Embed Size (px)
Citation preview
Thoracic mobilization and manipulation for the treatment
of shoulder painBrent Perdizet, PT, OCS and Patrick Cook, PT OCS FAAOMPT
Objectives
• Discuss current evidence for cervical, thoracic spine and rib mobilization and manipulation for shoulder pain.
• Engage with presenters as they introduce and demonstrate selected cervical, thoracic and rib manipulation and mobilization techniques.
• Explain Manual Therapy techniques for cervical, thoracic spine and ribs using Current Evidence.
• Upon return to clinical practice, improve management of shoulder pain through the use of cervical, thoracic spine and rib techniques.
IntroductionCervical, Thoracic Spine and Rib mobilization and manipulation techniques can be included with management for a client with shoulder impingement syndrome.
Systematic ReviewHo CC, Sole G, Munn J. The effectiveness of manual therapy in the management of musculoskeletal disorders of the shoulder: a systematic review. Manual Therapy. 2009(14); 463‐474
• Reviewed 14 RCTs, all performed shoulder MT, and 2 used cervical, thoracic and rib mobilization and manipulation.
• As a whole, conflicting results for patients with SIS, however studies were not of homogenous groups or treatments.
• “Based on findings of our review, clinicians should consider incorporating soft tissue and joint mobilization techniques in addition to therapeutic exercises for patients with SIS, based on an individual assessment”
Manual Therapy Approach vs. Injection
• Rhon DI, Boyles RE, Cleland JA, et al. A manual physical therapy approach versus subacromial corticosteroid injection for treatment of shoulder impingement syndrome: a protocol for a randomised clinical trial. BMJ Open. 2011;1:e000137.doi:10.1136/bmjopen‐2011‐000137
• Rhon DI, Boyles RE, Cleland JA. One‐Year Outcome of Subacromial Corticosteroid Injection Compared With Manual Physical Therapy for the Management of the Unilateral Shoulder Impingement Syndrome: A Pragmatic Randomized Trial. Ann Intern Med. 2014;161:161‐169
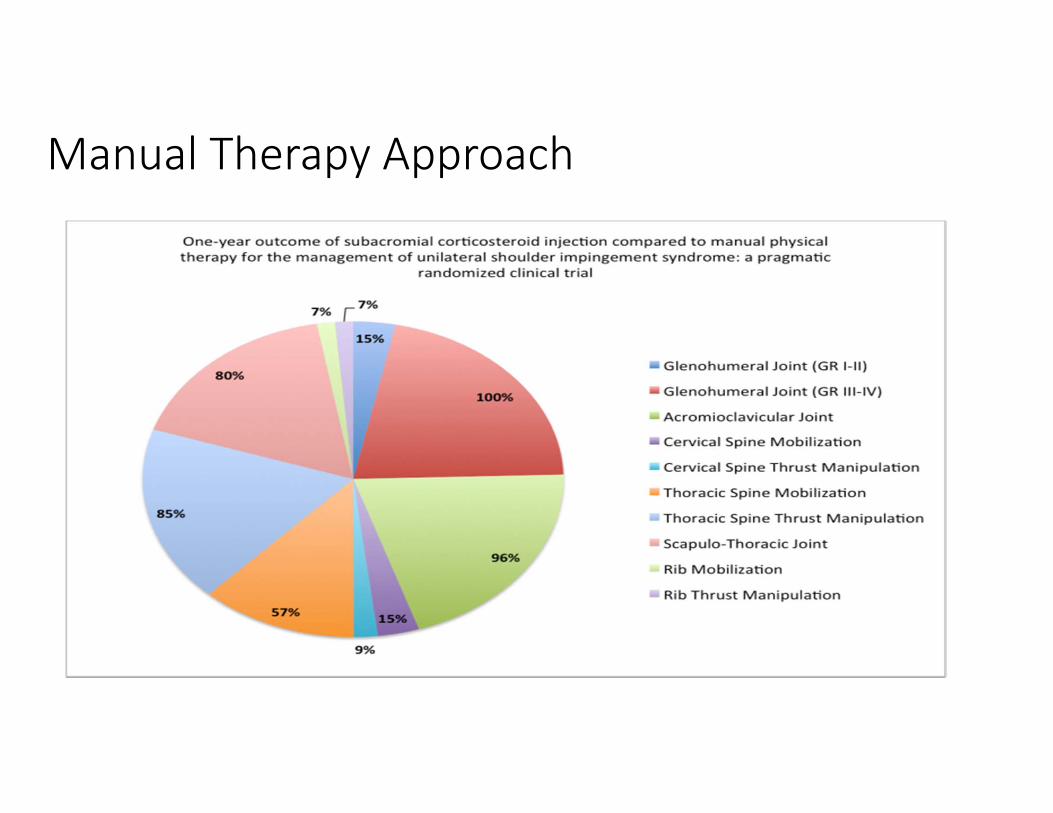
Manual Therapy Approach
Short term effects of isolated thoracic HVLA
Boyles RE, Ritland BM, et. al. The Short‐term effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. Manual Therapy. 2009(14); 375‐380.
• One group pre‐test/post‐test study• 56 patients with SIS treated with only thoracic spine manipulation• Outcomes collected at baseline and 48 hours post treatment
• NPRS (Neer, Hawkins, empty can, resisted ER, resisted IR, resisted abd)• Shoulder Pain and Disability index (SPADI)• Global Rating of Change Scale
• Changes were statistically significant but not clinically significant
Boyles et. al. 2009 Manual Therapy
Short term effects
Intervention techniques
• Seated mid‐thoracic thrust manipulation
• Seated cervicothoracic thrust manipulation
• Supine rib opening manipulation (provided if rib tenderness noted)
Boyles et. al. 2009 Manual Therapy
Short term effects
Results• All outcome measures were statistically significant
• 1/3 of subjects had clinically significant changes in NPRS
How do we identify the 1/3?
Boyles et. al. 2009 Manual Therapy
Subgroup of responders to thoracic OMT
Mintken PE, Cleland JA, et. al. Some Factors Predict Successful Short‐Term Outcomes in Individuals with Shoulder Pain Receiving Cervicothoracic Manipulation: A Single‐Arm Trial. Physical Therapy. 2010; 90‐26‐32.• Prospective single‐arm trial• Standardized examination and treatment
• 1 non‐thrust cervical technique and 5 thoracic thrust techniques• 2 ROM exercises for cervical the thoracic spine
• Successful outcome based on GROC score of +4 to +7• 61% of patients experienced a successful outcome
• 63% of those were achieved after one visit, other 37% after two visits
Mitken et. al. 2010 Physical Therapy
Subgroup of responders to thoracic OMT
Prognostic Variables1. Pain free shoulder flexion
<127°2. Shoudler internal rotation of
<53°3. Negative Neer test4. Not taking medications for
shoulder pain5. Symptoms duration of <90
days
Mitken et. al. 2010 Physical Therapy
Conclusions – 3 big questions
1. Can the prediction rule be validated in separate population?
2. What is the basis of the changes observed?• Biomechanical?• Neurophysiological?
3. Does it Matter?
1. Validity of the thoracic OMT rule
• The Mintekn et al. clinical prediction rule for SIS responding to Thoracic Manipulation has not yet been validated by RCT.
• Internal Validity; Single arm Trial.• External Validity; References demonstrate reductions of pain, improved function and greater patient satisfaction when OMPT directed at the shoulder and cervicothoracic spine is included with care. (list references)
2. Basis of changes observed?
Muth S, Barbe MF, et. al. The effects of thoracic spine manipulation in subjects with signs of rotator cuff tendinopathy. JOSPT. 2012; 42(12):1005‐1016• Controlled EMG laboratory study• 30 subjects with signs of RCT, high level overhead athletes not seeking treatment
• Same manipulation as Boyles et. al. 2009• No changes in range of motion or scapular kinematics• No changes in muscle activation except small middle trap change• Positive changes in Pain, force production, and function
2. Basis of changes observed?
Haik MN, Alburquerque‐Sendin F, et. al. Scapular kindmatics pre‐ and post‐thoracic thrust manipulaion in individuals with and without shoulder impingement sympoms: a randomized controlled study. JOSPT. 2104; 44(7): 475‐487.• Randomized controlled clinical trial• Seated mid thoracic manipulation and sham manipulation • Shoulder pain decreased in both groups• No clinically significant change in scapular kinematics
2. Basis of changes observed?
Kardouni JR, Pidcoe PE, Shaffer SW, Finucane SD, Cheatham SA, Sousa CO, Michener LA. Thoracic Spine Manipulation in Individuals With SubacromialImpingement Syndrome Does Not Immediately Alter Thoracic Spine Kinematics, Thoracic Excursion, or Scapular Kinematics: A Randomized Controlled Trial. J Orthop Sports Phys Ther 2015;45(7):527‐538. Epub 21 May 2015. • Randomized controlled clinical trial• Seated mid thoracic manipulation and sham manipulation • Shoulder pain decreased both groups 1.2 points; 95% CI: 0.3, 1.8; P<.001• Penn shoulder score improved 9.1 points; 95% CI: 6.5, 11.7;P<.001• No clinically significant changes in scapular kinematics or thoracic excursion in either group
2. What is the basis of changes?
• NOT – changes in scapular kinematics• NOT – changes in shoulder muscle activity
• Pain and Function more likely improved through neurophysiological mechanisms
• Mechanical Stimulus initiates a neurophysiologic effect. Bialosky 2009 Peripheral, Spinal and Supraspinal
2. What is the basis of changes? ‐ Peripheral
• Inflammatory mediators affect healing
• Peripheral nociceptors directly affect pain processing
• Reduction of blood and serum cytokine
• Beta‐endorphin, anandamide, N‐palmityolethanolamide, serotonin, endogenous cannabinoids
2. What is the basis of changes? ‐ Spinal
• Bombard spinal cord with sensory input from muscle proprioceptors
• Inhibition of dorsal horn following MT
• Hypoalgesia• Afferent discharge• Motorneuron pool activity• Changes in muscle activity
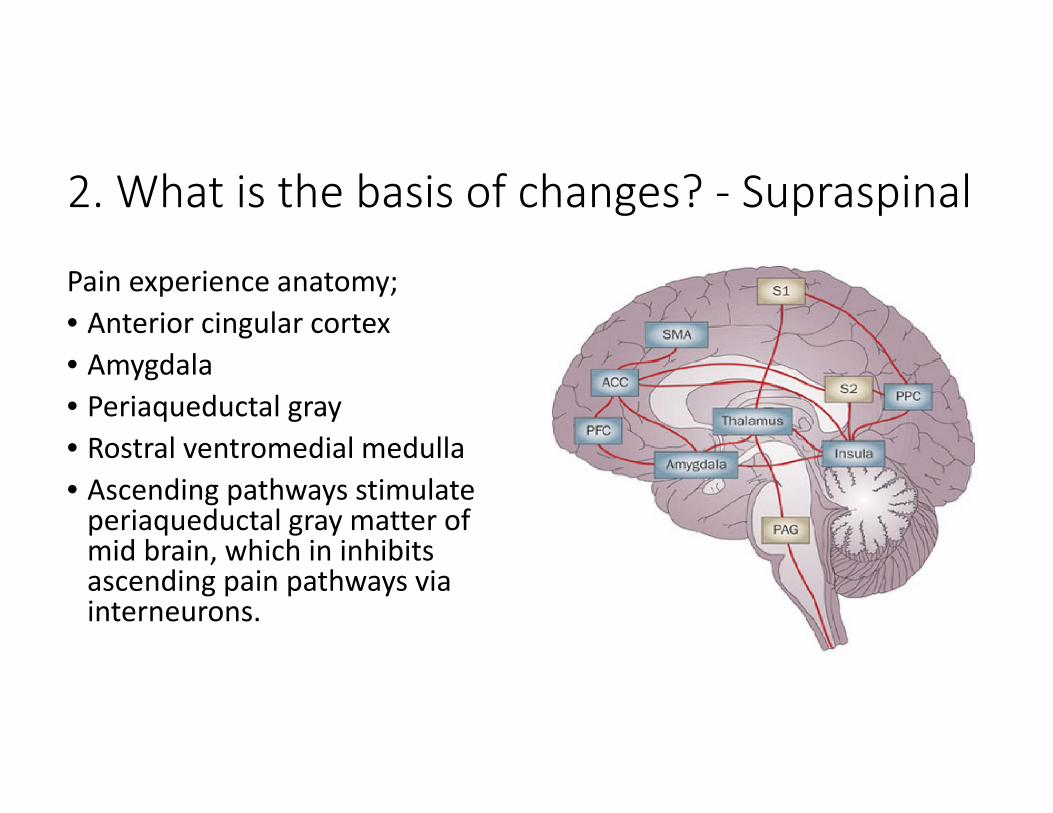
2. What is the basis of changes? ‐ Supraspinal
Pain experience anatomy;• Anterior cingular cortex• Amygdala• Periaqueductal gray• Rostral ventromedial medulla• Ascending pathways stimulate periaqueductal gray matter of mid brain, which in inhibits ascending pain pathways via interneurons.
2. What is the basis of changes? ‐Psychological• Placebo• Expectation• Psyhcosocial factors
3. Does it matter?
• Rebekah L. Lawrence, Jonathan P. Braman, Robert F. Laprade, Paula M. Ludewig Comparison of 3‐Dimensional Shoulder Complex Kinematics in Individuals With and Without Shoulder Pain, Part 1: Sternoclavicular, Acromioclavicular, and Scapulothoracic Joints J Orthop Sports Phys Ther 2014;44(9):636‐A8. Epub 7 Aug 2014. doi:10.2519/jospt.2014.5339
• Found no significant difference in scapular kinematics between subjects with/without SIS
• Similar improvements of pain and function were observed following thoracic manipulation or sham intervention.
Contraindications to Thrust Manipulation
• Vertebral Malignancy• Local infection, severe inflammation, osteoporosis, aneurysm
• Myelopathy• Multiple adjacent radiculopathies• Cauda Equina Syndrome• Vertebral bone disease• Bony Joint Instability• Cervical Rheumatoid Disease
• Vertebral Fractures• Systemic Anitcoagulation• Severe Diabetes or Atherosclerotic Disease
• Vertebral Basilar Artery Disease• Active Spondyloarthropathies• Ligamentous Joint Instability• Congenital Joint Laxity• Local Osteoporosis, Osteomalacia• Acute Disc Herniation
Precautions to Thrust Manipulation
• Unhealed fracture• Excessive pain or irritability• Hypermobility• Joint arthroplasty• Pregnancy of 1st Trimester• Spondylolisthesis• Muscle Guarding• Anticoagulants
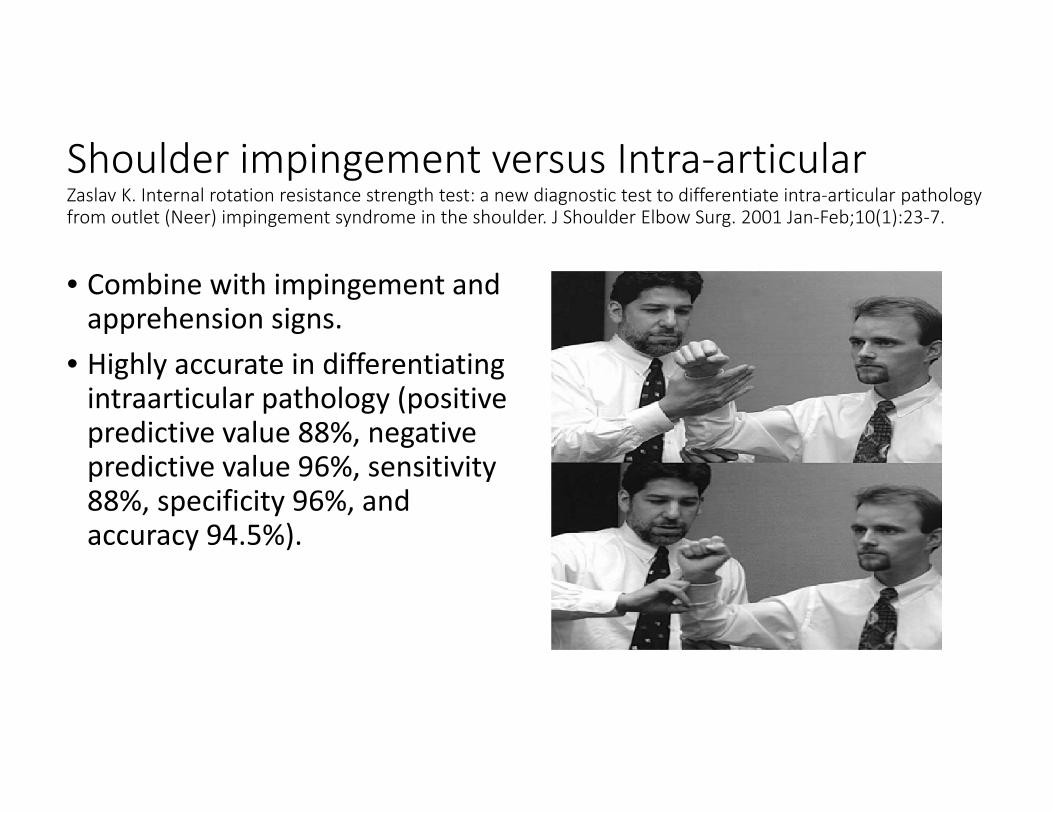
Shoulder impingement versus Intra‐articular Zaslav K. Internal rotation resistance strength test: a new diagnostic test to differentiate intra‐articular pathology from outlet (Neer) impingement syndrome in the shoulder. J Shoulder Elbow Surg. 2001 Jan‐Feb;10(1):23‐7.
• Combine with impingement and apprehension signs.
• Highly accurate in differentiating intraarticular pathology (positive predictive value 88%, negative predictive value 96%, sensitivity 88%, specificity 96%, and accuracy 94.5%).
Neck Pain, Radiculopathy
• Manipulation in the presence of multilevel radiculopathy is discouraged.
• Clinical predication rule for cervical radiculopathy; Spurling, Distraction, ULTT, less than 60 cervical rotation to involved side. All 4 variables present, + lR 30.3 Wainner et al. 2003
• Cervical Radiculopathy likely to respond to PT interventions; Age < 54, dominant arm not affected, looking down does not aggrevate symptoms, multi‐modal treatment > 50% visits (OMPT, traction, DNF, strengthening). 3 variables + LR 5.2 (95% CI 2.4, 11.3) 4 variables + LR 8.3 (95% CI 1.9, 63.9) Cleland 2007
• Pain radiates to beyond elbow
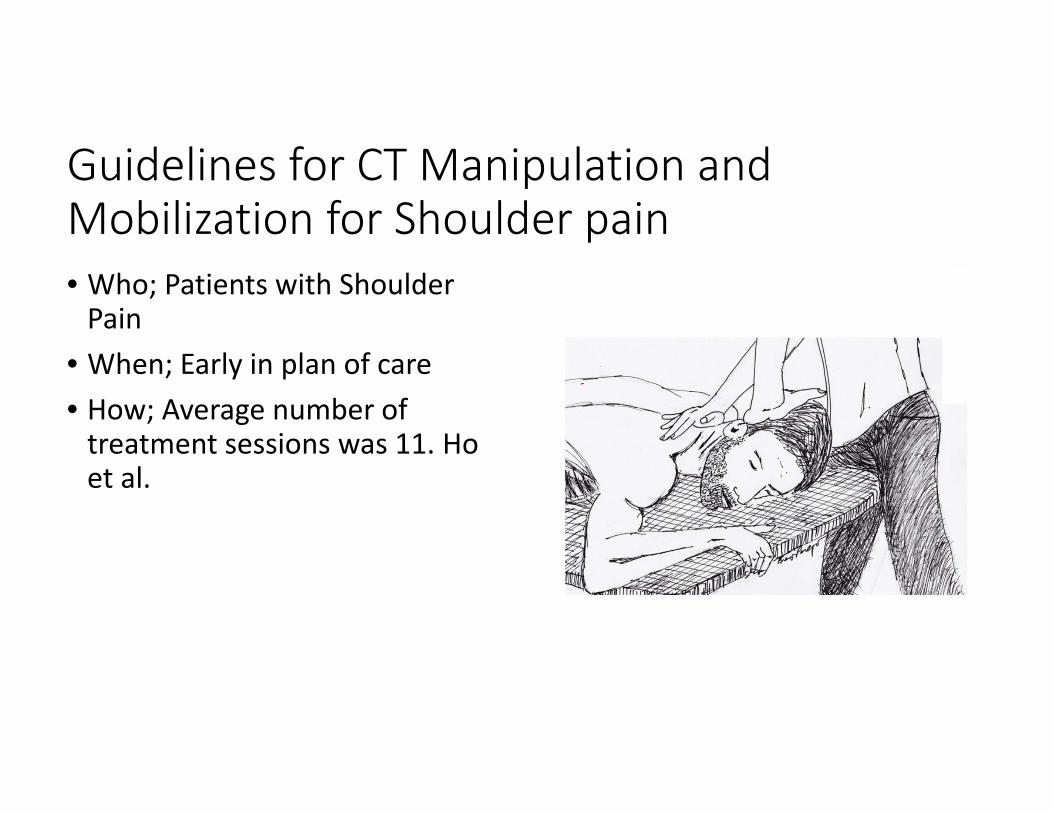
Guidelines for CT Manipulation and Mobilization for Shoulder pain • Who; Patients with Shoulder Pain
• When; Early in plan of care• How; Average number of treatment sessions was 11. Ho et al.
Cervciothoracic Manipulation and Mobilization Techniques suggested for Shoulder Impingement• Seated Cerviothoracic Manipulation and Mobilization• Seated Thoracic Manipulation• Seated Thoracic Distraction with Alligator Grip• Supine Thoracic Manipulation with flexion and extension bias• Supine Cervical Mobilization and Manipulation, Translation, Rotation, Upglide and Downglide
• Scapulothoracic Manipulation• Prone Cervical Posterior to Anterior Glide• Prone Cerviothoracic Manipulation• Prone Thoracic Manipulation
Seated Cerviothoracic Manipulation and MobilizationSeated Mid‐thoracic Manipulation• Patient seated with arms folded across chest, hands on shoulders
• PT places towel roll and chest at lower level of targeted segment
• PT wraps arms around patient and grasps elbows interlocking fingers
• Induce thoracic flexion by leaning patient back into PT, add compression by scooping elbows and distract thoracic spine through elevation of scapulas
• Thrust is provided as HVLAT distraction through legs, flexion through arms, and PA shift through chest
• VIDEO/Sketch HERE
https://www.dropbox.com/sh/3inezldxopvryca/AADOvSg7TvipoeqmHyOYzwYva?dl=0
Seated Thoracic Manipulation
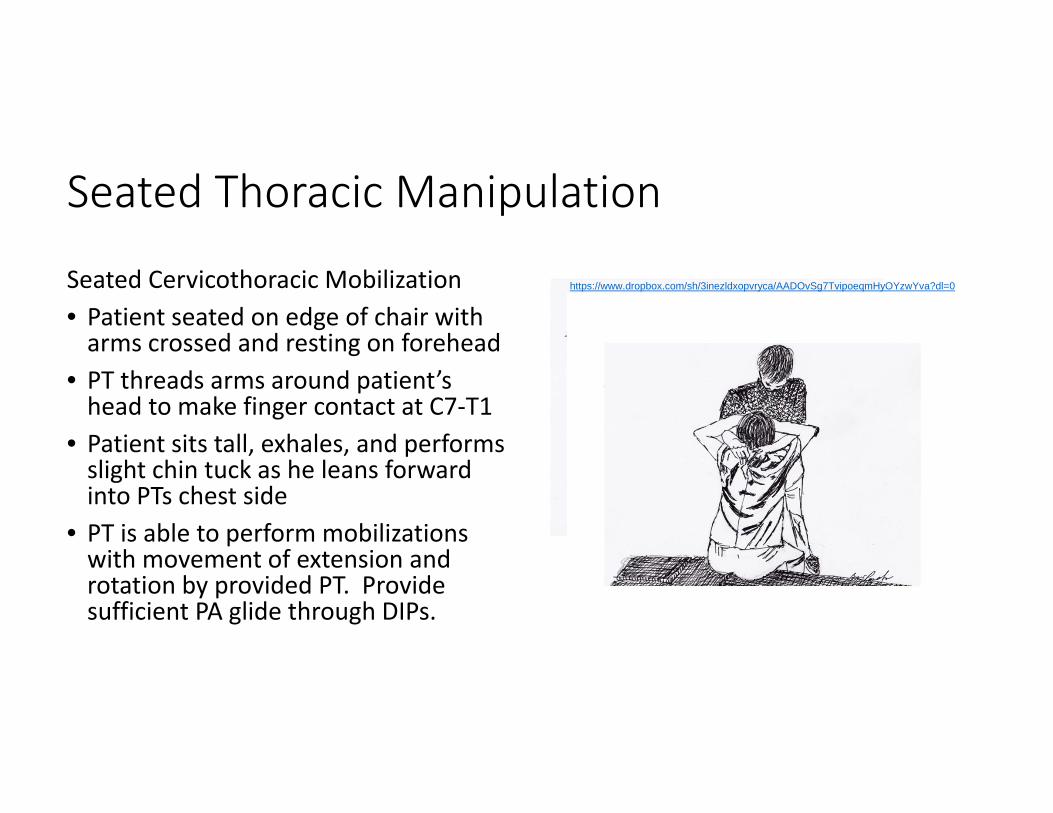
Seated Cervicothoracic Mobilization• Patient seated on edge of chair with arms crossed and resting on forehead
• PT threads arms around patient’s head to make finger contact at C7‐T1
• Patient sits tall, exhales, and performs slight chin tuck as he leans forward into PTs chest side
• PT is able to perform mobilizations with movement of extension and rotation by provided PT. Provide sufficient PA glide through DIPs.
https://www.dropbox.com/sh/3inezldxopvryca/AADOvSg7TvipoeqmHyOYzwYva?dl=0
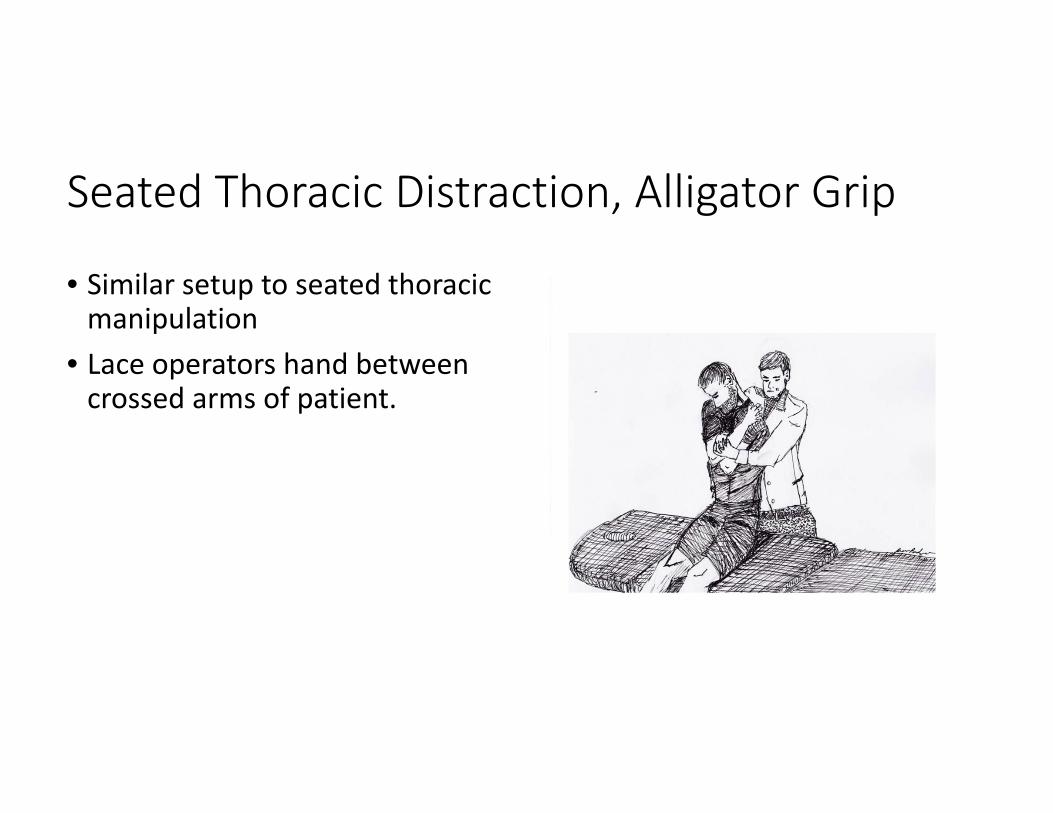
Seated Thoracic Distraction, Alligator Grip
• Similar setup to seated thoracic manipulation
• Lace operators hand between crossed arms of patient.
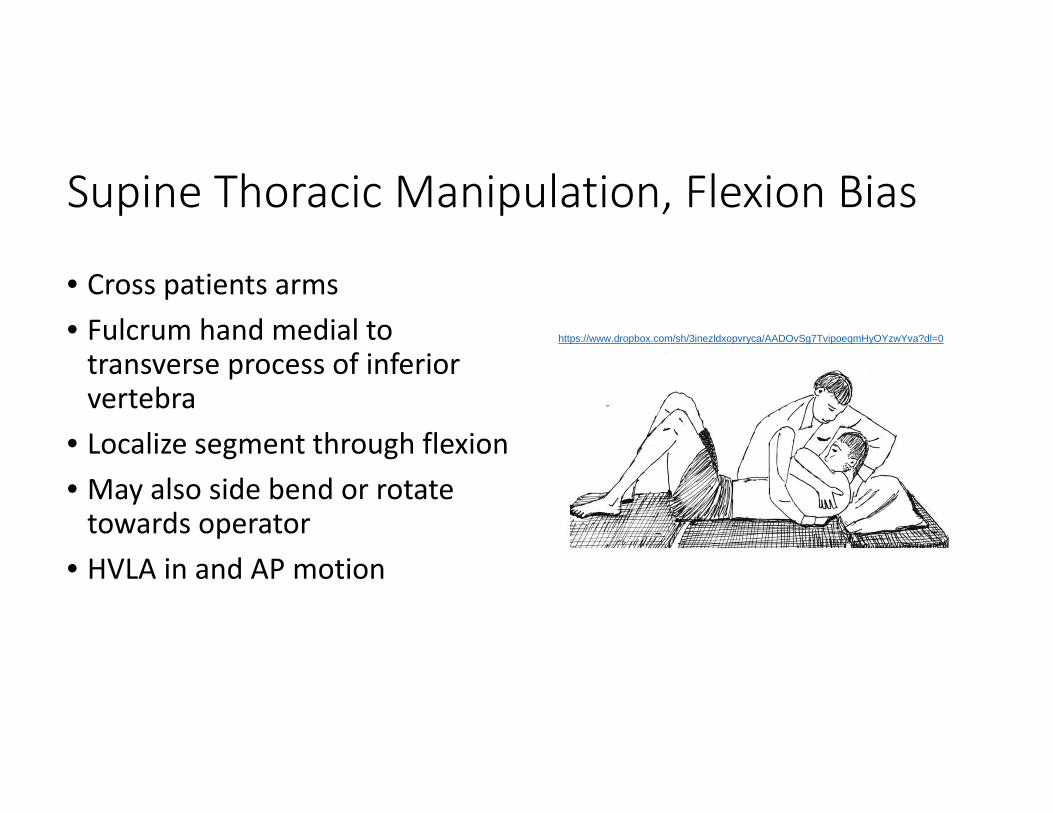
Supine Thoracic Manipulation, Flexion Bias
• Cross patients arms• Fulcrum hand medial to transverse process of inferior vertebra
• Localize segment through flexion• May also side bend or rotate towards operator
• HVLA in and AP motion
https://www.dropbox.com/sh/3inezldxopvryca/AADOvSg7TvipoeqmHyOYzwYva?dl=0
Supine Upper Thoracic Extension Bias
• Patients arms cross• Localize fulcrum• Patient performs bridge• AP thrust directed towards fulcrum
• VIDEO/Sketch HERE
https://www.dropbox.com/sh/3inezldxopvryca/AADOvSg7TvipoeqmHyOYzwYva?dl=0
Supine Cervical Manipulation, Upglide
• Cradle occiput with one hand• Engage lateral side glide with other
• Both induce side flexion, flex down to segment
• Add opposite rotation to engage barrier
• HVLA up towards the opposite eye socket with slight/rapid rotation
• VIDEO/Sketch HERE
Supine Cervical Manipulation, Downglide
• Cradle occiput with one hand• Engage lateral side glide with other
• Both induce side flexion• Add a small amount of opposite rotation to engage barrier
• HVLA downwards towards the opposite shoulder with slight/rapid side bending
• VIDEO/Sketch HERE
Supine Cervical Manipulation Translation
• Mid to Lower segments• Contact articular pillars• Flex head and neck up to segment
• Lateral side flexion glide to first barrier
• Apply gentle lateral thrust
• VIDEO/Sketch HERE
Supine Cervical Manipulation Rotational
• For mid to lower segments• Left MCP on articular pillar of C5• Gently glide into left rotation, skin lock
• Rotate left cervical spine 40‐50 without sidebending
• Right sidebend to barrir• Apply gentle thrust into left rotation
• VIDEO/Sketch HERE
https://www.dropbox.com/sh/3inezldxopvryca/AADOvSg7TvipoeqmHyOYzwYva?dl=0
Scapulothoracic Mobilization and Manipulation• Patient position in sidely• Circular motion in sagittal plane• Manipulative thrust increases posterior tipping of scapula
• VIDEO/Sketch HERE
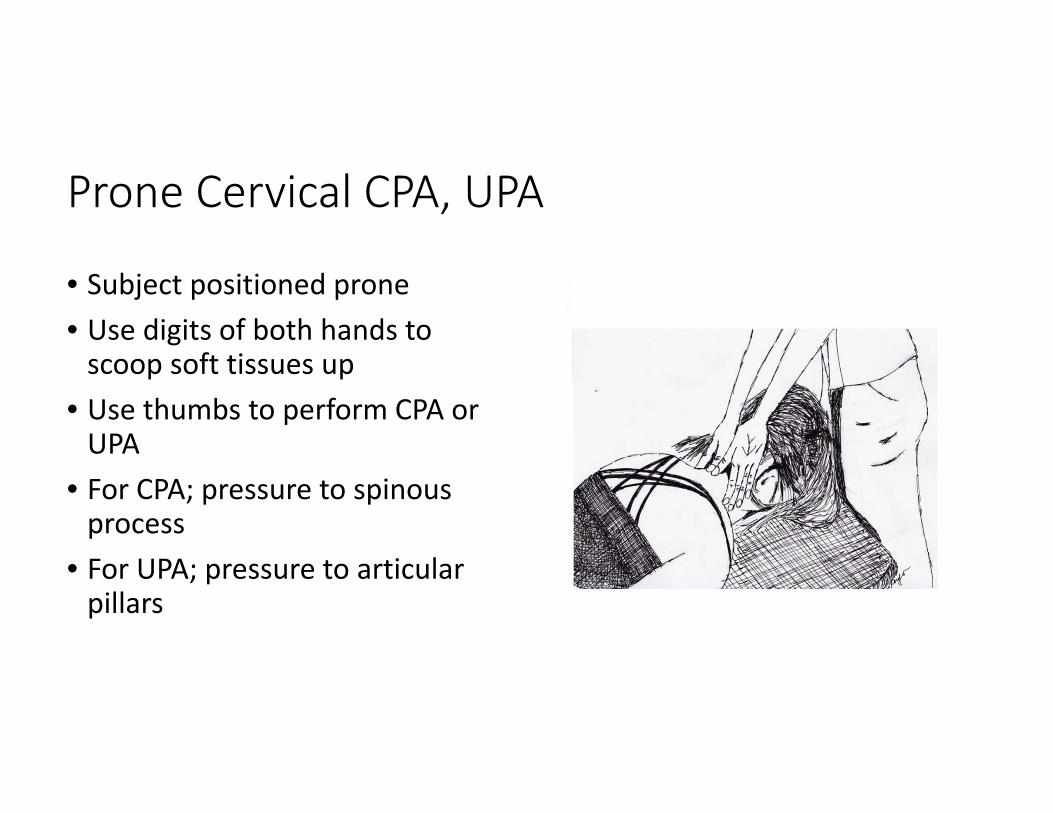
Prone Cervical CPA, UPA
• Subject positioned prone• Use digits of both hands to scoop soft tissues up
• Use thumbs to perform CPA or UPA
• For CPA; pressure to spinous process
• For UPA; pressure to articular pillars
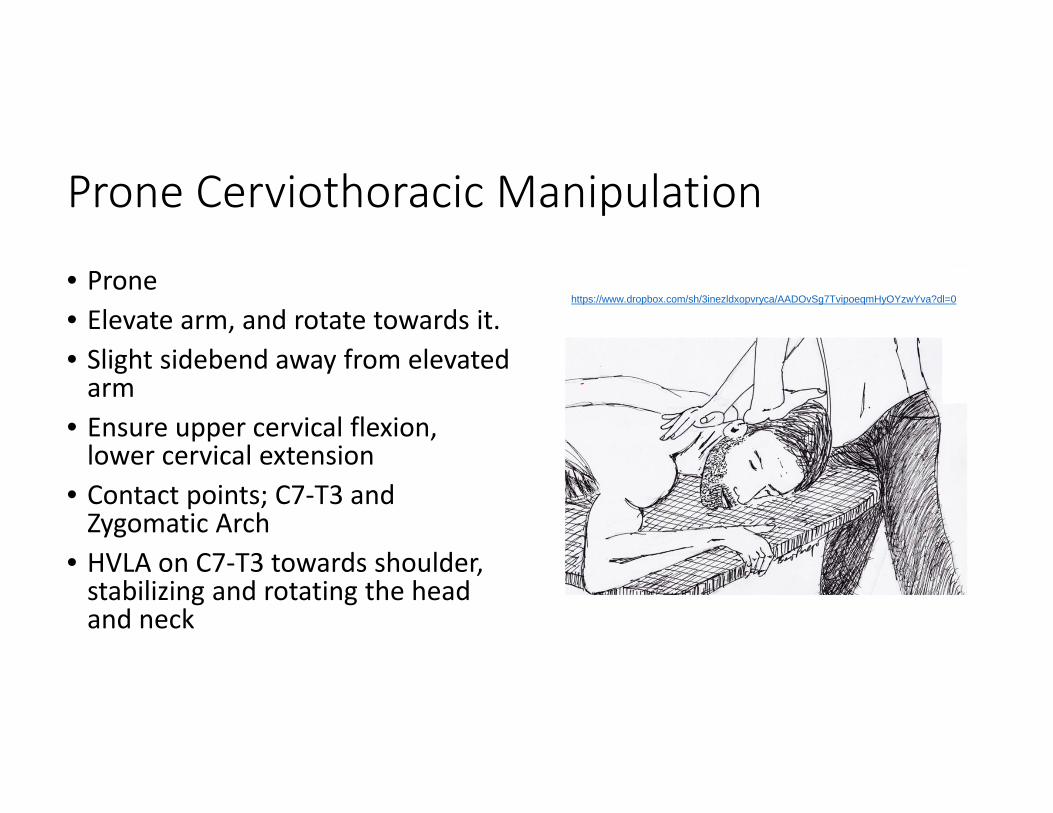
Prone Cerviothoracic Manipulation
• Prone• Elevate arm, and rotate towards it.• Slight sidebend away from elevated arm
• Ensure upper cervical flexion, lower cervical extension
• Contact points; C7‐T3 and Zygomatic Arch
• HVLA on C7‐T3 towards shoulder, stabilizing and rotating the head and neck
https://www.dropbox.com/sh/3inezldxopvryca/AADOvSg7TvipoeqmHyOYzwYva?dl=0
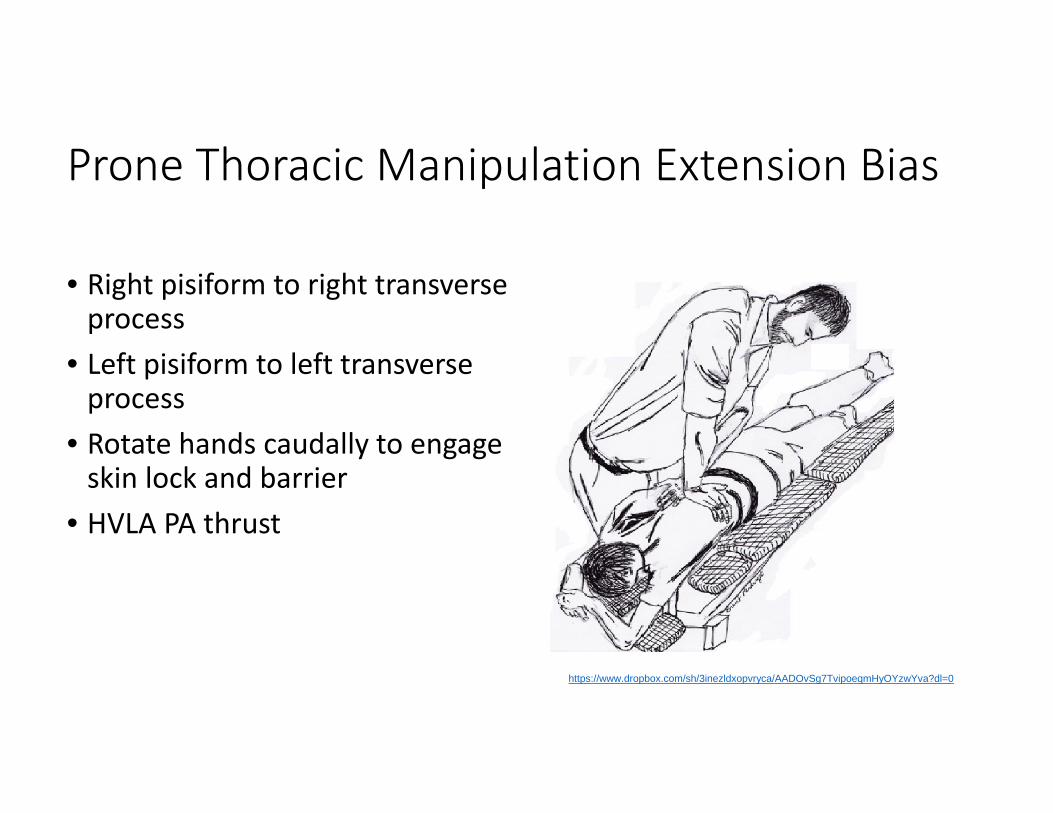
Prone Thoracic Manipulation Extension Bias
• Right pisiform to right transverse process
• Left pisiform to left transverse process
• Rotate hands caudally to engage skin lock and barrier
• HVLA PA thrust
https://www.dropbox.com/sh/3inezldxopvryca/AADOvSg7TvipoeqmHyOYzwYva?dl=0
References• Bialosky, J.E., Bishop, M.D., Price, D.D., Robinson, M.E., and George, S.Z. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model. Manual Therapy. 2009; 14: 531–538
DOI: http://dx.doi.org/10.1016/j.math.2008.09.001
• Boyles RE, Ritland BM, Miracle BM, Barclay DM, Faul MS, Moore JH, Koppenhaver SL, Wainner RS. The short‐term effects of thoracic spine thrust manipulation on patients with shoulder impingement syndrome. Manual Therapy, Vol. 14, Issue 4, p375–380. 2009
• Cleland JA, Fritz JM, Whitman JM, and Heath R. Predictors of Short‐Term Outcome in People With a Clinical Diagnosis of Cervical Radiculopathy PHYS THER December 2007 87:1619‐1632 doi:10.2522/ptj.20060287
• Haik MN, Alburquerque‐Sendín F, Silva CZ, Siqueira‐Junior AL, Ribeiro IL, Camargo PR. Scapular Kinematics Pre— and Post—Thoracic Thrust Manipulation in Individuals With and Without Shoulder Impingement Symptoms: A Randomized Controlled Study. J Orthop Sports Phys Ther 2014;44(7):475‐487. Epub 22 May 2014. doi:10.2519/jospt.2014.4760
• Ho CYC, Sole G, Munn J. The effectiveness of manual therapy in the management of musculoskeletal disorders of the shoulder: A systematic review Published Online: May 22, 2009 http://dx.doi.org/10.1016/j.math.2009.03.008
• Kardouni JR, Pidcoe PE, Shaffer SW, Finucane SD, Cheatham SA, Sousa CO, Michener LA. Thoracic Spine Manipulation in Individuals With Subacromial Impingement Syndrome Does Not Immediately Alter Thoracic Spine Kinematics, Thoracic Excursion, or Scapular Kinematics: A Randomized Controlled Trial. J Orthop Sports Phys Ther 2015;45(7):527‐538. Epub 21 May 2015. doi:10.2519/jospt.2015.5647
• Michener LA, Kardouni J, Lopes Albers AD, Ely JM. Development of a sham comparator for thoracic spinal manipulative therapy for use with shoulder disorders. Manual Therapy, Vol. 18, Issue 1, p60–64 Published online: August 9, 2012
• Mintken PE, Cleland JA, Carpenter KJ, Bieniek ML, Keirns M, Whitman JM. Some Factors Predict Successful Short‐Term Outcomes in Individuals With Shoulder Pain Receiving Cervicothoracic Manipulation: A Single‐Arm Trial PHYS THER January 2010 90:26‐42; published ahead of print December 3, 2009, doi:10.2522/ptj.20090095
• Muth S, Barbe MF, Lauer R, McClure P. The Effects of Thoracic Spine Manipulation in Subjects With Signs of Rotator Cuff Tendinopathy J Orthop Sports Phys Ther 2012;42(12):1005‐1016. doi:10.2519/jospt.2012.4142
• Strunce JB, Walker MJ, Boyles RE, Young BA, The Immediate Effects of Thoracic Spine and Rib Manipulation on Subjects with Primary Complaints of Shoulder Pain. J Man Manip Ther. 2009; 17(4): 230–236. PMCID: PMC2813499
• Wainner RS, Fritz JM, Irrgang JJ, Boninger ML, Delitto A, Allison S. Reliability and diagnostic accuracy of the clinical examination and patient self‐report measures for cervical radiculopathy. Spine (Phila Pa 1976). 2003 Jan 1;28(1):52‐62.
• Winters J, Sobel JS, Groenier KH, Arendzen HJ, Meyboom‐de Jong B. Comparison of physiotherapy, manipulation, and corticosteroid injection for treating shoulder complaints in general practice: randomised, single blind study. BMJ. 1997 May 3;314(7090):1320‐5. http://www.ncbi.nlm.nih.gov/pubmed/9158469?dopt=Abstract
• Video images: Patrick Cook Sketched Images: Brent Perdrizet
THE END
Outline
I. Evidence for cervical, thoracic spine, rib mobilization and manipulation for patients with SIS
II. Thoracic Manipulation and SIS, RCTs and CPR
III. Discussion of Thoracic Manipulation for SIS, Validity, Mechanisms of Action, Clinical Relevance
• IV. Selected Techniques





























