Embed Size (px)
Citation preview

Thrombosis Management in Cardiology:The relevance of direct Factor Xa inhibition
Prevention and Treatment of Venous Thromboembolism
Alexander G G TurpieProfessor of MedicineMcMaster University
Hamilton ONCanada

22
1.Goldhaber SZ Am Coll Cardiol. 1992;19:246-247 2.Heit JA,et al ASH Annual Meeting Abstracts 2005;106:9103.Cohen AT, et al. Thromb Haemost 2007;98:756−644.Cohen AT. Poster ISPOR 8th, 2005
3rd most common cardiovascular disease world-wide after ischaemic heart disease and stroke1
Causes ~300,000 deaths in the United States and over 500,000 deaths in Europe per year2,3
In the EU, more than twice as many people die from VTE than from AIDS, breast cancer, prostate cancer and transportation accidents combined3
3.1 billion Euros per year total estimated costs for VTE-associated care4
VTE is a Serious Disease that Affects Hundreds of Thousands People each Year

3
Known Consequences of VTE
Increased future risk of recurrent VTE
3-10% recurrent VTE at 1-year1
Chronic post-thrombotic syndrome (PTS)
Fatal Pulmonary Embolism (PE)
Chronic thromboembolic pulmonary hypertension
Markedly increased risk of disability and reduced quality of life for the patient
Costs of investigating and treating add considerable healthcare costs1,3
3
1. Kearon C. Circulation. 2003;107(23 Suppl 1):I22I30. 2. Cohen AT, et al. Thromb Haemost 2007;98:756–764.3. Ginsberg JS, et al. Arch Intern Med. 2000;160:669672.
Pulmonary embolus
Deep Venous Thromboembolism (DVT)

4
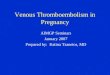
PTS is a Relatively Common but Serious Complication
PTS occurs in nearly one-third of pts within 5 years of initial DVT1
DVT-induced valvular incompetence leads to lower limb hypertension2
PTS is characterized by3: Pain Odema Hyperpigmentation Eczema Varicose collateral veins
Severe PTS can lead to intractable, painful venous leg ulcers requiring ongoing nursing and medical care4
4
© Diepgen TL, et al. Dermatology Online Atlas (Reprinted with permission).
1. Prandoni P, et al. Ann Intern Med. 1996;125:1–7.2. Kahn SR, et al. Arch Intern Med. 2004;164:17–26.3. Kahn SR. J Thromb Thrombolysis. 2006; 21(1) 41-48.4. Kahn SR, et al. J Gen Intern Med. 2000;15:425–429.

66
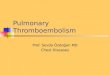
Prothrombin
FibrinFibrinogen
Thrombin Dabigatranand others
Factor Xa RivaroxabanApixaban, Endoxaban and others
Factor X
Prothrombinase-complex
PhospholipidsFactor Va – Factor XaCa2+
Factor IX Factor IXaFactor VIIaTissue factorPhospholipidsCa2+
Factor IXaFactor VIIIaPhospholipidsCa2+
Initiationphase
Propagation phase = thrombin-generation
phase
Thrombinphase
New Drugs in Phase III Development Directly Targeting Coagulation Factors
Adapted from: Kubitza & Haas. Expert Opin Investig Drugs 2006

8
1. Eriksson et al. New Engl J Med 2008; 2. Kakkar et al. Lancet 2008; 3. Lassen et al. New Engl J Med 2008; 4. Turpie et al. Lancet 2009
Enoxaparin
Rivaroxaban 10 mg odMandatory
bilateralvenography
Mandatorybilateral
venographyR
6–8 hours post-surgery in all RECORD studies
Day 1
Double blind
Last dose, daybefore venography
StudyRivaroxaban therapy
Dose DurationEnoxaparin therapy Dose Duration
THR 10 mg od 5 weeks 40 mg od 5 weeks1
THR 10 mg od 5 weeks 40 mg od 2 weeks*2
TKR 10 mg od 2 weeks 40 mg od 2 weeks3
TKR 10 mg od 2 weeks 30 mg bid 2 weeks4
*Followed by oral placebo for 3 weeks
RECORD1–3: Evening before surgery
RECORD4: 12–24 hours post-surgery
RECORD Phase III Programme: Study Design
SURGERY
FOLLOW
UP
8

9
Pooled analysis: Time points
Rivaroxaban Follow-upEnoxaparin Follow-up
Rivaroxaban
Enoxaparin Follow-up
Follow-up
Rivaroxaban
Follow up by: 30–35 days
after last dose
Follow up by: 30–35 days
after last dose
Day 12 (10–14)
Day 1 Day 35(31–39)
Enoxaparin Placebo
Follow-up
Day 12 (10–14)
Hip1
Hip2
Knee4
Total study duration
pool
Day 12±2 active treatment pool
Total treatment duration pool
Rivaroxaban
Rivaroxaban
Enoxaparin Follow-up
Follow-up
Follow-up
Knee3
91.Eriksson et al. New Engl J Med 2008; 2.Kakkar et al. Lancet 2008; 3.Lassen et al. New Engl J Med 2008; 4. Turpie et al. Lancet 2009

10
RECORD1–4* Pooled Analysis: Summary
1.3%
0.6%0.4%
RRR 58%‡
p<0.001
p=0.076 (NS)
Endpoints in total treatment
duration pool#
0.2%
p-values analysed using a Cox regression model; safety population, n=12,383; *RECORD2 compared extended-duration (35±4 days) rivaroxaban with short-duration (12±2 days) enoxaparin; #5 weeks in RECORD1 and RECORD2 (includes placebo-controlled period in RECORD2) and 2 weeks in RECORD3 and RECORD4; ‡Homogeneity test, p=0.313; ¶Homogeneity test, p=0.431
0
0.5
1.0
1.5
2.0
2.5
Major bleedingSymptomatic VTEand all-cause mortality
0.5%
0.3%0.2%
RRR 52%¶
p=0.001
p=0.175 (NS)
Endpoints in day 12±2 active
treatment pool
1.0%
Major bleedingSymptomatic VTEand all-cause mortality
Enoxaparin regimens
Rivaroxaban regimens
Inci
den
ce (
%)
10
Turpie et al. Oral presentation at the XXII Congress of the ISTH. Boston, MA, USA. July 11–16, 2009.
Turpie et al. Blood 2008;112(11):Abstract 36.

11
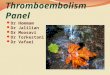
RECORD1–4*: PE and all-cause mortality#
HR = 0.61(95% CI: 0.39–0.98)p=0.039
0
0.5
1.0
2.0
1.5
Da
y 1
= d
ay
of
su
rge
ry
47 events
29 events
Enoxaparin regimens
Rivaroxaban regimens
Time-to-event relative to surgery (days)
0 10 20 30 40 50 60 70
Cu
mu
lati
ve e
ven
t ra
te (
%)
*RECORD2 compared extended-duration (35±4 days) rivaroxaban with short-duration (12±2 days) enoxaparin #Post-hoc analysis; safety population, n=12,383
Turpie et al. Blood (ASH Annual Meeting Abstracts) 200811
Total study duration pool

12
RECORD1–4*: Composite of Death, MI, Stroke, Symptomatic VTE, and Major Bleeding#
*RECORD2 compared extended-duration (35±4 days) rivaroxaban with short-duration (12±2 days) enoxaparin #Post-hoc analysis; safety population, n=12,383
HR = 0.69(95% CI: 0.53–0.89)p=0.004
Total study duration poolC
um
ula
tive
eve
nt
rate
(%
)
0 10 20 30 40 50 60 70
0.5
1.0
2.0
1.5
2.5
3.0
Da
y 1
= d
ay
of
su
rge
ry139 events
96 events
Time-to-event relative to surgery (days)
Enoxaparin regimens
Rivaroxaban regimens
0
12
Turpie et al. Oral presentation at the XXII Congress of the ISTH. Boston, MA, USA. July 11–16, 2009.
Turpie et al. Blood 2008;112(11):Abstract 36.

VTE prevention in hospitalized medically ill patients
http://clinicaltrials.gov/ct2/show/NCT00571649?term=rivaroxaban&rank=9

MAGELLAN: Study Design
Enoxaparin 40 mg once daily for 10 days
Patients hospitalized
for acute medical
illness with decreased
level of mobility
Rivaroxaban 10 mg once daily for 35 days
Day 1
R
N = 8000
Fo
llo
w-u
p
Day 10 Day 90Day 35
En
d o
f tr
ea
tme
nt
Oral placebofor 25 days
Randomization
Primary efficacy endpoint Composite of asymptomatic proximal DVT detected by bilateral ultrasound, symptomatic DVT,
non-fatal PE and VTE-related death.
Primary safety endpoint Major bleeding and clinically relevant non-major bleeding

15
VTE – Phases of the Disease and Conventional Treatment with Anticoagulants
Phases of the disease
Long-term
Types and intensity of conventional anticoagulation treatment
Initial, parenteral therapeutic dose anticoagulation
Early maintenance anticoagulation / Secondary prevention
Long-term maintenance anti-coagulation / Secondary prevention
UFH, LMWH, Fondaparinux
VKA INR 2.0-3.0
VKA INR 2.0-3.0 or 1.5-2.0
At least 5 days
At least 3 months
> 3 months / years/ indefinite**With re-assessment of the individual benefit–risk at periodic intervals.Kearon C, et al. Chest. 2008;133;454-545.
ESC Textbook of Cardiovascular Medicin 2nd Edition 2009; Chapter 37 Schellong S, Bounameaux H, Büller HR pp 1348-1349
Intermediate
Acute

16
VTE Treatment: Clinical Studies1 Phase II Phase III
Rivaroxaban Oral direct FXa inhibitor
EINSTEIN DVTRivaroxaban vs LMWH/UFH followed by VKA1
ODIXa DVTRivaroxaban vsenoxaparin followed by VKA2
EINSTEIN DVT/PE4
Rivaroxaban for 3, 6 or 12 months vs enoxaparin for > 5 days followed by VKA for 3, 6, or 12 months EINSTEIN EXT4
Pre-treatment with rivaroxaban or VKA for 6 or 12 months followed by rivaroxaban or placebo for 6 or 12 months
Dabigatran Oral direct thrombin inhibitor
RE-COVER4 & RE-COVER II4
5-10 days pre-treatment with LMWH bridging to dabigatran or VKA for 6 months RE-MEDY4
3-6 months treatment with approved anticoagulant; switch to dabigatran or warfarin RE-SONATE4
6-18 months VKA treatment followed by 6 months dabigatran or placebo
ApixabanOral direct FXa inhibitor
Botticelli-DVTApixaban vs LMWH or fondaparinux followed by VKA3
AMPLIFY4
Apixaban 10 mg bid followed by 5 mg bid for 6 months vs enoxaparin followed by warfarinAMPLIFY-EXT4
Apixaban 2.5 mg bid or 5 mg bid for extended 12 months period vs placebo
1. Büller HR et al. Blood 2008;112:2242–22472. Agnelli GA et al. Circulation 2007;116:180–187
3. Büller HR et al. J Thromb Haem 2008;6:1313–13184. www.clinicaltrials.gov

17
Dabigatran Study Programme
Confirmed symptomatic DVT or PE completing
6 to18 months VKA
Dabigatran Etexilate 150 mg BID
Placebo/warfarin
Day 1
R
N=1448
RE-SONATE/REMEDYTreatment period of 6 months
Symptomatic VTE
RE-COVER
R
N=2,564
ParenteralAnticoagulant
Day 1 Day 5-10
VKA target INR 2.5 (INR range 2–
3)
Symptomatic VTE
RE-COVER II
RE-COVER Pre-defined treatment period of 6 months
N=2,554
Dabigatran Etexilate 150 mg BID
17
1. RECOVER Study Information. Trial ID: NCT00291330 Available at http://clinicaltrial.gov/ct2/show/NCT00291330 Accessed 15 November 20092. RECOVER Study Information. Trial ID: NCT00680186 Available at http://clinicaltrial.gov/ct2/show/NCT00680186 Accessed 15 November 2009
3. RESONATE Study Information. Trial ID: NCT00558259 Available at http://clinicaltrial.gov/ct2/show/NCT00558259. Accessed 15 November 2009
ParenteralAnticoagulant

18
Events Dabigatran (n=1274) Warfarin (n=1265)Hazard ratios and
confidence intervals
Recurrent VTE (%) 30 (2.4) 27 (2.2)
Risk difference = 0.4% 95% CI; -0.8 to 1.5 p<0.0001 for prespecified non-inferiority
Recurrent VTE to the end of follow-up period (%)
34 (2.7) 32 (2.5)HR = 1 .05
95% CI; 0.065 to 1.70
Major bleeding (%) 20 (1.6) 24 (1.9)HR = 0.82
95% CI; 0.45 to 1.48
Any bleeding (%) 207 (16.2) 280 (22.1)HR = 0.71
95% CI; 0.59 to 0.85
RE-COVER: Study Results
Source – ASH 2009 Abstract

19
Rivaroxaban: VTE Treatment Studies
Phase II Phase III
Finished ODIXa-DVT EINSTEIN-DVT
EINSTEIN EXT
Ongoing EINSTEIN DVT EINSTEIN PE
http://clinicaltrials.gov19

2020
Day 1 Days 5–7 Day 21 Day 84 Day 114
ODIXa-DVT1
R
Enoxaparin(1 mg/kg)
VKA
10 mg bid20 mg bid
40 mg od30 mg bid
DOUBLE BLIND
OPEN LABEL
613 patients
randomized
INR 2–3
Rivaroxaban CC
US
FO
LLO
W-
UP
CCUS+PLS
CC
US
and
P
LS
EINSTEIN-DVT2
Rivaroxaban
CUS+ PLS R
LMWH/heparin
VKA
20 mg od30 mg od40 mg od C
US
and
P
LS
FO
LLO
W-
UPDOUBLE BLIND
OPEN LABEL
543 patients
randomized
INR 2–3
Day 1 Days 5–7 Day 21 Day 84 Day 114
Phase II Study Designs: ODIXa-DVT and EINSTEIN-DVT
Agnelli et al. Circulation 2007; Büller et al. Blood 2008

21
Phase II: ODIXa-DVT and EINSTEIN-DVT: Efficacy Outcome1,2
21
ODIXa-DVT1: Rivaroxaban showed similar efficacy to standard therapy
Rivaroxaban total daily dose (mg)LMWH/VKA
Ra
te o
f th
rom
bu
s r
eg
res
sio
n
wit
ho
ut
rec
urr
en
t V
TE
(%
) 80
70
60
50
40
30
20
10
0
6040200
bid rivaroxaban dosesod rivaroxaban dose
EINSTEIN-DVT2: Rivaroxaban showed similar efficacy to standard therapy
Ra
te o
f d
ete
rio
rati
on
(%
)
Rivaroxaban total daily dose (mg)LMWH/VKA10 30 40
201816141210 8 6 4 2 0
20
Recurrent DVT or PE, VTE-related death, and deterioration in CUS or PLS
Agnelli et al (ESC Annual Meeting, Poster presentation) 2006; Buller et al (ESC Annual Meeting, Oral Presentation) 2006: Agnelli et al. Circulation 2007; Büller et al. Blood 2008

22
EINSTEIN Phase III: Study Designs
Confirmed symptomatic DVT or PE completing 6 or 12 months of
rivaroxaban or VKA
Rivaroxaban 20 mg od
Placebo
Day 1
R
N=1,147
EINSTEIN EXT:Treatment period of 6 or 12 months
30
-da
y o
bs
erv
ati
on
p
eri
od
15 mg bid
Objectively confirmed DVT
without symptomatic PE
R
N=3,465 Rivaroxaban
Day 1 Day 21
Enoxaparin 1.0 mg/kg bid for at least 5 days, plus
VKA to start <48 hrs, target INR 2.5 (INR range 2–3)
Objectively confirmed PE
with or without symptomatic
DVT
EINSTEIN DVT/PE:Pre-defined treatment period of 3, 6, or 12 months
20 mg od
N=3,300
30
-da
y o
bs
erv
ati
on
p
eri
od
Rivaroxaban
22EINSTEIN DVT, PE, Extension Evaluation Study Information available at: http://clinicaltrials.gov. Accessed 15 November 2009

23
Primary and Secondary Outcome Measures of EINSTEIN DVT and EINSTEIN PE Evaluation
Primary outcome measures1,2
Symptomatic recurrent VTE, i.e., the composite of (recurrent) DVT or fatal or non-fatal PE
Principal safety outcome1,2
Combination of major and clinically relevant non-major bleeding
Secondary outcome measures1,2
All-cause mortality Vascular events
EINSTEIN DVT, PE Evaluation Study Information available at http://clinicaltrials.gov, Accessed 15 November 2009.23

Study design
Confirmed symptomatic DVT or PE
completing
6 or 12 months of rivaroxaban or
VKA in EINSTEIN VTE program
Rivaroxaban 20 mg od
PlaceboDay 1
R
N=1,197
Treatment period of 6 or 12 months
30-d
ay o
bse
rvat
ion
al p
erio
d
Confirmed symptomatic DVT or
PE completing
6 or 12 months
of VKA
~53%
~47%
Randomized, double-blind, placebo-controlled,
event-driven (n=30), superiority study
EINSTEIN Extension Trial ID: NCT00439725

Major outcomes
Primary efficacy outcome* Symptomatic recurrent VTE, i.e. composite of recurrent DVT, non-
fatal PE, or fatal PE, or unexplained death where PE cannot be excluded
Principal safety outcome* Major bleeding, defined as overt bleeding associated with:
A fall in hemoglobin of 2 g/dL or more, or A transfusion of 2 or more units of packed red blood cells or whole blood,
or Occurrence at a critical site: intracranial, intraspinal, intraocular,
pericardial, intra-articular, intramuscular with compartment syndrome, retroperitoneal, or
Death
*Adjudicated by the Central Independent Adjudication Committee

Patient flow
Mean duration of therapy Before study entry: placebo 249 days; rivaroxaban 248 days During study: placebo 190 days; rivaroxaban 190 days
Last patient enrolled Treated for at least 3 months
Safety population
ITT population for primary efficacy
Placebo
595
594
590
602
602
598
Rivaroxaban
Randomized (n=1,197)

Primary efficacy outcome and individual components
Placebo (n=594)
Rivaroxaban (n=602)
Symptomatic recurrent VTE* 42 7.1% 8 1.3%
Recurrent DVT 31
5.2% 5 0.8%
Non-fatal PE 13 2.2% 2 0.3%
Fatal PE 1 0.2% 0
Unexplained death (where PE cannot be excluded)
0 1 0.2%
ITT population; *some patients experienced more than one event

Number of subjects at risk
Rivaroxaban 602 590 583 573 552 503 482 171 138 132 114 92 81
Placebo 594 582 570 554 521 467 444 164 138 133 110 93 85
ITT population
Primary efficacy outcome analysis(time to first event)
10
9
8
7
6
5
4
3
2
1
0
Cu
mu
lati
ve e
ven
t ra
te (
%)
0 30 60 90 120 150 180 210 240 270 300 330 360
Time to event (days)
Rivaroxaban (n=602)
Placebo (n=594)
HR=0.184; p<0.0001
RRR=82%
Number needed to treat to prevent 1 primary efficacy outcome: 15

Placebo (n=590)
Rivaroxaban(n=598)
Major bleeding 0 4 (0.7%)*
Bleeding contributing to death 0 0
Bleeding in a critical site 0 0
Associated with fall in hemoglobin 2 g/dL and/or transfusion
Gastrointestinal bleeding 0 3 (0.5%)
Menorrhagia 0 1 (0.2%)
Principal safety outcome: major bleeding
Number needed to harm: approximately 139
*p=0.11
Safety population

Placebo (n=590)
Rivaroxaban(n=598)
Clinically relevant non-major bleeding 7 (1.2%) 32 (5.4%)*
Urogenital/uterus 2 (0.3%) 12 (2.0%)
Nasal 1 (0.2%) 8 (1.3%)
Rectal/anal 2 (0.3%) 6 (1.0%)
Skin 2 (0.3%) 4 (0.7%)
Ear 0 1 (0.2%)
Gastrointestinal 0 1 (0.2%)
Surgical site 0 1 (0.2%)
Other outcomes
Safety population; some patients experienced more than one event
*p<0.01

Placebo(n=594)
Rivaroxaban(n=602)
Cardiovascular outcomes 4 (0.7%) 4 (0.7%)
STEMI 0 1 (0.2%)
Unstable angina 1 (0.2%) 3 (0.5%)
Transient ischemic attack 1 (0.2%) 0
Ischemic stroke 1 (0.2%) 0
Non-CNS systemic embolism 1 (0.2%) 0
ITT population
Other outcomes
Total mortality 2 (0.3%) 1 (0.2%)
PE 1 (0.2%)
Cancer 1 (0.2%)
Unexplained death including where PE cannot be excluded
0 1 (0.2%)

ALT >3 x ULN(single measurement)
Continued Improved
n=1 n=6
ALT >3 x ULN(3 measurements)
ContinuedImproved
n=1• Allopurinol/statins/ multiple drugs
n=1• Hepatic steatosis, 8-year history of ALT
ALT >3 x ULN(single measurement)
DiscontinuedImproved
n=1• Unexplained
n=3• 1 liver hemangioma/ hepatic steatosis• 2 unexplained
ALT >8 x ULN(2 measurements)
DiscontinuedImproved
0 n=1• Alcohol abuse/ allopurinol/ hepatitis A
Asymptomatic ALT rises, study treatment, clinical history, and concomitant medication
Observation/ frequency
Treatment/ outcome
Placebo Rivaroxaban
Liver failure/ death 0 0
ALT >3x ULN + bilirubin >2x ULN 0 0
Safety population

35
Summary
VTE is a serious and potentially life-threatening condition Current standard of treatment usually requires initial parenteral
LMWH/UFH or fondaparinux followed by an oral VKA For many patients with VTE, secondary prevention with VKA is not
extended beyond 6 months since risk of VTE may be outweighed by risk of major bleeding1
Patients with VTE have a major risk of recurrent VTE that may persist for years2,3
New oral anticoagulants may have the potential to improve benefit-risk and simplify acute VTE treatment and secondary prevention
35
1. Schulman S: N Engl J Med 2003 Oct 30; 349(18):1713-212. Prandoni P, Lensing AWA, Cogo A, et al. Ann Intern Med 1996; 125: 1–7.3. Heit JA, Mohr DN, Silverstein MD, et al. Arch Intern Med 2000; 160: 761–768.