Embed Size (px)
Citation preview

CUADERNOS DE
39C. Med. Psicosom, Nº 105 - 2013
Department of Personality, Evaluation and PsychologicalTreatmentFaculty of Psychology. UNED UniversityJuan del Rosal, 1028040 Madrid - SpainCo rres po ndence to : [email protected] en castellano: C. Med. Psicosom, Nº 69 / 70 - 2004 15
Theory and physiology of meditationTeoría y fisiología de la meditación
Daniel M. Campagne
Summary
In Spain, meditation is generally considered to be one more relaxation method amongst manyused in psychotherapy. Nevertheless, an extensive body of experimental findings affirms thatmeditation has cognitive, physiological and psychotherapeutic characteristics that clearly diffe-rentiate it from other relaxation methods insofar as its origin, generic and specific effects, formsand methods of application.
Meditation can produce distinctive effects on the nervous system, especially in the long run,thus providing opportunities for therapeutic use in clinical psychology. This ‘clinical meditation’is the object of experimental investigation in biological psychology and is not to be confusedwith meditation as an exercise in mystic and religious disciplines.
Key wo rds : Meditation. Relaxation. Psychotherapy. Physiology.
Resumen
En España, generalmente se incluye la meditación entre las técnicas de relajación utilizadasen psicoterapia. Sin embargo, un cuerpo extenso de documentación experimental afirma que lameditación posee características cognitivas, fisiológicas y psicoterapéuticas propias, diferen-ciándose claramente de la relajación en cuanto a la procedencia, los efectos genéricos y especí-ficos, las formas y los métodos de aplicación. La meditación puede producir efectos diferencia-les en el sistema nervioso, sobre todo a largo plazo y, por tanto, ofrece posibilidades para apli-caciones terapéuticas en psicología clínica. Conviene distinguir esta “meditación clínica” quees objeto de investigación de la psicología biológica de la meditación, como ejercicio utilizadoen diversas disciplinas místicas o religiosas.
Pal abras cl av e: Meditación. Relajación. Psicoterapia. Fisiología.
MEDICINA PSICOSOMÁTICA Y PSIQUIATRÍA DE ENLACEREVISTA IBEROAMERICANA DE PSICOSOMÁTICA
ARTÍCULO

INTRODUCTION
Meditation is a technique, used in many cul-tural, religious and philosophical traditions andrecently, in the Western world, in sports such asfootball training. In order to understand the con-cept, one must accept that meditation is not a rela -xation technique, nor a method to achieve enlighten -ment or religious ecstasy, nor is it a form of trai-ning with which to obtain a greater tolerance ofpain or suffering. Meditation may produce all ofthis, but its objective it is not. Although there isno consensus as to a definition of meditation, inorder to offer a global description that may servethe reader as a starting point for the informationthis article will provide, let us accept that medi-tation is a learned technique with which tochange a state of being attentive to identified sti-muli, to a state of unfocused attention. We couldalso consider it a method to prevent repetitivethinking, or one of cognitive reorientation. Oneof the differences with popular relaxation techni-ques is that meditation is not about “control”. Itdoes not concern relaxing muscles at will, nor“sending a warm feeling” or concentrating oneselfon noticing a group of muscles or a specific partof the body. Nevertheless, meditation may be usedto ob tain relaxation, just as any other method,serving to reach a state of calm.
Thus, the short term effects of meditation andrelaxation may be similar in their consequencesfor the autonomous nervous system (ANS), asGelhorn and Kiely’s 1972 study confirms. It mayproduce a deceleration of physical parameters,therefore slowing the motor response, slowingbreathing, reducing muscular tension, reducingheart rate, slowing gamma brain waves, and so on,although certain types of meditation may producea different response (Peng et al.,1999). Never -theless, many other neurophysiological effects ofmeditation have been registered that are not found,or are found in the opposite sense, in relaxation.Table 1 reflects only part of the, by now exten-sive, research on physiological effects of medita-tion as compared with the ones relaxation typi-cally produces, and where noticeable differenceswere found, both short and long term.
Relaxation techniques make use of willpower(sometimes on the part of the patient and other
times on the part of the therapist) and concentra-tion in order to achieve peaceful harmony, thephysiological effects of which can be measuredand verified. When tension recedes, or distal tem-perature rises, we will have obtained relaxation.
Meditation also uses willpower not only torelax but to maintain alertness throughout thesession and to train the concentration, not torelax but to “de-concentrate”, that is, to lose all no -tion of content, of thinking, of oneself, withoutlosing alertness or clarity of mind. Meditation, asresearch using the most sophisticated technicalmeans demonstrates, increases several indicatorsof central nervous system activity instead of de -creasing them as do relaxation techniques. Thereis an apparent contradiction in the co-existence ofrelaxing effects on the one hand and activatingeffects on the other, but the cited study of ErnstGellhorn and William Kiely has already underli-ned that no habituation was observed in electro-encephalogram (EEG) alpha waves during themeditative state, demonstrating that trophotropicdominance is compatible with total presence ofmind. Moreover, a reduction of beta waves in theEEG is characteristic of relaxation. However, aswe see in figure A, the EEG and electromyogram(EMG) registers of the spectral analysis done byBanquet, also in 1972, indicated that meditationcombined the absence of muscular activity accor-ding to the EMG, with an increase of beta andtheta activity, although a theta activity that diffe-red from the one related to somnolence (Banquet,1973; Banquet & Sailhan, 1974). In 2000 Lazarobserved, with functional magnetic resonance ima -ging (fMRI), that meditation activated neuronalstructures related to attention and to the controlof the autonomous nervous system.
Relaxation techniques are useful for trainingto adequately respond to stressors, by contro-lling the negative effects stress provokes. Medi -tation produces training in responding to stres-sors by taking away their stressful character, butalso has a direct influence on blood cortisol le -vels. Re laxation intends that the subject concen-trates on relaxing. Meditation aims at the subjecthaving complete consciousness without focuson any specific action or aspect, with whichunwanted interferences in mental processing willbe reduced.
C. Med. Psicosom, Nº 105 - 201340

ROOTS AND FORMS OF MEDITATION
A fair part of what we nowadays understand tobe mediation comes from techniques used inBuddhism. It is relevant to briefly review someaspects of meditation practice in order to avoidmistaken interpretations by readers who are notfamiliar with the technique. Nothing is moreimportant in Buddhist tradition than mind andconsciousness as primary objects of introspectiveinvestigation. Its first task is to refine attentionand to balance the nervous system with which tomake the mind properly functional, free from thenegative influences of excitation and laxity. Atten -tion is trained with a discipline called Samatha orSamadhi, meaning tranquility in the sense ofabsorbed concentration. This is not a religious orphilosophical discipline but merely a “contem-plative technique”. The objects of Samatha are todevelop both the stability and the intensity ofattention. Usually this type of meditation com-mences by focusing on a specific mental image,such as a flower. Two mental faculties are requi-red: mindfulness and introspection, of which mind -fulness is first and foremost in terms of impor-tance. Introspection does not observe the mindbut polices the process and is a type of “qualitycontrol”.
Samatha develops in nine stages. When com-mencing meditation, the attention is purposefullyand without hesitation maintained on the objectchosen, instead of being permitted to dwell freelywherever. One concentrates on the image, butusually the beginner loses attention almostimmediately. William James already said: “No onecan possibly attend continuously to an objectthat does not change” (James, 1950, I, p.420).The well-known work of Posner established thatthe initial and limited capacity of sustained atten-tion lasts between one and three seconds (Posner,1978). Even so, Buddhism maintains that thisability of sustained attention can be increased bycultivated insistence. It is not a matter of increa-sing strength or power of concentration, but ofthe motivation to remain with the chosen image.Therefore in the beginning attention is practicedin several sessions of fifteen minutes during theday, until it can be maintained on the same objectup to a minute. In other words, from now and
during one minute, the attention does not at alllose contact with the chosen mental image.However, the mind is still vulnerable to interfe-rence: peripheral noise or mental “monkey chat-ter”. By reducing the number of daily sessionsand increasing their duration one gets to the pointwhere the intensity of attention varies but contactis not lost during the entire session. With thehelp of introspection one achieves complete men-tal quietness and reaches the singular attentionwhere the mind can be focused on the chosenobject with complete stability and clarity forhours on end. The ninth and last stage of Sa -matha is attained when a dramatic change comesover the mental state, characterized by a brief andnot disagreeable sensation of heaviness or numb-ness on the top of the head, followed by expe-riences of physical and mental enjoyment, whichdisappear rapidly whilst leaving the attentionfirmly and tranquilly sustained on the object ofmeditation but gradually uncoupling from thesame and leaving the person with an absence ofobjects in the mind, a sense of clarity and a sen-sation of understanding. This sensation is alsodescribed as “pure positive affect” (mahasukha;pure joy; pure consciousness; beauty; and soforth) and is independent of any discursive thin-king or specific phenomenal content (Shear, 1999,Alexander et al., 1990).
I repeat that meditation is just a contempla-tive technique, without religious or philosophicalaspects, although many religions and especiallymystical schools use it in one form or another.The mystification of meditation has been ridicu-led and criticized by Buddhism itself. One of itsbest known representatives in the Western world,Chögyam Trungpa, says: “We sit and meditate.Once we begin to realize that we are actually one-hundred-percent fools for doing such a thing, thenwe begin to see how the techniques function as acrutch… Meditation practice is not a matter oftrying to produce a hypnotic state of mind or cre-ate a sense of restfulness (…). Instead, meditationshould reflect a mentality of richness in the senseof using everything that occurs in the state ofmind (…). Acknowledging restlessness, identif-ying with it, requires mindfulness, whereas pro-viding a luscious meadow, a big space for the res-tless cow requires awareness or alertness. So
C. Med. Psicosom, Nº 105 - 2013 41

mindfulness and awareness always complementeach other (…). In mindfulness practice there isno goal, no journey; you are just mindful ofwhat is happening there. There is no promise oflove and light or visions of any kind – no angels,no devils. Nothing happens: it is absolutelyboring. Sometimes you feel silly. (…) Boredomis important because boredom is anti-credential(…) it increases the psychological sophisticationof the practitioners. They begin to appreciateboredom and they develop their sophisticationuntil the boredom begins to become cool bore-dom, like a mountain river. (…) Mountainsnever get tired of being mountains and waterfallsnever get tired of being waterfalls. Because oftheir patience we begin to appreciate them.(…) Itis a good feeling to be bored, constantly sittingand sitting.(. . .) We have to work hard at it.”(Trungpa, 1988, pp.44-54).
There are alternative techniques within Budd -hism which center from the beginning on nonconceptual attention and mentally cut all thoughtsof the past, future and present from the mind.The technique of “adjusting the mind to its natu-ral state” was developed within the Buddhist Indo-Tibetan tradition. It is promoted by the Dalai La -ma (1997) although it was already described inthe eighth century by the philosopher PadmaSambhava, and comes with the warning thatthere is nothing with which to meditate and, wit-hout any modification or adulteration, the atten-tion must simply and without hesitation be focu-sed on its own natural state, its natural bland-ness, its own character as it is. One must haveclarity and relax the mind in such a way that it isloose and free.
There are simpler meditation techniques thatmay produce quicker results. A good example is
Benson and his Harvard team’s Relaxation Res -ponse, which greatly condenses meditative prac-tice (Benson, 1975). Another well known exam-ple is Transcendental Meditation (TM), a standar-dized contemplative method made popular in the1960’s by the Maharishi, who gained followersamong known artists and musicians. TM doesnot require any “conversion” to Buddhism orsimilar philosophy. It is based upon the wish toenter in states of mind that help to find answersto essential questions, to better understand one-self, the world, life itself. One is taught to use amantra1, in this case a sound without an assignedsignificance, and to repeat it without effort untilthe mind is absorbed and the maelstrom ofthought is silenced. The repeated mantra acts as a“resonance” which obliges the mind to relax and,maintaining alertness, to enter “profound levels”of interior consciousness. All one does is effor-tlessly think the mantra. The training is based onthe simplicity of the technique and the impor-tance of the absence of effort. The mantra in TMis personal: each person is assigned a lifelongmantra. This way it is meant to acquire a specialrelationship with the meditator and his particularexperiences.
Understanding the descriptions of the experien-ces that are produced in a meditative state is oftencomplicated by the use of unknown and untransla-table terms. For the desired scientific approach inEnglish of the fascinating subject of conscious-ness it is necessary that we forego as much as pos-sible the use of words in Sanskrit, Chinese,Japanese and other languages of cultures which dif-fer substantially from the occidental culture, andthat we try to capture as much as possible the sig-nificance of these more or less transcendentalterms in operative and consensual definitions.
1Mantra: invocation based upon a sound repeated many times. It may consist of just a vocalization such as“Oúmmm”; a single word such as “One” in the Relaxation Response; or have a text as in the Gayathri Mantra:
Om Bhur Bhuva Swaha Tat Savitur Varenyam Bhargo Devasya DheemahiDhiyo Yo Nah Prachodayat
Mother who subsists as all three Kalas (Lapses oftime: past, present and future), in all three Lokas (worldsor realms of experience), and all three Gunas (UniversalAttributes: harmony, agitation and inertness), I pray toyou to illuminate my intellect and dispel my ignorance,just as the splendorous sunlight dispels all darkness. Ipray to you to make my intellect serene and bright.
42 C. Med. Psicosom, Nº 105 - 2013

43C. Med. Psicosom, Nº 105 - 2013
MEDITATION AND SCIENTIFICRESEARCH
Consciousness is a subject for controlled scien -tific study, for which meditation has proven to befundamental (Shear & Jevning, 1999). In view ofthe subjective character of the subject of study,some combination of objective and subjectiveapproximations is necessary. Psychophysiologi -cal studies examine the correlations between men -tal tasks and phenomena on the one hand, and dif-ferent types of brain images and other physiolo-gical measures on the other. But those studiessuffer from a significant asymmetry. Althoughtheir objective side employs sophisticated scienti-fic methodology capable of identifying and eva-luating variables which are entirely outside ofordinary sensorial perception, their subjectiveside typically uses ordinary introspection and isthus able to identify ordinary internal phenomenasuch as sensorial perception, imagination and ver -bal thought. As a consequence, whilst the objec-tive side of consciousness is supported by sop-histicated scientific methodology, the subjectiveseems somewhat more Aristotelian and in need ofnew “first hand” systematic methodologies, thatis, bridging techniques between introspection andphysiological measurement, or between cogni-tion and observable reply, with guarantees as toreliability and validity. This asymmetry is soughtby integrating meditative procedures with modernobjective scientific methodologies such as EEG,EMG, PET and FMRI. There are many studieson meditation, of which the references cited hereare just a small sample and which confirm thatthe variety of meditative procedures are usefulcomponents for neurophysiology and psychology.
OBJECTIVE: REDUCE INTERFERENCE
Asiatic meditation traditions (Vedanta, Yoga,Buddhism, Taoism, Zen, and so on) affirm that itis possible to learn how to transcend the surfaceof human consciousness and gain systematicexperience of the matter, structure and dynamicsof consciousness under every human experience.They say that the direction of attention should be“inverted” and changed from its habitual orienta-tion towards the exterior (towards sensations,
thoughts, perceptions, and interior objects) toconsciousness itself. We usually consider sensa-tions and thoughts to be “internal occurrences” asopposed to “external” consciousness of the physi-cal world in general, a fundamental distinction forlearning to distinguish the public physical realityfrom the private mental reality. But in meditationthe notion “internal” is used in a much more radi-cal way. Here, even being aware of one’s mostprivate and internal thoughts and sensations isstill external for consciousness itself becausethey still appear in one’s consciousness, beforeone’s “mind’s eye” so to speak, and therefore the“internal” meditation referred to implies a com-plete inversion of attention, away from thoughtsand sensations and external objects and backwardsand inwards to consciousness itself, a perception“without objects”, a mental “Ganzfeld”.
Of course these explanations carry serious con -ceptual problems. In the first place, it is not easyto understand how one can redirect attention out-side of any thinking, perception and mental con-tent whilst practicing what really is a procedurelike meditation, which one must conceive andlearn. In the second place, the experiences produ-ced with this technique are supposedly comple-tely un-imaginable; in effect, this absolute unrea-chable description is a recurrent theme in the lite-rature on the matter. In the third place, doubtsexist as to the possibility of extrapolating ageneral use from this type of experience, productof other cultures. As Jung warned, any seriousattempt to integrate traditional meditation proce-dures and experiences into contemporary scienti-fic studies on consciousness, must find a solu-tion for these questions (Jung, 1943). But, inessence, there is nothing paradoxical in the no -tion of a procedure that could, in the first place,bring one’s total attention to a single point, tothen transcend this focus –out of tiredness,through relaxation or by maintained stimulation(sic)– thus causing a halt not only in conceptualattention but in all conceptual activity, demons-trating that it is possible to arrive at non-concep-tual mental presence. Training of both attentionand de-concentration produces better control ofthe constant interferences that are not cognitivelycontrollable and of a visceral origin, and thatmake the mind a noisy place where thinking with

clarity is difficult as is distinguishing the essen-tial from the casual.
EXPERIMENTAL INVESTIGATION ANDMEDITATION
A search in Pubmed with the term “medita-tion” produces some 2,500 references of publica-tions in listed medical journals since the begin-
ning of the 1970’s. Also, a sizeable number ofbooks have been published on the subject.Although many studies can be criticized as to themethodology used, others are of acceptable design.A review of the most relevant described results ofthe effects of meditation –in several formats– onhealth in general and some pathologies in particu-lar, identified some 40 fields of possible influence(Andresen, 2000). See examples in Table 1.
Tabl e 1So me effects attri buted to medi tati o n
Field of action Results Reference1. Blood pressure/heart rate Reduction Benson, Rosner &
Marzetta, 1973;Taylor & Farquher, 1977Hafner, 1982; Delmonte 1984b,Muskatel & Woolfolk, 1984Lukoff et al. , 1995;Wenneberg 1997Barnes et al. , 2001Vyas y Dikshit, 2002
2. Blood pressure – compared More reduction Kinsman & Staudenmayer,1978to progressive relaxation Warrenburg et al. ,1980;
Kamen, 1978; Schneideret al. , 1995
3. Myocardial ischemia Reduction Zamarra et al. , 19964. Cerebral blood flow Increase Jevning,Wilson et al. ,1978
Jevning et al. , 19965. Left forearm blood flow Increase Levander et al. , 19726. Electrodermal response Increase Allison 1971; Elson e
al. , 1977; Janby 1977;Laurie 1977;Curtis & Wessberg, 1975
7. Changes autonomous nervous system Yes Orme-Johnson 1973Orme-Johnson et al. , 1977Parker et al., 1978; Corby 1978Lazar et al. , 2000
8. Heart rate variability Improvement Sun et al. , 19869. Arousal reduction Fenwick, 198310. Depression reduction Carlin & Lee, 199711. Promotion of rehabilitation Poulet, 199612. Improvement asthma Honsberger & Wilson,
1973; Wilson, 1975Davis et al.1998;Manocha et al 2002
13. Stuttering improvement McIntyre & Silverman,1974
44 C. Med. Psicosom, Nº 105 - 2013

14. Insomnia improvement Miskiman 1977 a,b;Jacobs, Benson &Friedman, 1993Jacobs, Rosenberget al. , 1993
15. Plasma prolactin and growth hormone Increase Jevning, Wilson & Vanderlaan, 1978
16. Palliative care Support Cole, 199717. Cancer, convalescence Support Gross, 1994; Simon, 199918. Mourning processes Support Edwards, 199719. Psychological health Improvement Linden, 1971;
Hjelle, 1974;Ferguson, 1980 (review)
20. Anxiety reduction Girodo, 1974; Otis, 1974;Daniels, 1975; Dillbeck,1977; Puryear & Cayce,1976; Lazar et al. , 1977;Schwartz et al. ,1978,1984Bahrke & Morgan, 1978Boswell & Murray, 1979Goleman et al. , 1979Lintel, 1980;Delmonte, 1985Eppley et al. ,1989;Sakairi,1992Miller et al. ,1995Barnes et al. , 2001
21. Fear of public speaking Reduction Kirsch & Henry, 197921. Fear of Magnetic Resonance Tests Reduction Thompson & Coppens,
1994; Lukins et al. , 1997Quirk et al. ,1989
22. Dominant tendency Reduction Fehr, 199623. Inflammation Reduction Klemons, 197724. Physiologic variables of age Improvement Wallace et al. , 198225. Effect of stress on immune system Modification Solberg et al. ,199526. Chronic pain Reduction Kabat-Zinn, 1982, 1990
Kabat-Zinn et al,1985Collura y Kabat-Zinn, 1997
27. Substance abuse Reduction Robins, 1969; Marzetta etal. , 1972; Wallace, 1972;Shafii 1974, 1975Lazar et al. , 1977; Klajner1984; Marlatt & Pagano,984; Alexander, Robinson& Rainforth 1994
28. Alcohol consumption Reduction Benson, 1974; Brautigam,1977; Alexander, Robinson& Rainforth 1994
45C. Med. Psicosom, Nº 105 - 2013

OTHER MEDITATION-PHISIOLOGYCORRELATIONS
Apart from the effects reflected in Table 1,there are several significant special correlationsthat we shall comment on as follows.
1. RespirationThe extensive scientific research on medita-
tion of the past 30 years started with the evalua-tion of some of the traditional revindications ofspecific physiologic correlates of the “pure cons-ciousness experience”. One persistent transcultu-ral revindication, encountered in Yoga, Vedanta,Taoism, Zen and other texts, is that the expe-rience is not only accompanied by a significantreduction of metabolic activity but also by thecessation of a normal respiratory activity of inha-ling and exhaling. Early Zen meditation studiesshowed a decrease in the respiration rate and oxy-gen consumption (Sugi & Akutsu, 1968). Re -sults obtained with TM led Austin to the conclu-sion that respiration is the most significant varia-ble to study “meditation from the viewpoint ofits basic physiologic mechanisms” (Austin, 1998,p.XX).
Contemporary studies reveal a significant co -rrelation between periods of complete respiratorysuspension and episodes of “pure consciousness”as informed by subjects that practiced TM techni-ques (Badawi et al., 1984). Some biochemical in -
dicators of metabolic activity were significantlylowered to cellular, tissue and corporal levels du -ring entire periods of meditation by experimentedmeditators. These studies also reflected a correla-tion between episodes of experiences of “pureconsciousness” and physiologic parameters thatdiffer from the ones mentioned or proposed bytraditional literature, such as a commonly eleva-ted inter-hemispheric EEG coherence (Travis yWallace, 1997). This “respiration suspension” re -fers to episodes of a respiration with predomi-nantly vertical pneumotachygraphic traces, signsof an in principle normal respiration, althoughslightly slower than normal, which is suddenlyinterrupted by a suspension of normal respirationwith straight horizontal traces for periods ofapproximately half a minute (Farrow & Herbert,1982). Thus, what is called suspension of respi-ration indicates here the absence of detectable nor-mal inhalation and exhalation; nevertheless, theairflow does not stop completely but continuesthanks to a fibrillation of the lungs with ordina-rily undetectable low amplitude of 2-7 Hz, whichcan be registered by Fourier analysis. The neu-rophysiologist James Austin concluded that thesestudies with subjects that practice TM connectthe transparent consciousness, free of thought,with two very different groups of physiologicevidence. The fact which impresses most is thesuspension of the respiratory impulse which cau-ses a relative hypoventilation (with “respiratory
29. Tension, guiltiness, addiction Reduction Carrington 1977, 1978,1979, 1984a,b, 1987
30. Violent deaths in communities Reduction Assimakis & Dillbeck,1995
31. Retarded ejaculation Improvement Delmonte, 1984a32. Basal and medial cortisol Reduction Maclean et al. , 1997
Michaels et al. , 197933. Affect disorders Relapse prevention Austin, 1997
Johnson y White, 197134. Sympathetic nervous system Activity reduction Brown et al. , 1984 a,b;
Delmonte, 198935. Metabolism Changes Wallace, todos; Benson, todos;
Fenwick et al.197736. Distal temperature Increase up to 8,3º C. Benson, 1982;
Benson et al. , 1982
46 C. Med. Psicosom, Nº 105 - 2013

47C. Med. Psicosom, Nº 105 - 2013
arrests” with posterior non-compensating extrabreathing). The second group of associated fin-dings is more subtle and variable. It includes auto-nomous peripheral changes and tendencies towardsan increased EEG coherence. Austin ob served alsothat short moments, transparent and silently cons-cious like these, are not merely indicative of slee-piness before falling asleep. On the contrary, whenwe are sleepy, the signs are a su perficial abdominalrespiration, slow times of cognition and reaction,and flatter Alpha waves in our EEG (none of thesecharacterize the experience referred to here). Neithercan anyone voluntarily produce similar momentsof mental clarity, whilst withholding respiration(Austin, 1998, p.97). The respiration studies withTM meditators could avoid certain specific metho-dological problems. The technique is standardized,memorized in a few hours, and does not implyattention to physiological processes. The result isan am ple availability of adequate experimentalsubjects. In general, the studies performed withother types of meditation confirm the resultsreflected here (Vyas & Dikshit, 2002).
Another type of study, carried out with TMsubjects, serves to better understand these results.Wallace (Wallace et al, 1971) noted a decrease inoxygen consumption (O2) and in the eliminationof carbon dioxide (CO2) without a change in therespiration coefficient during meditation periodsof thirty minutes. A decrease in oxygen consump -tion in the absence of a change in the breathingcoefficient is a sign of having reached a state ofrelaxation without manipulation of the respira-tion. When more “long-term” meditators (at least5 years of practice) became available, more sop-histicated respiration studies were performed. Forexample, Farrow & Herbert (1982), report a 40-50% decrease in respiration as well as a high co -rrelation of breathing suspensions with the subjec-tive experience of “pure consciousness”, referred toearlier. The same authors also compared breathingrates with ordinary relaxation with the eyes closed,and with TM meditation. They found significantslowing in respiration during TM and no signifi-cant changes during ordinary relaxation, results thatwere confirmed by Wolkove et al (1984).
2. MetabolismThe mentioned studies as to entire-body level
are complemented with studies as to organ levels.Meditation produces changes, both increases anddecreases, in the metabolism (Benson et al,1990). Blood flow studies measured greater chan-ges in the dependent values of respiration and O2
consumption in organs and metabolism, than inthe whole body. With diluted coloring and measu-res of radioactive separation of blood flow, a ge -neral relaxation of blood vessels was identified,as well as specific circulatory changes such as areduced blood flow in liver and kidneys (Jevninget al., 1978 a). A later study by the same authorsshowed that a lot of the decrease in O2 consump-tion of the whole body in meditation was due toa reduced metabolism of the skeletal muscles andalso revealed a direct relaxation of individual tis-sues (Jevning et al., 1983a). Significant differen-ces were found with the effects of common rela-xation, for instance in a study that found an in -crease in blood flow of 15-20% in the frontal andoccipital brain regions during meditation (Jev -ning et al., 1996). These studies on the level ofthe whole body and of the organs have been com-plemented with in-depth studies at tissue and ce -llular levels. One of these reports reveals the ces-sation of CO2 generation by the skeletal muscleof the forearm (Wilson et al., 1987). The meta-bolism of red blood cells decreases, an effect thatimplies that during meditation circulating chemi-cal compounds are produced which modulatecellular activity (Jevning et al., 1983b). A decre-ase was also seen in the thyroid stimulating hor-mone (TSH), another sign of a lesser metabolicexcitation (Jevning et al., 1987). Plasma corti-sol, an indicator of stress, decreased with long-term practice of meditation but not with short-term meditation and neither during ordinary rela-xation (Jevning et al., 1978b).
3. Brain activityAlthough the majority of the mentioned phy-
siological processes experience a decrease, thecentral nervous activity increases with medita-tion, as shown by EEG, the sensorimotor res-ponse, brain blood flow data and magnetic reso-nance images (Banquet & Sailhan, 1974; Jevninget al., 1987; Lang et al., 1979, Travis & Orme-Johnson 1990, Lazar et al., 2000) as well as bythe subjective reports of “pure consciousness” as

a level of increased instead of decreased alertness(Jevning, 1988; Jevning et al. , 1996), withwhich the meditative state distinguishes itselfclearly from a state of relaxation or sleep.Effectively, the main part of the changes in hor-monal and neurotransmitter concentration, cellu-lar metabolism and in organs, and the respiratoryfunction that accompany TM, differ from theirlevels during sleep or common relaxation. In astudy of the effects of certain drugs with centralactivity (diazepam, naloxone and flumazenil) onthe EEG during meditation, it was observed thatthe changes observed in the EEG during medita-tion were not causally related to the changes onaccount of the presence of endogenous opioids orsubstances similar to benzodiazepines, producedby the brain (Sim & Tsoi, 1992). Some measu-res, such as the respiration rate or EEG cohe-rence, are directly correlated with self-informedexperiences of “pure consciousness”. Others arenot sufficiently sensitive in time to be correlatedwith the episodes of “pure consciousness” astypically informed (of up to a minute, approxi-mately) but still indicate that the meditative pro-cedure generates a physiology that is characteris-tic at cellular, tissue, organ or entire body level.As a whole, these experimental data prove thatboth physiological and cognitive effects of ameditation technique are to be considered signifi-cantly distinguishable from the effects of relaxa-tion techniques.
CONCLUSION. CLINICAL USE OFMEDITATION
Experimental data indicate that meditationproduces a relaxation of the body and a particularactivation of the mind. Practicing this contem-plative technique may reduce the levels of stress,more than habitual relaxation techniques. Mo -reover, it appears to be an efficient technique tocontrol chaotic repetitive thinking –“monkeychatter”– so apt at diminishing both cognitivecapacity and emotional balance. With meditationone can learn to not pay attention to these uncon-trolled and noxious stimuli, and gain mental cla-rity but also –and probably more importantly–gain the confidence to be able to handle thoseinterferences. Automatic thoughts, even when not
negative by themselves but simply unsettling orun-coordinating, absorb much emotional energyand induce mood changes by giving a sensationof lack of control or even chaos, a sensation ofbeing at the mercy of this invasion of “mentalnoise”.
Apart from supplying us with specific data asto physiological characteristics of the humanmind, studies on meditation indicate one or seve-ral base-lines of utility in psychiatry and clinicalpsychology, as well as in certain medical pro-blems. They guide us towards new and non-phar-macological methods with which to promote fun-damental changes in the unbalances that underliethose manifestations we clinically qualify as“disorders”. Modern medication helps to controlthose symptoms and ever-more –specific psychot-herapies improve basic problems but, on top ofthese, disciplines are needed to improve the rela-tionship of a person with him– or herself. Ampleexperimental evidence shows that meditation isone such discipline and, thus, we may ask whyits use is not more extended. Since 1996, theNational Institute of Health of the United Statesrecommends doctors to accept meditation as anefficacious treatment for chronic pain, anxiety,panic attacks, insomnia, premenstrual syndromeand infertility (Carlin & Lee, 1997). In Spainmeditation may be labeled as something “mystic”or related to religions other than the Christianfaith, therewith resulting in a limited acceptanceof this non-religious and non-mystic techniquethat, moreover, has been practiced in Christianfaith for hundreds of years. It is time to acceptthe evidence that meditation may be clinicallyuseful in determined psychopathologies, as wellas being an instrument for improving psycholo-gical health.
Graph 1
48 C. Med. Psicosom, Nº 105 - 2013

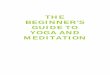
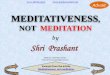
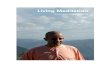
EEG IN MEDITATION (J.P. BANQUET,1973) GRAPH 1
Plots of EEG amplitude integrals in 4 diffe-rent frequency ranges: delta 0-3, theta 4-7, alpha8-14, beta and rapid frequencies 15-50 c/sec. X=time in units of 2,5 seconds. Y= relative abun-dance of each frequency range in total percentage.Each line is an upper limit to the surface thereun-der and moreover a lower limit to the surfaceabove. The delta and beta ranges have a horizon-tal axis for exterior limits. The areas betweenlines (but not between lines and the X axis) re -present the integration surfaces of each frequencyrange in proportion of its abundance. R1: Con -trol subject in relaxation. The presence of alphaactivity localizes him in the alpha plus group.R2: Control subject with hardly any alpha acti-vity. The isolated delta peak in the middle of thefigure is more an artifact or a movement than asomnolence period. M1: meditator in state of re -laxation just before meditation. Note the superiorquantity of alpha and theta compared to controls.M2: the same subject during the first phase ofmeditation. First the alpha range widens, then theslow activity increases dramatically and its betarange decreases. M3: the same subject after medi-tation in a period of concentration. There is animportant remainder of alpha and a beta peak inthe middle of the figure. The relative quantities ofthe different frequencies in meditators maintaincertain stability during the changes from medita-tion to other states of consciousness.
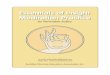
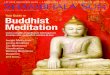
GRAPH 2
A and B are the same recording at different mo -ments of meditation. In B one can observe the in -
crease in alpha amplitude in all channels and theappearance of alpha waves in F3. C represents thechange from alpha to a disorganized pattern domi-nated by beta. The change is successively seen inF3, C3, and O1 at the left and later at the right.
BIBLIOGRAFÍA
1. Al ex ander CN, Dav i es JL, Di x o n CA,Di l beck MC, Druker SM, Oetze l RM,Muehl man JM, Orme-Jo hns o n DW. :Growth of higher stages of consciousness:Maharishi’s Vedic Psychology of human deve-lopment’, in: Higher Stages of Human Deve -lopment, Alexander CN y Langer EH(eds) NewYork: Oxford Univ. Press, 1990.
2. Al ex ander CN, Ro bi ns o n P, Orme-Jo hn -so n DW, Schnei der RH, Wal to n KG. : Theeffects of transcendental meditation comparedto other methods of relaxation and meditationin reducing risk factors, morbidity, and morta-lity. Homeostasis, 1994; 35(4-5): 243-63.
3. Al ex ander CN, Ro bi ns o n P, Rai nfo rthM. : Treating and preventing alcohol, nicoti -ne, and drug abuse through transcendental me -ditation: a review and statistical meta-analysis.Alcohol Treatment Quarterly, 1994; 11: 13-87.
4. Al l i s o n J. : Respiratory changes during trans-cendental meditation. Lancet 1, 1971; (7651), 883.
5. As s i maki s PD, Di l l beck MC. : Time seriesanalysis of improved quality of life in Canada:social change, collective consciousness, andthe TMSidhi program. Psychological Reports,1995; 76 (3Pt.2): 1171-93.
6. Aus t i n JA. : Stress reduction through mind-fulnes meditation. Effects on psychological symp -tomatology, sense of control, and spiritualexperiences. Psychotherapy & Psychosomatics,1997; 66(2): 97-106.
7. Aus t i n JH. : Zen and the Brain. Cambridge,MA: MIT Press, 1998.
8. Badawi K, Wal lace R, Orme-Johnson D, etal : Electrophysiologic characteristics of res-piratory suspension periods ocurring duringthe practice of the trascendental meditationprogram. Psychosomatic Medicine, 1984; 46,pp 267-76.
9. Bahrke MS, Morgan WP. : Anxiety reductionfollowing exercise and meditation. CognitiveTherapy and Research, 1978; 2, 323-33.
10. Banquet JP. : Spectral Analysis of the EEG inMeditation. Electroencephalography and Clini -cal Neurophysiology, 1973; 35, pp.143-51.
Graph 2
49C. Med. Psicosom, Nº 105 - 2013

11. Banquet JP, Sai l han M. : EEG analysis ofspontaneous and induced states of conscious-ness. Rev. Electroencephalogr. Neurophysiol.Clin, 1974; 4, pp. 445-54.
12. Barnes VA, Treiber FA, Dav i s H. : Impact oftranscendental meditation on cardiovascularfunction at rest and during acute stress in ado-lescents with high normal blood pressure. JPsychosom Res 2001; Oct; 51(4): 597-605.
13. Bens o n H. : Decreased alcohol intake asso-ciated with the practice of meditation: a retros-pective investigation. Ann NY Acad Sciences,1974; 233:174-7.
14. Bens o n H. : The Relaxation Response. NewYork: Morrow, 1975.
15. Bens o n H. : Body temperature changes duringthe practice of gTum-mo Yoga (MattersArising) Nature, 1982; 298: 402.
16. Bens o n H, Lehmann JW, Mal ho tg ra MS,Go l dman RF, Ho pki ns J, Eps te i n MD. :Body temperature changes during the practiceof gTum-mo Yoga. Nature, 1982; 295(5846):234-6.
17. Bens o n H, Mal ho tra MS, Go l dman RF,Jaco bs GD, Ho pki ns PJ. : Three case reportsof the metabolic and electroencephalographicchanges during advanced Buddhist meditationtechniques. Behav. Med. 1990; 16(2): 90-5.
18. Bens o n H, Ro s ner BA, Marzetta BR. :Decreased Blood Pressure in Hypertensive Sub -jects who Practised Meditation. J Clin Inv,1973; 52, p.8a.
19. Bo s wel l PC, Murray EJ. : Effects of medita-tion on psychological and physiological mea-sures of anxiety. J Consulting and ClinicalPsychology, 1979; 487: 606-7.
20. Brauti g am E. : Effects of transcendental me -ditation program on drug abusers: a prospecti -ve study, in: Scientific Research on the Trans -cendental Meditation Program: Collected Pa -pers, ed. D.W. Orme-Johnson & J.T. Farrow, 2ªEd. Weggis: Maharishi European Research Uni -versity Press, 1977.
21. Brown DP, Forte M, Dysart M. : Differencesin visual sensitivity among mindfulness medi-tators and non-meditators. Perceptual & MotorSkills, 1984a; 58(3): 727-33.
22. Brown DP, Forte M, Dysart M. : Visual sen -sitivity and mindfulness meditation. Percep -tual & Motor Skills, 1984b; 58:775-84.
23. Carlin P, Lee K. : Treat the body, health themind. Health, 1997; 11(1), 72-8.
24. Carri ng to n P. : Freedom in meditation. NewYork: Doubleday, 1977.
25. Carri ng to n P. : Clinically standardized medi-tation: Instructor’s Kit. Laurel, MD: Pace Edu -cational Systems, 1978.
26. Carri ng to n P. : Clinically standardized medi-tation: Instructor’s Manual. Laurel, MD: PaceEducational Press, 1979.
27. Carri ng to n P. : Modern forms of meditation,en: Principles and Practice of Stress Mana -gement, Woolfolk & Lehrer. New York:Guilford Press, 1984a.
28. Carri ng to n P. : Releasing. New York: Double -day, 1984b.
29. Carri ng to n P. : Managing meditation in cli-nical practice, en: The Psychology ofMeditation. Oxford: Clarendon Press, 1987.
30. Co l e R. : Meditation in palliative care - apracticed tool for self-management. PalliativeMed, 1997; 11(5), 411-3.
31. Co l l ura J & Kabat-Zi nn J. : The Zen ofPain Control: learning to let go of what ailsyou. Vegetarian Times, 1997; 233: 28-30.
32. Co rby JC, Ro th WT, Zarco ne J, Ko pel lBS. : Psychophysiological correlates of thepractice of tantric yoga meditation. Arch GenPsychiat, 1978; 35(5), 571-7.
33. Curt i s DW & Wes s berg HW. : A compari-son of heart rate, respiration, and galvanicskin response among meditators, relaxers, andcontrols. J Altered States of Consciousness,1975; 2, 319-24.
34. Dal ai Lama & Al ex ander Berzi n. : The Ge -lug/ Kagyü Tradition of Mahamudra. Ithaca:Snow Lion, 1997.
35. Dani e l s LK. : The treatment of psychophy-siological disorders and severe anxiety bybehavior therapy, hypnosis, and transcenden-tal meditation. Am J Clin Hypnosis, 1975; 17,267-9.
36. Dav i s PA, Go l d EB, Hackman RM, SternJS, Gers hwi n ME. : The use of complemen-tary/alternative medicine for the treatment ofasthma in the United States. J Investig Aller -gol Clin Immunol. 1998 Mar-Apr; 8(2): 73-7.
37. Del mo nte MM. : Case reports on the use ofmeditative relaxation as an intervention stra-tegy with retarded ejaculation. Biofeedback &Self Regulation, 1984a; 9(2): 209-14.
38. Del mo nte MM. : Physiological responses du -ring meditation and rest. Biofeedback and Self-Regulation, 1984b; 9(2),181-200.
39. Del mo nte MM. : Meditation and anxiety re -duction: a literature review. Clin Psychol Rev,1985; 5: 91-102.
40. Delmonte MM. : Meditation, the unconscious,
C. Med. Psicosom, Nº 105 - 201350

and psychosomatic disorders(review) Int J Psy -chosomatics, 1989; 36 (1-4): 45-52.
41. Di l l beck M. : The effect of the transcendentalmeditation technique on anxiety level. J ClinPsychol, 1977; 33, 1076-8.
42. Edwards M. : Being present: experientialconnections between zen buddhist practicesand the grieving process. Disability & Reha -bilitation, 1997; 19(10), 442-51.
43. Elson BD, Hauri P, Cunis D. : Physiologicalchanges in yoga meditation. Psychophysiolo -gy, 1977; 14(1), 52-7.
44. Eppl ey KR, Abrams AI, Shear J. : Differen -tial effects of relaxation techniques on trait an -xiety: a meta analysis. J Clin Psychol, 1989;45(6): 957-74.
45. Farro w JT & Herbert R. : Breath suspen-sion during the trascendental meditation tech-nique. Psychosom. Med., 1982; 44(2), pp.133-53.
46. Fehr TG. : Therapeutische relevante Effektedurch transzendentale Meditation? Psychothe -rapie, Psychosomatik, Medizinische Psycholo -gie, 1996; 46 (5): 178-88.
47. Fenwi ck PBC, Do nal ds o n S , Gi l l i s L,Bus hman J, Fento n GW, Perry I, Ti l s l eyC, S e raf i n o wi c z H. : Metabolic and EEGchanges during trascendental meditation. Biol.Psychol., 1977; 5, pp.101-18.
48. Fenwi ck P. : Can we still recommend medita-tion? (Ed.) Br Med J (Clinical research ed), 1983;287 (6403), 1401.
49. Ferg us o n P. : An integrative meta-analysis ofpsychological studies investigating the treat-ment outcomes of meditation studies. Disser -tation Abstracts International, 1980; 42(4-A),1547.
50. Fo rman R. : The Problem of Pure Conscio -usness. Oxford: Oxford Univ.Press, 1990.
51. Gel l ho rn E & Ki el y W. : Mystical States ofConsciousness: Neurophysiological and Clini -cal Aspects. J Nervous and Mental Disease,1972; Vol. 154,6, pp. 399-405.
52. Gi ro do M. : Yoga meditation and flooding inthe treatment of anxiety neurosis. J BehaviorTherapy and Experimental Psychiatry, 1974;5: 157-60.
53. Goleman BL, Doitor PJ, Murray EJ. : Effectsof zen meditation on anxiety reduction and per-ceptual functioning. J Consulting and ClinicalPsychology, 1979; 47: 551-6.
54. Gro s s S . : Surviving cancer: Mind & Body.New Orleans Magazine, 1994; 29(1), 62-7.
55. Hafner RJ. : Psychological treatment of essen-
tial hypertension: a controlled comparison ofmeditation and meditation plus biofeedback.Biofeedback and Self-Regulation, 1982; 7:305-16.
56. Hjel l e LA. : Transcendental meditation and psy -chological health. Perceptual & Motor Skills,1974; 39: 623-8.
57. Honsberger RW & Wilson AF. : Transcenden -tal meditation in treating asthma. RespiratoryTherapy: Journal of Inhalation Technology,1973; 3: 79-81.
58. Jacobs GD, Benson H, Friedman R. : Home-based central nervous system assessment of amultifactor behavioral intervention for chro-nic sleep-onset insomnia. Behavior, 1993;Ther 24: 159-74.
59. Jacobs GD, Rosenberg PA, Friedman, Ma -thes o n J, Guerry PM, Do mar AD, Bens o nH. : Multifactor behavioral treatment of chro-nic sleep-onset insomnia using stimulus con-trol and the relaxation response: a preliminarystudy. Behavior Modification, 1993; 17, 498-509.
60. James W. : The Principles of Psychology. NewYork: Dover, 1890/1950.
61. Janby J. : Immediate effects of the transcen-dental meditation technique: Increased skin re -sistance during the first meditation after ins-truction, en: Scientific Research on the Trans -cendental Meditation Program: Collected Papers,ed. D.W. Orme-Johnson & J.T. Farrow, 2ª Ed.Weggis: Maharishi European Research Univer -sity Press, 1977.
62. Jev ni ng R, Wi l s o n AF, Smi th WR, Mo r -to n ME. : Redistribution of blood flow inacute hypometabolic behavior. Am. J. Physiol.,1978a; 235(1), R89-R92.
63. Jev ni ng R, Wi l s o n AF, Dav i ds o n JM. :Adenocortical activity during meditation. Horm.And Behavior, 1978b; 40, pp.54-60.
64. Jev ni ng R, Wi l s o n AF, Vanderl aan EF. :Plasma prolactin and growth hormone duringmeditation. Psychosom Med, 1978; 40: 329-33.
65. Jev ni ng R, Wi l s o n AF, O’Hal l o ran JP,Wal s h RN. : Forearm blood flow and metabo-lism during stylized and unstylized states ofdecreased activation. Am. J. Physiol. , 1983a;245, R110-R116.
66. Jevning R, Wilson AF, Pirkle H, O’Hal lo -ran JP, Wal s h RN. : Metabolic control in astate of decreased activation: Modulation of redcell metabolism. Am. J. Physiol. 1983b; 245,Cell Phys, 14, C457-C461.
67. Jevning R, Wells I, Wilson AF. : Plasma thy-
C. Med. Psicosom, Nº 105 - 2013 51

roid hormones, thyroid stimulating hormone,and insulin during acute hypometabolic statesin man. Physiol. and Behavior, 1987; 40, pp.603-6.
68. Jev ni ng R. : Integrated metabolic regulationduring states of decreased metabolism, simila-rity to fasting: A biochemical hypothesis.Physiol. and Behavior, 1988; 43, pp.735-7.
69. Jev ni ng R, Anand R, Bi edebach M, Fer -nando G. : Effects on regional cerebral bloodflow of transcendental meditation. Physiol.andBehavior, 1996; 59(3), 399-402.
70. Jo hns o n SS & Whi te G. : Self-observationas an agent of behavioral change. Behavior,1971; Ther 2: 488-97.
71. Jung CG. : Collected Works, Vol.11: The Psy -chology of Eastern Meditation. Princeton, NJ:Princeton University Press, 1943.
72. Kabat-Zi nn J. : An out-patient program inbehavioral medicine for chronic pain patientsbased on the practice of mindfulness medita-tion: theoretical considerations and prelimi-nary results. Gen Hosp Psychiatry, 1982; 4:33-47.
73. Kabat-Zi nn J. : Full catastrophe living: usingthe wisdom of your body and mind to facestress, pain, and illness. New York: DelacortePress, 1990.
74. Kabat-Zi nn J, Li pwo rth L, Burney R. :The clinical use of mindfulness mediation forthe selfregulation of chronic pain. J BehaviorMed, 1985; 8: 163-190.
75. Kamen R. : Biofeedback and meditation effectsmuscle tension and locus of control. Perceptual& Motor Skills, 1978; 46: 955-8.
76. Ki ns man RA & Staudenmay er H. : Base -line levels in muscle relaxation training. Bio -feedback and Self-Regulation, 1978; 3: 97-104.
77. Ki rs ch I & Henry D. : Self-desensitizationand meditation in the reduction of public spea-king anxiety. J Consulting and Clinical Psycho -logy, 1979; 47: 536-41.
78. Klajner F, Hartman LM, Sobel l MB. : Treat -ment of substance abuse by relaxation training:a review of the literature. Addictive Behaviors,1984; 9: 41-45.
79. Kl emo ns IM. : Changes in inflammation inpersons practicing the transcendental medita-tion technique, in: Scientific Research on theTranscendental Meditation Program: CollectedPapers, ed. D.W. Orme-Johnson & J. T. Farrow,2ªEd. Weggis: Maharishi European ResearchUniversity Press, 1977.
80. Lang R, Deho f K, Meurer KA, Kaufman
W. : Sympathetic activity and trascendentalmeditation. J. Neural. Transm, 1979; 44, pp.117-35.
81. Lauri e G. : An investigation into the changesin skin resistance during the transcendentalmeditation technique, in: Scientific Researchon the Transcendental Meditation Program:Collected Papers, ed. D.W. Orme-Johnson &J.T. Farrow, 2ª Ed. Weggis: Maharishi EuropeanResearch University Press, 1977.
82. Lazar Z, Farwel l L, Farro w JT. : Effects oftranscendental meditation program on anxiety,drug abuse, cigarette smoking and alcohol con-sumption, in: Scientific Research on theTranscendental Meditation Program: CollectedPapers, ed. D.W. Orme-Johnson & J.T. Farrow,2ªEd. Weggis: Maharishi European ResearchUniversity Press, 1977.
83. Lazar SW, Bus h G, Go l l ub RL, Fri cchi o -ne GL, Khal s a G, Bens o n H. : Functionalbrain mapping of the relaxation response andmeditation. Neuroreport 2000 May 15; 11(7):1581-5.
84. Levander VL, Benson H, Wheeler RC, Wa -l l ace RK. : Increased forearm blood flow du -ring a wakeful hypometabolic state. Fed Proc,1972; 31: 405.
85. Li nden W. : Practicing of meditation by schoolchildren and their levels of fields dependence-independence, test anxiety, and reading achie-vement. J Consulting and Clinical Psycholo -gy, 1971; 41: 139-43.
86. Li ntel AG. : Physiological anxiety responsesin transcendental meditators and non-medita-tors. Perceptual & Motor Skills, 1980; 50:295-300.
87. Luki ns R, Dav an IG, Drummo nd PD. : Acognitive behavioural approach to preventinganxiety during magnetic resonance imaging. JBehavior Therapy & Experimental Psychiatry,1997; 28(2): 97-104.
88. Luko ff D, Lu FG, Turner R. : Cultural con-siderations in the assessment and treatment ofreligious and spiritual problems. PsychiatrClin North Am. 1995 Sep;18(3): 467-85.
89. Lu K’uan, Yu (Charl es Luk). : Ch’an and ZenTeaching. London:Rider & Co, 1961.
90. Maclean CR, Wal ton KG, Wenneberg SR,Levitsky DK, Mandarino JP, Waxiri R, Hi -l l i s SL, Schnei der RH. : Effects of the trans -cendental meditation program on adaptive me -chanism: changes in hormone leves and res-ponses to stress after 4 months of practice. Psy-choneuroendocrinology, 1997; 22(4): 277-95.
C. Med. Psicosom, Nº 105 - 201352

91. Mano cha R, Marks GB, Kenchi ng to n P,Peters D, Sal o me CM. : Sahaja yoga in themanagement of moderate to severe asthma: arandomised controlled trial. Thorax 2002 Feb;57(2): 110-5.
92. Marl att CA & Pag ano RR. : Effects of medi-tation and relaxation training upon alcohol usein male social drinkers, en: Meditation: Cla -ssic and Contemporary Perspectives, ed. J Sha -piro, Deane H, Walsh RN. New York: Aldine Pu -blishing Co., 1984.
93. Marzetta BR, Bens o n H, Wal l ace RK. :Combatting drug dependency in young people:a new approach. Counterpoint, 1972; 4: 13-36.
94. McInty re ME & Si l v erman FH. : Transcen -dental Meditation and stuttering: a preliminaryreport. Perceptual & Motor Skills, 1974; 39:294.
95. Mi chael s RR, Parra J, McCann DS, Van -der AJ. : Renin, cortisol, and aldosterone duringtranscendental meditation. Psychosomatic Medi -cine, 1979; 41(1): 50-4.
96. Mi l l er JJ, Fl etcher K, Kabat-Zi nn J. : 3Year follow-up and clinical implications of amindfulness meditation-based stress reductionintervention in the treatment of anxiety disor-ders. Gen Hosp Psychiatry, 1995; 17: 192-200.
97. Mi s k i man DE. : Long term effects of thetranscendental meditation program in the treat-ment of insomnia, in: Scientific Research onthe Transcendental Meditation Program: Collec -ted Papers, ed. D.W. Orme-Johnson & J.T.Farrow, 2ª Ed. Weggis: Maharishi European Re -search University Press, 1977a.
98. Mi s ki man DE. : The treatment of insomnia bytranscendental meditation program, in: Scien -tific Research on the Transcendental Medita -tion Program: Collected Papers, ed. D.W. Or -me-Johnson & J.T. Farrow, 2ª Ed. Weggis: Ma -harishi European Research University Press,1977b.
99. Mus katel N & Wo o l fo l k RL. : Effect of me -ditation training on aspects of coronary-pronebehavior. Perceptual & Motor Skills, 1984;58: 515-8.
100. Orme-Jo hns o n DW. : 1973 Autonomic stabi -lity and transcendental meditation. PsychosomMed, 1984; 16: 203-9.
101. Orme-Johnson DW, Kiehlbauch J, MooreR. : Personality and autonomic changes inprisoners practising the transcendental medi-tation technique, en: Scientific Research on theTranscendental Meditation Program: Collected
Papers, ed. D.W.Orme-Johnson & J.T.Farrow,2ª Ed. Weggis: Maharishi European ResearchUniversity Press.
102. Oti s L. : The facts on transcendental medita-tion: if well integrated, but anxious, try TM.Psychology Today, 1974; 7: 45-6.
103. Padasambhava Natural Liberation: Padma -sambhava’s Teachings on the Six Bardos, comm.Gyatrul Rinpoche, trad. B. Alan Wallace. Boston,MA: Wisdom, 1998.
104. Parker JC, Gi l bert GS, Tho res o n RW. :Reduction of autonomic arousal in alcoholics:a comparison of relaxation and meditation tech -niques. J Consulting and Clinical Psycholo -gy, 1978; 46: 879-85.
105. Peng CK, Mi etus JE, Li u Y, Khal s a G,Do ug l as PS, Bens o n H, Go l dberg er AI. :Exaggerated Heart Rate Oscillations duringTwo Meditation Techniques. Int J of Cardiolo -gy, 1999; 70, pp. 101-7.
106. Po s ner MI. : Chronometric Exploration ofMind. Lawrence Erlbaum Ass, 1878.
107. Po ul et R. : Entspannungstechniken in derRehabilitation. Z Gastroenterologie, 1996;34(suppl2), 80-4.
108. Puryear H, Cayce C. : Anxiety reduction asso -ciated with meditation: home study. Perceptual& Motor Skills, 1976; 43: 527-31.
109. Qui rk ME, Letendre AJ, Ci o t to ne RA,Li ng l ey JF. : Evaluation of three psycholo-gic interventions to reduce anxiety during MRimaging. Radiology, 1989; 173(3): 759-623.
110. Ro bbi ns T. : Eastern Mysticism and the reso-cialization of drug users: the meher baba cult.J Scientific Study Religion 8: 308-17, 1969.
111. Sakai ri Y. : Effects of transcendental medita-tion in reducing anxiety of japanese business-men, in: Perspectives on Relaxation and Me -ditation, ed.M. Blows y S. Srinivasan. Mel -bourne: Spectrum Publishers, 1992.
112. Schnei der RH, Stag g ers F, Al ex anderCN, Sheppard W, Rai nfo rth M, Ko nd -wani K, Smi th S , Ki ng CG. : A randomi-zed controlled trial of stress reduction for hy -pertension in older african americans. Hyper -tension, 1995; 26: 820-7.
113. Schwartz GE, Dav i ds o n RJ, Go l eman D. :Patterning of cognitive and somatic processesin the self-regulation of anxiety: effects ofmeditation versus exercise. Psychosom Med,1978; 40(4): 321-8.
114. Schwartz GE, Dav i ds o n RJ, Go l emanDJ. : Patterning of cognitive and somatic pro-cesses in the selfregulation of anxiety: effects
C. Med. Psicosom, Nº 105 - 2013 53

of meditation versus exercise, in: Meditation:Classic and Contemporary Perspectives, eds.J. Shapiro, Deane H, Walsh RN. Hawthorne:Aldine Publishing Co, 1984.
115. Shaf i i M, Lav el y RA, Jaffe R. : Medita -tion and marijuana. Am J Psychiatry, 1974;131(1): 60-3.
116. Shaf i i M, Lav el y RA, Jaffe R. : Medita -tion and the prevention of alcohol abuse. AmJ Psychiatry, 1975; 132(9): 942-5.
117. Shear J. : Ethics and the experience of happi-nes, in: Crossing Boundaries: Ethics, antino-mianism and the history of mysticism, ed. G.William Barnard and Jeffrey J. Kirpal. NewYork: SUNY Press, 1999.
118. Shear J, Jev ni ng R. : Journal of Conscious -ness Studies, 1999; 6, no 2-3, p. 189-209.
119. Si m MK, Ts o i WF. : The effects of centrallyacting drugs on the EEG correlates of medita-tion. Biofeedback Self. Regul. , 1992; 17(3):215-20.
120. Si mo n DB. : Returning to wholeness: embra-cing body, mind, and spirit in the face of can-cer. New York: Wiley, 1999.
121. So l berg EE, Hal v o rs en R, Sundg o t-Bo r -g en J, Ing l jer F, Ho l en A. : Meditation: amodulator of the immune response to physicalstress?A brief report. Br J Sports Med, 1995;29(4): 255-7.
122. Sug i Y, Akutsu K. : Studies on respiration andenergy-metabolism during sitting in Zazen.Res. J. Phys. Ed., 1968; 12: 190-206.
123. Sun FL, Li DM, Li GY. : Influence of diffe-rent combination of mental activity and respi-ratory cycle on heart rate variability (Chi -nese). Chin. J Integr Trad Western Med, 1986;16(3): 153-5.
124. Tay l o r CB, Farquher JW. : Relaxation The -rapy and High Blood Pressure. Arch Gen Psych,34: 339-42.
125. Tho mps o n MB, Co ppens NM. : The effectsof guided imagery on anxiety levels and move -ment of clients undergoing magnetic resonan -ce imaging. Holistic Nursing Practice, 1994;8(2): 59-69.
126. Trav i s FT, Orme-Jo hns o n DW. : EEG cohe -rence and power during Yogic Flying. Int JNeurosci. , 1990; 54(1-2): 1-12.
127. Trav i s F & Wal l ace R. : Autonomic markers
during respiratory suspensions; possible mar-kers of trascendental consciousness. Psycho -physiology, 1997; 34, pp. 39-46.
128. Trung pa Ch. : The Myth of Freedom and theWay of Meditation. Boston: Shambhala, 1988.
129. Vy as R, Di ks hi t N. : Effect of meditation onrespiratory system, cardiovascular system andlipid profile. J Physiol Pharmacol 2002 Oct;46(4): 487-91.
130.Wal l ace RK, Bens o n H, Wi l s o n AF. : Awakeful hypometabolic physiologic state.Am. J. Physiol. , 1971; 221(3), pp. 795-9.
131. Wal l ace RK, Bens o n H. : The physiologyof meditation. Scientific American, 1972;226: 84-90.
132. Wal l ace RK, Di l l beck M, Jaco be E, Ha -rri ng to n B. : The effects of the transcenden-tal meditation and TM-Sidhi program onaging. Int J Neuroscience, 1982; 16(1): 53-8.
133. Warrenburg S, Pag ano RR, Wo o ds M. : Acomparison of somatic relaxation and EEGactivity in classical progressive relaxationand transcendental meditation. J Behav Med,1980; 3(1): 73-93.
134. Wenneberg SR, Schnei der RH, Wal to nKG, Macl ean CR, Lev i ts ky DJ, Sal ernoJW, Wal l ace RK, Mandari no JV, Rai n -fo rth MV, Wazi ri R. : A controlled study ofthe effects of the transcendental meditationprogram on cardiovascular reactivity and am -bulatory blood pressure. Int J Neurosc, 1980;97(1-2), 15-28.
135. Wi l s o n AF, Ho ns berg er R, Chi u JT, No -v ey HS. : Transcendental meditation andasthma. Respiration, 1975; 32(1): 74-80.
136. Wi l s o n AF, Jev ni ng R, Gui ch S. : Markedreduction of forearm carbon dioxide produc-tion during states of decreased metabolism.Physiol. Behav., 1987; 41, pp. 347-52.
137. Wo l ko v e N, Krei s man H, Darrag h D, Co -hen C, Frank H. : Effect of trascendentalmeditation on breathing and respiratory con-trol. J. Appl. Physiol.: Respirat., Environ Exer -cise Physiol. , 1984; 56, pp.607-12.
138. Zamarra JW, Schnei der RH, Bes s eg hi niI, Ro bi ns o n DK, Sal erno JW. : Usefulnessof the transcendental meditation program inthe treatment of patients with coronary arterydisease. Am J Cardiol, 1996; 77: 867-70.
C. Med. Psicosom, Nº 105 - 201354









![Meditation [Dhyan] Versus Relaxation A Review With ... fileA Review With Comprehensive Bibliography Surekha D. Kaundinya*, Dilip V. Kaundinya** * Professor & Head- Physiology,**Ex-Prof](https://img.pdfslide.net/doc/110x75/5e177c627785c61c1a2af619/meditation-dhyan-versus-relaxation-a-review-with-review-with-comprehensive.jpg)