Embed Size (px)
Citation preview

Therapeutic Approach to Critical Heart Failure
Sebastian Tume MDAssistant Professor of Pediatrics, Baylor College of MedicineCICU Medical Director, Texas Children’s HospitalHouston TX

Burden of Acute Heart Failure• ~14,000 children are hospitalized annually with acute heart
failure syndromes.• 15–18 per 100,000 children are admitted each year for
evaluation and management of heart failure (2/3 have CHD). • A typical hospitalization lasts 2–3 weeks with an overall in-
hospital mortality ∼7%• Approximately 1/3 of children hospitalized with new-onset
heart failure either die or undergo cardiac transplantation within 1 year
Rosano et al. J Card Fail 2012

Pediatric Acute Heart Failure and CHD
• N=465,482 CHD hospitalizations, AHF was present in 2,712 (0.6%)
• Higher mortality associated with single ventricle heart disease, infancy, non-white race, chronic complex comorbidities

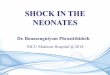
Cardiomyopathies in childrenDilated cardiomyopathies: 52.6%0.87cases/100K per yearInfants <1yo 4.7 cases/100K
Combined RCM/HCM: 1.5%
Hypertrophic cardiomyopathies: 22.1%
Restrictive cardiomyopathies: 3%
Others: 20.8%Arrhythmogenic RV cardiomyopathy
Hsu & Pearson Circulation 2009; Towbin et al. JAMA 2006; Webber et al. Circulation 2012
Freedom from transplant
Survival

Critical Heart Failure Syndromes• Acute Decompensated Heart Failure: a rapid onset
of or change in signs and symptoms of heart failure• Cardiogenic shock may be broadly defined as a state
in which oxygen delivery to the tissues is inadequate relative to demands secondary to inadequate cardiac function.

Phenotypes of Heart FailurePhysiologic state in
which cardiac output is insufficient to meet metabolic demands
HFrEF(systolic heart failure)
HFpEF(diastolic heart failure)
Dilated CardiomyopathyAcute myocarditis
Tachyarrhythmia CMCongenital Heart Disease
Hypertrophic CardiomyopathyRestrictive Cardiomyopathy
Acute Graft RejectionTransplant Coronary Artery
DiseaseCongenital Heart Disease
Combined systolic and diastolic heart
failure

Physiology of systolic heart failure
• Force–velocity relationship of cardiac fibers is altered and the ability of cardiomyocytes to generate force is reduced per unit time
• Ventricular loading conditions include elevated end systolic and end diastolic volumes with reduced stroke volume
Normal
ChronicAcute

Pathophysiology of heart failure
Zelis R, Prog Cardiovasc Dis 1975;18:181-99

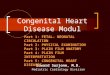
Cardiogenic Shock• Shock is defined when VO2 exceeds DO2
• Compensatory global & regional circulatory reflexes maintain tissue oxygenation by coupling blood flow to metabolism
• When cardiovascular reserve is exhausted, O2 extraction increases to maintain tissue oxygenation
• A critical threshold is reached “CRITICAL EXTRACTION” in which VO2 exceeds DO2and VO2 begins to decline and becomes dependent on supply
Figure from Costello et al. Cardiology in the Young (2015)
Critical extraction ratio
Lactate

Clinical Symptoms of CHFCLINICAL SIGNSTachycardiaTachypneaHypertensionHypotensionOxygen saturation <98%Capillary refill <2 secondsHepatomegalyGallop rhythmCool to touchRetractionsRalesPeripheral edemaJVD
%546330923286549402118215
PRESENTING SYMPTOMSFatigue or ↓activity levelDyspnea or ↑work of breathingCoughNausea or vomitingDiarrheaAbdominal painChest painDiaphoresisAny respiratory sign or symptomAny gastrointestinal sign or symptom
%57723862183624158387
Macicek et al. Pediatrics 2009;124

Diagnostic TestingChest radiograph:• Cardiomegaly (93%)• Prominent pulmonary vasculature/alveolar
edema (55%)• Pleural effusions (18%)
Echocardiogram:• Severely depressed systolic function
(65%)• Pericardial effusion (1%)
Electrocardiogram:• Abnormal rhythm (15%)• SVT, atrial flutter, complete AVB, high
grade second-degree AVB, VT• Abnormal morphology (62%)• Inverted T-waves, ST-segment elevation,
deep Q-waves
LAB MARKERSSerum sodium (mmol/L)
Serum bicarbonate (mmol/L)
Hemoglobin (gm/dL)
BUN (mg/dL)
Serum creatinine (mg/dL)
B-type natriuretic peptide
MEDIAN and IQR139 (135 to 140)
20 (16 to 25)
11.9 (9.9 to 13.1)
17 (11 to 25)
0.6 (0.4 to 0.9)
1975 (1060 to 4190)
Macicek et al. Pediatrics 2009;124

Infants vs. Children• Less cardiopulmonary reserve• Poorly organized contractile proteins of the cardiac myocyte
resulting in poor contractile reserve• Much higher VO2 per unit mass requiring higher CO and DO2 Poorly
developed sarcoplasmic reticulum with inefficient calcium delivery• High chest wall to lung compliance ratio with reduced end
expiratory lung volumes (atelectasis an hypoxemia) and inefficient generation of appropriate tidal volumes
• Immature diaphragm

Hemodynamic monitoring• The extent of monitoring will vary
depending on the presentation, clinical trajectory, and initial response to therapies
• Guidelines on use of monitoring exist from critical care societies
• Monitoring technology must be accurate and limitations of each technology must be clearly understood
• Published data on available technologies are typically limited to single-center case series.
Available advanced monitoring technologies
Pulse contour derived CO
Thermodilution derived CO
Swan Ganz CCO and TD
Bioimpedance
Venous oximetry
Doppler Ultrasound

Measuring Cardiac Output
STEWART HAMILTON FORMULA

Echocardiography• Doppler techniques • CO = LVOT Diam x VTI x HR• Great for assessment of
contractility, preload and structural heart disease
• Transthoracic Doppler (ex. USCOM)
Ultrasound Assessment of CO
Garcia et al. Med Intensiva. 2011

• Non invasive monitor of oxygen content
• Offers a favorable risk-benefit profile and can be effective and beneficial as a hemodynamic monitor
• Significant positive linear correlation shown between rSO2 & SjvO2
• Very helpful in dynamic patient populations (SV patients)
Non Invasive Venous Oximetry
Keeger et al Ann Thor Surg 2012

Treatment Goals• Timely diagnosis• Reverse hemodynamic
derangements and minimizemetabolic demand
• Preserve myocardial blood flow• Improve ventricular
performance• Relieve symptoms
Figure taken from Protectedpci.com

Decreasing metabolic demands• Primary interventions include the use
of positive pressure ventilation, sedation, and temperature control
• Muscles or respiration consume only ∼5% of the total body CO
• Substantial increase in work of breathing might increase CO to respiratory muscles byas much as 50%
• Total body oxygen consumption increases approximately by 10% for every degree Celsius increase in body temperature.
A
B

Mechanical Ventilation• PPV reduces myocardial VO2 by
decreasing LVEDV and LV systolic transmural pressure with resultant reduction in afterload and increase in stroke volume and CO.
• PPV unloads the respiratory pump allowing for a redistribution of CO from the respiratory apparatus to other vital organs
Broncki and Anas Pediatr Crit Care Med 2009

Achieving optimal myocardial conditionsOptimize ventricular loading conditions by judicious use of vasodilators and inotropy to improve SV and CO and minimize myocardial VO2

Managing Systolic Heart Failure• Modify the ventricular loading conditions to improve
stroke volume and CO while minimizing myocardial VO2
• Increase venous capacitance and decrease ventricular preload and diastolic stress
• Reduce ventricular afterload to increase CO and stroke volume

Treating Volume OverloadIndependent predictors of mortality at 1 year :• High PCWP (p=0.001)• Low serum sodium (p=0.002)• Increased LV end-diastolic dimension (p=0.01)• Low peak VO2 on cardiopulmonary exercise testing (p=0.001)
Fonarow G, Rev Cardiovasc Med2001;2:7-12Fonarow G, J Cardiac Fail2001;7(Supp2):038Stevenson L, Am J Cardiol1990;66:1348-54

Diuretics
• 65% of patients presenting with HF exacerbation present with hypervolemic state Anderone et al. Am J Cardiol 2004
• Diuretics reduce ventricular preload and diastolic stress
• One must ensure sufficient renal perfusion pressure to optimize diuresis
Chronic HF

Vasodilators
AgentVenus capacitance vessels
Arterial resistance vessels
Nitroglycerin +++ +
Nicardipine ++ ++
Nitroprusside ++ ++
Hydralazine + +++
Lasix +++
Targeting systemic vascular resistance and increasing venous capacitance lowers filling pressures, decreases myocardial oxygen demand, improves stroke volume and cardiac output

Inotropes• Remain a cornerstone of critical-care management
• Should be used cautiously and at the lowest dose and for the shortest duration possible as almost all increase myocardial oxygen consumption and are pro-arrhythmic

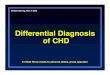
Inotropic agents-Bad Rep
Mebazaa A et al. 2011 Intensive Care Med 37 (2): 290-301
Data from ALARM-HF registry, N=4953
The use of inotropesin adults with acutely decompensated heartfailure has been associated with increased mortality inmultiple clinical trials and registry reports.
O’Connor et al., Am Heart J1999

Inotropic Agents• Positive affect on contractility result
in improved SV and CO while increasing myocardial oxygen demand and consumption
• + Chronotropic effects with increase in heart rate and consequently CO at expense of increased myocardial oxygen consumption
• Due to inverse force frequency relationship in failing myocardium increasing HR might actually lower SV and CO while shortening diastole
Milrinone
Epinephrine

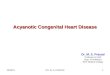
Molecular targets
Mechanisms of action
PharmacologicEffects
Therapeutic effects
Selective binding to the calcium saturated form of cardiac Troponin C
Calcium sensitization -Positive inotropic
- Increased EjectionFraction- Anti stunning
Opening of sarcolemma KATPchannels on smooth muscle cells in vasculature
Hyper-polarization-Vasodilation in all vascular beds (also coronary and peripheral circulation)
-Lowered Pre- and Afterload-Anti ischemic-Tissue Perfusion
Opening of mitochondrial KATPchannels in cardiomyocytes
Protection of mitochondria in ischemia-reperfusion
-Preconditioning-Antiapoptotic
-Cardioprotection-Anti ischemic-Long term benefits
Levosimendan

Adult HF Levosimendan Trials• Larger phase III studies showed no difference
– Against placebo in REVIVE (N=700)– Against dobutamine in SURVIVE (N=1327)
Packer M et al. J Am Coll Cardiol HF 2013;1:103–11
Mebazaa A et al. JAMA 2007;297:1883–91

Pediatric HF Levosimendan Experience

Texas Children’s Experience with Levosimendan
Unpublished data S Tume

Levosimendan Treatment Effect
Unpublished data S Tume

Vasopressors
Should have no role in treatment of systolic heart failure unlessevidence of low SVR state (ex sepsis)

Managing Diastolic Heart Failure• Characterized by low stroke
volume and CO as a result of impaired ventricular filling despite elevated end-diastolic pressures
• Determine optimal filling pressure
• Decrease systemic venous return without compromising SV and CO
• Avoid inotropy unless evidence of compromised systolic function

Single Ventricle Physiology• Characterized by systemic and
pulmonary circulations being in parallel
• Ratio of pulmonary (Qp) and systemic (Qs) vascular resistance determines systemic and pulmonary perfusion
• SVR is much greater then PVR and neurohormonal activation plays a large role in causing Qp/Qs imbalance

Use of Mechanical Circulatory Support• Shift from medical therapy to MCS should not be
seen as last resort but as simply the next step• Be proactive to avoid going onto MCS with end organ
failure• Define the end point of MCS• Decision of temporary vs. durable support

LVAD
OR
Ventricular Loading Conditions On MCS
Peripheral ECMO Direct ventricular unloading
↓ wall tension and myocardial O2demand
↑ myocardial DaO2
Reduces inotrope dependence

Summary• Rapid recognition of the critical heart failure phenotype is
crucial for design of appropriate therapy• Recognition of imbalance in oxygen demand and delivery is
critical and should be assessed with accurate monitoring and frequent reassessments for response to therapy
• Overarching goal of therapeutic approach to critical heart failure is to modify the ventricular loading conditions, improve stroke volume while minimizing myocardial VO2
• Therapeutic interventions must be titrated to each phenotype and their side effects recognized
• If all fails use mechanical support earlier rather late

THANK YOU Please help me improve my talk by completing a brief evaluation