Embed Size (px)
Citation preview

Three Mile Island
Accident

Outlines
Description of the event of the accident
Date of accident
Schematic diagram of TMI UNIT2
The sequence of events(SENARIO)
Lessons learned
Simulation of the accident
TMI-2 analysis
Mitigation of the accident
Timeline
References

Description of the Event
Location of the accident
The Three Mile Island accident was a partial
core meltdown in Unit 2 (a pressurized water
reactor manufactured by Babcock & Wilcox)
of the Three Mile Island Nuclear Generating
Station in Dauphin County, Pennsylvania near
Harrisburg. The plant was owned and operated
by General Public Utilities and the
Metropolitan Edison Co. Metropolitan Edison
pleads guilty to falsifying reactor leak rates
right before the emergency. In fact, if the reactor was shut down for repairs as per
regulations, the partial meltdown would not have occurred at that time. It was the
most significant accident in the history of the American commercial nuclear power
generating industry, resulting in the release of up to 481 PBq (13 million curies) of
radioactive gases, but less than 740 GBq (20 curies) of the particularly dangerous
iodine-131.
Date of accident
In March 1979, an event occurred at the Three Mile Island Unit 2 that resulted in
the first case of melted fuel in a full scale commercial nuclear power plant. There
had been prior cases of small scale fuel melting, e.g. the Fermi 1 reactor near
Monroe, Michigan. TMI-2 was a Babcock & Wilcox unit with a vertical once-
through steam generator. In the event a valve in the secondary system closed and
initiated the sequence of events.

Schematic diagram of the TMI unit 2
10. Pumps
1. Reactor building 11. Steam A. Primary circuit
2. Reactor core 12. Turbine
3. Reactor vessel 13. Alternator B. Secondary circuit
4. Control rods 14. Transformer
5. Pressurizer 15. Condenser C. Condenser circuit
6. Relief valve 16. Water
7. Block valve 17. Cooling tower
8. Drain tank
9. Steam generator
As shown in the last fig. the type of THI unit 2 is the PWR with initiating
event of LOCA(loss of coolant accident). due to inadequate training and
human factors, such as industrial design errors relating to ambiguous
control room indicators in the power plant's user interface.

The sequence of events (SENARIO) was
1- A valve in the condensate system
(between the condenser and the pump
on the secondary side) failed closed,
which reduced the amount of water
being supplied to the steam generator;
the main feed water pumps and the
turbine tripped within seconds.
2- The design of the vertical one-through steam generator is such that
there is not much water on the secondary (non- radioactive) outer side
of the steam generator tubes that will boil to steam when the plant is at
full power and the reactor continues to put out full power; thus all the
water on the secondary side was rapidly converted to steam within
minutes. The emergency feed water pumps, which started as expected,
were unable to inject water into the steam generators because several
valves in the system were closed.
3- The reactor continued to heat the reactor coolant. The reactor coolant
pumps continued circulating the water to the steam generators,
however no heat could be removed by the secondary side since there
was no water in the steam generators. The reactor coolant system
started to heat up.
4- Pressure rose in the reactor cooling system until the reactor shutdown.
A power operated relief valve opened in the line between the
pressurizer and the quench tank. This valve failed to reclose when it
was supposed to - after pressure dropped below the setpoint for
closure. This relief valve continued to discharge to the quench tank.
The fact that the valve was open allowed steam to continue
discharging to the quench tank. Pressure dropped in the reactor
cooling system because the valve was still open (however, due to poor
control board design and a failure to indicate the valve position
properly, the operators did not know the valve was open). The quench
tank has a rupture disc that opens at about 10-12 pounds per square
inch. When this happened, the steam was released to the containment.
5- The pressurizer is normally at about 650F. As pressure dropped in the
reactor cooling system, eventually water in the upper-most area of the
reactor (about 10-15 feet above the fuel) flashed to steam. The
indicated water level in the pressurizer stayed high (the relationship
between the pressurizer and the reactor was like a manometer).
6- The operators turned off the emergency water injection pumps
because they thought there was still water in the pressurizer.
7- The operators turned off the reactor cooling pumps because they were
concerned about damage due to potential excessive vibration.. This
resulted in a steam void forming in the reactor coolant loop. In
addition, a steam bubble formed in the upper part of the reactor above
the fuel. Eventually as the fuel heated, this void expanded. Eventually,
the fuel cladding material overheated. It is likely that some hydrogen
was produced by a chemical reaction between the zircaloy clad and
the steam in the reactor. In addition, the hydrogen normally present in
the reactor cooling system (used to reduce the presence of oxygen and
subsequent corrosion in the system) was released to the containment
through
8- At one point, containment pressure rapidly spiked to 28 pounds per
square inch; then rapidly dropped. This was most likely due to the
chemical reaction of hydrogen with the oxygen in the containment.
9- Water was added to the reactor cooling system and the level raised in
the pressurizer until cooling of the reactor was assured.
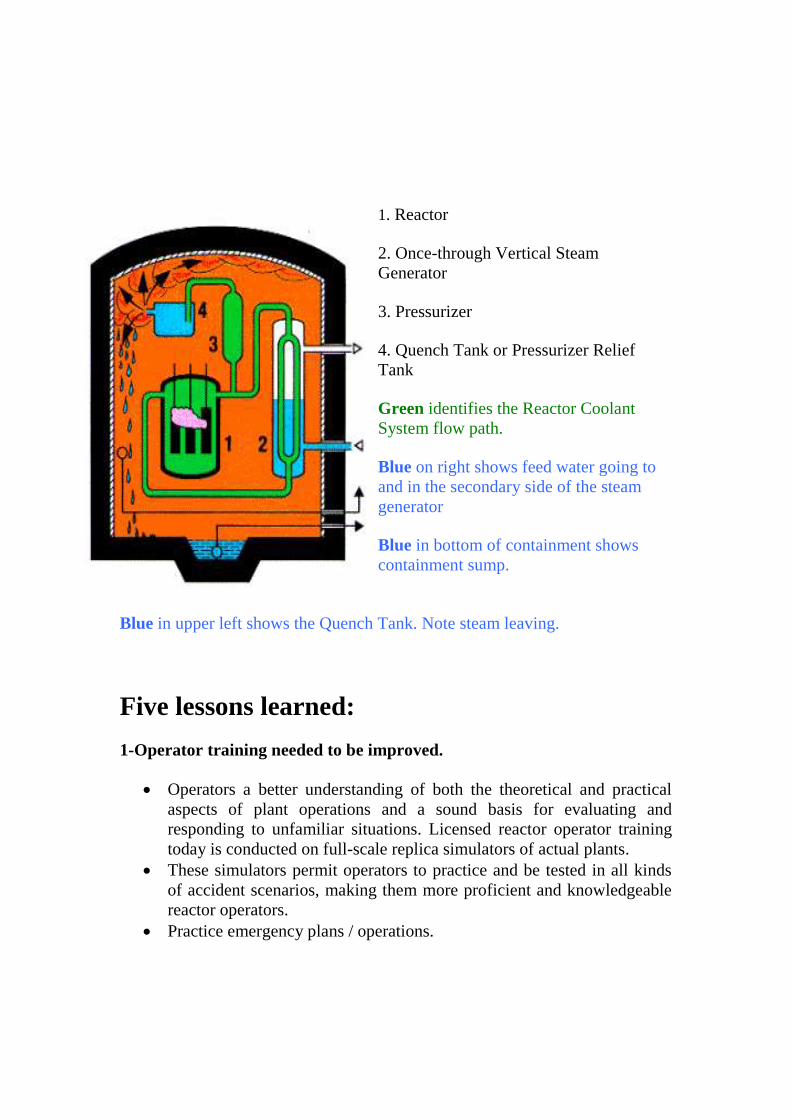
1. Reactor
2. Once-through Vertical Steam
Generator
3. Pressurizer
4. Quench Tank or Pressurizer Relief
Tank
Green identifies the Reactor Coolant
System flow path.
Blue on right shows feed water going to
and in the secondary side of the steam
generator
Blue in bottom of containment shows
containment sump.
Blue in upper left shows the Quench Tank. Note steam leaving.
Five lessons learned:
1-Operator training needed to be improved.
Operators a better understanding of both the theoretical and practical
aspects of plant operations and a sound basis for evaluating and
responding to unfamiliar situations. Licensed reactor operator training
today is conducted on full-scale replica simulators of actual plants.
These simulators permit operators to practice and be tested in all kinds
of accident scenarios, making them more proficient and knowledgeable
reactor operators.
Practice emergency plans / operations.

2-Sharing of industry knowledge needed to be more effective
TMI led to the establishment of the Atlanta-based Institute of
Nuclear Power Operations (INPO) and its National Academy for
Nuclear Training. These two industry organizations have been
effective in promoting excellence in the operation of nuclear
plants and accrediting their training programs.
INPO has had a profound impact on the way nuclear plants are
managed and operated. The proof is the steady improvement in
plant performance in the 30 years since TMI. Plant capacity
factors (the ratio of a power plant's average production to its
rated capability) have increased to 91.8 percent in 2007 from
58.4 percent in 1979. Meanwhile, the industry average of
significant events has decreased from an average of 0.9 per year
in 1989 to 0.01 per year in 2006.
3-Fission products don't escape in the real world.
The accident at TMI yielded insight into the "source term"--the
amount of radioactive fission products released in the event of a
major accident. From TMI data we learned that the release of
volatile fission products was three to four orders of magnitude
smaller than that provided for in the 1962 federal licensing
criteria.
This knowledge, that strict leak-tightness of the containment
wasn't a significant factor in reducing fission product leakage to
the biosphere, led to the downward revisions by the NRC toward
a more realistic source term in 1995.
Since that time, numerous experiments have examined the
timing, magnitude, and controlling processes for fission product
releases from the fuel, the primary system, and containment.
Today, the magnitude of the source term available for release in
an accident has been reduced significantly.
4-Control rooms were complex, poorly organized, and did not provide
important information.

Improve design of control room
Improve surveillance and instrumentation of critical
systems required to cool the reactor and stop the escape
of radio nuclides.
Control rooms in the TMI generation of plants weren't designed
with the needs of operators in mind. Craig Faust, one of the
control room operators during the event stated, "I would have
liked to have thrown away the alarm panel.
It wasn't giving us any useful information." The operators were
overwhelmed and unnerved from the "alarm avalanche."
Necessary information wasn't readily available in a convenient
and understandable form. After the event, important safety
system modifications were made to detect and mitigate
inadequate core cooling and post-accident conditions. The next
generation of reactors will have control rooms designed with
human factors in mind and with computer technology that
prioritizes the information operators receive.
5- The consequences of a nuclear accident were less than we thought.
A postulated "worst accident" happened--the TMI-2 core
melted. Yet, there was no "China syndrome." And in spite
of operator errors, there weren't thousands of casualties.
Similarly, the casualties from Chernobyl were largely
limited in number to first responders and, except for
seldom fatal thyroid cancers, far lower than what was
predicted. While these lessons have been learned, we must
not return to pre-TMI complacency.

TMI supervisors aril control roam operators confer in the Unit 2 control
room during the accident.

To simulate the accident
The TMI-2 accident provides a unique opportunity to assess the
capability of codes to simulate a severe accident on a full scale nuclear
power plant. The first two phases of TMI-2accident have been calculated
with ASTEC. The Phase 1 of the transient was characterized by loss of
primary coolant through the PORV until shutdown of all primary pumps.
The Phase 2started with core uncover and involved core heat up and
melting until core refold was initiated by restart of one primary pump.
The overall primary system behavior was well predicted by ASTEC
during both Phase1 and 2. The primary pressure history was well
reproduced (Fig.); it was just slightly underestimated towards the end of
Phase 2. Pressurizer level behavior, which played a key role in the
accident evolution, was very well simulated. Hot leg gas temperature
increase following core uncover and heat up in Phase 2 was reasonably
well predicted by ASTEC.The residual water level in the core at the end
of Phase 2 is in good agreement with TMI-2observations, as inferred
from bottom crust location in the central core ring.
TMI2 primary system pressure
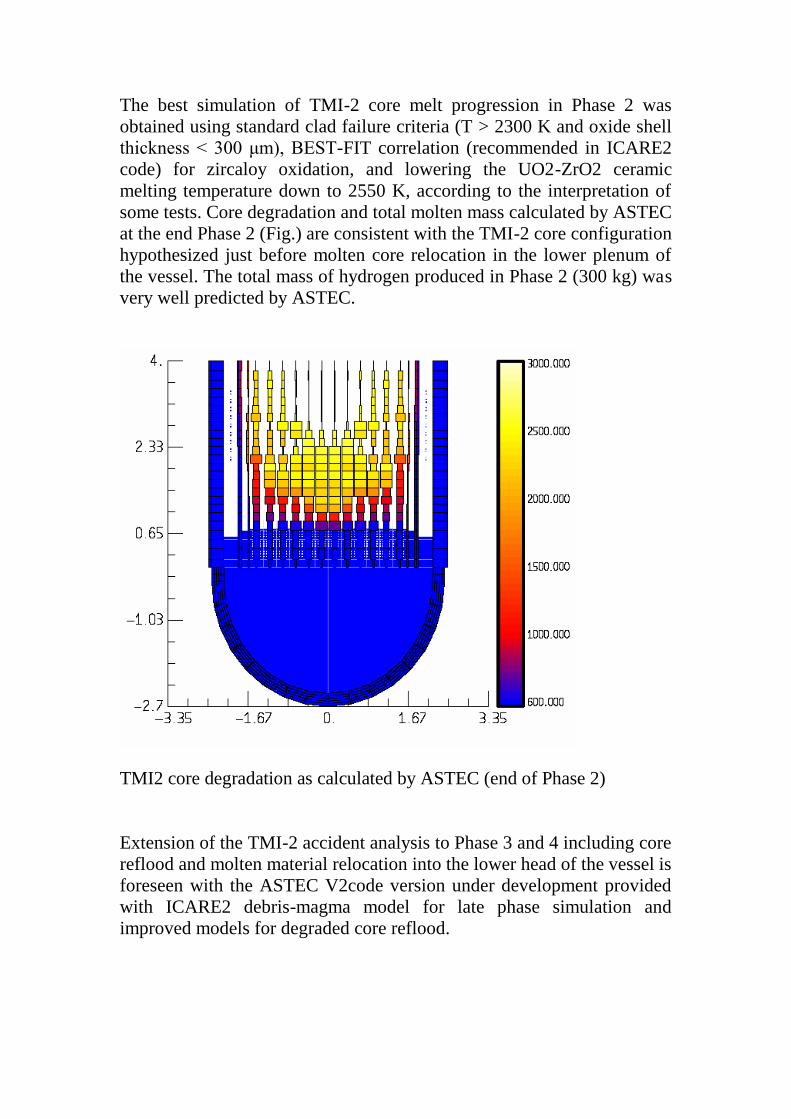
The best simulation of TMI-2 core melt progression in Phase 2 was
obtained using standard clad failure criteria (T > 2300 K and oxide shell
thickness < 300 μm), BEST-FIT correlation (recommended in ICARE2
code) for zircaloy oxidation, and lowering the UO2-ZrO2 ceramic
melting temperature down to 2550 K, according to the interpretation of
some tests. Core degradation and total molten mass calculated by ASTEC
at the end Phase 2 (Fig.) are consistent with the TMI-2 core configuration
hypothesized just before molten core relocation in the lower plenum of
the vessel. The total mass of hydrogen produced in Phase 2 (300 kg) was
very well predicted by ASTEC.
TMI2 core degradation as calculated by ASTEC (end of Phase 2)
Extension of the TMI-2 accident analysis to Phase 3 and 4 including core
reflood and molten material relocation into the lower head of the vessel is
foreseen with the ASTEC V2code version under development provided
with ICARE2 debris-magma model for late phase simulation and
improved models for degraded core reflood.

Final state:

Prompted Severe Accident Research
TMI-2 analysis
Early phase Late phase (corium in core) Late phase (corium in lower head)
ICARE/CATHARE Simulation (IRSN, M. Zabiego,2002)

Mitigation: denotes all measures taken to limit the radiological
consequences of an accident, including: limiting release into containment;
limiting release from the facility; reducing public radiation exposure by
sheltering, evacuation, off-site cleanup, etc. A narrower term, release
mitigation, refers only to measures taken to limit the release of
radioactive material from the facility.
The accident precursor program should have the following
characteristics:
1. The program should be owned by a recognized authority in the
industry and should be driven by consistent, robust goals and objectives
that address the needs of the future. Operational events should be
considered precursors to more serious events; from these precursors, the
program should provide insights into improving safety in the future.
2. The program must be supported by an infrastructure that can sustain it.
A system must be in place for gathering appropriate operational data and
providing access to data providers when more detailed information is
needed. Barriers to full and honest disclosure, such as proprietary
information and fear of repercussions, must be addressed. Also, industry
members must have incentives (either voluntary or by regulatory action)
for participating.
3. The program should provide a trending and tracking system to
correlate changes in industry design and practices with changes in the
occurrence and nature of observed precursors. The system should also be
able to distinguish between changes in trends that reflect real progress in
the field and changes attributable to maturing of the process and program.
The program could then provide excellent feedback to the industry on the
real impact of the precursor program.
4. Systems and methods should be sensitive enough to identify an
operational event as a precursor without generating too many “false
detects” of events of little interest. The event-reporting requirements and
event screening and selection criteria and processes must remain
consistent over time to support trending and analysis.
5. Risk assessment in the industry must be mature enough to instill
confidence that potential accident sequences have been identified and that
the models used to assess events are sufficient and only need changes that
reflect the configurations and operating practices of specific facilities.
Risk models must be updated to reflect improvements in facilities, but
these changes should be made in a way that does not change the level of
detail or the scope of coverage. This will facilitate trending and
comparison over the years.
6. Analysis should be performed on a continual basis by a consistent team
of analysts to ensure the timeliness and consistency of results.
Timeline
Date Event
March 1979 TMI operators are falsifying reactor leaks rates.
March 1979
TMI accident occurred. Containment coolant and unknown
amounts of radioactive contamination released into
environment.
April 1979 Containment steam vented to the atmosphere in order to
stabilize the core.
July 1980 Approximately 1591 TBq (43,000 curies) of krypton were
vented from the reactor building.
July 1980 The first manned entry into the reactor building took place.
Nov. 1980
An Advisory Panel for the Decontamination of TMI-2,
composed of citizens, scientists, and State and local officials,
held its first meeting in Harrisburg, PA.
July 1984 The reactor vessel head (top) was removed.
Oct. 1985 Defueling began.
July 1986 The off-site shipment of reactor core debris began.
Aug. 1988
GPU submitted a request for a proposal to amend the TMI-2
license to a "possession-only" license and to allow the
facility to enter long-term monitoring storage.
Jan. 1990 Defueling was completed.
July 1990 GPU submitted its funding plan for placing $229 million in
escrow for radiological decommissioning of the plant.
Jan. 1991 The evaporation of accident-generated water began.
April 1991 NRC published a notice of opportunity for a hearing on
GPU's request for a license amendment.
Feb. 1992 NRC issued a safety evaluation report and granted the
license amendment.
Aug. 1993 The processing of accident-generated water was completed
involving 2.23 million gallons.
Sept. 1993 NRC issued a possession-only license.
Sept. 1993 The Advisory Panel for Decontamination of TMI-2 held its
last meeting.
Dec. 1993 Post-Defueling Monitoring Storage began.
Oct. 2009 TMI-1 license extended from April 2014 until 2034 without
a public hearing

References:
G. Guillard et al., “ASTEC V1 code: DIVA physical modeling,”
Report ASTECV1/DOC/06-17 (2006).
http://www.nucleartourist.com/events/tmi.htm
http://www.efmr.org/edu/nuclear2009.pdf
http://en.wikipedia.org/wiki/Three_Mile_Island_accident#Lessons_learne
d