Embed Size (px)
Citation preview

REVIEW
The vascular depression hypothesis: mechanisms linking vasculardisease with depressionWD Taylor1, HJ Aizenstein2 and GS Alexopoulos3
The ‘Vascular Depression’ hypothesis posits that cerebrovascular disease may predispose, precipitate or perpetuate some geriatricdepressive syndromes. This hypothesis stimulated much research that has improved our understanding of the complexrelationships between late-life depression (LLD), vascular risk factors, and cognition. Succinctly, there are well-establishedrelationships between LLD, vascular risk factors and cerebral hyperintensities, the radiological hallmark of vascular depression.Cognitive dysfunction is common in LLD, particularly executive dysfunction, a finding predictive of poor antidepressant response.Over time, progression of hyperintensities and cognitive deficits predicts a poor course of depression and may reflect underlyingworsening of vascular disease. This work laid the foundation for examining the mechanisms by which vascular disease influencesbrain circuits and influences the development and course of depression. We review data testing the vascular depression hypothesiswith a focus on identifying potential underlying vascular mechanisms. We propose a disconnection hypothesis, wherein focalvascular damage and white matter lesion location is a crucial factor, influencing neural connectivity that contributes to clinicalsymptomatology. We also propose inflammatory and hypoperfusion hypotheses, concepts that link underlying vascular processeswith adverse effects on brain function that influence the development of depression. Testing such hypotheses will not only informthe relationship between vascular disease and depression, but also provide guidance on the potential repurposing ofpharmacological agents that may improve LLD outcomes.
Molecular Psychiatry advance online publication, 26 February 2013; doi:10.1038/mp.2013.20
Keywords: cerebrovascular; cognition; depression; geriatrics; neuroimaging; review
INTRODUCTIONThere is a substantial heterogeneity in the biological factors thatinfluence the risk of developing depression across the lifespan.Genetic and epigenetic factors influence gene expression orprotein function across a variety of molecular systems, resulting ina vulnerability to develop depression in context of psychosocialadversity.1 This heterogeneity is even more apparent indepression occurring in older adults, or late-life depression(LLD), as aging-related changes across multiple organ systemsalso contribute to depression. Aging-related changes in theneurological, immune and endocrine systems have all beenimplicated in depression, but one of the best studied changes inLLD is the role of vascular disease.
The ‘Vascular Depression’ hypothesis proposed that ‘cerebro-vascular disease may predispose, precipitate or perpetuate somegeriatric depressive syndromes’.2 The hypothesis wasaccompanied by two proposals on the core characteristics ofand how to define a vascular depression subtype. First,Alexopoulos and colleagues2,3 proposed a working definitionbased on the presence of vascular risk factors. The clinicalpresentation of ‘vascular depression’ was characterized bycognitive deficits, psychomotor retardation, lack of insight anddisability disproportional to the depression severity. Investigatorssubsequently focused on the cognitive dysfunction occurring inLLD and its relationship to response to antidepressants.4 Second,Krishnan and colleagues5 proposed a magnetic resonance
imaging (MRI)-based definition, requiring evidence of vascularchanges on neuroimaging, referred to as MRI hyperintensities.Both definitions are important as subsequent work demonstratedthe internal validity of a vascular depression diagnostic subtypecharacterized by MRI findings and executive dysfunction.6
WHITE MATTER LESIONS, WHITE MATTER HYPERINTENSITIESAND MRI-DEFINED VASCULAR DEPRESSIONThe hallmark of MRI-defined vascular depression is the presenceof white matter lesions (WMLs) identified as white matterhyperintensities (WMH) on T2-weighted or fluid-attenuatedinversion recovery MRI. Throughout this review we refer to theradiological findings as WMHs, while reserving the term WMLwhen discussing the underlying changes in the cerebral whitematter.
WMHs are associated with advanced age7 and cerebrovascularrisk factors, including diabetes, cardiac disease andhypertension.8–12 Vascular dysregulation contributes to WMHdevelopment, as white matter is sensitive to transientischemia,13 and many larger WMHs are ischemic in origin.14,15
Hypertension and blood pressure variability are associated withLLD16–18 and also contribute to WMH development,19,20
particularly when accompanied by impaired cerebral vasomotorreactivity and altered autoregulatory processes.21,22 Such deficitsreduce cerebral blood flow (CBF) and may lead to WMHs.23,24
1Center for Cognitive Medicine, Department of Psychiatry, Vanderbilt University, Nashville, TN, USA; 2Department of Psychiatry, University of Pittsburgh Medical Center,Pittsburgh, PA, USA and 3Department of Psychiatry, Weill-Cornell Medical College, New York, NY, USA. Correspondence: Dr WD Taylor, Center for Cognitive Medicine, Departmentof Psychiatry, Vanderbilt University, 1601 23rd Avenue South, Nashville, TN 37212, USA.E-mail: [email protected] 23 October 2012; revised 9 January 2013; accepted 18 January 2013
Molecular Psychiatry (2013), 1–12& 2013 Macmillan Publishers Limited All rights reserved 1359-4184/13
www.nature.com/mp

Article
Association of Gene Variants of the Renin-AngiotensinSystem With Accelerated Hippocampal Volume Loss
and Cognitive Decline in Old Age
Anthony S. Zannas, M.D., M.Sc.
Douglas R. McQuoid, M.P.H.
Martha E. Payne, Ph.D., M.P.H.
James R. MacFall, Ph.D., M.S.
Allison Ashley-Koch, Ph.D.
David C. Steffens, M.D., M.H.Sc.
Guy G. Potter, Ph.D.
Warren D. Taylor, M.D., M.H.Sc.
Objective: Genetic factors confer risk forneuropsychiatric phenotypes, but the poly-genic etiology of these phenotypes makesidentification of genetic culprits challenging.An approach to this challenge is to examinethe effects of genetic variation on relevantendophenotypes, such as hippocampalvolume loss. A smaller hippocampus isassociated with gene variants of the renin-angiotensin system (RAS), a system impli-cated in vascular disease. However, nostudies to date have investigated longitu-dinally the effects of genetic variation ofRAS on the hippocampus.
Method: The authors examined the ef-fects of polymorphisms of AGTR1, the geneencoding angiotensin-II type 1 receptor ofRAS, on longitudinal hippocampal volumesof older adults. In all, 138 older adults (age$60 years) were followed for an average ofabout 4 years. The participants underwentrepeated structural MRI and comprehen-sive neurocognitive testing, and they weregenotyped for four AGTR1 single-nucleotide
polymorphisms (SNPs) with low pairwiselinkage disequilibrium values and apoli-poprotein E (APOE) genotype.
Results: Genetic variants at three AGTR1SNPs (rs2638363, rs1492103, and rs2675511)were independently associated with accel-erated hippocampal volume loss over the4-year follow-up period in the right but notleft hemisphere. Intriguingly, these AGTR1risk alleles also predicted worse episodicmemory performance but were not re-lated to other cognitivemeasures. Two riskvariants (rs2638363 and rs12721331) inter-acted with the APOE4 allele to accelerateright hippocampal volume loss.
Conclusions: Risk genetic variants of theRAS may accelerate memory decline inolder adults, an effect that may be con-ferred by accelerated hippocampal vol-ume loss. Molecules involved in thissystem may hold promise as early thera-peutic targets for late-life neuropsychiatricdisorders.
Am J Psychiatry Zannas et al.; AiA:1–8
Genetic factors have long been hypothesized to conferrisk for neuropsychiatric phenotypes, but it has been chal-lenging to identify genetic culprits. The failure to identify riskgenes may be in large part a result of the polygenic etiologyand phenotypic heterogeneity of neuropsychiatric disor-ders (1). These disorders result from complex interactionsamongmultiple genes, tissue-specific epigenetic regulation,and environmental influences, which make identifying therelationships between single genes and distal phenotypeschallenging.An alternative approach is to examine endophenotypes,
measurable constructs that confer risk for complex dis-orders and are thought to lie in greater etiological prox-imity to genetic factors (2). One promising endophenotypefor late-life neuropsychiatric disorders is small hippocam-pal volume (3). Smaller hippocampal volume has beenassociated with treatment resistance in late-life depression(4) and predicts progressive cognitive decline in elderly in-dividuals (5). Therefore, efforts to link hippocampal volumereduction with risk genes may be particularly relevant forlate-life neuropsychiatric syndromes.
A novel and biologically plausible gene to investigate inthese relationships isAGTR1, the gene encoding angiotensin-II type 1 (AT1) receptor in humans. AT1 receptors are theprimary effector of the renin-angiotensin system (RAS) inseveral organs, including the brain. The RAS is an im-portant regulator of the stress response, and AT1 receptorsare expressed in brain regions that modulate stress andemotion, including the hypothalamus, amygdala, and hip-pocampus (6, 7). In animal studies, RAS activation leads tohyperactivity of the stress system and heightened anxiousbehavior, whereas blockade of AT1 receptors dampensstress responses and ameliorates anxious and depressivebehavior (6, 8). As the RAS also plays a central role in bloodpressure regulation and has been implicated in vasculardisease (9), examining this system may be particularly rel-evant for older adults with depression, since late-life de-pression is often characterized by vascular comorbidity (10).Despite these theoretical implications, few studies have
examined the relationship between genetic variation inAGTR1 and either neuropsychiatric phenotypes or hippo-campalmorphology. Studies on the common rs5186AGTR1
AJP in Advance ajp.psychiatryonline.org 1

(A-to-C) polymorphism have reported antidepressant re-sponse differences between genotypes in elderly depressedindividuals (11–13). In abroader analysis of single-nucleotidepolymorphisms (SNPs) in AGTR1 (14), our group reportedthat allele frequency differences in two AGTR1 SNPs in-creased the odds of late-life depression.We also found cross-sectional associations between right hippocampal volumeand fourAGTR1 intronic SNPs, namely rs2638363, rs1492103,rs2675511, and rs12721331 (14). To our knowledge, no stud-ies have examined the effects of AGTR1 polymorphisms onlongitudinal changes in hippocampal morphology in olderadults. This is particularly important as reduction in hip-pocampal volume is associated with subsequent cognitivedecline (5).
To extend our previous findings demonstrating cross-sectional relationships between AGTR1 and hippocampalmorphology (14), we examined the effects of AGTR1 geno-type on longitudinal change in hippocampal volume. Oura priori hypothesis was that the gene variants we previouslyassociated with smaller cross-sectional hippocampus vol-ume would also be associated with greater hippocampalvolume loss over time. We also sought to determine if thesegene variants were associated with differences in cognitivefunction over time, particularly in domains involving thehippocampus, such as episodic memory. To control forthe effects of depression that have been shown to lead tosmaller hippocampal volumes via chronic hyperactivity ofthe stress system (15), we examined two cohorts of elderlydepressed and nondepressed individuals. In secondaryanalyses, we examined whether depression diagnosis orapolipoprotein E (APOE) genotype had synergistic effectswith AGTR1 genotypes on hippocampal volume change.
Method
Study Participants and Clinical Care
All participants were age 60 years or older and participated inthe Conte Center for the Neuroscience of Depression in Late Lifeand the Neurocognitive Outcomes of Depression in the Elderlystudies conducted at Duke University Medical Center. The DukeUniversity Medical Center institutional review board approvedthese studies, and eligible individuals provided written informedconsent.
The two cohorts were made up of depressed patients and non-depressed comparison subjects. Depressed patients were recruitedprimarily by clinical referral and secondarily by advertisements,and they met DSM-IV criteria for major depressive disorder. Di-agnosis was based on the NIMH Diagnostic Interview Schedule(DIS) (16) and was confirmed by a geriatric psychiatrist during base-line clinical evaluation. Nondepressed individuals were communitydwelling older adults recruited either from the Duke UniversityAging Center Subject Registry or through advertisements. All par-ticpants underwent cognitive screening with the Mini-Mental StateExamination (MMSE) (17). Medical comorbidity was assessed witha previously used self-report questionnaire (18).
Exclusion criteria for all individuals were as follows: 1) presenceof other major psychiatric disorder such as schizophrenia orbipolar disorder; 2) history of substance abuse or dependence; 3)presence of neurological disease; 4) metal in the body or other
contraindication for MRI; and 5) a screening MMSE score lowerthan 25. Furthermore, nondepressed individuals were excluded ifthey had evidence of past psychiatric disorder based on the DIS.
Antidepressant treatment followed the Duke Somatic Treat-ment Algorithm for Geriatric Depression (19), which allows step-wise use of commercially available antidepressant modalities.The majority of depressed patients were prescribed sertraline onstudy entry, but treatment differed among participants and wasguided by previous medication trials and depression severity.Following failed trials, switches to other antidepressant agentsand augmentation strategies were allowed as clinically indicated.Treatment alternatives included psychotherapy and electrocon-vulsive therapy.
The current longitudinal study extends our past research (14),where in a separate cohort we found a relationship between fourAGTR1 SNPs and right hippocampal volumes. Although therewas some overlap in participants, the present sample is muchlarger (138 compared with 70 individuals) and imaging data differfrom our previous study. The previous study used 3-T MRI data;the present study used 1.5-T MRI data, as longitudinal 3-T datawere not available for the majority of participants. Similar to ourprevious report and based on research showing racial differencesin AGTR1 allele frequencies (14, 20), we limited the currentanalyses to Caucasian individuals who had genotype data for allfour AGTR1 SNPs and at least two hippocampal volume measure-ments (a baseline and at least one follow-up measurement).
Neuropsychological Assessments
Neuropsychological testing was administered to study partic-ipants at baseline and then annually, regardless of the presenceor absence of depressive symptoms. The battery is described fullyelsewhere (21) and has been successfully employed in a numberof clinical and epidemiological settings (22). Testing was ad-ministered by a trained psychometric technician supervised bya licensed clinical psychologist.
We created composite variables from the broader neuro-psychological test battery that represented cognitive domainsthat may be adversely affected by aging. This was achieved bygrouping neuropsychological tests into rational constructs,similar to previously published studies (23). We created Z scoresfor each measure based on the performance of all participantsand summed the Z scores for all tests within each domain. Internalconsistency for each domain was assured using Cronbach’scoefficient alpha. Following this approach, we created fourcomposite neurocognitive measures: 1) episodic memory (logicalmemory, Benton visual retention test, immediate word learning,and word list recall; Cronbach’s coefficient alpha=0.88); 2) executivespeed (speed in Trails A and Trails B and symbol-digit modalitytest; Cronbach’s coefficient alpha=0.86); 3) verbal fluency (verbalfluency test and controlled oral word association test; Cronbach’scoefficient alpha=0.74); and d) working memory (digits forward,digits backward, and digits ascending; Cronbach’s coefficientalpha=0.74).
Genotyping and Genetic Analyses
All genotyping was performed on DNA from whole peripheralblood using the Gentra PureGene system (Qiagen, Valencia,Calif.). Assays employed quality control procedures, whichincluded serial genotyping of blinded duplicate samples. Qualityrequirements for each assay were met only if duplicate samplesmatched 100%, and efficiency of 95% was further required foreach assay before statistical analyses. Deviations from Hardy-Weinberg equilibrium were previously tested for all SNPsseparately in the depressed and nondepressed cohorts (14) usingexact tests per the Genetic Data Analysis program (24).Genotyped SNPs were identified using Linkage DisequilibriumSelect (25). Selected SNPs had linkage disequilibrium of r2,0.64
2 ajp.psychiatryonline.org AJP in Advance
GENE VARIANTS OF THE RENIN-ANGIOTENSIN SYSTEM

and minor allele frequency of at least 0.10 in the HapMap project(www.hapmap.org), which was based on Utah residents ofEuropean ancestry and provided genetic coverage of the entireAGTR1. In this study, we focused on the four SNPs that displayedsignificant cross-sectional relationships with hippocampal vol-umes among the 10 SNPs tested in our previous report (14). Toexamine whether these four SNPs could be treated as indepen-dent signals in our analyses, we estimated the pairwise linkagedisequilibrium between all SNPs in our study population. Allpairwise r2 values were found to be below 0.5. APOE genotype wasdetermined using previously published methods (26).
MRI Acquisition and Analysis
Each participant was screened for contraindications andscanned with a 1.5-T whole-body MRI system (Signa, GE MedicalSystems, Milwaukee) approximately every 2 years. All acquisitionswere performed with the standard head (volumetric) radiofre-quency coil. Using a previously described MRI acquisition protocol(27, 28), we first confirmed alignment by a rapid sagittal localizerscan and then obtained two dual-echo fast spin-echo acquisitions:one in the axial plane for cerebral morphometry and one in acoronal oblique plane for hippocampal morphometry.
The images were then analyzed at the Duke NeuropsychiatricImaging Research Laboratory. Segmentation of tissue and mea-surement of total cerebral volume, which included total whiteand gray matter and CSF volumes in both hemispheres, were per-formed as previously described (27). Image analysts received ex-tensive training, and reliability was established before any dataprocessing by repeated measurements on multiple MRIs sepa-rated by at least a week. Intraclass correlation coefficients wereas follows: left hippocampus=0.8; right hippocampus=0.7; andtotal cerebral volume=0.997.
Delineation of the hippocampus was based on previouslydescribed methods (28). Analysts began with the most posteriorcoronal slice and moved anteriorly, measuring the hippocampuswhere the pulvinar nucleus of the thalamus obscured the crurafornicis on each side. The fimbria and the thin strip of graymatter along the medial border of the hippocampus weretransected at their narrowest points. Tracing continued aroundthe hippocampal body to the starting point. The anterior borderof the hippocampus was defined as the slice on which theinferolateral ventricle appeared horizontally without any body ofgray matter visible below it. The amygdala-hippocampal transi-tion zone, which was transected at its narrowest point, appearedas a diffuse area of gray matter between the anterior portion ofthe hippocampus and the posterior portion of the amygdala.
Statistical Analyses
All statistical tests were performed with SAS, version 9.2 (Cary,N.C.). The level of statistical significance was set a priori at a=0.05and all tests were two tailed. To maximize power in our analyses,we dichotomized each SNP into two genotype groups, the majorallele homozygotes and the minor allele carriers. This furtherincreased comparability with our previous report (14), where thesame genotype groups were used. The two diagnostic cohorts(depressed and nondepressed) were compared at baseline fordifferences in demographic variables and baseline measures.Categorical variables were compared with chi-square tests, equal-variance continuous variables with pooled two-sample t tests,and unequal-variance continuous variables with Satterthwaitet tests.
We next examined the longitudinal effects of AGTR1 poly-morphisms on hippocampal volumes and composite cognitivemeasures. We used linear mixed-effects models (29) using thePROC MIXED command in SAS 9.3 to analyze these longitudinaldata. Analyses included the maximum number of participantswith data for longitudinal time points and for all variables
included in the models. In these models, each individual was theindependent sampling unit, and each measurement at a partic-ular time point was the observation unit. Separate models werecreated for the right and left hippocampus and for each compositecognitive measure, with each AGTR1 SNP genotype group, time(as a continuous variable), and genotype-by-time interaction asthe main independent variables. In order to account for between-subject variability in brain volume, we included cerebral volumeas a covariate in models that used hippocampal volume as thedependent variable. Other covariates included in all models weresex, age, diagnostic group (depressed or nondepressed), and therespective baseline hippocampal volume or cognitive measure-ment. The primary effects of interest were the genotype maineffect, which examines the genotype effect irrespective of time,and the genotype-by-time interaction, which examines the rateof change in the mean hippocampal volume or cognitive mea-sure over time between the two genotype groups for each AGTR1SNP. Secondary analyses tested the three-way depression-by-genotype-by-time interaction and the AGTR1 genotype-by-APOEgenotype-by-time interaction. All models were initially run withthe interaction terms, and these terms remained in the model ifsignificant, but were excluded if nonsignificant.
Results
Sample Demographics and Baseline Measures
The primary sample included 138 elderly individuals (79depressed and 59 nondepressed) with genotype data forAGTR1 SNPs and at least two MRI scans (a baseline andone follow-up assessment). The demographic character-istics and clinical data are summarized in Table 1. Theirages ranged from 60 to 84 years for the depressed cohortand from 60 to 82 years for the nondepressed cohort. Thetwo groupswere similar in genotype frequencies, age,MMSEscores, and baseline left and right hippocampal volumes.However, the percentage of female participants and edu-cational levels were higher in the nondepressed group, andthe percentage of patients who reported hypertension washigher in the depressed group. Finally, we found that thenumber of patients who reported a history of either car-diac complaints or hypertension did not significantly differbetween the four AGTR1 or APOE genotype groups (datanot shown). The maximum number of MRI measures perparticipant was five, and no significant difference wasfound for length of study follow-up between diagnosticcohorts (a mean of 1,435.3 days [SD=502.5] for depressedpatients and a mean of 1,495.9 days [SD=785.8] for non-depressed patients; Satterthwaite t test=130, df=2, t=0.55,p=0.5855).
Longitudinal Effects of AGTR1 SNPs on HippocampalVolumes
We created mixed models examining hippocampusvolume in the left or right hemisphere as repeatedly mea-sured dependent variables. Independent variables includeddiagnosis (depressed or nondepressed), age, sex, cerebralvolume, baseline hippocampal volume, time, and AGTR1SNP genotype. To test the hypothesis that SNPs woulddifferentially affect hippocampal volume over time, we
AJP in Advance ajp.psychiatryonline.org 3
ZANNAS, MCQUOID, PAYNE, ET AL.

included a SNP-by-time interaction term. Table 2 summa-rizes the effects of the four AGTR1 SNPs examined andtheir interactions with time on left and right hippocampalvolumes. When examining models of right hippocampalvolume, three of the four SNPs (rs2638363, rs1492103,rs2675511) showed both a statistically significant primaryeffect and an interactive effect with time (Table 2). Theprimary effect of AGTR1 SNPs replicated our previousfindings (14), despite nearly double the sample size anddifferent MRI field strength. Again, individuals homozy-gous for the vascular risk alleles (rs2638363 GG, rs1492103TT, and rs2675511 AA) exhibited smaller hippocampal vol-umes when compared with individuals who were het-erozygous or homozygous for the alternate allele. TheSNP-by-time interaction tested for differences betweenSNP alleles on change in hippocampal volume over time.When examining these interactions, individuals homozy-gous for the risk alleles exhibited an accelerated decreasein right hippocampal volumeover time relative to individuals
with alternate genotypes. However, the four SNPs exhib-ited neither a significant primary effect nor a significantgene-by-time interaction on left hippocampal volume. Inother words, the effect of all three SNPs was selective andlateralized to the right hemisphere.In secondary analyses we tested whether AGTR1 genetic
variation has synergistic effects with depression or APOEgenotype on the rate of hippocampal volume change. Thethree-way depression-by-AGTR1-by-time interactions didnot reach significance for any of the SNPs for either the leftor right hippocampus. However, we did observe signifi-cant gene-gene interactions. The APOE genotype hadstatistically significant epistatic effects with rs2638363 andrs12721331 for the right hippocampus volume over time(Table 2). In both cases, the presence of both the riskAGTR1allele and the APOE4 allele was associated with acceleratedhippocampal volume loss. We observed a similar trend thatdid not achieve statistical significance for the interactionbetween rs1492103, APOE, and time (Table 2).
TABLE 1. Demographic Variables and Genotype Frequencies in a Study of the Renin-Angiotensin System, AcceleratedHippocampal Volume Loss, and Cognitive Decline in Old Agea
Variable Depressed Patients (N=79) Nondepressed Comparison Subjects (N=59) Analysis
Mean SD Mean SD t df pAge (years) 69.6 6.7 69.7 5.8 0.05 136 0.9611Education (years) 14.5 2.1 15.7 1.6 4.08 134 0.0004Mini-Mental State Examination score 28.8 1.3 29.1 1.1 1.35 132 0.1808Baseline right hippocampal volume, ml 3.08 0.39 3.13 0.42 0.85 136 0.3968Baseline left hippocampal volume, ml 2.97 0.4 3.00 0.45 0.47 136 0.6395Cerebrum, ml 1,164.8 128.3 1,140.6 117.2 1.12 136 0.2645
N N x2
Sex 4.08 1 0.0433Female 52 48Male 27 11
History of cardiac complaint 0.2 1 0.6517Yes 14 9No 63 50
History of hypertension 5.82 1 0.0158Yes 29 11No 48 48
rs2638363 (A/G) 2.39 1 0.1220GG 58 36AA/AG 21 23
rs1492103 (C/T) 0.87 1 0.3522TT 58 39CC/CT 21 20
rs12721331 (C/T) 1.43 1 0.2312TT 70 48CC/CT 9 11
rs2675511 (A/G) 1.03 1 0.3107AA 40 35GG/GA 39 24
APOE 0.46 1 0.4994APOE4 carriers 20 18No APOE4 59 41
a All continuous variables had equal variances and were tested with pooled t test, except for education, which exhibited unequal variancesbetween the two diagnostic groups and was thus tested using Satterthwaite t test. Reported p values are two-tailed.
4 ajp.psychiatryonline.org AJP in Advance
GENE VARIANTS OF THE RENIN-ANGIOTENSIN SYSTEM

Longitudinal Effects of AGTR1 SNPs on CompositeCognitive Measures
We next tested whether AGTR1 variants confer risk forcognitive decline. A total of 138 elderly participants (63depressed and 75 nondepressed) had both genotype andneurocognitive assessment data andwere included in theseanalyses. This sample partially overlaps with the sampleexamining hippocampal volumes, with 81 participants (36depressed and 45 nondepressed) included in both analyses.As expected, depressed individuals performed significantlyworse than nondepressed individuals on univariate compar-isons of the four composite cognitive measures of episo-dic memory (t=5.14, df=106, p,0.0001), executive speed(t=4.36, df=67, p,0.0001), verbal fluency (t=5.18, df=136,p,0.0001), and working memory (t=2.97, df=114, p=0.0037).We used mixed models to examine the effect of AGTR1
genotypes and their interaction with time on each of thecomposite cognitive measures. All models controlled fordiagnosis (depressed or nondepressed), age, sex, educa-tion, time, and baseline cognitive measure score. In thesemodels, only rs2638363 displayed a significant main effectof genotype on composite episodic memory performance(F=4.59, df=1, 126, p=0.0340), but the genotype-by-time in-teraction did not reach significance. Similarly, rs1492103exhibited a trend for a direct effect on episodic memory(F=3.85, df=1, 126, p=0.0519), but this did not reach sta-tistical significance. Finally, rs2675511 exhibited a gene-by-time interaction (F=5.61, df=1, 125, p=0.0194) predictingworsening episodic memory performance. In accordancewith SNP effects on hippocampal volumes, individualshomozygous for the vascular risk alleles (rs2638363 GG,rs1492103 TT, and rs2675511 AA) exhibited lower episodicmemory scores. None of the four genetic variants exhibitedeither a statistically significant direct effect or interactionwith time effect on executive speed, verbal fluency, orwork-ing memory.
Discussion
Replicating and extending our previous findings ofAGTR1 effects on right hippocampal morphology (14),three of the same SNPs predicted longitudinal hippocam-pal volume change in the right but not the left hemispherein elderly individuals. The direction of the observed re-lationships was similar to results from the previous cross-sectional study, that is, each of the previously identified“risk” genotypes (rs2638363 GG, rs1492103 TT, and rs2675511AA) predicted longitudinally greater shrinkage of the righthippocampus when compared with the alternate geno-types. Intriguingly, these AGTR1 risk alleles also predictedpoorer performance in episodicmemory, a neurocognitivemeasuremediated by the hippocampus, but had no effectson other cognitive measures. Additionally, two risk variants(rs2638363 and rs12721331) showed epistatic effects withthe APOE4 allele, a known risk factor for dementia (26), onright hippocampal volume loss over time. Importantly, theSNPs examined are in low pairwise linkage disequilibrium(r2,0.5) and thus represent independent signals. Thepresence of several signals within the AGTR1 locus thatare independently associated with hippocampal volumechanges and memory decline lends further support to thereliability of these associations. Taken together, ourfindingsstrongly support that AGTR1 gene variants may confervulnerability via both direct and epistatic effects for pro-gressive memory decline by accelerating hippocampalvolume loss. The main findings and the supported modelare schematically summarized in Figure 1.Our study offers novel insights into the role of the renin-
angiotensin system (RAS) in hippocampal atrophy and
cognitive decline. Hippocampal atrophy has been shown to
predict cognitive decline in late life and time-to-conversion
to Alzheimer’s disease (5, 30). Previous animal and human
studies support involvementof theRAS incognitive syndromes
TABLE 2. Longitudinal Effects of AGTR1 Single-Nucleotide Polymorphisms (SNPs) on Hippocampal Volumesa
Genotype
Right Hippocampal Volume Left Hippocampal Volume
F p F p
rs2638363 5.96 0.0160 0.81 0.3693rs2638363 by time 6.43 0.0124 0.11 0.7400rs2638363 by APOE by time 4.80 0.0303 0.14 0.7115rs1492103 5.01 0.0269 0.72 0.3967rs1492103 by time 5.90 0.0166 0.10 0.7558rs1492103 by APOE by time 3.78 0.0541 0.01 0.9100rs12721331 0.20 0.6564 0.96 0.3297rs12721331 by time 1.29 0.2574 0.09 0.7709rs12721331 by APOE by time 6.45 0.0123 0.07 0.7982rs2675511 4.06 0.0459 0.30 0.5842rs2675511 by time 4.62 0.0335 0.23 0.6352rs2675511 by APOE by time 0.75 0.3890 0.3 0.5876a Analyses conducted using linear mixed-effects models. These models tested for the effect of AGTR1 SNP genotype on hippocampal volumeand also examined AGTR1-by-time and AGTR1-by-APOE-by-time interactions. All models included 138 participants and controlled for sex, age,diagnostic group (depressed or nondepressed), baseline hippocampal volume, and total cerebral volume. Values in bold denote statisticallysignificant parameters, defined as p,0.05. Reported p values are two-tailed.
AJP in Advance ajp.psychiatryonline.org 5
ZANNAS, MCQUOID, PAYNE, ET AL.

(6, 14, 31). RAS activation modulates cerebral blood flow,increases brain vulnerability to ischemia, and promotesbrain inflammation (6, 32). These effects render this systemparticularly relevant in late life, where vascular and in-flammatory processes are hypothesized to contribute todepressive and cognitive syndromes (10, 33). On the otherhand, AT1 receptor blockade dampens stress responses,ameliorates anxious and depressive behaviors, and reducesbrain inflammation and vulnerability to ischemia (6, 8, 32).Thus, it is plausible that perturbations in the RAS couldheighten the risk for developing dementia by acceleratingage-related changes in brain morphology, particularly inbrain regionsmost vulnerable to the effects of aging, such asthe hippocampus. Although RAS activitymay bemodulatedby functional variants at the AGTR1 locus, the moleculareffects of the risk AGTR1 SNPs are currently not clear.Despite their intronic location, these SNPs could havefunctional effects. For instance, intronic SNPs may be locatedin enhancer regions that influence the three-dimensionalchanges in chromatin conformation necessary for transcrip-tion regulation (34). Alternately, these SNPs may be taggingother functional variants in nearby regions of the AGTR1locus. Finally, as supported by the epistatic effects withAPOE observed in our study, these SNPs may havefunctional effects via interaction with other genes that
lie in common biological pathways central for the develop-ment of brain pathology and dementia. Future studies on thefunctional effects of these genetic variants are warrantedand may shed light on the mechanisms linking AGTR1and cognitive syndromes.Intriguingly, the effects of AGTR1 variation were later-
alized to the right hippocampus, which is in accordancewith our previous cross-sectional study (14). Although thesignificance of this lateralization is unclear, hippocampalasymmetry may be an important endophenotype that hasbeen underemphasized by previous studies. Hippocampalasymmetry has been observed in patients with severedepression and in nondepressed relatives of depressedindividuals (35, 36). Furthermore, unilateral hippocampalvolume changes may be associated with decline in specificcognitive outcomes (5, 37) and with decreased likelihoodof achieving antidepressant remission (4). Thus, hippo-campal asymmetry may be an early step in the pathogen-esis of some late-life mood and cognitive syndromes. Thisasymmetry could be induced by differential hemisphericeffects of the RAS on the hippocampus. Notably, activity ofangiotensinase, an enzyme that metabolizes angiotensin,has been found to be distributed asymmetrically betweenthe left and right hippocampi of the rat brain (38, 39).This may also reflect differential activity of angiotensin and
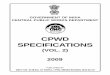
FIGURE 1. Graphic Summary of AGTR1 Single-Nucleotide Polymorphism (SNP) Associations With Accelerated RightHippocampal Volume Loss and Episodic Memory Decline in Old Agea
rs2638363
rs2675511
rs1492103
rs2638363
Episodic memorydecline
Right hippocampalvolume loss
Aging
rs12721331+ ApoE4
+ ApoE4
F=4.59p=0.03F=4.80
p=0.03
F=4.62p=0.03
F=5.90p=0.02
F=5.61p=0.02
F=6.43p=0.01
F=6.45p=0.01
a Genotype-by-time interactions are shown as arrows connecting aging and outcomes (right hippocampal volume loss and episodic memorydecline) after moderation by encircled SNPs. Direct genotype effects are shown on the right side of the figure as arrows directly connectingSNPs with episodic memory decline. The encircled numbers on each arrow represent the F values and p values as estimated from therespective mixed regression models. Further details are provided in text and Table 2.
6 ajp.psychiatryonline.org AJP in Advance
GENE VARIANTS OF THE RENIN-ANGIOTENSIN SYSTEM

potentially asymmetric effects of AGTR1 genetic variantsbetween the two hemispheres. Whether this mechanismholds true, and the clinical significance of these asymme-tries, remains to be determined.Several limitations should be considered when inter-
preting our findings. Althoughwe controlled for the effectsof depression diagnosis and basic demographic factors onhippocampal morphology, we did not control for antide-pressant treatments thatmay have neurotrophic effects onthe hippocampus (40) and may even reverse hippocampalvolume loss in some cases of depression (37). Depressedparticipants were treated based on an algorithm ratherthan a rigid clinical trial. Although this makes our ap-proach comparable to clinical practice, it makes it chal-lenging to elucidate the effects of antidepressants. Data onantidepressant use prior to enrollment, as well as specifictreatment modalities, duration, and dosages used over thestudy period, were not known for each participant. Thus, itis possible that variable treatments between genotypegroups may have influenced our results. However, theassignment of treatment modalities occurred randomlyand treating clinicians were blind to genotype groups, andthus systematic errors cannot account for our findings.Another limitation was our focus on variation at a singlegenetic locus and a single brain region. This was based onour sample size and the a priori plausible involvement ofAGTR1 and hippocampal pathology in late-life neuropsy-chiatric syndromes. Larger longitudinal studies are war-ranted for a more systematic examination of the multiplebrain regions, genes, and biological pathways involved inthe pathogenesis of these syndromes. Our study showsthat the RAS is one such pathway that should be includedin future pathogenetic models.In summary, this is the first study to our knowledge to
explore the longitudinal effects of AGTR1 genetic variationon hippocampalmorphology and cognitive decline. In con-trast with cross-sectional approaches that cannot establishtemporal relationships, the present study reveals that olderadults homozygous for AGTR1 risk variants exhibit accel-erated hippocampal volume loss and memory decline. Ourstudy exemplifies how examining the longitudinal effects ofbiologically plausible genotypes on relevant endopheno-types may provide novel insights into the pathogenesis ofcomplex phenotypes. It further suggests that moleculesinvolved in the RAS may serve as early therapeutic targetsfor late-life neuropsychiatric syndromes.
Received Nov. 23, 2013; revision received Apr. 21, 2014; acceptedMay 6, 2014 (doi: 10.1176/appi.ajp.2014.13111543). From theDepartment of Psychiatry and Behavioral Sciences, the Neuropsychi-atric Imaging Research Laboratory, the Department of Radiology, theCenter for Human Genetics, and the Department of Medicine, DukeUniversity Medical Center, Durham, N.C.; the Department of Trans-lational Research in Psychiatry, Max Planck Institute of Psychiatry,Munich, Germany; the Department of Psychiatry, University ofConnecticut Health Sciences Center, Farmington, Conn.; and theDepartment of Psychiatry, Vanderbilt University Medical Center andThe Geriatric Research, Education, and Clinical Center (GRECC), Department
of Veterans Affairs Medical Center, Tennessee Valley Healthcare System,Nashville, Tenn. Address correspondence to Dr. Zannas ([email protected]).The authors report no financial relationships with commercial
interests.The authors acknowledge Dr. Torsten Klengel for helpful discus-
sions on interpreting the single-nucleotide polymorphism data.Supported by research grants R01 MH077745, R01 MH054846, and
K24 MH070027.
References
1. Sullivan PF, Daly MJ, O’Donovan M: Genetic architectures ofpsychiatric disorders: the emerging picture and its implications.Nat Rev Genet 2012; 13:537–551
2. Gottesman II, Gould TD: The endophenotype concept in psy-chiatry: etymology and strategic intentions. Am J Psychiatry2003; 160:636–645
3. Hasler G, Drevets WC, Manji HK, Charney DS: Discovering en-dophenotypes for major depression. Neuropsychopharmacology2004; 29:1765–1781
4. Hsieh MH, McQuoid DR, Levy RM, Payne ME, MacFall JR, SteffensDC: Hippocampal volume and antidepressant response in ge-riatric depression. Int J Geriatr Psychiatry 2002; 17:519–525
5. Steffens DC, McQuoid DR, Payne ME, Potter GG: Change in hip-pocampal volume on magnetic resonance imaging and cogni-tive decline among older depressed and nondepressed subjectsin the neurocognitive outcomes of depression in the elderly study.Am J Geriatr Psychiatry 2011; 19:4–12
6. Saavedra JM, Sánchez-Lemus E, Benicky J: Blockade of brainangiotensin II AT1 receptors ameliorates stress, anxiety, braininflammation and ischemia: therapeutic implications. Psycho-neuroendocrinology 2011; 36:1–18
7. Tsutsumi K, Saavedra JM: Characterization and development ofangiotensin II receptor subtypes (AT1 and AT2) in rat brain. Am JPhysiol 1991; 261:R209–R216
8. Nayak V, Patil PA: Antidepressant activity of fosinopril, ramipriland losartan, but not of lisinopril in depressive paradigms ofalbino rats and mice. Indian J Exp Biol 2008; 46:180–184
9. Duprez DA: Role of the renin-angiotensin-aldosterone system invascular remodeling and inflammation: a clinical review. J Hyper-tens 2006; 24:983–991
10. Taylor WD, Aizenstein HJ, Alexopoulos GS: The vascular depres-sion hypothesis: mechanisms linking vascular disease with de-pression. Mol Psychiatry 2013; 18:963–974
11. Bondy B, Baghai TC, Zill P, Schule C, Eser D, Deiml T, ZwanzgerP, Ella R, Rupprecht R: Genetic variants in the angiotensinI-converting-enzyme (ACE) and angiotensin II receptor (AT1) geneand clinical outcome in depression. Prog NeuropsychopharmacolBiol Psychiatry 2005; 29:1094–1099
12. Kondo DG, Speer MC, Krishnan KR, McQuoid DR, Slifer SH,Pieper CF, Billups AV, Steffens DC: Association of AGTR1 with 18-month treatment outcome in late-life depression. Am J GeriatrPsychiatry 2007; 15:564–572
13. Saab YB, Gard PR, Yeoman MS, Mfarrej B, El-Moalem H, IngramMJ: Renin-angiotensin-system gene polymorphisms and de-pression. Prog Neuropsychopharmacol Biol Psychiatry 2007;31:1113–1118
14. Taylor WD, Benjamin S, McQuoid DR, Payne ME, Krishnan RR,MacFall JR, Ashley-Koch A: AGTR1 gene variation: associationwith depression and frontotemporal morphology. PsychiatryRes 2012; 202:104–109
15. Sheline YI, Gado MH, Kraemer HC: Untreated depression andhippocampal volume loss. Am J Psychiatry 2003; 160:1516–1518
16. Robins LN, Helzer JE, Croughan J, Ratcliff KS: National Instituteof Mental Health Diagnostic Interview Schedule: its history,
AJP in Advance ajp.psychiatryonline.org 7
ZANNAS, MCQUOID, PAYNE, ET AL.

characteristics, and validity. Arch Gen Psychiatry 1981; 38:381–389
17. Folstein MF, Folstein SE, McHugh PR: “Mini-mental state”:a practical method for grading the cognitive state of patients forthe clinician. J Psychiatr Res 1975; 12:189–198
18. Taylor WD, McQuoid DR, Krishnan KR: Medical comorbidity inlate-life depression. Int J Geriatr Psychiatry 2004; 19:935–943
19. Steffens DC, McQuoid DR, Krishnan KRR: The Duke SomaticTreatment Algorithm for Geriatric Depression (STAGED) ap-proach. Psychopharmacol Bull 2002; 36:58–68
20. Hindorff LA, Heckbert SR, Tracy R, Tang Z, Psaty BM, EdwardsKL, Siscovick DS, Kronmal RA, Nazar-Stewart V: Angiotensin IItype 1 receptor polymorphisms in the cardiovascular healthstudy: relation to blood pressure, ethnicity, and cardiovascularevents. Am J Hypertens 2002; 15:1050–1056
21. Steffens DC, Welsh-Bohmer KA, Burke JR, Plassman BL, Beyer JL,Gersing KR, Potter GG: Methodology and preliminary resultsfrom the neurocognitive outcomes of depression in the elderlystudy. J Geriatr Psychiatry Neurol 2004; 17:202–211
22. Tschanz JT, Welsh-Bohmer KA, Skoog I, West N, Norton MC,Wyse BW, Nickles R, Breitner JC: Dementia diagnoses fromclinical and neuropsychological data compared: the CacheCounty study. Neurology 2000; 54:1290–1296
23. Sheline YI, Pieper CF, Barch DM, Welsh-Bohmer K, McKinstry RC,MacFall JR, D’Angelo G, Garcia KS, Gersing K, Wilkins C, Taylor W,Steffens DC, Krishnan RR, Doraiswamy PM: Support for thevascular depression hypothesis in late-life depression: results ofa 2-site, prospective, antidepressant treatment trial. Arch GenPsychiatry 2010; 67:277–285
24. Zaykin D, Zhivotovsky L, Weir BS: Exact tests for associationbetween alleles at arbitrary numbers of loci. Genetica 1995; 96:169–178
25. Carlson CS, Eberle MA, Rieder MJ, Yi Q, Kruglyak L, NickersonDA: Selecting a maximally informative set of single-nucleotidepolymorphisms for association analyses using linkage disequi-librium. Am J Hum Genet 2004; 74:106–120
26. Saunders AM, Strittmatter WJ, Schmechel D, George-Hyslop PH,Pericak-Vance MA, Joo SH, Rosi BL, Gusella JF, Crapper-MacLa-chlan DR, Alberts MJ et al: Association of apolipoprotein E alleleepsilon 4 with late-onset familial and sporadic Alzheimer’sdisease. Neurology 1993; 43:1467–1472
27. Payne ME, Fetzer DL, MacFall JR, Provenzale JM, Byrum CE,Krishnan KRR: Development of a semi-automated method for
quantification of MRI gray and white matter lesions in geriatricsubjects. Psychiatry Res 2002; 115:63–77
28. Steffens DC, Byrum CE, McQuoid DR, Greenberg DL, Payne ME,Blitchington TF, MacFall JR, Krishnan KR: Hippocampal volumein geriatric depression. Biol Psychiatry 2000; 48:301–309
29. Cheng J, Edwards LJ, Maldonado-Molina MM, Komro KA, MullerKE: Real longitudinal data analysis for real people: buildinga good enough mixed model. Stat Med 2010; 29:504–520
30. Devanand DP, Pradhaban G, Liu X, Khandji A, De Santi S, SegalS, Rusinek H, Pelton GH, Honig LS, Mayeux R, Stern Y, TabertMH, de Leon MJ: Hippocampal and entorhinal atrophy in mildcognitive impairment: prediction of Alzheimer disease. Neu-rology 2007; 68:828–836
31. Wright JW, Harding JW: The brain RAS and Alzheimer’s disease.Exp Neurol 2010; 223:326–333
32. Saavedra JM, Nishimura Y: Angiotensin and cerebral blood flow.Cell Mol Neurobiol 1999; 19:553–573
33. Alexopoulos GS, Morimoto SS: The inflammation hypothesis ingeriatric depression. Int J Geriatr Psychiatry 2011; 26:1109–1118
34. Zannas AS, Binder EB: Gene-environment interactions at theFKBP5 locus: sensitive periods, mechanisms and pleiotropism.Genes Brain Behav 2014; 13:25–37
35. Boccardi M, Almici M, Bresciani L, Caroli A, Bonetti M,Monchieri S, Gennarelli M, Frisoni GB: Clinical and medialtemporal features in a family with mood disorders. NeurosciLett 2010; 468:93–97
36. Mervaala E, Föhr J, Könönen M, Valkonen-Korhonen M, VainioP, Partanen K, Partanen J, Tiihonen J, Viinamäki H, KarjalainenAK, Lehtonen J: Quantitative MRI of the hippocampus andamygdala in severe depression. Psychol Med 2000; 30:117–125
37. Hou Z, Yuan Y, Zhang Z, Bai F, Hou G, You J: Longitudinalchanges in hippocampal volumes and cognition in remittedgeriatric depressive disorder. Behav Brain Res 2012; 227:30–35
38. Banegas I, Prieto I, Alba F, Vives F, Araque A, Segarra AB, DuránR, de Gasparo M, Ramírez M: Angiotensinase activity is asym-metrically distributed in the amygdala, hippocampus and pre-frontal cortex of the rat. Behav Brain Res 2005; 156:321–326
39. Wu HM, Wang C, Wang XL, Wang L, Chang CW, Wang P, Gao GD:Correlations between angiotensinase activity asymmetries inthe brain and paw preference in rats. Neuropeptides 2010; 44:253–259
40. Castrén E: Neurotrophic effects of antidepressant drugs. CurrOpin Pharmacol 2004; 4:58–64
8 ajp.psychiatryonline.org AJP in Advance
GENE VARIANTS OF THE RENIN-ANGIOTENSIN SYSTEM

ORIGINAL RESEARCH
APOE ε4 associated with preserved executive functionperformance and maintenance of temporal and cingulate brainvolumes in younger adults
Warren D. Taylor1,2 & Brian Boyd2 & Rachel Turner2 & Douglas R. McQuoid3 &
Allison Ashley-Koch4 & James R. MacFall5 & Ayman Saleh1 & Guy G. Potter3
# Springer Science+Business Media New York 2016
Abstract The APOE ε4 allele is associated with cognitivedeficits and brain atrophy in older adults, but studies in youn-ger adults are mixed.We examined APOE genotype effects oncognition and brain structure in younger adults and whether ge-notype effects differed by age and with presence of depression.157 adults (32 % ε4 carriers, 46 % depressed) between 20 and50 years of age completed neuropsychological testing, 131 ofwhich also completed 3 T cranial MRI. We did not observe adirect effect of APOE genotype on cognitive performance orstructural MRI measures. A significant genotype by age interac-tion was observed for executive function, where age had less ofan effect on executive function in ε4 carriers. Similar interactionswere observed for the entorhinal cortex, rostral and caudal
anterior cingulate cortex and parahippocampal gyrus, where theeffect of age on regional volumes was reduced in ε4 carriers.There were no significant interactions between APOE genotypeand depression diagnosis. The ε4 allele benefits younger adultsby allowing them to maintain executive function performanceand volumes of cingulate and temporal cortex regions with ag-ing, at least through age fifty years.
Keywords Aging . Depression . Cognition .MRI . Apoe
Background
There is a need to identify early biomarkers indicative ofAlzheimer’s disease risk as the presentation of clinically evi-dent symptoms lag behind the development of neuropatholo-gy (Jack et al. 2013, Risacher and Saykin 2013). Supportingthis goal, it is important to understand how genetic differencesthat increase Alzheimer’s disease risk may influence cognitiveperformance and brain structure in pre-clinical populations.This is particularly relevant to younger adult populationswho could benefit from preventive strategies. When consider-ing genotypic effects, it is important to test not only for directrelationships but also whether genetic influences alter the ef-fect of age on clinical or imaging measures. Similarly, it isimportant to examine interactive effects of common condi-tions that are themselves associated with an increased risk ofdementia, such as depression (Byers et al. 2012).
Apolipoprotein E (apoE) is a very-low-density lipoproteininvolved in transporting cholesterol from the blood. In thecentral nervous system, the apoE lipoprotein is involved inmobilization of cholesterol and fatty acids, aids in recoveryfrom injury and promotes synaptic plasticity (Mahley andHuang 2012; Nathan et al. 1994). The human APOE genecoding for this protein is located on chromosome 19 and has
Preliminary data were previously presented at the 53rd Annual Meetingof the American College of Neuropsychopharmacology.
Electronic supplementary material The online version of this article(doi:10.1007/s11682-016-9522-9) contains supplementary material,which is available to authorized users.
* Warren D. [email protected]
1 The Geriatric Research, Education, and Clinical Center (GRECC),Department of Veterans Affairs Medical Center, Tennessee ValleyHealthcare System, Nashville, TN 37212, USA
2 The Center for Cognitive Medicine, Department of Psychiatry,Vanderbilt University Medical Center, 1601 23rd Avenue South,Nashville, TN 37212, USA
3 Department of Psychiatry and Behavioral Sciences, Duke UniversityMedical Center, Durham, NC 27710, USA
4 Center for Human Disease Modeling and Department of Medicine,Duke University Medical Center, Durham, NC 27710, USA
5 Department of Radiology, Duke University Medical Center,Durham, NC 27710, USA
Brain Imaging and BehaviorDOI 10.1007/s11682-016-9522-9
Author's personal copy

3 allelic variants: ε2, ε3, and ε4. A large body of work dem-onstrates that the APOE ε4 allele is the primary genetic riskfactor for the development of Alzheimer’s disease in later life(Corder et al. 1993, Strittmatter et al. 1993) and, comparedwith non-carriers, even healthy older ε4 carriers exhibit dif-ferences on cognitive testing (Caselli et al. 2004). Similarly,healthy older ε4 carriers exhibit smaller volumes and greaterrates of atrophy in multiple cortical and subcortical regions(Donix et al. 2010, Honea et al. 2009, Risacher et al. 2010,Taylor et al. 2014, Wishart et al. 2006). In contrast, the APOEε2 allele may have protective effects, as it is associated withreduced age-related cognitive decline and lower risk for de-veloping Alzheimer’s disease (Suri et al. 2013).
Studies investigating the APOE ε4 allele’s effects on cog-nition in younger adult carriers are less consistent. Comparedwith noncarriers, several reports found that younger adult ε4carriers exhibited better cognitive performance (Schultz et al.2008, Yu et al. 2000) on tasks of attention (Rusted et al. 2013),verbal memory (delayed recall) (Mondadori et al. 2007), ver-bal fluency (Alexander et al. 2007, Marchant et al. 2010), andprospective memory (Evans et al. 2014, Marchant et al. 2010).In context with observations in geriatric populations, thesefindings support a theory that APOE ε4 exhibits antagonisticpleiotropy, or different effects on cognition at different ages(Han and Bondi 2008). However, other studies failed to ob-serve differences on cognitive performance based on APOEgenotype (Bunce et al. 2011, Ihle et al. 2012, Jorm et al. 2007,Matura et al. 2014, Richter-Schmidinger et al. 2011), raisingquestions about this theory and whether APOE genotype hasany effect on cognition in younger adults.
There is less work in younger adults examining the effectsof APOE genotype on brain structure. Studies examiningsmall samples report that young adult and midlife ε4 carriersexhibit smaller hippocampal volumes (Lind et al. 2006,O’Dwyer et al. 2012) while others report that younger adultcarriers exhibit increased entorhinal cortex volumes(DiBattista et al. 2014). Analyses utilizing voxel-based ap-proaches are mixed: some find no difference in cortical graymatter volume (Dowell et al. 2013, Matura et al. 2014) whileothers report thinner cortex in frontal regions (Fennema-Notestine et al. 2011). Such differences may be reconciledby observations that the ε4 allele may be associated with re-gionally different effects, as a study examining gray matternetworks in younger carriers found the ε4 allele was associat-ed with gray matter reductions in frontal and cingulate re-gions, but relative increases in other regions including thehippocampus (Alexander et al. 2012).
Just as aging is a risk factor for developing Alzheimer’sdisease, so is depression (Byers et al. 2012, Diniz et al.2013). Depression increases the risk of dementia even occur-ring over a decade before dementia onset, although the effectof earlier life depression is primarily in APOE ε4 carriers(Karlsson et al. 2015). Early work concluded that APOE
genotype is not a risk factor for depression (Steffens et al.2003), but recent longitudinal population-based studies foundthat the ε4 allele was associated with prospectively identifieddepressive symptoms (Skoog et al. 2015). Studies in de-pressed older populations report that ε4 carriers exhibit greaterdepression severity, poorer cognitive performance, and small-er frontotemporal volumes (Corsentino et al. 2009, Kim et al.2002, Lavretsky et al. 2003, Niti et al. 2009, Qiu et al. 2009,Rajan et al. 2014, Yuan et al. 2010). This work suggests thereis an interactive or additive effect of depression and APOEgenotype on cognitive decline, brain atrophy and risk of de-mentia (Rajan et al. 2014). It is unclear if such relationshipsexist in younger adult populations where depression is asso-ciated with structural alterations in frontal, temporal, and cin-gulate regions (Kempton et al. 2011, Pizzagalli 2011) andneurocognitive differences (McClintock et al. 2010). Giventhe overlap in depressive and cognitive symptoms in olderadults, it is important to examine if depression and APOEgenotype may have interactive effects in younger adults.
The purpose of the study was to examine influences ofAPOE genotype on cognition and gray matter structure in ayoung to midlife adult sample. Given the nature of the rela-tionships between APOE ε4 genotype and pathological aging,we hypothesized we would observe an interactive effect be-tween APOE genotype and age on cognition and brain struc-ture. We also sought to determine whether APOE genotype’seffects on cognition and brain structure differs in individualswith current major depressive disorder.
Methods
Participants
Participants between the ages of 20 and 50 years were enrolledat Duke University and Vanderbilt University. Depressed par-ticipants had a DSM-IV diagnosis of recurrent MDD, asassessed by the Mini-International NeuropsychiatricInterview (MINI, version 5.0) (Sheehan et al. 1998) and inter-view with a study psychiatrist. Additional entry criteria in-cluded onset of first depressive episode before age 35 yearsand a Montgomery-Asberg Depression Rating Scale(MADRS) (Montgomery and Asberg 1979) of 15 or greater.Entry criteria specified no antidepressant use in the last month;however, most subjects reported no antidepressant use for atleast three months or longer. Eligible control subjects hadneither any lifetime history of psychiatric disorders nor anyhistory of psychotropic medication use.
Exclusion criteria included other lifetime DSM-IV Axis Idisorders including substance abuse or dependence. Subjectswere excluded for Axis II disorders determined by theStructured Clinical Interview for DSM-IV Axis IIPersonality Disorders (SCID-II) (First et al. 1997).
Brain Imaging and Behavior
Author's personal copy

Additional exclusion criteria included: history of psychosis,acute suicidality, use of illicit substances in the last month,ECT in the last 6 months, a family history of bipolar disorder,any unstable medical condition, any history of neurologicalillness or head injury, or MRI contraindications.
Both the Duke University Medical Center InstitutionalReview Board and the Vanderbilt University InstitutionalReview Board approved this study. All study participants pro-vided informed consent.
Neuropsychological testing
Participants completed a battery of neuropsychological teststhat covered cognitive domains relevant to depression. Atrained psychometric technician supervised by a licensed clin-ical psychologist administered neuropsychological testing.
Similar to our past approach in late-life depression (Shelineet al. 2010), we created rationally constructed composite do-main variables from a broad test battery. To combine tasks, wecreated Z-scores for each measure based on the performanceof all participants and averaged the Z-scores for all tests withineach domain for each individual. Internal consistency for eachdomain was assessed using Cronbach’s coefficient alpha(CoA). This resulted in four composite neuropsychologicalmeasures: a) episodic memory (Logical Memory 1 and 2;Benton Visual Retention Test, number correct; Rey’s VerbalLearning Test, total I-V and total VII, CoA = 0.87); b) execu-tive function (Controlled Oral Word Association [COWA] test(total score); Trails B time (reverse scored time to comple-tion); verbal fluency (total phonological and semantic);Stroop Color-Word interference condition (number complet-ed); CoA = 0.75); c) processing speed (Symbol-DigitModality (number completed); Trails A (reverse scored timeto completion); Stroop color naming condition (number com-pleted); CoA = 0.70); and d) working memory (Digit spanforward (number of trials correctly completed); digit spanbackward (number of trials correctly completed);CoA = 0.75).
MRI acquisition
To simplify data analyses across two sites using different MRIscanners by different manufacturers, only subjects with MRIdata acquired at Duke University was included in these anal-yses. Cranial MRI was performed using the eight-channelparallel imaging head coil on a whole-body MRI system(Trio, Siemens Medical Systems, Malvern, PA). Parallel im-aging was employed with an acceleration factor of 2.Duplicate T1-weighted image sets were acquired during thescan session using a sagittal MPRAGE sequence with TR/TE = 2300/3.46 msec, a 240 Hz/pixel bandwidth, a256 × 256matrix, a 240 mmdiameter field-of-view, 160 slices
with a 1.2 mm slice thickness, yielding an image with voxelsizes of 0.9 × 0.9 × 1.2 mm.
Analyses of volumetric and cortical thickness MRI data
All volumetric measures were calculated using FreeSurfer(version 5.1) software running in a high-performance Linuxcluster environment. The FreeSurfer methods used to derivecortical and subcortical brain volumes have been previouslydescribed. (Dale et al. 1999, Fischl et al. 2002, Fischl et al.2004a, Fischl et al. 2004b) Cortical parcellation used theDesikan-Killiany Atlas; (Desikan et al. 2006) in each hemi-sphere, this method identified 33 cortical and 7 subcorticalgray matter regions (nucleus accumbens, amygdala, caudate,hippocampus, pallidum, putamen, and thalamus). Intracranialvolume was assessed using the method implemented inFreeSurfer. We visually inspected the data by overlaying thesurfaces and subcortical segmentations over the T1 data.Individual slices in each orientation were assessed for errors.No manual corrections were needed.
We also tested for differences in cortical thickness usingFreesurfer’s QDEC module. This was an atheoretical ap-proach to test for differences not captured in atlas-based com-parisons. In this method, cortical thickness is computed as theshortest distance between any point on the pial surface and thegray/white boundary and vice-versa; these two values are av-eraged (Fischl and Dale 2000).Mapswere smoothed using thestandard Gaussian kernel of 10 mm. We used a general linearmodel (GLM) to test for differences in cortical thickness whilecorrecting for multiple comparisons using the Monte Carlosimulation method. Data were tested against an empirical nulldistribution of maximum cluster size by running 10,000 syn-thesized Gaussian noise simulations with an initial thresholdof p < 0.01. Right and left hemispheres were tested separately.
Selection of a priori regions of interest
Selection of a priori volumetric regions for primary analyseswas based on work that identified APOE genotype effects onregional volumes. These included: the amygdala, hippocam-pus, entorhinal cortex, parahippocampal gyrus, precuneus,and cingulate cortex (Donix et al. 2010, Honea et al. 2009,Hostage et al. 2014, O’Dwyer et al. 2012, Reinvang et al.2013, Risacher et al. 2010, Taylor et al. 2014). For the cingu-late cortex, we examined anterior divisions due to its implica-tion in depression (Pizzagalli 2011) and posterior divisionsdue to APOE genotype’s influence on metabolism in midlifepopulations (Protas et al. 2013).
Genotyping
Genotyping was conducted on blood samples. APOE alleles(corresponding to allele combinations at single nucleotide
Brain Imaging and Behavior
Author's personal copy

polymorphism (SNP) +3937/rs429358 and SNP + 4075/rs7412) were genotyped using the ABI 7900 TaqMan(Applied Biosystems, Foster City, California, USA) system.The two APOE single nucleotide polymorphisms exist at ami-no acid 112 and 158, which are targeted by the TaqManprobes. The individual genotypes at the two sites are thencombined to create a single standard APOE genotype.
Analytic plan
Our a priori hypotheses involved interactive effects betweenAPOE ε4 genotype, age, and depression diagnosis, so we tooka stepwise approach. All analyses were conducted with SAS9.4 (Cary, NC) using PROC MIXED. Our primary analysesincluded all participants regardless of APOE genotype, how-ever as the APOE ε2 allele may have protective effects (Suriet al. 2013) we also conducted follow-up analyses where ε2carriers were excluded.
First, we created initial models that did not include interac-tion terms but instead tested for a direct effect of APOE ε4genotype. In these models, either cognitive domain z-scores orMRI measures were the dependent variable, with APOE ε4genotype (presence or absence of an ε4 allele), diagnosis (de-pressed/never depressed), age, sex, and race (white or minor-ity). Analyses of cognitive data included the additional covar-iate of years of education, while analyses of imaging dataincluded total intracranial volume and hemisphere. After test-ing for initial effects, we subsequently created additionalmodels that included either an APOE by age interaction termor an APOE by diagnosis interaction term. Final models testedfor a three-way age by APOE by depression diagnosisinteraction.
For analyses of cognition, we focused on our a priori planof examining the z-transformed summary measures of pro-cessing speed, working memory, episodic memory, and exec-utive function. For domains with a statistically significant ge-notype effect or interaction term, we planned for subsequentanalyses that would examine the individual z-transformedtests within those domains.
For analyses of volumetric MRI data, we initially focusedon our a priori regions as described above. Subsequent analy-ses also considered other brain regions not specified in our apriori hypotheses but quantified by our image analysis meth-od. Given the large number of regions identified, for analysesof regions not included in our a priori hypotheses we correctedfor multiple comparisons using the false discovery rate (FDR)method. When testing for differences in cortical thicknessusing FreeSurfer’s QDEC module, we used a general linearmodel (GLM) to test for differences between genotypegroups, including age as an additional independent variable.This allowed us to examine the direct effects of APOE geno-type on cortical thickness as well as test for statistical interac-tions between genotype and age.
To elucidate the relationship between cognition and struc-ture, we examined cognitive domains and brain regions iden-tified as exhibiting statistically significant relationship in theabove planned analyses. In these analyses, we examined the z-transformed cognitive domain score as the dependent variable.Independent variables included age, sex, diagnosis, race, andeducation. We also included brain regions as independent var-iables, utilizing the mean volume across the hemispheres, nor-malized for total intracranial volume.
Results
APOE genotype effects on cognitive performance
The sample for cognitive analyses included participants re-cruited at both the Duke and Vanderbilt sites. This consistedof 107 APOE ε4 negative individual (48 % depressed,N = 51)and 50 APOE ε4 positive individuals (42 % depressed,N = 21; Table 1). There was no significant difference inAPOE ε4 frequency between diagnostic groups (χ2 = 0.44,p = 0.5070). The complete genotypic breakdown consisted of:2/2, N = 2; 2/3, N = 14; 2/4, N = 4; 3/3, N = 87; 3/4, N = 45;4/4, N = 5). The depressed cohort was significantly older andexhibited greater severity of depressive symptoms byMADRS than the nondepressed cohort, but there was no sig-nificant difference in age or MADRS score within each diag-nostic cohort between those who were and were not ε4 car-riers. After controlling for demographic covariates, we did notobserve any statistically significant differences in the z-transformed cognitive domain scores between individualsidentified by both genotype and diagnosis (Table 1).
In primary models without interaction terms, we did notfind direct effects of either APOE genotype or diagnosis onany cognitive domain score. We also did not observe anystatistically significant interactions between depression diag-nosis and genotype on cognitive domain scores. Similarly, wedid not find statistically significant three-way interactions be-tween APOE genotype, age, and depression.
On testing for an interaction between age and APOE geno-type, we found a significant interaction for executive function(F1,149 = 4.23, p = 0.0415) and a trend for episodic memory(F1,149 = 3.16, p = 0.0779) but no difference for other domains(working memory: F1,149 = 1.90, p = 0.1707; processingspeed: F1,149 = 0.01, p = 0.9038). In analysis of executivefunction, APOE ε4 noncarriers exhibited worse executivefunction with increasing age than did the ε4 carriers (Fig. 1).In other words, presence of the APOE ε4 allele reduced theeffect of age on executive function.
We conducted additional analyses for the executive func-tion and episodic memory domains, examining the z-transformed individual test items included in the compositedomain scores. Controlling for the same covariates as in
Brain Imaging and Behavior
Author's personal copy

primary models, for the executive function domain we foundsignificant interactions between age and genotype for Trails B(time to completion; F1,149 = 4.39, p = 0.0378) and COWAtotal score (F1,149 = 8.97, p = 0.0032), but not verbal fluency(F1,149 = 0.48, p = 0.4880) or Stroop color-word interference(F1,149 = 0.08, p = 0.7722). For the episodic memory domain,there was a significant interaction only for the Benton VisualRetention Test (number correct; F1,149 = 7.00, p = 0.0090).
The interactions were similar to those observed with the ex-ecutive function composite score, where ε4 carriers exhibitedless reduction in performance with age (Fig. 1). In the absenceof the age by genotype interaction term, APOE genotype didnot have a direct effect on test measures.
Secondary analyses where we excluded the twenty ε2 car-riers were largely concordant with the results described above.We continued to observe a significant interaction between age
Table 1 Demographic and cognitive domain score differences by APOE genotype and diagnostic group
APOE ε4 –Depressed(N = 51)
APOE ε4 –Nondepressed(N = 56)
APOE ε4 + Depressed(N = 21)
APOE ε4 + Nondepressed(N = 29)
TestStatistic
p value
Age (y) 36.5 (8.8) 29.2 (8.2) 36.8 (8.8) 31.4 (10.1) F = 7.69 p < 0.0001
Sex (% female) 66.7 % (34) 58.9 % (33) 76.2 % (16) 68.9 % (20) χ2 = 2.32 p = 0.5088
Race (% Caucasian) 64.7 % (33) 51.8 % (29) 61.9 % (13) 51.7 % (15) χ2 = 2.39 p = 0.4955
Education (y) 15.5 (2.5) 15.8 (1.9) 14.7 (2.1) 16.1 (2.4) F = 1.83 p = 0.1434
MADRS 23.9 (4.2) 0.6 (0.9) 24.4 (5.2) 1.31 (1.4) F = 692.83 p < 0.0001
Episodic memory - 0.76 (4.16) 0.92 (4.02) - 1.35 (4.22) 0.62 (3.40) F = 0.38 p = 0.7675
Executive function - 0.95 (3.07) 0.49 (3.12) 0.13 (2.97) 0.40 (3.06) F = 1.67 p = 0.1762
Processing speed - 0.76 (2.35) 0.57 (2.39) - 0.28 (1.89) 0.30 (2.46) F = 1.21 p = 0.3094
Working memory - 0.28 (1.68) 0.48 (1.75) - 0.10 (1.68) - 0.15 (1.72) F = 1.13 p = 0.3383
Continuous measures presented as mean (standard deviation). Group differences in demographic variables (age, education, MADRS score) tested usinganalysis of variance (ANOVA) where the model had a total 156 degrees of freedom. Categorical variables presented as percentage (number), differencestested using chi-square with 3 degrees of freedom. Cognitive domain data presented as z-transformed scores, mean (SD). These cognitive domainmodelstested for 4-way group differences and included 147 degrees of freedom, controlling for age, sex, education, and race
Fig. 1 Differential effect of age between APOE ε4 carriers andnoncarriers on z-transformed cognitive performance. Data presented arethe domain and tests exhibiting statistically significant age by genotypeinteractive effects on performance, after controlling for depressiondiagnosis, sex, race, and education. The executive function domain isthe averaged z-score over multiple neuropsychological tests, including
Trails Part B, COWA, verbal fluency and the Stroop color-wordcondition. The individual tests presented are those with statisticallysignificant interactions between genotype and age, and included BVRTfrom the episodic memory domain. APOE ε4 noncarriers are triangles/solid line, APOE ε4 carriers are squares/dashed line. Z-transformed testperformance score on the y-axis, age in years on x-axis
Brain Imaging and Behavior
Author's personal copy

and genotype for executive function (F1129 = 5.36,p = 0.0222), but there was no support for a trend with episodicmemory (F1129 = 2.63, p = 0.1074). Analyses of specific cog-nitive tests resulted in findings similar to those reportedabove, aside from Trails B time to completion that nolonger achieved statistical significance (F1129 = 3.84,p = 0.0523). Again, ε4 carriers exhibited less reductionin performance with age and in the absence of the ageby genotype interaction term, APOE genotype did nothave a direct effect on any test measure.
APOE genotype effects on regional brain volumes
To simplify analyses of MRI data across sites with differentMRI manufacturers, we only included MRI data from theDuke site. Notably, 9 participants recruited at Duke eithercould not complete MRI or had MRI data of poor qualityand so could not be included in analyses. The sample withMRI and APOE genotype data thus included 58 individualswith MDD and 73 never-depressed comparison subjects.There was no difference in APOE ε4 frequency between de-pressed and nondepressed groups in the MRI sample (ε4 –,MDDN = 41; ε4 –, noMDDN = 47; ε4 +,MDDN = 17; ε4 +,no MDD N = 26; χ2 = 0.58, p = 0.4452). Other demographiccomparisons were comparable to the larger sample(Supplemental Table 1).
In primary models examining a priori defined regionalbrain volumes, we did not find direct effects of either APOEgenotype or depression diagnosis on any region. Wealso did not observe any statistically significant interac-tions between depression diagnosis and genotype on re-gional volumes. Similarly, we did not find statisticallysignificant three-way interactions between APOE geno-type, age, and depression.
In analyses of our a priori defined regions, we observedstatistically significant interactions between APOE genotypeand age for the entorhinal cortex, rostral and caudal cingulatecortex (Table 2). Similar to what is observed in the cognitiveanalyses, the APOE ε4 allele reduced the effect of ageon regional volumes (Fig. 2). In other words, the rela-tionship between age and volume exhibits a more neg-ative slope in APOE ε4 noncarriers compared with ε4carriers. These findings persisted when removing the seventeenAPOE ε2 allele carriers, and we additionally observed an inter-action between age and genotype for the parahippocampalgyrus.
Additional analyses examined other regions measured byFreeSurfer that were not part of our a priori hypotheses, wherewe again created similar models testing for direct and interac-tive effects of APOE genotype. After FDR correction for mul-tiple comparisons, we observed neither statistically significantprimary effects nor interactive effects of APOE genotype.
APOE genotype effects on cortical thickness
We found no statistically significant effects where APOE ge-notype was directly associated with differences in corticalthickness. When examining age by genotype interactions,we did not observe any regions where the effect of age oncortical thickness differed significantly between the APOEgenotype groups. Similarly, we observed no differences whentesting for different effects of genotype between depressed andnondepressed participants.
Relationship between cognitive domains and regionalbrain volumes
Finally we sought to examine the relationship between cognitivedomains and regional volumes identified in the above analyses.These analyses focused on the z-transformed executive functiondomain score, examining the entorhinal cortex, parahippocampalgyrus, and caudal and rostral anterior cingulate cortex volumes.After controlling for demographic differences, normalizedparahippocamapal gyrus (F1,124 = 7.66, p = 0.0065) and rostralanterior cingulate cortex volumes (F1,124 = 6.18, p = 0.0143)were significantly associated with executive function. Therewas also a trend for the caudal anterior cingulate cortex volume(F1,124 = 3.86, p = 0.0518) but no relationship with entorhinalcortex volume (F1,124 = 2.06, p = 0.1536).
Discussion
Our major finding is that in a younger adult population, theAPOE ε4 allele reduces the effect of aging on executive func-tion and regional brain volumes in temporal and anterior cin-gulate regions. Overall APOE ε4 carriers exhibited less reduc-tion in executive function and regional volumes with age thandid APOE ε4 noncarriers. We did not observe a direct effect ofAPOE genotype on cognition or brain morphology. We alsodid not find evidence to support that depression diagnosisinteracted with APOE genotype to result in greater deficitsin cognition or altered brain morphology. These findings werepersistent across the entire sample, then also when we limitedthe sample to individuals who did not carry the ε2 allele.
Integration with aging literature
Our analyses of APOE genotype’s effect in younger adults areconcordant with and extend past work. These findings supportthe theory of antagonistic pleiotropy (Han and Bondi 2008),or that the ε4 allele has different effects on cognition at differ-ent ages. This may represent superior compensatory functionduring midlife. Had our sample’s age extended past age50 years, we anticipate that we would observe a downwardcurve in the age-cognition relationship in older ε4 carriers.
Brain Imaging and Behavior
Author's personal copy

Recent work suggests this more rapid rate of cognitive declinein ε4 carriers occurs around age 70 years (Jack et al. 2015),well beyond our current sample.
There is still uncertainty about what cognitive domains maybe differentially affected by APOE genotype. We found thatgenotype influenced the effect of age in our executive functiondomain (specifically performance on the Trails B and COWA)and visual memorymeasured with the BVRT. These findings aresupported by past studies (Marchant et al. 2010), althoughAPOEeffects on attention (Rusted et al. 2013) may also be influencingperformance on our executive function tests.
Our neuroimaging findings follow a pattern similar to ourcognitive findings. These results are discrepant with a previ-ous study that did not observe interactive effects of APOEgenotype and age on structural measures (Filippini et al.2011). However, that study examined a smaller sample withtwo distinct age populations rather than a young to midlifeadult sample with a continuous age range.
This work supports that aging is associated with poorer cog-nitive performance and smaller brain volumes, even in young tomidlife adults. Our observations occur before ages where signif-icant increases in amyloidosis occur (Jack et al. 2015) and suchaging effects are reduced in APOE ε4 carriers. Brain aging inyounger adults may be due tomultiple causes, including vascularrisk factors, early tauopathy (Crary et al. 2014, Jack et al. 2013),or occur in the absence of any specific pathology (Jagust 2013).Further work is needed to better understand what processes aremodified in APOE ε4 allele carriers and how that benefit tocognition and brain structure is obtained prior to later amyloiddeposition and cognitive decline.
Integration with depression literature
It is clear that neuropathology related to cognitive decline canoccur decades before the onset of clinical symptoms (Jack
et al. 2013) and that earlier-life onset is associated with in-creased dementia risk (Byers et al. 2012). However, there arefew studies examining the relationship between depressionand risk factors for Alzheimer’s disease in younger adult pop-ulations. We observed neither differential effects of APOEgenotype nor different genotype by age interactions betweendepressed and nondepressed individuals. This does not sup-port a theory that cognitive or morphological differences re-lated to APOE genotype may adversely affect neural circuitryin such a way that it would increase a predisposition to de-pression. Overall this suggests that the ultimate pathways bywhich depression increases dementia risk does not occurthrough apolipoprotein E mediated mechanisms in youngeradults. However, the underlying nature of the relationship be-tween depression and dementia remains an important questionand alternative pathways should be considered, such as therelationship between depression and proinflammatoryprocesses.
Study strengths and limitations
The study has several strengths, including a large sample sizeand comprehensive neuropsychological testing battery.Moreover image analyses utilized a combination ofhypothesis-testing and hypothesis-generating approaches.These methods are complementary, as we found no re-lationship between study measures and cortical thick-ness, but did find volumetric differences in cingulatecortex regions and subcortical structures. Finally, inpost-hoc analyses, we demonstrated a relationship be-tween the identified cognitive domain (executive func-tion) and identified brain regions (parahippocampal gy-rus and rostral anterior cingulate cortex).
The study also has limitations. Although we have a broadcognitive battery, specific domains such as attention (Rusted
Table 2 Interactive effects ofAPOE genotype and age on apriori brain region volumes
All MRI Subjects (N = 131) APOE ε3 and ε4 carriers only (N = 114)
Region F value p value F value p value
Amygdala F = 3.37 p = 0.0685 F = 2.09 p = 0.1514
Cingulate, Caudal Anterior F = 5.94 p = 0.0161 F = 4.18 p = 0.0434
Cingulate, Rostral Anterior F = 5.08 p = 0.0260 F = 3.94 p = 0.0496
Cingulate, Isthmus F = 0.14 p = 0.7057 F = 0.62 p = 0.4338
Cingulate, Posterior F = 0.86 p = 0.3565 F = 1.16 p = 0.2838
Entorhinal cortex F = 6.64 p = 0.0111 F = 5.35 p = 0.0226
Hippocampus F = 3.10 p = 0.0808 F = 2.71 p = 0.1025
Parahippocampal gyrus F = 3.06 p = 0.0828 F = 3.92 p = 0.0503
Precuneus F = 0.45 p = 0.5028 F = 0.15 p = 0.7009
Variables for the entire sample analyses had 1129 df. Variables in analyses where ε2 carriers were excluded had1112 df. Mixed models included the independent variables of APOE ε4 genotype, diagnosis (depressed/neverdepressed), age, sex, race, intracranial volume, and hemisphere
Brain Imaging and Behavior
Author's personal copy

et al. 2013) were not assessed. Additionally, this was a well-educated sample and it is unclear if these results would gen-eralize to populations with lower education. Moreover,although we examine age effects, this remains a cross-sectional study. Ultimately longitudinal studies are nec-essary to examine change in such measures and agingtrajectories. Finally, there are notable limitations relatedto the sample, including a lower number of APOE ε4allele carriers than ε4 noncarriers, although this limita-tion applies to much of the existent literature. The agedifference between the diagnostic cohorts is also impor-tant. The strong effect of age on both cognitive andbrain aging may have negatively affected our ability todetect a diagnosis by genotype interaction.
It should be emphasized that despite examining a relativelylarge sample, we made numerous statistical comparisons. For
our a priori hypotheses, we did not control for multiple com-parisons, thus increasing the risk for a type 1 error. Given thesignificance levels observed, correcting for multiple compar-isons would have resulted in null findings. Thus while ourfindings fit within past literature, they should be viewedcautiously.
Despite these limitations, this study advances our un-derstanding of the aging process by demonstrating thatthe APOE ε4 allele mitigates the effect of age on cog-nitive processes and brain structure in early- to midlife-adulthood. This occurs prior to significant increases in amy-loid deposition as detected by PETscanning (Jack et al. 2015),suggesting that the ε4 allele may modify other processesinfluencing brain aging. More work is needed to determinewhat those processes are, but also to determine how depres-sion may increase risk of dementia.
Fig. 2 Differences in age effectson regional brain volumesbetween APOE ε4 positive andnegative individuals. Datapresented are those regionsexhibiting statistically significantage by genotype interactiveeffects on regional volumes, aftercontrolling for depressiondiagnosis, sex, race, intracranialvolume and hemisphere. Similarfindings were observedunilaterally for the hippocampus,parahippocampus, and amygdala(figures not shown). APOE ε4noncarriers are triangles/solidline, APOE ε4 carriers aresquares/dashed line. Z-transformed test performancescore on the y-axis, age in yearson x-axis. Regional volume inmilliliters on the y-axis, age inyears on x-axis
Brain Imaging and Behavior
Author's personal copy

Acknowledgments This project was supported by National Institute ofMental Health (NIMH) grant R01 MH077745. It was further supportedby CTSA award UL1TR000445 from the National Center for AdvancingTranslational Sciences (NCATS) and conducted in part using the re-sources of the Advanced Computing Center for Research andEducation at Vanderbilt University, Nashville, TN.
Compliance with ethical standards
Disclosures All authors (including Dr. Taylor, Mr. Boyd, Ms. Turner,Mr. McQuoid, Dr. Ashley-Koch, Dr. MacFall, Dr. Saleh, and Dr. Potter)declare they have no conflict of interest.
Informed consent statement All procedures followed were in accor-dance with the ethical standards of the responsible committee on humanexperimentation (institutional and national) and with the HelsinkiDeclaration of 1975, and the applicable revisions at the time of the inves-tigation. Informed consent was obtained from all patients for being in-cluded in the study.
References
Alexander, D. M., Williams, L. M., Gatt, J. M., Dobson-Stone, C., Kuan,S. A., Todd, E. G., et al. (2007). The contribution of apolipoproteinE alleles on cognitive performance and dynamic neural activity oversix decades. Biological Psychology, 75(3), 229–238.
Alexander, G. E., Bergfield, K. L., Chen, K., Reiman, E. M., Hanson, K.D., Lin, L., et al. (2012). Gray matter network associated with riskfor alzheimer’s disease in young to middle-aged adults.Neurobiology of Aging, 33(12), 2723–2732.
Bunce, D., Anstey, K. J., Burns, R., Christensen, H., & Easteal, S. (2011).Does possession of apolipoprotein E varepsilon4 benefit cognitive func-tion in healthy young adults? Neuropsychologia, 49(7), 1693–1697.
Byers, A. L., Covinsky, K. E., Barnes, D. E., & Yaffe, K. (2012).Dysthymia and depression increase risk of dementia and mortalityamong older veterans. The American Journal of GeriatricPsychiatry, 20(8), 664–672.
Caselli, R. J., Reiman, E. M., Osborne, D., Hentz, J. G., Baxter, L. C.,Hernandez, J. L., & Alexander, G. G. (2004). Longitudinal changesin cognition and behavior in asymptomatic carriers of the APOE e4allele. Neurology, 62(11), 1990–1995.
Corder, E. H., Saunders, A. M., Strittmatter, W. J., Schmechel, D. E.,Gaskell, P. C., Small, G. W., et al. (1993). Gene dose of apolipopro-tein E type 4 allele and the risk of alzheimer’s disease in late onsetfamilies. Science, 261(5123), 921–923.
Corsentino, E. A., Sawyer, K., Sachs-Ericsson, N., & Blazer, D. G.(2009). Depressive symptoms moderate the influence of theapolipoproteine epsilon4 allele on cognitive decline in a sample ofcommunity dwelling older adults. The American Journal ofGeriatric Psychiatry, 17(2), 155–165.
Crary, J. F., Trojanowski, J. Q., Schneider, J. A., Abisambra, J. F., Abner,E. L., Alafuzoff, I., et al. (2014). Primary age-related tauopathy(PART): a common pathology associated with human aging. ActaNeuropathologica, 128(6), 755–766.
Dale, A. M., Fischl, B., & Sereno, M. I. (1999). Cortical surface-basedanalysis. I. Segmentation and surface reconstruction. NeuroImage,9(2), 179–194.
Desikan, R. S., Segonne, F., Fischl, B., Quinn, B. T., Dickerson, B. C.,Blacker, D., et al. (2006). An automated labeling system forsubdividing the human cerebral cortex on MRI scans into gyralbased regions of interest. NeuroImage, 31(3), 968–980.
DiBattista, A. M., Stevens, B.W., Rebeck, G. W., & Green, A. E. (2014).Two alzheimer’s disease risk genes increase entorhinal cortex vol-ume in young adults. Frontiers in Human Neuroscience, 8, 779.
Diniz, B.S., Butters, M.A., Albert, S.M., Dew, M.A., Reynolds, C.F.,3rd.(2013). Late-life depression and risk of vascular dementia andalzheimer’s disease: systematic review and meta-analysis ofcommunity-based cohort studies. The British Journal ofPsychiatry, 202(5), 329–335.
Donix, M., Burggren, A. C., Suthana, N. A., Siddarth, P., Ekstrom, A. D.,Krupa, A. K., et al. (2010). Longitudinal changes in medial temporalcortical thickness in normal subjects with the APOE-4 polymor-phism. NeuroImage, 53(1), 37–43.
Dowell, N. G., Ruest, T., Evans, S. L., King, S. L., Tabet, N., Tofts, P. S.,& Rusted, J. M. (2013). MRI of carriers of the apolipoprotein E e4allele-evidence for structural differences in normal-appearing braintissue in e4+ relative to e4- young adults. NMR in Biomedicine,26(6), 674–682.
Evans, S., Dowell, N. G., Tabet, N., Tofts, P. S., King, S. L., & Rusted, J.M. (2014). Cognitive and neural signatures of the APOE E4allele in mid-aged adults. Neurobiology of Aging, 35(7),1615–1623.
Fennema-Notestine, C., Panizzon, M. S., Thompson, W. R., Chen, C. H.,Eyler, L. T., Fischl, B., et al. (2011). Presence of ApoE epsilon4allele associated with thinner frontal cortex in middle age. Journalof Alzheimer's Disease, 26(Suppl 3), 49–60.
Filippini, N., Ebmeier, K. P., MacIntosh, B. J., Trachtenberg, A. J.,Frisoni, G. B., Wilcock, G. K., et al. (2011). Differential effects ofthe APOE genotype on brain function across the lifespan.NeuroImage, 54(1), 602–610.
First, M. B., Gibbon, M., Spitzer, R. L., Williams, J. B., & Benjamin, L. S.(1997). Structured clinical interview for DSM-IV axis II personalitydisorders (SCID-II). Washington, D.C.: American Psychiatric Press,Inc..
Fischl, B., & Dale, A. M. (2000). Measuring the thickness of the humancerebral cortex frommagnetic resonance images. Proceedings of theNational Academy of Sciences of the United States of America, 97,11050–11055.
Fischl, B., Salat, D. H., Busa, E., Albert, M., Dieterich, M., Haselgrove, C.,et al. (2002). Whole brain segmentation: automated labeling of neuro-anatomical structures in the human brain. Neuron, 33(3), 341–355.
Fischl, B., Salat, D. H., van der Kouwe, A. J., Makris, N., Segonne, F.,Quinn, B. T., & Dale, A. M. (2004a). Sequence-independent seg-mentation of magnetic resonance images.NeuroImage, 23(Suppl 1),S69–S84.
Fischl, B., van der Kouwe, A., Destrieux, C., Halgren, E., Segonne, F.,Salat, D. H., et al. (2004b). Automatically parcellating the humancerebral cortex. Cerebral Cortex, 14(1), 11–22.
Han, S. D., & Bondi, M. W. (2008). Revision of the apolipoprotein Ecompensatory mechanism recruitment hypothesis. Alzheimer’s &Dementia: the Journal of the Alzheimer’s Association, 4(4), 251–254.
Honea, R. A., Vidoni, E., Harsha, A., & Burns, J. M. (2009). Impact ofAPOE on the healthy aging brain: a voxel-based MRI and DTIstudy. Journal of Alzheimer's Disease, 18(3), 553–564.
Hostage, C. A., Choudhury, K. R., Murali Doraiswamy, P., Petrella, J. R., &Alzheimer’sDiseaseNeuroimaging, I. (2014).Mapping the effect of theapolipoprotein E genotype on 4-year atrophy rates in an Alzheimerdisease-related brain network. Radiology, 271(1), 211–219.
Ihle, A., Bunce, D., & Kliegel, M. (2012). APOE epsilon4 and cognitivefunction in early life: a meta-analysis. Neuropsychology, 26(3), 267–277.
Jack Jr., C. R., Knopman, D. S., Jagust, W. J., Petersen, R. C., Weiner, M.W., Aisen, P. S., et al. (2013). Tracking pathophysiological processesin alzheimer’s disease: an updated hypothetical model of dynamicbiomarkers. Lancet Neurology, 12(2), 207–216.
Brain Imaging and Behavior
Author's personal copy

Jack Jr., C. R., Wiste, H. J., Weigand, S. D., Knopman, D. S., Vemuri, P.,Mielke, M. M., et al. (2015). Age, sex, and APOE epsilon4 effectson memory, brain structure, and beta-amyloid across the adult lifespan. JAMA Neurology, 72(5), 511–519.
Jagust, W. (2013). Vulnerable neural systems and the borderland of brainaging and neurodegeneration. Neuron, 77(2), 219–234.
Jorm, A. F., Mather, K. A., Butterworth, P., Anstey, K. J., Christensen, H., &Easteal, S. (2007). APOE genotype and cognitive functioning in a largeage-stratified population sample. Neuropsychology, 21(1), 1–8.
Karlsson, I. K., Bennet, A. M., Ploner, A., Andersson, T. M.,Reynolds, C. A., Gatz, M., & Pedersen, N. L. (2015).Apolipoprotein E epsilon4 genotype and the temporal rela-tionship between depression and dementia. Neurobiology ofAging, 36(4), 1751–1756.
Kempton, M. J., Salvador, Z., Munafo, M. R., Geddes, J. R., Simmons,A., Frangou, S., & Williams, S. C. (2011). Structural neuroimagingstudies in major depressive disorder: meta-analysis and comparisonwith bipolar disorder. Archives of General Psychiatry, 68(7), 675–690.
Kim, D. H., Payne, M. E., Levy, R. M., MacFall, J. R., & Steffens, D. C.(2002). APOE genotype and hippocampal volume change in geriat-ric depression. Biological Psychiatry, 51, 426–429.
Lavretsky, H., Ercoli, L., Siddarth, P., Bookheimer, S., Miller, K., &Small, G. (2003). Apolipoprotein epsilon4 allele status, depressivesymptoms, and cognitive decline inmiddle-aged and elderly personswithout dementia. The American Journal of Geriatric Psychiatry,11(6), 667–673.
Lind, J., Larsson, A., Persson, J., Ingvar, M., Nilsson, L. G.,Backman, L., et al. (2006). Reduced hippocampal volumein non-demented carriers of the apolipoprotein E epsilon4:relation to chronological age and recognition memory.Neuroscience Letters, 396(1), 23–27.
Mahley, R. W., & Huang, Y. (2012). Apolipoprotein e sets thestage: response to injury triggers neuropathology. Neuron,76(5), 871–885.
Marchant, N. L., King, S. L., Tabet, N., & Rusted, J. M. (2010).Positive effects of cholinergic stimulation favor young APOEepsilon4 carriers. Neuropsychopharmacology, 35(5), 1090–1096.
Matura, S., Prvulovic, D., Jurcoane, A., Hartmann, D., Miller, J., Scheibe,M., et al. (2014). Differential effects of the ApoE4 genotype on brainstructure and function. NeuroImage, 89, 81–91.
McClintock, S. M., Husain, M. M., Greer, T. L., & Cullum, C. M. (2010).Association between depression severity and neurocognitive func-tion in major depressive disorder: a review and synthesis.Neuropsychology, 24(1), 9–34.
Mondadori, C. R., de Quervain, D. J., Buchmann, A., Mustovic, H.,Wollmer, M. A., Schmidt, C. F., et al. (2007). Better memory andneural efficiency in young apolipoprotein E epsilon4 carriers.Cerebral Cortex, 17(8), 1934–1947.
Montgomery, S. A., & Asberg, M. (1979). A new depression scale de-signed to be sensitive to change. The British Journal of Psychiatry,134, 382–389.
Nathan, B. P., Bellosta, S., Sanan, D. A., Weisgraber, K. H.,Mahley, R. W., & Pitas, R. E. (1994). Differential effectsof apolipoproteins E3 and E4 on neuronal growth in vitro.Science, 264(5160), 850–852.
Niti, M., Yap, K. B., Kua, E. H., & Ng, T. P. (2009). APOE-epsilon4,depressive symptoms, and cognitive decline in Chinese older adults:Singapore longitudinal aging studies. The Journals of GerontologySeries A, Biological Sciences and Medical Sciences, 64(2), 306–311.
O’Dwyer, L., Lamberton, F., Matura, S., Tanner, C., Scheibe, M., Miller,J., et al. (2012). Reduced hippocampal volume in healthy youngApoE4 carriers: an MRI study. PloS One, 7(11), e48895.
Pizzagalli, D. A. (2011). Frontocingulate dysfunction in depression: towardbiomarkers of treatment response. Neuropsychopharmacology, 36,183–206.
Protas, H. D., Chen, K., Langbaum, J. B., Fleisher, A. S., Alexander, G.E., Lee, W., et al. (2013). Posterior cingulate glucose metab-olism, hippocampal glucose metabolism, and hippocampalvolume in cognitively normal, late-middle-aged persons at 3levels of genetic risk for Alzheimer disease. JAMA Neurology,70(3), 320–325.
Qiu, A., Taylor, W. D., Zhao, Z., MacFall, J. R., Miller, M. I., Key, C. R.,et al. (2009). APOE related hippocampal shape alteration in geriatricdepression. NeuroImage, 44, 620–626.
Rajan, K. B., Wilson, R. S., Skarupski, K. A., Mendes de Leon,C. F., & Evans, D. A. (2014). Gene-behavior interaction ofdepressive symptoms and the apolipoprotein E {varepsilon}4allele on cognitive decline. Psychosomatic Medicine, 76(2),101–108.
Reinvang, I., Espeseth, T., & Westlye, L. T. (2013). APOE-related bio-marker profiles in non-pathological aging and early phases ofalzheimer’s disease. Neuroscience and Biobehavioral Reviews,37(8), 1322–1335.
Richter-Schmidinger, T., Alexopoulos, P., Horn, M., Maus, S.,Reichel, M., Rhein, C., et al. (2011). Influence of brain-derived neurotrophic-factor and apolipoprotein E genetic var-iants on hippocampal volume and memory performance inhealthy young adults. Journal of Neural Transmission,118(2), 249–257.
Risacher, S. L., & Saykin, A. J. (2013). Neuroimaging and otherbiomarkers for alzheimer’s disease: the changing landscape ofearly detection. Annual Review of Clinical Psychology, 9,621–648.
Risacher, S. L., Shen, L., West, J. D., Kim, S., McDonald, B. C., Beckett,L. A., et al. (2010). Longitudinal MRI atrophy biomarkers: relation-ship to conversion in the ADNI cohort. Neurobiology of Aging,31(8), 1401–1418.
Rusted, J. M., Evans, S. L., King, S. L., Dowell, N., Tabet, N., & Tofts, P.S. (2013). APOE e4 polymorphism in young adults is associatedwith improved attention and indexed by distinct neural signatures.NeuroImage, 65, 364–373.
Schultz, M. R., Lyons, M. J., Franz, C. E., Grant, M. D., Boake,C., Jacobson, K. C., et al. (2008). Apolipoprotein E genotypeand memory in the sixth decade of life. Neurology, 70(19 Pt2), 1771–1777.
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J.,Weiller, E., et al. (1998). The Mini-International NeuropsychiatricInventory (M.I.N.I.): the development and validation of a structureddiagnostic interview for DSM-IV and ICD-10. The Journal ofClinical Psychiatry, Suppl 20, 22–33.
Sheline, Y. I., Pieper, C. F., Barch, D. M., Welsh-Boehmer, K.,McKinstry, R. C., MacFall, J. R., et al. (2010). Support for thevascular depression hypothesis in late-life depression: results of a2-site, prospective, antidepressant treatment trial. Archives ofGeneral Psychiatry, 67(3), 277–285.
Skoog, I., Waern, M., Duberstein, P., Blennow, K., Zetterberg, H.,Borjesson-Hanson, A., et al. (2015). A 9-year prospectivepopulation-based study on the association between the APOE*E4allele and late-life depression in Sweden. Biological Psychiatry,78(10), 730–736.
Steffens, D. C., Norton, M. C., Hart, A. D., Skoog, I., Corcoran, C., &Breitner, J. C. (2003). Apolipoprotein E genotype and major depres-sion in a community of older adults. The cache county study.Psychological Medicine, 33, 541–547.
Strittmatter, W. J., Saunders, A. M., Schmechel, D., Pericak-Vance, M.,Enghild, J., Salvesen, G. S., & Roses, A. D. (1993). ApolipoproteinE: high-avidity binding to beta-amyloid and increased frequency oftype 4 allele in late-onset familial Alzheimer disease. Proceedings of
Brain Imaging and Behavior
Author's personal copy

the National Academy of Sciences of the United States of America,90, 1977–1981.
Suri, S., Heise, V., Trachtenberg, A. J., & Mackay, C. E. (2013).The forgotten APOE allele: a review of the evidence andsuggested mechanisms for the protective effect of APOEvarepsilon2. Neuroscience and Biobehavioral Reviews, 37(10Pt 2), 2878–2886.
Taylor, J. L., Scanlon, B. K., Farrell, M., Hernandez, B.,Adamson, M. M., Ashford, J. W., et al. (2014). APOE-epsilon4 and aging of medial temporal lobe gray matter inhealthy adults older than 50 years. Neurobiology of Aging,35(11), 2479–2485.
Wishart, H. A., Saykin, A. J., McAllister, T. W., Rabin, L. A., McDonald,B. C., Flashman, L. A., et al. (2006). Regional brain atrophy incognitively intact adults with a single APOE epsilon4 allele.Neurology, 67(7), 1221–1224.
Yu, Y. W., Lin, C. H., Chen, S. P., Hong, C. J., & Tsai, S. J. (2000).Intelligence and event-related potentials for young female humanvolunteer apolipoprotein E epsilon4 and non-epsilon4 carriers.Neuroscience Letters, 294(3), 179–181.
Yuan, Y., Zhang, Z., Bai, F., You, J., Yu, H., Shi, Y., & Liu, W. (2010).Genetic variation in apolipoprotein E alters regional gray mattervolumes in remitted late-onset depression. Journal of AffectiveDisorders, 121(3), 273–277.
Brain Imaging and Behavior
Author's personal copy

WMHs in LLDLLD is consistently associated with greater WMH severity25–28 andgreater measured WMH volumes.10,29–31 These observationsguided proposals for MRI-defined vascular depression diagnosticcriteria that include a lesion severity criterion.32,33 In suchconceptualizations, age at the initial depressive episode is animportant consideration. Compared with early-onset depression,individuals with a later onset (for example, after 50 years) exhibitgreater WMH severity5,18,31,34–38 and cognitive impairment.39,40
However, ‘vascular depression’ as a potential diagnostic entitymay not be limited to late-onset patients. Individuals with anearlier onset are at increased vascular risk, as precedentdepression is associated with increased risk of vascular diseaseand stroke.41–45 Depression in early and midlife may promoteinflammation46–48 or epigenetic modifications of genes related tovascular homeostasis.49 Thus, some individuals with early-onsetdepression may be prone to ‘vascular depression’ later in life.
Localization of WMHsAlthough many studies do not specify lesion location, distinctionsin WMH location are important in understanding their role in LLD.In nondepressed samples, periventricular WMHs are more closelyassociated with cognitive impairment than are deep WMHs.50–52 Itis possible that this is due to anatomical differences, as theperiventricular region has a high density of long associating fiberswith cortical–subcortical connections, whereas subcortical deepwhite matter has a high density of shorter U-fibers connectingadjacent cortical regions.52,53 However, as WMH severity acrossregions is highly correlated, distinctions between periventricularand deep WMH may be arbitrary and reflect total WMH disease.54
Nonetheless, others have localized WMHs associated withdepression to the frontal55–58 and temporal lobe.59 Morerecently several groups reported that LLD is associated withgreater WMH severity in specific white matter fiber tracts,including the cingulum bundle, uncinate fasciculus and superiorlongitudinal fasciculus.60–62
WMHs and cerebral functionA small number of studies suggest that greater WMH burden isassociated with disrupted function in motor, cognitive and affectivecircuits. During a simple motor task, high WMH burden is associatedwith low BOLD functional signal,63 suggesting that WMH diseaseinterferes with the neural circuit mediating the task. Otherstudies64,65 associated low BOLD activity with poorer performanceon executive tasks, supporting the model of altered white matterintegrity leading to cognitive network dysfunction. Greater WMHvolume is further associated with altered default mode networkconnectivity at rest between the posterior cingulate cortex andmedial prefrontal cortex (PFC).66 During affective tasks in LLD, WMHsare associated with altered functional activity with an exaggerationof the functional ‘depression’ fMRI patterns: individuals with highWMH burden showed hyperactivation in limbic regions whenpresented with fearful faces.67
Neuropathological studiesStudies utilizing both neuroimaging and neuropathologicaltechniques demonstrate that WMHs represent a wide range ofpathological processes, including perivascular demyelination,arteriosclerosis, ischemia, gliosis, or partial loss of myelin andaxons.15,68,69 Generally, confluent deep WMH but notperiventricular WMH appear to be related to ischemic processes.70
There are also regional differences in WMH etiology. Seminalwork by Thomas and colleagues14 showed that deep WMH andpunctate lesions of depressed older adults are most likely to haveischemic origins. In LLD ischemic lesions are also more likely tooccur in the dorsolateral prefrontal cortex, instead of the anterior
cingulate cortex or occipital lobe. Similarly, depressed eldersexhibit increased expression of cellular adhesion molecules in thedorsolateral prefrontal cortex, but not the anterior cingulate cortexor occipital lobe.71–73 Cellular adhesion molecules are inflam-matory markers whose expression is increased by ischemia,supporting a role for ischemia in LLD and highlighting therelationship between vascular and inflammatory processes.Although ischemic pathology is thus consistently localized tothe dorsolateral prefrontal cortex, other frontal regions may alsobe involved. Depressed elders exhibit decreased density ofpyramidal neurons in the orbitofrontal cortex, which may be theresult of vascular processes74 in arterioles and medium arteries,75
or alterations in astrocyte-associated immune function.76
Neuropathological studies also demonstrate that LLD candevelop in the absence of significant vascular abnormalities. In astudy of late-onset depressed elders, depression was not relatedto either lacunes or microvascular lesions.77 Similarly, in apopulation-based study in which depression was ascertained ina pre-mortem diagnostic interview, depression was associatedneither with cerebrovascular nor Alzheimer pathology.78 However,in contrast to prior studies,79 depression was associated with thepresence of Lewy bodies.78 Such findings highlight theheterogeneity of pathologies that present as depression.
THE DEPRESSION-EXECUTIVE DYSFUNCTION SYNDROME ANDCOGNITIVE DEFICITS IN LLDA ‘depression-executive dysfunction syndrome’4 wasconceptualized as the clinical expression of frontal networkimpairment caused by vascular and other age-related factors.Accordingly, this syndrome describes depressed patients withvascular disease and evidence of impairment in networks relatedto mood and executive function.80
Executive function is a frontally mediated domain81–83 thatencompasses cognitive processes including selective attention,response inhibition and performance monitoring. It is clinicallyexpressed as difficulty with planning, sequencing, organizing andabstracting. These deficits are common in LLD,84–87 particularly inlate-onset depression.40,86,88 Efforts to characterize thepresentation of the depression-executive dysfunction syndromehave dichotomized samples by their performance on executivefunction tasks. When compared with depressed elders withoutexecutive dysfunction, patients with depression-executivedysfunction exhibit reduced fluency, impaired visual naming,suspiciousness, anhedonia, psychomotor retardation andsignificant disability.89–91 As discussed later, studies across eightdifferent samples identified executive dysfunction as a predictorof poor antidepressant response.92–99
Broader cognitive deficits in LLD: relationship with vascular riskfactorsIndividuals with LLD exhibit executive dysfunction and deficitsacross other cognitive domains, including episodic memory,working memory, visuospatial ability and processingspeed.84,87,100–105 Processing speed deficits may influence othercognitive deficits103–105 and mediate in part executive taskperformance.106 Although cognitive performance improves withsuccessful antidepressant treatment, such deficits can persist andperformance may not be restored to a normal level.100,107–109
Cognitive deficits are associated with vascular dysfunction. Innondepressed cohorts, there are associations between episodicmemory, psychomotor speed and executive function, andmeasures of vascular dysfunction, such as hypertension, heartrate variability and orthostasis.110–112 In LLD, Framingham VascularRisk scores113 are associated with deficits in processing speed,executive function and episodic memory.98,104 Greater WMHburden is associated not only with executive dysfunction,
Mechanisms underlying vascular depressionWD Taylor et al
2
Molecular Psychiatry (2013), 1 – 12 & 2013 Macmillan Publishers Limited

perseveration and slowed processing speed12,61,114–117 but alsowith episodic and visuospatial memory deficits.102,110,118,119 Thesecross-sectional observations are supported by longitudinal studies,demonstrating that progression of WMH severity parallelscognitive decline.120–122
WMHs localized to specific fiber tracts are associated withspecific cognitive deficits. Executive function deficits are asso-ciated with WMHs in the uncinate fasciculus, superior longitudinalfasciculus and the cingulum bundle.123 Similarly, episodic memorydeficits are associated with WMHs in the cingulum bundle andinferior longitudinal fasciculus.123,124
VASCULAR DEPRESSION AND COURSE OF DEPRESSIONCognitive dysfunction and antidepressant outcomesIn LLD, the relationship between treatment outcome andexecutive dysfunction is well established. Multiple studiesdemonstrate that executive dysfunction predicts poor acuteresponse of LLD to antidepressants.92,94,96,97,99,125 Executivedysfunction is also associated with high relapse and recurrencerates,126 although not all studies found this association.127 Much ofthis work used the Mattis Dementia Rating Scale Initiation-Perseveration (I/P) subtest, which yields a composite score ofseveral executive skills.128 Notably, a recent meta-analysisexamined the relationship between antidepressant response andperformance across multiple executive tests, including the I/Psubtest, the Wisconsin Card Sort Test, the Stroop Color-Word testand others. The authors concluded that the I/P subtest was theonly test providing reliable discrimination between antidepressantresponders and nonresponders.129 Further analysis of I/P subtestcomponents showed that semantic strategy (semantic clustering)while performing the I/P verbal fluency task explained most of thevariance in predicting remission.130 Effective semantic strategyappears to be associated with treatment response regardless ofthe probing task; effective semantic strategy during verballearning task was also associated with high LLD remissionrate.131 These observations suggest that preserved semanticorganization, rather than fluency or verbal learning, is critical forremission during antidepressant treatment. However, impairedresponse inhibition is another aspect of executive dysfunction thatinfluences antidepressant response.92,95,125,132
Corroborating the role of the cognitive control network in LLDare reports examining resting state functional connectivity (FC).Low-resting FC in the cognitive control network, but not in thedefault network, predict poor, acute antidepressant remissionrates along with persistence of depression, apathy and dys-executive behavior.133
Other cognitive deficits can influence outcomes. Poorerperformance on tests of episodic memory, language processingand processing speed are associated with poorer acute anti-depressant response,98 and may predict poorer long-term courseof depression.134 Further analysis is needed to identify asuperordinate cognitive dysfunction that accounts for therelationship of these tests to antidepressant response.
WMHs as a predictor of antidepressant outcomesAlthough greater WMH severity is often associated with pooreracute antidepressant response,36,98,99,135–138 results areinconsistent.97,139–142 Importantly, these studies assess totalcerebral WMH severity, while the effect of WMLs on theantidepressant response may depend on lesion location.138
Unfortunately, methodological differences in assessing WMHseverity make it difficult to reconcile discrepant findings acrossstudies.143,144
Most studies used cross-sectional WMH measures to predictoutcome. However, WMHs are a progressive rather than a staticprocess,11,145 and rate of change may be a more important
predictor. The few studies in LLD cohorts examining this questionfound that greater increases in WMH volume over 2- and 4-yearintervals are associated with nonremission or relapse.146,147
Some have examined both WMH severity and cognitivedysfunction as predictors of outcome. In these studies cognitivemeasures are generally a better predictor of antidepressantresponse than are WMH measures. The largest published studyexamining a 12-week response to sertraline found that poorerresponse was independently associated with greater WMHseverity and poorer performance in cognitive domains of episodicmemory, language processing, processing speed and executivefunction. However, in models controlling for baseline depressionseverity, WMH severity was no longer associated with response.98
Smaller studies have found similar patterns, wherein initialassociations between WMH severity and response were not statis-tically significant in models incorporating cognitive measures.97,99
Other measures of white matter integrity are associated withantidepressant response. In voxel-wide analysis, microstructuralwhite matter abnormalities (low fractional anisotropy, FA) inmultiple frontolimbic brain areas, including the rostral and dorsalanterior cingulate, dorsolateral PFC, genu of the corpus callosum,hippocampus and posterior cingulate, were associated withnonremission.148 In region of interest analyses, low FA in thecorpus callosum, left superior corona radiata and right inferiorlongitudinal fasciculum, was associated with lower remissionrates.149 In contrast, others found that higher prefrontal whitematter FA was associated with a failure to remit toantidepressants,150 a finding that parallels reports in depressionof increased FC to a dorsal nexus.151 Notably, depressed elderly5-HTTLPR polymorphism short allele carriers had lower FA thanlong allele homozygotes in frontolimbic areas, including theanterior cingulate, posterior cingulate, dorsolateral and medialprefrontal regions.152 Such differences in FA can be caused byseveral pathologies, not all of which are vascular in nature.
VASCULAR RISK GENES IN DEPRESSIONThere is a wide literature examining genetic influences inLLD, including reports examining polymorphisms in BDNF,APOE and serotonin transporter (5-HTTLPR) genes, amongothers (see recent reviews by Lotrich153 and Benjamin andTaylor154). Within this field, there are an increasing number ofreports associating LLD with genetic polymorphisms, increasingvascular risk.
One example of this literature includes studies examininggenetic variation of the renin-angiotensin system (RAS). The RASregulates fluid homeostasis and blood pressure, and is a target fortwo classes of antihypertensive drugs. Beyond influencing vascularfunction, RAS polymorphisms may also increase the risk ofdepression via modulation of monoamines155 or contributing tohypothalamic–pituitary–adrenal axis dysregulation.156 Resultsfrom studies examining the common angiotensin-convertingenzyme (ACE) insertion/deletion polymorphism are mixed inadult depression157–162 and suicidality,162–164 although other ACEpolymorphisms may be important.161,165,166 Despite its key role inthe RAS, the gene encoding for the angiotensin II type 1 receptor(AGTR1) is less well studied. The CC genotype of the A1166C(rs5186) polymorphism is associated with increased responsive-ness to Ang-II.167 However, despite one study associating theCC genotype with increased risk of major depressive disorder,159
this was not replicated in an elderly sample.168
RAS variation is further related to differences in brain structureand function. Several studies in older adults have now associatedvariants in ACE and AGTR1 with altered cerebral frontotemporalstructure169–172 and abnormal default mode network activity.173
AGTR1 variants are associated with greater WMH progression,particularly in men,168 and this effect may be localized to specifictracts.60
Mechanisms underlying vascular depressionWD Taylor et al
3
& 2013 Macmillan Publishers Limited Molecular Psychiatry (2013), 1 – 12

RAS polymorphisms may also influence antidepressant out-comes. In a general adult population, the ACE D variant and theAGTR1 C1166 allele are associated with better acute antidepres-sant response.174,175 However, this contrasts with a study of LLD,wherein AGTR1 C1166 allele homozygous individuals exhibited apoorer antidepressant response over a longer period.176 Such agedifferences could be important, reflecting stress reactivity in earlierlife and allostatic effects of an overly active RAS later in life.
MECHANISTIC HYPOTHESESAccording to a model by Alexopoulos,1 the clinical expression ofLLD is mediated by altered brain activity in cognitive and affectivecircuits, characterized as hypometabolism of dorsal corticalregions and hypermetabolism of ventral limbic structures. Age-,disease- and stress-related neurobiological changes serve asetiological factors, contributing to alterations in circuitsregulating mood and cognition. The impact of theseneurobiological contributors can be increased by vulnerabilityfactors originating from preexisting differences in mood circuitry.
Arguably, such etiological factors may lead to depression onlyafter crossing a certain threshold, above which they acquire adose-effect relationship (Figure 1). In this conceptualization, singleor multiple potential ‘etiological factors’ may reach an initialseverity threshold and contribute to LLD ‘vulnerability’ due tofrontolimbic compromise evident through imaging or abnormalperformance on cognitive or affective tasks. When etiologicalfactors further increase in severity and cross a second threshold,they may have a greater and direct effect on mood circuitfunction, leading to affective and cognitive symptomatology. Ofcourse, instead of threshold effects such relationships could becumulative following linear or curvilinear patterns.
Such a threshold model can account for multifactorialcontributions to LLD. It also explains why our best clinical andbiological measures predict only a modest part of the variance indistinguishing LLD from controls and in predicting treatmentresponse as any individual measure may itself not cross a crucialthreshold. This model allows for mixed syndromes of multipleetiological contributors, if each disturbance alone or in combina-tion is strong enough to cross the threshold required to induceneural circuit changes mediating LLD.
Given the central role of vascular disease and WMHs in much ofthe literature, it is worth examining their role within this model.WMHs can be conceptualized as visible markers of ischemicdamage, although vascular compromise may result in insults to
white and/or gray matter that are not visible on conventionalneuroimaging.177 In this context, greater WMH severity representsa state of vascular compromise and ischemic injury in specificregions. Depending on the severity of the underlying WMLs andhow strongly they affect affective and cognitive circuitry, suchdamage may itself predispose individuals to depressive episodes.However, WMHs may also be an index of the severity ofunderlying vascular disease affecting neural circuits. In this case,the direct effect of WMHs on neural circuits may be modestcompared with that of the underlying vascular process.
The disconnection hypothesisBuilding on the concept of ‘disconnection syndromes,’ ischemiaand WMLs may contribute to depression by disrupting neuralconnections among regions regulating mood and cognition.178 Inthis model, global cerebral WMH severity is less germane to LLDthan is focal damage to specific fiber tracts and neural circuits.Such focal damage would adversely affect the tract’s structuraland functional connectivity. In turn, this state adversely affects thefunction of connected regions at rest and during cognitive tasks,and contribute to neural circuitry alterations that mediate clinicalsymptoms and influence antidepressant response.
This view is supported by studies examining WMH location.Recent work demonstrates that LLD is associated with greaterWMH severity in specific tracts including the cingulum bundle,uncinate fasciculus and superior longitudinal fasciculus.60–62
In addition, greater WMH severity in the uncinate andsuperior longitudinal fasciculi is associated with executivedysfunction61,123,124 and greater depression severity.179
These macrostructural MR findings are supported by diffusiontensor imaging (DTI) studies, examining white matter microstruc-ture. DTI changes reflect various pathologies leading to decreasedmyelin integrity, including demyelination secondary to cerebro-vascular and inflammatory changes. WMLs occurring in fiber tractsare also associated with DTI changes.177,180 LLD is associated withdifferences on DTI measures of the uncinate fasciculus, cingulumbundle, anterior thalamic radiation and superior longitudinalfasciculus.181,182 The uncinate fasciculus and cingulum bundle areparticularly relevant to LLD183–188 because of their role incognition and emotion processing,188,189 although other tractsare also associated with antidepressant response in LLD.149
Importantly, differences in the uncinate fasciculus and cingulumbundle are also observed in younger, depressed adults.190,191
Although those younger adult studies do not necessarily suggest avascular cause in that population, they support that structuralalterations in these fiber tracts are associated with depression.
Structural differences have functional effects. Fiber tractstructural connectivity is positively correlated with resting stateFC of connected regions.192–196 These data warrant acomprehensive examination of the relationships amongischemic focal WML injury, damage to tract microstructure,regional connectivity and circuit function. Examination of such a‘lesion model’ can identify neural circuit deficits contributing todepression and predictive of poor outcomes.
The inflammation hypothesisAging- and disease-related processes promote proinflammatorystates in older individuals.197,198 Further, immune activation canbe a characteristic of depression48,199 and precipitate depressivesymptoms.200 Alexopoulos and Morimoto201 recently proposedthat immune dysregulation may promote the development ofaffective and cognitive symptoms in LLD. This view is supportedby studies in midlife adult populations. Administration ofcytokines or induction of peripheral inflammation results in aninflammatory response, which in turn is correlated with fatigue,slowed reaction time202 and mood reduction.200,203 Even withoutmedical illness, depressed individuals exhibit increased levels of
Figure 1. Proposed progression of etiological processes affectingfrontolimbic function. After crossing an initial threshold, vascular orother processes may serve as one of many factors that increasevulnerability to depression through compromise of affective andcognitive brain circuits. As the underlying disease process pro-gresses, its adverse effects on the affective and cognitive circuitswould likewise increase, resulting in the circuit dysfunctions thatcharacterize depression.
Mechanisms underlying vascular depressionWD Taylor et al
4
Molecular Psychiatry (2013), 1 – 12 & 2013 Macmillan Publishers Limited

proinflammatory cytokines204,205 and reduced anti-inflammatorycytokine levels.206,207
Several mechanisms may explain these relationships. Proin-flammatory cytokines affect monoamine neurotransmitter path-ways,208 including indoleamine 2,3-dioxygenase upregulation andkynurenine pathway activation.209–211 This results in decreasedtryptophan and serotonin and increased synthesis of detrimentaltryptophan catabolites that promote hippocampal damage andapoptosis.211,212 Cytokines, including interleukin (IL)-1b, alsoreduce extracellular serotonin levels by activating the serotonintransporter.213 In addition, proinflammatory cytokines disruptglucocorticoid receptor function214 and reduce neurotrophicsupport.215
Peripheral inflammation is associated with altered brainfunction in areas mediating cognition and mood. In healthyindividuals, typhoid-induced IL-6 levels correlate with lower mood,increased subgenual anterior cingulate cortex activity duringaffective processing and altered subgenual cingulate connectiv-ity.203 Laboratory-administered social stressors increaseinflammatory maker levels that in turn are associated withactivation of the dorsal anterior cingulate cortex and anteriorinsula.216 In bereaved women undergoing grief elicitation,inflammatory markers were positively associated with subgenualcingulate and orbitofrontal cortex activation.217
Supporting this work is a growing literature demonstrating thatgenetic polymorphisms promoting proinflammatory processesmay contribute to depression,218,219 and in LLD may be related toage of onset.220 Such relationships are likely moderated throughan effect on cytokine levels that in turn are associated with sadmood221 and altered emotion processing.222
Regarding LLD, the aging process disrupts immune function,223
increasing peripheral immune activity and shifting the CNS into aproinflammatory state.198 Elevated peripheral cytokine levels areassociated with depressive symptoms in older adults, with the mostconsistent finding being for IL-6, but also implicating IL-1b, IL-8 andtumor necrosis factor-a.224–228 Proinflammatory states in older adultsare associated with cognitive deficits, including poorer executivefunction, poorer memory performance, worse global cognition andsteeper decline in cognition.229–231 Finally, greater IL-6 and C-reactiveprotein levels are associated with greater WMH burden.232–235
Successful antidepressant treatment may reduce proinflamma-tory markers.48 This action may be a direct effect as in vitro studiesdemonstrate that antidepressants reduce proinflammatory markerswhile increasing levels of anti-inflammatory cytokines.236–240 Resultsin clinical populations are inconsistent, but a recent meta-analysisconcluded that antidepressants, particularly SSRIs, reduce IL-6, IL-1band tumor necrosis factor-a.241 Additional evidence supports thatsome anti-inflammatory drugs may have antidepressantproperties,242–244 particularly in individuals with elevated pre-treatment proinflammatory markers.245
Importantly, proinflammatory processes also contribute toneurodegenerative processes. Increased peripheral inflammatorymarker levels are associated with increased risk for all-causedementia,246 and central inflammatory processes significantlycontribute to the pathogenesis of Alzheimer’s disease.247 How-ever, nonsteroidal anti-inflammatory drugs have not consistentlydemonstrated clinical benefit in Alzheimer’s disease,247 and in arecent consensus statement were considered but not recom-mended as a priority for further investigation.248
The hypoperfusion hypothesisVascular dysregulation is common in LLD249–254 and CBFreductions can impair regional brain function, contributing toaffective and cognitive symptoms. Regional cerebral metabolicactivity is tightly correlated with CBF, which is regulated by localinteractions between neurons, glia and the vasculature.255,256
Blood flow to the brain is influenced by systemic hemodynamics
and cerebrovascular autoregulation, with cerebral arteriescontracting or dilating as arterial pressure changes. Theseprocesses interact to maintain stable perfusion. However, theseprocesses are impaired in the context of vascular disease:256
hypertension, diabetes and atherosclerosis leading to vascular wallhypertrophy, reduced arterial lumen diameter, reduced arterialdistensibility and endothelial cell dysfunction.256–258 Such vascularchanges, including increased intima media thickness, increasedarterial stiffness and endothelial dysfunction are pronounced inLLD populations,249–254 and endothelial function may beparticularly poor in antidepressant nonresponders.259 Suchvascular pathology results in reduced blood flow velocities anddecreased vasomotor reactivity,260,261 thus adversely affecting CBF.
Perfusion deficits do not need to cause ischemia in order toinfluence brain function. Reduced CBF impairs protein synthesisthat is262 crucial for cognitive processing263,264 and formaintaining the integrity of cortical functional maps.265 Thus,mild CBF reduction may impair cognitive and affective processes,while greater CBF reduction in the context of autoregulatorydeficits may cause ischemic injury. The subcortical white matteris particularly sensitive to these changes because it is suppliedby terminal arterioles with limited collateral flow,266 and sosusceptible to infarction due to impaired autoregulation.267
Greater WMH severity may be a marker of broader deficits inperfusion and autoregulation as individuals with greater WMHseverity exhibit reduced CBF in both white matter and gray matterregions.268–270 Depressed elders with greater WMH severity alsoexhibit decreased perfusion in the cingulate gyrus,271 a regioninvolved in cognitive and affective processing.272
Positron emission tomography, single-photon emission com-puted tomography and MRI arterial spin labeling have identifiedCBF differences in midlife adult depressed populations.273–276
Advanced age is itself associated with decreased frontotemporalCBF,277 an effect mediated by vascular risk factors.278 In LLD,perfusion deficits are more severe, particularly in the medial andlateral PFC, subcortical and temporal structures.269,279–283 Deficitsin the dorsolateral PFC may improve with antidepressantresponse, while other perfusion deficits may not.281 Othersreport no change in CBF in antidepressant nonresponders,284–288
suggesting that persistently reduced regional CBF may be abiomarker of nonresponse.
Cerebral hypoperfusion is associated not only with Alzheimer’sdisease and mild cognitive impairment,289–291 but also withabnormal performance on specific cognitive tasks.291–294 Forexample, resting hippocampal blood flow is positively correlatedwith spatial memory performance.292 Although not specifically ameasure of perfusion, reduced arterial CBF predicts slowerprocessing speed,295 a domain that may mediate other deficitsin LLD.103 Perfusion deficits may thus contribute to the affectiveand cognitive symptoms observed in LLD. Intriguingly, these datasupport investigating the utility of agents that may improveperfusion or restore endothelial function.296,297
ROLE OF VASCULAR RISK FACTORS IN LLDFifteen years after the formulation of the ‘vascular depression’hypothesis,2 a confluence of findings suggests that:
1 Vascular risk factors and radiological findings are oftenassociated with LLD.
2 Cognitive deficits across multiple domains are common in LLDand associated with vascular risk factors and greater WMHseverity. Such deficits, particularly executive dysfunction,predict poor response to antidepressants.
3 WMHs, although associated with cognitive dysfunction, do notconsistently predict poor antidepressant response. However,progressive WMH disease is associated with poorer depressioncourse.
Mechanisms underlying vascular depressionWD Taylor et al
5
& 2013 Macmillan Publishers Limited Molecular Psychiatry (2013), 1 – 12

The link between progressive vascular disease and thedevelopment and persistence of LLD invites study of theunderlying mechanisms by which vascular disease alters brainfunction in such a way to mediate the development of clinicalsymptoms. The ultimate goal of this line of study is to developnovel treatments or repurpose existent agents to improve LLDoutcomes.
We propose three mechanistic paths to ‘vascular depression.’Although the processes of these pathways could proceedindependently, they are complementary and interconnected andso may all contribute to LLD (Figure 2). For example, inflammationparticipates in vascular remodeling, accelerates vasculardamage298 and can contribute to perfusion deficits. In turn,regional perfusion deficits adversely affect gray matter functionand contribute to the development of WMLs that disrupt regionalstructural and FC.
We are not proposing a single mechanism underlying LLD.Nonvascular factors clearly contribute to LLD. The same genetic,epigenetic and environmental factors that contribute to depres-sion in younger adults continue to confer vulnerability todepression in later life. Moreover, although alterations in immuneand endocrine regulation affect vascular risk, they may alsoincrease the risk of depression through independent mechanisms.
Just as there are nonvascular factors contributing to LLD, theremay be additional mechanisms linking vascular disease with LLD.Altered homocysteine metabolism is associated with LLD,299 withhyperhomocysteinuria potentially contributing to vascular risk byincreasing atherosclerosis and endothelial dysfunction.300 Another
example is altered sympatho–adrenomedullary system andhypothalamic-pituitary-adnenal axis function301 that, amongother activities, affects inflammation.302 These and othermechanisms may contribute to the development orperpetuation of LLD both through vascular and nonvascularpathways and require further study. Such studies would benefitfrom the incorporation of genomic approaches along withmeasures of systemic function, thus linking molecularmechanisms with clinically salient measures and outcomes.
Demonstrating that such mechanisms affect neural circuitfunction, it opens the door for intervention studies examiningwhether modulation of these mechanisms can improve depres-sion outcomes. There is already preliminary support for using anti-inflammatory drugs in depression. Etanercept, a soluble tumornecrosis factor-a receptor, and celecoxib, a cyclo-oxygenase-2inhibitor, may reduce depressive symptoms in patients withinflammatory diseases242,243 and infliximab may improvedepression in patients with greater pre-treatment inflam-mation.245 Similarly, omega-3 fatty acids are anti-inflammatoryand also affect monoamine neurotransmission,303 suggesting anantidepressant role for omega-3 supplementation. However,recent meta-analyses have not provided strong support foromega-3 supplementation for depression, although larger welldesigned trials may be warranted.304,305 Finally, drugs thatmodulate the RAS improve cerebral perfusion297 and mayimprove cognition,306–308 although they have not been wellstudied in depression. We suggest that study of these agents inLLD may produce a novel, targeted pharmacology for the largegroup of LLD patients who are unresponsive to conventionalantidepressants.
CONFLICT OF INTERESTDr. Alexopoulos reports serving as a consultant for Lilly and on the speakers’ bureaufor Astra Zeneca, Forest, Merck, Avanir and Lundbeck. Dr. Alexopoulos also is astockholder of Johnson and Johnson. The remaining authors declare no conflict ofinterest.
ACKNOWLEDGEMENTSThis project was supported by NIH grants R01 MH077745, R01 MH076079, R01MH079414 and P30 MH085943. Dr. Alexopoulos reports research grant support fromForest.
REFERENCES1 Alexopoulos GS. Depression in the elderly. Lancet 2005; 365: 1961–1970.2 Alexopoulos GS, Meyers BS, Young RC, Campbell S, Silbersweig D, Charlson M.
‘Vascular depression’ hypothesis. Arch Gen Psychiatry 1997; 54: 915–922.3 Alexopoulos GS, Meyers BS, Young RC, Kakuma T, Silbersweig D, Charlson M.
Clinically defined vascular depression. Am J Psychiatry 1997; 154: 562–565.4 Alexopoulos GS. ‘The Depression-Executive Dysfunction Syndrome of Late Life’: a
specific target for D3 agonists? Am J Geriatr Psychiatry 2001; 9: 22–29.5 Krishnan KRR, Hays JC, Blazer DG. MRI-defined vascular depression. Am J Psy-
chiatry 1997; 154: 497–501.6 Sneed JR, Rindskopf D, Steffens DC, Krishnan KR, Roose SP. The vascular
depression subtype: evidence of internal validity. Biol Psychiatry 2008; 64:491–497.
7 Awad IA, Spetzler RF, Hodak JA, Awad CA, Carey R. Incidental subcortical lesionsidentified on magnetic resonance imaging in the elderly. I. Correlation with ageand cerebrovascular risk factors. Stroke 1986; 17: 1084–1089.
8 Dufouil C, de Kersaint-Gilly A, Besancon V, Levy C, Auffray E, Brunnereau L et al.Longitudinal study of blood pressure and white matter hyperintensities. The EVAMRI cohort. Neurology 2001; 56: 921–926.
9 Longstreth WTJ, Manolio TA, Arnold A, Burke GL, Bryan N, Jungreis CA et al.Clinical correlates of white matter findings on cranial magnetic resonanceimaging of 3301 elderly people: the cardiovascular health study. Stroke 1996; 27:1274–1282.
10 Taylor WD, MacFall JR, Payne ME, McQuoid DR, Steffens DC, Provenzale JM et al.Greater MRI lesion volumes in elderly depressed subjects than in controlsubjects. Psychiatry Res 2005; 139: 1–7.
Figure 2. This model links the disconnection, inflammation andhypoperfusion processes proposed in late-life depression. Vasculardisease may contribute to altered brain function characteristic ofdepression (dorsal hypometabolism, ventral hypermetabolism)either through structural damage adversely affecting connectivity,through perfusion deficits altering regional function, or both.Proinflammatory processes increase vascular risk, but may alsoaffect brain function through independent processes. In this model,vascular disease is an important and central contributor to LLD. Notonly is vascular disease common and perhaps unavoidable in laterlife, but it also interacts with other pathological processes related todepression. However, vascular disease is not the only contributor toLLD. Other biological and environmental factors can increase therisk for depression by alterating neural circuit structure and function.Similarly, genetic influences may increase risk of depression byacting at multiple points, such altering function of neural circuits,changing the biological response to stress, adding to vascular risk,or predisposing to proinflammatory states.
Mechanisms underlying vascular depressionWD Taylor et al
6
Molecular Psychiatry (2013), 1 – 12 & 2013 Macmillan Publishers Limited

11 Taylor WD, MacFall JR, Provenzale JM, Payne ME, McQuoid DR, Steffens DC et al.Serial MR imaging of hyperintense white matter lesion volumes in elderly sub-jects: correlation with vascular risk factors. Am J Roentgenol 2003; 181: 571–576.
12 Jokinen H, Kalska H, Ylikoski R, Madureira S, Verdelho A, Gouw A et al. MRI-defined subcortical ischemic vascular disease: baseline clinical and neu-ropsychological findings. The LADIS Study. Cerebrovasc Dis 2009; 27: 336–344.
13 Pantoni L, Garcia JH, Gutierrez JA. Cerebral white matter is highly vulnerable toischemia. Stroke 1996; 27: 1641–1646.
14 Thomas AJ, O’Brien JT, Davis S, Ballard C, Barber R, Kalaria RN et al. Ischemic basisfor deep white matter hyperintensities in major depression. Arch Gen Psychiatry2002; 59: 785–792.
15 Thomas AJ, Perry R, Barber R, Kalaria RN, O’Brien JT. Pathologies and pathologicalmechanisms for white matter hyperintensities in depression. Ann NY Acad Sci2002; 977: 333–339.
16 Taylor WD, McQuoid DR, Krishnan KR. Medical comorbidity in late-life depres-sion. Int J Geriatr Psychiatry 2004; 19: 935–943.
17 Vasudev A, O’Brien JT, Tan MP, Parry SW, Thomas AJ. A study of orthostatichypotension, heart rate variability and baroreflex sensitivity in late-life depres-sion. J Affect Disord 2011; 131: 374–378.
18 Lavretsky H, Lesser IM, Wohl M, Miller BL. Relationship of age, age at onset, andsex to depression in older adults. Am J Geriatr Psychiatry 1998; 6: 248–256.
19 Matsubayashi K, Okumiya K, Wada T, Osaki Y, Fujisawa M, Doi Y et al. Posturaldysregulation in systolic blood pressure is associated with worsened scoring onneurobehavioral function tests and leukoaraiosis in the older elderly living in acommunity. Stroke 1997; 28: 2169–2173.
20 Puisieux F, Monaca P, Deplanque D, Delmaire C, di Pompeo C, Monaca C et al.Relationship between leuko-araiosis and blood pressure variability in the elderly.Eur Neurol 2001; 46: 115–120.
21 Isaka Y, Okamoto M, Ashida K, Imaizumi M. Decreased cerebrovascular dilatorycapacity in subjects with asymptomatic periventricular hyperintensities. Stroke1994; 25: 375–381.
22 Bakker SL, de Leeuw FE, de Groot JC, Hofman A, Koudstaal PJ, Breteler MM.Cerebral vasomotor reactivity and cerebral white matter lesions in the elderly.Neurology 1999; 52: 578–583.
23 Marstrand JR, Garde E, Rostrup E, Ring P, Rosenbaum S, Mortensen EL et al.Cerebral perfusion and cerebrovascular reactivity are reduced in white matterhyperintensities. Stroke 2002; 33: 972–976.
24 Oishi M, Mochizuki Y. Regional cerebral blood flow and cerebrospinal fluidglutamate in leukoaraiosis. J Neurol 1998; 245: 777–780.
25 Coffey CE, Figiel GS, Djang WT, Cress M, Saunders WB, Weiner RD. Leukoence-phalopathy in elderly depressed patients referred for ECT. Biol Psychiatry 1988;24: 143–161.
26 Coffey CE, Figiel GS, Djang WT, Saunders WB, Weiner RD. White matter hyper-intensities on magnetic resonance imaging: clinical and anatomic correlates inthe depressed elderly. J Neuropsychiatry Clin Neurosci 1989; 1: 135–144.
27 Dolan RJ, Poynton AM, Bridges PK, Trimble MR. Altered magnetic resonancewhite-matter T1 values in patients with affective disorder. Br J Psychiatry 1990;157: 107–110.
28 Fujikawa T, Yamawaki S, Touhouda Y. Incidence of silent cerebral infarction inpatients with major depression. Stroke 1993; 24: 1631–1634.
29 Greenwald BS, Kramer-Ginsberg E, Krishnan KRR, Ashtari M, Aupperle PM, PatelM. MRI signal hyperintensities in geriatric depression. Am J Psychiatry 1996; 153:1212–1215.
30 Kumar A, Bilker W, Jin Z, Udupa J. Atrophy and high intensity lesions: com-plementary neurobiological mechanisms in late-life depression. Neuropsycho-pharmacology 2000; 22: 264–274.
31 Herrmann LL, Le Masurier M, Ebmeier KP. White matter hyperintensities in late lifedepression: a systematic review. J Neurol Neurosurg Psychiatry 2008; 79: 619–624.
32 Steffens DC, Krishnan KRR. Structural neuroimaging and mood disorders: recentfindings, implications for classification, and future directions. Biol Psychiatry1998; 43: 705–712.
33 Krishnan KRR, Tayor WD, McQuoid DR, MacFall JR, Payne ME, Provenzale JM et al.Clinical characteristics of magnetic resonance imaging-defined subcorticalischemic depression. Biol Psychiatry 2004; 55: 390–397.
34 de Groot JC, de Leeuw F, Oudkerk M, Hofman A, Jolles J, MMB Breteler. Cerebralwhite matter lesions and depressive symptoms in elderly adults. Arch Gen Psy-chiatry 2000; 57: 1071–1076.
35 Figiel GS, Krishnan KRR, Doraiswamy PM, Rao VP, Nemeroff CB, Boyko OB.Subcortical hyperintensities on brain magnetic resonance imaging: a compar-ison between late age onset and early onset elderly depressed subjects.Neurobiol Aging 1991; 12: 245–247.
36 Hickie I, Scott E, Mitchell P, Wilhelm K, Austin MP, Bennett B. Subcorticalhyperintensities on magnetic resonance imaging: clinical correlates and prog-nostic significance in patients with severe depression. Biol Psychiatry 1995; 37:151–160.
37 Salloway S, Malloy P, Kohn R, Gillard E, Duffy J, Rogg J et al. MRI and neu-ropsychological differences in early- and late-life-onset geriatric depression.Neurology 1996; 46: 1567–1574.
38 Kumar A, Bilker W, Jin Z, Udupa J, Gottlieb G. Age of onset of depression andquantitative neuroanatomic measures: absence of specific correlates. PsychiatryRes 1999; 91: 101–110.
39 Dillon C, Allegri RF, Serrano CM, Iturry M, Salgado P, Glaser FB et al. Late- versusearly-onset geriatric depression in a memory research center. Neuropsychiatr DisTreat 2009; 5: 517–526.
40 Rapp MA, Dahlman K, Sano M, Grossman HT, Haroutunian V, Gorman JM.Neuropsychological differences between late-onset and recurrent geriatricmajor depression. Am J Psychiatry 2005; 162: 691–698.
41 Wassertheil-Smoller S, Applegate WB, Berge K, Chang CJ, Davis BR, Grimm Jr. Ret al. Change in depression as a precursor of cardiovascular events. SHEPCooperative Research Group (Systoloc Hypertension in the elderly). Arch InternMed 1996; 156: 553–561.
42 Krishnan M, Mast BT, Ficker LJ, Lawhorne L, Lichtenberg PA. The effects ofpreexisting depression on cerebrovascular health outcomes in geriatric con-tinuing care. J Gerontol A Biol Sci Med Sci 2005; 60: 915–919.
43 Frasure-Smith N, Lesperance F, Talajic M. Depression and 18-month prognosisafter myocardial infarction. Circulation 1995; 91: 999–1005.
44 Musselman DL, Evans DL, Nemeroff CB. The relationship of depression to car-diovascular disease: Epidemiology, biology, and treatment. Arch Gen Psychiatry1998; 55: 580–592.
45 Glassman AH, Bigger JT, Gaffney M, Shapiro PA, Swenson JR. Onset of majordepression associated with acute coronary syndromes: relationship of onset,major depressive disorder history, and episode severity to sertraline benefit. ArchGen Psychiatry 2006; 63: 283–288.
46 Frasure-Smith N, Lesperance F, Irwin MR, Sauve C, Lesperance J, Theroux P.Depression, C-reactive protein and two-year major adverse cardiac events inmen after acute coronary syndromes. Biol Psychiatry 2007; 62: 302–308.
47 Surtees PG, Wainwright NW, Boekholdt SM, Luben RN, Wareham NJ, Khaw KT.Major depression, C-reactive protein, and incident ischemic heart disease inhealthy men and women. Psychosom Med 2008; 70: 850–855.
48 Miller AH, Maletic V, Raison CL. Inflammation and its discontents: the role ofcytokines in the pathophysiology of major depression. Biol Psychiatry 2009; 65:732–741.
49 Zill P, Baghai TC, Schule C, Born C, Frustuck C, Buttner A et al. DNA methylationanalysis of the angiotensin converting enzyme (ACE) gene in major depression.PLoS ONE 2012; 7: e40479.
50 van den Heuvel DM, ten Dam VH, de Craen AJ, Admiraal-Behloul F, Olofsen H,Bollen EL et al. Increase in periventricular white matter hyperintensities parallelsdecline in mental processing speed in a non-demented elderly population.J Neurol Neurosurg Psychiatry 2006; 77: 149–153.
51 Debette S, Bombois S, Bruandet A, Delbeuck X, Lepoittevin S, Delmaire C et al.Subcortical hyperintensities are associated with cognitive decline in patientswith mild cognitive impairment. Stroke 2007; 38: 2924–2930.
52 de Groot JC, De Leeuw FE, Oudkerk M, Van Gijn J, Hofman A, Jolles J et al.Periventricular cerebral white matter lesions predict rate of cognitive decline.Ann Neurol 2002; 52: 335–341.
53 Filley CM. The behavioral neurology of cerebral white matter. Neurology 1998;50: 1535–1540.
54 DeCarli C, Fletcher E, Ramey V, Harvey D, Jagust WJ. Anatomical mapping ofwhite matter hyperintensities (WMH): exploring the relationships betweenperiventricular WMH, deep WMH, and total WMH burden. Stroke 2005; 36:50–55.
55 Firbank MJ, Lloyd AJ, Ferrier N, O’Brien JT. A volumetric study of MRI signalhyperintensities in late-life depression. Am J Geriatr Psychiatry 2004; 12: 606–612.
56 MacFall JR, Payne ME, Provenzale JM, Krishnan KRR. Medial orbital frontal lesionsin late-onset depression. Biol Psychiatry 2001; 49: 803–806.
57 MacFall JR, Taylor WD, Rex DE, Pieper S, Payne ME, McQuoid DR et al. Lobardistribution of lesion volumes in late-life depression: the Biomedical InformaticsResearch Network (BIRN). Neuropsychopharmacology 2005; 31: 1500–1507.
58 Taylor WD, MacFall JR, Steffens DC, Payne ME, Provenzale JM, Krishnan KRR.Localization of age-associated white matter hyperintensities in late-life depres-sion. Prog Neuropsychopharmacol Biol Psychiatry 2003; 27: 539–544.
59 O’Brien JT, Firbank MJ, Krishnan MS, van Straaten EC, van der Flier WM, PetrovicK et al. White matter hyperintensities rather than lacunar infarcts are associatedwith depressive symptoms in older people: the LADIS study. Am J Geriatr Psy-chiatry 2006; 14: 834–841.
60 Taylor WD, Zhao Z, Ashley-Koch A, Payne ME, Steffens DC, Krishnan RR et al.Fiber tract-specific white matter lesion severity Findings in late-life depressionand by AGTR1 A1166C genotype. Hum Brain Mapp 201122; 34: 295–303.
61 Sheline YI, Price JL, Vaishnavi SN, Mintun MA, Barch DM, Epstein AA et al.Regional white matter hyperintensity burden in automated segmentation
Mechanisms underlying vascular depressionWD Taylor et al
7
& 2013 Macmillan Publishers Limited Molecular Psychiatry (2013), 1 – 12

distinguishes late-life depressed subjects from comparison subjects matched forvascular risk factors. Am J Psychiatry 2008; 165: 524–532.
62 Dalby RB, Chakravarty MM, Ahdidan J, Sorensen L, Frandsen J, Jonsdottir KY et al.Localization of white-matter lesions and effect of vascular risk factors in late-onset major depression. Psychol Med 2010; 40: 1389–1399.
63 Patel MJ, Boada FE, Price JC, Sheu LK, Reynolds 3rd CF, Aizenstein HJ. Associationof small vessel ischemic white matter changes with BOLD fMRI imaging in theelderly. Psychiatry Res 2012; 204: 117–122.
64 Mayda AB, Westphal A, Carter CS, DeCarli C. Late life cognitive control deficits areaccentuated by white matter disease burden. Brain 2011; 134(Pt 6): 1673–1683.
65 Venkatraman VK, Aizenstein H, Guralnik J, Newman AB, Glynn NW, Taylor C et al.Executive control function, brain activation and white matter hyperintensities inolder adults. Neuroimage 2010; 49: 3436–3442.
66 Wu M, Andreescu C, Butters MA, Tamburo R, Reynolds 3rd CF, Aizenstein H.Default-mode network connectivity and white matter burden in late-lifedepression. Psychiatry Res 2011; 194: 39–46.
67 Aizenstein HJ, Andreescu C, Edelman KL, Cochran JL, Price J, Butters MA et al.fMRI correlates of white matter hyperintensities in late-life depression. Am JPsychiatry 2011; 168: 1075–1082.
68 Fazekas F, Kleinert R, Offenbacher H, Schmidt R, Kleinert G, Payer F et al.Pathologic correlates of incidental MRI white matter signal hyperintensities.Neurology 1993; 43: 1683–1689.
69 Chimowitz MI, Estes ML, Furlan AJ, Awad IA. Further observations on thepathology of subcortical lesions identified on magnetic resonance imaging. ArchNeurol 1992; 49: 747–752.
70 Schmidt R, Schmidt H, Haybaeck J, Loitfelder M, Weis S, Cavalieri M et al. Het-erogeneity in age-related white matter changes. Acta neuropathologica 2011;122: 171–185.
71 Thomas AJ, Ferrier IN, Kalaria RN, Davis S, O’Brien JT. Cell adhesion moleculeexpression in the dorsolateral prefrontal cortex and anterior cingulate cortex inmajor depression in the elderly. Br J Psychiatry 2002; 181: 129–134.
72 Thomas AJ, Ferrier IN, Kalaria RN, Woodward SA, Ballard C, Oakley A et al. Ele-vation in late-life depression of intercellular adhesion molecule-1 expression inthe dorsolateral prefrontal cortex. Am J Psychiatry 2000; 157: 1682–1684.
73 Thomas AJ, Perry R, Kalaria RN, Oakley A, McMeekin W, O’Brien JT. Neuro-pathological evidence for ischemia in the white matter of the dorsolateralprefrontal cortex in late-life depression. Int J Geriatr Psychiatry 2003; 18: 7–13.
74 Rajkowska G, Miguel-Hidalgo JJ, Dubey P, Stockmeier CA, Krishnan KR. Promi-nent reduction in pyramidal neurons density in the orbitofrontal cortex ofelderly depressed patients. Biol Psychiatry 2005; 58: 297–306.
75 Miguel-Hidalgo JJ, Jiang W, Konick L, Overholser JC, Jurjus GJ, Stockmeier CAet al. Morphometric analysis of vascular pathology in the orbitofrontal cortex ofolder subjects with major depression. Int J Geriatr Psychiatry advance onlinepublication, 3 December 2012.
76 Miguel-Hidalgo JJ, Overholser JC, Jurjus GJ, Meltzer HY, Dieter L, Konick L et al.Vascular and extravascular immunoreactivity for intercellular adhesion molecule1 in the orbitofrontal cortex of subjects with major depression: age-dependentchanges. J Affect Disord 2011; 132: 422–431.
77 Santos M, Gold G, Kovari E, Herrmann FR, Hof PR, Bouras C et al. Neuropatho-logical analysis of lacunes and microvascular lesions in late-onset depression.Neuropathol Appl Neurobiol 2010; 36: 661–672.
78 Tsopelas C, Stewart R, Savva GM, Brayne C, Ince P, Thomas A et al. Neuropathologicalcorrelates of late-life depression in older people. Br J Psychiatry 2011; 198: 109–114.
79 Thomas AJ, Ferrier IN, Kalaria RN, Perry RH, Brown A, O’Brien JT. A neuro-pathological study of vascular factors in late-life depression. J Neurol NeurosurgPsychiatry 2001; 70: 83–87.
80 Murphy CF, Gunning-Dixon FM, Hoptman MJ, Lim KO, Ardekani B, Shields JK etal. White-matter integrity predicts Stroop performance in patients with geriatricdepression. Biol Psychiatry 2007; 61: 1007–1010.
81 Lockwood KA, Alexopoulos GS, van Gorp WG. Executive dysfunction in geriatricdepression. Am J Psychiatry 2002; 159: 1119–1126.
82 Elderkin-Thompson V, Kumar A, Bilker WB, Dunkin JJ, Mintz J, Moberg PJ et al.Neuropsychological deficits among patients with late-onset minor and majordepression. Archives of Clinical Neuropsychology 2003; 18: 529–549.
83 Nebes RD, Butters MA, Houck PR, Zmuda MD, Aizenstein H, Pollock BG et al.Dual-task performance in depressed geriatric patients. Psychiatry Res 2001; 102:139–151.
84 Boone KB, Lesser IM, Miller BL, Wohl M, Berman N, Lee ABP et al. Cognitivefunctioning in older depressed outpatients: relationship of presence and severity ofdepression to neuropsychological test scores. Neuropsychology 1995; 9: 390–398.
85 Beats BC, Sahakian BJ, Levy R. Cognitive performance in tests sensitive to frontallobe dysfunction in the elderly depressed. Psychol Med 1996; 26: 591–603.
86 Lesser IM, Boone KB, Mehringer CM, Wohl MA, Miller BL, Berman NG. Cognitionand white matter hyperintensities in older depressed patients. Am J Psychiatry1996; 153: 1280–1287.
87 Sexton CE, McDermott L, Kalu UG, Herrmann LL, Bradley KM, Allan CL et al.Exploring the pattern and neural correlates of neuropsychological impairment inlate-life depression. Psychol Med 2011; 26: 1–8.
88 Herrmann LL, Goodwin GM, Ebmeier KP. The cognitive neuropsychology ofdepression in the elderly. Psychol Med 2007; 37: 1693–1702.
89 Alexopoulos GS, Kiosses DN, Klimstra S, Kalayam B, Bruce ML. Clinical pre-sentation of the ‘depression-executive dysfunction syndrome’ of late life. Am JGeriatr Psychiatry 2002; 10: 98–106.
90 Kim BS, Lee DH, Lee DW, Bae JN, Chang SM, Kim S et al. The role of vascular riskfactors in the development of DED syndrome among an elderly communitysample. Am J Geriatr Psychiatry 2011; 19: 104–114.
91 Hajjar I, Yang F, Sorond F, Jones RN, Milberg W, Cupples LA et al. A novel agingphenotype of slow gait, impaired executive function, and depressive symptoms:relationship to blood pressure and other cardiovascular risks. J Gerontol A Biol SciMed Sci 2009; 64: 994–1001.
92 Alexopoulos GS, Kiosses DN, Murphy C, Heo M. Executive dysfunction, heartdisease burden, and remission of geriatric depression. Neuropsychopharmacol-ogy 2004; 29: 2278–2284.
93 Bogner HR, Bruce ML, Reynolds 3rd CF, Mulsant BH, Cary MS, Morales K et al. Theeffects of memory, attention, and executive dysfunction on outcomes ofdepression in a primary care intervention trial: the PROSPECT study. Int J GeriatrPsychiatry 2007; 22: 922–929.
94 Kalayam B, Alexopoulos GS. Prefrontal dysfunction and treatment response ingeriatric depression. Arch Gen Psychiatry 1999; 56: 713–718.
95 Potter GG, Kittinger JD, Wagner HR, Steffens DC, Krishnan KR. Prefrontal neu-ropsychological predictors of treatment remission in late-life depression. Neu-ropsychopharmacology 2004; 29: 2266–2271.
96 Baldwin R, Jeffries S, Jackson A, Sutcliffe C, Thacker N, Scott M et al. Treatmentresponse in late-onset depression: relationship to neuropsychological, neuror-adiological and vascular risk factors. Psychol Med 2004; 34: 125–136.
97 Sneed JR, Roose SP, Keilp JG, Krishnan KR, Alexopoulos GS, Sackeim HA.Response inhibition predicts poor antidepressant treatment response in very olddepressed patients. Am J Geriatr Psychiatry 2007; 15: 553–563.
98 Sheline YI, Pieper CF, Barch DM, Welsh-Boehmer K, McKinstry RC, MacFall JR et al.Support for the vascular depression hypothesis in late-life depression: results ofa 2-site, prospective, antidepressant treatment trial. Arch Gen Psychiatry 2010; 67:277–285.
99 Bella R, Pennisi G, Cantone M, Palermo F, Pennisi M, Lanza G et al. Clinicalpresentation and outcome of geriatric depression in subcortical ischemic vas-cular disease. Gerontology 2010; 56: 298–302.
100 Nebes RN, Pollock BG, Houck PR, Butters MA, Mulsant BH, Zmuda MD et al.Persistence of cognitive impairment in geriatric patients following anti-depressant treament: a randomized, double-blind clinical trial with nortriptylineand paroxetine. J Psychiatr Res 2003; 37: 99–108.
101 Kramer-Ginsberg E, Greenwald BS, Krishnan KRR, Christiansen B, Hu J, Ashtari Met al. Neuropsychological functioning and MRI signal hyperintensities in geraitricdepression. Am J Psychiatry 1999; 156: 438–444.
102 Kohler S, Thomas AJ, Lloyd A, Barber R, Almeida OP, O’Brien JT. White matterhyperintensities, cortisol levels, brain atrophy and continuing cognitive deficitsin late-life depression. Br J Psychiatry 2010; 196: 143–149.
103 Butters MA, Whyte EM, Nebes RD, Begley AE, Dew MA, Mulsant BH et al. Thenature and determinants of neuropsychological functioning in late-life depres-sion. Arch Gen Psychiatry 2004; 61: 587–595.
104 Sheline YI, Barch DM, Garcia K, Gersing K, Piper C, Welsh-Bohmer KA et al.Cognitive function in late life depression: relationships to depression severity,cerebrovascular risk factors and processing speed. Biol Psychiatry 2006; 60:58–65.
105 Nebes RD, Butters MA, Mulsant BH, Pollock BG, Zmuda MD, Houck PR et al.Decreased working memory and processing speed mediate cognitive impair-ment in geriatric depression. Psychol Med 2000; 30: 679–691.
106 Delaloye C, Baudois S, de Bilbao F, Dubois Remund C, Hofer F, Lamon M et al.Cognitive impairment in late-onset depression. Limited to a decrement ininformation processing resources? Eur Neurol 2008; 60: 149–154.
107 Bhalla RK, Butters MA, Mulsant BH, Begley AE, Zmuda MD, Schoderbek B et al.Persistence of neuropsychologic deficits in the remitted state of late-lifedepression. Am J Geriatr Psychiatry 2006; 14: 419–427.
108 Butters MA, Becker JT, Nebes RD, Zmuda MD, Mulsant BH, Pollock BG et al.Changes in cognitive functioning following treatment of late-life depression. AmJ Psychiatry 2000; 157: 1949–1954.
109 Murphy CF, Alexopoulos GS. Longitudinal association of initiation/perseverationand severity of geriatric depression. Am J Geriatr Psychiatry 2004; 12: 50–56.
110 Vasudev A, Saxby BK, O’Brien JT, Colloby SJ, Firbank MJ, Brooker H et al. Rela-tionship between cognition, magnetic resonance white matter hyperintensities,and cardiovascular autonomic changes in late-life depression. Am J GeriatrPsychiatry 2012; 20: 691–699.
Mechanisms underlying vascular depressionWD Taylor et al
8
Molecular Psychiatry (2013), 1 – 12 & 2013 Macmillan Publishers Limited

111 Perlmuter LC, Sarda G, Casavant V, O’Hara K, Hindes M, Knott PT et al. A review oforthostatic blood pressure regulation and its association with mood and cog-nition. Clin Auton Res 2012; 22: 99–107.
112 Novak V, Hajjar I. The relationship between blood pressure and cognitivefunction. Nat Rev Cardiol 2010; 7: 686–698.
113 Wolf PA, D’Agostino RB, Belanger AJ, Kannel WB. Probability of stroke: A riskprofile from the Framingham Study. Stroke 1991; 22: 312–318.
114 Gunning-Dixon FM, Raz N. Neuroanatomical correlates of selected executivefunctions in middle-aged and older adults: a prospective MRI study. Neu-ropsychologia 2003; 41: 1929–1941.
115 Kramer JH, Mungas D, Reed BR, Wetzel ME, Burnett MM, Miller BL et al. Long-itudinal MRI and cognitive change in healthy elderly. Neuropsychology 2007; 21:412–418.
116 Vannorsdall TD, Waldstein SR, Kraut M, Pearlson GD, Schretlen DJ. White matterabnormalities and cognition in a community sample. Arch Clin Neuropsychol2009; 24: 209–217.
117 Wright CB, Festa JR, Paik MC, Schmiedigen A, Brown TR, Yoshita M et al. Whitematter hyperintensities and subclinical infarction: associations with psycho-motor speed and cognitive flexibility. Stroke 2008; 39: 800–805.
118 de Groot JC, de Leeuw FE, Oudkerk M, van Gijn J, Hofman A, Jolles J et al.Cerebral white matter lesions and cognitive function: the Rotterdam Scan Study.Ann Neurol 2000; 47: 145–151.
119 Au R, Massaro JM, Wolf PA, Young ME, Beiser A, Seshadri S et al. Association ofwhite matter hyperintensity volume with decreased cognitive functioning: theFramingham Heart Study. Arch Neurol 2006; 63: 246–250.
120 Marquine MJ, Attix DK, Goldstein LB, Samsa GP, Payne ME, Chelune GJ et al.Differential patterns of cognitive decline in anterior and posterior white matterhyperintensity progression. Stroke 2010; 41: 1946–1950.
121 Longstreth Jr. WT, Arnold AM, Beauchamp Jr. NJ, Manolio TA, Lefkowitz D,Jungreis C et al. Incidence, manifestations, and predictors of worsening whitematter on serial cranial magnetic resonance imaging in the elderly: the Cardi-ovascular Health Study. Stroke 2005; 36: 56–61.
122 Silbert LC, Nelson C, Howieson DB, Moore MM, Kaye JA. Impact of white matterhyperintensity volume progression on rate of cognitive and motor decline.Neurology 2008; 71: 108–113.
123 Smith EE, Salat DH, Jeng J, McCreary CR, Fischl B, Schmahmann JD et al. Cor-relations between MRI white matter lesion location and executive function andepisodic memory. Neurology 2011; 76: 1492–1499.
124 Bocti C, Swartz RH, Gao FQ, Sahlas DJ, Behl P, Black SE. A new visual rating scaleto assess strategic white matter hyperintensities within cholinergic pathways indementia. Stroke 2005; 36: 2126–2131.
125 Alexopoulos GS, Kiosses DN, Heo M, Murphy CF, Shanmugham B, Gunning-DixonF. Executive dysfunction and the course of geriatric depression. Biol Psychiatry2005; 58: 204–210.
126 Alexopoulos GS, Meyers BS, Young RC, Kalayam B, Kakuma T, Gabrielle M et al.Executive dysfunction and long-term outcomes of geriatric depression. Arch GenPsychiatry 2000; 57: 285–290.
127 Butters MA, Bhalla RK, Mulsant BH, Mazumdar S, Houck PR, Begley AE et al.Executive functioning, illness course, and relapse/recurrence in continuation andmaintenance treatment in late-life depression: Is there a relationship? Am JGeriatr Psychiatry, 2004; 12: 387–394.
128 Morimoto SS, Wexler BE, Alexopoulos GS. Neuroplasticity-based computerizedcognitive remediation for geriatric depression. Int J Geriatr Psychiatry 2012 27.
129 McLennan SN, Mathias JL. The depression-executive dysfunction (DED) syn-drome and response to antidepressants: a meta-analytic review. Int J GeriatrPsychiatry 2010; 25: 933–944.
130 Morimoto SS, Gunning FM, Murphy CF, Kanellopoulos D, Kelly RE, AlexopoulosGS. Executive function and short-term remission of geriatric depression: the roleof semantic strategy. Am J Geriatr Psychiatry 2011; 19: 115–122.
131 Morimoto SS, Gunning FM, Kanellopoulos D, Murphy CF, Klimstra SA, Kelly Jr. REet al. Semantic organizational strategy predicts verbal memory and remissionrate of geriatric depression. Int J Geriatr Psychiatry 2012; 27: 506–512.
132 Pimontel MA, Culang-Reinlieb ME, Morimoto SS, Sneed JR. Executive dysfunctionand treatment response in late-life depression. Int J Geriatr Psychiatry 2011; 27:893–899.
133 Alexopoulos GS, Hoptman MJ, Kanellopoulos D, Murphy CF, Lim KO, GunningFM. Functional connectivity in the cognitive control network and the defaultmode network in late-life depression. J Affect Disord 2012; 139: 56–65.
134 Story TJ, Potter GG, Attix DK, Welsh-Bohmer KA, Steffens DC. Neurocognitivecorrelates of response to treatment in late-life depression. Am J Geriatr Psychiatry2008; 16: 752–759.
135 Simpson S, Baldwin RC, Jackson A, Burns AS. Is subcortical disease associatedwith a poor response to antidepressants? Neurological, neuropsychological andneuroradiological findings in late-life depression. Psychol Med 1998; 28:1015–1026.
136 Patankar TF, Baldwin R, Mitra D, Jeffries S, Sutcliffe C, Burns A et al. Virchow-Robin space dilatation may predict resistance to antidepressant monotherapy inelderly patients with depression. J Affect Disord 2007; 97: 265–270.
137 Gunning-Dixon FM, Walton M, Cheng J, Acuna J, Klimstra S, Zimmerman MEet al. MRI signal hyperintensities and treatment remission of geriatric depression.J Affect Disord 2010; 126: 395–401.
138 Sneed JR, Culang-Reinlieb ME, Brickman AM, Gunning-Dixon FM, Johnert L,Garcon E et al. MRI signal hyperintensities and failure to remit following anti-depressant treatment. J Affect Disord 2011; 135: 315–320.
139 Janssen J, Pol HEH, Schnack HG, Kok RM, Lampe IK, de Leeuw FE et al. Cerebralvolume measurements and subcortical white matter lesions and short-termtreatment response in late life depression. Int J Geriatr Psychiatry 2007; 22:468–474.
140 Krishnan KR, Hays JC, George LK, Blazer DG. Six-month outcomes for MRI-relatedvascular depression. Depress Anxiety 1998; 8: 142–146.
141 Salloway S, Boyle PA, Correia S, Malloy PF, Cahn-Weiner DA, Schneider L et al.The relationship of MRI subcortical hyperintensities to treatment response in atrial of sertraline in geriatric depressed outpatients. Am J Geriatr Psychiatry 2002;10: 107–111.
142 Salloway S, Correia S, Boyle P, Malloy P, Schneider L, Lavretsky H et al. MRIsubcortical hyperintensities in old and very old depressed outpatients: theimportant role of age in late-life depression. J Neurol Sci 2002; 203-204: 227–233.
143 Sneed JR, Roose SP, Sackeim HA. Vascular depression: A distinct diagnosticsubtype? Biol Psychiatry 2006; 60: 1295–1298.
144 Sneed JR, Culang-Reinlieb ME. The vascular depression hypothesis: an update.Am J Geriatr Psychiatry 2011; 19: 99–103.
145 Raz N, Rodrigue KM, Kennedy KM, Acker JD. Vascular health and longitudinalchanges in brain and cognition in middle-aged and older adults. Neu-ropsychology 2007; 21: 149–157.
146 Taylor WD, Steffens DC, MacFall JR, McQuoid DR, Payne ME, Provenzale JM et al.White matter hyperintensity progression and late-life depression outcomes. ArchGen Psychiatry 2003; 60: 1090–1096.
147 Chen PS, McQuoid DR, Payne ME, Steffens DC. White matter and subcortical graymatter lesion volume changes and late-life depression outcome: a 4-yearmagnetic resonance imaging study. Int Psychogeriatr 2006; 18: 445–456.
148 Alexopoulos GS, Murphy CF, Gunning-Dixon FM, Latoussakis V, Kanellopoulos D,Klimstra S et al. Microstructural white matter abnormalities and remission ofgeriatric depression. Am J Psychiatry 2008; 165: 238–244.
149 Alexopoulos GS, Glatt CE, Hoptman MJ, Kanellopoulos D, Murphy CF, Kelly Jr. REet al. BDNF Val66met polymorphism, white matter abnormalities and remissionof geriatric depression. J Affect Disord 2010 24.
150 Taylor WD, Kuchibhatla M, Payne ME, MacFall JR, Sheline YI, Krishnan KR et al.Frontal white matter anisotropy and antidepressant response in late-lifedepression. PLoS ONE 2008; 3: e3267.
151 Sheline YI, Price JL, Yan Z, Mintun MA. Resting-state functional MRI in depressionunmasks increased connectivity between networks via the dorsal nexus. ProcNatl Acad Sci USA 2010; 107: 11020–11025.
152 Alexopoulos GS, Murphy CF, Gunning-Dixon FM, Glatt CE, Latoussakis V, Kelly Jr.RE et al. Serotonin transporter polymorphisms, microstructural white matterabnormalities and remission of geriatric depression. J Affect Disord 2009; 119:132–141.
153 Lotrich FE. Gene-environment interactions in geriatric depression. Psychiatr ClinNorth Am 2011; 34: 357–376viii.
154 Benjamin S, Taylor W. Nature and nurture: genetic influences and gene-envir-onment interactions in depression. Curr Psychiatry Rev 2010; 6: 82–90.
155 Annerbrink K, Jonsson EG, Olsson M, Nilsson S, Sedvall GC, Anckarsater H et al.Associations between the angiotensin-converting enzyme insertion/deletionpolymorphism and monoamine metabolite concentrations in cerebrospinalfluid. Psychiatry Res 2010; 179: 231–234.
156 Baghai TC, Schule C, Zwanzger P, Minov C, Zill P, Ella R et al. Hypothalamic-pituitary-adrenocortical axis dysregulation in patients with major depression isinfluenced by the insertion/deletion polymorphism in the angiotensin I-con-verting enzyme gene. Neurosci Lett 2002; 328: 299–303.
157 Wu Y, Wang X, Shen X, Tan Z, Yuan Y. The I/D polymorphism of angiotensin-converting enzyme gene in major depressive disorder and therapeutic outcome:a case-control study and meta-analysis. J Affect Disord 2012; 136: 971–978.
158 Arinami T, Li L, Mitsushio H, Itokawa M, Hamaguchi H, Toru M. An insertion/deletion polymorphism in the angiotensin converting enzyme gene is asso-ciated with both brain substance P contents and affective disorders. Biol Psy-chiatry 1996; 40: 1122–1127.
159 Saab YB, Gard PR, Yeoman MS, Mfarrej B, El-Moalem H, Ingram MJ. Renin-angiotensin-system gene polymorphisms and depression. Prog Neuropsycho-pharmacol Biol Psychiatry 2007; 31: 1113–1118.
160 Lopez-Leon S, Janssens AC, Hofman A, Claes S, Breteler MM, Tiemeier H et al. Noassociation between the angiotensin-converting enzyme gene and major
Mechanisms underlying vascular depressionWD Taylor et al
9
& 2013 Macmillan Publishers Limited Molecular Psychiatry (2013), 1 – 12

depression: a case-control study and meta-analysis. Psychiatr Genet 2006; 16:225–226.
161 Baghai TC, Binder EB, Schule C, Salyakina D, Eser D, Lucae S et al. Polymorphismsin the angiotensin-converting enzyme gene are associated with unipolardepression, ACE activity and hypercortisolism. Mol Psychiatry 2006; 11:1003–1015.
162 Sparks DL, Hunsaker 3rd JC, Amouyel P, Malafosse A, Bellivier F, Leboyer M et al.Angiotensin I-converting enzyme I/D polymorphism and suicidal behaviors. Am JMed Genet B Neuropsychiatr Genet 2009; 150: 290–294.
163 Hishimoto A, Shirakawa O, Nishiguchi N, Hashimoto T, Yanagi M, Nushida H et al.Association between a functional polymorphism in the renin-angiotensin systemand completed suicide. J Neural Transm 2006; 113: 1915–1920.
164 Fudalej S, Fudalej M, Kostrzewa G, Kuzniar P, Franaszczyk M, Wojnar M et al.Angiotensin-converting enzyme polymorphism and completed suicide: anassociation in Caucasians and evidence for a link with a method of self-injury.Neuropsychobiology 2009; 59: 151–158.
165 Angunsri R, Sritharathikhun T, Suttirat S, Tencomnao T. Association of angio-tensin-converting enzyme gene promoter single nucleotide polymorphisms andhaplotype with major depression in a northeastern Thai population. J ReninAngiotensin Aldosterone Syst 2009; 10: 179–184.
166 Firouzabadi N, Shafiei M, Bahramali E, Ebrahimi SA, Bakhshandeh H, Tajik N.Association of angiotensin-converting enzyme (ACE) gene polymorphism withelevated serum ACE activity and major depression in an Iranian population.Psychiatry Res 2012; 200: 336–342.
167 Spiering W, Kroon AA, Fuss-Lejeune MM, Daemen MJ, de Leeuw PW, de LeeuwPW. Angiotensin II sensitivity is associated with the angiotensin II type 1 receptorA(1166)C polymorphism in essential hypertensives on a high sodium diet.Hypertension 2000; 36: 411–416.
168 Taylor WD, Steffens DC, Ashley-Koch A, Payne ME, MacFall JR, Potocky C et al.Angiotensin receptor gene polymorphisms and 2-year change in cerebralhyperintense lesion volume in men. Mol Psychiatry 2010; 15: 816–822.
169 Sleegers K, den Heijer T, van Dijk EJ, Hofman A, Bertoli-Avella AM, Koudstaal PJ etal. ACE gene is associated with Alzheimer’s disease and atrophy of hippocampusand amygdala. Neurobiol Aging 2005; 26: 1153–1159.
170 Zhang Z, Deng L, Bai F, Shi Y, Yu H, Yuan Y et al. ACE I/D polymorphism affectscognitive function and gray-matter volume in amnestic mild cognitive impair-ment. Behav Brain Res 2011; 218: 114–120.
171 Taylor WD, Benjamin S, McQuoid DR, Payne ME, Krishnan RR, MacFall JR et al.AGTR1 gene variation: association with depression and frontotemporal mor-phology. Psychiatry Res 2012; 202: 104–109.
172 Hou Z, Yuan Y, Zhang Z, Hou G, You J, Bai F. The D-allele of ACE insertion/deletion polymorphism is associated with regional white matter volume chan-ges and cognitive impairment in remitted geriatric depression. Neurosci Lett2010; 479: 262–266.
173 Wang Z, Yuan Y, Bai F, You J, Li L, Zhang Z. Abnormal default-mode network inangiotensin converting enzyme D allele carriers with remitted geriatricdepression. Behav Brain Res 2012; 230: 325–332.
174 Baghai TC, Schule C, Zill P, Deiml T, Eser D, Zwanzger P et al. The angiotensin Iconverting enzyme insertion/deletion polymorphism influences therapeuticoutcome in major depressed women, but not in men. Neurosci Lett 2004; 363:38–42.
175 Bondy B, Baghai TC, Zill P, Schule C, Eser D, Deiml T et al. Genetic variants in theangiotensin I-converting-enzyme (ACE) and angiotensin II receptor (AT1) geneand clinical outcome in depression. Prog Neuropsychopharmacol Biol Psychiatry2005; 29: 1094–1099.
176 Kondo DG, Speer MC, Krishnan KR, McQuoid DR, Slifer SH, Pieper CF et al.Association of AGTR1 with 18-month treatment outcome in late-life depression.Am J Geriatr Psychiatry 2007; 15: 564–572.
177 Taylor WD, Bae JN, MacFall JR, Payne ME, Provenzale JM, Steffens DC et al.Widespread effects of hyperintense lesions on cerebral white matter structure.Am J Roentgenol 2007; 188: 1695–1704.
178 Alexopoulos GS. Frontostriatal and limbic dysfunction in late-life depression. AmJ Geriatr Psychiatry 2002; 10: 687–695.
179 Dalby RB, Frandsen J, Chakravarty MM, Ahdidan J, Sorensen L, Rosenberg R et al.Depression severity is correlated to the integrity of white matter fiber tracts inlate-onset major depression. Psychiatry Res 2010; 184: 38–48.
180 Taylor WD, Payne ME, Krishnan KRR, Wagner HR, Provenzale JM, Steffens DC etal. Evidence of white matter tract disruption in MRI hyperintensities. Biol Psy-chiatry 2001; 50: 179–183.
181 Sexton CE, Le Masurier M, Allan CL, Jenkinson M, McDermott L, Kalu UG et al.Magnetic resonance imaging in late-life depression: vascular and glucocorticoidcascade hypotheses. Br J Psychiatry 2012; 201: 46–51.
182 Taylor WD, MacFall JR, Gerig G, Krishnan KR. Structural integrity of the uncinatefasciculus in geriatric depression: Relationship with age of onset. NeuropsychiatrDis Treat 2007; 3: 669–674.
183 Ebeling U, Cramon DV. Topography of the uncinate fascicle and adjacent tem-poral fiber tracts. Acta Neurochir (Wien) 1992; 115: 143–148.
184 Kier EL, Staib LH, Davis LM, Bronen RAMR. imaging of the temporal stem: ana-tomic dissection tractography of the uncinate fasciculus, inferior occipitofrontalfasciculus, and Meyer’s loop of the optic radiation. AJNR Am J Neuroradiol 2004;25: 677–691.
185 Petrides M, Pandya DN. Efferent association pathways from the rostral prefrontalcortex in the macaque monkey. J Neurosci 2007; 27: 11573–11586.
186 Mufson EJ, Pandya DN. Some observations on the course and composition of thecingulum bundle in the rhesus monkey. J Comp Neurol 1984; 225: 31–43.
187 Morris R, Pandya DN, Petrides M. Fiber system linking the mid-dorsolateralfrontal cortex with the retrosplenial/presubicular region in the rhesus monkey.J Comp Neurol 1999; 407: 183–192.
188 Rudrauf D, Mehta S, Grabowski TJ. Disconnection’s renaissance takes shape:Formal incorporation in group-level lesion studies. Cortex 2008; 44: 1084–1096.
189 Gaffan D, Wilson CR. Medial temporal and prefrontal function: recent beha-vioural disconnection studies in the macaque monkey. Cortex 2008; 44: 928–935.
190 Zhang A, Leow A, Ajilore O, Lamar M, Yang S, Joseph J et al. Quantitative tract-specific measures of uncinate and cingulum in major depression using diffusiontensor imaging. Neuropsychopharmacology 2012; 37: 959–967.
191 Keedwell PA, Chapman R, Christiansen K, Richardson H, Evans J, Jones DK.Cingulum White Matter in Young Women at Risk of Depression: The Effect ofFamily History and Anhedonia. Biol Psychiatry 2012; 72: 296–302.
192 Damoiseaux JS, Greicius MD. Greater than the sum of its parts: a review ofstudies combining structural connectivity and resting-state functional con-nectivity. Brain Struct Funct 2009; 213: 525–533.
193 Skudlarski P, Jagannathan K, Calhoun VD, Hampson M, Skudlarska BA, PearlsonG. Measuring brain connectivity: diffusion tensor imaging validates resting statetemporal correlations. Neuroimage 2008; 43: 554–561.
194 Teipel SJ, Bokde AL, Meindl T, Amaro Jr. E, Soldner J, Reiser MF et al. Whitematter microstructure underlying default mode network connectivity in thehuman brain. Neuroimage 2010; 49: 2021–2032.
195 van den Heuvel M, Mandl R, Luigjes J, Hulshoff Pol H. Microstructural organi-zation of the cingulum tract and the level of default mode functional con-nectivity. J Neurosci 2008; 28: 10844–10851.
196 Steffens DC, Taylor WD, Denny KL, Bergman SR, Wang L. Structural integrity ofthe uncinate fasciculus and resting state functional connectivity of the ventralprefrontal cortex in late life depression. PLoS ONE 2011; 6: e22697.
197 Godbout JP, Johnson RW. Age and neuroinflammation: a lifetime of psycho-neuroimmune consequences. Neurol Clin 2006; 24: 521–538.
198 Dilger RN, Johnson RW. Aging, microglial cell priming, and the discordant centralinflammatory response to signals from the peripheral immune system. J LeukocBiol 2008; 84: 932–939.
199 Maes M. Depression is an inflammatory disease, but cell-mediated immuneactivation is the key component of depression. Prog Neuropsychopharmacol BiolPsychiatry 2011; 35: 664–675.
200 Raison CL, Demetrashvili M, Capuron L, Miller AH. Neuropsychiatric adverseeffects of interferon-alpha: recognition and management. CNS Drugs 2005; 19:105–123.
201 Alexopoulos GS, Morimoto SS. The inflammation hypothesis in geriatricdepression. Int J Geriatr Psychiatry advance online publication, 2 March 2011.
202 Brydon L, Harrison NA, Walker C, Steptoe A, Critchley HD. Peripheral inflam-mation is associated with altered substantia nigra activity and psychomotorslowing in humans. Biol Psychiatry 2008; 63: 1022–1029.
203 Harrison NA, Brydon L, Walker C, Gray MA, Steptoe A, Critchley HD. Inflammationcauses mood changes through alterations in subgenual cingulate activity andmesolimbic connectivity. Biol Psychiatry 2009; 66: 407–414.
204 Raison CL, Capuron L, Miller AH. Cytokines sing the blues: inflammation and thepathogenesis of depression. Trends Immunol 2006; 27: 24–31.
205 Zorrilla EP, Luborsky L, McKay JR, Rosenthal R, Houldin A, Tax A et al. Therelationship of depression and stressors to immunological assays: a meta-ana-lytic review. Brain Behav Immun 2001; 15: 199–226.
206 Sutcigil L, Oktenli C, Musabak U, Bozkurt A, Cansever A, Uzun O et al. Pro- andanti-inflammatory cytokine balance in major depression: effect of sertralinetherapy. Clin Dev Immunol 2007; 2007: 76396.
207 Kim YK, Na KS, Shin KH, Jung HY, Choi SH, Kim JB. Cytokine imbalance in thepathophysiology of major depressive disorder. Prog Neuropsychopharmacol BiolPsychiatry 2007; 31: 1044–1053.
208 Miller AH. Norman Cousins Lecture. Mechanisms of cytokine-induced behavioralchanges: psychoneuroimmunology at the translational interface. Brain BehavImmun 2009; 23: 149–158.
209 O’Connor JC, Andre C, Wang Y, Lawson MA, Szegedi SS, Lestage J et al. Inter-feron-gamma and tumor necrosis factor-alpha mediate the upregulation ofindoleamine 2,3-dioxygenase and the induction of depressive-like behavior inmice in response to bacillus Calmette-Guerin. J Neurosci 2009; 29: 4200–4209.
Mechanisms underlying vascular depressionWD Taylor et al
10
Molecular Psychiatry (2013), 1 – 12 & 2013 Macmillan Publishers Limited

210 O’Connor JC, Lawson MA, Andre C, Moreau M, Lestage J, Castanon N et al.Lipopolysaccharide-induced depressive-like behavior is mediated by indolea-mine 2,3-dioxygenase activation in mice. Mol Psychiatry 2009; 14: 511–522.
211 Maes M, Leonard BE, Myint AM, Kubera M, Verkerk R. The new ‘5-HT’ hypothesisof depression: Cell-mediated immune activation induces indoleamine 2,3-diox-ygenase, which leads to lower plasma tryptophan and an increased synthesis ofdetrimental tryptophan catabolites (TRYCATs), both of which contribute to theonset of depression. Prog Neuropsychopharmacol Biol Psychiatry 2010; 35:702–721.
212 Stone TW, Behan WM. Interleukin-1beta but not tumor necrosis factor-alphapotentiates neuronal damage by quinolinic acid: protection by an adenosineA2A receptor antagonist. J Neurosci Res 2007; 85: 1077–1085.
213 Tsao CW, Lin YS, Chen CC, Bai CH, Wu SR. Cytokines and serotonin transporter inpatients with major depression. Prog Neuropsychopharmacol Biol Psychiatry 2006;30: 899–905.
214 Pace TW, Hu F, Miller AH. Cytokine-effects on glucocorticoid receptor function:relevance to glucocorticoid resistance and the pathophysiology and treatmentof major depression. Brain Behav Immun 2007; 21: 9–19.
215 Koo JW, Duman RS. IL-1beta is an essential mediator of the antineurogenic andanhedonic effects of stress. Proc Natl Acad Sci USA 2008; 105: 751–756.
216 Slavich GM, Way BM, Eisenberger NI, Taylor SE. Neural sensitivity to socialrejection is associated with inflammatory responses to social stress. Proc NatlAcad Sci USA 2010; 107: 14817–14822.
217 O’Connor MF, Irwin MR, Wellisch DK. When grief heats up: pro-inflammatorycytokines predict regional brain activation. Neuroimage 2009; 47: 891–896.
218 Wong ML, Dong C, Maestre-Mesa J, Licinio J. Polymorphisms in inflammation-related genes are associated with susceptibility to major depression and anti-depressant response. Mol Psychiatry 2008; 13: 800–812.
219 Cerri AP, Arosio B, Viazzoli C, Confalonieri R, Vergani C, Annoni G. The -308 (G/A)single nucleotide polymorphism in the TNF-alpha gene and the risk of majordepression in the elderly. Int J Geriatr Psychiatry 2010; 25: 219–223.
220 Hwang JP, Tsai SJ, Hong CJ, Yang CH, Hsu CD, Liou YJ. Interleukin-1 beta -511C/Tgenetic polymorphism is associated with age of onset of geriatric depression.Neuromolecular Med 2009; 11: 322–327.
221 Halder I, Marsland AL, Cheong J, Muldoon MF, Ferrell RE, Manuck SB. Poly-morphisms in the CRP gene moderate an association between depressivesymptoms and circulating levels of C-reactive protein. Brain Behav Immun 2010;24: 160–167.
222 Baune BT, Dannlowski U, Domschke K, Janssen DG, Jordan MA, Ohrmann P et al.The interleukin 1 beta (IL1B) gene is associated with failure to achieve remissionand impaired emotion processing in major depression. Biol Psychiatry 2010 Mar15; 67: 543–549.
223 Gruver AL, Hudson LL, Sempowski GD. Immunosenescence of ageing. J Pathol2007; 211: 144–156.
224 Penninx BW, Kritchevsky SB, Yaffe K, Newman AB, Simonsick EM, Rubin S et al.Inflammatory markers and depressed mood in older persons: results from theHealth, Aging and Body Composition study. Biol Psychiatry 2003; 54: 566–572.
225 Dentino AN, Pieper CF, Rao MK, Currie MS, Harris T, Blazer DG et al. Association ofinterleukin-6 and other biologic variables with depression in older people livingin the community. J Am Geriatr Soc 1999; 47: 6–11.
226 Tiemeier H, Hofman A, van Tuijl HR, Kiliaan AJ, Meijer J, Breteler MM. Inflam-matory proteins and depression in the elderly. Epidemiology 2003; 14: 103–107.
227 Bremmer MA, Beekman AT, Deeg DJ, Penninx BW, Dik MG, Hack CE et al.Inflammatory markers in late-life depression: results from a population-basedstudy. J Affect Disord 2008; 106: 249–255.
228 Baune BT, Smith E, Reppermund S, Air T, Samaras K, Lux O et al. Inflammatorybiomarkers predict depressive, but not anxiety symptoms during aging: Theprospective Sydney Memory and Aging Study. Psychoneuroendocrinology 2012;37: 1521–1530.
229 Elderkin-Thompson V, Irwin MR, Hellemann G, Kumar A. Interleukin-6 andmemory functions of encoding and recall in healthy and depressed elderlyadults. Am J Geriatr Psychiatry 2012; 20: 753–763.
230 Schram MT, Euser SM, de Craen AJ, Witteman JC, Frolich M, Hofman A et al.Systemic markers of inflammation and cognitive decline in old age. J Am GeriatrSoc 2007; 55: 708–716.
231 Marioni RE, Strachan MW, Reynolds RM, Lowe GD, Mitchell RJ, Fowkes FG et al.Association between raised inflammatory markers and cognitive decline inelderly people with type 2 diabetes: the Edinburgh Type 2 Diabetes Study.Diabetes 2010; 59: 710–713.
232 Fornage M, Chiang YA, O’Meara ES, Psaty BM, Reiner AP, Siscovick DS et al.Biomarkers of inflammation and MRI-defined small vessel disease of the brain:The Cardiovascular Health Study. Stroke 2008; 39: 1952–1959.
233 van Dijk EJ, Prins ND, Vermeer SE, Vrooman HA, Hofman A, Koudstaal PJ et al.C-reactive protein and cerebral small-vessel disease: the Rotterdam Scan Study.Circulation 2005; 112: 900–905.
234 Raz N, Yang Y, Dahle CL, Land S. Volume of white matter hyperintensities inhealthy adults: contribution of age, vascular risk factors, and inflammation-related genetic variants. Biochim Biophys Acta 2012; 1822: 361–369.
235 Satizabal CL, Zhu YC, Mazoyer B, Dufouil C, Tzourio C. Circulating IL-6 and CRPare associated with MRI findings in the elderly: the 3C-Dijon Study. Neurology2012; 78: 720–727.
236 Janssen DG, Caniato RN, Verster JC, Baune BT. A psychoneuroimmunologicalreview on cytokines involved in antidepressant treatment response. Hum Psy-chopharmacol 2010; 25: 201–215.
237 Xia Z, DePierre JW, Nassberger L. Tricyclic antidepressants inhibit IL-6, IL-1 betaand TNF-alpha release in human blood monocytes and IL-2 and interferon-gamma in T cells. Immunopharmacology 1996; 34: 27–37.
238 Maes M, Song C, Lin AH, Bonaccorso S, Kenis G, De Jongh R et al. Negativeimmunoregulatory effects of antidepressants: inhibition of interferon-gammaand stimulation of interleukin-10 secretion. Neuropsychopharmacology 1999; 20:370–379.
239 Szuster-Ciesielska A, Tustanowska-Stachura A, Slotwinska M, Marmurowska-Michalowska H, Kandefer-Szerszen M. In vitro immunoregulatory effects ofantidepressants in healthy volunteers. Pol J Pharmacol 2003; 55: 353–362.
240 Kenis G, Maes M. Effects of antidepressants on the production of cytokines. Int JNeuropsychopharmacol 2002; 5: 401–412.
241 Hannestad J, DellaGioia N, Bloch M. The effect of antidepressant medicationtreatment on serum levels of inflammatory cytokines: a meta-analysis. Neu-ropsychopharmacology 2011; 36: 2452–2459.
242 Tyring S, Gottlieb A, Papp K, Gordon K, Leonardi C, Wang A et al. Etanercept andclinical outcomes, fatigue, and depression in psoriasis: double-blind placebo-controlled randomised phase III trial. Lancet 2006; 367: 29–35.
243 Kekow J, Moots RJ, Emery P, Durez P, Koenig A, Singh A et al. Patient-reportedoutcomes improve with etanercept plus methotrexate in active early rheuma-toid arthritis and the improvement is strongly associated with remission: theCOMET trial. Ann Rheum Dis 2010; 69: 222–225.
244 Muller N, Schwarz MJ, Dehning S, Douhe A, Cerovecki A, Goldstein-Muller B et al.The cyclooxygenase-2 inhibitor celecoxib has therapeutic effects in majordepression: results of a double-blind, randomized, placebo controlled, add-onpilot study to reboxetine. Mol Psychiatry 2006; 11: 680–684.
245 Raison CL, Rutherford RE, Woolwine BJ, Shuo C, Schettler P, Drake DF et al. Arandomized controlled trial of the tumor necrosis factor antagonist infliximab fortreatment-resistant depression: the role of baseline inflammatory biomarkers.Arch Gen Psychiatry 2012; 3: 1–11.
246 Koyama A, O’Brien J, Weuve J, Blacker D, Metti AL, Yaffe K. The role of peripheralinflammatory markers in Dementia and Alzheimer’s disease: a meta-analysis.J Gerontol A Biol Sci Med Sci advance online publication, 14 September 2012.
247 Rubio-Perez JM, Morillas-Ruiz JM. A review: inflammatory process in Alzheimer’sdisease, role of cytokines. Scientific World Journal 2012; 2012: 756357.
248 Corbett A, Pickett J, Burns A, Corcoran J, Dunnett SB, Edison P et al. Drugrepositioning for Alzheimer’s disease. Nat Rev Drug Discov 2012; 11: 833–846.
249 Paranthaman R, Greenstein AS, Burns AS, Cruickshank JK, Heagerty AM, JacksonA et al. Vascular function in older adults with depressive disorder. Biol Psychiatry2010; 68: 133–139.
250 Greenstein AS, Paranthaman R, Burns A, Jackson A, Malik RA, Baldwin RC et al.Cerebrovascular damage in late-life depression is associated with structural andfunctional abnormalities of subcutaneous small arteries. Hypertension 2010; 56:734–740.
251 Broadley AJ, Korszun A, Jones CJ, Frenneaux MP. Arterial endothelial function isimpaired in treated depression. Heart 2002; 88: 521–523.
252 Rajagopalan S, Brook R, Rubenfire M, Pitt E, Young E, Pitt B. Abnormal brachialartery flow-mediated vasodilation in young adults with major depression.Am J Cardiol 2001; 88: 196–198.
253 Tiemeier H, Breteler MM, van Popele NM, Hofman A, Witteman JC. Late-lifedepression is associated with arterial stiffness: a population-based study. J AmGeriatr Soc 2003; 51: 1105–1110.
254 Chen CS, Chen CC, Kuo YT, Chiang IC, Ko CH, Lin HF. Carotid intima-mediathickness in late-onset major depressive disorder. Int J Geriatr Psychiatry 2006;21: 36–42.
255 Iadecola C. Neurovascular regulation in the normal brain and in Alzheimer’sdisease. Nat Rev Neurosci 2004; 5: 347–360.
256 de la Torre JC. Cerebral hemodynamics and vascular risk factors: setting thestage for Alzheimer’s disease. J Alzheimers Dis 2012 27.
257 Touyz RM. Intracellular mechanisms involved in vascular remodelling of resistancearteries in hypertension: role of angiotensin II. Exp Physiol 2005; 90: 449–455.
258 Dandona P, Chaudhuri A, Aljada A. Endothelial dysfunction and hypertension indiabetes mellitus. Med Clin North Am 2004; 88: 911–931x-xi.
259 Paranthaman R, Greenstein A, Burns AS, Heagerty AM, Malik RA, Baldwin RC.Relationship of endothelial function and atherosclerosis to treatment responsein late-life depression. Int J Geriatr Psychiatry 2012; 27: 967–973.
Mechanisms underlying vascular depressionWD Taylor et al
11
& 2013 Macmillan Publishers Limited Molecular Psychiatry (2013), 1 – 12

260 Tiemeier H, Bakker SL, Hofman A, Koudstaal PJ, Breteler MM. Cerebral haemo-dynamics and depression in the elderly. J Neurol Neurosurg Psychiatry 2002; 73:34–39.
261 Direk N, Koudstaal PJ, Hofman A, Ikram MA, Hoogendijk WJ, Tiemeier H. Cerebralhemodynamics and incident depression: the rotterdam study. Biol Psychiatry2012; 72: 318–323.
262 Mies G, Ishimaru S, Xie Y, Seo K, Hossmann KA. Ischemic thresholds of cerebralprotein synthesis and energy state following middle cerebral artery occlusion inrat. J Cereb Blood Flow Metab 1991; 11: 753–761.
263 Martin KC, Barad M, Kandel ER. Local protein synthesis and its role in synapse-specific plasticity. Curr Opin Neurobiol 2000; 10: 587–592.
264 Debiec J, LeDoux JE, Nader K. Cellular and systems reconsolidation in thehippocampus. Neuron 2002; 36: 527–538.
265 Kleim JA, Bruneau R, Calder K, Pocock D, VandenBerg PM, MacDonald E et al.Functional organization of adult motor cortex is dependent upon continuedprotein synthesis. Neuron 2003; 40: 167–176.
266 Moody DM, Bell MA, Challa VR. Features of the cerebral vascular pattern thatpredict vulnerability to perfusion or oxygenation deficiency: an anatomic study.AJNR Am J Neuroradiol 1990; 11: 431–439.
267 Matsushita K, Kuriyama Y, Nagatsuka K, Nakamura M, Sawada T, Omae T. Peri-ventricular white matter lucency and cerebral blood flow autoregulation inhypertensive patients. Hypertension 1994; 23: 565–568.
268 Markus HS, Lythgoe DJ, Ostegaard L, O’Sullivan M, Williams SC. Reduced cerebralblood flow in white matter in ischaemic leukoaraiosis demonstrated usingquantitative exogenous contrast based perfusion MRI. J Neurol NeurosurgPsychiatry 2000; 69: 48–53.
269 Oda K, Okubo Y, Ishida R, Murata Y, Ohta K, Matsuda T et al. Regional cerebralblood flow in depressed patients with white matter magnetic resonancehyperintensity. Biol Psychiatry 2003; 53: 150–156.
270 Brickman AM, Zahra A, Muraskin J, Steffener J, Holland CM, Habeck C et al.Reduction in cerebral blood flow in areas appearing as white matter hyper-intensities on magnetic resonance imaging. Psychiatry Res 2009; 172: 117–120.
271 Vardi N, Freedman N, Lester H, Gomori JM, Chisin R, Lerer B et al. Hyper-intensities on T2-weighted images in the basal ganglia of patients with majordepression: cerebral perfusion and clinical implications. Psychiatry Res 2011; 192:125–130.
272 Nitschke JB, Mackiewicz KL. Prefrontal and anterior cingulate contributions tovolition in depression. Int Rev Neurobiol 2005; 67: 73–94.
273 Videbech P, Ravnkilde B, Pedersen TH, Hartvig H, Egander A, Clemmensen K etal. The Danish PET/depression project: clinical symptoms and cerebral bloodflow. A regions-of-interest analysis. Acta Psychiatr Scand 2002; 106: 35–44.
274 Lui S, Parkes LM, Huang X, Zou K, Chan RC, Yang H et al. Depressive disorders:focally altered cerebral perfusion measured with arterial spin-labeling MR ima-ging. Radiology 2009; 251: 476–484.
275 Duhameau B, Ferre JC, Jannin P, Gauvrit JY, Verin M, Millet B et al. Chronic andtreatment-resistant depression: a study using arterial spin labeling perfusion MRIat 3Tesla. Psychiatry Res 2010; 182: 111–116.
276 Jarnum H, Eskildsen SF, Steffensen EG, Lundbye-Christensen S, Simonsen CW,Thomsen IS et al. Longitudinal MRI study of cortical thickness, perfusion, andmetabolite levels in major depressive disorder. Acta Psychiatr Scand 2011; 124:435–446.
277 Asllani I, Habeck C, Borogovac A, Brown TR, Brickman AM, Stern Y. Separatingfunction from structure in perfusion imaging of the aging brain. Hum Brain Mapp2009; 30: 2927–2935.
278 Claus JJ, Breteler MM, Hasan D, Krenning EP, Bots ML, Grobbee DE et al. Regionalcerebral blood flow and cerebrovascular risk factors in the elderly population.Neurobiol Aging 1998; 19: 57–64.
279 Dotson VM, Beason-Held L, Kraut MA, Resnick SM. Longitudinal study of chronicdepressive symptoms and regional cerebral blood flow in older men andwomen. Int J Geriatr Psychiatry 2009; 24: 809–819.
280 Lesser IM, Mena I, Boone KB, Miller BL, Mehringer MC, Wohl M. Reduction ofcerebral blood flow in older depressed patients. Arch Gen Psychiatry 1994; 51:677–686.
281 Ishizaki J, Yamamoto H, Takahashi T, Takeda M, Yano M, Mimura M. Changes inregional cerebral blood flow following antidepressant treatment in late-lifedepression. Int J Geriatr Psychiatry 2008; 23: 805–811.
282 Vasile RG, Schwartz RB, Garada B, Holman BL, Alpert M, Davidson PB et al. Focalcerebral perfusion defects demonstrated by 99mTc-hexamethylpropyleneamineoxime SPECT in elderly depressed patients. Psychiatry Res 1996; 67: 59–70.
283 Ebmeier KP, Glabus MF, Prentice N, Ryman A, Goodwin GM. A voxel-basedanalysis of cerebral perfusion in dementia and depression of old age. Neuro-image 1998; 7: 199–208.
284 Vangu MD, Esser JD, Boyd IH, Berk M. Effects of electroconvulsive therapy onregional cerebral blood flow measured by 99mtechnetium HMPAO SPECT. ProgNeuropsychopharmacol Biol Psychiatry 2003; 27: 15–19.
285 Kohn Y, Freedman N, Lester H, Krausz Y, Chisin R, Lerer B et al. 99mTc-HMPAOSPECT study of cerebral perfusion after treatment with medication andelectroconvulsive therapy in major depression. J Nucl Med 2007; 48:1273–1278.
286 Milo TJ, Kaufman GE, Barnes WE, Konopka LM, Crayton JW, Ringelstein JG et al.Changes in regional cerebral blood flow after electroconvulsive therapy fordepression. J ECT 2001; 17: 15–21.
287 Vlassenko A, Sheline YI, Fischer K, Mintun MA. Cerebral perfusion response tosuccessful treatment of depression with different serotoninergic agents. J Neu-ropsychiatry Clin Neurosci 2004; 16: 360–363.
288 Bench CJ, Frackowiak RS, Dolan RJ. Changes in regional cerebral blood flow onrecovery from depression. Psychol Med 1995; 25: 247–261.
289 Mazza M, Marano G, Traversi G, Bria P, Mazza S. Primary cerebral blood flowdeficiency and Alzheimer’s disease: shadows and lights. J Alzheimers Dis 2011;23: 375–389.
290 Chao LL, Buckley ST, Kornak J, Schuff N, Madison C, Yaffe K et al. ASL perfusionMRI predicts cognitive decline and conversion from MCI to dementia. AlzheimerDis Assoc Disord 2010; 24: 19–27.
291 Chao LL, Pa J, Duarte A, Schuff N, Weiner MW, Kramer JH et al. Patterns ofcerebral hypoperfusion in amnestic and dysexecutive MCI. Alzheimer Dis AssocDisord 2009; 23: 245–252.
292 Heo S, Prakash RS, Voss MW, Erickson KI, Ouyang C, Sutton BP et al. Restinghippocampal blood flow, spatial memory and aging. Brain Res 2010; 1315:119–127.
293 Terada S, Sato S, Honda H, Kishimoto Y, Takeda N, Oshima E et al. Perseverativeerrors on the Wisconsin Card Sorting Test and brain perfusion imaging in mildAlzheimer’s disease. Int Psychogeriatr 2011; 23: 1552–1559.
294 Takeda N, Terada S, Sato S, Honda H, Yoshida H, Kishimoto Y et al. Wisconsincard sorting test and brain perfusion imaging in early dementia. Dement GeriatrCogn Disord 2010; 29: 21–27.
295 Rabbitt P, Scott M, Thacker N, Lowe C, Jackson A, Horan M et al. Losses in grossbrain volume and cerebral blood flow account for age-related differences inspeed but not in fluid intelligence. Neuropsychology 2006; 20: 549–557.
296 Ghiadoni L, Virdis A, Magagna A, Taddei S, Salvetti A. Effect of the angiotensin IItype 1 receptor blocker candesartan on endothelial function in patients withessential hypertension. Hypertension 2000; 35(1 Pt 2): 501–506.
297 Nagata R, Kawabe K, Ikeda K. Olmesartan an angiotensin II receptor blocker,restores cerebral hypoperfusion in elderly patients with hypertension. J StrokeCerebrovasc Dis 2010; 19: 236–240.
298 Virdis A, Schiffrin EL. Vascular inflammation: a role in vascular disease inhypertension? Curr Opin Nephrol Hypertens 2003; 12: 181–187.
299 Almeida OP, McCaul K, Hankey GJ, Norman P, Jamrozik K, Flicker L.Homocysteine and depression in later life. Arch Gen Psychiatry 2008; 65:1286–1294.
300 Weiss N. Mechanisms of increased vascular oxidant stress in hyperhomocys-teinemia and its impact on endothelial function. Curr Drug Metab 2005; 6: 27–36.
301 Pariante CM. Risk factors for development of depression and psychosis. Gluco-corticoid receptors and pituitary implications for treatment with antidepressantand glucocorticoids. Ann N Y Acad Sci 2009; 1179: 144–152.
302 Grinevich V, Harbuz M, Ma XM, Jessop D, Tilders FJ, Lightman SL et al. Hypo-thalamic pituitary adrenal axis and immune responses to endotoxin in rats withchronic adjuvant-induced arthritis. Exp Neurol 2002; 178: 112–123.
303 Chalon S. Omega-3 fatty acids and monoamine neurotransmission. Pros-taglandins, leukotrienes, and essential fatty acids 2006; 75: 259–269.
304 Bloch MH, Hannestad J. Response to critiques on ’Omega-3 fatty acids for thetreatment of depression: systematic review and meta-analysis’. Mol Psychiatry2012; 17: 1163–1167.
305 Bloch MH, Hannestad J. Omega-3 fatty acids for the treatment of depression:systematic review and meta-analysis. Mol Psychiatry 2012; 17: 1272–1282.
306 Fogari R, Mugellini A, Zoppi A, Derosa G, Pasotti C, Fogari E et al. Influence oflosartan and atenolol on memory function in very elderly hypertensive patients.J Hum Hypertens 2003; 17: 781–785.
307 Saxby BK, Harrington F, Wesnes KA, McKeith IG, Ford GA. Candesartan andcognitive decline in older patients with hypertension: a substudy of the SCOPEtrial. Neurology 2008; 70: 1858–1866.
308 Hajjar I, Hart M, Chen YL, Mack W, Milberg W, Chui H et al. Effect of anti-hypertensive therapy on cognitive function in early executive cognitiveimpairment: a double-blind randomized clinical trial. Arch Intern Med 2012; 172:442–444.
Mechanisms underlying vascular depressionWD Taylor et al
12
Molecular Psychiatry (2013), 1 – 12 & 2013 Macmillan Publishers Limited