattery, 1992). For several years,
facial grading systems have been compared to one another, yet a universally accepted
grading system for facial rneasurement that is reliable, valid, responsive and clinically useful
continues to elude the investigators of facial nerve palsy (Burres & Fisch, 198613; House,
1983; Muw, Diver, Kelly, ODonoghue, & Bradley, 1994; Ross, Fradet, & Nedzelski, 1996;
Rickenmann, Jaquenod, Cerenko, & Fisch, 1997; Smith et al. 1992).
Facial measurement systems cm be classified into three categories: subjective, indirect
objective, and objective assessments. Subjective assessments that describe the clinical
outcomes following facial re-animation surgery include case reports that are typically written
by the surgeon who has performed the surgery and patient self-report questionnaires.
Indirect objective assessments are grading scales that have a set of criteria for making
jucigements, and objective assessrnenu use direcr measuremenr rechniques thar foilow the
principles of physics and mathematics.
SUBJECTIVE ASSESSMENTS
Throughout the facial palsy literature there are a number of published case reports. Zuker
and Manktelow (1 993) illustrated the fiuictional and aesthetic results following facial re-
animation surgery with two case reports. They described the outcomes for a 27-year-old as
follows:
the patient developed spontaneous contraction of the muscle, which provided a
pleasing lift to her mouth and obtained good soft tissue reconstruction of the cheek.
The muscle provided symmetry at rest and near syrnmetry with srnile. The patient
was very pleased and no longer felt that she was deformed. (p. 63)
Equaily positive results were achieved in a 9-year-old girl.
Suficient range of movement was accomplished and was reasonably symmetrical.
Most important, the activity was spontaneous and synchronous with emotional
expression. Her ability to handle social situations, her self-confidence and her
interpersonal relationships were greatly aided by her improved facial appearance.
@.64,65)
Kumar (1995) demonstrated the fiinctional results following facial re-animation surgery with
three case reports. A 23-year-old woman was described as having "good movements of the
transferred muscle, with good elevation but some asymmetry of the upper lip during smiling"
(p. 84). A 56-year-old man demonstrated "good movement symmetry on rest and animation.
Some asymmetry persisted on smiling. He had independent movement on both sides. He no
ionger has dificuities in eating and drinking" (p.85j. AI i i-yearsid boy was reponed to
have improved tone and symmetry of the face and does not drool. The elevation of his lip is
weak and the two sides of the face do not move independently. The scar on the left
cheek was hypertrophie. Although this settled down, the scar was stretched. His
results was assessed as fair. (p.85)
Case reports are descriptive studies that involve a detailed investigation of a number of
variables on a single subject (Hemekens & Buring, 1987, p. 18). This strategy allows for the
reporting of new therapeutic techniques and the presentation of individual clinical outcomes.
Case reports are helpful in the formulation of hypotheses; however, the results are not
generalizabie and are subject to bias since it is often the attending surgeon who is interpreting
the results (Burns & Grove, 1997, p. 256).
Selforeport questionnaires allow for the documentation of the patient's appraisal of the
surgical outcomes. O'Brien et al (1 990) and Sassoon, Poole and Rushworth (1 99 1) both used
patient questionnaires to cornplement their methods of assessrnent Some items in the
questionnaires included appraisal of symmetry in smiling, satisfaction with resuits, and
identification of complications such as pain and functional difnculties. Both investigations
reported the majority of patients had a hi& satisfaction post-operatively and felt the surgical
procedure was worthwhile and their appearance was improved. To evaluate the child's
perceptions of surgical outcornes, the questionnaire needs to be developmentally sensitive to
the issues of children. Unfominately, these researchers do not supply the reader with the
methods of administration or a sample of the questionnaires. This makes it impossible for the
reader to evaluate the validity of their methods.
I~JDIREC~ OBJECTIVE GRADING SYSTEMS
Indirect objective measurement systems use an ordinal grading scale with multiple
categories. The categones have a rank order but the interval between the ranks is not
necessarily equal. The patient's progress is evaiuated by set cnteria, thereby ailowing for
increased objectivity (Burns & Grove, 1997, p. 325). Ordinal grading scales can be M e r
classified into gross and regional grading scales. Gross grading scdes are descriptive scdes,
which consider the overall function of the face and give one grade for the degree of facial
paralysis. Regionai grading scales delineate separate areas of facial function, which are
observed and scored independently then added together for a total score (House, 1983). For
the purposes of this review three indirect objective grading scales are critiqued: House-
Brackmann Facial Grading Scale (Houe & Brackmann, 1985), Fisch Detailed Evaluation of
Facial Symmetry (Fisch, 198 1) and the Sunnybrook Facial Grading System (Ross, Fradet, &
Nedzelski, 1996). For a summary of the critical d y s i s of indirect objective grading scales
see Table 1. The taxonomy for this table is based on the research by Law (1987) as well as
the practical clinical requirements of this investigator. The acceptable test qualities have
been highiighted.
paisai ION paisai ION paisai ION 1 s a i a ~ - i s a ~ paisai ION 66'0 sL4-0. 1 3 1 8 J - l l ) U I
paisai WN pasai ION paisai ION ra i~~ -or iu l paisai ION %L8 %E6 wauiaa~%e J O laha1
pa1uauin3op iou a i s y d o ~ d d y a8v-
Conmittee of the American Academy of Otolaryngology adopted the HBFGS as the
international standard method for reporting results (Pearson, 1985).
In 1983, as his candidate's thesis to the Arnerican Laryngological, Rhinological, and
Otological Society, John Houe developed a six-point facial grading scale. He completed an
extensive analysis of eigh~ orchal masurement scales that had bcen developed ard used
between the years 1955 to 198 1. AU of the scales reviewed were successful in distinguishing
patients with varying degrees of nerve function. However, patients with moderate to severe
dysfunction are difncult to classify and it is this group which deterrnined the competence of
the scale. House theorized that the intent of a measurement scale was to rate the patient
according to general categories and not give specific details about facial fùnction. He
concluded that overall gross grading scales are preferred by dinicians and have the potentiai
to be just as reliable as the more detailed scales (House, 1983).
House (1983) developed a gross facial gradhg scale that M e r defined the moderate to
severe ranges of facial palsy and included secondary deficit. Secondary deficits are
described as contractures of the facial muscles, hemifacial spasm, andlor synkinesis.
Synkuiesis is an involuntary muscle contraction associated with facial movement (Ross et ai.
1996). Grade I on the HBFGS depicts norrnd facial function. Grade III indicates disfigurllig
clifFerences between the two sides of the face, the secondary deficits are minimal, there is
normal symmetry at rest and facial motion is weak. Grade VI indicates total paralysis
(House, 1983).
Brackrnann and Barn (1984) devised a facial grading system in a patient questionnaire
format to assess the degree of facial nerve recovery following acoustic neuroma surgery. The
objective h e m measurements (raise eyebrows and smile) were used in the development of
the HBFGS. In this study there was no evaluation of the insrniment itself to determine its
reliability, validity or responsiveness. The landmarks for the linear measurements were not
clearly defïned and the patient evaluated their own movements. The linear rneasurements
have added littie scientific value to the HBFGS and subsequent investigations refer
exclusively to the ordinal-scaie of measurement. The scaie continues to be referred to as the
HBFGS (see Appendix A, Table 1 for the complete scale).
Evans, Hanies, Baguley, and Moffat (1 989) tested the inter-rater reliability of the HBFGS
grading scale. Forty patients representing a complete range of unilateral facial palsy were
reviewed and tested on the same day by three skilled observers. The frequency of responses
was assessed and of the one hundred and twenty judgements, eight were in dispute by a
maximum of one grade resulting, in a level of agreement of 93%. These investigatoa
concluded that the HBFGS is a simple robust method of assessing facial function. The
limitation in this analysis is that level of agreement does not necessarily relate to the
reliability of the measurement scale and has the potential to overestimate the reliability of the
measure (S treiner & Norman, 1 995, p. 1 07). A superior statistical test of reliabiliv uses a
correlational design (Streiner & Norman, 1995, p.328) that takes into account agreement by
chance, such as Cohen's weighted kappa (Burns & Grove, 1997, p. 1 17).
Smith et al. (1992) compared nine facial grading systems (the grading scales examined by
House in 1983 as well as the HBFGS) to determine the reliability and constmct validity of
these scales. Construct validity was defined as the ability of the gradhg scale to differentiate
the degree of seventy of facial palsy.
This sniciy by Smith et ai. (1992) involved the assessrnent of ien subjrcts who reflectrd the
cornpiete range of recovery one-year subsequent to the onset of facial palsy by four
independent observers. Infra- and inter-rater reliability was estimated by the quadratically
weighted kappa statistic; an acceptable level is greater than .60. For each grading system
there was a reasonable degree of infra- and inter-rater reliability.
The accuracy of each grading scale to describe the degree of severity was evaluated and \
compared to the overall impression of facial function and there was no significant difference
between systems. The average Kappa value for al1 the systems was 0.74, suggesting that
most systems offer a reasonable level of construct validity (Smith et al. 1992). Although,
clinical judgement and overail impression is a poor test of construct validity (Ross et al.
1996). No single experiment can prove the constnict vdidity of a test. This is an ongoing
process that is satisfied over multiple investigations (Streiner & Norman, 1995, p. 152).
Smith, et al. concluded that gross grading systems are the most convenient to use, and
although the HBFGS did not give superior results, it was the grading system preferred by
most cihicians.
The development of the HBFGS was based on an excellent systematic review of the facial
grading systems in clinical use at that the . The HBFGS is an ordinal scale of measurement
that provides a good gross classification of facial nerve palsy. Clinically this measurement
tool is easy to use and is reported to have a good degree of inter-rater reliability (Evans et al.
1989; Smith, et al. 1992; Johnson et al. 1994; Ross et al. 1996).
The disadvantages of the HBFGS are that it is a discontinuou scale that inadequately
considers secondary deficits such as synkmesis. It is also questionable if the scale will
detect small yet clinically important change within a patient (Ross et al. 1996). This is a
gross grading scale therefore the properties of the test do not allow for the specific movement
analysis required to assess the range of movement of &le (Murty et al. 1994; Johnson et al.
1994).
Fisch Detailed Evaluation ofFacial Symmetry (DEFS)
The DEFS is a regionai evaluation of 5 standard facial poses: face at rest, raising eyebrows,
closure of eye with minimal effort and maximal effort, smiling, and pursing the lips. Patients
are given a percentage of function score: 0% = total paralysis, 30% = facial movement closer
to total paralysis than to normal symmetry, 70% = facial rnovement doser to normal
syrnmetry than to total pardysis and 100% = normal symmetry. The percentages of bc t ion
scores are then converted to a weighted point scale, with higher weighting given to eye
closure and smiling (see Appendix A, Table 2 for the complete scale) (Fisch, 1% 1).
Rickenmann et ai. (1997) compared the DEFS and the HBFGS grading scales with the intent
of determinhg whether the DEFS allowed for reliable sub-classifications of facial
rnovements to supplement the HBFGS. The major difference between these two systerns is
the division of facial movements; the 6 grades of the HBFGS, versus the percentage scale of
the DEFS. The DEFS reduces the number of assijped options, is weighted to emphasize the
esthetics and function of the mouth, and represents a more accurate sub-classification of
overall facial movement. The HBFGS scale has a wide numeric range within certain grades
and does not allow for M e r differentiation.
Rickenmann et al. (1 997) concluded that both systems have good reliability, minimal inter-
observer variability and reasonable agreement. Although both scales are a reliable grading of
facial movement, the DEFS is a finer scale. The investigators recommend a combination of
the nuo systems for a more accurate evaluation of facial palsy, particdarly after a facial
nerve repair.
The benefits of the DEFS are that it is a regional grading scale that is weighted to emphasize
the importance of the mouth. Overail this scale provides a good gross classification of facial
nerve palsy, is easy to use and is reported to have a good degree of inter-rater reliability
(Rickenmann et al. 1997).
The disadvantage with the DEFS is that synkinesis is assessed as a mass movement only
when it affects facial motion (Rickenmann et al. 1997). Furthemore, tests of validity and
responsiveness have not been completed. Again, this is a gross grading scale, therefore the
properties of the test do not allow for specific ROM analysis.
The Sunnybrook Facial Grading Sysfern (SFGS)
Ross et al. (1996) recently studied the literature regarding facial grading systems and
identified that the questions of validity and responsiveness have not been aciequateiy
addressed. This group of investigators set out to develop a clear, well-defined grading
system that provided an accurate description of facial motor function and that is responsive to
change. The necessary components of a facial grading system were identified, a measure
constructed, and its validity and responsiveness tested.
The SFGS is a regional gradmg scde that is based on resting symmetry, the degree of
voluntary excursion of facial muscles and the de gree of synkinesis associated with speci fic
voluntary movement. Resting symmetry is evaluated by comparing the resting position of
the eye, nasolabid fold and corner of the mouth to the nomai side. Symmetry of voluntary
movement and the degree of synkinesis associated with the movement are regionally
examined with 5 standard expressions: forehead wrinkle, gentle eye closure, mouth open
smile, snarl and lip pucker. These items are evaluated on a point scale and a cumulative
composite score is tabulated: 100 for nomai facial function and O for complete facial
paralysis (see AppendYt A Figure 1 for the complete scale) (Ross et al. 1996).
Content validity was established through a judgmental process. A review of the Iiterature
identified important content areas to measure dong with appraisal by expenenced chicians.
The construction of h a 1 measure was achieved after use with a broad spectnim of patients
with facial nerve paral ysis and informai exchange with physicians, facial phy siotherapists
and patients. To determine the constnict vaiidity of the SFGS these researchers elected to
compare the SFGS with the HBFGS (House, 1983) and a linear measurement system (Burres
& Fisch, 1986b). The responsiveness of this assessrnent was also investigated (Ross et al.
1996).
For the validation study, the SFGS was used to score the pretreatment and post treatment
videotapes of patients by an independent blinded assessor. The Pearson correlation
coefficient test detennined the inter-relationship between the individual components of the
SFGS. The components are independent and each component demonstrated an equally
significant correlation to the composite score. Each component of the SFGS is sensitive to
change and contributes to a change in the composite score. Significant correlation between
linear meamremeats and the voluntary movements occurred with forehead movements only.
The student t-test detected highly signûicant changes with pre- and post-test scores for each
component of the SFGS as well as the composite score. No statistical significance was found
with the IIBFGS (Ross et al. 1996).
In conclusion the SFGS reported results in a more continuous manner, had a wider response
range than the HBFGS and was sensitive to the severity of dyshction. Change was
detected in the individual components of the facial grading system and these were reflected
in the composite score. This facial grading system was shown to be a valid rneasure that was
responsive to cbically important change (Ross et ai. 1996).
The psychometric analysis of the SFGS was well designed and executed. This ordinal scale
provides a good clinical description of facial function and secondary deficits. The
measurement scale is easy to use and the validity and responsiveness of the measure has been
established. The disadvantages for the SFGS are that reliability of the scale has not yet been
tested and being a gross gradhg scale specific ROM analysis is not included.
Critical Analysis of Indirect Gruding Systems
House (1983) believed the purpose of a measurement scale was to rate the patient according
to generai categories and not give specific details about facial function, thus the development
of the HBFGS. Regional gradhg scales are a refinement of the gross gradhg systems.
Regional scales delineate separate areas of facial function so that the scores can be weighted
to reflect importance of facial function. This is usually based on the researchers' preference.
For example, the DEFS places higher weighting on the region of the mouth in contrat to
Ross, et al. (1996) who place a different emphasis on resting symmetry, voluntary
movement, and synkmesis.
Indirect grading scales rely on observer interpretation. Clinician may overrate or underrate
with respects to each other when evduating patients (Burres & Fisch, 1986b). Another
potentid difficuity in using these types of scdes is that the gradation of change that can be
detected is limited. Burres (1985) contends that observers are not able to discriminate arnong
more than three or four gradations of dysfunction. More specifically, grading scales have
been criticized for not being sensitive enough to document the changes in facial palsy as a
resdt of surgical intervention (Rickenmann et al. 1997). It therefore seems necessary to find
a system that limits observer interpretation (Smith et al. 1992) and cm detect finer gradations
of change in order to increase accuracy of evaluation.
The surgical re-animation for patients with facial palsy has becorne more sophisticated with
the introduction of the surgical fiee-muscle transfer. With these surgical advances the
methods used to clinically analyze facial motion are undergohg a rekemenr Born indirect
grading scales to objective measurement techniques.
The next section examines the characteristics of a typical srnile. The intent of this review is
to gain an understanding of the typicai srnile in order to make reasonabie judgements as to
what landmarks on the face should be analyzed with this facial motion. This knowledge base
is a prerequisite to the critical analysis of objective grading systems.
CHARACTERIST~CS OF THE TYPICAL SMILE
Facial expressions are a way of communicating our emotional condition to one another.
Srnihg to express happhess has been described as an intrinsic response that is culturaily
universai. Darwin (as cited in delatanzaro, 1999, pages 2 19-221) in 1872 documented one
of the original description of srnile. This scientist described a strong srnile as involving the
raising of the upper Lip that cause the cheeks to be drawn upward which in tum cause
wrinkles to form in the lower eye lids. As well the skin on the bridge of the nose becomes
wrinkled and the eyes becorne bnght and sparkling.
In 1974 Rubin proposed a qualitative description of a srnile that is based on the number of
teeth exposed. He determined that srnile cm be classified into three categories: the corner of
the mouth srnile, the canine srnile and the full denture smile. Although this classification is a
u s e M descriptor of smile, the quantitative analysis of movernent is overlooked.
Paletz, Manktelow and Chaban (1 994) investigated the shape of the nomal srnile. Eight
points dong the vermilion cutaneous boarder of the mouth were identified: each commisure
corner and the center and mid-Iateral points of the upper and lower lips. As well, two other
points were identified: the infenor border of the alar rim, and a point on a 45degree angle
fiom the oral commisure on the nasolabial crease (see Figure 1, page 20). The direction and
extent of movement of the upper and lower lips, nasolabial fold and the nasal base during
smile were analysed using stop h m e analysis with a 16-mm movie projector.
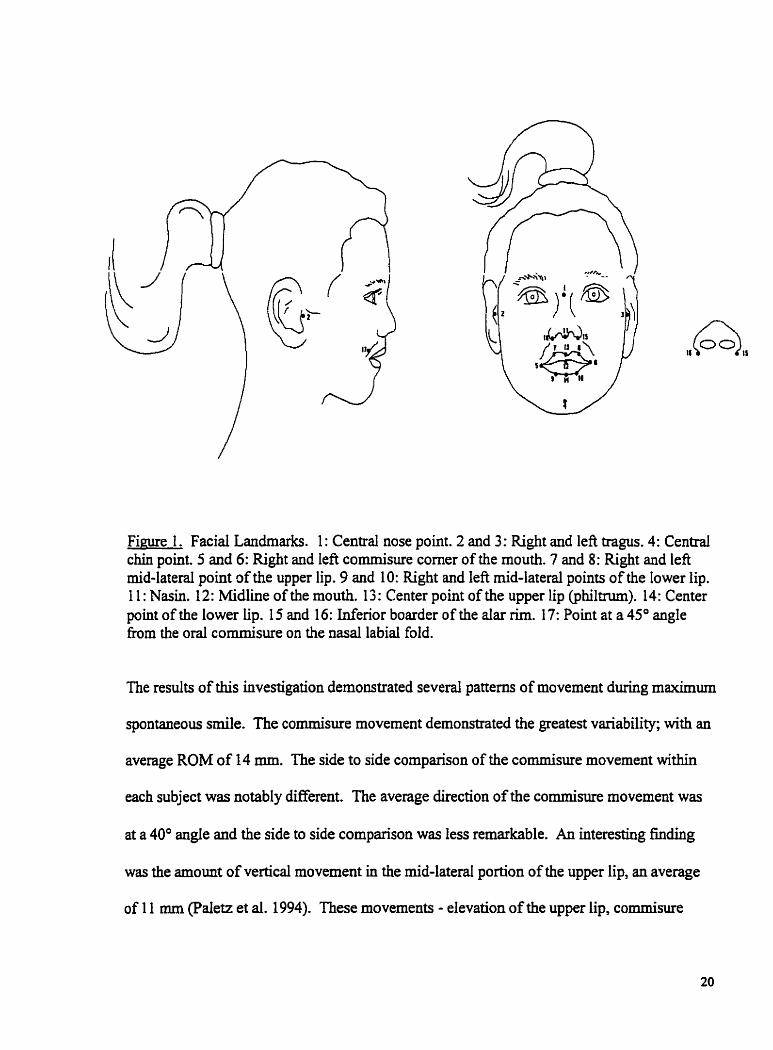
F i m 1 . Facial Landrnarks. 1 : Central nose point. 2 and 3: Right and left tragus. 4: Centrai chin point 5 and 6: Right and Ieft commisure corner of the mouth. 7 and 8: Right and lefi mid-lateral point of the upper lip. 9 and 10: Right and lefi rnid-lateral points of the lower lip. 1 1 : Nasin. 12: Midline of the mouth. 13 : Center point of the upper lip @hiltrum). 14: Center point of the lower lip. 15 and 16: uifenor boarder of the dar Rm. 1 7: Point at a 45" angle fiom the oral commisure on the n a d labial fold.
The results of this investigation demonstrated several patterns of movement during maximum
spontaneous d e . The cornmisure movement demonstrated the greatest variability; with an
average ROM of 14 mm. The side to side comparison of the cornmisure movement withh
each subject was notably different. The average direction of the cornmisure movement was
at a 40" angle and the side to side comparison was less remarkable. An interesting fincihg
was the amount of vertical movement in the mid-laterd portion of the upper lip, an average
of 1 1 mm (Paletz et al. 1994). These movements - elevation of the upper lip, commisure
movement and direction of the commisure movement - are valuable objective measurements
to document in the analysis of s d e .
Frey et al. (1994) also identified specific points (static and dynamic) on the face in order to
quanti@ facial movement. As well, this group explored the distances and the movements
that wouid be the most representaUve of the 3 regionai areas of the face jiiontal, eye, an8
nose/mouth). The VICON three dimensional, computer-assisted measurement system was
used for the motion analyses. For this review, discussion will be limited to the results
associated with the mouth region.
Three static reference points were required for three-dimensional motion analyses; the left
and right tragus of the ear and a central nose point were favored. Paletz et al. (1994) had
identified the centrai chin point as a static reference point and this was also tested in this
study. The dynamic points investigated were as follows: the commisure corner of the mouth?
the philtrum, and the mid-Iaterai points of the upper and lower lip (see Figure 1 .) (Frey et al.
1 994).
The resuits indicated that the most reliable static points were the tragus of the ear and the
cenaal nose point. In the mouth region, a greater number of points were required to reflect
the complexity of motion in this area. The commisure corner of the mouth showed the
greatest excursion and the philbxm point described the aesthetic of middle upper lip.
Symmetry of the mouth is an important parameter to measure in order to assess the quality of
therapeutic intervention. The mid-lateral points of the upper and lower lips best assess
symmetry (Frey et al. 1 994)
Once the static and dynamic points were identified the relevant distances for measurernents
were determined. For the nose and mouth, 6 relevant distances were identified. To assess
lateral movement in the mouth, measurements are taken fiom the tragus and cornmisure
comer of the mouth. The central nose point and the mid-lateral point of the upper lip descnbe
the upward movement of the mouth. The centrai nose point and the mid-lateral point of the
lower lip describe the asymriletry in the lower lip. The distance between the ph i l tm and
tragus give a clear picture of the shifting of the philtrum, and the distance between the comer
of the mouth and the philtnim provide information on the intrinsic movements of the lips
(Frey et al. 1994).
Throughout this last section the normal patterns of movement dwhg srnile have been
examined including a review of suitable reference points and distance measurements to
quantify smile. Prior to cntiquing the objective grading systems it is beneficial to have an
understanding of these concepts.
OBJECTIVE MEASUREMENT SYSTEMS
Over the past decade there has been a shift in focus fiom grading scales to detailed objective
data collection systems. Many investigators have attempted to quanti@ facial movement by
using a variety of direct measurernent techniques and computer technologies. These systems
have been developed in reaction to the perceived weakness of indirect grading scales and
other observer-dependent systems. The purpose of quantitative systems is to reduce observer
bias, reduce rater variability and detect h e r gradations of change.
Objective measurement systems use a ratio measurement scale and have the ability to present
a Iess biased and more sensitive assessment. Ratio level of measurement refers to the use of
a quantitative variables with a meaningful zero point (Law, 1987). For the purposes of this
review five objective measurement systems will be cntiqued: Linear Measurement Index
(Bures, 1985), Faciorneter (Frey et al. 1994), Computerized Quantitative Assessrnent of
Dynamic Facial Motion (Neely, Cheung, Wood, Byers, & Rogerson, 1992), The Maximal
Static Response Assay (Johnson et al., 1994) and Three Dimensional Tracking (Trotman,
Stohler, & Johnston, 1997). For a summary of the critical anaiysis of objective grading scaies
see Table 2. The acceptable test qualities have been highlighted.
l~able 2. Criticai Anaivsis of Direct Facial Gradhg &stems 1
Insbiunent Construct'n Items w11 Developed Levei of Meamemnt Wes Weipfrting
1 -Age Appropriate 1 not doCumaNd Ion one 1 l y.0. lonane 16 y.0.
I
> 1 Hour -i-i
Memurement Index
use ~nchil~-- not documentai
Clinical Application Format cos
by Frey
Acapdiiiiy -Ti to Complete > 1 Hour > 1 Hour > 1 Hour
Use on children Documented .Docuniented
Good Uear
Moderate.
Limited Cornplex &
Xes .:.-. . -; -. .-
-Rtdi"oY- Xo Yes
Limited Cornplex
Escpensive
Measurement of Smile L
Comniisure
Computerized QAF.M.
Not correct vector (Tested . . 1 Not testeci Elevation of upper lip M o n of CM Shifüng of thephiltnrm LOW I ~ D
Tested Not tested C a l a Tested Not tested
L I
Responsiveness INot testecl lNot tested ~Y&L ' . - L [ Y ~ - I~otte~ted *Ratio level of cneasuremer9 a w v e IeveI of measuremait with a sxwhgiFiil zero point (Law, 1987).
Max. Static Resp Assay
Yi= Ratio* Ys I
No
Yes-. bYes.. ' . . 11Yes -
l
Tested UncIear cdoulM Unc Iear Tested
Not correct vector Not tested Not tested N0t tested
Valid@ Coldent Construct
Tracking by Trotman
. W o * .
Ys No
Ratio* No No
Not correct vedor Not testeci Tested 'ks&!d
: Yes Yes
Not tested Nat tested Not tested Not tested
Not descn'bed fiPgelliiiél/el~@ '
In deue1opm't Not tested
Not descri i In developm't Nottested
Not described In âevelopm't
Desgibe In developm't
Not tested lNot tested

Liner Memurement Index (LM)
To quanti@ motor function, Burres (1985) proposed a LM1 in which a hand held caliper tool
is used to assess facial ROM. Linear measurements (distance measurements) are defined as
the distance between each of the facial landmarks at rest and at maximum rnotor capacity for
specinc facial expressions. in the preliminary investigations tàcial expressions were
evaiuated in normal subjects by linear measurements and integrated electromyography. This
inqujr is limited to the linear measurements that characterize srnile.
Burres (1985; 1986a) related the amount of displacement of facial landmarks to the motor
recovery of the muscles. Through his own review of the literature and his own study using
integrated electromyography, he concluded that skin displacement, force and electrical
activity are ail related and codependent. To determine the reliability of the measurements, a
coefficient of variance score was caiculated (a cornparison of the distance moved with the
variation of displacement). In total eight measures were classified as the most reliable to
esthate the total facial motion. To depict smile, three facial landmarks were identified and
two distances measured. They are as follows: the midine of mouth to the cornmisue comer
of the mouth and fiom the nasin to the comer of the mouth (see Figure 1, page 20). Based on
these measurements Burres proposed a linear measurement index for maximum voluntary
facial motion.
Bmes (1986a) studied subjects with facial paralysis using the LMI. To account for the
pathology of facial palsies such as: negative displacement, comed exposure and resting
asymmetry, the L M required significant revisions. The raw scores continue to be converted
to a percentage of displacement followed by a minimum of seven mathematical steps to
arrive at the h a 1 score. He concluded that it was impossible to establish an absoiute
standard measure due to the fact that with the facial palsy group, the displacement of the
paralyzed side of the face was fiequently in the range of the normal side of the face.
Although, significant clifferences are documented when an individual side to side cornparison
was made.
The L M has been compared to the DEFS and HBFGS indirect grading scales which were
discussed earlier (Burres & Fisch, 1 986b). Subjects were studied through the use of video
analysis and photographs. At the tirne of recording the video, linear measurements were
collected, and a total of seven observers assessed each patient. The level of agreement, the
correlation between grading scales and the inter-observer variability were tested. Al1 scales
demonstrated satisfactory level of agreement and the coreIation between the scaies was
excellent at r=. 92 to .95. This would indicate that facial grading systems founded on
reasonable criteria would tend to correlate with each other. As weil, the superiority of the
LM was established, as it was able to accurateiy match the mean score of the judges. In
conclusion, Burres (1986) purports the LMI to be a clinically valid method of objectively
grading facial palsy (Burres, 1986a).
The simplicity of linear measurements has the potential to be a c l i n i d y useful approach in
documenting facial motion. The hand held caliper tooI is a practical measurernent tool that is
easily adaptable in the clinical setting. In more recent studies, Ross et al. (1991) used the raw
data fiom the linear measurements to determine the efficacy of biofeedback training. These
investigators evaiuated the in~a-rater reliability of the linear measurements and the midline
of the mouth to the commisure corner was chosen to represent smile. The interclass
correlation coefficient (ICC) of .98 demonstrated substantial ina-rater reliability with a
lower 95% confidence limit of .96.
In practice the proposed LM1 is hown for being complex and time consumuig to administer
and calculate the linear measurernent index score. M e r precise measurements are taken and
there is a conversion to an index score, valuable information is lost. Moreover, the
assessrnent does not take into account the correct vectors of movement in the examination of
srnile. The LM1 may be too arduous to be useful in clinical practice.
Faciorneter by Frey
Frey et al. (1 994) introduced the concept of three-dimensionai tracking. He recognized that
cornputers are usehl for research purposes but are not suitable in day to day practice
therefore, the hand held electronic faciometer (S&T Marketing Ltd.Q, Switzerland.) was
developed. The faciometer is an electronic caliper tool with sofl rounded tips, which aiiows
for direct skin contact. When measuring the distance between two points a foot switch is
used and the actual distance is digitally displayed in rnillirneters.
The first clinical trial with the faciometer was completed with twenty healthy subjects, and
ten subjects with a unilateral facial palsy. The landmarks chosen and the distances measured
have been previously described within the section "characteristics of the typical smile". in
this investigation the statistical analyses of the results are not clearly presented and it was
inferred that inha and inter rater reliability was good. The results were reported as a mean
score. The mean range of scores and the standard deviations for the resting positions = 0.67
t 0.66 mm and for maximal exercises = 0.86 t 0.80 mm denoting a low degree of variability.
For sub-maximal exercises the mean range of scores and the standard deviations =1.13 t 1 .O7
indicating a higher degree of variability. A recomrnendation was made that oniy intra-
individual comparison is made with the sub-maximal scores but the maximal exercises were
suitable for inter-individual comparison. These researchen ascertain this to be a valid and
reliable tool that was comparable to the VICON cornputer system although a direct
comparison was not made (Frey et al. 1994).
The overall assessrnent with respects to identification of landmarks and the distances
measured have been well developed. The faciometer has a few good qualities as a
rneasurement tool, for example soft tips and the ability to reach al1 data points on the face.
The reliability and validity of the tool is reported as being good and responsive to change
although no specific reliability testing was reported. Reliability represents the consistency of
the rneasure obtained. Typically this is best represented by a correlation coefficient score
that takes into account three sources of variance: patient, observer, and error (Streiner &
Norman, 1995, pages 106-109). Intuitively the faciometer appears to be highly reliable tool,
although the interclass correlation coefficient would have more accurately represented the
reliability of the i n m e n t .
There are a few difficuities with the faciometer in that the long lever amis make it difficult
for the observer to stabilize the device and achieve accurate measures. The digital reading is
displayed on a separate piece of equipment that typically sits on a table. The protocol also
suggests that two observes should complete the assessment, one to measure and the other to
read and document the digital read out. The faciorneter is not a tool that is widely utilized in
clinical practice and no M e r studies on its psychomeac properties have been published to
date. Moreover, this assessment does not evaluate the directionality of movement.
Computerized Quantitative Assesment of Dynam ic Facial Motion (QAFIY)
Neely et al. (1 992) developed a computerized quantitative assessment of dynamic facial
motion. This system is extremely complex and based on the reflection of light fkom a black
and white video image. The initial study involved subjects with and without facial palsy and
the QAFM was compared to the HBFGS.
Facial movements were recorded with a black and white video under specific light condition
and compared to a baseline resting position. Movements included: forehead wrinkle, eye
closing, nose wrinkiing and mouth smiling. The video was played into a rnicroprocessor for
analysis that involved digitization, subtraction and image enhancement. in brief, the
digitization process coded each pixel; the more intense the Light the higher the digital
number. In the subtraction step, the sequential fiames of the face in motion were paired and
subtracted fiorn the reference rest image. The areas of the face relocated by movement
changed the pixel values signincantly and this was reported as a positive number. Image
enhancement involved the following: any areas of the face that changed were rendered white,
and areas that remained the same were black (Neely et al. 1992).
The computer then generated x-y plots and a curve of motion was identified. The curve was
divided into the initial contraction slope (S-50), the falling relaxation slope (Fs), and the area
under the curve for the total pixel count. A ratio score was calculated to reduce the
variability of the absolute pixel values and to enhance the differential cornparison between
sides. No difference in the score would produce a ratio of 1 .O and 0.0 would approximate
extreme differences. Results indicated that the cornputer-generated data was highly
significant except for the falling slope of the eye motion, and there was a reasonable
comlation with the HBFGS (Neely et al. 1992).
Neely, Joanquin, Kohn, and Cheung (1996) continued to refhe this method for quantifying
facial motion. The grading system consists now of three components: the restrained human
observer index, the computer generated strength duration cuve in which five typical curves
are recognized and coded, and the computed c w e maximum amplitude. Weighted values
are assigned to each of the three components and a composite index score is calculated
ranging Born O to 102. The QAFM was again tested on twenty-seven subjects in various
stages of recovery h m facial palsy. When c6mpared to the HBFGS, this system was more
precise and better able to dserentiate within the grades. They concluded that this was a
discrete objective outcome measurement system. The degree of facial movernent was
defined by specinc regions and for the face as a whole. This system was able to document
individuai case progression and recovery.
This cornputer measurernent system is cornplex, expensive and not practical for day to day
clinical use. Neely, Cheung, et al. (1992) recognized that this system was not capable of
vector analysis and was ody able to identiS a change in the image. There are many
variables in the system creathg noise in the generated data and the weighting of the scale
was not criteria based and may change with M e r research. No validity or reliability
experiments have been conducted on this memurement system.
The Mmeimal Slatic Respome Assay (MSRA)
The MSRA was developed by a group of investigators in Pittsburgh. The evaluation allows
for simdtaneous measurernent of both global and regional specific zones. nie MSRA used
photographs or video analysis to record a rest position and maximal displacement of nine
landmarks during six movements: brow lie eye closure, smile, fiown with jaw open, whistle,
and fiown with jaw closed (see Appendix B, Figure 1 .). The displacements of facial
landmarks were measured and the data was analyzed as coordinates on a grid using a
digitizer board and hand-held puck (Johnson et al., 1.994).
The MSRA was aialed on seven normal subjects and three subjects with abnormal facial
movernents. To assess the intra- and inter-rater variations the photographie data was
rneasured independently by three observers and each photograph was analyzed three times by
each observer. The results of this analysis are not reported. The variability of dot
assignment was 0.07 cm for normal subjects (Johnson et al ., 1 994).
These researchers conclude that the MRSA has the ability to detect region specific facial
movements, region specific decreased movement, and the dinical absence of movement and
synkuiesis. As an adjunct to the ordinal scales, the MSRA was designed to give a
quantitative evduation of the retum of facial movement f i e r therapeutic intervention
(Johnson et ai., 1994).
In an attempt to assess the quality as well as the quantity of facial motion the MSRA was
modified to account for matornical motion versus non-anatomicd motion. Anatomical
motion is the primary movement of the regional facial muscies and non-anatomical motion is
the secondas, movement that occurs on the involved side of the face. Anatoinical and non-
anatomical index scores are calcuiated to summarize the data generated by the MSRA in a
clinically meaningful way. Through the digitization process each dot is assigned a x and y-
axis thereby indicating the direction of movement. The vecton of movement are
mathematically defined in degrees of movement from the horizontal line. A ratio score of the
affected side versus the unaffected side is calculated (Bajaj-Luthra, Mueller, & Johnson,
1997).
The revised MRSA was tested on thirty-four subjects with complete facial paralysis. To
evaiuate the indexes over time a sepamte cohort group of five subjects with Bell's pdsy,
fiom whom multiple assays were available, were studied and compared to twenty-six healthy
controls. The results indicated that the group of subjects with complete unilateral faciai palsy
demonstrated a signincant amount of non-anatomical motion that was not present in the
healthy group. When assessed over t h e the group of Bell's palsy subjects demonstrated
recovery of facial nerve function (Bajaj-Luthra et al. L 997).
The MSRA was used to study the movement outcornes of functional fiee-muscle transfers for
re-animation of smile. A retrospective study of six subjects who underwent smile re-
animation surgery was completed. They were cornpareci to a conkoi goup of twsnty-seven
heaithy subjects with normal facial hction. The results indicated that the change in the
direction and magnitude of the smile was statistically significant. Symmetry was improved
by decreasing the magnitude of pull from the other side (Johnson, Bajaj-Luthra, Llull, &
Johnson, 1997).
Johnson et al. (1994) identified that the misplacement of dots, misplacement of the grid,
change in head position, reading the results and entry errors are weaknesses to this
assessment. The major limitation to the MSRA is the two dimensional technique. A smile is
a three dimensional process and the MSRA is unable to assess the change in the
antenor/posterior direction, the z-axis. Therefore the results of the vector analysis are not
accurate (Johnson, Bajaj-Luth et ai. 1997). Furthemore, despite the evidence that the
MRSA is a reliable quantitative tool that will assess the severity of facial palsy and measure
motor recovery, it is very complicated and may not be reasonable for the busy practitioner
(Bajaj-Luthra et ai. 1997).
Three Dimenrional Tracking Sjstem (TDTS)
A group of investigators fiom Michigan explored the use of a TDTS to report facial mobility.
Subjects are video taped perfomiing six maximal facial expressions and each frame is
digitized for analysis. It was determined that a head cap with three stable markers is the best
method to account for head movement and a total eighteen skin based landmarks evaluated
facial movement. Face validity was documented and the analysis to assess displacement of
angles introduced (Trotman, Stohler, & Johnston, 1997).
To evaluate vector displacement a stable maxillary dentition was fabricated for each subject
and three markers attached. Thirty points on the faces of six subjects with different functiond
problems were identified (see Appendix B, Figure 2.). Vector displacement was based on
means and CO-variances and a percentile score computed. Two measures of functional
impairment were proposed: a total impairment score and a maximal impairment score. To
determine the sensitivity of these scores, resdts were compared to residents rating motor
impairment on a Msual analog scale. These investigaton concluded that the TDTS has the
ability to detect and characterize a range of clinically significant fiinctional deficits (Trotman,
Faraway, Silvester, Greenlee, & Johaston, 1998).
Further attempts were made to quant@ facial movement based on separation of landmarks.
A total of thirty landmarks were identified (see Appendix B, Figure 3.). The separations
between twenty landmark pairs during six maximal facial animations were evduated in five
normal subjects. This research determined that for each facial animation a pattern of
landmark separation was identifiable, quantifîable and representative (Trotman & Faraway,
2000). The correct direction of movement for smile was not accounted for in this study.
The TDTS is a very complex assessment and is not practical for the day to day use in the
clinical setting. In order to assess movement in the anterior/posterior plane each subject
needs to be fitted with a dental plate, and it is possible that this dental plate will interfere with
the natural motion of srnile. The TDTS computer assessment is in the early stages of
development but has the potential to provide three-dimensional analysis of vector movement.
These investigatoe recognized that for displacements less than 3 to 5 mm it may not be
possible to clinical resolve the direction of movement with this technique (Trotman, Stohler,
& Johnston, 1997). No reliability or tests of responsiveness have been conducted on this
measurement system.
Critical Analysis of Objective Memurement Systems
The mathematical analysis of facial movement has several advantages. It is objective,
quantifiable and has continuous variables (Ross et al. 1996). There are also many Limitations
to this nethod in that linear measures of facial movements are highiy variable fiorn day to
day, linear excursions do not address syokinetic movernent, methods can be time consuming,
and the calculation of a linear index score can be complex (Murty et al. 1994; Ross et al.
1996).
Several computer systems designed to measure facial movement have been discussed. These
systems do present with a few advantages, for example facial movement is recorded by
photography andor video therefore the facial image cari be retrieved at anytime for fûrther
investigations. With this technique several measurements can be performed at the same time
and this is important factor to consider for muscle fatigue can be an issue with this patient
population.
Overall these computer systems are complex, expensive, take t h e to complete and are
limited in everyday clinicai application. The assessments were primarily tested on an adult
population and it is questionable if young children wodd be able to comply with ihz
administration procedures. The majority of the computer assessments fail to provide an
analysis of vectors in the anterior/posterior plane of motion. In addition, the computerized
assessments are deficient in the development of reliability and validity studies as well as tests
for responsiveness.
SUMMARY OF LITERATURE REVIEW
This literature review highlights the fact that researchers of facial palsy are attempting to
describe facial hc t i on , to document change in facial function and to evaluate treatment
approaches. Indirect objective grading scales and objective measurernent systems produce
different results. The purpose of indirect objective grading scales are to grade the overall
functionai performance, they are not intended to give detailed information on facial
movernent. Three indirect grading scales were reviewed: the House-Brackmann Facial
Grading Scale (House & Brackmann, 1985), the Fisch Detailed Evaluation of Facial
Symmeûy (Fisch, 1981) and the Sunnybrook Facial Grading System (Ross et al. 1996).
Indirect grading systems present with several limiting factors. These assessments do not give
specific details about facial bc t ion , they rely on observer interpretation and are not
responsive to the s m d c l in id changes seen as a result of facial re-animation surgery. Whiie
the scientific value of these systems may be limited (Frey et al. 1994), the gross description
of facial palsy has been uaiversally accepted and can be helpful in the description of a
population.
In contrast to the indirect objective grading scales, objective measurement systems provide
very specific details on facial motion. Objective methods have the abiiity to give a lzss
biased and more sensitive assessment. Five objective measurement systems were reviewed:
the Lhear Measurement Index (Burres, 1 9 8 5), the Faciorneter (Frey et al. 1 994), the
Computerked Quantitative Assessrnent of Dynamic Facial Motion (Neely et al. 1992), the
Maximal Static Response Assay (Johnson et al. 1994) and the Three Dimensionai Tracking
System (Trotman, Stohler, & Johnston, 1997). To document facial ROM two investigatoa
used direct linear measurements. (Burres, 1985; Frey et al. 1994) The simplicity of this
approach has significant potential for day to day dinical use. As well, the caliper tool is a
practical measurement tool that is easily adaptable in the clinical setting. The three computer
assessments that were reviewed are expensive, complicated to administer, and do not
necessarily provide the analysis of vectors. To date computer assessments maybe useful for
research purposes but are not suitable for day to day clinical use with children.
In conclusion, a review of the literature has demonstrated that a suitable tool to measure the
ROM of srnile in children with facial palsy is not available. It is the intent of this research
study to develop an assessment tool that is suitable for day tu day clinical application with
children and considers the important parameters to measure in the ROM assessment of smile.
RATIONALE FOR THE CURRENT STUDY
With the advances made in the surgical treatment of facial palsy, ordinal grading systems are
not suniciently sensitive to document the detailed functional changes. Fuahermore, the
children typically folIowed at HSC do not present with the secondary deficits that the indirect
objective grading systems attempt to measure for there is often an absence of the facial nerve
and muscles. The few cornputer assessments in use may be of benefit in an aciuit researcii
setting however these systems are limited in the everyday application with children. In a
hospital based milieu children can be fearfbl of complex technical equipment and
consequently do not readily comply with testing procedures. Children c m present with a
limited attention span and they tend to require severd breaks fiom the testing procedures. To
date there is not a simple assessment battery that is suitable for the daily evaluation of
children in the dinical setting.
It is the opinion of this investigator that a direct objective measurement system that uses a
caliper method of measurement seems to have a number of advantages. The assessment can
be completed in a timely manner; it is easy to administer, portable, and inexpensive. The
hand held caliper tool that was originally designed for the measurements of various objects
requires a few adaptations in order to facilitate the assessment of linear measurements on the
face. These modification have been descnbed in the methods section of this thesis (pages 45
and 51). The MCT has superior clinical potential when compared to the electronic
faciorneter. The proposed MCT is easier to manipulate as it is held closer to the
meanirement point. The digital reading is directly on the caliper tool and at eye level of the
assessor allowing one therapist to complete the assessment. The digital reading is to a tenth
of a millimeter and this provides an accurate measurement that can be sensitive to small
changes. The caliper tool is inexpensive costing $52.75 Canadian where as the approximate
cost of the electronic faciorneter is $2000.00 American.
The modified hand held caliper tool will not be able to capture al1 the facial movements of
clinical interest therefore, a tlat transparent plastic goniorneter and straight ruier werç aiso
considered. niere have been no previous studies that have documented the application of
these two tools in the measurement of facial movement nevertheless these tools continue to
be used in clinical practice. In addition to evaluating the MCT it is of interest to this
investigator to also test the reliability of the goniorneter and the straight d e r in the ROM
assessment of srnile in children with facial palsy.
PURPOSE
The purpose of this shidy is to develop a valid and reliable assessment that will rneasure the
range of movement of smile in children with facial palsy. The identification of pertinent
facial landmarks, distance measurements (Iinear measurements), and the direction of
movement are addressed in the development of the ROM assesment. As well, the selection
of suitable instruments to masure the facial rnovement of smile are considered and the inter-
rater reliabiiity detennined.
OBJECTIVES
The specific objectives of this study are as follows:
a) to develop a range of motion assessment of srnile for children with facial palsy and
establish the content validity of the assessment, and
b) to determine the inter-rater rdiability of the clinicaiiy derived measures of smile
using three measurement tools: the MCT, the d e r and the goniorneter in the
assessment of srnile in children with facial palsy. It is not the intent of this study
to complete a comparative analysis of the three measurement tools. The most
clinically appropriate one of the three tools has been selected to complete each
measurement.
HYPOTBESES
Once the content validity for the ROM assessment of srnile has been established the
following hypotheses wili be tested:
1) In each designated measurement there is an almost perfect relationship (.8 1 - 1 .O)
between the ratings of two observes on the distance measurements in the assessment of
srnile when using the modined hand held caliper tool.
2) In each designated measurement there is a substantial relationship (-61 - 30) between the
ratings of two obsewers on the distance measurements in the assesment of smile when using
the de r .
3) ïhere is a substantial relationship (.61 - 30) between the ratings of two observers on the
direction measurements in the assessment of srnile when using the goniorneter.
4) There is a substantial relationship (.61 - .80) between the ratings of two observers on the
depth measurements in the assessment of srnile when usmg the modified hand heici caiiper
tool.
METHODOLOGY
E s investigation has been subdivided into three phases. Phase one delineates the
methodology for developing the ROM assessment of srnile. Phase two outlines the
procedures for the primary study that evaluates the inter-rater reliability of this assessment.
Based on the resdts of phase one and two, four of the measurements required refmement and
phase thtee outlines the methodology for the follow-up inter-rater reliability midy.
PHASE ONE: DEVELOPMENT OF THE ROM ASSESSMENT
Validity of a test refers to its ability to measure what it is design to measure (Law, 1987).
For an assessment to have appropriate content validity the evaluation must include ail the
necessary components relevant to the coostnict being measured. Content validity for the
facial ROM assessment wiIl be established and documented through a judgmental process.
No quantification with statistics is necessary as the overall opinion or consensus is sufncient
(Benson & Clarke, 1982).
Criterion validity is the correlation of the measurement tool with some other measure that has
been widely used and accepted in practice (Streiner & Noman, 1995, p. 147). To date there
is no such clinical tool for the direct measurement of a smile; therefore, criterion validity will
not evaluated in this shidy.
Constnict validity refers to the ability of a measurement to WIy describe the cnaracteristic
being meamred (Law, 1987). Establishing constmct validity is important when evaluating
abstract variables that are not readily observable; for example, sweaty paims, tachycardia and
difficulties concentrating are variables which dl can describe anxiety (Streiner & Norman,
1995, p. 150). In the ROM assessment, srnile is measured as a physical artnbute that is
readily observable and defined by the way it was measured, in millimeters.
DESIGN
The content validity of this srnile ROM assessment was established through an extensive
review of the Literature and with consultation with four expert clhicians. The facial ROM
assessment presented in the result section of this thesis was based on the scientific
investigations of Bunes, (1986a), Paletz et ai. (1 994) and Frey et ai. (1994). In addition Dr.
Manktelow and Dr. Zuker who are experts in the field of facial re-animation surgery
provided their recommendations on a routine basis. Dr. Farkas was also consulted in regards
to the parameters of the smile ROM assessment. He is a Plastic Surgeon who is world
renown for his scientinc research of the anthropological documentation of facial
measurements. Additionally, the facial ROM assessment was informally trialed by the
Occupational Therapist who routinely evaluates the children who present to therapy with
facial palsy.
PHASE TWO: PRIMARY RIELLABILITY STUDY
SUBJECT S E L E ~ O N
Children 5 - 18 years of age with a diagnosis of faciai palsy were recmited through the
Plastic Surgery Clinic at HSC. As well, the Division of Plastic Surgery facial palsy data base
was accessed and appropriate children and their parents were contact by mail requesting their
participation in the study (see Appendix D for recruitment letter, information sent to families,
and letter of response). niose children with cognitive irnpairments who were unable to
follow the assessrnent format were exciuded fiom the study. The minimum age of 5 yean
old was chosen to ensure the child would be able to comply with the testing procedures and
18 is the maximum age of children seen at HSC.
A convenience sample of thirteen subjects with facial palsy volunteered for the snidy. Both
sides of the face were measured and each side was considered an independent sample,
therefore, doubling the sample size to twenty-six. Subjects with facial palsy do present with
facial asymmetry and this will reduce the expectation bias of the rater. To consider each side
of the face as independent sarnples is a common practice in the facial measurement literature
(Frey et al. 1994; Neely et al. 1992).
There were ten girls and three boys who participated in the study. The chilcken's ages
mged nom 5.6 years - 15.3 years with a mean age of 1 1.8 years. The sample was
representative of a variety of diagnoses: three children presented with congenital facial palsy,
five children with prenatal acquired facial palsy and five children with an acquired a facial
@Y -
RATERS
Two Occupationai Therapists currently employed at HSC on the Plastic Surgery Program
served as the raters. Both therapists have considerable experience in the assessment of
children with facial palsy and are familiar with facial ROM assessments. One of the raters is
the primary investigator for this study. The raters received specific training in the protocol of
the measurement procedures, the identification of landmarks and each therapist practice
performing the measurements. This established a common baseline berneen the two raten to
decrease the inter-rater variability associated with the execution of the assessment technique.
TESTING PROCEDURES
Pnor to the completion of the facial ROM assessment inf'ormed consent was obtained.
Subjects older than 16 years of age provided informed consent. Parents for subjects less than
16 years of age signed a consent form and the children signed an assent fom. (see Appendix
E for consent forms)
Each subject was tested independently by the two raters in the Rehabilitation Department at
HSC. The testing room was quiet and fkee fiom distractions and only the rater, the child and
hidher parent(s) were present The subjects were seated on a chair during the measurement
session and the rater was seated directly in fiont of the subject at eye level. A picture was
placed on the wall facing the subject to serve as a place to focus while the rater identified the
facial landmarkS. Milky Gel RollersN (Pente1 Stationary 0, Richmond B.C.) were used to
draw a 1 mm dot at each facial landmark. The subjects were allowed to choose their own
color of millcy pen and the rater demonstrated on the child's hand how easily the marks were
removed.
Each rater completed a facial ROM assessment following a standard protocol for
administration (see Appendix F). The distance measurements and the direction of the
cornmisure corner of the mouth were assessed once ody. The depth of the nasolabial fold
measurement is a new measwernent therefore three triais were recorded. Each measurement
was taken in the resting position and while smiling with maximal teeth showing. Data were
collected and recorded on the Data Base: Range of Motion Assessrnent of Smile (see
Appendix F, Table 1). Rater one completed the facial ROM examination, which was
followed by a 15-minute break. During this break the landmarks were removed. Rater two
then completed the assessment for a second time. The total evduation was approximately
one hou. The younger children required more frequent breaks fiom the assessment
procedure.
THE MEASUREMENT TOOLS
The tips of the hand held caliper tool were lengthened so that al1 data points on the face could
be reached easily. To mesure the depth of the nasolabial fold a platform base was added
dong with a telescoping point. To improve the stabitity of the instrument in the coronal plane
for the depth measurement a s m d level was attached to the platfom base. This level was
able to pivot to facilitate measurernent on the nght and left sides of the face and to ensure
consistency in the placement of the level a mark was etched into the platform base. The
modifications of the tool were conducted through the Medical Engineering Department at
HSC. (see Appendix C, Figure 1 .) In consultation with Andrew Baziw, medical engineer at
HSC (personal communication, 1999), the modifications to the tool did not effect the digital
measurement scale and there was no loss in the accuracy of the tooi. The MCT has been
utilized Ui clinical practice at HSC on the facial paralysis program for several months with
positive findings.
The MCT will not be able to capture the directionality of movement at the cornmisure corner
of the mouth. A standard transparent flat plastic goniometer was used to document this
motion (see Appendix C, Figure 2.). The diameter of the goniometer was nine centimeters
and the resolution of this instrument was rnarked in individual degrees. As wefl, distance
rneasurements of small magnitudes such as lip droop and shifting of the philtrum were
measured with a standard 15 centimeter transparent straight d e r with a resolving power of 1
millimeter (see Figure 3, page 6 1).
DESIGN
Reiiability refers to the consistency of a measurement. It is dehed as the ability of the
assessrnent to measure the tme dineremes between subjects on the characteristics being
measured (Law, 1987). More specincdy, intramter reliability is the degree of agreement
between the obsewation made by the same rater on two different occasions and inter-rater
reliability refer to the consistency(.U of results between different raters. It has been proposed
that both intra and inter-rater reliability testing may not be necessary for the reason that al1
the sources of error that would contribute to inira-rater reliability will become apparent in the
testing of inter-rater reliability (Streiner & Norman, 1995, p. 114). To lessen the arnount of
testing the children were required to undergo this investigation was limited to the evaluation
of inter-rater reliability. Using a correlational design the inter-rater reliability between two
raters was investigated.
POWER AND SAMPLE SIZE
According to the estimates by Donner and Elisaziw (1987) fifieen subjects were required to
have 80% power to measure an inter-rater reliability of .80 or above. The lower 95%
confidence limit has been set at .81 (almost perfect relationship) as per the guidelines by
Donner and Eliasziw. An obtained ICC value of less than .8 1 would indicate a problem with
the inter-rater reliability of the measure.
ANALYSES
The interclass correlation coefficient (ICC) was used to deterrnine the inter-rater reliability of
the motor assessrnent of smile. The ICC is an index score that estimates the amount of
variation in a set of measurements. Due to the fact that there are successive measurements
the ICC is based on the variances obtained through the repeated measures analysis of
variance (ANOVA). ANOVA is a statistical method that is used to anaiyze the relationship
between variables and the total variance is broken down into three components: the rater
(independent variable), the subject (dependent variable) and enor (Portney & Watkins, 1993,
p. 509-5 10). To interpret inter-rater reliability scores general guidelines have been
established. Slight reliability is indicated by an ICC value betweenO - .20, fair .21 - .40,
moderate .41 - .60, substantial.61 - .80 and almost perfect .81 - 1 .O (Donner & Eliasziw,
1987).
The literature that considers what an appropriate cut point shouid be for a reliability
coefficient is divers. ui determining how reliable a test should be is reiateci to iiow the resr
will be used. For example if the test is to be used for making individual judgements it should
be more reliable (Streiner & Norman, 1995, p. 12 1). In keeping with the guidelines set by
Donner & Eliasziw (1 987) a cut point for an acceptable level of reliability for this assessrnent
was chosen to be .8 1, an almost perfect. Due to the fact that no previous studies in the facial
measurernent literature have used the d e r and goniorneter a lower ICC of -6 1 was chosen for
hypothesis testing. Although, this investigator recognizes that for theses measurements to be
considered for clinical use a reliability coefficient of .8 1 is required.
The inter-rater reliability for the eleven measurements of facial distance and the two
measurements for the direction of cornmisure movement were calculated using the ICC
random effects mode1 for absolute agreement. The random effects mode1 for absolute
agreement will take into account the variance produced by the raters. This mode1 is based on
a repeated measures analysis of variance with the rater as the independent variable (Portney
& Watkins, 1993).
ICC = BMS - EMS BMS + (k-1)EMS + klRMS - EMS)
n
The @&--rater reliability of the depth of the nasolabial fold was based on the three scores
taken by each rater. In this design, the ICC for absolute agreement was estimated by using
the likelihood method in the variance components procedures within the computer program,
Statistical Package for Social Science 9.0. With this method the enor variance is divided by
the number of trials, which would be three for this investigation.
- ICC =
I
os- os2 + o R 2 + b $
3
The 95% confidence interval was also calculated for each ICC (McGraw & Wong, 1996).
Reporting the lower limit of the confidence interval serves two purposes. Firstly to test the
underlying assumption that the value of the ICC is O and if this is true the confidence interval
will inciude the value of O. Secondly to determine the limit of uncertainty conceming the
degree of reliability present is one's data. The lower limit of the confidence interval may
suggest a much poorer reliability that the acnial ICC (Fleiss, 1986, p. 13). The lower 95%
confidence limit has been set at .8 1 (almost perfect relationship) as per the guidelines by
Donner and Eliasziw (1 987).
PHASE THREE: FOLLOWIUP RELIABILITY STUDY
Based on the poor results of the primary research study fou. of the facial measurements were
re-examined. Lip droop, the depth of the nasolabial fold and shifting of the philtnun required
modifications to the facial landmarks and measurement procedures. The procedures for the
direction of d e facial meamernent were aiso reviewed. These revisions have been
presented in the result section of this thesis.
At this point in the investigation it was difncult to recniit children with facial palsy, therefore
eight addts through the Rehabilitation Department at HSC volunteered for the study. No
subject presented with a facial impairment. Both sides of the face were measured, therefore,
doubling the sarnple size to sixteen. There were four fernale and four male subjects who
participated in this snuiy. The ages ranged from 27.0 y e m - 43.6 years with a mean age of
35.2 years.
RATERS
The same two raten completed the follow-up study. The raters reviewed the protocol for the
revised measurement procedures and the identification of landmarks. Each therapist
practiced performing the measurements. This established a comrnon baseline between the
two raten to decrease the inteprater variability associateci with the execution of the
assessrnent technique.
TESTMG PROCEDURES
Each subject was tested independently by the two raten in the Rehabilitation Department at
HSC. The testing room was quiet and fiee fiom distractions and only the rater and the
subject were present. The mbjects were seated on a chair during the measurement session
and the rater was seated directly in fiont of the subject at eye level. A pichue was placed on
the wd facing the subject to serve as a place to focus while the rater identifîed the facial
landmarks. Millcy Gel RoUersm (Pentel Stationary @, Richmond B.C.) were used to draw a
1 mm dot at each facial landmark.
Each rater completed a facial ROM assessment following a standard protocol for
administration as described in Phase Two. Data were collected and recorded on the Data
Base: Range of Motion Assessment of Smile (see Appendix H). The distance measurement to
document the shifting of the philtnim was assessed once. Three triais were recorded for the
measurements: depth of the nasolabid fold and the direction of the cornmisure corner of the
mouth. Each measurement was taken in the resting position and while smiling with maximal
teeth showing. Rater one completed the facial ROM examination, which was followed by a
IO-minute break. During this break the landmarks were removed. Next, rater two completed
the assessment for a second time. The total evaluation was approximately thirty minutes.
THE MEASUREMENT TOOLS
Further modifications to the hand held caliper tool were made in an attempt to improve the
inter-rater reliability of the depth measurement of the nasal-labial fold. With improved facial - land-rnarking the coronal level became redundant but a new level was attached to the
platform base to limit the movement of the device in the saggitd plane (see Appendix G).
The modification of the tool was conducted through the Medical Engineering Department at
HSC. In consdtation with Andrew Baziw, medicai engineer at HSC (personal
communication, 1 999), the modincations to the tool did not effect the digital meamrement
scale and there was no loss in the accuracy of the tool.
DESIGN
Validity
In an attempt to improve the inter-rater reliabifity of facial measurements: Lip droop, depth of
the nasolabid fold and shifüng of the philtrum the landmarks were revised. The new facial
measurements are presented within the result section of this thesis and are outlined in figures
5 and 6, pages 67 and 68 respectively.
The inter-rater reliability for shifting of the philtnim was calculated using the ICC random
eEecrs modei for absolute agreement. T'ne random effrçts mode1 for absolute agreement
takes into account the variance produced by the ratee. This mode1 is based on a repeated
measures analysis of variance with the rater as the independent variable (Portney & Watkins,
K C = BMS - EMS BMS + O<-1)EMS + k(RMS - EMS)
n
The inter-rater reliability of the depth of the nasolabid fold and the direction of srnile was
based on the three scores taken by each rater. Based on this design, the ICC for absolute
agreement was e h a t e d by using the likelihood method in the variance components
procedures within the computer program, Statisticd Package for Social Science 9.0. With
this method the error variance is divided by the number of trials, which would be three for
this investigation.
ICC = os2 oS2+az+bE
The 95% confidence interval was aIso cdculated for each ICC and the lower limit recorded
(McGraw & Wong, 1996).
RESULTS
PHASE ONE: DEVELOPMENT OF ASSESSMENT
The first objective of this investigation was to develop a ROM assessment of smile for
children with facial pdsy and establish the content vaiidity of the assessment. The concept
of direct measurements is not new in the facial palsy Iiterature and Burres (1986a) was one of
h e fust investigatoa to apply Lhis technique to racial rneasurements. He idenufieci faciai
landmarks and linear measurements (distance measurements) as the necessary parameters to
document facial movement. Frey et al. (1 994) highlighted the fact that facial landmarks need
to be reproducible and in locations that will not be dismpted as a result of surgicai
intervention. As weii this group recognized that the distance measurements need to be
representative of the actual movement that occurs during smile. nirough the investigation by
Paletz et al. (1994) the direction of movement was also identified as a factor that should be
considered during smile. In children who present with unilateral facial paralysis the direction
of the commisure rnovement is possibly more important that the extent of movement. As a
result of this review one can conclude that the important parameters for the ROM assessment
of smile are facial landrnarks, distance measurements and the direction of the commisure
movement.
The construction of the final assessment was achieved after a review of the literature;
consultation with experienced cliniciaos and informal use with a variety of children with
facial palsy. The presentation of this ROM assessment for smile has been subdivided into
îhree categories : facial landmmks, distance rnemwernents and the direction of movement.
FACIAL LANDMARKS
In the Iiterature static and fünctiondly representative dynamic points have been empirically
evaluated. Static reference points are necessary for three-dimensionai motion analysis,
although with the use of static landmarks the variability in direct measurements can be
partially controlled. The central chin point, the tragus and the central nose point have d l
been ,aidisil. Through tomputer andysis the centrai nose poin~ aad the tragus of the ear
were identifieci as the supenor static points. It has been determined that the movement of the
mandibular joint affects the center point of the tragus, therefore the upper border of the tragus
has been recommended (Frey et ai. 1994). Dr. Farkas @enonal communication, August 4,
1998) has suggested that the tragion be used as the most consistent static landmark, this is
located at the most supenor point of the tragus. It appears that these hvo points may in fact
be the sarne and for the purposes of this investigation this point will be referred to as the
tragion.
The cornplexity of the motion around the mouth necessitates that several dynamic points are
required to measure smile. Through computer analysis the cornmisure corner of the mouth
showed the greatest excursion. The midline of the philtrum best described the aesthetic of
the upper lip and symmetry of the mouth was best characterize by the mid-lateral points on
the upper and lower lips (Frey et al. 1994). With re-constructive surgery it is necessary to
concentrate on the cornminire rnovement but attention must also be paid to the
vertical/lateral movement of the upper Iip (Paletz et al. 1994). Dr. Manktelow (personal
communication, 1999) has recommended that a landmark at the superior attachment of the
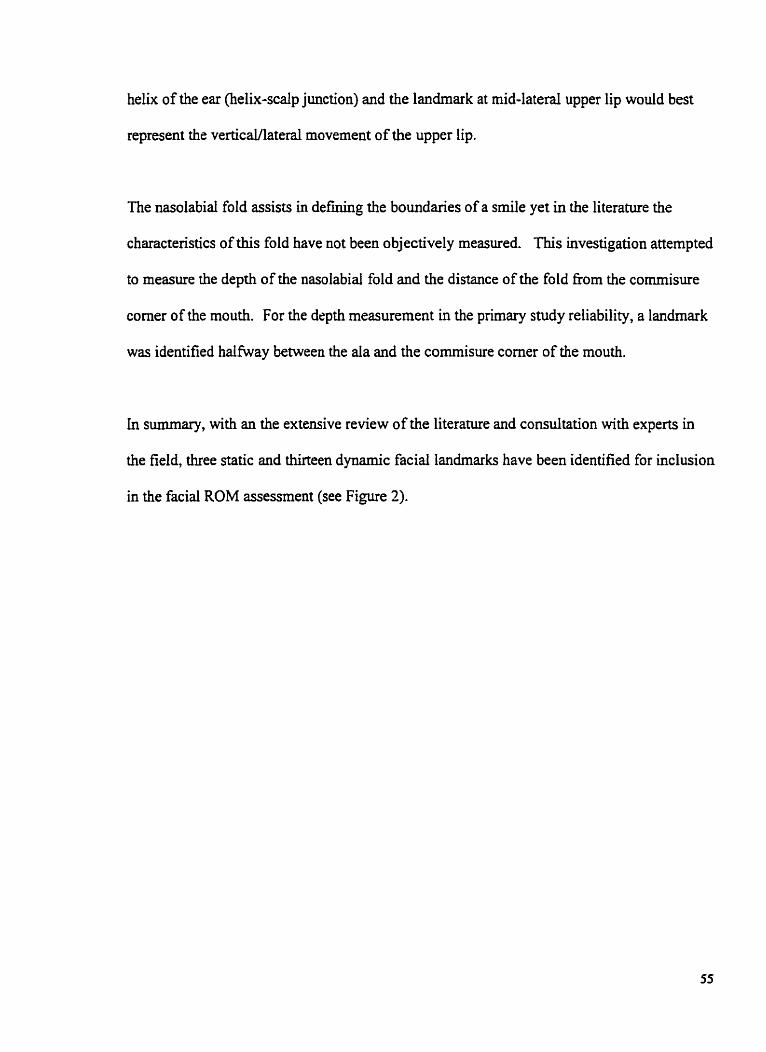
helix of the ear (helix-scalp junction) and the landmark at mid-lateral upper lip would best
represent the verticaVlatera1 movement of the upper lip.
The nasolabial fold assists in defining the boundaries of a smile yet in the literature the
charactenstics of this fold have not been objectively measured. This investigation attempted
to measure the depth of the nasolabial fold and the distance of the fold fkom the commisure
comer of the mouth. For the depth rneasurement in the primary snidy reliability, a landmark
was identified halfway between the ala and the commisure comer of the mouth.
in summary, with an the extensive review of the literature and consultation with experts in
the field, three static and ihirteen dynamic facial landmarks have been identified for inclusion
in the facial ROM assessrnent (see Figure 2).
F i w e 2. Facial Landmarks. 1 : Central nose point. 2 and 3: Right and left tragion. 4 and 5: Right and left cornmisure corner of the mouth. 6 and 7: Right and Iefi rnid-laterd point of the upper lip. 8 and 9: Right and Ieft mid-lateral points of the lower lip. 10: Philmim. 1 1 and 12: Iderior boarder of the alar nm. 13 and 14: Mid-point between the inferior boarder of the d a rim and the cornmisure corner of the mouth dong the nasolabial fold. 15: Rîght ear helix - scalp junction.
In the evaiuation of smile, Paletz et ai (1 994) identified the elevation of the upper Lip, the
lateral movement of the commisure corner of the mouth and the direction of the conunisure
movement as essential movements in the anaiysis of smile. Another important component to
assess is symmetry of the mouth while in a resting position and during srnile (Frey et ai.
1994; Paletz, et al). For distance meanirements to be representative of smile rnovements
they need to be representative of the actual movement that occurs during smile (Frey et al.).
The commisure comer of the mouth moves in an upward and lateral direction at
approximately a 40' angle (Paletz et ai. 1994). To represent this movement Frey et al. (1 994)
measured nom the tragus (tragion) of the ear to the commisure corner of the mouth. Burres
(1986) chose to measure fiorn the comrnisure comer of the mouth to the lateral canthus
(outside corner of the eye), fkom the commisure comer to the nasal spine, and fkom the
commisure comer to the midine of the lips. None of the distance rneasurements
recommended by Burres represent the actual movement during smile, which should be at an
approximate 40' angle fiom the commisure corner of the mouth. The best distance
measurement was determined to be fkom the tragion to the commisure comer of the mouth
(see Figure 3 #1, page 60).
The mid-lateral portion of the upper lip moves in a more veriical/lateral direction at
approximately a 43' angle (Paletz et al. 1994). Frey et al. (1994) recommended a
measurement nom the Md-laterd upper lip to the central nose point. This direction of
movement is not entirely correct for it does not take into account the movement in the lateral
direction. The movernent of the mid-Iateral portion of the upper lip is best measured b e ~ e e n
the helix point and the midpoint of the upper lip (Dr. R. Manktelow, personal
co~lllflUILication, 1999) (see Figure 3, #2).
The symmetry of the lower lip is best detennined through the distance measurement fiom the
midpoint of the lower iip to the central nose point. This has been recommend by Frey et al.
(1994) and is reasonable for the actual direction of movement (Dr. R Manktelow, personal
communication, 1999) (see Figure 3, #3).
Direct objective measurements for lip droop have not been described in the literature.
Clinically, Lip droop demonstrates asyrnrnehy in the mouth at rest and during smile. Dr.
Manktelow (personal communication, 1999) has recommended that the negative
displacement of the commisure corner of the mouth be directly measured with a ruler, fiom
the horizontal line at the base of the teeth to the commisure comer of the mouth (see Figure
3. M, page 61).
The aesthetics of the upper lip are best described by the symmetry of the philtrum (Frey et al.
1994). Dr. Manktelow (personal communication, 1999) suggested that the shifüng of the
philtrum be directly rneasured with a ruler, from the mid-point of the two front incisors to the
philtmm (see Figure 3, #5, page 61).
The distance the nasolabial foId fiom the commisure corner of the mouth is a valuable
measurement to document during smile (see Figure 3, #6). This distance measurernent is
particularly important to assess in the outcornes following fiee muscle transfers, as the
muscle is inserted dong the commisure comer of the mouth @r. R. Zuker and Dr. R.
Manktelow, personal communication, 1999). The depth of the nasolabial fold is a new
measurement and the procedures have been outlined (see Figure 3, #7, page 62).
This literature has determined that the most consistent movement is smiling with the
maximal showing of teeth @mes, 1985; Frey et al. 1994; Neely et al. 1996; Johnson et al.,
1994; Trotman et ai. 1997). Each distance measurement with the exception of the distance
fiom the commisure corner of the mouth to the nasolabial fold is measured with the mouth in
a resting position and at maximal smile with teeth showing. The distance tiom the
commisure corner of the mouth to the nasolabid fold is measured at maximal srnile oniy. A
total of eleven distance measurements are documented in this range of motion assessrnent of
smile. In addition to the distance measurements, depth measurements are evaluated in an
attempt to characterize the contour of the nasolabid fold.
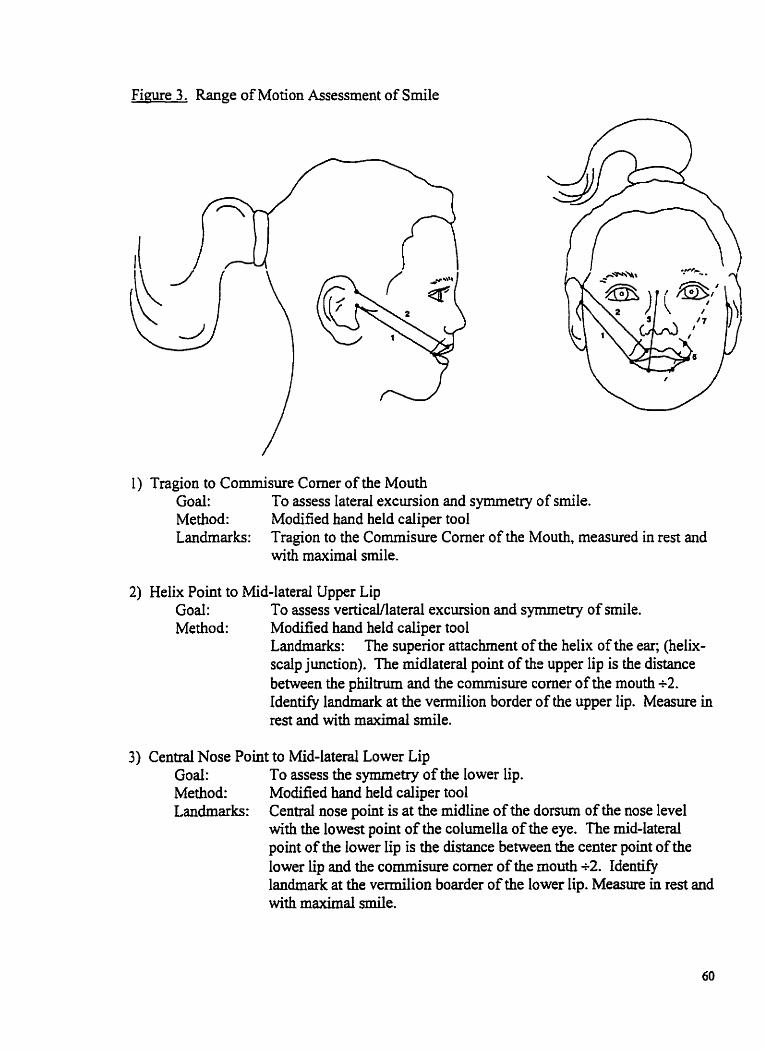
F i w e 3. Range of Motion Assessrnent of Smile
1) Tragion to Commisure Comer of the Mouth Goal: To assess lateral excursion and symrnetry of smile. Method: Modified hand held caliper tool Landmarks: Tragion to the Commisure Comer of the Mouth, rneasured in rest and
with maximal smile.
2) Helix Point to Mid-lateral Upper Lip Goal: To wess verticaYlatera1 excursion and symrnetry of smile. Method: Modified hand held caliper rool
Landmarks: The superior attachent of the helix of the ear; (helix- scalp junction). The micilateral point of the upper Iip is the distance between the philtrum and the commisure corner of the mouth i 2 . Identify landmark at the vermilion border of the upper iip. Measure in rest and with maximal srnile.
3) Centrai Nose Point to Mid-lateral Lower Lip Goal: To assess the symmetry of the lower lip. Method: Modified hand held caliper tool Landmarks: Central nose point is at the midline of the domun of the nose level
with the lowest point of the columella of the eye. The mid-lateral point of the lower lip is the distance between the center point of the lower lip and the cornmisure corner of the mouth R. Identify landmark at the vermilion boarder of the lower iip. Measure in rest and with maximal srnile.
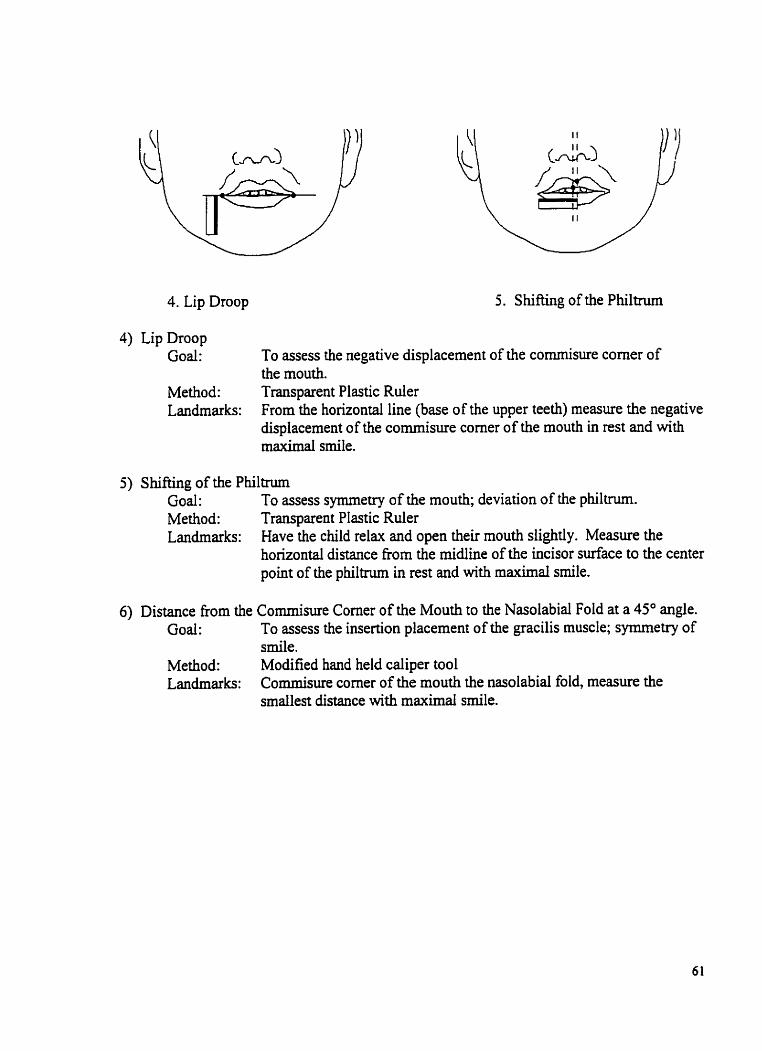
4. Lip Droop 5. S h i h g of the Philtnim
4) Lip Droop Goal: To assess the negative displacement of the cornmisure corner of
the rnouth. Method: Transparent Plastic Ruler Landmarks: From the horizontal line (base of the upper teeth) measure the negative
displacement of the cornmisure corner of the mouth in rest and with maximal srnile.
5) Shifüng of the Phi1hu-n Goal: To assess symmetry of the mouth; deviation of the philtrum. Method: Transparent Plastic Ruler Landmarks: Have the child relax and open their mouth slightly. Measure the
horizontal distance fiom the midine of the incisor surface to the center point of the philtnim in rest and with maximal smile.
6) Distance from the Cornmisure Corner of the Mouth to the Nasolabid Fold at a 45" angle. Goal: To assess the insertion placement of the gracilis muscle; symmetry of
smile. Method: Modified hand held caliper tool Landmarks: Cornmisure corner of the mouth the nasolabid fold, measure the
srnailest distance with maximal smile.
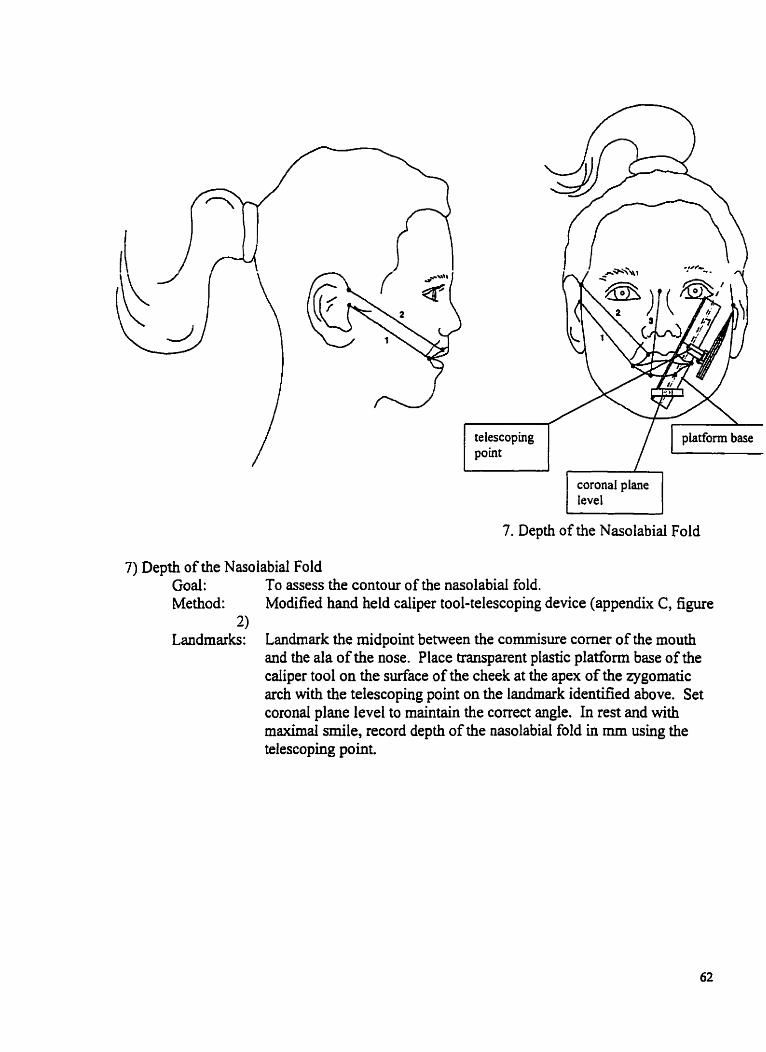
coronal plane tevel - r-l
- -
7. Depth of the Nasolabial Fold
7) Depth of the Nasolabial Fold Goal : To assess the contour of the nasolabid fold. Method: Modified hand held caliper tool-telescoping device (appendix C, figure
3) Landmarks: Landmark the midpoint between the cornmisure corner of the mouth
and the da of the nose. Place transparent plastic platform base of the caliper tool on the surface of the cheek at the apex of the zygomatic arch with the telescoping point on the landmark identified above. Set coronal plane level to maintain the correct angle. In rest and with maximal smile, record depth of the nasolabid fold in mm using the telescoping point
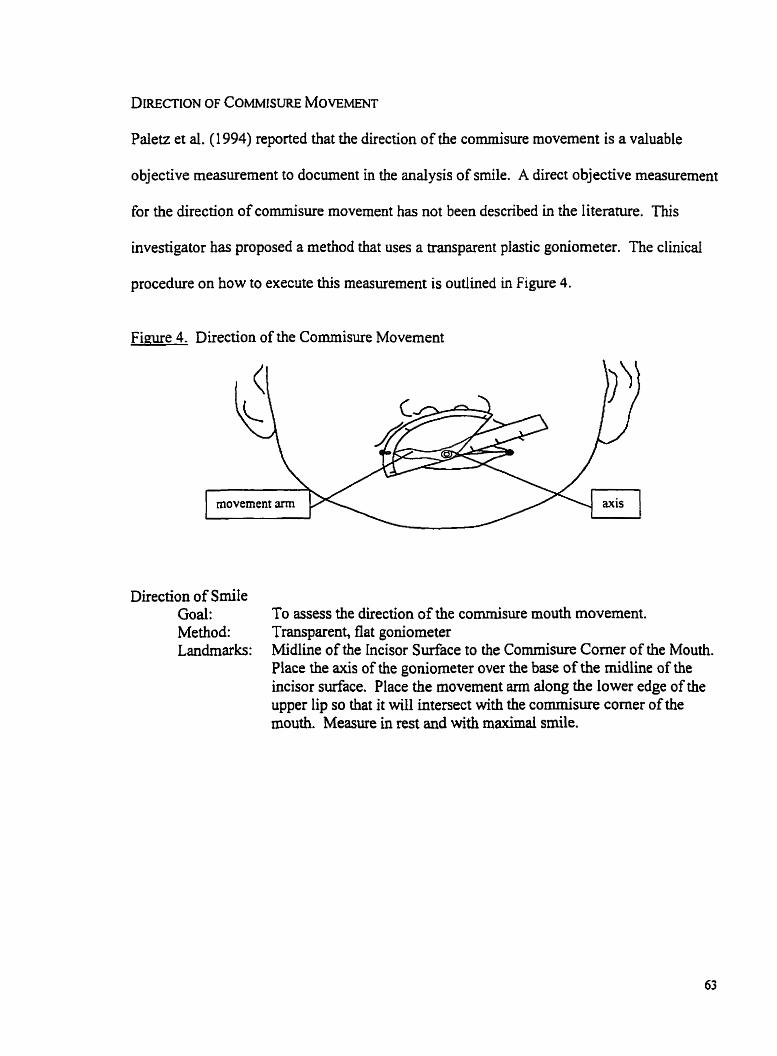
DIRECTION OF COMMISURE MOVEMENT
Paletz et al. (1 994) reported that the direction of the cornmisure movement is a valuable
objective measurement to document in the analysis of srnile. A direct objective measurement
for the direction of commisure movement has not been described in the literature. This
investigator has proposed a method that uses a transparent plastic goniorneter. The clinical
procedure on how to execute this measurement is outlined in Figure 4.
Figure 4. Direction of the Comrnisure Movement
Direction of S d e Goal: To assess the direction of the cornmisure mouth movement. Method: Transparent, flat goniorneter Landmarks: Midline of the incisor Surface to the Cornmisure Corner of the Mouth.
Place the axis of the goniometer over the base of the midline of the incisor surface. Place the movement arm dong the lower edge of the upper lip so that it will intersect with the commisure corner of the mouth. Measure in rest and with maximal smile.
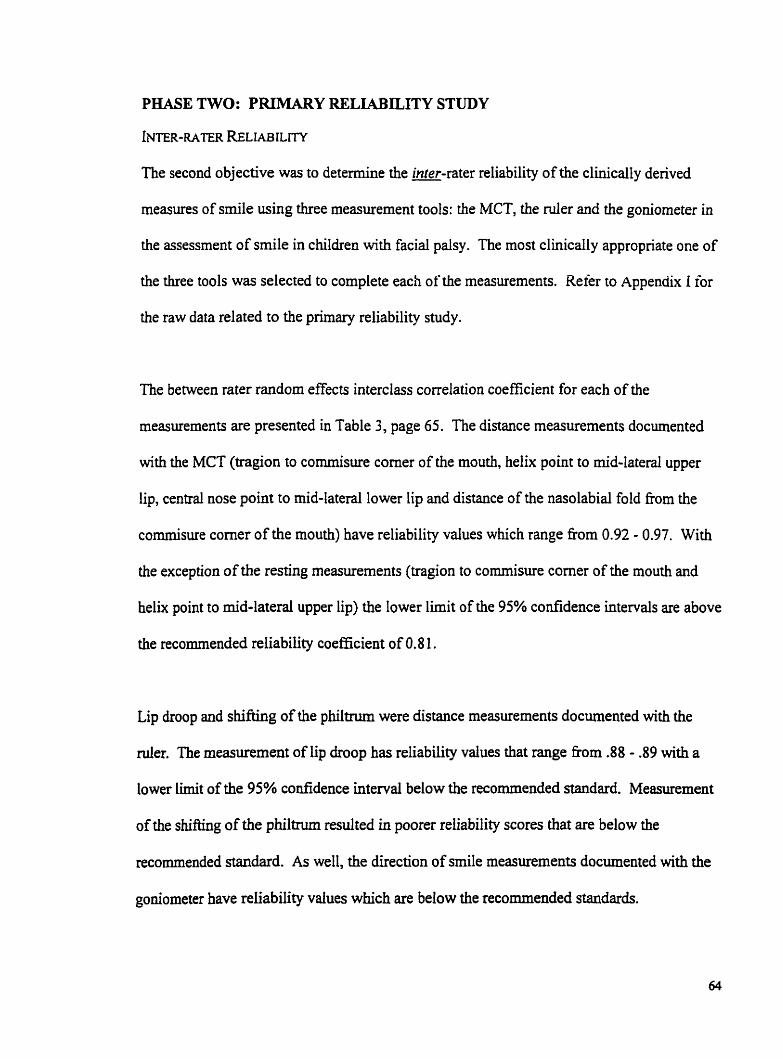
PHASE TWO: PRIRlARY RELIABILITY STUDY
INTER-RATER RELIAB ILITY
The second objective was to determine the inter-rater reliability of the clinically derived
measures of srnile using k e measurement took: the MCT, the d e r and the goniorneter in
the assessment of srnile in children with facial palsy. The most clinically appropriate one of
the three tools was selected to complete each of* the measurements. Refer to AppendUt I for
the raw data related to the prllnary reliability study.
The between rater random effects interclass conelation coefficient for each of the
measurements are presented in Table 3, page 65. The distance measurements documented
with the MCT (tragion to commisure corner of the mouth, helix point to mid-laterai upper
lip, central nose point to nid-lateral lower lip and distance of the nasolabial fold fiom the
commisure comer of the mouth) have reliability values which range fiom 0.92 - 0.97. With
the exception of the resting measurements (tragion to commisure comer of the mouth and
helk point to mid-lateral upper Iip) the lower limit of the 95% confidence intervals are above
the recommended reliability coefficient of 0.8 1.
Lip droop and shifting of the philtnim were distance measurements documented with the
der . The measurement of fip droop has reliability values that range fiom .88 - .89 with a
lower limit of the 95% confidence interval below the recommended standard. Measurement
of the shifting of the philûum redted in poorer reliability scores that are below the
recommended standard. As well, the direction of srnile measurements documented with the
goniorneter have reliability values which are below the recornmended standards.
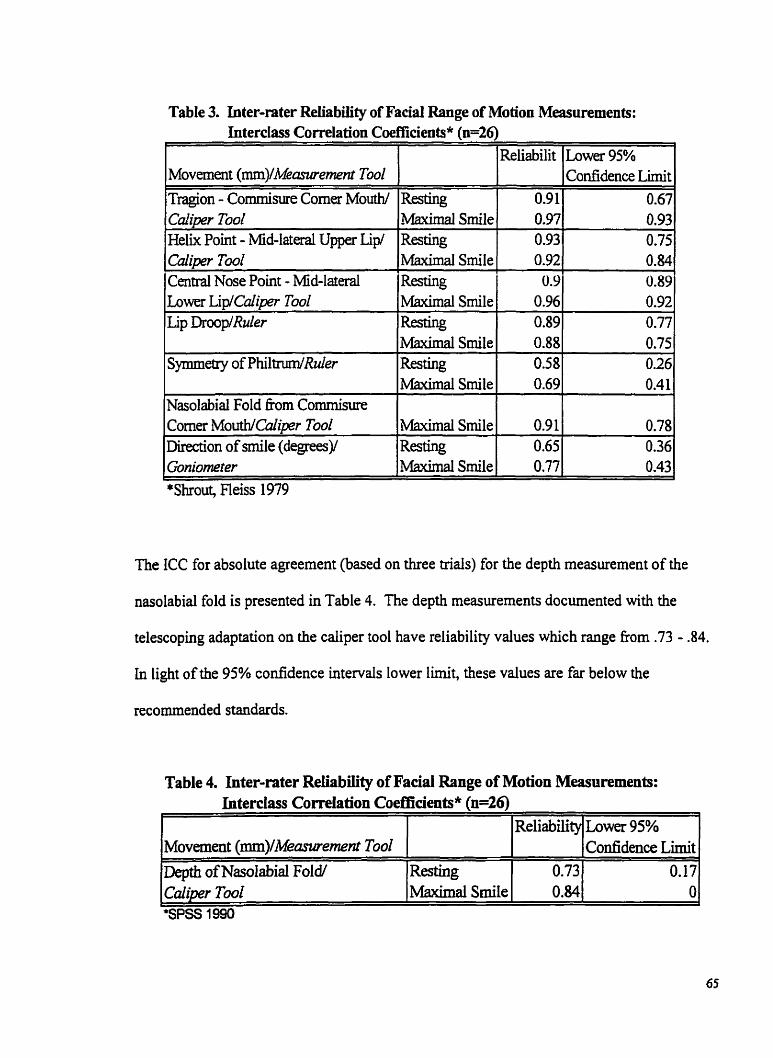
Table 3. Inter-rater Reliability of Facial Range of Motion Measurements: Interclass Correlation Cd~cients* h=26)
The ICC for absolute agreement (based on three ûials) for the depth measurement of the
C
Movment (mm)/Measzirement Tool
Tragion - Commisure Corner Mouth/ Caliper T d Heik Point - Mid-lataal Upper Lip/ C d i p Tu02 Central Nose Point - Mid-lateral hwer LiplCaliper Toul Lip DrooplRuler
Symmetry ofPhiltrum/Ruler
Nasolabid Fold f?om Cornmisure Corner MouthlC'iper Tool Direction of &le (degreesy Gonimeter
nasolabid fold is presented in Table 4. The depth measurements documented with the
telescoping adaptation on the caliper tool have reliability values which range fkom .73 - 34.
*Shrout, Fleiss 1979
Resting Maximal Smile
Resting Maximai Srnile Resting Maximai Smile ReSting Maximal Smile Resting MPùmal Smile
Maximal Smile Resting
,Maximal Smile
In light of the 95% confidence intervals lower limit, these values are far below the
recommended standards.
Reliabilit
0.9 1 0.97 0.93 0.92 0.9 0.96 0.89 0.88 OS8 0.69
0.9 1 0.65 0.77
h w e r 95% Confidence T.imit
0.67 0.93
I
0.75 0.84 0.89 0.92 0.77 0.75 0.26 0.4 1
0.78 0.36 0.43
Table 4. Inter-rater Reliability of Facial Range of Motion Measnrements: Interclas Correlation Coefficients* (n=26)
f
Lower 95% Confidence Lirnit
0.17 O
Reliability
0.73 0.84
Movement (mm)lMeanaement Tool Depth of Nasdabial FoW C d i m Tool
Resting Maximal S d e
PHASE THREE: FOLLOW-UIP RELIABILITY STUDY
In view of the poor reliability results in phase two, four of the facial measurements required
refinement. These included: lip droop, s h i h g of the philtmm, depth of the nasolabid fold
and direction of smile. Phase three of this investigation outhes the methodology for the
follow-up inter-rater reliability study.
CONTENT VALIDITY
Facial Landmarks and Distance Measurements
In the evaluation of lip droop this investigator considered revising the facial landmarks to
reflect a distance measurement from the central nose point to the cornmisure corner of the
mouth. As a resuit the MCT could be used to measure this distance. With this anaiysis, the
reliability may improve yet the assessrnent of the negative displacement of the lip droop kom
the horizontal line is not documented. Consequentiy the clinical relevance of this
measurement would be lost. No alternative measurement was tested in this study.
To assess the symmetry of the philtnim the landmarks were revised to retlect the previous
work of Frey et ai. (1994). This group of investigaton determined that the symmetry of the
philtrum was bea evaiuated by measuring the distance from the tragus (tragion) to the
philtnim. As a result of this modification the MCT could then be used to document this
distance (see Figure 5, page 67).
In codta t ion with Dr. Manktelow and Dr. Zuker (personal communication, 2000) the
laadmark for the nasolabid fold needed to be closer to the commisure corner of the mouth in
order to capture the greatest depth of the nasolabid fold. The distance between the da and
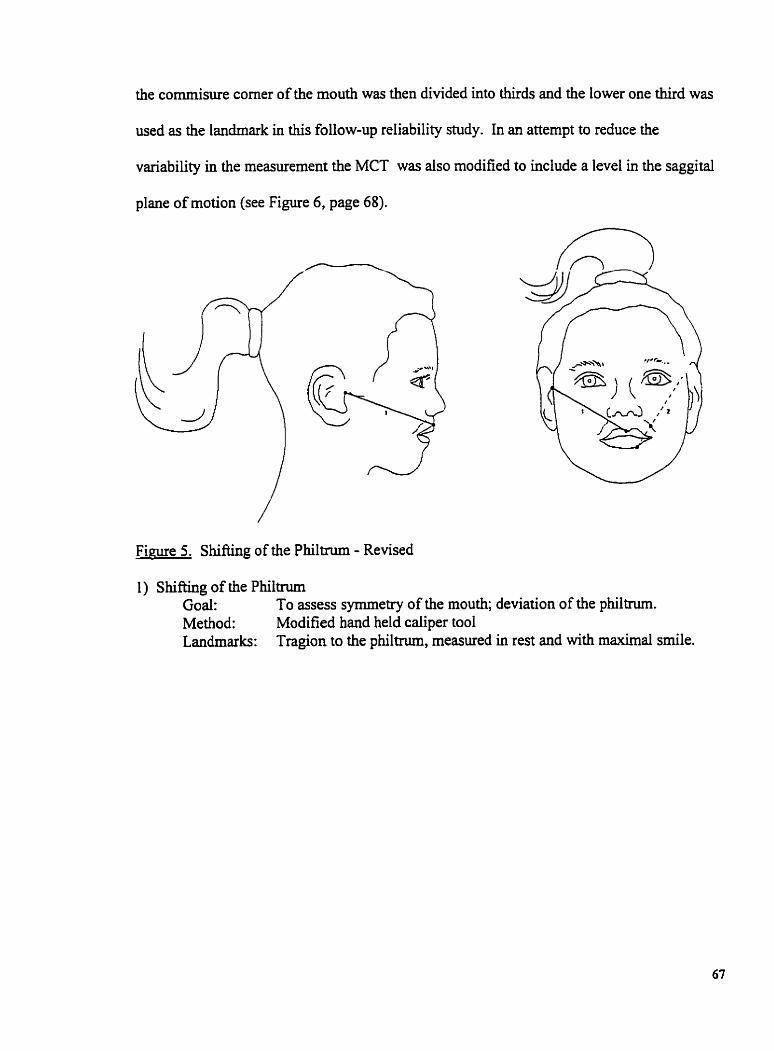
the cornmisure corner of the mouth was then divided into thirds and the lower one third was
used as the landmark in this follow-up reliability shidy. In an attempt to reduce the
variability in the measurement the MCT was aiso modified to include a level in the saggital
plane of motion (see Figure 6 , page 68).
Fime 5. Shifting of the Philtrum - Revised
1) Shifting of the Phiitnun Goal: To assess symmetry of the mouth; deviation of the philûum. Method: Modified hand held caliper tool Landmarks Tragion to the philtrum, measured in rest and with maximal smile.
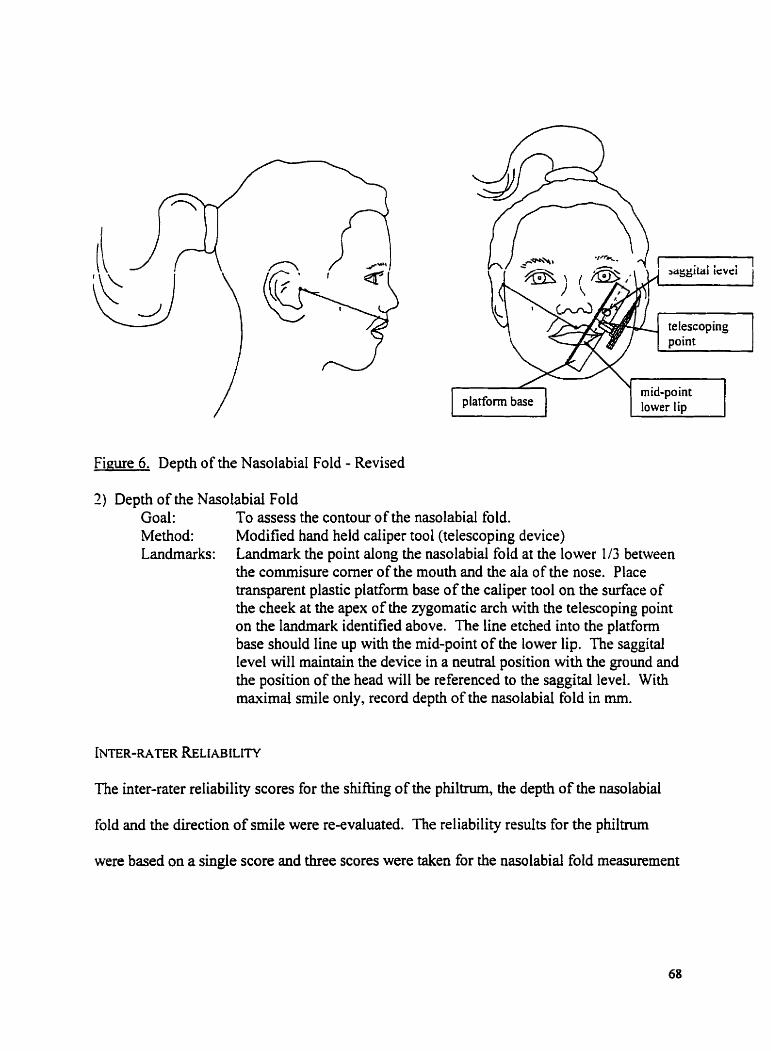
Fiwe 6. Depth of the Nasolabial Fold - Revised
2) Depth of the Nasolabial Fold Goal: To assess the contour of the nasolabial fold. Method: Modified hand held caliper tool (telescoping device) Landrnarks: Landmark the point dong the nasolabiai fold at the lower l/3 between
the cornmisure corner of the mouth and the d a of the nose. Place transparent plastic platform base of the caliper tool on the surface of the cheek at the apex of the zygomatic arch with the telescoping point on the landmark identified above. The line etched into the platform base should line up with the mid-point of the lower lip. The saggital Ievel will maintain the device in a neutrai position with the ground and the position of the head will be referenced to the saggital level. With maximal srnile only, record depth of the nasolabiai fold in mm.
The inter-rater reliability scores for the shifang of the philtnim, the depth of the nasolabial
fold and the direction of smile were re-evaluated. The reliability results for the philtnim
were based on a single score and three scores were taken for the nasolabid fold measurement
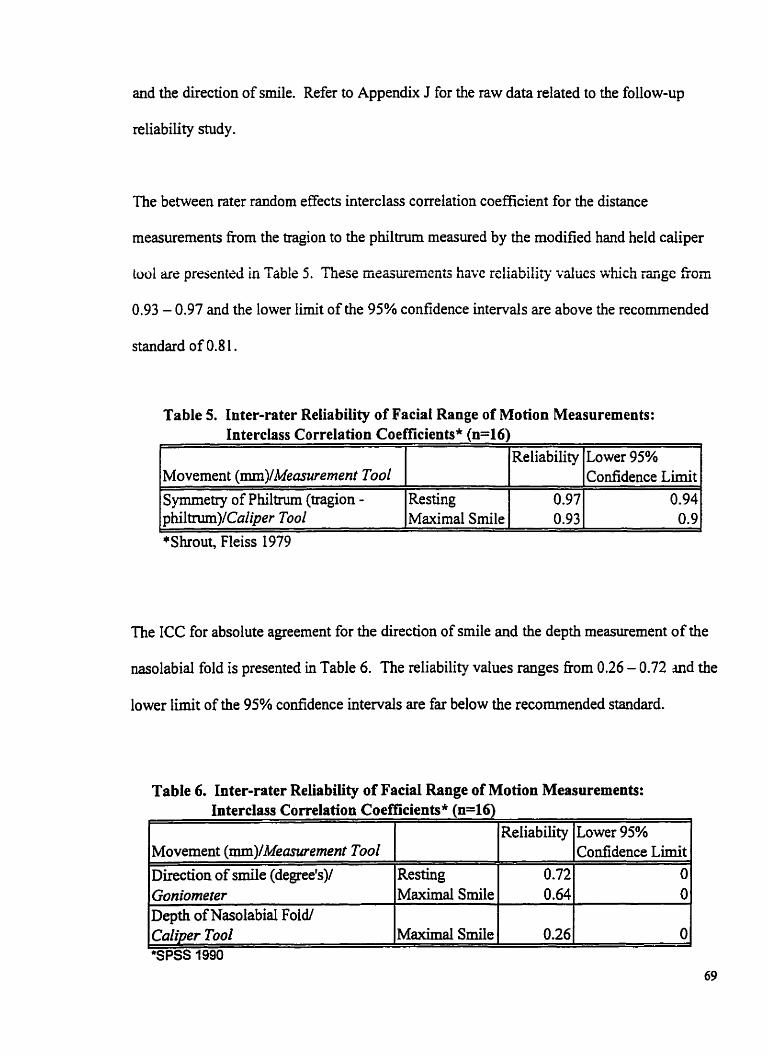
and the direction of smile. Refer to Appendix J for the niw data related to the foliow-up
reliability study.
The between rater random effects interclass correlation coefficient for the distance
measurements fiom the tragion to the philtrum measured by the modified hand held caliper
toul are presentzd in Table 5. Thzse measurements have icliability ~alucs ivhich =ge h m
0.93 - 0.97 and the lower Iimit of the 95% confidence intervals are above the recornmended
standard of 0.8 1 .
Table 5. Inter-rater Reliability of Faciai Range of Motion Measurements: Interclass Correlation Coefficients* (1146)
The ICC for absolute agreement for the direction of srnile and the depth measurement of the
nasolabid fold is presented in Table 6. The reliability values ranges kom 0.26 - 0.72 and the
lower Iimit of the 95% confidence intervals are far below the recommended standard.
Movement (mm)lMeasurernent Tool Symmetry of Philtrum (tragion - philtnim)/CuZiper Tool
Table 6. Inter-rater Reliabüity of Facial Range of Motion Measuremeats: Interclass Correlation Coefficients* (n=16)
L
*Shrout, Fleiss 1979
Resting Maximal Smile
1 1 (Reliability ILower 95% 1
Reliability
0.97 0.93
Lower 95% Confidence Limit
0.94 0.9
Movement (mm)/Meawement Tool Direction of smile (degreefs)/
l~aliper Tool 1 ~aximal Smile 1 0.26 1 01 "SPSS 7990
Goniorneter Depth of Nasolabid Foldf
Resting Maximal SrniIe
0.72 Confidence Lirnit
I
O 0.64 O
DISCUSSION
The primary purpose of this study was to develop a valid and reliable assessment that would
mesure the range of movement for smile in children with facial palsy. An extensive
literature review and consultation with experts within the field has delineated the clinically
appropriate parameters for the ROM assessment of srnile and has established the content
validity of these measurements. The incer-racer reliabiiiry oirhe faciai ROM assessment was
dso investigated. For the purposes of this discussion al1 three phases of this investigation
will be considered concurrently.
DEVELOPMENT OF THE ASSESSMENT
Validity is an important aspect to consider when choosing and developing a measure. This
psychometric property refers to the suitability of a measure and of the inferences that cm be
made from the scores (Cole, Finch, Gowland, & Mayo, 1994). in fact, Silva (1993, p. 63)
believes that the reliability of a measure is dependent on it's vaiidity, the score that is the
moa reliable is one that accurately reflects the attribute of interest. Unfominately, validity
cm never be proven; it is only esùmated and not measured directly (Law, 1987). This
process is continuou and evidence increases the more the instrument is used and studied
(Duan, 1989).
This investigation addressed the content validity of the ROM assessment of smile. The
parameters of the evaiuation and the selection of instruments were detennined through an
extensive iiterahue review and consultation with expert clinicai opinions. It was concluded
h t in the ROM assessment of smile one must consider the identification of pertinent facal
l ~ d m a r h (Paletz et al. 1994; Frey et ai. 1994), the distance m e w e m e n t s , @unes, l986a;
Paietz et al. 1994; Frey et al. 1994) and the direction of movement (Paletz et al. 1994).
Several of the investigators of facial measurement agree bat the most consistent movement
is smiling with the maximal showing of teeth (Burres, 1985; Frey et ai. 1994; Neely et al.
1996; Johnson et al. 1994; Trotman et al. 1997).
Dr. Manktelow, Dr. Zuker and an Occupational Therapist who used the ROM assessment
clinically perfonned an informa1 qualitative review of the facial ROM assessment. The
parameters of this assessment have been thoroughiy examined and are presented in the
results section of this thesis. As well, the methods of measurement and protocol for
measurement were determined to be appropriate to answer the objectives of this assessment.
INTER-RATER RELIABILITY
The inter-rater reliability was evaluated by using the ICC. The advantages to using the ICC
is that it can assess the reliability among two or more rating, the analysis does not require the
same number of raters for each subject and most importantly the ICC supports the
generalizability model. The generalizability model recognizes that differences between
observed scores are due to a variety of factors not just tme variance and random error
(Portney & Wakins, 1993, p. 509-5 10). For example, in this investigation the ICC accounts
for the variances between the raters, the subjects, and error.
nie disadvantages in using the ICC are two fold. The fint consideration is that the reliability
coefficient is based on an average correlation across raters. Consequently, if the ICC is low
and the variance between the raters is high, the individual variance of the raters c m o t be
determined. A follow-up inna-rater reliability study would be necessary to discem the
variability of the individuai raters.
The second concem in utilizing the ICC relates to the actual study sample. When evaiuating
a reliability study it is important to consider the characteristics of the study sample. The pre-
requisite for a good reiiabiiity study is a sample with a wide range of scores, for as the total
mie variance increases the error component will account for a smaller proportion and
reliability will improve (Portney & Watkins, 1993, p. 508). In this investigation the sample
in the primary reliability study was comprised of children who presented with facial paisy
and the raw data collected represented a wide range of possible scores. The follow-up
sample was drawn fkom the nomal addt population. The range of raw scores in the addt
sample were less variable and this may have been a factor in the poor reliability resuits.
This investigation delineated four research hypotheses each relating to the reliability of the
proposed facial ROM assessment. At this point each hypothesis will be reviewed and the
interpretation for the current results discussed.
Hypothesis One
In ench location, there is an alrnost per-ct relationship (81 - 1.0) b e ~ e e n the ratings of two
observers on the distance measurements in the assessment of smile when using the modijed
hand held caliper too l.
The MCT is a reliable assessment tooi for the measurement of facial distances. Of the nine
distances measurements assessed in this investigation there were three exceptions to this
statement. It is not clea. as to the discrepancy in two resting measurements that indicated a
low reliability: the tragion to the commisure corner of the mouth (lower limit .67) and the
helix point to the mid-lateral upper lip (lower limit .75). The same two measurements
indicate a high reliability in the maximal smile position denoting adequate assessment
technique. Variability in the subject resting positions is not a typical h d i n g and this is more
likely to occur with movement. It is possible that one of the raters measured to the incorrect
landmark on a few of the subjects, for example fiom the tragion to the mid-lateral upper lip
and this could account for the less than desirabIe results.
A low reliability was also docurnented in the distance measurement of the commisure corner
of the mouth to the nasolabial fold (lower limit .78). The majority of variance was fiom
between the subjects and secondly from error. In children who present with an abnormal
nasolabial fold it cm be difficuït to determine at what point the fold begins moreover there
cm acnially be an absence of the fold. This factor may increase the error component in the
variance. Another element to consider is the statistical power used in this investigation.
With the statistical power set at 80% it is expected that 20% of the scores will not f d with in
the desked range of .8 1 or above. Consequently, these findings maybe more of a result
regarding statistical power than with an achial deficiency in the measurement system.
The remainder of the distance measurements do present with reasonable ICC's. With a lower
limit of the 95% confidence intelvals of .84 or greater one cm conclude that the differences
between measurements on diffèrent subjects primarily represent subject to subject
differences. The landmarks chosen for these measurements were well defïned and there was
a wide range of scores within the raw data. The caliper tool is able to measure to a tenth of a
millimeter dlowing for a more accurate measurement of distance. Through the ANOVA the
majority of variance was fiom between the subjects and secondly from error. Although
smiling with maximal teeth showing has been detemiined to be the most consistent
movement this may account for a degree of the variability between subjects.
Of al1 the direct measurement systems reviewed in this thesis none have reported on the
reliability of the measure. As previously discussed Ross et al. (1 99 1) reported on the inna-
rater reliability of linear measurements assessed with a caliper tool. An ICC of -98
demonstrated substantial infra-rater reliability with a lower 95% confidence limit of .96.
Inter-rater reliability was not evaluated in the investigation therefore a direct cornparison to
the cunent study cannot be made.
With the exception of two resting meanirements and the distance fkom the cornmisure corner
of the mouth to the nasolabid fold, there is evidence to conclude that there is an dmost
perfect relationship between the ratings of two observers on the distance measurernents in the
assessment of srnile when using the MCT.
Hypothesis Two
In each location there is a substantial relationship (. 61 - .80) between the ratings of two
observers on the distance measuremenrs in the assessment of'smile when using the d e r .
Two distance measurements were evaluated with the d e r : lip droop and shifüng of the
philtnun. The measurements for lip droop presented with reasonable ICC's and lower limit
confidence intervals for this hypothesis, although the reliability is below the recommended
standard of. 8 1 . Again, these maybe as a result of the statisticai power rather than limitations
in the measurernent tool. The reliability of measurements for shifting of the philtnim were
poor, and below the recommend standard of .8 1. Based on the ANOVA, the majority of
variance was fiom between the subjects and secondly h m error. Linear meanirements are
inherently variable and continue to be a limiting factor. The landmarks chosen for these
measurements were well defined but there was a small range of scores in the raw daîa
therefore the error component accounted for a larger proportion and reliability decreased.
These two movements were technicdy more difficult to measure for example, the distances
were mal1 and the horizontal line for lip droop required visualization on the part of the rater.
As well the d e r is not as fine a meamernent tool and may be less accunite than the caliper
tool. Al1 of these factors wiIl increase the error component in the variance.
Frey et al. (1994) recommended that the distance measurement from the tragus (tragion) to
the philtnim be used the document symmetry of the philtrum. In the follow-up study
excellent results were obtained ushg the MCT and a lower 95% confidence i h i t of -90 was
achieved. The rationde for these resdts have been discussed within the hrst hypothesis.
In the measurement of lip droop there is evidence to conclude there is a substantial
relationship between the ratings of two observers on the distance measurements in the
assessment of smile when using the d e r . Although, the reliability obtained is below the
recommended standard of .8 1. in the measurement of the shifting of the philtnim there is
evidence to conclude that there is a less than a substantid relationship between the ratings of
two observers on the distance measurements in the assessment of srnile when using the d e r .
Hpothesis Three
For each memurernent there is a substantial relutionship (. 61 - .80) between the ratings of
two observers on the direction measurements in the assessment of smile when using the
goniorneter.
The ICC's for the direction of the cornmisure movement were substantial in both studies but
the lower limit 95% confidence level was very low indicating poor reliability with this
measurement. Based on the ANOVA, the major@ of variance was fiom between the
subjects and secondly fiom the error. The landmarks chosen for this measurement were well
defined but there was a s m d range of scores in the raw data. Therefore, the error component
accounted for a larger proportion of the variance and reliability decreased. As well, this
facial measurement is inherentiy variable and the goniometer is not as fine a measurement
tool. Ail of these factors will increase the error component of the variance.
The direction of commisure movement does have clinical importance in the assessrnent of
smile therefore an attempt was made to improve its reliability. When rneasurements are
unstable it may be necessary to take a mean of several scores and use the mean of repeated
independent measures to obtain a satisfactory reliability. This has the effect of increasing the
reliability due to the fact that mean scores are considered better estimates of tnie scores,
thereby reducing the error variance (Portney & Watkins, 1 993, p. 5 1 1). In the follow-up
study the direction of the cornmisure movement was evduated again and an average of three
scores was taken. The ICC's obtained were comparable with the primary study yet the lower
level confidence limit was very poor. The low reliability scores may in part be due to the
fact that the subjects in the second study were fiom a homogenous sample with limited
variability (Pormey & Watkins, 1993, p. 508).
The evaluation of the direction of the commisure movement presented with several negative
factors. As a result there is no evidence to conclude that there is a substantial relationship
between the ratings of two observers on the direction rneasurements in the assessment of
smile when using the goniometer.
Hypothesis Four
For each rnemrement there is a substantial relatiomhip 661 - -80) beiween the ratings of
two observers on the depth rneanaemenis in the assessment of smile when using the modified
hand held caliper tool.
The ICC's for the depth of the nasolabid fold measurements were initially substantid in both
studies yet the lower Iimit 95% confidence level was consistently low indicating poor
reliability with this measurement. Based on the ANOVA, the majority of variance was fiom
between the raters and secondly from between the subjects. EEorts to improve the reliability
of this measurernent were made; for example, landmark identification, modification to the
measurement tool and calculation of the ICC's using the mean of repeated independent
measures. In the follow-up study a saggital level was added to the device in order to
maintain the position of the instrument parallel to the ground. As well, the head was held in
a stable position in relation the caliper tool. The caliper tool was still able to rock on the
surface of the cheek thereby decreasing or increasing the distance between the tool and the
landmark on the nasolabid fold. As a result this increase in the variance between raters.
Despite these corrections this measurement remained technicaily difficult to record. Other
factors such as the small range of movement and the homogenous sarnple in the second study
will negatively impact on the reliability of this measurement.
In spite of the attempts to improve the testing procedures, the testing hsmiment and the
statistical analysis there continued to be several negative factors intluencing the reliability of
this measurernent, As a result there is no evidence to conclude that there is a substantial
relationship between the ratings of two observers on the depth meannements in the
assessrnent of s d e when using the MCT.
In summary, this investigation has identified the important parameters to measure in the
ROM assessment of smile and has established the content validity of the assessment. The
inter-rater reliability of the facial ROM assessment was evaluated and the MCT appears to be
reasonably constant in the documentation of distance measurements in the assessment of
smile.
CONTRIBUTIONS OF THIS THESIS
Based on previous investigations and expert opinion this current research study proposed
four new facial landmarks and fifteen new distance measurements in the evaluation of facial
ROM. The methodology for seven of the rneasurements presented were exclusive to this
study and are as follows: lip droop, the depth of the nasolabid fold, the direction of srnile
(resting and maximal smile) and the distance of the nasal-labial fold fiom the commisure
corner of the mouth (maximal smile).
Rigorous reliability testing of direct measurement techniques have not been presented in the
facial movement literature and in order for an instrument to be useful in the clinical
environment proven inter-rater reliability is a necessary component. This research study
assessed the inter-rater reliability of the proposed facial ROM assessment using three
measurernent tools. The resdts of this investigation clearly indicate that the MCT presents
with the highest reliability. As well, one of the new landmarks: helix point; and four of the
distance measurements: tragion to cornmisure corner of the mouth (maximal smile), helk
point to mid-lateml upper lip (maximal smüe), and tragion to philtmm (resting and maximal
smile) are the measurement parameters that support a reliability above the recommend
standards of. 8 1.
Facial motion is complex and difficult to measure in a way that is reproducible. The
assessment of lip droop, the direction of commisure movement and the distance of the
nasolabial fold fiom commisure corner of the mouth were not reliable yet continue to be
important characteristics to measure in the assessment of srnile. These measurements
continue to require refinement in order to improve their reliability. An attempt was made to
objectively measure the depth of the nasolabid fold, but this was also proven to be
unreliable. Reliability of these measurements may be improved through more ngorous land
marking and testing procedure, intensive rater training, and perhaps a superior measurement
tool.
A unique and important feature of this investigation was that the initial study sample
consisted entirely of children with facial palsy. Furthemore, the children were able to
comply with the testing procedures and did not appear to find the instruments intimidating.
The raten reported the MCT was easy to use and the assessment was quick to admuiiner.
LIMITATIONS
Throughout this research snidy every effort was made to ensure a sound scientific approach.
Despite the established research protocol some methodological limitations did occur which
may have effected the intemal and extemal validity of this study.
The intemal validity of the reiiability study may have improved if the raters were evaluated
on the assessment techniques following the training period. An evaluation by an independent
assessor wouid ensure the consistency between the raters. As wel1, facial movement is
innately variable and despite the efforts to implement a standardized protocol this variability
may have negatively irnpacted on the reliability results. Another threat to the intemal
validity of this study was the decision to limit the amount of testing to which the children
were exposed and to calculate the reliability of several measurements based on a single score.
From a statistical perspective this may have had a negative impact on the reliability of the
measmement for mean scores are consiciered better esGmotzs of tniz scorzs (I>ortney $
Watkins, 1993, p. 5 1 1).
The follow-up reliability study used a convenience sample of normal adult subjects. Due to
the fact that the subjects presented with no facial asymmetry, expectation bias may have
influenced the rater's scores. The results obtained from the follow-up reliability study may
not be generalizable to the target population of children with facial palsy.
FUTURE DIrnCTION
The empincal investigations regarding objective measwement of facial ROM are in their
infancy stages of development. To capture the smaller facial movements such as Iip droop,
direction of smile and facial contours the community of researchers need to continue to
perfect the computer analysis of facial movement. Computer analysis needs to become cost
effective and less complex so that it can be used in the clinical setting and be acceptable to
c hildren.
The MCT does have cIinical value as an assessrnent tool for facial ROM and further
reliability midies are warranted. Streiner and Norman (1 995, p. 1 14) recommend that if the
inter-rater reliability is low it maybe necessary to continue with an inûa-rater reliability shidy
in order to determine the source of unreliability; for example, between the raters, within the
raters or both. As well, it is also necessary to test the sensitivity of this rneasurement tool to
record clinically important changes. A reliability study to assess the responsiveness of this
facial ROM assessment is a fundamental step in the development of this assessrnent.
Despite the adequate reiiabiliv of this motor assessment of smile for ciinical activities, in
order to assist in the surgical decision rnaking for children with facial palsy a highly reliable
instrument is required. An ICC with a point estimate of .99 with the lower 95% confidence
lirnit set at .96 indicates minimal variability in the rneasurement and would be preferred.
This high reliability may be achieved with the MCT by using the same rater, or an alternate
assessrnent tool may prove to be the method of choice; for example, cornputer analysis.
The limitations in facial ROM is only one aspect that may effect the overall function in
children who present with facial palsy. The research literature to date focuses on the clinical
outcornes of adults with face nerve palsy and very little has been devoted to children.
Clearly it is important to research and publish on the fûnctional implication impairment in
smile has on children who present with facial palsy. More specifically to assess the impact
of a facial impairment on ones self-perception and ability to participate in the tasks of daily
living.
CONCLUSIONS
The predominant request fiom children who present with facial palsy is to be able to srnile
and with new surgical techniques this wish has become a reality. Ordinal grading systems
are not sensitive enough to document the detailed functional changes that occur as a result of
these interventions and the few compter systems in use may be of benefit in an adult
research setting.
The results of this investigation have produced an adequate ROM assessment that will
reliably measure most of the important motor components of m i l e in the clinical setting:
commisure rnovement, upper lip movement, symmetry of the upper and lower lips and
symmetry of the philtrum. To document the changes in the nasolabial fold a descriptive
classification has been proposed. Although there is a significant amount of research to be
done in this area this study has provided therapists with a basic facial ROM assessment that
is inexpensive, acceptable to children and can be used in the clhical setthg (Table 7, page
84).
The assessment of lip droop, the direction of commisure movement and the distance of the
nasolabial fold fiom commisure corner of the rnouth were not reliable yet continue to be
important characteristics to measure in the assessrnent of srnile and will benefit fiom M e r
investigations.
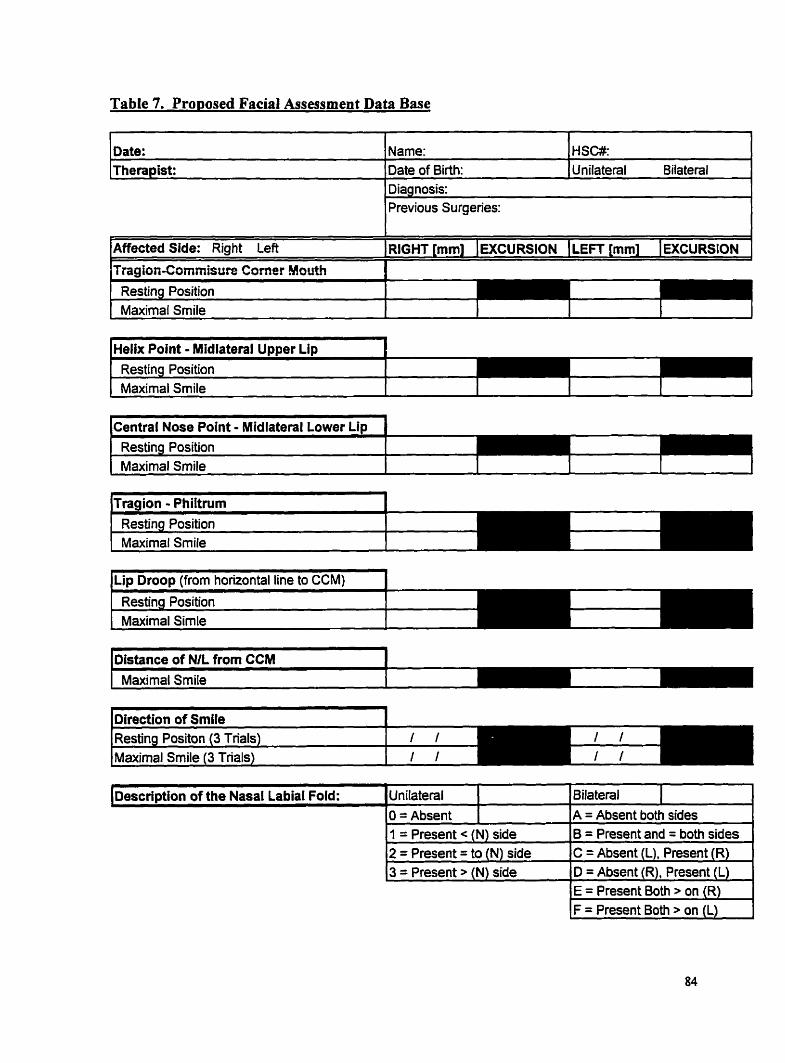
Table 7. Pro~osed Facial Assessrnent Data Base
l Previous Surgeries:
Date: Therapist:
Affected Side: Right Left IRIGHT [mm] IEXCURSION (LEFT [mm] IEXCURSION 1 I
Resting Position 1 r
Name: Date of Birth:
1 Maximal Smile 1 1 1 1
HSW Unilateral Bilateral
l ~ e l i x Point - Midlateral U ~ p e r Lin 1
1 Maximal Srnile 1 1 1 1 1 - - - - --
(central Nose Point -
1 Maximal Smile 1 1 1 1 1
Resting Position Maximal Smile
IL~D D r o o ~ (from horizontal line to CCM) 1 . . Resting Position Maximal Simle
kMance of NIL from CCM 1 - - l
Maximal SmiIe 1
Direction of Smile Resting Positon (3 Trials)
1 ~aximal Smile (3 Trials) fil
Bilateral 1 A = Absent both sides
Description of the Nasal Labial Ford:
1 = Present c (N) side 2 = Present = to (N) side 3 = Present > (N) side
Unilateral O = Absent
B = ~resent and = both sides C = Absent (L), Present (R) O = Absent (R), Present (L) E = Present Both > on (R) F = Present Both > on (L)
REFERENCE LIST
Bajaj-Luthra, A., Mueller, T., & Johnson, P.C. (1997). Quantitative analysis of facial
motion components: Anatomic and nonanatomic motion in normal persons and in
patients with complete facial paralysis. Plastic and Reconstnictive Surgerv. 99(7),
1 894-1 902.
Benson, J., & Clarke, F. (1982). A guide for instrument development and validation.
Amencan Journal of Occupational Therapy, 36(12), 789-800.
Brackrnm, D.E., & Bam, D.M. (1984). Assessing recovery of facial b c t i o n following
acoustic neuroma surgery. Otolarniaoloq Head and Neck Sur~erv, 92(88), 88-93.
Burns, N., & Grove, S. (1 997). The ~ractice of nuninc! research: conduct critique &
utilization. (3rd ed.). Philadelphia, Pennsylvania: W.B . Saunders Company.
Burres, S. (1985). Facial biornechanics: The standards of normal. Larvngosco~e. 95,
708-7 14.
Burres, S. (1 986a). Objective grading of facial paralysis. Annals of Otolom, Rhinolow,
and Lamieolow. 95(3 Pt 1 ), 23 8-24 1.
Burres, S., & Fisch, U. (1986b). The cornparison of facial grading systems. Arch
Otolamgolow Head and Neck Surpem 112(7), 755-758.
Cole, B., Finch, E., Gowland, C. & Mayo, N. (1994). Physical rehabilitation outcomes
measures. @p. 21 -33). Toronto: CPA, Health and Welfare Canada, and Canada
Communications Group.
decatanzaro, D.A. (1 999). Motivaton and Emotion - evolutionarv. ohvsiolopical.
dea7clo~mentd. md social ~ e s ~ e c t i r e s . Yew Jersey: Prenticc-Hal1 hc.
Donner, A., & Eliasziw, M. (1987). Sarnple size requirements for reliability studies.
Statistics in medicine. 6,44 1-448.
Dunn, W. W. (1 989). Validity. [Speciai issue: Developing nom-referenced standardized
tests]. In Miller, L.J. (Ed.) Physical and Occu~ational Theraw in Pediatrics. 9(1),
149-1 68.
Evans, R.A., Harries, M.L., Baguley, D.M., & Moffat, D.A. (1989). Reliability of the
Houe and Brachann grading system for facial palsy. Journal of Laqneolow and
Otologv. 1 O3 (1 1 ), 1 045- 1046.
Fisch, U. (1 98 1). Surgery for Bell's paisy. Archives Otolaryn~olopv, 1 07(0 1 ), 1 - 1 1.
Fleiss, J.L. (1986). The design and analysis of clinical experiments. In Reliabilitv of
measurement. @p. 1-32). New York: Wiley.
Frey, M., Jemy, A., Giovanoli, P., & Stüssi, E. (1994). Development of a new
documentation system for facial movements as a b a i s for the international registry
for neurornuscular reconstmction in the face. Plastic and Reconstructive Surgew, - -
93(7), 133491349. -
Goldberg, C., & Zuker, R. (in press). Facid reanimatiition in children uith Mocbius
syndrome using gracilis muscle transplants. Plastic and Reconstnictive Su~erv.
Hennekens, C.H., & Buring, LE. (1987). Epidemiolom in medicine. Toronto: Littie
Brown Company.
Hepner, W.R. (1 95 1). Some observations of facial paralysis in the newbom infant:
Ideology and incidence. Pediatrics. 8,494-497.
House, 1. W. (1 983). Facial nerve grading systems. Laryngoscope. 93(8), 1056-1 067.
House, J.W., & Brackmann, D.E. (1985). Facial nerve grading system. Otolanmeolo~ -
Head and Neck Suraerv. 93(2), 146- 147.
Johnson, P.C., Brown, H., Kuzon, W.M., Bailiet, R., Gaxrison, J.L., & Campbell, J.
(1994). Simultaneous quantitation of facial movements: The maximal static response
assay of facial nerve function. Annals of Plastic Surgerv. 32(2), 17 1 - 179.
Johnson, P.J., Bajaj-Luthra, A., Llull, R., & Johnson, P.C. (1997). Quantitative facial
motion analysis for hinctiond fiee muscle reanimation procedures. Plastic and
Reconstructive Sur~erv. 100(7), 1 7 10-1 7 19.
Kumar, V. (1995). Cross-face reanimation of the pardysed face, with a single stage
Law, M. (1987). Measurement in Occupational Therapy: Scientific criteria for evaluation.
Canadian Journal of Occu~ational Therapy. 54(3), 133-1 3 8.
McGraw, K.O., & Wong, S.P. (1 996). Psvchological-Methods. 1(1), 30-46.
McHugh, H.E., Sowden, KA., & Levitt, M.N. (1969). Facial paraiysis and muscle
agenesis in the newbom. Archives Otolaqmgologv. 89, 157-169.
M~rty , G.E., Diver, J.P., Kelly, P.J., OtDonoghue, G.M., & Bradley, P.J. (1 994). The
Nottingham System: Objective assessrnent of facial nerve function in the chic .
Otolamiirolo~ Head and Neck Sur~ery. 1 1 O@), 156- 16 1.
Neely, J.G., Cheung, J.Y ., Wood, M., Byers, J., & Rogerson, A. (1 992). Computenzed
quantitative dynamic andysis of facial motion in the paralyzed and synkinetis face.
The American Journal of Otologv. 1 3 (2), 97- 1 0%
Neely, J.G., Joaquin, A.H., Kohn, L.A., & Cheung, J.Y. (1996). Quantitative assessments
of the variation within grades of facial paralysis. Larvngosco~e. 1 O6(4), 438-442.
O'Brien, B.M., Pederson, W.C., Khazanchi, R.K., Momson, W.A., MacLeod, A.M., &
Kumar, V. (1 990). Results of management of facial paisy with rnicrovascuiar fiee-
inuscle tnnsfcr. Pladc and Rcconstnictive S u r ~ e n . 56(1), 12-22.
Orobello, P. (1991). Congenital and acquired facial nerve paralysis in children.
Otolarvnirolo~icai Clinics of North Amerka 24(3), 647-652.
Padwa, B.L., Evans, C.A., & Pil1emer.F.C. (1991). Psychosocial adjustment in children
with hemifacial microsornia and other craniofaciai deforrnities. Cleft Palate -
Craniofacial. 28(4), 354-359.
Paletz, J.L., Manktelow, R.T., & Chaban, R. (1994). The shape of a normal srnile:
Implications for facial paralysis reconstruction. Plastic and Reconstnictive Sur~erv,
93(4), 784-789. -
Pearson, B. W. (1 985). Editorial. Otolanm~o~ogv Head and Neck Sureery. 93 (2), 145-
145.
Pertschuk, M.J., & Whitaker, L.A. (1 985). Psychosocid adjustment and craniofacial
malformations in childhood. Plastic and Reconstnictive Surnery. 75(2), 177-1 84.
Pope, A.E., & Wood, J. (1 997). Self-perceived facial appearance and psychosocial
adjustment in preadolescents with craniofacial anomalies. Cleft Palate - Craniofacial,
3 5(5), 396-40 1. -
Portney, L.G., & Watkins, M.P. (1993). Statistical rneasure of reliability. In Foundations
of Chical Research: A~~licat ion to ~raciice. @p. 505-528). Nom&, Connecticut:
Appleton & Lange.
Rickenmann, J., Jaquenod, C., Cerenko, D., & Fisch, U. (1997). Comparative value of
facial nerve grading systems. Otolarvneoloev Head and Neck Sur~ew. 1 17(4), 322-
Ross, B.G., Fradet, G., & Nedzelski, J.M. (1 996). Development of a sensitive clinical
facial grading system. Otolaryncrolop Head and Neck Surgew. 1 14(3), 3 80-386.
Ross, B.G., Nedzelski, LM., & McLean, A. (1991). Efficacy of feedback training in long-
standing facial nerve paresis. Larvne;osco~e. 10 1 (7), 744-750.
Rubin, L.R. (1974). The anatomy of a srnile: Its importance in the treatment of facial
paralysis. Plastic and Reconstnictive Surgery. 53,384
Sassoon, E.M., Poole, M.D., & Rushworth, G. (1991). Reanimation for facial palsy using
gracilis muscle grafts. British Journal of Plastic Sur~erv. 44, 195-200.
Silva, F. (1993). Psvchometnc Foundations and Behavioural Assessment. Newbury Par:
SAGE Publications.
Smith, LM., Murray, J.A.M., Cdl, RE., & Slattery, J. (1 992). A cornparison of facial
grading systems. Chical Otolaryngolow. 17(4), 303-307.
Streiner, D.L., & Norman, G.R. (1995). Health measurernent scaies: A ~racticai mide to
their develooment and use. (second ed.). New York: Oxford University Press Inc.
Trotman, C., & Faraway, J.J. (2000). Sensitivity of a method for the analysis of facial
mobility: Interlandmark separation. C M Palate - Craniofacial. 3 5(2), 142- 153.
Trotman, C., Faraway, J.J., Silvester, KT., Greenlee, G.M., & Johnston, L.E. (1 998).
Sensitivity of a method for the analysis of facial mobility: vector of displacement.
Clefi Paiate - Craniofacial. 3 S(2), 1 32- 14 1.
Trotman, C., Stohler, C.S., & Johnston, L.E. (1 997). Measurement of facial soft tissue
rnobility in man. Clefi Palate - Craniofacial, 35(1), 16-25.
Zuker, R., & Manktelow, R.T. (1993). Functiond and aesthetic muscle transplants.
Advances in Plastic and Reconstnictive Surgew, 9? 37-66.
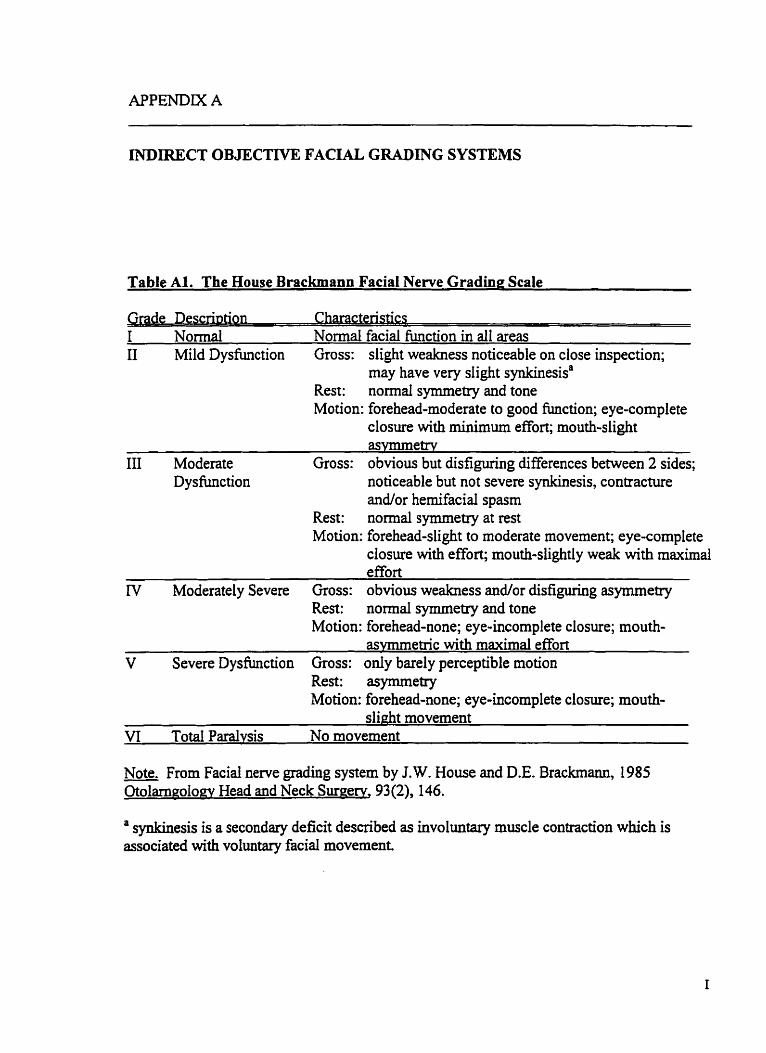
INDIRECT OBJECTIVE FACIAL GRADING SYSTEMS
Table Al. The House Brackmann Facial Nerve Grading Scale
. . non Charactemcs 1 Normal Normal facial fiinction in al1 areas II Mild Dysfunction Gross: slight weakness noticeable on close inspection;
may have very slight synkmesisa Rest: normal symmeîxy and tone Motion: forehead-moderate to good function; eye-complete
closure with minimum effort; mouth-slight asvmmetrv
III Moderate Gross: obvious but disfiguring differences between 2 sides; noticeable but not severe synkmesis, contracture andor hernifacial spasm
Rest: normal symmetry at rest Motion: forehead-slight to moderate movement; eye-complete
closure with effort; mouth-slightly weak with maximal effort
N Moderately Severe Gross: obvious weakness andior disfiguring asymmetry Rest: normal symrnetry and tone Motion: forehead-none; eye-incomplete closure; mouth-
asvmmetric with maximal effort V Severe Dysfunction Gross: only barely perceptible motion
Rest: asymmetry Motion: forehead-none; eye-incomplete closure; mouth-
s k h t movement VI Total Paralysis No niovement
Note. From Facial nerve grading system by J.W. House and D.E. Brackmann, 1985 Otolarnnoloev Head and Neck Surgerv, 93(2), 146.
a synkinesis is a secondary deficit described as involuntary muscle contraction which is associated with vo1untary facial movernent.
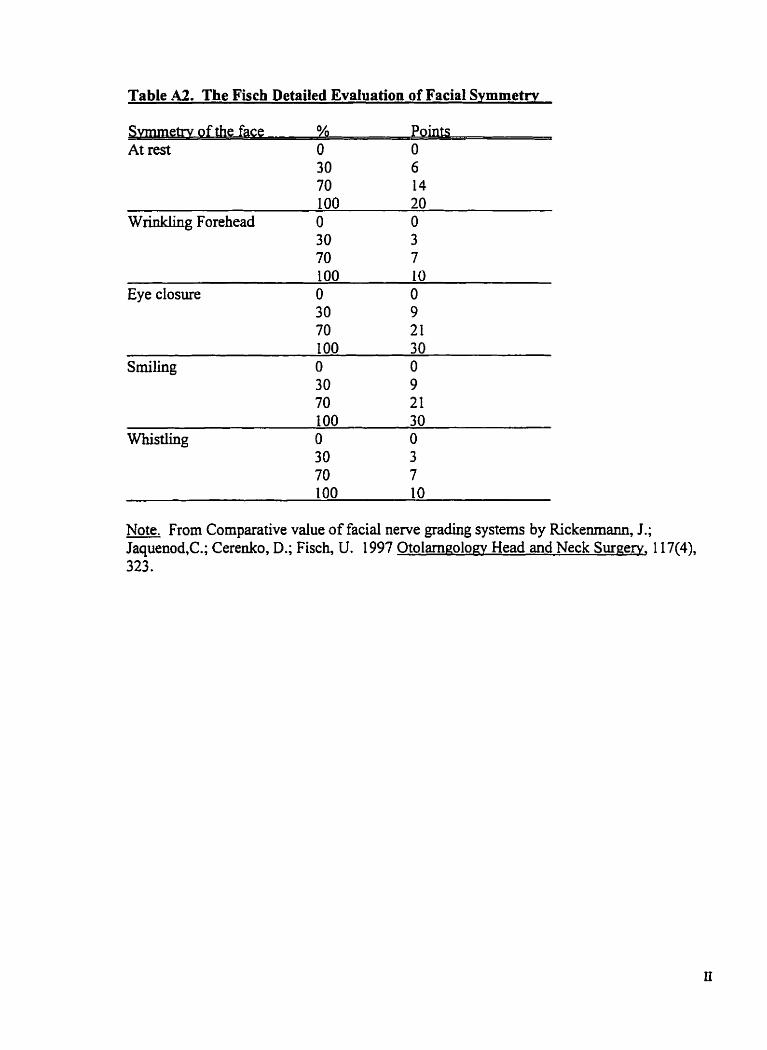
Table A2. The Fisch Detailed EvaIuation of Facial S v r n m e t ~
etry of the face Points At rest O O
30 6 70 14
Wrinkling Forehead O O 30 3 70 7
Eye closure
Note. From Comparative value of facial nerve grading systems by Rickenrnann, J.; Jaquenod,C.; Cerenko, D.; Fisch, U. 1997 Otolmnolow Head and Neck Suroerv, 1 17(4), 323.
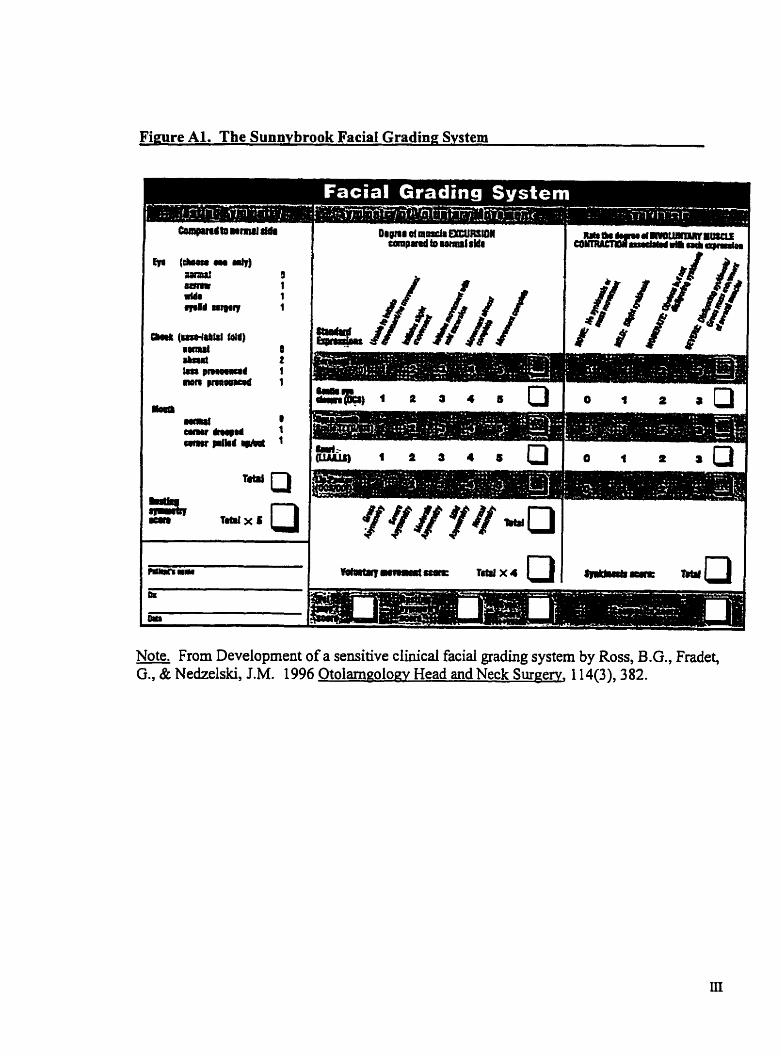
Fimre Al. The Sunnybrook Facial gradin^ Svstem
-- -- I"&.( 2 J 4 6 Q I * 1 t i [ 7
Note. From Development of a sensitive dinicd facial grading system by Ross, B.G., Fradet, G., & Nedzelski, J.M. 1996 Otoiarneolow Head and Neck Surgerv, - 114(3), 382.
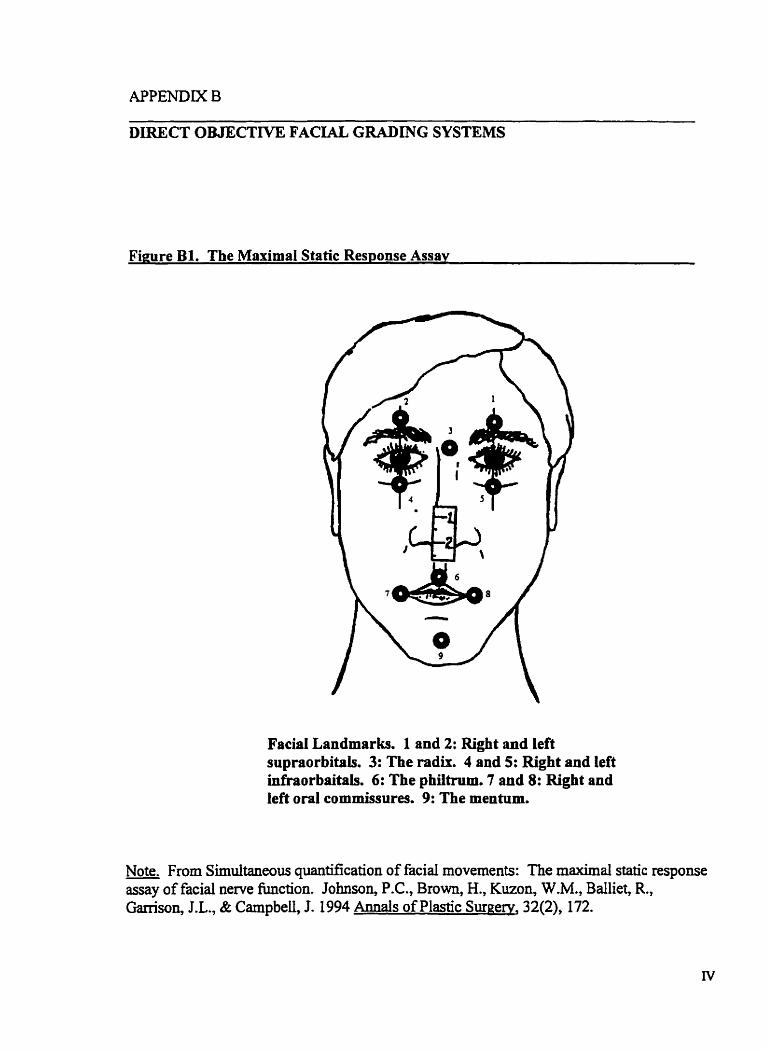
Figure B1. The Maximal Static Response Assav
Facial Landmarks. 1 and 2: Right and left supraorbitais. 3: The radir. 4 and 5: Right and left infraorbaitais. 6: The philtram. 7 and 8: Right and Iefi oral commissures. 9: The mentum.
Note. From Sirnuitaneou quantifkation of facial movements: The maximal static response assay of facial nerve function. Johnson, P.C., Brown, H., Kuzon, W.M., Balliet, R., Ganison, J.L., & Campbell, J. 1994 Annals of Plastic Sumerv, 32(2), 172.
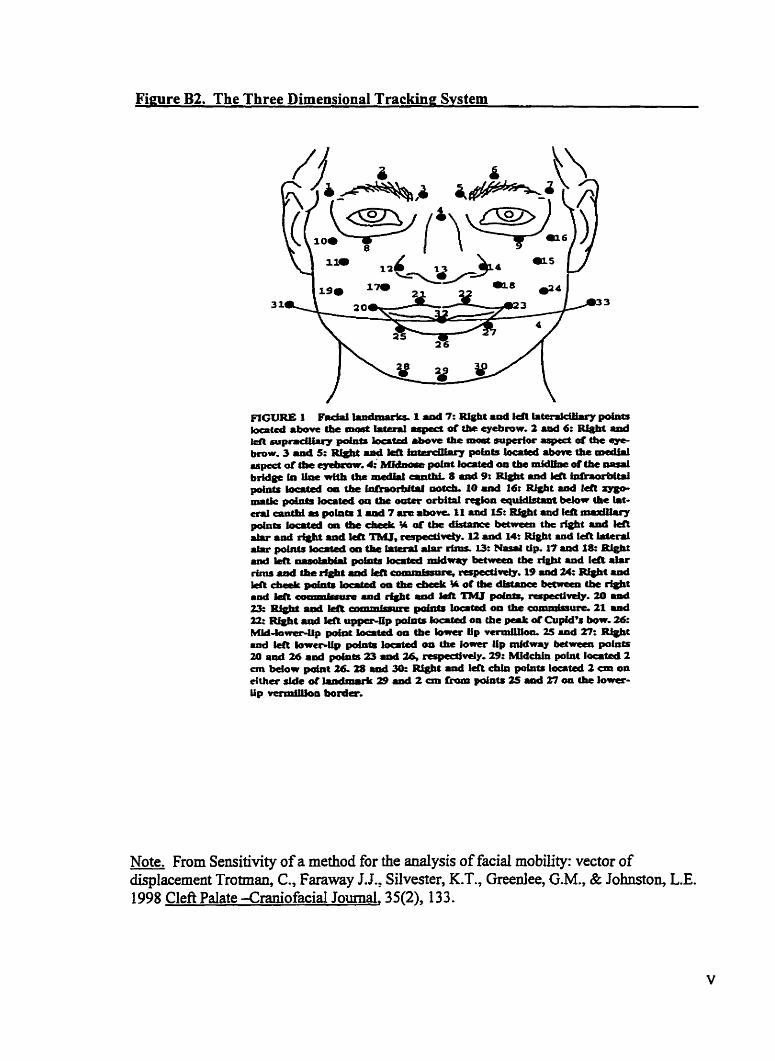
Figure B2. The Three Dimensional Trackine System
Note. From Sensitivity of a method for the d y s i s of facial mobility: vector of - displacement Trotman, C., Faraway J.J., Silvester, K.T., Greenlee, G.M., & Johnston, L.E. 1 998 Cleft Palate -CraniofaciaI Journal, 35(2), 1 3 3.
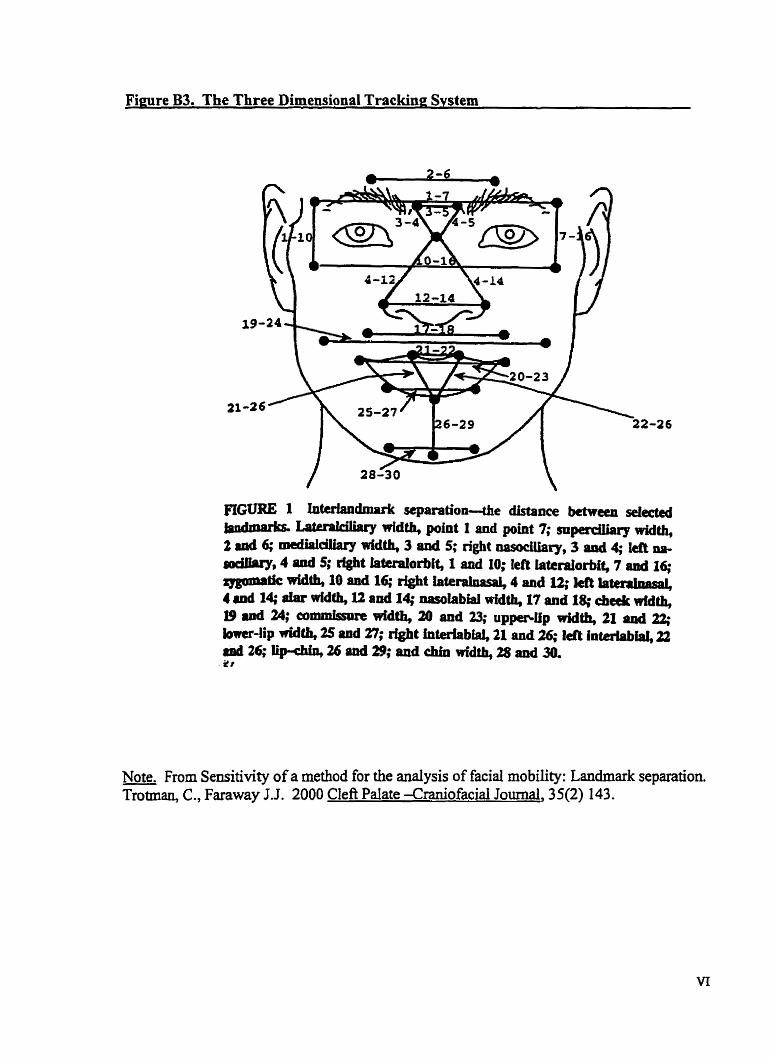
Fieure B3. The Three Dimensional Trackine System
FIGURE 1 l&ria~~dmnrk scparation4e distance bctween selm
Note. From Sensitivity of a method for the analysis of facial rnobility: Landmark sepration. Trotman, C., Faraway J.J. 2000 Clef? Pdate -Craniofacial Journal, 35(2) 143.
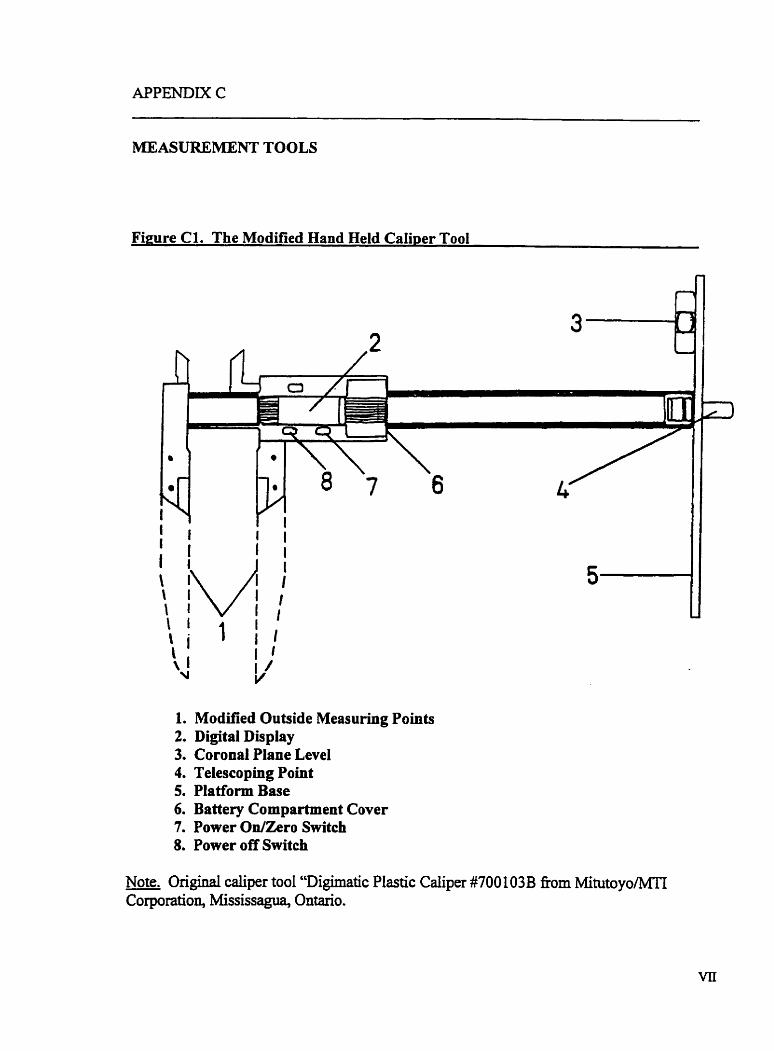
APPENDIX C
MEASUREMENT TOOLS
m r e Cl. The Modified Hand Held CaIiper Tool
1. Modified Outside Measuring Points 2. Digital Dis play 3. Coronal Plane Level 4. Telescoping Point 5. Platform Base 6. Battery Cornpartment Cover 7. Power On/Zero Switch 8. Power off Switch
Note. Original caliper tool "Digimatic Plastic Caliper #7OO 1 O3B fiom MihitoyoMTI Corporation, Mississagua, Ontario.
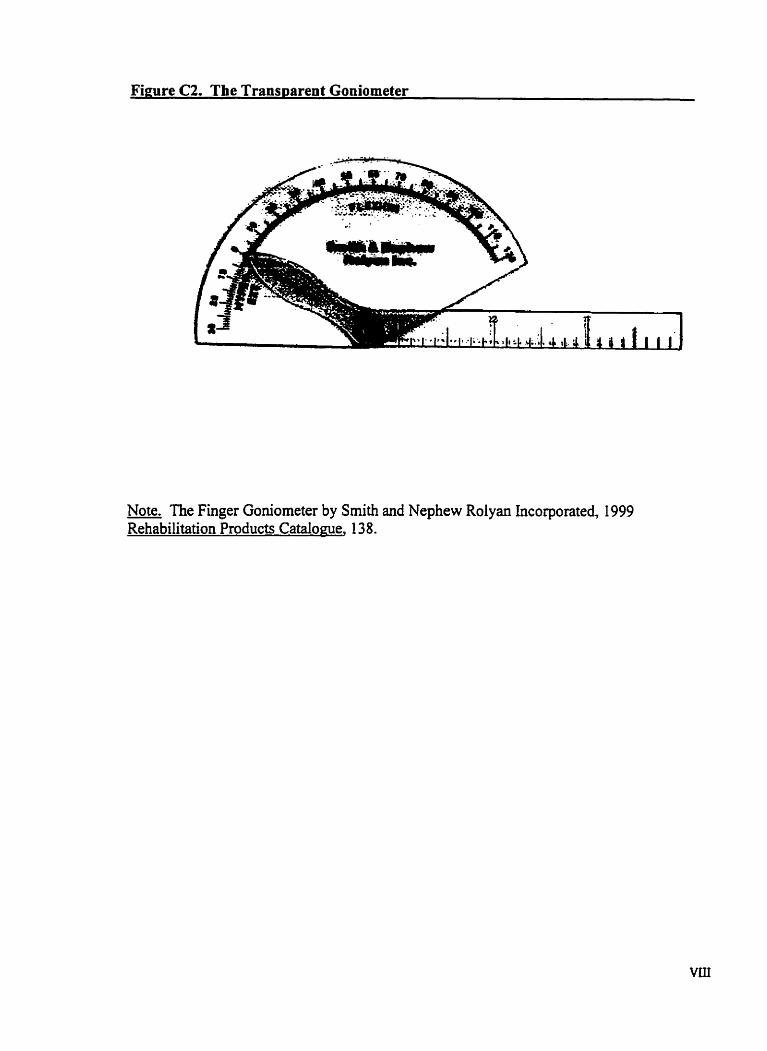
Figure C2. The Transparent Goniometer
Note. The Finger Goniometer by Smith and Nephew Rolyan Incorporated, 1999 Rehabilitation Producr Catalome, 13 8.
INFORMATION SENT TO FAMILES
Recmitment Letter Date
Insert Address
Dear Mr. and Mrs. and child's name,
Facial palsy in children is a fairly uncommon condition that affects how the muscles of the face work. Many children with facial paisy have surgery a d o r therapy to help them use their facial muscles. The changes seen as a result of these interventions are hard to measure and the tool that is used m u t be accurate. In an effort to improve how to mesure facial movement we are currentiy doing a study at the Hospital for Sick Children to determine the most accurate way to mesure facial movement in the clinicai setting. From this study we hope to improve our ability to measure facial motion and to gain a better understanding of the long-term results of therapeutic interventions for children with facial paisy.
In order to complete this study we require that children with facial palsy undergo two separate clinical assessments of facial motion. This c m ail be done at the time of a clhic visit to Plastic Surgery in order to make this as convenient as possible. In the event you do not have a scheduled appointment, a mutuaily convenient assessrnent time can be arranged. For more information about the study please refer to the attached information form. Once the study results are complete, results will be made available to interested participants.
If you would like to participate in this study please contact S h n a Wade at 8 136755 and press 7-2 to leave a message on voice mail indicaihg your name and what number(s) you may be contacted at. Or, you may fill out the response letter included and return it in the self-addressed stamped envelope.
Again, thank you for considering this request.
Sincerel y,
Dr. R Zuker, MD, FRCSC, FACS, FAAP Shawna Wade BMR OT [Cl Head, Division of Plastic Surgery Department of Rehabilitation Services Hospital for Sick Children Hospital for Sick Children Tel: (416) 813-6447 Tel: (416) 8 13-6755 Voice Mail 7-2
Information for Families
Title of Research Project: The Validity and Reliability of a Range of Motion Assessment of Smile for Children with Facial Palsy
Primary Investigator: Shawna Wade, MSc[candidate], BMR O.T. [Cl
Co-lnvestigatoa: Dr. R.T. Manktelow, Dr. R. Zuker, Dr. L. Mainwaring and Dr. C. Graveline
Purnose of the studv Facial palsy is a condition that affects how the muscles of the face work. Many children who have facial palsy have therapy to help them use their facial muscles. The changes seen as a result of therapy are hard to measure and the tool that is used m u t be accurate. The purpose of this study is to test a measurement tool and how well we use it.
What will hamen? If you agree to participate in this study, you will undergo two separate clinical assessments that will be CO-ordinated with your scheduled r e m visit to the Plastic Surgery Clinic a d o r Occupational Therapy. In the event you do not have a scheduled appointment, a mutuaily convenient assessment time will be ananged at the Hospital for Sick Children. The 30-minute assessments will be cornpleted one d e r the other, with a 15-minute break in between. The assessment will include, marking specific measurernent points on your face with a special pencil [the marks will wash o q , and measuring what your face is like when your are not smiling, and when you are smiling. M e r a break another therapist will complete the same assessrnent over again. This is done to make sure our resdts are accurate.
Benefits You and your child will help to improve our ability to measure facial motion in a more accurate way. You will make a significant contribution to the curent literature for very little has been devoted to children on this topic. This will assist the health care professionals to better understand the long-term resdts of therapeutic interventions for children with facial palsy.
mks - There are no hown hanns associated with participation in this study. By taking part in this study, you will undergo an assessment that will take approximately 1 hour to complete. You may become tired during the study and a rest period can be requested at any tirne. You can decide not to participate in the study at any the. This will not affect your treatment at the Hospital for Sick Children.
Letter of Response
Please place a checkmark in the appropriate response:
O 1 would older)
O 1 would
be interested in participating in this study (16 years or
like my child to participate in this study
O 1 am not interested in participating in this study
Telephone Number(s) where you may be contacted:
Home:
Business:
Comments:
Signature:
Date:
CONSENT FORMS
Consent Form For Participants 16 Years and Older
1 Name:
Date of Birth:
HSC #:
Title of Research Proiect: The Vaiidity and Reliability of a Range of Motion Assessment of Srnile for Children with Facial Palsy.
Investi~ator(s): Primary Investigator: Shawna Wade, MSc[candidate], BMR O .T. [Cl
Department of Rehabilitation Services: Division of Occupational Therapy Hospital for Sick Children [416] 813-6755
Co-Investigatoa: Dr. R.T. Manktelow Department of Plastic Surgery The Toronto General Hospital [416] 340-4800 ext. 6720
Dr. RI Zuker Division of Plastic Surgery The Hospital for Sick Children [41q 813-6447
Dr. L. Mainwaring Assistant Professor, Faculty of Physical Education and Health University of Toronto [416] 946-5134
Dr. C. Graveline Director, the Department of Rehabilitation SeMce The Hospital for Sick Children [416] 813-6755
XII
Purpose of the Research: Facial palsy is a condition that affects how the muscles of the face work. Many children who have facial palsy have therapy to help them use their facial muscles. The changes seen as a result of therapy are hard to rneasure and the tool that is used must be accurate. The purpose of this study is to test a measurement tool and how well we use it.
Description of the Research: If you agree to participate in this study, you will undergo two separate clinicai assessments that will be CO-ordinated with your scheduled retum visit to the Plastic Surgery C h i c andor Occupational Therapy. In the event you do not have a scheduled appointment, a mutually convenient assessment time will be arranged at the Hospital for Sick Chddren. The assessments will be completed one after the other, with a 15-minute break in between. The assessment will include, marking specific measurement points on your face with a special pencil [the marks will wash off], and rneasuring what your face is like when your are not smiling, and when you are smiling. After a break another therapist will complete the same assessment over again. This is done to make sure our results are accurate.
Potential Harms, Iniuries, Discornforts or Inconvenience: There are no known hamis associated with participation in this study. By taking part in this study, you will undergo an assessment that will take approximately 1 hour to complete. You may become tired during the study and a rest penod can be requested at any tirne. You cm decide not to participate in the study at any tirne. This will not affect your treaûnent at the Hospital for Sick Children.
Potential Benefits: You will not benefit directly fiom participating in this study.
You will help to irnprove our ability to measure facial motion in a more accurate way. You will make a significant contribution to the cunent literature for very little has been devoted to chilchen on this topic. This will assist the health care professiods to better understand the long- temi results of therapeutic interventions for children with facial palsy.
Confiden tialitv: Confidentiality will be respected and no information that discloses your identity will be released or published &thout consent unless required by law. For your information, the research consent fom wili be inserted into your health record.
Partici~ation: Participation in research is voluntary. If you choose not to participate, you and your family will continie to have access to quality care at HSC. If you choose to participate in this study you can withdraw fiom the study at any time. Again, you and your farnily will continue to have access to quality care at HSC.
Sponsorshi~: If you would like to know the source of funding, please discuss this with the investigator.
Consent : '1 acknowledge that the research procedures described above have been exphined to me and that any questions that I have asked have been a w e r e d to my satisfaction. I have been infirmed of the alternatives to participation in this study, including the right not to pmticipate and the right to withdraw without compromising the quality of medical care ut The Hospital for Sick Children for me and for other members of my family. As well. the potential harms and discornforts have been expkained to me and I also understand the benefts (if any) of participating in the research study. 1 know that I rnay ask now, or in the future, any questions I have about the study or the resemch procedures. I have been assured that records relating [O me and my care wilZ be kept confidential and that no information will be reZeased or printed thnt would disclmi? p2rsoizal &dzlr;is. witltour i i ~ ~ pémission urile~~s required by l m . "
I hereby consent to participate.
Name ofPatient and Age The Person who rnay be contacted about the research is:
Shawna Wade
who rnay be reached at telephone #: Signature (if1 6 yrs. or over)
Signature Name ofperson who obtained cornent
Date
Consent Form For Partichants less than 16 Years of Age
Name:
Date of Birth:
HSC #:
Title of Research Proiect: The Validity and Reliability of a Range of Motion Assessrnent of Smile for Children with Facial
Investi~ator(s): Primary Investigator: Shawna Wade, MSc [candidate], BMR O .T. [Cl
Depariment of Rehabilitation SeMces Division of Occupational Therapy Hospital for Sick Children [416] 813-6755
Co-Investigators: Dr. R.T. Mankteiow Department of Plastic Surgery The Toronto General Hospital [416] 340-4800 ext. 6720
Dr. R Zuker Division of Plastic Surgery The Hospital for Sick Children [416] 8 13-6447
Dr. L. Mainwaring Assistant Professor, Faculty of Physical Education and Health University of Toronto [416] 946-5 134
Dr. CI Graveline Director, the Department of Rehabilitation Service The Hospital for Sick Children [41q 813-6755
Purpose of the Research: Facial palsy is a condition that affects how the muscles of the face work. Many children who have facial palsy have therapy to help them use their facial muscles. n i e changes seen as a result of therapy are hard to measure and the tool that is used must be accurate. The purpose of this study is to test a measurement tool and how well we use it.
Descri~tion of the Research: If your child agrees to participate in this study, he/she will undergo two separate clinicai assessments that will be co-urdinated with a schedded r e m visit to the Plastic Surgery Clinic andor Occupational Therapy. In the event your child does not have a scheduled appointment, a m u W y convenient assessment time will be arranged at the Hospital for Sick Children. The assessments will be completed one d e r the other, with a 15-minute break in between. The assessment will include, marking specific measurement points on your child's face with a special pencil [the marks will wash off], and measuring what your child's face is like when he/she is not smiling, and when he/she is smiling. M e r a break another therapist will complete the same assessrnent over again. This is done to make sure our results are accurate.
Potential Harms, Iniuries, Discornforts or Inconvenience: There are no known harms associated with participation in this study. By taking part in this study, your child will undergo an assessment that will take approximately 1 hour to complete. Some children can become tired and your child may request rest penods at any tirne during the shidy. Your child can decide not to participate in the study at any t h e . This will not affect hisher treatment at the Hospital for Sick Children.
Potential Benefits: Your child will not benefit directly fiom participating in this study.
Your child will help to improve our ability to measure facial motion in a more accurate way. This information will make a significant contribution to the current iiterature for very linle has been devoted to children on this topic. This wili assis the health care professionals to better understand the long-term results of therapeutic interventions for children with facial palsy.
Con fiden tialitv: Confidentiality will be respected and no information that discioses the identity of your child will be released or published without consent unless required by law. For your information, the research consent form will be inserted into your child's health record.
Partici~ation: Participation in research is volmtary. If you or your child choose not to participate, you and your family wili continue to have access to quality care at HSC. If you choose on behaifof your child to participate in this study you c m withdraw your child fkom the study at any tirne. Again, you and your family will continue to have access to quality care at HSC.
Sponsorshi~: If you would like to know the source of fûnding, please discuss this with the investigator.
Consent: I acknowledge that the research procedures described above have been explained to me and thut any questions that I have asked have been answered to my satisfaction 1 have been Nifomed of the alternatives to participation NI this study, including the right not tu participate and the right to withdraw without compromising the quality of medical care at The Hospital for Sick Children for my child and for other mernbers of my family. As well, the potential harms and discornforts have been explained to me and 1 ulso understand the benefts (ïf any) of participating in the research study. I know that I may ask now, or in t h e f h r e , riny questions I have about the study or the research procedures. I have been assured that recordr relating to my child and rny child's care will be kept confidential and that no information will be released or printed ihat would discIose persund irlrntity without my permission unless required by law.
I hereby consent for my child to part icipate.
The Person whu may be contacted Name oflarent about the research is:
Shawna Wade
who may be reached at teiephone #: Signature
14167 813-6755
Nome ofperson who obtained consent.
Signature
Assent Form
Name:
Date of Birth:
HSC #:
Title of Research Proiect: The Validity and Reliability of a Range of Motion Assessrnent of Srnile for Children with Facia Palsy .
Investigator(s): Primary Investigator: Shawna Wade, MSc[candidate], BMR O .T. [Cl
Department of Rehabilitation Services Division of Occupational Therapy Hospital for Sick Children [416] 8 13-6755
Co-Investigaton: Dr. R.T. Manktelow Department of Plastic Surgery The Toronto General Hospital [416] 340-4800 ext. 6720
Dr. R. Zuker Division of Plastic Surgery The Hospital for Sick Children [416] 813-6447
Dr. L. Mainwaring Assistant Professor, Faculty of Physical Education and Health University of Toronto [4 161 946-5 134
Dr. C. Graveline Director, the Department of Rehabilitation Service The Hospital for Sick Children [416] 813-6755
Whv are we doing this studv? Children with facial palsy can not move the muscles in their face very well and many children have therapy to help them get better. It is very hard to measure how rnuch the children get better. The purpose of this project is to test a measuring tool and see how well we use it.
What wil1 happen during the study? If' you participate in this study, you will be seen by two Occupational Therapists at separate times. The assessment will include, marking specific points on your face with a special pencil [the marks will wash off], and measuring what your face is like when your are not smiling, and when you are smiling. Mer a break another therapist will complete the same assessment over again. This is done to make sure the therapists test the same.
Are there good things and bad things about the studv? We know of no bad things that will happen to you if you do this study. If you become tired you may ask for a rest penod at any tirne.
Who will know about what 1 did in the study? Only the people doing the study will know how you did. Your name or address will not be given to anyone.
Can 1 decide if I want to be in the study? Yes you can. If you do not want to be part of this study, that's okay, no one will be upset with you. You will still have your regular appointment with the doctor if you are here for an appointment at the Plastic Surgery Clinic. You can ask the therapist any questions that you have. He/she will try to answer your questions and help you to understand. If you Say yes now but change your mind later, that is okay. If you Say no, it d l not change the way you are treated at the Hospital for Sick Children.
Assent: "1 was present when read this form and gave hisher verbal assent."
Name of person who obtained
Signature
Date
ASSESSMENT PROCEDURES
Standard Protocol for the Administration of the Assessrnent
Procedure: Children will be tested one at a time by the two raters. The participants will be seated on a chair during the measurement. The room for measurement should be quiet and fiee from distractions. Only the rater, the child and hisher parent[s] should be in the roorn.
The rater will be seated directly in fiont of the child at the same eye level as the child. A picture poster will be placed on the wail facing the child to serve as a place for the child to focus while the rater identifies the landmarks [Part II]. The rater m u t record the results of each separate measurement immediately upon completing the measure on the data sheet [Part a* Script for testhg: I wanf to rneawe how much you can mi le with this new meamring tool. I am going to measure f i o m dzjjierent points onyour face and I will memure before you smile and then I will askyou to give me the biggest smile you cun and I will measure again. I am going to do this for both sides of your face. This will not hurt you.
Before I meanrre I would iike to phce a few srnail dots on your face like you see in this picture. We will wash these dots off when we are finished This helps me to mak sure thnt I measure the right spots. Pieme look struighr ahead at the poster on the wull. Now we are ready to measure.
Example of script for assessment: Lookstraight a k d ut me without smiling. I will memure fiom the corner of you mouth to your ear /@eTfm m e m e m e n t and record]. N w 0 to mi le as much as you c m and hold YOM srnile @er$brm the meawement and record]. ïE~hat good! Now lets do the same memrements on the other side ofyour face.
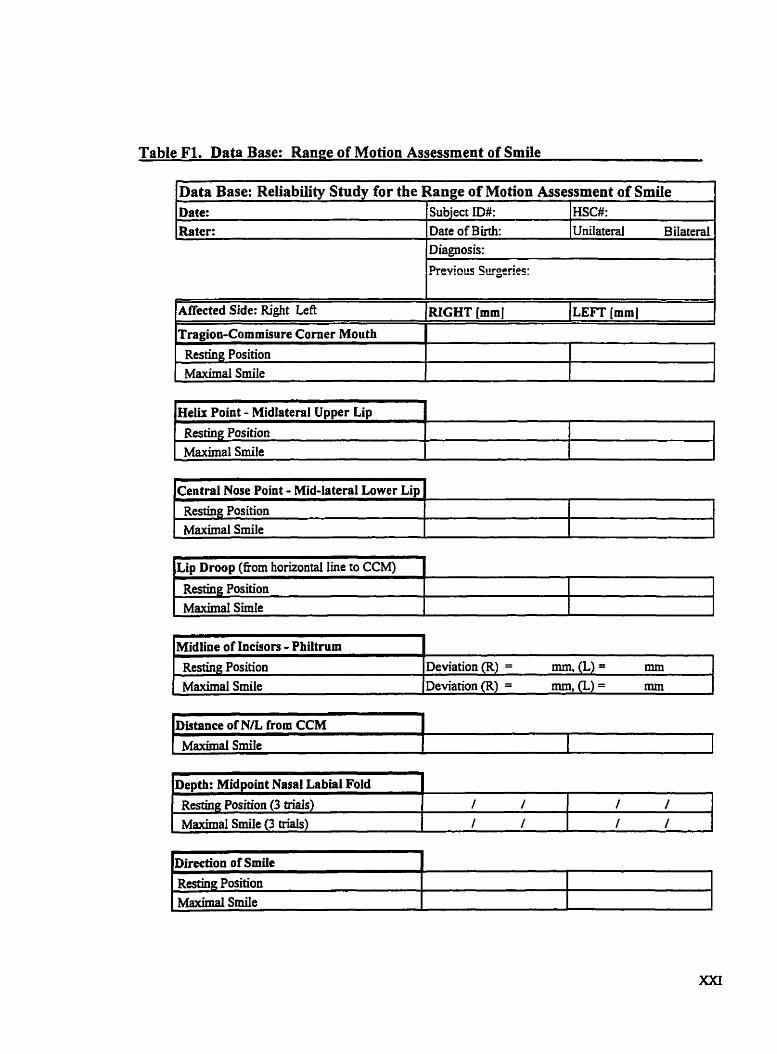
Table FI. Data Base: Range of Motion Assessment of Smile
Data Base: Reiiabiüty Study for the Range of Motion Assessment of Smile
Resting Position Maximal Srnile
Affected Side: Right Left L
Tragioo-Cornmisure Corner Mouth
Helü Point - Midlateral Upper Lip 1 d
HSC#: Unilateral Bilateral
"
Date: Rater:
RIGHT [mmJ (LEFT [mm J I
1 Resting Position 1 1 1
Diagnosis:
Previots Surgeries: I
Subject ID#: Date of Birth:
[ Maximal Smile -
I I l kentral Nose Point - Mid-lateral Lower Lip 1 -
Resting Position Maximal Srnile
l~istance of N/L from CCM 1
-- -
Restùrg Position Maximal Smile
Depth: Midpoint Nasal Labial Fold Resting Position (3 bids) / / 1 1 1 I
Deviation (R) = mm, (L) = mm Deviation (R) = mm, (L) = mm
1 MW Srnile (3 triais) I I I I I I
m
Ï%ction of Srnile Restiug Position Msucmial SmiIe
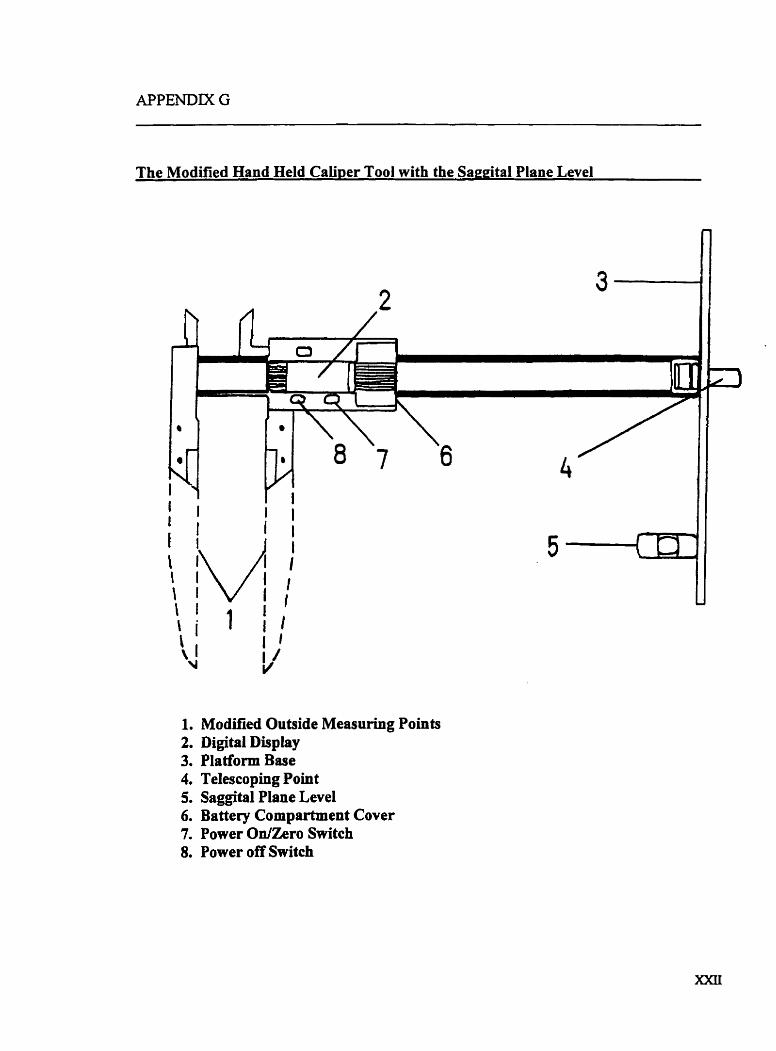
The Modified Hand HeId Cab per Tool with the Saegîtal Plane Level
1. Modified Outside Measuring Points 2. Digital Display 3. Platform Base 4. Telescoping Point 5. Saggîtal Plane Level 6. Battery Cornpartment Cover 7. Power OnIZero Switch S. Power off Switch
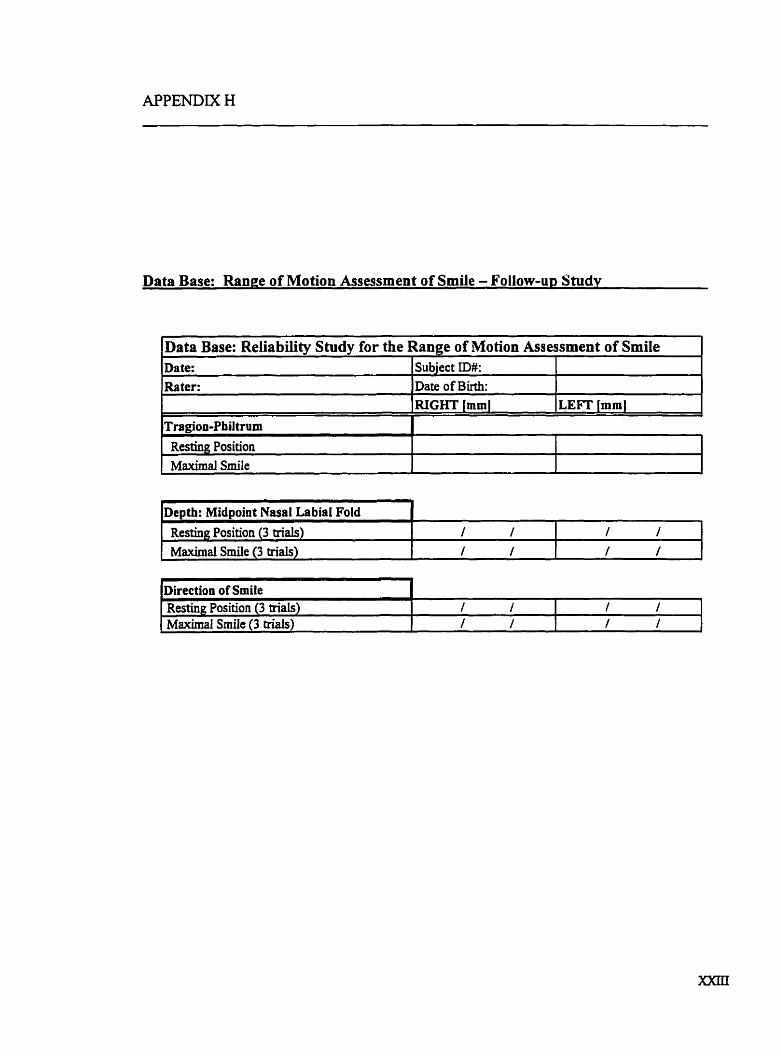
Data Base: Range of Motion Assessment of Smile - Follow-up Studv
bats Base: Reliabilitv Studv for the Rauee of Motion Assessrnent of Srnite 1
Restinpr Position Maximal Smile
Date: Rater:
epth: Midpoint Nasal La biai Fold 1 1
Subject ID#: Date of Birth:
[ Resting Position (3 trials) 1 1 1 / 1 , I
Direction of Smile Resting Position (3 trials) Maximal Smile (3 trials)
1 / 1 1 1 1 / / J
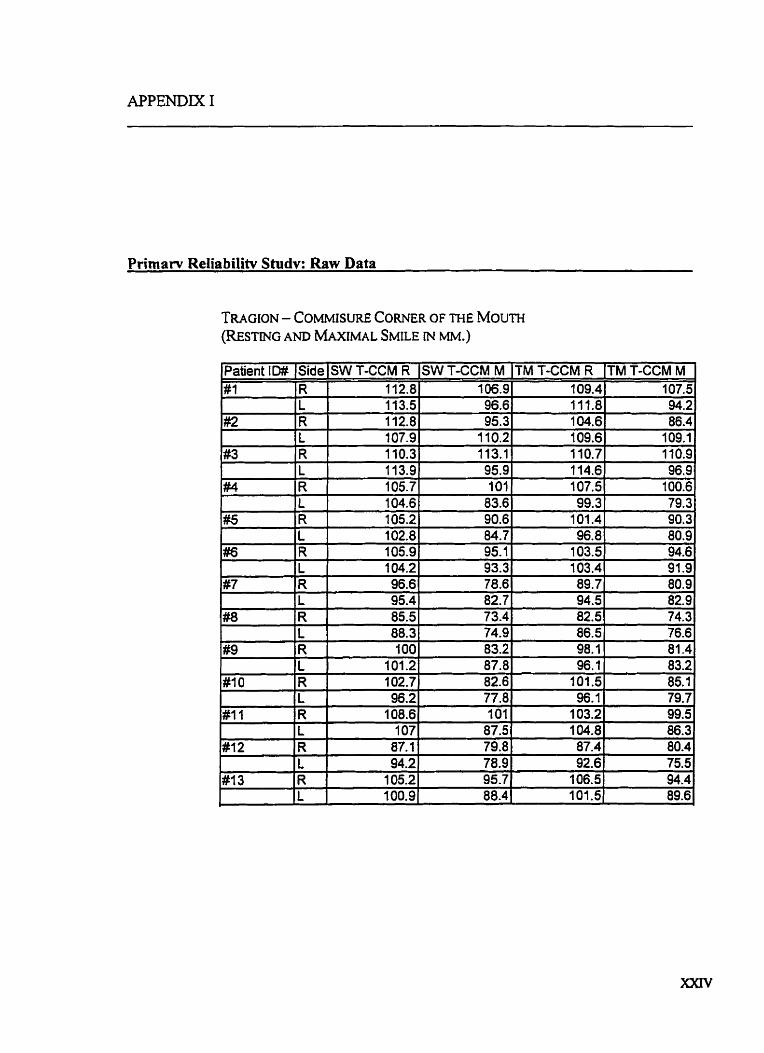
Primarv Reliabilitv Studv: Raw Data
Patient ID# #1
#2
#3 1
#
. #5
#6
#7
#8
#9
#10
# I l
#12
#-l3
TM T-CCM R 109.4 111.8 104.6 109.6 1 10.7 1 14.6 107.5 99.3
101.4 96.8
103.5 103.4 89.7 94.5 82.5 86.5 98.1 96.1
101.5 96.1
103.2 104.8 87.4 92.6
106.5 IO1 -5
Side R L R L R L R L R L R L R L R L R L R L R L R L R L
SW T-CCM R 112.8 113.5 112.8 107.9 110.3 1 13.9 105.7 104.6 105.2 102.8 105.9 104.2 96.6 95.4 85.5 88.3 100
101.2 102.7 96.2
108.6 1 07
87.1 94.2
105.2 100.9
(TM T-CCM M 107.5 94.2 86.4
109.1 110.9 96.9
100.6 79.3 90.3 80.9 94.6 91.9 80.9 82.9 74.3 76.6 81.4 83.2 85.1 79.7 99.5 86.3 80.4 75.5 94.4 89.6
SW T-CCM M 106.9 96.6 95.3
1 10.2 113.1 95.9 101
83.6 90.6 84.7 95.1 93.3 78.6 82.7 73.4 74.9 83.2 87.8 82.6 77.8 101
87.5 79.8 78.9 95.7 88.4
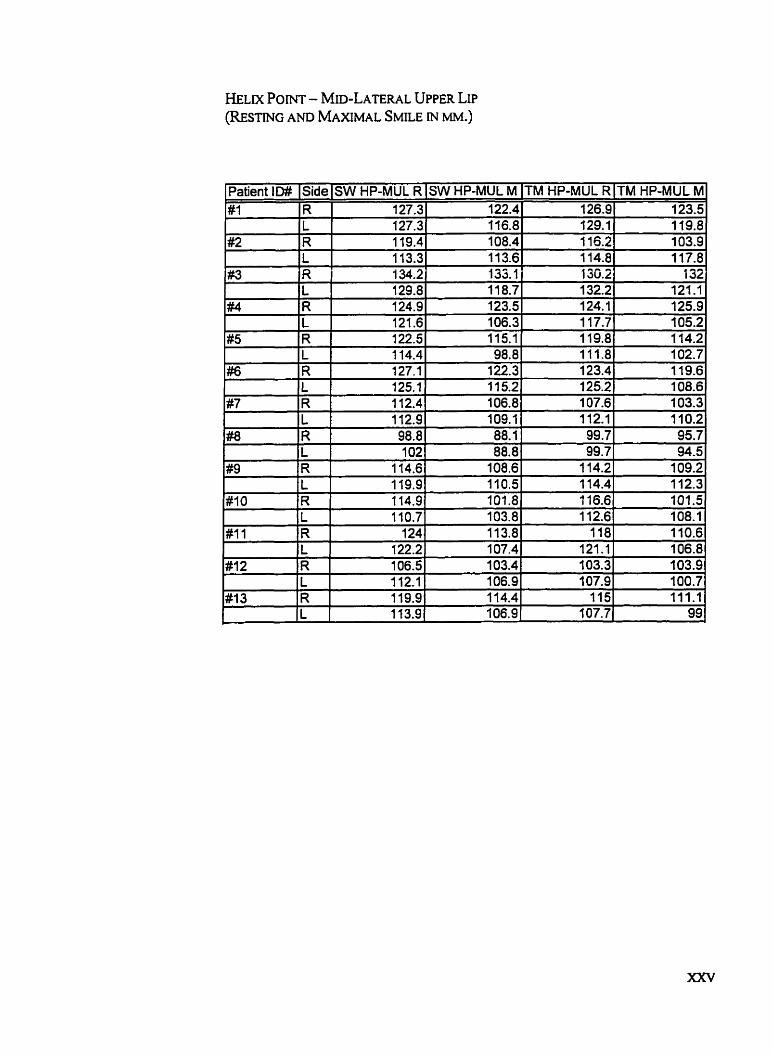
Patient ID# #1
1 #2
1
#3
#4
#5
#6
#7
#8
#9 -
#IO
SW HP-MUL 122.4 116.8 108.4 11 3.6 133.1 11 8.7 123.5 106.3 11 5.1 98.8
122.3 1 15.2 106.8 109.1 88.1 88.8
108.6 11 0.5 101.8 103.8 113.8 107.4 103.4 106.9 114.4 106.9
Side R L R L R L R L R L R L R
M-TM HP-Mm R 126.9 129.1 1 15.2 114.8 136.2 132.2 124.1 1 17.7 1 19.8
SW HP-MUL Fi 127.3 127.3 11 9.4 1 13.3 134.2 129.8 124.9 121.6 122.5 1 14.4 127.1 125.1 1 12.4
TM HP-MUL M 123.5 119.8 103.9 1 17.8
132 121.1 125.9 105.2 114.2
1 10.7 124
122.2 106.5 112.1 119.9 1 13.9
L #11 )R
IL
L R L R L
IR
#12
#13
111.8 123.4 125.2 107.6 112.1 99.7 99.7
114.2 1 14.4 1 16.6 1 12.6
118 121.1 103.3 107.9
115 107.7
112.9 98.8 102
,. 1 14.6 1 19.9 114.9
R L R L
102.7 1 19.6 108.6 103.3 1 10.2 95.7 94.5
109.2 112.3 101.5 108.1 110.6 106.8 3 03.9 100.7 111.1
99
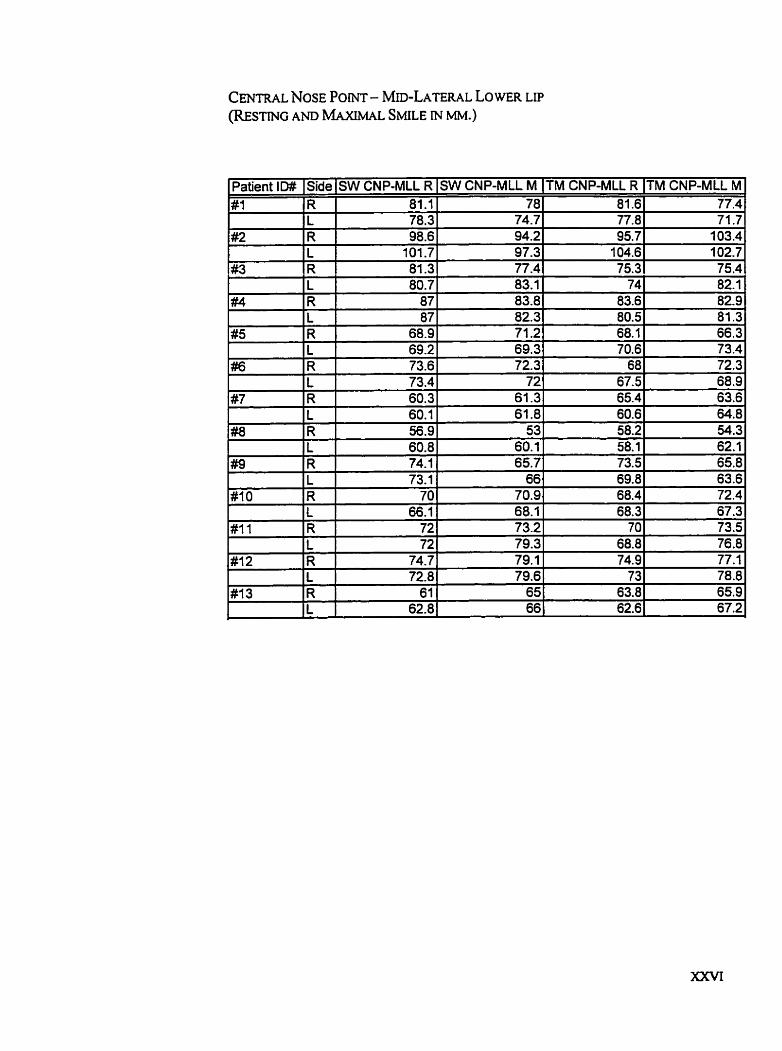
,
SW CNP-ML1 M 78
74.7 94.2 97.3 77.4
TM CNP-MLL R 81.6 77.8 95.7
104.6 75.3
TM CNP-MLL M 77.4 71 .7
103.4 102.7 75.4
SW CNP-ML1 R 81.1 78.3 98.6
101.7
Patient ID# #1
#2
83.1 83.8 82.3 71.2 69.3
74 83.6 80.5 68.1 70.6
Side R L R L
#4
#5
82.1 82.9 81.3 66.3 73.4
#3 R 1 81.3
##6
#7
#8
#9
# l O
#11
#12
#13
L 1 80.7 R 1 87 L 1 87 R L
72.3 68.9 63.6 64.8 54.3
68.9 69.2
R L R L R L R L R L R L R L R L
72.3 72
61.3 61.8
53
73.6 73.4 60.3 60.1 56.9 60.8 74.1 73.1
70 66.1
72 72
74.7 72.8
61 62.8
68 67.5 65.4 60.6 58.2
60.1 65.7
66 70.9 68.1 73.2 79.3 79.1 79.6
65
58.1 73.5 69.8 68.4 68.3
70 68.8 74.9
73 63.8
62.1 65.8 63.6 72.4 67.3 73.5 76.8 77.1 78.8 65.9
- 66 1 62.6 67.2
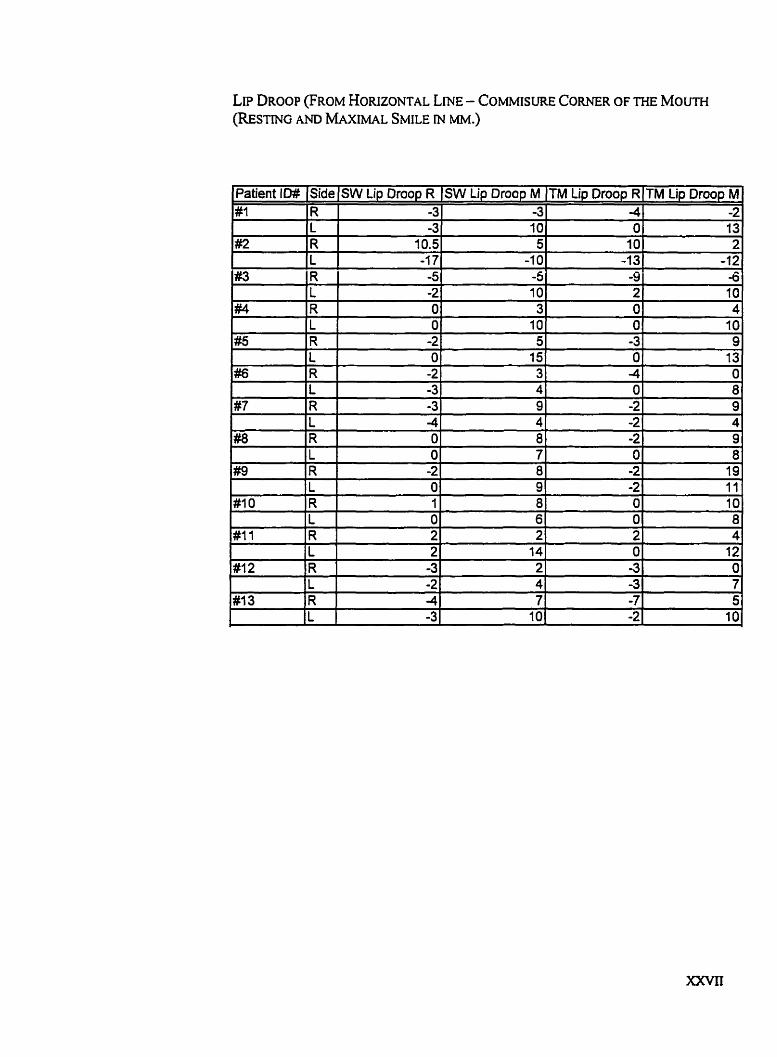
LIP DROOP (FROM HORIZONTAL LME - COMMISURE CORNER OF THE MOUTH (REsTING AND MAXIMAL SMILE M MM.)
Patient Iû# #1
#2
#3
#4
#5
##6
#7
#a
#9
#10
#11
#12
Side R L R L R 1 R L R L R L Fi L R L R L R L R L , R L
SW Lip Droop R -3 -3
10.5 -1 7 -5 -2 O O
-2 O -2 -3 -3 4 O O -2 O 1 O 2 2 -3 -2 -4 -3
SW Lip Droop M -3 10 5
-1 0 -5 10 3 10 5 15 3 4 9 4 8 7 8 9 8 6 2
14 2 4 7
10
TM Lip Droop R 4 O 10 -1 3 -9 2 O O
-3 O -4 O -2
- -2 -2 O
-2 -2 O O 2 O
-3 -3 -7 -2
#13
TM Lip Droop M -2 13 2
-12 -6 10 4 10 9 13
O 8 9 4 9 8 19 11 10 8 4
12 O 7 5
10 R
1 L
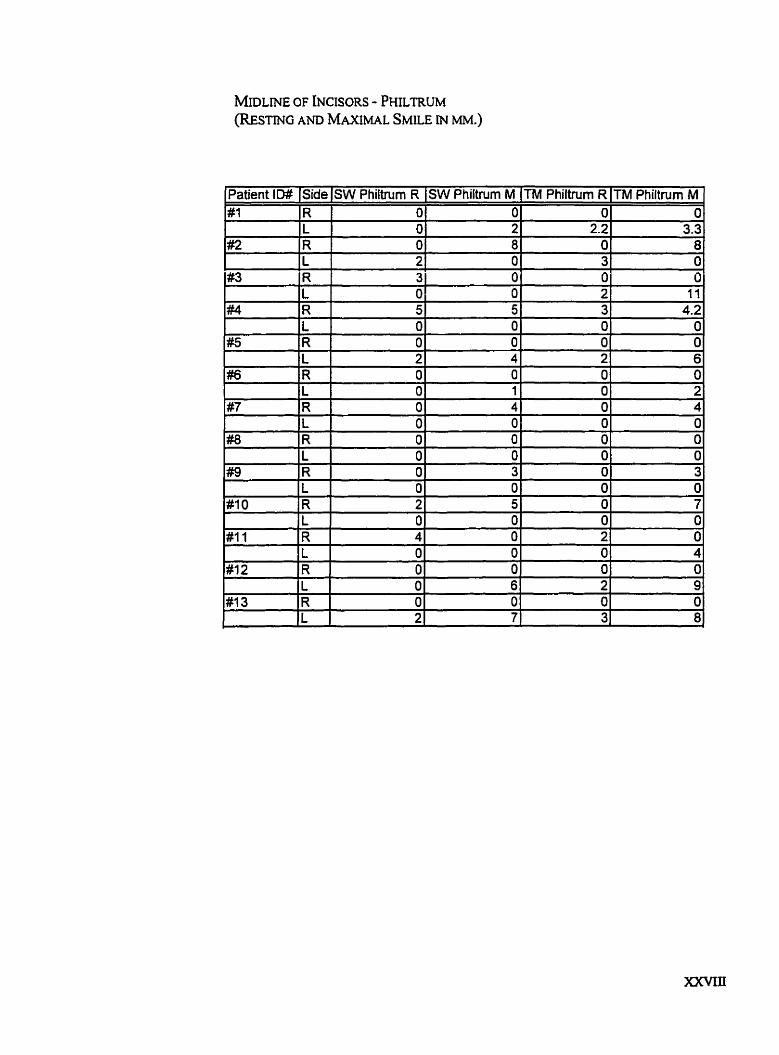
WLME OF INCISORS - PHILTRUM (REsTING AND ~ ~ A X M A L SMILE IN MM.)
Patient ID# Side SW Philtntm R SW Philtrurn M TM Philtnim R TM Philtnim M #1 R O O O O
L 1 O 2 2.2 3.3 #2 R 1 O 8 O 8
L 1 2 1 O 3 O #3 Fi 3 O O O
L O O 2 II #4 R 5 5 3 4.2
L O O O O
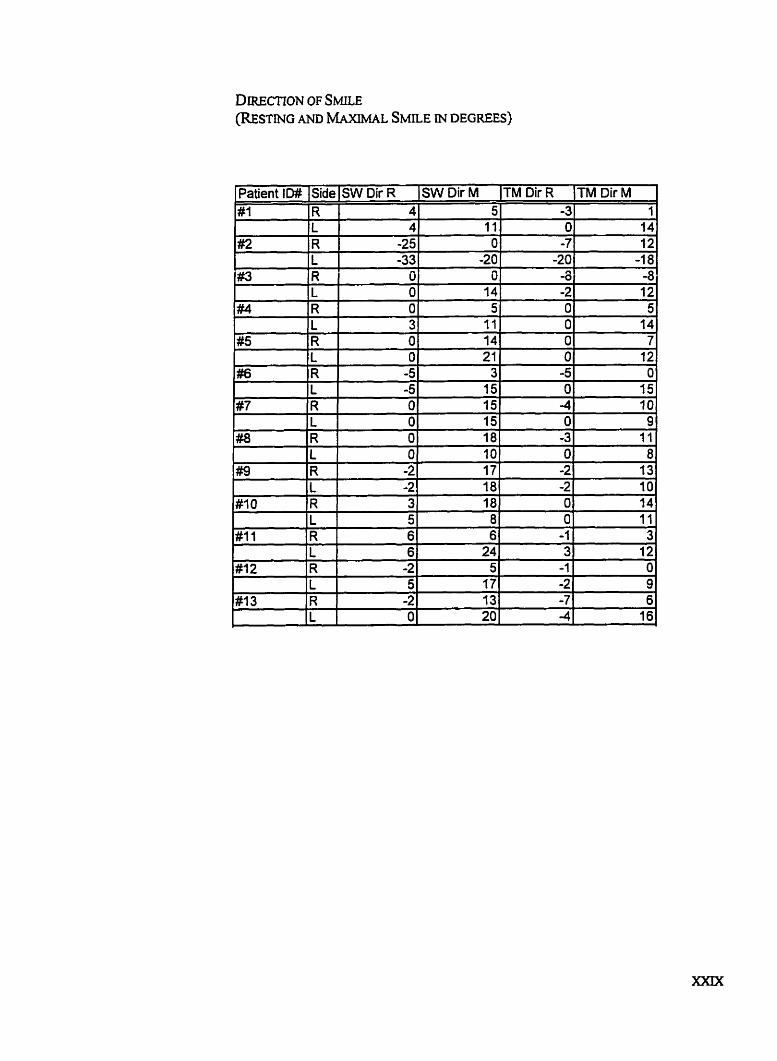
DIRECTION OF S ~ E (RESTMG AND MAXMAL SMLE iN DEGREES)
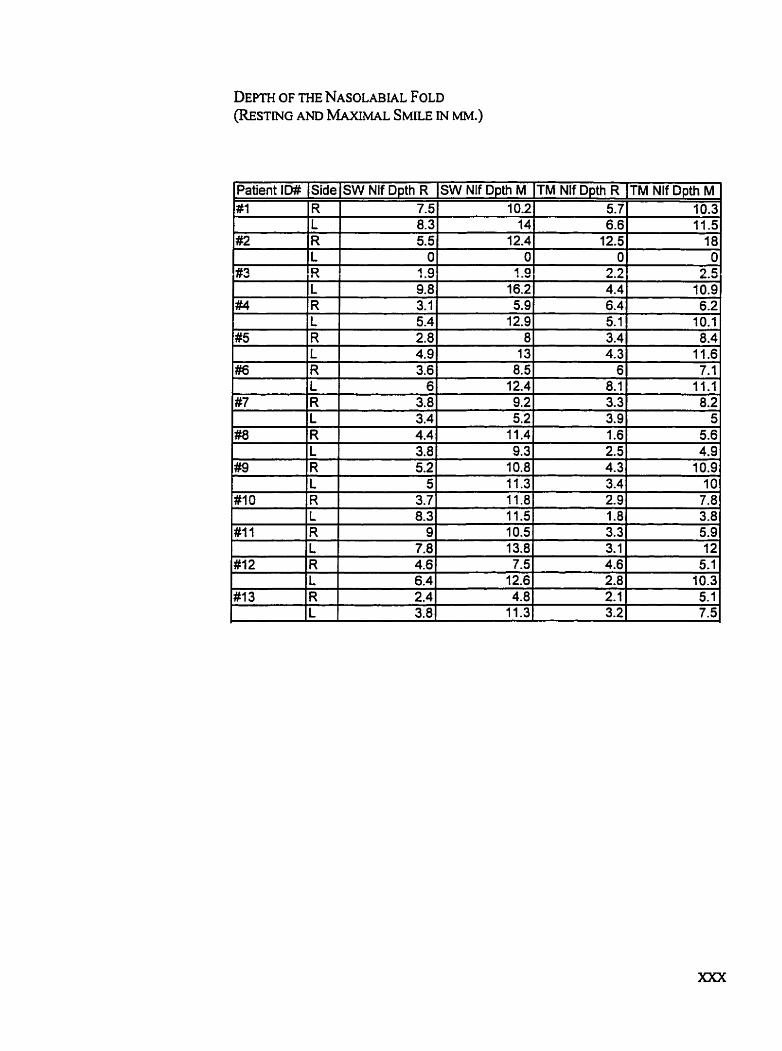
Patient ID# SidelSW Nlf Dpth R SW Nlf Dpth M ITM Nlf Dpth R !TM Nlf Dpth M # l R 7.5 10.21 5.7 1 10.3
L 8.3 14 6.6 11.5 #2 R 5.5 12.4 12.5 18
L O O O O #3 fi 1.9 1.9 2.2 2.5
L 1 9.81 16.2 4.4
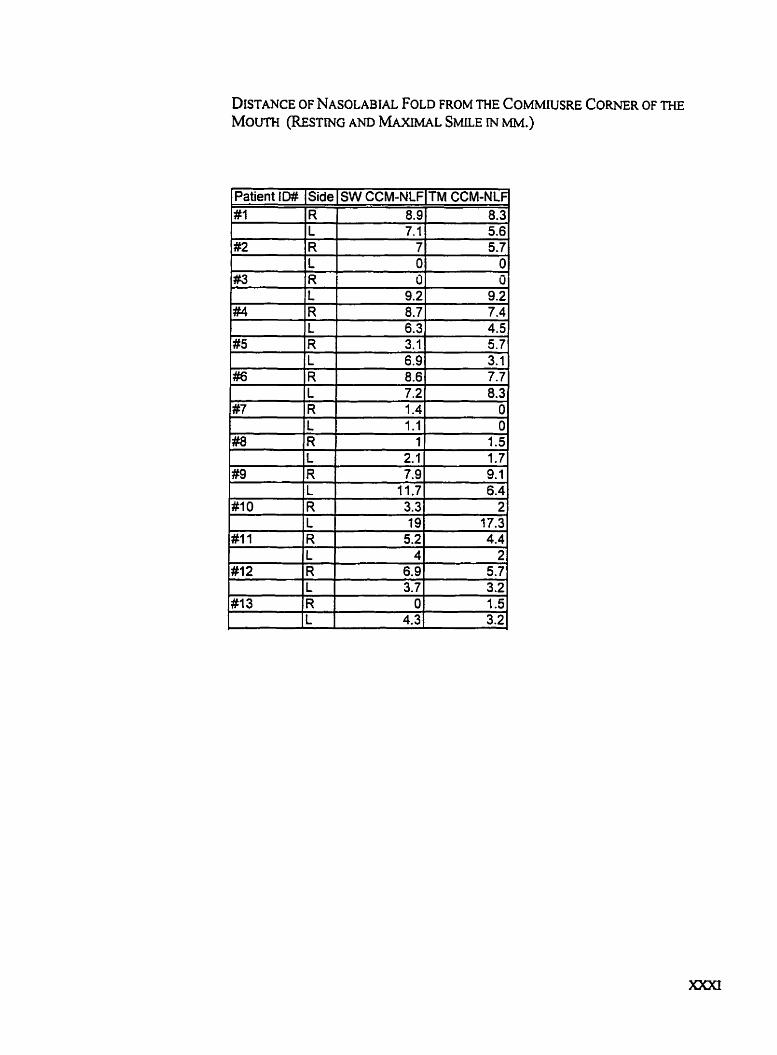
DISTANCE OF NASOLABIAL FOLD FROM THE COMMIUSRE CORNER OF THE MOUTH (RESTING AND MAXIMAL SMILE M MM.)
Patient ID# Side SW CCM-NLF TM CCM-NL
5.7
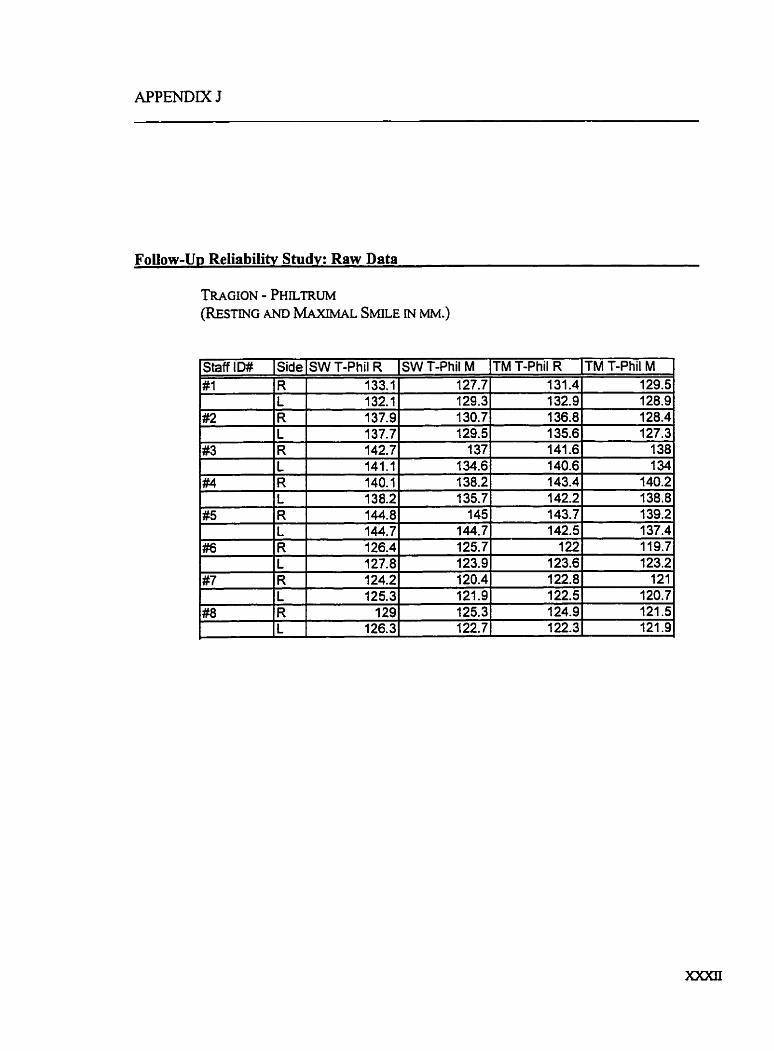
Foilow-Up Reliabilitv Study: Raw Data
TRAGION - PHILTRUM (REsTING AND MAXIMAL S ~ E M MM.)
TM T-Phil M 129.5 128.9 128.4 127.3 138 1 34
140.2 138.8 139.2 137.4 11 9.7 123.2 121
120.7 121.5 121.9
TM T-Phil R 131.4 132.9 136.8 135.6 141.6
- Staff ID# #l
#2
#3
#4
#5
#/6
#7
SW T-Phil M 127.7 129.3 130.7 129.5 137
Side R L R L R
SW T-Phil R 133.1 132.2 137.9 137.7 142.7
L R 1 R L R L R L
141.1 140.1 138.2 144.8 144.7 126.4 127.8 124.2 125.3
134.6 1 140.6 138.21 143.4
129 126.3
135.7' 145
144.7 125.7 123.9 120.4 121.9 125.3 122.7.
#8
142.2 143.7 142.5 122
123.6 122.8 122.5 124.9 122.3=
R L
J
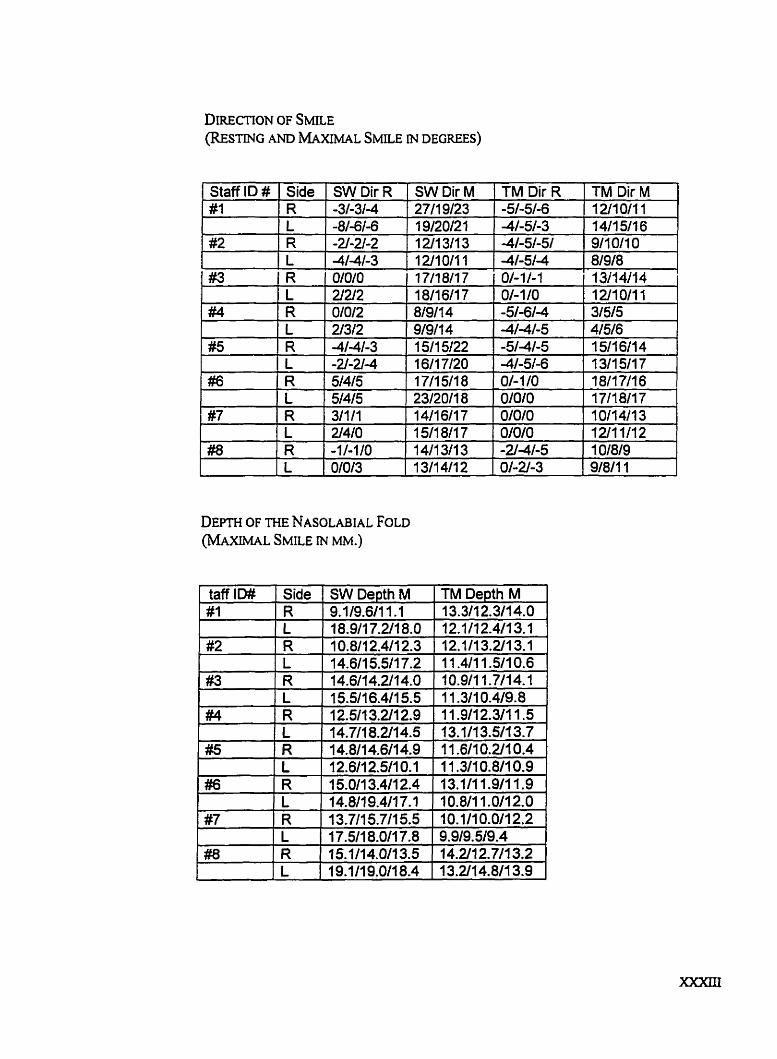
DIRECTION OF S ~ E (RESTING AND MAXIMAL SMLE DEGWS)
DEPTH OF THE NASOLABIAL FOLD (MAXIMAL SMILE IN MM.)
Staff ID # # l
#2
Side R L R L
1 311 411 4 1 2/10111 31515 4/5/6 1 511 611 4 1 311 511 7 18ll7ll6 17/18/17 i
TM Dir M 1 U10111 14/15/16 911 O11 O 81918
.
#3
#4
TM Dir R . -51-51-6 4-51-3 41-51-51 -41-51-4
SW Dir R -3/-3/-4 -8/-6/06 -21-2l-2 4-41-3
R L R
OlO/O ZIZI2 0/0/2 Z3/2 -41-41-3
SW Dir M 27119123 1 912012 1 1211 311 3 1 1 1 1 17/18/17 1 811 611 7 8191 1 4 91911 4 1 511 5122 #5
#6
O/-11-1 01-1 /O -51-61-4 4 / 4 5 -51-41-5
L R L R
-41-51-6 O/-110
i 1 L 1
-2l-U4 5/46 51415 1 23/20/18 1 O/O/O 1
' 16/17/20 17115/18





























