Embed Size (px)
Citation preview

Suppose your patient has edema—indicating that there’s enough fluid inhis body—but his vital signs and urineoutput suggest that he’s hypovolemic.What’s going on? He’s experiencingthird-spacing, a shifting of fluid intointerstitial spaces. Find out whatneeds to be done to get that fluidback where it belongs.
MARCIA BIXBY, RN, CS, CCRN, MSCritical Care Nurse Specialist • Beth Israel DeaconessMedical Center • Boston, Mass. Consultant for Critical Care Education • Randolph, Mass.
The author has disclosed that she has no significant relationships with or financialinterest in any commercial companies that pertain to this educational activity.
YOU’RE TAKING REPORT on JohnMiller, who had a colectomy 2 days agobecause of a ruptured diverticulus. Youlearn that his heart rate has increased overthe past 24 hours, yet his blood pressurehas been gradually falling and he’s hadmarginal urine output (30 mL/hr). Mr.Miller weighs 4 kg more than beforesurgery, and he has generalized edema.
The health care team has decided not toincrease Mr. Miller’s maintenance intra-venous (I.V.) infusion of lactated Ringer’ssolution. The nurse from the previous shiftsays not to worry: His fluid will “mobilize”and he’ll “make urine” soon.
Not sure what she means by that, youhead off to check out Mr. Miller’s conditionfor yourself.
During your assessment, you find that Mr.
Miller has 2+ edema, warm skin, and palpa-ble peripheral pulses. His heart rate is 108beats/min, his blood pressure is 110/64 mmHg, and his urine output remains marginalat 30 mL/hr. Mr. Miller’s abdomen is firmand distended, with hypoactive bowelsounds. He says his pain is well controlledwith his patient-controlled analgesia infu-sion.
Mr. Miller’s edema indicates that he hasenough fluid in his body. But his vital signsand urine output seem to tell a differenttale—hypovolemia. How can you reconcilethese differences?
Who’s on third?Mr. Miller is experiencing third-spacing,which happens when fluid is trapped inthe interstitial spaces. It can occur in the
42 Nursing made Incredibly Easy! September/October 2006
Where has all the fluid gone?Third-spacing:
2.5ANCC/AACN
CONTACT HOURS

brain, lungs, abdomen, and extremities.Let’s look at the physiology of third-spacingand what you need to know to care forMr. Miller.
You may remember from your patho-physiology class that fluid moves fromintravascular (inside the blood vessel) toextravascular (outside the blood vessel)spaces and from intracellular (inside the cell)to extracellular (outside the cell) spaces (seeFluids 101). Fluid is constantly on the moveto maintain balance (see On the move).
Intravascular-to-extravascular movementof fluid occurs through diffusion, which iscontrolled by hydrostatic and capillary plas-ma oncotic pressures.
Hydrostatic pressure is the pressure thatfluid places on the wall of a blood vessel. Ifthe vessel wall is strong, as with an artery,
September/October 2006 Nursing made Incredibly Easy! 43
all the fluid gone?
On the moveFluids are constantly on the move, seeking tokeep the body in equilibrium. Here’s howthey do it. • Diffusion: This is passive movement of mol-ecules across a membrane from an area ofhigher concentration to an area of lower con-centration.• Osmosis: Water moves through a selective-ly permeable membrane from an area oflower concentration of ions to an area ofhigher concentration of ions.• Active transport: This is movement of mole-cules against a concentration as they movefrom an area of lower concentration to anarea of higher concentration. The movementrequires energy.

fluid will be held in. But if the wall is weakor semipermeable, as with a capillary,hydrostatic pressure will force fluid out ofthe vessel. Hydrostatic pressure pushes fluidfrom the arterial side of the capillary into theinterstitial space.
Intravascular or intracapillary oncotic pres-sure is determined by plasma proteins in thebloodstream. The proteins keep fluid in theblood vessel, with albumin protein mole-cules doing 70% of the work.
When oncotic pressure goes badLoss of albumin or protein leads to de-creased oncotic pressure. Fluid can nowleak from the intravascular space into theinterstitial space and stay there, causingedema. Because this fluid is lost from thecirculating blood volume, cardiac outputdecreases. You can see albumin loss in pa-tients with liver failure, liver dysfunction,or malnutrition. The low albumin levelslead to loss of fluid into the peritoneum,causing ascites.
At some point, a patient with decreased
oncotic pressure might need hypertonic orcolloid fluids, such as albumin, to “pull” thefluid in the interstitial space back into theintravascular space and increase the circulat-ing volume. Giving hypotonic fluids causesfluid to shift from the intravascular spaceinto the interstitial space, increasing intersti-tial fluid and edema. I.V. fluids that are iso-tonic should move in and out of the vascularspace equally, so that’s what Mr. Miller isreceiving (see How fluids affect cells and Quickguide to I.V. solutions).
And another thing…Even when the oncotic pressure and albu-min levels are normal, fluid can still leak outof the vessels if there’s damage to the capil-lary membranes. That’s what happened toMr. Miller. During surgery, his bowel washandled, poked, and prodded as it was re-paired, damaging tissues and destroying theendothelial cells lining the capillaries. Notgood news for Mr. Miller: Endothelial cellshelp maintain vascular integrity, which facil-itates osmosis, diffusion, and active trans-port of fluids and electrolytes.
Once Mr. Miller’s endothelial cells weredestroyed, permeability of his capillarymembranes increased, allowing fluid tomove from the intravascular space to theinterstitial space, but not back again. Oncoticpressure fell and fluid was trapped, causingedema. (Remember Mr. Miller’s 2+ general-ized edema?) The excessive fluid in theabdomen (ascites) causes increased pressureand firmness. The fluid in the interstitialspace and tissue compliance determine thelevel of pressure.
Periods of hypotension, which causehypoperfusion, along with hypoxia andischemia, can also destroy endothelial cellsand trap fluid in the interstitial space. Thiscan occur in the brain as a result of a car-diac arrest. In the lungs, fluid accumulationcan lead to cardiogenic or noncardiogenicpulmonary edema. As you saw with Mr.Miller, excessive fluid in the extremitiesleads to peripheral edema. And if the fluid
44 Nursing made Incredibly Easy! September/October 2006
Those hard-working plasmaproteins helpkeep thingswhere they
belong!
Fluids 101Fluids bring nutrition and oxygen to cells andtake away cell waste for metabolism orexcretion. This important role may be why60% of an adult’s weight is fluid. This fluid isdivided into two compartments: intracellularand extracellular.
Intracellular fluid, located inside the cells,makes up 40% of the body’s total fluid. Theremaining 60% of the body’s total fluid isextracellular fluid, which is, logically, locatedoutside the cell. Extracellular fluid is furtherdivided into interstitial (between cells, in tis-sue) and intravascular (inside the blood ves-sels) fluid.
The body’s fluid should be in balance, withthe volume entering the body equal to what’sleaving. Fluid loss can occur through urine,sweat, stool, and incidental losses from res-piratory effort.

Quick guide to I.V. solutionsA solution is isotonic if its osmolarity falls within (or near) the normal range for serum (240 to 340mOsm/L). A hypotonic solution has a lower osmolarity; a hypertonic solution, a higher osmolarity.This chart lists common examples of the three types of I.V. solutions and provides key considera-tions for administering them.
Solution Examples Nursing considerationsIsotonic • Lactated Ringer’s • Because isotonic solutions expand the
(275 mOsm/L) intravascular compartment, closely monitor the• Ringer’s injection patient for signs of fluid overload, especially if (275 mOsm/L) he has hypertension or heart failure.• 0.9% sodium chloride • Because the liver converts lactate to bicarbon-(308 mOsm/L) ate, don’t give lactated Ringer’s solution if the • 5% dextrose in water patient’s pH exceeds 7.5.(D5W; 260 mOsm/L) • Avoid giving D5W to a patient at risk for • 5% albumin increased intracranial pressure (ICP) because it (308 mOsm/L) acts like a hypotonic solution. (Although usually • Hetastarch considered isotonic, D5W is actually isotonic (310 mOsm/L) only in the container. After administration, dex-• Normosol (295 mOsm/L) trose is quickly metabolized, leaving only (295 mOsm/L) water—a hypotonic fluid.)
Hypotonic • 0.45% sodium chloride • Administer cautiously. Hypotonic solutions (154 mOsm/L) cause a fluid shift from blood vessels into cells.• 0.33% sodium chloride This shift could cause cardiovascular collapse (103 mOsm/L) from intravascular fluid depletion and increased• 2.5% dextrose in water ICP from fluid shift into brain cells.(126 mOsm/L) • Don’t give hypotonic solutions to patients at
risk for increased ICP from stroke, head trauma, or neurosurgery.• Don’t give hypotonic solutions to patient atrisk for third-space fluid shifts (abnormal shiftsinto the interstitial space)—for example, patientswith burns, trauma, or low serum protein levelsfrom malnutrition or liver disease.
Hypertonic • 5% dextrose in 0.45% sodium • Because hypertonic solutions greatly expand chloride (406 mOsm/L) the intravascular space, administer them by I.V. • 5% dextrose in 0.9% sodium pump and closely monitor the patient for circu-chloride (560 mOsm/L) latory overload.• 5% dextrose in lactated • Hypertonic solutions pull fluid from the inter-Ringer’s (575 mOsm/L) stitial space, so don’t give them to a patient with • 3% sodium chloride a condition that can cause cellular dehydration, (1,025 mOsm/L) such as diabetic ketoacidosis.• 25% albumin • Don’t give hypertonic solutions to a patient(1,500 mOsm/L) with impaired heart or kidney function—his sys-• 7.5% sodium chloride tem can’t handle the extra fluid.(2,400 mOsm/L)
September/October 2006 Nursing made Incredibly Easy! 45

46 Nursing made Incredibly Easy! September/October 2006
accumulates in the abdomen, the patientcan develop edema of the bowel, whichmay result in intra-abdominal hyperten-sion or abdominal compartment syndromeif not reversed over the first 24 to 48 hoursafter surgery.
What’s going on inside the cells?Interstitial fluid trapping causes compres-sion of the microvasculature in the distalcirculation. As the cells swell and com-press the capillaries around them, bloodflow is further impaired, leading to hy-poperfusion and ischemia. Anaerobic me-tabolism kicks in (except in the brain cells)
to sustain the cells until perfusion is re-stored. But when anaerobic metabolism
eventually fails, the sodium/potas-sium pump inside the cell starts tofail too. Sodium and potassium
switch places: Sodium moves into theintracellular space while potassiummoves into the extracellular space.
An increased level of intracellularsodium causes water to be pulled into
the cell. The cell wall membrane stretchesand releases cytokines and other mediators.Once released, mediators become active andcreate local inflammation, which furtherdamages the cells.
Mediators also get into the systemic cir-culation, where the blood gives them aride to other parts of the body. This freeride can lead to systemic inflammatoryresponse syndrome (SIRS). Organ failuremay also occur, which leads to furtherinflammation and dysfunction, release ofmediators, and progression to multipleorgan dysfunction syndrome (MODS),which increases the incidence of mortality(see Mediators of SIRS and MODS). Let’shope Mr. Miller doesn’t go down this road!
Back to Mr. MillerNow that you understand more about thefluid changes that occur with third-spacing,Mr. Miller’s vital signs aren’t surprising.
The shift of fluid into the interstitial tis-sues decreased his intravascular circulat-ing volume. The baroreceptors in the aortaand carotid arches sensed the lower vol-ume and told the sympathetic nervoussystem (SNS) to get busy. The SNS did itsjob by causing release of epinephrine andnorepinephrine, which lead to vasocon-striction of the peripheral vessels and anincreasing heart rate. Let’s take a closerlook at this process.
Vasoconstriction shunts blood from theperiphery to the major organs, which cancompromise circulation to the extremities.Compromised circulation may lead tohypoxia, ischemia, and SIRS.
You’ll want to keep a sharp eye on Mr.Miller’s perfusion: Check peripheral pulses,skin temperature and sensation, and capil-lary return on the hands and feet.
An increased heart rate kicks up cardiac out-put so that the body’s oxygen requirementscan be met. But the heart can only do somuch. If myocardial oxygen demand keepsrising, the heart won’t be able to supplyenough oxygen; myocardial ischemia orinfarction may result. Be ready to respondquickly if Mr. Miller shows signs or symp-toms of myocardial ischemia, such as chestpain.
Mr. Miller’s kidneys are doing their part tohelp out. When they sensed the decrease inglomerular filtration rate, which would hap-pen with his marginal urine output, theylaunched the renin-angiotensin-aldosteronesystem. This system causes peripheral vaso-constriction from the effects of angiotensin IIand fluid retention from the release of aldos-terone. Antidiuretic hormone is also releasedin response to low circulatory volume, and ittells the kidneys to absorb more sodiumfrom the tubules; this will also increase theabsorption of water. The goal is to increasecirculating volume, thereby boosting cardiacoutput and blood pressure. Without thiscompensatory mechanism, Mr. Miller’sblood pressure would be lower than it isright now.
This sodium andpotassium
switcheroo cancause a lot of
trouble!

September/October 2006 Nursing made Incredibly Easy! 47
Blood vessel
Normal cell
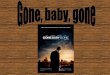
An isotonic solution has the same solute concentration(or osmolarity) as serum and other body fluids. Infusingthe solution doesn’t alter the concentration of serum;therefore, osmosis doesn’t occur. (For osmosis to occur,there must be a difference in solute concentrationbetween serum and the interstitial fluid.)
The isotonic solution stays where it’s infused, insidethe blood vessel, and doesn’t affect the size of cells.
Order up lactatedRinger’s for me and
my buddies; we couldall use some balance.
That’s right. An isotonic
solutionmaintains bodyfluid balance.
Why not? I hear it’s an
excellent choicefor hydration.
May I suggestan isotonic
I.V. solution?
How fluids affect cells: Isotonic solutions

48 Nursing made Incredibly Easy! September/October 2006
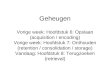
How fluids affect cells: Hypertonic solutions
A hypertonic I.V. solution has a solute concentrationhigher than the solute concentration of serum.Infusing a hypertonic solution increases the soluteconcentration of serum. Because the solute concen-tration of serum is now different from the interstitialfluid, osmosis occurs. Fluid is pulled from the cellsand the interstitial compartment into the blood ves-sels.
Many patients receive hypertonic fluids postoper-atively. The shift of fluid into the blood vesselsreduces the risk of edema, stabilizes blood pressure,and regulates urine output.
Blood vessel
Shrunken cell
Great! Thishypertonic solutionwill cause fluid toflow from the cells
into the bloodvessels.
Gulp! Thishypertonicstuff dries
me out.
Wanna try ahypertonic I.V.
solution?Yeah. I
could standto lose a
little fluid.

September/October 2006 Nursing made Incredibly Easy! 49
How fluids affect cells: Hypotonic solutions
A hypotonic I.V. solution is the opposite of a hyper-tonic solution. It has a lower solute concentrationthan serum. Infusion of a hypotonic solution causesthe solute concentration of serum to decrease.Because the solute concentration of serum is nowdifferent from the interstitial fluid, osmosis occurs.
This time, the fluid shift is in the opposite directionthan that of a hypertonic fluid. Fluid shifts out of theblood vessels and into the cells and interstitialspaces, where the solute concentration is higher.
Swollen cell
Blood vessel
Have you everhad a hypotonic
solution?Can’t say
I have.
Burp! Great stuff.
But this fluidshift has left mea little bloated.
You should try one. Ahypotonic I.V. solution
hydrates cells whilereducing fluid in thecirculatory system.

How does your patient’s
abdominal girth measure
up?
50 Nursing made Incredibly Easy! September/October 2006
One more thing: Know what Mr. Miller’sheart rate and blood pressure normally areso you can determine if his current readingsare adequate.
Big bellyOK, now you understand Mr. Miller’s vi-tal signs, but what about his abdomen?What’s causing its distension?
Remember our earlier discussion aboutfluid shifts? When fluidshifts into the interstitialspace of the bowel tissue,as has happened with Mr.
Miller, the tissue becomesedematous. The
swelling causes thebowel to expand in
the peritoneum.The abdominalskin stretches toaccommodate theedema, similar to
the way a balloon expands when you blowair into it.
We monitor this effect by measuringabdominal girth, and now we can also mea-sure bladder pressure to determine theamount of pressure the edematous bowel isgenerating.
To measure abdominal girth, wrap a tapemeasure around the patient’s abdomen atthe umbilicus and record the measurement.Remeasure abdominal girth every 4 to 8hours, making sure to place the tape mea-sure on the same spot. Report any increasedmeasurements to the health care team.
If the patient has a urinary catheter inplace, you can measure abdominal pres-sure by obtaining bladder pressure mea-surements (if you have the capability ofdoing these measurements). After clamp-ing the urinary catheter, aseptically insertan 18-gauge Angiocath in the catheter’ssampling port or connect an IAP bladderpressure monitor. Connect the system to a
Mediators of SIRS and MODSMediator EffectsTumor necrosis factor • Vasodilation
• Activation of other proinflammatory mediators
Histamine • Intense vasodilation• Increased capillary membrane permeability
Bradykinins • Vasodilation• Activation of the coagulation cascade
Platelet-activating factor • Platelet aggregation• Activation of the coagulation cascade
Myocardial depressant factor • Depressed myocardial function
Arachidonic acid cascade, an inflammation-related cascade, including:• Leukotrienes • Increased tissue permeability• Thromboxanes • Vasoconstriction of arterioles• Prostaglandins • Vasodilation

pressure transducer and level the transduc-er to the iliac crest. Instill 50 mL of sterile0.9% sodium chloride into the bladder, turnthe stopcock or valve, and obtain the pres-sure measurement at end expiration. If theintra-abdominal pressure is more than 12mm Hg, suspect that the patient has intra-abdominal hypertension (see Making thegrade).
Elevated pressure in the abdomen indi-cates increased bowel edema. As the boweledema progresses (as a result of cellularischemia and hypoperfusion) and there’smore pressure in the abdomen, the bloodreturn to the right side of the heart is im-paired; so is blood flow out of the left ven-tricle. The increased abdominal pressurecan impair lung expansion as well, leadingto respiratory distress. It can also exertpressure on the renal circulation, leading torenal dysfunction.
Mr. Miller’s edema happened quicklybecause of his surgery, so his skin can’tkeep pace with the swelling. That’s whyhis abdomen is firm. Rising pressure in theabdomen from third-spacing compressesthe major blood vessels running throughit, which causes the following problems:n in the vena cava, reduced preload (ve-nous return to the heart), leading to de-creased cardiac output, which results indecreased blood pressuren in the aorta and the iliac and femoral ar-teries, increased afterload (pressure in theperipheral circulation), further reducingcardiac output and blood pressuren in the renal vessels, impaired kidneyfunctionn in the spleen’s vasculature, impairedblood flow to the bowel, liver, and spleen.
If the fluid shift isn’t corrected and pres-sure keeps rising, Mr. Miller will developintra-abdominal hypertension or abdominalcompartment syndrome. This situationresults in a downward spiral of bowelischemia and tissue death leading to necro-sis. So you’ll want to watch him closely forsigns of intra-abdominal hypertension and
abdominal compartment syndrome: increas-ing abdominal girth or bladder pressure andincreasing pain not controlled with the pre-vious medication dosing. Early suspicion ofintra-abdominal hypertension or abdominalcompartment syndrome will allow time forinterventions to prevent or minimize tissuedamage.
What’s next?Mr. Miller’s vital signs are slightly abnor-mal but stable, so he seems to be tolerat-ing the fluid shifting. Over the next sev-eral hours (up to 48 hours), the fluid shiftwill be resolved or he will continue to de-velop bowel edema and, eventually, is-chemia.
During this time, closely monitor Mr.Miller’s vital signs, urine output, and periph-eral perfusion. Report any changes to thehealth care provider. Here are other areas tokeep tabs on:n Mental status. Is Mr. Miller responsiveand able to communicate and answerquestions appropriately? If not, his bloodpressure isn’t high enough for adequateperfusion.n Ventilation/perfusion status. Can hemaintain adequate ventilation to supporthis oxygen needs? Does he have crackles?Is his oxygen saturation greater than 97%on room air, or does he need supplemen-
September/October 2006 Nursing made Incredibly Easy! 51
Making the gradeA patient’s intra-abdominal pressure (IAP) determines if he has intra-abdominal hypertension. In a consensus statement, the World Society ofAbdominal Compartment Syndrome defines intra-abdominal hyperten-sion as “sustained or repeated pathologic elevation of IAP $ 12 mm Hg.”There are four grades of intra-abdominal hypertension, according to thisgroup: • Grade I: IAP of 12 to 15 mm Hg• Grade II: IAP of 16 to 20 mm Hg• Grade III: IAP of 21 to 25 mm Hg• Grade IV: IAP of > 25 mm Hg.
The higher the number, the more severe the condition and the greaterthe risk of complications.

tal oxygen therapy?n Hematocrit and hemoglobin. Risinghematocrit and hemoglobin levels indicatehemoconcentration of serum due to fluidshifting to the interstitial space; decreasesin these values may indicate bleeding—unless Mr. Miller’s had several liters offluid replacement solution, causing a dilu-tional effect.n Serum electrolytes. Increased sodiummay occur with hemoconcentration. Potas-sium may rise due to intracellular shiftingor if Mr. Miller is developing renal dys-function.
Elevated blood urea nitrogen (BUN) andcreatinine levels may be due to hemoconcen-
tration, but a rising creatinine with a normalBUN level may signal intrarenal dysfunction.
Lactate is produced as a byproduct ofanaerobic metabolism. In patients who’vehad bowel surgery, an elevated lactate levelmay indicate bowel ischemia—unless thepatient has liver dysfunction or failure andreceived several liters of lactated Ringer’ssolution for fluid resuscitation. The lactate inlactated Ringer’s solution is converted tobicarbonate in a healthy liver. But in a dys-functional or diseased liver, lactate isn’t con-verted; it remains in the blood.n Abdominal pressure. Measure abdomi-nal girth or bladder pressure at leastevery 4 to 8 hours while Mr. Miller’s vitalsigns are abnormal and his urine outputis low. n Fluid resuscitation. You’ll continue to
give Mr. Miller amaintenance I.V.infusion of isotonicfluid, as well as in-termittent bolusesof a colloid, such asalbumin. Albuminwill pull fluid fromthe interstitialspace into the in-travascular space.If the kidneys can’tget rid of the extrafluid on their own,a small dose of aloop diuretic likefurosemide (Lasix)can help. Remem-ber, colloid fluidsare plasma pro-teins, so theirhigher molecular structures allow you togive less volume to support Mr. Miller’sblood pressure.
If his hemoglobin is low, infusing bloodproducts, such as packed red blood cells, asneeded will help increase oxygen-carryingcapacity, as well as increase intravascularoncotic pressure and pull fluid from theinterstitial space.
What if…?If the health care provider suspects bowelischemia or necrosis, he may order a kidney-ureter-bladder (KUB) X-ray andcomputed tomography (CT) scan.
A KUB image will show the extent ofbowel edema and any “free” air, whichwould indicate bowel perforation. A CTscan detects worsening bowel edema, lackof adequate perfusion, or hematomasformed from bleeding.
A patient whose vital signs are deteriorat-ing and who has decreasing urine outputand increasing abdominal girth or bladderpressure readings will likely return to theoperating room; he may have a perforatedbowel that needs to be repaired. If the bowel
52 Nursing made Incredibly Easy! September/October 2006
Listen, I knowthings are
shifting rightnow, but give it some time
to resolve.
did youknow?Why does fluid fol-low a protein likealbumin? Proteinis a large moleculewith a negativecharge. It attractsthe most abundantextracellular fluidion—sodium—which has a posi-tive charge. Youprobably remem-ber that water fol-lows sodium. So,sodium followsprotein, and waterfollows sodium..

September/October 2006 Nursing made Incredibly Easy! 53
isn’t perforated, the surgeon still may haveto open up the abdomen to allow the edemato subside; it’ll be closed later.
A trip to the operating room is definitelyin order if the patient’s KUB film shows freeair; he needs to have that perforated bowelrepaired STAT! While they’re in there, thesurgical team will also explore the abdomenfor any further damage to the bowel relatedto perforation or edema.
It’s up to youYour clinical assessments and index of sus-picion as to what could be going on in Mr.Miller’s abdomen will help put him on thepath of continued recovery. And, yes, nowyou know just what the nurse on the othershift meant by “mobilize fluid.” n
Learn more about itAmerican Association of Critical-Care Nurses. AACNProcedure Manual for Critical Care, 5th edition. Philadelphia,Pa., Elsevier, 2005.
Klabunde RE. Cardiovascular Physiology Concepts. Philadel-phia, Pa., Lippincott Williams & Wilkins, 2004.
Kruse JA, et al (eds.). Saunders Manual of Critical Care. St.Louis, Mo., W.B. Saunders, 2003.
Macklin D, Chernecky C. Real World Nursing SurvivalGuide: IV Therapy. St. Louis, Mo., W.B. Saunders, 2004.
Malbrain ML, Cheatham ML. Cardiovascular effects andoptimal preload markers in intra-abdominal hypertension,in Yearbook of Intensive Care and Emergency Medicine. J-LVincent (ed.). Berlin, Germany, Springer-Verlag, 2004.
Rosenthal K. The whys and wherefores of I.V. fluids.Nursing made Incredibly Easy! 4(3):8-11, May/June 2006.
Urden LD, et al (eds). Priorities in Critical Care Nursing,4th edition. St. Louis, Mo., Mosby, 2004.
Urden LD, et al. Thelan’s Critical Care Nursing: Diagnosisand Management, 5th edition. St. Louis, Mo., Mosby, 2006.
World Society on Abdominal Compartment Syndrome.http://www.wcacs.org. Accessed June 29, 2006.
INSTRUCTIONS
Third-spacing: Where has all the fluid gone?TEST INSTRUCTIONS• To take the test online, go to our secure Web site at www.nursingcenter.com/ce/nmie.• On the print form, record your answers in the test answer sectionof the CE enrollment form on page 55. Each question has only onecorrect answer. You may make copies of these forms.• Complete the registration information and course evaluation. Mailthe completed form and registration fee of $22.95 to: LippincottWilliams & Wilkins, CE Group, 2710 Yorktowne Blvd., Brick, NJ08723. We will mail your certificate in 4 to 6 weeks. For faster service,include a fax number and we will fax your certificate within 2 businessdays of receiving your enrollment form. Deadline is October 31, 2008.• You will receive your CE certificate of earned contact hours and ananswer key to review your results. There is no minimum passinggrade.
DISCOUNTS and CUSTOMER SERVICE• Send two or more tests in any nursing journal published byLippincott Williams & Wilkins together and deduct $0.95 from the
price of each test.• We also offer CE accounts for hospitals and other health care facili-ties on nursingcenter.com. Call 1-800-787-8985 for details.
PROVIDER ACCREDITATION:Lippincott Williams & Wilkins, the publisher of Nursing madeIncredibly Easy!, will award 2.5 contact hours for this continuingnursing education activity. Lippincott Williams & Wilkins is accred-ited as a provider of continuing nursing education by theAmerican Nurses Credentialing Center’s Commission onAccreditation. This activity is also provider approved by theCalifornia Board of Registered Nursing, Provider Number CEP11749 for 2.5 contact hours. Lippincott Williams & Wilkins is alsoan approved provider by the American Association of Critical-CareNurses (AACN 00012278, CERP Category A), Alabama#ABNP0114, Florida #FBN2454, and Iowa #75. LippincottWilliams & Wilkins home study activities are classified for Texasnursing continuing education requirements as Type 1. Your certifi-cate is valid in all states.
Earn CE credit online: Go to http://www.nursingcenter.com/CE/nmie and receive a certificate within minutes.

54 Nursing made Incredibly Easy! September/October 2006
1. Third-spacing refers to fluid trapped in thea. intravascular spaces.b. interstitial spaces.c. intracellular spaces.
2. Third-spacing typically occurs in the extremities, ab-domen, and a. lungs.b. liver.c. kidneys.
3. In third-spacing, fluid in the body moves from thea. intravascular spaces to the extravascular spaces.b. extravascular spaces to the intracellular spaces.c. extracellular spaces to the extravascular spaces.
4. Hydrostatic pressure primarily affects thea. lymph system.b. veins.c. capillaries.
5. Loss of albumin or protein can causea. increased cardiac output.b. decreased oncotic pressure.c. decreased hydrostatic pressure.
6. Ascites is caused bya. a low albumin level and fluid accumulation in the peri-
toneum.b. decreased plasma proteins in the peritoneum.c. excess fluid in the intracellular spaces of the liver.
7. Hypertonic I.V. fluids are used as therapy because theya. pull fluid from intravascular space into interstitial space.b. replace lost proteins.c. increase circulating volume.
8. Normally, the body’s fluid is distributed asa. 75% intracellular and 25% extracellular.b. 60% extracellular and 40% intracellular.c. 20% intracellular and 80% extracellular.
9. Albumin is effective in treating third-spacing because ita. decreases oncotic pressure.b. attracts sodium and water.c. increases hydrostatic pressure.
10. How does third-spacing relate to systemic inflamma-tory response syndrome (SIRS)?a. Swollen cells of interstitial edema release mediators.b. Histamine release causes capillary vasoconstriction. c. Bradykinin release inhibits the coagulation cascade.
11. Decreased intravascular circulating volume leads toa. vasoconstriction and increased heart rate. b. vasodilation and decreased heart rate.c. vasodilation and increased blood pressure.
12. Compression of the vena cava from abdominal third-spacing can cause a. increased blood pressure.b. decreased cardiac output. c. increased preload.
13. Which lab finding may indicate postoperative bowel ischemia?a. increased sodium b. increased blood urea nitrogenc. increased lactate
14. Five percent dextrose in 1⁄2 normal saline is classified asa. isotonic.b. hypotonic.c. hypertonic.
15. Patients receiving hypertonic I.V. solutions should bemonitored for which adverse effect? a. circulatory overload b. increased peripheral edemac. decreased intravascular volume
16. Signs of abdominal compartment syndrome includeeach of the following excepta. increased abdominal girth.b. decreased bladder pressure.c. increased pain levels.
17. Rising hemoglobin and hema-tocrit in a postoperative patientprobably result from a. acute bleeding.b. fluid shifts to inter-
stitial space.c. compensation for
hypoxemia.
Third-spacing: Where has all the fluid gone?GENERAL PURPOSE: To provide the registered professional nurse with an overview of the pathophysiology, signs and symptoms,and nursing care of a patient who is experiencing third-spacing of fluids. LEARNING OBJECTIVES: After reading this article andtaking this test, you should be able to: 1. Describe the pathophysiology and complications of third-spacing. 2. Identify nursing as-sessments, monitoring, and interventions for patients with third-spacing.
2.5 ANCC/AACN CONTACT HOURS
Go to the next page for the CE Enrollment Form.
Ready to shiftinto test-taking
mode?

September/October 2006 Nursing made Incredibly Easy! 55
CE ENROLLMENT FORM Nursing made Incredibly Easy! September/October 2006A. Registration Information:
Last name ____________________________ First name ________________________ MI ______
Address _______________________________________________________________________________
City _______________________________________ State _________________ ZIP ______________
Telephone ___________________________________ Fax ___________________________________
E-mail __________________________________________________________________________________
q LPN q RN q CNS q NP q CRNA q CNM q other _______________________
Job title _________________________________ Specialty _________________________________
Type of facility _________________________________ Are you certified? q Yes q No
Certified by __________________________________________________________________________
State of license (1) __________________________ License # ___________________________
State of license (2) __________________________ License # ___________________________
q From time to time, we make our mailing list available to outside organizations to announce specialoffers. Please check here if you do not wish us to release your name and address.
q Please fax my certificate to me.
Third-spacing: Where has all the fluid gone? (page 42)B. Test Answers: Darken one circle for your answer to each question.
a b c1. m m m2. m m m3. m m m4. m m m
a b c5. m m m6. m m m7. m m m8. m m m
a b c9. m m m
10. m m m11. m m m12. m m m
a b c13. m m m14. m m m15. m m m16. m m m
a b c17. m m m
a b c1. m m m2. m m m3. m m m4. m m m
a b c5. m m m6. m m m7. m m m8. m m m
a b c9. m m m
10. m m m11. m m m12. m m m
a b c13. m m m14. m m m15. m m m16. m m m
a b c17. m m m
a b c1. m m m2. m m m3. m m m4. m m m
a b c5. m m m6. m m m7. m m m8. m m m
a b c9. m m m
10. m m m11. m m m12. m m m
a b c13. m m m14. m m m15. m m m16. m m m
a b c17. m m m
C. Course Evaluation*
1. Did this CE activity's learning objectives relate to its general purpose? q Yes q No
2. Was the journal home study format an effective way to present the material? q Yes q No
3. Was the content relevant to your nursing practice? q Yes q No
4. How long did it take you to complete this CE activity?___ hours___minutes
5. Suggestion for future topics
____________________________________________________________________________________
D. Two Easy Ways to Pay:q Check or money order enclosed (Payable to Lippincott Williams & Wilkins)q Charge my q Mastercard q Visa q American Express
Card # _____________________________________________ Exp. date __________________ Signature __________________________________________________________________________
Photocopies of this page will be accepted.*In accordance with the Iowa Board of Nursing administrative rules governing grievances, a copy of your evaluation of the CE offering may be submitted directly to the Iowa Board of Nursing.
Acute pancreatitis: Inflammation gone wild (page 18)B. Test Answers: Darken one circle for your answer to each question.
C. Course Evaluation*
1. Did this CE activity's learning objectives relate to its general purpose? q Yes q No
2. Was the journal home study format an effective way to present the material? q Yes q No
3. Was the content relevant to your nursing practice? q Yes q No
4. How long did it take you to complete this CE activity?___ hours___minutes
5. Suggestion for future topics
____________________________________________________________________________________
Bad blood: Tips for preventing CR-BSIs (page 30)B. Test Answers: Darken one circle for your answer to each question.
C. Course Evaluation*
1. Did this CE activity's learning objectives relate to its general purpose? q Yes q No
2. Was the journal home study format an effective way to present the material? q Yes q No
3. Was the content relevant to your nursing practice? q Yes q No
4. How long did it take you to complete this CE activity?___ hours___minutes
5. Suggestion for future topics
____________________________________________________________________________________
Registration deadline:
October 31, 2008
Contact hours: 2.5
Fee: $22.95
Test code: NMIE1206
Registration deadline:
October 31, 2008
Contact hours: 2.5
Fee: $22.95
Test code: NMIE1306
Registration deadline:
October 31, 2008
Contact hours: 2.5
Fee: $22.95
Test code: NMIE1106
Mail completed test with registration fee to: Lippincott Williams & Wilkins,CE Group, 2710 Yorktowne Blvd., Brick, NJ 08723.





![Explicit strategies for incompressible fluid-structure ... · amountofadded-massinthesystemisstrong(see,e.g.,[7,21]). Inviewofthis,muchresearch effort has gone into the design of](https://img.pdfslide.net/doc/110x75/5ebafd1ce1762160253c9810/explicit-strategies-for-incompressible-fluid-structure-amountofadded-massinthesystemisstrongseeeg721.jpg)