Embed Size (px)
Citation preview
Thoracic
Thoracic surgical radiologyrachel hyland
hilary Moss
Abstractchest radiographs of patients in the intensive care or postoperative set-
ting can be difficult to interpret. Postoperative complications may be life-
threatening and require prompt management. Knowledge of the diverse
radiological appearances of these complications as well as familiarity with
the clinical settings in which specific complications are likely to occur is vital
for prompt, effective treatment. Following pulmonary resection, patients
often have postoperative complications that differ according to the type
of surgery and the time elapsed since surgery was performed. This article
describes the potential complications and gives illustrated explanations of
normal postoperative appearances, for example following pneumonectomy,
as well as demonstrating important complications such as bronchopleural
fistula. The article highlights the differences in the appearance of the chest
radiograph of atelectasis and consolidation, with illustrated examples.
Keywords atelectasis; chest radiograph; complications of thoracic
surgery; consolidation; pneumonectomy; postoperative appearance
Collapse
Lungs or lobes of lungs collapse because of obstruction of the bronchus leading to the lobe or lung. The bronchus may become obstructed by something within the lumen such as a foreign body or a mucous plug, narrowing of the bronchial wall by, for example, a carcinoma or scarring from tuberculosis, or some-thing compressing the bronchus from outside the wall, such as a mediastinal lymph node mass.
There are two main signs seen on the plain radiograph (Figures 1–4). First, the collapsed lobe is more opaque than usual, as the same amount of lung parenchyma occupies a smaller vol-ume and there is retention of mucus within the lobe. In addition, there are signs of volume loss – direct signs with displacement of fissures, blood vessels and bronchi, and indirect signs where
Rachel Hyland, MBChB, FRCR, is a Specialist Registrar in Radiology on
the Leeds Training Scheme. She qualified from Sheffield in 1999, and
has been working in the Leeds Teaching Hospitals NHS Trust since
2002, with a specialist interest in cross-sectional imaging. Competing
interests: none declared.
Hilary Moss, MRCP, FRCR, is a Consultant Radiologist in Harrogate
and District NHS Foundation Trust. She trained in radiology in
Addenbrooke’s and Papworth hospitals, Cambridge, before becoming
a Consultant in the Leeds Teaching Hospitals NHS Trust from 1999 to
2005. Her specialist interests are thoracic and oncological imaging.
Competing interests: none declared.
aNaESThESia aND iNTENSiVE carE MEDiciNE 9:11 47
there is shift of other structures to compensate for the volume loss of the collapsed lobe. Indirect signs of volume loss include overexpansion of the adjacent lobe which therefore appears less dense than normal as it contains relatively more air with stretched parenchyma, elevation of the ipsilateral hemidiaphragm, tracheal or mediastinal shift and narrowing of the space between ribs.
Consolidation
Consolidation occurs when the air spaces are filled with cells (carcinoma), pus (pneumonia), blood (pulmonary haemor-rhage), fluid (inflammatory or cardiac failure) or protein (alve-olar proteinosis) rather than air. Consolidation (Figures 5–7)
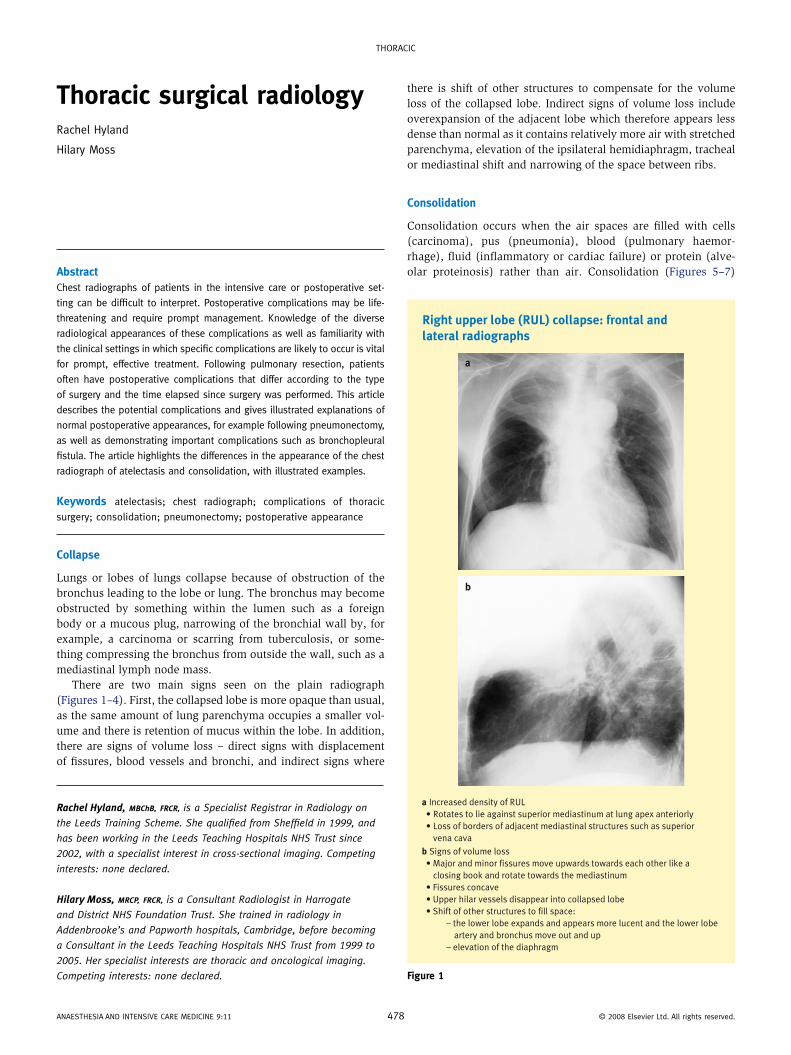
Right upper lobe (RUL) collapse: frontal and lateral radiographs
a
b
a Increased density of RUL
• Rotates to lie against superior mediastinum at lung apex anteriorly
• Loss of borders of adjacent mediastinal structures such as superior
vena cava
b Signs of volume loss
• Major and minor fissures move upwards towards each other like a
closing book and rotate towards the mediastinum
• Fissures concave
• Upper hilar vessels disappear into collapsed lobe
• Shift of other structures to fill space:
– the lower lobe expands and appears more lucent and the lower lobe
artery and bronchus move out and up
– elevation of the diaphragm
Figure 1
8 © 2008 Elsevier Ltd. all rights reserved.
Thoracic
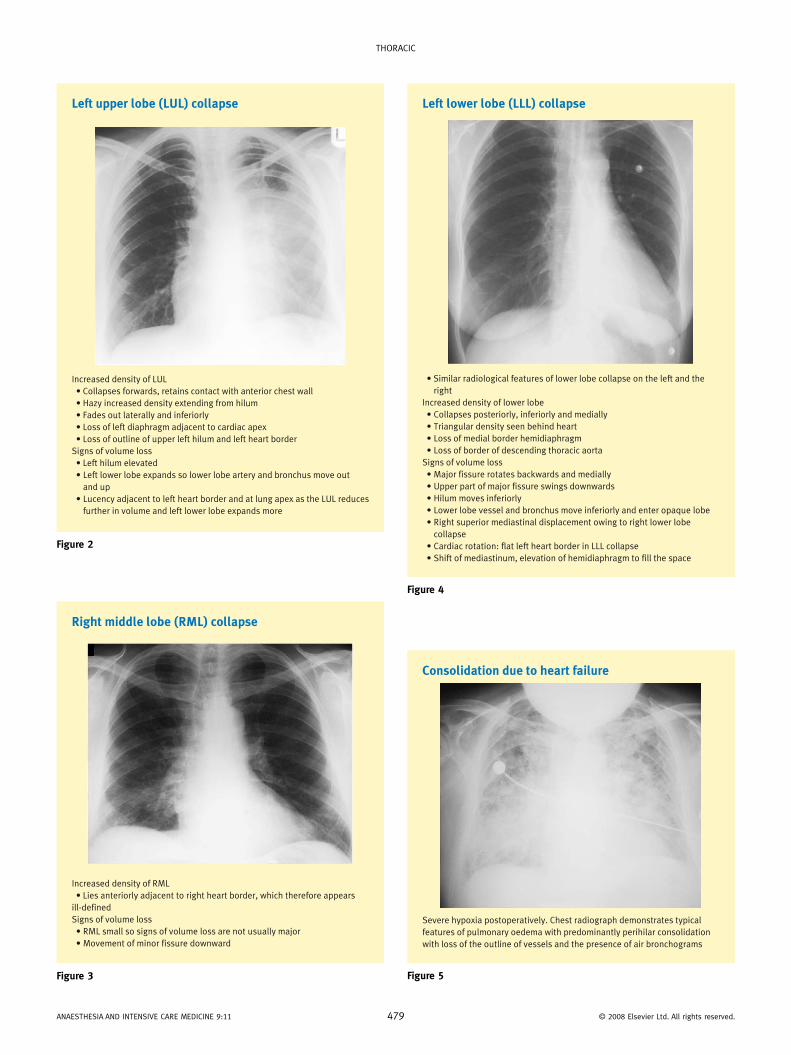
Left upper lobe (LUL) collapse
Increased density of LUL
• Collapses forwards, retains contact with anterior chest wall
• Hazy increased density extending from hilum
• Fades out laterally and inferiorly
• Loss of left diaphragm adjacent to cardiac apex
• Loss of outline of upper left hilum and left heart border
Signs of volume loss
• Left hilum elevated
• Left lower lobe expands so lower lobe artery and bronchus move out
and up
• Lucency adjacent to left heart border and at lung apex as the LUL reduces
further in volume and left lower lobe expands more
Figure 2
Right middle lobe (RML) collapse
Increased density of RML
• Lies anteriorly adjacent to right heart border, which therefore appears
ill-defined
Signs of volume loss
• RML small so signs of volume loss are not usually major
• Movement of minor fissure downward
Figure 3
aNaESThESia aND iNTENSiVE carE MEDiciNE 9:11 479
Left lower lobe (LLL) collapse
• Similar radiological features of lower lobe collapse on the left and the
right
Increased density of lower lobe
• Collapses posteriorly, inferiorly and medially
• Triangular density seen behind heart
• Loss of medial border hemidiaphragm
• Loss of border of descending thoracic aorta
Signs of volume loss
• Major fissure rotates backwards and medially
• Upper part of major fissure swings downwards
• Hilum moves inferiorly
• Lower lobe vessel and bronchus move inferiorly and enter opaque lobe
• Right superior mediastinal displacement owing to right lower lobe
collapse
• Cardiac rotation: flat left heart border in LLL collapse
• Shift of mediastinum, elevation of hemidiaphragm to fill the space
Figure 4
Consolidation due to heart failure
Severe hypoxia postoperatively. Chest radiograph demonstrates typical
features of pulmonary oedema with predominantly perihilar consolidation
with loss of the outline of vessels and the presence of air bronchograms
Figure 5
© 2008 Elsevier Ltd. all rights reserved.
Thoracic
appears as an area of increase in lung density which is ill defined except at a pleural margin such as a fissure. There is no volume loss with pure consolidation; in fact, there may be an increase in the volume of the lobe. Normal vessels are not seen as they are no longer surrounded by contrasting air. Air bronchograms which are seen as branching linear lucencies may be seen in an area of consolidation and are due to air present in normal bron-chi which is now contrasted against the increased density of the filled airspaces. Signs of consolidation localize an abnormality to the pulmonary parenchyma.
Thoracic surgery: pneumonectomy and its complications
Complications following pneumonectomy may be classified as early or late (Table 1). Sequential chest radiographs are used to screen for these complications in the early postoperative period (Figure 8).
Bronchopleural fistula
Bronchopleural fistula (BPF) occurs when there is a communica-tion between the airway and the pleural space and is a poten-tially fatal complication of pneumonectomy. The incidence is reported to be up to 9%,1 with an associated mortality rate of 16–23%,2 usually due to aspiration pneumonia with subsequent acute respiratory distress syndrome.3 A BPF is more likely to occur after right pneumonectomy than after left pneumonec-tomy.2,3 In the early postoperative period the aetiology is usu-ally either infection or operative technique. Late development of a BPF is most likely due to local recurrence at the bronchial stump. As there is a communication between the airway and the pleural space there is an increase in or reappearance of air in the pneumonectomy space and so it is important to monitor changes in the air–fluid level in patients who have undergone a pneumo-nectomy.4 The features of BPF on chest radiograph are shown in Table 2 and Figure 9.
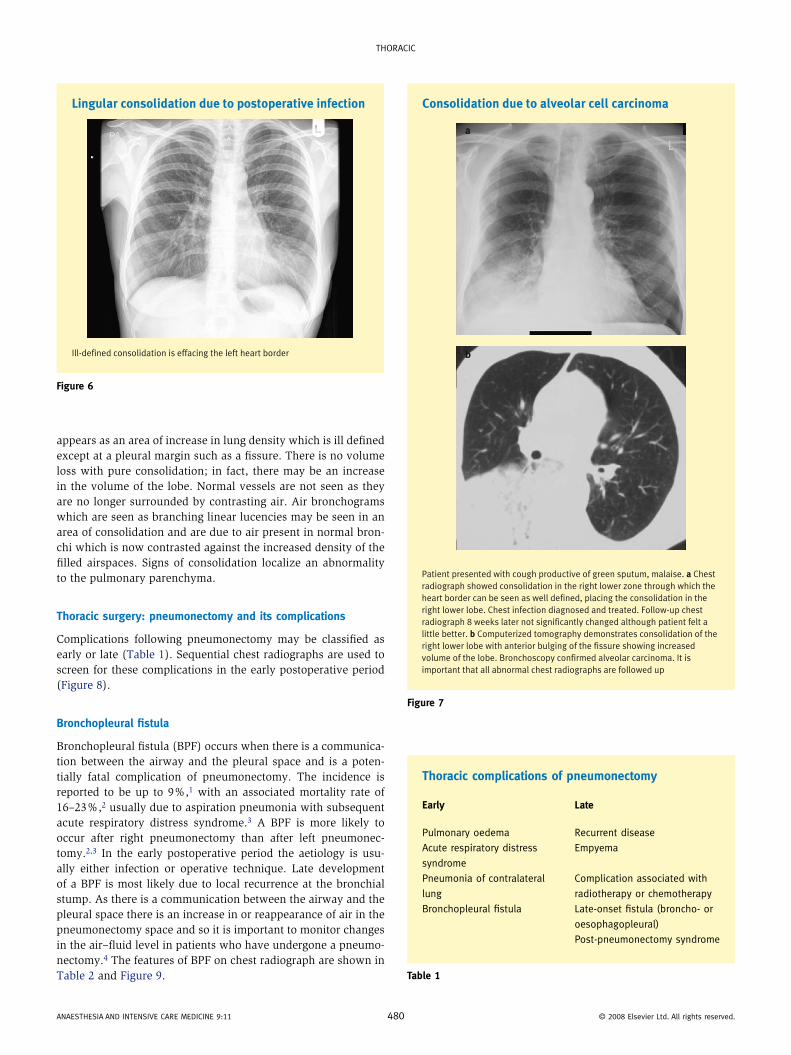
Lingular consolidation due to postoperative infection
Ill-defined consolidation is effacing the left heart border
Figure 6
aNaESThESia aND iNTENSiVE carE MEDiciNE 9:11 480
Thoracic complications of pneumonectomy
Early Late
Pulmonary oedema recurrent disease
acute respiratory distress
syndrome
Empyema
Pneumonia of contralateral
lung
complication associated with
radiotherapy or chemotherapy
Bronchopleural fistula Late-onset fistula (broncho- or
oesophagopleural)
Post-pneumonectomy syndrome
Table 1
Consolidation due to alveolar cell carcinoma
a
b
Patient presented with cough productive of green sputum, malaise. a Chest
radiograph showed consolidation in the right lower zone through which the
heart border can be seen as well defined, placing the consolidation in the
right lower lobe. Chest infection diagnosed and treated. Follow-up chest
radiograph 8 weeks later not significantly changed although patient felt a
little better. b Computerized tomography demonstrates consolidation of the
right lower lobe with anterior bulging of the fissure showing increased
volume of the lobe. Bronchoscopy confirmed alveolar carcinoma. It is
important that all abnormal chest radiographs are followed up
Figure 7
© 2008 Elsevier Ltd. all rights reserved.
Thoracic
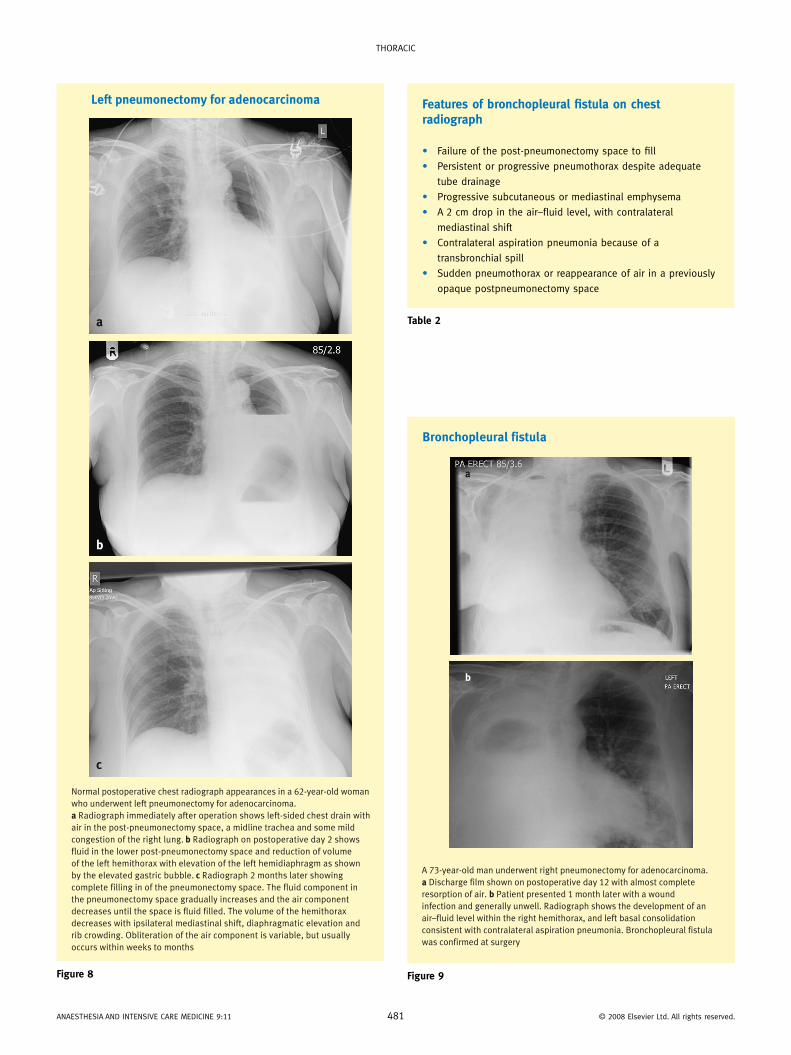
Left pneumonectomy for adenocarcinoma
a
b
c
Normal postoperative chest radiograph appearances in a 62-year-old woman
who underwent left pneumonectomy for adenocarcinoma.
a Radiograph immediately after operation shows left-sided chest drain with
air in the post-pneumonectomy space, a midline trachea and some mild
congestion of the right lung. b Radiograph on postoperative day 2 shows
fluid in the lower post-pneumonectomy space and reduction of volume
of the left hemithorax with elevation of the left hemidiaphragm as shown
by the elevated gastric bubble. c Radiograph 2 months later showing
complete filling in of the pneumonectomy space. The fluid component in
the pneumonectomy space gradually increases and the air component
decreases until the space is fluid filled. The volume of the hemithorax
decreases with ipsilateral mediastinal shift, diaphragmatic elevation and
rib crowding. Obliteration of the air component is variable, but usually
occurs within weeks to months
Figure 8
aNaESThESia aND iNTENSiVE carE MEDiciNE 9:11 481
Table 2
Features of bronchopleural fistula on chest radiograph
• Failure of the post-pneumonectomy space to fill
• Persistent or progressive pneumothorax despite adequate
tube drainage
• Progressive subcutaneous or mediastinal emphysema
• a 2 cm drop in the air–fluid level, with contralateral
mediastinal shift
• contralateral aspiration pneumonia because of a
transbronchial spill
• Sudden pneumothorax or reappearance of air in a previously
opaque postpneumonectomy space
Bronchopleural fistula
a
b
A 73-year-old man underwent right pneumonectomy for adenocarcinoma.
a Discharge film shown on postoperative day 12 with almost complete
resorption of air. b Patient presented 1 month later with a wound
infection and generally unwell. Radiograph shows the development of an
air–fluid level within the right hemithorax, and left basal consolidation
consistent with contralateral aspiration pneumonia. Bronchopleural fistula
was confirmed at surgery
Figure 9
© 2008 Elsevier Ltd. all rights reserved.
Thoracic
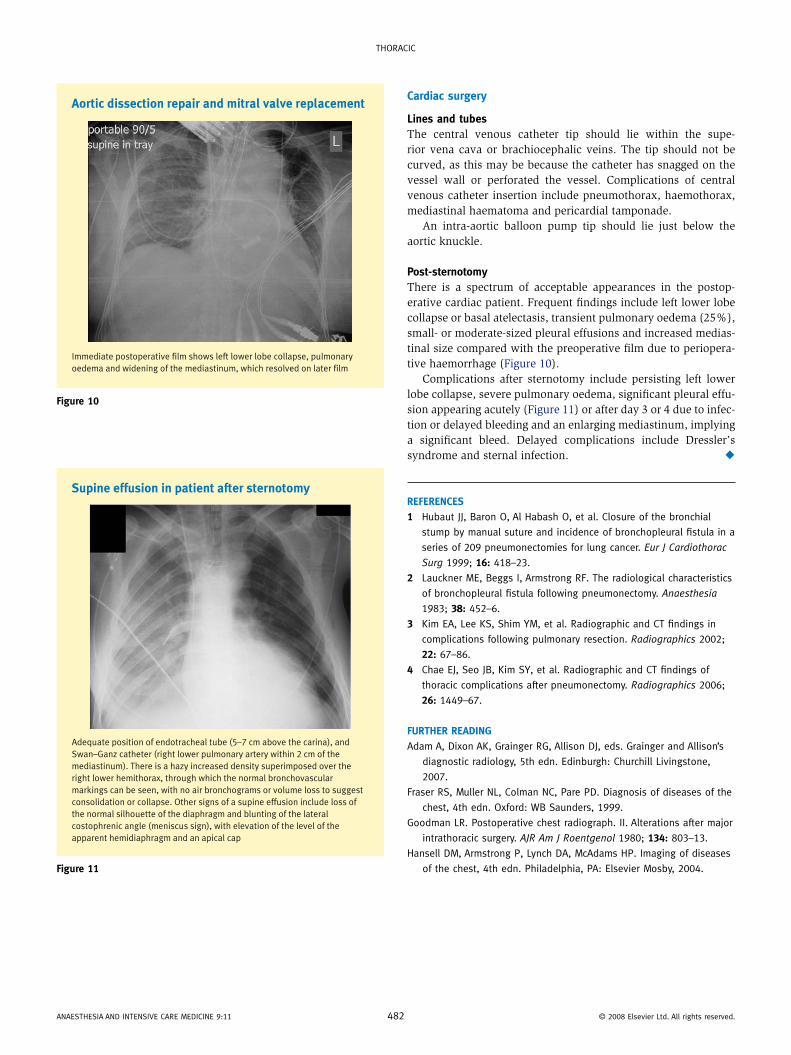
Aortic dissection repair and mitral valve replacement
Immediate postoperative film shows left lower lobe collapse, pulmonary
oedema and widening of the mediastinum, which resolved on later film
Figure 10
Supine effusion in patient after sternotomy
Adequate position of endotracheal tube (5–7 cm above the carina), and
Swan–Ganz catheter (right lower pulmonary artery within 2 cm of the
mediastinum). There is a hazy increased density superimposed over the
right lower hemithorax, through which the normal bronchovascular
markings can be seen, with no air bronchograms or volume loss to suggest
consolidation or collapse. Other signs of a supine effusion include loss of
the normal silhouette of the diaphragm and blunting of the lateral
costophrenic angle (meniscus sign), with elevation of the level of the
apparent hemidiaphragm and an apical cap
Figure 11
aNaESThESia aND iNTENSiVE carE MEDiciNE 9:11 48
Cardiac surgery
Lines and tubesThe central venous catheter tip should lie within the supe-rior vena cava or brachiocephalic veins. The tip should not be curved, as this may be because the catheter has snagged on the vessel wall or perforated the vessel. Complications of central venous catheter insertion include pneumothorax, haemothorax, mediastinal haematoma and pericardial tamponade.
An intra-aortic balloon pump tip should lie just below the aortic knuckle.
Post-sternotomyThere is a spectrum of acceptable appearances in the postop-erative cardiac patient. Frequent findings include left lower lobe collapse or basal atelectasis, transient pulmonary oedema (25%), small- or moderate-sized pleural effusions and increased medias-tinal size compared with the preoperative film due to periopera-tive haemorrhage (Figure 10).
Complications after sternotomy include persisting left lower lobe collapse, severe pulmonary oedema, significant pleural effu-sion appearing acutely (Figure 11) or after day 3 or 4 due to infec-tion or delayed bleeding and an enlarging mediastinum, implying a significant bleed. Delayed complications include Dressler’s syndrome and sternal infection. ◆
REFEREnCEs
1 hubaut JJ, Baron o, al habash o, et al. closure of the bronchial
stump by manual suture and incidence of bronchopleural fistula in a
series of 209 pneumonectomies for lung cancer. Eur J Cardiothorac
Surg 1999; 16: 418–23.
2 Lauckner ME, Beggs i, armstrong rF. The radiological characteristics
of bronchopleural fistula following pneumonectomy. Anaesthesia
1983; 38: 452–6.
3 Kim Ea, Lee KS, Shim YM, et al. radiographic and cT findings in
complications following pulmonary resection. Radiographics 2002;
22: 67–86.
4 chae EJ, Seo JB, Kim SY, et al. radiographic and cT findings of
thoracic complications after pneumonectomy. Radiographics 2006;
26: 1449–67.
FuRThER REAding
adam a, Dixon aK, Grainger rG, allison DJ, eds. Grainger and allison’s
diagnostic radiology, 5th edn. Edinburgh: churchill Livingstone,
2007.
Fraser rS, Muller NL, colman Nc, Pare PD. Diagnosis of diseases of the
chest, 4th edn. oxford: WB Saunders, 1999.
Goodman Lr. Postoperative chest radiograph. ii. alterations after major
intrathoracic surgery. AJR Am J Roentgenol 1980; 134: 803–13.
hansell DM, armstrong P, Lynch Da, Mcadams hP. imaging of diseases
of the chest, 4th edn. Philadelphia, Pa: Elsevier Mosby, 2004.
2 © 2008 Elsevier Ltd. all rights reserved.