Embed Size (px)
Citation preview

Thromboembolic
Disease in Pregnancy –
The Silent DisorderHassan Nasrat FRCS, RCOG
Professor of Obstetric and Gynecology Fetal and Maternal MedicineFaculty of Medicine King Abdul Aziz university Jeddah – Saudi Arabia

Anticoagulation Is Highly Effective Therapy For Both Conditions
Tests Designed To Diagnose DVT Are Also Of Importance For The Diagnosis Of Acute PE.
Thromboembolic Disease (VTE) Refer to Deep Vein Thrombosis (DVT) And Pulmonary Embolism (PE)
Over 90 % Of Acute PE Are Emanating From Emboli Of The Lower Extremities.

Incidence And Incidence And EpidemiologyEpidemiology Incidence And Incidence And EpidemiologyEpidemiology
Pulmonary Embolism (PE) Is Responsible For
Approximately 150,000 To 200,000 Deaths
Per Year In The USA.
PE Remains The Most Common
Preventable Cause Of Hospital Death

The Incidence: 4 To 50 Times Higher In Pregnant Versus Non-pregnant Women (Age-adjusted)
Absolute Incidence: 1 In 500 To 2000 Pregnancies (0.025 To 0.10 Percent)
Pregnancy and Pregnancy and VTE VTE
Pregnancy and Pregnancy and VTE VTE

5
VTE in Pregnancy: A Major Cause of Maternal Death
VTE in Pregnancy: A Major Cause of Maternal Death
VTE Is The Leading Direct Cause Of
Maternal Death In Western Obstetric
Practice (11 cases = 27% Of Cases)
“Confidential enquiries into maternal death in UK”

VTE in Pregnancy: A Major CauseVenous Insufficiency
and VTE in Young Women
VTE in Pregnancy: A Major CauseVenous Insufficiency
and VTE in Young Women
71 women (mean age 35.5 years) with VTE
Assessed about 4 years after event – 52 DVT & 19 PTE– 79% mild / moderate post thrombotic
syndrome
Risk of VI after DVT: OR 10.9 (95% CI 4.2-28.0)
Risk of VI after PTE: OR 3.8 (95% CI 1.2-12.3)
McColl, Ellison, Greer et al 1999

PATHOGENESIS AND RISK PATHOGENESIS AND RISK FACTORSFACTORS
PATHOGENESIS AND RISK PATHOGENESIS AND RISK FACTORSFACTORS
Part IPart IPart IPart I
Antithrombotic Strategies Antithrombotic Strategies
Part Part IIII
Part Part IIII
Part Part IIIIII
Part Part IIIIIIUse of LMWHs in PregnancyUse of LMWHs in Pregnancy
Part Part IVIV
Part Part IVIVSummary and RecommendationsSummary and Recommendations
Thromboembolic Disease in Pregnancy – The Silent
Disorder

PATHOGENESIS AND RISK PATHOGENESIS AND RISK FACTORSFACTORS
PATHOGENESIS AND RISK PATHOGENESIS AND RISK FACTORSFACTORS
Part IPart IPart IPart I
Antithrombotic Strategies Antithrombotic Strategies
Part Part IIII
Part Part IIII
Part Part IIIIII
Part Part IIIIIIUse of LMWHs in PregnancyUse of LMWHs in Pregnancy
Part Part IVIV
Part Part IVIVSummary and RecommendationsSummary and Recommendations
Thromboembolic Disease in Pregnancy – The Silent
Disorder

PATHOGENESIS PATHOGENESIS AND PregnancyAND PregnancyPATHOGENESIS PATHOGENESIS AND PregnancyAND Pregnancy
Proper Blood Proper Blood FlowFlow
Balance Balance between between
coagulation coagulation and and
anticoagulatianticoagulation on
mechanism: mechanism:
Healthy Vessel Healthy Vessel wallswalls
Increases Increases coagulaticoagulati
ononReduces Reduces fibrinolysfibrinolys
isis
Increases Increases coagulaticoagulati
ononReduces Reduces fibrinolysfibrinolys
isis
Vessel Wall Vessel Wall Trauma At Trauma At deliverydelivery
Vessel Wall Vessel Wall Trauma At Trauma At deliverydelivery
> 30% > 30% reducreduction tion by 15 by 15 weekweek
ss> 60% > 60% reducreduction tion
by 36 by 36 weekweek
ss
> 30% > 30% reducreduction tion by 15 by 15 weekweek
ss> 60% > 60% reducreduction tion
by 36 by 36 weekweek
ss

A longitudinal Follow Up of 24 pregnant women with monthly Doppler ultrasound examinations found:
Progressive dilation of the deep veins of the legs.
Decreased flow velocity in the left common femoral vein and inferior vena cava that was most severe in the supine position.
The left lateral decubitus position significantly increased the velocity in both lower extremities
An ultrasound study of gestational and postural changes in the deep venous system of the leg in pregnancy. Macklon NS; BrJOG1997, 104]
Circulatory stasisCirculatory stasis

The Incidence Of Is Nearly Twice As Many Postpartum Than Antepartum Events.
Pelvic Vein DVT Is More Likely In Pregnancy.
More Common In The Left Than The Right Leg.
Antepartum VTE Is Roughly Equally Distributed Across Trimester’s.
Features of DVT in PregnancyFeatures of DVT in Pregnancy

Among 5451 Patients With Ultrasound-confirmed DVT.
1 % Had DVT Confined To The Pelvis.
While 12 % Of Pregnant And 11 % Of Post-partum Women Had Isolated Pelvic DVT

Conclusion -Conclusion - Part I Part IConclusion -Conclusion - Part I Part I
A Serious Disease
High Mortality Rate
Serious Morbidities
Appropriate Prophylactic Measures
Appropriate Diagnosis
Appropriate Treatement
VTE

PATHOGENESIS AND RISK PATHOGENESIS AND RISK FACTORSFACTORS
PATHOGENESIS AND RISK PATHOGENESIS AND RISK FACTORSFACTORS
Part IPart IPart IPart I
Antithrombotic Strategies Antithrombotic Strategies
Part Part IIII
Part Part IIII
Part Part IIIIII
Part Part IIIIIIUse of LMWHs in PregnancyUse of LMWHs in Pregnancy
Part Part IVIV
Part Part IVIVSummary and RecommendationsSummary and Recommendations
Thromboembolic Disease in Pregnancy – The Silent
Disorder

16
Antithrombotic Strategies
Antithrombotic Strategies
Vitamin K Antagonists
Un-Fractionated Heparin
Low-Molecular-Weight Heparins
Physical methods Vena Cava Filter

Mechanical ThromboprophylaxisMechanical Thromboprophylaxis

18
Antithrombotic Antithrombotic
Safety (Maternal and Fetal)
Effectiveness
Compliance
Cost

Safety (Maternal and Fetal)
Safety (Maternal and Fetal)
Two potential fetal complications of maternal anticoagulant therapy:
Teratogenicity
Bleeding

20
Vitamin K AntagonistsVitamin K Antagonists
Cross the placenta
Risk of maternal and fetal bleeding throughout gestation
Embryopathy: 6-12 wks of gestation - 4-5% Chondrodysplasia punctata Nasal (midface) hypoplasia Stippled epiphyses, short proximal limbs, short phalanges,
scoliosis
Central nervous system abnormalities Adverse fetal outcomes if Warfarin > 5 mg/day

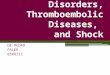
Warfarin EmbryopathyWarfarin Embryopathy
Embryopathy– chondrodysplasia punctata– midface hypoplasia– short proximal limbs– short phalanges– scoliosis Increased risk of low
IQ and neurological dysfunction (RR 7.6 for 2 or more defects)1
Maternal and foetal haemorrhage
X-ray: Wellesley D, et al. Br J Obstet Gynecol. 1998;105:805. 1Wesseling J, et al. Thromb Haemost. 2001;85:609-13.

UFH in pregnancy:no placental transfer but…
UFH in pregnancy:no placental transfer but…
AllergySkin Necrosis
Heparin-induced thrombocytopenia
Osteoporosis
Frequent monitoringFrequent monitoring

23
UF-Heparin Induced Osteoporosis
UF-Heparin Induced Osteoporosis
• >30% of women on prolonged UFH therapy will lose ≥10% of bone mass
• 2% symptomatic vertebral fractures on UFH thromboprophylaxis (Dahlman 1993)

24
Potential Advantages of LMWH over UFH
Potential Advantages of LMWH over UFH
Like UFH: Do not cross
the placenta Safe in nursing
mother
less monitoring Ease of administration Efficacy comparable Greater safety: allergy
and HIT, bleeding, and osteoporosis
less monitoring Ease of administration Efficacy comparable Greater safety: allergy
and HIT, bleeding, and osteoporosis
But Also

26
Safety & Effectiveness of LMWHSystematic Review of LMWH in
Pregnancy81 reports
2931
2777 11reports heart valvePul hypertension
2 reports duplicate 3 reports methodological
Most Common: Enoxaparin 1287, Dalteparin 789Least Common: Rivaparin 40, Tinzaparin 3.
Greer & Nelson Piercy Blood 2005

ComplicationsComplications Rate% 95% C.I.
Thrombosis VTE Arterial
1.370.860.50
0.97-1.870.55-1.280.28-0.84
Bleeding Antenatal PPH > 500ml Wound haematoma
1.980.430.940.61
1.50-2.570.22-0.750.61-1.370.36-0.98
Allergy 1.80 1.37-2.34
Thrombocytopaenia Platelet HIT
0.110.00
0.02-0.320.00-0.11
osteoporosis 0.04 < 0.01-0.20

Conclusion - Part IIConclusion - Part II
The Two Major Concerns with
Pharmacologic Antithrombotic Agents
Are (1) Teratogenicity And (2)
Bleeding.
Currently The evidence that LMWH Is
The Antithrombotic Agent Of Choice. It
Confer: Safety (Maternal And Fetal)
And Efficacy.

PATHOGENESIS AND RISK PATHOGENESIS AND RISK FACTORSFACTORS
PATHOGENESIS AND RISK PATHOGENESIS AND RISK FACTORSFACTORS
Part IPart IPart IPart I
Antithrombotic Strategies Antithrombotic Strategies
Part Part IIII
Part Part IIII
Part Part IIIIII
Part Part IIIIIIUse of LMWHs in PregnancyUse of LMWHs in Pregnancy
Part Part IVIV
Part Part IVIVSummary and RecommendationsSummary and Recommendations
Thromboembolic Disease in Pregnancy – The Silent
Disorder

Use of LMWHs in Use of LMWHs in PregnancyPregnancy
Use of LMWHs in Use of LMWHs in PregnancyPregnancy
Thromboprophylaxis
Treatment of VTE
Women with artificial heart valves
Fetal survival

8/13 (62%) women with Fatal Antenatal PTE died in the first Trimester.
8/14 (71%) of postpartum deaths followed vaginal delivery.
There is a need for guideline on thromboprophylaxis after normal delivery
Pregnancy and Pregnancy and VTE VTE
Pregnancy and Pregnancy and VTE VTE
“Confidential enquiries into maternal death in UK”

Risk Assessment In PregnancyRisk Assessment In Pregnancy
All women should undergo an All women should undergo an assessment of risk factors for VTE in assessment of risk factors for VTE in early pregnancy or before pregnancy. early pregnancy or before pregnancy.
It should be repeated if the woman is It should be repeated if the woman is admitted to hospital or develops other admitted to hospital or develops other intercurrent problems (Grade C)intercurrent problems (Grade C)
Women with VTE should be screened Women with VTE should be screened for inherited and acquired for inherited and acquired Thrombophilia ideally before Thrombophilia ideally before pregnancy (Grade B)pregnancy (Grade B)
Royal College of Obstetricians and Gynecologists Guidelines No 37 (January Royal College of Obstetricians and Gynecologists Guidelines No 37 (January 2004)2004)

Risk Factors for VTE in pregnancy and the Risk Factors for VTE in pregnancy and the PuerperiumPuerperium
Risk Factors for VTE in pregnancy and the Risk Factors for VTE in pregnancy and the PuerperiumPuerperium
RCOG guidelinesRCOG guidelines

Risk Factors in PregnancyRisk Factors in Pregnancy
Pregnancy: 10 fold increase in risk of VTE beginning from 1st trimester
ImmobilizationSurgery-CS
Prior VTE
Thrombophilia (Congenital and acquired)
Obesity And Advanced Age:All women dying from PTE following vaginal delivery were either obese or > 35 years of age. Only 1/10 deaths followed operative delivery.

35
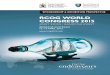
Role of Age and Delivery in the Incidence of Postpartum VTE
Macklon et al. Scott Med J 1996;41:83-6.
Role of Age and Delivery in the Incidence of Postpartum VTE
Macklon et al. Scott Med J 1996;41:83-6.
Vaginal delivery
Emergency CSElective CS
Rate
per
1,0
00 e
ven
ts
Age (years)

Obesity and DVTObesity and DVT

A retrospective cohort study of 159 women who had at least one pregnancy after an episode of VTE
6% VTE among women who did not receive antepartum thromboprophylaxis.
50 to 100 times higher than the overall incidence of antepartum VTE (0.6 to 1.3 of every 1000 deliveries)
Prior VTE and Prior VTE and pregnancypregnancy
Prior VTE and Prior VTE and pregnancypregnancy
Women with a history of VTE (with or without thrombophilia) are believed to have a higher risk of recurrence in subsequent pregnancies.)

Higher Risk Thrombophilia
Low Risk Thrombophilia
Antithrombin Deficiency.
Persistent Antiphospholipid Antibodies.
compound heterozygotes for prothrombin G20210A and factor V Leiden, and homozygotes for these conditions
e.g. Protein C, Protein S Deficiency, And Hyperhomocysteinemia
ThrombophiliaThrombophiliaThrombophiliaThrombophilia

Pharmacologic Thromboprophylaxis
Timing
Pharmacologic Thromboprophylaxis
Timing
PostpartumPostpartum
AntepartumAntepartum
Intrapartum- Cesarean SectionIntrapartum- Cesarean Section

Single prior episode of VTE plus a higher risk thrombophilia Single idiopathic episode of VTE who are not receiving long-term anticoagulants Multiple prior episodes of VTE Antithrombin deficiency Single prior episode of VTE that was related to pregnancy or estrogen use (e.g., contraceptives)
Single episode of VTE associated with a transient risk factor that is no longer present Single prior episode of VTE in a patient with thrombophilia that is not considered higher risk
Antepartum
Antepartum Thromboprophylaxis Should be AdministeredThromboprophylaxis Should be Administered
Thromboprophylaxis on Case by Case Basis:Thromboprophylaxis on Case by Case Basis:
The 2008 American College of Chest Physicians guidelines on VTE and pregnancy The 2008 American College of Chest Physicians guidelines on VTE and pregnancy

Postpartum Thromboprophylaxis Is Indicated For Women Who Have Had One Or More Episodes Of VTE Or Who Have Any Type Of Thrombophilia, Even Those That Are Not Considered Higher Risk
Postpartum
Postpartum
The 2008 American College of Chest Physicians guidelines on VTE and pregnancy The 2008 American College of Chest Physicians guidelines on VTE and pregnancy
Women who receive Epidural: LMWH may be initiated 4-6 hours after insertion or removal of the catheter
In High Risk women Postpartum Thromboprophylaxis should be continued for at least 6 weeks

For most postpartum women who are unwilling to receive subcutaneous injections, a Warfarin-based regimen, rather than no pharmacologic thromboprophylaxis (Grade 2B).
For most postpartum women who are willing to receive subcutaneous injections, a LMWH-based regimen, rather than an UFH- or Warfarin-based regimen (Grade 2B). thromboprophylaxis be continued for four to six weeks

Thromboprophylaxis Is NOT Recommended For Women Whose Only Risk Factors For VTE Are The Pregnancy And CS.
Intrapartum – Cesarean Section
Intrapartum – Cesarean Section
The 2008 American College of Chest Physicians guidelines on VTE and pregnancy The 2008 American College of Chest Physicians guidelines on VTE and pregnancy
Women Who Have Only One Additional Risk Factor For VTE Should Receive Either Pharmacological or Mechanical Thromboprophylaxis
Women who have multiple additional risk factors should receive Pharmacological Plus Mechanical Thromboprophylaxis

Antenatal throboprophylaxis should Antenatal throboprophylaxis should begin as early in pregnancy as practical.begin as early in pregnancy as practical.
Postpartum prophylaxis should begin Postpartum prophylaxis should begin as soon as possible after delivery. as soon as possible after delivery. (Grade B)(Grade B)
Low Molecular Weight Heparins are Low Molecular Weight Heparins are the agents of choice for antenatal the agents of choice for antenatal thromboprophylaxis. They are as thromboprophylaxis. They are as effective as and safer than effective as and safer than Unfractionated heparin in pregnancy. Unfractionated heparin in pregnancy. (Grade B)(Grade B)
Royal College of Royal College of Obstetricians and Obstetricians and
Gynecologists Guidelines Gynecologists Guidelines No 37 (January 2004)No 37 (January 2004)
Royal College of Royal College of Obstetricians and Obstetricians and
Gynecologists Guidelines Gynecologists Guidelines No 37 (January 2004)No 37 (January 2004)

RCOG guidelinesRCOG guidelines

Antenatal Prophylactic and Therapeutic Doses of LMWH
Antenatal Prophylactic and Therapeutic Doses of LMWH
BMI > 30 in early pregnancyBMI > 30 in early pregnancy
RCOG guidelinesRCOG guidelines

Use of LMWHs in Use of LMWHs in PregnancyPregnancy
Use of LMWHs in Use of LMWHs in PregnancyPregnancy
Thromboprophylaxis
Treatment of VTE
Women with artificial heart valves
Fetal survival

Two Ways to Reduce Maternal mortality from PE:
•by investigating women aggressively when they present with a clinical suspicion of deep vein thrombosis (DVT) or PE, and treating those with a diagnosis of venous thromboembolism (VTE)
•by prophylaxis of those who have an increased risk for DVT and/or PE.
Both approaches are problematic

The S&S Compatible With DVT And PE Are Common and Usually Nonthrombotic In Origin During Pregnancy.
Dilemmas in Clinical Diagnosis of DVT in pregnancy
The compressive effects of the gravid alter the interpretation and sensitivity of the tests.
Concern about performing procedures that expose the fetus to radiation
The Significance of Identifiable Laboratory Abnormality Associated With Thrombophilia And Its Management Remain Controversial.

Diagnosis Of DVT in Diagnosis Of DVT in PregnancyPregnancy
Diagnosis Of DVT in Diagnosis Of DVT in PregnancyPregnancy
High ProbabilityHigh Probability2 (1.8%)2 (1.8%)
113 Patients suspected PE113 Patients suspected PEVentilation Perfusion Lung Ventilation Perfusion Lung
ScanScanNormalNormal
83 (73%)83 (73%)Non DiagnosticNon Diagnostic
28 (25%) 28 (25%)
Hull et al Ann Int Med 1990, 112chan et Arch Int. Med. 2002, 162l
PregnantPregnant
Non-PregnantNon-Pregnant High ProbabilityHigh Probability10 - 30%10 - 30%
Diagnosis Of PE in PregnancyDiagnosis Of PE in PregnancyDiagnosis Of PE in PregnancyDiagnosis Of PE in Pregnancy
PregnantPregnant Non-PregnantNon-Pregnant
Clinical DVTClinical DVT < 10%< 10% > 25%> 25%

Diagnosis of VTE – Importance of Confirming the Diagnosis
Diagnosis of VTE – Importance of Confirming the Diagnosis
Long Term Treatment
Implication on Future pregnancy
Implications on Hormonal OC
Implications on HRT

Risk Factors For DVT
Diagnosis of VTE - Clinical Examination
Diagnosis of VTE - Clinical Examination
Non Invasive TestsNon Invasive Tests
Clinical Symptoms and signs
Serum D-DimerSerum D-Dimer::
Invasive Test: Contrast Invasive Test: Contrast VenographyVenography

Diagnosis of VTE - Serum D-dimer
Diagnosis of VTE - Serum D-dimer
A product of the degradation of fibrin by plasmin Has A High Sensitivity But Rather Low Specificity.
Elevations In D-dimer Are Found In: Uncomplicated Pregnancy. Increase With Gestational Age And Peaking At The Time Of Delivery And In The Early Postpartum Period.

Compression Ultrasonography Compression Ultrasonography (Doppler ultrasound)(Doppler ultrasound)
Compression Ultrasonography Compression Ultrasonography (Doppler ultrasound)(Doppler ultrasound)
Accuracy: Sensitivity And Specificity Of 100 And 99 Percent, Respectively.
Limitation:
Does Not Detect Isolated Thrombi In The Iliac Vein Or The Femoral Vein Within The Adductor Canal.
Approximately 2 % With Initially Negative Us Develop A Positive Study When Retested Seven Days Later.
False Positive Test Patients With Pelvic Neoplasms Or Abscesses A systematic review of the accuracy of ultrasound in the diagnosis of deep venous thrombosis in asymptomatic patients. Kassai B; et al, Thromb Haemost 2004; 91

Abnormal change in diameter during the Valsalva Abnormal change in diameter during the Valsalva maneuver: maneuver:
Compression Ultrasonography Compression Ultrasonography (Doppler ultrasound)(Doppler ultrasound)
Compression Ultrasonography Compression Ultrasonography (Doppler ultrasound)(Doppler ultrasound)
Abnormal compressibility of the Abnormal compressibility of the
veinvein: :
Abnormal Doppler color flowAbnormal Doppler color flow: :
The presence of an echogenic bandThe presence of an echogenic band::

Magnetic resonance imaging Magnetic resonance imaging (MRI)(MRI)
Magnetic resonance imaging Magnetic resonance imaging (MRI)(MRI)
Can Detect Both Thigh And Pelvic Vein DVT With A Sensitivity That Approaches 100 Percent In The Non-pregnant Population.

Is the gold standard for the diagnosis of lower extremity DVT
Diagnosis of VTE - Contrast Venography
Diagnosis of VTE - Contrast Venography
Reserved For Situations If Non Invasive Studies Are:
Not Feasible Equivocal,
Discordant With A Strong Clinical Impression
Requires Ionizing Radiation And Percutaneous Requires Ionizing Radiation And Percutaneous Veins Cannulation Veins Cannulation
Fetal Radiation (<500 Mcgy) With Abdominal-Fetal Radiation (<500 Mcgy) With Abdominal-pelvic Shielding, Shielding Renders The Test pelvic Shielding, Shielding Renders The Test Relatively Insensitive To Isolated Iliofemoral Relatively Insensitive To Isolated Iliofemoral Thrombosis.Thrombosis.

Diagnostic algorithm for deep venous thrombosisDiagnostic algorithm for deep venous thrombosis

PULMONARY EMBOLISMPULMONARY EMBOLISM PULMONARY EMBOLISMPULMONARY EMBOLISM
In Many Cases Of Proximal DVT, Silent PE Has Already Occurred By The Time That The Patient Is Seen (Meignan M; Et Al Arch Intern Med 2000 Jan 24).
Thus negative studies for DVT are not definitive In unselected population less that 30% of patients with PE have radiologic evidence of DVT

PULMONARY EMBOLISMPULMONARY EMBOLISM PULMONARY EMBOLISMPULMONARY EMBOLISM
Because the treatments for DVT and submassive PE are identical, documentation of a DVT is sufficient to terminate the diagnostic evaluation and institute therapy.

Pulmonary Embolus - Pulmonary Embolus - DiagnosisDiagnosisPulmonary Embolus - Pulmonary Embolus - DiagnosisDiagnosis
Clinical Signs and SymptomsTachypnea (>20 breaths per minute) and tachycardia (>100 bpm) are present in 90 percent of patients with acute PEPresyncope and syncope are rarer symptoms and indicate a massive embolus
Scoring Scoring systemssystemsScoring Scoring systemssystemsRISK OR SIGN POINT
S
Clinical signs and symptoms of DVT
+3
Alternative diagnosis deemed less likely than PE
+3
Heart rate > 100bpm + 1.5
Immobilization or surgery in previous 4 weeks
+ 1.5
Prior VTE + 1.5
Hemoptysis + 1
Active Cancer + 1
““PE unlikely” PE unlikely” score is ≤4score is ≤4
““PE unlikely” PE unlikely” score is ≤4score is ≤4
““PE likely” PE likely” score > 4score > 4
““PE likely” PE likely” score > 4score > 4
2/3 of Patients
N Engl J Med 349:1247, 2003

Nonspecific StudiesNonspecific StudiesNonspecific StudiesNonspecific Studies•electrocardiographic changes
•Chest Radiograph
Pulmonary Arteriography
Ventilation-Perfusion Scanning
Spiral Computed Tomographic Pulmonary Angiography (Spiral Computed Tomography)
Magnetic Resonance Angiography
Pulmonary Embolus - Pulmonary Embolus - Diagnostic TestsDiagnostic TestsPulmonary Embolus - Pulmonary Embolus - Diagnostic TestsDiagnostic Tests
Specific Studies Specific Studies Specific Studies Specific Studies
As with evaluation of DVT, D-dimer is a very sensitive, but not specific, test for PE
D-Dimer AssaysD-Dimer AssaysD-Dimer AssaysD-Dimer Assays

Diagnostic algorithm for PEDiagnostic algorithm for PE

Radiation Exposure in PregnancyRadiation Exposure in PregnancyRadiation Exposure in PregnancyRadiation Exposure in Pregnancy
Exposure to < 5 rads has not been associated with
increases in pregnancy loss or fetal anomalies.
However exposure to ionizing radiation doses
above 1 rad increase risk of childhood leukemia from
1/3000 baseline to 1/2000
A combination of chest radiograph, V/Q scan and
pulmonary angiography exposes the fetus to less than
0.5 rads. The American College of Obstetricians and Gynecologists

Investigations Fetal Exposure RADS
Chest X-ray <0.01
Limited venography (shielded) <0.05
Unilat venography without shield 0.31
Perfusion lung scan 0.006 – 0.012
Ventilation lung scan Xenon-133 0.001- 0.019
Pul. Angiography via Brachial 0.05
Pul. Angiography via Femoral 0.22 – 0.37
Spiral CT 0.013
Estimated radiationEstimated radiation

Diagnosis and Treatment of VTEDiagnosis and Treatment of VTE
High Index Of Clinical Suspicion
High Risk Index
Initiate Therapy Diagnostic Studies
LOW Risk Index
Diagnostic Studies
Initiate Therapy

Use of LMWHs in Use of LMWHs in PregnancyPregnancy
Use of LMWHs in Use of LMWHs in PregnancyPregnancy
Thromboprophylaxis
Treatment of VTE
Women with artificial heart valves
Fetal survival

Anticoagulation of pregnant women with mechanical Anticoagulation of pregnant women with mechanical heart valves: a systematic review of the literature. heart valves: a systematic review of the literature.
Chan, et al, Arch Intern Med 2000;160.Chan, et al, Arch Intern Med 2000;160.
Anticoagulation of pregnant women with mechanical Anticoagulation of pregnant women with mechanical heart valves: a systematic review of the literature. heart valves: a systematic review of the literature.
Chan, et al, Arch Intern Med 2000;160.Chan, et al, Arch Intern Med 2000;160.
Pregnant women with prosthetic heart valves
pose a problem because of the lack of reliable
RCT
The overview consisted of prospective and
retrospective cohort studies.
Women with artificial heart Women with artificial heart valvesvalves
Women with artificial heart Women with artificial heart valvesvalves

(1)use of VKAs throughout pregnancy (in widespread use in Europe)
(2)replacement of VKAs with UFH from 6 to 12 weeks, and
(3) UFH use throughout pregnancy.
Outcomes Measures: pregnancy loss, fetopathic effects (including Warfarin embryopathy), maternal bleeding, thromboembolic complications, and death.
Three commonly used approaches:
Anticoagulation of pregnant women with mechanical heart valves: a Anticoagulation of pregnant women with mechanical heart valves: a systematic review of the literature. systematic review of the literature. Chan, et al, Arch Intern Med 2000;160.Chan, et al, Arch Intern Med 2000;160.Anticoagulation of pregnant women with mechanical heart valves: a Anticoagulation of pregnant women with mechanical heart valves: a
systematic review of the literature. systematic review of the literature. Chan, et al, Arch Intern Med 2000;160.Chan, et al, Arch Intern Med 2000;160.

Warfarin embryopathy occurred in 6.4% if used throughout pregnancy
The substitution of heparin at or prior to 6 weeks eliminate this risk .
The Overall rate of fetal wastage were similar in all groups.
The overall maternal mortality was 2.9 %.
Major bleeding: occurred in 2.5% of all pregnancies
Use of VKAS throughout was associated with the lowest risk of valve thrombosis/systemic embolism (3.9%)
The reported high rates of Thromboembolism with UFH The reported high rates of Thromboembolism with UFH might be explained by inadequate dosing and/or the use might be explained by inadequate dosing and/or the use of an inappropriate target therapeutic range.of an inappropriate target therapeutic range.
The reported high rates of Thromboembolism with UFH The reported high rates of Thromboembolism with UFH might be explained by inadequate dosing and/or the use might be explained by inadequate dosing and/or the use of an inappropriate target therapeutic range.of an inappropriate target therapeutic range.
ResultsResultsResultsResults

VKAs are more efficacious than UFH for thromboembolic prophylaxis of women with mechanical heart valves in pregnancy; however,
However it increases the risk of embryopathy(6.3%)
Substituting VKAs with heparin between 6 weeks and 12 weeks reduces the risk of fetopathic effects but possibly subjects the woman to an increased risk of thromboembolic complications.
ConclusionConclusionConclusionConclusion

Adjusted-dose bid LMWH throughout pregnancy in doses adjusted according to weight (Grade 1C),
Aggressive adjusted-dose UFH throughout pregnancy, (Grade 1C)
UFH or LMWH (as above) until the thirteenth week, change to Warfarin until the middle of the third trimester, and then restart UFH or LMWH (Grade 1C)
Long-term anticoagulants should be resumed postpartum with all regimens.
In women with prosthetic heart valves at high risk, suggest the addition of low-dose aspirin, 75 to 162 mg/d (Grade 1C)
RecommendationsRecommendationsRecommendationsRecommendations
The 2008 American College of Chest Physicians guidelines on VTE and pregnancy The 2008 American College of Chest Physicians guidelines on VTE and pregnancy

Women Requiring Long-term Vitamin K Antagonist Therapy Who Are Attempting Pregnancy,
Should Perform Frequent Pregnancy Tests And Substituting Unfractionated Heparin (UFH) Or Low Molecular Weight Heparin (LMWH) For Warfarin When Pregnancy Is Achieved (Grade 2C)
Women Requiring Long-term Vitamin Women Requiring Long-term Vitamin K Antagonist Therapy K Antagonist Therapy
Women Requiring Long-term Vitamin Women Requiring Long-term Vitamin K Antagonist Therapy K Antagonist Therapy

Use of LMWHs in Use of LMWHs in PregnancyPregnancy
Use of LMWHs in Use of LMWHs in PregnancyPregnancy
Thromboprophylaxis
Treatment of VTE
Women with artificial heart valves
Fetal survival

MATERNAL THROMBOPHILIAS ARE ASSOCIATED WITH: INCLUDING FETAL LOSS IUGR PREECLAMPSIA ABRUPTION INTRAUTERINE DEATH.
Fetal survivalThrombophilia and Pregnancy
Complications
Fetal survivalThrombophilia and Pregnancy
Complications
KUPFERMINC ET AL NEJM, 1999, 341

Women With Recurrent Pregnancy Loss ( > Miscarriages) And Women With Prior Severe Or Recurrent PET, Abruptions, Or Otherwise Unexplained IUFD, Should Receive Screening For Congenital Thrombophilia And APLAS (Grade 2C).
Women With APLAS And A History Of Multiple (>) Early Pregnancy Losses Or One Or More Late Pregnancy Losses, PET, IUGR, Or Abruption, Antepartum Aspirin Plus Minidose Or Moderate-dose UFH Or Prophylactic LMWH May Be Administered (Grade 2B).

For women with a congenital thrombophilic
deficit and recurrent miscarriages, a second-
trimester or later loss, severe or recurrent
PET, or abruption, low-dose aspirin therapy
plus either minidose heparin or prophylactic
LMWH therapy (Grade 2C).
In addition to postpartum anticoagulants
should be administered to these women (Grade
2C)

Patients with APLAS and NO PRIOR VTE OR
PREGNANCY LOSS should be considered to
have an increased risk for the development of
venous thrombosis and, perhaps, pregnancy
loss.
One of the following approaches for these
women: Surveillance. Minidose heparin, prophylactic LMWH, and/or low-dose aspirin, 75 to 162 mg/d (all Grade 2C).

Key PointsKey Points
Complication And Pathogenesis:
VTE Is A Leading Cause Of Mortality And Serious Long Term Morbidity Among Pregnant Women
VTE Is A Leading Cause Of Mortality And Serious Long Term Morbidity Among Pregnant Women
Pregnancy Is A Leading Risk Factor For VTE Attention Should Be Paid To The Presence And / Or Development Of Additional Risk Factor (S)
Pregnancy Is A Leading Risk Factor For VTE Attention Should Be Paid To The Presence And / Or Development Of Additional Risk Factor (S)

Key Points (cont.)Key Points (cont.)
Diagnosis:
D-dimer because of its high negative predictive value given the higher rate of false-positive D-dimer results in pregnancy.
Venous compression US has sensitivity of 90 – 100 % for proximal vein thrombosis.
Spiral computed tomographic pulmonary angiography (spiral CT) is now the preferred screening and diagnostic modality for PE
D-dimer because of its high negative predictive value given the higher rate of false-positive D-dimer results in pregnancy.
Venous compression US has sensitivity of 90 – 100 % for proximal vein thrombosis.
Spiral computed tomographic pulmonary angiography (spiral CT) is now the preferred screening and diagnostic modality for PE
The diagnosis of either DVT or PE in pregnancy is a challenging.
the PPV of a test increase with the prevalence of the disease to be detected The Key To Accurate Diagnosis Of Either DVT Or PE Is Initial Risk Assessment
The diagnosis of either DVT or PE in pregnancy is a challenging.
the PPV of a test increase with the prevalence of the disease to be detected The Key To Accurate Diagnosis Of Either DVT Or PE Is Initial Risk Assessment

LMWH is as effective but safer than Unfractionated heparin
Further Studies are needed for defining:
oAppropriate / individualized Dose.
oDuration of prophylaxis / Treatment
oThe High risk groups who likely to get the most benefit
Key Points (cont.)Key Points (cont.)
Prophylaxis and Treatment:

ThanksThanksFor Great AudienceFor Great Audience