Embed Size (px)
Citation preview

Results:
Achievements: Tested Model of Care
Aim & Driver Diagram:
Vision: To enable patients at high risk of readmission to self-manage and remain well at home Problem: • In the year ending February 2010:
• 64,409 patients presented to ED 88,565 times • Total bed days for the year were 25,768
Example: Over $2,500 worth of unused medications retrieved
from one home visit
Impact: • The VHIU model of care is effective at reducing EC
presentations and readmissions for high risk patients
• The inter-disciplinary team (IDT) assessment of the patient in their home is key to understanding and providing for their healthcare needs
• The combined perspective of the range of disciplines involved, provides a holistic and practical plan to meet the needs of the patient
• The integrated case management approach bridges the gap between the hospital and community, improving the quality of care for the patient and their quality of life
Next Steps: • This model of care will translate well to include teams
based in community settings
To increase the number of patients enrolled into Very High Intensity User programme from 120 cases to 600* cases by July 2013. This may result in a reduction in unplanned presentation and admission to Middlemore Hospital.
Referral
Pa$ent & Family
Secondary care referrals
Primary Drivers Secondary Drivers
Network and relationship
Model of Care
GP Referral
Resource – Skilled Team
Shared Documenta$on
Home Visit
Assessment & Care Plans
Mul$ple EC presenta$on
Healthcare Professions
Community Resources
Measures: 1. Readmission 2. Presenta1on 4. Admissions 5. LOS 6. Days between presenta1on
The VHIU* – Link Team A model of integrated care that helps patients at high risk of readmission
*Very High Intensity Users
The Collaborative Team:
Clinical Lead: Project Lead: Professor Harry Rea Ta-Mera Rolland
Team: Collaborative Support: Contributors:
Pamela Hill Alison Howitt Amanda Seabrook Tanya Naea Lucy Hall Rosie Whittington Olive Wilson Clare Moss Gray Maingay Prem Kumar Lavinia Buchanan Kate Martin Karen Long Katy Boulton Tua Teara Fiona Smyth Richard Small Priya Francis
Fay Burke Christine Lynch Meg Goodman Fiona Horwood
Numbers of Patients Enrolled into VHIU
149
14
23 25
34
46
28
49
4138
35 35
48
3943
47
0
5
10
15
20
25
30
35
40
45
50
January/12
February/12
March/12
April/12
May/12
June/12
July/12
August/12
September/12
October/12
November/12
December/12
January/13
February/13
March/13
April/13
May/13
Month/Year
Patie
nts
Series2
Preliminary data for 205 patients for 6 months.
Analysis of controls required.
Average days between referral and First Home Visit
17
8
13 13
22
13 14
6
10
14
4
18
7
11 119
6
0
5
10
15
20
25
30
35
40
45
50
January/12
February/12
March/12
April/12
May/12
June/12
July/12
August/12
September/12
October/12
November/12
December/12
January/13
February/13
March/13
April/13
May/13
Month/Year
Ave
rage
Day
s
Patient
Right Place• Home Visit• GP surgery• Pt venue choice
Right Health Care Professional• Consultant Physician• Health Psychologist• Nurse• Pharmacist• Physiotherapist• Social Worker
Right Assessments• Triage• Risk Assessment Guide • QoL - EQ-5D• Case Review
Right TimeContacting patient within • 48hrs urgent • 10 working days non-urgent
Right Follow-up• Monitoring• Review• Discharge
Right ReferralsLinking patients to• Community Care• GP practice • Whanau Ora & Fanau Ola • WINZ / HNZ (Income / Housing)• Community Pharmacy
Right Care Plan• Shared care plan• Individualised• IDT Case Review
Patient
Right Place• Home Visit• GP surgery• Pt venue choice
Right Health Care Professional• Consultant Physician• Health Psychologist• Nurse• Pharmacist• Physiotherapist• Social Worker
Right Assessments• Triage• Risk Assessment Guide • QoL - EQ-5D• Case Review
Right TimeContacting patient within • 48hrs urgent • 10 working days non-urgent
Right Follow-up• Monitoring• Review• Discharge
Right ReferralsLinking patients to• Community Care• GP practice • Whanau Ora & Fanau Ola • WINZ / HNZ (Income / Housing)• Community Pharmacy
Right Care Plan• Shared care plan• Individualised• IDT Case Review
Acute Bed Days Saved(Data for 6 months prior and 6 months post enrolment)
2110
1382
0
500
1000
1500
2000
2500
Pre VHIU Enrolment Post VHIU Enrolment
Acute bed days
728 days saved35% reduction following VHIU Intervention
Reduction in ED Presentations(Data for 6 months prior and 6 months post enrolment)
718
398
0
100
200
300
400
500
600
700
800
Pre VHIU Enrolment Post VHIU Enrolment
ED presentations
320 presentations saved45% reduction following VHIU Intervention
Collaborative Team:Clinical Lead: Professor Harry Rea Team: Ta-Mera Rolland, Pamela Hill, Lucy Hall, Gray Maingay, Karen Long, Fiona Smyth, Alison Howitt, Rosie Whittington, Prem Kumar
Problem: In the year ending February 2010:• 64,409 patients presented to Emergency Care (EC) 88,565 times • Total bed days for the year were 25,768
Example:Over $2,500 worth of unused medications retrieved from one home visit.
Driver Diagram:
To increase the number of patients enrolled into Very High Intensity User programme from 120 cases to 600 cases by July 2013. This may result in a reduction in unplanned presentation and admission to Middlemore Hospital.
Referral
Pa$ent & Family
Secondary care referrals
Primary Drivers Secondary Drivers
Network and relationship
Model of Care
GP Referral
Resource – Skilled Team
Shared Documenta$on
Home Visit
Assessment & Care Plans
Mul$ple EC presenta$on
Healthcare Professions
Community Resources
Measures: 1. Readmission 2. Presenta1on 4. Admissions 5. LOS 6. Days between presenta1on
Achievements: Tested Model of Care
Results:
www.koawatea.co.nzH E A L T H S Y S T E M I N N O V A T I O N A N D I M P R O V E M E N T
“ Last year I went to hospital 28 times! By looking after myself and having a better understanding of my condition I’ve only been twice so far this year.”George Patient
towa r ds s u sta I n a B l e h e a lt h c a r e
Contributors:Amanda Seabrook, Tanya Naea, Olive Wilson, Clare Moss, Lavinia Buchanan, Kate Martin, Katy Boulton, Tua Teara, Richard Small, Priya Francis, Fay Burke, Christine Lynch, Meg Goodman, Fiona Horwood, Rajiv Gupta, Juliet Ireland, Christine Scott and John Griffiths
Our Aim:To expand the integrated case management programme aimed at keeping people with complex heath needs well and at home by bridging the gaps between healthcare providers and their patients.
Impact:• The VHIU model of care reduced EC presentations and readmissions for high risk patients• The inter-disciplinary team (IDT) assessment of the patient in their home is key to understanding and providing for their healthcare needs• The combined perspective of the range of disciplines involved, provides a holistic and practical plan to meet the needs of the patient• The integrated case management approach bridges the gap between the hospital & community, improving the quality of care for the patient and their quality of life.
Next Steps:• Refining the interdisciplinary (IDT) Model of Care including patient feedback• Ongoing networking and relationship building with our primary care and community partners• Coaching and mentoring to improve IDT practice throughout the Counties Manukau healthcare system• Further development of team processes, including patient centric care plans to align with the National Shared Care IT framework• Evaluate change in patient specific clinical measures, for example HbA1c, International Normalised Ratio (INR) and attendance at outpatient appointments
The VHIU* - Link Team A model of integrated care that helps patients at high risk of readmission
*Very High Intensity Users
Aug
-13
Jul-13
Jun-
13
May
-13
Apr
-13
Mar
-13
Feb-
13
Jan-
13
Dec
-12
Nov
-12
Oct
-12
Sep
-12
Aug
-12
Jul-12
Jun-
12
May
-12
Apr
-12
Mar
-12
Feb-
12
Jan-
12
100
80
60
40
20
0
Month/Year
Num
ber
of P
atie
nts
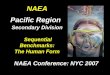
_X=29.7
UCL=52.6
LCL=6.7
Baseline
I Chart of Total Number of Patients Enrolled to VHIU
with primary careTesting of V HIU model
GP referralIncrease in
Aug
-13
Jul-13
Jun-
13
May
-13
Apr
-13
Mar
-13
Feb-
13
Jan-
13
Dec
-12
Nov
-12
Oct
-12
Sep
-12
Aug
-12
Jul-12
Jun-
12
May
-12
Apr
-12
Mar
-12
Feb-
12
Jan-
12
35
30
25
20
15
10
5
0
Month/Year
Num
ber
of D
ays
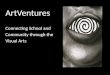
_X=12.58
UCL=30.86
Baseline
I Chart of Time to First Home Visit in Days
Triage processA cuity included in
display testedWhiteboard for v isual
Target number of patients enrolled into VHIU exceeded. Total Patients 843.
There is a shift in process indicating a decrease in the time to first home visit.