Embed Size (px)
Citation preview
Thrombosis Prophylaxis, Treatment and
Coagulopathy in COVID-19 Patients Clinical Guideline
V1.0
April 2020
Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 2 of 15
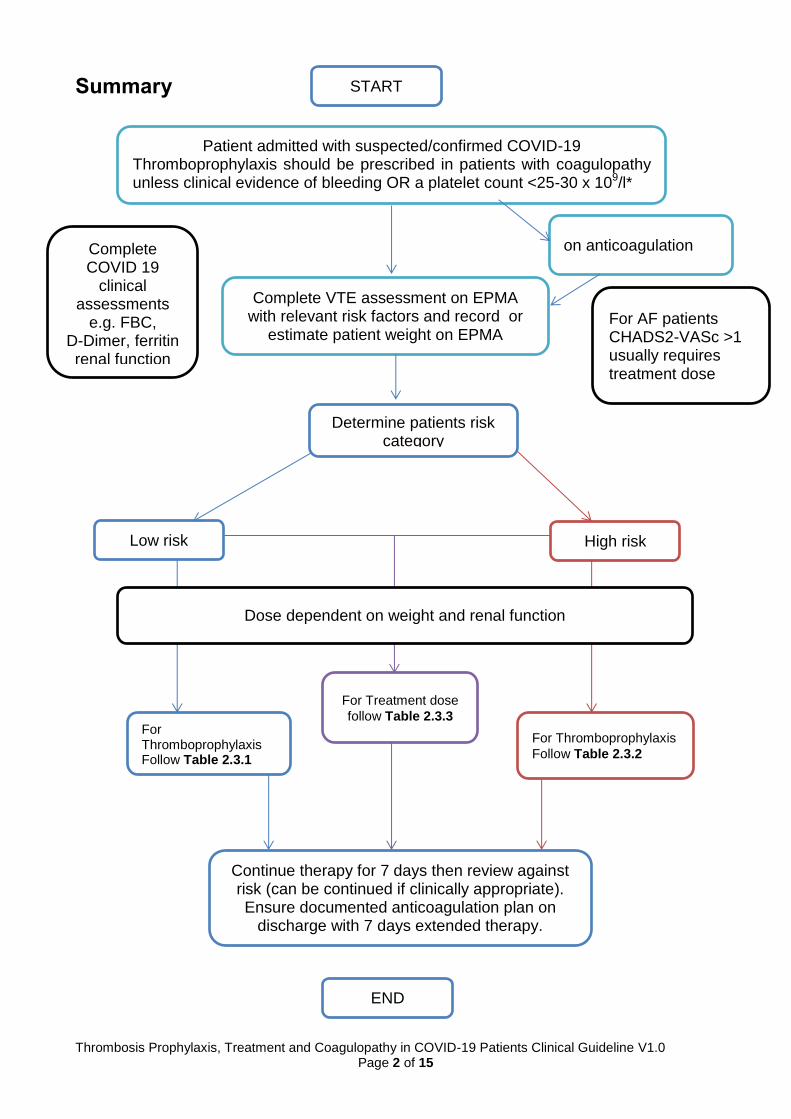
Summary
Patient admitted with suspected/confirmed COVID-19 Thromboprophylaxis should be prescribed in patients with coagulopathy unless clinical evidence of bleeding OR a platelet count <25-30 x 109/l*
Complete VTE assessment on EPMA with relevant risk factors and record or
estimate patient weight on EPMA
Determine patients risk category
Low risk High risk
on anticoagulation
For Thromboprophylaxis Follow Table 2.3.1
For Thromboprophylaxis
Follow Table 2.3.2
For Treatment dose
follow Table 2.3.3
Continue therapy for 7 days then review against risk (can be continued if clinically appropriate). Ensure documented anticoagulation plan on
discharge with 7 days extended therapy.
Complete COVID 19
clinical assessments
e.g. FBC, D-Dimer, ferritin renal function
Dose dependent on weight and renal function
For AF patients CHADS2-VASc >1 usually requires treatment dose
START
END

Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 3 of 15
1. Aim/Purpose of this Guideline
1.1 Despite the use of pharmacological thromboprophylaxis in symptomatic COVID-19 patients there appears to be increased risk of pulmonary embolism (PE) in these patients. There is little evidence to guide altering or intensifying standards of care and limited national or international guidance on how to manage the resultant prothrombotic state, coagulopathy and disseminated intravenous coagulation (DIC) in patients with COVID-19. This guideline has a pragmatic approach to patient management based on the expertise from Consultant Haematologists, Intensivists, Medics, consensus interim guidance from the International Society on Thrombosis and Haemostasis (ISTH) of March 2020 , together with current published evidence, shared anecdotal evidence within the NHS secondary care network.and guidance in use at NHS centres with significant experience of patients with COVID-19
1.2 COVID-19 is an infectious disease caused by a novel coronavirus severe acute
respiratory syndrome coronavirus 2 (SARS-CoV-2). The World Health Organization (WHO) declared COVID-19 a pandemic on 11 March 2020. The clinical presentation is that of a respiratory infection with a symptom severity ranging from a mild common cold-like illness, to a severe viral pneumonia leading to acute respiratory distress syndrome that is potentially fatal. Mild symptoms including fever, fatigue and cough. In severe cases, patients can progress rapidly and develop the acute respiratory distress syndrome, septic shock, metabolic acidosis and coagulopathy including, but not limited to, disseminated intravascular coagulation (DIC). DIC is often evident in advanced COVID-19 cases, and the D-dimer is routinely significantly elevated.
1.3 The majority of patients requiring secondary care input for management of
COVID-19 are immobile therefore have a reduced venous flow with an need for prophylaxis, with a primary acute inflammatory response leading to a hypercoagulable state, and endothelial cell activation/damage possibly due to binding of the virus to ACE2 receptor
1.4 Increased rates of venous and arterial thrombosis are reported, for example
amongst Dutch patients a 27% (95%CI 17-35) incidence of VTE and 3.7% arterial vascular events have been reported, despite use of standard weight based low molecular weight heparin (LMWH) thromboprophylaxis. It is of note than in reports of VTE from Chinese studies, the general incidence of VTE Asian populations is low and so routine VTE prophylaxis is uncommon, as is commonly the case in COVID-19 reports. It has also been commented that chemical thromboprophylaxis is not common for ITU practice outside of the UK.
1.5 Patients with COVID-19 are presenting with complex derangements of normal haemostasis, with pro-coagulant factors such as raised levels of fibrinogen and FVIII, which increase their risk of thrombotic complications. There is evidence for DIC, however unlike that seen in sepsis or massive transfusion bleeding is uncommon. DIC is an acquired syndrome characterised by activation of coagulation pathways, resulting in formation of intravascular thrombi and commonly depletion of platelets and coagulation factors. Thrombi may lead to vascular obstruction/ischaemia and multi-organ failure. A hyperfibrinolyic consumptive DIC has not been reported, with COVID-19 rather fibrinogen is
Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 4 of 15
often raised. DIC is often evident in advanced COVID 19 cases, The D-dimer degradation fragment of cross linked fibrin is routinely significantly elevated from a likely combination including inflammatory pathways, eg macrophage activation and DIC.
1.6 Increased doses of LMWH may be required to combat dramatic elevation in procoagulant factors, and it has been suggested that increased doses appear to dampen the pro-thrombotic effect of the marked inflammatory response to COVID_19. Increased doses of LMWH do not appear to be associated with increased bleeding with precedent from other areas such as bariatric surgery and pregnancy VTE care and thromboprophylaxis,
1.7 The purpose of this guideline is to support clinical decisions for prophylaxis, treatment and management of thrombosis and coagulopathy in COVID 19 patients.
1.8 This version supersedes any previous versions of this document.
1.9 Data Protection Act 2018 (General Data Protection Regulation – GDPR)
Legislation
The Trust has a duty under the DPA18 to ensure that there is a valid legal basis to process personal and sensitive data. The legal basis for processing must be identified and documented before the processing begins. In many cases we may need consent; this must be explicit, informed and documented. We can’t rely on Opt out, it must be Opt in. DPA18 is applicable to all staff; this includes those working as contractors and providers of services.
For more information about your obligations under the DPA18 please see the ‘information use framework policy’, or contact the Information Governance Team [email protected]
2. The Guidance
2.1. Clinical review of patient and determination of risk category in COVID 19 patient This guidance should be used based on a confirmed or clinically significant picture of a COVID 19 positive patient. The patients risk score should be based on a full clinical picture including oxygen requirements, risk of hypoxia, D-Dimer levels, FBC, likelihood of clotting, observations and symptoms. The risk category should not be based on D-Dimer levels alone. Examples of low risk and high risk patients are as follows:
Low Risk Flu like symptoms, no organ support. Mobile patient. No clinical suspicion of VTE.
High Risk Hypoxia (relevant to chest findings) raised D-dimers, raised ferritin but low CRP. No other clinical signs of VTE, denoting likely COVID diagnosis.
Therapeutic Clinical suspicion of, or recent confirmed, VTE
Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 5 of 15
2.2. Electronic Prescribing and Medicines administration
An Electronic Prescribing and Medicines Administration system (JAC) has been introduced to RCHT. A similar system (Carevue) is utilised on critical care. These systems allows for the electronic prescribing of all anticoagulation agents and enables, through reporting, a real-time overview of oral and parenteral anticoagulation prescribed for inpatients as well as being able to collate data on levels of prescribing, correct thromboprophylaxis, and missed doses.
2.2.1. VTE Assessment Completion
To ensure appropriate management of these patients VTE assessments must be completed to signify COVID status either as positive or considered positive due to clinical presentation. The DoH VTE risk assessment tool which is available on JAC (excluding VTE risk assessment in pregnancy) is part of a ‘gate-keeping’ system thus promoting the completion of assessments for all applicable patients. A comparable process occurs daily in critical care with Carevue.
2.2.2. Recording patient weight
To ensure minimal patient contact and enable remote chart reviews the patients weight must be recorded on the electronic chart. The dosing is weight dependent therefore an actual body weight must be obtained and recorded prior to prescribing and administration of therapy. In exceptional circumstances where a patient weight cannot be obtained an estimated weight should be used and recorded under “estimated weight” on JAC.
2.3. Dosing for Thromboprophylaxis in COVID 19 patients
The duration of therapy should be 7 days with the option to continue based on a documented clinical decision for prophylaxis. The thromboprophylaxis should then reviewed and potentially revert back to the standard prophylaxis as appropriate for non-COVID 19 patients (see Thrombosis Prevention Investigation and Management of Anticoagulation Clinical Guideline for further details).
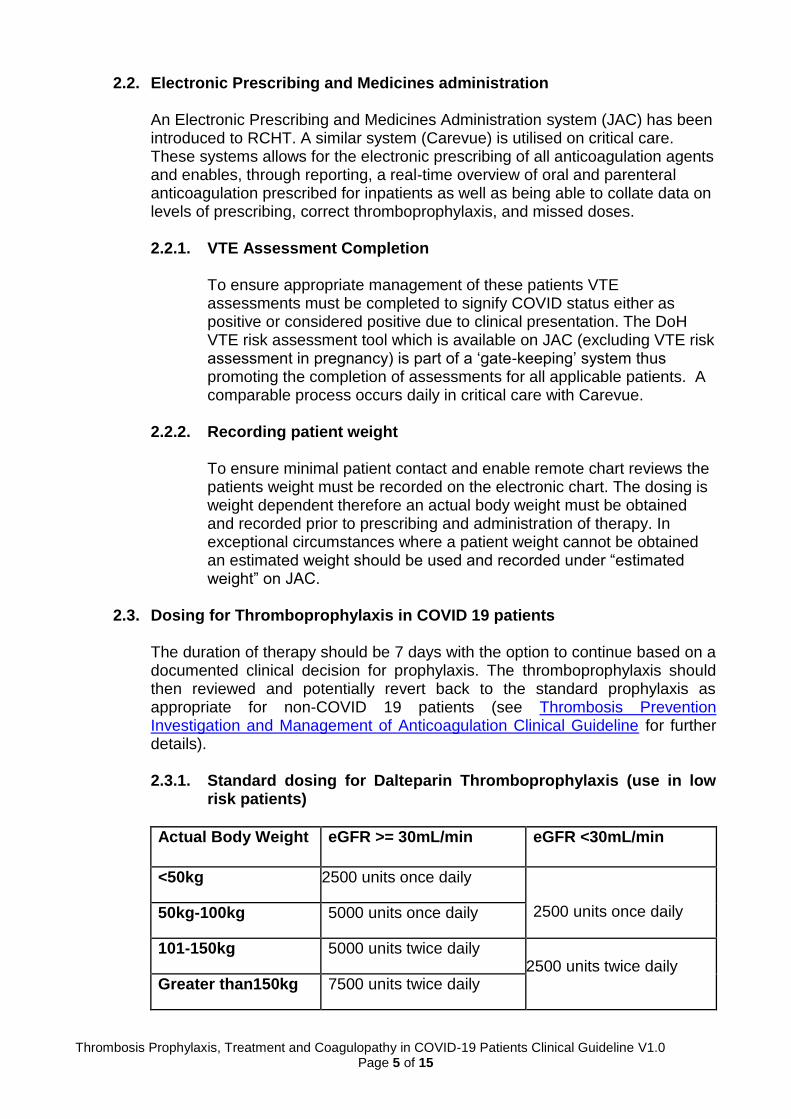
2.3.1. Standard dosing for Dalteparin Thromboprophylaxis (use in low
risk patients)
Actual Body Weight eGFR >= 30mL/min eGFR <30mL/min
<50kg 2500 units once daily
2500 units once daily 50kg-100kg 5000 units once daily
101-150kg 5000 units twice daily 2500 units twice daily
Greater than150kg 7500 units twice daily
Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 6 of 15
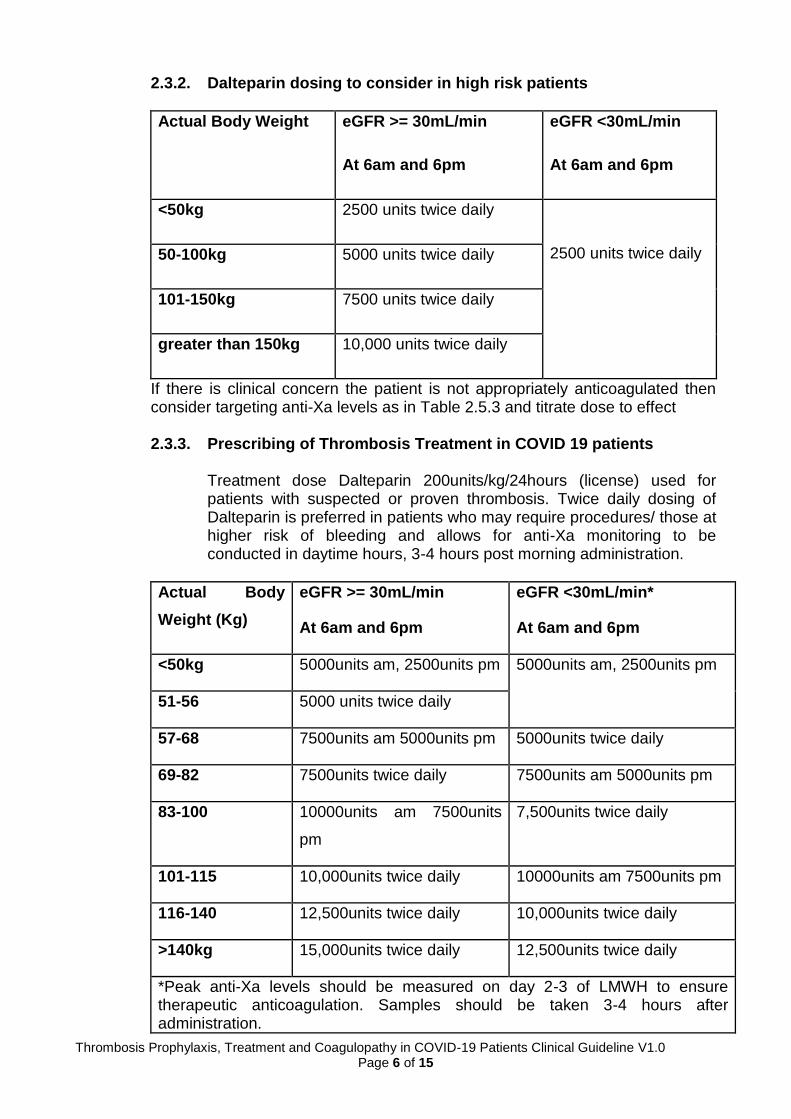
2.3.2. Dalteparin dosing to consider in high risk patients
Actual Body Weight eGFR >= 30mL/min
At 6am and 6pm
eGFR <30mL/min
At 6am and 6pm
<50kg 2500 units twice daily
2500 units twice daily 50-100kg 5000 units twice daily
101-150kg 7500 units twice daily
greater than 150kg 10,000 units twice daily
If there is clinical concern the patient is not appropriately anticoagulated then consider targeting anti-Xa levels as in Table 2.5.3 and titrate dose to effect
2.3.3. Prescribing of Thrombosis Treatment in COVID 19 patients
Treatment dose Dalteparin 200units/kg/24hours (license) used for patients with suspected or proven thrombosis. Twice daily dosing of Dalteparin is preferred in patients who may require procedures/ those at higher risk of bleeding and allows for anti-Xa monitoring to be conducted in daytime hours, 3-4 hours post morning administration.
Actual Body
Weight (Kg)
eGFR >= 30mL/min
At 6am and 6pm
eGFR <30mL/min*
At 6am and 6pm
<50kg 5000units am, 2500units pm 5000units am, 2500units pm
51-56 5000 units twice daily
57-68 7500units am 5000units pm 5000units twice daily
69-82 7500units twice daily 7500units am 5000units pm
83-100 10000units am 7500units
pm
7,500units twice daily
101-115 10,000units twice daily 10000units am 7500units pm
116-140 12,500units twice daily 10,000units twice daily
>140kg 15,000units twice daily 12,500units twice daily
*Peak anti-Xa levels should be measured on day 2-3 of LMWH to ensure therapeutic anticoagulation. Samples should be taken 3-4 hours after administration.
Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 7 of 15
2.3.4. Patients requiring haemofiltration This section relates only to patients who require haemofiltration (not dialysis) and will usually only happen on critical care (or designated critical care areas during the pandemic period). Any patients requiring haemofiltration need treatment dose therapy and targeted anti-Xa monitoring under supervision of a critical care consultant.
2.3.5. Patients undergoing dialysis
These patients should be treated as per standard Trust guidance if further anticoagulation is needed please discuss with the renal team.
2.4. Cautions and Contraindications to Heparin use:
2.4.1. Relative contraindications are untreated haemophilia and other
haemorrhagic disorders, history of heparin-induced thrombocytopenia, peptic ulcer, recent cerebral haemorrhage, severe hypertension, severe liver disease, oesophageal varices, active bleeding, major trauma and recent neurosurgery or eye surgery.
2.4.2. Thrombocytopenia with platelets <25-30 x109/l (note this is lower than
in non-covid 19 patients where the contraindication is <75 x109/l) and in the absence of clinical bleeding may require anticoagulation however this should be a considered clinical decision with consultants and may warrant discussion with Haematology.
2.5. Laboratory Monitoring 2.5.1. Practical Monitoring
All necessary clinical tests are available in the COVID 19 pathology bundle.
A general haematology form is used, detailing the prescribed anticoagulant and the required test e.g. INR, APTT ratio, or anti-Xa level. Tests are performed on a CITRATED sample (sky blue topped bottle), which should be correctly filled to the line (adults 2.7ml) to avoid a dilutional effect of the anticoagulant.
2.5.2. D-Dimer monitoring
D-Dimers are significantly higher in COVID 19 patients. There are links with patient prognosis and D-Dimer levels. Patients with D-Dimers >500ng/ml should be considered high risk. Repeat D-dimer estimation should not be the basis of decision making. A raised D-dimer in isolation does not define the need for screening for VTE
Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 8 of 15
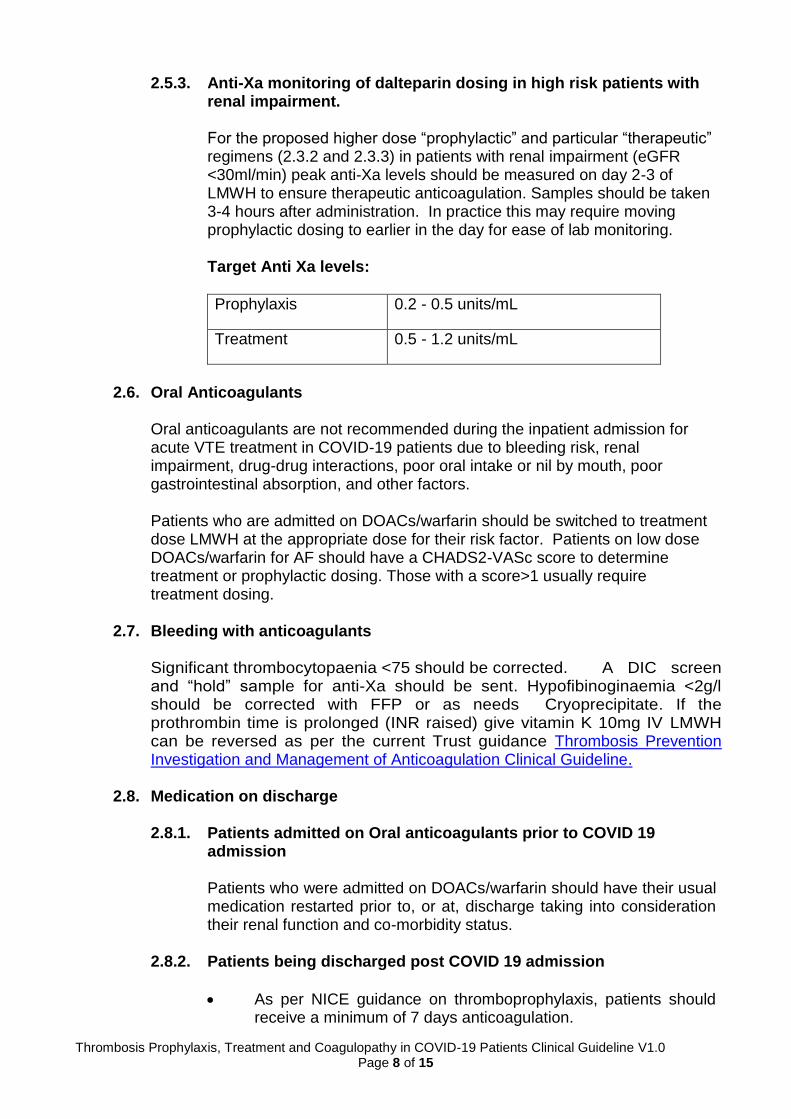
2.5.3. Anti-Xa monitoring of dalteparin dosing in high risk patients with renal impairment. For the proposed higher dose “prophylactic” and particular “therapeutic” regimens (2.3.2 and 2.3.3) in patients with renal impairment (eGFR <30ml/min) peak anti-Xa levels should be measured on day 2-3 of LMWH to ensure therapeutic anticoagulation. Samples should be taken 3-4 hours after administration. In practice this may require moving prophylactic dosing to earlier in the day for ease of lab monitoring.
Target Anti Xa levels:
Prophylaxis 0.2 - 0.5 units/mL
Treatment 0.5 - 1.2 units/mL
2.6. Oral Anticoagulants
Oral anticoagulants are not recommended during the inpatient admission for acute VTE treatment in COVID-19 patients due to bleeding risk, renal impairment, drug-drug interactions, poor oral intake or nil by mouth, poor gastrointestinal absorption, and other factors. Patients who are admitted on DOACs/warfarin should be switched to treatment dose LMWH at the appropriate dose for their risk factor. Patients on low dose DOACs/warfarin for AF should have a CHADS2-VASc score to determine treatment or prophylactic dosing. Those with a score>1 usually require treatment dosing.
2.7. Bleeding with anticoagulants
Significant thrombocytopaenia <75 should be corrected. A DIC screen and “hold” sample for anti-Xa should be sent. Hypofibinoginaemia <2g/l should be corrected with FFP or as needs Cryoprecipitate. If the prothrombin time is prolonged (INR raised) give vitamin K 10mg IV LMWH can be reversed as per the current Trust guidance Thrombosis Prevention Investigation and Management of Anticoagulation Clinical Guideline.
2.8. Medication on discharge
2.8.1. Patients admitted on Oral anticoagulants prior to COVID 19
admission Patients who were admitted on DOACs/warfarin should have their usual medication restarted prior to, or at, discharge taking into consideration their renal function and co-morbidity status.
2.8.2. Patients being discharged post COVID 19 admission
As per NICE guidance on thromboprophylaxis, patients should receive a minimum of 7 days anticoagulation.
Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 9 of 15
Patients should receive 7 days of anticoagulation on discharge with the option to extend if deemed clinically appropriate at the point of discharge.
If a prolonged period of post-discharge anticoagulation is considered this must be clearly documented in the discharge plan with rationale. This decision should be made by the attending clinical team.
2.9. References
https://www.gov.uk/government/publications/wuhan-novel-coronavirus-initial-investigation-of-possible-cases
https://bestpractice.bmj.com/topics/en-gb/3000168
https://www.livescience.com/coronavirus-pandemic-who.html
Bush S et al. Once- versus twice-daily enoxaparin for venous thromboembolism prophylaxis in high-risk trauma patients. J Intensive Care Med (2011); 26 (2): 111-5. doi: 10.1177/ 0885066610384462
Cohen A et al. Extended Thromboprophylaxis with Betrixaban in Acutely Ill Medical Patients (APEX trial) N Engl J Med. 2016 Aug 11;375 (6):534-44. doi: 10.1056/NEJMoa1601747
Hunt BJ. Bleeding and coagulopathies in critical care. N Engl J Med
(2014) 27; 370(9): 847-59. doi: 10.1056/NEJMra1208626
Hunt BJ, Retter DRA and McClintock C. Practical guidance for the prevention of thrombosis and management of coagulopathy and disseminated intravascular coagulation of patients infected with COVID-19. International Society on Thrombosis and Haemostasis (2020)
Kramme K, Sarraf P, Munene G. Prophylactic Enoxaparin Adjusted by Anti-Factor Xa Peak Levels Compared with Recommended Thromboprophylaxis and Rates of Clinically Evident Venous Thromboembolism in Surgical Oncology Patients. J Am Coll Surg (2020); 230(3): 314-321. doi: 10.1016/j.jamcollsurg.2019.11.012
Levi M, Toh CH, Thachil J, Watson HG. Guidelines for the diagnosis and management of disseminated intravascular coagulation. Br J Haematol (2009); 145 (1): 24-33
Minze MG. Low-Molecular-Weight Heparin Prophylaxis Dosing: Is Weight an Issue? Journal of Pharmacy Technology (2016); 32(2): 75–80 doi: 10.1177/8755122515617200
Song JQ et al. Low molecular weight heparin once versus twice a day for thromboprophylaxis following esophagectomy: a randomised, double-blind and placebo-controlled trial. J Thorac Dis. (2015); 7 (7): 1158-64. doi: 10.3978/j.issn.2072-1439.2015.06.15
Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 10 of 15
Tang N, Li D, Wang X, Sun Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J Thromb Haemost (2020); 10.1111/jth.14768
https://www.gmjournal.co.uk/study-identifies-covid-19-risk-factors-associated-with-death
https://emcrit.org/ibcc/COVID19/
Bikdeli B, Madhavan MV, Jimenez D, Chuich T, Dreyfus I, Driggin E, Nigoghossian CD, Ageno W, Madjid M, Guo Y, Tang LV, Hu Y, Giri J, Cushman M, Quéré I, Dimakakos EP, Gibson CM, Lippi G, Favaloro EJ, Fareed J, Caprini JA, Tafur AJ, Burton JR, Francese DP, WangEY, Falanga A, McLintock C, Hunt BJ, Spyropoulos AC, Barnes GD, Eikelboom JW, Weinberg I,Schulman S, Carrier M, Piazza G, Beckman JA, Steg PG, Stone GW, Rosenkranz S, Goldhaber SZ, Parikh SA, Monreal M, Krumholz HM, Konstantinides SV, Weitz JI, Lip GYH, COVID-19 and Thromboticor Thromboembolic Disease: Implications for Prevention, Antithrombotic Therapy, and Follow-up,Journal of the American College of Cardiology (2020), doi: https://doi.org/10.1016/j.jacc.2020.04.031.
ISTH interim guidance on recognition and management of coagulopathy in
COVID-19. https://onlinelibrary.wiley.com/doi/epdf/10.1111/jth.14810
Klok FA, Kruip MJHA et al. Incidence of thrombotic complications in
critically ill ICU patients with COVID-19. Thrombosis Research
https://doi.org/10.1016/j.thromres.2020.04.013
3. Monitoring compliance and effectiveness
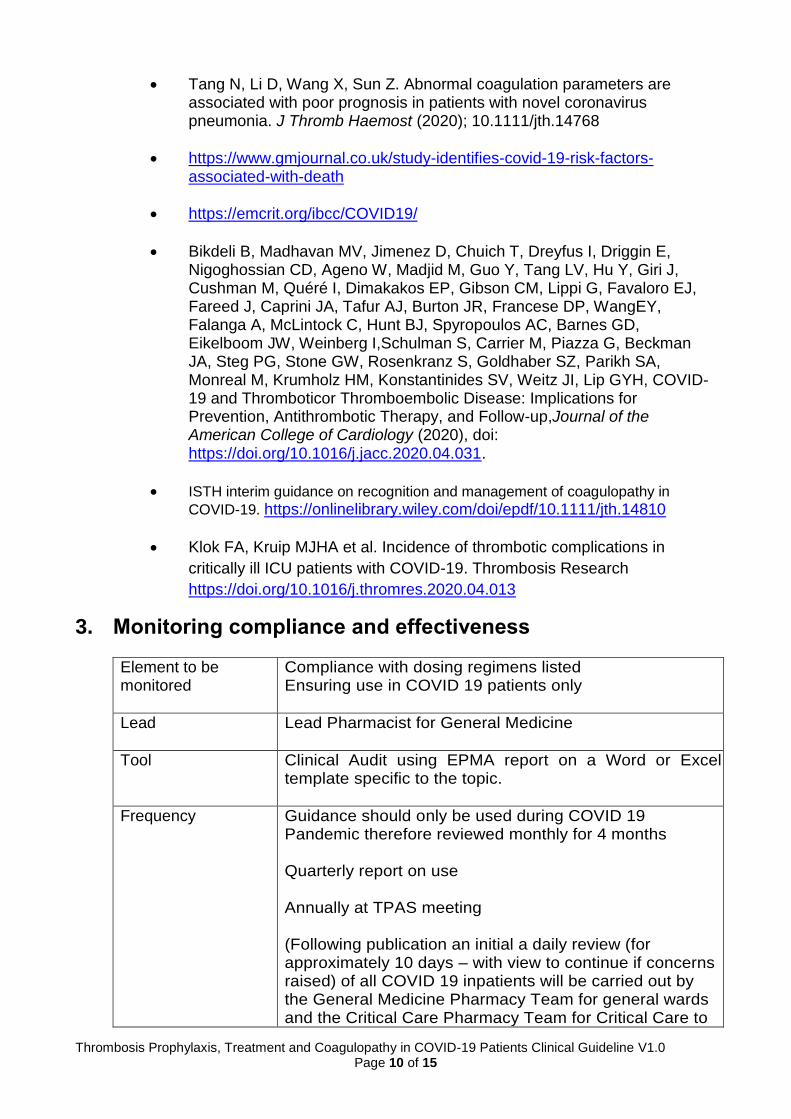
Element to be monitored
Compliance with dosing regimens listed Ensuring use in COVID 19 patients only
Lead Lead Pharmacist for General Medicine
Tool Clinical Audit using EPMA report on a Word or Excel template specific to the topic.
Frequency Guidance should only be used during COVID 19 Pandemic therefore reviewed monthly for 4 months Quarterly report on use Annually at TPAS meeting (Following publication an initial a daily review (for approximately 10 days – with view to continue if concerns raised) of all COVID 19 inpatients will be carried out by the General Medicine Pharmacy Team for general wards and the Critical Care Pharmacy Team for Critical Care to
Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 11 of 15
highlight any unexpected risks or complications) - Daily report generated by EPMA team highlighting
all patients with COVID 19 (positive or awaiting results) on maxims and prescribed anticoagulation.
Reporting arrangements
TPAS, MPC Relevant clinical governance and feedback meeting minutes. Consider stating this responsibility in committee terms of reference
Acting on recommendations and Lead(s)
TPAS will lead on amendments and changes TPAS is an annual group who will update changes on an annual basis Consider stating this responsibility in committee terms of reference
Change in practice and lessons to be shared
Required changes to practice will be identified and actioned within 3 months. A lead member of the team will be identified to take each change forward where appropriate. Lessons will be shared with all the relevant stakeholders
4. Equality and Diversity
4.1 This document complies with the Royal Cornwall Hospitals NHS Trust service Equality and Diversity statement which can be found in the 'Equality, Inclusion & Human Rights Policy' or the Equality and Diversity website.
4.2. Equality Impact Assessment The Initial Equality Impact Assessment Screening Form is at Appendix 2.

Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 12 of 15
Appendix 1. Governance Information
Document Title Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0
Date Issued/Approved: 24th April 2020
Date Valid From: April 2020
Date Valid To: April 2021
Directorate / Department responsible (author/owner):
Pollyanna Bastian Lead Pharmacist for General Medicine Lorraine Moore Lead Pharmacist for Critical Care and Anaesthetics
Contact details: 01872 252598
Brief summary of contents COVID 19 Thrombosis, Thromboprophylaxis management in adult patients including monitoring
Suggested Keywords: COVID 19 Thrombosis, Thromboprophylaxis management, anticoagulation, adult
Target Audience RCHT CFT KCCG
Executive Director responsible for Policy:
Medical Director
Date revised: 19th April 2020
This document replaces (exact title of previous version):
New document
Approval route (names of committees)/consultation:
Medicines Management Committee
Care Group General Manager confirming approval processes
Richard Andrzejuk
Name and Post Title of additional signatories
Not Required
Name and Signature of Care Group/Directorate Governance Lead confirming approval by specialty and care group management meetings
{Original Copy Signed}
Name: Kevin Wright
Signature of Executive Director giving approval
{Original Copy Signed}
Publication Location (refer to Policy on Policies – Approvals and Ratification):
Internet & Intranet Intranet Only
Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 13 of 15
Document Library Folder/Sub Folder Clinical / Pharmacy
Links to key external standards None required
Related Documents:
RCHT Thrombosis Prevention Investigation and Management of Anticoagulation Clinical Guideline
Training Need Identified? No
Version Control Table
Date Version
No Summary of Changes
Changes Made by (Name and Job Title)
19/04/2020 V1.0
Initial version
Pollyanna Bastian Lead Pharmacist for General Medicine Lorraine Moore Lead Pharmacist for Critical Care and Anaesthetics
All or part of this document can be released under the Freedom of Information
Act 2000
This document is to be retained for 10 years from the date of expiry. This document is only valid on the day of printing
Controlled Document
This document has been created following the Royal Cornwall Hospitals NHS Trust Policy for the Development and Management of Knowledge, Procedural and Web
Documents (The Policy on Policies). It should not be altered in any way without the express permission of the author or their Line Manager.
Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 14 of 15
Appendix 2. Initial Equality Impact Assessment Form
Are there concerns that the policy could have differential impact on:
Equality Strands: Yes No Unsure Rationale for Assessment / Existing Evidence
Age X Only suitable for Adult patients
Name of the strategy / policy /proposal / service function to be assessed Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients
Clinical Guideline V1.0
Directorate and service area: Pharmacy
New or existing document: New
Name of individual completing assessment: Pollyanna Bastian
Telephone: 01872 25 2598
1. Policy Aim* Who is the strategy / policy / proposal / service function aimed at?
Clinical staff within RCHT managing COVID 19 patients
2. Policy Objectives*
To support clinical management and prescribing of anticoagulation in COVID 19 patients
3. Policy – intended Outcomes*
To ensure safe and appropriate anticoagulation management of COVID 19 patients
4. *How will you measure the outcome?
Auditing compliance with guidance
5. Who is intended to benefit from the policy?
RCHT clinical staff, patient safety
6a Who did you consult with b). Please identify the groups who have been consulted about this procedure.
Workforce Patients Local groups
External organisations
Other
X X
Critical Care Consultants, Medical Consultants, Haematology Consultant, Chelsea and Westminster Hospital, University Hospital Sheffield. Guys & St Thomas guidance, UKCPA clinical discussion forums
What was the outcome of the consultation?
Formulation of the guidance
7. The Impact Please complete the following table. If you are unsure/don’t know if there is a negative impact you need to repeat the consultation step.

Thrombosis Prophylaxis, Treatment and Coagulopathy in COVID-19 Patients Clinical Guideline V1.0 Page 15 of 15
Sex (male, female, trans-gender / gender reassignment)
X
Race / Ethnic communities /groups
X
Disability - Learning disability, physical impairment, sensory impairment, mental health conditions and some long term health conditions.
X
Religion / other beliefs
X Need to consider LMWH contain porcine derived products and provide alternative for belief purpose as per current Trust policy
Marriage and Civil partnership
X
Pregnancy and maternity
X Policy does not cover maternity patients
Sexual Orientation, Bisexual, Gay, heterosexual, Lesbian
X
You will need to continue to a full Equality Impact Assessment if the following have been highlighted:
You have ticked “Yes” in any column above and
No consultation or evidence of there being consultation- this excludes any policies which have been identified as not requiring consultation. or
Major this relates to service redesign or development
8. Please indicate if a full equality analysis is recommended. Yes No X
9. If you are not recommending a Full Impact assessment please explain why.
Not indicated
Date of completion and submission
19th April 2020 Members approving screening assessment
Policy Review Group (PRG APPROVED
This EIA will not be uploaded to the Trust website without the approval of the Policy Review Group. A summary of the results will be published on the Trust’s web site.









![Praziquantel Treatment is Recommended: Active Schistosoma ... · ulcers, gastric ulcers and gastritis [3]. The ideal treatment offered for patients diagnosed with oesophageal varices](https://img.pdfslide.net/doc/110x75/5d0b42f388c993f87c8b6090/praziquantel-treatment-is-recommended-active-schistosoma-ulcers-gastric.jpg)