Embed Size (px)
Citation preview
94
ORIGINAL ARTICLE
Acta Medica Indonesiana - The Indonesian Journal of Internal Medicine
The Value of Fecal Tumor M2 Pyruvate Kinase as a Diagnostic Tool for Colorectal Cancer Screening
Murdani Abdullah, Abdul A. Rani, Marcellus Simadibrata, Ahmad Fauzi, Ari F. SyamDepartment of Internal Medicine, Faculty of Medicine, University of Indonesia - Cipto Mangunkusumo Hospital.Jl. Diponegoro No. 71, Jakarta 10430, Indonesia. Correspondence mail: [email protected].
ABSTRAKTujuan: untuk mengevaluasi kemampuan M2 piruvat kinase tinja sebagai penanda diagnostik untuk
penapisan kanker kolorektal (colorectal cancer – CRC) pada populasi risiko tinggi atau simtomatik. Metode: sebanyak 328 pasien yang menjalani pemeriksaan kolonoskopi elektif direkrut secara konsekutif. Sampel tinja berukuran kacang walnut diambil dari tiap pasien untuk kemudian diuji kandungan M2PK-tumor dengan menggunakan ELISA. Tidak ada pembatasan asupan makan pada pasien. Ahli patologi klinik yang menganalisa kandungan M2PK disamarkan terhadap diagnosis pasien. Kadar tumor M2PK tinja kemudian dibandingkan dengan hasil histopatologis dari biopsi kolorektal. Hasil: dari 328 pasien yang menjalani pemeriksaan kolonoskopi, didapatkan 197 orang (60.1%) lelaki dan 131 orang (39.9%) perempuan. Berdasarkan pemeriksaan histopatologis, 83 (25.3%) pasien memiliki gambaran histologi usus normal, 42 pasien (12.8%) memiliki CRC, 67 pasien (20.4%) pasien memiliki adenoma, 19 pasien (5.8%) memiliki inflammatory bowel disease, 3 pasien (0.9%) memiliki kolitis amuba, dan 114 pasien (34.8%) memiliki kolitis infektif. Batas kadar M2PK-tumor tinja adalah 4.0 U/ml. Sensitivitas, spesifitas, positive predictive value dan negative predictive value secara berurutan adalah 71.4%, 71%, 73.5% dan 94.4%. Didapatkan hubungan yang signifikan antara CRC dengan kadar M2PK-tumor tinja (p<0.001). Uji M2PK mendeteksi adanya 16 tumor di antara 67 kasus (23.9%) adenoma, 8 tumor di antara 19 kasus (42.1%) inflammatory bowel disease, 35 tumor di antara 114 kasus (30.7%) kolitis infektif, dan 2 tumor di antara 3 kasus (66.7%) kolitis amuba. Kesimpulan: uji M2PK-tumor tinja memiliki sensitivitas dan spesifisitas yang baik untuk mendeteksi kasus CRC, terutama pada populasi risiko tinggi atau simtomatik.
Kata kunci: kanker kolorektal, M2PK-tumor tinja, penanda diagnostik, penyaring
ABSTRACTAim: to evaluate the performance of fecal tumor M2 pyruvate kinase (M2PK) as a diagnostic biomarker for
colorectal cancer (CRC) screening in high-risk or symptomatic populations. Methods: consecutive patients (N = 328) who were referred for elective colonoscopy were prospectively enrolled. One walnut-sized stool sample was collected from each patient for analysis of tumor M2PK content using an ELISA kit. No dietary restrictions were applied. The clinical pathologists who conducted the M2PK analyses were blinded to the patients’ confirmed diagnoses. Levels of fecal tumor M2PK were compared with histopathological results from colorectal biopsies. Results: of the 328 patients who underwent colonoscopy examinations, 197 (60.1%) were men and 131 (39.9%) were women. Based on histopathological examination, 83 (25.3%) patients had normal bowel histology, 42 (12.8%) patients had CRC, 67 (20.4%) patients had adenoma, 19 (5.8%) patients had inflammatory bowel disease, three (0.9%) patients had amoebic colitis, and 114 (34.8%) patients had infective colitis. The cutoff level for tumor M2PK concentration was defined as 4.00 U/mL. The sensitivity, specificity, positive predictive value, and negative predictive value of the M2PK test were 71.4%, 71.0%, 73.5%, and 94.4%, respectively. There

Vol 44 • Number 2 • April 2012 The Value of Fecal Tumor M2 Pyruvate Kinase as a Diagnostic Tool
95
INTRODUCTIONColorectal cancer (CRC) is a malignant
disease that constitutes a serious health care problem. According to GLOBOCAN 2002, the worldwide prevalence of CRC is second to that of breast cancer. One million new cases of CRC and 529,000 deaths from CRC were recorded in 2002.1 The GLOBOCAN 2002 database also shows that the incidence of CRC is increasing rapidly in countries where the overall risk of CRC was previously low, especially in Japan and elsewhere in Asia. In high-risk countries, the incidence of CRC has gradually increased, stabilized (North and West Europe), or declined (North America).2 Attenuation of the incidence of CRC over time is particularly evident in the younger age groups (less than 50 years old).
Analysis of data collected between 1985 and 2005 by the Asia-Pacific Working Group on CRC has shown that the incidence of CRC increased by two- to fourfold over this period in many Asian countries, including China, Japan, South Korea, and Singapore. Based on this fact, the Asia-Pacific Working Group on Colorectal Cancer stated that prompt action should be taken to prevent and diagnose CRC as early as possible. One of the actions that should be undertaken is to increase public awareness of CRC screening.3 Routine screening is effective for detecting CRC because it may be present for an extended period before clinical symptoms become evident. This provides clinicians with a window of opportunity for screening, effective intervention, and prevention.4–8 If the cancer is found at an early, preinvasive stage, the 5-year survival rate is about 95%.9–11
The most commonly used screening method for CRC is the fecal occult blood test (FOBT). A meta-analysis in which data from three studies and a Swedish trial were pooled estimated that FOBT screening could reduce CRC mortality by as much as 16%–23%.12 CRC screening using
the FOBT is associated with a high probability of false-positive results, which may be caused by occult blood from nonneoplastic lesions (hemorrhoid, diverticulosis, colitis) or NSAID-associated gastrointestinal bleeding. False-negative results can occur because of bleeding from some carcinomas and most adenomas are occult or intermittent. False-negative results are usually observed with small lesions (less than 1 cm in diameter) or proximal lesions in which globin is degraded before it can appear in the stool. The immunochemical FOBT (iFOBT) is a development of the FOBT that can differentiate between peroxidase and heme in dietary components from human hemoglobin. However, the iFOBT has limitations. Lieberman et al.13 reported that among 3,121 asymptomatic people who underwent colonoscopy, the FOBT was positive for only 23.9% of cases of advanced neoplasia; thus, FOBT failed to detect 76.1% cases of advanced neoplasia.14 In addition, there is increasing demand for a more reliable screening tool for CRC because nonpolypoidal (flat or depressed) lesions and colorectal neoplasm, which develop without a preceding adenoma (i.e., de novo cancer), seem to be more common in Asians than in other populations. There is also a trend towards an increase in the proportion of proximal CRC in several Asian countries.3 These findings stimulated work on the development of a more reliable CRC screening tool that is not affected by the presence of hemoglobin and detects metabolic changes in CRCs cells directly.
The aim of this study was to evaluate the performance of fecal tumor M2 pyruvate kinase (M2PK) as a diagnostic biomarker for CRC screening in high-risk or symptomatic populations. Pyruvate kinase, which converts phosphoenolpyruvate to pyruvate, is a key enzyme in glucose metabolism and is present in organ-specific isoforms (the L, R, M1, and M2 isoforms). In normal proliferating cells, M2PK
was a significant association between CRC and fecal tumor M2PK level (P < 0.001). The M2PK test detected 16 tumors among 67 (23.9%) cases of adenoma, eight tumors among 19 (42.1%) cases of inflammatory bowel disease, 35 tumors among 114 (30.7%) cases of infective colitis, and two tumors among three (66.7%) cases of amoebic colitis. Conclusion: the fecal tumor M2PK test has good sensitivity and specificity for CRC detection, especially in high-risk or symptomatic populations.
Key words: colorectal cancer, fecal tumor M2PK, diagnostic biomarker, screening.

Murdani Abdullah Acta Med Indones-Indones J Intern Med
96
is mainly tetrameric and has a high affinity for phosphoenolpyruvate. In contrast, the M2PK isoenzyme found in tumor cells is usually dimeric and has a low affinity for phosphoenolpyruvate. Dissociation of the tetrameric form to the dimeric form in tumor cells is induced by direct interaction of M2PK with various oncoproteins. For this reason, the dimeric form of M2PK has been named tumor M2PK. Because of its low affinity for phosphoenolpyruvate, tumor M2PK is easily released from tumor cells and is quantitatively detectable in body fluids.15 Tumor M2PK can also be detected and quantified in stool samples using an ELISA.16–18
METHODS
Study ProtocolThree hundred twenty-eight consecutive
patients who were admitted to six centers in Jakarta between August 2009 and April 2010 participated in this study. The samples were collected from six hospitals in Jakarta (Cipto Mangunkusumo Hospital, Abdi Waluyo Hospital, Pluit Hospital, Gading Pluit Hospital, Islam Cempaka Putih Hospital and Mitra Keluarga Kelapa Gading Hospital). These high-risk or symptomatic patients underwent colonoscopy for various indications such as CRC screening, investigation of colonic symptoms, CRC high-risk subject examination, a family history of colorectal neoplasia (CRN), and clinically suspected CRC. Patients who underwent removal surgery or chemotherapy for CRC or polyps were excluded.
One walnut-sized stool sample was collected before preparation of the bowel for the endoscopy procedure or after the colonoscopy when the patient’s stool had become sufficiently firm. A clean plastic container (100 mL) and a plastic spoon were provided for stool sample collection. No dietary restrictions were imposed. The stool sample collection procedure was explained to the patient by the study coordinator or a nurse.
Patients who returned very watery stool samples were asked to collect a firm stool sample. Patients were instructed not to contaminate stool samples with toilet bowl water. Fecal M2PK is stable for 48 hours at room temperature, 72 hours at 4–8 0C, and 1 year at –20 0C. Undiluted stool extracts may be stored without adverse effects for 1 day at 4–8 0C or for 4 weeks at –20 0C.
Clinical history data were recorded on standardized forms. Demographic data (age, sex, ethnicity, and the location size and histology of the CRC) were recorded. The results of histopathological analyses were obtained from patients with neoplastic abnormalities. The location of the most advanced lesion was noted. Irritable bowel disease (IBD) patients were included to investigate the influence of inflammation on fecal tumor M2PK level. Dukes’ stage and tumor node metastasis stage were not determined. The adenomas were classified as nonadvanced or advanced (i.e., an adenoma with significant villous features [>25%], a diameter of 1 cm or more, high-grade dysplasia, or an adenoma containing early invasive cancer).19
The study protocol was approved by the ethics committee of Cipto Mangunkusumo Hospital Faculty of Medicine, University of Indonesia. Written informed consent was obtained from all patients before they were enrolled in the study.
Measurement of Fecal Tumor M2PK Concentrations
Stool extraction was done using the Fecal Tumor M2PK Quick Prep kit (ScheBo Biotech AG, Giessen, Germany). Fecal tumor M2PK level was measured using an ELISA kit (ScheBo Biotech AG) in accordance with the manufacturer’s protocol. The kit was validated for quantification of fecal tumor M2PK levels between 1 U/mL and 30 U/mL; values outside this range are specified as <1 U/mL or >30 U/mL. An M2PK cutoff level of 4 U/mL was used according to the manufacturer’s instructions and other similar studies.16,20 Patients whose fecal tumor M2PK levels were greater than the cutoff level were classified as positive for tumor M2PK.
Statistical AnalysisDescriptive statistics were used to analyze
and report the data. Specificity and sensitivity were calculated using the colonoscopy and histopathology results as references.
RESULTSThe general characteristics of the 328 patients
who underwent colonoscopic examinations between August 2009 and April 2010 are shown in Table 1. The sample consisted of 197 (60.1%) males and 131 (39.9%) females. The ethnicities of the patients were Javanese (42.6%), Chinese (23.5%), Malay (17.4%) and others (16.5%).
Vol 44 • Number 2 • April 2012 The Value of Fecal Tumor M2 Pyruvate Kinase as a Diagnostic Tool
97
Twenty patients (6.1%) had a personal history of malignancy and 42 (12.8%) patients had a family history of malignancy.
The indications for colonoscopic examination were gastrointestinal bleeding (36.0%), abdominal pain (30.5%), change in bowel habits (33.8%), screening (6.4%), and an abdominal mass (4.6%). Hemorrhoids were observed in 241 (73.5%) patients and the colonoscopy findings were colitis, 123 patients (37.5%); polyps, 83 patients (25.3%); tumor, 59 patients (18.0%); IBD, 31 patients (9.5%); and amoebic colitis, seven patients (2.1%). Based on histopathological examination, 83 (25.3%) patients had normal bowel histology, 42 (12.8%) patients had CRC, 67 (20.4%) patients had adenoma, 19 (5.8%) patients had IBD, three (0.9%) patients had amoebic colitis, and 114 (34.8%) patients had infective colitis.
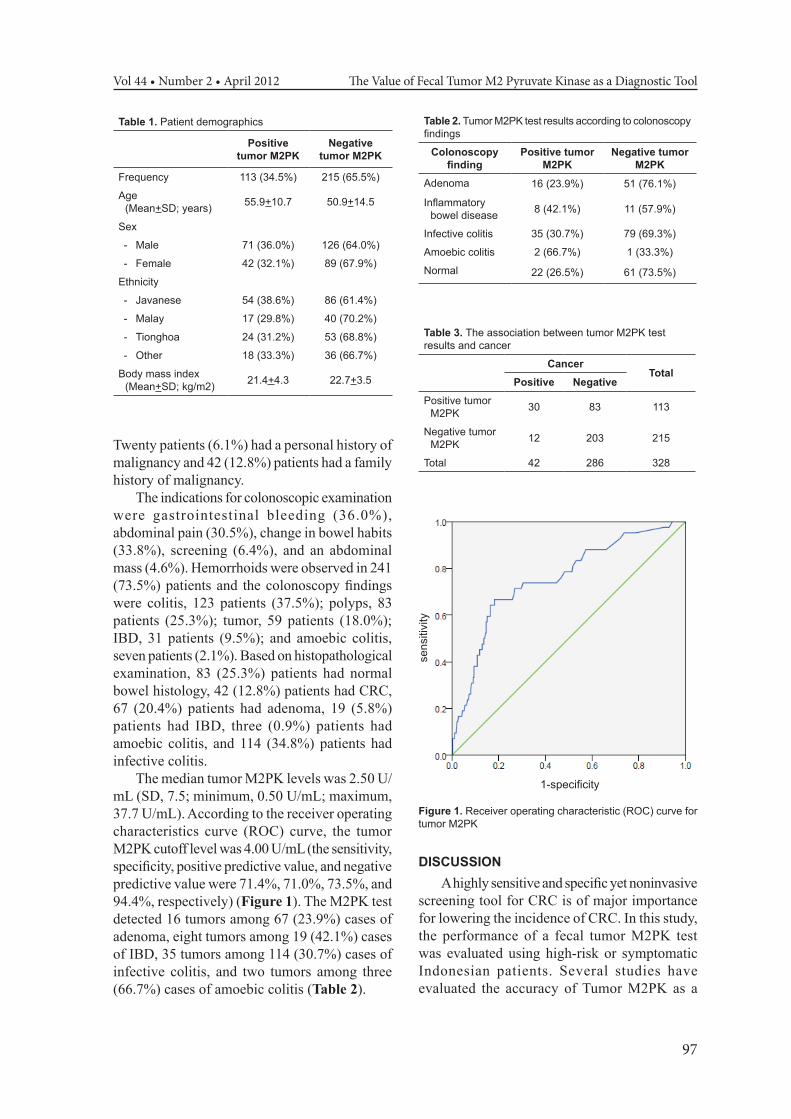
The median tumor M2PK levels was 2.50 U/mL (SD, 7.5; minimum, 0.50 U/mL; maximum, 37.7 U/mL). According to the receiver operating characteristics curve (ROC) curve, the tumor M2PK cutoff level was 4.00 U/mL (the sensitivity, specificity, positive predictive value, and negative predictive value were 71.4%, 71.0%, 73.5%, and 94.4%, respectively) (Figure 1). The M2PK test detected 16 tumors among 67 (23.9%) cases of adenoma, eight tumors among 19 (42.1%) cases of IBD, 35 tumors among 114 (30.7%) cases of infective colitis, and two tumors among three (66.7%) cases of amoebic colitis (Table 2).
Table 1. Patient demographics
Positive tumor M2PK
Negative tumor M2PK
Frequency 113 (34.5%) 215 (65.5%)
Age (Mean+SD; years) 55.9+10.7 50.9+14.5
Sex
- Male 71 (36.0%) 126 (64.0%)
- Female 42 (32.1%) 89 (67.9%)
Ethnicity
- Javanese 54 (38.6%) 86 (61.4%)
- Malay 17 (29.8%) 40 (70.2%)
- Tionghoa 24 (31.2%) 53 (68.8%)
- Other 18 (33.3%) 36 (66.7%)
Body mass index (Mean+SD; kg/m2) 21.4+4.3 22.7+3.5
Table 2. Tumor M2PK test results according to colonoscopy findings
Colonoscopy finding
Positive tumor M2PK
Negative tumor M2PK
Adenoma 16 (23.9%) 51 (76.1%)
Inflammatory bowel disease 8 (42.1%) 11 (57.9%)
Infective colitis 35 (30.7%) 79 (69.3%)
Amoebic colitis 2 (66.7%) 1 (33.3%)
Normal 22 (26.5%) 61 (73.5%)
Table 3. The association between tumor M2PK test results and cancer
CancerTotal
Positive NegativePositive tumor
M2PK 30 83 113
Negative tumor M2PK 12 203 215
Total 42 286 328
sensitiv
ity
1-specificity
Figure 1. Receiver operating characteristic (ROC) curve for tumor M2PK
DISCUSSIONA highly sensitive and specific yet noninvasive
screening tool for CRC is of major importance for lowering the incidence of CRC. In this study, the performance of a fecal tumor M2PK test was evaluated using high-risk or symptomatic Indonesian patients. Several studies have evaluated the accuracy of Tumor M2PK as a

Murdani Abdullah Acta Med Indones-Indones J Intern Med
98
CRC screening tool. It was shown that fecal tumor M2PK is more accurate for CRC screening than serum or plasma tumor M2PK.16,21–23 The sensitivity and specificity of fecal tumor M2PK in previous studies ranged from 69% to 85% and from 65% to 93%, respectively.24,25 The sensitivity and specificity of the fecal tumor M2PK test evaluated in this study (71.4% and 71.0%, respectively) were within the range of reported values. In addition, there was significant association between CRC and fecal tumor M2PK level (P < 0.000).
The cutoff value for fecal tumor M2PK levels was defined as 4 U/mL, as recommended by the manufacturer and other similar studies.16,20 However, further study with larger number of patients and a more adequate stool sample size is needed to determine the most appropriate cutoff value for CRC in the Indonesian population. This can be accomplished by comparing the predictive value of fecal tumor M2PK level over a wide range of cutoff values using ROC curve analysis.
We observed that fecal tumor M2PK had low sensitivity for detecting adenomas. Shastri et al.24,25 and Mulder et al.26 showed that the sensitivity of fecal tumor M2PK for detection of adenomas is between 25.8% and 37.7% (cutoff value >4 U/mL). The iFOBT also has a low sensitivity for detecting adenomas (30–40%).24–26 The sensitivity of fecal tumor M2PK level for detecting adenomas should be evaluated using a larger sample size. Recent studies suggest that inflammatory reactions in the bowel can cause an elevation in fecal tumor M2PK level.24–26 In our study, eight of 19 patients with IBD (42.1%) had positive M2PK test results. Most IBD patients with positive results had colitis IBD. Colitis IBD is a risk factor for the development of CRC. It is possible that IBD patients with positive fecal tumor M2PK test results also had ulcerative colitis associated with a neoplastic premalignant process.27 The iFOBT also showed a high positivity rate in IBD patients, which is consistent with Mulder et al.26 They reported that of IBD patients, 79% were positive according to the fecal tumor M2PK and iFOBT immoCARE tests and 89% were positive according to the iFOBT OC-Light test.26 Further study with a follow-up is needed to determine the positivity rate of the fecal tumor M2PK test for ulcerative colitis-associated neoplasia.
False-negative results may have been produced in our study because of dilution of stool samples with toilet bowl water. Positive results in patients with normal colonoscopy results (22/83 patients; 26.5%) may have been caused by inflammation, which could have been detected by microscopic examination. Therefore, further studies using several CRC diagnostic tools are required. Shastri et al.25 showed that 26.2% of normal subjects, including patients with irritable bowel syndrome, (135/156; cutoff value >4 U/mL) had positive fecal tumor M2PK test results.
Cancer cells have higher rates of glucose uptake than normal cells. However, only a small fraction of the glucose taken up is used for oxidative phosphorylation. The decrease in aerobic glycolysis in these cells may be due to reprogramming of metabolic genes, enabling cancer cells to partition glucose metabolites away from oxidation towards the synthesis of macromolecules. In cancer cells, M2PK regulates the balance between the synthesis of ATP and macromolecules (fatty acids and nucleic acids). M2PK is crucial for rapid tumor growth and aerobic glycolysis during tumorigenesis.28,29 Therefore, M2PK can be used as a noninvasive biomarker and a diagnostic tool for the detection of cancer. M2PK level may also be of use for prognostic purposes because a proteomic study revealed that M2PK expression is predictive of patient response during treatment oxaliplatin.30
CONCLUSIONFecal tumor M2PK has potential as a
screening diagnostic biomarker for CRC and has high overall sensitivity and acceptable specificity. It is expected that the tumor M2PK test will be more specific for cancer than the iFOBT. The specificity of the fecal tumor M2PK test is acceptable for screening diagnostic purposes because the positivity rate in IBD patients was less than that reported for other tests.24–26
ACKNOWLEDGEMENTS
We acknowledge the Directorate for Research and Public Service of the University of Indonesia for supporting the study. We thank all the gastroenterologists who recruited patients and performed the endoscopy procedures and the clinical pathologists who examined the samples.

Vol 44 • Number 2 • April 2012 The Value of Fecal Tumor M2 Pyruvate Kinase as a Diagnostic Tool
99
We thank Vita Kurniati Lubis, MD, PhD., Vinci Lorensia, MD., Aan Santi, BSc., and Cecilia Anggraini, MSc., for their support and assistance in managing, analyzing, and compiling the data and Irwin Tedja, MD for editing the manuscript.
REFERENCES1. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer
statistics, 2002. CA Cancer J Clin. 2005;55:74–108. 2. Parkin DM, Bray F, Devesa S. Cancer burden in the year
2000: the global picture. Eur J Cancer. 2001;37:S4–S66.
3. Sung JJY, Lau JYW, Goh KL, Leung WK. Increasing incidence of colorectal cancer in Asia: implications for screening. Lancet Oncol. 2005;6:871–6.
4. Morson B. The polyp-cancer sequence in the large bowel. Proc R Soc Med. 1974;67:451–7.
5. Fearon ER, Vogelstein B. A genetic model for colorectal tumorigenesis. Cell. 1990;61:759–67.
6. Winawer SJ, Zauber AG, O’Brien MJ. Randomized comparison of surveillance intervals after colonoscopic removal of newly diagnosed adenomatous polyps. N Engl J Med. 1993;328:901–6.
7. Winawer SJ, Zauber AG, Ho MN, et al. The National Polyp Study Workgroup. Prevention of colorectal cancer by colonoscopic polypectomy. N Engl J Med. 1993;329:1977–83.
8. Lieberman DA. Cost-effectiveness model for colon cancer screening. Gastroenterol. 1995;109:1781–90.
9. Jemal A, Tiwari RC, Murray T, et al. Cancer statistics, 2004. CA Cancer J Clin. 2004;54:8–29.
10. Peeters M, Haller DG. Therapy for early stage colorectal cancer. Oncol. 1999;13:307–15.
11. Burt RW. Colon cancer screening. Gastroenterol. 2000;119:837–53.
12. Towler B, Irwig L, Glasziou P, et al. A systemic review of the effects of screening for colorectal cancer using the faecal occult blood test, hemoccult. BMJ. 1998;317:559–65.
13. Lieberman DA, Weiss DG, Bond JH, et al. Use of colonoscopy to screen asymptomatic adults for colorectal cancer. Veterans Affairs Cooperative Group 380. N Engl J Med. 2000;343:162–8.
14. Lieberman DA, Weiss DG. One-time screening for colorectal cancer with combined fecal occult blood testing and examination of the distal colon. Veterans Affairs Cooperative Group 380. N Engl J Med. 2001; 345:555–60.
15. Mazurek S, Boschek CB, Hugo F, Eigenbrodt E. Pyruvate kinase type M2 and its role in tumor growth and spreading. Semin Cancer Biol. 2005;15:300–8.
16. Hardt PD, Mazurek S, Toepler M, et al. Faecal tumour M2 pyruvate kinase: a new sensitive screening tool for colorectal cancer. Br J Cancer. 2004;91:980–4.
17. Naumann M, Schaum B, Oremek GM, et al. Faecal pyruvate kinase type M2 - a valid screening parameter for colorectal cancer? Preliminary results from a multicenter comparative study. Dtsch Med Wochenschr. 2004;129:1806–7.
18. Tonus C, Neupert G, Sellinger M. Colorectal cancer screening by noninvasive metabolic biomarker fecal tumor M2PK. World J Gastroenterol. 2006;12:7007–11.
19. Winawer SJ, Zauber AG, O’Brien MJ, et al. Randomized comparison of surveillance intervals after colonoscopic removal of newly diagnosed adenomatous polyps. The National Polyp Study Workgroup. N Engl J Med. 1993;328:901–6.
20. Vogel T, Driemel C, Hauser A, et al. [Comparison of different stool tests for the detection of cancer of the colon.] Dtsch Med Wochenschr. 2005;130:872–7.
21. Hardt PD, Toepler M, Ngoumou B, Rupp J, Kloer HU. Measurement of fecal pyruvate kinase type M2 (tumor M2PK) concentrations in patients with gastric cancer, colorectal cancer, colorectal adenomas and controls. Anticancer Res. 2003;23:851–3.
22. Zhang B, Chen JY, Chen DD, Wang GB, Shen P. Tumor type M2 pyruvate kinase expression in gastric cancer, colorectal cancer and controls. World J Gastroenterol. 2004;10:1643–6.
23. Hardt PD, Ngoumou BK, Rupp J, Schnell-Kretschmer H, Kloer HU. Tumor M2-pyruvate kinase: a promising tumor marker in the diagnosis of gastro-intestinal cancer. Anticancer Res. 2000;20:4965–8.
24. Shastri YM, Naumann M, Oremek GM, et al. Prospective multicenter evaluation of fecal tumor pyruvate kinase type M2 (M2PK) as a screening biomarker for colorectal neoplasia. Int J Cancer. 2006;119:2651–6.
25. Shastri YM, Loitsch S, Hoepffner N, et al. Comparison of an established simple office-based immunological FOBT with fecal tumor pyruvate kinase type M2 (M2PK) for colorectal cancer screening: Prospective multicenter study. Am J Gastroenterol. 2008;103:1496–504.
26. Mulder S, Van Leerdamb ME, Van Vuurenb, et al. Tumor pyruvate kinase isoenzyme type M2 and immunochemical fecal occult blood test: performance in screening for colorectal cancer. Eur J Gastroenterol Hepatol. 2007;19:878–82.
27. Hardy RG, Meltzer SJ, Jankowski JA. ABC of colorectal cancer: Molecular basis for risk factors. Br Med J. 2000;321:886–9.
28. Christofk HR, Heiden MGV, Wu N, Asara JM, Cantley LC. Pyruvate kinase M2 is a phosphotyrosine-binding protein. Nature. 2008;452:181–6.
29. Christofk HR, Heiden MGV, Harris MH, et al. The M2 splice isoform of pyruvate kinase is important for cancer metabolism and tumour growth. Nature. 2008;452:230–3.
30. Balibrea EM, Plasencia C, Gines A, et al. A proteomic approach links decreased pyruvate kinase M2 expression to oxaliplatin resistance in patients with colorectal cancer and in human cell lines. Mol Cancer Ther. 2009;8:771–8.