Upload
others
View
7
Download
0
Embed Size (px)
Citation preview
537
Reference to apparently unhealthy lifestyles in modernsociety is now common in popular and academic media.Contemporary diseases and conditions most often men-tioned as having an association with physical inactivityinclude obesity, diabetes, heart disease, and some cancers.Indeed, obesity seems to be the health issue most worry-ing politicians and health professionals, and lack of physi-cal activity is a key element of the energy imbalance thatis causing current obesity trends (Bouchard, 2000;Bouchard & Blair, 1999). However, the beneficial effectsof physical activity go far beyond healthy weight manage-ment. The magic pill of physical activity is powerful, witheffects demonstrated on numerous health outcomes,including positive mental health (Dishman, Washburn, &Heath, 2004). Indeed, physical activity research pioneerProfessor Jeremy Morris (1994, p. 807) once referred tophysical activity as “ today’s best buy for public health,”and we now have strong advocacy documents promotingthe importance of regular, moderate-intensity physicalactivity on most days of the week (Department of Health,2004; U.S. Department of Health and Human Services &Centers for Disease Control and Prevention, 1996; Pateet al., 1995). In addition, recommendations can be tailoredto individual needs, such as those of young people, adults,older adults, and those with certain medical conditions(Department of Health, 2004).
The five-phase behavioral epidemiology frameworkadvocated by Sallis and Owen (1999) is a useful way ofviewing various processes in the understanding of physi-cal activity and health. Behavioral epidemiology consid-ers the link between behaviors, health, and disease, suchas why some people are physically active and others arenot. In relation to physical activity, this framework has
five main phases. The first is to establish the link betweenphysical activity and health. The second phase is to devel-op methods for the accurate assessment of physical activ-ity. The third phase is to identify factors that areassociated with different levels of physical activity. Giventhe evidence supporting the beneficial effects of physicalactivity on health, it is important to identify factors thatmight be associated with the adoption and maintenance ofthe behavior. This area is referred to as the study of cor-relates or determinants of physical activity. The fourthphase is to evaluate interventions designed to promotephysical activity, and the fifth is to translate findingsfrom research into practice.
In this chapter, we focus on theoretical frameworks andperspectives that assist in the understanding of determi-nants and correlates of physical activity, thus addressingissues in phase 3 of the behavioral epidemiological frame-work. A theory is “a set of interrelated constructs (con-cepts), definitions, and propositions that present asystematic view of phenomena by specifying relationsamong variables, with the purpose of explaining and pre-dicting phenomena” (Kerlinger, 1973, p. 9). Physical activ-ity behavior researchers have adopted theories and modelsfrom general, social, educational, and health psychology(Sutton, 2004) and tested and applied them in the contextof physical activity. Given the emphasis of this book onpsychology, we, too, adopt an individual psychologicalapproach to understanding physical activity. However, werecognize the importance of a wider set of influences,including the broader social, environmental, and culturalcontext of behaviors (Sallis & Owen, 1999).
To assist in the organization of diverse theories, we haveplaced key theoretical frameworks into a classification
CHAPTER 24
Theoretical Frameworks in Exercise Psychology
STUART J. H. BIDDLE, MARTIN S. HAGGER, NIKOS L. D. CHATZISARANTIS, and SONIA LIPPKE
ClaudioText BoxBiddle, S. J. H., Hagger, M. S., Chatzisarantis, N. L. D., & Lippke, S. (2007). Theoretical frameworks in exercise psychology. In G. Tenenbaum & R. Eklund (Eds.), Handbook of sport psychology (3rd ed., pp. 537-559). Hoboken, NJ: Wiley.
538 Exercise and Health Psychology
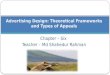
Figure 24.1 A framework for classifying theories of physical activity. Adapted from S. J. H. Biddle and C. R. Nigg, 2000, “Theo-ries of Exercise Behavior,” International Journal of Sport Psychology, 31, pp. 290–304. Adapted with permission.
Theories ofexercise behavior
Belief-attitudetheories
Competence-basedtheories
Control-basedtheories
Stage-basedtheories
Hybridmodels
Example:Theory of
planned behavior
Example:Self-efficacy
theory
Example:Self-determination
theory
Example:Transtheoretical
model
Example:HAPA
system (Biddle & Nigg, 2000), as shown in Figure 24.1.Such a system is a heuristic, and there will be overlapbetween categories, as we discuss later concerning imple-mentation intentions. Moreover, part of the classificationmay reflect different types of theories, such as continuousapproaches like the theory of planned behavior, and stagemodels that assume discontinuity between the differentstages, at least for some variables. In addition, Armitageand Conner (2000) have made the distinction betweenmotivational and behavioral enaction models. The former,such as the theory of planned behavior, tend to predictbehavior from a series of variables. The key variable isintention or motivation that mostly mediates the influencesof predictors on behavior. Behavioral enaction models, onthe other hand, focus on the translation of intentions intobehavior by postintentional variables, such as implementa-tion intentions (discussed later).
Throughout the chapter we refer to physical activityin the context of sport, exercise, and physical activityfor health rather than high performance, some of themodels and frameworks may be appropriate beyond thiscontext.
BELIEF-ATTITUDE APPROACHES
Attitude has been one of the most influential and enduringconstructs in social psychology and has been incorporated
into many theoretical approaches adopted for the under-standing of physical activity behavior (Hagger, Chatzis-arantis, & Biddle, 2002b). The fascination of attitudes insocial psychology has been largely due to the premise thatattitudes predict behavior (Wicker, 1969). However, stud-ies have often reported a considerable gap in the attitude-behavior relationship (Chatzisarantis, Hagger, Biddle, &Smith, 2005; Sheeran, 2002). Social cognitive theoriesdeveloped in the past 2 decades or so have done much toresolve this disparity, and contemporary theories incorpo-rate attitude alongside measures of other fundamentalbelief-based constructs in an attempt to understand themechanisms underlying social behavior such as physicalactivity (Hagger & Chatzisarantis, 2005a). A briefoverview of attitudes as an important theoretical constructin the context of physical activity is presented in this sec-tion, with a focus on the theories of reasoned action andplanned behavior (Ajzen, 1985, 1991; Ajzen & Fishbein,1980) as an example of a popular social cognitive approachthat has adopted attitude and belief-based constructs tostudy physical activity.
Attitude is commonly defined as an individual’s favor-able or unfavorable evaluation of an attitude object or tar-get behavior (Ajzen, 1991; Eagly & Chaiken, 1993).Attitudes have typically been measured with semanticdifferential scales using bipolar word adjectives (Ajzen,2001). These scales have often been validated using
Theoretical Frameworks in Exercise Psychology 539
exploratory factor-analytic procedures to arrive at multi-item scales that capture the essence of the person’s beliefsregarding the target behavior. In the domain of physicalactivity, the adjectives that have been most frequentlyused to measure attitudes reflect moral (e.g., good-bad),instrumental (e.g., harmful-beneficial), and affective(e.g., pleasant-unpleasant) beliefs about the target behav-ior (Ajzen & Driver, 1991). Such measures are known asdirect measures of attitudes because they focus on atti-tudes at the global level rather than the beliefs that under-pin the construct.
The use of semantic differential attitude scales can beproblematic because their use may be susceptible tomethod and context effects. Method effects describeresponses to attitude items that are triggered by similari-ties in the method used to measure attitudes rather than bythe content of the items (Mulaik & Millsap, 2000). Contextor order effects refer to biases in responses to attitudeitems caused by responses to previously presented items(Ajzen, 2002). For example, the presentation of an affec-tive attitude item to which a person responds positivelymay affect his or her response to an instrumental attitudeitem presented subsequently. In fact, this often occurs inattitude research in physical activity involving the adminis-tration of multi-item attitude inventories.
Problems associated with context and method effectscan be overcome by constructing a large set of belief state-ments that are relevant to physical activity and then askingpeople to rate these statements on Likert-type scales(Ajzen, 2002). Responses to these belief statements consti-tute an indirect or belief-based measure because attitudesare inferred from the beliefs themselves (Fishbein &Ajzen, 1975). Another popular conceptualization of atti-tudes that has been used in physical activity studies is theexpectancy-value model (Fishbein & Ajzen, 1975; Pender& Pender, 1986; Riddle, 1980). This model also constitutesan indirect measure of attitudes. It posits that a combina-tion or multiplicative function of beliefs that behavior willlead to certain consequences, known as behavioral beliefs,and evaluations of these consequences, known as outcomeevaluations, are indicators of attitudes. Expectancy-valuemeasure of attitudes can be formulated by asking respon-dents to rate available behavioral beliefs on expectancyscales (e.g., “Engaging in physical activities will make mefitter”) and then multiplying each of the likelihood ratingswith ratings of the desirability of behavioral beliefs (e.g.,“Getting fitter is good/bad”). Such indirect measures ofattitude are often used in social cognitive theories tovalidate the direct measures by correlating the composite
expectancy-value items with the direct measures (Hagger,Chatzisarantis, & Biddle, 2001).
The Theory of Reasoned Action
The theory of reasoned action (TRA; Ajzen & Fishbein,1980) is a popular and widely cited social cognitive modelthat incorporates attitudes in a belief-based frameworkaimed at explaining behavioral intentions, the proximalprecursor of actual behavior. It preceded the more com-monly studied model in contemporary literature, the theo-ry of planned behavior. In the TRA, intention indicates thedegree of planning and effort people are willing to invest intheir performance of future behavior. It is therefore a con-struct that is motivational in nature and function. Intentionis the most immediate or proximal antecedent of behaviorand is a function of a set of personal and normative expec-tations regarding the performance of the behavior, termedattitudes and subjective norms, respectively. Attitudes rep-resent an overall positive or negative evaluation toward thetarget behavior and have a dominant role in the formationof intentions. Subjective norms are defined as the per-ceived influences that significant others may exert on theexecution of behavior. Generally speaking, the TRA pre-dicts that the more favorable an individual’s attitude andsubjective norm, the stronger his or her intentions to per-form the behavior. Finally, intentions are hypothesized tolead directly to behavioral engagement and are proposed tomediate the effects of attitudes and subjective norms onbehavior. This means that intentions explain the attitude-behavior and subjective norm-behavior relationships.Intentions are therefore necessary to convert attitudes andsubjective norms into behavior.
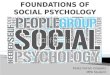
Expectancy-value models of behavioral beliefs and out-come evaluations, identical to those outlined previously, arethought to be the antecedents of attitudes (Ajzen & Fish-bein, 1980). Similarly, the origins of subjective norms canbe traced to belief-based judgments that include normativebeliefs and motivation to comply. Normative beliefs refer tobehavioral expectations that important referent individuals(or groups) approve or disapprove of performing the behav-ior. Motivation to comply is the actor’s general tendency togo along with the wishes of the salient referents (Ajzen &Fishbein, 1980). These constitute indirect measures of atti-tude and subjective norms, respectively, and are expectedto correlate with the direct measures of these constructs(Hagger, Chatzisarantis, & Biddle, 2001). The TRA isshown in Figure 24.2.
The major hypotheses of the TRA have been supportedin numerous studies across a number of different behaviors
540 Exercise and Health Psychology
Figure 24.2 The theories of reasoned action and plannedbehavior. Note: Constructs and relationships above the brokenline represent the theory of reasoned action, and constructsabove and below the broken line taken together represent the the-ory of planned behavior.
Behavioralbeliefs xvalues
Attitudes
Subjectivenorms Intentions Behavior
Perceivedbehavioral
control
Controlbeliefs xpower
Normativebeliefs x
compliance
(Sheppard, Hartwick, & Warshaw, 1988), including exer-cise (Hagger et al., 2002b) and sports training (Theodor-akis, Goudas, Bagiatis, & Doganis, 1993). In the exercisedomain, tests of the theory have provided strong evidencefor the overall predictive value of intentions and haveshown that attitudes have a pervasive effect on intentions.A lesser role has been observed for subjective norms (Hag-ger et al., 2002b). In addition, panel studies have indicatedthat the strong effects of attitudes on intentions remain sta-ble over time (Chatzisarantis & Hagger, in press; Hagger,Chatzisarantis, Biddle, & Orbell, 2001).
Applications of the theory have also revealed thesalient behavioral and normative beliefs related to physi-cal activity. The beliefs are typically elicited from open-ended questionnaires administered to a pilot sample andare used to develop belief-based measures of the attitudeand subjective norm constructs (Ajzen & Fishbein, 1980).Behavioral beliefs identified in this research include“good companionship,” “weight control,” “benefit myoverall health,” “ take too much time,” “fun,” “get fit,”“stay in shape,” “improve skills,” “get an injury,” and“makes you hot and sweaty” (Hagger, Chatzisarantis,Biddle, et al., 2001). Important referents for measures ofnormative beliefs and motivation to comply tend to befamily members, such as parents, grandparents, and sib-lings, along with friends and schoolteachers (Hagger,Chatzisarantis, Biddle, et al., 2001). However, thesebeliefs have not been shown to unequivocally account forunique variance in the directly measured attitude and sub-jective norm constructs, and alternative subsets of beliefsmay exist (Hagger, Chatzisarantis, Biddle, et al., 2001).
The TRA has not been without critics. It is a unidirec-tional model and so fails to offer the possibility that vari-ables in the model can act in a reciprocal manner. Inaddition, the model relies solely on cognitions and omitsother potentially important determinants of action, such asenvironmental influences, and it usually predicts behaviorfrom measures of behavioral intention taken at one point intime. Moreover, insufficient attention has been paid to themeasurement of behavior within the TRA. Without anaccurate measure of the behavior, the principle of corre-spondence cannot be applied. This casts some doubt on sev-eral studies, such as when assessment relies on unvalidatedself-reports or inappropriate “objective” measures (e.g.,use of pedometers for people who are physically active pre-dominantly through cycling or swimming). Finally, theTRA allows the investigation of the interrelationshipsamong attitudes, subjective norms, intentions, and a singlebehavior. It does not account for alternative behaviors. Forexample, although many people intend to be more physical-ly active, few see this through to action in a sustained way.This could be due to physical activity being of lower prior-ity than other behaviors, and so just does not get to the topof the list of things to do.
In summary, the TRA has been at the forefront ofreestablishing attitude research as a powerful force insocial psychology, and both health and exercise psychologyhave been quick to utilize such an approach. The TRA hasproved to be a viable unifying theoretical framework thathas been successful in furthering understanding of exerciseintentions and behaviors. It has also been instrumental inmoving research on physical activity correlates from beinglargely atheoretical to theoretical.
The Theory of Planned Behavior
Although the TRA has been successful in predicting andexplaining participation in physical activities, a major lim-itation of the theory noted by Ajzen (1985) is that not allbehaviors are under volitional control. This led to Ajzen topropose an alternative theory, the theory of plannedbehavior (TPB), to resolve this limitation. As with the the-ory of reasoned action, it is proposed in the theory ofplanned behavior that intention is a central determinant ofsocial behavior and a function of attitudes and subjectivenorms with corresponding behavioral beliefs and norma-tive beliefs, respectively. However, it is also proposed inthe TPB that when perceived control over behavior is prob-lematic, an additional factor, termed perceived behavioralcontrol (PBC), can inf luence intention and behavior(Ajzen, 1985).
Theoretical Frameworks in Exercise Psychology 541
For Ajzen (1991), the PBC construct refers to generalperceptions of control (see competence-based approaches inthe next section). He overtly compared it with Bandura’s(1977) construct of self-efficacy that captures judgments ofhow well one can execute volitional behaviors required toproduce important outcomes. The construct of PBC is alsounderpinned by a set of control beliefs and the perceivedpower of these beliefs (Ajzen & Fishbein, 1980). Controlbeliefs refer to the perceived presence of factors that mayfacilitate or impede performance of behavior, and per-ceived power refers to the perceived impact that facilitativeor inhibiting factors may have on performance of behavior(Ajzen, 1991). In the same way that an expectancy-valuemodel is used to form indirect antecedents of attitudes andsubjective norm, an indirect measure of PBC can be formedfrom the multiplicative composite of each control beliefmultiplied by its corresponding perceived power rating(Ajzen, 1991).
The inclusion of perceived behavioral control in theTPB is important because it reveals the personal and envi-ronmental factors that affect behavior (Ajzen, 1985). Tothe extent that PBC influences intentions and behavior, theresearcher can evaluate which behaviors are under thevolitional control of the individual and the degree to whichthe behavior is impeded by personal and/or environmentalfactors. Ajzen (1991) hypothesized that when control overthe behavior was problematic, PBC would exert two typesof effects. First, it would influence intentions alongsideattitudes and subjective norms; this additive effectreflects the motivational influence of perceived control ondecisions to exercise. Second, PBC may predict behaviordirectly, especially when perceptions of behavioral controlare realistic; this direct effect reflects the effect of actual,real constraints or barriers to doing the behavior. In thiscase, PBC is a proxy measure of actual control over thebehavior (Ajzen, 1991). These relationships are shown inFigure 24.2.
A number of studies have shown the TPB to be superiorto the TRA in predicting and explaining volitional behavioracross many settings (Armitage & Conner, 2001), includ-ing physical activity behavior (Dzewaltowski, Noble, &Shaw, 1990; Hagger et al., 2002b). In terms of the relativecontribution of the theory constructs, a number of studieshave shown that attitude and perceived behavioral controlpredict intentions equally well (Hagger & Chatzisarantis,2005a; Hagger, Chatzisarantis, & Biddle, 2002a). A num-ber of control beliefs have also been identified, includingbarriers and facilitating factors related to exercise, suchas “bad weather,” “age,” “heart pain,” “costs,” “fatigue,”
and “no time” (Godin, Valois, Jobin, & Ross, 1991; Hagger,Chatzisarantis, & Biddle, 2001). As with behavioral andnormative beliefs, control beliefs have been demonstratedto vary considerably across different populations andbehaviors. For example, “age” and “fear of having a heartattack” have been identified among the physical activitycontrol beliefs for older and clinical populations (Godinet al., 1991), but these beliefs do not feature among thecontrol beliefs of younger populations (Hagger, Chatzis-arantis, & Biddle, 2001).
We conducted a comprehensive synthesis of the extantTPB research in the physical activity domain (Haggeret al., 2002b). We meta-analyzed 72 studies that allowedcalculations of the relationships proposed in either theTRA or TPB. In addition to reporting correlations betweenvariables, we did three things:
1. By using the correlation matrix, we tested the TRA andTPB through path analysis.
2. We tested the additional variance accounted for byadding variables to the TRA. This was done by firstadding PBC (hence testing the TPB), then self-efficacy,and finally past behavior.
3. We tested three moderator variables: age, attitude-intention strength, and the time between the assessmentof past behavior and (present) behavior.
Results supported the TPB. Intention was the only directpredictor of behavior, intention was predicted more strong-ly by attitudes than by subjective norms (the latter showinga small contribution), and PBC was associated with behav-ior through intention. Self-efficacy (which some mightargue is a more internal or “personal” aspect of PBC)added to the prediction of both intentions and behavior, andpast behavior was associated with all TPB variables. Ofmost importance was the finding that by adding past behav-ior to the model, other paths were reduced, suggesting thatstudies that do not assess past behavior may be obtainingartificially high correlations. Nevertheless, the relation-ship between attitude and intentions remained even whenpast behavior was included. We concluded:
While past behavior had a significant and direct inf luence onintention, attitude, PBC, and self-efficacy, these cognitionsare also necessary for translating past decisions about behav-ioral involvement into action. This is consistent with thenotion that involvement in volitional behaviors such as regu-lar physical activity involves both conscious and automaticinfluences. (Hagger et al., 2002b, p. 23)
542 Exercise and Health Psychology
One problem with the TPB, in addition to some of thecriticisms given for the TRA, is the lack of consistency indefining and assessing perceived behavioral control. Forexample, Ajzen (1988) originally said that perceivedbehavioral control was “closely related to self-efficacybeliefs” (p. 106) and that it “refers to the perceived easeor difficulty of performing the behavior and it is assumedto reflect past experience as well as anticipated impedi-ments and obstacles” (p. 132). The similarity with self-efficacy has also been noted by Stroebe and Stroebe(1995). Ajzen (1991), however, defines perceived behav-ioral control in terms of both perceived resources andopportunities as well as perceived power to overcomeobstacles; thus, the construct represents both controlbeliefs and perceived power.
It is often found in studies incorporating self-efficacyand PBC that they make independent contributions to theprediction of intentions or behavior. For example, Terryand O’Leary (1995) found items reflecting self-efficacyand PBC to be factorially distinct. Moreover, they foundthat self-efficacy predicted intentions to be physicallyactive, but not activity itself, whereas PBC predicted phys-ical activity but not intention.
Reasons for the success and popularity of the TPB canbe attributed to its efficacy in accounting for variance inintention and behavior, its relative parsimony, and its f lex-ibility. Furthermore, the original constructs of the TPBhave been shown to mediate the direct effect of other con-structs on intentions and behavior, suggesting that thebelief systems that underpin the directly measured theoryconstructs are able to account for the effects of other vari-ables that have previously accounted for unique variance inbehavior (Conner & Abraham, 2001). However, researchershave also indicated that the theory does not account for allof the variance in intention and behavior, nor does it medi-ate the effects of certain “external variables” (Rhodes &Courneya, 2003), personality and belief-based constructson intentions and behavior (Bagozzi & Kimmel, 1995; Con-ner & Abraham, 2001; Conner & Armitage, 1998; Rhodes,Courneya, & Jones, 2002). Paradoxically, this weaknesshas become the theory’s greatest strength. Ajzen (1991)states that the theory should be viewed as a flexible frame-work into which other variables can be incorporated pro-vided they make a meaningful and unique contribution tothe prediction of intentions and there is a theoretical prece-dence for the inclusion of such variables.
As a consequence, the theory has demonstrated consid-erable flexibility and has been adopted by researchers as a
general framework to investigate the effect of a number ofadditional social cognitive constructs on intention andbehavior (Conner & Armitage, 1998). To the extent thatsuch constructs have a unique effect on intention or behav-ior and are not mediated by the core theory variables ofattitude, subjective norm, and PBC, the researcher has evi-dence to support the inclusion of that construct in the the-ory. A number of constructs have been found to have aunique effect on intentions and/or behavior in this regard,including anticipated affect and anticipated regret (Sheer-an & Orbell, 1999a), self-schemas (Sheeran & Orbell,2000), self-efficacy (Sparks, Guthrie, & Shepherd, 1997),descriptive norms (Sheeran & Orbell, 1999a), desires(Perugini & Bagozzi, 2001), and self-identity (Hagger &Chatzisarantis, in press; Sparks & Guthrie, 1998).
In addition to the effects of other constructs, the influ-ence of variations in the characteristics and nature of thecore theory of planned behavior constructs on intentions,and of intention itself, on behavior have been investigated(Sheeran, 2002). Examples include the stability of inten-tions (Sheeran, Orbell, & Trafimow, 1999), the accessibil-ity of attitudes (Verplanken, Hofstee, & Janssen, 1998),and hypothetical bias (Ajzen, Brown, & Carvahal, 2004).In the same vein, researchers have also investigated theextent to which individuals are oriented toward or basetheir intentions on each of the core theory constructs(Sheeran, Norman, & Orbell, 1999; Trafimow & Finlay,1996). These modifications suggest that the antecedents ofvolitional behaviors, such as physical activity, may be morecomplex than originally conceived in the theory (Conner &Armitage, 1998). Notwithstanding these modifications, thetheory still performs relatively well in terms of explainingphysical activity behavior, and in its most parsimoniousform can inform successful interventions to promote phys-ical activity (Chatzisarantis & Hagger, in press; Hagger &Chatzisarantis, 2005a).
Implementation Intentions
One reason the theories of reasoned action and plannedbehavior do not fully explain the processes by which inten-tions are translated into action is that people often fail tocarry out their intentions (Gollwitzer, 1999; Orbell, 2000;Orbell, Hodgkins, & Sheeran, 1997; Sheeran & Orbell,1999b). Alternatively, individuals’ execution of their inten-tions may be interrupted because other, competing goal-directed behaviors gain priority over the original intendedbehavior (Verplanken & Faes, 1999). Social cognitive the-ories like the theories of reasoned action and planned
Theoretical Frameworks in Exercise Psychology 543
behavior do not address these difficulties associated withenactment of intentions, and as a result may not fullyexplain the intention-behavior relationship.
One approach that has been put forward to resolve theinadequacies of the intention-behavior relationship in theTPB is implementation intentions (Gollwitzer, 1999).These are self-regulatory strategies that involve the for-mation of specific plans that specify when, how, andwhere performance of behavior will take place. Implemen-tation intentions were developed from concerns about theintention-behavior gap.
Experimental paradigms using implementation intentionstrategies require research participants to specify explicit-ly when, where, and how they will engage in an intendedbehavior to achieve their behavioral goals (Orbell, 2000).According to Gollwitzer (1999), implementation intentionshelp people move from a motivational phase to a volitionalphase, ensuring that intentions are converted into action.Research has indicated that forming implementation inten-tions decreases the probability of people failing to initiatetheir goal-directed intentions at the point of initiation(Orbell, 2000; Orbell et al., 1997; Sheeran & Orbell,1999b). This is because planning when and where to initi-ate a prospective action strengthens the mental associationbetween representations of situations and representationsof actions. Research has also shown that increased accessi-bility of situational representations in memory increasesthe probability of action opportunities getting noticed andof action initiation occurring, given that the mere percep-tion of action opportunities can automatically trigger abehavioral response (Orbell et al., 1997; Sheeran & Orbell,1999b). Of particular importance, implementation inten-tions increase behavioral engagement through these postde-cisional, automatic mechanisms, and not by concomitantincreases in motivation or intention (Orbell et al., 1997).
Recent research has evaluated the effectiveness of inter-ventions that combine motivational techniques with voli-tional techniques, such as implementation intentions, ininfluencing the performance of social and exercise behavior(Koestner, Lekes, Powers, & Chicoine, 2002; Milne, Orbell,& Sheeran, 2002; Prestwich, Lawton, & Conner, 2003;Sheeran & Silverman, 2003). The rationale behind thiscombined approach is that motivational strategies focus onincreasing intention levels but do not facilitate the enact-ment of intentions, and volitional strategies, such as imple-mentation intentions, increase the probability that thesestrong intentions will be converted into action withoutchanging intentions. Research has corroborated the utility
of these combined techniques in increasing exercise behav-ior. For example, Prestwich et al. demonstrated that anintervention that had a combination of a rational decision-making strategy, or decisional balance sheet (weighing upthe pros and cons), and implementation intentions wasmore effective in promoting physical activity behavior thaneither of the strategies alone. These results support theexistence of two distinct phases of motivation: a motiva-tional or predecisional phase, during which people decidewhether or not to perform a behavior, and a volitional, post-decisional, or implemental phase, during which people planwhen and where they will convert their intentions intobehavior (Gollwitzer, 1999). As a consequence, interven-tions that combine motivational and volitional techniquesare likely to be most effective in promoting physical activ-ity behavior.
COMPETENCE-BASED APPROACHES
The social-cognitive perspectives currently favored whenstudying individual motivation in the exercise psychologyliterature have drawn extensively on self-efficacy theory.This approach has had a large impact in both exercise(McAuley & Blissmer, 2000; McAuley, Pena, & Jerome,2001) and health (Stroebe & Stroebe, 1995) research.Other confidence- and competence-related perspectivesare achievement motivation (Roberts, 2001) and self-presentation (Leary, 1992). In addition, theories ofself-perceptions are relevant and will be discussed inbrief later.
Self-Efficacy Theory
Confidence has been identified at the anecdotal and empir-ical level as an important construct in exercise motivation.Statements associated with self-perceptions of confidenceare commonplace in studies on exercise and sport and arelikely to be associated, in one way or another, with the ini-tiation and maintenance of physical activity. Bandura(1986, p. 391) defines perceived self-efficacy as
people’s judgments of their capabilities to organize and exe-cute courses of action required to attain designated types ofperformances. It is concerned not with the skills one possess-es but rather, with judgments of what one can do with what-ever skills one possesses.
Beliefs related to the ability to carry out a particularbehavior are self-ef ficacy expectations, whereas beliefs as
544 Exercise and Health Psychology
to whether the behavior will produce a particular result areoutcome expectations. People are likely to be concernedabout both types of expectancy, and both require study inexercise psychology research. For example, it is importantto know whether efficacy expectations are influential inthe adoption of exercise programs, yet it is also likely thatoutcome expectations will affect the maintenance of suchprograms and the reinforcement necessary for continuedinvolvement.
It is thought that people gain or lose self-efficacy in fourmain ways (Bandura, 1986, 1997):
1. Prior success and performance attainment
2. Imitation and modeling, particularly of people similarto oneself
3. Verbal and social persuasion
4. Judgments of physiological states, such that states of re-laxation can be achieved
C. Ewart (1989, p. 684) summarized the application ofthese in the context of promoting exercise in a rehabilita-tion setting by saying that
the most effective way to encourage patients to adopt exer-cise activities for which they lack self-efficacy is to exposethem to the recommended activity in gradually increasingdoses [performance], arrange for them to see others similarto themselves performing the activity [modeling], haverespected health care providers offer encouragement by pro-viding reassurance and emphasizing the patient’s accom-plishments [persuasion], and arrange the setting of theactivity so as to induce a relaxed but “upbeat” mood [arous-al, physiological state].
Research Findings for Self-Efficacy in Exercise
Early work in this area tended to focus on patients, such asthose in cardiac rehabilitation. For example, C. E. Ewart,Taylor, Reese, and DeBusk (1983) studied self-efficacy inthe context of treadmill running with post-myocardialinfarction patients. Before and after treadmill exercise,assessment of self-efficacy to take part in walking, run-ning, stair climbing, sexual intercourse, lifting, and gener-al exertion was made. Results showed that positive changesin self-efficacy took place following treadmill exercise,and that this was greatest for running, suggesting that effi-cacy effects can generalize but appear to have strongereffects on similar exercise modes. When counseling alsotook place, it was found that efficacy perceptions for some
of the activities significantly increased above the levelattained after treadmill running. Studies on medicalpatients in exercise rehabilitation have suggested that self-efficacy judgments can generalize but will be strongest foractivities similar to the activity experienced, that self-efficacy in “dissimilar” activities can be enhanced throughcounseling, and that self-efficacy better predicts changesin exercise behavior than generalized expectancies of locusof control (Biddle & Mutrie, 2001).
A number of researchers have now investigated nonpa-tient groups in physical activity. For example, self-efficacyhas been shown to predict walking in a large adult samplecontacted by mail (Hofstetter et al., 1991), has discrimi-nated adherers from dropouts in an exercise weight lossprogram (Rodgers & Brawley, 1993), and has predictedpositive affect after exercise (Bozoian, Rejeski, &McAuley, 1994).
McAuley’s work on exercise self-efficacy has beeninfluential (e.g., McAuley, 1992; McAuley & Courneya,1993; McAuley & Mihalko, 1998). In particular, McAuleyand colleagues have studied self-efficacy responses ofolder adults, a population previously underrepresented inthe exercise psychology literature. Several studies byMcAuley and coworkers focus on a group of previouslysedentary 45- to 64-year-olds. These studies have shownthat for older adults, exercise self-efficacy:
• Can be increased through intervention
• Will predict participation, particularly in the earlystages of an exercise program
• Declines after a period of inactivity
• Is associated with positive exercise emotion
In summary, the studies investigating self-efficacy innonpatient exercise groups show a consistent relationshipbetween efficacy and exercise participation, as well asrelationships with other important factors, such as postex-ercise emotion.
Self-efficacy needs to be assessed in relation to specif-ic behaviors if increased magnitude of behavioral predic-tion is required. Generalized perceptions of confidence arenot the same as perceptions of efficacy. Nevertheless, weneed more studies on the generalizability of self-efficacyacross different physical activity and exercise settings.Similar to the attitude-behavior correspondence issue dis-cussed earlier, the utility of self-efficacy is likely to begreater when measures correspond closely to the behaviorin question, such as walking to work 4 days per week,rather than using a general reference such as “exercise.”
Theoretical Frameworks in Exercise Psychology 545
Assessing self-efficacy in any meaningful way requiresthe behavior to be associated with effort, potential barri-ers, and behavioral self-regulation. “Easy” habitual behav-iors, such as tooth brushing, are likely to be unrelated tofeelings of efficacy, whereas physical exercise may behighly associated with efficacy beliefs if exercise requiresplanning, effort, and the overcoming of considerable barri-ers. This is probably why self-efficacy emerges as one ofthe most consistent predictors of physical activity behav-iors, particularly when physical activity includes elementsof vigorous exercise.
Physical Self-Perceptions and Competence
Dominant theories of competence-based motivation ofteninvolve constructs related to self-perception, and thesehave been a central feature in the exercise psychology lit-erature. In contemporary self-esteem theory, it is proposedthat global self-esteem (how we view ourselves overall) isunderpinned by perceptions of specific domains of ourlives, such as social, academic, and physical domains(Shavelson, Hubner, & Stanton, 1976). Based on thisapproach, Fox (1997; Fox & Corbin, 1989) has developedan operational measure of physical self-perceptions where-by psychometrically sound scales assess the higher-orderconstruct of physical self-worth (PSW) and its self-perception subdomains of sport competence, perceivedstrength, physical condition, and attractive body. It is pro-posed that everyday events are likely to affect more spe-cific perceptions of self (e.g., the belief that one can walkto work), which, if reinforced over time, may eventuallycontribute to enhanced self-perceptions of physical condi-tion or even PSW. As such, self-perceptions can be viewedin terms of being more general in their orientation (i.e.,domain-general) when they operate at the level of generalself-perceptions of competence and worth, such as PSW.Self-perceptions can also be viewed in more specificterms, such as specific competency perceptions like “CanI finish this bike ride?” and “I have just walked to work forthe first time.”
At least two perspectives on competence perceptionsand motivation can be considered relative to Fox’s (1997)model of physical self-worth. The self-enhancement modelof self-esteem is where positive self-perceptions play amotivational role in behavior. For example, if I feel compe-tent in physical activity, it is more likely that I will want todemonstrate that competence, and hence be motivated tobe active. The reverse could also be true, whereby a lack ofmotivation through perceptions of incompetence becomesa determinant of sedentary habits. The personal develop-
ment model views self-esteem or physical self-perceptionsas outcomes of physical activity, such that positive out-comes will reinforce competence and boost self-perceptions, and negative outcomes will have the reverseeffect (Biddle & Mutrie, 2001).
CONTROL-BASED THEORIES
The research and lay literatures contain numerous refer-ences to the fact that changes in physical activity behaviorsare thought to be associated with the need for personal con-trol of our lifestyles. The information that many of themodern diseases linked with premature mortality arelifestyle-related has the implicit message that we, as indi-viduals, are at least partly responsible for our health andwell-being, thus implying the need for personal control andchange. However, it could be argued that a greater empha-sis should be placed on social determinants of health.Whatever the outcome of such a debate, it is clear that per-ceptions of control are important psychological correlatesof health-related behavior at the individual level.
Definitions of Control and Autonomy
The construct of control is one of the most popular and oft-cited in the social psychology literature (Skinner, 1995,1996). Its popularity stems primarily from the fact thatmany theories of human motivation either make a refer-ence to control or explicitly include a construct of controlin their proposed models (Biddle, 1999). Corresponding tothe popularity of the construct of control has been the pro-liferation of terms and confusion of theoretical definitionsused to describe this construct. According to Skinner(1995) and Biddle (1999), the construct of control has beenused in the literature in three different ways.
First, the term control has been used to describe beliefsthat one has the capacity to control performance of themeans (i.e., behaviors) leading to outcomes. These controlbeliefs, which are termed “capacity beliefs” (Skinner,1995), are similar to Bandura’s (1997) self-efficacybeliefs. Second, the construct of control has been used todescribe beliefs (strategy beliefs) concerning the necessaryavailability of means to produce the desired outcome.Third, the construct of control has been used to describebeliefs (control beliefs) that an agent (person) has thecapacity to produce a desirable outcome. These controlbeliefs are very similar to White’s (1963) and Deci andRyan’s (1985) definition of the need for competence,which refers to the need that one has the capacity to pro-duce outcomes and also understand the instrumentalities
546 Exercise and Health Psychology
leading to these outcomes. In fact, because Skinner’s andWhite’s definitions of control beliefs and of the need forcompetence are very similar, some researchers suggestedthat the perceptions related to control are energized by theneed for competence (Hagger, Chatzisarantis, & Biddle,2001; Hagger et al., 2002a).
There has also been some confusion about the constructof autonomy. Autonomy and control are not the same (Deci& Ryan, 1987). Autonomy describes the extent to whichperformance of behavior is volitional and is endorsed witha sense of choice and willingness. Autonomy does not meanbeing able to control outcomes or have the capacity to per-form behaviors leading to outcomes. The two constructs areconceptually and empirically distinct: One can be com-pelled to engage in behaviors over which one has completecontrol, and one can try to self-initiate a behavior overwhich one has little control (i.e., people self-initiate chal-lenging tasks; Deci & Ryan, 1985; Hagger et al., 2002a).Applications of self-determination theory (SDT) arereviewed in this section of the chapter because this is oneof the few theories in social psychology that explicitly rec-ognizes the importance of the distinction between controland autonomy in understanding social phenomena such asphysical activity.
Self-Determination Theory
Self-determination theory is a popular theory proposingthat human motivation and psychological well-being can beexplained on the basis of psychological needs for compe-tence, self-determination (autonomy), and relatedness(Deci & Ryan, 1985). Self-determination refers to the needfor experiencing oneself as an initiator and regulator ofone’s actions. Competence refers to the need for producingbehavioral outcomes and understanding the production ofthese behavioral outcomes. Relatedness refers to the needfor experiencing satisfactory relationships with others andwith the social order in general (Deci & Ryan, 1991).
Psychological Needs and the Energizationof Behavior
The concept of psychological needs differs from the morecommon usage that equates a need with any personal desireor goal that people may try to achieve. According to Ryan(1995), psychological needs are necessary for human devel-opment and growth. For example, it has been suggested thatas human beings require water and food to survive, in thepsychological domain human motivation requires experi-ences of autonomy, competence, and relatedness to sustain
and grow (Sheldon, Elliot, Kim, & Kasser, 2001). Individ-uals do not necessarily need, for example, fancy cars andprivate jets to grow psychologically. These other needs arenot essential but substitute needs that are not universal butlearned through social processes (Deci & Ryan, 1980).
The concept of psychological needs is also importantbecause it makes motivation a dynamic concept (Ryan,1995). By definition, a psychological need is an energizingstate that, if satisfied, enhances health and psychologicalwell-being; if not satisfied, then “ill-being” will result(Ryan & Deci, 2000). Several studies in social andsport /exercise psychology have consistently supported thishypothesis (Gagne, Ryan, & Bargman, 2003; Hagger,Chatzisarantis, & Harris, in press; Ntoumanis, 2001; Sar-razin, Vallerand, Guillet, Pelletier, & Cury, 2002; Wilson,Rodgers, Blanchard, & Gessell, 2003). For example, in astudy of young gymnasts, Gagne et al. documented thatneed satisfaction experienced during practice explainedchanges in daily well-being. In addition, we have recentlydocumented that need satisfaction was associated withpositive physical activity attitudes, strong intentions toexercise, and physical activity participation (Hagger et al.,in press).
Interpersonal Context and the Fostering of HumanMotivation and Psychological Well-Being
In addition to addressing issues related to the energizing ofhuman motivation, SDT places importance on the environ-ment and interpersonal contexts within which motivationoccurs. According to Ryan (1995), psychological needs andthe inputs that those psychological needs generate arenecessary but not sufficient for human development andgrowth. For intrinsic motivational tendencies to sustainand grow, psychological needs must be supported becauseotherwise individuals will be alienated from these needs(Deci & Ryan, 1980). It is evident, therefore, that SDT is adialectic theory that assigns to the environment the role ofa nurturer that actually does or makes efficient motivationoccur (Aristotle, 1993). The conceptual analogue of therole of environment, as viewed by SDT, is that of a seedthat grows into a tree only if the greater environment (i.e.,climatic conditions, soil) is conducive to its growth.
Self-determination theory differentiates among threetypes of interpersonal contexts that either support or frus-trate psychological needs. The general ambience of inter-personal context is said to be chaotic when the greaterenvironment is unstructured and significant others do notprovide feedback at all (Deci & Ryan, 1991). Chaotic envi-
Theoretical Frameworks in Exercise Psychology 547
ronments undermine competence and promote amotivation,as demonstrated in physical education by Ntoumanis andcolleagues (Ntoumanis, Pensgaard, Martin, & Pipe, 2004).The interpersonal context is said to be supportive of psy-chological needs (autonomy-supportive contexts) when sig-nificant others encourage choice and participation indecision making, provide a meaningful rationale, use neu-tral language (e.g., “may,” “could” rather than “should,”“must ”) during interpersonal communication, andacknowledge people’s feelings and perspectives (Deci,Koestner, & Ryan, 1999). For example, an instructor whouses neutral language in conducting an exercise class andexplains reasons behind different exercise tasks is likely tocontribute to the development of an autonomy-supportiveclimate. The interpersonal context is said to frustrate psy-chological needs (controlling contexts) when significantothers do not explain why performance of certain behav-iors may be important, use pressuring language duringinterpersonal communication (e.g., use of “should” and“must”), or do not acknowledge difficulties associatedwith performance of a behavior. An exercise instructorwho makes people think, feel, or behave in particular waysis likely to contribute to the development of a controllinginterpersonal context.
The importance of adopting autonomous-supportiveversus controlling interpersonal styles has been examinedin numerous studies and across different life domains.Autonomy-supportive health care providers, parents,coaches, physical educators, and peers have been found todevelop a better quality of motivation (Goudas, Biddle, &Underwood, 1995; Hagger & Chatzisarantis, 2005b; Hag-ger, Chatzisarantis, Culverhouse, & Biddle, 2003;Ntoumanis, 2001; Standage, Duda, & Ntoumanis, 2003;Standage, Duda, & Ntoumanis, in press; G. C. Williams,Gagné, Ryan, & Deci, 2002), promote adherence to sportand physical activity (Chatzisarantis, Hagger, Smith, &Sage, in press), and promote enhanced levels of satisfac-tion of psychological needs and psychological well-being(Gagne et al., 2003; Levesque, Zuehlke, Stanek, & Ryan,2004; Sarrazin et al., 2002). In contrast, young people andadults develop less persistent forms of motivation(Goudas, Biddle, & Fox, 1994; Goudas et al., 1995; Hagger& Chatzisarantis, 2005b, in press; Vansteenkiste & Deci,2003), tend to drop out from physical activity and sport(Sarrazin et al., 2002; G. C. Williams & Deci, 1998), andare left unsatisfied (Gagne et al., 2003) when significantothers pressure them or make them think, feel, and behavein particular ways.
Forms and Quality of Human Motivation
Self-determination theory distinguishes not only betweenautonomous and controlling interpersonal contexts but alsobetween autonomous and controlling motivational styles.The conceptual analogue of motivational form is that of theshape of materials and describes the structure by whichmotivation is identified (Aristotle, 1993). Cognitive evalu-ation theory (a subtheory of SDT) initially distinguishedbetween two general forms of motivation. Intrinsic motiva-tion refers to the doing of an activity for its inherent satis-factions rather than for some separable outcomes. Extrinsicmotivation refers to the doing of an activity for outcomesthat are separable from the activity itself (Ryan & Deci,2000). However, subsequent studies have shown that extrin-sic motivation can be further differentiated into externalregulation, introjection, identification, and integration.
External regulation refers to a behavior that is per-formed to obtain a reward or approval from a significantother (Ryan & Connell, 1989). For example, people whoexercise because their spouse pressures them to do so areexternally regulated. Introjection lies next to external reg-ulation; it refers to a behavior that is performed to avoid apressuring emotion of guilt or shame. A person who exer-cises for reasons of weight management and feels guiltywhen missing some exercise sessions is said to be intro-jected. External regulation and introjection describe con-trolling forms of motivation because they describebehaviors that are performed under some form of internal(e.g., introjection) or external (e.g., external regulation)pressure. A less controlling and more self-determined formof motivation is identification. This refers to a behaviorthat is performed because the individual values it. Duringidentification, individuals accept and endorse the value ofphysical activity, and for this reason, identified behaviorrepresents a more self-determined form of motivation. Themost autonomous and least controlling form of behavior isintegrated regulation. This refers to identifications that arebrought into congruence with other behaviors and roles thatare enacted in life. This definition presupposes that identi-fication is a less autonomous form of behavioral regulationthan integration because regulation through identificationmay conflict with preexisting values and behaviors.
In the domain of sport and physical activity, manyinstruments measure the motivational styles proposed bySDT. The Sport Motivation Scale, developed by Pelletierand colleagues (1995), assesses amotivation, external regu-lation, introjection, identification, and three types ofintrinsic motivation: intrinsic motivation to know (e.g.,
548 Exercise and Health Psychology
“for the pleasure it gives me to know more about the sportthat I practice”), to accomplish (e.g., “because I feel lot ofpersonal satisfaction while mastering certain difficultmovements”), and to experience stimulation (e.g., “ for theintense emotions”).
In the context of physical activity, there is the Behav-ioral Regulation in Exercise Questionnaire (Markland &Tobin, 2004; Mullan, Markland, & Ingledew, 1997) and theExercise Motivation Scale (EMS; Li, 1999). Both of theseinstruments measure amotivation, external regulation,introjection, identification, and intrinsic motivation. How-ever, the EMS measures integrated regulation as well.Finally, Goudas et al. (1994) adapted Ryan and Connell’s(1989) self-regulation questionnaire and Vallerand et al.’s(1992) academic motivation scale in the physical educationcontext. Goudas et al.’s scale measures external regulation,introjection, identification, and intrinsic motivation but notintegrated regulation.
The importance of adopting an autonomy-supportiveversus controlling motivational style has been examinedin numerous studies across different domains. Supportingassumptions underling SDT, we have documented thatmotivational styles form a motivational continuum(Chatzisarantis, Hagger, Biddle, Smith, & Wang, 2003).In this continuum, which is often described as a develop-mental continuum of self-determination (Deci & Ryan,1991), external regulation and intrinsic motivation arelocated at the opposite ends, and introjection and identifi-cation lie in between external regulation and intrinsicmotivation. In addition, several prospective studies haveshown that autonomous motivational styles are morestrongly associated with intentions to exercise, prolongedparticipation in sport, adherence to physical activity, andpsychological well-being than controlling motivationalstyles (Chatzisarantis & Biddle, 1998; Chatzisarantis,Biddle, & Meek, 1997; Chatzisarantis, Hagger, Biddle, &Karageorghis, 2002; Gagne et al., 2003; Hagger et al.,2002a; Matsumoto & Takenaka, 2004; Vansteenkiste &Deci, 2003). In addition, empirical evidence supportsrelationships between autonomy-supportive interpersonalcontexts and autonomous motivational styles on the onehand ( identif ication and intrinsic motivation), andbetween controlling interpersonal contexts and control-ling motivational styles on the other (Hagger & Chatzis-arantis, 2005b, in press; Hagger et al., 2003; Ntoumanis,2001; Standage et al., 2003, in press).
Research in sport and physical activity has also exam-ined relationships between motivational styles and otherpsychological variables not necessarily included in SDT.
For example, in the context of physical education, Goudaset al. (1994) found relationships between motivationalstyles and task and ego achievement goal orientations, per-ceived competence, and intentions. Wilson, Rodgers, Blan-chard, et al. (2003) documented that motivational stylesare related to different imagery techniques used by exer-cisers. Appearance imagery was associated with introjec-tion, and identification and intrinsic motivation wereassociated with imagery techniques reflecting techniqueand energy.
In summary, SDT has emerged as an important theoret-ical approach in exercise psychology (Biddle, Chatzisaran-tis, & Hagger, 2001; Chatzisarantis et al., 2003). Buildingon prior work concerning intrinsic and extrinsic motiva-tion, SDT now embraces a wider view of human motiva-tion, including differentiated types of extrinsic motivation,and the role of need satisfaction (Deci & Ryan, 2002). Thechallenge for practitioners remains how to create an auton-omy-supportive climate whereby self-determined forms ofmotivation dominate in the physical activity context.
STAGE-BASED MODELS
The theoretical approaches discussed so far tend to be con-tinuous models; that is, constructs are reflected as contin-uous variables rather than discrete stages. The mostwell-known stage conceptualization is that of the transthe-oretical model (TTM), developed by Prochaska andDiClemente (1984, 1986; Prochaska, Norcross, &DiClemente, 1994; Prochaska & Velicer, 1997). The TTMemerged from an analysis of change systems used in psy-chotherapy to treat addictive behaviors such as smokingand drug use. More recently, it has been offered as a coher-ent framework to help understand readiness to begin physi-cal activity. Literature on the TTM in physical activity isnow diverse, including descriptive studies (Marcus, Rossi,Selby, Niaura, & Abrams, 1992; Mullan & Markland,1997), interventions (Mutrie et al., 2002), narrativeoverviews (Prochaska & Marcus, 1994), a meta-analysis(Marshall & Biddle, 2001), and practical guidelines (Mar-cus & Forsyth, 2003). The TTM treats behavior change asa dynamic process rather than an all-or-nothing phenome-non. Evidence suggests that individuals attempting tochange their physical activity behavior move through aseries of stages. The stages are characterized by a tempo-ral dimension of readiness to change. Five stages have beenproposed that differ according to an individual’s intentionand behavior, the latter being defined in relation to a crite-rion level. Whether people move into a more advanced
Theoretical Frameworks in Exercise Psychology 549
stage will partly be determined by how the level of thebehavioral criterion is defined. The stages have beenlabeled precontemplation, contemplation, preparation,action, and maintenance (see Table 24.1).
Original formulations of the model proposed that indi-viduals moved through the stages in a linear fashion. It isnow recognized that stage progression is more likely to fol-low a cyclical pattern whereby individuals progress andregress through the stages in an effort to create lastingchange. This is analogous to the board game “Snakes andLadders,” where you make progress up the ladders butsometimes regress down the snakes before climbing anoth-er ladder.
Four factors are hypothesized to mediate the changeprocess: (1) an individual’s self-efficacy for change, (2) theweighing up of perceived advantages (pros) and (3) disad-vantages (cons) of change (decisional balance), and (4) thestrategies and techniques individuals use to modify theirthoughts, feelings, and behavior (referred to as the process-es of change). As such, it is possible to identify how peoplechange through the stages and why people change throughthe mediators. Changes in the mediators should result inbehavior change.
The importance of self-efficacy for initiating and main-taining a pattern of regular physical activity derives fromsocial cognitive theories of behavior (Bandura, 1986) andwas discussed earlier in the chapter. Numerous studieshave revealed a consistent positive relationship betweenexercise self-efficacy and stage of change (Marcus, Eaton,Rossi, & Harlow, 1994). Narrative reviews of the literatureare unequivocal that higher efficacy is associated withadvancing stage, with many concluding the relationship tobe linear (Prochaska & Marcus, 1994). Self-efficacy alsoappears to successfully differentiate between individualsat most stages, as shown in our meta-analysis (Marshall &Biddle, 2001).
Behavior change is assumed to involve a systematicevaluation of the potential gains (pros) and losses (cons)associated with adopting the new behavior. Our meta-
analysis showed that pros increase for every forward stagetransition, with the largest change being from precontem-plation to contemplation, whereas the change from con-templation to preparation was virtually zero. All otherstage transitions had small effects. For the cons of behav-ior change, we showed that these generally decreasedacross stages, as predicted, and that the largest change wasfrom precontemplation to contemplation, whereas thesmallest was from action to maintenance (Marshall & Bid-dle, 2001). Our results, therefore, suggest that interven-tions might usefully focus on increasing pros and reducingcons, particularly at the important transition from precon-templation to contemplation. For example, a decisionalbalance exercise could be adopted in self-help changeleaflets for community-level interventions or could beused in individual exercise counseling (Biddle, 2004;Breckon, 2002; Loughlan & Mutrie, 1997).
Ten basic processes of change have been proposed thatdescribe the techniques and strategies individuals use tomodify their thoughts, feelings, and behavior (Prochaska &DiClemente, 1983). These processes have been organizedinto two higher-order constructs: cognitive processes(thinking or experiential processes) and behavioral (doing)processes (Prochaska, Velicer, DiClemente, & Fava, 1988).Narrative reviews in the physical activity domain have alsoconcluded that a two-factor model is appropriate, andstage-specific trends exist for these higher-order con-structs (Prochaska & Marcus, 1994). The general consen-sus is that cognitive processes are more important duringthe early stages, with behavioral processes important atlater stages, but our meta-analysis was not able to supportthis (Marshall & Biddle, 2001). Indeed, the majority ofconclusions in previous reviews are based on a single pri-mary study that found the correlation between cognitiveand behavioral processes to be .91 (Marcus et al., 1992), afinding that actually argues against a two-factor model.
Few studies are available that make process-specificpredictions at each stage of change. It has been suggestedthat consciousness raising is particularly important when
Table 24.1 Defining Stages of the Transtheoretical Model
StageMeeting Criterion Level
of Physical Activity? Current BehaviorIntention to Meet CriterionLevel of Physical Activity?
Precontemplation No Little or no physical activity No
Contemplation No Little or no physical activity Yes
Preparation No Small changes in physical activity Yes
Action Yes Physically active for less than 6 months Yes
Maintenance Yes Physically active for more than 6 months Yes
550 Exercise and Health Psychology
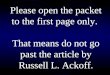
Figure 24.3 Differences in effect sizes in physical activityacross stages for physical activity studies. Source: “The Trans-theoretical Model of Behavior Change: A Meta-Analysis ofApplications to Physical Activity and Exercise,” by S. J. Mar-shall and S. J. H. Biddle, 2001, Annals of Behavioral Medicine,23, pp. 229–246. Reprinted with permission.
Effect size2.5
2
1.5
1
0.5
0Precontem
plation
Contemplation
Preparation
Action
Maintenance
moving from precontemplation to contemplation (Reed,1999), and the findings from our meta-analysis were insupport of this. However, the greatest effect size from pre-contemplation to contemplation was for self-liberation.This is the belief that change is possible and that responsi-bility for change lies within the individual. Items measur-ing self-liberation appear theoretically consistent withconcepts of autonomy, as discussed earlier in the section onself-determination theory, and this has predicted interestin and adherence to physical activity. Based on our meta-analysis, we believe that processes of change for physicalactivity require further investigation before definitivestatements about their use can be made for interventions.
The vast majority of studies investigating the TTM inphysical activity (Marshall & Biddle, 2001) and otherhealth behavior contexts (Sutton, 2000) are cross-sectional.This presents difficulties in establishing causal relation-ships between constructs and stages. Moreover, manystudies using such a design provide support for what Wein-stein and colleagues (Weinstein, Rothman, & Sutton,1998) have called “pseudo-stage” models, where there is alinear pattern of change (actually “difference” in a cross-sectional design) between variables rather than having ana priori assumption of discontinuity whereby a variable ispredicted to act differently at different stages (Sutton,2000). Data from our meta-analysis are more supportive ofa pseudo-stage model, as shown in Figures 24.3 and 24.4.
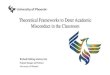
In Figure 24.3, physical activity differences betweenstages follow essentially a linear pattern, with only a hintof discontinuity through a flat S-shaped curve. In Figure24.4, self-efficacy is largely linear across the stages. Sim-ilarly, in a study we conducted on the extent and determi-nants of promoting physical activity for patients by mentalhealth professionals (Faulkner & Biddle, 2001), weassessed mean score differences in variables from the the-ory of planned behavior among three stages: no promotionof physical activity, irregular promotion, and regular pro-motion. Again, results supported a pseudo-stage modelrather than a true stage model because the differencesacross the three groups for each variable were essentiallylinear (see Figure 24.5). Future studies on the TTM andphysical activity need to test for the discontinuity ofvariables across stages and establish whether the variableis an antecedent or consequence of stage transition (Sut-ton, 2000).
THEORETICAL INTEGRATION
Recent investigations have combined stage models with lin-ear, continuous models. One approach is to investigate themeans in variables derived from continuous theories, suchas the TPB, across the different stage groups. Anotherstrategy might be to test the architecture of a linear modelwithin each stage group separately.
Figure 24.4 Differences in effect sizes in self-efficacy acrossstages for physical activity studies. Source: “The Transtheoreti-cal Model of Behavior Change: A Meta-Analysis of Applicationsto Physical Activity and Exercise,” by S. J. Marshall and S. J. H.Biddle, 2001, Annals of Behavioral Medicine, 23, pp. 229–246.Reprinted with permission.
Effect size2.5
2
1.5
1
0.5
0Precontem
plation
Contemplation
Preparation
Action
Maintenance
Theoretical Frameworks in Exercise Psychology 551
Cross-Sectional Patterns
As described previously, the TPB variables often show lin-ear patterns (Faulkner & Biddle, 2001). However, for vari-ables that might operate in a more stage-specific way, wehave found nonlinear patterns and support for stageassumptions (Lippke & Plotnikoff, 2005). Strongest sup-port for discontinuity patterns were revealed for percep-tions of vulnerability (subjective chances of contracting adisease if one is not physically active). Individuals in theprecontemplation stage felt least vulnerable, those in con-templation and action reported the highest vulnerability,and individuals in preparation and maintenance hadreduced vulnerability. The higher level of vulnerability inthe contemplation stage, in comparison to precontempla-tion, is in accordance with the stage definition. Individualsin precontemplation are either unaware of the risk behavior(such as not being physically active enough) or subjectivelyreduce their vulnerability due to an incorrect optimisticmind-set. In contemplation, persons become aware of theirrisk. However, if they plan to start performing the behaviorin question in the near future, or if they are already per-forming some behavior, their vulnerability estimationbecomes relevant and they may express feelings of vulner-
ability. Individuals in action are more realistic, and thosein maintenance are actually reducing their vulnerabilitybecause of their behavior. However, such a pattern is notexpected in variables such as self-efficacy due to its coreimportance in all stages (Bandura, 1986, 1997). Therefore,it is important to employ the appropriate test variables forinvestigating discontinuity patterns (Lippke & Plotnikoff,2005; Lippke, Sniehotta, & Luszczynska, 2005).
Longitudinal Patterns
Another strategy is to combine a linear model with a stagemodel. In some studies, the stage membership has beenpredicted additionally or alternatively to intention andbehavior in these linear estimations, as, for example, in theTPB (Courneya, Nigg, & Estabrooks, 1998). Because stageis conceptualized as analogous to intention and behaviorprobability, the advantage of including the stage variablealongside intention and behavior additionally or alterna-tively is rather small. In contrast, to investigate stage as amoderator and to examine stage-dependent processes hasbeen shown to be fruitful (Lippke, Nigg, & Maddock,2004). These processes are analogous to the assumption ofmost social cognitive models, intention formation, actionplanning, and behavior change. With this strategy onemight also test discontinuity patterns by testing whether,depending on the stage, different social cognitive variablesare more or less influential (Weinstein et al., 1998).
By testing the TPB over 1 year, we found that attitudeand intention were highly associated in all stages. Per-ceived behavioral control, subjective norm, and intentionwere significantly and positively related. In all other stagegroups, the subjective norm and intention relations werenot significant. Perceived behavioral control was not relat-ed to intention or behavior except in the maintenance stage.If individuals who performed physical activity over alonger period of time perceived more control, they also hada higher intention and performed more behavior. Intentionand physical activity were correlated in precontemplation,preparation, action, and maintenance, but not in contem-plation (Lippke, Nigg, et al., 2004).
A Hybrid Model: The Health ActionProcess Approach
The health action process approach (HAPA; Schwarzer,1992, 2001) is a model that explicitly integrates continuousand stage assumptions and is thereby a hybrid model. At thesame time, the HAPA integrates motivational (predictionof intention) and behavior-enabling models (inclusion ofpostdecisional facets such as implementation intentions).
Figure 24.5 Mean scores for variables from the theory ofplanned behavior across three stage groups based on the extentof physical activity promotion by mental health professionals.Note: PBC = Perceived behavioral control. Source: “PredictingPhysical Activity Promotion in Health Care Settings,” by G.Faulkner and S. Biddle, 2001, American Journal of Health Pro-motion, 16(2), pp. 98–106. Reprinted with permission.
Promotion of physical activity
RegularIrregularNo0
1
2
3
4
5
6
Mea
n
IntentionAttitudeSubjective normPBC
552 Exercise and Health Psychology
Figure 24.6 The health action process approach, with itsarchitecture and stages adapted from Lippke, Ziegelmann, andSchwarzer (2005). Note: SE = Self-efficacy; Risk = Risk per-ception. Dashed arrows indicate stage-specific effects andmechanisms; solid arrows show generic effects. Source: “Self-Efficacy in the Adoption and Maintenance of Health Behaviors:Theoretical Approaches and a New Model” (pp. 217–243), by R.Schwarzer, in R. Schwarzer (Ed.), Self-Ef ficacy: Thought Controlof Action, 1992, Bristol, PA: Taylor & Francis. Reprinted withpermission.
Intention
IntentionalStage
NonintentionalStage
ActionStage
Cons
Risk
Pros
SE
Plan Behavior
The HAPA makes a distinction between a motivationphase and a volition/postdecision phase of health behaviorchange. The basic idea is that individuals experience a shiftof mind-set when moving from the first phase (motivation-al) to the second (volitional). The moment people committhemselves to an intention to exercise, for example, theyenter the volitional phase. In this phase, a division into twosubphases appears to be meaningful, wherein people can belabeled as either intenders or actors. First, they intend toact but they remain inactive. Second, they initiate theintended action. Thus, three phases or stages can be distin-guished, as shown in Figure 24.6. In the (a) nonintentionalstage, a behavioral intention is being developed, which issimilar to the contemplation stage in the TTM. Afterward,individuals enter (b) the intentional stage, where they havealready formed an intention but still remain inactive (or atleast not active at the recommended level), while the exer-cise behavior is being planned and prepared. If these plansare translated into action, individuals reside in (c) theaction stage. They are then physically active at the recom-mended goal behavior level.
In the nonintentional stage, an intention has to be devel-oped. In this phase, risk perception is a distal antecedentwithin the motivational phase. Risk perception is sufficientto enable the undecided person to form an intention. Fur-thermore, it is a prerequisite for a contemplation process
and further elaboration of thoughts about consequences andcapacities. Risk perception operates at a stage-specificlevel, and therefore its effect on intention is represented bya dashed line in Figure 24.6; in the intentional stage, riskperception has no effect (Lippke, Ziegelmann, & Schwarz-er, 2005). The belief in one’s capabilities to perform adesired action (self-efficacy) is necessary for goal pursuit.That is, perceived self-efficacy promotes intention forma-tion and behavior implementation in all stage groups (Lipp-ke, Ziegelmann, et al., 2005); the arrow is therefore drawnas a solid line, not dashed, in Figure 24.6.
After a decision has been made, the intentional stage isentered: The individual has a high intention but is not per-forming the behavior. The intention has to be transformedinto detailed plans on how to perform the behavior.Instructions on the goal pursuit may contain assistingintentions and precise implementation intentions or plans.These plans involve when, where, and how the goal behav-ior will be initiated (Lippke, Ziegelmann, & Schwarzer,2004) whereby cognitive links between concrete opportu-nities and the intended behavior will be built. Social cogni-tive variables change in dominance and interplay. Riskperception has no further influence, but outcome expectan-cies remain important. Self-efficacy is also important inthe planning and initiation process, especially if barriersoccur or no enabling situation arises. Self-efficacy keepsthe intention high and the plans flexible to compensate forsetbacks and stay on track to initiation.
If the goal behavior has been initiated, the individualenters the action stage. The behavior has to be controlled bycognitions in order to be maintained. Self-regulatory skillsare substantial for the maintenance process. Effort has to beinvested, useful situations for implementation of the newbehavior have to be detected, and distractions have to beresisted. The behavior will mainly be directed by self-efficacy (Schwarzer, 2001) because it regulates how effort isinvested and persistence is managed if barriers and setbacksoccur. The performed behavior has to be maintained, andrelapses have to be managed by action control strategies.
Due to individuals having to first set a goal that then maybe translated into plans and behavior, this process is stage-specific; only persons in intentional and action stages aremore likely to make plans and subsequently perform thegoal behavior (dashed lines in Figure 24.6; Lippke, Ziegel-mann, et al., 2005). Also, the influence of self-efficacy onpostdecisional processes, such as planning and behaviorperformance, depends on whether one has decided tochange (here it is crucial to believe in one’s own competen-cies) or not (here only intention formation can be support-
Theoretical Frameworks in Exercise Psychology 553
ed by self-efficacy). The HAPA also includes aspects suchas situational barriers and resources (Schwarzer, 1992,2001), but not much work has been done on these to date.
CONCLUSION
In this chapter, we have summarized the most popular the-ories in exercise psychology. One objective was to provide aframework or heuristic to differentiate the various theories.This is challenging due to the multiple overlaps of differenttheories and constructs (Armitage & Conner, 2000). Thecorrespondence of the TRA and the TPB is obvious. How-ever, there also are similarities in other theories, as, forexample, the TPB and self-efficacy theory due to relation-ships between perceived behavior control and self-efficacy(Bandura, 2004). Perceived behavioral control and controlvariables might not be clearly separable (Schwarzer, 2001).Another example of overlap is attitudes in the TPB, outcomeexpectancies in self-efficacy theory, and the decisional bal-ance (pros and cons) in the TTM (D. M. Williams, Ander-son, & Winett, 2005). In the future, investigators need tostate which theory is the most appropriate for a particularresearch question or intervention strategy. With the currentoverlap in constructs, however, it might be difficult to com-pare the theories because one might not easily test the dis-criminant validity of the constructs. One solution would beto assume that the constructs match each other and thus canbe used for comparing the theories, as Garcia and Mann(2003) have done. They identified the HAPA as being supe-rior to other models, such as the TPB, by investigatingexplained variances. With this method, we can comparehow well the different theories explain the variation inbehavior and which theoretical constructs might be mostvaluable. Other methods to assess the appropriateness of atheory could be to evaluate (a) whether the theory providesstatistically significant outcomes (e.g., tested in an experi-mental design); (b) its effect size and whether it is clinicalmeaningful; (c) the public health impact if the theory istested in a public health intervention; and (d) how general-izable the theory is to different populations, cultural sub-groups, and circumstances (Nigg & Jordan, 2005).
One other approach in the future is not necessarily com-paring and separating the theories but, instead, combiningthem to explain more variance. However, researchers andpragmatists have to avoid overloading theories and inter-vention plans. Theories have to be complete but also parsi-monious—in other words, clear and simple (Michie et al.,2005). One model that aims to achieve this end is theHAPA due to its integration of motivational and volitional
stages and generic factors of self-efficacy and stage-spe-cific features, such as translating intentions into behaviorvia implementation intentions. With this model, we havelearned, depending on the stage of the target group, thatdifferent mechanisms are important. For example, for thosedescribed as “intentional individuals,” implementationintentions or plans are most crucial to translate their inten-tions into successful behavior.
Most of the theories in this chapter focus on the indi-vidual, but environmental factors are also important (Bid-dle & Mutrie, 2001). Some theories include externalfactors such as the TPB with subjective norms and SDTwith its external forms of motivation. In these models,external factors are included as a subjective representationin the individual. However, numerous studies have alsoshown that objective features of the environment canexplain why individuals are likely to be physically active ornot. For instance, if there are more parks and pavement andsidewalks in the neighborhood, people walk more (Sumins-ki, Poston, Petosa, Stevens, & Katzenmoyer, 2005). In thefuture, individual approaches should be tested under dif-ferent environmental circumstances. This could test, forexample, whether more variance is accounted for usingTPB in a positive physical activity environment (e.g.,where people perceive that they just have to change theirown behavior to be active) than in unattractive environ-ments (where individuals feel they cannot change theirbehavior just by individual decisions and become subject tolearned helplessness in terms of their exercise behavior).These thoughts require further testing.
Empirically supported models are useful for creatinginterventions by identifying and altering particular factors(e.g., derived from continuous social cognitive models) thathelp people move from one stage to the next. Stage modelsoffer the possibility of designing programs and treatmentsthat will be more effective and efficient than one-size-fits-all interventions (Weinstein et al., 1998). Therefore, trans-lating research into practice is important, and theory-basedinterventions are imperative for successful exercise andhealth-enhancing physical activity promotion.
REFERENCES
Ajzen, I. (1985). From intentions to actions: A theory ofplanned behavior. In J. Kuhl & J. Beckmann (Eds.), Actioncontrol: From cognition to behavior (pp. 11–39). New York:Springer-Verlag.
Ajzen, I. (1988). Attitudes, personality and behavior. MiltonKeynes, England: Open University Press.
554 Exercise and Health Psychology
Ajzen, I. (1991). The theory of planned behavior. Organization-al Behavior and Human Decision Processes, 50, 179–211.
Ajzen, I. (2001). Nature and operation of attitudes. AnnualReview of Psychology, 52, 27–58.
Ajzen, I. (2002). Residual effects of past on later behavior:Habituation and reasoned action perspectives. Personalityand Social Psychology Review, 6, 107–122.
Ajzen, I., Brown, T. C., & Carvahal, F. (2004). Explaining thediscrepancy between intentions and actions: The case ofhypothetical bias in contingent valuation. Personality andSocial Psychology Bulletin, 30, 1108–1121.
Ajzen, I., & Driver, B. (1991). Prediction of leisure participationfrom behavioral, normative and control beliefs: An applica-tion of the theory of planned behavior. Leisure Sciences, 13,185–204.
Ajzen, I., & Fishbein, M. (1980). Understanding attitudes and pre-dicting social behavior. Englewood Cliffs, NJ: Prentice-Hall.
Aristotle, N. (1993). Nichomachian ethics. Athens: Cactus.
Armitage, C. J., & Conner, M. (2000). Social cognition modelsand health behavior: A structured review. Psychology andHealth, 15, 173–189.
Armitage, C. J., & Conner, M. (2001). Efficacy of the theory ofplanned behavior: A meta-analytic review. British Journal ofSocial Psychology, 40, 471–499.
Bagozzi, R. P., & Kimmel, S. K. (1995). A comparison of lead-ing theories for the prediction of goal-directed behaviors.British Journal of Social Psychology, 34, 437–461.
Bandura, A. (1977). Self-efficacy: Toward a unifying theory ofbehavioral change. Psychological Review, 84, 191–215.
Bandura, A. (1986). Social foundations of thought and action: Asocial cognitive theory. Englewood Cliffs, NJ: Prentice-Hall.
Bandura, A. (1997). Self-ef ficacy: The exercise of control. NewYork: Freeman.
Bandura, A. (2004). Health promotion by social cognitivemeans. Health Education and Behavior, 31(2), 143–164.
Biddle, S. J. H. (1999). Motivation and perceptions of control:Tracing its development and plotting its future in exercise andsport psychology. Journal of Sport and Exercise Psychology,21, 1–23.
Biddle, S. J. H. (2004). Individual and small group interventions.In P. Oja & J. Borms (Eds.), Perspectives—The multidiscipli-nary series of physical education and sport science: Vol. 6.Health enhancing physical activity (pp. 343–368). Oxford:Meyer & Meyer.
Biddle, S. J. H., Chatzisarantis, N. L. D., & Hagger, M. S.(2001). Theorie de l’autodetermination dans le domaine dusport et de l’exercice physique [Self-determination theory insport and exercise]. In F. Cury & P. Sarrazin (Eds.), Theo-ries de la motivation et pratiques sportives: Etats desrecherches [Theories of motivation and sport practice: The
state of research] (pp. 19–55). Paris: Presse Universitairesde France.
Biddle, S. J. H., & Mutrie, N. (2001). Psychology of physicalactivity: Determinants, well-being and interventions. London:Routledge.
Biddle, S. J. H., & Nigg, C. R. (2000). Theories of exercise behav-ior. International Journal of Sport Psychology, 31, 290–304.
Bouchard, C. (2000). Introduction. In C. Bouchard (Ed.), Physi-cal activity and obesity (pp. 3–19). Champaign, IL: HumanKinetics.
Bouchard, C., & Blair, S. N. (1999). Introductory comments forthe consensus on physical activity and obesity. Medicine andScience in Sports and Exercise, 31(11, Suppl.), S498–S501.
Bozoian, S., Rejeski, W. J., & McAuley, E. (1994). Self-efficacyinfluences feeling states associated with acute exercise. Jour-nal of Sport and Exercise Psychology, 16, 326–333.
Breckon, J. (2002). Motivational interviewing and exercisepreparation. In D. Lavallee & I. Cockerill (Eds.), Counselingin sport and exercise contexts (pp. 48–60). Leicester,England: British Psychological Society, Sport and ExercisePsychology.
Chatzisarantis, N. L. D., & Biddle, S. J. H. (1998). Functionalsignificance of psychological variables that are included inthe theory of planned behavior: A self-determination theoryapproach to the study of attitudes, subjective norms, percep-tions of control, and intentions. European Journal of SocialPsychology, 28, 303–322.
Chatzisarantis, N. L. D., Biddle, S. J. H., & Meek, G. A. (1997).A self-determination theory approach to the study of inten-tions and the intention-behavior relationship in children’sphysical activity. British Journal of Health Psychology, 2,343–360.
Chatzisarantis, N. L. D., & Hagger, M. S. (in press). Effects of abrief intervention based on the theory of planned behavior onleisure time physical activity participation. Journal of Sportand Exercise Psychology.
Chatzisarantis, N. L. D., Hagger, M. S., Biddle, S. J. H., & Kara-georghis, C. (2002). The cognitive processes by which per-ceived locus of causality predicts participation in physicalactivity. Journal of Health Psychology, 7, 685–699.
Chatzisarantis, N. L. D., Hagger, M. S., Biddle, S. J. H., &Smith, B. (2005). The stability of the attitude-intention rela-tionship in the context of physical activity. Journal of SportsSciences, 23, 49–61.
Chatzisarantis, N. L. D., Hagger, M. S., Biddle, S. J. H., Smith, B.,& Wang, C. K. J. (2003). A meta-analysis of perceived locus ofcausality in exercise, sport, and physical education contexts.Journal of Sport and Exercise Psychology, 25, 284–306.
Chatzisarantis, N. L. D., Hagger, M. S., Smith, B