Embed Size (px)
Citation preview

Vosmar et al, The value of ultrasonic placental grading 137
J. Perinat. Med.17 (1989) 137
The value of ultrasonic placental grading: No correlation with intra-uterine growth retardation or with maternal smoking
Mieke B. J. G. Vosmar, Henk W. Jongsma, and Pieter W. J. van Dongen
Department of Obstetrics and Gynecology, University Hospital St. Radboud,Nijmegen, The Netherlands
1 Introduction
For some years now, ultrasound has taken its placein the daily practice of prenatal care by obstetri-cians. Initially it was used as a method to assessgestational age and placental localization. Becauseof improvement of the technical equipment it alsobecame possible to observe fetal behaviour in vivo.Ultrasound created the possibility to evaluate theplacental tissue and its structure.The first echoscopic description in placental tissueis from 1973 [28]: a distinction was made betweenhomogenic and irregular placentae, which con-tained rounded transonic areas. Later specificchanges in placental tissue were observed as preg-nancy progressed [6]. A useful grading system (fig-ures 1 and 2) was developed describing these ul-trasonic changes of the placenta [8]. Originally theplacental grading system was used as method ofpredicting fetal lung maturity. A 100% correlation[8, 19] was found between a Grade III placentaand a mature Lecithin/Sphingomyelin ratio. Whenother investigators [2, 5, 10, 13, 21, 24, 25] foundGrade III placentae in women, where accordingto the immature L/S ratio or negative phosphati-dylglycerol (PG) no fetal lung maturity could exist,more attention was paid to the possible relationbetween premature appearance of Grade IIIchanges in placental tissue and intrauterine growthretardation (IUGR). Placentae of newborn infantswho are small-for-gestational age (SGA) showmore ischemic lesions (fibrin and calcium deposi-tions, infarcts) [1, 3, 26] than those in placentaeof neonates who are appropriate for gestationalage (AGA). Combined histological, radiologicaland ultrasound examination of the placentashowed that ultrasonic densities are caused by
Curriculum vitae
MDEKE B. J. G. VOSMARwas born in Ammerzoden,Holland. She studied me-dicine at the University ofNijmegen. During herstudy she spent half a yearas student-doctor in Tan-zania. From 1985 to 1987she worked at the St. Rad-boud University Hospitalin Nijmegen. In 1988 shestarted her residency inObstetrics and Gynecology at the Groot Ziekengasthuis,'s-Hertogenbosch.
reticular calcification and fibrinoid degeneration[6, 8, 9, 12, 26]. Therefore one would expect anassociation between Grade III placentae andIUGR. Several studies pointed out the relationbetween the occurrence of a 'premature' Grade IIIand IUGR [6, 8, 9, 18, 20-23]. Kazzi et al. [14,15] investigated the predictive value of a GradeIII placenta in the growth-retarded fetus. A sig-nificant relationship was seen between a Grade IIIplacenta and a SGA infant in a full term high-riskpregnancy group.In order to study the usefulness of the placentalgrading by ultrasound, we decided to study thisgrading versus the outcome of the pregnancy, es-pecially the occurrence of intrauterine growth re-tardation. Also the effect of smoking on pregnancywas evaluated, in order to investigate the possiblerelation between smoking and placental grading.
1989 by Walter de Gruyter & Co. Berlin · New York

138 Vosmar et al, The value of ultrasonic placental grading
GRADE 0
UTERINEWALL
SMOOTHCHORIONICPLATE
CORDINSERTION
(T)
PLACENTALSUBSTANCE
GRADE I
ECHOGENIC AREASRANDOMLY DISPERSED
IN PLACENTALSUBSTANCE
SUBTLE INDENTATIONS -OF CHORIONIC PLATE '
GRADE Π GRADE
BASAL ECHOGENICENSITIES
ECHOSPARED ORFALLOUT AREAS
UTERINEWALL
UTERINEWALL
COMMA LIKEDENSITIES
©INDENTATIONSOF CHORIONIC
PLATE
IRREGULARDENSITIESWITH ACOUSTICSHADOWING
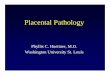
Figure 1. Schematic diagram illustrating the ultrasonic appearance of the four placental grades. (Reproduced withpermission from Grannum [8]).
2 Material and methods
During September and October 1984, echoscopicobservations were made in patients from a mini-mum of 26 weeks amenorrhoe onwards. Thesepregnant women were recruited from the outpa-tient department of Obstetrics of the St. RadboudUniversity Hospital Nijmegen. All pregnantwomen planned to deliver within our investigationperiod were included.The same two observers examined each patientwith a Toshiba linear array realtime scanner witha 3.5 MHz transducer. Patients who deliveredwithin one week after examination were taken intothis survey (n = 137). An anterior or posteriorplacental location was noted when more than two-thirds of the placental width was seen on theanterior or posterior uterine wall, respectively. Theplacenta was in a fundal location when in verticalplane one half of the placenta was on the anteriorand the other half on the posterior wall of theuterus.
The placenta was ultrasonically graded accordingto the system described by Grannum et al. [8],Whenever possible the entire placenta was evalu-ated. If in two different parts of the placenta twodifferent grades were seen, the most mature partwas noted.Unaware of the given ultrasonic grade, all placen-tae were macroscopically examined and describedwithin 24 hours post partum in a standardizedway. The following grading system was used, pre-suming that the macroscopic structures are grosslycomparable with the ultrasonic structures:
Grade 0: no calcium or fibrinoid depositions wereseen and the placental surface was smooth.
Grade 1: some diffuse calcium and fibrinoid dep-osition.Grade 2: beginning formation of septa, at thematernal side clear calcium deposition.
J. Perinat. Med. 17 (1989)

Vosmar et al, The value of ultrasonic placental grading 139
Ο
l GRADE M
Figure 2. Ultrasonic appearance of the four placental grades.
Grade 3: cotyledons are present, a great numberof calcium and flbrinoid deposition at the mater-nal and fetal sides, with infarcts and 'holes' bysectioning.The smoking habit of each patient in every trimes-ter was noted. A distinction was made betweennon-smokers, mild (< 10 cigarettes daily), mod-erate (10 — 20 cigs/day) and heavy smokers (> 20cigs/day).In evaluating the relation between a Grade III andIUGR, a neonate was called SGA whose birthweight was less than the tenth birth weight per-centile for the Dutch population, when gestationalage, infant sex and parity were taken into consid-eration [16].Statistical analysis was performed by means ofStudent's t, analysis of variance, Spearman rankcorrelation or X2 tests. A p of < 0.05 was consid-ered to be significant.
3 ResultsA total of 595 ultrasonic evaluations of 176 pa-tients were made within a period of 8 weeks.Patients seen within one week before delivery weretaken into the study; 137 patients entered thissurvey and 39 patients were excluded due to notyet been delivered (n = 28), the last ultrasonicexamination was more than one week prior todelivery (n = 7), ungradable placentae (n = 3) orbecause of unknown term (n = 1). In these 137patients 466 examinations were made. The earliestgestational age was 26 weeks, the latest 43 weeks.All patients were seen every time they visited theoutpatients department or weekly when they wereadmitted in the wards. The maximum of exami-nations performed in one patient was 7.
In 53.3% (73/137) the placenta could entirely beevaluated on ultrasonic examination. In the re-maining group not all parts of the placenta could
J. Perinat. Med. 17 (1989)

140 Vosmar et al, The value of ultrasonic placental grading
be seen, but enough to be graded. Separate anal-ysis of the two groups showed no statistical dif-ferences in the results of this study. Therefore, the137 subjects were considered as belonging to onegroup only. Of the 137 patients in our study, 76(55.5%) had an anterior, 46 (33.6%) a posteriorplacental location and 14 (10.2%) had a fundalplacenta. Placental morphology and placentalgrading were significantly correlated (Spearmanrank correlation coeff. 0.77, p = 0.0001). Therewas an agreement between placental grading andplacental morphology with an accuracy of 80.5%(table I).
Table I. Correlation of macroscopic examination postpartum and placental grading.
Placental morphology
PERCENTAGE OF PLACENTA GRADE II AND I I I -C W I T H 95% CONFIDENCE INTERVAL)
Placentalgrade
0IIIIII
0
10000
1
22600
2
25
163
3
292
51
unknown*
0331
correct
62.5%65.0%88.9%94.4%
Accuracy 80.5%
* accidentally destroyed
In this study population a significant relationshipwas found between increasing placental gradingand gestational age (figure 3). In all five cases ofpost datism (gestational age > 42 weeks) a GradeIII was seen. In 57 cases (41.6%) pregnancy endedwith a Grade III placenta; only five before 37weeks of gestational age and five times after 42weeks. Thus the incidence of Grade III placentaat term was 34% (47/137).Comparing the Grade III placenta group with thenon-Grade III placenta group, no significant as-sociation could be found in the prevalence of chil-dren who were small-for-gestational age (table II).Thus no predictive value was present for a GradeIII placenta and a subsequent SGA-delivery. How-ever, three out of five cases before 35 weeks ofpregnancy with a Grade III placenta showed anIUGR.Placental grading and smoking. There were 134pregnancies with known smoking habits in everytrimester. Data on birth weight, placental weightand placental ratio (placental weight/birth weight)are given in table III.
38 40 42GESTATIONAL AGE CWEEKSD
Figure 3. The relation between placental grading andincreasing gestational age, for grades II and III only.
Table Π. Contingency table showing Grade III placentain relation with IUGR (SGA, p < 10).
Placental grade SGA AGA Total
Grade IIINon-Grade III
Total
711
18
5069
119
5780
137
X2 = 3.5, ρ = 0.32 (not significant)SGA = small for gestational ageAGA = appropriate for gestational age
Table ΠΙ. The effect of mothers smoking habit on birthweight, placental weight and placental ratio (n = 134).
Smoking habit η Mean birth* Mean pla- Placen-weight (g) cental** tal***
weight (g) ratio
Non-smokers< 10 cigs/day10-20 cigs/day> 20 cigs/day
7518329
3408321330743167
(536)(589)(613)(379)
507446473512
(106)(97)(93)
(103)
0.1490.1400.1560.161
0^ standard deviation* ρ = 0.03; ** ρ = 0.08, *** ρ = 0.06 (one way analysisof variance)
The sample showed 44% smokers. The mean birthweight decreased significantly the more theysmoked (p = 0.03), but there was no significantdifference among the mean placental weights andplacental ratio. In comparing the placental ratios,a trend could be detected (p = 0.06) that as theamount of smoking increased, the placental ratioincreased as well.
J. Perinat. Med. 17 (1989)

Vosmar et al, The value of ultrasonic placental grading 141
The effect of smoking on birth weight may becomplicated by differences in age, parity, sex andgestational age between the three smoking groups.Regarding both gestational age and maternal agethere was no difference between these threegroups. To eliminate the effects of sex and parityon birth weight, the effect of smoking or notsmoking on the birth weight percentile was eval-uated (table IV). If the pregnant woman smokedthen the birth weight percentile decreased signifi-cantly (p = 0.0008).No relation was found between the effect of smok-ing on placental grading (table V) (Spearman rankcorrelation coefficient 0.007; p = 0.93).
Table IV. The effect of smoking on the birth weightpercentile.
Birth weightpercentile
<plOplO-p50>p50Total
non-smokersn
6234675
smokersn
11311759
X2 = 14.3, p = 0.0008
Table V. Effect of smoking on placental grading(n = 134).
Placental grading
Smoking habit 0 I II III Total
Non-smokers< 10 cigs/day^10 cigs/day
1015
248
10
749
345
17
751841
pared to other studies (15% [8], 20% [11]), couldbe related to the strict criteria kept in this studyfor the determination of the placental grade ac-cording to Grannum [7]. In spite of those criteria,placental grading still remains a subjective inter-pretation of an echoscopic picture; accurate in-struction and interpretation is necessary.
Post partum examination of the placentae corre-lated well with the ultrasound grading, so theultrasonic image is likely to be the in vivo repre-sentation of the placenta.Much value has been attributed to the ultrasoundassessment of the biophysical profile to improvethe quality of perinatal care [17]. As an extra itemVintzileos et al. [27] added the placental gradingto the biophysical profile. Key finding in our sur-vey is that ultrasonic determination of a Grade IIIplacenta at term is not helpful in predicting IUGR.However, one may suggest that the prematureoccurrence of Grade III placenta might predictIUGR.There have been many reports on the effect ofsmoking in pregnant women, proving that smok-ing causes growth retardation of the fetus. We canconfirm this observation. The relation betweensmoking and placental weight is more controver-sial. Christianson [4] found a striking higher pre-valence of calcification and subchorionic fibrindeposits in the placentae of smokers as comparedto non-smokers. The placentae of smokers werealso heavier. These and other observations suggestthat in placentae of smokers an acceleration existsof the normal aging process of the placenta. Asincreasing placental grading represents the normalmaturation process of the placenta, a relation wasexpected between the amount of cigarette con-sumption and placental grading. This couldn't beconfirmed, may be due to the small number ofheavy smokers.
4 Discussion
In this prospective study the placental grade wascorrelated with the outcome of pregnancy in orderto determine its usefulness for predicting IUGR.Previous reports were concentrated upon high riskpatients. In this survey an unselected high and lowrisk population was investigated.Changes in placental tissue increased clearly aspregnancy progressed and 42% (57/137) of theplacentae reached Grade III. The discrepancy inthe incidence of Grade III at term (34%), com-
5 Conclusions
1. Increasing placental grading is associated withnormal maturation of the placenta.
2. In an unselected term group there is no relationbetween Grade III placenta and IUGR.
3. Smoking correlates well with a decrease in birthweight, but not with an accelerated placentalgrading.
J. Perinat. Med. 17 (1989)

142 Vosmar et al, The value of ultrasonic placental grading
Summary
In a prospective study the usefulness of placental gradingin detecting IUGR has been evaluated. Those who wereechoscopically examined within one week before deliverywere taken into the study (n = 137). Changes in placen-tal tissue increased clearly as pregnancy progressed andin 42% (57/137) the placentae reached Grade III. In-creasing placental grading is associated with normalmaturation of the placenta. Post partum examination ofthe placenta correlated well with the echoscopic picture(accuracy = 80.5%). No relationship was found in anunselected group between Grade III and IUGR at term.
When a Grade III placenta was first seen before 36weeks, in three out of five cases a growth retardedneonate was born.The effects of maternal smoking habits during pregnancyon birth weight and placenta were examined. There wereno significant differences in mean placental weight, pla-cental ratio and placental grading as the amount ofcigarettes increased. The mean birth weight and birthweight percentile decreased significantly when themother smoked more than 10 cigarettes per day.
Keywords: Intrauterine growth retardation, placental grading, smoking, ultrasound.
Zusammenfassung
Sonographisches Grading der Plazenta: keine Korrelationmit intrauteriner Wachstumsretardierung oder mütterli-chem RauchenIn einer prospektiven Studie wurde untersucht, ob einGrading der Plazenta zur Aufdeckung einer intrauteri-nen Wachstumsretardierung (IUGR) sinnvoll ist. Alleinnerhalb einer Woche vor Entbindung sonographischuntersuchten Patientinnen wurden in die Studie aufge-nommen (n = 137). Veränderungen des Plazentagewebesnahmen mit fortschreitendem Schwangerschaftsalterdeutlich zu und in 42% (57/137) erreichte die PlazentaGrad III. Die Zunahme des Gradings ist mit der nor-malen Reifung der Plazenta assoziiert. Untersuchungender Plazenta post partum korrelierten gut mit dem so-
nographischen Bild (Genauigkeit = 80.5%). In einemunselektierten Kollektiv zeigte sich kein Zusammenhangzwischen einem Grad III und einer IUGR am Termin.Wurde eine Plazenta mit Grad III vor der 36. Schwan-gerschaftswoche gesehen, kam es in drei von fünf Fällenzur Geburt eines wachstumsretardierten Neugeborenen.Wir untersuchten die Auswirkungen von mütterlichemRauchen während der Schwangerschaft auf das Geburts-gewicht und die Plazenta. Eine Zunahme des Nikotin-abusus beeinflußte das mittlere Plazentagewicht, die Pla-zenta-Ratio sowie das plazentare Grading nicht signifi-kant. Es kam jedoch zu einem deutlichen Abfall desmittleren Geburtsgewichtes und der Geburtsgewichts-perzentile bei mehr als 10 Zigaretten pro Tag.
Schlüsselwörter: Intrauterine Wachstumsretardierung, plazentares Grading, Rauchen, Ultraschall.
Resume
Valeur du grading placentaire echographique: absence decorrelation avec le retard de croissance intra-uterin et avecle tabagisme maternelOn a evalue dans une etude prospective Futilite d'unclassement placentaire pour le depistage du RCIU.Ont etc pris dans Fetude des patientes qui avaient subiune echographie au cours de la derniere semaine prece-dant Faccouchement (n: 137). II y a une augmentationdes modifications du tissu placentaire avec Fevolutionde la grossesse et dans 42% des cas (57/137) les placentasattaignent le grade III.L'augmentation du grade placentaire s'accompagned'une maturation normale du placenta. L'examen post-partum du placenta est bien correle avec les imagesechographicques (fiabilite: 80,5%).
On n'a pas trouve de correlation dans un groupe nonselectionne entre le grade III et le RCIU ä terme.Lorsqu'un placenta de grade III est observe avant la 36eme semaine, dans 3 des 5 cas, il y a eu naissance d'unenfant hypotrophique.On a examine les effets tu tabagisme maternel pendantla grossesse sur le poids de naissance et sur le placenta.II n'y pas de differences significatives entre le poidsplacentaire moyen, le ratio placentaire et le grade pla-centaire, avec Felevation du nombre de cigarettes,Le poids de naissance moyen et le percentile du poidsde naissance diminuent de facon significative lorsque lamere fume plus de 10 cigarettes par jour.
Mots-cles: Classification placentaire, retard de croissance intra uterin, tabagisme, ultrasons.
J. Perinat. Med. 17 (1989)

Vosmar et al, The value of ultrasonic placental grading 143
References
[1] ALTSHULER G, P RÜSSEL, R ERMOCILIA: The pla-cental pathology of small-for-gestational age in-fants. Am J Obstet Gynecol 121 (1975) 351
[2] ASHTON SS, MP Russo, NV SIMON, DM SHEARER:Relationship between Grade III placentas and bi-parietal diameter determinations. J UltrasoundMed 2 (1983) 127
[3] BERNISCHKE K: Examination of the placenta. ObstetGynecol 18 (1961) 309
[4] CHRISTIANSON RE: Gross differences observed inthe placentas of smokers and nonsmokers. Am JEpidemiol 110 (1979) 178
[5] CLAIR MR, E ROSENBERG, D TEMPKIN, RF AN-DREOTTI, JD BOWIE: Placental grading in the com-plicated or high-risk pregnancy. J Ultrasound Med2 (1983) 297
[6] FISHER CC, W GARRETT, G KOSSOFF: Placental ag-ing monitored by gray scale echography. Am JObstet Gynecol 124 (1976) 483
[7] GRANNUM PAT: Ultrasound examination of the pla-centa. Clinics in Obstetrics and Gynecology 10(1983) 459
[8] GRANNUM PAT, RL BERKOWITZ, JC HOBBINS: Theultrasonic changes in the maturing placenta andtheir relation to fetal pulmonic maturity. Am JObstet Gynecol 133 (1979) 915
[9] HANEY AF, WS TROUGHT: The sonolucent placentain high-risk obstetrics. Obstet Gynecol 55 (1980) 38
[10] HARMAN CR, FA MANNING, E STEARNS, I MORRI-SON: The correlation of ultrasonic placental gradingand fetal pulmonary maturation in five hundredsixty-three pregnancies. Am J Obstet Gynecol 134(1982) 941
[11] HILL LM, R BRECKLE, MW RAGOZZINO, KR WOLF-GRAM, PC O'BRIEN: Grade 3 placentation: Incidenceand neonatal outcome. Obstet Gynecol 61 (1983)728
[12] UWAMOTO VM, T HASHIMOTO, T TSUZAKI, KMAEDA: Ultrasonographic study of the placenta invitro. Gynecol Obstet Invest 11 (1980) 265
[13] KAZZI GM, TL GROSS, MG ROSEN, NY JAATOUL-KAZZI: The relationship of placental grade, fetallung maturity and neonatal outcome in normal andcomplicated pregnancies. Am J Obstet Gynecol 148(1984) 54
[14] KAZZI GM, TL GROSS, RJ SOKOL: Fetal biparietaldiameter and placental grade: Predictors of intra-uterine growth retardation. Obstet Gynecol 62(1983) 755
[15] KAZZI GM, TL GROSS, RJ SOKOL, NJ KAZZI: De-tection of intrauterine growth retardation: a newuse for sonographic placental grading. Am J ObstetGynecol 145 (1983) 733
[16] KLOOSTERMAN GJ: De voortplanting van de mens.Centen. Haarlem 1977
[17] MANNING FA, LD PLATT, L SIPOS: Antepartumfetal evaluation. Development of a fetal biophysicalprofile score. Am J Obstet Gynecol 136 (1980) 787
[18] PATTERSON RM, RH HAYASHI, D CAVAZOS: Ultra-sonographically observed early placental matura-tion and perinatal outcome. Am J Obstet Gynecol147 (1983) 773
[19] PETRUCHA RA, SH GOLDE, LD PLATT: Real-timeultrasound of the placenta in assessment of fetalpulmonic maturity. Am J Obstet Gynecol 142(1982) 463
[20] PETRUCHA RA, LD PLATT: Relationship of placen-tal grade to gestational age. Am J Obstet Gynecol144 (1982) 733
[21] QUINLAN RW, AC CRUZ: Ultrasonic placental grad-ing and fetal pulmonary maturity. Am J ObstetGynecol 142 (1982) 110
[22] QUINLAN RW, AC CRUZ, WC Bum, M MARTIN:Changes in placental ultrasonic appearance. I. In-cidence of Grade III changes in the placenta incorrelation to fetal pulmonary maturity. Am J Ob-stet Gynecol 144 (1982) 468
[23] QUINLAN RW, AC CRUZ, WC Bum, M MARTIN:Changes in placental ultrasonic appearance. II.Pathologic significance of Grade III placentalchanges. Am J Obstet Gynecol 144 (1982) 471
[24] RAGOZZINO MW, LM HILL, R BRECKLE, RD EL-LEFSON, RC SMITH: The relationship of placentalgrade by ultrasound to markers of fetal lung ma-turity. Radiology 148 (1983) 805
[25] TABSH KMA: Correlation of real-time ultrasonicplacental grading with amniotic fluid lecithin/sphin-gomyelin ratio. Am J Obstet Gynecol 145 (1983)504
[26] VANDENBERGHE K: Ultrasonography of the pla-centa. J Perinat Med (Suppl 1) 9 (1981) 75
[27] VINTZILEOS AM, WA CAMPBELL, CJ INGARDIA, DJNOCHIMSON: The fetal biophysical profile and itspredictive value. Obstet Gynecol 62 (1983) 271
[28] WINSBERG F: Echographic changes with placentalageing. J Clin Ultrasound 1 (1973) 52
Received April 3,1987. Revised November 11,1988.Accepted January 12, 1989.
M. B. J. G. VosmarDepartment of Obstetrics and GynaecologySt. Radboud HospitalP.O. Box 91016500 HB NijmegenThe Netherlands
J. Perinat. Med. 17 (1989)