Embed Size (px)
Citation preview
THERAPEUTIC VALUE OF IODIZED OIL IN BRONCHIAL ASTHMA”
LEO H. CRIEP, M.D., AND JOSEPH W. HdMPSEY, M.D. PITTSBURGH, PA.
T HE rational management of bronchial asthma includes attention to allergic factors, eradication of foci of infection, correction of nasal
pathology, and improvement in the general health of the patient. Symp- tomatic treatment aims at overcoming local obstruction in the bronchi and bronchioles. But in spite of t,horough management there still remains a large group of patients whose asthma is intractable. Any new procedure which offers hope of relief or recovery, particularly in this group of patients, is bound to attract the attention of the profession. It is not surprising, therefore, that a great deal of interest has been aroused in the recent uniformly enthusiastic reports on the successful treatment of bronchial asthma by the intratracheal instillation of iodized oil.
LITERATURE
Very brief reference is found in the literature as early as 1925 con- cerning the instillation of iodized oil in bronchitis, bronchiectasis, and asthma.
Pritchard, Whyte and Jordan1 referred to the value of iodized oil in the treatment of diseases of the bronchi in a paper published in 1926. Also in 1926, Ochsne? stated that the beneficial results obtained from the use of iodized oil are due to its mechanical and bactericidal effect. In a paper published in 1929,3 he again referred to its therapeutic use- fulness in bronchitis and bronchiectasis. It was not, however, until 1932, that a series of papers appeared dealing with the use of iodized oil in the treatment of bronchial asthma. In the order of their appearance, the following are cited: Taylor4 obtained excellent results in two cases of asthmatic bronchitis. Fink5 concluded he had obtained satisfactory im- provement in 13 cases of bronchial asthma. The third paper, published later in the year, a preliminary report by Anderson,G indicated uni- versally good results in a series of 50 cases of asthma of long duration. Cole and Harper7 in 1933 reported on the use of iodized oil in 26 cases of intractable asthma having obtained beneficial effects in the entire group. Ahsons in a paper published a few months later in 1933 likewise reported good results in ten cases of asthmatic bronchitis. Amberson, Riggins and McLeod,g in a paper appearing shortly afterward, discussed
*From the Department of Medicine and the Allergy Clinic of the School of Medi- cine, University of Pittsburgh, Pittsburgh, Pa.
Read before the annual meeting of the Society for the Study of Asthma and Allied Conditions, Atlantic City, N. J., May 1, 1937.
23

24 THE JOIJRNAL OF I&ERG\-
the subject wit,hout considering therapeutic results. Balyeat and
Seylerl” in 1934 stated their experience based on the treatment of 100 asthma patients with iodized oil. n.riable degrees of improvement were observed in this series but in only 5 per cent slight or no improvement was obtained. In a paper which appeared the following pear,ll the same authors stated that in treating 50 cases of intractable asthma by this method they obtained excellent results in 14 per cent, good results in 56 per cent, fair results in 12 per cent, slight results in 25 per cent, and no improvement in 10 per cent.
AndersonI in 1936 supplied us with the most optimistic account. His paper dealt with results obtained in the treatment of 260 patients. Out of this group he excluded from consideration 60 patients because these showed such complications as hypertrophic emphysema, pneumoconiosis, healed tuberculosis, chronic laryngitis, and tracheitis in which this form of treatment has proved of no value. He obtained, however, “ complet,e relief” for a period of one to eight years in 90 per cent of the remainder of the group, that is, in 200 patients, the average duration of whose asthma was twelve years. In only 10 per cent, or in 20 patients, he ob- tained no satisfactory relief. It is difficult to see why the group of 60 asthmatic patients in whom this treatment is not of value is not included in the percentage of failures. The type of asthma in which this observer obtained his best results may be illustrated by citing some of his typical cases :
CASE REPORTS
CASE L-A fifteen-year-old boy who had asthma and hay fever for twelve years was sensitive to several pollens. After ten injections of lipiodol his asthma and hay fever disappeared.
CASE 2.-A thirty-three-year-old patient who had asthma for twenty-four years was sensitive to horse dander, onions, and cabbage. After the eighth injection of oil, he became clinically desensitized to horse dander and after the tenth to onions and cabbage, and he has obtained complete relief for three and a half years.
CASE 3.-A twenty-five-year-old patient with an asthmatic history of twelve years’ duration was entirely relieved of both her asthma and her sensitivity to aspirin by seven injections of oil, after which she could take aspirin without showing any ill effect.
Other instances are cited in which clinical desensitization was brought about by means of iodized oil insufflation in patients sensitive to fish. tomatoes, and, in one patient who developed asthma as result of contact with water, iodized oil desensitized him to water. Nothing is found in the above quoted paper on whether allergic investigations were carried out to substantiate the author’s conclusion that clinical desensitization is effected in allergic patients by iodized oil therapy.
Finally, the most recent contribution to this subject is that of Harris and TurkeLI Fifty patients with asthma were treated with iodized oil. These patients were thoroughly treated previously for at least three years by other methods unsuccessfully. They were intractable asthmatics. The results reported arc as follows: In four patients, or 8 per cent,
CRIEP AND HAMPSEY: IODIZED OIL IN BRONCHIAL ASTHMA 25
excellent (complete freedom from attacks) ; in 24 patients, or 48 per cent, good (75 per cent relief or better) ; in 14 patients, or 28 per cent, fair (35 to 50 per cent) ; and in 8 patients, or 16 per cent, the treatment was a total failure.
We shall attempt in this paper to evaluate the therapeutic procedure referred to above by analyzing the results thus far reported; by pre- senting the experience of the writers and the experience of a large group of well-known rhinologists and allergists with this form of treatment.
PERSONAL OBSERVATIONS
These observations are based on the study of a total of 40 asthmatic patients, divided int,o three groups.
INTRATRACHEAL INSUBFLATION OF IODIZED OIL
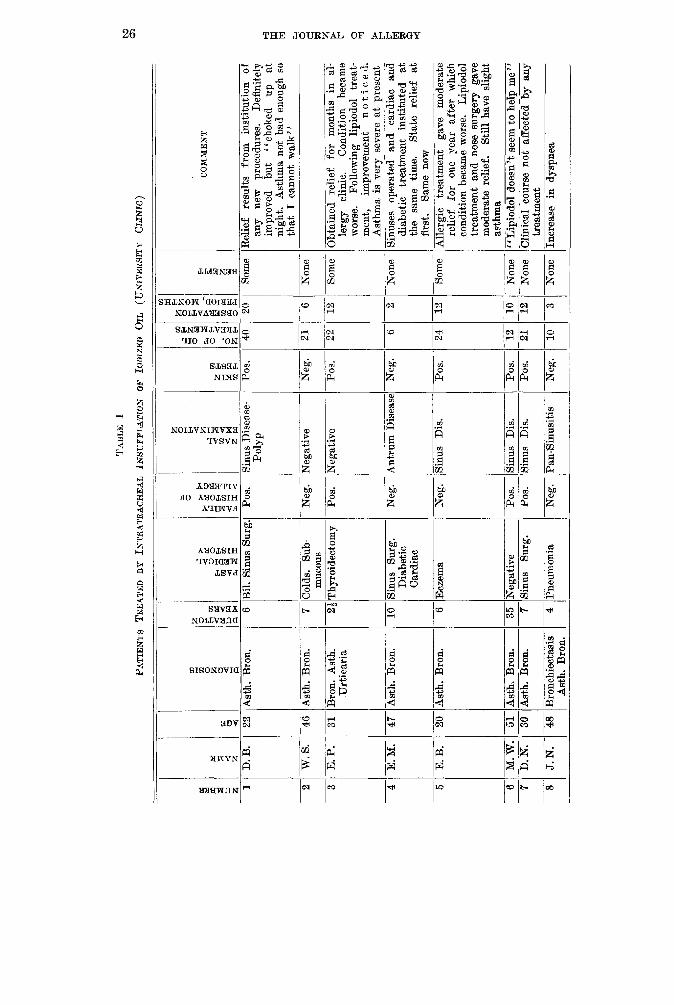
GROUP 1 (Table I) .-This group consists of 20 cases of intractable asthma, all of whom responded poorly to medical and allergic treatment. Because of this, these patients were given iodized oil (lipiodol or lipiodine) by intratracheal instillation. Cocaine was used as an anes- thetic. The technique employed is that described by Balyeat, Seyler, and Shoemaker.ll A laryngeal syringe was used. Information presented in Table I indicates some interesting data in this connection. Some of these patients are frankly allergic as evidenced by the presence of a personal and family allergic history, the presence of eosinophilia, symptomatic response to epinephrine, and positive skin tests. Several patients have asthmatic bronchitis as evidenced by the presence of definite infection in the sinuses or complicating bronchiectasis. The rest of the group presents a combination of both the allergic and infectious type of asthma. There are in this number no patients with pollen (seasonal) asthma because it is generally conceded that in these instances allergic manage- ment is the treatment of choice. The age of the group ranges from twenty to sixty-five years, the duration of asthma from two to fifty years. Iodized oil therapy, as may be seen from Table I, did not bring about a cure, that is, total and absolute freedom from asthmatic symptoms over the period of observation of one to two years in any of these patients. Three patients showed definite temporary improvement and in 17 patients the treatment was a complete failure. Analysis of the three patients who showed temporary improvement reveals the following:
CASE REPORTS
The first patient, D. B. (Table I), is a highly emotional young girl who has been under treatment in the allergy clinic for about five years. During this time there were periods ranging from two to seven months when she would be entirely comfortable. She would show marked improvement for a variable length of time fotiowing an operation on the sinuses or the institution of some new therapeutic procedure. Following the second treatment with iodized oil, she stated that she obtained great relief and that “for the first time in a year she was able to get a night ‘s sleep. ’ ’ It is difficult to know whether to attribute this improvement to iodized oil, especially in view of the fact that roentgen ray study at the time she
ii 2 D.
B.
ii is
9 2 i;
22
Asth.
Br
on.
2 w.
8.
46
3 E.
P.
31
4 E.
M.
5 E.
B.
J. N.
--
--
--
--
--
-
6 M.
W
. 7
D.
N.
8
-
- 47
- 20
- 51
- 30
- 48
TABL
E I
PATI
ENTS
TR
EATE
D UT
IA
Y~RA
TRAC
HESL
IN
~UFF
LATI
ON
OF
IODM
ED
OIL
(UNI
VERS
ITY
CLIN
IC)
8 2 2 2:
33
Gn
us
Dise
ase-
Po
lyp
Asth.
Br
on.
&on.
A&
h.
Urtie
aria
-: _- -. _. __
-7 -
7 Co
lds.
Sub-
mu
cous
23
Thy
roide
otomy
Neg.
Pos.
rega
tive
qega
tive
-
_-__
_..-
Asth.
Br
on.
10
Sinu
s Bu
rg.
Diab
etic
Card
iac
Neg.
Lntru
m Di
seas
ksth.
Br
on.
T-Ec
zem
a Ne
g. lin
us
Dis.
Asth.
Br
on.
35
Nega
tive
Pos.
GiG
Dis
. LG
iiiTBr
7
Sinu
surg
. Po
s. lin
us
Dis.
Bron
chiec
tasis
Asth.
Br
on.
I
4 Pn
eumo
nia
Neg.
‘an-S
inusit
is
-
= - e -~
-
z;::
E& -m
Po
s.
Neg.
Pos.
21
22
Neg.
6
.- Po
s. 24
Pos.
Pos.
Neg.
12
21
10
> > i -
2 ii ---
EL-
Some
None
Some
None
Some
None
No
ne
None
COM
MEN
T
Relie
f res
ults
from
institu
tion
of an
y ne
w pr
oced
ures
. De
finite
ly im
prov
ed
but
“chok
ed
up
at nig
ht.
Asthm
a no
t ba
d en
ough
so
tha
t I
cann
ot wa
lk”
Obtai
ned
relie
f for
mo
nths
in ai:
ler
gy
clinic
. Co
nditio
n be
came
wo
rse.
Follo
wing
lip
iodol
treat-
me
nt,
impr
ovem
ent
notic
ed.
Asthm
a is
verv
seve
re at
ures
ent
“___
. A
~ E-
ted
and
card
iac
and
diabe
tic
treatm
ent
institu
ted
at the
sa
me
time.
St
ate
relie
f at
first.
Same
no
w Al
lergic
tre
atmen
t ga
ve
mode
rate
relie
f for
on
e ye
ar aft
er
which
co
nditio
n be
came
wo
rse.
Lipiod
ol tre
atmen
t an
d no
se
surge
ry ga
ve
mode
rate
relie
f. St
ill ha
ve
sligh
t as
thma
l‘Lrp
iodo1
do
esn’t
se
em
to he
lp me
” Cl
inica
l co
urse
not
affex
d-bs
_ -
treatm
ent
Increa
se
in dy
spne
a
TABL
E I.-
CONT
'D
- 10
si 2 R.
K.
M.
P.
11
J. D.
12
J.
K.
- -_
_ 13
F.
D.
14
15
S. F
. 65
~~
-
M.J.M
. - 65
- 16
E.
P.
17
-.- 18
19
20
-
G. H
. 42
ist
h. Br
on.
-__ W.
H.
C. B
.
L. P.
52
Ist
h. Br
on.
- -
3 - 60
c(1
z E 3 8 As
th.
Bron
.
50
Asth.
Br
on.
- 61
- 53
Bsth.
Br
on.
Asth.
Br
an.
Bron
chiec
t.
- ---
42
4sth.
Br
on.
Asth.
Br
on.
isth.
Bron
.
- 40
Isth.
Bron
.
45
- 54
k&h.
Bron
. Ist
h. Br
on.
=
, /
_!
-. -_
_ .- .- . .
.- .- . .
. .
-
33
Nega
tive
53
Pneu
monia
12
Pn
eumo
nia
I
24
Nega
tive
20
Nega
tive
-- 3
Polyp
ectom
ies
I
10
Nega
tive
12
Nega
tive
Neg.
Sinu
sitis
9 Ne
gativ
e 7
Nega
tive
Neg.
Sinu
s Su
rg.
-. __
Ne
g. Po
lyps
14
INeg
ative
- ~ I
/ - -
Neg.
Hype
rtrop
hic
Sinu
sitis
Pos.
Nega
tive
- Ne
g. --
__~
Neg.
Nega
tive
Pos.
I Po
s. Ch
r. Su
pp.
Sinu
sitis
Neg.
/Neg
ative
* BZ
M
W
mR
Neg.
__. Ne
g.
Pos.
Neg.
Neg.
__. Ne
g.
Neg.
Neg.
Neg.
Neg.
11
- 10
- 14 5 7
- 3 23
- 18
27
B z $ p1
Noue
None
None
No
ne
None
None
No
ne
None
None
None
No
ne
None
CO
MM
ENT
“At
first
some
what
easie
r bu
t ha
ve
notic
ed
no
impr
ovem
ent”
-- -
Trea
ted
in all
ergy
cli
nic
five
years
wi
th
varia
ble
resu
lts.
‘ ‘ M
arke
d im
prov
emen
t at
first
from
oil,
but
very
bad
again
for
pa
st few
mo
nths”
Refus
es
treatm
ent.
No
impr
ovem
ent
Evide
nceo
f xfe
mn
bron
chial
tre
e. No
res
ults
from
aller
gic
or iod
ized
oil
treatm
ent
Obtai
ned
good
res
ults
for
one
year
while
tre
ated
in all
ergy
cli
nic.
Refus
ed
‘ ‘iod
ized
oil
treatm
ents
beca
use
it ma
de
him
worse
” -.--
- P&
-to
admi
ssion
rec
erved
8
treat-
me
nts
with
oi
l els
ewhe
re
Asthm
a wo
rse
at firs
t Se
vere
re
actio
n fo
ilowi
ng
seco
nd
treatm
ent
28 THE JOURNlL OF ALLERGY
experienced the marked relief indicated that none of the oil reached the lungs. Her condition continued to be satisfactory over a period of twenty months although she states at present that “she chokes up frequently at night but her asthma is not bad enough to keep her from walking.”
The second patient, E. P. (Table I), is also a very emotional young woman who has had allergic asthma for two and a half years. There were period8 of two months or more when, while under allergic treatment, she was quite comfortable. When her symptoms returned, lipiodol treatment was instituted. This wa8 followed by definite relief over a period of one year, but her condition is now as unsatis- factory a8 ever,
The third patient, E. B. (Table I), also a young woman, suffers from allergic asthma complicated by sinus infection. She obtained marked relief for months at a time while treated in the allergy clinic. When she became wor8e, iodized oil was administered. Her condition improved. It must be st,ated, however, that simultaneously with the institution of oil therapy her no8e was operated on and her antra were irrigat,ed.
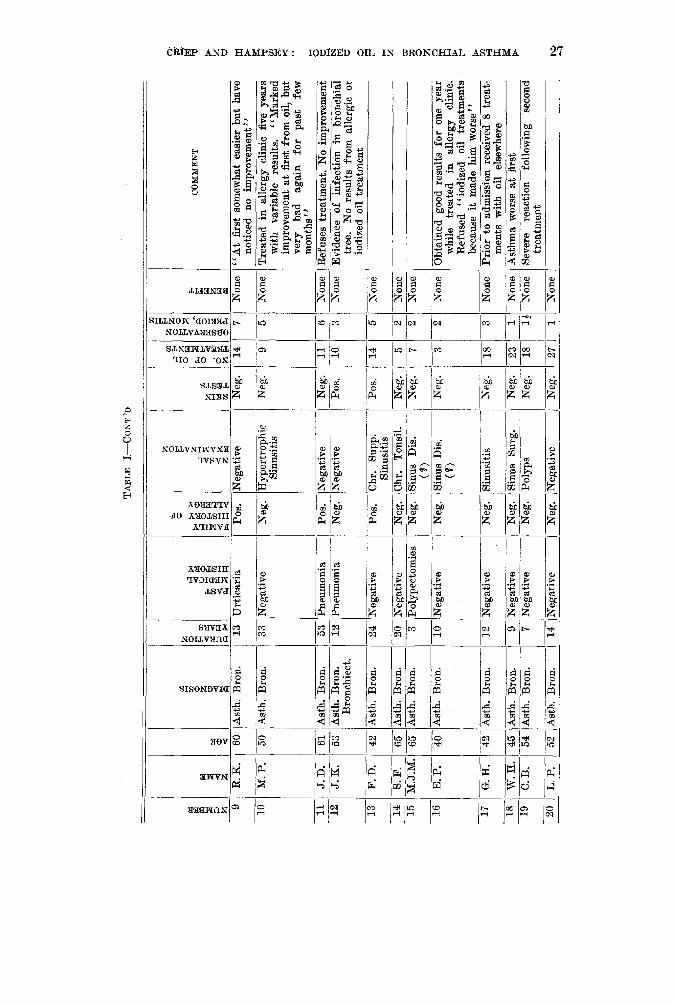
It appears, therefore, from the above that what must be considered transient and satisfactory relief follows the institution of treatment with iodized oil in only 3 out of 20 patients with intractable asthma; that is, in 15 per cent. Those who know the influence of psychogenic factors on the course of this condition and are familiar with the vagaries of the disease will be slow in attributing to the oil and the oil alone, even in such a small percentage of cases, a curative value. The question naturally comes up, how could the oil have had anything to do with the improvement in the condition of the first patient when it did not even reach the lung? What was the role played by the correction of nasal pathology in the improvement of the third patient? Many of us have seen asthmatic patients suddenly and unexplainably get better after such empiric procedures as ether anesthesia, roentgen ray of the lung, or as shown in a recent experience from just getting a patient prepared for bronchoscopy without actually passing the bronchoscope.
BRONCHOSCOPIC INTRODUCTION OF THE OIL
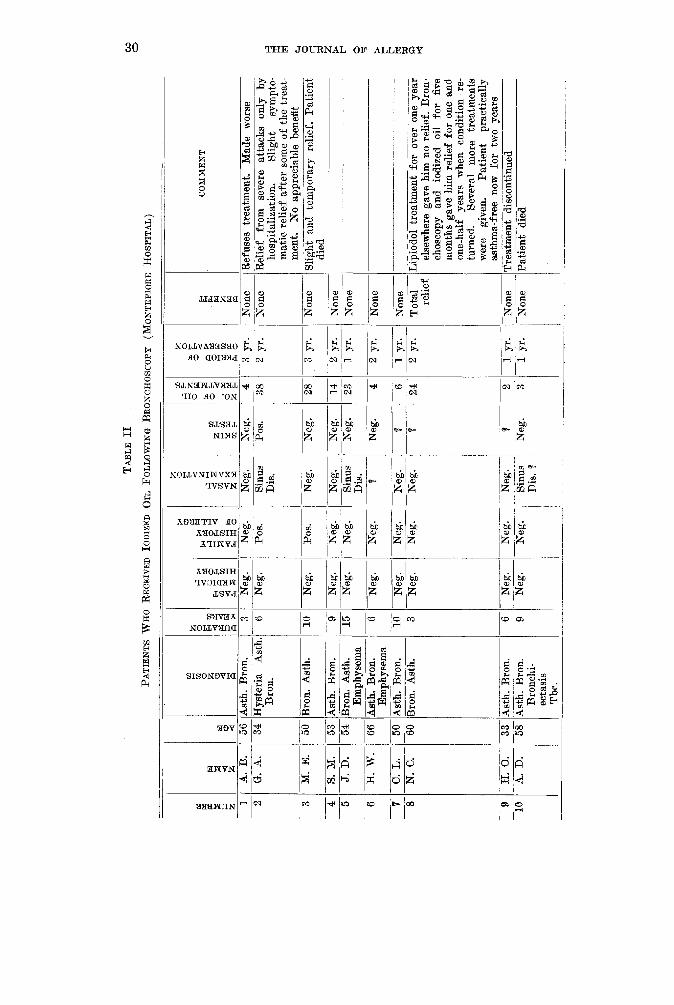
In view of the fact that some observers hold that the bronchoscopic introduction of iodized oil yields better results, we are enclosing observa- tions on a second group of 10 patients (Table II). These patients have intractable asthma. Many of them have sinus and bronchial infection. Only one has definite evidence of allergy to foods and other substances. In all of these patients, iodized oil therapy was combined with bronchos- copy performed by Dr. Simon Seegman. In the entire series, complete relief occurred in only one patient (N. C.) . This sixty-year-old man began to be troubled with asthmatic breathing, especially on exposure to gas fumes, about two years before the institution of iodized oil therapy in another clinic. He received such treatment at weekly intervals for one year without any results. Subsequently, he was bronchoscoped and given iodized oil in the Bronchoscopic Clinic of the Montefiore Hospital. He received this treatment for five months at weekly intervals and be- came symptom-free for one and a half years when the condition re-
GRIEF AND HAMPSEY: IODIZED OIL IN BRONCHIAL ASTHMA 29
turned. Several more treatments were administered, and the patient has been comfortable for two years. As for the rest of the patients in this group, it was felt that whatever relief was obtained it was only tempo- rary and in practically every instance due to the removal of mucus with the bronchoscope.
RESULTS OBTAINED IN GROUP TREATED IN ANOTHER CLINIC
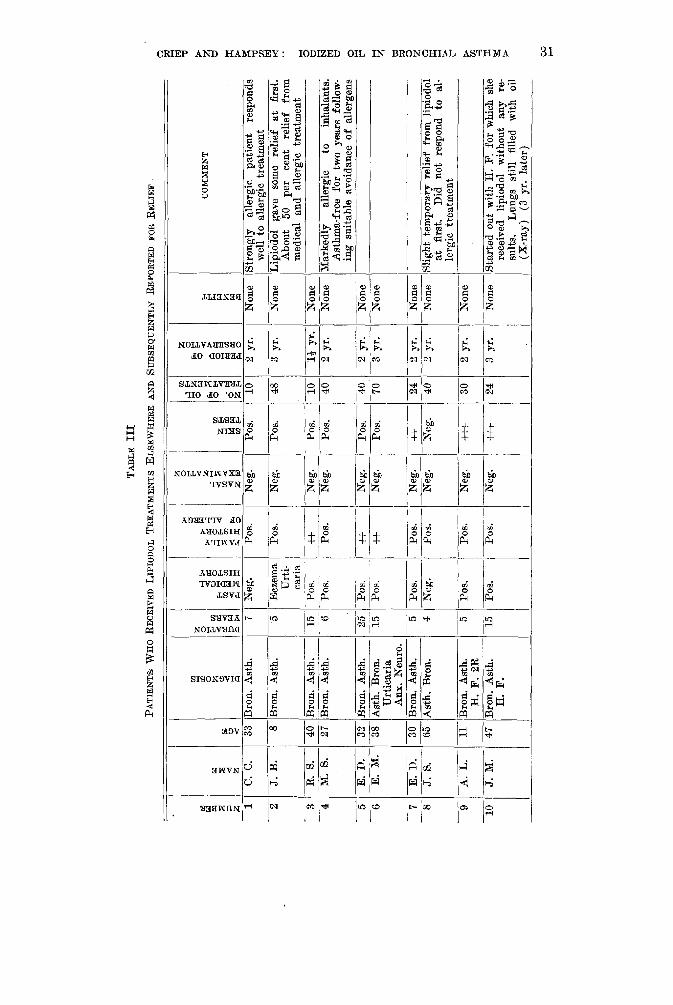
The third group under observation is a group of 10 patients (Table III), nine of whom received lipiodol treatments over a long period of time in one of the clinics from which come encouraging reports referred to elsewhere in this paper. This group is presented in order to eliminate faulty or inadequate technique as a possible explanation for the high percentage of failures obtained in our own series. (Tables I and II.) Examination of the records of these 10 patients shows that they have received from 10 to 70 treatments. It is apparent that none derived lasting relief or they would not have sought further medical attention. What is more, many of these patients are still definitely allergic to many substances as evidenced by the clinical history and the presence of posi- tive intradermal tests. In these patients at least, lipiodol treatment, therefore, did not bring about loss of clinical sensitivity. It is interest- ing to point out that one patient, J. M. (Table III), received 24 oil in- jections for ragweed hay fever and asthma without any benefit but was definitely relieved by prophylactic pollen therapy. Another patient, &I. S. (Table III), had a similar experience. She had received 40 in- &illations of oil at weekly intervals but continued to have bronchial asthma. This patient has been symptom free for a year and one half since she has been avoiding exposure to offending substances.
RESULTS OP QUESTIONNAIRE
It further occurred to us that in an attempt to evaluate accurately this form of therapy, it would be well to obtain the views of a large num- ber of physicians who have had experience with this procedure. Such an expression of opinion based on personal knowledge and obtained from many rather than a few observers would tend to overcome both bias and enthusiasm. With this idea in mind, 335 questionnaires were mailed to all the members of the Association for the Study of Allergy. The So- ciety for the Study of Asthma and Allied Conditions, The American Bronchoscopic Association, and 100 members of the American Laryngo- logical, Rhinological, and Otological Society. The questionnaire asked these physicians whether they had any experience with iodized oil in the treatment of bronchial asthma. If so, on the treatment of how many cases was their opinion based% In what percentage of allergic and in what percentage of infectious asthma did the observer obtain results which he could interpret as a cure, improvement, or total failure t Were there any untoward reactions from this form of therapy? Was the treatment still in use in his clinic?
8 B E 1 2
Fi
2 A.
B.
G.
A.
3 4 5 6 7 --
8
M.
E.
S.
M.
J. D.
H.
W.
-__ c.
L. N.
c.
9 H.
0.
10
A.
D.
TABL
E II
PATI
ENTS
W
HO
RECE
IVED
IO
DIZE
D Or
r, FO
LLOW
ING
BRON
CHOS
COPY
(M
ONTE
F-IO
RE
HOSP
ITAL
)
z * g z
3 ij 56
A&
h.
Bron
. 34
Hy
steria
As
th Br
on.
50
Bron
. As
th.
53
A&h.
Br
on.
54
Bron
. A&
h.
Emph
ysem
a 66
A&
h.
Bron
. Em
phys
ema
50
Asth.
Br
on.
60
Bron
. As
th.
33
Asth.
Br
on.
58
Asth.
Br
on.
Bron
chi-
ectas
is Tb
c.
10 9 15 6
-- 10 3 6 9
Neg.
Neg.
Neg.
Neg.
Neg.
Neg.
__- Ne
g. Ne
g.
Pos.
Neg.
-Neg
.
Neg.
Neg.
-__ Ne
g.
Neg.
Neg.
Neg.
Neg.
-iGK Di
s. ---
B
__- Ne
g. Ne
g.
-___
Neg.
Sinu
s Di
s. ?
ZE?
LIZ
Neg.
1'05
.
Neg.
Neg.
Neg.
Neg.
iB
9 B Ne
g.
28
14
23 4 6 _-
24
2 3
-
3 yr.
2 yr.
1
yr.
2 yr.
1 yr.
2
yr.
1 yr.
-._
_ 1 yr.
E 3 B m
No
ne
None
None
None
No
ne
None
None
- To
tal relie
f
-~ None
-~ No
ne
I ‘I --
I
COMM
ENT
tefus
es
treatm
ent.
Made
wo
rse
-___
__~
belie
f fro
m se
vere
attac
ks
only
by
hosp
italiz
ation
. Sl
ight
symp
to-
matic
re
lief
after
so
me
of the
tre
at-
ment
. No
ap
prec
iable
bene
fit {lig
ht
and
tempo
rary
relie
f. Pa
tient
die
d
$iodo
l tre
atmen
t for
ov
er on
e ye
ar els
ewhe
re
gave
him
no
re
lief.
Bron
- ch
osco
py
and
iodize
d oi
l for
fiv
e mo
nths
gave
him
re
lief
for
one
and
one-
half
years
wh
en
cond
ition
re-
turne
d. Se
vera
l mo
re
treatm
ents
were
giv
en.
Patie
nt
prac
ticall
y as
thma-
free
now
for
two
years
‘re
atmen
t di&
%nt
inued
- *&
mdied
I B E
E -I+
-J. 2
-3 R.
8.
-~ -4
M.
8.
-E. 5
-6
E.
M.
-7 E.
D.
-~
~__
8 J.
S.
TABL
E III
PATI
ENTS
W
HO
RECE
IVED
LIP
IODO
L TR
EATM
ENTS
EL
SEW
HERE
AN
D SU
BSEQ
UENT
LY
REPO
RTED
FO
B RE
LIEF
I 8
Bron
. A&
h.
I i
TEcz
ema
Urti-
i I
caria
40
IB
ron.
Asth.
-~
___~
-
15
Pos.
- 27
Bron
. As
th.
32
&-on
. A&
h.
25
Pos.
~ __
- 38
As
th.
Bron
. 15
Po
s. Ur
ticar
ia An
x. Ne
uro.
- __
_ 30
Br
on.
Asth.
5
Pos.
65
Asth.
Br
on.
-qNe
g.
I ?l!
?Bro
n As
th H:
F.
2R
5 Po
s.
47
Bron
. As
th.
15po
s. H.
F.
%
*g
$83
-h4
3m
4ib
k 0
Pos.
POS.
+I-
Pos.
__-~
+t +?-
-__ Po
s. Po
s.
Pos.
__.- Po
s.
L - - - - - - - -
Neg.
Neg.
Neg.
Neg.
Neg.
Neg.
Neg.
Neg.
Neg.
Pos.
Pos.
POS.
Po
s.
-__ -l-
t Ne
g.
t+t
ttt
-
XT--
-- 1
: yr.
~~
~-
___
40
2 yr.
40-
2 yr.
-7
0 .--
- 3
yr.
24-
2 yr.
-
-___
40
2
yr.
30-
2 yr.
24-
3 yr.
- --
--
-
3 CO
MMEN
T
None
St
rong
ly all
ergic
pa
tient
res
pond
s we
ll to
aller
gic
treatm
ent
None
Lip
iodol
gave
- so
me
relie
f at
first.
Abou
t 50
pe
r ce
nt re
lief
from
medic
al an
d all
ergic
tre
atmen
t -_
_ None
No
ne
Marke
dly
aller
gic
to inh
alants
. As
thma-
free
for
two
years
fol
low-
ing
suita
ble
avoid
ance
of
aller
gens
No
ne
-Non
e
None
__
__
None
Sl
ight
tempo
rary
relie
f fro
m lip
iodol
at firs
t. Di
d no
t re
spon
d to
al-
lergic
tre
atmen
t No
ne
-__ No
ne
Star
ted
out
with
H.
F.
for
which
sh
e re
ceive
d lip
iodol
with
out
any
re-
sults
. Lu
ngs
still
filled
wi
th
oil
(X-ra
y) (3
vr.
later
)
TAEZ
E IV
USE
OF
IODI
ZED
OIL
IN
ASTH
MA
ANAL
YSIS
OK
RE
SPON
SE
F~M
QUES
TION
NAIR
ES
RECE
IVED
FR
OM
64
PHYS
ICIA
NS
- A
BRON
CHIA
L AS
THM
A I
ASTH
MAT
IC
BRON
CHIT
IS
I TO
TAL
PHYS
ICIA
NS
CURE
26
5 (1
.9 pe
r ce
nt)
55
64
T IM
PRO
VED
; FA
ILUR
E 'I'O
TAL
CURE
7 -m
-i~6
(24.7
iz
cent)
’ (7
3.4
per
cent)
26
7
(0.8
peT
cent)
IMPR
OVE
D NU
MBE
R FA
ILUR
E TO
TAL
CASE
S 26
7
214
717
(22.8
pe
r ce
nt)
(76.4
pe
r ce
nt)
938
938
1205
CRIEP AND HAMPSEY: IODIZED OIL IN BRONCHIAL -4STHMA 33
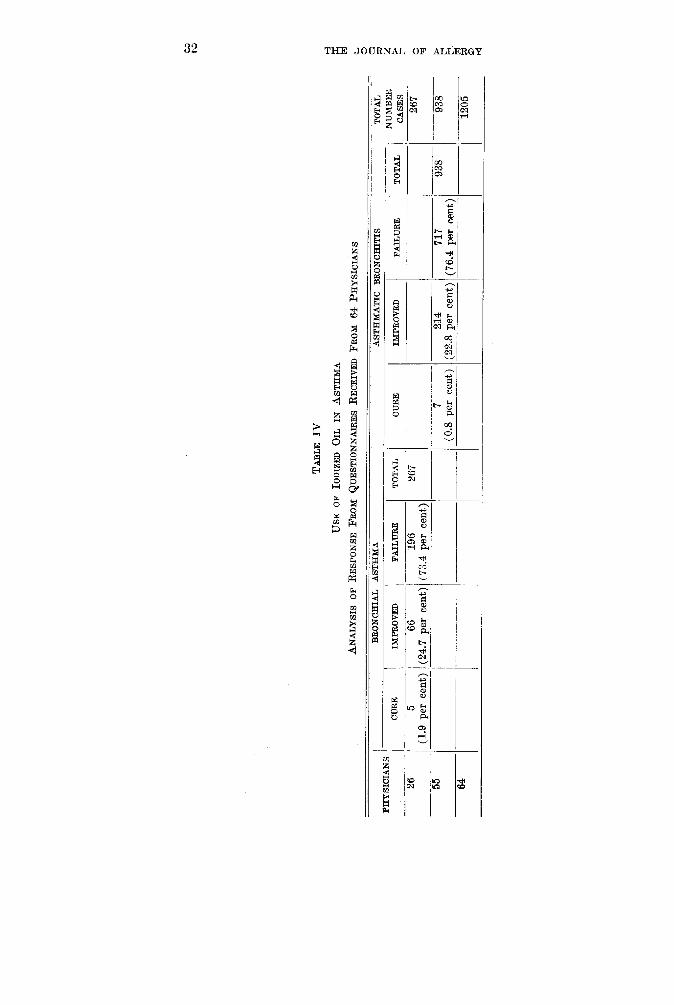
Of a total of the 335 questionnaires mailed, 230 replies were received. In these, 166 physicians had no opinion to offer because they had no experience with this form of treatment. Of the 64 who have used iodized oil in the treatment of asthma, only 22 or one third were still using it, but for the most part only as an adjunct to medical and allergic treat- ment, and after all other forms of therapy have failed.
The 64 replies are analyzed in Table IV. A total of 1205 patients with asthma are represented. Twenty-six physicians reported treatment of a total of 267 patients with bronchial asthma with the following results: “ Cures” were obtained in five patients or 1.9 per cent. “Improve- ment” occurred in 66 patients or 24.7 per cent; “total failure” in 196 patients or 73.4 per cent. Fifty-five physicians reporting on the treat- ment of a total of 938 patients with asthmatic bronchitis recited the fol- lowing results : “Cures” were obtained in seven patients or 0.8 per cent; “improvement” in 2.4 patients or 22.8 per cent; “total failure” in 7.7 or 76.4 per cent. Thus it is seen that therapeutic results from the use of the oil almost parallel those of intractable asthma whether it is of the allergic of infectious type or in the combined form.
REPORTS OF UNTOWARD REACTIONS
In view of the fact that the beneficial results obtained from treatment appear rather limited, it becomes important to determine whether un- pleasant or dangerous reactions following the administration of iodized oil occur with sufficient frequency to render its use objectionable. Balyeatll referred to the possibility of iodine sensitivity and to other contraindicat,ions but stated that it would be unusual to find these in a chronic asthmatic. AndersonI observed that some patients may become exhausted from convulsive cough; in others, there may be acute collapse of lung. He noticed severe iodism in only eight patients and reports eight cases of pneumonia in the entire group of which number all but one recovered. Our own experience is similar. Following oil therapy two patients developed severe dyspnoea, cyanosis, and circulatory failure from which they recovered.
Other reactions, either due to allergy to iodine or poppyseed oil, or due to circulatory failure are found mentioned in the literature or in the replies to our questionnaire. Plehnl” reported one case in which the pa- tient developed a coughing seizure after lipiodol instillation and rup- tured the terminal bronchioles with resulting traumatic bronchiectasis. Reactions presumably allergic and characterized by fever, urticaria, arthritis, asthma, and acute asphyxia are reportedI by Kern, Rappaport, Cooke, Vaughan, Unger, Waldbott, Casort, Figley, Ramirez, Davidson, Davison, Hudson, and others.
Some observers12 report oil in the lung for three years after treatment was discontinued. That the oil may cause damage to lung such as mas- sive consolidation, infection, caseation necrosis, and fibrosis is evident from the reports of LaughlinI’ and Pierson.lT According to Brown,ls
34 THE JOURNAL OF ALLERGY
and Bettman, Kelly and Crohn,l” the oil is t,aken up by phagocytes and may accumulate in the lung as tumor-like masses-oil being at t,imes absorbed into the lymphatics or into the capillaries, Fried and Whitaker,*O JacobeusZ1 and others, and Pinchin and MorlockZ2 have described massive collapse of lung caused by iodized oil. In our own experience a sixty-year-old man developed bronchopneumonia twenty- four hours after treatment and died. Waldbott, Kahn, Brown, and Cooke also reportI the occurrence of pneumonia following the admin- istration of oil. Phillips noted one case of massive atelectasis and Sheldon found increasing pulmonary fibrosis.
Fatal termination following treatment with iodized oil is not alto- gether rare. MacDonaldz3 reported one case t,hat developed nausea, vomiting, cyanosis, and died in twenty hours. Amberson!’ and others cited several cases that terminated fatally following instillation of oil. One asthmatic patient was stood up before the fluoroscope and in a few minutes collapsed. The pulse was irregular and weak, the patient be- came cyanotic and dyspnoeic and in spite of treatment, died within an hour. Similar instances are found in the answers to our question- naires.14
SUMMARY AND COSCLUSIONS
1. The literature dealing with the therapeutic value of iodized oil in bronchial asthma is reviewed. All of these reports indicate very favorable therapeutic results.
2. Therapeutic results observed by the writers in 40 cases of in- tractable asthma treated with iodized oil are analyzed.
a. Of 20 patients treated by intratracheal insufflation, only three patients obtained prolonged relief. In 17 patients, the treatment was a total failure. Improvement, however, cannot always he attributed to the effect of the oil.
b. Of 10 patients who received oil following bronchoscopy, only one showed complete relief.
c. A group of 10 patients treated with iodized oil elsewhere failed to show either clinical improvement or loss of clinical sensitivity to substances to which they were allergic.
3. In an effort to obtain an expression of opinion based on personal experience, 335 questionnaires were mailed to members of the two Societies for the Study of Allergy, the American Bronchoscopic So- ciety and The Triological Society. Two hundred thirty replies were received. One hundred sixty-six of these indicated no experience with this form of treatment. The remaining 64 replies revealed the fol- lowing :
a. Only one-third of the physicians who tried this therapeutic pro- cedure are still using it, but, for the most part, only as an adjunct to medical and allergic management in a well selected group of asthma patients.
CRIEP AND HAMPSEY: IODIZED OIL IN BRONCHIAL ASTHMA 35
b. In bronchial asthma (267 ca.ses) : Cure, 1.9 per cent; improvement, 24.7 per cent; failure, 73.4 per cent were obtained.
c. In asthmatic bronchitis (39) : Cure, 0.8 per cent; improvement, 22.8 per cent; failure, 76.4 per cent was reported.
4. The replies further demonstrated: a. A particular lack of en- thusiasm if not direct opposition to this form of therapy.
5. Untoward reactions to iodized oil are reported by many. These reactions may be due to allergy to iodine and poppyseed oil, to cir- culatory failure, spread of infection and damage to lung tissue. Fatal reactions are not rare.
6. It is, therefore, concluded that in a very small percentage of a well selected group of patients with intractable asthma some tempo- rary benefit may reasonably be expected from the use of iodized oil. This benefit is due to the mechanical effect of the oil on the bronchi and bronchioles. The disadvantages cited in this paper should be carefully considered before the institution of treatment with iodized oil.
REFERENCES
I. Pritchard, S., Whyte, B., and Jordan, J. K. M.: Use of Iodized Oil in Diagnosis and Treatment of Bronchial Affections. J. A. M. A. 86: 1119. 1926.
2. Ochsner, A. : Bronchography Following the Passive Introductions of Contrast Media Into the Tracheobronchial Tree, Wisconsin M. J. 25: 544, 1926.
3. Ochsner, A. : An Unappreciated Cause of Chronic Bronchitis, J. A. M. A. 93: 188, 1929.
4. Taylor, J. H.: Treatment of Asthmatic Bronchitis With Iodized Oil. Minnesota Med. 15: 408, 1932.
5. Fink, L. W.: Liuiodol as Theraueutic Agent. Minnesota Med. 15: 522. 1932. 6. Anderson, W.: Some Observations on the Value of Intratracheal Injections of
Iodized Oil for Bronchial Asthma, J. ALLERGY 4: 44, 1932. 7. Cole, D. B., and Harper, Edgar, C.: Therapeutic Use of Iodized Oil in Pulmon-
ary Disease, J. Lab. & Clin. Med. 18: 704, 1933. 8. Alison, J. F.: Treatment of Asthmatic Bronchitis With Iodized Oil. South.
M. J. 26: 696, 1933. 9. Amberson, J. B., Jr., Riggins, H. M., and McLeod: Lipiodol in Bronchography :
Its Disadvantages and Dangers and Uses, J. Roentgenol. 30: 727, 1933. 10. Balyeat, R. N., Seyler, E.: The Therapeutic Value of the Intratracheal Use of
Iodized Oil in Bronchial Asthma, Lancet 54: 563, 1934. 11. Balyeat, R. M., Seyler, E., and Shoemaker, H. A.: The Diagnostic and Ther-
apeutic Value of the Intratracheal Use of Iodized Oil in Cases of Intractable Asthma, Radiol. 24: 303, 1935.
12. Anderson, W.: The Treatment of Bronchial Asthma by Intratracheal Injections of Iodized Oil, New York State J. Med. 36: 1151, 1936.
13. Harris, M. Coleman, and Turkel, Henry, L.: The Treatment of Bronchial Asthma by Intratracheal Iodized Oil Instillations, M. J. & Rec., 1937.
14. Personal Communications. 15. Plehn, G. J.: Discussion of Paper by Anderson, (Ref. 12). 16. Laughlin, G. F.:
J. Path. 1: Pneumonia Following Nasopharyngeal Injection of Oil. Am.,
407, 1925. 17. Pierson, J. W.: Some Unusual Pneumonias Associated With Aspiration of
Fats and Oils in the Lungs, Am. J. Roentgenol. 27: 572, 1932. 18. Brown, A. L.: The Fate of Iodized Oil (Lipiodol) in the Lungs, Surg., Gynec.,
& Obst. 45: 597, 1928. 19. Bettman, R. B., Kelly, J., and Crohn, N.: Effect of Intrabronchial Injections
of Iodized Poppyseed Oil; Experimental Study on Dogs, Arch. Surg. 19: 471, 1929.
20. Fried, B. M., and Whitaker, L. R.: Arch. Int. Med. 40: 726, 1927.
Intratraeheal Injections of Iodized Oil,
36
31.
22.
23.
THE JOUR,NAL OF ALLERGY
Jacobeus, H. C., Selander, G., and Westmark, N.: A Study of Acute Massive Atelectatic Collapse of the Lung, Acta. med. Scandinav. 71: 439, 1929.
Pinchin, A. J. S.., and Morlock, H. V.: Acute Massive Collapse of the Lung Following Lipiodol Injections, Brit. M. J. 1: 930, 1931.
MacDonald, I. G.: The Local and Constitutional Pathology of Bronchial Asthma, Ann. Int. Med. 6: 253, 1932.
MAY BUILDING
DISCUSSION
DR. GEORGE FLAMM, Brooklyn.-Dr. Criep’s analysis of results from the use of instillations of iodized oil for the treatment of Asthma con- form very closely to our own, both at the Roosevelt and Gouveneur Hospitals. In no case have I been able to see a result which approaches anything that might be considered a “cure.” In a small percentage of cases patients have been temporarily relieved for several weeks and months.
However, we must not be unmindful of the untoward reactions and bad results which sometimes follow. That the use of lipiodol or other iodized oils is sometimes attended by serious complications is illustrated by the following two cases, which I briefly wish to call t,o the atten- tion of the Society. The complete report is in the process of publication.
CASE REPORTS CASE L-J. L., aged thirty years, insurance clerk, was admitted to our clinic on
January 15, 1937, suffering from severe asthma. In 1934, he showed symptoms of rhinitis, for which he received no relief from local nose treatments. In 1935 he started to attend one of the allergy clinics for his rhinitis. In March 1936, phenol cauterization of his nose was followed by acute attacks of asthma for the first time in his life. In August 1936, he received four instillations of lipiodol about a week apart. His asthma has become progressively worse, and it has been necessary to keep him hospitalized. X-rays in October 1936, seven weeks after lipiodol, showed shadows of opaque substances with inflammatory reaction in both bases. X-ray examination in January 1937, five months after lipiodol, still showed oil present in both bases with an especially large accumulation in the left lower base, resembling a localized patch of pneumonitis. The patient is still very acutely il l and confined to the hospital.
CASE 2.-M. B. Ii., housewife, aged fifty-eight years, was first seen on July 27, 1933, because of nonseasonal bronchial asthma of four years’ duration. The patient gave a positive family history of allergy. In 1931 and again in 1932, she received three instillations of lipiodol. On July 27, 1933, X-rays showed opaque shadows in both bases, which the roentgenologist reported to be due to lipiodol. The right base revealed pronounced markings and the left showed a large cavity with greater accumulation of lipiodol than on the right side. The patient’s attacks of asthma became progressively worse and she died on March 7, 1935, during a paroxysm. Autopsy findings were bilateral atelectasis with areas of calcitbzation. An histologic report was unobtainable.
The question naturally arises as to the frequency of such occurrences. This, I am not prepared to answer just now. However, I believe that retention of lipiodol is more common than we suspect. In spite of these complications, if we are to favor the use of iodized oil in the treatment of bronchial asthma, are the benefits obtained satisfactory enough to warrant it?