Embed Size (px)
Citation preview
Therese M. Grant, Ph.D. Therese M. Grant, Ph.D. Associate Professor, UW School of MedicineAssociate Professor, UW School of Medicine
LaShaunda HarrisLaShaunda HarrisClinical Supervisor, Yakima Parent Child Assistance Program (PCAP)
Intervention as Prevention:Intervention as Prevention: Working Effectively with High-Risk Working Effectively with High-Risk
Mothers who Abuse Alcohol and DrugsMothers who Abuse Alcohol and Drugs
2007 Washington State Institute on Addictions Treatment 2007 Washington State Institute on Addictions Treatment Partnerships for Recovery: Meeting the Challenge Partnerships for Recovery: Meeting the Challenge
June 27-29, 2007June 27-29, 2007Sheraton Tacoma Hotel, Tacoma, WashingtonSheraton Tacoma Hotel, Tacoma, Washington
Children, Youth, and Family TrackChildren, Youth, and Family Track
Workshop Objectives:• Describe prevention strategies that have been
demonstrated among substance abusing women to prevent future alcohol and drug exposed births.
• Describe effective methods for collaborating with community service providers to better understand and serve high-risk clients.
• Discuss how strong state policies can work together with community prevention programs to enhance outcomes.
Focus: Continuum of family services

The ProblemThe Problem
• Possible effects of prenatal exposure on the Possible effects of prenatal exposure on the child’s healthchild’s health
• Likelihood of a compromised home environmentLikelihood of a compromised home environment
• Likelihood that these mothers will have more Likelihood that these mothers will have more exposed, affected childrenexposed, affected children
These problems are costly to society These problems are costly to society and are completely preventableand are completely preventable
Maternal alcohol and drug use Maternal alcohol and drug use puts children at risk because of:puts children at risk because of:
Parent-Child Assistance Parent-Child Assistance Program (PCAP)Program (PCAP)
An intensive, 3-year home visitation An intensive, 3-year home visitation
intervention for high-risk intervention for high-risk
alcohol and/or drug abusing mothers alcohol and/or drug abusing mothers
WHEN CASE MANAGEMENT WHEN CASE MANAGEMENT ISN’T ENOUGHISN’T ENOUGH
Primary Goal:Primary Goal:
To Prevent Future Births To Prevent Future Births
of Alcohol and Drug of Alcohol and Drug
Exposed ChildrenExposed Children
PCAP BackgroundPCAP Background
1991-present1991-present• WA State locations: King, Pierce, Yakima, Grant, WA State locations: King, Pierce, Yakima, Grant,
Spokane, Cowlitz, Skagit Counties Spokane, Cowlitz, Skagit Counties • Replication sites: MN, NC, AK, TX, NV, LA, PA; Replication sites: MN, NC, AK, TX, NV, LA, PA;
multiple sites in Canadamultiple sites in Canada
We thank our funders:We thank our funders:SAMHSA (CSAP)SAMHSA (CSAP)WA State Dept. Social and Health Services WA State Dept. Social and Health Services (Division of Alcohol and Substance (Division of Alcohol and Substance
Abuse)Abuse)March of DimesMarch of DimesNesholm Family FoundationNesholm Family FoundationPrivate PhilanthropyPrivate Philanthropy
PCAP Enrollment CriteriaPCAP Enrollment Criteria
1)1) Used alcohol/drugs heavily during Used alcohol/drugs heavily during pregnancypregnancy
2)2) Not effectively engaged with Not effectively engaged with community resourcescommunity resources
3)3) Are currently pregnant, up to six Are currently pregnant, up to six months postpartummonths postpartum
-or--or-
Have delivered a child with a diagnosis of FAS/EHave delivered a child with a diagnosis of FAS/E
Advocate CharacteristicsAdvocate Characteristics
• • Have experienced some of the same Have experienced some of the same types of adverse life circumstances as types of adverse life circumstances as clients, but seldom to same degreeclients, but seldom to same degree
• • Have subsequently achieved success in Have subsequently achieved success in important waysimportant ways
• • Are positive role models and offer clients Are positive role models and offer clients hope and motivation from a realistic hope and motivation from a realistic
perspective perspective
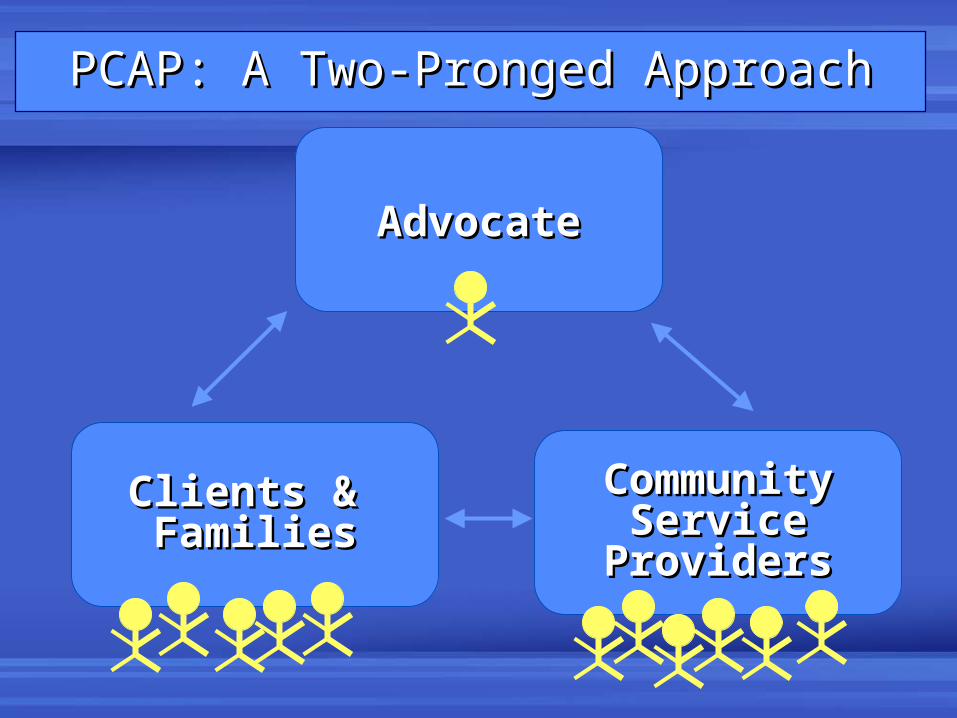
AdvocateAdvocate
Community Community Service Service
ProvidersProviders
Clients & Clients & FamiliesFamilies
PCAP: A Two-Pronged ApproachPCAP: A Two-Pronged Approach
Core Components of the InterventionCore Components of the Intervention
PCAP is a 3-year home visitation model implemented by PCAP is a 3-year home visitation model implemented by well trained, supervised advocates.well trained, supervised advocates.
Caseload recommendation: 15-16 active client familiesCaseload recommendation: 15-16 active client families
Advocates:Advocates:• Assess client’s strengths, needs.Assess client’s strengths, needs.
• Help clients identify goals and “baby” steps to meet Help clients identify goals and “baby” steps to meet goals (every 4 months).goals (every 4 months).
• Develop a network among client’s service providers to Develop a network among client’s service providers to facilitate effective treatment planning.facilitate effective treatment planning.
• Link clients with appropriate community services; Link clients with appropriate community services; assure clients receive servicesassure clients receive services. .
• Provide advocacy for all family members as needed.Provide advocacy for all family members as needed.

The Scope of AdvocacyThe Scope of AdvocacyCommunity ProvidersCommunity Providers
Juvenile Juvenile JusticeJustice
ProbationProbation
Alc/DrugAlc/DrugTxTx
Mental HealthMental HealthTxTx
Health CareHealth Care
FamilyFamilyPlanningPlanning
Job Job TrainingTraining
SchoolsSchools
Bio DadBio Dad
Room-Room-matesmates
FriendsFriends
PartnersPartners
NeighborsNeighbors
ExtendedExtendedFamilyFamily
CaretakersCaretakers
ChildrenChildren
CPSCPS
SiblingsSiblings
The Formula for Preventing The Formula for Preventing Alcohol/Drug Exposed BirthsAlcohol/Drug Exposed Births
• Motivate women to stop drinking or Motivate women to stop drinking or using drugs before and during using drugs before and during pregnancypregnancy
– – OR – OR –
• • Help women who can’t stop drinking Help women who can’t stop drinking or using drugs to avoid becoming or using drugs to avoid becoming pregnantpregnant
Preventing Alcohol and Drug Exposed Preventing Alcohol and Drug Exposed
Births in Washington State: Births in Washington State:
Intervention Findings from Three Intervention Findings from Three
Parent-Child Assistance Program Sites Parent-Child Assistance Program Sites
American Journal of Drug and Alcohol Abuse, 2005American Journal of Drug and Alcohol Abuse, 2005
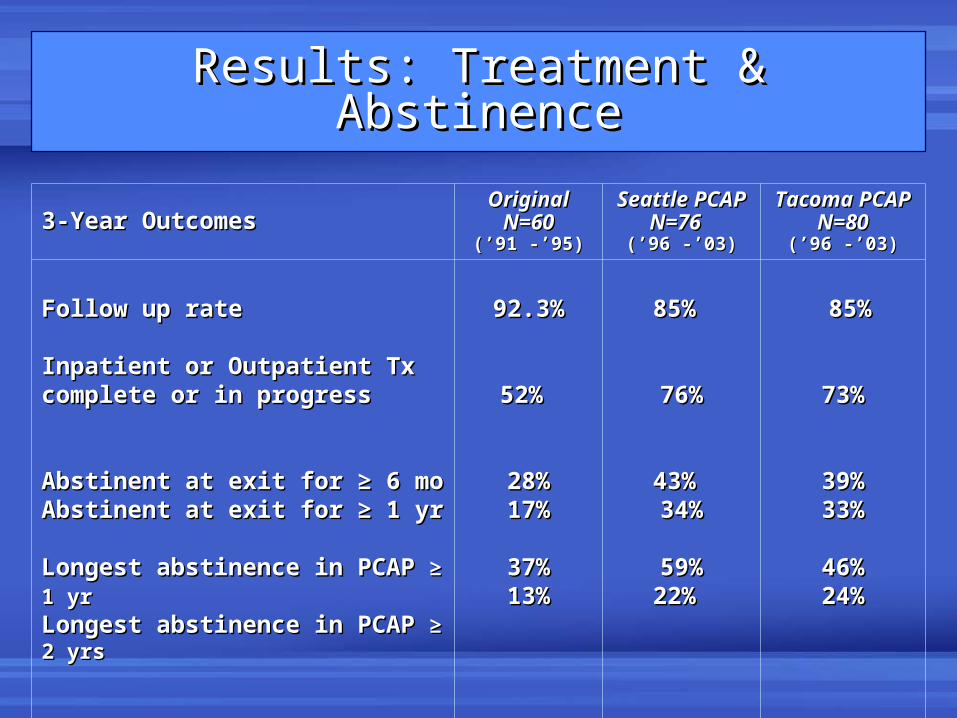
Results: Treatment & AbstinenceResults: Treatment & Abstinence
3-Year Outcomes3-Year OutcomesOriginalOriginal
N=60N=60(’91 -’95)(’91 -’95)
Seattle PCAPSeattle PCAPN=76N=76
(’96 -’03)(’96 -’03)
Tacoma PCAPTacoma PCAPN=80N=80
(’96 -’03)(’96 -’03)
Follow up rate Follow up rate
Inpatient or Outpatient Tx Inpatient or Outpatient Tx complete or in progresscomplete or in progress
Abstinent at exit for ≥ 6 moAbstinent at exit for ≥ 6 moAbstinent at exit for ≥ 1 yrAbstinent at exit for ≥ 1 yr
Longest abstinence in PCAP Longest abstinence in PCAP ≥ 1 yr≥ 1 yr Longest abstinence in PCAP Longest abstinence in PCAP ≥ 2 yrs≥ 2 yrs
92.3%92.3%
52% 52%
28%28%17%17%
37%37%13%13%
85% 85%
76%76%
43% 43% 34%34%
59%59%22% 22%
85%85%
73%73%
39%39%33%33%
46%46%24%24%
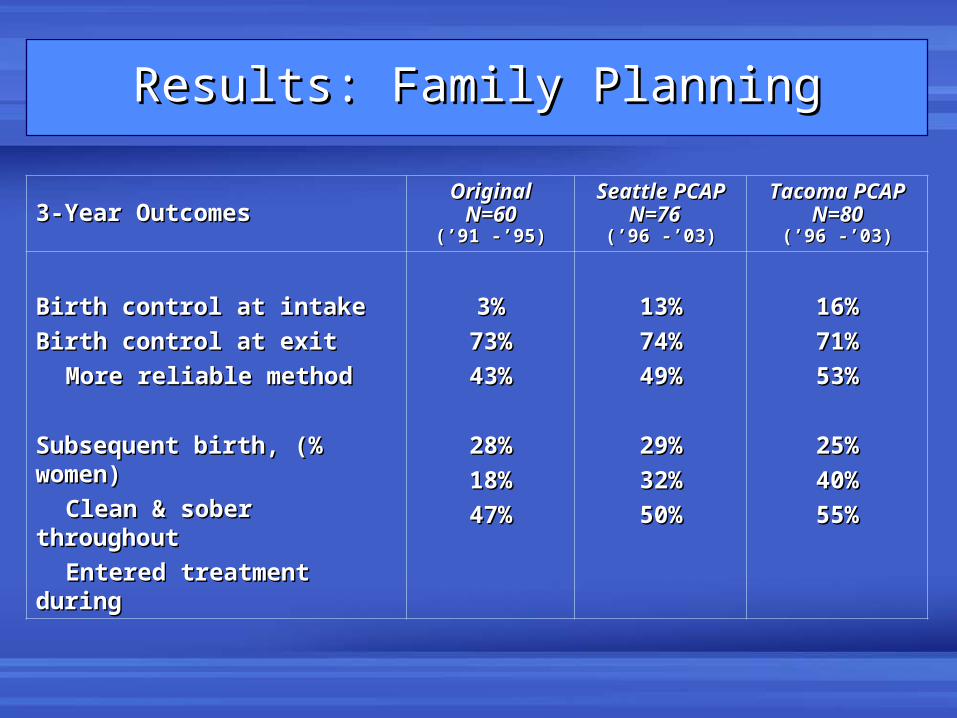
3-Year Outcomes3-Year OutcomesOriginalOriginal
N=60N=60(’91 -’95)(’91 -’95)
Seattle PCAPSeattle PCAPN=76N=76
(’96 -’03)(’96 -’03)
Tacoma PCAPTacoma PCAPN=80N=80
(’96 -’03)(’96 -’03)
Birth control at intakeBirth control at intake
Birth control at exitBirth control at exit
More reliable methodMore reliable method
Subsequent birth, (% women)Subsequent birth, (% women)
Clean & sober throughout Clean & sober throughout
Entered treatment during Entered treatment during
3%3%
73%73%
43%43%
28%28%
18%18%
47%47%
13%13%
74%74%
49%49%
29%29%
32%32%
50%50%
16%16%
71%71%
53%53%
25%25%
40%40%
55%55%
Results: Family PlanningResults: Family Planning
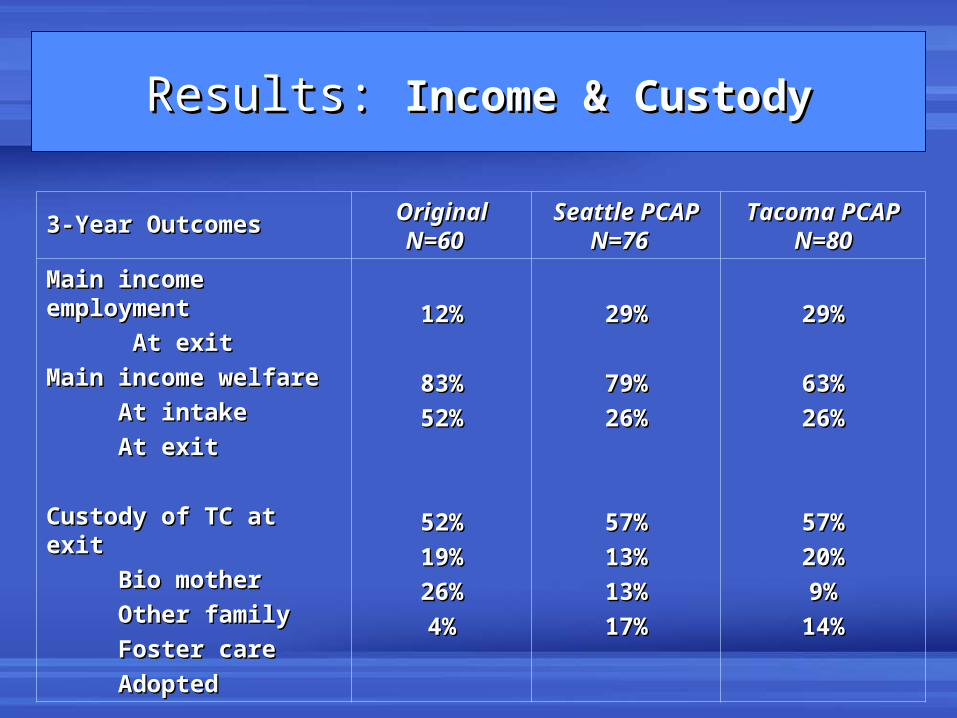
Results: Results: Income & CustodyIncome & Custody
3-Year Outcomes3-Year Outcomes OriginalOriginalN=60N=60
Seattle PCAPSeattle PCAPN=76N=76
Tacoma PCAPTacoma PCAPN=80N=80
Main income employmentMain income employment
At exitAt exit
Main income welfareMain income welfare
At intakeAt intake
At exitAt exit
Custody of TC at exitCustody of TC at exit
Bio motherBio mother
Other familyOther family
Foster careFoster care
AdoptedAdopted
12%12%
83%83%
52%52%
52%52%
19%19%
26%26%
4%4%
29%29%
79%79%
26%26%
57%57%
13%13%
13%13%
17%17%
29%29%
63%63%
26%26%
57%57%
20%20%
9%9%
14%14%
An Ongoing ChallengeAn Ongoing Challenge• Pregnant and parenting women who abuse Pregnant and parenting women who abuse substances are unfailingly characterized as substances are unfailingly characterized as “bad “bad mothers.” mothers.”
• They have been labeled unmotivated and difficult They have been labeled unmotivated and difficult — if not impossible — to reach.— if not impossible — to reach.
• These mothers become distrustful of “helping” These mothers become distrustful of “helping” agencies. agencies.
The result is that the women at highest risk for The result is that the women at highest risk for delivering children with serious medical, developmental, delivering children with serious medical, developmental, and behavioral problems are the least likely to seek and and behavioral problems are the least likely to seek and receive assistance. receive assistance.
Mothers in PCAP Mothers in PCAP were themselveswere themselves
the abused, neglected children the abused, neglected children
in our communities just 10-15 years in our communities just 10-15 years
ago.ago.
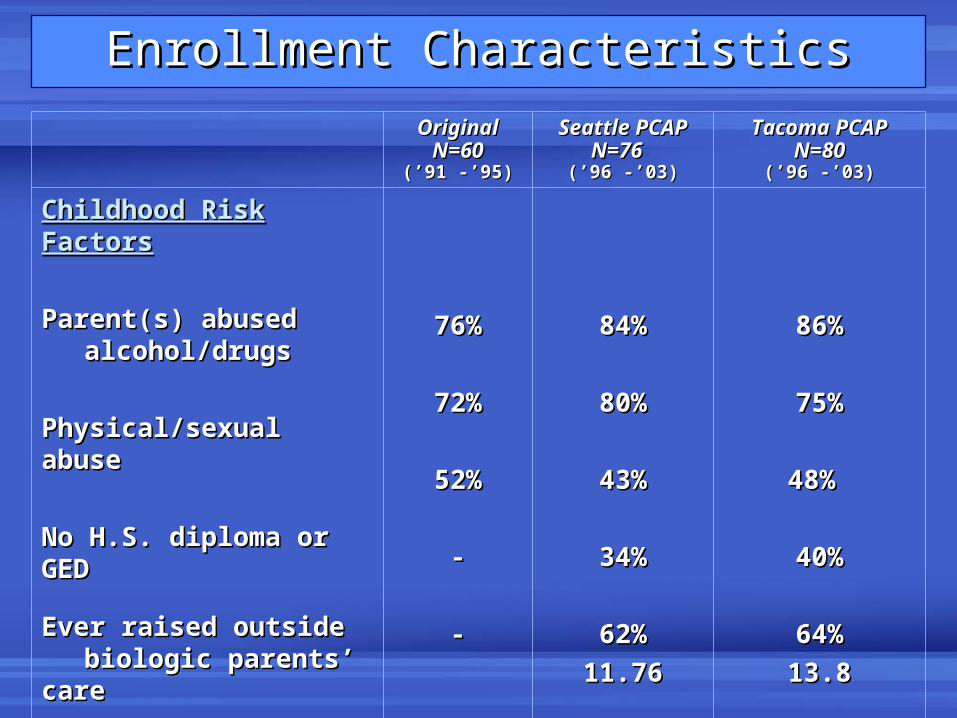
Enrollment CharacteristicsEnrollment Characteristics
OriginalOriginalN=60N=60
(’91 -’95)(’91 -’95)
Seattle PCAPSeattle PCAPN=76N=76
(’96 -’03)(’96 -’03)
Tacoma PCAPTacoma PCAPN=80N=80
(’96 -’03)(’96 -’03)
Childhood Risk FactorsChildhood Risk Factors
Parent(s) abused Parent(s) abused alcohol/drugsalcohol/drugs
Physical/sexual abusePhysical/sexual abuse
No H.S. diploma or GEDNo H.S. diploma or GED
Ever raised outside Ever raised outside biologic parents’ carebiologic parents’ care
Ran away from homeRan away from home
mean agemean age
76%76%
72%72%
52%52%
--
--
84%84%
80%80%
43%43%
34%34%
62%62%
11.7611.76
86%86%
75%75%
48% 48%
40%40%
64%64%
13.813.8
Our challenge is to engage these Our challenge is to engage these
mothers and their children mothers and their children
together to break this together to break this
intergenerational pattern.intergenerational pattern.
Good things happen Good things happen when communities when communities implement effective implement effective programs and states programs and states
implement strong implement strong policy.policy.
Systems Working TogetherSystems Working Together
Division of Alcohol & Substance AbuseDivision of Alcohol & Substance Abuse (DASA)(DASA)
treatment expansiontreatment expansion
IIncreased treatment beds for women: 55 to 153 ncreased treatment beds for women: 55 to 153 (1991 - 2007)(1991 - 2007)
Systems Working Together for:Systems Working Together for: Substance Substance
Abuse Treatment Abuse Treatment
DSHS “Take Charge” programDSHS “Take Charge” program (1989-present) (1989-present)
Developed to help low income pregnant women Developed to help low income pregnant women obtain servicesobtain services
Recent development:Recent development:Free family planning supplies for women Free family planning supplies for women and men at 200% below FPLand men at 200% below FPL
Systems Working Together for:Systems Working Together for:
Family Planning Family Planning
Systems Working TogetherSystems Working Together
““Work First” Welfare to Work program (1997)Work First” Welfare to Work program (1997)
State:State: 41% reduction in families on welfare (1997-04)41% reduction in families on welfare (1997-04)
PCAP:PCAP: 42% reduction (1995-03)42% reduction (1995-03)
PCAP subjects were higher risk compared to general PCAP subjects were higher risk compared to general welfare population (fewer white, fewer married, all welfare population (fewer white, fewer married, all substance abusers).substance abusers).
Systems Working Together for:Systems Working Together for:
Safe, Stable CustodySafe, Stable Custody
WA Permanency FrameworkWA Permanency Framework developed to increase developed to increase rates of permanent placement for children in foster care rates of permanent placement for children in foster care (1998)(1998)
State reunification rate:State reunification rate: consistent consistent decreasedecrease (1997-02) (1997-02)
PCAP:PCAP: with bio mom at exit: 52% (1991-95) and 57% with bio mom at exit: 52% (1991-95) and 57% (1996-03)(1996-03)
1996-03 cohort half as likely to be in foster care and 3x 1996-03 cohort half as likely to be in foster care and 3x more likely to be adopted compared to 1991-95 cohort.more likely to be adopted compared to 1991-95 cohort.
Implementing a Implementing a
Home-Visitation Model:Home-Visitation Model:
Lessons LearnedLessons Learned
Relational TheoryRelational TheoryA woman’s sense of connectedness to others is A woman’s sense of connectedness to others is central to her growth, development, definition of self.central to her growth, development, definition of self.
Positive relationships within the intervention, Positive relationships within the intervention, treatment, and recovery setting are critical.treatment, and recovery setting are critical.
The quality of interpersonal relationships The quality of interpersonal relationships • • may determine whether or not a woman may determine whether or not a woman remains in an intervention; remains in an intervention;• • may be more important than the concrete may be more important than the concrete services received. services received.
Lessons Learned: Lessons Learned: Develop a Theoretically-Based ModelDevelop a Theoretically-Based Model
Theoretical FrameworkTheoretical Framework
Relational TheoryRelational Theory
InterventionIntervention
Long term, positive interpersonal Long term, positive interpersonal
relationship with case manager and relationship with case manager and
PCAP team.PCAP team.
Theoretical FrameworkTheoretical Framework
Stages of ChangeStages of Change
Clients will be at different stages of readiness Clients will be at different stages of readiness for change. for change.
InterventionIntervention
Motivational Interviewing:Motivational Interviewing:
• • acknowledge client’s perception of situationacknowledge client’s perception of situation• • encourage her to explore + and – aspectsencourage her to explore + and – aspects
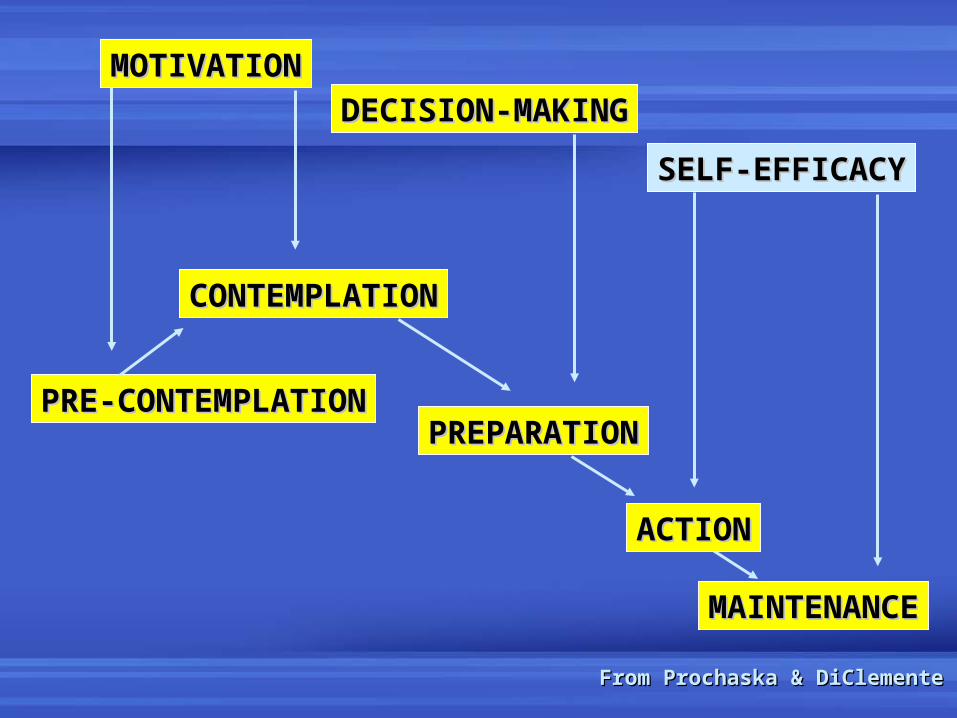
From Prochaska & DiClementeFrom Prochaska & DiClemente
MOTIVATIONMOTIVATION
DECISION-MAKINGDECISION-MAKING
SELF-EFFICACYSELF-EFFICACY
CONTEMPLATIONCONTEMPLATION
PRE-CONTEMPLATIONPRE-CONTEMPLATIONPREPARATIONPREPARATION
ACTIONACTION
MAINTENANCEMAINTENANCE
Theoretical FrameworkTheoretical Framework
Self-EfficacySelf-Efficacy
““An individual’s belief in her ability to An individual’s belief in her ability to accomplish the behaviors required to accomplish the behaviors required to produce desired outcomes.”produce desired outcomes.”
Your expectations about self-efficacy are Your expectations about self-efficacy are
influenced influenced mostmost powerfully by your powerfully by your
own history of accomplishment.own history of accomplishment.
Theoretical FrameworkTheoretical Framework
Harm ReductionHarm Reduction Addiction and associated risks are on a Addiction and associated risks are on a continuum. The goal is to reduce continuum. The goal is to reduce harmful harmful consequences of the habit for consequences of the habit for mother and mother and her child.her child.
InterventionIntervention
Any steps toward decreased risk are Any steps toward decreased risk are steps in the right direction.steps in the right direction.
IT WOULD MAKE A DIFFERENCE IN MY LIFE IF I HAD:
MORE EDUCATION
IT WOULD MAKE A DIFFERENCE IN MY
LIFE IF I HAD:
MORE EDUCATION
IT WOULD MAKE A DIFFERENCE IN MY
LIFE IF I HAD:
MORE EDUCATION
IT WOULD MAKE A DIFFERENCE IN MY
LIFE IF I HAD:
HELP WITH CHILDCARE
IT WOULD MAKE A
DIFFERENCE IN MY
LIFE IF I HAD:
BIRTH CONTROL
IT WOULD MAKE A
DIFFERENCE IN MY
LIFE IF I HAD:
DRUG AND ALCOHOL
TREATMENT
The The Difference Difference GameGame
Lessons Learned: Lessons Learned: Help Client Identify GoalsHelp Client Identify Goals
The Difference GameThe Difference Game• Identify the “baby” steps it will take to reach Identify the “baby” steps it will take to reach
each goal.each goal.
• Make sure at least some of these baby steps Make sure at least some of these baby steps are attainable in the 4-month period.are attainable in the 4-month period.
• The client must observe herself succeeding The client must observe herself succeeding in order for her to build self efficacy and in order for her to build self efficacy and move toward change.move toward change.
Client GoalsClient Goals
Lessons Learned: Lessons Learned: Quality Control Through Outcome and Process Quality Control Through Outcome and Process
EvaluationEvaluation
• • Identify program outcomesIdentify program outcomes • • Evaluate progressEvaluate progress • • Identify areas for improvement Identify areas for improvement • • Develop protocols (e.g., boundaries)Develop protocols (e.g., boundaries)
Individualized feedback helps staff see their outcomes Individualized feedback helps staff see their outcomes relative to others, encourages them to learn relative to others, encourages them to learn improvement strategies from othersimprovement strategies from others
Weekly, monthly, biannual feedbackWeekly, monthly, biannual feedback
Measure & MonitorMeasure & Monitor
Lessons Learned: Lessons Learned: Supervision, Group Staffing, Team SupportSupervision, Group Staffing, Team Support
Supervisor mSupervisor meets individually with advocates eets individually with advocates every other week:every other week:
• Review each caseReview each case• Make recommendationsMake recommendations• Discuss how the focus can be re-directed to the Big Picture and Discuss how the focus can be re-directed to the Big Picture and
client goals, and away from small crises the client can client goals, and away from small crises the client can handlehandle• Listen for common issues/problems that should be Listen for common issues/problems that should be
addressed with the group in weekly staffingaddressed with the group in weekly staffing
Group staffing once a week: Group staffing once a week: • Brain-storming, problem–solving sessions that leave Brain-storming, problem–solving sessions that leave participants in a positive frame of mind for the challenges participants in a positive frame of mind for the challenges they they faceface
Close-knit state team interaction: Close-knit state team interaction: • Meetings every 3 monthsMeetings every 3 months• Annual retreatAnnual retreat
Strategies for Preventing Strategies for Preventing
Alcohol/Drug Exposed BirthsAlcohol/Drug Exposed Births
• Alcohol/Drug TreatmentAlcohol/Drug Treatment
• Family PlanningFamily Planning
Alcohol & Drug TreatmentAlcohol & Drug Treatment
BEFOREBEFORE
• Mandated treatment may be necessary.Mandated treatment may be necessary.
• Seek women-only treatment setting.Seek women-only treatment setting.
• Seek treatment where children can stay.Seek treatment where children can stay.
• Gain cooperation of client support Gain cooperation of client support system.system.
• Prepare the client for what to expect.Prepare the client for what to expect.
Alcohol & Drug TreatmentAlcohol & Drug Treatment
DURINGDURING• Get Releases of Information signed. Get Releases of Information signed.
• Maintain boundaries with treatment Maintain boundaries with treatment agency.agency.
• Arrange for child visitation.Arrange for child visitation.
• Stay in close touch.Stay in close touch.
• Arrange for post-treatment, transitional Arrange for post-treatment, transitional housing.housing.
Alcohol & Drug TreatmentAlcohol & Drug Treatment
AFTERAFTER• Relapse is part of the disease; be explicit Relapse is part of the disease; be explicit
and honest about consequences.and honest about consequences.
• Help client identify triggers and make a Help client identify triggers and make a plan, e.g. call advocate immediately.plan, e.g. call advocate immediately.
• Introduce client to relevant support Introduce client to relevant support groups.groups.
• Consider relocation to new neighborhood.Consider relocation to new neighborhood.
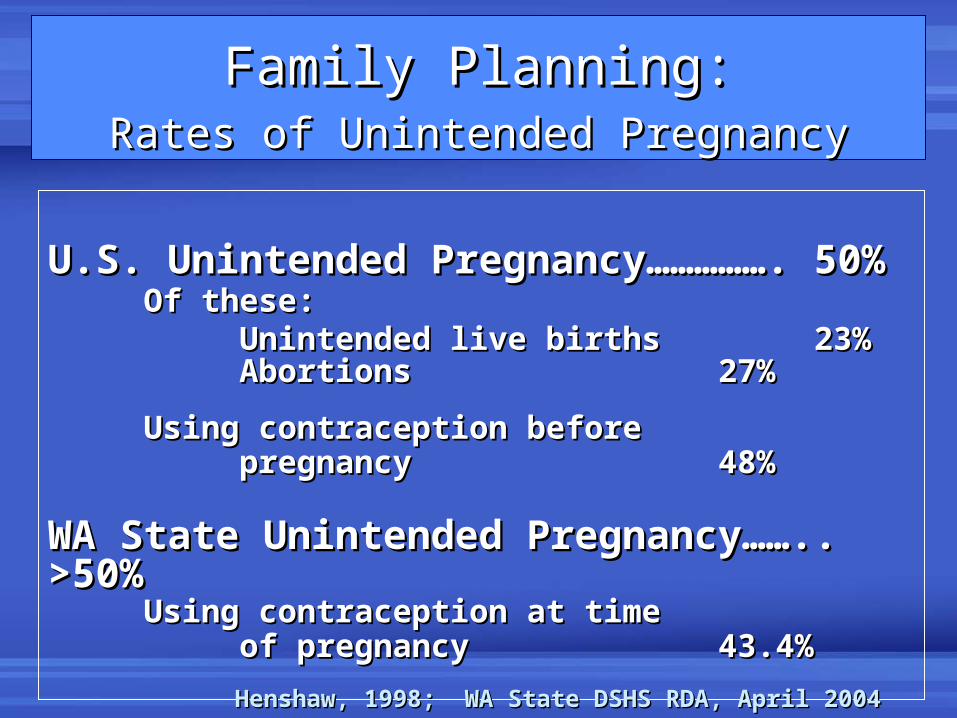
Family Planning:Family Planning:Rates of Unintended PregnancyRates of Unintended Pregnancy
U.S. Unintended Pregnancy……………. 50%U.S. Unintended Pregnancy……………. 50%Of these: Of these:
Unintended live birthsUnintended live births 23%23%AbortionsAbortions 27%27%
Using contraception before Using contraception before pregnancypregnancy 48%48%
WA State Unintended Pregnancy…….. >50%WA State Unintended Pregnancy…….. >50%Using contraception at time Using contraception at time
of pregnancyof pregnancy 43.4%43.4%
Henshaw, 1998; WA State DSHS RDA, April 2004Henshaw, 1998; WA State DSHS RDA, April 2004
Family Planning Family Planning
• Does NOT mean never having Does NOT mean never having another babyanother baby
• DOES mean having more control DOES mean having more control over whether, and when, to over whether, and when, to
have another childhave another child
Family Planning StrategiesFamily Planning Strategies
EducationEducation• Basic anatomy, how pregnancy occursBasic anatomy, how pregnancy occurs
• How various family planning methods workHow various family planning methods work
• Possible contraindicationsPossible contraindications
• Consider lifestyle and health statusConsider lifestyle and health status
• Consider cognitive and functional statusConsider cognitive and functional status
Family Planning StrategiesFamily Planning Strategies
Encourage clients to discuss, acknowledge Encourage clients to discuss, acknowledge previous experiences.previous experiences.
Motivational Interviewing: help client identify Motivational Interviewing: help client identify pros and cons of having another child; pros and cons of having another child;
revisit this topic.revisit this topic.
Reestablish client goals every 4 months. How Reestablish client goals every 4 months. How will having another child affect achieving will having another child affect achieving goals?goals?
Preventing Future Preventing Future Alcohol-Exposed BirthsAlcohol-Exposed Births
At PCAP replication sites, 78 women were binge At PCAP replication sites, 78 women were binge drinkers (drinkers (>>5 drinks/occasion) during the index 5 drinks/occasion) during the index pregnancy. pregnancy.
At PCAP exit, 51 (66%) were no longer at present At PCAP exit, 51 (66%) were no longer at present risk of having another alcohol exposed risk of having another alcohol exposed pregnancy:pregnancy:
• • 24 (31%) using reliable contraception;24 (31%) using reliable contraception;
• • 18 (23%) abstinent from alcohol/drugs >= 6 months;18 (23%) abstinent from alcohol/drugs >= 6 months;
• • 9 (12%) both reliable contraceptive and abstinent.9 (12%) both reliable contraceptive and abstinent.
Preventing Future Preventing Future Alcohol-Exposed BirthsAlcohol-Exposed Births
• Without PCAP about 30% (or 23) of 78 drinking mothers Without PCAP about 30% (or 23) of 78 drinking mothers would have had another highly exposed birth. would have had another highly exposed birth.
• We reduced that by 66%, preventing about 15 alcohol-We reduced that by 66%, preventing about 15 alcohol-exposed births. exposed births.
• The incidence of FAS is estimated at 4.7% to 21% The incidence of FAS is estimated at 4.7% to 21% among heavy drinkers.among heavy drinkers.
Therefore, we estimate PCAP prevented at least one Therefore, we estimate PCAP prevented at least one and up to three new cases of FAS.and up to three new cases of FAS.
Preventing Future Preventing Future Alcohol-Exposed Births: Alcohol-Exposed Births:
Cost SavingsCost Savings
The average lifetime cost for an individual with The average lifetime cost for an individual with FAS is $1.5 million.FAS is $1.5 million.
PCAP costs about $15,000 / client for 3 years PCAP costs about $15,000 / client for 3 years (intervention, administration, evaluation). (intervention, administration, evaluation).
If we prevented just If we prevented just oneone new case of FAS, the new case of FAS, the estimated lifetime cost savings = cost of estimated lifetime cost savings = cost of
PCAP for 102 women. PCAP for 102 women.
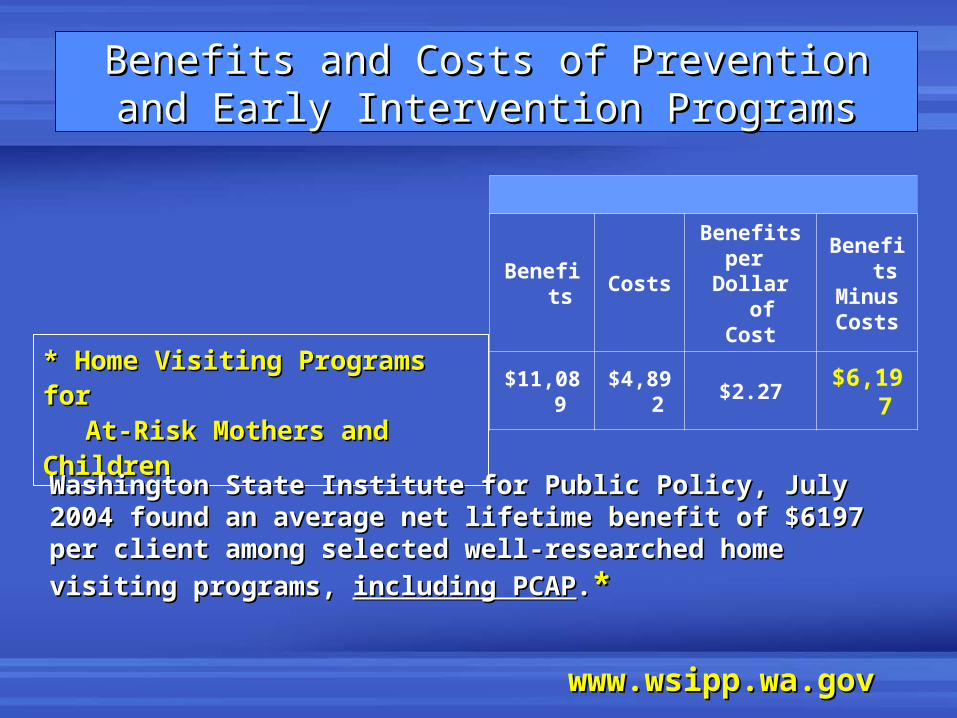
Benefits Costs
Benefitsper
Dollar of Cost
Benefits
MinusCosts
$11,089 $4,892 $2.27 $6,197* Home Visiting Programs for * Home Visiting Programs for
At-Risk Mothers and ChildrenAt-Risk Mothers and Children
Washington State Institute for Public Policy, July 2004 found an Washington State Institute for Public Policy, July 2004 found an average net lifetime benefit of $6197 per client among selected average net lifetime benefit of $6197 per client among selected
well-researched home visiting programs, well-researched home visiting programs, including PCAPincluding PCAP..**
www.wsipp.wa.govwww.wsipp.wa.gov
Benefits and Costs of Prevention and Benefits and Costs of Prevention and Early Intervention ProgramsEarly Intervention Programs

Working With Women Who Have Working With Women Who Have Fetal Alcohol Spectrum DisordersFetal Alcohol Spectrum Disorders
Pilot project funded by Pilot project funded by the March of Dimes Birth Defects Foundation the March of Dimes Birth Defects Foundation
(2001-2002)(2001-2002)
A pilot community intervention for young women with fetal alcohol spectrum disorders. A pilot community intervention for young women with fetal alcohol spectrum disorders. Community Mental Health JournalCommunity Mental Health Journal 2004, 40(6): 499–511. 2004, 40(6): 499–511.
Quality of life and psychosocial profile among young women with fetal alcohol spectrum Quality of life and psychosocial profile among young women with fetal alcohol spectrum disorders. disorders. Mental Health Aspects of Developmental DisabilitiesMental Health Aspects of Developmental Disabilities 2005, 8(2): 33–39. 2005, 8(2): 33–39.
Profile: PCAP FASD Clients (N=19)Profile: PCAP FASD Clients (N=19)
• Average age = 22 YearsAverage age = 22 Years• Mostly white (60%), unmarried(85%), and poorly educated Mostly white (60%), unmarried(85%), and poorly educated
(45%)(45%)• Troubled life history profilesTroubled life history profiles
• High levels of psychiatric distress and behavioral problemsHigh levels of psychiatric distress and behavioral problems• Poor quality of life relative to other at-risk populationsPoor quality of life relative to other at-risk populations
Family history drug/alcohol abuse (100%)Family history drug/alcohol abuse (100%) Sexual abuse (79%)Sexual abuse (79%) Physical abuse (84%)Physical abuse (84%) Unstable and disrupted care giving (100%)Unstable and disrupted care giving (100%)
Community Service Providers: Community Service Providers:
What We FoundWhat We Found• Providers knew very little about FASD.Providers knew very little about FASD.
• Providers had limited direct experience with Providers had limited direct experience with this population.this population.
• Few services were suited for individuals with Few services were suited for individuals with FASD.FASD.
• Obtaining a diagnosis in adulthood was Obtaining a diagnosis in adulthood was difficult.difficult.
• Even for experienced PCAP advocates, Even for experienced PCAP advocates, working with an FASD client was more working with an FASD client was more difficult than working with a typical PCAP difficult than working with a typical PCAP client.client.
Educating ProvidersEducating Providers
• We identified key providers interested in We identified key providers interested in the problem, and willing to work with a the problem, and willing to work with a PCAP client who has FASD.PCAP client who has FASD.
• We provided: FASD education, a PCAP We provided: FASD education, a PCAP case manager, and follow-up case manager, and follow-up consultation. consultation.
Providers learned to deliver services Providers learned to deliver services appropriately tailored to specific needs of appropriately tailored to specific needs of FASD patients. FASD patients.
Education + hands-on experience = FASD demystifiedEducation + hands-on experience = FASD demystified
Advocates’ Experience: Advocates’ Experience:
“She just doesn’t get it!”“She just doesn’t get it!”
• The impact of neuropsychological deficits The impact of neuropsychological deficits was obvious.was obvious.
• Advocates had to modify their usual Advocates had to modify their usual approaches.approaches.
• Clients were often unable to learn new Clients were often unable to learn new skills or learned them very slowly.skills or learned them very slowly.
Strategies to Use with Clients Strategies to Use with Clients Who Have FASDWho Have FASD
• Use short sentences, concrete examples, Use short sentences, concrete examples, and avoid analogies and avoid analogies
• Present information using multiple modesPresent information using multiple modes
• Simple step-by-step instructions (written Simple step-by-step instructions (written and/or with pictures)and/or with pictures)
• Role-playing Role-playing
• Ask patient to demonstrate skills (don’t rely Ask patient to demonstrate skills (don’t rely solely on verbal responses)solely on verbal responses)
• Revisit important points during each sessionRevisit important points during each session
Strategies to Use with Clients Strategies to Use with Clients Who Have FASDWho Have FASD
• Teach generalization: Don’t assume a lesson Teach generalization: Don’t assume a lesson learned in one context will transfer to learned in one context will transfer to anotheranother
• Help client identify physical releases when Help client identify physical releases when escalating emotions become overwhelmingescalating emotions become overwhelming
• Be alert for changes/transitions—monitor Be alert for changes/transitions—monitor more carefully, do advance problem-solvingmore carefully, do advance problem-solving
An experienced and clinically supported An experienced and clinically supported
case manager, working in collaboration case manager, working in collaboration
with her client and a network of educated with her client and a network of educated
providers, might reasonably expect to providers, might reasonably expect to
accomplish a number of intervention accomplish a number of intervention
steps over a 12-month period.steps over a 12-month period.
1.1. Secure stable housing, and safe placements Secure stable housing, and safe placements for the children. for the children.
2.2. Secure some financial stability for the future Secure some financial stability for the future (SSI, DDD).(SSI, DDD).
3.3. Assist clients in choosing a reliable Assist clients in choosing a reliable contraceptive method.contraceptive method.
4.4. Establish an educated network of service Establish an educated network of service providers and committed mentors who will providers and committed mentors who will continue to work with clients.continue to work with clients.
FASD clients may need life long advocacy, but FASD clients may need life long advocacy, but intervention steps can be taken in the short term:intervention steps can be taken in the short term:
““Think Younger”Think Younger”
Adjust expectations to be more Adjust expectations to be more
congruent with the individual’s congruent with the individual’s
developmental level of functioning.developmental level of functioning.
Diane Malbin: FASCETS (Fetal Alcohol Syndrome Consultation Diane Malbin: FASCETS (Fetal Alcohol Syndrome Consultation Education and Training Services, Inc.) www.fascets.org; Education and Training Services, Inc.) www.fascets.org;
[email protected]@fascets.org
Ongoing Challenge: Ongoing Challenge:
Maternal Alcohol Use During Maternal Alcohol Use During PregnancyPregnancy
It’s not “It’s not “just alcohol just alcohol ””
February 21, 2005February 21, 2005U.S. Surgeon General Releases U.S. Surgeon General Releases
Advisory on Alcohol Use in Pregnancy Advisory on Alcohol Use in Pregnancy
Women who are pregnant or who may become Women who are pregnant or who may become
pregnant should abstain from alcohol pregnant should abstain from alcohol
consumption in order to eliminate the chance consumption in order to eliminate the chance
of giving birth to a baby with any of the of giving birth to a baby with any of the
harmful effects of the Fetal Alcohol Spectrum harmful effects of the Fetal Alcohol Spectrum
Disorders (FASD).Disorders (FASD).
This updates a 1981 Surgeon General's Advisory.
If I’m pregnant, can If I’m pregnant, can I …I ………fly a plane?fly a plane?““Yes – if you could before, says Yes – if you could before, says Dr. Donald Gibb of London’s Dr. Donald Gibb of London’s Portland Hospital. In commercial Portland Hospital. In commercial jets, he says, short rides are fine jets, he says, short rides are fine up to 36 weeks.”up to 36 weeks.”
……have a beer?have a beer?““The Centers for Disease Control The Centers for Disease Control says “no level of alcohol…has says “no level of alcohol…has been determined safe,” but some been determined safe,” but some doctors feel limited drinking – no doctors feel limited drinking – no more than a pint a day, suggests more than a pint a day, suggests Dr. Gibb – after the first trimester Dr. Gibb – after the first trimester is okay.”is okay.”
……bleach or dye my hair?bleach or dye my hair?““Many doctors give a thumbs up Many doctors give a thumbs up after the first 12 weeks, so long after the first 12 weeks, so long as chemicals are kept away from as chemicals are kept away from the scalp.”the scalp.”
- People Magazine, April 17, 2006, pp 102-107- People Magazine, April 17, 2006, pp 102-107





























