Embed Size (px)
Citation preview

Measures That Matter: Simplifying Clinical Quality Misty Roberts, MSN, RN, PMP
Toyosi Morgan, MD, MPH, MBA
12/12/17 1:30-2:45
Session Code: C16
This presenter has nothing to disclose

2
Learning Objectives
Show how refining clinical quality measures can increase efficiency, lower costs, reduce burden for physicians, and ultimately improve health outcomes
Walk through specific ways that health care organizations can simplify quality measures
Demonstrate how simplifying clinical quality measures will help physicians in their transition to value-based care
3
“Measures” Making Headlines
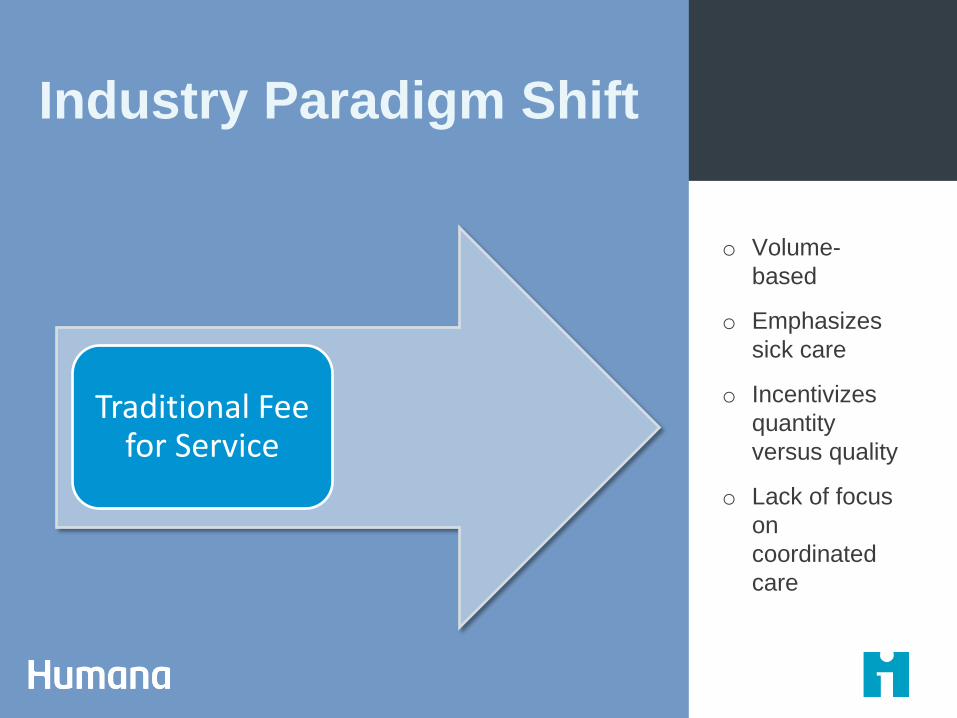
Industry Paradigm Shift
o Volume-
based
o Emphasizes
sick care
o Incentivizes
quantity
versus quality
o Lack of focus
on
coordinated
care
Traditional Fee for Service

Industry Paradigm Shift
o Outcomes-
based
o Promotes
preventive care
o Focus on
quality versus
quantity
o Highly
coordinated
care
Value-Based Care

Physician Burden
“Each year US physician practices in four common specialties spend, on average, 785
hours per physician and more than $15.4 billion dealing with the reporting of
quality measures.”

Lack of Industry Alignment
Source: Bailit Health Analysis
48 Measure Sets in 25 States and 3 Regions: 1367 Individual Measures 509 Distinct Measures
NOT A SINGLE measure was used by every program
Only 20% of measures
were used by more than
one program
Breast cancer screening most
frequent used (63% of programs)
40% of programs created at least one new measure for use

Show me the Numbers
Centers for Medicare and
Medicaid Services
2189 (by Title)
National Quality Measures
Clearinghouse
2522
National Quality Forum
1101
US Department of Human
Health and Services
2222
Quality
Payment Program
271

Total Measures
2522
What Percentage are Outcome-Based?
*Related health care delivery and population health measures
• Access (21) • Outcome (282) • Patient Experience (418) • Process (1400) • Structure (113) • Other* (288)
11%
Measurement Breakdown

Example diabetes measures…
National Quality Measures Clearinghouse
Diabetes Specific Measures = 351
Health and Human Services
Diabetes Specific Measures = 34
Diabetes
QPP
NQMC
HHS
Quality Payment Program ( MIPS )
Diabetes Specific Measures = 11
National Quality Forum
Diabetes Specific Measures = 66
NQF
Centers for Medicare and Medicaid Services
Diabetes Specific Measures = 58
CMS

Measurement Breakdown
Diabetes Measures
351
What Percentage of Diabetes Measures are Outcome-Based?
*Related health care delivery and population health measures
• Outcome (60) • Patient Experience (10) • Process (220) • Structure (12) • Other* (49)
17%

Common Measures
Of the measures corresponding to
diabetes…
What does this tell us?
…7 were accounted for in all governing entities (NQMC, HHS, CMS, QPP,
NQF)
• Variance • Key measures

1
3
Examining Our Current State
Gathering the Pieces
Multiple data
sources Inconsistencies
Multiple departments
and silos
CMO and sponsor buy-in
Minimal clinical input
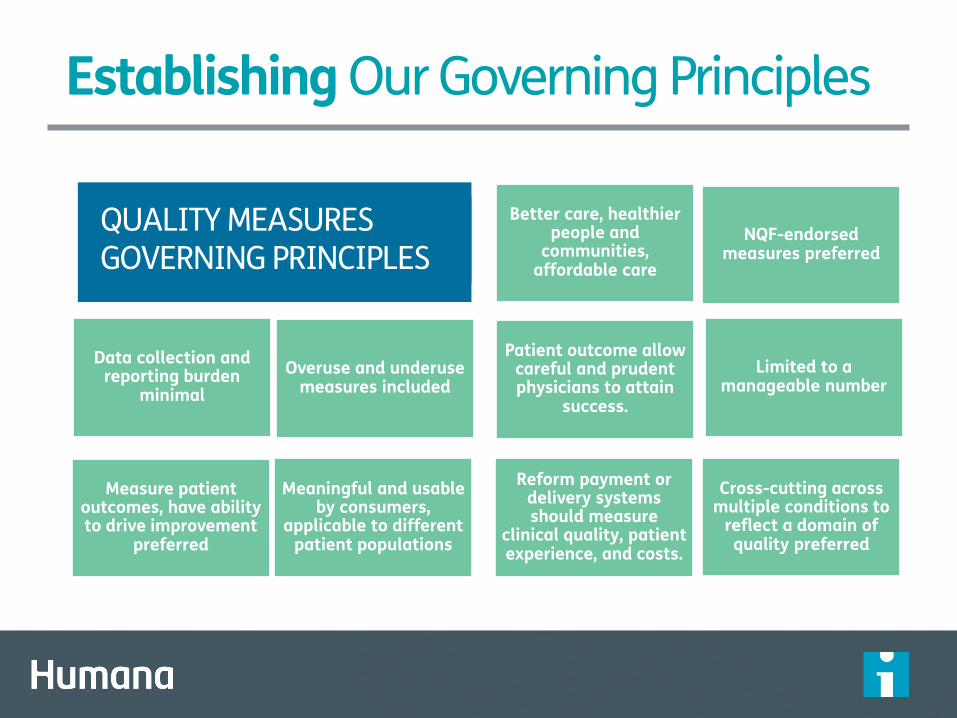
Better care, healthier people and
communities, affordable care
NQF-endorsed measures preferred
Data collection and reporting burden
minimal
Overuse and underuse measures included
Patient outcome allow careful and prudent physicians to attain
success.
Limited to a manageable number
Measure patient outcomes, have ability to drive improvement
preferred
Cross-cutting across multiple conditions to
reflect a domain of quality preferred
Meaningful and usable by consumers,
applicable to different patient populations
Reform payment or delivery systems should measure
clinical quality, patient experience, and costs.
Establishing Our Governing Principles
QUALITY MEASURES GOVERNING PRINCIPLES

15 Simplifying Metrics: Our Process
1. Receive Data and Consolidate
2. Pre-Analysis Work
3. Initial Review
4. Filtering and Initial Identification of Key Metrics
5. “Key Metrics” Analysis
6. External Research
7. Gap Analysis and Future State
8. Final Recommendations
ANALYSIS STATE COUNT
Reduce
Refine/ Relate
Reduce
Refine/ Relate
1116
208
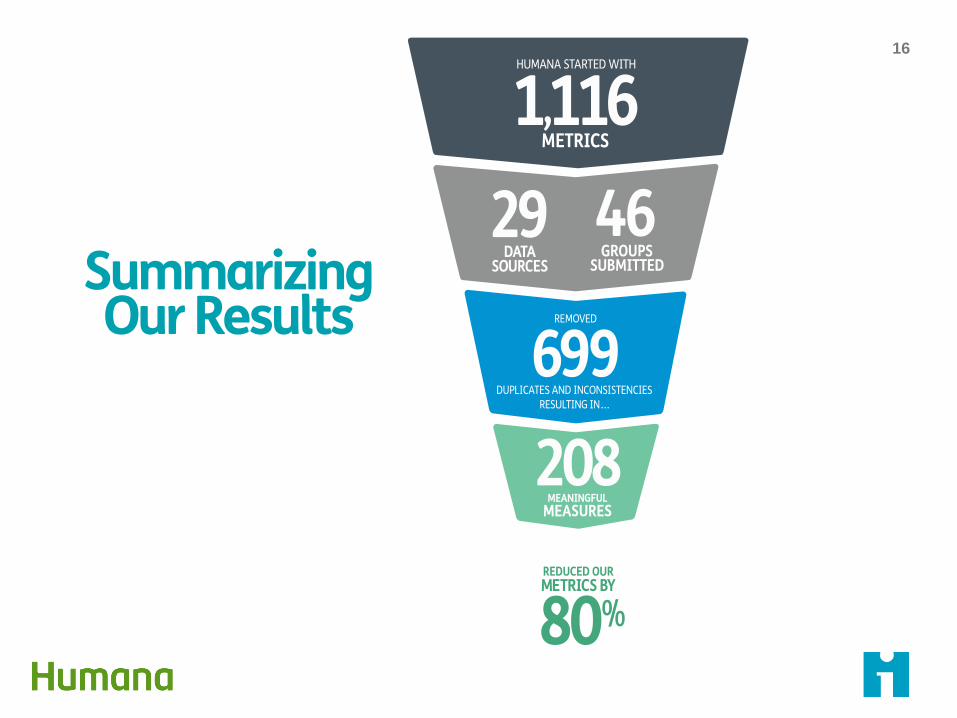
16
Summarizing Our Results

17 Building Our Future State
Communication Plan and
SharePoint Site One-on-
Ones
Assign Business Owners
Monthly Stakeholder
Meetings
Sustainability Plan
Leadership and
Stakeholder Buy-in
Determine Business Needs
Identify Measure Owners
Clinical Quality Metrics
Alignment Governance
18
Creating Sustainability
The Clinical Quality Metrics Alignment (CQMA) Governance Committee
Manage and maintain meaningful measures that matter to consumers Reduce variability in measure selection Reduce collection burden and cost

19
Creating Sustainability
• Regularly review current measures and any proposed changes.
• Discuss evidence-based guidelines, metric stewards, metric efficacy, feasibility, reliability, ease of tracking and application.
Review
• Deliver continuity, awareness and collaboration across the enterprise.
Sustain
• Determine the inclusion or retirement of metrics based on review discussions and enterprise/industry priorities.
• Reach consensus on which metrics to maintain, retire, add or revise.
Approve
CQMA Governance
• Maintain standard review criteria and decision-making process based on governing principles and criteria.
20
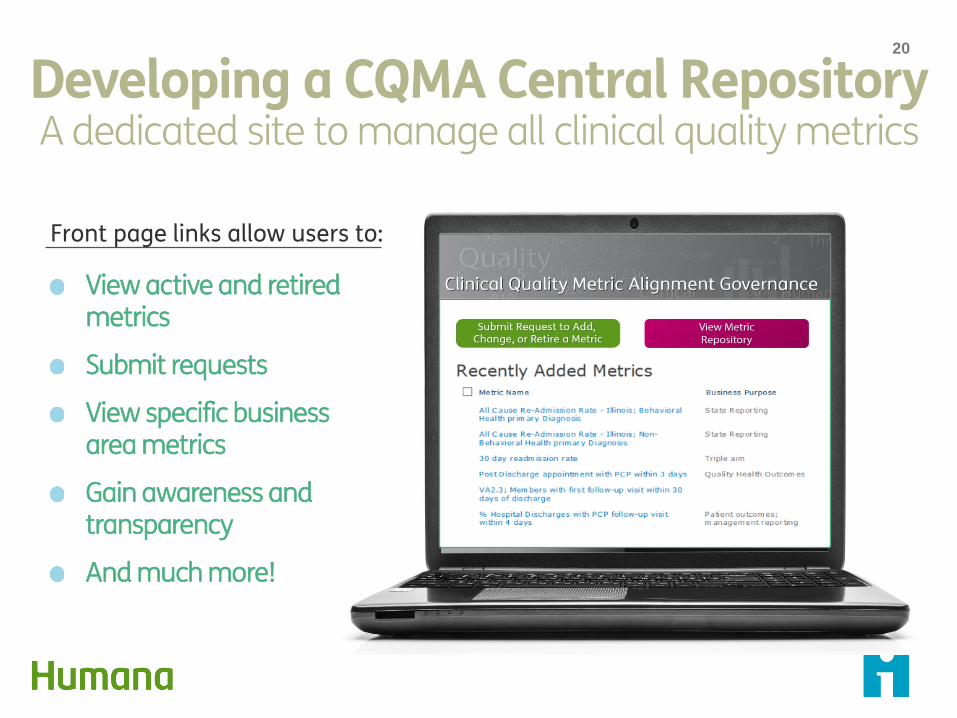
View active and retired metrics
Submit requests
View specific business area metrics
Gain awareness and transparency
And much more!
Developing a CQMA Central Repository A dedicated site to manage all clinical quality metrics
Front page links allow users to:
21
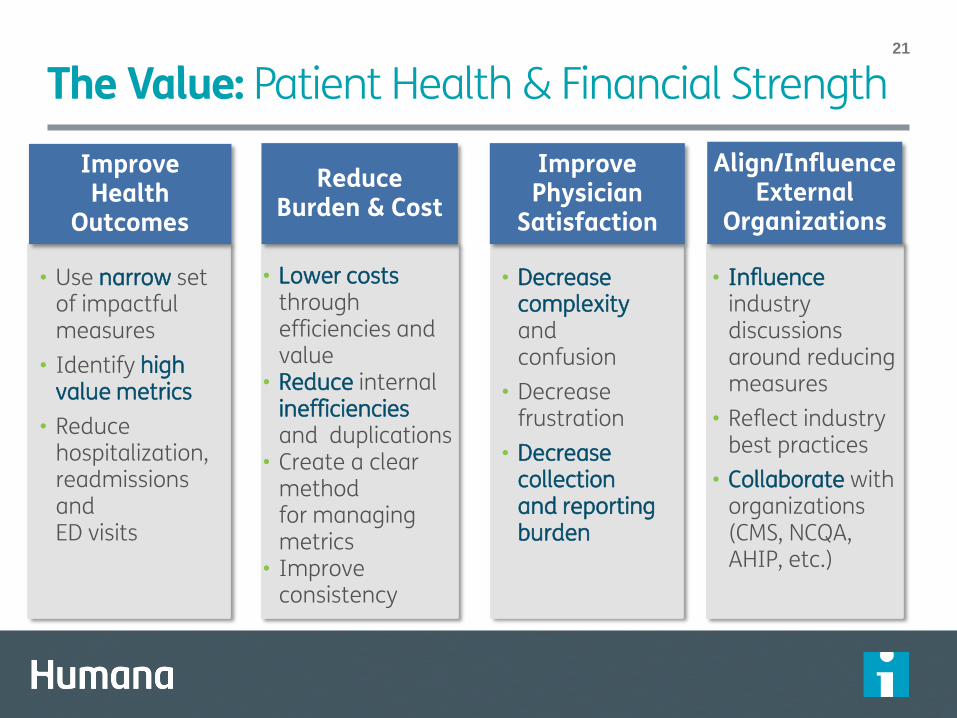
The Value: Patient Health & Financial Strength
• Decrease complexity and confusion
• Decrease frustration
• Decrease collection and reporting burden
Improve Physician
Satisfaction
• Influence industry discussions around reducing measures
• Reflect industry best practices
• Collaborate with organizations (CMS, NCQA, AHIP, etc.)
Align/Influence External
Organizations
Reduce Burden & Cost
• Lower costs
through efficiencies and value
• Reduce internal inefficiencies and duplications
• Create a clear method for managing metrics
• Improve consistency
Improve Health
Outcomes
• Use narrow set of impactful measures
• Identify high value metrics
• Reduce hospitalization, readmissions and ED visits
22
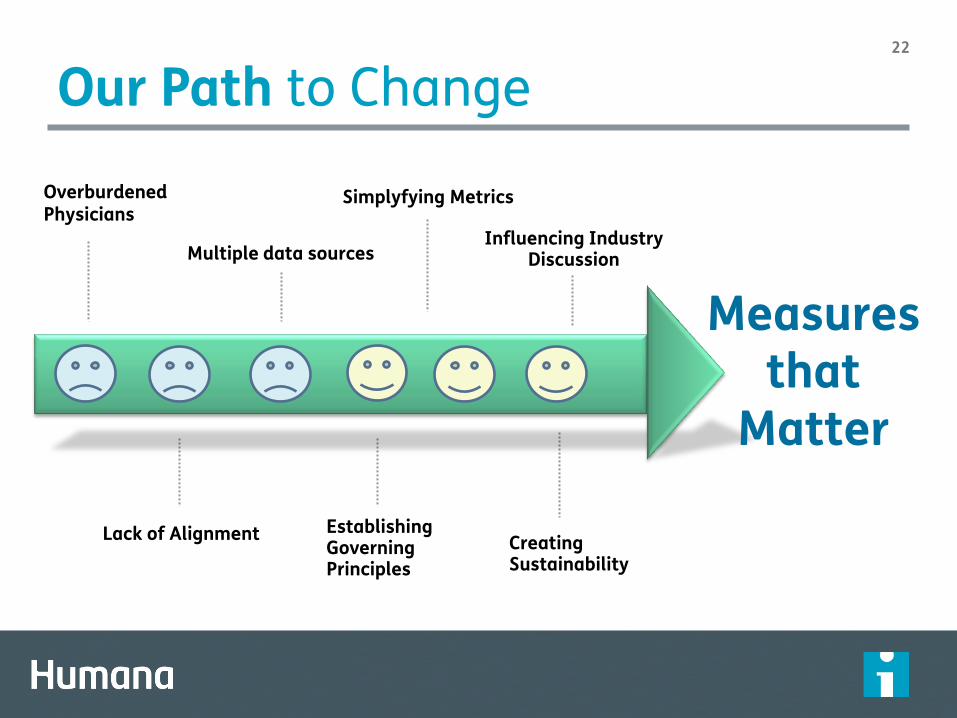
Our Path to Change
Lack of Alignment Establishing Governing Principles
Creating Sustainability
Overburdened Physicians Multiple data sources
Simplyfying Metrics
Measures that
Matter
Influencing Industry Discussion

2
3
Questions?

2
4
Thank you
![Clarinet in B Trio voor Klarinet , Altviool en piano files/Chamber/[Clarinet_Institute] Ostijn... · misty misty misty misty 3 3 Trio voor Klarinet , Altviool en piano Willy Ostyn](https://img.pdfslide.net/doc/110x75/5ac4c16d7f8b9af91c8d36c3/clarinet-in-b-trio-voor-klarinet-altviool-en-clarinetinstitute-ostijnmisty.jpg)