Embed Size (px)
Citation preview

1
This Handbook Belongs to

2

3
CCOONNTTEENNTTSS Introduction 44 Patient Assessment 55 Wound Assessment-Key Tasks 66 Wound Aetiology 77 Leg Ulcers 77 Diabetic Foot Ulceration 99 Pressure Damage 1100 Issues That May Complicate Healing Wound pain 1155 Lymphoedema 1166 Lacerations 1177
Debridement of slough (including Larvae) 1188 Topical Negative Pressure (TNP) 1188 Excessive exudate 1199 Infection & critical colonisation 2200
Other wound types 2211 Peri-wound dermatology problems 2211 Emollients 2233 Over granualtion 2233
Nutrition 2233 The Wound Continuum 2244 The Wound Formulary Products
Dressing packs 2288
Wound measurement 2288 Tapes 2288 Cleansing solutions 2288 Emollients 2299 Skin protective’s 2299
Steroid Tape 3300 Retention bandages 3300 Low adherent contact layers 3311 Non adherent contact layers 3311 High absorbent 3322
Hydrogels 3322 Pressure relieving devices 3333 Foams 3344 Alginates 3355 Hydrocolloids 3355
Film 3366 Antimicrobial 3377 Compression 4400 Hosiery applicators 4422
Shoes 4444

4
IINNTTRROODDUUCCTTIIOONN
This handbook aims to assist clinicians in making good clinical decisions with regard to caring for patients with a wound or other tissue viability related problems. It includes a wound care formulary intended to act as a guide for choosing dressings within each specified category. Products have been chosen following consideration of efficacy, safety, patient acceptability and value. A wide range of clinical evidence has been used in this decision making. The information in this formulary should support the provision of cost effective practice- this does not mean a cheap option but a rational approach that provides:
Optimal healing environment based on available evidence. Dressings that are comfortable and acceptable to patients Dressings that are quick, easy to apply/ remove and have appropriate wear time. Detailed information about products listed is available from the manufacturers literature. If necessary, medical prescribers, nurse prescribers and non-medical prescribers may prescribe or order wound management products not detailed within the formulary. Prescribers are encouraged to contact the tissue viability team to discuss individual cases. The rationale for choosing a product should be documented in detail in the patients’ notes. In scenarios where patients are shared care e.g. dermatology, podiatry, vascular and community services, it is helpful to communicate any care plan changes and their rationale with all the involved teams. All wound care prescribing will be monitored through ongoing audit of PACT data and supplies ordering. The clinical advice given in this document are key points only and further training regarding wound assessment and wound care/ prevention will also be required to support this documentation. Company representatives who visit should do so in accordance with trust policy and should only discuss products that are within this wound care formulary. Representatives may give additional support for product use that is outside the wound care formulary for individual cases. All new tissue viability related products should be directed to theTissue Viability Speciality Nurses. We thank the members of the multi-disciplinary team for their help in updating this handbook. We thank the many companies for the information provided on products and support given.

5
Patient Assessment
For your own safety and security, risk assessments should be used when there are
increased complexities for example constrained environment for leg care, manual handling.
Patients move between wards, hospitals, nursing homes and their own homes. It is vital
that up to date information is communicated regarding tissue viability at all times. Identify who else is or will be involved in providing ongoing wound care of your patient
e.g. podiatry, dermatology, vascular surgeons, relatives, district nurses and practice nurses.
Holistic assessment of the patient and goals should be specific and realistic to your
patients’ requirements. Concordance can sometimes be an issue in tissue viability. Patients’ values and
agreement must be incorporated within care plans, with accurate documentation especially when planned care is not accepted and alternative treatment plans are initiated.
A continual programme of study days including wound assessment, leg ulcer
management, pressure ulcer prevention, diabetic foot care, lymphoedema and competency training for HCA’s is regularly delivered by the TVN’s.
Assessment is of paramount importance for optimal skin/ wound care.

6
WOUND ASSESSMENT
Key tasks Diagnose the aetiology (type) of the wound
Identify and address any issues that may delay healing (i.e. pathological, nutritional or social problems associated with wound healing)
Record the wound details to provide a baseline against which planned interventions can be measured Set specific and realistic goals
Diagnosis of wound aetiology (type)
Possible aetiologies include: Leg Ulceration (venous, arterial, mixed) Diabetic Foot Ulceration Pressure Ulceration Fungating wounds
Burns Laceration Post surgical wounds
Issues that may delay healing include:
Pain Presence of slough Excessive exudate Infection Peri-wound dermatology problems (allergy, excoriation, varicose eczema) Overgranulation
Lymphoedema Inadequate nutrition Unrelieved pressure / trauma Lower leg venous hypertension Arterial insufficiency Psychological problems relating to
wounding including compliance issues.
Wound care documentation:
The stage of wound healing; The depth of the wound; The shape and size of the wound; The wound edges; The amount of wound exudate;
The position of the wound Odour Pain Infection Condition of surrounding skin
Specific and realistic treatment aims may be:
To reduce wound pain To reduce pressure To debride slough To manage of exudate To promote granulation To promote epithelialisation To promote venous return To promote lymphatic drainage To promote arterial supply To reduce microbial load (infection) To rehydrate Peri-wound skin To protect peri-wound skin To improve nutrition
Please seek advice from the Tissue Viability team if you are unsure about the most
appropriate way to manage a particular wound.

7
The Wound Continuums Clinicians are encouraged to use the wound continuums (which can be found in the middle pages of this handbook) to assess, document and evaluate the treatment in a common language.
DIAGNOSIS OF AETIOLOGY
Leg Ulceration
Definition: “an open lesion between the knee and the ankle joint that remains unhealed for at least four weeks and occurs in the presence of venous disease” (3) Assessment Full clinical history and physical examination Detailed visual examination of both legs for signs of venous and arterial disease Measurement of blood pressure, weight, urinalysis and Doppler assessment of Ankle
Brachial Pressure Index (ABPI) ABPI (Doppler)
Right ABPI = Highest right ankle reading Highest brachial reading
Left ABPI = Highest left ankle reading
Highest brachial reading
Formally record ulcer size
Treatment Simple non-adherent dressings are recommended in the management of venous leg
ulcers. Simple emollient to dry skin as required Topical steroid ointment to areas of varicose eczema
Venous Leg Ulceration with adequate arterial supply (ABPI = 0.8 - 1.2) 40mmHg Multi-layer graduated compression therapy (bandaging or hosiery) to be
changed weekly or more frequently if there is heavy exudate. On healing, life time ongoing assessment with compression hosiery
Venous Leg Ulceration with reduced arterial supply (ABPI = <0.8 or >1.2) Discuss with a tissue viability nurse Reduced graduated multi-layer compression systems (bandaging or hosiery) Discuss with GP/Medical staff possible referral to vascular surgeon
Arterial Leg Ulceration or Venous Leg Ulceration with very reduced arterial supply (ABPI =< 0.6) Discuss with Tissue Viability Nurse Wadding and Crepe bandage (type 2A bandage) bandaging applied with no
compression Urgent referral to GP/Medical staff for potential vascular surgeon referral.
Do NOT carry out Doppler Assessment with;
Uncontrolled pain If the patients clinical condition excludes it (i.e. Palliative) Active DVT without therapeutic levels of anticoagulation therapy Informed consent not obtained

8
Ongoing Assessment
Doppler Assessment of ABPI should also be conducted when:
An ulcer is deteriorating If not fully healed by 12 weeks When ulceration recurs Before recommencing compression therapy When a patient is to commence wearing compression hosiery as a preventative
measure There is a sudden increase in ulcer size There is a sudden increase in ulcer pain Foot colour and / or temperature of foot change Ongoing assessment (three monthly)
References
1. NHS CRD (1997) Compression therapy for venous leg ulcers. Effective Health Care Bulletin 3 (4) 1-12
2. RCN (2006) Clinical Practice guidelines. The nursing management of patients with venous leg ulcers
3. Scottish Intercollegiate Guidelines Network (2010) Management of Chronic Venous Leg ulcers (guideline No. 120)

9
High Risk Foot Ulceration (Including diabetes) Ulcers on the foot have additional factors (e.g. callus, walking, and deformity) which can prevent them from healing. Some dressings will behave differently when walked on. For this reason all ulcers on the foot should be referred to Podiatry for assessment. High risk feet are considered to be those which have neuropathy or ischaemia. Any diabetes related foot ulcer should be referred to Podiatry within 24 hours for assessment (NICE 2004)
Assessment Refer to a podiatrist for assessment, which should include:
Vascular assessment Neurological assessment Assessment of foot deformity Ulcer assessment Neuropathic origin Ischaemic origin
Swabbing and culture of an ulcer is usually only indicated if there are clinical signs of infection (heat, redness, swelling, or pain)
Treatment Multi-disciplinary approach involving a diabetes specialist podiatrist, community nurse & GP
Key points in the management of high risk foot ulcers are: Mechanical control (relief of pressure) Wound control (debridement and dressings) Vascular control (interventions to improve the vascular supply to the foot) Microbiological control
Refer diabetic patients to a multidisciplinary foot care team within 24 hours if any of the following occur:
New ulceration New swelling New discolouration (redder, bluer, paler, blacker over all or part of the foot) Signs or symptoms of infection (redness, pain, swelling or discharge) Suspected Charcot’s foot
An urgent medical opinion should be sought if any of the following occur: Pink or pale, painful, pulseless foot (indicating critical ischaemia) Spreading cellulitis, lymphangitis Crepitus Systemic symptoms of infection Lack of response to oral antibiotics for infection Suspicion of bone involvement (osteomyelitis) Immunocompromise or physiological instability of the patient
NHS Clinical Knowledge Summary – Diabetes- Foot Disease 2007

10
Pressure Ulcer Prevention
Key tasks (Refer to Appendix A, ‘Guidance on pressure ulcer prevention and management’ contained within the Wound Prevention and Management Policy)
Ensure the patient/carers are aware of the risk of pressure ulceration, how, when and
where to check skin for colour changes. All patients should receive written information about pressure ulcer prevention in both acute and community settings.
Pressure ulcer risk assessment is completed Early reporting is crucial and be guided by policy When skin changes are reported - Confirm diagnosis ( exclude moisture lesion) Explore history of the patient in the days pre - development of the ulcer Recording no pressure damage is as important as recording pressure damage Set specific and realistic goals with the patient All mattresses as minimum should be High Specification static foam, if not a reason
must be documented within the patients notes. Ensure Root cause analysis of all Category 3, 4 and unstageable pressure ulcers.
Category 4 pressure ulcers are to be reported as SI’s- refer to matron or TVN for advice.
Issues that may increase the risk
Length of time in contact with a surface Hardness of the contact surface Movement between the 2 surfaces ( e.g. friction on a heel or during a fall) Level of moisture between the 2 surfaces ( e.g. incontinence, air flow) Clothing, bedding and pads in use Pain from clinical conditions decreasing the stimulus to move Patients preferred position in bed Patients who sleep in their chairs and sitting posture Faulty, incorrect equipment and inappropriate use Disease progression Ensure patient/carers/ staff know who to report faulty equipment to. Equipment usage
and condition is audited regularly. If not in use return.
Pressure Ulcer Documentation Categorise and report as soon as possible, if unstageable recategorise as depth
becomes evident Wound assessment, care plan, progress and evaluation. Equipment in use / requested / confirmation that equipment has been received and
installed correctly and patient using. Repositioning Schedule is being accepted ( record if the patient repositions
themselves back into their favourite position or refuses repositioning offered) Patients/carers acceptance and involvement in care plan Complete skin bundles/ comfort rounds if used
Pressure Ulcers and Podiatry
Please refer in patients to Podiatry for heel ulcers, as they need additional off loading and protecting from shear /stress.

11
Pressure Ulcer Categorisation (EPUAP, 2009)
Category 1
Non-Blanchable Erythema of intact skin with non-blanchable redness of a localised area, usually over a bony prominence. Darkly pigmented skin may not have visible blanching; its colour may differ from the surrounding area. The area may be painful, firm, soft warmer or cooler as compared to adjacent tissue.
Action to take: Document in nursing records. Ensure Waterlow / PURAT and nutritional risk assessments have been undertaken and appropriate action instigated. Implement comfort rounding High risk static foam mattress recommended. Assess for pressure relieving cushion.
Category 2
Partial Thickness Skin Loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough. May also present as an intact or open/ ruptured serum-filled or sero-sanginous filled blister. Not to be confused with skin tears, tape burns, leg ulcers, incontinence associated dermatitis, maceration or excoriation. Bruising indicates deep tissue injury.
Action to take: As Grade 1 plus… Assess for alternating pressure relieving mattress and cushion Implement comfort rounding. Implement wound care plan Datix report.
Category 3
Full Thickness Skin Loss where subcutaneous fat may be visible but no bone, tendon or muscle. Slough may be present. May include undermining or tunnelling. The depth of the ulcer varies by the anatomical location as some areas do not have subcutaneous tissue and therefore grade 3 maybe shallow. In contrast, areas of certain anatomical location can be extremely deep.
Action to take: As grade 2 plus… Admitted with – TVN Discharge Liaison team. Safeguarding Since admission– TVN, Matron, and Safeguarding Vulnerable Adult team Community acquired – TVN, Datix report and root cause analysis. Safeguarding vulnerable adults team. Inform manager. Nursing Homes- Refer TVN, report to CQC. Safeguarding. TVN to Datix.
Category 4
Full Thickness Tissue Loss with exposed bone, tendon or muscle. Slough or eschar may be present. The depth of a grade 4 varies by anatomical location. Grade 4 pressure ulcers extend down to the muscle and/ or supporting structures (facia, tendon or joint capsule) making osteomylitis or osteitis likely to occur. Exposed bone or muscle is visible or directly palpable.
Action to take: As above and Root cause analysis Serious Untoward Incident

12
Unstageable Full thickness tissue loss in which actual depth of the ulcer is completely obscured by slough (yellow, tan, grey, green or brown) and/ or eschar (tan, brown or black) in the wound bed. Until they devitalised tissue is removed to expose the base of the wound, the true depth cannot be determined; but it will be either grade/ category 3 & 4. Stable eschar on the heel serves as the body's natural (biological) cover and should not be removed.
Action to take:
• As grade 3. • Re-classify when true grading is
apparent. • Admitted with – TVN, Discharge
Liaison team . safeguarding • Since admission– TVN, Matron,
and Safeguarding Vulnerable Adult team.
• Root cause analysis
DATIX Reporting All categories 2 s and above MUST be entered to DATIX system. Report via datix for each pressure ulcer, you will be asked to complete the on line form. All category 3, 4 and unstageable ulcers will be investigated through Root Cause Analysis, initiated by the line manager. If a problem relating to safeguarding is suspected then follow guidelines regarding the procedure. Nursing Homes MUST report all grade 2 and above to CQC.

13
Skin Management of Incontinent Patients
Skin Condition Type: Treatment:
Normal intact
skin Moisturise if skin dry
Faecal and/or urinary incontinent intact skin. Erythema and dermatitis but no broken areas
Keep skin clean and dry. Document. Determine the cause of incontinence. Use barrier cream.
Faecal and/ or urinary incontinence, excoriated and weeping
Keep skin clean and dry. Document. Determine the cause of incontinence. Use barrier cream. Use barrier film. Analgesia. More frequent hygiene.
Kissing ulcer. Caused by moist skin surfaces
Assess depth; decide whether dressing or barrier cream is appropriate. More frequent hygiene.
Prevention
Liquid or loose stool? Bed bound? At risk of skin damage?
Discuss with TVN & Infection Control. Use of faecal management system, for example Flexi-Seal in accordance with colorectal surgeon advice.

14
COMMUNITY TEAMS ONLYComplete Pressure Ulcer Risk Assessment Tool (PURAT)
Does the patient have a pressure ulcer?
Yes No Is the patient at risk of pressure damage?
Yes NoWhat is the location of the
damage / potential damage?
Consider need for OT referral and/or TVSN referral for equipment
Body (except heel)
Body and heel
Heel onlyReposition to achieve
zero pressure. (Pressure relieving
equipment is unlikely to be beneficial)
Is it a grade 2 or above?
NoYes
Complete a Datix report and refer all Grade 3 and
4’s to TVSN
Can the pressure be relieved by repositioning?
NoYesCommence repositioning/carer /patient education on repositioning
What is level of risk?
Low (Green)
Medium (Amber)
High (Red)
Is the patient mostly cared for in bed? (20-24 hrs/day)
Yes
Alternating replacement mattress
No
High Spec Foam overlay/replacement mattress and repositioning
Document care/ equipment offered and
patient’s informed decision
Complete CELS request form and fax on day of assessment

15
Wound Pain Assessment - Carry out assessment to identify type of pain. An assessment tool is required e.g numerical rating scale of 1-10 at rest and during dressing change. Nociceptive pain is a response to painful or noxious stimuli ( tissue damage) and is usually time limited. Can be described as dull, aching or tender with various intensities. Neuropathic Neuropathic pain is pain initiated or caused by a primary lesion or dysfunction in the peripheral or central nervous system. For example pain following shingles, or an amputation, or spinal cord trauma. Pain that occurs in diabetics or in patients with multiple sclerosis .Can be shooting, burning or stabbing. Treatment
Treat cause e,g infection. Minimise trauma by selecting a less adherent dressing Refer to GP/Medical staff for assessment and analgesia regime Non medical prescribers may prescribe from the nurse prescibers formulary within their
sphere of competence.

16
Lymphoedema – lower limb Definition: the accumulation of fluid and other tissue elements in the interstitial space due to
insufficiency in the transport capacity of the lymphatic system. Primary lymphoedema – due to congenital malformation of the lymph conducting
system Secondary lymphoedema – results from damage to the lymphatic vessels or lymph
nodes due to trauma, disease, surgery, infection, irradiation, immobility and dependency syndrome
Assessment
Full clinical history and physical examination Detailed visual examination of both legs for signs of lymphoedema, venous and
arterial disease Measurement of blood pressure, weight, urinalysis and doppler assessment of
ankle brachial pressure index (ABPI) Formal record of ankle and calf measurement
Treatment
Good skin care (gentle hygiene with adequate moisturisation) Exercise and movement Patient education including understanding Multilayer inelastic compression bandaging or hosiery
Caution in patients with:
Acute cellulitis Uncontrolled cardiac failure Acute DVT Untreated trunk or genital oedema Latex allergies / sensitivities Arterial insufficiency (ABPI <0.8 or >1.2) Diabetes and rheumatoid arthritis

17
Lacerations Treatment Options for Skin Tears & Haematomas Type 1
Wound is clean. Skin edges are easily apposed without applying tension to the flap. May be ‘glued’ or have Steristrip if no fear of flap tension. If surrounding skin is vulnerable Soft silicone dressing or non adherent hydrocolloid would be most appropriate. May require compression bandaging (APBI must be assessed prior) Leave intact 7days unless leakage evident to outer layer.
Type 2 Laceration / flap with minimal necrosis Gentle cleaning. Application of soft silicone or none adherent dressing. Limb elevation. May require compression bandaging (ABPI must be assessed prior). Leave intact 7days unless leakage evident to outer layer.
Type 3
Laceration with flap, moderate to severe haematoma and/or necrosis – may require surgical intervention Requires debridement & possible skin graft. If for conservative management, treat as Type 2.
Type 4
Major Degloving Injury Emergency transfer to Trauma unit only

18
Debridement of Slough Slough is the presence of devitalised tissue within the wound bed, which is thought to increase the risk of infection, malodour and delay healing. Assess vascular supply before considering hydrating necrotic tissue. Treatment - Options Autolytic debridement - slough separates from the wound bed as part of the healing
process. Dry wounds - use fluid donating dressings (e.g. hydrogels or hydrocolloids). Moist wounds - use absorbent dressings (e.g. alginates, foam)
Sharp debridement - dead tissue is removed using a scalpel Sharp debridement should only be undertaken by clinicians with proven skills in this area. Sharp debridement of the foot should only be undertaken by registered podiatrists or surgeons.
Surgical debridement - dead tissue is removed using a scalpel down to the level of a bleeding wound bed. Surgical debridement should only be undertaken by clinicians with surgical qualifications Surgical debridement of the foot should only be undertaken by registered podiatrists or surgeons
Biosurgical debridement – dead tissue is removed by the application of clinical larvae. Biosurgical debridement should only be undertaken following consultation with the Tissue Viability Nurse.
Topical Negative Pressure
TNP Therapy (also known as Topical Negative Pressure or Negative Pressure Wound Therapy) TNP therapy uses continuous and/or intermittent negative pressure to remove infectious materials and/or fluids from the wound bed. The manufacturers propose that TNP therapy promotes wound healing. TNP therapy may be considered as a possible treatment option for patients with chronic, acute, traumatic, subacute and dehisced wounds, partial-thickness burns, ulcers (such as diabetic or pressure), flaps and grafts when complicated healing is anticipated due to: very heavy exudate which requires very frequent dressing change (at least daily) e.g.
orthopaedic trauma wounds, dehisced wounds, reduced arterial supply where stimulation of blood flow may enable an adequate
circulation to be established. e.g. arterial leg ulcers, diabetic foot ulcers The advice of the Tissue Viability team must be sought prior to use. There are several TNP systems available, please speak to your TVN.

19
Excessive Exudate
Chronic wound exudate contains elevated levels of inflammatory mediators and protein-digesting enzymes and can cause excoriation Possible causes of excessive exudate include: Infection Venous hypertension Lymphoedema Heart failure
Colour Possible Cause Clear amber Normal serous exudateCloudy, milky / creamy Possible presence of fibrin strands (inflammatory response) OR infectionPink or red Presence of blood cells – capillary damageGreen Possible bacterial infection Yellow or brown Presence of slough or material from enteric or urinary fistula Grey or blue May be related to use of silver productsConsistency Possible Cause Thick / sticky High protein content possibly due to:
Inflammatory process Infection Necrotic tissue Enteric fistula Residue from dressing
Thin / runny Low protein content due to: Venous or congestive disease Malnutrition Urinary, lymphatic or joint space fistula
Odour and quantity should also be assessed Treatment
Commence appropriate treatment for underlying cause Protect the peri-wound skin using a skin protectant Ensure sufficiently frequent dressing changes Use absorbent dressings Consider use of advanced therapies (e.g. Topical Negative Pressure therapy)

20
Infection Assessment 1. Diagnose infection or critical colonisation from clinical signs and symptoms
Signs of infection in chronic wounds Increased intensity and / or change in character of pain Discoloured or friable granulation tissue Increasing malodour Wound breakdown Delayed healing
The classical signs of infection may be reduced or masked by dermatological problems. 2. Send a wound swab for C & S only if the wound is diagnosed as clinically
infected and microbiology information is needed to inform the choice of antibiotics.
To swab a wound:
Thoroughly clean wound bed with saline Moisten swab prior to use if wound is dry and swab across the
abnormal areas of the wound bed, localised pressing of the swab into the ulcer bed until it has
absorbed visible amounts of tissue fluid Avoid areas of slough. Place swab in transport medium. refrigerate. Complete the request form, with as much relevant information as
possible and send to the laboratory ASAP Do not use topical antibiotics as they will be ineffective and the risk of developing resistance 3. Please refer to the Infection Continuum on pages 25&26 for further information
and the appropriate treatment. 4. The request form for all samples needs to indicate clearly the clinical features indicating
the presence of spreading/systemic infection. Comments such as "leg ulcer? Infected" are unhelpful.

21
Other Wound Types
Fungating Wounds These wounds may present at an advanced stage. Care plans must incorporate patient wishes and issues. Aroma, risk of severe bleeding and exudate may increase the risk of social isolation and fear. Products may be available to address these issues,please consult TVN.
Radiotherapy Skin exposed to radiotherapy requires care when washing and certain creams and dressings may affect the therapy. Please consult the radiotherapy centre for guidance especially if skin damage presents post therapy.
Surgical Wounds Details of the skin closure method should be included in the discharge information. Most wounds heal with minimal no complications. Remember the inflammatory stage of wound healing extends 2 -3 days post op – do not confuse with signs of infection. Exudate (serous fluid) produced by a wound requires a dressing. Do not disturb too frequently without good reason. Ensure the patient is aware of the signs of infection and who to report to. Do not automatically resort to antibiotics – consider treatment with antimicrobial dressings
Trauma, Thermal and Chemical Injuries The time, mechanism and circumstances of an injury will determine subsequent tissue damage both internal and external. These with immediate and subsequent first aid are crucial pieces of information for paramedics and A & E staff.
Peri-wound dermatology problems
A referral to a specialist dermatologist should be sought for any unidentifiable or complex dermatological problems. However, these more simple conditions may be managed as follows:
Eczema
Varicose eczema Associated with increased capillary pressure due to venous hypertension Often confused with cellulitis
Treatment: Soften any skin scales (Soak for 10-20 minutes in warm water then massage with simple
bland emollient) If inflamed apply ointment-based topical moderately potent corticosteroid - Treatment
should usually only be for a few days. Once inflammation has subsided, replace corticosteroid ointment with simple emollient Reverse venous hypertension through compression therapy providing there is adequate
arterial supply (Calculate ABPI using Doppler) (See p7 ). Exogenous eczema - e.g. irritant and allergic contact dermatitis Appears on second contact with allergen. If reaction is severe may spread beyond area of direct contact 60% of patients with chronic leg ulcers demonstrate contact sensitivity associated with
treatment

22
More common in patients with co-existing stasis eczema. Common allergens for leg ulcer patients: lanolin, topical antibiotics, cetylstearyl alcohol,
cetyl alcohol, stearyl alcohol, cetostearyl alcohol, rubber, parabens (hydrobenzoates), fragrance, and hydrocortisone.
Assessment Patch testing of suspected dressings (by taping a small piece of the suspected dressing
to the patient’s inner arm) Treatment Avoid allergen Steroid ointment to reduce inflammation Referral to dermatologist if unable to resolve allergic issues
Topical Steroids (not exhaustive) Strength Generic Name Frequency of application/notes Mild Hydrocortisone 0.1%-2.5% Once or twice daily
Moderately potent
Clobetasone butyrate 0.05% Once or twice daily
Potent Beclometasone dipropionate 0.025% Once or twice daily Expensive +++ for primary care
consider better value alternative Betamethasone dipropionate 0.05% Once or twice daily Betamethasone valerate 0.1% Once or twice daily Fluticasone propionate 0.05% or 0.005% Once or twice daily – note difference
in strength of cream and ointment Hydrocortisone butyrate 0.1% Once or twice daily Fluocinolone acetonide 0.025% Once or twice daily Mometasone furoate 0.1% Once daily
Very potent Clobetasol propionate 0.05% Once or twice daily for up to 4 weeks; max 50g of 0.05% preparation applied per week
Please note some steroid preparations are listed as “1 in 4 dilutions”, refer to current BNF
regarding strength and subsequent potency Advice on using topical steroids
Never use instead of moisturisers – use as well Use as second line interventions after moisturisers and to control flare ups. Steroid should be applied to all areas of active eczema, i.e. any reddened, thickened,
excoriated or raw areas. Information in the packaging advises against the application to open areas, but this means to cuts and grazes rather than the open areas, which are part of the eczematous process.
Use only on eczematous areas and use lowest potency possible Apply sparingly, e.g. ‘enough to make the skin look shiny. Use ointment formulations rather than creams as they are greasier; the exception is very
wet or weepy eczema where creams should be used. Apply steroid 20-30 minutes after applying moisturiser to prevent dilution of steroid effect.
For this reason mixtures of steroid and moisturiser are not recommended. Carers should wear gloves when applying steroids or wash their hands after doing so.

23
Emollients
Emollients- Soothe, smooth and hydrate the skin. Affects are short lived and frequent application is necessary. Useful for dry eczema. Apply in direction of hair growth. Patients own choice is important. Patients should be told to keep away from fire or flames and not to smoke when using these preparations. Consider the following option when prescribing emollients:
a) Use the patients own emollient where possible incorporating own choice. b) Use aqueous cream as a wash and as an emollient only if the patient has no reactions
to aqueous cream and this is a light emollient only. c) Then consider other products (examples are listed in the formulary but other products
are available). d) Use a pump dispenser for hygiene reasons. e) Use correct dilution when using emollient bath additives. f) Antimicrobial skin washes should be re-assessed regularly.
Overgranulation/Hypergranulation Excessive granulation that prevents re-epithelialisation Treatment: Reduce moisture level at wound bed through use of a more absorbent dressing Consider use of topical antimicrobial (e.g. Inadine) Consider use of topical steroid cream or steroid tape.(Haelan tape)
Nutrition Assessment Patients judged at risk of malnutrition should be assessed using a nutritional screening
tool to assist in the decision whether to refer to a dietician. Treatment If a patient is malnourished or dehydrated advice should be given to the patient/carers on
how to improve nutrition and hydration. Severely malnourished patients should be referred to the GP and dietician if available for
advice

24
WWOOUUNNDD DDRREESSSSIINNGG GGUUIIDDEELLIINNEESS
HEALING INFECTION EXUDATE
Necrotic Sloughy Granular Epithelial
*Spreading Local Critically Colonised Infection Infection Colonised
Viscosity
Volume High Medium Low
High 10 8 6
Medium 8 6 4 Low 6 4 2
SI LI CC Col High
(10 – 8) Medium
(6) Low
(4 – 2)
AIM Attain 100% ‘Epithelial’ tissue Attain a healthy bacterial wound bed Attain exudate of ‘low’ volume &
‘low’ viscosity
OBJECTIVE Remove Necrotic and/or Sloughy Tissue
Promote Granulation and Epithelial tissue
Treat infection
Treat infection
Reduce bacterial
levels
Maintain bacterial
levels
Manage exudate
Manage exudate Manage exudate
TREATMENT Autolysis or re-hydration
Use dressing to promote a moist wound healing.
*Use systemic antibiotic on Spreading Infection
No antim
icrobial required
Highly absorptive products
Moderate exudate
absorption
Low exudate absorption
NECROTIC (Dry)
HYDROGEL
HONEY
HYDROCOLLOID
SLOUGHY (Moist/wet)
HONEY
HYDROCOLLOID
ALGINATE
CADEXOMER IODINE
FOAMS HYDROCOLLOID ALGINATE FILM LOW ADHERENT (Leg ulcers) NON ADHERENT (if required)
ANTIMICROBIAL
- Silver Dressings - Iodine Dressings - Honey - PHMB
FOAM ALGINATE SUPER ABSORBENT
FOAM ALGINATE
LOW ADHERENT HYDROCOLLOID
Skin protectant creams/ lotions to surrounding skin may be required to prevent maceration
Other treatments to consider in consultation with Tissue Viability Nurse Specialist
Larvae Therapy TNP Dermatological Treatments Wound Managers
PLEASE REFER TO WOUND DRESSING GUIDELINES FOR FULL PRODUCT PRESCRIBING INFORMATION 24 25

25
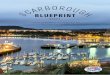
HHooww ttoo uussee tthhee CCoonnttiinnuuuummss ffoorr WWoouunndd AAsssseessssmmeenntt
DDiiaaggrraamm 11 -- TThhee WWoouunndd HHeeaalliinngg CCoonnttiinnuuuumm
BBLLAACCKK BBLLAACCKK //YYEELLLLOOWW YYEELLLLOOWW YYEELLLLOOWW //RREEDD RREEDD RREEDD //PPIINNKK PPIINNKK
DDiiaaggrraamm 22 -- TThhee WWoouunndd IInnffeeccttiioonn CCoonnttiinnuuuumm Spreading Infection Local Infection Critically Colonised Colonised
3 2 1 0
DDiiaaggrraamm 33 -- TThhee WWoouunndd EExxuuddaattee CCoonnttiinnuuuumm
Viscosity
VOLUME HHiigghh 55 MMeeddiiuumm 33 LLooww 11
HHiigghh 55
MMeeddiiuumm 33
LLooww 11
STEP ONE – The Wound Healing Continuum
This is an aid to understanding the type of tissue present in the wound and how it should progress. Thought of as a continuum of colour changes (See diagram 1) from black to pink, it correlates with the healing stages of the wound. Not all wounds progress across the whole spectrum e.g. not all wounds will have a black stage.
USING THE WOUND HEALING CONTINUUM
Identify the colour of the wound that is furthest to the left of the continuum. For example, if the wound contains yellow slough and red granulating tissue it would be defined as a yellow/red wound. The management plan would focus on the removal of the yellow, sloughy tissue and promotion of red granulation tissue. As this objective is achieved, the patient can progress along the wound healing continuum towards the right and therefore a pink / healing status.
STEP TWO – The Wound Infection Continuum There are four criteria which work from left to right with the most severe, “Spreading Wound Infection” on the left (Diagram 2). The continuum moves right, through “Local Infection”, “Critical Colonisation”, to “Colonisation.”
USING THE WOUND INFECTION CONTINUUM
Spreading infection can be a life threatening condition. Local signs & symptoms associated with a spreading soft tissue infection includes; spreading redness (>2cm around wound margin), very high exudate levels, pain, malodour, heat in the surrounding tissues & blistering.
Localised infection is characterised by <2cm of redness around the wound margin, symptoms similar to spreading infection may also be present but to a lesser degree.
Critical colonisation is characterised by delayed healing, malodour & raised exudate levels, (slough may also be present). However, the wound will not present as if locally infected.
A Colonised wound is the normal healing state of a wound. A reduction in wound size over a two-week period would suggest an acceptable level of colonisation.
This Wound Infection Continuum is a simple sliding scale to aid clinical decision-making regarding the level of bacterial colonisation of a wound. A patient may never move to the furthest point on the right (Colonised) on the continuum during their entire treatment. However, lower bacterial levels found in colonised wounds generally lead to better healing. The status of a wound, which has Spreading Infection, Localised Infection or is Critically Colonised, should be considered when developing a treatment plan.
STEP THREE – The Wound Exudate Continuum
The Wound Exudate Continuum is an aid to quantifying wound exudate. The viscosity as well as the volume of the exudate can be an important indicator of wound status. The gradings are HIGH, MEDIUM & LOW for both. This allows wound exudate to be categorised by a score (See Diagram 3). For example, a low volume of medium viscosity would be a Low/Medium category and would score 4, placing it in the Low Exudate portion of the continuum. Using the continuum: - If a wound scores 8-10 points (red zone – spreading infection) it would be regarded as giving serious concern. Any wound scoring 6 points (amber zone), may indicate early signs of critical colonisation or infection and would require regular review. A wound scoring 2-4 points (green zone) would be classed as normal.

28
WWOOUUNNDD FFOORRMMUULLAARRYY PPRROODDUUCCTTSS 2013-14
TTyyppee,, IInnddiiccaattiioonnss && CCoommmmeennttss
PPRROODDUUCCTT NNaammee SSiizzeess ((ccmm))
CCoosstt ((££--pp))
((eeaacchh))
PPiipp--CCooddee // OOrrddeerr CCooddee
STERILE DRESSING PACK / SWABS Only available on prescription, please state size of gloves required on prescription. Only available from NHS Supply Chain (Stores), packs available with different sized gloves. To be used to cleanse a wound in addition or as an alternative to dressing pack.
Polyfield Patient Pack Dressit Softdrape
- Small - Medium - Large
Gauze swabs (Topper 8) Sterile pack 5 x 4ply swabs
1 Small/med Med/large 1 7.5x7.5
0.53
0.60 0.34 0.21
324-3961 301-0675 EJA045 EJA046 EJA047 042-0992
WOUND MEASUREMENT GRIDS Only available from NHS Supply Chain (Stores) or direct from manufacturers
Comfeel Wound Care Grid
Box of 50
14.69
ELZ090
TAPES Fabric based. Suitable for securing dressings, catheters & cannulae Paper-based. Suitable for tape sensitive patients & long term use. Firstline for securing bandages.
Hypafix (5m role) Clinipore (5m role)
5cm 10cm 1.25cm 2.5cm 5cm
1.36 2.28 0.35 0.59 0.99
335-3711 335-3703 299-0091 299-0109 299-0117
CLEANSING SOLUTIONS (Sodium Chloride 0.9%) and accessories Use at body temperature. Use to wash legs in lined bucket. Use kettle for hot water in homes. Active debridement cloth for hyperkeratosis
IIrrrriippoodd Stericlens (aerosol)
Tap water Debrisoft
20ml 100ml 240ml 10x10cm
0.22 1.94 2.95 6.19
313-7155 305-9458 305-9482
358-1287

29
EMOLLIENTS See Emollient section for further advice. Appropriate for washing legs. Not always suitable as an emollient. Ointment – occlusive & rehydrate skin Rich cream for dry skin Foam cleanser emollient wash Dry skin treatment Leave on emollient similar to Diprobase. Leave on emollient similar to E45 Leave on emollient and soap substitute Spray on emollient for non-touch application.
Aqueous cream
Liquid Paraffin / White Soft Paraffin QV cream QV gentle wash QV intensive ointment Zerobase Zerocream Aquamol Emollin
500g 500g 100g 500g 250ml 450g 50g 500g 50g 500g 50g 500g 150ml 240ml
1.51 3.76 1.95 5.60 3.00 5.40 1.04 5.26 1.17 4.08 1.22 6.40 3.78 6.05
327-3315 327-3323 363-9176 363-9150 356-4127 305-4681 348-5000 339-7205 356-4135 356-4143 344-0351 328-7794
SKIN PROTECTIVES To be used as a barrier against body fluids or adhesives. Provides up to 72hours protection. Can be used on broken skin To be used as a Barrier against irritation from body fluids & prevention of skin damage. Not for use on broken skin
Cavilon - No Sting Barrier Film
Cavilon - Durable Barrier Cream
1ml (5) 3ml (5) 28ml spray 92g tube 28g tube 2g sachets (20)
7.47 11.98 10.01 12.22 6.00 11.37
252-8941 252-8958 252-8966 277-1079 301-7480 288-2272

30
STEROID TAPE Tape impregnated with fludroxycortide. For chronic localised recalcitrant dermatoses. Useful for overgranulation. Cut tape to fit lesion and leave for 12 hours daily
Haelan Tape See BNF for contraindications and side effects
7.5x50cm
9.27
017-3104
RETENTION BANDAGES Conforming Bandage for dressing retention Light Support (type 2 light support bandage Used for light support in sprains & strains. Elasticated viscose stockinette for retaining & securing dressings
Knit-Band
Comfifast
- Very small
- Small Limb (green)
- Medium limb (blue)
- Large Limb (yellow)
- Extra large (beige)
5cm x 4m 7cm x 4m 10cm x 4m 15cm x 4m 3.5 x 1m 5cm x 1m 5cm x 3m 5cm x 5m 7.5cm x 1m 7.5cm x 3m 7.5cm x 5m 10.75 x 1m 10.75 x 3m 10.75 x 5m 17.5 x1m
0.12 0.15 0.17 0.30 0.56 0.58 1.62 2.81 0.77 2.13 3.74 1.20 3.49 6.04 1.83
229-0125 229-0133 229-0141 229-0158
289-1745 289-1729 289-1794 289-1828 289-1760 289-1802 289-1836 289-1778 289-1810 289-1844 289-1786

31
NON-ADHERENT DRESSINGS
For patients with compromised / fragile skin ONLY. NNoonn-- aaddhheerreenntt ppoollyyeesstteerr mmeesshh iimmpprreeggnnaatteedd wwiitthh hhyyddrrooccoollllooiidd aanndd ppeettrroolleeuumm jjeellllyy ppaarrttiicclleess.. A secondary absorbent dressing is required (changed as necessary). Non-adherent made of cellulose acetate mesh coated with soft tack silicone A secondary absorbent dressing is required (changed as necessary) Wear time for Urgotul and Adaptic touch =14 days.
UUrrggoottuull AAddaappttiicc TToouucchh
5 x 5 10 x 10 15 x 20 10 x 40 20 x 30 5 x 7.6 7.6 x 11 12 x 15 20 x 32
1.50 3.00 8.49 10.08 13.65 1.13 2.25 4.65 12.50
354-5498 354-5506 354-5514 298-3260 354-5480 359-0411 359-0429 359-0437
LOW ADHERENT DRESSINGS LOW ABSORBENCY Knitted Viscose Primary Dressing First choice wound contact layer for leg ulcers being treated with multi layer compression bandaging. Wear time = 7 days.
N-A
N-A Ultra (silicone coated)
9.5 x 9.5 9.5x 19 9.5 x 9.5 9.5 x 19
0.35 0.67 0.33 0.63
006-8288 259-1006 230-4095 259-0990
ADHESIVE
Low absorption capacity, only suitable for lightly exuding superficial wounds. Wear time = 7 days Showerproof
Softpore
6 x 7 10 x 10 10 x 15 10 x 20 10 x 25 10 x 30 10 x 35
0.06 0.13 0.20 0.35 0.40 0.49 0.58
304-0920 304-0938 304-0946 304-0953 304-0961 304-0979 304-0987

32
HIGH ABSORBENT DRESSINGS Highly absorbent cellulose pad with fluid repellent backing. Non-sterile – ideal for outside of compression for breakthrough exudate. For self management. A thinner dressing thus greater conformability, with a waterproof backing. Super absorbent dressing Super absorbent dressing for heavily exuding wound. Aids removal of slough and locks away bacteria.
ZZeettuuvviitt EE ((SStteerriillee)) ZZeettuuvviitt EE ((nnoonn--sstteerriillee)) Eclypse Kerramax Drymax Extra
10 x 10 10 x 20 20 x 20 20 x 40 10X10 10X20 20X20 10X40 15 X 15 20X30 60X40 10x10 10x22 20x22 30x20 10x10 10x20 20x20 20x30
0.20 0.23 0.37 1.02 0.06 0.08 0.13 0.26 0. 97 2.14 8.15 0.91 1.20 2.12 2.43 1.80 2.38 4.20 4.80
322-7618 322-7584 322-7592 322-7600 322-7618 322-7584 322-7592 322-7600 305-1349 306-1272 232-1131 352-3446 342-3308 342-3290 352-3453 346-7047 346-6935 346-6968 346-6992
HYDROGEL DRESSINGS (Moisture donating dressings)
For dry “sloughy” or necrotic wounds/ lightly exudating wounds/ granulating wounds. Have a high water content to provide a moist wound surface. A secondary occlusive dressing is required. Not suitable for infected or moderate to heavily-exuding wounds. For dry necrotic wounds A non-woven dressing impregnated with a hydrogel. For lightly exuding and moderately to highly exuding wounds, also suitable for painful wounds
AAqquuaaffoorrmm GGeell IInnttrraassiittee CCoonnffoorrmmaabbllee AAccttiiffoorrmm CCooooll (Use with top liner intact when minimal exudate)
8g 10x10 10 x20 6.5x5 10x10 10x15
158 1.70 2.30 1.70 2.49 3.58
330-7861 267-8043 267-8084 315-5553 304-8352 304-8360

33
Pressure Relieving Device
Designed to be used directly on the skin’s surface in order to offer maximum protection. Should not be used directly on an open wound as it is non-sterile. Hard wearing and long lasting (estimated around 3 weeks’ continuous use) and can be repeatedly re-used on the same patient. It can be cleaned in plain soap and water.
Aderma Standard Heel
Extra Large Heel
Sacrum / ankle Wrap
30 x 5x 0.3cm strip
50 x 2.5x 0.3 strip
10x 10 x 0.3 Sheet
10 x 10 x 1.2 Sheet
20x20x0.3 Sheet
Single Single Single Single Single Single Single Single
14.47 16.49 16.25 6.21 5.18 4.14 12.42 16.53
365-5032 365-5040 365-5057 328-3926 365-5024 328-3918 328-3934 328-3900

34
FOAM DRESSINGS (Absorbent dressings) Moderate to heavily exuding wounds All foams wear time = 7 days or when saturated. Allevyn and Biatian Adhesive range has waterproof backing. Allevyn Gentle and Mepilex Range is suitable for very fragile skin.
Biatain and Mepilex non- adhesive can be cut to shape. Foams not recommended under compression bandaging as can macerate. Good for small wounds in awkward areas e.g heel or elbow.
AAlllleevvyynn GGeennttllee BBoorrddeerr BBiiaattaaiinn NNoonn--AAddhhééssiivvee
BBiiaattaaiinn AAddhheessiivvee TTiieellllee PPlluuss HHeeeell MMeeppiilleexx MMeeppiilleexx BBoorrddeerr
MMeeppiilleexx LLiittee MMeeppiilleexx BBoorrddeerr LLiittee TTeeggaaddeerrmm FFooaamm HHiigghh PPeerrffoorrmmaannccee AAddhheessiivvee
7.5 x 7.5 10 x 10 12.5 x 12.5 17.5 x 17.5 5x7 10x10 10x20 15x15 10x10 12.5x12.5 18 x18 20 x 26.5 10x11 11x20 15x16 20x21 7.5x7.5 10x12.5 10x20 10x30 15x17.5 17x20 6x8.5 10x10 15x15 4x5 5 x 12.5 7.5x7.5 10x10 15x15 10x11 (Oval)
1.46 2.48 3.20 6.23 1.21 2.20 3.63 3.97 1.65 2.41 4.86 4.45 2.57 4.24 4.66 7.03 1.33 2.63 3.56 5.36 4.53 5.87 1.74 2.08 4.03 0.91 1.98 1.37 2.49 4.06 2.33
334-2052 334-2060 334-2102 334-2045
254-3228 265-3236 315-7674 265-3236 285-7027 259-6203 259-6211 316-8838 339-1109 339-1091 339-1083 339-1034 339-0986 339-0978 332-1590 327-1608 339-0952 339-0945 303-5565 303-5573 303-5581 317-7011 317-7029 317-7037 317-7045 317-7060 304-1589

35
HYDROCOLLOID DRESSINGS ( (Moisture donating / conserving dressings) Facilitate rehydration & autolytic debridement of dry, sloughy, or necrotic wounds. Suitable also for promoting granulation. These types of dressings are not suitable for infected wounds, unless the infection is being treated. These products are not suitable for moderate to heavily exuding wounds Hydrocolloids are NOT recommended to be used on diabetic foot ulcers. For light to medium exudate Dressing should seal round the borders of the wound. CChhaannggee wwhheenn bbuubbbbllee eexxppaannddss ttoo aannyy ppaarrtt ooff ddootttteedd ddrreessssiinngg cchhaannggee iinnddiiccaattoorr.. Hydrocolloids wear time = 7 days. For none to lightly exuding wounds. Waterproof Sacral hydrocolloid – cheaper than foams and can be wiped down.
DDuuooddeerrmm SSiiggnnaall
DDuuooddeerrmm EExxttrraa tthhiinn Tegaderm Hydrocolloid Sacral
10 x 10 14 x 14 20 x 20 18.5 x 19.5
(Heel) 11 x19 (Oval)
7.5 x 7.5 10 x 10 15 x 15
16.1 x 17.1
2.00 3.52 6.99 4.92 3.05
0.76 1.27 2.73 4.71
299-6858 299-6866 299-6874 299-6882 308-2336 027-7798 027-7897 027-8036 311-9799 004-5336
ALGINATE DRESSINGS – (Absorbent dressings) Suitable for absorbing moderate to heavy exudate on wounds with or without slough. NOT suitable for dry or necrotic wounds. Can lie over the wound and skin margin.Haemostatic. Change the dressing when fully gelled or saturated. Alginate containing hydrocolloid thus greater absorbency with debridement and dressing retention. For Cavity Wounds: Ribbon or rope for small, deep, open, wet wounds.
SSoorrbbssaann (can be used on infected wounds) SSoorrbbssaann PPlluuss (has greater absorbency) Sorbsan Plus SA (As above but with showerproof adhesive border) Urgosorb Sorbsan Ribbon (with Probe) Urgosorb Rope Aquacel Ribbon
5 x 5 10 x 10 10 x 20 7.5 x 10 10 x 15 10 x 20 15 x 20 11.5 x 14 14 x 19 14 x 24 19 x 24 5 x 5 10 x 10 10 x 20 40cm 30cm 1 x 45
0.79 1.66 3.10 1.67 2.96 3.77 5.24 2.92 4.25 5.14 6.45 0.83 1.99 3.64 1.95 2.65 1.76
019-0579 034-8839 019-0975 002-9702 002-9702 238-4915 261-0988 302-2522 302-2530 302-2548 302-2555 298-3278 293-8413 293-8439 003-5212 293-8421 361-5978

36
Hydrocolloid with an adhesive foam border for extra adherence. Cheaper than foam dressings and can be wiped down. An absorbent acrylic pad encased between a top layer of breathable film and abottom layer of perforated film. Transparant for visibility and no upper wear time.
Granuflex Bordered Tegaderm Absorbent Clear Acrylic dressing
6x6 10x10 15x15 10x13triangular
15x18triangular
7.6 x 9.5 oval 11.1x12.7 14.2x15.8
(square) 14.9x15.2
1.66 3.14 5.99 3.71 5.78 3.02 3.91 5.51 8.26
004-5351 004-5393 004-5468 004-5567 346-6224 346-6340 346-6273 353-5796
FILM DRESSINGS - Vapour-Permeable Adhesive (Moisture conserving dressings) Use on superficial, shallow wounds such as cuts, abrasions, scalds, donor sites, postoperative wounds.Useful also to reduce friction on susceptible areas. Self-adhesive & waterproof to allow showering. Contra-Indications Do not use on infected wounds, deep cavity wounds, third degree burns or wounds with copious exudate. The exudate may become trapped beneath the film causing skin maceration and inflammation Film dressings to be used only as a primary (1o) dressing on lightly exudating wounds. Post op dressing. Vapour-permeable adhesive film dressing with absorbent pad. Wear time = 7 days
HHyyddrrooffiillmm
Hydrofilm Plus
6x7 10x12.5 10x15 10x25 12x25 15x20 20x30 5 x 7.2 9x10 9x15 10x20 10x25 10x30
0.21 0.39 0.49 0.76 0.80 0.90 1.49 0.15 0.20 0.22 0.34 0.36 0.53
342-6665 342-6228 266-7350 342-6236 266-7368 342-6244 342-6251 342-4322 342-4330 342-4348 342-4363 342-4355 342-4371

37
ANTI-MICROBIAL DRESSINGS Antimicrobials should be used for no more than 14 days initially, following which a review and assessment of progress should take place.
If there is significant improvement they should be discontinued If there is only some improvement they may be continued for a further 14 days If there is no improvement advice should be sought from the TVN.
ALL ANTIMICROBIAL DRESSINGS MUST BE PLACED IN DIRECT CONTACT WITH THE WOUND BED SILVER DRESSINGS LOW ABSORBENCY Non-adherent wound contact layer. MODERATE ABSORBENCY Silver impregnated polyurethane foam film dressing. HIGH ABSORBENCY Alginate dressing with silver Alginate containing hydrocolloid & silver (thus more absorbent) Silver alginate with waterproof backing. Absorbent calcium alginate and hydrocolloid dressing impregnated with silver. Activated charcoal cloth impregnated with silver. Traps and kills bacteria while absorbing odour.
UUrrggoottuull SSiillvveerr Allevyn Ag Gentle Allevyn Ag Gentle Border Sorbsan Silver flat Sorbsan silver Ribbon Sorbsan Silver Plus Sorbsan Silver Plus SA Urgosorb Silver Actisorb Silver Aquacel Ag Ribbon
11 x 12 15 x 20 5 x 5 10 x 10 10 x 20 15 x 15 20 x 20 7.5 x 7.5 10 x 10 12.5 x 12.5 17.5 x 17.4 5 x 5 10 x 10 10 x 20 40 cm 7.5 x 10 10 x 15 10 x 20 15 x 20 11.5 x 14 14 x 19 14 x 24 5 x 5 10 x 10 10 x 20 2.5x30 Ribbon
6.5x9.5 10.5x10.5 10.5x19 1 x 45cm
3.34 9.09 3.18 5.93 9.79 11.02 16.32 4.06 6.10 7.84 14.95 1.54 3.91 7.13 4.08 3.25 5.41 6.58 8.82 5.28 7.60 8.36 1.44 3.44 6.48 3.46 1.64 2.58 4.70 2.97
329-5995 329-6605 346-7511 346-7529 346-7537 346-7545 346-7552 346-7677 346-7685 346-7693 346-7701 327-0824 327-0816 327-0808 327-0766 333-0784 3330792 333-0800 333-0818 333-0826 333-0834 333-0842 327-4719 327-4272 327-4735
327-4743 272-8327 048-7264 255-1901 361-5978

38
PHMB- Polyhexamethylene Biguanide Is effective against gram positive bacteria, gram negative bacteria, fungi & yeast including MRSA, VRE. Do not use as a primary treatment for full 3rd degree burns or on patients with known sensitivity to PHMB Absorbent foam impregnated with broad spectrum antimicrobial PHMB 0.5%
Kendall AMD Antimicrobial Foam Dressing Kendall AMD Antimicrobial Foam Border Dressing
5 x 5 10 x 10 10 x 20 15 x 15 20 x 20 4.4 x 8.3 8.9 x 8.9 8.9 x 14 14 x 14 19 x 19
2.45 4.62 8.75 8.75 12.82 2.47 3.08 4.85 6.37 12.25
347-0697 347-0721 347-0747 347-0754 347-0689 363-9416 363-9390 363-9424 363-9432 363-9408
IODINE DRESSINGS Caution in patients with severe renal impairment or history of thyroid disorders (See BNF for full details). Contra-indications: lithium therapy, thyroid disorders, pregnancy & breast-feeding (See BNF for full details). For chronic, medium exudating, infected or sloughy wounds. Maximum single application ≤ 50g. Weekly max. not to exceed 150g. Any single course of treatment not to exceed 3 months. Povidine Iodine Fabric Dressing – Recommended for diabetic/podiatric/trauma use Used as a primary wound contact layer. In diabetic wounds up to 4 layers can be applied.
IIooddoofflleexx Apply to wound surface, remove gauze backing and cover; renew when saturated (usually 2–3 times weekly, daily for heavily exuding wounds) IIooddoossoorrbb ooiinnttmmeenntt.. Apply to depth of 3mm & cover. IInnaaddiinnee
5g 10g 17g 10g 20g 5 x 5
9.5 x 9.5
3.88 7.76 12.29 4.29 0.08 0.31 0.46
073-1547 014-9617 216-3269 036-6658 033-3906 0371195 037-1229

39
HONEY DRESSINGS Creates a moist wound environment. Suitable for dry sloughy, necrotic, lightly exuding or granulating wounds Please inform patients these dressings may cause pain and may increase exudate levels initally. Contains 47% medical grade honey. (MGH) Ointment (s) contains 40% (MGH) & is a gentle alternative for patients with sensitive wounds Absorbent semi-permeable dressings impregnated with honey 30% (MGH) Absorbs low to moderate levels of exudate. Can be left on up to 5 days
Mesitran Ointment
- S (lower strength) Mesitran Mesitran Border
15g 15g 10 x 10 10 x 17.5 15 x 20 10 x 10 15 x 15 13 x 15 (sac)
3.41 3.39 2.46 4.43 5.12 2.56 4.53 4.33
314-0928 314-0944 314-0951 314-0977 314-0969 314-0985 314-0993 314-1009
Antimicrobial Gels Alginate gel containing two antimicrobial enzymes: glucose oxidase and lactoperoxidase Debrides & desloughs wounds. Non toxic to Fibroblasts & Keratinocytes. Single patient use can be recapped. Do not irrigate out of wound, just reapply. Nozzles available for pilonidal sinus use.
Flaminal Forte (absorbs moisture) Flaminal Hydro (donates moisture)
15g 50g 15g 50g
7.26 24.04 7.26 24.04
324-2963 344-9592 324-2971 344-9600

40
*A full leg ulcer assessment must be carried out before using any compression system.* The following compression systems are for venous leg ulcerations without significant arterial impairment i.e. ABPI (Doppler) = >0.8mmHg and <1.2 mmHg Refer to Tissue Viability Nurse for advice on readings outside this range Ankle measurement is crucial for achieving correct compression
CCOOMMPPRREESSSSIIOONN BBAANNDDAAGGEESS
HIGH COMPRESSION BANDAGES (Short Stretch Bandage)
A full leg ulcer assessment must be carried out before using any compression system.
Sub-compression wadding bandage For venous leg ulceration and oedema. Applied at full stretch over padding, which protects areas of high pressure & sites at high risk of pressure damage.
KK--SSoofftt AAccttiiccoo ((SShhoorrtt SSttrreettcchh CCoohheessiivvee))
10cm x 3.5m 10cm x 4.5m 8cm x 6m 10cm x 6m 12cm x 6m
0.41 0.51
2.90 3.01 3.83
266-8374 325-7177 314-0886 271-5431 314-0894
Latex Free Compression Bandages 40mmHg For ankle circumference 18-25cm
PPrrooffoorree KKiitt LLaatteexx FFrreeee
18-25cm
ankle
9.70
320-2793

41
HIGH COMPRESSION = 40mmHg ankle pressure MULTI-LAYER ELASTIC HIGH COMPRESSION BANDAGING
K-FOUR COMPONENTS Ankle sizes - sizes < 18cm For 18-25cm ankle sizes
Ankle sizes 25-30cm Ankle sizes >30cm Individual components can also be prescribed in longer versions
KK--FFoouurr ##11 ((KK--SSoofftt xx22)) KK--FFoouurr ##22 ((KK--LLiittee)) KK--FFoouurr ##33 ((KK--PPlluuss)) KK--FFoouurr ##44 ((KKoo--FFlleexx)) KK--FFoouurr ##11 ((KK--SSoofftt)) KK--FFoouurr ##22 ((KK--LLiittee)) KK--FFoouurr ##33 ((KK--PPlluuss)) KK--FFoouurr ##44 ((KKoo--FFlleexx))
KK--FFoouurr ##11 ((KK--SSoofftt LLoonngg)) KK--FFoouurr ##22 ((KK--TThhrreeee CC)) KK--FFoouurr ##33 ((KKoo--FFlleexx LLoonngg)) KK--FFoouurr ##11 ((KK--SSoofftt LLoonngg)) KK--FFoouurr ##22 ((KK--TThhrreeee CC)) KK--FFoouurr ##33 ((KK--PPlluuss LLoonngg)) KK--FFoouurr ##44 ((KKoo--FFlleexx LLoonngg))
KK--SSoofftt LLoonngg KK--LLiittee LLoonngg KK--PPlluuss LLoonngg KKoo--FFlleexx LLoonngg KK--tthhrreeee CC
10cm x 3.5m 10cm x 4.5m 10cm x 8.7m 10cm x 6.0m
10cm x 3.5m 10cm x 4.5m 10cm x 8.7m 10cm x 6.0m
10cm x 4.5m 10cm x 3.0m 10cm x 7.0m 10cm x 4.5m 10cm x 3.0m 10cm x10.25m 10cm x 7.0m
10cm x 4.5m 10cmx5.25m 10cmx 10.25 10cm x 7.0m 10cmx 3m
6.73 (Kit)
6.44 (Kit)
6.44 (Kit) 8.87 (Kit) 0.54 1.09 2.52 3.30 2.66
342-5089
266-8382
342-5113 342-5147 325-7177 325-7110 325-7201 325-7151 342-4975

42
REDUCED Multi-layer Elastic High Compression Bandaging
A full leg ulcer assessment must be carried out before using any compression system. These bandage regimes may be appropriate for patients with a Doppler reading <0.8mmHg but >0.6 or >1.2 . The advice of the Tissue Viability Nurse should be sought prior to implementation Estimated Compression Level at the ankle on an ankle measuring 18-25 cm circumference 36-40mm Hg approximately 20mm Hg approximately 1188--2200mmmmHHgg aapppprrooxxiimmaatteellyy
11 xx KK SSoofftt 11 xx KK--LLiittee ((ffiigg ooff 88 oorr ssppiirraall)) 22 xx KK--PPlluuss -- ((ssppiirraall oorr ffiigg.. ooff 88 aatt 5500%% ssttrreettcchh)) 11 xx KK SSoofftt 11 xx KK--LLiittee 11 xx KKoo--FFlleexx –– ((ssppiirraall aatt 5500%% ssttrreettcchh)) 11 xx KK SSoofftt 11 xx KK--LLiittee 11 xx KK--PPlluuss -- ((ssppiirraall oorr ffiigg..ooff 88 aatt 5500%% ssttrreettcchh)) ((ffiigg ooff 88 ggiivveess sslliigghhttllyy hhiigghheerr ccoommpprreessssiioonn))
HIGH COMPRESSION VENOUS ULCER HOSIERY
Hosiery is essential in maintaining healing in venous leg ulcers and following a DVT or for control
of chronic oedema and lymphoedema Doppler prior to commencing hosiery. Measure leg in the standing position and ask companies for measurements and current hosiery
options
The companies listed on the next page offer many ranges of sizes, colours, shapes and level of compression for men and women, choose for acceptability.
CLASS UK CLASS EUROPEA
N CLASS ULCER CARE HOSIERY KITS
CLASS 1 14-17mmHg
18-22mmHg
Liner stocking 10mmHg
CLASS 2 18-24mmHg
23-33mmHg
+ secondary stockings
CLASS 3 25-35 mmHg
34-46mmHg
30mmHg

43
CONTACT THE COMPANIES ON NUMBERS SUPPLIED FOR UP TO DATE INFORMATION ON
ALL HOSIERY.
HIGH COMPRESSION VENOUS ULCER HOSIERY SYSTEMS – 40mmHg
Activa hosiery kit (Activa) 2 x piece hosiery kit 10mm Hg and 30mm Hg stocking £21.36 Also extensive range of compression hosiery including lymphoedema options Activa = 08450606707 / 07973862780 www.activahealthcare.co.uk
Mediven ulcer kit (Medi) 2 x piece hosiery kit 20mm Hg liner and 20mm Hg stocking £26.21 Also vast range of hosiery styles including lymphoedema options Medi Uk Ltd = 01432 373500 / 07976710044 E mail FP10 @mediuk.co.uk
Carolon multilayer compression system. £26.50 Available in two compression systems 35-40mm Hg and 30-35mm Hg Widest calf circumference up to 66cm H&R Healthcare= 01482 631606 www.hrhealthcare.co.uk
Jobst ulcercare zippered / unzippered graduated compression hosiery system £29.95 Also extensive range of hosiery of all types.
01482 670100 / 07772 281224
www.BSN medical .com
Altiform hosiery and Altiform made to measure – British standard hosiery and made to measure
hosiery. Range of styles. From £6.95 and made to measure from £23.64
Only 72 hours from chemist to delivery.
Contact Urgo on 01509 502051 / 07909926350
Cliniduo 2 x piece hosiery kit 10mm Hg liner and 30mm Hg stocking £13.07 Clini Supplies = 0208 863 4168 / 07793 424737 www.clinisupplies.co.uk

44
SHOES A shoe to accommodate bulky bandages - available in a range of sizes
Kerraped
SSIIZZEE SShhooee SSiizzee FFoooott WWiiddtthh FFoooott wwiitthh bbaannddaaggee ((bbaassee ooff ttooeess)) ((CCiirrccuummffeerreennccee)) Small 2 - 5.5 7.6 - 8.6 23.8 - 27.1 Medium 6 - 7.5 8.8 - 9.2 27.6 - 29 Large 8 - 10 9.4 - 10 29. - 31.4 X-Large 10.5 - 13 10.1 - 10.9 31.8 - 34.2
16.95
329-4741 329-4758 329-4774 329-4782
HOSIERY APPLICATION AIDS / SHOES
Application systems to allow the easier application of compression hosiery Allows patient to bath or shower without getting dressing wet
Acti-glide Seal-tight
Sockaid
One size
Adult foot / ankle
Adult short leg Ad. wide /
short leg One size
12.76
10.50 10.50 10.50 12.73
284-5196
314-4896 314-4904 314-4912 319-4016

45
Notes

46
SCARBOROUGH ,WHITBY AND RYEDALE (COMMMUNITY)
Gemma Hancock
Malton Hospital, Middlecave Rd, Malton, North Yorks
Tel: 01653 604549 Mobile: 07919627649 Fax :01653 600589
E-mail: [email protected]
Ali Horton
Malton Hospital, Middlecave Rd, Malton, North Yorks
Tel: 01653 604549 Mobile: 07769978170 Fax :01653 600589
E-mail: [email protected]
TTIISSSSUUEE VVIIAABBIILLIITTYY SSPPEECCIIAALLIISSTT NNUURRSSEESS CCOONNTTAACCTT DDEETTAAIILLSS
YORK AND SELBY COMMUNITY Joyce Sims Clementhorpe Health Centre ,Cherry Street ,York YO23 1AP Direct line 01904 724532 Mobile 07535 640494 Fax. 01904 724538 E mail: [email protected]
YORK TEACHING HOSPITAL NHS FOUNDATION TRUST Ceri Elliott York District Hospital Clinical Nurse Specialist Office, 3rd Floor Admin Block, York Teaching Hospital NHS FoundationTrust, Wiggington Rd, York,YO318HE Direct Line 01904 725942 E Mail: [email protected]
SCARBOROUGH GENERAL HOSPITAL Samantha Haigh Scarborough General Hospital, Woodlands Drive, Scarborough, Tel 01723 368111 extension 2455 Mobile 07917243687, Pager #6582 E mail: [email protected] Helen Williams Scarborough General Hospital, Woodlands Drive, Scarborough, Tel 01723 368111 extension 2455 Mobile 07917243687, Pager #6582 E mail: [email protected]