Embed Size (px)
Citation preview

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y VO L . 7 1 , N O . 7 , 2 0 1 8
ª 2 0 1 8 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N
P U B L I S H E D B Y E L S E V I E R
THE PRESENT AND FUTURE
REVIEW TOPIC OF THE WEEK
The Burden of Iron Deficiency inHeart FailureTherapeutic Approach
Bruno M.L. Rocha, MD,a Gonçalo J.L. Cunha, MD,a Luiz F. Menezes Falcão, MD, PHDb,c
ABSTRACT
ISS
Fro
Po
rel
Ma
Heart failure (HF) is highlighted by its burdening symptom-limited exercise capacity and recurrent hospitalizations.
Despite substantial advances regarding disease-modifying drugs in HF with reduced ejection fraction, additional thera-
peutic strategies to improve quality of life are invaluable. Currently, iron deficiency (ID) is overwhelmingly recognized in
over 30% to 50% of patients with stable chronic HF, which worsens prognosis. The established pathophysiological
mechanisms of progressive HF may be intertwined with increasing myocardial iron scarcity, wherein one begets the other.
Most importantly, ID constitutes a novel target for symptom relief in carefully selected patients. In this regard, intra-
venous iron may be a safe and efficacious intervention, potentially reducing HF hospitalizations. We discuss the evidence
and gaps in knowledge concerning iron therapy in HF and propose a practical, comprehensive, clinically oriented
algorithm for timely adequate iron replenishment in different clinical scenarios. Finally, we further debate imperative
decision-making before intervention and the drawbacks of such a strategy. (J Am Coll Cardiol 2018;71:782–93)
© 2018 by the American College of Cardiology Foundation.
H eart failure (HF) is a chronic disabling syn-drome with a prevalence of 1% to 2% in theglobal population and $10% in those
age $65 years, and is being increasingly recognizedin younger patients (1,2). Acute on chronic HF is theleading cause of recurrent hospitalizations and earlyreadmissions, which accounts for its notably highmorbidity and costs. Patients have a lower quality oflife, and their survival is gravely compromised (3,4).
Given the burden of HF, contemporary researchhas also been focusing on interventions with animpact on quality of life (5,6). On this matter, the roleof iron abnormalities is being widely acknowledged.Therefore, we sought to discuss the definition,epidemiology, pathophysiology, and prognosis ofiron deficiency (ID); to debate the main trials of oraland intravenous (IV) iron in HF and gaps in evidence;and to propose an algorithm for careful and timely
N 0735-1097/$36.00
m the aHospital Amadora-Sintra, Lisbon, Portugal; bDepartment of Inte
rtugal; and the cFaculty of Medicine, University of Lisbon, Lisbon, Port
ationships relevant to the contents of this paper to disclose.
nuscript received October 22, 2017; revised manuscript received Decemb
adequate selection of candidates for IV ironreplenishment.
DEFINITION AND EPIDEMIOLOGY
DEFINING ID IN HF. ID in the adult general popula-tion is defined by the World Health Organization asplasma ferritin <15 mg/l. However, a higher cutoff forferritin (an acute-phase reactant) in chronic inflam-matory conditions is recommended (7,8). Accord-ingly, in chronic HF, absolute ID is defined asferritin <100 mg/l and functional ID is defined asferritin between 100 and 300 mg/l when transferrinsaturation (TSAT) is <20% (5,6). These definitions arederived from studies in patients with chronic kidneydisease (7,8), in whom the cutoff values are alreadycontroversial (9). On a related note, a study by Nanaset al. (10) in patients admitted for decompensated
https://doi.org/10.1016/j.jacc.2017.12.027
rnal Medicine, Hospital Santa Maria/CHLN, Lisbon,
ugal. The authors have reported that they have no
er 18, 2017, accepted December 19, 2017.

AB BR E V I A T I O N S
AND ACRONYM S
AHF = acute heart failure
FCM = ferric carboxymaltose
HFrEF = heart failure with
reduced ejection fraction
ID = iron deficiency
LVEF = left ventricular
ejection fraction
MID = myocardial iron
deficiency
pVO2 = peak oxygen
consumption
sTfR = soluble transferrin
receptor
= transferrin saturation
J A C C V O L . 7 1 , N O . 7 , 2 0 1 8 Rocha et al.F E B R U A R Y 2 0 , 2 0 1 8 : 7 8 2 – 9 3 Iron Deficiency in Heart Failure
783
advanced HF and ID (defined by the absence of iron inbone marrow biopsy) showed a mean plasma ferritinof 75.3 � 59.1 mg/l (10), which is in accordance with thehigher cutoff value to define absolute ID.
Defining ID in acute heart failure (AHF) poses evena greater challenge. A small observational studypointed toward a significant variation of both meanferritin and TSAT in acute decompensated HF; thisled to a surprising apparent decrease in ID prevalenceat 30-day follow-up, which weakly correlated withinflammatory status (11). One may hypothesizewhether plasma volume variations and additionalunknown factors regulating serum ferritin, other thaninflammation, render it unsuitable to define ID inacute decompensated HF.
Alternative plasma surrogate markers may be moreaccurate to identify ID. Specifically, serum solubletransferrin receptor (sTfR) may correlate withmyocardial ID in the failing heart (12) and has prog-nostic value in chronic HF (13). Likewise, sTfR($1.59 ng/ml) and/or hepcidin (<14.5 ng/ml) might bemore adequate to unveil significant ID in acute set-tings (14). Further studies are warranted, as volume-independent or plasma volume-corrected indexeswould ideally reveal true ID.
For the remainder of this review, ID and HF will bedefined as stated by the guidelines (5,6) and anemiaas stated by the World Health Organization, unlessotherwise specified.
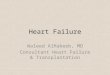
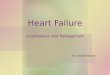
EPIDEMIOLOGY. ID is overwhelmingly common instable chronicHF (30% to 50%) (15–17),most ofwhich isabsolute (Figures 1 and 2). It remains prevalent (>30%)in patients without anemia or abnormalities in hema-tologic indexes (17), underscoring its burgeoningpervasiveness even in a low-risk HF population (15). IDin chronic HF is more often found in women (15,16,18)and in patients with advanced HF (as noted by highernatriuretic peptide levels [15,16,19,20] and/or NewYork Heart Association [NYHA] functional class[15,16,18–20]), heightened inflammation (as noted byhigh-sensitivity C-reactive protein [15]), and/or ane-mia (16,18,20). Remarkably, studies have supported ahigher prevalence in AHF (50% to 80%) (10,11,21,22),most of which is surprisingly absolute (21,22).
PATHOPHYSIOLOGY. Myocard ia l i ron defic iency .Iron has an important role beyond oxygen transportand storage (Central Illustration), as it is also funda-mental for the normal activity of key enzymes of thecitric acid cycle and reactive oxygen species (ROS)scavenging enzymes (23,24). Indeed, a study (n ¼ 129)with samples of the left ventricle of the human heartshowed that myocardial iron content was lower in HFcomparedwith control subjects (p<0.001). The former
had reduced activity of all examined mito-chondrial enzymes (p < 0.001). Additionally,patients with both HF and myocardial irondeficiency (MID), compared with those withHF but no MID, had reduced activity of thecitric acid cycle enzymes aconitase and citratesynthase (by 26% and 15%; both p < 0.05), aswell as reduced expression of the ROS scav-enging enzymes catalase, glutathione peroxi-dase, and superoxide dismutase (by 23%, 21%,and 20%, respectively; all p < 0.05). Interest-ingly, MID had no association with inflamma-tion (25).
One may hypothesize that lower citric acidcycle activity impairs the normal bio-energetics in the cardiomyocytes, similar to
the phenomenon observed in myocytes of the exer-cising skeletal muscle in HF (26). Abnormal bio-energetics could lead to impaired maximal exercisecapacity, for instance, due to limited left ventricularcontractile reserve (inability to increase cardiacoutput with exercise), as shown in ID heart failurewith reduced ejection fraction (HFrEF) (27). With re-gard to decreased ROS scavenging enzymes in MID,local oxidative stress may intensify with ensuingmyocardial damage (28).MID may parallel the impaired iron uptake by pe-ripheral tissues. A small study in advanced systolic(left ventricular ejection fraction [LVEF] <35%) HFhas shown that myocardial iron content and trans-ferrin receptor (TfR)-1 expression are significantlyreduced in the failing heart. Moreover, in isolated ratventricular cardiomyocytes, TfR-1 expression wasdown-regulated after in vitro exposure to catechol-amines (beta-agonists) and aldosterone (29), whichmay constitute the fundamental link between thecurrently known HF pathophysiology, with over-activity of both sympathetic nervous (30) and renin-angiotensin systems (31), and MID.
Iron content in the myocardium may be measuredby T2* cardiac magnetic resonance imaging (CMR),validated in iron overload states (32). The potential ofimaging to detect MID is currently emerging. In thisregard, a study (n ¼ 198) in symptomatic HF hasshown that a lower iron myocardial content(measured by T2* CMR) predicted nonischemic HF(particularly when LVEF <35%; C-statistic: 0.78) andrisk of future major adverse cardiac events (C-statis-tic: 0.66) (33). A small study in a similar population(nonischemic HF in 7 of 8 patients) used T2* CMRbefore and after 1,000 mg of ferric carboxymaltose(FCM). The authors found a significant replenish-ment of myocardial iron (p ¼ 0.012), as well asNYHA functional class improvement and reverse
TSAT

FIGURE 1 Prevalence of ID in HF
Country/continent
N
Mean age
Mean LVEF
Mean NYHA
Pola
nd
443
54
26
2.4
Pola
nd
546
55
26
2.5
Germ
any
1198
69
35
2.4
Euro
pe
1506
64
33
-
Euro
pe
1821
66
35
2.4
Euro
pe
923
70
-
-
Euro
pe
1278
68
38
2.4
Unite
dKi
ngdo
m
157
71
32
2.6
Fran
ce832
78
-
2.9Sp
ain
626
73
-
-
Fran
ce
47
70
39
-
Euro
pe
331
64
35
2.2
Chronic Heart Failure
Studies marked with include patientswith both chronic and acute Heart Failure
ADHF
First daysafter
admission
30daysafteradm.
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
35%
Jank
owsk
aet
al.
2011
(39)
Perc
enta
ge
Jank
owsk
aet
al.
2010
(15)
von
Hae
hlin
g et
al. 2
017
(19)
Ebne
r et a
l. 20
16 (3
8)
Klip
el a
l. 20
13 (1
6)
Tkac
zysz
ynel
al.
2017
(17)
Wie
nber
gen
et a
l. 20
16 (1
8)
Enju
anes
et.
al 2
014
(20)
Oko
nko
et a
l.20
11 (3
6)
Cohe
n-So
lal
et a
l. 20
14 (2
2)
Van
Aels
t et a
l.20
17 (1
1)
37%43% 45%
50% 52% 55%58%
69% 72% 74%
83%
68%
~Nù
nez
et a
l.20
16 (2
1)
It should be noted that volume variations during the acute phase might dilute ferritin, rendering traditional criteria to define iron deficiency (ID) in ADHF potentially
unsuitable. ADHF ¼ acute decompensated heart failure; HF ¼ heart failure; LVEF ¼ left ventricular ejection fraction; NYHA ¼ New York Heart Association.
Rocha et al. J A C C V O L . 7 1 , N O . 7 , 2 0 1 8
Iron Deficiency in Heart Failure F E B R U A R Y 2 0 , 2 0 1 8 : 7 8 2 – 9 3
784
remodeling in 50% of patients, accompanied by in-creases in 6-min walking test (6MWT) (34).
Trials in ID symptomatic HF are currently investi-gating whether IV iron improves skeletal muscleenergetics: FERRIC-HF-II (Ferric Carboxymaltose toImprove Skeletal Muscle Metabolism in Heart FailurePatients With Functional Iron Deficiency; EudraCTNumber: 2012-005592-13) and Ferric Carboxymaltoseto Improve Skeletal Muscle Metabolism in HeartFailure Patients With Functional Iron Deficiency(NCT03218384) and its impact on mitochondrial geneexpression (NCT01978028) and myocardial iron con-tent (MYOCARDIAL-IRON [Changes in MyocardialIron Content Following Administration of Intrave-nous IRon; EudraCT Number: 2016-004194-40]).
ID IN THE NATURAL HISTORY OF HF
Iron homeostasis is distinctively impaired in HF,because neither hepcidin nor ferritin levels parallel
those of inflammatory markers. Asymptomatic (NYHAfunctional class I) patients with HF have normal orhigh serum ferritin levels in the presence of a lowinflammatory status, yet hepcidin is disproportion-ately elevated (p < 0.001). Whether such earlyincrease of hepcidin in asymptomatic patients has arole in progressive ID is unknown. As severity in-creases (NYHA functional class II to IV), ID emerges(as measured by ferritin, TSAT, and sTfR) andinflammation exacerbates (as measured by high-sensitivity C-reactive protein and interleukin-6);however, paradoxically, hepcidin levels are signifi-cantly reduced (all p < 0.001), predicting highermortality rates (35). We may hypothesize that theobservation of such low hepcidin levels are the resultof profound ID overshadowing the effects of low-grade inflammation (35,36).
Not only may progressive HF cause ID, but ID ap-pears to also be able to induce HF. Indeed, in an MID

FIGURE 2 Iron and Anemia Status in HF
~
Chronic Heart Failure
Studies marked with include patientswith both chronic and acute Heart Failure
ADHF
First daysafter adm.
Without anemia With anemia No information Absolute iron deficiency Relative iron deficiency
30daysafteradm.
100
90
80
70
60
50
40
30
20
10
0
Perc
enta
ge
Jank
owsk
aet
al.
2011
(39)
von
Hae
hlin
g et
al. 2
017
(19)
Ebne
r et a
l. 20
16 (3
8)
Klip
el a
l. 20
13 (1
6)
Tkac
zysz
ynel
al.
2017
(17)
Wie
nber
gen
et a
l. 20
16 (1
8)
Enju
anes
et.
al 2
014
(20)
Oko
nko
et a
l.20
11 (3
6)
Cohe
n-So
lal
et a
l. 20
14 (2
2)
Nùne
z et
al.
2016
(21)
Van
Aels
t et a
l.20
17 (1
1)
Most patients with ID and chronic HF are nonanemic. Moreover, absolute ID predominates over relative ID in chronic HF. These observations may not be noted in the
acute phase using traditional plasma surrogate markers. Abbreviations as in Figure 1.
J A C C V O L . 7 1 , N O . 7 , 2 0 1 8 Rocha et al.F E B R U A R Y 2 0 , 2 0 1 8 : 7 8 2 – 9 3 Iron Deficiency in Heart Failure
785
model, TfR-1 knockout mice died shortly after birthdue to a lethal dilated cardiomyopathy unless largedoses of IV iron were administered (37). A bold hy-pothesis of a vicious cycle could be formulatedwherein progressive HF begets MID. In this manner,ID could even be perceived as a secondary cause of HFdecompensation.
PROGNOSIS. ID, regardless of anemia, has beenshown to be independently related to increasedmortality, hospitalization, and early readmission(Table 1). Remarkably, patients with isolated ID had aworse prognosis compared with those with anemiaand no ID (36). Higher mortality rates are alreadynoted after 6-month follow-up (16). Furthermore, IDis associated with burdensome impaired exercise ca-pacity, as measured by peak oxygen consumption(pVO2) (19,36,38,39), 6MWT (13,38,40), EuroQol FiveDimensions Questionnaire (18,40), Kansas CityCardiomyopathy Questionnaire (KCCQ) (40), PatientGlobal Assessment (40), and Minnesota Livingwith HF Questionnaire (20). It should be emphasizedthat disease-modifying therapies in HF are ofthe utmost importance (5,6), but these may not pro-vide symptomatic improvement (e.g., beta-blockers).
Interestingly, one may hypothesize whether IDcorrection would allow higher tolerance to initiateand/or up-titrate these drugs.
MANAGEMENT OF ID IN HF
ORAL IRON SUPPLEMENTATION. The multicenter,double-blinded, randomized controlled trial (RCT)IRONOUT HF (Oral Iron Repletion Effects On OxygenUptake in Heart Failure), which randomized 255 IDchronic symptomatic HFrEF patients to either ironpolysaccharide (150 mg twice daily orally) or placeboover a 16-week follow-up, has shown no significantdifferences between groups in natriuretic peptides,KCCQ score, 6MWT, or pVO2 (41). Accordingly, theavailable evidence does not support a role for oraliron in ID HFrEF patients, and one should refrainfrom futile polypharmacy and unwanted adverseevents.
In the IRONOUT HF trial, patients in the highestTSAT increment quartile (i.e., with lower hepcidinlevels) did have a meaningful improvement in KCCQscore (p ¼ 0.047) and tended toward an improvementin pVO2 (p ¼ 0.08) in response to oral iron (41).

CENTRAL ILLUSTRATION Pathophysiology of ID in HF
Patient with heart failure with reduced ejection fraction (HFrEF)
Inhibition of Transferrin receptor protein 1 (TfR1)required for iron import into cells
Reduced exercise capacity; fatigue;worsening HF prognosis; increased hospitalizations
InflammationRenin-Angiotensin-Aldosterone System (RAAS) overactivity
Sympathetic nervous system overactivity
Iron deficiency leads to:Decreased cellular oxygen storing and carrying capacity
Impaired cellular energy release (citric acid cycle)Impaired cellular Reactive Oxygen Species (ROS) metabolism
Intravenous ironmay alleviateworsening HF
symptoms and reducehospitalizations
in carefully selected patients
Rocha, B.M.L. et al. J Am Coll Cardiol. 2018;71(7):782–93.
Contrary to oral formulations, intravenous iron bypasses intestinal absorption. The pathophysiology of heart failure (HF) intertwines with that of iron deficiency (ID), as
inflammation and overactivity of both the RAAS and sympathetic nervous system may inhibit iron cellular uptake by blocking transferrin receptor. Iron scarcity in both
myocyte and erythroid cells lead to symptoms similar to those of HF. RAAS ¼ renin-angiotensin-aldosterone system; ROS ¼ reactive-oxygen species.
Rocha et al. J A C C V O L . 7 1 , N O . 7 , 2 0 1 8
Iron Deficiency in Heart Failure F E B R U A R Y 2 0 , 2 0 1 8 : 7 8 2 – 9 3
786
Accordingly, blunted responsiveness to oral irontherapy was reported in ID anemia with up-regulatedhepcidin levels (42). Furthermore, pitfalls such as lowbioavailability, gastrointestinal adverse effects, lowrates of adherence, polypharmacy (24,43), and a
TABLE 1 ID as a Marker of Prognosis
First Author, Year (Ref. #) MortalityMortality andHospitalization 6MWT p
Tkaczyszyn et al., 2017 (17) U — —
Klip et al., 2013 (16) U — —
Jankowska et al., 2010 (15) U — —
Martens et al., 2016 (27) — U —
von Haehling et al., 2017 (19) — — �Ebner et al., 2016 (38) — — —
Jankowska et al., 2011 (39) — — —
Wienbergen et al., 2016 (18) — — —
Enjuanes et al., 2014 (20) — — —
Núñez et al., 2016 (21) — U —
ADHF ¼ acute decompensated heart failure; CHF ¼ chronic heart failure; HFrEF ¼ hearejection fraction; NYHA ¼ New York Heart Association; pVO2 ¼ peak oxygen consumpti
potentially longer time interval to fully restore irontransportation capacity and storage (44) (TSATincreased significantly but minimally [þ3.3%;p ¼ 0.003] in IRONOUT HF [41] compared with IV iron[i.e., TSAT þ11%; p < 0.001] in FAIR-HF [Ferinject
VO2 QoL N Mean Age Population LVEF Mean NYHA
— — 1,821 66 CHF All 2.4
— — 1,506 64 CHF All —
— — 546 55 CHF HFrEF 2.5
— — 541 72 CHF HFrEF 2.6
U — 1,198 69 CHF HFrEF 2.4
U — 331 64 CHF All 2.2
U — 443 54 CHF HFrEF 2.4
— U 923 70 All HFrEF —
— U 1,278 68 All All 2.4
— — 626 73 ADHF All —
t failure with reduced ejection fraction; ID ¼ iron deficiency; LVEF ¼ left ventricularon; QoL ¼ quality of life; 6MWT ¼ 6-min walk test.

J A C C V O L . 7 1 , N O . 7 , 2 0 1 8 Rocha et al.F E B R U A R Y 2 0 , 2 0 1 8 : 7 8 2 – 9 3 Iron Deficiency in Heart Failure
787
Assessment in Patients With IRon Deficiency andChronic Heart Failure] [45]; ferritin levels increasedsignificantly but minimally [þ32 mg/l; p < 0.0001]with oral iron [46] compared with IV iron [i.e.,ferritin þ259 mg/l; p < 0.001] in FAIR-HF [45]), just toname a few, hamper the usefulness of oral iron.
Whether oral liposomal iron is appropriate,considering that it bypasses ferroportin-dependentiron absorption, is unknown. Although seeminglyinferior to the IV route in long-term iron reservereplenishment (47), it could potentially be advanta-geous as coadjuvant therapy.
INTRAVENOUS IRON THERAPY. In comparison to theoral route, IV iron allows restoration of storesregardless of hepcidin blocking mechanisms. Addi-tionally, iron may be administered in larger doses,hence expeditiously correcting the deficit (43). Inchronic HF, iron sucrose (48–51) and FCM (45,52,53)are the most studied IV formulations. The mainRCTs comparing IV iron with placebo or control areextensively reviewed elsewhere and are briefly sum-marized in Table 2.
The FAIR-HF RCT (45) has shown symptomaticimprovement in patients receiving FCM comparedwith placebo. The CONFIRM-HF (A Study to Comparethe Use of Ferric Carboxymaltose With Placebo in Pa-tients With Chronic Heart Failure and Iron Deficiency)(52) RCT strengthened these findings using highersingle iron doses and extending the observed benefitsto 1 year in patients with hemoglobin <15 g/dl. Bothtrials found benefits regardless of anemia. Recently,the results of the multicenter, open-label, endpoint-blinded EFFECT-HF (Effect of Ferric Carboxymaltoseon Exercise Capacity in Patients with Chronic HeartFailure and Iron Deficiency) (53) RCT were published.Compared with placebo, treatment with FCM (mean1,204 mg) significantly improved NYHA functionalclass from week 6 onwards and Patient GlobalAssessment from week 12 onwards, with sustainedpVO2 levels at 24 weeks (�1.19 � 0.389 ml/min/kgvs.�0.16� 0.387ml/min/kg; p¼ 0.020). However, thisstatistical significance disappeared (p ¼ 0.23) onsensitivity analysis after removing patients who diedduring the study (4 deaths in control vs. 0 deaths inFCM), whose imputed value for 24-week pVO2 waszero. Thus, the authors conclude that the effects ofFCM on pVO2, an objective measurement of exercisecapacity in HF, were not conclusive, demandingfurther research.
Ameta-analysis including 839 patients with chronicHF enrolled in 4 double-blinded RCTs (FER-CARS-01,FAIR-HF [45], EFFICACY-HF [EFfect of Ferric Car-boxymaltose on exercIse CApacity and Cardiac
Function in Patients With Iron deficiencY and ChronicHeart Failure] [NCT00821717], and CONFIRM-HF [52])suggested that, compared with placebo, FCM reducedrecurrent HF hospitalizations (relative risk [RR]: 0.41;95% confidence interval [CI]: 0.23 to 0.73; p ¼ 0.003)and recurrent cardiovascular hospitalizations (RR:0.54; 95% CI: 0.36 to 0.83; p ¼ 0.004) (54). A system-atic review with meta-analysis including 5 RCTsshowed a robust reduction in hospitalizations for HF(odds ratio: 0.28; 95% CI: 0.16 to 0.50; p < 0.0001) inpatients receiving IV iron compared with placebo.However, these results weremainly driven by the FCMtrials (n ¼ 760 of 851). Also, the HF hospitalizationreduction was only borderline (nonstatistically) sig-nificant in nonanemic patients (55).
SAFETY CONCERNS. IV iron has been shown to besafe in HF, without increasing the rate of severeadverse events, namely infections or anaphylacticreactions (56). A systematic review with meta-analysis, including 10,390 patients, in diverse acuteand chronic conditions beyond HF has shown that IViron increased the risk of acute nonsevere adverseevents, including hypotension (RR: 1.39; 95% CI: 1.09to 1.77; number needed to harm [NNH]: 97); electro-lyte abnormalities (RR: 2.45; CI: 1.84 to 3.26; NNH:19), particularly hypophosphatemia; mild skin re-actions (RR: 1.60; CI: 1.05 to 2.45; NNH: 99); andmusculoskeletal side effects, especially with FCM(RR: 3.42; CI: 2.02 to 5.79; NNH: 32), none of which ledto drug discontinuation (57).
As for iron overload concerns, a study innondialysis-dependent chronic kidney disease pa-tients (n ¼ 304) with ID anemia receiving FCM foundthat high ferritin levels ($800 mg/l) occurred at leastonce in approximately one-quarter of the cohort at1-year follow-up, with no associated increase inadverse events. However, <10% of these patients hadHF, and these safety findings, albeit reassuring,should not be generalized (58).
COST-EFFECTIVENESS. Economic evaluations sup-port the cost-effectiveness of FCM driven by NYHAfunctional class shift and/or hospitalization ratereduction (59,60). Because total iron dosemay be givenin fewer infusions with FCM compared with otherformulations, costs per treatment may be lower in theformer (61). Accordingly, an IV iron replenishmentstrategy may be advantageous not only for the indi-vidual patient, but also to lessen recurring HF hospi-talizations, mitigating the overwhelming HF costs.
OTHER FORMULATIONS. IV formulations other thaniron sucrose and FCM have not been extensivelystudied in HF. Iron dextran is associated with

TABLE 2 Main Trials Comparing IV Iron to Placebo or Control
Iron Sucrose vs. Placebo Ferric Carboxymaltose vs. Placebo
Toblli et al. (48,49) FERRIC-HF (50) IRON-HF (51) FAIR-HF (45) CONFIRM-HF (52) EFFECT-HF (53)
Inclusion criteria
HF population Chronic HF Chronic HF Chronic HF Chronic HF Chronic HF Chronic HF
Stability >4 weeks >4 weeks >4 weeks >2 weeks >4 weeks >4 weeks
NYHA functional class II–IV II–III II–IV II–III II–III II–III
Hb, g/dl <12.5 men,<11.5 women
<14.5 9–12 9.5–13.5 <15 <15
ID definition Ferritin <100 mg/land/orTSAT #20%
Ferritin <100 mg/l or100–300 mg/l ifTSAT <20%
Ferritin <500 mg/land TSAT <20%
Ferritin <100 mg/l or100–299 mg/l ifTSAT <20%
Ferritin <100 mg/l or100–300 mg/l ifTSAT <20%
Ferritin <100 mg/lor 100–300 mg/lif TSAT <20%
LVEF #35% #45% <40% <40 or 45% (if NYHAII or III)
#45% #45%
Other Nondialyzed CKD pVO2 #18 ml/kg/min Creatinine #1.5mg/dl
— BNP >100 pg/ml andNT-proBNP >400 pg/ml
— pVO2 10–20ml/kg/min
Study design
Center(s) Single Multiple Multiple Multiple Multiple Multiple
Design Double-blinded RCT Open-label endpoint-blinded RCT
Double-blinded RCT Double-blinded RCT Double-blinded RCT Open-labelendpoint-blinded RCT
Mean IV iron dose 1,000 mg 928 mg 1,000 mg 1,850 mg 1,500 mg 1,204 mg
Correction phase 200 mg/week for5 weeks
200 mg/week for4 weeks orferritin $500 mg/l
IS: 200 mg/weekFS: 200 mg orally
3 times/day
200 mg/week untilrepletion
500-2,000 mg atweeks 0 and 6
500-2,000 mg atweeks 0 and 6
Maintenance phase 200 mg every4 weeks
200 mg every4 weeks
500 mg every12 weeks if ID
500 mg every12 weeks if ID
Treatment duration 5 weeks 16 weeks 5 (IS) vs 8 (FS) weeks 24 weeks 0-36 weeks 0-12 weeks
Follow-up 24 weeks 18 weeks 12 weeks 24 weeks 52 weeks 24 weeks
Patients (active vs.control)
N ¼ 60 (20 þ 10 ISvs. 20 þ 10controls)
N ¼ 35 (24 IS vs. 11controls)
N ¼ 23 (10 IS vs. 7 FSvs. 6 placebo)
N ¼ 459 (304 FCMvs. 155 placebo)
N ¼ 301 (150 FCM vs.151 placebo)
N ¼ 172 (86 FCMvs. 86 placebo)
Continued on the next page
Rocha et al. J A C C V O L . 7 1 , N O . 7 , 2 0 1 8
Iron Deficiency in Heart Failure F E B R U A R Y 2 0 , 2 0 1 8 : 7 8 2 – 9 3
788
increased risk of anaphylactic reactions (62), limitingits clinical utility. Iron (III) isomaltoside 1,000 is astable, low-immunogenicity IV iron compound thatmay offer advantages in profoundly iron-depletedpatients, as it may be administered in higher indi-vidual doses (63). A large RCT (NCT02642562) will testthis IV formulation (maximum 2,000 mg) in high-risksymptomatic HF (LVEF <45%) and absolute ID over2.5-year follow-up.
ID CORRECTION ALGORITHM
DEFINING THE PROBLEM. Despite being a highlyprevalent comorbid condition in HF, ID (isolated orcombined with anemia) is often overlooked andinappropriately managed in “real-world” settings(18). Clinical manifestations of ID, anemia, and/orHF (i.e., fatigue, exercise intolerance, dyspnea) arenot enlightening for differential diagnosis, nor arethe hematologic surrogate markers beyond ferritinand/or TSAT (7,24). Thus, to identify potentialcandidates for iron repletion, one may have toconsider screening all stable patients with chronic
HF (17). Given the inclusion criteria for the mainRCTs (45,52,53), IV iron may at least be beneficial inthose with hemoglobin <13.5 to 15 g/dl andLVEF <40% to 45%. Accordingly, with the intent tomitigate the often-missed opportunities, we proposea simplified algorithm (Figure 3) to accuratelydiagnose and treat selected patients based on theenrollment criteria of the main trials (Table 2).
SETTINGS FOR ID CORRECTION
AHF hospitalization may be an opportunity for IDcorrection; yet, thus far, it is a nonevidence-basedintervention. Ferritin may be inadequate for IDdetection in AHF; bone marrow biopsy is inappro-priately invasive for routine iron status evaluation;HF decompensation may be secondary to activeinfection, a controversial contraindication for iron;and no RCT that we know of has specifically assessedIV iron in AHF; hence, efficacy and safety in thissetting is obscure, and further studies are warranted.
Patients in the early (<30 to 90 days) vulnerablepost-discharge transition phase should be closely

TABLE 2 Continued
Iron Sucrose vs. Placebo Ferric Carboxymaltose vs. Placebo
Toblli et al. (48,49) FERRIC-HF (50) IRON-HF (51) FAIR-HF (45) CONFIRM-HF (52) EFFECT-HF (53)
Baseline characteristics (active arm – IV iron)
Mean age, yrs 75 � 6 64 � 14 67 � 8 68 � 10 69 � 10 63 � 12
Male, % 47 71 67 48 55 70
Mean LVEF, % 30 � 4 30 � 7 25 � 9 32 � 6 37 � 8 33 � 9
NYHA I/II/III/IV Mean 3.0 � 0.7 0/13/11/0 — 0/53/251/0 0/80/70/0 0/61/25/0
Ischemic etiology, % 70 75 39 81 83 —
Mean Hb, g/dl 10.1 � 0.8 12.6 � 1.2 11.2 � 0.6 11.9 � 1.3 12.4 � 1.4 12.9 � 1.3
Mean ferritin, mg/l 71 � 25 62 � 37 185 � 146 53 � 55 57 � 49 48
Mean TSAT, % 19 � 1.8 20 � 8 19 � 9.7 18 � 12.6 20 � 17.6 17.3
Surrogate laboratorial outcomes at follow-up in the active arm compared with placebo/control
Hb [* NS NS [* [* [*
Ferritin [* [* [† [* [* [*
TSAT [* [* [† [* [* [*
Symptomatic outcomes at follow-up in the active arm compared with placebo/control
NYHA functional class Y* Y† — Y* (from week 4) Y* (from week 24) Y† (from week 6)
6MWT [† — — [* (from week 4) [* (from week 24) —
QoL scales MLHFQ† PGA†MLHFQ†
— PGA* (from week 4)EQ—5D* (fromweek 4)KCCQ* (from week 4)
PGA* (from week 12)EQ—5D* (fromweek 36)KCCQ* (from week 12)
PGA† (fromweek 12)
pVO2 — [*‡ NS — — [†§
Major outcomes at follow-up in the active arm compared with placebo/control
Hospitalizationsoutcomes
Reducedhospitalization*
— — NS Reducedhospitalizationfor worsening HF†k
—
Mortality — — — NS NS —
*p < 0.001. †p < 0.05. ‡only statistically significant in anemic patients in subgroup analysis. §nonsignificant (p ¼ 0.23) after removing deaths from analysis. ||post hoc analysis.
BNP ¼ brain natriuretic peptide; CKD ¼ chronic kidney disease; CONFIRM-HF ¼ A Study to Compare the Use of Ferric Carboxymaltose With Placebo in Patients With Chronic Heart Failure and IronDeficiency; EFFECT-HF ¼ Effect of Ferric Carboxymaltose on Exercise Capacity in Patients with Chronic Heart Failure and Iron Deficiency; EQ-5D¼ EuroQol Five Dimensions Questionnaire; FAIR-HF¼ FerinjectAssessment in Patients With IRon Deficiency and Chronic Heart Failure; FCM ¼ ferric carboxymaltose; FERRIC-HF II ¼ Ferric Carboxymaltose to Improve Skeletal Muscle Metabolism in Heart Failure PatientsWith Functional Iron Deficiency; FS ¼ ferrous sulfate; Hb ¼ hemoglobin; HF ¼ heart failure; ID ¼ iron deficiency; IRON-HF ¼ Iron Supplementation in Heart Failure Patients With Anemia; IS ¼ iron sucrose;IV ¼ intravenous; KCCQ ¼ Kansas City Cardiomyopathy Questionnaire score; LVEF ¼ left ventricular ejection fraction; MLHFQ ¼ Minnesota Living With Heart Failure Questionnaire; NS ¼ not significant; NT-proBNP ¼ N-terminal pro-brain natriuretic peptide; NYHA ¼ New York Heart Association; PGA ¼ Patient Global Assessment; pVO2 ¼ peak oxygen consumption; QoL ¼ quality of life; RCT ¼ randomizedcontrolled trial; TSAT ¼ transferrin saturation; 6MWT ¼ 6-min walking test.
J A C C V O L . 7 1 , N O . 7 , 2 0 1 8 Rocha et al.F E B R U A R Y 2 0 , 2 0 1 8 : 7 8 2 – 9 3 Iron Deficiency in Heart Failure
789
followed, as medication adherence decreases overtime (5,6). Therapy optimization (i.e., diuretic doseadjustment and up-titration of disease-modifyingdrugs) and eventually IV iron (in selected ID stablepatients with chronic HF) can improve outcomes andpotentially reduce early rehospitalizations. We pro-pose that a HF day-hospital could provide themeans to articulate these interventions (Table 3).Most patients will only need 1 or 2 FCM infusions(#6 weeks) for complete replenishment over 6 to12 months (52,53).
HIGHLIGHTS AND SHORTCOMINGS
RECOMMENDATIONS. The 2017 ACC/AHA/HSAguidelines (6) state that IV iron may be reasonable inselected NYHA functional class II to III patients withHF (recommendation level II-B), and the 2016 ESCguidelines (5) recommend (II-A) IV iron in
symptomatic HFrEF to alleviate symptoms andimprove functional status. Our proposed algorithmemphasizes the paramount importance of a carefullyselected population with regard to stability, NYHA,LVEF, and hemoglobin levels.
ANEMIA. ID anemia may be due to underlyinggastrointestinal losses, especially in high-risk pop-ulations. Therefore, to rule out secondary causes,upper and lower endoscopy should be consideredamong elderly patients (5,64). However, given theuncertain pathophysiology, the appropriateness ofroutine investigation of isolated ID (without anemia)is debatable. It should be noted that endoscopicevaluation is not without risk (65).
FUNCTIONAL ID. Most patients enrolled in FCM trials(45,52,53) had absolute ID (80% to 90%), whereasfunctional ID was under-represented, contrastingwith the known epidemiology in the “real-world” HF

FIGURE 3 ID Correction Algorithm
Iron deficiency - Ferritin <100µg/L, or 100-300µg/L with Transferrin saturation <20%
Heart Failure
ADHF CHF on OMT
STOP STOPNot enough data
Not enough dataNot enough data
Not enough data
Not enough data
Not e
noug
h da
ta
Iron DeficiencyNo Iron Deficiency No Iron DeficiencyIron Deficiency
Echocardiogram
Day-hospital referral and re-evaluation
LVEF <40-45% LVEF >45%
NYHA I NYHA II-III NYHA IV
Hb <12g/dL ♀Hb <13g/dL ♂
Hb <13.5g/dL(possibly 13.5-15g/dL) Hb >15g/dL
• Exclude secondarycauses for IronDeficiency anemia
• Correct other causesfor anemia (folate, B12,hypothyroid)
Exclude:• Active infection• Active malignancy• Ferric carboxymaltosehypersensitivity
Hb ≥10 g/dL
Hb <10 g/dL
Hb <10 g/dL
Hb ≥10 g/dL
1000mg
1000mg
1000mg
1000mg
1000mg
500mg
500mg
0 mg
Intr
aven
ous i
ron
500
mg
If ID
per
sists
500
mg
If ID
per
sists
500
mg
If ID
per
sists
Pt w
eigh
t>7
0kg
Pt w
eigh
t35
-70k
g
Correction phase Maintenance phase
Wk. 0 Wk. 6 Wk. 12 Wk. 24 Wk. 36 Wk. >36
Built on the premise: would my patient with HF and ID be enrolled in a main trial of FCM? CHF ¼ chronic heart failure; Hb ¼ hemoglobin;
OMT ¼ optimized medical therapy; other abbreviations as in Figure 1.
Rocha et al. J A C C V O L . 7 1 , N O . 7 , 2 0 1 8
Iron Deficiency in Heart Failure F E B R U A R Y 2 0 , 2 0 1 8 : 7 8 2 – 9 3
790
population. Although evidence may be limited in thelatter subgroup, a large (n ¼ 1,821) pooled analysisstudy has suggested that worse prognosis was onlydetected in the presence of impaired iron trans-portation (i.e., TSAT <20%, contrarily to isolated low
[<100 mg/l] ferritin levels [TSAT $20%]) (66). Thesefindings may hint at the possibility that a low TSATlevel is the hallmark of ID in chronic HF. It would beinteresting to explore whether differences in thesesubgroups are noted in response to IV iron.

TABLE 3 ID Treatment in Different Clinical Scenarios
Setting Advantages Disadvantages
Oral iron
Ambulatory chronic HF � Safe and simple oral administration.� Inexpensive
� No proven efficacy compared with placebo(IRONOUT HF trial [41]).
� Slow inefficient minor replenishment of iron stores.� Poor adherence.� Considerable gastrointestinal toxicity.� Polypharmacy and possible drug interactions.
IV iron
Acute HF admission � Opportunity to identify and treat ID beforedischarge, once HF is stabilized.
� The evidence supporting efficacy and safety isawaited:
� PRACTICE-ASIA-HF (NCT01922479).� AFFIRM-AHF (NCT02937454).� FAIR-HF2 (NCT03036462) (AHF stabilized
planned to discharge within 24 h).
� Tools to diagnose meaningful ID are not clearlydefined in acute HF settings.
� Functional ID has not been found to be correlatedwith worse prognosis in acute HF (21).
Ambulatory chronic HFroutine evaluation
� Robust available evidence supporting symp-tomatic improvement.
� Safety and efficacy beyond 1 year is awaited:� HEART-FID: (NCT03037931).� FAIR-HF2 (NCT03036462) (stable ambulatory
chronic HF).� ID as a therapeutic target in HF with preserved
ejection fraction will be assessed in the FAIR-HFpEF (LVEF $45%) trial (NCT03074591).
� Unstructured intervention usually every3–12 months.
� May lack the adequate infrastructure and personnelfor routine IV iron administration.
HF day hospital � Opportunity to identify and treat ID in thepost-discharge vulnerable transition phase(concurrently with HF drug optimization).
� Possibility for a structured long-term IV ironfull-dosage plan (as required).
� Requires a rigorous post-discharge plan andmethodical schedule.
� Requires the infrastructure and personnel forroutine IV iron administration (or coordination withother hospital services).
� Expensive (although it may be arguablycost-effective).
AFFIRM-AHF ¼ Study to Compare Ferric Carboxymaltose With Placebo in Patients With Acute Heart Failure and Iron Deficiency; FAIR-HFpEF ¼ Effect of IV Iron in Patients WithHeart Failure With Preserved Ejection Fraction; HEART-FD ¼ Randomized Placebo-controlled Trial of FCM as Treatment for Heart Failure With Iron Deficiency; IRONOUTHF ¼ Oral Iron Repletion Effects On Oxygen Uptake in Heart Failure; PRACTICE-ASIA-HF ¼ Pilot Study of Ferric Carboxymaltose to Treat Iron Deficiency in Asians With HeartFailure; other abbreviations as in Table 2.
J A C C V O L . 7 1 , N O . 7 , 2 0 1 8 Rocha et al.F E B R U A R Y 2 0 , 2 0 1 8 : 7 8 2 – 9 3 Iron Deficiency in Heart Failure
791
CONCLUSIONS
Future investigations are eagerly awaited.Currently, the potential benefits of IV iron in AHF,asymptomatic and advanced chronic HF, as well asHF with preserved ejection fraction are unknown.The efficacy and safety of this therapy in patientswith hemoglobin >15 g/dl and/or a broader IDdefinition, as well as of repeated doses over alonger follow-up interval (>1 year), are unexplored.Gaps in evidence also include a poorly understoodpathophysiology of impaired iron metabolism in HF,whether patients should be routinely screened forsecondary causes of isolated ID (i.e., in the absence
of anemia), and how often iron status should beassessed after IV iron.
ACKNOWLEDGMENT The final version of this workwould not be conceivable without the collaboration ofDr. Marta Melo, who invested considerable time andeffort in the review process and provided tirelesssupport during the writing of this paper. For this, theauthors are grateful.
ADDRESS FOR CORRESPONDENCE: Prof. Luiz F.Menezes Falcão, Hospital Santa Maria/CHLN, Lisbon,and the Faculty of Medicine, University of Lisbon,Avenida Professor Egas Moniz, 1649-028 Lisboa,Portugal. E-mail: [email protected].
RE F E RENCE S
1. Mosterd A, Hoes AW. Clinical epidemiology ofheart failure. Heart 2007;93:1137–46.
2. Christiansen MN, Køber L, Weeke P, et al.Age-specific trends in incidence, mortality,and comorbidities of heart failure inDenmark, 1995 to 2012. Circulation 2017;135:1214–23.
3. Rocha BM, Menezes Falcão L. Acute decom-pensated heart failure (ADHF): a comprehensivecontemporary review on preventing early read-missions and postdischarge death. Int J Cardiol2016;223:1035–44.
4. Dokainish H, Teo K, Zhu J, et al. Global mor-tality variations in patients with heart failure:
results from the International Congestive HeartFailure (INTER-CHF) prospective cohort study.Lancet Glob Health 2017;5:e665–72.
5. Ponikowski P, Voors AA, Anker SD, et al. 2016ESC guidelines for the diagnosis and treatment ofacute and chronic heart failure: the Task Force forthe Diagnosis and Treatment of Acute and Chronic

Rocha et al. J A C C V O L . 7 1 , N O . 7 , 2 0 1 8
Iron Deficiency in Heart Failure F E B R U A R Y 2 0 , 2 0 1 8 : 7 8 2 – 9 3
792
Heart Failure of the European Society of Cardiol-ogy (ESC). Eur Heart J 2016;37:2129–200.
6. Yancy CW, Jessup M, Bozkurt B, et al. 2017ACC/AHA/HFSA focused update of the 2013 ACCF/AHA Guideline for the Management of HeartFailure: A Report of the American College of Car-diology/American Heart Association Task Force onClinical Practice Guidelines and the Heart FailureSociety of America. J Am Coll Cardiol 2017;70:776–803.
7. Wish JB. Assessing iron status: beyond serumferritin and transferrin saturation. Clin J Am SocNephrol 2006;1 Suppl 1:S4–8.
8. Kalantar-Zadeh K, Lee GH. The fascinating butdeceptive ferritin: to measure it or not to measureit in chronic kidney disease? Clin J Am Soc Nephrol2006;1 Suppl 1:S9–18.
9. Chapter 2: Use of iron to treat anemia in CKD.Kidney Int Suppl (2011) 2012;2:292–8.
10. Nanas JN, Matsouka C, Karageorgopoulos D,et al. Etiology of anemia in patients with advancedheart failure. J Am Coll Cardiol 2006;48:2485–9.
11. Van Aelst LNL, Abraham M, Sadoune M, et al.Iron status and inflammatory biomarkers in pa-tients with acutely decompensated heart failure:early in-hospital phase and 30-day follow-up. EurJ Heart Fail 2017;19:1075–6.
12. Leszek P, Sochanowicz B, Szperl M, et al.Myocardial iron homeostasis in advanced chronicheart failure patients. Int J Cardiol 2012;159:47–52.
13. Enjuanes C, Bruguera J, Grau M, et al. Ironstatus in chronic heart failure: impact on symp-toms, functional class and submaximal exercisecapacity. Rev Esp Cardiol (Engl Ed) 2016;69:247–55.
14. Jankowska EA, Kasztura M, Sokolski M, et al.Iron deficiency defined as depleted iron storesaccompanied by unmet cellular iron requirementsidentifies patients at the highest risk of death afteran episode of acute heart failure. Eur Heart J 2014;35:2468–76.
15. Jankowska EA, Rozentryt P, Witkowska A,et al. Iron deficiency: an ominous sign in patientswith systolic chronic heart failure. Eur Heart J2010;31:1872–80.
16. Klip IT, Comin-Colet J, Voors AA, et al. Irondeficiency in chronic heart failure: an internationalpooled analysis. Am Heart J 2013;165:575–82.e573.
17. Tkaczyszyn M, Comín-Colet J, Voors AA, et al.Iron deficiency and red cell indices in patients withheart failure. Eur J Heart Fail 2017 Apr 6 [E-pubahead of print].
18. Wienbergen H, Pfister O, Hochadel M, et al.Usefulness of iron deficiency correction in man-agement of patients with heart failure [from theRegistry Analysis of Iron Deficiency-Heart Failure(RAID-HF) Registry]. Am J Cardiol 2016;118:1875–80.
19. von Haehling S, Gremmler U, Krumm M, et al.Prevalence and clinical impact of iron deficiencyand anaemia among outpatients with chronic heartfailure: The PrEP Registry. Clin Res Cardiol 2017;106:436–43.
20. Enjuanes C, Klip IT, Bruguera J, et al. Irondeficiency and health-related quality of life inchronic heart failure: results from a multicenterEuropean study. Int J Cardiol 2014;174:268–75.
21. Núñez J, Comín-Colet J, Miñana G, et al. Irondeficiency and risk of early readmission following ahospitalization for acute heart failure. Eur J HeartFail 2016;18:798–802.
22. Cohen-Solal A, Damy T, Terbah M, et al. Highprevalence of iron deficiency in patients with acutedecompensated heart failure. Eur J Heart Fail2014;16:984–91.
23. Levi S, Rovida E. The role of iron in mito-chondrial function. Biochim Biophys Acta 2009;1790:629–36.
24. Jankowska EA, von Haehling S, Anker SD,Macdougall IC, Ponikowski P. Iron deficiency andheart failure: diagnostic dilemmas and therapeuticperspectives. Eur Heart J 2013;34:816–26.
25. Melenovsky V, Petrak J, Mracek T, et al.Myocardial iron content and mitochondrial func-tion in human heart failure: a direct tissue analysis.Eur J Heart Fail 2017;19:522–30.
26. Wilson JR, Fink L, Maris J, et al. Evaluation ofenergy metabolism in skeletal muscle of patientswith heart failure with gated phosphorus-31 nu-clear magnetic resonance. Circulation 1985;71:57–62.
27. Martens P, Verbrugge FH, Nijst P, Dupont M,Mullens W. Limited contractile reserve contributesto poor peak exercise capacity in iron-deficientheart failure. Eur J Heart Fail 2017 Sep 18 [E-pubahead of print].
28. Dai DF, Johnson SC, Villarin JJ, et al. Mito-chondrial oxidative stress mediates angiotensin II-induced cardiac hypertrophy and Galphaqoverexpression-induced heart failure. Circ Res2011;108:837–46.
29. Maeder MT, Khammy O, dos Remedios C,Kaye DM. Myocardial and systemic iron depletionin heart failure implications for anemia accompa-nying heart failure. J Am Coll Cardiol 2011;58:474–80.
30. Triposkiadis F, Karayannis G, Giamouzis G,Skoularigis J, Louridas G, Butler J. The sympa-thetic nervous system in heart failure physiology,pathophysiology, and clinical implications. J AmColl Cardiol 2009;54:1747–62.
31. Patel VB, Zhong JC, Grant MB, Oudit GY. Roleof the ACE2/angiotensin 1-7 axis of the renin-angiotensin system in heart failure. Circ Res2016;118:1313–26.
32. Patel AR, Kramer CM. Role of cardiac magneticresonance in the diagnosis and prognosis of non-ischemic cardiomyopathy. J Am Coll Cardiol Img2017;10 Pt A:1180–93.
33. Nagao M, Matsuo Y, Kamitani T, et al. Quan-tification of myocardial iron deficiency in non-ischemic heart failure by cardiac T2* magneticresonance imaging. Am J Cardiol 2014;113:1024–30.
34. Núñez J, Monmeneu JV, Mollar A, et al. Leftventricular ejection fraction recovery in patientswith heart failure treated with intravenous iron: apilot study. ESC Heart Fail 2016;3:293–8.
35. Jankowska EA, Malyszko J, Ardehali H, et al.Iron status in patients with chronic heart failure.Eur Heart J 2013;34:827–34.
36. Okonko DO, Mandal AK, Missouris CG, Poole-Wilson PA. Disordered iron homeostasis in chronicheart failure: prevalence, predictors, and relationto anemia, exercise capacity, and survival. J AmColl Cardiol 2011;58:1241–51.
37. Xu W, Barrientos T, Mao L, Rockman HA,Sauve AA, Andrews NC. Lethal cardiomyopathy inmice lacking transferrin receptor in the heart. CellRep 2015;13:533–45.
38. Ebner N, Jankowska EA, Ponikowski P, et al.The impact of iron deficiency and anaemia on ex-ercise capacity and outcomes in patients withchronic heart failure. Results from the StudiesInvestigating Co-morbidities Aggravating HeartFailure. Int J Cardiol 2016;205:6–12.
39. Jankowska EA, Rozentryt P, Witkowska A,et al. Iron deficiency predicts impaired exercisecapacity in patients with systolic chronic heartfailure. J Card Fail 2011;17:899–906.
40. Cooper TJ, Anker SD, Comin-Colet J, et al.Relation of longitudinal changes in quality of lifeassessments to changes in functional capacity inpatients with heart failure with and without ane-mia. Am J Cardiol 2016;117:1482–7.
41. Lewis GD, Malhotra R, Hernandez AF, et al.Effect of oral iron repletion on exercise capacity inpatients with heart failure with reduced ejectionfraction and iron deficiency: the IRONOUT HFrandomized clinical trial. JAMA 2017;317:1958–66.
42. Bregman DB, Morris D, Koch TA, He A,Goodnough LT. Hepcidin levels predict non-responsiveness to oral iron therapy in patientswith iron deficiency anemia. Am J Hematol 2013;88:97–101.
43. McDonagh T, Macdougall IC. Iron therapy forthe treatment of iron deficiency in chronic heartfailure: intravenous or oral? Eur J Heart Fail 2015;17:248–62.
44. Moore RA, Gaskell H, Rose P, Allan J. Meta-analysis of efficacy and safety of intravenous ferriccarboxymaltose (Ferinject) from clinical trial re-ports and published trial data. BMC Blood Disord2011;11:4.
45. Anker SD, Comin Colet J, Filippatos G, et al.Ferric carboxymaltose in patients with heart fail-ure and iron deficiency. N Engl J Med 2009;361:2436–48.
46. Niehaus ED, Malhotra R, Cocca-Spofford D,Semigran M, Lewis GD. Repletion of iron storeswith the use of oral iron supplementation in pa-tients with systolic heart failure. J Card Fail 2015;21:694–7.
47. Pisani A, Riccio E, Sabbatini M, Andreucci M,Del Rio A, Visciano B. Effect of oral liposomal ironversus intravenous iron for treatment of irondeficiency anaemia in CKD patients: a randomizedtrial. Nephrol Dial Transplant 2015;30:645–52.
48. Toblli JE, Lombraña A, Duarte P, Di Gennaro F.Intravenous iron reduces NT-pro-brain natriureticpeptide in anemic patients with chronic heartfailure and renal insufficiency. J Am Coll Cardiol2007;50:1657–65.

J A C C V O L . 7 1 , N O . 7 , 2 0 1 8 Rocha et al.F E B R U A R Y 2 0 , 2 0 1 8 : 7 8 2 – 9 3 Iron Deficiency in Heart Failure
793
49. Toblli JE, Di Gennaro F, Rivas C. Changes inechocardiographic parameters in iron deficiencypatients with heart failure and chronic kidneydisease treated with intravenous iron. Heart LungCirc 2015;24:686–95.
50. Okonko DO, Grzeslo A, Witkowski T, et al.Effect of intravenous iron sucrose on exercisetolerance in anemic and nonanemic patients withsymptomatic chronic heart failure and iron defi-ciency FERRIC-HF: a randomized, controlled,observer-blinded trial. J Am Coll Cardiol 2008;51:103–12.
51. Beck-da-Silva L, Piardi D, Soder S, et al. IRON-HF study: a randomized trial to assess the effectsof iron in heart failure patients with anemia. Int JCardiol 2013;168:3439–42.
52. Ponikowski P, van Veldhuisen DJ, Comin-Colet J, et al. Beneficial effects of long-termintravenous iron therapy with ferric carbox-ymaltose in patients with symptomatic heart fail-ure and iron deficiency. Eur Heart J 2015;36:657–68.
53. van Veldhuisen DJ, Ponikowski P, van derMeer P, et al. Effect of ferric carboxymaltose onexercise capacity in patients with chronic heartfailure and iron deficiency. Circulation 2017;136:1374–83.
54. Anker SD, Kirwan BA, van Veldhuisen DJ, et al.Effects of ferric carboxymaltose on hospital-isations and mortality rates in iron-deficient heart
failure patients: an individual patient data meta-analysis. Eur J Heart Fail 2017 Apr 24 [E-pubahead of print].
55. Jankowska EA, Tkaczyszyn M, Suchocki T,et al. Effects of intravenous iron therapy in iron-deficient patients with systolic heart failure: ameta-analysis of randomized controlled trials. EurJ Heart Fail 2016;18:786–95.
56. Keating GM. Ferric carboxymaltose: a reviewof its use in iron deficiency. Drugs 2015;75:101–27.
57. Avni T, Bieber A, Grossman A, Green H,Leibovici L, Gafter-Gvili A. The safety of intrave-nous iron preparations: systematic review andmeta-analysis. Mayo Clin Proc 2015;90:12–23.
58. Roger SD, Gaillard CA, Bock AH, et al. Safetyof intravenous ferric carboxymaltose versus oraliron in patients with nondialysis-dependent CKD:an analysis of the 1-year FIND-CKD trial. NephrolDial Transplant 2017;32:1530–9.
59. Gutzwiller FS, SchwenkglenksM,BlankPR, et al.Health economic assessment of ferric carbox-ymaltose in patientswith iron deficiency and chronicheart failure based on the FAIR-HF trial: an analysisfor the UK. Eur J Heart Fail 2012;14:782–90.
60. Theidel U, Väätäinen S, Martikainen J, Soini E,Hardt T, Doehner W. Budget impact of intravenousiron therapy with ferric carboxymaltose in patientswith chronic heart failure and iron deficiency inGermany. ESC Heart Fail 2017;4:274–81.
61. Brock E, Braunhofer P, Troxler J,Schneider H. Budget impact of parenteral irontreatment of iron deficiency: methodological is-sues raised by using real-life data. Eur J HealthEcon 2014;15:907–16.
62. Drozd M, Jankowska EA, Banasiak W,Ponikowski P. Iron therapy in patients with heartfailure and iron deficiency: review of iron prepa-rations for practitioners. Am J Cardiovasc Drugs2017;17:183–201.
63. Kalra PA, Bock K, Meldal M. Iron isomaltoside1000: a new high dose option for parenteral irontherapy. Port J Nephrol Hypert 2012;26:13–24.
64. Goddard AF, James MW, McIntyre AS,Scott BB, for the British Society of Gastroenter-ology. Guidelines for the management of irondeficiency anaemia. Gut 2011;60:1309–16.
65. Levy I, Gralnek IM. Complications of diagnosticcolonoscopy, upper endoscopy, and enteroscopy.Best Pract Res Clin Gastroenterol 2016;30:705–18.
66. Moliner P, Jankowska EA, van Veldhuisen DJ,et al. Clinical correlates and prognostic impact ofimpaired iron storage versus impaired iron trans-port in an international cohort of 1821 patientswith chronic heart failure. Int J Cardiol 2017;243:360–6.
KEY WORDS ferric carboxymaltose,heart failure, iron deficiency